
Submitted:
24 May 2023
Posted:
26 May 2023
You are already at the latest version
Abstract
Tumor-associated macrophages (TAMs) play critical roles in the tumor microenvironment (TME), where they are recruited by signals released by cancer cells. Although they have great potential as therapeutic targets for cancer treatment, the dual roles of TAMs in promoting or inhibiting tumor growth, invasion, and metastasis make their function in cancer progression complex. In this review, we provide an overview of the current understanding of TAMs, including their phenotypic diversity, regulatory signaling pathways, and interactions with other cells in the TME. We also discuss the challenges related to the standard isolation protocols of TAMs, inconsistent research results, and translation of TAM knowledge into clinical applications. Additionally, we review the status of clinical trials involving TAMs and potential strategies to overcome the limitations. The future direction of TAM research should focus on developing more targeted therapies that specifically regulate TAM function and non-invasive methods for monitoring TAM activity in cancer patients. A comprehensive understanding of the complex role of TAMs in cancer may lead to the development of more effective treatments and improved outcomes for cancer patients.
Keywords:
Tumor-associated macrophages (TAM)
; Tumor microenvironment (TME)
; Cytokine
; Immunosuppression
; Pro-tumor functions
; Anti-tumor functions
; Clinical application.
1. Introduction
Tumor-associated macrophages (TAMs) are a type of macrophages (Mφ) that contribute to the formation of the tumor microenvironment (TME) and have critical and at least double-faced roles in cancer progression [1,2,3]. Although some of the TAM sub-populations exhibit anti-tumor properties, others promote tumor growth and immune evasion [4,5,6]. These characteristics make them a challenging target for cancer therapy. Although significant progress has been made in understanding TAMs’ functions and mechanisms, there are still some challenges remaining, which include identifying different TAM subpopulations and developing targeted therapies [7]. The interactions of TAMs with other cells within the TME increase the difficulty and challenge of developing effective therapies [8]. In addition, the plasticity and adaptability of TAMs in response to different stimuli make it difficult to predict the outcome of therapies targeting these cells [9]. However, understanding the biology and function of TAMs in the TME is essential for the development of effective cancer treatments.
Targeting TAMs offers a promising avenue to develop novel cancer therapies. Promising results have been seen in preclinical and clinical studies of therapies that inhibit TAM recruitment, depletion, or reprograming TAM polarization [8,10,11,12]. Since TAMs have been shown to be involved in all stages of cancer progression, from initiation to metastasis and drug resistance [9,13], a better and deeper understanding of their biology and function in the TME is essential for the development of targeted cancer therapies. Such therapies have demonstrated efficacy in reducing tumor growth, enhancing response to chemotherapy, and improving patient outcomes.
This review provides a comprehensive and up-to-date overview of the TAMs with multifaceted roles in cancer progression and treatment. It covers TAM polarization, TAM-derived cytokines, chemokines, and TAM metabolism, as well as the potential of combination therapy together with chemotherapy, radiation therapy, or immunotherapy to maximize the effectiveness of TAM-targeted therapies.
TAMs play a critical and complex role in cancer progression, with some subpopulations exhibiting anti-tumor properties while others promote tumor growth and immune evasion. Therefore, it is essential to understand the mechanisms underlying this complex interplay between TAMs and the TME for the development of effective cancer immunotherapies targeting TAMs.
This review aims to provide readers including researchers and clinicians, etc. a better and deeper understanding of the paradoxical functions of TAMs, the significance of TAMs in cancer progression, the importance of developing TAM-targeted therapies, and recent advances, controversies, and translational challenges in cancer immunotherapy. It will contribute to advancing knowledge in the field, highlight the current challenges and future directions of TAM-targeted therapies, and identify areas for further research.
2. TAMs in Cancer Progression
TAMs are immune cells found within the TME of various types of cancer [5]. These cells are derived from circulating monocytes, which can differentiate into macrophages when receiving signals from damaged or infected tissues [14]. Cancer cells often release signals that attract monocytes to the tumor site, where they differentiate into TAMs [14,15]. TAMs are a heterogeneous cell population that can have both pro-tumor and anti-tumor effects, which depend on their phenotype and the specific cytokine environment in the TME [1,16]. Pro-tumorigenic TAMs promote cancer growth and progression by regulating angiogenesis, remodeling the extracellular matrix (ECM), inhibiting the immune system, and phagocytosing cancer cells [17,18]. In contrast, anti-tumorigenic TAMs can limit tumor progression and promote anti-tumor immunity [19,20]. In addition, TAMs can influence the efficacy of chemotherapy drugs and other therapies, and their presence can impact patient prognosis [1,21]. Therefore, TAMs are a critical component of the TME and play a vital role in cancer development, progression, and response to therapy. Understanding the origin and function of TAMs is crucial for the development of novel therapies that target these cells and improve cancer outcomes. The multifaceted and complex role of TAMs in cancer progression underscores the importance of further research in this field [15,22].
2.1. Classification of Macrophages
Macrophages can undergo polarization and differentiate into two main subtypes: classically activated macrophages (M1-type) and alternatively activated macrophages (M2-type) [23,24]. M1-type macrophages are associated with inflammation and are typically induced by interferon-gamma (IFN-γ) and lipopolysaccharide (LPS) [5,25,26]. They play a vital role in the anti-tumor immune response by producing pro-inflammatory cytokines like interleukin-12 (IL-12) and tumor necrosis factor-alpha (TNF-α). Additionally, M1-type macrophages contribute to antigen presentation, phagocytosis, and the elimination of tumor cells [26,27,28].
On the other hand, M2-type macrophages are abundant in the TME and are associated with anti-inflammatory responses [5,26]. They are mainly induced by interleukin-4 (IL-4), and IL-13 [29,30], and perform functions that promote tumor cell survival, angiogenesis, and metastasis [31,32]. M2 macrophages can be further categorized into four subtypes based on cell surface markers, secreted cytokines, and biological functions [33].
M2a macrophages exhibit a pro-tumor phenotype and are induced by Th2 cytokines, particularly IL-4 and IL-13 [33]. They produce anti-inflammatory cytokines such as IL-10 and transforming growth factor-beta (TGF-β), which contribute to inflammation resolution, wound repair, and tissue remodeling. M2b macrophages, also known as regulatory macrophages (Mregs), are induced by toll-like receptor (TLR) agonists, immune complexes, and cytokines like IL-1β [34]. They have a mixed phenotype and can be pro- or anti-tumor, producing various cytokines involved in immune regulation and tissue repair [33,34]. M2c macrophages, also known as inactivated macrophages, are induced by glucocorticoids, IL-10, and TGF-β [33]. They produce anti-inflammatory cytokines (i.e., IL-10, TGF-β), which help inhibit immune cell activation and promote the differentiation of Treg. Additionally, M2c macrophages contribute to the clearance of apoptotic cells, preventing autoimmune reactions [35,36]. M2d macrophages are a unique subtype induced by exposure to adenosine, uric acid crystals, and immune complexes [37]. They have both pro- and anti-inflammatory properties and are induced by TLR ligands and A2 adenosine receptor (A2R) agonists, or by IL-6 [38]. M2d macrophages contribute to tumor angiogenesis, growth, and metastasis, making them a crucial player in cancer progression [39,40].
It is important to note that the phenotype of macrophages can switch in response to the TME. For example, M1 macrophages can be converted to M2 phenotype in response to tumor-derived factors [41,42]. In addition, the phenotype of TAMs can vary depending on the stage of tumor progression and the location of the tumor in the body. In short, both subtypes play different roles in the TME. M1 macrophages contribute to the anti-tumor immune response, while M2 macrophages promote tumor cell survival and angiogenesis [5,32,43,44].
2.2. Pro-tumor functions of TAMs
TAMs play a multifaceted and significant role in promoting tumor growth and progression through several pro-tumor functions such as immunosuppression, angiogenesis, ECM remodeling, and metastasis [45,46]. TAMs can promote angiogenesis by producing pro-angiogenic factors such as vascular endothelial growth factor (VEGF), which is essential for tumor growth and metastasis [47]. They can also inhibit the activity of immune cells by producing immunosuppressive cytokines such as interleukin-10 (IL-10) and TGF-β, as well as inhibiting the function of cytotoxic T cells (CTLs), natural killer cells (NK cells), and dendritic cells (DCs) [46,48].
In addition, TAMs can promote tumor growth and progression through ECM remodeling through secretases (e.g., matrix metalloproteinases, MMPs) that break down ECM components, creating space for tumor growth and invasion [49,50,51]. They can also deposit new ECM components, such as fibronectin and tenascin, which promote tumor growth and invasion [52,53,54]. In addition, TAMs secrete growth factors such as epidermal growth factor (EGF) and platelet-derived growth factor (PDGF) that stimulate tumor cell growth and survival [5,46,55,56]. In addition, TAMs can also stimulate the proliferation of cancer cells by releasing lactate, which stimulates the growth of cancer cells [57,58].
TAMs promote tumor growth and progression through metastasis by secreting pro-tumor factors that can promote several steps of the metastatic cascade, including invasion, internal infiltration, survival in the circulation, extravasation, and colonization of distant organs [15,55,59]. Additionally, TAMs can create a favorable microenvironment for metastatic tumor cells by promoting angiogenesis and inhibiting the immune system, further enhancing the survival and growth of tumor cells in distant areas [1,15,45,60].
TAMs not only promote tumor growth and progression through pro-tumor functions, but they can also suppress the immune response in the TME [1,22,45,55]. They can inhibit the activity of T cells and other immune cells by secreting cytokines such as TGF-β, IL-10, and prostaglandin E2 (PGE2) [11,61,62]. Additionally, TAMs can promote the activity of Tregs and myeloid-derived suppressor cells (MDSCs) by secreting cytokines such as IL-10, CCL22, IL-6, and GM-CSF [63,64]. Finally, TAMs can induce immune checkpoint molecules such as PD-L1, which can inhibit the activity of T cells by binding to PD-1 receptors on T cells, resulting in T cell exhaustion and dysfunction [65,66]. Modulating these mechanisms is a promising approach to developing new cancer therapies. However, the heterogeneity of TAMs [22,67,68] and the lack of standardized protocols for isolating TAMs from the TME have resulted in inconsistent research results and a limited clinical translation [69,70]. Addressing these issues could lead to a better understanding of TAMs’ complex role in cancer progression, which may ultimately lead to the development of more effective treatments and improved outcomes for cancer patients.
2.3. Anti-tumor functions of TAMs
TAMs can exhibit anti-tumor functions by promoting inflammation, recruiting other immune cells into the TME, and directly killing tumor cells through the phagocytosis [1,5,11,28,71]. Typically, M1-typeTAMs are associated with anti-tumor functions, and their activation leads to increased production of pro-inflammatory cytokines and chemokines, promoting an immune response to tumors [9,72,73]. In addition, TAMs, as antigen-presenting cells (APCs), can directly present tumor antigens to T cells, activating them and inducing an anti-tumor immune response [74,75]. The anti-tumor functions of TAMs depend on their activation state and the context of the TME [73,76].
Inducing TAMs to switch from a pro-tumor to an anti-tumor phenotype is a key strategy for cancer immunotherapy. To achieve this purpose, several methods have been developed, including targeting TAM recruitment, reprogramming TAMs, targeting TAM metabolism, and using combination therapies [5,8,77,78]. Moreover, combining different immunotherapeutic agents can enhance their anti-tumor effects by targeting multiple aspects of the TME, including TAMs [45,79].
Although TAMs typically promote tumor growth by releasing cytokines and growth factors that stimulate angiogenesis and suppress anti-tumor immune responses [1,5,45,55], under certain conditions, they can also promote tumor cell apoptosis or programmed cell death (i.e., apoptosis). TAMs promote tumor cell apoptosis by inducing the expression of death receptors on the surface of cancer cells [71,80,81,82]. TAMs can also release cytotoxic molecules such as reactive oxygen species (ROS) and nitric oxide (NO), which can directly induce apoptosis in cancer cells [5,9,27]. TAMs can inhibit pro-survival signaling pathways in cancer cells, such as the Akt/mTOR pathway, and sensitize cancer cells to apoptosis [13,83,84].
Furthermore, TAMs can inhibit tumor growth by inducing an anti-tumor immune response and directly inhibiting tumor cell proliferation [85,86]. As APCs, TAMs induce an anti-tumor immune response by presenting tumor antigens to T cells and activating them [75]. They can also secrete cytokines that further activate T cells and stimulate anti-tumor immune responses [55,87]. In addition, TAMs can secrete cytokines that activate pro-apoptotic signaling pathways in cancer cells, leading to cell cycle arrest or apoptosis [10,71,79]. TAMs can also compete with cancer cells for nutrients and oxygen, leading to nutrient and oxygen deprivation, thereby inhibiting tumor growth [45,88].
Moreover, TAMs can promote tissue remodeling by promoting the differentiation of fibroblasts into myofibroblasts and the deposition of ECM, resulting in decreased tumor growth [89]. TAMs can inhibit angiogenesis, which is necessary for tumor growth and metastasis, by secreting anti-angiogenic factors that inhibit the proliferation and migration of endothelial cells and inhibit angiogenesis [47,90].
In summary, TAMs can inhibit tumor growth through various mechanisms, including induction of anti-tumor immune responses, direct inhibition of tumor cell proliferation, tissue remodeling, and inhibition of angiogenesis. However, the balance between pro-tumor and anti-tumor functions of TAMs is complex and context-dependent, and further research is needed to better understand the mechanisms of TAM-mediated tumor growth inhibition.
3. Regulatory Signaling Pathways of TAMs in the TME
TAMs exhibit a dual role in the TME. On one hand, they can promote tumor growth and suppress anti-tumor immune responses. On the other hand, they can also inhibit tumor growth, and promote anti-tumor immunity. The balance between these two roles is influenced by various factors, such as the activation state and polarization of TAMs, the stage and type of cancer, and the composition of the TME [1,18,45,91,92]. Therefore, it is essential to comprehend the intricate interplay between TAMs and the TME to develop effective cancer immunotherapies that target TAMs.
3.1. Regulation of TAM phenotype and function
The regulation of TAM phenotypes and functions is complex and influenced by various factors in the TME. A couple of factors affect TAMs, which include cytokines, hypoxia, metabolism, and ECM [93,94,95,96]. Cytokines present in the TME can activate TAMs towards either M1 or M2 phenotype [18,32,55]. For example, IFN-γ and lipopolysaccharide (LPS) can activate TAMs towards an M1 phenotype, which is associated with anti-tumor immunity [70,97,98]. Conversely, interleukin-4 (IL-4) and interleukin-13 (IL-13) can polarize TAMs towards M2 phenotype, which promotes tumor growth [99,100,101,102]. Hypoxia or low oxygen levels promotes the polarization of TAMs towards an M2 phenotype and enhance their immunosuppressive function [103,104]. TAMs also exhibit a unique metabolic profile that enables them to promote tumor growth. Targeting key metabolic pathways in TAMs, such as glucose and lipid metabolism, can potentially impair their function and promote anti-tumor immunity [105,106]. Additionally, the ECM in the TME can affect TAM phenotype and function by influencing their migration and adhesion to tumor cells. ECM remodeling can promote the infiltration of TAMs into the TME and also enhance their immunosuppressive function [10,11,17,107].
Understanding the regulation of TAMs is important for the development of effective cancer immunotherapies that target TAMs, potentially shifting their phenotype towards an anti-tumor profile and enhancing their anti-tumor activity.
3.2. Crosstalk between TAMs and other cell types in the TME
TAMs can interact with immune cells, cancer cells, and stromal cells in the TME through various mechanisms, including cytokine secretion and cell-cell contact [108,109]. This crosstalk between TAMs and other cells in the TME can affect the polarization, and function of TAMs, as well as the overall composition of TME. Therefore, targeting TAMs in combination with other immune or stromal cells is a potential strategy to improve the efficacy of cancer immunotherapies [45,79]. TAMs can interact with cancer cells either directly or indirectly, promoting tumor growth and metastasis by enhancing angiogenesis, immune suppression, and invasion [15,55,74]. TAMs can suppress T cell activity and promote T cell exhaustion by producing immunosuppressive cytokines and by presenting tumor antigens in a manner that inhibits T cell activation [65,110]. However, TAMs can also promote T-cell activation and infiltration in the TME by secreting chemokines and cytokines [5,8,15,19]. TAMs can interact with cancer-associated fibroblasts (CAFs) to promote ECM remodeling and facilitate tumor invasion. Additionally, TAMs can also promote the activation of CAFs, resulting in increased production of cytokines and growth factors that promote tumor growth and metastasis [89,111]. In addition, TAMs can promote angiogenesis by secreting pro-angiogenic factors such as vascular endothelial growth factor (VEGF) and by directly interacting with endothelial cells to promote their proliferation and migration [47,55,112]. Finally, TAMs can interact with myeloid-derived suppressor cells (MDSCs) in the TME, leading to immune suppression and promote tumor growth. This interaction involves the secretion of cytokines and growth factors by TAMs that recruit and activate MDSCs, ultimately resulting in the inhibition of T cell activity and the promotion of tumor growth [63,113,114].
Therefore, understanding the complex crosstalk between TAMs and other cell types in the TME is essential to optimize current therapies and improve patient outcomes. The development of effective cancer immunotherapies targeting TAMs and their interactions with other cells in the TME may lead to more successful outcomes for cancer patients.
3.3. The factors in TME affecting the polarization of TAM
Several factors in the TME can affect the recruitment and polarization of TAMs. CD8+ T cells that secrete IFN-γ induce TAM polarization towards an M1-phenotype, while Tregs promote TAM recruitment and polarization towards an M2-phenotype. In addition, the immune checkpoint molecule PD-L1 is expressed on tumors and can interact with PD-1 on TAMs, impacting TAM polarization and function [5,10,26,47,115]. In addition, hypoxia, inflammatory cytokines, ECM components, and metabolic stress all affect the polarization of TAMs [93,104]. Hypoxia induces the expression of hypoxia-Inducible Factor (HIF) and other transcription factors that promote the secretion of pro-angiogenic factors and immunosuppressive cytokines, polarizing TAMs towards a pro-tumor phenotype [93,104,116]. Inflammatory cytokines such as IFN-γ and TNF-α polarize TAMs towards an anti-tumor (M1) phenotype, while potent Th2 cytokines such as IL-4 and Il-13, and hypoxia can polarize macrophages towards the TAM2 phenotype. [9,21,32,104]. Therefore, targeting Th2 cytokines or their downstream signaling pathways is a potential strategy for inhibiting the polarization of TAMs towards the TAM2 phenotype and reducing their pro-tumor functions. Doxycycline, an antibiotic, has been shown to inhibit TAM2 polarization and reduce tumor growth in preclinical models [117]. ECM components, including hyaluronan and collagen, promote the expression of matrix metalloproteinases (MMPs) and other enzymes that remodel the ECM, promoting tumor invasion and influencing TAM polarization [17,118,119].
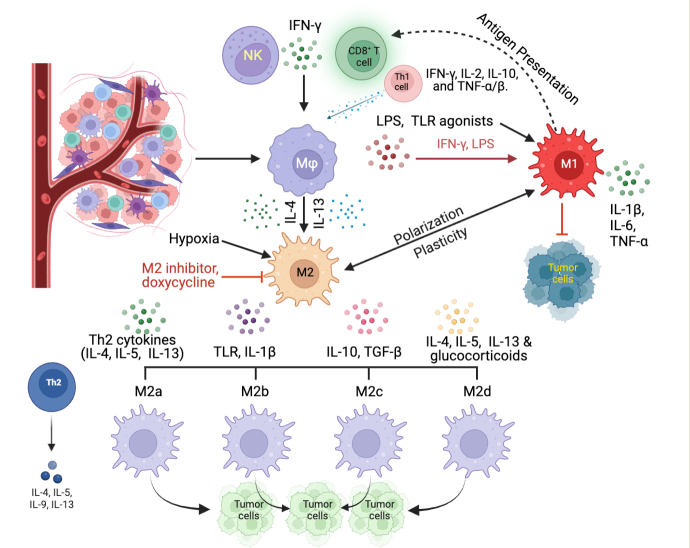
Figure 1.
Polarization and function of M1 and M2 macrophages in the TME. TAMs within the TME are derived from circulating monocytes, which can be stimulated and differentiated into macrophages when receiving signals such as cytokine IFN-γ released from activated CD8+ T cells, NK cells, or lFN-γ, IL-2, IL-10, and TNF-α/β released from Th1 cells (i.e., CD4+ T cells). Macrophages can be activated by LPS, TLR agonists released from bacteria, or damaged cells towards the TAM1 phenotype. Potent Th2 cytokines such as IL-4 and IL-13, and hypoxia can polarize macrophages towards the TAM2 phenotype. TAM1 polarization is induced by IFN-γ and LPS and is associated with a pro-inflammatory response. TAM1 cells produce pro-inflammatory cytokines (e.g., IL-1β, IL-6, TNF-α, etc.), which promote tumor cell death. TAM2 polarization is driven by IL-4 and IL-13 and is associated with an anti-inflammatory response. TAM2s produce anti-inflammatory cytokines (e.g., IL-10) and TGF-β, which suppress immune responses and promote angiogenesis.
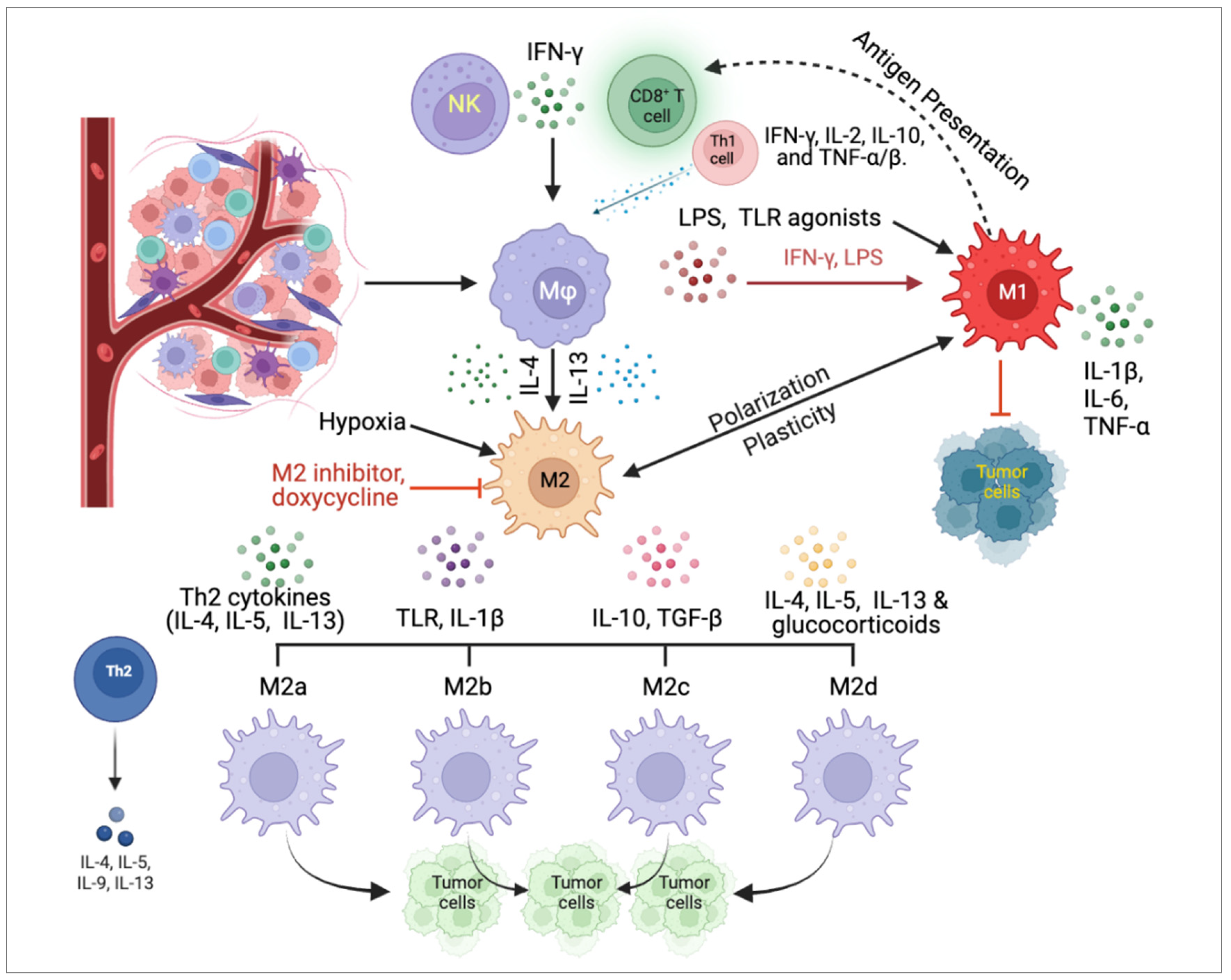
Figure 1.
Polarization and function of M1 and M2 macrophages in the TME. TAMs within the TME are derived from circulating monocytes, which can be stimulated and differentiated into macrophages when receiving signals such as cytokine IFN-γ released from activated CD8+ T cells, NK cells, or lFN-γ, IL-2, IL-10, and TNF-α/β released from Th1 cells (i.e., CD4+ T cells). Macrophages can be activated by LPS, TLR agonists released from bacteria, or damaged cells towards the TAM1 phenotype. Potent Th2 cytokines such as IL-4 and IL-13, and hypoxia can polarize macrophages towards the TAM2 phenotype. TAM1 polarization is induced by IFN-γ and LPS and is associated with a pro-inflammatory response. TAM1 cells produce pro-inflammatory cytokines (e.g., IL-1β, IL-6, TNF-α, etc.), which promote tumor cell death. TAM2 polarization is driven by IL-4 and IL-13 and is associated with an anti-inflammatory response. TAM2s produce anti-inflammatory cytokines (e.g., IL-10) and TGF-β, which suppress immune responses and promote angiogenesis.
Finally, metabolic stress, such as nutrient deprivation and acidosis, can alter TAM metabolism and promote the secretion of pro-tumor cytokines and growth factors, which also influence TAM polarization [104,120,121]. Therefore, a better and deeper understanding of the diverse TME factors that influence TAM polarization is essential for the development of TAM-targeted therapies that are capable of modulating TAM function and improving patient outcomes.
4. Challenges in Clinical Applications of TAMs
The clinical applications of TAMs face several challenges. TAMs exhibit high levels of heterogeneity, both within tumors and among patients, this heterogeneity makes it challenging to develop effective therapeutic strategies that target all TAM populations. In addition, TAMs exhibit plasticity, which means they can change their phenotype and functions in response to various stimuli, this plasticity makes it difficult to develop targeted therapies, effectively modulating TAM function. The interactions between TAMs and other cells in the TME are complex and multifaceted, which poses another challenge to the development of TAM-targeted therapies [8,22,45]. Therefore, it is crucial to identify reliable biomarkers that can predict response to TAM-targeted therapies, but this is challenging due to the heterogeneity of TAM populations and the complex interactions between TAMs and other cells in the TME [11,122]. In addition, targeting TAMs is further complicated by their location within the TME and the presence of physical barriers, such as the blood-brain barrier (BBB) [123]. Consequently, it is necessary to continue research and development in the field of TAM-targeted therapies, with a particular focus on identifying reliable biomarkers, understanding the complex interactions between TAMs and other cells in the TME, and developing effective drug delivery strategies.
4.1. Heterogeneity and plasticity of TAMs
TAMs are a heterogeneous population of immune cells that can exhibit a range of functional and phenotypic characteristics [5,15,124]. These heterogeneities include different activation states, tissue localization, genetic and epigenetic variability, plasticity, and functional heterogeneity [7,13,67,125]. The two major subsets of TAMs are M1-type macrophages with pro-inflammatory and anti-tumor properties and M2-type macrophages with anti-inflammatory and pro-tumor properties [5,11,32,126]. TAMs can be found in various regions within the TME and may exhibit genetic and epigenetic variability that can influence their phenotype and function [127,128]. TAMs are also highly plastic and can switch between different activation states in response to environmental cues, which demonstrates a wide range of functional heterogeneity [11,16,89]. Hence, comprehending the heterogeneity of TAMs is essential for the development of effective cancer therapies that target these cells.
4.2. Limited efficacy of TAM-targeted therapies
TAMs are an attractive target for cancer therapy, but there are several limitations that affect the efficacy of TAM-targeted therapies [1,8,9,129]. As described before, TAMs is a heterogeneous cell population that exhibits different activation states, tissue localizations, and functional properties [7,11,67,130]. They are also highly plastic and can switch between different activation states, which can limit the effectiveness of therapies that target a specific activation state of TAMs [131,132,133]. Therapeutic penetration into the hypoxic and nutrient-poor regions of the TME where TAMs are often located can also be restricted, thereby reducing drug exposure and efficacy [112,134,135]. Targeting TAMs may induce resistance mechanisms in cancer cells, leading to the development of more aggressive and therapy-resistant tumors [10,19,136]. In addition, targeting TAMs may affect the function of macrophages in normal tissues, leading to potential toxicity and adverse effects [1,10,11,137]. Furthermore, the absence of dependable biomarkers poses a significant challenge in accurately predicting the response to TAM-targeted therapies [93,133,138]. Overcoming these limitations will be essential to enhance the efficacy of TAM-targeted therapies and unlock their full potential in cancer treatment.
4.3. Lack of reliable biomarkers for TAM identification and characterization
TAMs exhibit a high degree of heterogeneity and require biomarkers that can accurately distinguish TAMs from other immune cells in the TME [7,40,67,68]. In addition, identifying biomarkers that can distinguish between different subsets of TAMs (such as M1-type and M2-type) could help to guide the development of TAM-targeted therapies that selectively modulate specific TAM subsets [5,129,139]. The development of non-invasive imaging and diagnostic techniques that can identify and quantify TAMs in tumors could also help to develop and monitor TAM-targeted therapies [140,141,142]. The identification of reliable biomarkers for TAMs is essential to improve our understanding of the role of TAMs in cancer progression and the development of effective TAM-targeted therapies.
5. Standardizing TAM Isolation Protocols
TAMs are a diverse population of immune cells that reside within the TME and play a key role in tumor progression and treatment response [9,126]. Isolation of TAMs from the TME is an important step in understanding their phenotype and function and developing effective cancer therapies [5,69]. The following summarizes some current methods for TAM isolation. (1) The enzymatic digestion method involves isolating cells from the TME by digesting the ECM with enzymes such as collagenase, hyaluronidase, and DNase. CD14, CD11b, HLA-DR, CD163, and CX3CR1 antigens are used to identify human resident macrophages and TAMs [69]. (2) The resulting cell suspension for TAMs can then be further enriched for TAMs using magnetically activated cell sorting (MACS) using CD14 microbeads (Miltenyi Biotec GmbH, Bergisch Gladbach, Germany) [143] or fluorescence-activated cell sorting (FACS) based on the expression of TAM-specific markers [144,145,146]. (3) Adhesion-based isolation method takes advantage of the fact that TAMs adhere to plastic or tissue culture plates more strongly than other cells in the TME [147,148]. Tumor tissue is mechanically dissociated and plated on plastic or tissue culture plates, and TAMs are then isolated from the adherent cells using MACS/FACS. (4) Density gradient centrifugation method involves layering the cell suspension from the TME over a density gradient, such as Ficoll-Paque, and centrifuging it [149]. This separates cells based on their density, with TAMs typically found in the low-density fraction. The resulting cell suspension can then be enriched for TAMs using MACS/FACS. (5) Laser capture microdissection (LCM) method involves using a laser to isolate TAMs directly from histological sections of tumor tissue [126,150]. This allows for the isolation of TAMs in their native tissue context but requires specialized equipment and expertise.
Each of the methods mentioned above for TAM isolation has its advantages and disadvantages, and the choice of method depends on the research question and available resources. A combination of these methods can provide a more comprehensive understanding of TAM phenotype and function within the TME. However, the current methods for TAM isolation have several limitations and challenges, which include (1) lack of specificity of some isolation methods that rely on the expression of surface markers not exclusive to TAMs, such as CD11b and F4/80, may lead to contamination of TAM populations with other myeloid cells [151,152], (2) enzymatic digestion of tumor tissue is required by many methods [153,154], which may cause cell damage and alter gene expression profiles, potentially affecting the interpretation of the results, (3) the complexity and heterogeneity of the TME, with multiple cell types and signaling pathways interacting with each other, may not accurately reflect TAM phenotype and function in vivo [126,127,155], (4) technical variabilities, such as differences in tissue digestion and antibody staining, may lead to inconsistencies in the isolation and characterization of TAM populations, (5) some methods such as single-cell sequencing can be costly and time-consuming, limiting their feasibility for large-scale studies. Finally, obtaining tumor tissue for research purposes can pose ethical challenges, especially when it involves invasive procedures or animal models. Therefore, improving the standardization and development of new TAM isolation methods is necessary to address all these potential limitations and overcome these challenges, which will lead to more accurate and reliable findings in TAM research.
6. Clinical Trials Involving TAMs
Currently, clinical trials are investigating the role of TAMs in cancer progression and response to therapy. Table 1 summarizes some ongoing clinical trials involving TAMs according to www.clinicaltrials.gov.
Colony-stimulating factor 1 receptor (CSF1R) is a class III receptor tyrosine kinase that is expressed on TAM and is a promising therapeutic target in Oncology since it is involved in the proliferation and survival of TAMs [156,157]. Inhibitors of CSF1R are being developed and tested in clinical trials for the treatment of various types of cancer, including a Phase 2 clinical trial investigating the CSF1R inhibitor pexidartinib in combination with pembrolizumab for advanced melanoma [11,158,159,160]. There are currently 20 ongoing clinical trials related to CSF1R in cancer patients that are in the recruiting phase. These trials have been summarized in Table 2.
Targeting TAMs through the depletion of CSF1R with drugs may improve the response to chemotherapy and immunotherapy [19,86,161]. Another promising and challenging approach is to reprogram TAMs to an anti-tumor phenotype, which can be achieved by inducing a shift from M2- to M1-type TAMs [5,13,162,163]. M2-type polarization inhibitor drug screens identify drugs that selectively block M2- but not M1-type polarization [102,117]. Clinical trials are investigating the efficacy of targeting TAM-derived cytokines and chemokines to enhance the response to immunotherapy [11,19,20,129]. CAR-T cells that target TAM-specific antigens are also being investigated to eliminate TAMs and enhance the response to the immunotherapy [164,165,166].
Some completed clinical trials have shown that targeting TAMs can improve the response to chemotherapy and that high TAM density is associated with poor prognosis and increased risk of recurrence [86,94,123,167]. Additionally, a Phase 1 clinical trial investigating the combination of an anti-PD-L1 antibody and an anti-CSF1R antibody in patients with advanced solid tumors showed a higher response rate and longer progression-free survival (PFS) compared to the anti-PD-L1 antibody alone [11,168,169,170]. These findings highlight the importance of TAMs in cancer progression and suggest that targeting TAMs may be a promising therapeutic strategy.
7. Conclusions
TAMs are a group of macrophages that can either help or inhibit cancer growth. Targeting TAMs for cancer therapy is challenging because of their complexity and interaction with other cells in the TME [171]. Several clinical trials are exploring strategies to manipulate TAM function. Further research is essential to identify specific TAM subpopulations and develop personalized cancer therapies. TAM-targeted approaches such as inhibition of TAM recruitment, repolarization of TAMs, and targeting TAM-mediated immunosuppression have shown promise. Combination therapy with other cancer treatments may also enhance TAM-targeted therapy. Overall, TAM-targeted therapy has the potential to improve cancer patients’ outcomes and represents a promising area of research in cancer immunotherapy.
8. Future Directions
Based on the current understanding of TAMs, there are several future directions that could be explored to overcome the challenges and limitations discussed in the review. (1), efforts should be made to improve the standardization of TAM isolation protocols to ensure consistency in research results. This could involve the development of standardized protocols and the validation of existing methods to ensure they are reliable and reproducible. (2), there is a need to further investigate the phenotypic diversity of TAMs and their interactions with other cells in the TME [126]. This could involve the use of single-cell analysis techniques and the development of new models that better mimic the TME in vivo. (3), the development of novel therapeutics that target TAMs could be explored. This could involve the identification of specific TAM subpopulations that promote tumor growth and metastasis and the development of drugs that selectively target these cells. (4), clinical trials involving TAM-targeted therapies should be expanded and evaluated rigorously to determine their effectiveness in improving outcomes for cancer patients. This could involve the use of biomarkers to identify patients who are most likely to benefit from TAM-targeted therapies and the development of combination therapies that target TAMs in conjunction with other components of the TME.
Overall, a better and deeper understanding of TAMs and their paradoxical and complex role in cancer progression could lead to the development of more effective treatments and improved outcomes for cancer patients.
Author Contributions
Conceptualization, writing, and editing: S.S., H.M., and W.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
This paper represents the authors’ interpretation of the most recent relevant and latest publications and existing literature on the topic.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Yang, Q.; Guo, N.; Zhou, Y.; Chen, J.; Wei, Q.; Han, M. The role of tumor-associated macrophages (TAMs) in tumor progression and relevant advance in targeted therapy. Acta Pharm Sin B 2020, 10, 2156-2170. [CrossRef]
- Dallavalasa, S.; Beeraka, N.M.; Basavaraju, C.G.; Tulimilli, S.V.; Sadhu, S.P.; Rajesh, K.; Aliev, G.; Madhunapantula, S.V. The Role of Tumor Associated Macrophages (TAMs) in Cancer Progression, Chemoresistance, Angiogenesis and Metastasis - Current Status. Curr Med Chem 2021, 28, 8203-8236. [CrossRef]
- Zhang, J.; Gao, J.; Cui, J.; Wang, Y.; Jin, Y.; Zhang, D.; Lin, D.; Lin, J. Tumor-associated macrophages in tumor progression and the role of traditional Chinese medicine in regulating TAMs to enhance antitumor effects. Front Immunol 2022, 13, 1026898. [CrossRef]
- Noy, R.; Pollard, J.W. Tumor-associated macrophages: From mechanisms to therapy. Immunity 2014, 41, 49-61. [CrossRef]
- Pan, Y.; Yu, Y.; Wang, X.; Zhang, T. Tumor-Associated Macrophages in Tumor Immunity. Front Immunol 2020, 11, 583084. [CrossRef]
- Schupp, J.; Krebs, F.K.; Zimmer, N.; Trzeciak, E.; Schuppan, D.; Tuettenberg, A. Targeting myeloid cells in the tumor sustaining microenvironment. Cell Immunol 2019, 343, 103713. [CrossRef]
- Wu, K.; Lin, K.; Li, X.; Yuan, X.; Xu, P.; Ni, P.; Xu, D. Redefining Tumor-Associated Macrophage Subpopulations and Functions in the Tumor Microenvironment. Front Immunol 2020, 11, 1731. [CrossRef]
- Xiang, X.; Wang, J.; Lu, D.; Xu, X. Targeting tumor-associated macrophages to synergize tumor immunotherapy. Signal Transduct Target Ther 2021, 6, 75. [CrossRef]
- Tan, Y.; Wang, M.; Zhang, Y.; Ge, S.; Zhong, F.; Xia, G.; Sun, C. Tumor-Associated Macrophages: A Potential Target for Cancer Therapy. Front Oncol 2021, 11, 693517. [CrossRef]
- Li, M.; He, L.; Zhu, J.; Zhang, P.; Liang, S. Targeting tumor-associated macrophages for cancer treatment. Cell Biosci 2022, 12, 85. [CrossRef]
- Mantovani, A.; Allavena, P.; Marchesi, F.; Garlanda, C. Macrophages as tools and targets in cancer therapy. Nat Rev Drug Discov 2022, 21, 799-820. [CrossRef]
- Liu, M.; Yang, J.; Xu, B.; Zhang, X. Tumor metastasis: Mechanistic insights and therapeutic interventions. MedComm (2020) 2021, 2, 587-617. [CrossRef]
- Kumari, N.; Choi, S.H. Tumor-associated macrophages in cancer: Recent advancements in cancer nanoimmunotherapies. J Exp Clin Cancer Res 2022, 41, 68. [CrossRef]
- Richards, D.M.; Hettinger, J.; Feuerer, M. Monocytes and macrophages in cancer: Development and functions. Cancer Microenviron 2013, 6, 179-191. [CrossRef]
- Lin, Y.; Xu, J.; Lan, H. Tumor-associated macrophages in tumor metastasis: Biological roles and clinical therapeutic applications. J Hematol Oncol 2019, 12, 76. [CrossRef]
- Vitale, I.; Manic, G.; Coussens, L.M.; Kroemer, G.; Galluzzi, L. Macrophages and Metabolism in the Tumor Microenvironment. Cell Metab 2019, 30, 36-50. [CrossRef]
- Yuan, Z.; Li, Y.; Zhang, S.; Wang, X.; Dou, H.; Yu, X.; Zhang, Z.; Yang, S.; Xiao, M. Extracellular matrix remodeling in tumor progression and immune escape: From mechanisms to treatments. Mol Cancer 2023, 22, 48. [CrossRef]
- Li, C.; Xu, X.; Wei, S.; Jiang, P.; Xue, L.; Wang, J.; Senior, C. Tumor-associated macrophages: Potential therapeutic strategies and future prospects in cancer. J Immunother Cancer 2021, 9. [CrossRef]
- Petty, A.J.; Owen, D.H.; Yang, Y.; Huang, X. Targeting Tumor-Associated Macrophages in Cancer Immunotherapy. Cancers (Basel) 2021, 13. [CrossRef]
- Hourani, T.; Holden, J.A.; Li, W.; Lenzo, J.C.; Hadjigol, S.; O’Brien-Simpson, N.M. Tumor Associated Macrophages: Origin, Recruitment, Phenotypic Diversity, and Targeting. Front Oncol 2021, 11, 788365. [CrossRef]
- Mantovani, A.; Marchesi, F.; Malesci, A.; Laghi, L.; Allavena, P. Tumour-associated macrophages as treatment targets in oncology. Nat Rev Clin Oncol 2017, 14, 399-416. [CrossRef]
- Munir, M.T.; Kay, M.K.; Kang, M.H.; Rahman, M.M.; Al-Harrasi, A.; Choudhury, M.; Moustaid-Moussa, N.; Hussain, F.; Rahman, S.M. Tumor-Associated Macrophages as Multifaceted Regulators of Breast Tumor Growth. Int J Mol Sci 2021, 22. [CrossRef]
- Udeabor, S.E.; Adisa, A.O.; Orlowska, A.; Sader, R.A.; Ghanaati, S. Tumor-associated macrophages, angiogenesis, and tumor cell migration in oral squamous cell carcinoma. Ann Afr Med 2017, 16, 181-185. [CrossRef]
- Italiani, P.; Boraschi, D. From Monocytes to M1/M2 Macrophages: Phenotypical vs. Functional Differentiation. Front Immunol 2014, 5, 514. [CrossRef]
- Atri, C.; Guerfali, F.Z.; Laouini, D. Role of Human Macrophage Polarization in Inflammation during Infectious Diseases. Int J Mol Sci 2018, 19. [CrossRef]
- Liu, J.; Geng, X.; Hou, J.; Wu, G. New insights into M1/M2 macrophages: Key modulators in cancer progression. Cancer Cell Int 2021, 21, 389. [CrossRef]
- Aminin, D.; Wang, Y.M. Macrophages as a “weapon” in anticancer cellular immunotherapy. Kaohsiung J Med Sci 2021, 37, 749-758. [CrossRef]
- Reis-Sobreiro, M.; Teixeira da Mota, A.; Jardim, C.; Serre, K. Bringing Macrophages to the Frontline against Cancer: Current Immunotherapies Targeting Macrophages. Cells 2021, 10. [CrossRef]
- Duan, Z.; Luo, Y. Targeting macrophages in cancer immunotherapy. Signal Transduct Target Ther 2021, 6, 127. [CrossRef]
- Qiu, S.Q.; Waaijer, S.J.H.; Zwager, M.C.; de Vries, E.G.E.; van der Vegt, B.; Schroder, C.P. Tumor-associated macrophages in breast cancer: Innocent bystander or important player? Cancer Treat Rev 2018, 70, 178-189. [CrossRef]
- Wang, H.W.; Joyce, J.A. Alternative activation of tumor-associated macrophages by IL-4: Priming for protumoral functions. Cell Cycle 2010, 9, 4824-4835. [CrossRef]
- Boutilier, A.J.; Elsawa, S.F. Macrophage Polarization States in the Tumor Microenvironment. Int J Mol Sci 2021, 22. [CrossRef]
- Yao, Y.; Xu, X.H.; Jin, L. Macrophage Polarization in Physiological and Pathological Pregnancy. Front Immunol 2019, 10, 792. [CrossRef]
- Wang, L.X.; Zhang, S.X.; Wu, H.J.; Rong, X.L.; Guo, J. M2b macrophage polarization and its roles in diseases. J Leukoc Biol 2019, 106, 345-358. [CrossRef]
- Funes, S.C.; Rios, M.; Escobar-Vera, J.; Kalergis, A.M. Implications of macrophage polarization in autoimmunity. Immunology 2018, 154, 186-195. [CrossRef]
- Zizzo, G.; Hilliard, B.A.; Monestier, M.; Cohen, P.L. Efficient clearance of early apoptotic cells by human macrophages requires M2c polarization and MerTK induction. J Immunol 2012, 189, 3508-3520. [CrossRef]
- Ferrante, C.J.; Pinhal-Enfield, G.; Elson, G.; Cronstein, B.N.; Hasko, G.; Outram, S.; Leibovich, S.J. The adenosine-dependent angiogenic switch of macrophages to an M2-like phenotype is independent of interleukin-4 receptor alpha (IL-4Ralpha) signaling. Inflammation 2013, 36, 921-931. [CrossRef]
- Klaver, D.; Thurnher, M. Control of Macrophage Inflammation by P2Y Purinergic Receptors. Cells 2021, 10. [CrossRef]
- Xu, Y.; Wang, X.; Liu, L.; Wang, J.; Wu, J.; Sun, C. Role of macrophages in tumor progression and therapy (Review). Int J Oncol 2022, 60. [CrossRef]
- Wang, X.; Wu, Y.; Gu, J.; Xu, J. Tumor-associated macrophages in lung carcinoma: From mechanism to therapy. Pathol Res Pract 2022, 229, 153747. [CrossRef]
- Lichtnekert, J.; Kawakami, T.; Parks, W.C.; Duffield, J.S. Changes in macrophage phenotype as the immune response evolves. Curr Opin Pharmacol 2013, 13, 555-564. [CrossRef]
- Kohno, K.; Koya-Miyata, S.; Harashima, A.; Tsukuda, T.; Katakami, M.; Ariyasu, T.; Ushio, S.; Iwaki, K. Inflammatory M1-like macrophages polarized by NK-4 undergo enhanced phenotypic switching to an anti-inflammatory M2-like phenotype upon co-culture with apoptotic cells. J Inflamm (Lond) 2021, 18, 2. [CrossRef]
- Mills, C.D. M1 and M2 Macrophages: Oracles of Health and Disease. Crit Rev Immunol 2012, 32, 463-488. [CrossRef]
- Gao, J.; Liang, Y.; Wang, L. Shaping Polarization Of Tumor-Associated Macrophages In Cancer Immunotherapy. Front Immunol 2022, 13, 888713. [CrossRef]
- Feng, Y.; Ye, Z.; Song, F.; He, Y.; Liu, J. The Role of TAMs in Tumor Microenvironment and New Research Progress. Stem Cells Int 2022, 2022, 5775696. [CrossRef]
- Zhu, S.; Luo, Z.; Li, X.; Han, X.; Shi, S.; Zhang, T. Tumor-associated macrophages: Role in tumorigenesis and immunotherapy implications. J Cancer 2021, 12, 54-64. [CrossRef]
- Larionova, I.; Kazakova, E.; Gerashchenko, T.; Kzhyshkowska, J. New Angiogenic Regulators Produced by TAMs: Perspective for Targeting Tumor Angiogenesis. Cancers (Basel) 2021, 13. [CrossRef]
- Lu, C.; Liu, Y.; Ali, N.M.; Zhang, B.; Cui, X. The role of innate immune cells in the tumor microenvironment and research progress in anti-tumor therapy. Front Immunol 2022, 13, 1039260. [CrossRef]
- Afik, R.; Zigmond, E.; Vugman, M.; Klepfish, M.; Shimshoni, E.; Pasmanik-Chor, M.; Shenoy, A.; Bassat, E.; Halpern, Z.; Geiger, T.; et al. Tumor macrophages are pivotal constructors of tumor collagenous matrix. J Exp Med 2016, 213, 2315-2331. [CrossRef]
- Niland, S.; Riscanevo, A.X.; Eble, J.A. Matrix Metalloproteinases Shape the Tumor Microenvironment in Cancer Progression. Int J Mol Sci 2021, 23. [CrossRef]
- Quintero-Fabian, S.; Arreola, R.; Becerril-Villanueva, E.; Torres-Romero, J.C.; Arana-Argaez, V.; Lara-Riegos, J.; Ramirez-Camacho, M.A.; Alvarez-Sanchez, M.E. Role of Matrix Metalloproteinases in Angiogenesis and Cancer. Front Oncol 2019, 9, 1370. [CrossRef]
- Winkler, J.; Abisoye-Ogunniyan, A.; Metcalf, K.J.; Werb, Z. Concepts of extracellular matrix remodelling in tumour progression and metastasis. Nat Commun 2020, 11, 5120. [CrossRef]
- Foster, D.S.; Jones, R.E.; Ransom, R.C.; Longaker, M.T.; Norton, J.A. The evolving relationship of wound healing and tumor stroma. JCI Insight 2018, 3. [CrossRef]
- Marangio, A.; Biccari, A.; D’Angelo, E.; Sensi, F.; Spolverato, G.; Pucciarelli, S.; Agostini, M. The Study of the Extracellular Matrix in Chronic Inflammation: A Way to Prevent Cancer Initiation? Cancers (Basel) 2022, 14. [CrossRef]
- Chen, Y.; Song, Y.; Du, W.; Gong, L.; Chang, H.; Zou, Z. Tumor-associated macrophages: An accomplice in solid tumor progression. J Biomed Sci 2019, 26, 78. [CrossRef]
- Butti, R.; Khaladkar, A.; Bhardwaj, P.; Prakasam, G. Heterotypic signaling of cancer-associated fibroblasts in shaping the cancer cell drug resistance. Cancer Drug Resist 2023, 6, 182-204. [CrossRef]
- Gao, Y.; Zhou, H.; Liu, G.; Wu, J.; Yuan, Y.; Shang, A. Tumor Microenvironment: Lactic Acid Promotes Tumor Development. J Immunol Res 2022, 2022, 3119375. [CrossRef]
- Wang, Z.H.; Peng, W.B.; Zhang, P.; Yang, X.P.; Zhou, Q. Lactate in the tumour microenvironment: From immune modulation to therapy. EBioMedicine 2021, 73, 103627. [CrossRef]
- Jing, H.; Wu, X.; Xiang, M.; Wang, C.; Novakovic, V.A.; Shi, J. Microparticle Phosphatidylserine Mediates Coagulation: Involvement in Tumor Progression and Metastasis. Cancers (Basel) 2023, 15. [CrossRef]
- Bejarano, L.; Jordao, M.J.C.; Joyce, J.A. Therapeutic Targeting of the Tumor Microenvironment. Cancer Discov 2021, 11, 933-959. [CrossRef]
- Wang, J.; Li, D.; Cang, H.; Guo, B. Crosstalk between cancer and immune cells: Role of tumor-associated macrophages in the tumor microenvironment. Cancer Med 2019, 8, 4709-4721. [CrossRef]
- Hinshaw, D.C.; Shevde, L.A. The Tumor Microenvironment Innately Modulates Cancer Progression. Cancer Res 2019, 79, 4557-4566. [CrossRef]
- Davis, R.J.; Van Waes, C.; Allen, C.T. Overcoming barriers to effective immunotherapy: MDSCs, TAMs, and Tregs as mediators of the immunosuppressive microenvironment in head and neck cancer. Oral Oncol 2016, 58, 59-70. [CrossRef]
- Yang, Y.; Li, C.; Liu, T.; Dai, X.; Bazhin, A.V. Myeloid-Derived Suppressor Cells in Tumors: From Mechanisms to Antigen Specificity and Microenvironmental Regulation. Front Immunol 2020, 11, 1371. [CrossRef]
- Zhang, Z.; Liu, S.; Zhang, B.; Qiao, L.; Zhang, Y.; Zhang, Y. T Cell Dysfunction and Exhaustion in Cancer. Front Cell Dev Biol 2020, 8, 17. [CrossRef]
- Pu, Y.; Ji, Q. Tumor-Associated Macrophages Regulate PD-1/PD-L1 Immunosuppression. Front Immunol 2022, 13, 874589. [CrossRef]
- Laviron, M.; Petit, M.; Weber-Delacroix, E.; Combes, A.J.; Arkal, A.R.; Barthelemy, S.; Courau, T.; Hume, D.A.; Combadiere, C.; Krummel, M.F.; et al. Tumor-associated macrophage heterogeneity is driven by tissue territories in breast cancer. Cell Rep 2022, 39, 110865. [CrossRef]
- Li, S.; Yu, J.; Huber, A.; Kryczek, I.; Wang, Z.; Jiang, L.; Li, X.; Du, W.; Li, G.; Wei, S.; et al. Metabolism drives macrophage heterogeneity in the tumor microenvironment. Cell Rep 2022, 39, 110609. [CrossRef]
- Cassetta, L.; Noy, R.; Swierczak, A.; Sugano, G.; Smith, H.; Wiechmann, L.; Pollard, J.W. Isolation of Mouse and Human Tumor-Associated Macrophages. Adv Exp Med Biol 2016, 899, 211-229. [CrossRef]
- Jayasingam, S.D.; Citartan, M.; Thang, T.H.; Mat Zin, A.A.; Ang, K.C.; Ch’ng, E.S. Evaluating the Polarization of Tumor-Associated Macrophages Into M1 and M2 Phenotypes in Human Cancer Tissue: Technicalities and Challenges in Routine Clinical Practice. Front Oncol 2019, 9, 1512. [CrossRef]
- Lecoultre, M.; Dutoit, V.; Walker, P.R. Phagocytic function of tumor-associated macrophages as a key determinant of tumor progression control: A review. J Immunother Cancer 2020, 8. [CrossRef]
- Lee, C.C.; Lin, J.C.; Hwang, W.L.; Kuo, Y.J.; Chen, H.K.; Tai, S.K.; Lin, C.C.; Yang, M.H. Macrophage-secreted interleukin-35 regulates cancer cell plasticity to facilitate metastatic colonization. Nat Commun 2018, 9, 3763. [CrossRef]
- Cendrowicz, E.; Sas, Z.; Bremer, E.; Rygiel, T.P. The Role of Macrophages in Cancer Development and Therapy. Cancers (Basel) 2021, 13. [CrossRef]
- Zhao, H.; Wu, L.; Yan, G.; Chen, Y.; Zhou, M.; Wu, Y.; Li, Y. Inflammation and tumor progression: Signaling pathways and targeted intervention. Signal Transduct Target Ther 2021, 6, 263. [CrossRef]
- Liu, J.; Fu, M.; Wang, M.; Wan, D.; Wei, Y.; Wei, X. Cancer vaccines as promising immuno-therapeutics: Platforms and current progress. J Hematol Oncol 2022, 15, 28. [CrossRef]
- Huang, Y.; Ge, W.; Zhou, J.; Gao, B.; Qian, X.; Wang, W. The Role of Tumor Associated Macrophages in Hepatocellular Carcinoma. J Cancer 2021, 12, 1284-1294. [CrossRef]
- Xu, W.; Cheng, Y.; Guo, Y.; Yao, W.; Qian, H. Targeting tumor associated macrophages in hepatocellular carcinoma. Biochem Pharmacol 2022, 199, 114990. [CrossRef]
- Beltraminelli, T.; De Palma, M. Biology and therapeutic targeting of tumour-associated macrophages. J Pathol 2020, 250, 573-592. [CrossRef]
- Ge, Z.; Ding, S. The Crosstalk Between Tumor-Associated Macrophages (TAMs) and Tumor Cells and the Corresponding Targeted Therapy. Front Oncol 2020, 10, 590941. [CrossRef]
- Hartley, G.P.; Chow, L.; Ammons, D.T.; Wheat, W.H.; Dow, S.W. Programmed Cell Death Ligand 1 (PD-L1) Signaling Regulates Macrophage Proliferation and Activation. Cancer Immunol Res 2018, 6, 1260-1273. [CrossRef]
- Zhao, W.; Hu, X.; Li, W.; Li, R.; Chen, J.; Zhou, L.; Qiang, S.; Wu, W.; Shi, S.; Dong, C. M2-Like TAMs Function Reversal Contributes to Breast Cancer Eradication by Combination Dual Immune Checkpoint Blockade and Photothermal Therapy. Small 2021, 17, e2007051. [CrossRef]
- Liu, T.; Zhu, C.; Chen, X.; Guan, G.; Zou, C.; Shen, S.; Wu, J.; Wang, Y.; Lin, Z.; Chen, L.; et al. Ferroptosis, as the most enriched programmed cell death process in glioma, induces immunosuppression and immunotherapy resistance. Neuro Oncol 2022, 24, 1113-1125. [CrossRef]
- Porta, C.; Paglino, C.; Mosca, A. Targeting PI3K/Akt/mTOR Signaling in Cancer. Front Oncol 2014, 4, 64. [CrossRef]
- Wu, D.; Liu, X.; Mu, J.; Yang, J.; Wu, F.; Zhou, H. Therapeutic Approaches Targeting Proteins in Tumor-Associated Macrophages and Their Applications in Cancers. Biomolecules 2022, 12. [CrossRef]
- Cheng, Y.; Song, S.; Wu, P.; Lyu, B.; Qin, M.; Sun, Y.; Sun, A.; Mu, L.; Xu, F.; Zhang, L.; et al. Tumor Associated Macrophages and TAMs-Based Anti-Tumor Nanomedicines. Adv Healthc Mater 2021, 10, e2100590. [CrossRef]
- Zhang, S.Y.; Song, X.Y.; Li, Y.; Ye, L.L.; Zhou, Q.; Yang, W.B. Tumor-associated macrophages: A promising target for a cancer immunotherapeutic strategy. Pharmacol Res 2020, 161, 105111. [CrossRef]
- Monnier, M.; Paolini, L.; Vinatier, E.; Mantovani, A.; Delneste, Y.; Jeannin, P. Antitumor strategies targeting macrophages: The importance of considering the differences in differentiation/polarization processes between human and mouse macrophages. J Immunother Cancer 2022, 10. [CrossRef]
- Crezee, T.; Rabold, K.; de Jong, L.; Jaeger, M.; Netea-Maier, R.T. Metabolic programming of tumor associated macrophages in the context of cancer treatment. Ann Transl Med 2020, 8, 1028. [CrossRef]
- Gunaydin, G. CAFs Interacting With TAMs in Tumor Microenvironment to Enhance Tumorigenesis and Immune Evasion. Front Oncol 2021, 11, 668349. [CrossRef]
- Lee, W.S.; Yang, H.; Chon, H.J.; Kim, C. Combination of anti-angiogenic therapy and immune checkpoint blockade normalizes vascular-immune crosstalk to potentiate cancer immunity. Exp Mol Med 2020, 52, 1475-1485. [CrossRef]
- Gambardella, V.; Castillo, J.; Tarazona, N.; Gimeno-Valiente, F.; Martinez-Ciarpaglini, C.; Cabeza-Segura, M.; Rosello, S.; Roda, D.; Huerta, M.; Cervantes, A.; et al. The role of tumor-associated macrophages in gastric cancer development and their potential as a therapeutic target. Cancer Treat Rev 2020, 86, 102015. [CrossRef]
- Balazova, K.; Clevers, H.; Dost, A.F.M. The role of macrophages in non-small cell lung cancer and advancements in 3D co-cultures. Elife 2023, 12. [CrossRef]
- Bai, R.; Li, Y.; Jian, L.; Yang, Y.; Zhao, L.; Wei, M. The hypoxia-driven crosstalk between tumor and tumor-associated macrophages: Mechanisms and clinical treatment strategies. Mol Cancer 2022, 21, 177. [CrossRef]
- Raskov, H.; Orhan, A.; Gaggar, S.; Gogenur, I. Cancer-Associated Fibroblasts and Tumor-Associated Macrophages in Cancer and Cancer Immunotherapy. Front Oncol 2021, 11, 668731. [CrossRef]
- Riera-Domingo, C.; Audige, A.; Granja, S.; Cheng, W.C.; Ho, P.C.; Baltazar, F.; Stockmann, C.; Mazzone, M. Immunity, Hypoxia, and Metabolism-the Menage a Trois of Cancer: Implications for Immunotherapy. Physiol Rev 2020, 100, 1-102. [CrossRef]
- Kolesnikoff, N.; Chen, C.H.; Samuel, M.S. Interrelationships between the extracellular matrix and the immune microenvironment that govern epithelial tumour progression. Clin Sci (Lond) 2022, 136, 361-377. [CrossRef]
- Hao, N.B.; Lu, M.H.; Fan, Y.H.; Cao, Y.L.; Zhang, Z.R.; Yang, S.M. Macrophages in tumor microenvironments and the progression of tumors. Clin Dev Immunol 2012, 2012, 948098. [CrossRef]
- Lv, C.; Li, S.; Zhao, J.; Yang, P.; Yang, C. M1 Macrophages Enhance Survival and Invasion of Oral Squamous Cell Carcinoma by Inducing GDF15-Mediated ErbB2 Phosphorylation. ACS Omega 2022, 7, 11405-11414. [CrossRef]
- de Groot, A.E.; Myers, K.V.; Krueger, T.E.G.; Brennen, W.N.; Amend, S.R.; Pienta, K.J. Targeting interleukin 4 receptor alpha on tumor-associated macrophages reduces the pro-tumor macrophage phenotype. Neoplasia 2022, 32, 100830. [CrossRef]
- Zhang, M.Z.; Wang, X.; Wang, Y.; Niu, A.; Wang, S.; Zou, C.; Harris, R.C. IL-4/IL-13-mediated polarization of renal macrophages/dendritic cells to an M2a phenotype is essential for recovery from acute kidney injury. Kidney Int 2017, 91, 375-386. [CrossRef]
- Little, A.C.; Pathanjeli, P.; Wu, Z.; Bao, L.; Goo, L.E.; Yates, J.A.; Oliver, C.R.; Soellner, M.B.; Merajver, S.D. IL-4/IL-13 Stimulated Macrophages Enhance Breast Cancer Invasion Via Rho-GTPase Regulation of Synergistic VEGF/CCL-18 Signaling. Front Oncol 2019, 9, 456. [CrossRef]
- He, L.; Jhong, J.H.; Chen, Q.; Huang, K.Y.; Strittmatter, K.; Kreuzer, J.; DeRan, M.; Wu, X.; Lee, T.Y.; Slavov, N.; et al. Global characterization of macrophage polarization mechanisms and identification of M2-type polarization inhibitors. Cell Rep 2021, 37, 109955. [CrossRef]
- Wu, L.; Kohno, M.; Murakami, J.; Zia, A.; Allen, J.; Yun, H.; Chan, M.; Baciu, C.; Liu, M.; Serre-Beinier, V.; et al. Defining and targeting tumor-associated macrophages in malignant mesothelioma. Proc Natl Acad Sci U S A 2023, 120, e2210836120. [CrossRef]
- He, Z.; Zhang, S. Tumor-Associated Macrophages and Their Functional Transformation in the Hypoxic Tumor Microenvironment. Front Immunol 2021, 12, 741305. [CrossRef]
- Zhu, L.; Zhu, X.; Wu, Y. Effects of Glucose Metabolism, Lipid Metabolism, and Glutamine Metabolism on Tumor Microenvironment and Clinical Implications. Biomolecules 2022, 12. [CrossRef]
- Bader, J.E.; Voss, K.; Rathmell, J.C. Targeting Metabolism to Improve the Tumor Microenvironment for Cancer Immunotherapy. Mol Cell 2020, 78, 1019-1033. [CrossRef]
- Deligne, C.; Midwood, K.S. Macrophages and Extracellular Matrix in Breast Cancer: Partners in Crime or Protective Allies? Front Oncol 2021, 11, 620773. [CrossRef]
- Mun, J.Y.; Leem, S.H.; Lee, J.H.; Kim, H.S. Dual Relationship Between Stromal Cells and Immune Cells in the Tumor Microenvironment. Front Immunol 2022, 13, 864739. [CrossRef]
- Pernot, S.; Evrard, S.; Khatib, A.M. The Give-and-Take Interaction Between the Tumor Microenvironment and Immune Cells Regulating Tumor Progression and Repression. Front Immunol 2022, 13, 850856. [CrossRef]
- Fang, L.; Liu, K.; Liu, C.; Wang, X.; Ma, W.; Xu, W.; Wu, J.; Sun, C. Tumor accomplice: T cell exhaustion induced by chronic inflammation. Front Immunol 2022, 13, 979116. [CrossRef]
- Mao, X.; Xu, J.; Wang, W.; Liang, C.; Hua, J.; Liu, J.; Zhang, B.; Meng, Q.; Yu, X.; Shi, S. Crosstalk between cancer-associated fibroblasts and immune cells in the tumor microenvironment: New findings and future perspectives. Mol Cancer 2021, 20, 131. [CrossRef]
- Lugano, R.; Ramachandran, M.; Dimberg, A. Tumor angiogenesis: Causes, consequences, challenges and opportunities. Cell Mol Life Sci 2020, 77, 1745-1770. [CrossRef]
- Li, K.; Shi, H.; Zhang, B.; Ou, X.; Ma, Q.; Chen, Y.; Shu, P.; Li, D.; Wang, Y. Myeloid-derived suppressor cells as immunosuppressive regulators and therapeutic targets in cancer. Signal Transduct Target Ther 2021, 6, 362. [CrossRef]
- Tumino, N.; Fiore, P.F.; Pelosi, A.; Moretta, L.; Vacca, P. Myeloid derived suppressor cells in tumor microenvironment: Interaction with innate lymphoid cells. Semin Immunol 2022, 61-64, 101668. [CrossRef]
- Zou, Z.; Lin, H.; Li, M.; Lin, B. Tumor-associated macrophage polarization in the inflammatory tumor microenvironment. Front Oncol 2023, 13, 1103149. [CrossRef]
- Wang, B.; Zhao, Q.; Zhang, Y.; Liu, Z.; Zheng, Z.; Liu, S.; Meng, L.; Xin, Y.; Jiang, X. Targeting hypoxia in the tumor microenvironment: A potential strategy to improve cancer immunotherapy. J Exp Clin Cancer Res 2021, 40, 24. [CrossRef]
- He, L.; Marneros, A.G. Doxycycline inhibits polarization of macrophages to the proangiogenic M2-type and subsequent neovascularization. J Biol Chem 2014, 289, 8019-8028. [CrossRef]
- Henke, E.; Nandigama, R.; Ergun, S. Extracellular Matrix in the Tumor Microenvironment and Its Impact on Cancer Therapy. Front Mol Biosci 2019, 6, 160. [CrossRef]
- Jurj, A.; Ionescu, C.; Berindan-Neagoe, I.; Braicu, C. The extracellular matrix alteration, implication in modulation of drug resistance mechanism: Friends or foes? J Exp Clin Cancer Res 2022, 41, 276. [CrossRef]
- Hasan, M.N.; Capuk, O.; Patel, S.M.; Sun, D. The Role of Metabolic Plasticity of Tumor-Associated Macrophages in Shaping the Tumor Microenvironment Immunity. Cancers (Basel) 2022, 14. [CrossRef]
- Liu, J.; Cao, X. Glucose metabolism of TAMs in tumor chemoresistance and metastasis. Trends Cell Biol 2023. [CrossRef]
- Cassetta, L.; Fragkogianni, S.; Sims, A.H.; Swierczak, A.; Forrester, L.M.; Zhang, H.; Soong, D.Y.H.; Cotechini, T.; Anur, P.; Lin, E.Y.; et al. Human Tumor-Associated Macrophage and Monocyte Transcriptional Landscapes Reveal Cancer-Specific Reprogramming, Biomarkers, and Therapeutic Targets. Cancer Cell 2019, 35, 588-602 e510. [CrossRef]
- Lopez-Yrigoyen, M.; Cassetta, L.; Pollard, J.W. Macrophage targeting in cancer. Ann N Y Acad Sci 2021, 1499, 18-41. [CrossRef]
- Zhang, X.M.; Chen, D.G.; Li, S.C.; Zhu, B.; Li, Z.J. Embryonic Origin and Subclonal Evolution of Tumor-Associated Macrophages Imply Preventive Care for Cancer. Cells 2021, 10. [CrossRef]
- Niu, Y.; Chen, J.; Qiao, Y. Epigenetic Modifications in Tumor-Associated Macrophages: A New Perspective for an Old Foe. Front Immunol 2022, 13, 836223. [CrossRef]
- Ma, R.Y.; Black, A.; Qian, B.Z. Macrophage diversity in cancer revisited in the era of single-cell omics. Trends Immunol 2022, 43, 546-563. [CrossRef]
- Baghban, R.; Roshangar, L.; Jahanban-Esfahlan, R.; Seidi, K.; Ebrahimi-Kalan, A.; Jaymand, M.; Kolahian, S.; Javaheri, T.; Zare, P. Tumor microenvironment complexity and therapeutic implications at a glance. Cell Commun Signal 2020, 18, 59. [CrossRef]
- Hass, R.; von der Ohe, J.; Ungefroren, H. Impact of the Tumor Microenvironment on Tumor Heterogeneity and Consequences for Cancer Cell Plasticity and Stemness. Cancers (Basel) 2020, 12. [CrossRef]
- Truxova, I.; Cibula, D.; Spisek, R.; Fucikova, J. Targeting tumor-associated macrophages for successful immunotherapy of ovarian carcinoma. J Immunother Cancer 2023, 11. [CrossRef]
- Buonfiglioli, A.; Hambardzumyan, D. Macrophages and microglia: The cerberus of glioblastoma. Acta Neuropathol Commun 2021, 9, 54. [CrossRef]
- Malfitano, A.M.; Pisanti, S.; Napolitano, F.; Di Somma, S.; Martinelli, R.; Portella, G. Tumor-Associated Macrophage Status in Cancer Treatment. Cancers (Basel) 2020, 12. [CrossRef]
- Shen, X.; Zhou, S.; Yang, Y.; Hong, T.; Xiang, Z.; Zhao, J.; Zhu, C.; Zeng, L.; Zhang, L. TAM-targeted reeducation for enhanced cancer immunotherapy: Mechanism and recent progress. Front Oncol 2022, 12, 1034842. [CrossRef]
- Wang, D.R.; Wu, X.L.; Sun, Y.L. Therapeutic targets and biomarkers of tumor immunotherapy: Response versus non-response. Signal Transduct Target Ther 2022, 7, 331. [CrossRef]
- Anderson, K.G.; Stromnes, I.M.; Greenberg, P.D. Obstacles Posed by the Tumor Microenvironment to T cell Activity: A Case for Synergistic Therapies. Cancer Cell 2017, 31, 311-325. [CrossRef]
- Jing, X.; Yang, F.; Shao, C.; Wei, K.; Xie, M.; Shen, H.; Shu, Y. Role of hypoxia in cancer therapy by regulating the tumor microenvironment. Mol Cancer 2019, 18, 157. [CrossRef]
- Zhan, C.; Jin, Y.; Xu, X.; Shao, J.; Jin, C. Antitumor therapy for breast cancer: Focus on tumor-associated macrophages and nanosized drug delivery systems. Cancer Med 2023. [CrossRef]
- Cheng, K.; Cai, N.; Zhu, J.; Yang, X.; Liang, H.; Zhang, W. Tumor-associated macrophages in liver cancer: From mechanisms to therapy. Cancer Commun (Lond) 2022, 42, 1112-1140. [CrossRef]
- Lasagna, A.; Muzzana, M.; Ferretti, V.V.; Klersy, C.; Pagani, A.; Cicognini, D.; Pedrazzoli, P.; Brugnatelli, S.G. The Role of Pre-treatment Inflammatory Biomarkers in the Prediction of an Early Response to Panitumumab in Metastatic Colorectal Cancer. Cureus 2022, 14, e24347. [CrossRef]
- Brady, R.V.; Thamm, D.H. Tumor-associated macrophages: Prognostic and therapeutic targets for cancer in humans and dogs. Front Immunol 2023, 14, 1176807. [CrossRef]
- Li, X.; Wang, R.; Zhang, Y.; Han, S.; Gan, Y.; Liang, Q.; Ma, X.; Rong, P.; Wang, W.; Li, W. Molecular imaging of tumor-associated macrophages in cancer immunotherapy. Ther Adv Med Oncol 2022, 14, 17588359221076194. [CrossRef]
- Hu, J.; Xu, X.; Du, Y. Targeting Tumor-Associated Macrophages for Imaging. Pharmaceutics 2022, 15. [CrossRef]
- Fernandes, B.; Feltes, P.K.; Luft, C.; Nazario, L.R.; Jeckel, C.M.M.; Antunes, I.F.; Elsinga, P.H.; de Vries, E.F.J. Potential PET tracers for imaging of tumor-associated macrophages. EJNMMI Radiopharm Chem 2022, 7, 11. [CrossRef]
- George, S.; Georgouli, M.; Sanz-Moreno, V. Protocol to drive human monocyte-to-macrophage polarization in vitro using tumor conditioned media. STAR Protoc 2022, 3, 101666. [CrossRef]
- Madsen, D.H.; Jurgensen, H.J.; Siersbaek, M.S.; Kuczek, D.E.; Grey Cloud, L.; Liu, S.; Behrendt, N.; Grontved, L.; Weigert, R.; Bugge, T.H. Tumor-Associated Macrophages Derived from Circulating Inflammatory Monocytes Degrade Collagen through Cellular Uptake. Cell Rep 2017, 21, 3662-3671. [CrossRef]
- Haque, A.; Moriyama, M.; Kubota, K.; Ishiguro, N.; Sakamoto, M.; Chinju, A.; Mochizuki, K.; Sakamoto, T.; Kaneko, N.; Munemura, R.; et al. CD206(+) tumor-associated macrophages promote proliferation and invasion in oral squamous cell carcinoma via EGF production. Sci Rep 2019, 9, 14611. [CrossRef]
- Modak, M.; Mattes, A.K.; Reiss, D.; Skronska-Wasek, W.; Langlois, R.; Sabarth, N.; Konopitzky, R.; Ramirez, F.; Lehr, K.; Mayr, T.; et al. CD206+ tumor-associated macrophages cross-present tumor antigen and drive antitumor immunity. JCI Insight 2022, 7. [CrossRef]
- Bennett, S.; Breit, S.N. Variables in the isolation and culture of human monocytes that are of particular relevance to studies of HIV. J Leukoc Biol 1994, 56, 236-240. [CrossRef]
- Kubala, M.H.; DeClerck, Y.A. Conditional Knockdown of Gene Expression in Cancer Cell Lines to Study the Recruitment of Monocytes/Macrophages to the Tumor Microenvironment. J Vis Exp 2017. [CrossRef]
- Zhang, X.; Zeng, Y.; Qu, Q.; Zhu, J.; Liu, Z.; Ning, W.; Zeng, H.; Zhang, N.; Du, W.; Chen, C.; et al. PD-L1 induced by IFN-gamma from tumor-associated macrophages via the JAK/STAT3 and PI3K/AKT signaling pathways promoted progression of lung cancer. Int J Clin Oncol 2017, 22, 1026-1033. [CrossRef]
- Massalha, H.; Bahar Halpern, K.; Abu-Gazala, S.; Jana, T.; Massasa, E.E.; Moor, A.E.; Buchauer, L.; Rozenberg, M.; Pikarsky, E.; Amit, I.; et al. A single cell atlas of the human liver tumor microenvironment. Mol Syst Biol 2020, 16, e9682. [CrossRef]
- Subramanian, S.; Busch, C.J.; Molawi, K.; Geirsdottir, L.; Maurizio, J.; Vargas Aguilar, S.; Belahbib, H.; Gimenez, G.; Yuda, R.A.A.; Burkon, M.; et al. Long-term culture-expanded alveolar macrophages restore their full epigenetic identity after transfer in vivo. Nat Immunol 2022, 23, 458-468. [CrossRef]
- Tsubaki, T.; Kadonosono, T.; Sakurai, S.; Shiozawa, T.; Goto, T.; Sakai, S.; Kuchimaru, T.; Sakamoto, T.; Watanabe, H.; Kondoh, G.; et al. Novel adherent CD11b(+) Gr-1(+) tumor-infiltrating cells initiate an immunosuppressive tumor microenvironment. Oncotarget 2018, 9, 11209-11226. [CrossRef]
- Wang, X.; Shen, Y.; MengLv, L.; Zhang, X.; Yang, J.; Wang, F.; Yang, J. Thalidomide suppresses breast cancer tumor growth by inhibiting tumor-associated macrophage accumulation in breast tumor-bearing mice. Eur J Pharm Sci 2020, 151, 105302. [CrossRef]
- Clark, N.M.; Bos, P.D. Tumor-Associated Macrophage Isolation and In Vivo Analysis of Their Tumor-Promoting Activity. Methods Mol Biol 2019, 1884, 151-160. [CrossRef]
- Rodrigues, J.; Heinrich, M.A.; Teixeira, L.M.; Prakash, J. 3D In Vitro Model (R)evolution: Unveiling Tumor-Stroma Interactions. Trends Cancer 2021, 7, 249-264. [CrossRef]
- Barca, C.; Foray, C.; Hermann, S.; Herrlinger, U.; Remory, I.; Laoui, D.; Schafers, M.; Grauer, O.M.; Zinnhardt, B.; Jacobs, A.H. The Colony Stimulating Factor-1 Receptor (CSF-1R)-Mediated Regulation of Microglia/Macrophages as a Target for Neurological Disorders (Glioma, Stroke). Front Immunol 2021, 12, 787307. [CrossRef]
- Zhu, M.; Bai, L.; Liu, X.; Peng, S.; Xie, Y.; Bai, H.; Yu, H.; Wang, X.; Yuan, P.; Ma, R.; et al. Silence of a dependence receptor CSF1R in colorectal cancer cells activates tumor-associated macrophages. J Immunother Cancer 2022, 10. [CrossRef]
- Benner, B.; Good, L.; Quiroga, D.; Schultz, T.E.; Kassem, M.; Carson, W.E.; Cherian, M.A.; Sardesai, S.; Wesolowski, R. Pexidartinib, a Novel Small Molecule CSF-1R Inhibitor in Use for Tenosynovial Giant Cell Tumor: A Systematic Review of Pre-Clinical and Clinical Development. Drug Des Devel Ther 2020, 14, 1693-1704. [CrossRef]
- Johnson, M.; Dudek, A.Z.; Sukari, A.; Call, J.; Kunk, P.R.; Lewis, K.; Gainor, J.F.; Sarantopoulos, J.; Lee, P.; Golden, A.; et al. ARRY-382 in Combination with Pembrolizumab in Patients with Advanced Solid Tumors: Results from a Phase 1b/2 Study. Clin Cancer Res 2022, 28, 2517-2526. [CrossRef]
- Belli, C.; Antonarelli, G.; Repetto, M.; Boscolo Bielo, L.; Crimini, E.; Curigliano, G. Targeting Cellular Components of the Tumor Microenvironment in Solid Malignancies. Cancers (Basel) 2022, 14. [CrossRef]
- Yan, S.; Wan, G. Tumor-associated macrophages in immunotherapy. FEBS J 2021, 288, 6174-6186. [CrossRef]
- Genard, G.; Lucas, S.; Michiels, C. Reprogramming of Tumor-Associated Macrophages with Anticancer Therapies: Radiotherapy versus Chemo- and Immunotherapies. Front Immunol 2017, 8, 828. [CrossRef]
- Zhang, F.; Parayath, N.N.; Ene, C.I.; Stephan, S.B.; Koehne, A.L.; Coon, M.E.; Holland, E.C.; Stephan, M.T. Genetic programming of macrophages to perform anti-tumor functions using targeted mRNA nanocarriers. Nat Commun 2019, 10, 3974. [CrossRef]
- Rodriguez-Garcia, A.; Palazon, A.; Noguera-Ortega, E.; Powell, D.J., Jr.; Guedan, S. CAR-T Cells Hit the Tumor Microenvironment: Strategies to Overcome Tumor Escape. Front Immunol 2020, 11, 1109. [CrossRef]
- Sanchez-Paulete, A.R.; Mateus-Tique, J.; Mollaoglu, G.; Nielsen, S.R.; Marks, A.; Lakshmi, A.; Khan, J.A.; Wilk, C.M.; Pia, L.; Baccarini, A.; et al. Targeting Macrophages with CAR T Cells Delays Solid Tumor Progression and Enhances Antitumor Immunity. Cancer Immunol Res 2022, 10, 1354-1369. [CrossRef]
- Guerra, E.; Di Pietro, R.; Basile, M.; Trerotola, M.; Alberti, S. Cancer-Homing CAR-T Cells and Endogenous Immune Population Dynamics. Int J Mol Sci 2021, 23. [CrossRef]
- Anfray, C.; Ummarino, A.; Andon, F.T.; Allavena, P. Current Strategies to Target Tumor-Associated-Macrophages to Improve Anti-Tumor Immune Responses. Cells 2019, 9. [CrossRef]
- Machiels, J.P.; Gomez-Roca, C.; Michot, J.M.; Zamarin, D.; Mitchell, T.; Catala, G.; Eberst, L.; Jacob, W.; Jegg, A.M.; Cannarile, M.A.; et al. Phase Ib study of anti-CSF-1R antibody emactuzumab in combination with CD40 agonist selicrelumab in advanced solid tumor patients. J Immunother Cancer 2020, 8. [CrossRef]
- Marin-Acevedo, J.A.; Kimbrough, E.O.; Lou, Y. Next generation of immune checkpoint inhibitors and beyond. J Hematol Oncol 2021, 14, 45. [CrossRef]
- Przystal, J.M.; Becker, H.; Canjuga, D.; Tsiami, F.; Anderle, N.; Keller, A.L.; Pohl, A.; Ries, C.H.; Schmittnaegel, M.; Korinetska, N.; et al. Targeting CSF1R Alone or in Combination with PD1 in Experimental Glioma. Cancers (Basel) 2021, 13. [CrossRef]
- Amer, H.T.; Stein, U.; El Tayebi, H.M. The Monocyte, a Maestro in the Tumor Microenvironment (TME) of Breast Cancer. Cancers (Basel) 2022, 14. [CrossRef]

Table 1.
Factors involved in the polarization of circulating macrophages towards M1 or M2 TAMs.
| Mφ Types | M1 Mφ | M2 Mφ | |||
|---|---|---|---|---|---|
| M2a Mφ | M2b Mφ | M2c Mφ | M2d Mφ | ||
| Stimuli | IFN-γ and/ or LPS |
IL-4 and/ or IL-13 |
immune complexes and/or TLR agonists | IL-10 and/or TGF-β | Th2 cytokines glucocorticoids |
| Function | Pro-inflammatory | Anti-inflammatory | Pro-inflammatory | Anti-inflammatory | Pro-angiogenic |
| Cytokine profile | Produce IL-12, IL-23, and iNOS |
Produce IL-10 and arginase 1 |
Produce IL-1β, IL-6, and TNF-α |
Produce IL-10 and TGF-β |
Produce IL-4, IL-10, and TGF-β |
| Cell response |
Promote Th1 cell response |
Promote Th2 cell response |
Promote Th2 cell response |
Promote Th2 cell response |
Promote Th2 cell response |
| Function | Inhibit tumor growth | Promote tumor growth | Promote angiogenesis |
Promote angiogenesis |
Promote tumor growth |
| Chemokine profile | CCL3, CCL4, CXCL9, CXCL10, CXCL11 | CCL17, CCL18, CCL22, CCL24 | |||
| Surface markers | CD80, CD86, MHC II | CD206, CD163, MRC1, IL-10 receptor | |||
Table 2.
Clinical trials involving TAMs in cancers.
| Row | NCT Number | Phases | Study title | Conditions | Completion Date |
|---|---|---|---|---|---|
| 1 | NCT00690261 | N/A | The Impact of M1/M2 TAM Polarization on Cancer Progression and Prognosis Prediction | Tumor, Lung Cancer | August, 2010 |
| 2 | NCT01551251 | N/A | Tumor-Associated Macrophage in Advanced Non-small Cell Lung Cancer | Advanced Non-small Cell Lung Cancer | December, 2010 |
| 3 | NCT05053750 | Early Phase 1 | A Pilot Study of Weekly Paclitaxel, Bevacizumab, and Tumor-Associated Macrophage Targeted Therapy (Zoledronic Acid) in Women with Recurrent, Platinum-resistant, Epithelial Ovarian, Fallopian Tube or Primary Peritoneal Cancer | Epithelial Ovarian, Fallopian Tube, Primary Peritoneal Cancer | March 31, 2023 |
| 4 | NCT01770353 | Phase 1 | MM-398 (Nanoliposomal Irinotecan, Nal-IRI) to Determine Tumor Drug Levels and to Evaluate the Feasibility of Ferumoxytol Magnetic Resonance Imaging to Measure Tumor-Associated Macrophages and to Predict Patient Response to Treatment | Solid Tumors, ER/PR Positive Breast Cancer, Triple Negative Breast Cancer, Metastatic Breast Cancer, Metastatic Breast Cancer with Active Brain Metastasis | Oct. 2, 2018 |
| 5 | NCT03888638 | N/A | The Role of Tumor-associated Macrophages in Colorectal Liver Metastases | Colorectal Liver Metastases, Colorectal Cancer, Liver Metastases, Immunotherapy | March 1, 2019 |
| 6 | NCT01493817 | N/A | Biomarkers in Samples from Younger Patients with Wilms Tumor | Wilms Tumor and Other Childhood Kidney Tumors | Completed |
| 7 | NCT02472275 | Phase 1 | PLX3397, Radiation Therapy, and Antihormone Therapy in Treating Patients with Intermediate- or High-Risk Prostate Cancer | Stage I Prostate Adenocarcinoma, Stage II Prostate Adenocarcinoma, Stage III Prostate Adenocarcinoma | August 5, 2019 |
| 8 | NCT04776980 | Early Phase 1 | Multimodality MRI and Liquid Biopsy in GBM | Multiforme Glioblastoma, Brain Tumor, Adult Glioblastoma, Recurrent Brain Tumor, Primary Brain Tumor | June 22, 2022 |
| 9 | NCT04168528 | Phase 1, Phase 2 | Phase I/IIa Study of 68GaNOTA-Anti-MMR-VHH2 for PET/CT | Malignant Solid Tumor, Breast Cancer, Head and Neck Cancer, Melanoma (Skin) | April 2023 |
| 10 | NCT04663126 | Early Phase 1 | Feasibility of IV Tc-99m-tilmanocept for Imaging of M2-typeTAMs in Metastatic Melanoma | Melanoma | December 2022 |
| 11 | NCT03397238 | N/A | Myeloid Cell Reprogramming in Thyroid Carcinoma | Thyroid Cancer | January 5, 2021 |
| 12 | NCT01316822 | Phase 1 | A Study of ARRY-382 in Patients with Selected Advanced or Metastatic Cancers | Metastatic Cancer | October 2012 |
| 13 | NCT00979277 | N/A | Transcriptional and Molecular Characterization of Tumor-Associated Monocytes/Macrophages in Human Cancers | Tumor, Cancer | Unknown |
Table 3.
Recruiting clinical trials involving CSF1R in cancers (www.clinicaltrials.gov).
Table 3.
Recruiting clinical trials involving CSF1R in cancers (www.clinicaltrials.gov).
| Rank | NCT Number | Phases | Study Title | Conditions | Completion Date |
|---|---|---|---|---|---|
| 1 | NCT04648254 | Phase 1 | Oral Axl/Mer/CSF1R Selective Tyrosine Kinase Inhibitor in Patients with Advanced Solid Tumor | Solid Tumor, Advanced Cancer, Metastatic Cancer | 11/18/2023 |
| 2 | NCT05438420 | Phase 1/ Phase 2 | Oral Axl/Mer/CSF1R Selective Tyrosine Kinase Inhibitor Q702 in Combination with Pembrolizumab in Patients with Selected Advanced Solid | Esophageal Cancer, Gastric Cancer, Hepatocellular Cancer, Cervical Cancer | 6/30/2026 |
| 3 | NCT05438420 | Phase 1 /Phase 2 | Study of NMS-03592088 in Patients with Relapsed or Refractory AML or CMML | Acute Myeloid Leukemia (AML), Chronic Myelomonocytic Leukemia (CMML) |
9/30/2023 |
| 4 | NCT03993873 | Phase 1/ Phase 2 | Study of TPX-0022 in Patients with Advanced NSCLC, Gastric Cancer, or Solid Tumors Harboring Genetic Alterations in MET | Advanced Solid Tumor, Metastatic Solid Tumors, MET Gene Alterations | 11/1/2023 |
| 5 | NCT04848116 | Phase 2 | Neoadjuvant Targeting of Myeloid Cell Populations in Combination with Nivolumab in Head & Neck Ca | Head and Neck Squamous Cell Carcinoma |
4/1/2026 |
| 6 | NCT05020743 | Phase 1/ Phase 2 | Study of DCC-3014 in Patients with Advanced Tumors and Tenosynovial Giant Cell Tumor | Advanced Malignant Neoplasm, Pigmented Villonodular Synovitis, Giant Cell Tumor of Tendon Sheath, Tenosynovial Giant Cell | 6/1/2024 |
| 7 | NCT05020743 | Phase 1 | Phase Ib/II Study of Chiauranib in Patients with Small Cell Lung Cancer | Small Cell Lung Cancer | 12/30/2022 |
| 8 | NCT05494580 | Phase 1/ Phase 2 | Pamiparib Plus Surufatinib in Patients with Platinum-resistant Ovarian Cancer | Ovarian Cancer, Platinum-resistant Ovarian Cancer, Fallopian Tube Carcinosarcoma, Primary Peritoneal Cancer | 8/10/2025 |
| 9 | NCT05627427 | Phase 2 | Multi-cohort Study of Surufatinib Plus Sintilimab in Metastatic NEN and Pancreatic Carcinoma Who Failed Standard Chemotherapy | Neuroendocrine Tumor Grade 3, Neuroendocrine Carcinoma, Pancreatic Carcinoma | 12/31/2024 |
| 10 | NCT05627427 | N/A | Mass Balance Study of [14C] Chiauranib | Small Cell Lung Cancer (SCLC) | 6/30/2023 |
| 11 | NCT04830813 | Phase 3 | Phase 3 Clinical Study of Chiauranib Capsule in Patients with Small-cell Lung Cancer | Small Cell Lung Cancer (SCLC) | 12/31/2024 |
| 12 | NCT05273099 | N/A | Molecular Biomarkers Predicting Early Development of Endometrial Carcinoma | Cancer of Endometrium | 12/1/2023 |
| 13 | NCT05273099 | N/A | Early Rebiopsy to Identify Biomarkers of Tumor Cell Survival Following EGFR, ALK, ROS1 or BRAF TKI Therapy | NSCLC TNM Stage 4, NSCLC, EGFR Gene Mutation, ALK Gene Mutation, ROSE Cluster 1|BRAF V600E | 9/30/2027 |
| 14 | NCT04622865 | Phase 2 | APUR: Testing the Use of FDA Approved Drugs That Target a Specific Abnormality in a Tumor Gene in People with Advanced Stage Cancer | Non-Hodgkin Lymphoma, Multiple Myeloma, Advanced Solid Tumors | 12/31/2025 |
| 15 | NCT04622865 | Phase 2 | Biomarker Driven Trial of VEGFR2 Inhibitor in Advanced Sarcoma | Sarcoma | 8/25/2023 |
| 16 | NCT02171104 | Phase 2 | A Study Evaluating the Activity of Anti-cancer Treatments Targeting Tumor Molecular Alterations/Characteristics in Advanced / Metastatic Tumors. | Malignant Solid Tumor | 11/1/2026 |
| 17 | NCT02171104 | Phase 2 | Canadian Profiling and Targeted Agent Utilization Trial (CAPTUR) | Non-Hodgkin Lymphoma, Multiple Myeloma, Advanced Solid Tumors | 1/31/2027 |
| 18 | NCT02029001 | Phase 2 | Adapting Treatment to the Tumor Molecular Alterations for Patients with Advanced Solid Tumors | Malignant Solid Neoplasms | 10/1/2026 |
| 19 | NCT02029001 | Phase 3 | Molecular Profiling of Advanced Soft-tissue Sarcomas | Soft Tissue Sarcoma | 10/1/2025 |
| 20 | NCT02029001 | Phase 1 | A Phase I Trial of Simmitinib in Advanced Solid Tumors | Advanced Solid Tumor | 3/31/2025 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



