Submitted:
18 May 2023
Posted:
19 May 2023
You are already at the latest version
Abstract
Autism spectrum disorder (ASD) is a neurodevelopmental disorder with high heterogeneity and has a prevalence of 0.7% to 3.2% in children. Gut microbiota are a collection of microorganisms that inhabit in human guts, which can produce various metabolites that affect the homeostasis and functions of nervous and endocrine systems. There are many studies on the relationship between various gut microbiota and ASD, but the alteration pattern of microbial profiles in ASD children is not conclusive. In order to more robustly describe the deregulations of gut microbiota compositions in ASD, a meta-analysis was performed. The related investigations from PubMed, Embase and Web of Science were collected and manually reviewed. By procedure, 26 eligible studies until 2023, with a total of 1021 ASD and 951 typically developed children and adolescents, were included for the meta-analysis. RevMan5.4 was used to assess the overall effect of 8 microbes at the phylum level and 19 microbes at the genus level. Results demonstrated relatively up-regulated abundance of Bacteroidetes, Verrucomicrobia, Bacteroides, Clostridium, Dorea and Sutterella, and down-regulated abundance of Proteobacteria, Bifidobacterium, Coprococcus, and Akkermansia in ASD children, indicating partly agreement in the ASD-associated microbes, albeit the heterogeneity of ASD.
Keywords:
Autism spectrum disorder
; microbiota
; meta-analysis
1. Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by social communication and interaction deficits, as well as restricted and repetitive behaviors, interests, or activities, which has high clinical and etiologic heterogeneity[1]. In recent years, the prevalence of ASD has significantly increased worldwide, possibly due to the joint effects of environmental, genetic and epigenetic factors, as well as improvements in diagnostic criteria, better detection methods and increased awareness[2]. According to the latest data from the Centers for Disease Control and Prevention in 2023, the prevalence of ASD among 8-year-old children in the United States is as high as 1 in 36, about four times that in 2000, and the male-to-female ratio is about 4:1[3]. Studies reports a prevalence of ASD ranging from 0.7% to 3.2%, indicating a public health issue[4,5,6,7]. In terms of GI dysfunction, including constipation, diarrhea, abdominal pain, bloating, gastroesophageal reflux, and intestinal inflammation, the comorbidity rate reaches 46.8% (4.2%-96.8%), which is about 3 times higher than that of typically developed (TD) children[8,9]. Research has reported that children with frequent diarrhea and constipation scored higher on the Autism Behavior Checklist (ABC), representing a greater likelihood of irritable, socially withdrawn, and stereotypical, and hyperactive behaviors[9].
The gut microbiome is the collection of microorganisms inhabiting the intestine, numbering ~1014 or more, which is approximately 10 times the total number of cells in the body[10]. It has been found that children with ASD have widespread gut microbiota dysbiosis and that metabolites associated with energy metabolism, gut microbiota metabolism and oxidative stress differ significantly from TD[11,12,13]. Studies have also found a positive correlation between gastrointestinal symptoms and the repetitive/stereotyped behaviors and behavioral problems in children with ASD, indicating that gastrointestinal problems may be related to the nervous system in some way[14].
As the microbiome-gut-brain axis theory develops, many studies have shown that the gut microbiota might play an important role in the bidirectional regulation of the brain-gut axis through the nervous, immune, and endocrine systems[15,16,17]. Animal research has discovered that the provision of Lactobacillus farciminis and Lactobacillus salivarius, two types of probiotic bacteria, resulted in regulation of their disrupted gut microbiota in ASD model mice. Additionally, disrupted cortical hormone secrection and neural development as well as abnormal stress behavior were significantly restored, suggesting the association between the microbiota and ASD[18]. Some clinical trials have also demonstrated that ASD patients have alterations in both the structure and the abundance of gut microbiota compared to TD subjects[19,20,21]. However, the reported patterns of microbial alterations vary greatly among different studies and the data from meta-analyses are outdated. To better understand the role of microbiota in the development of ASD, we conducted a review and meta-analysis to identify differences in gut microbiota profiles between ASD and TD as well as to provide a theoretical basis for targeted interventions and treatments for ASD through gut microbiota.
2. Methods
2.1. Search Strategy and Selection Criteria
The review and meta-analysis were carried out following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines[22]. We performed a systematic study search of PubMed, Embase and Web of Science as far as April 2023. The search strategy for the PubMed was as follows:
#1 “autism spectrum disorder”[MeSH Terms] OR “autistic disorder”[MeSH Terms]
#2 “ASD”[Title/Abstract] OR “Autism”[Title/Abstract] OR “Autistic”[Title/Abstract] OR “PDD”[Title/Abstract] OR “Asperger Syndrome” [Title/Abstract]
#3 #1 OR #2
#4 “microbiota"[MeSH Terms] OR “Microbiome”[Title/Abstract] OR “Microflora” [Title/Abstract] OR “Fecal microbiota”[Title/Abstract] OR “Gastrointestinal”[Title/Abstract] OR “Intestinal flora”[Title/Abstract] OR “Mycobiome”[Title/Abstract]
#5 #3 AND #4
No restrictions were applied in terms of language or year of publication. Moreover, the reference lists of original records and relevant reviews were also checked for additional studies. The titles and abstracts of records were screened to filter irrelevant papers and full text were checked to identify studies met the eligibility criteria.
The inclusion criteria were: (1) design: case-control studies or observed studies; (2) subjects: the case group consisted of individuals diagnosed with ASD based on ICD, DSM, or clinical physician assessment, and the control group consisted of healthy individuals without psychiatric disorders and with normal cognitive function, both groups were under the age of 18; (3) content: the composition of the gut microbiota of the study population, including the mean and standard deviation (SD) of microbial relative abundance. The exclusion criteria were: (1) meta-analyses, reviews, conferences, case reports, research protocols, or animal studies; (2) subjects with other neurological disorders or taking other medications; (3) inconsistent with study content or small sample size (n<5); (4) unavailable full text or missing data; (5) duplicate studies.
2.2. Data Extraction and Study Quality Assessment
The following information was extracted from the eligible studies: (1) general items: title, first author, year of publication and country; (2) subjects: sample size, age, sex, gastrointestinal symptoms and diet, and diagnostic criteria for the ASD group; (3) microbiota: detection methods, and relative abundance (mean and SD) at phylum and genus level.
The Newcastle–Ottawa Scale (NOS) was used for study quality assessment, and articles were classified into high (7~9), medium (4~6), and low (0~3) quality, based on the total score of three dimensions: study-participant selection (0~4), the comparability of study participants (0~2) and the exposure or outcome of studies (0~3).
2.3. Statistical Analysis
For each bacteria phylum and genus, the random-effects model and the inverse-variance method were used to calculate the overall effect size and 95% confidence interval (95% CI) through mean ± SD of children and adolescents with and without ASD, using Review Manager 5.4 software. The standard mean difference (SMD) measure of effect was accessed to compare the differences in microbiota between two groups of children. SMD > 0 indicated that the relative abundance of the bacteria was significantly higher in ASD group compared to TD group, while SMD < 0 indicated that ASD group had a lower bacterial relative abundance. Heterogeneity was measured using both Cochran's Q test and the I2 statistic, whereby I2 represented the proportion of heterogeneity present, with I2 ≥ 50% indicative of a more pronounced level of heterogeneity. In order to test the reliability of the findings, sensitivity analyses were performed by excluding one individual study at a time. All statistical analyses were considered significant at p < 0.05.
3. Results
3.1. Characteristics of the Included Studies
Figure 1 shows the PRISMA flow diagram of the identification of the included studies. A total of 1922 records were retrieved through three databases: 620 records in PubMed, 873 records in Embase, and 429 records in Web of Science. The title and abstract of 1135 articles were screened after discarding the duplicated studies. Among these publications, 74 studies were selected for a further review of the full texts while 1061 publications were excluded for the following reasons: not access the association of the study, reviews and case reports, studies on animals, age of participants exceeding 18 years old, meta-analysis and others. Finally, 26 eligible records of a total of 2152 participants were included in this meta-analysis.
The summary characteristics of the eligible studies were shown in Table 1. In total, this meta-analysis integrated gut microbiota results from 26 studies of 1021 ASD and 951 age-matched TD children and adolescents aged 2-17 years old. Generally, these articles were published between 2010 and 2023 with the sample size ranging from 6 to 143. The majority of the investigations were conducted in China[21,23,24,25,26,27,28,29,30,31], the United States[32,33,34,35,36,37], Australia[38,39,40] and Italy[20,41,42], with one article each from India[43], Japan[44] and Spain[45]. About half of the literatures reported the gastrointestinal condition of the subjects, and the results showed that the frequency and severity of gastrointestinal dysfunction in children and adolescents with ASD were higher than those of TD to varying degrees. In terms of microbial detection, all the studies provided microbial variation data at the phylum or genus level, while only a small portion of the studies reported microbial variation at the family or species level[29,31,41], therefore, the meta-analysis was performed at the levels of phylum and genus. In regard to the quality assessment of the studies, only 4 records were of moderate quality[26,35,37,38], and the rest 22 were of high quality according to NOS.
3.2. Decreased Alpha Diversity in ASD
The Shannon index and Chao 1 index are alpha diversity indicators used to measure diversity and richness of species, respectively. In the meta-analysis of Shannon index, 5 studies were included, but there was no significant difference between ASD and TD (p = 0.82). While 4 studies were included in the meta-analysis of Chao 1 index, leading to a significant reduction in ASD, indicating a decreased richness of species in ASD.
In Shannon's meta-analysis, 5 articles were included, but there was no difference between two groups of children. However, in Chao 1's meta-analysis, 4 articles were included, and the results showed a significant reduction in Chao 1 in ASD (SMD = -0.51; 95% CI: -0.76, -0.27; p < 0.001) with a low heterogeneity (I2 = 27%), indicating a decrease in species abundance in ASD.
3.3. Microbes Upregulated in ASD
Table 2 shows the results of meta-analysis of the microbiota compositions in children and adolescents with and without ASD at the phylum and genus levels. The genera, belonging to their respective phyla, were grouped together and displayed in italics, while the phyla were displayed in boldface. Totally, we compared the differences of 8 phyla and 19 genera between two groups of subjects.
The results demonstrated that Bacteroidetes, Verrucomicrobia, Bacteroides, Clostridium, Dorea and Sutterella were upregulated in ASD. Twelve articles were included in the meta-analysis of Bacteroidetes, and 7 articles were included in the meta-analysis of Verrucomicrobia at the phylum level, arriving at the following results: ASD had 0.42% higher relative abundance of Bacteroidetes (95% CI: 0.02, 0.82; p = 0.04) (Figure 2) and 0.25% higher relative abundance of Verrucomicrobia (95% CI: 0.01, 0.49) (Figure 3) than those in TD, which were similar to results of the previous meta-analysis[47].
At the genus level, the relative abundance of Bacteroides was evaluated on the basis of 13 clinical trials and was confirmed upregulated in children and adolescents with ASD (SMD = 0.47; 95% CI: 0.01, 0.93). The effect size was moderate and significant (Z = 2.01, p = 0.04) (Figure 4). Similarly, the increased relative abundance of Clostridium (SMD = 1.01; 95% CI: 0.15, 1.87; p = 0.02), Dorea (SMD = 0.5; 95% CI: 0.31, 0.70; p < 0.001) and Sutterella (SMD = 1.04; 95% CI: 0.04, 2.05; p = 0.04) were also observed in ASD. However, the heterogeneity among studies was very high in the meta-analysis of Bacteroides, Clostridium and Sutterella (91%, 85% and 95%).
3.4. Microbes Downregulated in ASD
The random effect meta-analysis of Proteobacteria was conducted on the basis of 9 studies supporting the down-regulation of Proteobacteria in ASD (SMD = -0.31; 95% CI: -0.59, -0.04; p = 0.03) (Figure 5).
From the 13 eligible records, we found that relative abundance of Bifidobacterium was significantly decreased in ASD compared to TD children and adolescents (SMD = -0.85; 95% CI: 0.01, 0.93). The effect size was moderate and significant (Z = 3.27, p = 0.001) (Figure 6) In the meta-analysis of Coprococcus involving 7 studies (SMD = -0.43; 95% CI: 0.01, 0.93; p = 0.02) and Akkermansia involving 4 articles (SMD = -0.41; 95% CI: -0.77, -0.05; p = 0.02), the results demonstrated that the level of both bacteria significantly decreased in ASD compared to TD.
3.5. Microbes with No Difference between ASD and TD
The random-effect meta-analysis of Actinobacteria, Cyanobacteria, Firmicutes, Fusobacteria and Tenericutes at the phylum level showed no significantly difference between ASD and TD. The overall effect ranged from 0.38 in Cyanobacteria to 1.48 Tenericutes, and the heterogeneity amongthe studies ranged between 71% to 94%. Although the evidence was insufficient to observe a statistically significant difference between children and adolescents with and without ASD, the disparity in microbe relative abundance suggested that ASD had a lower level of Tenericutes compared to TD.
Meanwhile, there was not enough sufficient evidence to indicate significant differences in 12 microbes at the genus level between ASD and healthy controls. The overall effect ranged from 0.04 in Prevotella to 1.37 Bilophila, and the heterogeneity between studies ranged between 66% to 85%. Regardless, the relative abundance of Collinsella (SMD = 0.23; 95% CI: 0.14, 0.60) and Lactobacillus (SMD = 0.27; 95% CI: -0.36, 0.89) was higher in ASD, and relative abundance of Streptococcus (SMD = -0.47; 95% CI: -1.04, 0.10) and Bilophila (SMD = -0.36; 95% CI: -0.87, 0.15) was lower in ASD, respectively.
4. Discussion
This study updated the other published meta-analysis of gut microbiome composition in ASD[47,48] with substantially increased number of eligible studies. A total of 26 articles were included, of which 9 literatures were performed in the past three years. As far as we know, this has been the meta-analysis with the most records included of ASD gut microbiota. In fact, our study consisted of 2152 subjects, including 1201 ASD and 951 TD children and adolescents, and analyzed 8 microbes at the phylum level and 19 microbes at the genus level.
In accordance with our results, there was a disruption of various gut microbes in individuals with ASD. Specifically, in the 8 microbes at the phylum level analyzed in the meta-analysis, Firmicutes, Bacteroidetes, Proteobacteria and Actinobacteria had the highest relative abundance in both ASD and TD. Among them, the relative abundance of Firmicutes was mostly reported to be over 40%, and in most studies, the relative abundance of Bacteroidetes was over 30%. In contrast, Cyanobacteria, Fusobacteria, Verrucomicrobia, and Tenericutes had relatively low levels, especially Tenericutes, whose relative abundance was less than 0.55%. For Bacteroidetes, the overall effect and most studies showed its upregulation in ASD, while 3 studies found its downregulation in ASD. The same situation could also be observed for Verrucomicrobia. For Proteobacteria, the overall effect and most studies indicated a higher level in ASD, while the records of Ding et al. [29] and Ma et al. [21] reported its upregulation in ASD. As for Firmicutes, which had the highest relative abundance, we did not find significant differences between the two groups. At the genus level, increased relative abundance of Bacteroides, Clostridium, Dorea and Sutterella, and decreased relative abundance of Bifidobacterium, Coprococcus and Akkermansia were observed in ASD children and adolescents.
It is noteworthy that harmful bacteria, such as Clostridium and Sutterella, were significantly upregulated in ASD, while beneficial bacteria, such as Bifidobacterium and Akkermansia, were significantly downregulated. Clostridium can produce neurotoxic substances such as cresol and propionic acid[27], which may block the transmission of neurotransmitters and damage neuron activities after entering the brain through the blood-brain barrier, thereby increasing abnormal behavior in ASD[49]. Propionic acid could also be produced by Sutterella and studies have reported a positive correlation between Sutterella and gut inflammation and diarrhea[50]. Moreover, IgA protease would be over-secreted with increased Sutterella, leading to a decrease of IgA in the mucosa and disruption of the intestinal antibacterial immune response function[51].
Bifidobacterium plays an important role in inhibiting the growth of harmful bacteria and promoting the release of anti-inflammatory cytokines, thereby promoting intestinal homeostasis and improving gastrointestinal function[10]. Additionally, Bifidobacterium can also improve the host's memory function by promoting the expression of brain-derived neurotrophic factors and N-methyl-D-aspartate receptors[10]. A study has found that Bifidobacterium longum intervention could reduce abnormal behavior and gastrointestinal symptoms in children with ASD[52]. Akkermansia has anti-inflammatory effects[53]. Accompanied by the downregulated of Akkermansia, toxins in the intestines are more easily able to invade the human body, with thinning of the mucosal layer and weakening intestinal barrier function[54]. Additionally, Akkermansia produces more than 60 enzymes that can degrade oligosaccharides, providing energy for beneficial bacteria[54].
Currently, characteristics and alterations of gut microbiota in ASD individuals is gradually being discovered, revealing the potential correlation between ASD pathogenesis and the dysbiosis of gut microbiota. Nonetheless, it is unneglectable that inconsistency among conclusions still remains across studies. This may due to genetic and environmental confounders such as ethnics, habitual diet, daily lifestyle, etc. One study has found significant similarities in gut microbiome compositions of genetically unrelated healthy individuals who share a household, indicating that there has been a tight correlation between gut microbiome composition and habitual diet, whereas the host genetics play a minor role[55]. Furthermore, another study has found that individuals with greater healthy food intake have higher abundance of beneficial gut microbiota[56]. This also suggests that the disrupted microbiome of ASD individuals may be reformed not only through supplementing probiotics or fecal microbiota transplantation but also by altering the dietary structure. Further research is needed to investigate personalized intervention strategies, and by facilitating gut microbiotal-related treatments may ultimately improve the quality of life of ASD individuals.
Author Contributions
Formal Analysis, Z.T.; Investigation, Z.T., Z.X.; Resources, Z.T., Z.X.; Data Curation, Z.T., Writing----Original Draft Preparation, Z.T.; Writing----Review & Editing, J.W., Y.Z., Z.T.; Z.X.; Supervision, J.W.; Y.Z. Project Administration, Z.T. All authors have read and agreed to the published version of the manuscript.
Acknowledgement
This study is supported by the grants from National Natural Science Foundation of China (82171169 to WANG Juan).
Conflicts of Interest
The authors declared no conflict of interest.
References
- American Psychiatric Association. The Diagnostic and statistical manual of mental disorders, 5th ed.; American Psychiatric Publishing Inc: Washington, DC, USA, 2013. [Google Scholar]
- Salari, N.; Rasoulpoor, S.; Rasoulpoor, S.; Shohaimi, S.; Jafarpour, S.; Abdoli, N.; Khaledi-Paveh, B.; Mohammadi, M. The global prevalence of autism spectrum disorder: A comprehensive systematic review and meta-analysis. Ital J Pediatr 2022, 48, 112. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Data & Statistics on Autism Spectrum Disorder 2022. Available online: https://www.cdc.gov/ncbddd/autism/data.html.
- Baron-Cohen, S.; Scott, F.J.; Allison, C.; Williams, J.; Bolton, P.; Matthews, F.E.; Brayne, C. Prevalence of autism-spectrum conditions: UK school-based population study. Br J Psychiatry 2009, 194, 500–509. [Google Scholar] [CrossRef] [PubMed]
- BLL, Y.S.K.; Koh, Y.-J.; Fombonne, E.; Laska, E.; Lim, E.-C.; Cheon, K.-A.; Kim, S.-J.; Kim, Y.-K.; Lee, H.; Song, D.-H.; Grinker, R.R. Prevalence of autism spectrum disorders in a total population sample. Am J Psychiatry 2011, 168, 904–912. [Google Scholar]
- Saito, M.; Hirota, T.; Sakamoto, Y.; Adachi, M.; Takahashi, M.; Osato-Kaneda, A.; Kim, Y.S.; Leventhal, B.; Shui, A.; Kato, S.; Nakamura, K. Prevalence and cumulative incidence of autism spectrum disorders and the patterns of co-occurring neurodevelopmental disorders in a total population sample of 5-year-old children. Mol Autism. 2020, 11, 35. [Google Scholar] [CrossRef]
- Zhou, H.; Xu, X.; Yan, W.; Zou, X.; Wu, L.; Luo, X.; Li, T.; Huang, Y.; Guan, H.; Chen, X.; et al. Prevalence of Autism Spectrum Disorder in China: A Nationwide Multi-center Population-based Study Among Children Aged 6 to 12 Years. Neurosci Bull. 2020, 36, 961–971. [Google Scholar] [CrossRef]
- Holingue, C.; Newill, C.; Lee, L.C.; Pasricha, P.J.; Daniele Fallin, M. Gastrointestinal symptoms in autism spectrum disorder: A review of the literature on ascertainment and prevalence. Autism Res. 2018, 11, 24–36. [Google Scholar] [CrossRef]
- Chaidez, V.; Hansen, R.L.; Hertz-Picciotto, I. Gastrointestinal problems in children with autism, developmental delays or typical development. J Autism Dev Disord. 2014, 44, 1117–1127. [Google Scholar] [CrossRef]
- Hsiao, E.Y.; McBride, S.W.; Hsien, S.; Sharon, G.; Hyde, E.R.; McCue, T.; Codelli, J.A.; Chow, J.; Reisman, S.E.; Petrosino, J.F.; Patterson, P.H.; Mazmanian, S.K. Microbiota modulate behavioral and physiological abnormalities associated with neurodevelopmental disorders. Cell. 2013, 155, 1451–1463. [Google Scholar] [CrossRef]
- Nadeem, A.; Ahmad, S.F.; Attia, S.M.; Al-Ayadhi, L.Y.; Al-Harbi, N.O.; Bakheet, S.A. Dysregulated enzymatic antioxidant network in peripheral neutrophils and monocytes in children with autism. Prog Neuropsychopharmacol Biol Psychiatry 2019, 88, 352–359. [Google Scholar] [CrossRef]
- Roduit, C.; Frei, R.; Ferstl, R.; Loeliger, S.; Westermann, P.; Rhyner, C.; Schiavi, E.; Barcik, W.; Rodriguez-Perez, N.; Wawrzyniak, M.; et al. High levels of butyrate and propionate in early life are associated with protection against atopy. Allergy. 2019, 74, 799–809. [Google Scholar] [CrossRef]
- Liu, S.; Li, E.; Sun, Z.; Fu, D.; Duan, G.; Jiang, M.; Yu, Y.; Mei, L.; Yang, P.; Tang, Y.; Zheng, P. Altered gut microbiota and short chain fatty acids in Chinese children with autism spectrum disorder. Sci Rep. 2019, 9, 287. [Google Scholar] [CrossRef] [PubMed]
- Rattaz, C.; Michelon, C.; Munir, K.; Baghdadli, A. Challenging behaviours at early adulthood in autism spectrum disorders: Topography, risk factors and evolution. J Intellect Disabil Res. 2018, 62, 637–649. [Google Scholar] [CrossRef] [PubMed]
- Bravo, J.A.; Forsythe, P.; Chew, M.V.; Escaravage, E.; Savignac, H.M.; Dinan, T.G.; Bienenstock, J.; Cryan, J.F. Ingestion of Lactobacillus strain regulates emotional behavior and central GABA receptor expression in a mouse via the vagus nerve. Proc Natl Acad Sci U S A 2011, 108, 16050–16055. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.R.; Osadchiy, V.; Kalani, A.; Mayer, E.A. The Brain-Gut-Microbiome Axis. Cell Mol Gastroenterol Hepatol. 2018, 6, 133–148. [Google Scholar] [CrossRef] [PubMed]
- Zegarra-Ruiz, D.F.; Kim, D.V.; Norwood, K.; Kim, M.; Wu, W.H.; Saldana-Morales, F.B.; Hill, A.A.; Majumdar, S.; Orozco, S.; Bell, R.; Round, J.L.; Longman, R.S.; Egawa, T.; Bettini, M.L.; Diehl, G.E. Thymic development of gut-microbiota-specific T cells. Nature 2021, 594, 413–417. [Google Scholar] [CrossRef]
- Ait-Belgnaoui, A.; Colom, A.; Braniste, V.; Ramalho, L.; Marrot, A.; Cartier, C.; Houdeau, E.; Theodorou, V.; Tompkins, T. Probiotic gut effect prevents the chronic psychological stress-induced brain activity abnormality in mice. Neurogastroenterol Motil. 2014, 26, 510–520. [Google Scholar] [CrossRef]
- Dinan, T.G.; Cryan, J.F. The impact of gut microbiota on brain and behaviour: Implications for psychiatry. Curr Opin Clin Nutr Metab Care. 2015, 18, 552–558. [Google Scholar] [CrossRef]
- Strati, F.; Cavalieri, D.; Albanese, D.; De Felice, C.; Donati, C.; Hayek, J.; Jousson, O.; Leoncini, S.; Renzi, D.; Calabrò, A.; De Filippo, C. New evidences on the altered gut microbiota in autism spectrum disorders. Microbiome. 2017, 5, 24. [Google Scholar] [CrossRef]
- Ma, B.; Liang, J.; Dai, M.; Wang, J.; Luo, J.; Zhang, Z.; Jing, J. Altered Gut Microbiota in Chinese Children With Autism Spectrum Disorders. Front Cell Infect Microbiol. 2019, 9, 40. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef]
- Li, D.; Chen, Q.; Zhuang, Z.; Chen, H. Correction between gut microbiota and symptom severity in children with autism spectrum disorder (in chinese). Chin J Child Health Care. 2023, 31, 497–501. [Google Scholar]
- Wong, O.W.H.; Lam, A.M.W.; Or, B.P.N.; Mo, F.Y.M.; Shea, C.K.S.; Lai, K.Y.C.; Ma, S.L.; Hung, S.F.; Chan, S.; Kwong, T.N.Y.; Wong, S.; Leung, P.W.L. Disentangling the relationship of gut microbiota, functional gastrointestinal disorders and autism: A case-control study on prepubertal Chinese boys. Sci Rep. 2022, 12, 10659. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lu, H.; Tang, W.; Hao, X. Difference in fecal intestinal flora instructure and short chian fatty acids between children with autism spectrum disorder and healthy children(in Chinese). Chin J Child Health Care. 2022, 30, 1390–1394. [Google Scholar]
- Chen, Z.; Shi, K.; Liu, X.; Dai, Y.; Liu, Y.; Zhang, L.; Du, X.; Zhu, T.; Yu, J.; Fang, S.; Li, F. Gut Microbial Profile Is Associated With the Severity of Social Impairment and IQ Performance in Children With Autism Spectrum Disorder. Front Psychiatry. 2021, 12, 789864. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Yuan, B. Relationship between intestinal flora and autism grade in children with autism (in Chinese). Chin J Microecol. 2021, 33, 560–563. [Google Scholar]
- Dan, Z.; Mao, X.; Liu, Q.; Guo, M.; Zhuang, Y.; Liu, Z.; Chen, K.; Chen, J.; Xu, R.; Tang, J.; Qin, L.; Gu, B.; Liu, K.; Su, C.; Zhang, F.; Xia, Y.; Hu, Z.; Liu, X. Altered gut microbial profile is associated with abnormal metabolism activity of Autism Spectrum Disorder. Gut Microbes. 2020, 11, 1246–1267. [Google Scholar] [CrossRef]
- Ding, X.; Xu, Y.; Zhang, X.; Zhang, L.; Duan, G.; Song, C.; Li, Z.; Yang, Y.; Wang, Y.; Wang, X.; Zhu, C. Gut microbiota changes in patients with autism spectrum disorders. J Psychiatr Res. 2020, 129, 149–159. [Google Scholar] [CrossRef]
- Zeng, J.; Wei, S.; Wang, M. Association between intestinal flora and symptom severity in children with autism spectrum disorders (in Chinese). J. Psychiatry. 2020, 33, 62–65. [Google Scholar]
- Zou, R.; Xu, F.; Wang, Y.; Duan, M.; Guo, M.; Zhang, Q.; Zhao, H.; Zheng, H. Changes in the Gut Microbiota of Children with Autism Spectrum Disorder. Autism Res. 2020, 13, 1614–1625. [Google Scholar] [CrossRef]
- Kang, D.W.; Adams, J.B.; Gregory, A.C.; Borody, T.; Chittick, L.; Fasano, A.; Khoruts, A.; Geis, E.; Maldonado, J.; McDonough-Means, S. Microbiota Transfer Therapy alters gut ecosystem and improves gastrointestinal and autism symptoms: An open-label study. Microbiome. 2017, 5, 10. [Google Scholar] [CrossRef]
- Kang, D.W.; Ilhan, Z.E.; Isern, N.G.; Hoyt, D.W.; Howsmon, D.P.; Shaffer, M.; Lozupone, C.A.; Hahn, J.; Adams, J.B.; Krajmalnik-Brown, R. Differences in fecal microbial metabolites and microbiota of children with autism spectrum disorders. Anaerobe. 2018, 49, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.W.; Park, J.G.; Ilhan, Z.E.; Wallstrom, G.; Labaer, J.; Adams, J.B.; Krajmalnik-Brown, R. Reduced incidence of Prevotella and other fermenters in intestinal microflora of autistic children. PLoS ONE 2013, 8, e68322. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.B.; Johansen, L.J.; Powell, L.D.; Quig, D.; Rubin, R.A. Gastrointestinal flora and gastrointestinal status in children with autism--comparisons to typical children and correlation with autism severity. BMC Gastroenterol. 2011, 11, 22. [Google Scholar] [CrossRef] [PubMed]
- Son, J.S.; Zheng, L.J.; Rowehl, L.M.; Tian, X.; Zhang, Y.; Zhu, W.; Litcher-Kelly, L.; Gadow, K.D.; Gathungu, G.; Robertson, C.E. Comparison of Fecal Microbiota in Children with Autism Spectrum Disorders and Neurotypical Siblings in the Simons Simplex Collection. PLoS ONE 2015, 10, e0137725. [Google Scholar] [CrossRef] [PubMed]
- Finegold, S.M.; Dowd, S.E.; Gontcharova, V.; Liu, C.; Henley, K.E.; Wolcott, R.D.; Youn, E.; Summanen, P.H.; Granpeesheh, D.; et al. Pyrosequencing study of fecal microflora of autistic and control children. Anaerobe. 2010, 16, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Christophersen, C.T.; Sorich, M.J.; Gerber, J.P.; Angley, M.T.; Conlon, M.A. Increased abundance of Sutterella spp. and Ruminococcus torques in feces of children with autism spectrum disorder. Mol Autism. 2013, 4, 42. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Christophersen, C.T.; Sorich, M.J.; Gerber, J.P.; Angley, M.T.; Conlon, M.A. Low relative abundances of the mucolytic bacterium Akkermansia muciniphila and Bifidobacterium spp. in feces of children with autism. Appl Environ Microbiol. 2011, 77, 6718–6721. [Google Scholar] [CrossRef]
- Gondalia, S.V.; Palombo, E.A.; Knowles, S.R.; Cox, S.B.; Meyer, D.; Austin, D.W. Molecular characterisation of gastrointestinal microbiota of children with autism (with and without gastrointestinal dysfunction) and their neurotypical siblings. Autism Res. 2012, 5, 419–427. [Google Scholar] [CrossRef]
- Coretti, L.; Paparo, L.; Riccio, M.P.; Amato, F.; Cuomo, M.; Natale, A.; Borrelli, L.; Corrado, G.; Comegna, M.; Buommino, E.; Castaldo, G.; Bravaccio, C.; Chiariotti, L.; Berni Canani, R.; Lembo, F. Gut Microbiota Features in Young Children With Autism Spectrum Disorders. Front Microbiol. 2018, 9, 3146. [Google Scholar] [CrossRef]
- De Angelis, M.; Piccolo, M.; Vannini, L.; Siragusa, S.; De Giacomo, A.; Serrazzanetti, D.I.; Cristofori, F.; Guerzoni, M.E.; Gobbetti, M.; Francavilla, R. Fecal microbiota and metabolome of children with autism and pervasive developmental disorder not otherwise specified. PLoS ONE 2013, 8, e76993. [Google Scholar] [CrossRef]
- Pulikkan, J.; Maji, A.; Dhakan, D.B.; Saxena, R.; Mohan, B.; Anto, M.M.; Agarwal, N.; Grace, T.; Sharma, V.K. Gut Microbial Dysbiosis in Indian Children with Autism Spectrum Disorders. Microb Ecol. 2018, 76, 1102–1114. [Google Scholar] [CrossRef] [PubMed]
- Inoue, R.; Sakaue, Y.; Sawai, C.; Sawai, T.; Ozeki, M.; Romero-Pérez, G.A.; Tsukahara, T. A preliminary investigation on the relationship between gut microbiota and gene expressions in peripheral mononuclear cells of infants with autism spectrum disorders. Biosci Biotechnol Biochem. 2016, 80, 2450–2458. [Google Scholar] [CrossRef] [PubMed]
- Plaza-Diaz, J.; Gomez-Fernandez, A.; Chueca, N.; Torre-Aguilar, M.J.; Gil, A.; Perez-Navero, J.L.; Flores-Rojas, K.; Martin-Borreguero, P.; Solis-Urra, P.; Ruiz-Ojeda, F.J.; Garcia, F.; Gil-Campos, M. Autism Spectrum Disorder (ASD) with and without Mental Regression is Associated with Changes in the Fecal Microbiota. Nutrients 2019, 11, 337. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Ma, W.; Zhang, J.; He, Y.; Wang, J. Analysis of gut microbiota profiles and microbe-disease associations in children with autism spectrum disorders in China. Sci Rep. 2018, 8, 13981. [Google Scholar] [CrossRef] [PubMed]
- Iglesias-Vázquez, L.; Van Ginkel Riba, G.; Arija, V.; Canals, J. Composition of Gut Microbiota in Children with Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 792. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Xu, X.; Li, J.; Li, F. Association Between Gut Microbiota and Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. Front Psychiatry 2019, 10, 473. [Google Scholar] [CrossRef]
- Parracho, H.M.; Bingham, M.O.; Gibson, G.R.; McCartney, A.L. Differences between the gut microflora of children with autistic spectrum disorders and that of healthy children. J Med Microbiol. 2005, 54 Pt 10, 987–991. [Google Scholar] [CrossRef]
- Hiippala, K.; Kainulainen, V.; Kalliomäki, M.; Arkkila, P.; Satokari, R. Mucosal Prevalence and Interactions with the Epithelium Indicate Commensalism of Sutterella spp. Front Microbiol. 2016, 7, 1706. [Google Scholar] [CrossRef]
- Kaakoush, N.O. Sutterella Species, IgA-degrading Bacteria in Ulcerative Colitis. Trends Microbiol. 2020, 28, 519–522. [Google Scholar] [CrossRef]
- Xue, L.; He, J.; Gao, N.; Lu, X.; Li, M.; Wu, X.; Liu, Z.; Jin, Y.; Liu, J.; Xu, J.; Geng, Y. Probiotics may delay the progression of nonalcoholic fatty liver disease by restoring the gut microbiota structure and improving intestinal endotoxemia. Sci Rep. 2017, 7, 45176. [Google Scholar] [CrossRef]
- Png, C.W.; Lindén, S.K.; Gilshenan, K.S.; Zoetendal, E.G.; McSweeney, C.S.; Sly, L.I.; McGuckin, M.A.; Florin, T.H. Mucolytic bacteria with increased prevalence in IBD mucosa augment in vitro utilization of mucin by other bacteria. Am J Gastroenterol. 2010, 105, 2420–2428. [Google Scholar] [CrossRef] [PubMed]
- Everard, A.; Belzer, C.; Geurts, L.; Ouwerkerk, J.P.; Druart, C.; Bindels, L.B.; Guiot, Y.; Derrien, M.; Muccioli, G.G.; Delzenne, N.M.; de Vos, W.M.; Cani, P.D. Cross-talk between Akkermansia muciniphila and intestinal epithelium controls diet-induced obesity. Proc Natl Acad Sci U S A. 2013, 110, 9066–9071. [Google Scholar] [CrossRef] [PubMed]
- Rothschild, D.; Weissbrod, O.; Barkan, E.; Kurilshikov, A.; Korem, T.; Zeevi, D.; Costea, P.I.; Godneva, A.; Kalka, I.N.; Bar, N.; et al. Environment dominates over host genetics in shaping human gut microbiota. Nature. 2018, 555, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Asnicar, F.; Berry, S.E.; Valdes, A.M.; Nguyen, L.H.; Piccinno, G.; Drew, D.A.; Leeming, E.; Gibson, R.; Le Roy, C.; Khatib, H.A.; et al. Microbiome connections with host metabolism and habitual diet from 1,098 deeply phenotyped individuals. Nat Med. 2021, 27, 321–332. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flow diagram of the identification of the included studies.
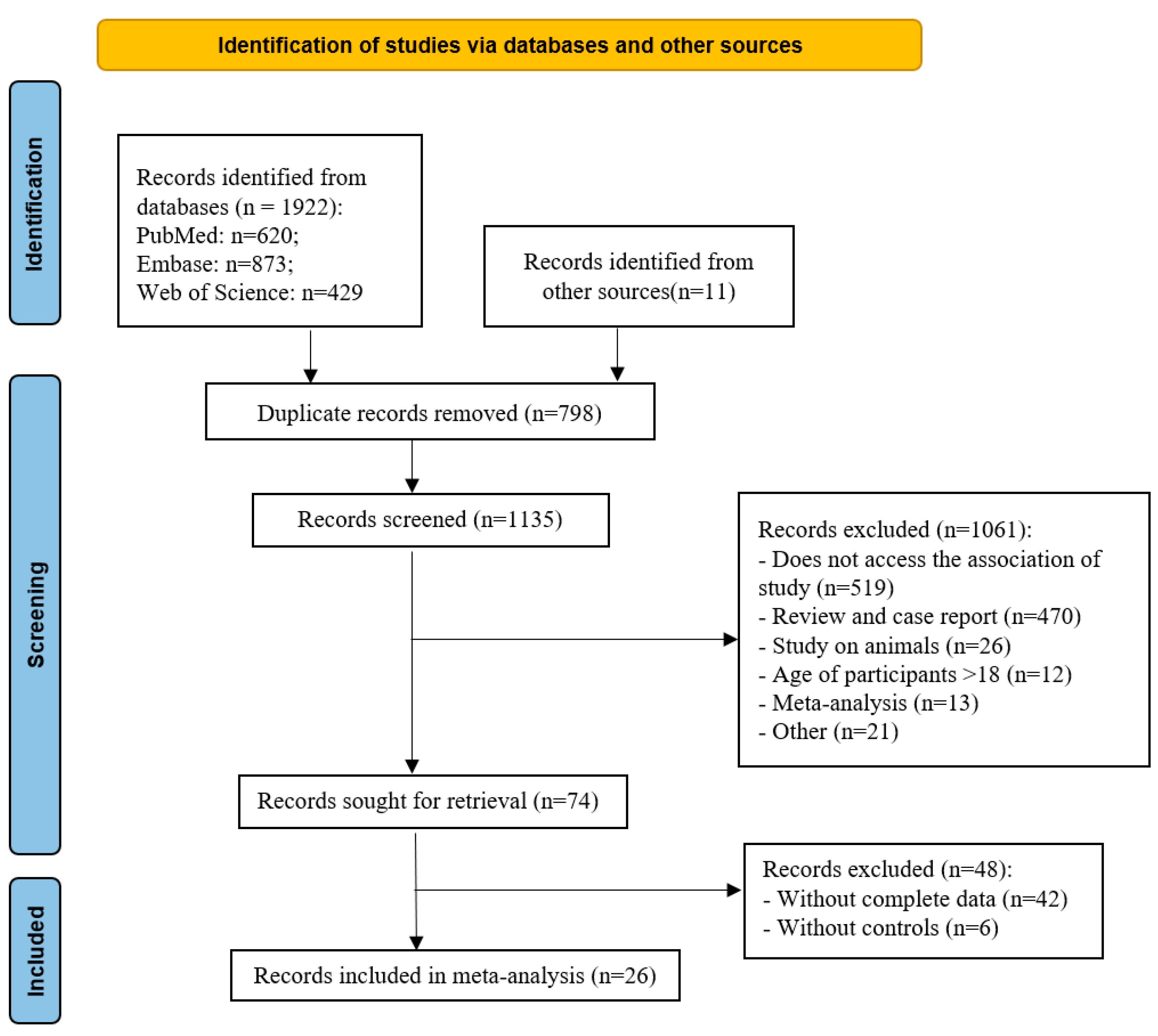
Figure 2.
Forest plot of relative abundance of Bacteroidetes in ASD and TD.
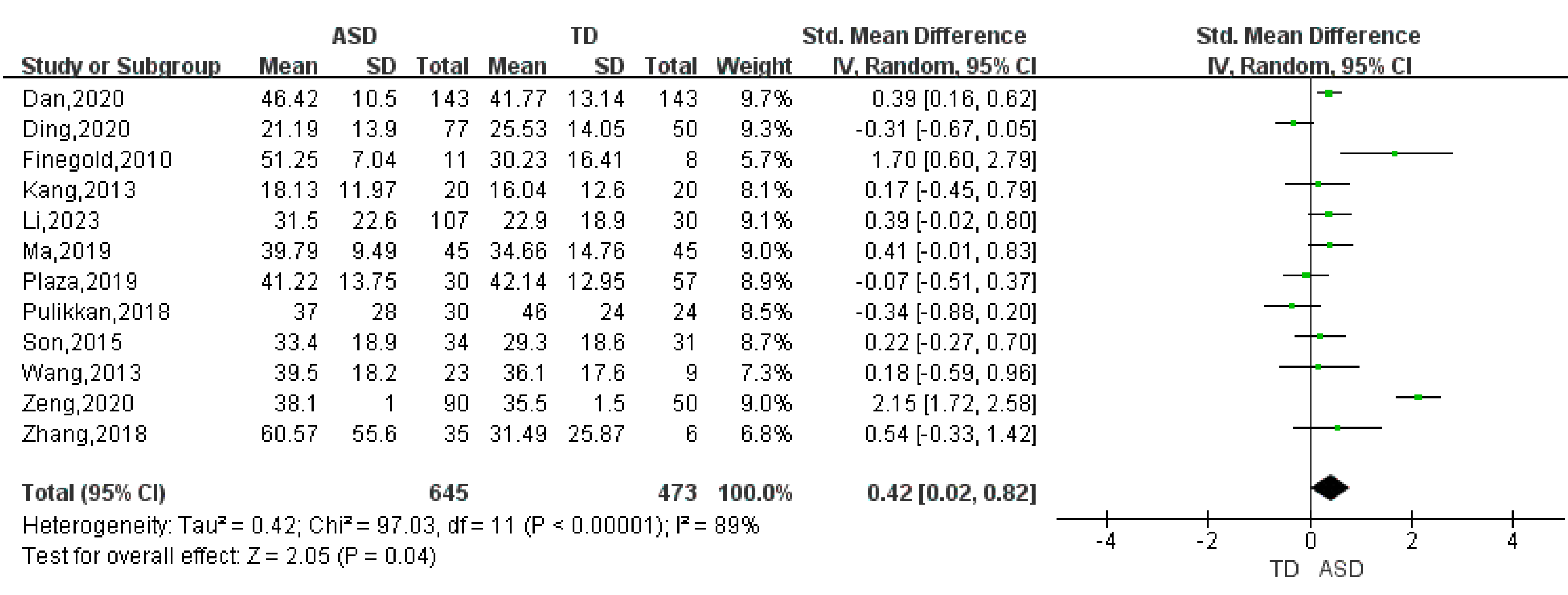
Figure 3.
Forest plot of relative abundance of Verrucomicrobia in ASD and TD
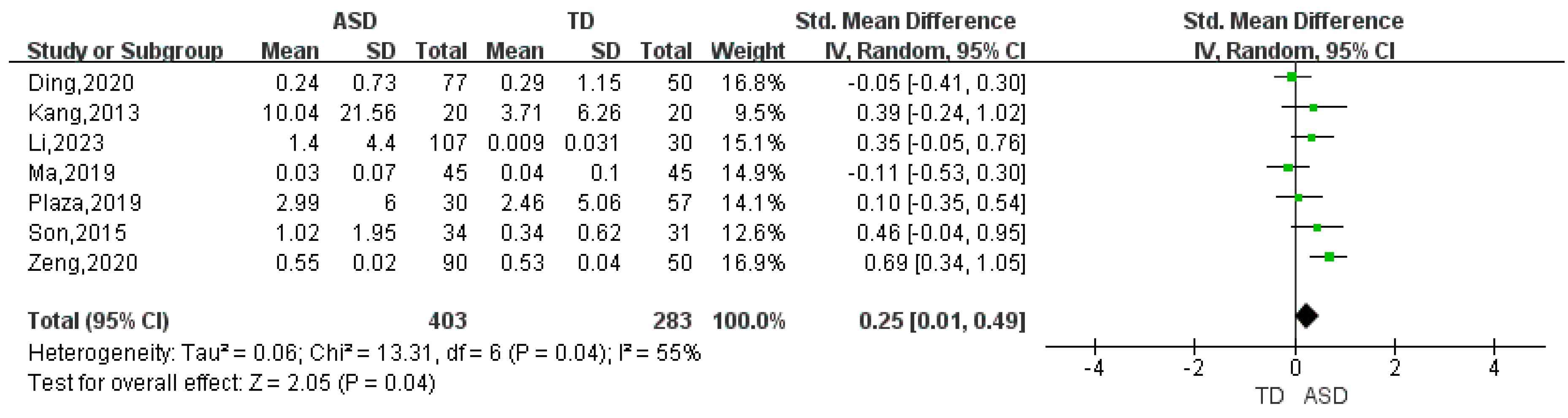
Figure 4.
Forest plot of relative abundance of Bacteroides in ASD and TD.
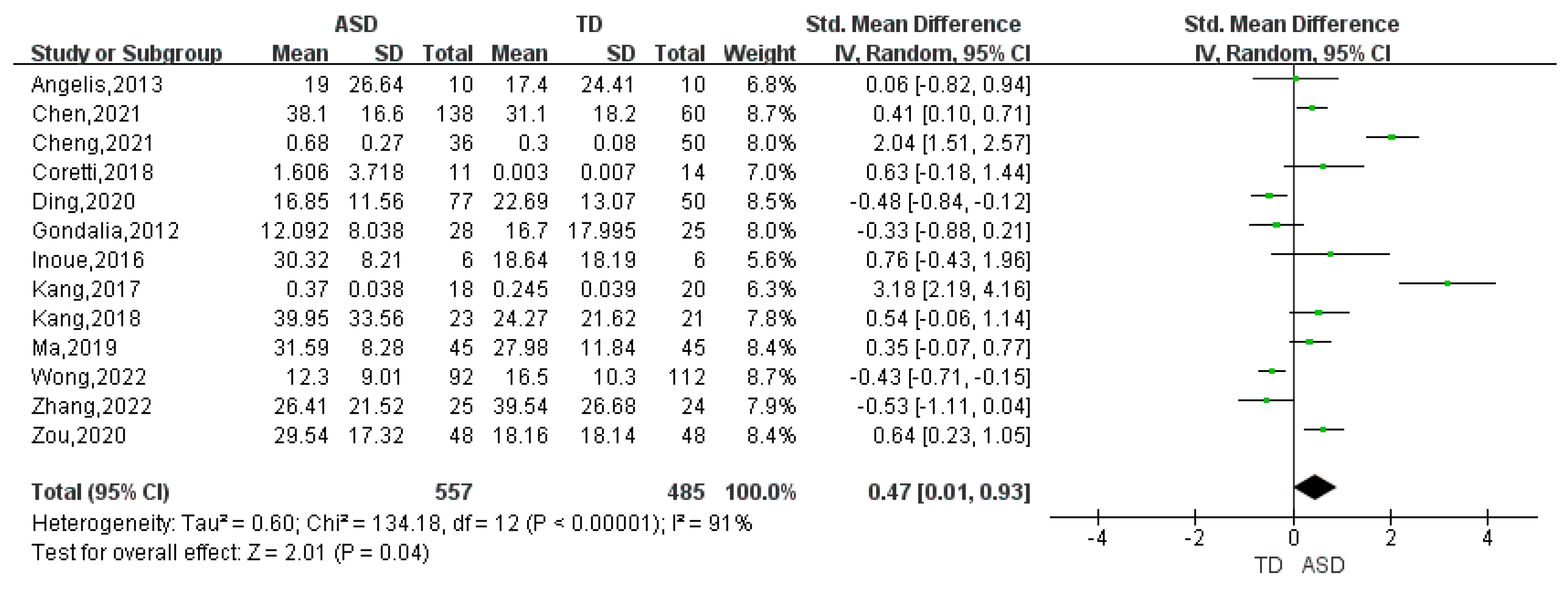
Figure 5.
Forest plot of relative abundance of Proteobacteria in ASD and TD.
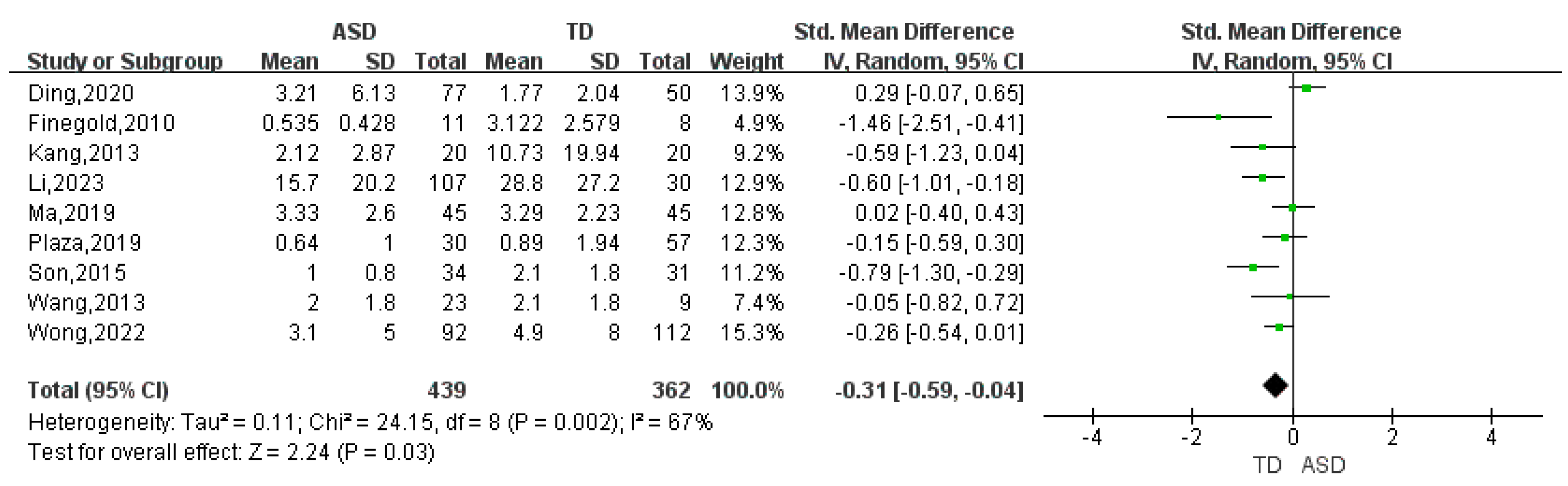
Figure 6.
Forest plot of relative abundance of Bifidobacterium in ASD and TD.
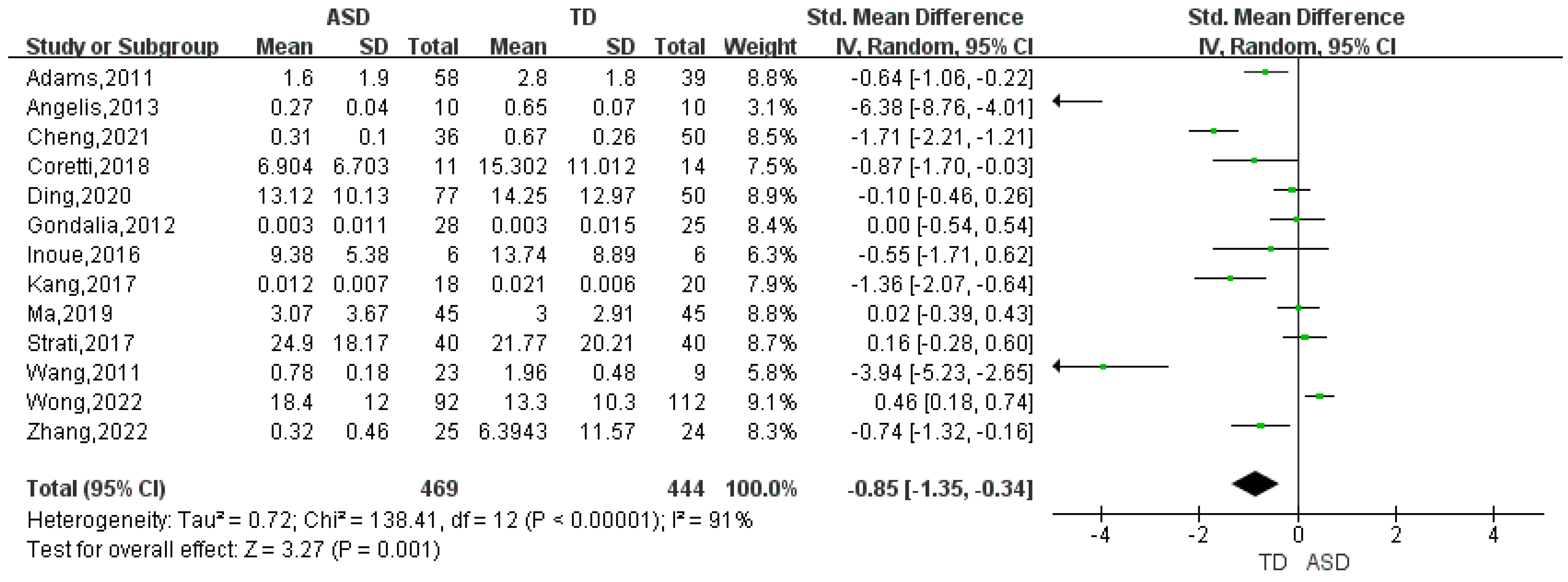

Table 1.
Summary characteristics of the studies included in the meta-analysis.
| Study | Country | ASD | TD | Bacteria Detected | ||||
|---|---|---|---|---|---|---|---|---|
| n | Age(y) | male: female | n | age(y) | male: female | |||
| Li et al. (2023)[23] | China | 107 | 3.34 ± 0.75 | 79: 28 | 30 | 3.61 ± 0.48 | 21: 9 | Phylum: Actinobacteria, Bacteroidetes, Firmicutes, Fusobacteria, Proteobacteria, Verrucomicrobia |
| Wong et al.(2022)[24] | China | 92 | 8.43 ± 1.54 | 92: 0 | 112 | 8.12 ± 1.99 | 112: 0 | Phylum: Actinobacteria, Bacteroidetes, Firmicutes, Fusobacteriota, Proteobacteria, VerrucomicrobiaGenus: Bacteroides, Bifidobacterium, Bilophila, Blautia, Collinsella, Dorea, Fusobacterium, Parabacteroides, Phascolarctobacterium, Sutterella |
| Zhang et al.(2022)[25] | China | 25 | 6.72 ± 2.56 | 18: 7 | 24 | 7.68 ± 2.93 | 14: 10 | Phylum: Actinobacteria, FirmicutesGenus: Bacteroides, Bifidobacterium, Blautia, Clostridium, Streptococcus, Sutterella |
| Chen et al.2021[26] | China | 138 | 6.11 ± 2.00 | 117: 21 | 60 | 6.65 ± 2.22 | 27: 33 | Genus:Bacteroides, Collinsella, Coprococcus, Faecalibacterium,Prevotella,Megamonas, Sutterella |
| Cheng et al.(2021)[27] | China | 36 | 7.44 ± 1.53 | 21: 15 | 50 | 7.33 ± 1.49 | 27: 23 | Genus: Bacteroides, Bifidobacterium, Clostridium |
| Table 1. Summary characteristics of the studies included in the meta-analysis (Cont.) | ||||||||
| Study | Country | ASD | TD | Bacteria Detected | ||||
| n | age(y) | male: female | n | age(y) | male: female | |||
| Dan et al.(2020)[28] | China | 143 | 4.94 ± 0.16 | 130:13 | 143 | 5.19 ± 0.17 | 127:16 | Phylum: Bacteroidetes, Cyanobacteria, FusobacteriaGenus: Blautia, Fusobacterium, Parabacteroides, Paraprevotella, Prevotella |
| Ding et al.(2020)[29] | China | 77 | 38.50±11.70m | 59: 18 | 50 | 42.9±14.5m | 39: 11 | Phylum: Actinobacteria, Bacteroidetes, Firmicutes, Proteobacteria, VerrucomicrobiaGenus: Bacteroides, Bifidobacterium, Blautia, Collinsella, Dorea, Faecalibacterium,Paraprevotella, Streptococcus |
| Zeng et al.(2020)[30] | China | 90 | 3.50 ± 1.20 | 70: 20 | 50 | 3.00 ± 1.50 | 39: 11 | Phylum: Actinobacteria, Bacteroidetes, Cyanobacteria, Firmicutes, Fusobacteria, Tenericutes, Verrucomicrobia |
| Zou et al.(2020)[31] | China | 48 | 5 (2–7) | 38: 10 | 48 | 4 | 24: 24 | Genus:Akkermansia, Bacteroides, Megamonas, Prevotella |
| Ma et al.(2019)[21] | China | 45 | 7.27 ± 1.07 | 39: 6 | 45 | 7.04 ± 1.19 | 39: 6 | Phylum: Actinobacteria, Bacteroidetes, Cyanobacteria, Firmicutes, Fusobacteria, Proteobacteria, Tenericutes, Verrucomicrobia |
| Table 1. Summary characteristics of the studies included in the meta-analysis. (Cont.) | ||||||||
| Study | Country | ASD | TD | Bacteria Detected | ||||
| n | age(y) | male: female | n | age(y) | male: female | |||
| Ma et al.(2019)[21] | China | 45 | 7.27 ± 1.07 | 39: 6 | 45 | 7.04 ± 1.19 | 39: 6 | Genus: Bacteroides, Bifidobacterium, Bilophila, Faecalibacterium, Fusobacterium, Lactobacillus, Megamonas, Parabacteroides |
| Plaza et al.(2019)[45] | Spain | 30 | 44.19 ± 1.60m | - | 57 | 51±2.59 m | - | Phylum: Actinobacteria, Bacteroidetes, Firmicutes, Proteobacteria, Verrucomicrobia |
| Coretti et al.(2018)[41] | Italy | 11 | 35 ± 5.7m | 9: 2 | 14 | 35 ± 8.40m | 8: 6 | Genus: Bacteroides, Bifidobacterium, Blautia, Coprococcus, Streptococcus |
| Kang et al.(2018)[33] | USA | 23 | 10.1 ± 4.1 | 22:1 | 21 | 8.4 ± 3.4 | 15:6 | Genus: Akkermansia, Bacteroides, Coprococcus, Faecalibacterium, Prevotella |
| Pulikkan et al(2018)[43] | Indian | 30 | 9.5 (3–16) | 28: 2 | 24 | 9.5 (3.5–16) | 15: 9 | Phylum: Bacteroidetes, Firmicutes |
| Zhang et al.(2018)[46] | China | 35 | 4.9±1.5 | 29: 6 | 6 | 4.6±1.1 | 5: 1 | Phylum: Bacteroidetes, Firmicutes |
| Kang et al.(2017)[32] | USA | 18 | 7-16 | - | 20 | 7-16 | - | Genus: Bacteroides, Bifidobacterium, Clostridium, Coprococcus, Parabacteroides, Phascolarctobacterium |
| Table 1. Summary characteristics of the studies included in the meta-analysis. (Cont.) | ||||||||
| Study | Country | ASD | TD | Bacteria Detected | ||||
| n | age(y) | male: female | n | age(y) | male: female | |||
| Strati et al.(2017)[20] | Italy | 40 | 10 (5–17) | 31: 9 | 40 | 7 (3.6–12) | 28: 12 | Genus:Akkermansia,Bifidobacterium, Blautia, Collinsella, Coprococcus, Dorea, Faecalibacterium, Lactobacillus, Paraprevotella, Prevotella, Streptococcus |
| Inoue et al.(2016)[44] | Japan | 6 | 3-5 | - | 6 | 3-5 | - | Genus:Akkermansia, Bacteroides,Bifidobacterium, Bilophila, Blautia, Clostridium, Collinsella, Coprococcus, Dorea, Faecalibacterium |
| Son et al.(2015)[36] | USA | 34 | 7–14 | - | 31 | 7–14 | - | Phylum: Actinobacteria, Bacteroidetes, Cyanobacteria, Firmicutes, Proteobacteria, Tenericutes, Verrucomicrobia |
| Angelis et al.(2013)[42] | Italy | 10 | 4-10 | - | 10 | 4-10 | - | Genus:Bacteroides,Bifidobacterium, Clostridium, Faecalibacterium, Parabacteroides |
| Kang et al.(2013)[34] | USA | 20 | 6.70 ± 2.70 | 18: 2 | 20 | 8.30 ± 4.40 | 17: 3 | Phylum: Actinobacteria, Bacteroidetes, Firmicutes, Proteobacteria, Verrucomicrobia |
| Wang et al.(2013)[38] | Austrilia | 23 | 10.25 ± 0.75 | 21: 2 | 9 | 9.50 ± 1.25 | 4: 5 | Phylum: Actinobacteria, Bacteroidetes, Firmicutes, ProteobacteriaGenus: Sutterella |
| Table 1. Summary characteristics of the studies included in the meta-analysis. (Cont.) | ||||||||
| Study | Country | ASD | TD | Bacteria Detected | ||||
| n | age(y) | male: female | n | age(y) | male: female | |||
| Gondalia et al(2012)[40] | Australia | 28 | 2-12 | - | 25 | 2-12 | - | Genus:Bacteroides,Bifidobacterium, Coprococcus, Faecalibacterium, Parabacteroides, Phascolarctobacterium |
| Adams et al.(2011)[35] | USA | 58 | 6.91 ± 3.40 | 50: 8 | 39 | 7.70 ± 4.40 | 18: 21 | Genus: Bifidobacterium, Lactobacillus |
| Wang et al.(2011)[39] | Austrilia | 23 | 10.25 ± 0.75 | 21: 2 | 9 | 9.50 ± 1.25 | 4: 5 | Genus: Bifidobacterium, Lactobacillus, Prevotella |
| Finegold et al.(2010)[37] | USA | 11 | - | - | 8 | - | - | Phylum: Actinobacteria, Bacteroidetes, Cyanobacteria, Firmicutes, Fusobacteria, Proteobacteria, Tenericutes |
Table 2.
Results of meta-analysis at phylum and genus level in ASD and TD.
| Phylum/Genus | Studies included | SMD | 95% CI | I2 | Overall effect(Z) | p value |
|---|---|---|---|---|---|---|
| Actinobacteria | 11 | -0.1 | (-0.46, 0.26) | 87 | 0.53 | 0.60 |
| Bifidobacterium | 13 | -0.85 | (-1.35, -0.34) | 91 | 3.27 | 0.001 |
| Collinsella | 5 | 0.23 | (-0.14, 0.60) | 76 | 1.21 | 0.23 |
| Bacteroidetes | 12 | 0.42 | (0.02, 0.82) | 89 | 2.05 | 0.04 |
| Bacteroides | 13 | 0.47 | (0.01, 0.93) | 91 | 2.01 | 0.04 |
| Parabacteroides | 6 | -0.05 | (-0.40, 0.31) | 76 | 0.26 | 0.79 |
| Prevotella | 6 | -0.01 | (-0.44, 0.42) | 85 | 0.04 | 0.97 |
| Paraprevotella | 3 | -0.12 | (-0.46, 0.21) | 66 | 0.72 | 0.47 |
| Cyanobacteria | 5 | -0.09 | (-0.59, 0.40) | 86 | 0.38 | 0.71 |
| Firmicutes | 13 | -0.24 | (-0.81, 0.33) | 94 | 0.83 | 0.41 |
| Blautia | 7 | -0.13 | (-0.54, 0.28) | 84 | 0.61 | 0.54 |
| Clostridium | 5 | 1.01 | (0.15, 1.87) | 85 | 2.31 | 0.02 |
| Coprococcus | 7 | -0.43 | (-0.80, -0.06) | 65 | 2.25 | 0.02 |
| Dorea | 4 | 0.5 | (0.31, 0.70) | 0 | 5.03 | <0.001 |
| Faecalibacterium | 8 | -0.02 | (-0.43, 0.40) | 81 | 0.07 | 0.94 |
| Lactobacillus | 4 | 0.27 | (-0.36, 0.89) | 85 | 0.84 | 0.40 |
| Megamonas | 3 | 0.04 | (-0.40, 0.48) | 76 | 0.19 | 0.85 |
| Phascolarctobacterium | 4 | -0.21 | (-0.62, 0.21) | 71 | 0.99 | 0.32 |
| Streptococcus | 4 | -0.47 | (-1.04, 0.10) | 79 | 1.63 | 0.10 |
| Fusobacteria | 6 | -0.1 | (-0.49, 0.28) | 71 | 0.99 | 0.32 |
| Fusobacterium | 3 | 0.05 | (-0.26, 0.36) | 69 | 0.32 | 0.75 |
| Proteobacteria | 9 | -0.31 | (-0.59, -0.04) | 67 | 2.24 | 0.03 |
| Bilophila | 3 | -0.36 | (-0.87, 0.15) | 68 | 1.37 | 0.17 |
| Sutterella | 4 | 1.04 | (0.04, 2.05) | 95 | 2.03 | 0.04 |
| Tenericutes | 4 | -0.47 | (-1.08, 0.15) | 84 | 1.48 | 0.14 |
| Verrucomicrobia | 7 | 0.25 | (0.01, 0.49) | 55 | 2.05 | 0.04 |
| Akkermansia | 4 | -0.41 | (-0.77, -0.05) | 38 | 2.26 | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



