
Submitted:
27 May 2023
Posted:
30 May 2023
You are already at the latest version
Abstract
It is unclear how maternal glycemic status and maternal iodine status influence birth weight in mild-to-moderate iodine deficiency (ID). We studied the association between birth weight and both maternal glucose levels and iodine intake in pregnant women with mild-to-moderate ID. Glucose values were assessed using a glucose challenge test (GCT), non-fasting glucose before delivery; iodine status was assessed using an iodine food frequency questionnaire, serum thyroglobulin (Tg) and urinary iodine concentrations (UIC). Thyroid antibodies and free thyroxine (FT4) were measured. Obstetric and an-thropometric data were also collected. Large for gestational age (LGA) was predicted using a Cox proportional hazards model with multiple confounders. Tg>13g/L was in-dependently associated with LGA (adjusted hazard ratio = 3.4, 95% CI: 1.4–10.2, p=0.001). Estimated iodine intake correlated with FT4 among participants reporting io-dine-containing supplements (ICS) after adjusting for confounders (β = 0.4 95 %CI: 0.0002-0.0008, p=0.001). Newborn weight percentiles were inversely correlated with maternal FT4 values (β=-0.2 95 %CI:-0.08 - -56.49, p=0.049). We conclude that in mild-to-moderate ID regions, maternal insufficient iodine status may increase LGA risk. Iodine status and ICS intake may modify the effect maternal dysglycemia has on offspring weight.
Keywords:
iodine deficiency
; glucose challenge test
; large for gestational age
; thyroglobulin
; io-dine-containing supplements
; maternal dysglycemia
1. Introduction
Birth weight is considered the most important marker for fetal growth and development in utero and reflects the adaptation of the fetus to the intrauterine environment. Small for gestational age (SGA) newborns have an increased risk of prenatal mortality and an increased risk of suffering later in life from diseases such as metabolic syndrome, coronary heart disease, hypertension, stroke, kidney disease, osteoporosis, depression and persistent anemia [1,2,3,4]. Large for gestational age (LGA) newborns have a higher risk of neonatal metabolic abnormalities including hyperglycemia, birth trauma, stillbirth and neonatal death [5]. Individuals with LGA might also be at increased risk for overweight, obesity, cardiovascular disease and diabetes later in life [5,6]. Gestational Diabetes Mellitus (GDM) is associated with increased risk for LGA. Moreover, preliminary data hve shown that even elevated maternal glucose levels, that do not meet the diagnostic threshold for GDM, are associated with increased birth weight [7]. Additionally, results from a retrospective study including screening tests that use the 50-g 1-h post oral glucose challenge test (GCT), performed at 24–28 weeks of pregnancy, suggest that the 50-g GCT can be used to identify women at risk of delivering offspring with excessive delivery weight. [8]. Importantly, GCT is typically performed in the second half of pregnancy.I However, interventions aimed at reducing the risk of fetal overgrowth and its associated health complications may not be effective if implemented at this late stage of pregnancy.
Iodine is essential for the synthesis of the thyroid hormones L-triiodothyronine (T3) and L-tetraiodothyronine or thyroxine (T4). These hormones are important for normal human development, including the development of the fetal brain and nervous system, as well as cell metabolism. Early in the first trimester, before the fetalthyroid is functioning, maternal thyroid hormones are transferred to the fetus as its sole source of thyroid hormones.
Moreover, although the fetal thyroid is functionally mature around the gestational age of 18-20 weeks, the contribution of maternal thyroid hormones to fetal thyroid hormone availability is still considerable. Studies show a strong association between maternal thyroid function and fetal thyroid function [10,11]. Furthermore, studies show a maximum of 30% to 50% of newborn T4 concentrations can be reached in the absence of fetal thyroid hormone production [12,13]. Thus, late-pregnancy maternal thyroid function may play an important role on fetal development. Essentially, in utero growth depends on adequate maternal iodine intake throughout pregnancy. Moreover, pregnant women are at a high risk of iodine deficiency (ID) due to increased urinary iodine clearance and fetal iodine requirements [9].
We recently reported that inadequate maternal iodine intake may increase the risk of LGA among newborns, using thyroid function tests (N=134) [14]. Following this, a study from China has reported increased birthweight among newborns of mothers with ID (N=726, nearly significant [p=0.07]) [15]. This study assessed maternal iodine status using UIC and thyroid function tests. [14].
In this study, we used UIC measurements and examined maternal circulating glucose levels to assess the contribution of elevated- subclinical GDM glucose levels on birth weight. [7]. Our study aimed to assess the relationship between birth weight, glucose levels and iodine intake in pregnant women with mild-to-moderate iodine deficiency
2. Materials and Methods
2.1. Design, participants, settings and ethics
The study was a longitudinal prospective cohort study; Methods have previously been described in detail [16]. Briefly, the study was conducted between June 2018 and April 2020. 202 pregnant women who attended the Obstetrics and Gynecology Department were included in the study. The screening process, study sample and follow up flow chart are described in detail elsewhere [16]. The study was approved by BUMCA’s ethical committee (approval number 001-17-BRZ dated 7 August 2017). All participants provided written informed consent after the research protocol was explained to them in detail. All dietary interviews were performed by experienced registered dietitians.
2.2. Data collection and considerations
Obstetrics data, such as parity, gravidity, in vitro fertilization (IVF) treatments, gestation week, anthropometrics, GCT results and non-fasting glucose values at delivery admission were collected from participants’ medical files. Any GCT result above 140 mg/dL were considered abnormal [17]. Any initial diabetes diagnosed during pregnancy was considered as GDM. Recorded abnormal GCT result or GDM diagnosis were considered maternal dysglycemia [17]. Advanced maternal age was considered when delivery was preformed at age > 35 years [18]. The questionnaire used in the study included self-reported information about participants' health status, as well as their knowledge, attitudes, and behaviors regarding nutrition and health. Smoking history was assessed using medical records and interviews. Body mass index (BMI) at delivery was calculated based on weight and height obtained from electronic medical records. Normal, Overweight and obesity were considered when BMI was 18.5-24.9, 25.0-29.9 and above 30.0 kg/m2, respectively [19]. Interview and other data collection have been described previously in detail [16].
2.3. Assessment of maternal iodine intake, status and thyroid function
The study assessed the iodine status of participants using three different measurements: (a) a validated, semi-quantitative iodine food frequency questionnaire (sIFFQ) to estimate long-term iodine intake (up to a year), (b) serum thyroglobulin (Tg) to indicate intermediate-term iodine intake (weeks to months), and (c) urinary iodine concentration (UIC) as an indicator of recent iodine intake (days). The details of these measurements were previously described in full [16] (b) sIFFQ was administered by three registered dietitians (YSO, SRR, and YAB) who have experience working with pregnant women and who were trained in the use of the sIFFQ. The questionnaire included questions about both the initiation and duration of iodine-containing supplements (ICS) and the estimated amount of iodized salt (IS) consumed to address potential recall bias. We classified participants as having achieved the recommended iodine intake if their sIFFQ calculated result was equal to or greater than 220 μg/day, which is the Dietary Allowance (RDA) for iodine intake during pregnancy [21]. The UIC was determined by inductively coupled plasma mass spectrometry method (ICP-MS) according to the US CDC ICP-MS method [22]. Subgroup iodine status was considered sufficient, mild-to-moderate ID or severe ID when the median UIC was >150, 50-150 or < 50 μg/L (respectively) according to the World Health Organization (WHO) and the American Thyroid Association (ATA) guidelines [23,24].
Thyroid function was assessed using an electrochemiluminescence immunoassays, as previously described [16]. Briefly, free T4 (FT4), free T3 (FT3), thyrotropin (TSH), thyroid peroxidase antibodies (TPOAb), thyroglobulin antibody (TgAb) and Tg were determined. Reference ranges were 0.27–4.2 mU/L for TSH and 0.93–1.7 ng/dL for FT4 according to the manufacturer. TgAb above 40 IU/ml and TPOAb above 35 IU/ml were considered positive as reported in previous studies [25]. Subclinical hypothyroidism (SCH) was considered when FT3 and FT4 values were normal, but TSH values were above 2.5 or 4.0 mU/L during 1st and both 2nd 3rd trimester, respectively [24]. In the absence of a consensus regarding the definition of isolated hypothyroxinemia (IHT) and established trimester-specific thyroid function tests values from iodine deficient areas, reference intervals of FT4 from BUMCA with trimester-specific cutoffs for TSH (2.5 mU/L for the first trimester, and 4.0 mU/L for both the second and third trimesters) were used to define IHT at different gestational ages [24]. A median cutoff ≤13 μg/L for Tg levels was considered sufficient for the entire study sample according to a recently suggested standard for populations [25].
2.4. Neonatal birth data and antheropometrics
Information on date of birth, gender, Apgar score as well as birth weight, length, and head circumference were obtained from the participants medical records at BUMCA. Gestational age at birth was calculated on the basis self-reported last menstrual period, and confirmed using fetal crown–rump length. This parameter was calculated in single numbers of days added to completed weeks. Delivery room midwives performed the Apgar test and measured the newborns weight, length, and head circumference. Newborn birth weight percentiles were calculated and standardization by the Israeli birth population index using gestational age and gender as described in details elsewhere [26]. Percentiles below 10th and above 90th were considered as SGA and LGA, respectively. Low birth weight (LBW) was defined as birth weight below 2,500 g among full-term newborns, and preterm was defined as birth before 37 completed weeks of gestation. Any case of newborn with weight above 4,000 g was considered as macrosomia. Length and head circumference calculated and standardization for the Israeli birth population using gestational age and gender as described in detail elsewhere [27].
2.5. Statistical analysis
Statistical analyses were performed with the JMP Pro software, version 16 (SAS Institute, Cary, NC, USA). We used multiple linear regression models to study the association of GCT (also overlayed by severe ID vs. sufficiency assessed by UIC) and FT4 with birth weight percentile as well as estimated iodine intake (overlayed by reported ICS intake vs. none) with FT4. To test the multiplying relationship between possible predictors of LGA we used Proportional Hazards platform that fits the Cox proportional hazards model (semiparametric regression model for survival data with covariates). This model was performed with LGA as the hazard function, gestational age as the time-to-event function and the following 15 possible predictors as the covariates: Tg (above vs. below 13 μg/L), UIC (above vs. below 150 μg/L), parity (multiparous vs. nulliparous), ICS (any consumption during pregnancy vs. none), gravidity (multigravida vs. nulligravida), estimated iodine intake (below vs above 220 μg/day), maternal age (advanced vs. none advanced), GDM (recorded diagnosis vs. none), GCT (abnormal vs. normal result), SCH (found vs. none), IS use (reported vs. none), delivery BMI (overweight vs. normal), FT3 (highest vs. lowest quartile), IHT (found vs. none), IVF (prepregnancy treated vs. none) and recruitment BMI (overweight vs. normal). In order to choose optimum split for Tg values as a LGA predictor we used the Partition platform that recursively partitions data, creating a decision tree. The partition algorithm searched all possible splits of Tg values to best predict LGA. These splits (partitions) formed a tree of decision rules. The splits continue until the desired fit is reached. The partition algorithm chooses optimum splits from many possible splits (according to JMP Pro software manufacturer). Categorical parameters were summarized by number and percentage and were compared by group (classified by Tg below or above the Partition value) using the chi-squared test, likelihood test, Pearson test or Fisher's exact test as appropriate. Odds ratios (OR) were also calculated for likelihood of LGA across Tg subgroups. Continuous parameters that were not distributed normally were summarized by median and interquartile range (IQR). Normally distributed continuous parameters were presented as mean ± standard deviation (SD). To test whether continuous parameters (such as estimated iodine intake levels, anthropometric measurement results and thyroid function serum values) had a normal distribution, a Goodness-of-fit test was performed and determined by the Shapiro-Wilk W or Cramer-von Mises W tests. These parameters were compared by one-way analysis of variance (ANOVA) with Student's t (for means), Welch's ANOVA (for unequal variances) and Kruskal-Wallis (for non-parametric parameters) and median test (for medians) when appropriate. Serum Tg values were log-transformed before the analysis in order to normalize distribution. Geometric means of serum Tg values were calculated on back-transformed data. The association of continuous GCT, FT4 and UIC values as well as estimated iodine intakes levels was determined by linear regression (adjusting for possible confounding parameters, when necessary). A two-tailed P value<0.05 was considered statistically significant.
3. Results
3.1. Study population
Of the 202 consecutive participants screened, results of 188 (median age, 31; range, 20-46 years) met eligibility criteria and were included in the study. The sociodemographic, obstetrics, health and iodine intake characteristics of the study group were described in detail previously [16].
3.2. Maternal nutritional, hormonal and clinical characteristics
Median UIC value was 60 μg/L, demonstrating mild-to-moderate ID in our study population [24]. Estimated dietary iodine intake median was 179 μg/day, demonstrating low dietary iodine intake using the RDA for pregnancy [21]. Median Tg value was 18 μg/L, this is above the cutoffs considered for iodine sufficiency in pregnancy, indicating iodine insufficiency [25]. Detailed nutritional, hormonal and clinical characteristics of the study population were previously described [16].
3.3. Maternal characteristics, pregnancy outcomes and newborn weight
Values of GCT correlated significantly with non-fasting glucose at delivery admission, but this correlation was found non-significant after multivariate analysis, adjusting for maternal age, BMI, gravidity and parity. However, both univariate and multivariate regression analyses adjusting for age, smoking status, BMI at delivery, parity and gravidity revealed positive correlations between maternal GCT values and adjusted newborn weight percentiles (Figure 1A). According to Figure 1B, this significant positive correlation also occurred among participants with UIC values below 150 μg/L (presumably indicating severe ID). However, this correlation did not appear among participants with UIC values above 150 μg/L (indicating presumably sufficient iodine status) as shown in Figure 1B.
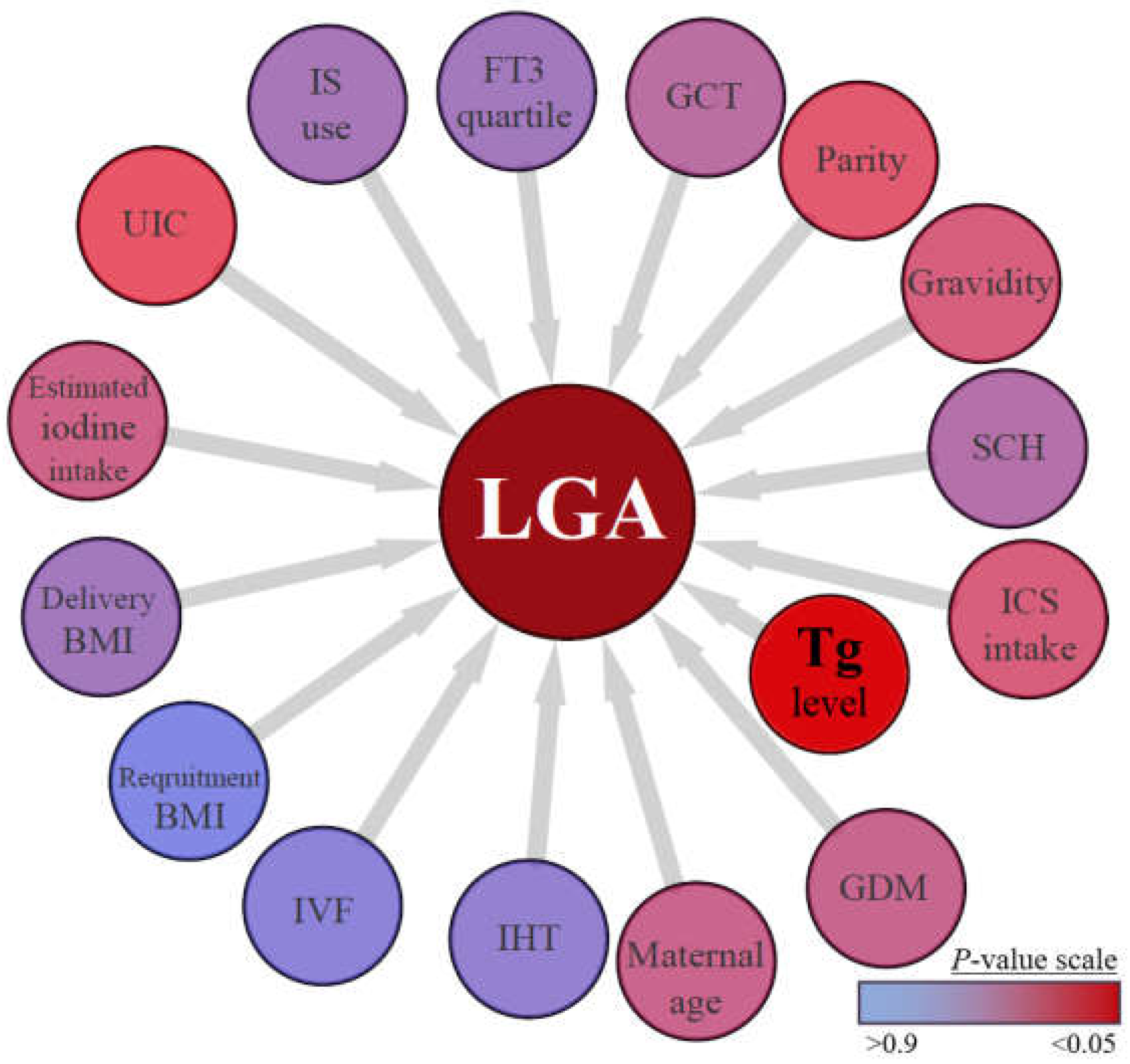
Based on the Cox model comprising 15 variables with a known or probable association with neonatal weight, maternal Tg values were the only significant predictor for LGA (adjusted hazard ratio = 3.4, 95% CI: 1.4–10.2, p=0.001). As shown in Figure 2, other variables were not independently associated with LGA. The Partition algorithm chose maternal Tg value of 17 μg/L for optimum splits to best predict LGA at birth. Accordingly, the study population split to two subgroups by Tg above and below 17 μg/L (Table 1). The Tg>17 μg/L exhibited significantly lower estimated iodine intake and lower ICS intake. Additionally, gravidity, parity and LGA prevalence were significantly higher in this subgroup. Other maternal and newborn characteristic did not differ significantly across subgroups. Detailed comparisons are described in Table 1. In addition, maternal Tg>17μg/L values were five times more likely to result in LGA newborn (OR = 5 [95% CI 1, 18]; p < 0.01, Fisher exact test).
Figure 1.
Demonstration of the correlation between maternal GCT and newborns birth percentiles.
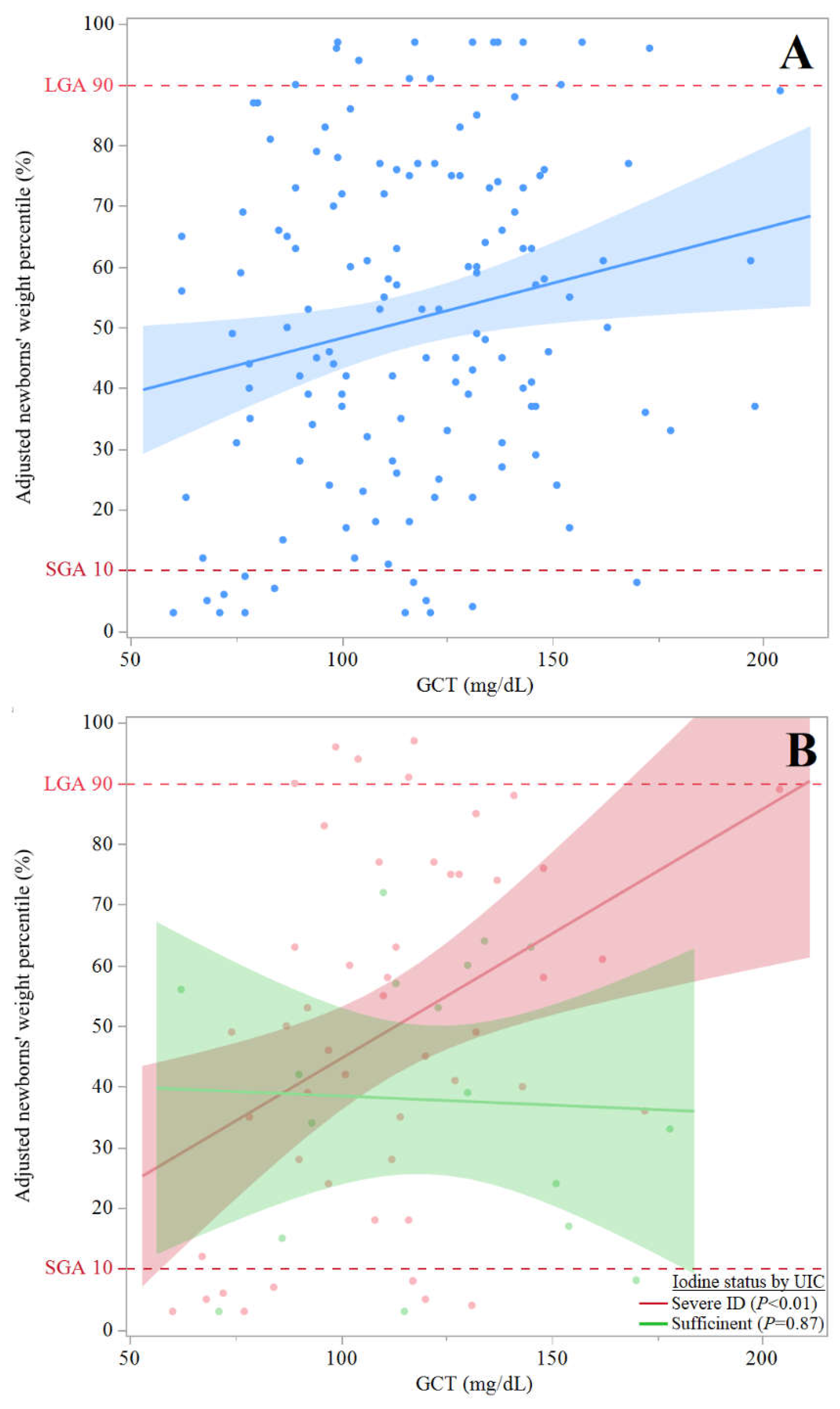
- (A)
- Scattered plot of adjusted newborns' weight percentiles (y axis) by GCT values (n=171) (x axis) of all participants with available GCT results (n=171) with dashed vertical lines to show LGA and SGA): y = 30.2 + 0.2(x), and R2 = 0.039; β (95% CI) = 0.20 (0.03, 0.33), P=0.018. The association remained significant in multivariate regression analysis adjusting for pregnant women age, smoking status, BMI at delivery, parity and gravidity: β (95 %CI) = -0.21 (0.03, 0.36), P=0.022.
- (B)
- Scattered plot of adjusted newborns' weight percentiles (y axis) by GCT values (n=86), excluding participants with mild-to-moderate ID (x axis) with lines to show linear fit (dashed vertical lines to show LGA and SGA); For participants with sufficient iodine status (by UIC): y= 41.4 + 0.03(x), R2=0, P=NS; For participants with severe ID (by UIC): y = 3.5 + 0.4(x), and R2 = 0.16, β (95% CI) = 0.33 (0.09, 0.55), P<0.01. The association remained significant in multivariate regression analysis adjusting for pregnant women age, smoking status, BMI at delivery, parity and gravidity: β (95 %CI) = 0.4 (0.37, 1.62), P<0.01.
Abbreviations: GCT, glucose challenge test; LGA, large for gestational age; SGA, small for gestational age; CI, confidence intervals; ID, iodine deficiency; UIC, urinary iodine concentrations; BMI, body mass index.
Figure 2.
Illustrated multiple possible maternal variables with possible contribution for LGA risk according to Proportional Hazards model.Tg>13g/L was independently associated with LGA (adjusted hazard ratio = 3.4, 95% CI: 1.4–10.2, p=0.001, Cox proportional hazards model; time for event – total gestational age at birth), while all others did not.LGA, large-for-gestational-age; GDM, gestational Diabetes Mellitus; IHT, isolated hypothyroxinemia (FT4 < 0.93 ng/L, TSH < 2.5 mU/L or 4.0 mU/L during 1st and both 2nd 3rd trimester, respectively); IVF, In vitro fertilization; BMI, body mass index; UIC, urinary iodine concentration; IS, iodized salt; FT3, Free triiodothyronine; GCT, glucose challenge test; SCH, subclinical Hypothyroidism (TSH > 2.5 mU/L or 4.0 mU/L during 1st and both 2nd 3rd trimester, respectively, along with normal FT3 and FT4); ICS, iodine-containing supplement.
Figure 2.
Illustrated multiple possible maternal variables with possible contribution for LGA risk according to Proportional Hazards model.Tg>13g/L was independently associated with LGA (adjusted hazard ratio = 3.4, 95% CI: 1.4–10.2, p=0.001, Cox proportional hazards model; time for event – total gestational age at birth), while all others did not.LGA, large-for-gestational-age; GDM, gestational Diabetes Mellitus; IHT, isolated hypothyroxinemia (FT4 < 0.93 ng/L, TSH < 2.5 mU/L or 4.0 mU/L during 1st and both 2nd 3rd trimester, respectively); IVF, In vitro fertilization; BMI, body mass index; UIC, urinary iodine concentration; IS, iodized salt; FT3, Free triiodothyronine; GCT, glucose challenge test; SCH, subclinical Hypothyroidism (TSH > 2.5 mU/L or 4.0 mU/L during 1st and both 2nd 3rd trimester, respectively, along with normal FT3 and FT4); ICS, iodine-containing supplement.
Estimated iodine intake levels correlated differently with maternal FT4 values. Estimated iodine intake levels among participant reporting no ICS intake were significantly and inversely correlated with maternal FT4 values, but significance did not survive adjustments for age, smoking status, BMI at delivery, parity and gravidity as reported in detail in Figure 3A. On the other hand, estimated iodine intake levels among participant reporting ICS intake were significantly and positively correlated with maternal FT4 values that remained significant after adjustment for age, smoking, BMI, parity and gravidity (Figure 3A). As shown in Figure 3B, maternal FT4 values negatively correlated with birthweight percentiles. This correlation remained significant after adjustment for age, smoking, BMI, parity and gravidity.
(A) Scattered plot of FT4 values (y axis) by estimated iodine intake levels (x axis), divided (overlay) by self-report on ICS intake at any period of pregnancy (n=178); For participants reporting no ICS intake throughout all gestation: y = 1.1 – 0.001(x), R2 = 0.06, β (95% CI) = -0.25 (0, -0.0001), P=0.044. The association did not remain significant in multivariate regression analysis adjusting for pregnant women age, smoking status, BMI at delivery, parity and gravidity; For participants reporting ICS intake at any time-period of pregnancy: y = 0.9 – 0.001(x), R2 = 0.13, β (95% CI) = 0.36 (0.0003, 0.0008), P<0.001. The association remained significant in multivariate regression analysis adjusting for pregnant women age, smoking status, BMI at delivery, parity and gravidity: β (95 %CI) = 0.35 (0.0002, 0.0008), P=0.001.
(B) Scattered plot of adjusted newborns' weight percentiles (y axis) by FT4 values (n=173), excluding participants with GDM (x axis) with dashed vertical lines to show LGA and SGA (dark purple points are participants with IHT): y = 82.6 – 30.1(x), R2 = 0.038, β (95% CI) = -0.17 (-1.64, -59.52), P=0.024. The association remained significant in multivariate regression analysis adjusting for pregnant women age, smoking status, BMI at delivery, parity and gravidity: β (95 %CI) = -0.15 (-0.08, -56.49), P=0.049.
The solid lines represent the estimated linear fit and the shaded areas illustrate the 95% CIs. Abbreviations: FT4 = Free thyroxine, ICS = iodine-containing supplement, LGA = large for gestational age, SGA = small for gestational age, IHT = isolated hypothyroxinemia, CI = confidence interval.
4. Discussion
This was a longitudinal prospective cohort study testing the association of both glucose and iodine intake levels with birthweight in pregnant women. Although GCT values correlated with adjusted newborn weight percentiles (Figure A), we revealed a strong independent association of lower iodine status and increased birthweight percentiles as well as LGA (severe ID by UIC, Figure 1B and suggestive of iodine insufficiency, Figure 2, respectively). Additionally, estimated iodine intake positively correlated with serum FT4 levels among participants reporting ICS (Figure 3A). Moreover, adjusted maternal FT4 values inversely correlated with newborn weight percentiles (Figure 3B). These findings may indicate that sufficient iodine status and ICS intake restrain, and perhaps modify, the impact of maternal hyperglycemia on offspring weight.
Along with the possibility that iodine intake can modify hyperglycemia effect on birthweight, we observed that sufficient maternal iodine status, as measured by UIC >150 μg/L, was not associated with increased birth weight, even among participants with maternal dysglycemia (Figure 1B). This observation is not in line with a recent meta-analysis conducted on 23 cohorts with 42,269 participants [28]. Birth weight was similar between UIC ≥ 150 μg/L and <150 μg/L, with no evidence of linear trends [28]. The difference in the findings between this meta-analysis and our study may stem from adjustments for confounding, with variation in urine sample collection and exposure definition. Additionally, our study used birthweight percentiles that were standardized for the Israeli population while some of the other studies included in the meta-analysis used a z-score to determine weight percentiles [26,28]. Moreover, the meta-analysis did not include findings regarding stratified iodine status by UIC into severe-ID, while we did include such findings in the current study (Figure 1B). Moreover, our results are in line with a recent single-center study from China, showing nearly significant (p=0.07) higher birthweight among offspring of mothers with ID (N=726) [15]. In our study population, an overall mild-to-moderate ID was detected. Hence, it can be suggested that the impact of maternal dysglycemia on birthweight may be also differentiated by ID severity.
The trend shown in Figure 3, as well as the full mechanism behind a possible ID-FT4-LGA axis in humans, are not fully established [29]. While the patterns underlying this association may be complex and need to be clarified, it is likely that ID leads to low FT4 levels (as iodine is an essential substrate for T4 synthesis) [30,31]. In turn, it is well established that low thyroid hormone levels underlie insulin resistance [32,33,34] which is characterized by increased insulin secretion both in GDM and type 2 diabetes [35,36]. Further, maternal insulin can act as a growth factor in fetuses, which might lead to LGA [37,38]. On a molecular level, thyroid hormone deficiency in fetuses has been implicated with decreased lipolysis in adipocytes and decrease de novo lipogenesis in the liver, via Sterol regulatory element binding proteins-1, 2 (SREBP1 and -2) [39]. Moreover, T3 has been shown to regulate Carbohydrate response element binding protein (ChREBP) in the liver, brown adipose tissue and Pancreas [40,41,42], which is a key regulator of de novo lipogenesis in various metabolic tissues. Therefore, providing a possible molecular mechanism for how ID during pregnancy could influence in utero growth and development (by thyroid function) in the fetus can be constructive, but remains to be elucidated.
Although we found an association between estimated iodine intake (among participants reporting ICS intake) and FT4 (Figure 3A), no cause-and-effect relationship was established. Among Asian populations, an interventional study found that ICS intake does not improve maternal thyroid function among pregnant women with mild-to-moderate ID [43]. According to our interpretation of the current study, we believe iodine status is the cause, while thyroid hormone is the effect, as supported by another interventional trial conducted among pregnant Norwegian women with mild-to-moderate ID [44]. As the current study did not explore the iron status of the participants or the iron content of the self-reported ICS, we cannot exclude the possibility that supplementary iron contributed to FT4. It has been shown in recent studies involving Chinese pregnant women that FT4 levels can change with iron status during pregnancy as well as that maternal anemia at delivery is a risk factor for low birth weight [45,46]. It is therefore important to investigate the effect of both iron and iodine intakes on maternal thyroid function as well as the weight of offspring.
Our study has several notable strengths. The cohort was of sufficient size to monitor iodine status in the studied population. The parallel quantification of three iodine status biomarkers (sIFFQ, Tg and UIC) allowed for a detailed assessment of the iodine status and provided a comprehensive status of the prevalent ID among participants. Also, it contributed to a deeper understanding of our hypothesis that iodine intake may modify the effect of maternal dysglycemia on excessive fetal growth.
Our study also had several limitations. One is the use of spot UIC to estimate subgroups. Of note, the minimal number of spot urine samples needed to estimate population iodine status within a precision range of ±10% should include about 125 participants [47]. However, the same pattern of GCT-ID-LGA axis was also observed by using the sIFFQ (Figure 3A) as well as Tg (Figure 1 and Table 1). Another potential limitation was the absence of data regarding maternal iron statuses throughout pregnancy which could affect both thyroid function and fetal growth [35]. Moreover, we did not measure estimated fetal weight percentile during pregnancy. Thus, the lack of maternal iron status and estimated fetal weight gain during pregnancy might weaken the hypothesis regarding a human ID-FT4-LGA axis. Nevertheless, we plan to explore this hypothesis in future work.
5. Conclusions
This study suggests that insufficient iodine status during pregnancy might increase LGA risk in mild-to-moderate ID regions. Sufficient iodine status and ICS intake may modify and restrain the effect of maternal hyperglycemia on offspring overgrowth. Further investigations should focus on the relationship between maternal ID and newborn weight via maternal T4, among pregnant women with maternal dysglycemia.
Author Contributions
Conceptualization, Yaniv Ovadia; Data curation, Simon Shenhav, Yoel Toledano and Yaniv Ovadia; Formal analysis, Yaniv Ovadia; Funding acquisition, Simon Shenhav Dov Gefel and Yaniv Ovadia; Investigation, Shani Rosen, Yael Avrahami-Benyounes and Yaniv Ovadia; Methodology, Simon Shenhav, Eyal Anteby and Yaniv Ovadia; Project administration, Yaniv Ovadia; Resources, Simon Shenhav, Dov Gefel, Shani Rosen, Shlomo Fytlovich, Eyal Anteby and Yaniv Ovadia; Software, Yaniv Ovadia; Supervision, Eyal Anteby; Validation, Ludmila Groisman, Efrat Rorman and Shlomo Fytlovich; Visualization, Yaniv Ovadia; Writing – original draft, Yaniv Ovadia; Writing – review & editing, Yaniv Ovadia, Dov Gefel, Shani Rosen, Liora S. Katz, Lihi Hen, Yoel Yoledano & Simon Shenhav. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by Barzilai University Medical Center Ashkelon intramural fund. Partial support was also provided by a grant from the Materna Institute for Research and Infant Nutrition Promotion (grant number 01082019). The funders did not have a role in the design, implementation, analysis, or interpretation of this study. The funding parties were not involved in the study.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of Barzilai University Medical Center Ashkelon (approval number 001-17-BRZ dated 7 August 2017).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data described in the manuscript, code book, and analytic code will be made available upon request pending application and approval.
Acknowledgments
We are indebted to all study participants. We thank Dr. Arie Budovsky from BUMCA’s research authority for discussing and reviewing this manuscript. We acknowledge Mr Amit Shama from the Robert H Smith Institute of Plant Sciences and Genetics, Faculty of Agriculture, The Hebrew University of Jerusalem, Rehovot, Israel, for his assistance with statistical analysis. We extend our gratitude to Dr Bruce Rosen from the The Myers-JDC-Brookdale Institute, whose expertise enriched this article. We also thank Ms. Ruhama Kremer and Ms. Hagit Afuta of BUMCA’s Department of Obstetrics and Gynecology for their assistance with the study’s ethical and administrative procedures.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Thompson C, Syddall H, Rodin I, Osmond C, Barker DJ. Birth weight and the risk of depressive disorder in late life. Br J Psychiatry. 2001;179:450-5. https://doi.org/10.1192/bjp.179.5.450. [CrossRef]
- Koller-Smith LI, Shah PS, Ye XY, Sjörs G, Wang YA, Chow SSW, Darlow BA, Lee SK, Håkanson S, Lui K; Australian and New Zealand Neonatal Network; Canadian Neonatal Network; Swedish Neonatal Quality Register. Comparing very low birth weight versus very low gestation cohort methods for outcome analysis of high risk preterm infants. BMC Pediatr. 2017;17(1):166. https://doi.org/10.1186/s12887-017-0921-x. [CrossRef]
- Barker DJ. The developmental origins of chronic adult disease. Acta Paediatr Suppl. 2004 Dec;93(446):26-33. https://doi.org/10.1111/j.1651-2227.2004.tb00236.x. PMID: 15702667. [CrossRef]
- Li N, An H, Jin M, Li Z, Zhang Y, Zhang L, Liu J, Ye R. Association of Infants Small for Gestational Age with Anemia under Five Years Old in Two Large Longitudinal Chinese Birth Cohorts. Nutrients. 2022;14(5):1006. https://doi.org/10.3390/nu14051006. [CrossRef]
- Scifres CM. Short- and Long-Term Outcomes Associated with Large for Gestational Age Birth Weight. Obstet Gynecol Clin North Am. 2021 Jun;48(2):325-337. https://doi.org/10.1016/j.ogc.2021.02.005. PMID: 33972069. [CrossRef]
- Johnsson IW, Haglund B, Ahlsson F, Gustafsson J. A high birth weight is associated with increased risk of type 2 diabetes and obesity. Pediatr Obes. 2015;10(2):77-83. https://doi.org/10.1111/ijpo.230. [CrossRef]
- HAPO Study Cooperative Research Group, Metzger BE, Lowe LP, Dyer AR, Trimble ER, Chaovarindr U, Coustan DR, Hadden DR, McCance DR, Hod M, McIntyre HD, Oats JJ, Persson B, Rogers MS, Sacks DA. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med. 2008;358(19):1991-2002. https://doi.org/10.1056/NEJMoa0707943. [CrossRef]
- Beksac MS, Tanacan A, Hakli DA, Ozyuncu O. Use of the 50-g glucose challenge test to predict excess delivery weight. Int J Gynaecol Obstet. 2018 Jul;142(1):61-65. https://doi.org/10.1002/ijgo.12504. [CrossRef]
- Eastman CJ, Ma G, Li M. Optimal Assessment and Quantification of Iodine Nutrition in Pregnancy and Lactation: Laboratory and Clinical Methods, Controversies and Future Directions. Nutrients. 2019;11(10):2378. https://doi.org/10.3390/nu11102378. [CrossRef]
- Shields BM, Knight BA, Hill A, Hattersley AT, Vaidya B. Fetal thyroid hormone level at birth is associated with fetal growth. J Clin Endocrinol Metab. 2011 Jun;96(6):E934-8. https://doi.org/10.1210/jc.2010-2814. [CrossRef]
- Korevaar TI, Chaker L, Jaddoe VW, Visser TJ, Medici M, Peeters RP. Maternal and Birth Characteristics Are Determinants of Offspring Thyroid Function. J Clin Endocrinol Metab. 2016 Jan;101(1):206-13. https://doi.org/10.1210/jc.2015-3559. [CrossRef]
- Vulsma T, Gons MH, de Vijlder JJ. Maternal-fetal transfer of thyroxine in congenital hypothyroidism due to a total organification defect or thyroid agenesis. N Engl J Med. 1989;321(1):13-6. https://doi.org/10.1056/NEJM198907063210103. [CrossRef]
- Mortimer RH, Galligan JP, Cannell GR, Addison RS, Roberts MS. Maternal to fetal thyroxine transmission in the human term placenta is limited by inner ring deiodination. J Clin Endocrinol Metab. 1996;81(6):2247-9. https://doi.org/10.1210/jcem.81.6.8964859. [CrossRef]
- Ovadia YS, Zangen S, Rosen SR, Gefel D, Almashanu S, Benbassat C, Fytlovich S, Aharoni D, Anteby EY, Shenhav S. Maternal iodine deficiency: a newborns' overweight risk factor? A prospective study. Arch Gynecol Obstet. 2022;305(3):777-787. https://doi.org/10.1007/s00404-021-06261-x. [CrossRef]
- Zhang X, Yuan N, Sun J, Zhao X, Du J, Nan M, Zhang Q, Ji L. Association Between Iodine Nutritional Status and Adverse Pregnancy Outcomes in Beijing, China: a Single-Center Cohort Study. Biol Trace Elem Res. 2022;200(6):2620-2628. https://doi.org/10.1007/s12011-021-02887-9. [CrossRef]
- Shenhav S, Benbassat C, Gefel D, Zangen S, Rosen SR, Avrahami-Benyounes Y, Almashanu S, Groisman L, Rorman E, Fytlovich S, Anteby EY, Ovadia YS. Can Mild-to-Moderate Iodine Deficiency during Pregnancy Alter Thyroid Function? Lessons from a Mother-Newborn Cohort. Nutrients. 2022;14(24):5336. https://doi.org/10.3390/nu14245336. [CrossRef]
- Silva CM, Arnegard ME, Maric-Bilkan C. Dysglycemia in Pregnancy and Maternal/Fetal Outcomes. J Womens Health (Larchmt). 2021;30(2):187-193. https://doi.org/10.1089/jwh.2020.8853. [CrossRef]
- Pregnancy at Age 35 Years or Older: ACOG Obstetric Care Consensus No. 11. Obstet Gynecol. 2022;140(2):348-366. https://doi.org/10.1097/AOG.0000000000004873. [CrossRef]
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins–Obstetrics. Obesity in Pregnancy: ACOG Practice Bulletin, Number 230. Obstet Gynecol. 2021;137(6):e128-e144. https://doi.org/10.1097/AOG.0000000000004395. [CrossRef]
- Zimmermann, M.B.; Andersson, M. Assessment of iodine nutrition in populations: past, present, and future. Nutr Rev 2012, 70, 553-570. https://doi.org/10.1111/j.1753-4887.2012.00528.x. [CrossRef]
- IOH. Standing committee on the Scientific Evaluation of Dietary Reference Intakes, Institute of Health; Press, N.A., Ed. National Academy Press: USA, 2001.
- CDC. Laboratory Procedure Manual: Iodine in Urine. NHANES 2003–2004 Inorganic Toxicology and Nutrition Branch, Division of Laboratory Sciences, National Center for Environmental Health: 2007.
- WHO. Assessment of iodine deficiency disorders and monitoring their elimination. A guide for programmed managers. Third Edition; World Health Organization: France, 2007.
- Alexander, E.K.; Pearce, E.N.; Brent, G.A.; Brown, R.S.; Chen, H.; Dosiou, C.; Grobman, W.A.; Laurberg, P.; Lazarus, J.H.; Mandel, S.J., et al. 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid 2017, 27, 315-389. https://doi.org/10.1089/thy.2016.0457. [CrossRef]
- Ma, Z.F.; Skeaff, S.A. Thyroglobulin as a biomarker of iodine deficiency: a review. Thyroid 2014, 24, 1195-1209. https://doi.org/10.1089/thy.2014.0052. [CrossRef]
- Dollberg, S.; Haklai, Z.; Mimouni, F.B.; Gorfein, I.; Gordon, E.S. Birth weight standards in the live-born population in Israel. Isr Med Assoc J 2005, 7, 311-314.
- Davidson, S.; Sokolover, N.; Erlich, A.; Litwin, A.; Linder, N.; Sirota, L. New and improved Israeli reference of birth weight, birth length, and head circumference by gestational age: a hospital-based study. Isr Med Assoc J 2008, 10, 130-134.
- Greenwood, D.C.; Webster, J.; Keeble, C.; Taylor, E.; Hardie, L.J. Maternal Iodine Status and Birth Outcomes: A Systematic Literature Review and Meta-Analysis. Nutrients 2023, 15, 387. https://doi.org/10.3390/nu15020387. [CrossRef]
- Dosiou C, Medici M. MANAGEMENT OF ENDOCRINE DISEASE: Isolated maternal hypothyroxinemia during pregnancy: knowns and unknowns. Eur J Endocrinol. 2017;176(1):R21-R38. https://doi.org/10.1530/EJE-16-0354. [CrossRef]
- Glinoer D. Maternal and fetal impact of chronic iodine deficiency. Clin Obstet Gynecol. 1997;40(1):102-116. https://doi.org/10.1097/00003081-199703000-00011. [CrossRef]
- Rousset B, Dupuy C, Miot F, Dumont J. Chapter 2 Thyroid Hormone Synthesis And Secretion. In: Feingold KR, Anawalt B, Blackman MR, et al., eds. Endotext. South Dartmouth (MA): MDText.com, Inc.; September 2, 2015.
- Fernández-Real JM, López-Bermejo A, Castro A, Casamitjana R, Ricart W. Thyroid function is intrinsically linked to insulin sensitivity and endothelium-dependent vasodilation in healthy euthyroid subjects. J Clin Endocrinol Metab. 2006;91(9):3337-3343. https://doi.org/10.1210/jc.2006-0841. [CrossRef]
- Roos A, Bakker SJ, Links TP, Gans RO, Wolffenbuttel BH. Thyroid function is associated with components of the metabolic syndrome in euthyroid subjects. J Clin Endocrinol Metab. 2007;92(2):491-496. https://doi.org/10.1210/jc.2006-1718. [CrossRef]
- Fontenelle LC, Feitosa MM, Severo JS, et al. Thyroid Function in Human Obesity: Underlying Mechanisms. Horm Metab Res. 2016;48(12):787-794. https://doi.org/10.1055/s-0042-121421. [CrossRef]
- Reaven GM. Banting lecture 1988. Role of insulin resistance in human disease. Diabetes. 1988;37(12):1595-1607. https://doi.org/10.2337/diab.37.12.1595. [CrossRef]
- Barbour LA, McCurdy CE, Hernandez TL, Kirwan JP, Catalano PM, Friedman JE. Cellular mechanisms for insulin resistance in normal pregnancy and gestational diabetes [published correction appears in Diabetes Care. 2007 Dec;30(12):3154]. Diabetes Care. 2007;30 Suppl 2:S112-S119. https://doi.org/10.2337/dc07-s202. [CrossRef]
- Schwartz R, Gruppuso PA, Petzold K, Brambilla D, Hiilesmaa V, Teramo KA. Hyperinsulinemia and macrosomia in the fetus of the diabetic mother. Diabetes Care. 1994;17(7):640-648. https://doi.org/10.2337/diacare.17.7.640. [CrossRef]
- Langer O. Fetal macrosomia: etiologic factors. Clin Obstet Gynecol. 2000;43(2):283-297. https://doi.org/10.1097/00003081-200006000-00006. [CrossRef]
- Damiano F, Rochira A, Gnoni A, Siculella L. Action of Thyroid Hormones, T3 and T2, on Hepatic Fatty Acids: Differences in Metabolic Effects and Molecular Mechanisms. Int J Mol Sci. 2017;18(4):744. https://doi.org/10.3390/ijms18040744. [CrossRef]
- Katz LS, Xu S, Ge K, Scott DK, Gershengorn MC. T3 and Glucose Coordinately Stimulate ChREBP-Mediated Ucp1 Expression in Brown Adipocytes From Male Mice. Endocrinology. 2018;159(1):557-569. https://doi.org/10.1210/en.2017-00579. [CrossRef]
- Katz LS, Argmann C, Lambertini L, Scott DK. T3 and glucose increase expression of phosphoenolpyruvate carboxykinase (PCK1) leading to increased β-cell proliferation. Mol Metab. 2022;66:101646. https://doi.org/10.1016/j.molmet.2022.101646. [CrossRef]
- Hashimoto K, Ishida E, Matsumoto S, et al. Carbohydrate response element binding protein gene expression is positively regulated by thyroid hormone. Endocrinology. 2009;150(7):3417-3424. https://doi.org/10.1210/en.2009-0059. [CrossRef]
- Verhagen NJE, Gowachirapant S, Winichagoon P, Andersson M, Melse-Boonstra A, Zimmermann MB. Iodine Supplementation in Mildly Iodine-Deficient Pregnant Women Does Not Improve Maternal Thyroid Function or Child Development: A Secondary Analysis of a Randomized Controlled Trial. Front Endocrinol (Lausanne). 2020 Oct 6;11:572984. https://doi.org/10.3389/fendo.2020.572984. [CrossRef]
- Wang F, Zhang Y, Yuan Z, et al. The association between iron status and thyroid hormone levels during pregnancy. J Trace Elem Med Biol. 2022;74:127047. https://doi.org/10.1016/j.jtemb.2022.127047. [CrossRef]
- Chu FC, Shaw SW, Lo LM, Hsieh TT, Hung TH. Association between maternal anemia at admission for delivery and adverse perinatal outcomes [published correction appears in J Chin Med Assoc. 2020 Nov;83(11):1054]. J Chin Med Assoc. 2020;83(4):402-407. https://doi.org/10.1097/JCMA.0000000000000215. [CrossRef]
- Andersen S, Karmisholt J, Pedersen KM, Laurberg P. Reliability of studies of iodine intake and recommendations for number of samples in groups and in individuals. Br J Nutr. 2008;99(4):813-818. https://doi.org/10.1017/S0007114507842292. [CrossRef]
- Luo J, Wang X, Yuan L, Guo L. Iron Deficiency, a Risk Factor of Thyroid Disorders in Reproductive-Age and Pregnant Women: A Systematic Review and Meta-Analysis. Front Endocrinol (Lausanne). 2021;12:629831. https://doi.org/10.3389/fendo.2021.629831. [CrossRef]
Figure 3.
Overview of the possible association between maternal estimated iodine intake and newborns birth percentiles.
Figure 3.
Overview of the possible association between maternal estimated iodine intake and newborns birth percentiles.
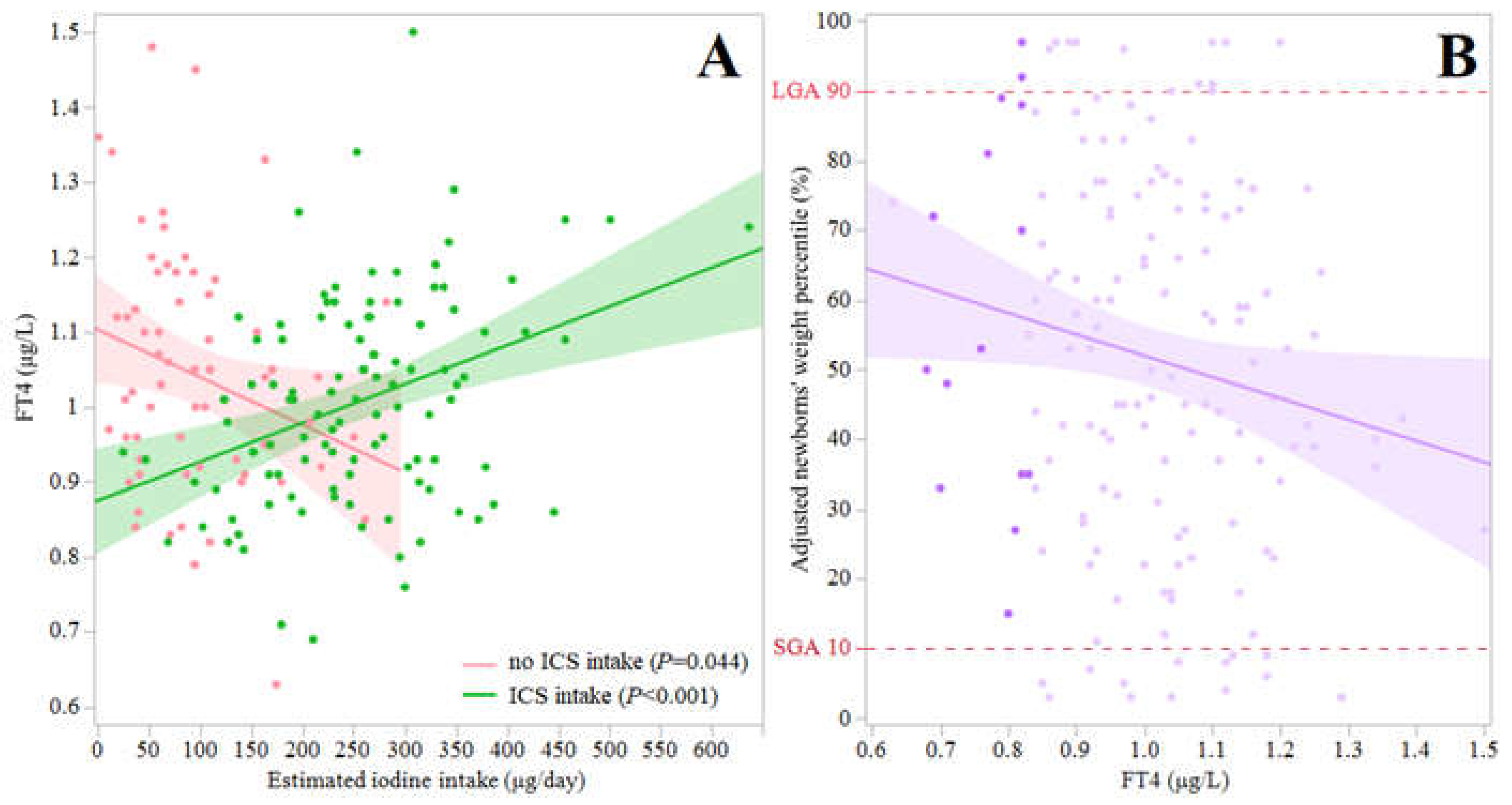

Table 1.
Sociodemographic, anthropometric and clinical characteristics of pregnant women and their offspring.
Table 1.
Sociodemographic, anthropometric and clinical characteristics of pregnant women and their offspring.
| Sub-group by maternal Tg values | >17μg/L | ≤17μg/L | P value |
|---|---|---|---|
| Pregnant women, n | 96 | 92 | |
| Age (y), mean±SD | 31±6 | 32±5 | NS |
| Gestational age (weeks) at recruitment, mean±SD | 32±7 | 31±7 | NS |
| Israeli born, n(%) | 52(54) | 42(46) | NS |
| Tertiary education, n(%) | 42(44) | 52(56) | NS |
| Secular n(%) | 28(30) | 35(38) | NS |
| IVF | 6(6) | 10(11) | NS |
| Smoking | |||
| Current smoker | 13(14) | 11(12) | NS |
| Past smoker | 18(19) | 18(20) | NS |
| Alcohol, n(%) | 0(0) | 0(0) | NS |
| Post-psychological stressful event, n(%) | 14(15) | 18(20) | NS |
| GCT (mg/dL), mean±SD | 119±28 | 114±31 | NS |
| BMI (kg/m2) | |||
| At recruitment, mean±SD | 29±5 | 28±5 | NS |
| At delivery, mean±SD | 31±6 | 29±4 | NS |
| Gravidity, mean±SD* | 4±2 | 3±2 | 0.05 |
| Parity, mean±SD* | 3±2 | 2±1 | 0.03 |
| Iodine Intake | |||
| Estimated dietary Iodine intake (μg/d), mean±SD* | 163±104 | 221± 114 | <0.01 |
| Iodine intake < RDA, n (%)F | 69(72) | 44(48) | <0.01 |
| Iodized salt use, n(%) ם | 4(4) | 5(5) | NS |
| ICS intake, n (%) F | 44(46) | 62(67) | <0.01 |
| Estimated iodine intake from ICS (μg/d), median (IQR)K ****MIQR |
1 (0-150) | 150 (0-220) | <0.01 |
| Dietary goitrogens exposure, n (%) F | 20(22) | 12(13) | NS |
| UIC | |||
| Median UIC, μg/L (IQR) | 53(39-86) | 65(41-97) | NS |
| Participants with UIC <150 μg/L, n(%) | 77(80) | 72(86) | NS |
| Participants with UIC <50 μg/L, n (%) | 34(35) | 30(33) | NS |
| TSH | |||
| Mean±SD (mIU/L), n(%)) | 1.8±1.0 | 1.8±1.0 | NS |
| Participants with SCH, n(%) | 4 (4) | 2 (2) | NS |
| FT4 | |||
| Mean±SD (μg/L), n(%) | 1.0±0.2 | 1.0±0.1 | NS |
| Participants with IHT, n(%) | 7(7) | 8(9) | NS |
| FT3 (pmol/L), mean±SD | 4.1±0.7 | 3.9±0.7 | NS |
| TPO Ab | |||
| TPO Ab (mIU/L), median(IQR) | 13(11-16) | 13(11-17) | NS |
| Positive TPO Ab, n(%) | 1(1) | 4(4) | NS |
| Tg Ab | |||
| Tg Ab (mIU/L), median(IQR) | 10(10-11) | 10(10-12) | NS |
| Positive Tg Ab, n(%) | 1(1) | 4(5) | NS |
| Newborns at birtha, n | 85 | 84 | |
| Gestational age (days), mean±SD | 266±29 | 270±13 | NS |
| Preterm birth, n (%) | 13 (15) | 11 (13) | NS |
| Gender (Female, Male) | 36, 47 | 36,48 | NS |
| Apgar score | |||
| At 1 minute after delivery, mean±SD | 8.9±0.1 | 8.9±0.1 | NS |
| At 5 minutes after delivery, mean±SD | 9.9±0.4 | 9.9±0.3 | NS |
| Birthweight | |||
| Crude weight (g), mean±SD | 3,176±652 | 3,029±580 | NS |
| LBW | 3(4) | 8(10) | NS |
| Macrosomia | 6(7) | 2(2) | NS |
| Adjusted weight percentile (%), mean±SD Do | 56±28 | 49±26 | 0.07 |
| SGA | 5(6) | 10(12) | NS |
| LGAF | 13(15) | 3(3) | 0.02 |
| Length percentile (%), mean±SDDa | 74.4±26.3 | 70.6±25.9 | NS |
| Head circumference (cm) | |||
| Mean±SD | 34.4±2.1 | 34.0±1.7 | NS |
| > 90th percentileDa, n(%) | 27(28) | 17(18) | NS |
Tg, thyroglobulin; SD, standard deviation; NS, not significant; IVF, in vitro fertilization; GCT, 50-g 1-h post oral glucose challenge test; BMI, Body mass index; RDA, recommended daily allowance (220 μg/d); ICS, iodine-containing supplement; IQR, interquartile range; UIC, urinary iodine concentration; TSH, thyrotropin - thyroid stimulating hormone; SCH, subclinical Hypothyroidism (TSH < 2.5 mU/L or 4.0 mU/L during 1st and both 2nd 3rd trimester); FT4, free thyroxine; IHT, isolated hypothyroxinemia (FT4 < 0.93 ng/L, TSH > 2.5 mU/L or 4.0 mU/L during 1st and both 2nd 3rd trimester); FT3, Free triiodothyronine; TPO Ab, thyroid peroxidase antibodies; Tg Ab, thyroglobulin antibodies; LBW, birth weight below 2,500 g among full-term newborns; SGA, small-for-gestational age; LGA, large-for-gestational age. * Significant difference (Student's t test, α = 0.05); ם Iodized salt, 3 μg iodine/100 gr; F Significant difference (Fisher's Exact test, α = 0.05); K Significant difference (Kruskal-Wallis test, α = 0.05); Do Adjusted for gestational age and gender according to birth weight Israeli standards [26].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



