
Submitted:
19 May 2023
Posted:
22 May 2023
You are already at the latest version
Abstract
Programmed-death-1 (PD-1) receptor plays a major physiological role in maintainance of im-mune tolerance, and, by interaction with its ligands (PD-L1 and PD-L2), prevents the develop-ment of multiple immune-mediated diseases. There is growing evidence of an important role of PD-1/PD-L1 pathway in pathogenesis of psoriasis. 84 subjects with psoriasis were included into the study, together with 29 healthy subjects as a control group. 28 of psoriatic patients were treated with biologice therapy (TNF-alpha, interleukin (IL)-12/23 or IL-17 inhibitors). Amounts of PD1 and PD-L1 positive T-cells in peripheral blood were evaluated using flow cytometry. Significantly lower levels of peripheral blood mononuclear cells (PBMCs) with the expression of PD-1 and PD-L1 were found in psoriatic patients when compared to healthy individuals, i.e. CD3/PD1, CD3/PDL1, CD4/PD1, CD4/PDL1, CD8/PDL1, CD19/PD1, CD19/PDL1 positive cells. Biologic treatment resulted in elevation of CD3/PDL1, CD8/PDL1 and decrease of CD8/PD1 posi-tive PBMCs. Our results confirm previous observations of disrupted PD-1/PD-L1 pathway in psoriasis, and that this disturbances may play an important role in development of the disease. Biologic drugs may reverse several abnormalities observed within this pathway, which may ex-plain their excellent efficacy in the treatment of psoriasis. Further research should be conducted to fully explain the results obtained.
Keywords:
psoriasis
; systemic treatment
; biologic treatment
; immune checkpoint
1. Introduction
Psoriasis is a chronic, immune mediated disease which manifests with clinically typical, erythematous, scaling papules and plagues, that may appear anywhere on the skin surface. The understanding of psoriasis as an only cutaneous problem changed completely during last decades; now it is considered a systemic condition with multiple associated problems, including psoriatic arthritis, metabolic syndrome and atherosclerosis with its complications [1].
Pathogenesis of psoriasis is complex and still not fully understood. The appearance of psoriatic plagues on the skin result from pathological activity of several subtypes of lymphocytes, including Th1, Th17, secreting proinflammatory cytokines, i.e. IFN-γ, TNF-α and IL-17. Disruption in mechanisms ensuring immunotolerance is thought to play an important role in activation of this mechanisms in psoriasis, as well as in other immune-mediated diseases [2,3]. Programmed death 1 (PD-1) is an inhibitory co-receptor encoded by PDCD1 gene and expressed on various white blood cells. Via interaction with its ligands (PD-L1 and PD-L2), which are present on multiple peripheral cells it mediates self-immunotolerance, in particular by reduction of CD4+ T-cells activity, and induction of T regulatory lymphocytes (Tregs) [2,4].
Therapy of various neoplasms with monoclonal antibodies inhibiting PD-1 may result with new-onset psoriasis or exacerbation of pre-existing psoriatic skin lesions. Boenigen et al. described 21 of such cases during treatment of lung cancer with anti PD-1 agents: nivolumab and pembrolizumab [5]. Bartosińska et al. demonstrated, that in patients with psoriatic arthritis (PsA), the levels of circulating CD4+ PD-1+ and CD8+ PD-1+ T cells were significantly decreased than in healthy control subjects [6]. In peripheral blood mononuclear cells (PBMCs), the expression of PDCD1 gene was also lower in patients with psoriasis than in healthy control group [7]. This results seem to be reasonable, for lack of PD-1 activity may lead to sustained activation of T-cells, production of inflammatory cytokines and, as a consequence, development of psoriatic skin lesions.
Biologic drugs have revolutionized the approach to patients suffering from moderate-to-severe forms of plaque psoriasis since their first approval in the beginning of 21st century. By inhibition of selected cytokines playing key roles in immunopathogenesis of psoriasis, they are characterized by better efficacy and safety profile than standard systemic therapies. [8]
In this study we sought to evaluate the expression of PD-1, PD-L1 and PD-L2 on different types of PBMCs in patients with psoriasis and healthy controls. Another aim was to determine, whether and how treatment of psoriasis with biologic therapies impact the expression of inhibitory co-receptor PD-1 and it’s ligands on PBMCs, as no such studies were published to-date.
2. Materials and Methods
2.1. The Study Group
84 subjects with chronic plague psoriasis treated in Department of Dermatology, Venerology and Paediatric Dermatology, Medical University of Lublin, Poland were qualified to the study. Inclusion criteria were as follows: age >=18 years, active psoriatic skin lesions and >1 year of disease duration, Subjects with other types of psoriasis (i.e. erythrodermic, pustular and guttate), concomitant immune-mediated diseases, neoplasms and currently on systemic antipsoriatic treatment were excluded from the study. Detailed clinical characteristics of the study subjects are presented in Table 1. In 28 of studied subjects with psoriasis blood samples were collected twice: before and during biologic therapy for psoriasis (not earlier than 16 weeks after therapy was introduced). Control group included 29 subjects not suffering from psoriasis and any other immune-mediated conditions.
Among subjects treated with biologic drugs 12 received adalimumab, 6 secukinumab, 6 ustekinumab, 3 ixekizumab , 1 risankizumab and 1 infliximab. All patients qualified to biologic therapy must have fulfilled following criteria: have initial PASI score > 18, BSA >10 and DLQI >10, moreover, must have been treated with at least two standard systemic therapies for their psoriasis without response or with unacceptable side effects.
The study was approved by Bioethics Commitee of Medical Univeristy of Lublin. Written informed consent was taken from each study subject before inclusion into the study.
2.2. Assessment of PD-1, PD-L1
The material used for the study was peripheral blood collected from an ulnar vein in 30 ml into tubes containing EDTA. The collected blood was immediately used to perform lymphocyte immunophenotype evaluation.
To evaluate PD-1, PDL-1 surface antigens, 100 ul of whole peripheral blood and the manufacturer's recommended volume of appropriate monoclonal antibodies were used. After collecting, the samples were incubated for 20 minutes in the dark at room temperature. In the next step, 2 ml each of erythrocyte lysing liquid Lysing Solution (BD Pharmingen, USA) was added to the tubes. After 10 minutes, the samples were centrifuged at 300xg, washed with 2x buffered saline solution (PBS) without Ca2+ and Mg2+ ions and immediately subjected to cytometric analysis. For this purpose, an R1 gate was created in coordinates describing the scattering of laser light (FSC/SSC), isolating lymphocytes, and 10,000 cells were acquired.
Table 2 shows the set of monoclonal antibodies and fluorochromes used to perform lymphocyte surface antigen expression studies. Analysis of the obtained data was performed using CellQuest Pro software (Becton Dickinson, USA).
Antibodies were added to 4 cytometric tubes in the following combinations:
1.anti-CD3 FITC/ anti-CD274 PE/ anti-CD279 APC
2.anti-CD4 FITC/ anti-CD274 PE/ anti CD279 APC
3.anti-CD8 FITC/ anti-CD274 PE/ anti CD279 APC
4.anti-CD19 FITC/ anti-CD274 PE/ anti CD279 APC
The results of the cytometric analysis were presented as the percentage of cells stained with fluorescent dye-conjugated monoclonal antibodies and as mean fluorescence intensity (MFI), which is an exponent of the amount of expression of a given antigen on the cell surface. Representative flow cytometry analysis of PD-1 and PD-L1 expression in patient with psoriasis and healthy control is presented on Figure 1.
2.3. Statistical Methods
STATISTICA 13.1 software (STATSOFT, Kraków, Poland) was used in statistical analyses.
We estimated median and interquartile range (IQR) for continuous variables, or absolute numbers (n) and relative numbers (%) of occurrence of items of categorical variables.
U Mann-Whitney test was used to compare percentage rates of each PBMC subsets between psoriatic patients and control group. In psoriatic patients before and during biologic treatment we applied Wilcoxon test to compare differences between levels of each PBMC subsets. Pearson correlation coefficient was used to correlate PD-1 and PD-L1 expression on different PBMC with PASI, BSA and duration of psoriasis. In all the statistical tests p-value less than 0.05 was interpreted as statistically significant.
3. Results
Significantly lower concentrations of CD3/PD-1, CD3/PD-L1, CD4/PD-1, CD4/PD-L1, CD8/PD-L1, CD19/PD-1, CD19/PD-L1 positive PBMCs were present in subjects with psoriasis, when compared to healthy control group (Table 3).
With regard to PASI, BSA and duration of psoriasis, only a positive correlation between expression of CD4/PD1 and duration of disease was found, the longer duration of psoriasis the higher CD4/PD1 expression was (Table 4).
In psoriatic patients treated with biologic drugs, levels of CD3/PD-L1 and CD8/PD-L1 positive PBMC were significantly higher, and CD8/PD-1 positive PBMC were significantly lower than before therapy (Table 5).
4. Discussion
Despite many research conducted, exact cause of enhanced immune response in psoriasis remain unknown. Proper function od PD-1/PD-L1 is crucial in maintaining peripheral immunotolerance in health conditions [4]. The suppressive effect on immune response is achieved by interaction between PD-1 and its ligands, PD-L1 and PD-L2, expressed on various, hematopoietic and non-hematopoietic cells. PD-1/PD-L ligation leads to reduction in CD4+ T cells activity and, importantly, up-regulation of T regulatory lyphocytes (Tregs) amounts and function. Tregs are a subtype of T-cells responsible for suppression of immune response and maintainance of immunotolerance [2].
PD-1 is classified among markers of T-cell activation – it’s expression was found increased on T-cells in variuos immune mediated diseases, including systemic lupus erythematosus, rheumatoid arthritis and psoriatis arthritis [9,10]. Increase of PD-1 expression seems to be inconsistent in inflammatory diseases, for its inhibitory properties, but it is known that PD-1/PD-L1 patchway functioning is modulated in the conditions of chronic inflammation [2]. I.e. it was demonstrated, that CD4+ T cells derived from synovial fluid from subjects with rheumatoid arthritis require higher concentrations of PD-L1 to achieve inhibition when compared with peripheral blood T-cells [11]. This may be explained by increased concentration of soluble PD-1 (sPD-1), which inhibits proper PD-1/PD-L1 ligation by binding to PD-L1 on immune cells [2].
In the context of psoriasis and PD-l/PD-L1, the highest amounts of literature data refer to quite frequently observed cases of new onset or worsening of psoriasis in subjects treated for malignant tumors with anti PD-1 biologic drugs, in particular nivolumab and pembrolizumab [5]. Most of this cases are mild and can be sufficiently controlled with topical agents, not being a reason for treatment cessation [12].
In murine model of imiquimod-induced psoriasis, Imai et al. proved, that in PD-1 gene knock-out mice there was more severe keratinocyte hyperproliferation, higher levels of neutrophils in inflammatory infiltrates and expressed higher levels of Th17 cytokines, than in wild-type mice [13].
Bommarito et al. demonstrated, that in psoriatic arthritis (PsA) and rheumatoid arthritis, inflammatory cytokines, including TNF-α, IL-1 and IL-6 increase the levels of soluble PD-1 (sPD-1). sPD-1 binds to PD-1 ligands and prevents proper PD-1/PD-L ligation, disrupting its inhibitory function, which promotes inflammatory reaction. The authors found that despite increased expression of PD-1, CD4+ T-cells derived from peripheral blood and synovial fluid of patients were resistant to PD-1 mediated suppression, and this effect was probably caused by increased levels of sPD1 [14]. To date, no studies evaluated the expression of sPD1 and its importance in psoriasis, either in peripheral blood or psoriatic plague environment.
In line with the above findings, Peled et al. found that expression levels of PD-1 on circulating T-cells were signifficantly higher in PsA than in healthy controls, moreover they inversely correlated with disease activity measured by DAS28. Furthermore, they found a strong correlation between PD-1 expression levels and number of tender and swollen joints [10].
Bartosińska et al. demonstrated contradictory data: in their studies they found decreased expression of PDCD1 gene in PMBCs derived from subjects with psoriasis, when compared to healthy control. [7] The same authors found that absolute and percentage levels of CD4+PD-1+ and CD8+PD-1+ T cells in peripheral blood of psoriatic patients with and without psortiatic arthritis were significantly decreased when compared to healthy individuals [6,15]. Our present work is in agreement with this findings, but we have analyzed wider range of PBMNCs, including those with expression of PD-L1. We have showed signifficant reduction of PD1 and PD-L1 expression on majority of PBMC subsets: CD3+, CD4+ and CD19+, except from CD8/PD1 positive cells [Table 3]. Reduced PD/PD-L1 expression may explain lack of inhibitory effect of this pathway on immune response in psoriasis, that may be responsible for inflammatory response exacerbation and lead to development of skin lesions.
The same as in other Bartosińska et al. study, we did not show any correlations between levels of PBMCs expressing PD-1/PD-L1 and clinical characteristics of psoriasis (including PASI, BSA and duration pf psoriasis), except from CD4/PD1 positive cells and duration of disease [16]. However, despite this correlation was significant, it was not strong (p=0.049, Table 4).
No studies published to date evaluated expression of PD-1 and PD-L1 on PBMCs before and during treatment of psoriasis with biologic drugs. Our data show, that biologic drugs with different mechanisms of action have an impact on several of this cells, as the treatment resulted with significant increase of CD3/PD-L1 and CD8/PD-L1 positive PMNCs and significant decrease of CD8/PD-1 positive PBMCs [Table 5]. Increase of T-cells expressing PD-L1 may contribute to enhanced PD-1/PD-L1 ligation and induction of immune tolerance mechanisms. Interestingly, the only subset of examined PBMCs that decreased after biologic treatment (CD8/PD-1 positive) was that only one that was not found different between psoriatic patients and healthy controls in current study [Table 3]. Above observations may justify superior efficacy of biologic therapies in psoriasis treatment.
The limitations of present study include relatively small number of subjects included, and that evaluations were performed on peripheral blood only, not in psoriatic-changed skin. We did not perform separate analyzes for subjects on different biologic drugs due to small number of subjects included into the study. Further research should be conducted on larger population of patients with respect to different therapies received.
5. Conclusions
Our results confirm that PD-1/PD-L1 pathway disturbances are observed in subjects with psoriasis and may play an important role in development of the disease. Biologic therapy may reverse observed abnormalities, which may be one of the factors explaining their excellent efficacy in the treatment of disease. Further research is needed on larger populations to fully explain results observed.
Author Contributions
M.A.; writing—original draft preparation, writing—review and editing, investigation, J.B.; writing—review and editing, formal analysis, D.R.; formal analysis, A.M.S.; review, D.K.; supervision, review
Funding
This research received no external funding
Data Availability Statement
All data presented in this study are reported in this manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Armstrong, A.W.; Read, C. Pathophysiology, clinical presentation, and treatment of psoriasis: A review. JAMA 2020, 323, 1945–1960. [Google Scholar] [CrossRef] [PubMed]
- Adamczyk, M.; Krasowska, D. PD1/PD-L1 pathway in psoriasis and psoriatic arthritis: a review. Postepy Dermatol Alergol. 2021, 38, 925–930. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Chang, C.; Lu, Q. The inflammatory response in psoriasis: A comprehensive review. Clin Rev Allergy Immunol. 2016, 50, 377–389. [Google Scholar] [CrossRef] [PubMed]
- Parry, R.V.; Chemnitz, J.M.; Frauwirth, K.A.; Lanfranco, A.R.; Braunstein, I.; Kobayashi, S.V; Linsley, P.S.; Thompson, C.B.; Riley, J.L. CTLA-4 and PD-1 receptors inhibit T-cell activation by distinct mechanisms. Mol Cell Biol. 2005, 25, 9543–9553. [Google Scholar] [CrossRef] [PubMed]
- Bonigen, J.; Raynaud-Donzel, C.; Hureaux, J.; Kramkimel, N.; Blom, A; Jeudy, G. ; Breton, A.L.; Hubiche, T.; Bedane, C.; Legoupil, D.; et al. Anti-PD1-induced psoriasis: a study of 21 patients. J Eur Acad Dermatol Venereol. 2017, 31, e254–e257. [Google Scholar] [CrossRef] [PubMed]
- Bartosińska, J.; Zakrzewska, E.; Król, A.; Raczkiewicz, D.; Purkot, J.; Majdan, M.; Krasowska, D.; Chodorowska, G.; Giannopoulos, K. Differential expression of programmed death 1 (PD-1) on CD4+ and CD8+ T cells in rheumatoid arthritis and psoriatic arthritis. Pol Arch Intern Med. 2017, 22, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Bartosińska, J.; Purkot, J.; Kowal, M.; Michalak-Stoma, A.; Krasowska, D.; Chodorowska, G.; Giannopoulos, K. The expression of selected molecular markers of immune tolerance in psoriatic patients. Adv Clin Exp Med. 2018, 27, 721–725. [Google Scholar] [CrossRef] [PubMed]
- Mahil, S.K.; Ezejimofor, M.C.; Exton, L.S.; Manounah, L.; Burden, A.D.; Coates, L.C.; de Brito, M.; McGuire, A.; Murphy, R.; et al. Comparing the efficacy and tolerability of biologic therapies in psoriasis: an updated network meta-analysis. Br J Dermatol. 2020, 183, 638–649. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, T.; Wang, J. PD-1/PD-L pathway and autoimmunity. Autoimmunity 2005, 38, 353–357. [Google Scholar] [CrossRef]
- Peled, M.; Strazza, M.; Azoulay-Alfaguter, I.; Silverman, G.J.; Scher, J.U.; Mor, A. Analysis of Programmed Death-1 in Patients with Psoriatic Arthritis. Inflammation. 2015, 38, 1573–1579. [Google Scholar] [CrossRef]
- Raptopoulou, A.P.; Bertsias, G.; Makrygiannakis, D.; Verginis, P.; Kritikos, I.; Tzardi, M.; Klareskog, L; Catrina, A. I.; Sidiropoulos, P.; Boumpas, D.T. The programmed death 1/programmed death ligand 1 inhibitory pathway is up-regulated in rheumatoid synovium and regulates peripheral T cell responses in human and murine arthritis. Arthritis Rheum. 2010, 62, 1870–1880. [Google Scholar] [CrossRef]
- Sibaud, V.; Meyer, N.; Lamant, L.; Vigarios, E.; Mazieres, J.; Delord, J.P. Dermatologic complications of anti-PD-1/PD-L1 immune checkpoint antibodies. Curr Opin Oncol. 2016, 28, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Imai. Y.; Ayithan, N.; Wu, X.; Yuan, Y.; Wang, L.; Hwang, S.T. Cutting Edge: PD-1 Regulates Imiquimod-Induced Psoriasiform Dermatitis through Inhibition of IL-17A Expression by Innate γδ-Low T Cells. J Immunol. 2015, 15, 421–425. [Google Scholar] [CrossRef]
- Bommarito, D.; Hall, C.; Taams, L.S.; Corrigall, V.M. Inflammatory cytokines compromise programmed cell death-1 (PD-1)-mediated T cell suppression in inflammatory arthritis through up-regulation of soluble PD-1. Clin Exp Immunol. 2017, 188, 455–466. [Google Scholar] [CrossRef]
- Bartosińska, J.; Zakrzewska, E.; Raczkiewicz, D.; Purkot, J.; Michalak-Stoma, A.; Kowal, M.; Krasowska, D.; Chodorowska, G.; Giannopoulos, K. Suppressed Programmed Death 1 Expression on CD4+ and CD8+ T Cells in Psoriatic Patients. Mediators Inflamm. 2017, 5385102. [Google Scholar] [CrossRef] [PubMed]
- Bartosińska, J.; Zakrzewska, E.; Purkot, J.; Michalak-Stoma, A.; Kowal, M.; Krasowska, D.; Chodorowska, G.; Giannopoulos, K. Decreased blood CD4+PD-1+ and CD8+PD-1+ T cells in psoriatic patients with and without arthritis. Postepy Dermatol Alergol. 2018, 35, 344–350. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Representative flow cytometry analysis of PD-1 (A, C, E, G, I, K, M, O) and PD-L1 (B, D, F, H, J, L, N, P) expression in patient with psoriasis (A-H) and healthy control (I-P). Pink color – CD3+ T-cells, blue - CD4+ T-cells, red – CD8+ t-cells and purple – CD19+ cells.
Figure 1.
Representative flow cytometry analysis of PD-1 (A, C, E, G, I, K, M, O) and PD-L1 (B, D, F, H, J, L, N, P) expression in patient with psoriasis (A-H) and healthy control (I-P). Pink color – CD3+ T-cells, blue - CD4+ T-cells, red – CD8+ t-cells and purple – CD19+ cells.
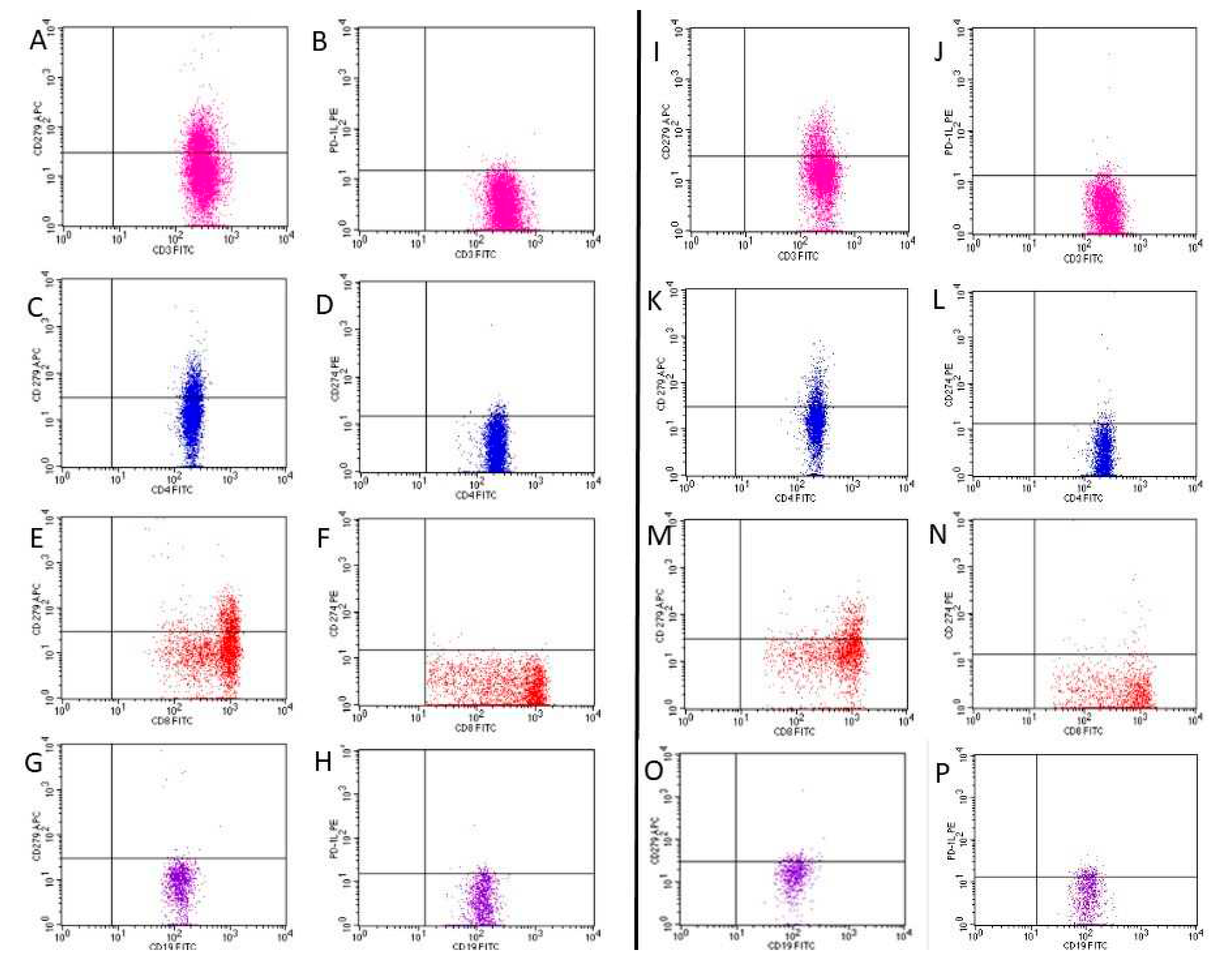

Table 1.
Characteristics of the study subjects with psoriasis (N = 84).
| Characteristics | Unit or Category | Results |
|---|---|---|
| Age, min–max, M | Years | 18–68, 42.8 |
| Gender, n (%) | Male | 60 (71.4) |
| Female | 24 (28.6) | |
| Weight, min–max, M | kg | 47–125, 84.3 |
| Smoking status, n (%) | Non-smokers | 30 (38.0) |
| Smokers | 54 (62.0) | |
| Psoriasis type, n (%) | I | 72 (88.1) |
| II | 12 (11.9) | |
| Duration of psoriasis, min–max, M | Years | 1–50, 20.5 |
| PASI, min–max, M | 5.5-47.0, 17.5 | |
| BSA, min–max, M | 6-80.0, 28.6 | |
| DLQI, min–max, M | 6-30, 17.4 | |
| PsA, n (%) | Yes | 27 (30.9) |
Table 2.
Set of monoclonal antibodies and fluorochromes used to perform lymphocyte surface antigen expression studies.
Table 2.
Set of monoclonal antibodies and fluorochromes used to perform lymphocyte surface antigen expression studies.
| Specificity | Fluorochrome | Producer |
|---|---|---|
| Mouse anti human- CD3 | FITC | BD Biosciences, USA |
| Mouse anti human-CD4 | FITC | BD Biosciences, USA |
| Mouse anti human-CD8 | FITC | BD Biosciences, USA |
| Mouse anti human-CD19 | FITC | BD Biosciences, USA |
| Mouse anti human-CD279 | APC | BD Biosciences, USA |
| Mouse anti human -CD274 | PE | BD Biosciences, USA |
Table 3.
A comparison of percentage rates of PBMCs expressing PD-1 and PD-L1 between psoriatic patients (N=84) and control group (N=29).
Table 3.
A comparison of percentage rates of PBMCs expressing PD-1 and PD-L1 between psoriatic patients (N=84) and control group (N=29).
| PBMC subtype | Psoriasis | Control | p |
| Median (IQR) | Median (IQR) | ||
| CD3/PD1 | 13.78 (11.03-18.42) | 17.26 (14.51-21.00) | 0.021 |
| CD3/PDL1 | 1.23 (0.74-2.72) | 3.26 (1.67-8.20) | <0.001 |
| CD4/PD1 | 13.58 (9.94-17.46) | 18.10 (13.77-25.25) | 0.002 |
| CD4/PDL1 | 2.14 (1.14-4.49) | 4.30 (3.28-5.28) | 0.001 |
| CD8/PD1 | 13.70 (9.78-17.32) | 14.90 (8.80-18.61) | 0.576 |
| CD8/PDL1 | 0.58 (0.28-1.57) | 1.72 (0.87-3.10) | <0.001 |
| CD19/PD1 | 2.48 (1.44-4.34) | 10.65 (6.14-12.20) | <0.001 |
| CD19/PDL1 | 5.94 (1.39-11.11) | 10.95 (4.67-20.00) | 0.002 |
p for U Mann-Whitney test, IQR – interquartile range. Statistically significant differences in bold.
Table 4.
Correlations of PD-1 and PD-L1 expression on different PBMC with PASI, BSA and duration of psoriasis.
Table 4.
Correlations of PD-1 and PD-L1 expression on different PBMC with PASI, BSA and duration of psoriasis.
| PBMC subtype | PASI | BSA | Duration of psoriasis | |||
| r | p | r | p | r | p | |
| CD3/PD-1 | -0.172 | 0.119 | -0.150 | 0.173 | 0.096 | 0.390 |
| CD3/PD-L1 | -0.053 | 0.634 | -0.045 | 0.683 | -0.049 | 0.661 |
| CD4/PD-1 | -0.051 | 0.648 | -0.083 | 0.455 | 0.218 | 0.049 |
| CD4/PD-L1 | -0.013 | 0.908 | 0.035 | 0.750 | -0.106 | 0.343 |
| CD8/PD-1 | -0.150 | 0.174 | -0.126 | 0.253 | 0.148 | 0.186 |
| CD8/PD-L1 | 0.124 | 0.263 | -0.146 | 0.187 | 0.005 | 0.963 |
| CD19/PD-1 | -0.006 | 0.960 | -0.017 | 0.876 | 0.052 | 0.642 |
| CD19/PD-L1 | -0.015 | 0.892 | 0.211 | 0.054 | -0.079 | 0.483 |
Statistically significant differences in bold.
Table 5.
A comparison of percentage rates of PBMCs expressing PD-1 and its ligands in psoriatic patients before and during treatment with biologic drugs (N=28).
Table 5.
A comparison of percentage rates of PBMCs expressing PD-1 and its ligands in psoriatic patients before and during treatment with biologic drugs (N=28).
| PBMC subtype | Before treatment | During treatment | p |
| Median (IQR) | Median (IQR) | ||
| CD3/PD1 | 13.59 (10.08-20.77) | 13.72 (9.32-16.24) | 0.078 |
| CD3/PDL1 | 1.33 (0.92-2.36) | 3.74 (1.85-11.11) | 0.002 |
| CD4/PD1 | 15.64 (10.00-17.69) | 12.11 (9.78-16.32) | 0.471 |
| CD4/PDL1 | 2.11 (1.43-3.37) | 3.1 (1.42-6.03) | 0.428 |
| CD8/PD1 | 14.73 (10.04-21.10) | 12.84 (7.00-15.73) | 0.041 |
| CD8/PDL1 | 0.59 (0.28-1.36) | 1.65 (0.63-5.84) | 0.006 |
| CD19/PD1 | 3.74 (1.79-4.36) | 2.91 (1.14-6.11) | 0.737 |
| CD19/PDL1 | 4.77 (1.77-10.00) | 9.6 (2.67-13.39) | 0.302 |
p for Wilcoxon rank test, IQR – interquartile range. Statistically significant differences in bold.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



