
Submitted:
25 May 2023
Posted:
26 May 2023
You are already at the latest version
Abstract
Endobronchial Ultrasound has been widely used in the lymph node staging of lung tumors and the diagnosis of mediastinal diseases. In the last decades this procedure has evolved in several technical aspects, with new tools available to optimize the tissue sampling and to increase the diagnostic yield, like elastography, different types of needles and, most recently, miniforceps and cryobiopsy. Then, also the indications for EBUS have extended beyond the thoracic boundaries to sample lesions of the liver, left adrenal gland and retroperitoneal lymph nodes via the gastroesophageal tract. In this review we will analyze the actual indication of EBUS, even the more unusual, to underline the multiple use of EBUS in clinical practise.
Keywords:
Endobronchial ultrasound
; Transbronchial needle aspiration
; bronchoscopy
1. Introduction
The use of transbronchial needle aspiration (TBNA) for sampling mediastinal lymph nodes was first described in 1949 by Schieppati [1], an Argentinian physician, via a rigid bronchoscope. This technique was relatively neglected until 1978, when Wang and colleagues successfully diagnosed lung carcinoma adjacent to the trachea and paratracheal nodal metastasis using an esophageal varices needle [2], and one year later it was developed a new needle to insert in the fiberoptic bronchoscope [3]. Finally, in 1983, Wang reported his first experience on 35 patients concluding that the procedure was relatively safe and efficient in performing a correct diagnosis and in staging lung cancer [4].
Since then, TBNA has become a widely used method to sample targets (e.g. mass, nodes, etc.) which are outside, but adjacent, the central airways, by inserting the needle in the hypothetical position suggested by a careful pre-procedural analysis of thoracic CT scan when available, otherwise only by chest X-rays and endobronchial anatomic landmarks [5].
In 2002, the development of the convex probe to perform endobronchial ultrasound was a crucial turning point, because it allowed the bronchoscopist to perform real-time transbronchial needle aspiration guided by endobronchial ultrasound (EBUS-TBNA) [6]. The high diagnostic yield and safety profile of EBUS-TBNA were soon recognized and, as a result, this technique spread all around the world for his excellent diagnostic capabilities [7]. However, only after the ASTER trial [8], that showed similar sensitivity for EBUS-TBNA compared to mediastinoscopy (85% vs 79%, respectively) with lower complications and fewer unnecessary thoracotomies, EBUS-TBNA became the preferred choice to stage the mediastinum in lung cancer, as reported in multiple guidelines [9,10].
More recently, the clinical application of EBUS has extended. Indeed, the higher amount of tissue required by the pathologist to perform not only a correct diagnosis of cancer but also a precise molecular analysis challenges the clinician that performs the procedure to upgrade his technique routine to maintain sample adequacy. Then, new opportunities to use EBUS outside the “conventional” endobronchial route are emerging, expanding the indication of this procedure even beyond the thoracic boundaries.
Therefore, the aim of this comprehensive review is to emphasize the various applications for EBUS, highlighting also the newest approaches and techniques available.
2. The role of EBUS-TBNA in the molecular profiling of lung cancer
Nowadays, in the era of precision medicine, cancer treatments include an increasing number of targeted therapies, which means drugs that specifically interfere with molecules involved in the growth and progression of tumors.
In recent years, research on the molecular mutations in non-small cell lung cancer (NSCLC) has enriched the knowledge on biological pathways driving tumor development, as for the mutations of the epidermal growth factor receptor (EGFR) gene [11]. The efficacy on both overall and progression-free survival of molecular targeted therapies and immune checkpoint inhibitors in NSCLC forces the clinicians to obtain adequate specimens for a precise tumor genotyping [12]. Several prospective trials have established the non-inferiority, or even superiority, of EBUS-TBNA compared to surgical mediastinoscopy to achieve a correct diagnosis and mediastinal staging [13,14,15], with an excellent safety profile and a complication rate lower than 1% [12]. The suitability of EBUS-TBNA, which is a cytological methodology, to ensure a complete molecular analysis is still debated [16,17,18]. Labarca et al. recently reported in a systematic review and meta-analysis that the adequacy of EBUS-TBNA to evaluate EGFR and anaplastic lymphoma kinase (ALK) mutations was feasible in 94.5% (28 studies, n=2497 patients) and 95% of the patients (12 studies, n=607), respectively [19].
There are different aspects of the EBUS-TBNA technique that may impact on the sample adequacy for molecular analysis.
Lee et al. reported that three needle passes for each target site are sufficient to perform a correct diagnosis in NSCLC [20]; however, to obtain an exhaustive molecular analysis it is recommended that supplementary needle passes should be performed [21,22,23].
Rapid on-site evaluation (ROSE) provides real-time pathologic evaluation of the sample adequacy and at the beginning was developed especially for the conventional TBNA to enhance the diagnostic yield [24,25,26]. Its role in EBUS-TBNA is still controversial, and few randomized controlled trials available in literature showed that ROSE did not increase the diagnostic yield [27], but reduces the punctures per-site (2.2 vs 3.1, respectively) and the need of further diagnostic procedures (11% vs 57%, respectively) [28]. Moreover, in the context of molecular profiling, it was reported that ROSE could increase the rate of a complete tumor genotyping up to 10%, which is a relevant clinical data even though it did not reach statistical significance [29].
Further dissecting the potential factors influencing EBUS-TBNA performance, the utilization of high-pressure suction, compared to standard vacuum syringe suction, did not increase the diagnostic yield; however, Tsakinis described bigger samples (11.2 vs. 9.1 mm3, p=0.036) and fewer additional procedures (3.8% vs. 17.5%, p=0.042) to reach a complete molecular profiling in NSCLC with a necrotic component [30]. The complete or partial retraction of stylet, as retrospectively assessed in 50 patients, does not seem to influence molecular testing adequacy [31].
A large cohort study of prospectively enrolled patients undergoing EBUS-TBNA specifically focused on the determining factors for lung cancer histotype and molecular profile showing that, at least for EGFR mutation and ALK rearrangements, more passes and bigger nodes (long-axis diameter) may increase the sensitivity [32].
Another variable influencing the sample adequacy is related to the pathologist’s choice of specimen preservation. In accordance with the College of American Pathologists guidelines, cell blocks are recommended over smear preparations because of their ability to correlate with malignant cell content and the possible conservation of more material for additional studies [33]. Gross pathological specimens can be preserved in paraffin blocks, the so called “cell block”, that can be cut and stained for histopathological analysis. This technique preserves the cytological architecture and allows for immunochemical staining, thereby providing a proper characterization of the malignancy [34]. As compared with conventional smear method, cell block analysis can improve the yield of EBUS-TBNA by 7% and can provide data for genetic analysis in patients with adenocarcinoma [35].
On this line, Martin-Delon et al. prospectively assessed stage III and IV NSCLC to evaluate the adequacy of EBUS-TBNA samples for detailed molecular characterization - tested by next-generation sequencing (NGS), nCounter and immunohistochemistry (PD-L1) - and to compare its performance to the reference standard of biopsy samples. EBUS-TBNA showed a high concordance with biopsies: 88.9% for PD-L1, 100% for NGS and nCounter [36]. Looking at the details of this study, ROSE was regularly performed and the average number of needle passes was six, much higher than suggested [21], possibly favoring the good performance of EBUS-TBNA sampling. Indeed, the 92.8% of them provided material to successfully perform the evaluation of all tumor predictors, exceeding the 75.8% obtained with biopsies. On the other hand, although PD-L1 testing was achievable in the majority of EBUS-TBNA samples, a lower agreement was observed in higher PD-L1 immunohistochemistry scores. As previously observed, a worrisome discrepancy can be found between PD-L1 testing on EBUS-TBNA and other tissue specimens, as suggested by the wide range of concordance rates reported in literature, between 69.8 and 91.3% [37,38,39]. A possible reason of such discordant results is related to the intrinsic spatial and temporal heterogeneity of PD-L1 expression that characterize NSCLC [40], which increases the risk of false negatives in small samples with low tumor cellularity, such as those obtained from EBUS-TBNA. So far, the potential misclassification of PD-L1 status in EBUS-TBNA specimens still represents a considerable risk, especially when the PD-L1 cutoff of tumor proportion score ≥ 50% is applied. Nonetheless, a recent real-life study suggests that EBUS-TBNA results are as effective as histological specimens to guide immune check-point inhibitor therapy, with comparable treatment outcomes, supporting the regular testing for PD-L1 in EBUS-TBNA samples [41].
A meta-analysis on 21 studies (n=1.175 patients) conducted last year reported that EBUS-TBNA provided adequate samples for next generation sequencing (>80%) and the accuracy was related to the number of passes. Therefore, they suggested that increasing that number may raise the molecular yield [42].
Notably, in the supernatant of the needle aspiration, after centrifugation, is reported the presence of free-floating DNA. This innovative technique can help in providing supplementary DNA, increasing the diagnostic yield for NGS analysis and eventually reducing further repeated biopsy or turnaround time [43,44,45]. However, the evaluation of supernatant needs to be further studied in larger cohorts of patients, to establish diagnostic accuracy and impact on NGS [46].
Treatment of the early stages of NSCLC for several years was surgical resection, less frequently associated with radio-chemotherapy or neoadjuvant/adjuvant chemotherapy [47]. Especially in the last scenario, recently, favorable results are emerging from clinical trials. Adjuvant therapy in EGFR mutated NSCLC, as well as preoperative immunotherapy in early stages, showed less relapses or post-operative tumor progression [48,49]. In the ADAURA study osimertinib, a third-generation tyrosine kinase inhibitor, was administered as an adjuvant in EGFR mutated NSCLC, and it was reported a reduction of recurrence by 80% compared to placebo, after surgical lung tumor resection. Moreover, in the NeoADAURA study, a clinical trial on osimertinib in a neoadjuvant setting in early operable stages of NSCLC is recruiting participants (NCT04351555) [50].
Given these premises, the preoperative assessment will soon be crucial to study the molecular profile of lung cancer, since it is now mandatory the evaluation of EGFR and ALK status before considering neoadjuvant immunotherapy or neoadjuvant immunotherapy and chemotherapy [51]. However, the small size of samples obtained by bronchoscopy and EBUS may represent a challenge for pathologists and analysis optimization will require great teamwork between pulmonologists, oncologists and pathologists [52,53].
In view of the present limitations, molecular testing in stage I–III is not recommended by current guidelines and the broad molecular assessment is overall suggested only in metastatic NSCLC [54]. Nonetheless, recent updated guidelines including National Comprehensive Cancer Network® (NCCN®), Canadian, and Chinese/Asian guidelines propose to test at least EGFR mutations [54].
Collectively, accumulating evidence highlights the need of optimizing diagnostic samples management according to lung cancer stage and promoting the early recognition of molecular/immune prognostic markers not only in metastatic disease but also in the pre-operative stage of resectable cancer.
3. Elastography
There are several echographyc features during EBUS-TBNA that may orient towards the suspicion of a malignant lymph node such as echogenicity, margins, diameter or the presence of necrosis. However, none of these characteristics have proven to be consistent with malignancy in the studies reported in literature [55].
In this regard, endobronchial elastography is a relatively new technology combined with the endoscopic ultrasound procedure that aims at better differentiating malignant versus benign lymph nodes. Elastography assesses the relative elasticity or stiffness of the tissue according to the degree of deformation after compression, in a color-based output. Blue signal represents hard tissue like malignancy, while benign lesions which are softer exhibit a red-green color.
Tissue elasticity can be measured by qualitative or semi-quantitative modality.
The most widely used qualitative classification is the Izumo score, which identifies three types of findings: predominantly nonblue (type 1), partially blue (type 2) and predominantly blue (type 3) [56]. However, even though type 3 lymph nodes should suggest malignant involvement, up to 20% may have pathological discordance [57,58]. Moreover, no correlation to the maximum standardized uptake value of positron emission tomography-computed tomography (PET-CT) images was found [57].
Discrepancies may arise by the different judgment of elastography images, which is an operator-dependent evaluation. As a result, some changes have been applied to the observation method of elastography, like the stiffness ratio, strain histogram or strain ratio to predict lesion elasticity characteristics [59,60]. However, these semi-quantitative measurements require additional softwares for image processing, calculations and for the analysis, which are time consuming by increasing procedure complexity.
Multiple factors related to the final results during EBUS elastography. False positive results are mostly due to increased stiffness in cases of tuberculosis, pneumoconiosis, or sarcoidosis, while necrosis, hemorrhage or liquefaction in malignant lesions can cause false negatives [61,62].
Therefore, elastography is useful to evaluate multistation lymph nodes involvement, but also when multiple nodes are present in the same station, either to prevent unnecessary punctures focusing especially on type 3 lymph node, or to avoid implantation metastasis in the same stage lymph node, performing puncture from type 1 to 3. Notably, to the previously reported limits of this procedure, elastography cannot replace lymph node aspiration.
4. “Unusual” applications of EBUS
Pulmonary embolism
EBUS allows an excellent visualization of structures surrounding the airways, pulmonary artery included. Casoni et al. in 2008 reported a case where pulmonary angiography did not permit distinguishing between pulmonary emboli or sarcoma. The use of EBUS showed “in real-time, a blood clot floating into the right main pulmonary artery not infiltrating the wall of blood vessel”, permitting a correct diagnosis of pulmonary embolism (PE) [63]. This was the first report in literature about the use of EBUS to evaluate pulmonary emboli. Then, a multicenter pilot study [64] showed that EBUS had an accuracy ratio of 96% in detecting PE, which reached 100% if only centrally located PE were considered.
To evaluate and estimate pulmonary embolism severity, the preferred technique is the computed tomography (CT) angiography; however, EBUS should be considered in the diagnostic flow-chart in patients for whom angiography is contraindicated, as in chronic renal failure, previous anaphylactic reactions to intravenous contrast agents and pregnancy [65]. Moreover, when PE is suspected in intensive care patients unable to be transferred to the radiology suite for CT scan, EBUS could be performed bedside as reported by Bertini et al. By combining bedside EBUS and echocardiography, this group rapidly performed a diagnosis of PE as the cause of cardiac arrest in a 64 year old woman, avoiding the potentially dangerous transfer to radiology department [66].
An ongoing clinical trial, even though is not currently updated, is evaluating the added value of EBUS in diagnosing pulmonary embolism in critically ill patients (Pilot Study to Evaluate the Role of EBUS in the Diagnosis of Acute PE in Critically Ill Patients-VEBUS- NCT04047784).
In the experience of our Interventional Pneumology Centre, the most representative case of pulmonary embolism evaluated with EBUS is shown in Figure 1.
Pleural lesions
In suspected pleural neoplastic involvement, especially when pleural effusion is present, thoracoscopy with pleural biopsy is the preferred method for tissue sampling and performing diagnosis. However, thoracoscopy might be invasive and may pose relevant risks in selected patients, especially those with multiple and severe comorbidities [67]. In this regard, EBUS can offer a minimally invasive option for sampling pleural tissue next to large airways or esophagus, as reported by few case reports. Kassier et al. sampled both mediastinal lymph nodes and a pleural mass by a transesophageal approach in the same procedure in a case of metastatic renal cell carcinoma [68].
EBUS could be particularly useful when pleural abnormalities are not in the context of pleural effusion. Lococo et al. sampled a single PET positive pleural lesion located in the right costovertebral recess finding a suspect epithelioid tumor, supporting the diagnosis of epithelioid-type malignant mesothelioma, that was then confirmed at the surgical resection [69].
Therefore, EBUS-TBNA in a subgroup of patients may allow pleural samples in a less invasive technique compared to thoracoscopy, sparing risky surgical procedures especially when surgical thoracoscopy is required.
Pleural and pericardial effusion
EBUS-TBNA can offer an alternative therapeutic and diagnostic tool to standard thoracentesis especially when its distribution is loculated and the site of the pleural effusion is located toward the mediastinum. Endoscopic US (EUS) guidance to drain pleural effusion was firstly reported in a retrospective study in 2008 by DeWitt et colleagues. [70]. In 9 cases the EBUS scope was introduced in the esophagus and was successfully applied to drain pleural effusion without significant complications and providing adequate samples for cytological analysis. Similarly, Cocciardi et al. drained a loculated pleural effusion not accessible through traditional thoracentesis [71].
An appropriate concern regards the infectious risk; indeed the needle is not sterile once it passes through the working channel, potentially inoculating bacteria in the pleural space. However the risk is low and an antibiotic prophylaxis could be performed to avoid this possibility.
Thyroid lesions
Intrathoracic goiter and thyroid lesions can represent a clinical challenge, always requiring the exclusion of potential malignancy. The percutaneous approach, applicable in the diagnostic workout of common thyroid lesions, is not suitable when the target is intrathoracic, thus requiring mediastinoscopy or surgical biopsy. In these conditions, less invasive procedures like EBUS might represent an option, as suggested by a few cases revised by Madan et al. [74]. Overall, aspiration of the thyroid lesion was mainly a secondary indication (60%) of EBUS-TBNA but all the samples were adequate. Most of the procedures were safe except one case reporting the development of iatrogenic thyroid abscess [75]. This risk is greater for cystic lesions and an antibiotic prophylaxis may be rational in such circumstances.
Intratumoral therapy
According to the expanding scenario of lung cancer treatment, a discrete range of oncogene driven drugs is now available. When molecular analysis does not identify a specific target, the immune status of NSCLC can be addressed. Standard chemotherapy protocols, with and without radiotherapy still represent an optional or complementary approach. Nevertheless, lung cancer still represents the first cause of death worldwide [76]. Among the possible alternative strategies, intratumoral therapies may have a logic to get over checkpoint resistance and to reduce the systemic side effects [77]. In the last decades, the knowledge of endobronchial chemotherapy delivery has grown, widening the available approaches to malignant airways obstruction. Moreover, the injection permits to achieve higher local concentration of the drug compared to that delivered systematically, up to 30-fold more [77,78], reducing side effects because of the decreased systemic concentration [79].
Conventional TBNA has been used for several years for injection into the airways, lung parenchyma and surrounding tissues. Aside from delivery of cancer therapies, transbronchial needles have been utilized for the injection of corticosteroids, antimicrobials, tranexamic acid, radioisotopes to identify lung lesions or tissue sealants to close bronchopleural fistula [77]. Since 2013, the use of endobronchial ultrasound improved the transbronchial injection technique by the direct visualization of drug delivery, avoiding the risk of puncture blood vessels or other mediastinal structures [80].
Thereafter, this technique has been widely applied and both standard chemotherapy [81,82,83] and immunotherapy [84] have been delivered effectively. This technique might be further improved by preoperative stratification of dose and site of injection according to computational modeling which allows to plan the procedure according to precise estimation of tumor size and localization [85].
Non-ordinary applications of endoscopic ultrasound are summarized in Table 1.
5. EUS-B Fine Needle Aspiration
EBUS scope can also be used in the esophagus (EUS-B) by the pulmonologist, and this technique is proceeding forward because of its usefulness either as a supplement to the endobronchial approach or to additional lymph node sampling [86,87,88]. Indeed, European guidelines for combined EBUS and EUS recommend both techniques, endobronchial and esophageal, to stage mediastinal lymph nodes to increase the diagnostic yield compared to one technique alone [10]. Moreover, it is also recommended the evaluation of the left adrenal gland (LAG) for suspected metastasis, performing a more accurate stage of lung cancer including the M evaluation [10]. Indeed, up to 7% of patients with resectable cancer have adrenal masses, which in approximately two thirds of cases are benign adenomas [89,90,91]. As a result, it is mandatory to perform a precise pathological confirmation of suspicious adrenal gland to correctly stage the patients and for the suitable treatment.
Crombag and Annema reported that the diagnostic yield of LAG EUS-B-FNA was comparable to conventional EUS-FNA performed with gastrointestinal echoendoscope [92].
More recently, in a large cohort of patients (n=135), safety and feasibility of this procedure was confirmed, with nearly 90% of samples adequate, and, as previously reported, a proven malignancy in one third of the cases [91].
Even though the use of EUS-B-FNA is reported also for sampling suspected left liver lobe lesions or retroperitoneal lymph nodes, guidelines still do not mention these approaches. The diagnostic yield described by Christiansen et al. was higher than 80% for the left liver lobe lesions, and a little lower (63%) for the retroperitoneal lymph nodes, with no complication observed [93].
All the possible site that can ben evaluated by EBUS, as previously reported, are shown in Figure 2.
6. Novel devices improving EBUS TBNA performance and future perspectives
New complementary tools have been developed to obtain biopsy specimens for histological analysis for EBUS TBNA.
The Acquire® 22 G fine needle (produced by Boston Scientific Co., Natick, MA, USA) is characterized by a Franseen tip 22 G FNB device equipped with three cutting edges. This needle has shown a better performance than FNA when applied to sample solid lesions by EUS in a prospective study [94]. Its feasibility and potential advantages in granulomatous diseases have been described [95], and a randomized trial assessing whether, compared to TBNA, the biopsies obtained by this needle provide more or better quality tissue to allow a definite diagnosis on TBNA is still ongoing (NCT04200105).
The ProCore® needle (produced by Cook Medical, Bloomington, IN, USA) has a core trap designed to collect a histological sample by shearing material from the lesion during the needle motion [96]. By now, studies reported in literature showed that this needle have similar diagnostic accuracy than standard 22-gauge needle either for malignancy or in suspected sarcoidosis [96,97].
Another tool to augment the tissue sampled is the EBUS-guided intranodal forceps biopsy (IFB), which is performed by introducing the mini forceps through the initial hole made by the TBNA needle. When compared EBUS-TBNA, the addition of IFB determined a higher diagnostic yield especially in patients with sarcoidosis (93% vs. 58%, p<0.001) and lymphoma (86% vs. 30%, p=0.03) [98]. The complication rates (pneumothorax and pneumomediastinum 1%, bleeding, 0.8%) were higher than what had been reported with EBUS-TBNA alone (pneumothorax, 0.03% and bleeding, 0.68%) but lower than with mediastinoscopy [98].
A new tool to obtain lymph node sampling is transbronchial cryobiopsy under EBUS guidance. Technically, a 1.1 mm cryobiopsy probe is inserted in the hole created by the TBNA, with a 3 seconds freeze-time [99].
The first randomized control trial (n=197) was performed in 2021 by Zhang and colleagues, which compared standard EBUS-TBNA to cryobiopsy to sample mediastinal lesions of at least 1 cm [100]. The overall diagnostic yield was significantly higher for cryobiopsy (91.8% vs 79.9%;,p=0.001). However, performing subgroup analysis, when metastatic lymph nodes were analyzed, the diagnostic yields were similar (94.1% vs. 95.6%, p=0.58) between the two procedures. Conversely, cryobiopsy was more accurate than EBUS-TBNA in benign disorders (80.9% vs. 53.2%, p=0.004) and uncommon tumours (91.7% vs. 25.0%, p=0.001).
Especially in the latter group, which was mainly constituted by lymphoma, mediastinal cryobiopsy showed great efficacy, with a diagnostic rate of nearly 90%, and successfully subtype of all cases [101].
Moreover, in cases of lung cancer, almost all of the cryobiopsy materials (93.3%) were advisable for gene mutation PCR testing, compared to TBNA (73.5%), which is consistent with previous reports [102,103].
Interestingly, no differences in the diagnostic yield were found between “Cryobiopsy first” and “TBNA first” groups. Regarding adverse events, two cases of pneumothorax and one of pneumomediastinum were reported, highlighting the safety of the procedure.
In a recent randomized multicenter study (n=297) published on Lancet Respiratory Journal, it was compared the addition of cryobiopsy to standard needle sampling to evaluate the overall diagnostic yield for mediastinal lesions [104]. The complementary use of EBUS cryobiopsy determined a 12% increase in the overall diagnostic yield compared to EBUS-TBNA alone. Moreover, in subgroup analyses the combined approach permitted also a higher diagnostic yield in benign disorders while were similar for mediastinal metastasis, even for uncommon tumours [104].
The combined approach permitted also a more precise molecular and immunological analyses of lung cancer, without higher adverse events.
7. Conclusion
Since its first application in 2002, the real time transbronchial vision provided by EBUS has revolutionized the approach to lung lesions. Day by day, the development of new complementary technologies, briefly reviewed here, has improved the diagnostic yield and expanded possible EBUS applications to several diseases involving the mediastinum and beyond. The increasing demand of tissue for diagnostic assessment, parallel to the growing knowledge on pathological and molecular features of lung cancer, will push further the optimization of EBUS as a crucial diagnostic tool in respiratory diseases.
Funding
This research received no external funding
Conflicts of Interest
The authors declare no conflict of interest
References
- Schieppati, E. La puncion mediastinal a traves del espolon traqueal [Mediastinal puncture through the tracheal spur]. Rev As Med Argent 1949, 663, 497–499. [Google Scholar]
- Wang, K.P.; Terry, P.; Marsh, B. Bronchoscopic needle aspiration biopsy of paratracheal tumors. Am Rev Respir Dis 1978, 118, 17–21. [Google Scholar] [PubMed]
- Oho, K.; Kato, H.; Ogawa, I.; Hayashi, N.; Hayata, Y. A new needle for transfiberoptic bronchoscope use. Chest 1979, 76, 492. [Google Scholar] [CrossRef]
- Wang, K.P.; Terry, P. Transbronchial needle aspiration in the diagnosis and staging of bronchogenic carcinoma. Am Rev Respir Dis 1983, 127, 344–347. [Google Scholar]
- Yarmus, L.; Feller-Kopman, D.; Browning, R.; Wang, K. TBNA: should EBUS be used on all lymph node aspirations? J Bronchology Interv Pulmonol 2011, 18, 115–117. [Google Scholar] [CrossRef]
- Yasufuku, K.; Chiyo, M.; Sekine, Y.; Chhajed, P.N.; Shibuya, K.; Iizasa, T.; Fujisawa, T. Real-time endobronchial ultrasound-guided transbronchial needle aspiration of mediastinal and hilar lymph nodes. Chest 2004, 126, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Zhao, H.; Garfield, D.H.; Teng, J.; Han, B.; Sun, J. Endobronchial ultrasound-guided transbronchial needle aspiration in the diagnosis of non-lymph node thoracic lesions. Ann Thorac Med 2013, 8, 14–21. [Google Scholar]
- Annema, J.T.; van Meerbeeck, J.P.; Rintoul, R.C.; Dooms, C.; Deschepper, E.; Dekkers, O.M.; De Leyn, P.; Braun, J.; Carroll, N.R.; Praet, M.; et al. Mediastinoscopy vs endosonography for mediastinal nodal staging of lung cancer: a randomized trial. JAMA 2010, 304, 2245–2252. [Google Scholar] [CrossRef]
- Silvestri, G.A.; Gonzalez, A.V.; Jantz, M.A.; Margolis, M.L.; Gould, M.K.; Tanoue, L.T.; Harris, L.J.; Detterbeck, F.C. Methods for staging non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians' evidence-based clinical practice guidelines. Chest 2013, 143, e211S–e250S. [Google Scholar] [CrossRef]
- Vilmann, P.; Clementsen, P.F.; Colella, S.; Siemsen, M.; De Leyn, P.; Dumonceau, J.M.; Herth, F.J.; Larghi, A.; Vazquez-Sequeiros, E.; Hassan, C.; et al. Combined endobronchial and esophageal endosonography for the diagnosis and staging of lung cancer: European Society of Gastrointestinal Endoscopy (ESGE) Guideline, in cooperation with the European Respiratory Society (ERS) and the European Society of Thoracic Surgeons (ESTS). Endoscopy 2015, 47, 545–559. [Google Scholar] [CrossRef]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2018, 29, iv192–iv237. [Google Scholar] [CrossRef] [PubMed]
- McLean, A.E.B.; Barnes, D.J.; Troy, L.K. Diagnosing Lung Cancer: The Complexities of Obtaining a Tissue Diagnosis in the Era of Minimally Invasive and Personalised Medicine. J Clin Med 2018, 7, 163. [Google Scholar] [CrossRef]
- Um, S.W.; Kim, H.K.; Jung, S.H.; Han, J.; Lee, K.J.; Park, H.Y.; Choi, Y.S.; Shim, Y.M.; Ahn, M.J.; Park, K.; et al. Endobronchial ultrasound versus mediastinoscopy for mediastinal nodal staging of non-small-cell lung cancer. J Thorac Oncol 2015, 10, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Yasufuku, K.; Pierre, A.; Darling, G.; de Perrot, M.; Waddell, T.; Johnston, M.; da Cunha Santos, G.; Geddie, W.; Boerner, S.; Le, L.W; et al. A prospective controlled trial of endobronchial ultrasound-guided transbronchial needle aspiration compared with mediastinoscopy for mediastinal lymph node staging of lung cancer. J Thorac Cardiovasc Surg 2011, 142, 1393–1400.e1. [Google Scholar] [CrossRef]
- Ernst, A.; Anantham, D.; Eberhardt, R.; Krasnik, M.; Herth, F.J. Diagnosis of mediastinal adenopathy-real-time endobronchial ultrasound guided needle aspiration versus mediastinoscopy. J Thorac Oncol 2008, 3, 577–582. [Google Scholar] [CrossRef]
- Navani, N.; Brown, J.M.; Nankivell, M.; Woolhouse, I.; Harrison, R.N.; Jeebun, V.; Munavvar, M.; Ng, B.J.; Rassi, D.M.; Falzon, M; et al. Suitability of endobronchial ultrasound-guided transbronchial needle aspiration specimens for subtyping and genotyping of non-small cell lung cancer: A multicenter study of 774 patients. Am J Respir Crit Care Med 2012, 185, 1316–1322. [Google Scholar] [CrossRef]
- Rooper, L.M.; Nikolskaia, O.; Carter, J.; Ning, Y.; Lin, M.T.; Maleki, Z. A single EBUS-TBNA procedure can support a large panel of immunohistochemical stains, specific diagnostic subtyping, and multiple gene analyses in the majority of non-small cell lung cancer cases. Hum Pathol 2016, 51, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Esterbrook, G.; Anathhanam, S.; Plant, P.K. Adequacy of endobronchial ultrasound transbronchial needle aspiration samples in the subtyping of non-small cell lung cancer. Lung Cancer 2013, 80, 30–34. [Google Scholar] [CrossRef]
- Labarca, G.; Folch, E.; Jantz, M.; Mehta, H.J.; Majid, A.; Fernandez-Bussy, S. Adequacy of samples obtained by endobronchial ultrasound with transbronchial needle aspiration for molecular analysis in patients with non-small cell lung cancer: systematic review and meta-analysis. Ann Am Thorac Soc 2018, 15, 1205–1216. [Google Scholar] [CrossRef]
- Lee, H.S.; Lee, G.K.; Lee, H.S.; Kim, M.S.; Lee, J.M.; Kim, H.Y.; Nam, B.H.; Zo, J.I.; Hwangbo, B. Real-time endobronchial ultrasound-guided transbronchial needle aspiration in mediastinal staging of non-small cell lung cancer: how many aspirations per target lymph node station? Chest 2008, 134, 368–374. [Google Scholar] [CrossRef]
- Wahidi, M.M.; Herth, F.; Yasufuku, K.; Shepherd, R.W.; Yarmus, L.; Chawla, M.; Lamb, C.; Casey, K.R.; Patel, S.; Silvestri, G.A.; Feller-Kopman, D.J. Technical Aspects of Endobronchial Ultrasound-Guided Transbronchial Needle Aspiration: CHEST Guideline and Expert Panel Report. Chest 2016, 149, 816–835. [Google Scholar] [CrossRef]
- Yarmus, L.; Akulian, J.; Gilbert, C.; Feller-Kopman, D.; Lee, H.J.; Zarogoulidis, P.; Lechtzin, N.; Ali, S.Z.; Sathiyamoorthy, V. Optimizing endobronchial ultrasound for molecular analysis: how many passes are needed? Ann Am Thorac Soc 2013, 10, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Wang, H.; Zerbo, A.; Beaudoin, S.; Ofiara, L.; Fiset, P.O.; Benedetti, A.; Gonzalez, A.V. Programmed Death Ligand 1 Testing of Endobronchial Ultrasound-guided Transbronchial Needle Aspiration Samples Acquired For the Diagnosis and Staging of Non-Small Cell Lung Cancer. J Bronchology Interv Pulmonol 2020, 27, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Diacon, A.H.; Schuurmans, M.M.; Theron, J.; Louw, M.; Wright, C.A.; Brundyn, K.; Bolliger, C.T. Utility of rapid on-site evaluation of transbronchial needle aspirates. Respiration 2005, 72, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Trisolini, R.; Cancellieri, A.; Tinelli, C.; Paioli, D.; Scudeller, L.; Casadei, G.P.; Forti Parri, S.; Livi, V.; Bondi, A.; Boaron, M.; Patelli, M. Rapid on-site evaluation of transbronchial aspirates in the diagnosis of hilar and mediastinal adenopathy: a randomized trial. Chest 2011, 139, 395–401. [Google Scholar] [CrossRef]
- Yarmus, L.; Van der Kloot, T.; Lechtzin, N.; Napier, M.; Dressel, D.; Feller-Kopman, D. A randomized prospective trial of the utility of rapid on-site evaluation of transbronchial needle aspirate specimens. J Bronchol Int Pulmonol 2011, 18, 121–127. [Google Scholar] [CrossRef]
- Marcoux, M.; Ost, D.E. What's new in endobronchial ultrasound for mediastinal staging? Curr Opin Pulm Med 2020, 26, 346–358. [Google Scholar] [CrossRef] [PubMed]
- Oki, M.; Saka, H.; Kitagawa, C.; Kogure, Y.; Murata, N.; Adachi, T.; Ando, M. Rapid on-site cytologic evaluation during endobronchial ultrasound-guided transbronchial needle aspiration for diagnosing lung cancer: a randomized study. Respiration 2013, 85, 486–492. [Google Scholar] [CrossRef]
- Trisolini, R.; Cancellieri, A.; Tinelli, C.; et al. Randomized trial of endobronchial ultrasound-guided transbronchial needle aspiration with and without rapid on-site evaluation for lung cancer genotyping. Chest 2015, 148, 1430–1437. [Google Scholar] [CrossRef]
- Tsaknis, G.; Naeem, M.; Rathinam, S.; Caswell, A.; Haycock, J.; McKenna, J.; Reddy, R.V. Utilization of high-pressure suction for EBUS-TBNA sampling in suspected lung Cancer. J Bronchology Interv Pulmonol 2022, 29, 115–124. [Google Scholar] [CrossRef]
- Fernandez-Bussy, S.; Biswas, A.; Labarca, G.; et al. Comparison of endobronchial ultrasound-guided transbronchial needle aspiration with stylet retracted partially versus completely for molecular testing. J Bronchol Int Pulmonol 2019, 26, 222–224. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xie, F.; Mao, X.; Zheng, X.; Li, Y.; Zhu, L.; Sun, J. Determining factors of endobronchial ultrasound-guided transbronchial needle aspiration specimens for lung cancer subtyping and molecular testing. Endosc Ultrasound 2019, 8, 404–411. [Google Scholar] [PubMed]
- Leighl, N.B.; Rekhtman, N.; Biermann, W.A.; Huang, J.; Mino-Kenudson, M.; Ramalingam, S.S.; West, H.; Whitlock, S.; Somerfield, M.R. Molecular testing for selection of patients with lung cancer for epidermal growth factor receptor and anaplastic lymphoma kinase tyrosine kinase inhibitors: American Society of Clinical Oncology endorsement of the College of American Pathologists/International Association for the study of lung cancer/association for molecular pathology guideline. J Clin Oncol 2014, 32, 3673–3679. [Google Scholar] [PubMed]
- Krogerus, L.; Kholov√°, I. Cell Block in Cytological Diagnostics: Review of Preparatory Techniques. Acta Cytol 2018, 62, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Santos, J.; Serra, P.; Andreo, F.; Llatjós, M.; Castellà, E.; Monsó, E. Contribution of cell blocks obtained through endobronchial ultrasound-guided transbronchial needle aspiration to the diagnosis of lung cancer. BMC Cancer 2012, 12, 34. [Google Scholar] [CrossRef]
- Martin-Deleon, R.; Teixido, C.; Lucena, C.M.; Martinez, D.; Fontana, A.; Reyes, R.; García, M.; Viñolas, N.; Vollmer, I.; Sanchez, M.; et al. EBUS-TBNA Cytological Samples for Comprehensive Molecular Testing in Non-Small Cell Lung Cancer. Cancers 2021, 13, 2084. [Google Scholar] [CrossRef]
- Jug, R.; Giovacchini, C.X.; Liu, B.; Green, C.L.; Clarke, J.M.; Mahmood, K.; Pavlisko, E.N. EBUS-FNA cytologic-histologic correlation of PD-L1 immunohistochemistry in non-small cell lung cancer. J Am Soc Cytopathol 2020, 9, 485–493. [Google Scholar] [CrossRef]
- Yoshimura, K.; Inoue, Y.; Karayama, M.; Tsuchiya, K.; Mori, K.; Suzuki, Y.; Iwashita, Y.; Kahyo, T.; Kawase, A.; Tanahashi, M.; et al. Heterogeneity analysis of PD-L1 expression and copy number status in EBUS-TBNA biopsy specimens of non-small cell lung cancer: Comparative assessment of primary and metastatic sites. Lung Cancer 2019, 134, 202–209. [Google Scholar] [CrossRef]
- Sakata, K.K.; Midthun, D.E.; Mullon, J.J.; Kern, R.M.; Nelson, D.R.; Edell, E.S.; Schiavo, D.N.; Jett, J.R.; Aubry, M.C. Comparison of Programmed Death Ligand-1 Immunohistochemical Staining Between Endobronchial Ultrasound Transbronchial Needle Aspiration and Resected Lung Cancer Specimens. Chest 2018, 154, 827–837. [Google Scholar] [CrossRef]
- 40 Ben Dori, S.; Aizic, A.; Sabo, E.; Hershkovitz, D. Spatial heterogeneity of PD-L1 expression and the risk for misclassification of PD-L1 immunohistochemistry in non-small cell lung cancer. Lung Cancer 2020, 147, 91–98. [Google Scholar] [CrossRef]
- Tajarernmuang, P.; Ofiara, L.; Beaudoin, S.; Wang, H.; Benedetti, A.; Gonzalez, A.V. Real-World Outcomes of Patients With Advanced Non-small Cell Lung Cancer Treated With Anti-PD1 Therapy on the Basis of PD-L1 Results in EBUS-TBNA vs Histological Specimens. Chest 2021, 160, 743–753. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.J.; Chan, H.P.; Soon, Y.Y.; Huang, Y.; Soo, R.A.; Kee, A.C.L. A systematic review and meta-analysis of the adequacy of endobronchial ultrasound transbronchial needle aspiration for next-generation sequencing in patients with non-small cell lung cancer. Lung Cancer 2022, 166, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Roy-Chowdhuri, S.; Mehrotra, M.; Bolivar, A.M.; Kanagal-Shamanna, R.; Barkoh, B.A.; Hannigan, B.; Zalles, S.; Ye, W.; Duose, D.; Broaddus, R. Salvaging the supernatant: next generation cytopathology for solid tumor mutation profiling. Mod Pathol 2018, 31, 1036. [Google Scholar] [CrossRef] [PubMed]
- Guibert, N.; Tsukada, H.; Hwang, D.H.; Chambers, E.; Cibas, E.S.; Bale, T.; Supplee, J.; Ulrich, B.; Sholl, L.M. Liquid biopsy of fine-needle aspiration supernatant for lung cancer genotyping. Lung Cancer 2018, 122, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Hannigan, B.; Ye, W.; Mehrotra, M.; Lam, V.; Bolivar, A.; Zalles, S.; Barkoh, B.A.; Duose, D.; Hu, P.C.; Broaddus, R. Liquid biopsy assay for lung carcinoma using centrifuged supernatants from fine-needle aspiration specimens. Ann Oncol 2019, 30, 963–969. [Google Scholar] [CrossRef] [PubMed]
- Marcoux, M.; Ost, D.E. What's new in endobronchial ultrasound for mediastinal staging? Curr Opin Pulm Med 2020, 26, 346–358. [Google Scholar] [CrossRef]
- Chaft, J.E.; Rimner, A.; Weder, W.; Azzoli, C.G.; Kris, M.G.; Cascone, T. Evolution of systemic therapy for stages I-III non-metastatic non-small-cell lung cancer. Nat Rev Clin Oncol 2021, 18, 547–557. [Google Scholar] [CrossRef]
- Wu, Y.L.; Tsuboi, M.; He, J.; John, T.; Grohe, C.; Majem, M.; Goldman, J.W.; Laktionov, K.; Kim, S.W.; Kato, T.; et al. Osimertinib in Resected EGFR-Mutated Non-Small-Cell Lung Cancer. N Engl J Med 2020, 383, 1711–1723. [Google Scholar] [CrossRef]
- Shukla, N.; Hanna, N. Neoadjuvant and Adjuvant Immunotherapy in Early-Stage Non-Small Cell Lung Cancer. Lung Cancer 2021, 12, 51–60. [Google Scholar] [CrossRef]
- Tsuboi, M.; Weder, W.; Escriu, C.; Blakely, C.; He, J.; Dacic, S.; Yatabe, Y.; Zeng, L.; Walding, A.; Chaft, J.E. Neoadjuvant osimertinib with/without chemotherapy versus chemotherapy alone for EGFR-mutated resectable non-small-cell lung cancer: NeoADAURA. Future Oncol 2021, 17, 4045–4055. [Google Scholar] [CrossRef]
- Cao, C.; Guo, A.; Chen, C.; Chakos, A.; Bott, M.; Yang, C.J.; Zielinski, R.; Melfi, F. Systematic Review of Neoadjuvant Immunotherapy for Patients With Non-Small Cell Lung Cancer. Semin Thorac Cardiovasc Surg 2021, 33, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Hofman, P. The challenges of evaluating predictive biomarkers using small biopsy tissue samples and liquid biopsies from non-small cell lung cancer patients. J Thorac Dis 2019, 11, S57–S64. [Google Scholar] [CrossRef]
- Hofman, P. EGFR Status Assessment for Better Care of Early Stage Non-Small Cell Lung Carcinoma: What Is Changing in the Daily Practice of Pathologists? Cells 2021, 10, 2157. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, C.; Bubendorf, L.; Cooper, W.A.; Illei, P.; Borralho Nunes, P.; Ong, B.H.; Tsao, M.S.; Yatabe, Y.; Kerr, K.M. Molecular testing in stage I-III non-small cell lung cancer: Approaches and challenges. Lung Cancer 2021, 162, 42–53. [Google Scholar] [CrossRef]
- Agrawal, S.; Goel, A.D.; Gupta, N.; Lohiya, A.; Gonuguntla, H.K. Diagnostic utility of endobronchial ultrasound (EBUS) features in differentiating malignant and benign lymph nodes-a systematic review and meta-analysis. Respir Med 2020, 171, 106097. [Google Scholar] [CrossRef] [PubMed]
- Izumo, T.; Sasada, S.; Chavez, C.; Matsumoto, Y.; Tsuchida, T. Endobronchial ultrasound elastography in the diagnosis of mediastinal and hilar lymph nodes. Jpn J Clin Oncol 2014, 44, 956–962. [Google Scholar] [CrossRef]
- Fournier, C.; Dhalluin, X.; Wallyn, F.; Machuron, F.; Bouchindhomme, B.; Copin, M.C.; Valentin, V. Performance of Endobronchial Ultrasound Elastography in the Differentiation of Malignant and Benign Mediastinal Lymph Nodes: Results in Real-life Practice. J Bronchology Interv Pulmonol 2019, 26, 193–198. [Google Scholar] [CrossRef]
- Hern√°ndez Roca, M.; P√©rez Pallar√©s, J.; Prieto Merino, D.; Del Mar Valdivia Salas, M.; Solano, J.G.; Fern√°ndez √Ålvarez, J.; Lozano Vicente, D.; Wasniewski, S.; Mart√≠nez D√≠az, J.J.; Torregrosa, C.E.; et al. Diagnostic Value of Elastography and Endobronchial Ultrasound in the Study of Hilar and Mediastinal Lymph Nodes. J Bronchology Interv Pulmonol 2019, 26, 184–192. [Google Scholar] [CrossRef]
- Verhoeven, R.L.J.; de Korte, C.L.; van der Heijden, E. Optimal endobronchial ultrasound strain elastography assessment strategy: an explorative study. Respiration 2019, 97, 337–347. [Google Scholar] [CrossRef]
- Fujiwara, T.; Nakajima, T.; Inage, T.; Sata, Y.; Sakairi, Y.; Tamura, H.; Wada, H.; Suzuki, H.; Chiyo, M.; Yoshino, I. The combination of endobronchial elastography and sonographic findings during endobronchial ultrasound-guided transbronchial needle aspiration for predicting nodal metastasis. Thorac Cancer 2019, 10, 2000–2005. [Google Scholar] [CrossRef]
- Trisolini, R.; Verhoeven, R.L.J.; Cancellieri, A.; De Silvestri, A.; Natali, F.; Van der Heijden, E. Role of endobronchial ultrasound strain elastography in the identification of fibrotic lymph nodes in sarcoidosis: a pilot study. Respirology 2020, 25, 1203–1206. [Google Scholar] [CrossRef] [PubMed]
- Abedini, A.; Razavi, F.; Farahani, M.; Hashemi, M.; Emami, H.; Mohammadi, F.; Kiani, A. The utility of elastography during EBUS-TBNA in a population with a high prevalence of anthracosis. Clin Respir J 2020, 14, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Casoni, G.L.; Gurioli, C.; Romagnoli, M.; Poletti, V. Diagnosis of pulmonary thromboembolism with endobronchial ultrasound. Eur Respir J 2008, 32, 1416–1417. [Google Scholar] [CrossRef]
- Aumiller, J.; Herth, F.J.; Krasnik, M.; Eberhardt, R. Endobronchial ultrasound for detecting central pulmonary emboli: a pilot study. Respiration 2009, 77, 298–302. [Google Scholar] [CrossRef]
- Hunsaker, A.R.; Lu, M.T.; Goldhaber, S.Z.; Rybicki, F.J. Imaging in acute pulmonary embolism with special clinical scenarios. Circ Cardiovasc Imaging 2010, 3, 491–500. [Google Scholar] [CrossRef]
- Bertini, P.; Ribechini, A.; Guarracino, F. Improved diagnosis of pulmonary embolism causing cardiac arrest by combined endobronchial ultrasound and echocardiography. Cardiovasc Ultrasound 2020, 18, 25. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, R.; Corcoran, J.P.; Maldonado, F.; Feller-Kopman, D.; Janssen, J.; Astoul, P. Advanced medical interventions in pleural disease. Eur Respir Rev 2016, 25, 199–213. [Google Scholar] [CrossRef]
- Kassier, M.; et al. Sampling pleural nodules with an EBUS scope: A novel application. Respiratory Medicine Case Reports 2018, 25, 36–38. [Google Scholar] [CrossRef]
- Lococo, F.; Rossi, G.; Agostini, L.; Filice, A.; Paci, M.; Rapicetta, C. "Dry" pleural mesothelioma successfully diagnosed on endobronchial ultrasound (EBUS)-guided transbronchial needle aspiration (TBNA). Intern Med 2014, 53, 467–469. [Google Scholar] [CrossRef]
- DeWitt, J.; Kongkam, P.; Attasaranya, S.; LeBlanc, J.K.; Sherman, S.; Sheski, F.D. Endoscopic ultrasound-guided transesophageal thoracentesis. Endoscopy 2008, 40, E118–E119. [Google Scholar] [CrossRef]
- Cocciardi, S.; Borah, A.; Terrigno, R.; Abouzgheib, W.; Boujaoude, Z. A case report of an expensive yet necessary thoracentesis. Expanding the boundaries of endoscopic ultrasound transbronchial needle aspiration. Medicine (Baltimore) 2019, 98, e17555. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.K.; Khanna, A.; Talwar, D. Endobronchial ultrasound: A new technique of pericardiocentesis in posterior loculated pericardial effusion. Chest 2016, 150, e121–e123. [Google Scholar] [CrossRef] [PubMed]
- Ceron, L.; Manzato, M.; Mazzaro, F.; Bellavere, F. A new diagnostic and therapeutic approach to pericardial effusion: transbronchial needle aspiration. Chest 2003, 123, 1753–1758. [Google Scholar] [CrossRef]
- Madan, K.; Mittal, S.; Hadda, V.; Jain, D.; Mohan, A.; Guleria, R. Endobronchial ultrasound-guided transbronchial needle aspiration of thyroid: Report of two cases and systematic review of literature. Lung India 2016, 33, 682–687. [Google Scholar] [CrossRef]
- Kennedy, M.P.; Breen, M.; O'Regan, K.; McCarthy, J.; Horgan, M.; Henry, M.T. Endobronchial ultrasound-guided transbronchial needle aspiration of thyroid nodules: Pushing the boundary too far? Chest 2012, 142, 1690–1691. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Deng, Y.; Tin, M.S.; Lok, V.; Ngai, C.H.; Zhang, L.; Lucero-Prisno, D.E.; Xu, W.; Zheng, Z.J.; Elcarte, E.; Withers, M.; Wong, M.C.S. Distribution, Risk Factors, and Temporal Trends for Lung Cancer Incidence and Mortality: A Global Analysis. Chest 2022, 161, 1101–1111. [Google Scholar] [CrossRef]
- DeMaio, A.; Sterman, D. Bronchoscopic intratumoural therapies for non-small cell lung cancer. Eur Respir Rev 2020, 29, 200028. [Google Scholar] [CrossRef]
- Celikoglu, F. Intratumoural chemotherapy of lung cancer for diagnosis and treatment of draining lymph node metastasis. J Pharm Pharmacol 2010, 62, 287–295. [Google Scholar] [CrossRef]
- Marabelle, A.; Tselikas, L.; de Baere, T.; et al. Intratumoural immunotherapy: using the tumour as the remedy. Ann Oncol 2017, 28, xii33–xii43. [Google Scholar] [CrossRef]
- Hohenforst-Schmidt, W.; Zarogoulidis, P.; Darwiche, K.; Vogl, T.; Goldberg, E.P.; Huang, H.; Simoff, M.; Li, Q.; Browning, R.; Turner, F.J.; Le Pivert, P.; et al. Intratumoural chemotherapy for lung cancer: re-challenge current targeted therapies. Drug Des Devel Ther 2013, 7, 571–583. [Google Scholar]
- Mori, V.; Roy, G.S.; Bates, J.H.T.; Kinsey, C.M. Cisplatin pharmacodynamics following endobronchial ultrasound-guided transbronchial needle injection into lung tumours. Sci Rep 2019, 9, 6819. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Anker, C.J.; Garrison, G.; Kinsey, C.M. Endobronchial ultrasound-guided transbronchial needle injection for local control of recurrent non-small cell lung cancer. Ann Am Thorac Soc 2015, 12, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Lu, B.; Sun, L.; Yan, X.; Ai, Z.; Xu, J. Intratumoral chemotherapy with paclitaxel liposome combined with systemic chemotherapy: a new method of neoadjuvant chemotherapy for stage III unresectable non-small cell lung cancer. Med Oncol 2015, 32, 345. [Google Scholar] [CrossRef] [PubMed]
- Zarogoulidis, P.; et al. Intratumoral Treatment with Chemotherapy and Immunotherapy for NSCLC with EBUS-TBNA 19G. J Cancer 2021, 12, 2560–2569. [Google Scholar] [CrossRef] [PubMed]
- Mori, V.; Bates, J.H.T.; Jantz, M.; Mehta, H.J.; Kinsey, C.M. A computational modeling approach for dosing endoscopic intratumoral chemotherapy for advanced non-small cell lung cancer. Sci Rep 2022, 12, 44. [Google Scholar] [CrossRef] [PubMed]
- Hwangbo, B.; Lee, H.S.; Lee, G.K.; Lim, K.Y.; Lee, S.H.; Kim, H.Y.; Lee, J.; Zo, J.I. Transoesophageal needle aspiration using a convex probe ultrasonic bronchoscope. Respirology 2009, 14, 843–849. [Google Scholar] [CrossRef]
- Herth, F.J.; Krasnik, M.; Kahn, N.; Eberhardt, R.; Ernst, A. Combined endoscopic-endobronchial ultrasound-guided fine-needle aspiration of mediastinal lymph nodes through a single bronchoscope in 150 patients with suspected lung cancer. Chest. 2010, 138, 790–794. [Google Scholar] [CrossRef]
- Oki, M.; Saka, H.; Ando, M.; Tsuboi, R.; Nakahata, M.; Oka, S.; Kogure, Y.; Kitagawa, C. Transbronchial vs transesophageal needle aspiration using an ultrasound bronchoscope for the diagnosis of mediastinal lesions: a randomized study. Chest 2015, 147, 1259–1266. [Google Scholar] [CrossRef]
- Chapman, G.S.; Kumar, D.; Redmond, J.; Munderloh, S.H.; Gandara, D.R. Upper abdominal computerized tomography scanning in staging non-small cell lung carcinoma. Cancer 1984, 54, 1541–1543. [Google Scholar] [CrossRef]
- Ettinghausen, S.E.; Burt, M.E. Prospective evaluation of unilateral adrenal masses in patients with operable non-small-cell lung cancer. J Clin Oncol 1991, 9, 1462–1466. [Google Scholar] [CrossRef]
- Christiansen, I.S.; Ahmad, K.; Bodtger, U.; Naur, T.M.H.; Sidhu, J.S.; Nessar, R.; Salih, G.N.; H√∏egholm, A.; Annema, J.T.; Clementsen, P.F. EUS-B for suspected left adrenal metastasis in lung cancer. J Thorac Dis 2020, 12, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Crombag, L.M.; Annema, J.T. Left Adrenal Gland Analysis in Lung Cancer Patients Using the Endobronchial Ultrasound Scope: A Feasibility Trial. Respiration 2016, 91, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, I.S.; Bodtger, U.; Naur, T.M.H.; Ahmad, K.; Singh Sidhu, J.; Nessar, R.; Salih, G.N.; H√∏egholm, A.; Annema, J.T.; Clementsen, P.F. EUS-B-FNA for Diagnosing Liver and Celiac Metastases in Lung Cancer Patients. Respiration 2019, 98, 428–433. [Google Scholar] [CrossRef] [PubMed]
- El, H.I.; Wu, H.; Reuss, S.; Randolph, M.; Harris, A.; Gromski, M.A.; Al-Haddad, M. Prospective Assessment of the Performance of a New Fine Needle Biopsy Device for EUS-Guided Sampling of Solid Lesions. Clin. Endosc 2018, 51, 576–583. [Google Scholar]
- Balwan, A.; Bixby, B.; Grotepas, C.; Witt, B.L.; Iravani, A.; Ansari, S.; Reddy, C.B. Core needle biopsy with endobronchial ultrasonography: single center experience with 100 cases. J Am Soc Cytopathol 2020, 9, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Gu, Y.; Wang, H.; Yu, D.; Zhang, H.; Wang, H. Novel ProCore 25-gauge needle for endobronchial ultrasound-guided transbronchial needle aspiration reduces the puncture time and frequency, with comparable diagnostic rate for mediastinal and hilar lymphadenopathy. Thorac Cancer 2020, 11, 748–753. [Google Scholar] [CrossRef]
- Dhooria, S.; Sehgal, I.S.; Prasad, K.T.; Muthu, V.; Gupta, N.; Bal, A.; Ram, B.; Aggarwal, A.N.; Agarwal, R. Diagnostic yield and safety of the ProCore versus the standard EBUS-TBNA needle in subjects with suspected sarcoidosis. Expert Rev Med Devices 2021, 18, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Ghori, U.; Chaddha, U.; Murgu, S. Combined EBUS-IFB and EBUS-TBNA vs EBUS-TBNA Alone for Intrathoracic Adenopathy: A Meta-Analysis. Ann Thorac Surg 2021. [Google Scholar] [CrossRef]
- Gonuguntla, H.K.; Shah, M.; Gupta, N.; Agrawal, S.; Poletti, V.; Nacheli, G.C. Endobronchial ultrasound-guided transbronchial cryo-nodal biopsy: a novel approach for mediastinal lymph node sampling. Respirol Case Rep 2021, 9, e00808. [Google Scholar] [CrossRef]
- Zhang, J.; Guo, J.R.; Huang, Z.S.; Fu, W.L.; Wu, X.L.; Wu, N.; Kuebler, W.M.; Herth, F.J.F.; Fan, Y. Transbronchial mediastinal cryobiopsy in the diagnosis of mediastinal lesions: a randomised trial. Eur Respir J 2021, 58, 2100055. [Google Scholar] [CrossRef]
- Bandyopadhyay, D.; Panchabhai, T.S.; Mehta, A.C. EBUS-TBNA for the diagnosis of lymphoma. Still an Achilles heel. Ann Am Thorac Soc 2015, 12, 1263–1264. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Oliv√©, I.; Mons√≥, E.; Andreo, F.; Sanz-Santos, J.; Taron, M.; Molina-Vila, M.A.; Llatj√≥s, M.; Castell√†, E.; Moran, T.; Bertran-Alamillo, J.; et al. Endobronchial ultrasound-guided transbronchial needle aspiration for identifying EGFR mutations. Eur Respir J 2010, 35, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Rooper, L.M.; Nikolskaia, O.; Carter, J.; Ning, Y.; Lin, M.; Maleki, Z. A single EBUS-TBNA procedure can support a large panel of immunohistochemical stains, specific diagnostic subtyping, and multiple gene analyses in the majority of non-small cell lung cancer cases. Hum Pathol 2016, 51, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Zhang, A.; Wu, X.; Huang, Z.; Kontogianni, K.; Sun, K.; Fu, W.; Wu, N.; Kuebler, W.M.; Herth, F.G.F. Transbronchial needle aspiration combined with cryobiopsy in the diagnosis of mediastinal diseases: a multicentre, open-label, randomised trial. Lancet Respir Med 2023, 11, 256–264. [Google Scholar] [CrossRef]
Figure 1.
Echoendoscopic (A) and CT scan (B) image of pulmonary embolism of the right pulmonary artery.
Figure 1.
Echoendoscopic (A) and CT scan (B) image of pulmonary embolism of the right pulmonary artery.
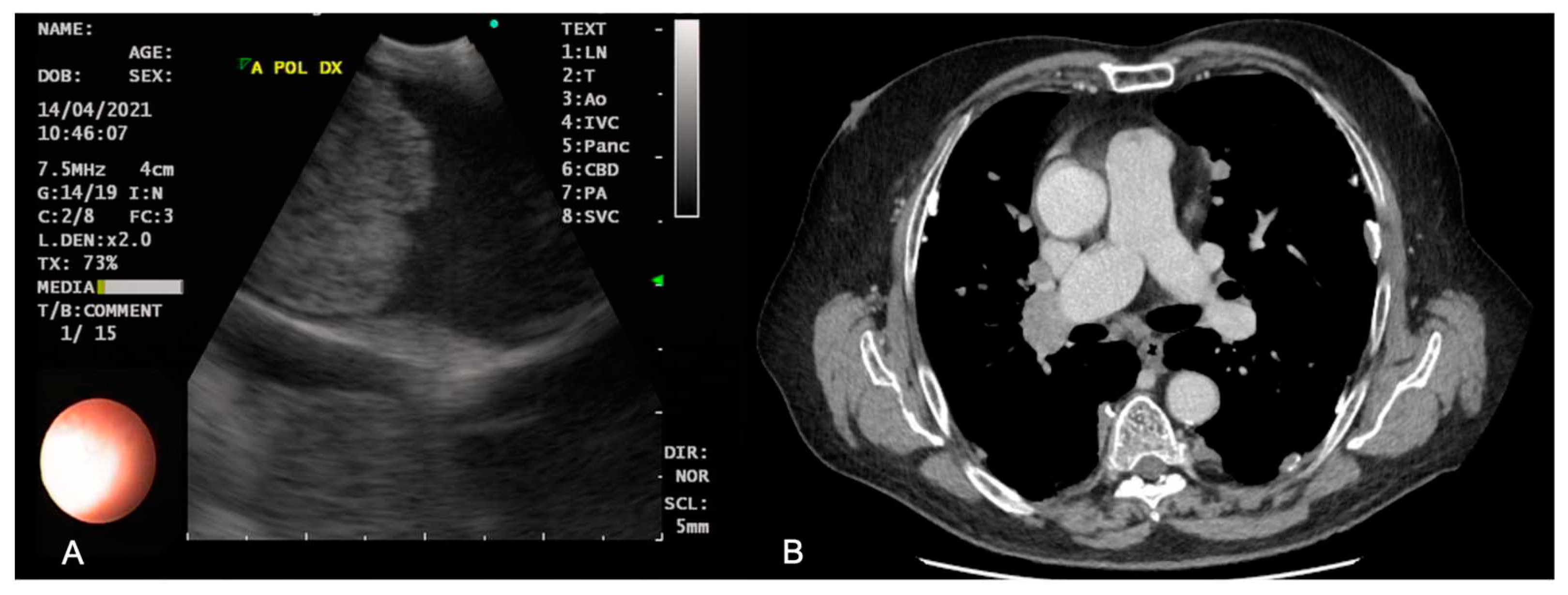
Figure 2.
Sites available to perform EBUS-TBNA. Blue circles represent the main mediastinal stations reachable only by EBUS, light blue circles represent lymph node stations reachable only by EUS-B-FNA and green circles represent lymph node stations reachable by both EBUS and EUS-B-FNA.
Figure 2.
Sites available to perform EBUS-TBNA. Blue circles represent the main mediastinal stations reachable only by EBUS, light blue circles represent lymph node stations reachable only by EUS-B-FNA and green circles represent lymph node stations reachable by both EBUS and EUS-B-FNA.
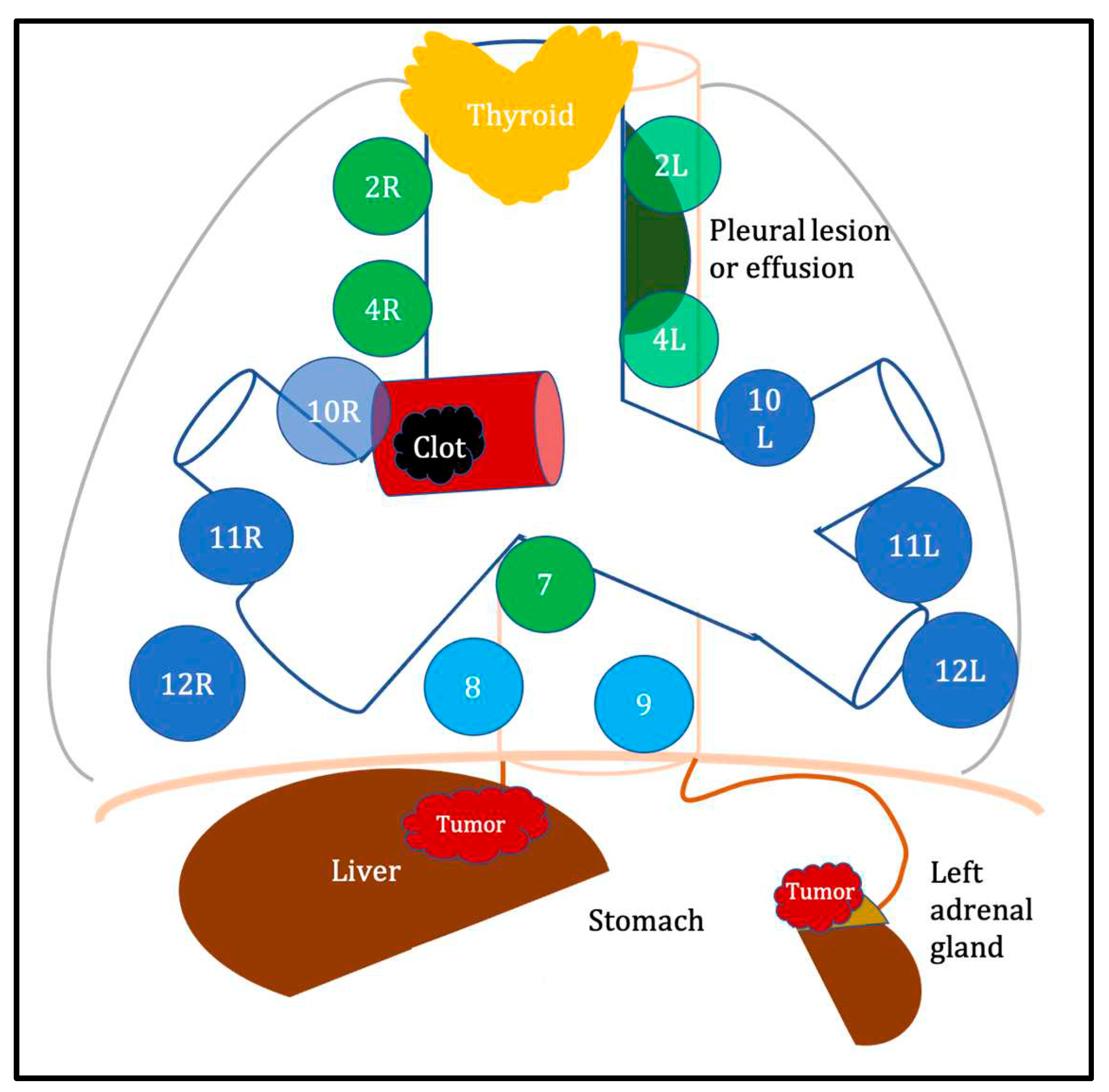

Table 1.
Non-ordinary applications of endoscopic ultrasound.
| Indication | Specific complementary tools | Advantages | Disadvantages | References |
|---|---|---|---|---|
| Pulmonary vessel assessment | Color Doppler; echocardiography | Bedside feasibility; not contraindicated in kidney failure, pregnancy and allergy to contrast medium | Poor sensibility in peripheral pulmonary embolism | [63,64,65,66] |
| Pleural lesion sampling | - | Minimally invasive compared to surgery | Limited to lesions located next to airways or esophagus | [67,68] |
| Pleural/pericardial effusion drainage/sampling | - | Valuable option in loculated effusions | Potential infection | [70,71,72,73] |
| Thyroid lesion sampling | - | Valuable option in intrathoracic goiter/thyroid lesions | Potential infection | [74,75] |
| Intratumoral therapy | Computational modeling to design delivery strategy | Higher concentration at tumor site with lower systemic side effects | Risk of extravasation and airway irritation | [77,78,79,80,81,82,83,84,85] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



