
Submitted:
25 May 2023
Posted:
26 May 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The coronavirus disease 2019 (COVID-19) pandemic has disrupted health care worldwide. As the pandemic has been prolonged, quarantine restrictions have been lightened gradu-ally, which can influence outcomes of pediatric patients with chronic disease such as epi-lepsy by increase of susceptibility of the COVID-19 infection. The aim of this study was to determine impacts of COVID-19 pandemic on seizure control and identify potential risk factors that might worsen seizure attacks during the pandemic in children with epilepsy. We performed a retrospective chart review of 48 pediatric patients with epilepsy during the COVID-19 pandemic from January 2016 to July 2022.
During the COVID-19 pandemic period, 25% of pediatric patients experienced sei-zure worsening, showing an increase in seizure frequency or duration or both.
Factors associated with worsening seizures during pandemic were: diagnosis of epi-lepsy less than one year, comorbid conditions with cerebral palsy or having a tracheosto-my or a PEG, and infection with other viruses (respiratory syncytial virus, influenza virus A, influenza virus B) rather than COVID-19 infection.
Our finding highlights the need to proactively monitor and regularly follow up (es-pecially short period of time) patients after they are diagnosed with epilepsy. It is also important to properly manage those who are susceptible to serious illness and keep sea-sonal viral infections under surveillance to manage exacerbated seizure in children with epilepsy. Furthermore, pediatric physicians should not overlook surveillance of seasonal respiratory viruses since quarantine restrictions are getting eased.
Keywords:
COVID19
; Children
; Epilepsy
; Adolescents
; Pediatric
; Pandemic
1. Introduction
Epilepsy is one of the most frequent neurological conditions in children. It is associated with a high economic cost, development of intellectual disability, psychiatric and cognitive comorbidities, and a high risk of injury and mortality [1,2,3,4,5].
Although childhood onset epilepsy has self-limiting seizures in most cases, about one-third of these children develop antiseizure medication (ASM) resistant epilepsy requiring more optimizing, advanced, and sophisticated medical therapy.
The World Health Organization (WHO) declared the new coronavirus disease (COVID-19) to be a pandemic on March 11, 2020. The COVID-19 pandemic has affected the health system in the entire world, resulting in significant economic damage [6]. It is well known that the COVID-19 pandemic is psychologically stressful for people worldwide, including patients with epilepsy. Patients with epilepsy are more vulnerable to psychological effects of the COVID-19 pandemic than the normal population [7]. Since psychological stress and psychiatric disorder such as anxiety and depression might exacerbate seizures, comorbidities associated with epilepsy should also be taken into account.
Fortunately, children are less frequently affected by COVID-19 infection. They show less severe symptoms, lower morbidity, and mortality than adults after COVID-19 infection [6,8,9]. In addition, people with epilepsy are not considered to have a greater risk of COVID-19 infection overall than normal population.
Moreover, acute symptomatic seizures do not seem to occur very often. Complications of COVID-19 infection in children resulting from the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) occur in approximately less than 0.5% [10].
Given that the COVID-19 pandemic period is prolonged, the rate of COVID-19 infection in children began to increase, including in children with epilepsy, which significantly impacted epilepsy outcome [11]. Since it has been three years into the COVID-19 pandemic, seizure control might hit a new turning point in this group. Thus, considering the relationship between epilepsy and COVID-19 pandemic era is crucial. So far, very limited studies have published outcomes of seizure controls. Studies on seizure risk factors during the COVID-19 pandemic in pediatric population have not been reported yet.
Hence, the purpose of this retrospective longitudinal cohort study was to assess impacts of the COVID-19 pandemic on epilepsy characteristics and seizure control (type, frequency etc.) for pediatric patients with epilepsy and to identify potential risk factors that might exacerbate seizures during the pandemic period.
2. Materials and Methods
We retrospectively reviewed charts of children and adolescents with epilepsy aged 0 to 18 years at The Catholic University of Korea Yeouido St. Mary's Hospital from January 2016 to July 2022. Children were eligible for inclusion if they were treated for epilepsy at least 6 months before the COVID-19 pandemic and followed up for more than 6 months since April 2020. Patients who were diagnosed with psychological disorders or psychogenic nonepileptic seizures and those who were not followed up during the COVID-19 pandemic were excluded.
One pediatric neurologist reviewed medical charts and collected data including demographics (age, gender, socioeconomic state), age at a diagnosis of epilepsy, electroencephalography (EEG) findings, the number of ASM, and comorbidities associated with epilepsy. Outcomes of seizures during the COVID-19 pandemic were assessed and defined based on unchanged, increased and decreased seizure frequency or seizure duration. Psychologic and physiological factors (sleep cycle, physical activity, exposure to other viruses and SARS-CoV-2, and accessibility to healthcare) during the COVID-19 pandemic era were also obtained.
Definition of epilepsy and classification of seizures were performed according to categories proposed by the International League Against Epilepsy (ILAE) in 2014 and 2017, respectively [12,13].
All statistical analyses were conducted with SSPS software version 26.0 (IBM Corp., Armonk, NY, USA). Two-tailed chi-square or Fisher exact test was used for comparisons of categorical data. Continuous variables with normal distributions were evaluated with independent t-test. Mann-Whitney test was used for continuous variables with non-normal distributions. Multivariate logistic regression was used to identify potential risk factors exacerbating seizures during the COVID-19 pandemic. Probability values less than 0.05 were considered as statistically significant. This study was approved by the Institutional Review Board of The Catholic University of Korea (SC23RISI0028).
3. Results
3.1. Demographic and clinical characteristics of children with epilepsy before COVID-19 pandemic
In our study, a total of 84 pediatric patients (38 girls, 46 boys) with epilepsy during the COVID-19 pandemic were included in this study. Demographic and clinical characteristics of children before the COVID-19 pandemic are shown in Table 1. Mean age of the 84 patients was 10.8 years (range, 2-15 years) and mean age at onset of seizures was 3.5 years (range, 1 month-13 years). A quarter of patients had a middle/high socioeconomic status with caregivers employed, health insured, and having adequate income whereas 20% of patient were living with unearned incomes.
Half patients with epilepsy had both localized and generalized or unclassified seizures, 30% had generalized seizures, and 14% had localized seizures. More than two-third (77%) of patients were taking antiseizure medication (ASM) as a single treatment (monotherapy) before the COVID-19 pandemic. Patients who had no comorbidities or were not classified accounted for the most (two-thirds), followed by those with neuropsychiatric disorders (13%) and those with developmental delay and intellectual disability (8%).
3.2. Seizure changes during the COVID-19 pandemic era
Among 85 patients, 25% experienced seizure worsening, with either an increase in seizure frequency (18%) or duration (13%) or both (6%) during the pandemic period (Table 2). Vice versa, half of their EEG data were unchanged or better whereas only 8% of those showed worsen EEG data. Furthermore, 42% of patients’ EEG data were missing or undone.
3.3. Risk factors of significantly worsening seizures during the COVID-19 pandemic
Twenty-one (25%) of 85 patients experienced significantly worsening seizures (Table 3). The duration for diagnosis of epilepsy in patients without worsening seizures was significantly longer (more than three years) than those with worsening seizures (p = 0.043). Moreover, patients with comorbid conditions such as cerebral palsy, living with percutaneous gastrostomy (PEG), or tracheostomy state in addition to epilepsy had significantly worsening seizures (p = 0.035). However, a quarter of patients were exposed to SARS-CoV-2 with or without worsening seizures during the COVID pandemic, showing no significant difference (p = 0.065) between two groups. Interestingly, infection by other viruses (e.g., respiratory syncytial virus, influenza viruses) was significantly higher in patients with worsening seizures (p < 0.001) than those without worsening seizures.

Table 3.
Comparison of risk factors aggravating seizures during the COVID pandemic.
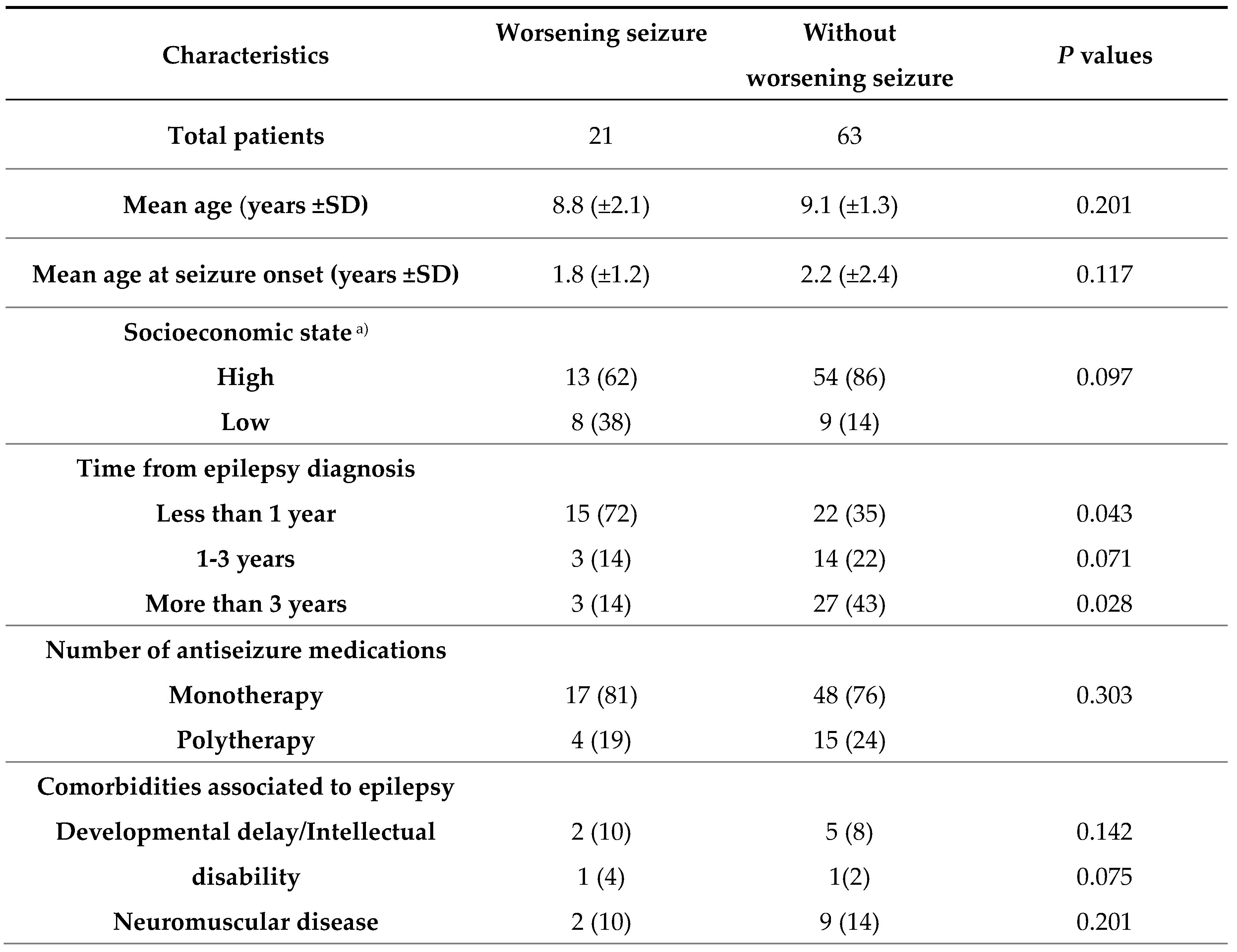
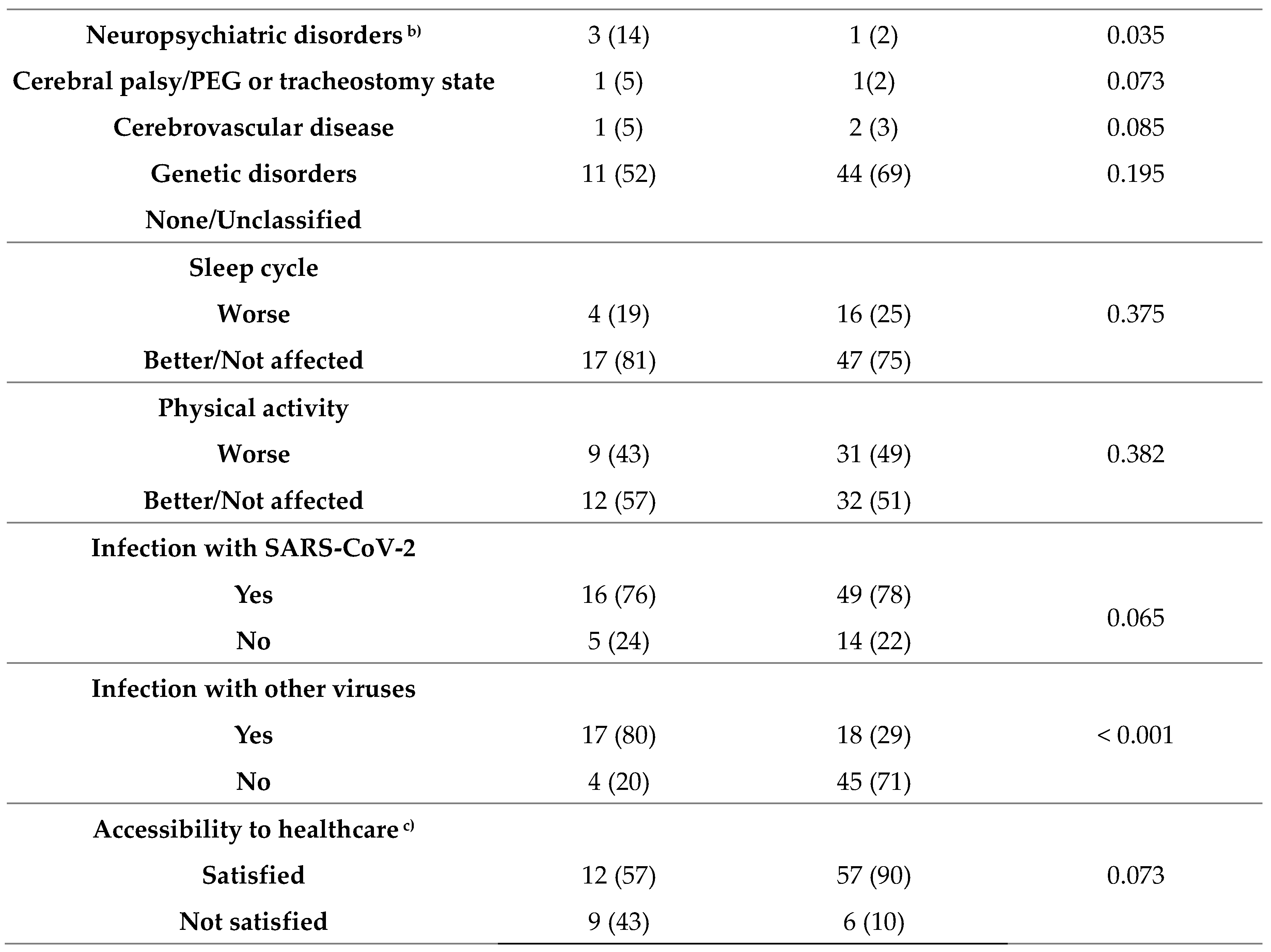
SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; a) high socioeconomic state included health insurance. b) neuropsychiatric disorder included autism spectrum disorders or attention deficit hyperactivity disorders. c) accessibility to healthcare included obtaining antiseizure medication, accessing outpatient care and emergency department.
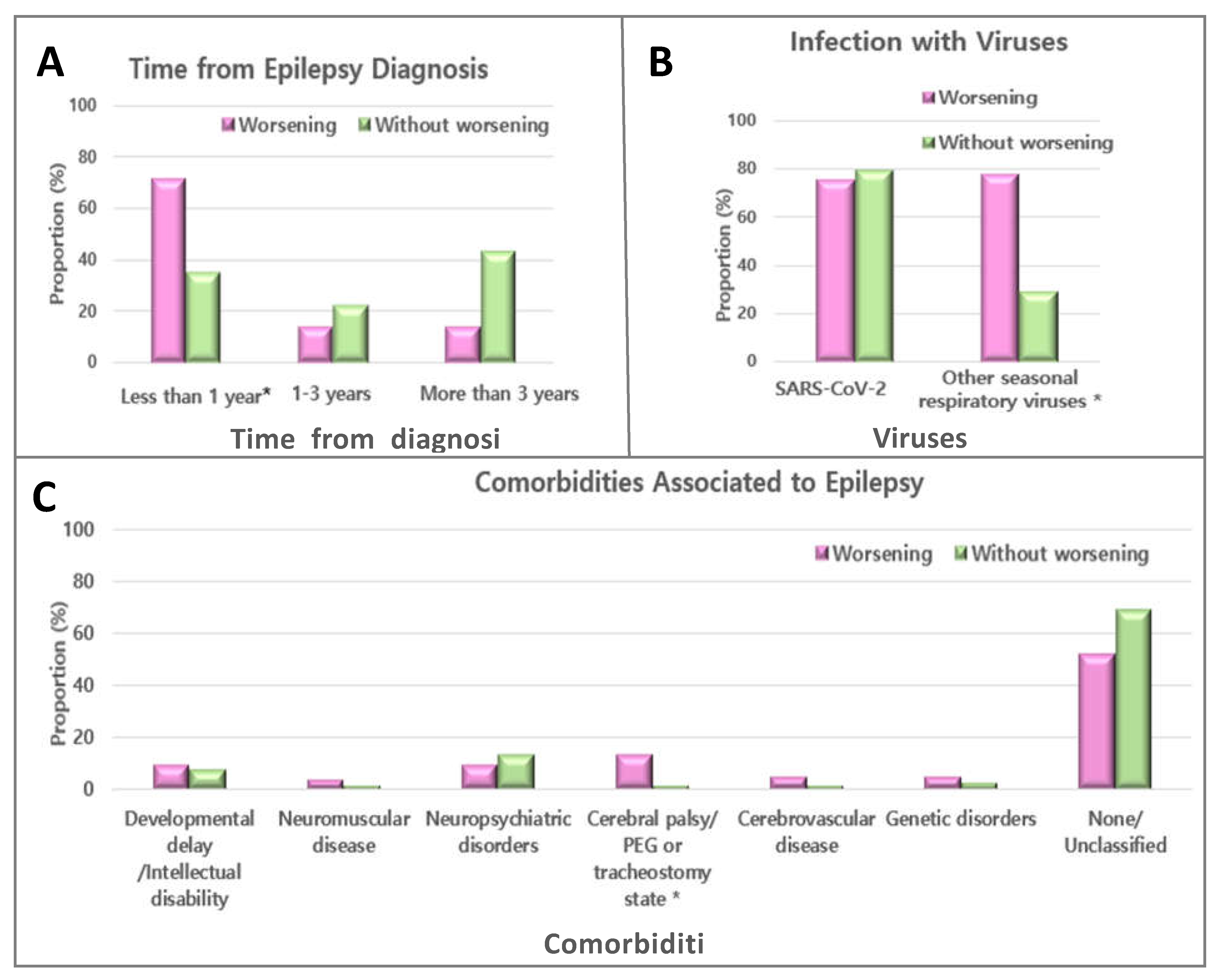
Figure 1.
Factors with and without worsening seizures during the coronavirus disease 19 pandemic in pediatric patients with epilepsy.
Figure 1.
Factors with and without worsening seizures during the coronavirus disease 19 pandemic in pediatric patients with epilepsy.
4. Discussion
The COVID-19 pandemic has afflicted multiple fields including epilepsy-associated field worldwide. Since the pandemic and risks to patients with epilepsy are getting longer and higher, it is important to discuss risk factors affecting seizure exacerbation during the COVID-19 pandemic in children with epilepsy.
In this study, we investigated the impact of COVID-19 pandemic on pediatric patients with epilepsy and risk factors for worsening seizures. While some patients did not show significant changes, not a few proportions suffered from deterioration in their health and quality of life. Overall, a total 25% experienced seizure worsening during the COVID-19 pandemic, leaving three-quarter of patients showed stable or unchanged seizure frequency and duration. This result is consistent with the literature conducted by Momani et al. showing that 22.7% of children under the age of 16 reported worsened seizure control during the COVID-19 pandemic lockdown in 2021 in Jordan [14]. Studies that supporting similar results have been reported not only in children, but also in adults. In Saudi Arabia and Spain, seizure frequency was increased in 27% and 29.5% of adult patients of epilepsy, respectively [7,15]. Likewise, one-fourth showed increased seizure frequency during the pandemic in Brazil in 2021 [16]. However, many studies including our cohort study evaluating patients with epilepsy around the COVID-19 lockdown period in 2020 revealed that the prevalence of worsening seizure control was lower than that in the current study [17,18,19,20]. Such difference might be due to different sample size and age as current studies targeted patients younger than those of previous studies. Given that most studies were conducted before winter 2020, the rise of other respiratory viruses causing severe respiratory infection starting from late autumn in 2020 [21] might have also contributed to various neurological issues including worsening of seizures.
Of 25% of patients with worsening seizures, only 8% showed worsened EEG since EEG was not done or cancelled for 42% of patients due to their difficulties accessing medicine. Thus, both outpatient EEG and EEG monitoring were affected by the pandemic. Similarly, two surveys of pediatric neurologists have reported that the COVID-19 pandemic has reduced chances of EEG evaluation to 75 and 90% [22,23], respectively. Thus, the social impact of COVID-19 changed dramatically during the lockdown period. Accessibility of patients with epilepsy to healthcare facilities was greatly restricted, especially during the early phase when the spread of COVID-19 was rapid around the world.
Our results showed that patients were highly susceptible to COVID-19. One-third patients were infected with SARS-CoV-2. However, reasons for seizure worsening were not due to COVID-19 infection, but due to other factors that already existed or emerged during the pandemic.
Our findings showed that risks of seizures during the pandemic were significantly increased for children who were diagnosed with epilepsy less than 1 year, those who were having cerebral palsy or having a tracheostomy or a PEG, and those who were infected with other viruses (respiratory syncytial virus, influenza virus A, influenza virus B). Some similar factors such as poor access to healthcare and difficulties to obtain ASMs have been reported from separate literatures [24]. Children with shorter duration of epilepsy (diagnosed for less than 1 year) might have variable seizure frequency at baseline. Their ASMs should be adjusted more precisely by checking side effects routinely and by monitoring EEG. However, problems in accessing health system for epilepsy treatment including changing of ASMs regimen and restricted access to EEG or monitoring units might have played a role in worsening seizure control in our study, in accordance with data published previously regardless of ethics or national income [24]. According to previous studies, more than 90% of pediatric neurological health care service have been affected by difficulty accessing epilepsy professionals and medicine, decreased access to EEG, restricted outpatient or admission in epilepsy units, and cancellations [17,24] that might have contributed to their worsening seizure control and exacerbated their comorbidities.
However, two-third of patients with epilepsy satisfied with accessibility to healthcare regardless seizure frequency in the current study. Most of Korean hospitals transformed outpatients’ face-to-face clinics into phone-based remote clinics during the COVID-19 pandemic. A previous Italian study on the view of changing to telehealth during the pandemic reported that most responders considered remote consultations more advantageous than traditional health care system [19]. This finding was in agreement with a previous study describing that telemedicine can save cost by avoiding long journey (transportation, accommodation) and by preventing patients from missing work, leading to a high level of satisfaction [25].
Most children’s caregivers and patients with epilepsy are well followed up beyond the health crisis. However, those with hearing impairments or cognitive disorders who have difficulty adapting without support from a third person should be taken into account. In the same context, we discovered that children with cerebral palsy or tracheostomy/PEG had worsening seizure which might have resulted from difficulty accessing health care systems, especially difficulty obtaining ASMs. Furthermore, children who suffer from breathing and swallowing dysfunction, chest deformities, and muscle weakness resulting in tracheostomy or PEG are at a higher risk for a wide range of severe illness that might put them at an elevated risk for neurologic complications including seizures [26,27,28]. Children with epilepsy who have other comorbidities might be at even higher risk of worsening seizures. Prolonged bed rest and immobility as widely known problems of children with severe cerebral palsy can greatly weaken their immunity and increase risks of severe illness and hospitalization. Hence, those who have neurological impairment leading to bed ridden state have a likelihood of a developing severe illness or other complications [29]. On the contrary, Balestrini et al. have reported that even adult patients with epilepsy and multiple comorbidities show a high percentage of asymptomatic conditions, indicating that comorbidities factors do not necessarily lead to poor outcomes [30].
COVID-19 not only affects public health, but also affects psychological and physical stress, especially depression, anxiety, mental stress and sleep related problems, at both individual and global levels probably due to enforced changes in routines due to COVID-19-related lockdown [7,17,18,31,32,33]. Previous population-based studies have demonstrated that mood disorders are frequently associated with patients with epilepsy regardless of adults or children [34]. Besides, worsening seizure due to psychological stress is well known in epilepsy. Several previous studies have mentioned that psychological stress plays a leading part in failure of epilepsy control during the pandemic period [18,35]. Sleep disturbance and reduction in physical activities are frequently associated with psychological stress including depressive and anxiety moods [36,37,38]. Although we did not use a questionnaire, apart from other studies showing that sleep disturbance and reduced physical activities exacerbate seizures [7,39], sleep alteration (23%) and physical activities (49%) did not affect the probability of worsening seizures in this study (Table 2). This result might be explained by variations between different populations probably reflecting differences in age, national health system and income, lockdown rules, ethics, and differences in the timing of data collection.
Regardless of psychological stress, disturbance of the sleep-wake cycle might be explained by the excitatory and inhibitory balance of EEG epileptiform discharge regarding circadian rhythm in both patients with and without epilepsy [40,41]. Additionally, sleep deprivation and sleep fragmentation in patients with epilepsy could further induce EEG epileptiform abnormalities [42], leading to failure of epilepsy control. In early and middle phases of the pandemic, most children carried out their physical activities and schooling at home. In a recent study [43], about 30% of patients reported a reduction in physical activities during the pandemic. These low levels of physical activities might have further negatively influenced mental health of patients with epilepsy, thus increasing the frequency of seizure worsening. This has been described previously [44]. Likewise, carrying out physical exercise could positively influence their moods [44,45], which could minimize seizure aggravation. Granata et al. have mentioned that stay-at home or quarantine can allow patients with epilepsy to live regular life such as improved compliance with ASMs and sleep regularity, these might have led to better seizure control [10]. In the same manner, caregivers could spend more time at home taking care of their children closely, resulting in better seizure control with better adherence to ASMs [17,20].
Interestingly, infection with other respiratory viruses (RSV, influenza) except SARS-CoV-2 was revealed to be a potential risk factor of worsening seizures during the ongoing pandemic in current study. This finding has not been previously reported.
This could be explained by our study, which included a long lockdown period involving variant factors that might influence the probability of seizure worsening identified only during the outbreak of the new virus, which has not been studied in the past. During the first pandemic year, nonpharmaceutical interventions (NPIs) such as social distancing policies, school closure, mandatory use of face mask, hand sanitation, partial lockdown, and travel restrictions were the most available and effective form of controlling COVID-19, both locally and globally. Several studies have previously demonstrated potential benefits of NPIs adopted to reduce the spread of seasonal respiratory viruses [46,47]. In other words, same restrictions applied to SARS-CoV-2 also suppressed seasonal respiratory viruses’ circulations that epidemics were substantially reduced in the early phases of the COVID-19 pandemic [21,48]. However, as quarantine restrictions including reopening of schools were gradually eased after the first wave of COVID-19, infections by seasonal respiratory viruses by transmission via the respiratory route were notably increased in late 2020 and early 2021 [49,50]. Most importantly and relevant for transmission, childcare and daycare centers mostly reopened and remained open during these restriction periods. Acute symptomatic seizures of children with epilepsy resulting from poor general condition, mainly fever arising from viral infections, subsequently could lead to worsening of seizures. By mid-2022, quarantine restrictions had been more relaxed at variable levels either fully or partly, resulting in delayed and severe unpredictable outbreaks of various respiratory viruses [51] that might have increased the susceptibility of infection throughout the world. Thus, pediatric neurologists must provide not only appropriate epilepsy care, but also modify their previous routine medical practice against these viruses causing potentially life-threatening infections.
Whether the COVID-19 pandemic could aggravate seizures largely depends on how their lives and societies are affected by COVID-19, supporting the view that quality of life in people with epilepsy is multifactorial. Through our study, regular monitoring and follow-up, proper ASM adjustments, decompensation of comorbidities, and monitoring seasonal respiratory viruses are crucial. Furthermore, our study highlights that not only SARS-CoV-2, but also concurrent epidemic respiratory viruses should be inevitably prioritized to reduce worsening seizures for pediatric patients with epilepsy.
The strength of our study was that we included a long lockdown period between before and during the COVID-19 pandemic and variously aged children tested for various respiratory viruses including SARS-CoV-2. However, our study has several limitations. Main limitations of this study were its retrospective nature of review from medical charts and a small sample of pediatric patients. In addition, our data were obtained for subjects from only one city, making it difficult to compare other specific socioeconomic status. Since there were no data on mental health issues before or during the pandemic, further conclusions are limited. Therefore, prospective studies using larger cohorts are needed to clarify the association of COVID-19 with seizure outcomes and risk factors for seizure worsening.
5. Conclusions
In conclusion, our results identified that some children with epilepsy suffered from worsening seizures and several potential risk factors during the COVID-19 pandemic. Our results suggest that proactive monitoring and regular follow-up, proper ASM adjustments (especially for children diagnosed epilepsy within 1 year), decompensation of comorbidities (which could increase susceptibility to serious infections) and surveillance of seasonal respiratory viruses during the COVID-19 pandemic could contribute to early identification of exacerbation of seizures. Furthermore, during the pandemic, physicians need to be aware of the evolution of respiratory viruses through epidemiological surveillance to manage worsening seizures in children with epilepsy. Future research can be strengthened by adding assessments that quantify various clinical variables and expanding the number of patients.
Author Contributions
Conceptualization, J.U.M.; Data curation, J.U.M., D.H.Y, M.H.J; Formal analysis, J.U.M.; Methodology J.U.M., D.H.Y, M.H.J.; Writing—original draft, J.U.M.; Writing—review and editing, J.U.M. The author has read and agreed to the published version of the manuscript.
Funding
This work was supported by grant of National Research Foundation of Korea (NRF) funded by the Korean Government (MSIT; 2021R1F1A1063568).
Institutional Review Board Statement
This study protocol was approved by the Institutional Review Board of the Catholic University of Korea (Approval number: SC23RISI0028; Date of approval: 10. March. 2023).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of this study.
Data Availability Statement
The data presented in this study are available from the corresponding author upon reasonable request.
Acknowledgments
The author is grateful to College of Medicine of The Catholic University of Korea for their assistance in performing the present study.
Conflicts of Interest
The author has no potential conflicts of interest relevant to this study (with respect to the research, authorship, and/or publication of this article) to disclose.
References
- Abdel-Mannan, O.; Taylor, H.; Donner, E.J.; Sutcliffe, A.G. A systematic review of sudden unexpected death in epilepsy (SUDEP) in childhood. Epilepsy Behav 2019, 90, 99–106. [Google Scholar] [CrossRef]
- Dagar, A.; Falcone, T. Psychiatric Comorbidities in Pediatric Epilepsy. Curr Psychiatry Rep 2020, 22, 77. [Google Scholar] [CrossRef] [PubMed]
- Prasad, V.; Kendrick, D.; Sayal, K.; Thomas, S.L.; West, J. Injury among children and young adults with epilepsy. Pediatrics 2014, 133, 827–835. [Google Scholar] [CrossRef]
- Fiest, K.M.; Birbeck, G.L.; Jacoby, A.; Jette, N. Stigma in epilepsy. Curr Neurol Neurosci Rep 2014, 14, 444. [Google Scholar] [CrossRef]
- Begley, C.E.; Beghi, E. The economic cost of epilepsy: a review of the literature. Epilepsia 2002, 43 Suppl 4, 3–9. [Google Scholar] [CrossRef]
- Jiang, F.; Deng, L.; Zhang, L.; Cai, Y.; Cheung, C.W.; Xia, Z. Review of the Clinical Characteristics of Coronavirus Disease 2019 (COVID-19). J Gen Intern Med 2020, 35, 1545–1549. [Google Scholar] [CrossRef] [PubMed]
- Alkhotani, A.; Siddiqui, M.I.; Almuntashri, F.; Baothman, R. The effect of COVID-19 pandemic on seizure control and self-reported stress on patient with epilepsy. Epilepsy Behav 2020, 112, 107323. [Google Scholar] [CrossRef]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D. , et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol 2020, 77, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Xiong, W.; Liu, D.; Liu, J.; Yang, D.; Li, N.; Mu, J.; Guo, J.; Li, W.; Wang, G. , et al. New onset acute symptomatic seizure and risk factors in coronavirus disease 2019: A retrospective multicenter study. Epilepsia 2020, 61, e49–e53. [Google Scholar] [CrossRef]
- Granata, T.; Bisulli, F.; Arzimanoglou, A.; Rocamora, R. Did the COVID-19 pandemic silence the needs of people with epilepsy? Epileptic Disord 2020, 22, 439–442. [Google Scholar] [CrossRef]
- Pinzon, R.T.; Wijaya, V.O.; Jody, A.A.; Nunsio, P.N.; Buana, R.B. Persistent neurological manifestations in long COVID-19 syndrome: A systematic review and meta-analysis. J Infect Public Health 2022, 15, 856–869. [Google Scholar] [CrossRef] [PubMed]
- Fisher, R.S.; Acevedo, C.; Arzimanoglou, A.; Bogacz, A.; Cross, J.H.; Elger, C.E.; Engel, J., Jr.; Forsgren, L.; French, J.A.; Glynn, M. , et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia 2014, 55, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Fisher, R.S.; Cross, J.H.; French, J.A.; Higurashi, N.; Hirsch, E.; Jansen, F.E.; Lagae, L.; Moshe, S.L.; Peltola, J.; Roulet Perez, E. , et al. Operational classification of seizure types by the International League Against Epilepsy: Position Paper of the ILAE Commission for Classification and Terminology. Epilepsia 2017, 58, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Al Momani, M.; Almomani, B.A.; Sweidan, P.; Al-Qudah, A.; Aburahma, S.; Arafeh, Y. Impact of COVID-19 pandemic on pediatric patients with epilepsy in Jordan: The caregiver perspective. Seizure 2021, 92, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Larsen, A.; Gonzalez-Villar, E.; Diaz-Maroto, I.; Layos-Romero, A.; Martinez-Martin, A.; Alcahut-Rodriguez, C.; Grande-Martin, A.; Sopelana-Garay, D. Influence of the COVID-19 outbreak in people with epilepsy: Analysis of a Spanish population (EPICOVID registry). Epilepsy Behav 2020, 112, 107396. [Google Scholar] [CrossRef] [PubMed]
- Guilhoto, L.M.; Mosini, A.C.; Susemihl, M.A.; Pinto, L.F. COVID-19 and epilepsy: How are people with epilepsy in Brazil? Epilepsy Behav 2021, 122, 108115. [Google Scholar] [CrossRef] [PubMed]
- Assenza, G.; Lanzone, J.; Brigo, F.; Coppola, A.; Di Gennaro, G.; Di Lazzaro, V.; Ricci, L.; Romigi, A.; Tombini, M.; Mecarelli, O. Epilepsy Care in the Time of COVID-19 Pandemic in Italy: Risk Factors for Seizure Worsening. Front Neurol 2020, 11, 737. [Google Scholar] [CrossRef]
- Huang, S.; Wu, C.; Jia, Y.; Li, G.; Zhu, Z.; Lu, K.; Yang, Y.; Wang, F.; Zhu, S. COVID-19 outbreak: The impact of stress on seizures in patients with epilepsy. Epilepsia 2020, 61, 1884–1893. [Google Scholar] [CrossRef] [PubMed]
- Trivisano, M.; Specchio, N.; Pietrafusa, N.; Calabrese, C.; Ferretti, A.; Ricci, R.; Renzetti, T.; Raponi, M.; Vigevano, F. Impact of COVID-19 pandemic on pediatric patients with epilepsy - The caregiver perspective. Epilepsy Behav 2020, 113, 107527. [Google Scholar] [CrossRef]
- Rosengard, J.L.; Donato, J.; Ferastraoaru, V.; Zhao, D.; Molinero, I.; Boro, A.; Gursky, J.; Correa, D.J.; Galanopoulou, A.S.; Hung, C. , et al. Seizure control, stress, and access to care during the COVID-19 pandemic in New York City: The patient perspective. Epilepsia 2021, 62, 41–50. [Google Scholar] [CrossRef]
- Hsu, H.T.; Huang, F.L.; Ting, P.J.; Chang, C.C.; Chen, P.Y. The epidemiological features of pediatric viral respiratory infection during the COVID-19 pandemic in Taiwan. J Microbiol Immunol Infect 2022, 55, 1101–1107. [Google Scholar] [CrossRef] [PubMed]
- Wirrell, E.C.; Grinspan, Z.M.; Knupp, K.G.; Jiang, Y.; Hammeed, B.; Mytinger, J.R.; Patel, A.D.; Nabbout, R.; Specchio, N.; Cross, J.H. , et al. Care Delivery for Children With Epilepsy During the COVID-19 Pandemic: An International Survey of Clinicians. J Child Neurol 2020, 35, 924–933. [Google Scholar] [CrossRef] [PubMed]
- Assenza, G.; Lanzone, J.; Ricci, L.; Boscarino, M.; Tombini, M.; Galimberti, C.A.; Alvisi, L.; Tassi, L.; Broglia, L.; Di Lazzaro, V. , et al. Electroencephalography at the time of Covid-19 pandemic in Italy. Neurol Sci 2020, 41, 1999–2004. [Google Scholar] [CrossRef] [PubMed]
- Samanta, D.; Elumalai, V.; Desai, V.C.; Hoyt, M.L. Conceptualization and implementation of an interdisciplinary clinic for children with drug-resistant epilepsy during the COVID-19 pandemic. Epilepsy Behav 2021, 125, 108403. [Google Scholar] [CrossRef] [PubMed]
- Blottner, S.; Bertram, R.; Pitra, C. [Species specific motility patterns of hyperactivated mammalian spermatozoa and quantitative analysis of the hyperactivation of bull spermatozoa]. Andrologia 1989, 21, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Bonello, M.; Michael, B.D.; Solomon, T. Infective Causes of Epilepsy. Semin Neurol 2015, 35, 235–244. [Google Scholar] [CrossRef]
- Vezzani, A.; Lang, B.; Aronica, E. Immunity and Inflammation in Epilepsy. Cold Spring Harb Perspect Med 2015, 6, a022699. [Google Scholar] [CrossRef] [PubMed]
- Yuen, A.W.C.; Keezer, M.R.; Sander, J.W. Epilepsy is a neurological and a systemic disorder. Epilepsy Behav 2018, 78, 57–61. [Google Scholar] [CrossRef]
- Sillanpaa, M.; Saarinen, M.M.; Karrasch, M.; Schmidt, D.; Hermann, B.P. Neurocognition in childhood epilepsy: Impact on mortality and complete seizure remission 50 years later. Epilepsia 2019, 60, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Balestrini, S.; Koepp, M.J.; Gandhi, S.; Rickman, H.M.; Shin, G.Y.; Houlihan, C.F.; Anders-Cannon, J.; Silvennoinen, K.; Xiao, F.; Zagaglia, S. , et al. Clinical outcomes of COVID-19 in long-term care facilities for people with epilepsy. Epilepsy Behav 2021, 115, 107602. [Google Scholar] [CrossRef]
- French, J.A.; Brodie, M.J.; Caraballo, R.; Devinsky, O.; Ding, D.; Jehi, L.; Jette, N.; Kanner, A.; Modi, A.C.; Newton, C.R. , et al. Keeping people with epilepsy safe during the COVID-19 pandemic. Neurology 2020, 94, 1032–1037. [Google Scholar] [CrossRef] [PubMed]
- Aledo-Serrano, A.; Mingorance, A.; Jimenez-Huete, A.; Toledano, R.; Garcia-Morales, I.; Anciones, C.; Gil-Nagel, A. Genetic epilepsies and COVID-19 pandemic: Lessons from the caregiver perspective. Epilepsia 2020, 61, 1312–1314. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, E.; Quintana, M.; Lallana, S.; Luis Restrepo, J.; Abraira, L.; Santamarina, E.; Seijo-Raposo, I.; Toledo, M. Epilepsy in time of COVID-19: A survey-based study. Acta Neurol Scand 2020, 142, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Ribot, R.; Kanner, A.M. Neurobiologic properties of mood disorders may have an impact on epilepsy: Should this motivate neurologists to screen for this psychiatric comorbidity in these patients? Epilepsy Behav 2019, 98, 298–301. [Google Scholar] [CrossRef]
- Millevert, C.; Van Hees, S.; Siewe Fodjo, J.N.; Wijtvliet, V.; Faria de Moura Villela, E.; Rosso, B.; Gil-Nagel, A.; Weckhuysen, S.; Colebunders, R. Impact of COVID-19 on the lives and psychosocial well-being of persons with epilepsy during the third trimester of the pandemic: Results from an international, online survey. Epilepsy Behav 2021, 116, 107800. [Google Scholar] [CrossRef]
- Tsuno, N.; Besset, A.; Ritchie, K. Sleep and depression. J Clin Psychiatry 2005, 66, 1254–1269. [Google Scholar] [CrossRef]
- Ramsawh, H.J.; Stein, M.B.; Belik, S.L.; Jacobi, F.; Sareen, J. Relationship of anxiety disorders, sleep quality, and functional impairment in a community sample. J Psychiatr Res 2009, 43, 926–933. [Google Scholar] [CrossRef]
- Stein, M.B.; Belik, S.L.; Jacobi, F.; Sareen, J. Impairment associated with sleep problems in the community: relationship to physical and mental health comorbidity. Psychosom Med 2008, 70, 913–919. [Google Scholar]
- Thorpe, J.; Ashby, S.; Hallab, A.; Ding, D.; Andraus, M.; Dugan, P.; Perucca, P.; Costello, D.; French, J.A.; O'Brien, T.J. , et al. Evaluating risk to people with epilepsy during the COVID-19 pandemic: Preliminary findings from the COV-E study. Epilepsy Behav 2021, 115, 107658. [Google Scholar]
- Khan, S.; Duan, P.; Yao, L.; Hou, H. Shiftwork-Mediated Disruptions of Circadian Rhythms and Sleep Homeostasis Cause Serious Health Problems. Int J Genomics 2018, 2018, 8576890. [Google Scholar] [CrossRef]
- Daley, J.T.; DeWolfe, J.L. Sleep, Circadian Rhythms, and Epilepsy. Curr Treat Options Neurol 2018, 20, 47. [Google Scholar] [CrossRef] [PubMed]
- Jin, B.; Aung, T.; Geng, Y.; Wang, S. Epilepsy and Its Interaction With Sleep and Circadian Rhythm. Front Neurol 2020, 11, 327. [Google Scholar] [CrossRef] [PubMed]
- Koh, M.Y.; Lim, K.S.; Fong, S.L.; Khor, S.B.; Tan, C.T. Impact of COVID-19 pandemic on people with epilepsy: An interventional study using early physical consultation. Epilepsy Behav 2021, 122, 108215. [Google Scholar] [CrossRef]
- Arida, R.M.; Cavalheiro, E.A.; da Silva, A.C.; Scorza, F.A. Physical activity and epilepsy: proven and predicted benefits. Sports Med 2008, 38, 607–615. [Google Scholar] [CrossRef]
- Arida, R.M.; de Almeida, A.C.; Cavalheiro, E.A.; Scorza, F.A. Experimental and clinical findings from physical exercise as complementary therapy for epilepsy. Epilepsy Behav 2013, 26, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Oster, Y.; Michael-Gayego, A.; Rivkin, M.; Levinson, L.; Wolf, D.G.; Nir-Paz, R. Decreased prevalence rate of respiratory pathogens in hospitalized patients during the COVID-19 pandemic: possible role for public health containment measures? Clin Microbiol Infect 2020, 27, 811–812. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, H.; Song, K.H.; Kim, E.S.; Park, J.S.; Jung, J.; Ahn, S.; Jeong, E.K.; Park, H.; Kim, H.B. Impact of Public Health Interventions on Seasonal Influenza Activity During the COVID-19 Outbreak in Korea. Clin Infect Dis 2021, 73, e132–e140. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.P.; Chu, I.Y.; Yeh, M.L.; Chen, Y.Y.; Lee, C.L.; Lin, H.H.; Chan, Y.J.; Chen, H.P. Differentiating impacts of non-pharmaceutical interventions on non-coronavirus disease-2019 respiratory viral infections: Hospital-based retrospective observational study in Taiwan. Influenza Other Respir Viruses 2021, 15, 478–487. [Google Scholar] [CrossRef]
- Eden, J.S.; Sikazwe, C.; Xie, R.; Deng, Y.M.; Sullivan, S.G.; Michie, A.; Levy, A.; Cutmore, E.; Blyth, C.C.; Britton, P.N. , et al. Off-season RSV epidemics in Australia after easing of COVID-19 restrictions. Nat Commun 2022, 13, 2884. [Google Scholar] [CrossRef]
- Shen, D.P.; Vermeulen, F.; Debeer, A.; Lagrou, K.; Smits, A. Impact of COVID-19 on viral respiratory infection epidemiology in young children: A single-center analysis. Front Public Health 2022, 10, 931242. [Google Scholar] [CrossRef]
- Ali, S.T.; Lau, Y.C.; Shan, S.; Ryu, S.; Du, Z.; Wang, L.; Xu, X.K.; Chen, D.; Xiong, J.; Tae, J. , et al. Prediction of upcoming global infection burden of influenza seasons after relaxation of public health and social measures during the COVID-19 pandemic: a modelling study. Lancet Glob Health 2022, 10, e1612–e1622. [Google Scholar] [CrossRef] [PubMed]
Table 1.
Demographic and clinical characteristics of subjects before COVID19 pandemic.
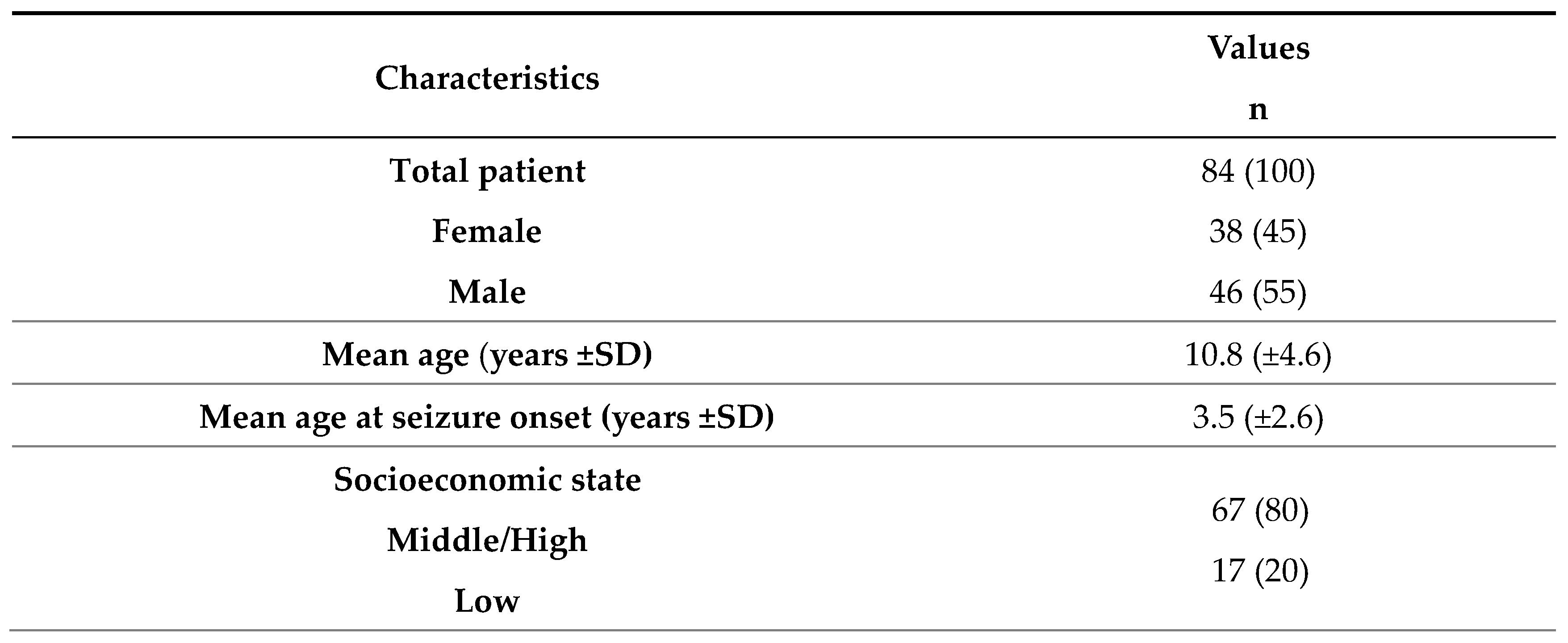
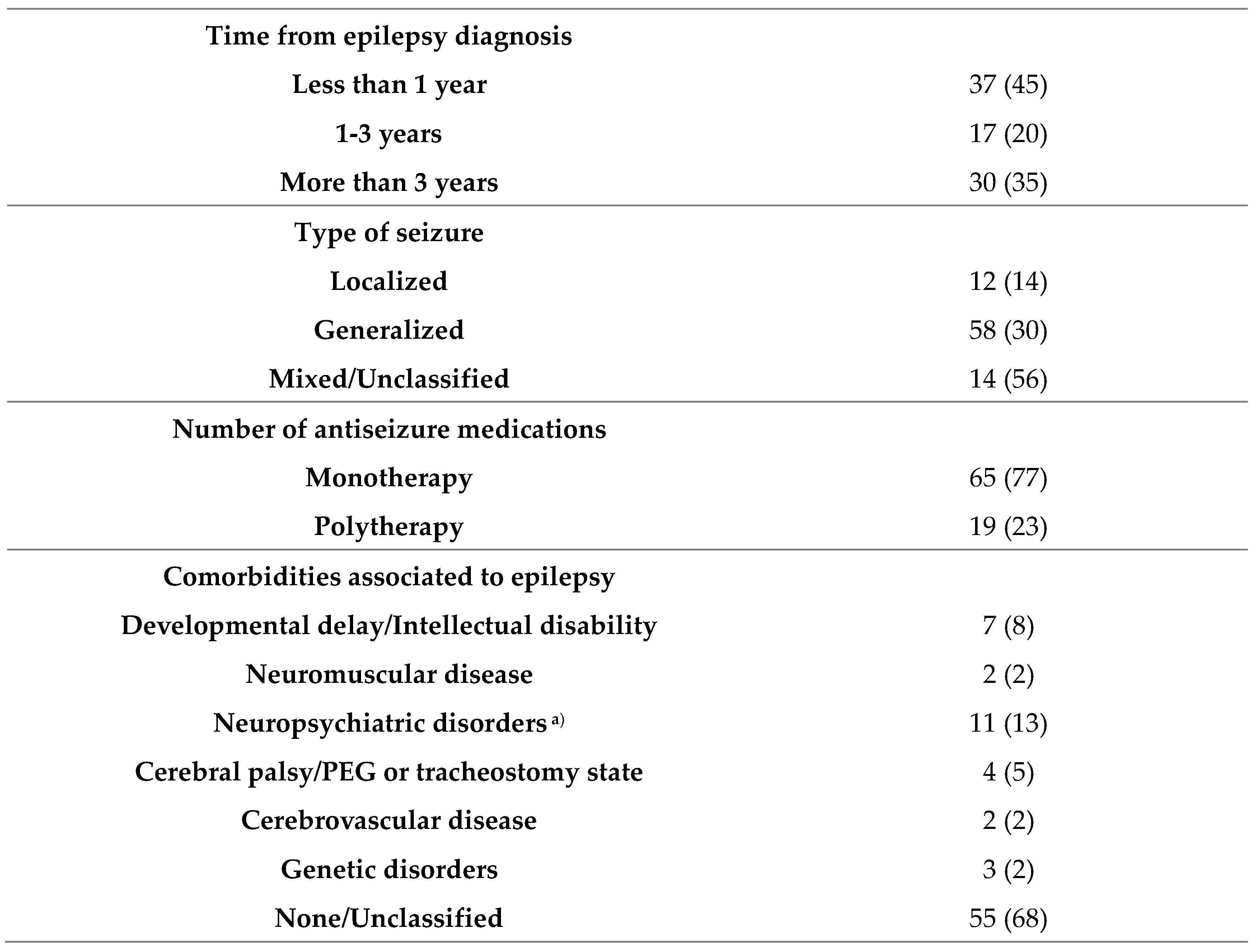
Values are presented as mean ± standard deviation or number (%). SD, standard deviation; PEG, percutaneous endoscopic gastrostomy. a) neuropsychiatric disorder included such as attention deficit hyperactivity disorder or autism spectrum disorders.
Table 2.
Seizure profile during the COVID-19 pandemic.
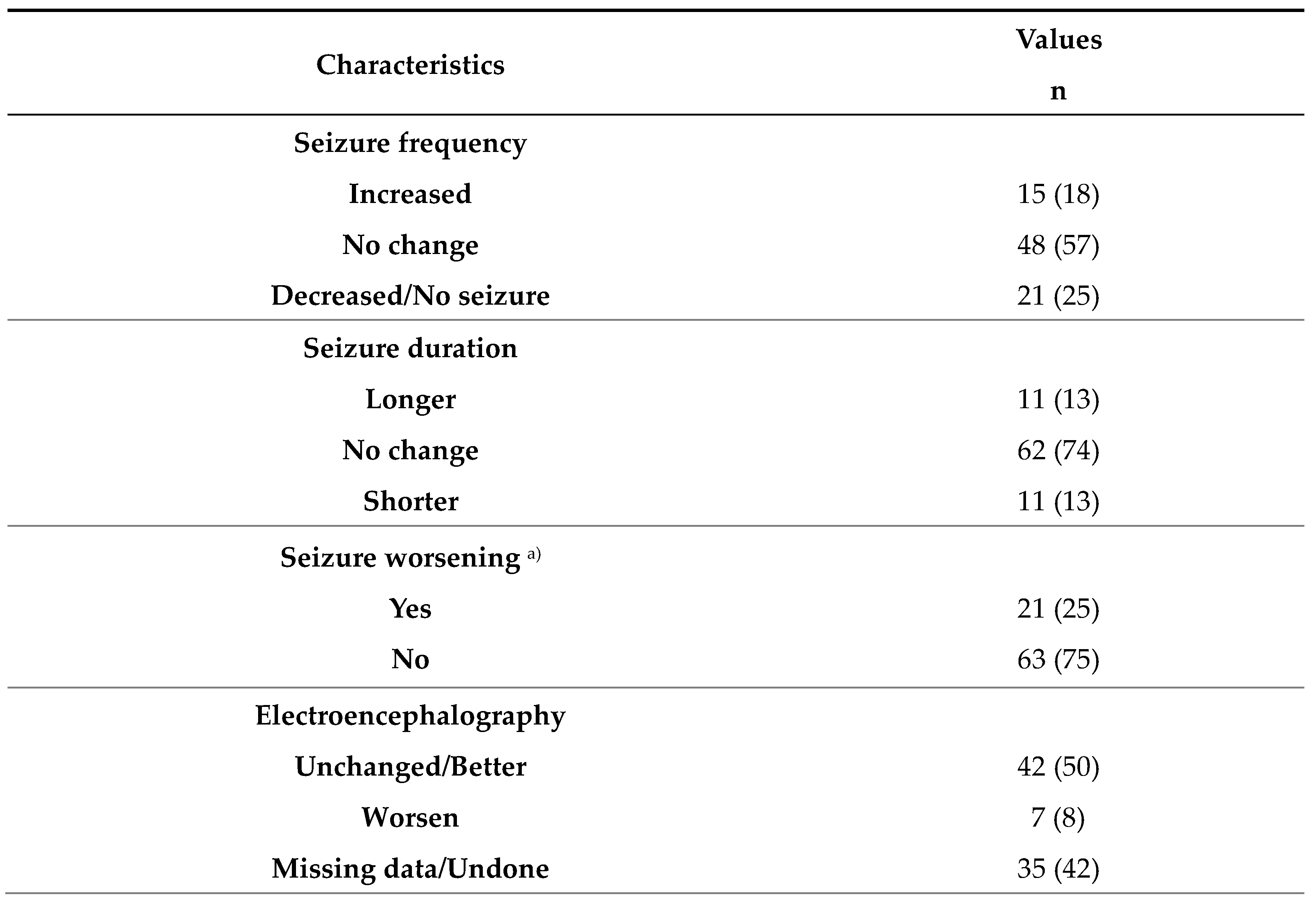
Values are presented as number (%). a) seizure worsening is defined as an increase in frequency or duration or both of seizures during the COVID-19 pandemic.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



