
Submitted:
26 May 2023
Posted:
30 May 2023
You are already at the latest version
Abstract
The aim of this systematic scoping review was to provide scientific evidence on the efficacy and methods of application of hyaluronic acid in the coverage of gingival recessions in terms of recession depth (RD) reduction, clinical attachment level (CAL) gain, probing depth (PD). An electronic search of the literature on the main databases was conducted. Initially, 405 articles were identified. Finally, 4 studies were included after the review process. It was not possible to perform a meta-analysis of the articles selected because of the differences among the surgical treatments and commercial formulations and compositions of hyaluronic acid. Both randomized controlled trials in this research examined Recession Type 1 gingival treated with coronally advanced flap. Recessions were treated with either modified coronally advanced tunnel or laterally closed tunnel combined with subepithelial connective tissue graft and hyaluronic acid (HA) in all case series. The studies analyzed no significant variation was found in PD variable. The results of RD reduction are in accordance with the literature. Modifications of CAL are connected to variations of RD. HA seems to improve the clinical outcomes of the described surgical treatment.
Keywords:
gingival recession
; linear hyaluronic acid
; cross-linked hyaluronic acid
; root coverage procedure
; surgical treatment of recession
1. Introduction
Gingival Recession defect is defined as the apical shift of the gingival margin with respect to Cementoenamel Junction [1]. This condition is associated to a moderate difficulty in correct oral hygiene maintenance, dentinal hypersensitivity and a higher occurrence of carious or non-carious cervical lesions [2]. Patients have a relevant perception of a visible gingival recession, especially in maxillary anterior areas. As periodontal health was defined as the main variable able to influence smile patterns, this condition can consequently affect quality of life. People not able to express their emotions are negatively conditioned in smiling and can appear more insecure, introverted and unsatisfied [3].
Plenty of mucogingival surgery procedures and strategies have been reported in literature to conjugate more and more stringent esthetic demand to the restoration of a healthy and functional periodontal anatomy. In the literature, different root covering procedures (RCPs) are described alone or in combination with subepithelial connective tissue grafts (sCTG) or biomaterials. Surgical procedures used in the treatment of recession defects may basically be classified as pedicle soft-tissue graft procedures and free soft-tissue graft procedures [4]. Currently, the most frequently used surgical techniques for both single and multiple gingival recessions are coronal advanced flaps (CAF) and tunnel techniques. In addition to the speculations developed over the years on surgical techniques, another approach proposed to improve the effectiveness of root cover treatment is the application of enamel matrix derivative (EMD) [5]. Studies showed that CAF combined with sCTG or EMD increases the probability of achieving complete root coverage (CRC) in Miller class I and II [6] (Cairo type I) [7] recession defects compared to CAF alone [8,9,10]. The successes achieved with the use of EMD have encouraged clinicians to introduce another organic molecule in periodontal therapy: hyaluronic acid (HA). This molecule seems to have enhanced the clinical outcomes in terms of clinical attachment level (CAL) gain, reduction of bleeding on probing (BoP) of surgical and non-surgical periodontal procedures [11].
HA is a linear glycosaminoglycan (GAG) consisting of repeated units of D-glucoronic acid (1-B-3) N-Acetyl –D- glucosamine (1-B4) [12]. First isolated in early twentieth century [13], this molecule is ubiquitously distributed in vertebrated tissues in different concentrations and molecular weights [14]. Hyaluronic acid is able to bind to a large amount of water, forming a highly viscous gel. HA inhibits tissue breakdown by activating metalloproteinase inhibitors [15]. Hyaluronic acid stimulates cell migration and differentiation during the development and repair of soft and hard tissues [16]. Due to their unique biological and physico-chemical properties and to their safety profile, native HA and many of its derivatives represent interesting biomaterials for a variety of medical and cosmetic applications [17] including periodontal therapy [18]. At the beginning of this millennium, the enthusiasm about properties of hyaluronic acid led Pini Prato et al. to publish a case series reporting the use of HA in mucogingival therapy [19]. Nowadays, although the potential and role of this molecule is not entirely defined, hyaluronan has been applied in different way and in many oral surgical procedures demonstrating gratifying results [20]. The topical application of HA may lead to additional clinical benefits when used as an adjunctive to non-surgical and surgical periodontal therapy. In surgical treatment of gingival recession coverage, few clinical studies have resorted to application of HA. In these studies, it was observed an enhancing of the performance of the chosen surgical technique. Clinical outcomes seem to be improved when HA was applied during the surgical procedures [21,22]. The aim of this systematic scoping review is to provide further scientific evidence on the efficacy and methods of application of hyaluronic acid in the coverage of single and multiple gingival recessions in terms of recession depth (RD) reduction, clinical attachment level (CAL) gain, probing depth (PD).
2. Materials and Methods
2.1. Protocol
The present systematic scoping review was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA- ScR) guidelines for the purpose of mapping the evidence on a topic and identifying major concepts and knowledge gaps [23]. The protocol of the present scoping review was registered at the National Institute for Health Research PROSPERO, International Prospective Register of Systematic Reviews (https://www.crd.york.ac.uk/PROSPERO) with the registration ID: CRD42022346135.
An adaptation of the PICO (Population, Intervention, Comparison, and Outcome) model was used to construct a targeted question consisting of a PEO (Population, Exposure, and Outcome) framework to determine the association between a particular exposure and outcomes [24]. This strategy was developed to perform qualitative systematic reviews of health care interventions [25], including oral surgery procedures [26]. The main question was, "In surgical treatment of recessions, did the use of hyaluronic acid improve healing?" The primary outcome was RD reduction, while the secondary outcome was PD and consequently CAL.
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
All sources of evidence had to meet specific inclusion criteria to be included. Only articles written in English and without time exclusion criteria until May 2022 were screened. Studies included in the screening procedure were randomized controlled trials (RCTs), controlled clinical trials (CCTs), and retrospective and prospective case-control studies. No limitations were imposed on population characteristics, number of patients, age, or systemic conditions.Studies discussing the healing of gingival recessions treated surgically in combination with hyaluronic acid were included.
2.2.2. Exclusion criteria
All studies that did not meet the inclusion criteria were excluded, such as (1) in vitro and in vivo animal studies; (2) articles written in a language other than English; (3) case reports, literature reviews; (4) studies that did not report surgical treatment of recessions in combination with the use of hyaluronic acid; (5) studies that treated periodontal regeneration in conjunction with the use of hyaluronic acid.
2.2.3. Sources of Evidence
An electronic search of the literature on PubMed through the MEDLINE, Scopus, EMBASE and Web of Science databases was conducted. The search aimed to find relevant information on the use of hyaluronic acid in the surgical treatment of recessions. The years from 1968 to May 2022 were considered in all databases.
2.2.3. Search Strategies
For all libraries, a combination of specific keywords, medical topic titles [MeSH], and other non-indexed terms such as MeSH was used to identify all relevant studies according to the precise directions of the PEO query. Articles were selected on electronical databases using the following terms: (Hyaluron* acid) AND ((mucogingival surgery) OR (periodontal surgery) OR (recession coverage) OR (gingival recession*) OR (root coverage)). Additional screening of the reference lists of all pertinent articles was performed but no additional relevant studies were identified. No filters were applied to each search string during electronic research.
2.2.4. Selection of Sources of Evidence
Two reviewers (F.E.S and M.T.), working independently, have completed the preliminary screening of titles and abstracts of all included articles with a Cohen’s K of 0.7 (substantial agreement). Full-text articles were independently evaluated, and selections were compared between the two researchers. The final list and any disagreement between the two researchers were taken to the attention of a third and fourth researcher (M.M. and P.P.P.). Duplicate articles in the databases were identified and removed using EndNote Web reference manager software (Clarivate Analytics, Philadelphia, PA, USA).
Initially, 154 articles were identified in EMBASE, 104 in PubMed, 69 in SCOPUS, and 78 trials in the Web of Science. After duplicate removal, 214 articles remained for the screening phase. Following the evaluation of titles and abstracts, 196 publications were excluded. The full texts of the remaining 19 articles were read thoroughly. Overall, 14 studies had to be excluded after full text examination because they did not meet the above-mentioned inclusion criteria. Nandanwar’s article [27], although it reported employing HA in the RCP, was excluded because of clinical parameters that could not be compared with other studies. Finally, 4 studies [22,28,29,30] were included after the review process. The selection strategy was conducted as shown in flowchart represented in Figure 1.
3. Results
All data collection was performed using a spreadsheet designed to express all data on study characteristics and outcomes as tables in the results (Table 1 and Table 2). It was not possible to perform a meta-analysis of the articles selected because of the differences among the surgical treatments and commercial formulations and compositions of hyaluronic acid. A qualitative descriptive statistical approach was used to present the data.
3.1. Kumar (2014) – RCT [22]
3.1.1. Sample Analysis
3.1.2. Hyaluronic acid used
Linear hyaluronic acid (gengigel 0.2% gel which is 0.2% hyaluronan gel marketed by Ricerfarma pharmaceuticals, Milan, Italy).
3.1.3. Data
RD was measured regularly at baseline 1, 3, 6, 12 and 24 weeks postoperatively. PD and CAL were also measured along with RD at baseline and 12 and 24 weeks. Only measurements taken at baseline and 24 weeks will be reported below. In the test group at baseline the RD was 3.20 mm, at 24 weeks it was 1.10 mm, while in the control group at baseline the RD was 2.90 mm, at 24 weeks it was 1.00 mm. At 24 weeks, the change in RD was statistically significant (p = 0.00) in both groups
In the test group at baseline the PD was 1.80 mm, at 24 weeks it was 1.70 mm, while in the control group at baseline the PD was 2.00 mm, at 24 weeks it was 2.00 mm. In the test group at baseline the CAL was 5 mm, at 24 weeks it was 2.80 mm, while in the control group at baseline the CAL was 4.90 mm, at 24 weeks it was 3.00 mm. There was no statistically significant difference between experimental and control group in terms of PD and CAL but after 24 weeks the root coverage of the control group appeared more stable.
At 24 weeks in the test group the mean root coverage (MRC) achieved was 68.3% while in the control group it was 61,6%. In the test group at 24 weeks, complete root coverage (CRC) was achieved in 40% of cases, in the control group in 20% of cases. The MRC and CRC values at follow up were higher for the test group than the control group and the difference was statistically significant.
3.2. Pilloni (2017) – RCT [21]
3.2.1. Sample Analysis
Thirty patients with single RT1[7] (Cairo 2011) gingival recessions were enrolled in this RCT. Fifteen patients were treated with CAF + HA and 15 patients with CAF [32] (Zucchelli 2016). In the test group, seven females and eight males were treated with CAF + HA. The median age was 30 years. The control group consisted of seven women and eight men with a median age of 30 years.
3.2.2. Hyaluronic acid used
1,6% cross-linked HA, 0.2% linear HA (Hyadent BG, Regedent).
3.2.3. Data
Clinical outcomes were measured at baseline and at 18.
At baseline in both the case and control groups the RD was 3.0[1.0] mm, at 18 months in the test group RD was 0.0[0.0] mm while in the control group RD was 1.0[1.0] mm.
The comparison between the two groups showed statistically significant differences (p = 0.011).
At baseline in both the case and control groups PD was 1.0[0.0] mm, at 18 months in the test group PD was 1.0[1.0] mm while in the control group PD was 2.0[1.0] mm.
The comparison between the two groups showed no statistically significant differences (p = 0.717).
At baseline in both the case and control groups CAL was 4.0[1.0] mm, at 18 months in the test group CAL was 1.0[0.0] mm while in the control group CAL was 2.0[0.0] mm.
The comparison between the two groups showed no statistically significant differences (p = 0.023).
At baseline in both the case and control groups keratinized tissue (KT) was 2.0[1.0] mm, at 18 months in the test group KT was 2.0[0.0] mm while in the control group KT was 2.0[1.0] mm, no difference was found between the two groups.
No differences were found between the two groups (p = 0.116).
At 18 months in the test group MRC achieved was 93.8 ± 13.0% while in the control group it was 73.1%.
In the test group at 18 months, CRC was achieved in 80% of cases, in the control group in 33% of cases.
The MRC and CRC values at follow up were higher for the test group than the control group and the difference was statistically significant (p = 0.003 and 0.025, respectively).
3.2.4. Additional data
After 7 days after surgical treatment, postoperative morbidity (pain intensity, discomfort and swelling) was evaluated using the visual analog scale (VAS), swelling and discomfort were statistically lower in the test group (p = 0.010 and p = 0.029, respectively), no difference was found in pain intensity (p = 0.151).
3.3. Guldener (2020) - Case series [30]
3.3.1. Sample Analysis
Twelve patients presenting with isolated RT1[7] gingival recessions were included in the case series.
All 12 patients were treated consecutively as follows, using modified coronally advanced tunnel (MCAT) [33] or laterally closed tunnel (LCT) [34] in combination with sCTG.
Subsequently, HA was applied to the root surface and under the surrounding soft tissues using a sterile syringe.
Two males and ten females were included in this case series. The average age of the patients was 26.8±9.2.
3.3.2. Hyaluronic acid used
1,6% cross-linked HA, 0.2% linear HA (Hyadent BG, Regedent).
3.3.3. Data
In Guldener case series[30], clinical outcomes were measured at baseline and at 6±33 months.
At baseline the RD was 4.6[0.9]mm, at follow up it was 0.5[0.6].
At baseline the PD was 1.8[0.9]mm, at follow up it was 1.3[0.5].
At baseline the CAL was 6.4 mm, at follow up it was 1.8[0.5].
At baseline the KT was 1.6[0.9] mm, at follow up it was 4.9[1.3].
CRC was achieved in 50% of case and MRC was 96.09%.
3.4. Lanzrein (2020) - Case series [29]
3.4.1. Sample Analysis
In this case series fifteen healthy patients presenting with multiple mandibular RT1 and RT2 gingival recessions or multiple adjacent maxillary RT1 and RT2 [7] gingival recessions were treated with MCAT [33] or LCT [34] in combination with cross-linked hyaluronic acid and sCTG.
Five males and ten females were included in the case series. The average age of the patients was 38.6±15.8.
3.4.2. Hyaluronic acid used
1,6% cross-linked HA, 0.2% linear HA (Hyadent BG, Regedent).
3.4.3. Data
In Lanzrein case series [29], clinical outcomes were measured at baseline and at 6±30 months.
At baseline the RD was 3.3[0.8]mm, at follow up it was 0.8[1.0].
At baseline the PD was 1.3[0.5]mm, at follow up it was 1.5[0.5].
At baseline the CAL was 4.6 mm, at follow up it was 2.3.
At baseline the KT was 2.5[1.0] mm, at follow up it was 3.7[0.8].
CRC was achieved in 20% of case and MRC was 85.1%.
3.4.4. Additional data
In this article was evaluated the esthetic outcome of the surgical procedures by root coverage esthetic score (RES). Mean RES was 7.9 ± 1.9.
4. Discussion
Hyaluronic acid (HA) is a biodegradable, biocompatible, and nontoxic linear polysaccharide found in extracellular matrices [12]. The major function of HA is to bind water and facilitate the transfer of essential metabolites, hence preserving the structural and homeostatic integrity of these tissues [18]. Recent in vitro and animal studies have shown that HA induces angiogenesis [35], stimulates clot formation [36], has bacteriostatic activity [37] significantly increases the tensile strength of granulation tissue [38], stimulates osteogenesis [39] without interfering with the formation of new bone tissue [40]. These properties probably decrease healing range and consequently enhance the wound stability [41]. Recently, the use of HA has been introduced in dentistry for nonsurgical treatment of periodontitis [42], as an adjunct to the healing of mouth ulcers and gingivitis [43], and in papilla regeneration [44]. On the surgical side, the application of hyaluronic acid has been associated with bone regeneration procedures including sinus lift and socket preservation, surgical treatment of periodontal defects [45] and gingival recessions and recently hyaluronic acid has been placement in post-extraction socket [20,21,22,29,30,46,47].
Regarding this, there was no study in the literature that provided to describe the use of hyaluronic acid in the surgical treatment of gingival recessions.
In this research, both RCTs examined RT1 [7] gingival recessions are treated with CAF.
Recessions were treated with either MCAT or LCT combined with sCTG and HA in all case series. Lanzrein [29] treated single RT1 [7] recessions, while Guldener [30] treated multiple adjacent RT1 and RT2 recessions [7].
The reduction of RD in the test group compared to the control group was statistically significant in both RCT studies, respectively Kumar [22] reported p = 0.00, and Pilloni [28] (p = 0.011). In case series analyzed in this review it is not possible to determine whether hyaluronic acid affected root coating. Regardless, RD in Guldener's[30] study were comparable to the results obtained in the study of Sculen [34] and Stähli [48]. In the other hand in Lanzrein’s study [29], RD has a higher value at follow-up than in Górski's study [49]. This could be caused by a different value of RD at baseline, in fact in Lanzrein's study [29] it is higher than reported by Górski [49]. The flap design used in all selected articles unavoidably result in flap displacement [50]. Despite proper passivation, the flap is vulnerable to the tractive force induced by the new flap placement, wound contraction and the activation of neighboring muscles [41,51].
The mechanical and chemical properties of hyaluronic acid could reduce the severity of tensile strains tolerated by the flap and consequently an excellent reduction of RD.
Nevertheless, positive results in the control group should be confirmed by double-blind studies. The use of HA might influence the clinician differentially in performing the surgical treatment.
In addition, the position of the gingival margin at the end of surgery seems to be important in achieving a reduction in RD. Suturing the gingival margin at least 2 mm coronally to the CEJ resulted in complete root coverage [52]. Due to reduce clinical bias, it would be appropriate to specify or quantify the grade of flap passivation before sutures. Anyway, the obtained results of RD reduction are in accordance with the literature in both the two RCTs and the two Case Series [4,33,34].
Mucogingival surgery should be performed in selected patients with very strict inclusion criteria. Absence of bleeding on probing, no trauma and plaque control planning may promote a rapid healing and maintenance of normal PD values at six months follow-up. PD maintenance occurs either in new attachment or wound restoration with healthy junctional epithelium [53]. In fact, the studies analyzed no significant variation was found in PD variable. As reported in the literature, root covering (RC) procedures of RT1 [7] recessions can provide significant reduction in RD and CAL gain without altering PD [54]. Clinical attachment level is a variable directly related to PD and RD.
Modifications of CAL are connected to variations of RD since, as was already indicated, the PD parameter in the included studies remained relatively constant.
The exciting results of CAL in Guldener’s case series [30] could be due to the use of subepithelial connective graft. There is consensus in the literature that the presence of a sCTG provides stability and reduces soft tissue contraction improving clinical outcomes in terms of reduced RD and CAL gain [55].
Among all included studies, Lanzrein[29] reveals lower CRC and MRC than the other included studies. Probably, these results are comparable to those reported in the literature since treatment of multiple recessions resulted in decreased CRC and MRC than treatment of a single recession. Anatomically and technically, multiple recessions are more difficult to treat. Multiple recessions need more challenging and time-consuming surgical treatment of soft tissues, and wound healing is more susceptible to complications due to a large avascular surface area, inadequate blood supply, and/or poor tooth position [56]. In RCTs test groups had improved results than control groups in terms of CRC and MRC. However, the reported percentages are comparable with those in the literature. The success rate treating RT1 [7] defects has been demonstrated to be high, with a mean root coverage of 80.9% (50% to 97.3%) and total root coverage obtained in 46.6% (7.7% to 91.6%) of cases [54,57]. As indicated previously, future RCTs on the use of HA in the surgical treatment of recessions should be performed double-blind, specify and quantify the factors that influence root coverage. Such as the position and tension of the flap [51,58], the dimension of the adjacent papillae [59], and the thickness of the flap [31,60]. The purpose is reduced bias and enable the advantages of HA application really quantifiable. Hyaluronic acid composition and application methods should be studied because they could have an influence on MRC and CRC.
Different physical and chemical conformations of hyaluronic acid are available. In fact, the native molecular design is subject to faster degradation than the cross-linked formulation which involves joining by covalent bonds the HA chains[61].
Two different conformations of hyaluronic acid were applied in the analyzed studies.
Specifically, Pilloni [21], Guldener [30], and Lanzrein [29] used a formulation consisting of 1.6% cross-linked HA and 0.2% linear HA (Hyadent BG, Regedent) while Kumar[22] Linear hyaluronic acid (Gingigel 0.2%). It is possible that some structures and concentrations have an inhibitory effect on cell proliferation and migration during wound healing. In an in vitro study was investigated the relationship between the concentrations of HA solutions and the physicochemical properties and the biocompatibility of blended Cs–Gel–HA membranes. It was noted that only the concentrations of HA in certain range (0.01–0.1%) could enhance the cell adhesion, migration and proliferation, and when the concentration was above 0.1% it would reduce or even inhibit the effect. [62].
In the studies analyzed, the same application method as EMD is used [63,64]. HA is placed on the roots of the elements to be coated without the prior use of ethylenediaminetetraacetic (EDTA), instead used as etching for EMD.
Although both biomolecules are employed with the aim of improving healing [40,65], it does not justify the same method of use. EMD, aided EDTA, is a molecule that promotes the proliferation of cells involved in the regulation of bone remodeling and periodontal ligament regeneration [40].
In the other hand, hyaluronic acid, due to the properties previously described, can reduce healing time and stabilize wound. Consequently, having different mechanisms of action, it should be considered if is better place the HA in direct contact with the root or the cruentate surfaces, because tooth root is not a bioactive surface.
Furthermore, the appropriate time of application would need to be established. During surgical procedures external factors, such as physiological saline washings, could change the effectiveness of HA. The biomolecule could be applied immediately before or even after the suture was performed, with infiltration inside the flap, to ensure permanence in the wound. Future studies will need to investigate what formulation and application technique is best in order to increase the performance of hyaluronic acid.
Follow-up is another important variable. The studies included in the present review presented ranges from 18 weeks to 30 months [21,22,29,30].
Although short-term follow-up was evaluated, an assessment of the evolution of surgical treatment long-term would be appropriate. Pini Prato et. Al observed that in recessions treated only with CAF at 5 years presented apical displacement of the gingival margin. While sites treated with CAF and sCTG at 5 years due to creeping attach presented increased percentage of CRC [66].
Correctly, Pilloni [21] evaluated the pain variable in the short term. Seven days after surgery, postoperative morbidity (pain intensity, discomfort, and edema) was assessed using a visual analog scale (VAS). Pain was described as an acute symptom which, if persistent, is difficult to tolerate and necessitates analgesics. There was no difference in pain intensity between the case group and the control group.
A recent study analyzed the effects of two different doses of topical HA on postoperative discomfort and wound healing at palatal donor sites in patients who had undergone free gingival graft (FGG) surgery. This RCT indicated that topical use of HA decreases postoperative pain and burning sensations while also increasing palatal wound healing in terms of epithelization and color match [67]. However, it would be useful to understand whether hyaluronic acid actually reduces postoperative morbidity.
On the other hand, in the long term, it might be useful to evaluate the root coverage esthetic score (RES). This parameter evaluates five variables for each recession a minimum of six months following surgery, when tissues have achieved the stability and maturity sufficient for esthetic evaluation [68,69,70].
In the case report of Lanzrein[29], RES was examined. The mean RES measured is 7.9.
However, since there is no control group, no objective conclusions can be drawn about the improvement in aesthetic performance when HA is used in surgical procedure.
The number of studies selected, the different types of HA used, and the lack of a well-structured and standardized protocols did not allow objective conclusions to be drawn
5. Conclusions
The limitations of this systematic scoping review doesn’t allow to draw significant conclusions about the application of HA in surgical gingival recession treatment. HA seems to improve the clinical outcomes of this surgical treatment.
The promising clinical results of this molecule in dentistry should be confirmed by more RCT studies in order to develop an efficient and functional protocol. It would be desirable to define the optimal chemical concentration biomolecular structure, timing and application method of HA for more predictable outcomes in mucogingival surgery.
Since the esthetic variable is one of the reasons why patients undergo treatment of recessions future studies may demonstrate whether there is a correlation between the use of hyaluronic acid and improved aesthetic performance in mucogingival surgery. It should be investigated how HA interference the entity of postoperative pain, although pain is a subjective variable. In this regard, the authors of this article refrain from providing guidance on the bases of a mere description of restricted data.
Author Contributions
Mattia Manfredini: Visualization; Federica Eugenia Salina and Marco Tandurella: Formal Analysis; Pier Paolo Poli: Investigation and Methodology; Federica Eugenia Salina and Marco Tandurella: Writing - original draft; Pier Paolo Poli MB: Writing - Review & Editing; Carlo Maiorana: Project Administration and Supervision.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Data Availability Statement
Not applicable
Acknowledgments
Not applicable
Conflicts of Interest
The authors declare no competing interests.
References
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol 2018, 89 Suppl 1, S313–s318. [Google Scholar] [CrossRef]
- Cortellini, P.; Bissada, N.F. Mucogingival conditions in the natural dentition: Narrative review, case definitions, and diagnostic considerations. J Periodontol 2018, 89 Suppl 1, S204–s213. [Google Scholar] [CrossRef]
- Patel, R.R.; Richards, P.S.; Inglehart, M.R. Periodontal health, quality of life, and smiling patterns--an exploration. J Periodontol 2008, 79, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; Mounssif, I. Periodontal plastic surgery. Periodontol 2000 2015, 68, 333–368. [Google Scholar] [CrossRef] [PubMed]
- Meza Mauricio, J.; Furquim, C.P.; Bustillos-Torrez, W.; Soto-Peñaloza, D.; Peñarrocha-Oltra, D.; Retamal-Valdes, B.; Faveri, M. Does enamel matrix derivative application provide additional clinical benefits in the treatment of maxillary Miller class I and II gingival recession? A systematic review and meta-analysis. Clin Oral Investig 2021, 25, 1613–1626. [Google Scholar] [CrossRef] [PubMed]
- Miller, P.D., Jr. A classification of marginal tissue recession. Int J Periodontics Restorative Dent 1985, 5, 8–13. [Google Scholar]
- Cairo, F.; Nieri, M.; Cincinelli, S.; Mervelt, J.; Pagliaro, U. The interproximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: an explorative and reliability study. J Clin Periodontol 2011, 38, 661–666. [Google Scholar] [CrossRef]
- McGuire, M.K.; Scheyer, E.T.; Schupbach, P. A Prospective, Case-Controlled Study Evaluating the Use of Enamel Matrix Derivative on Human Buccal Recession Defects: A Human Histologic Examination. J Periodontol 2016, 87, 645–653. [Google Scholar] [CrossRef]
- McGuire, M.K.; Cochran, D.L. Evaluation of human recession defects treated with coronally advanced flaps and either enamel matrix derivative or connective tissue. Part 2: Histological evaluation. J Periodontol 2003, 74, 1126–1135. [Google Scholar] [CrossRef]
- França-Grohmann, I.L.; Sangiorgio, J.P.M.; Bueno, M.R.; Casarin, R.C.V.; Silvério Ruiz, K.G.; Nociti, F.H., Jr.; Casati, M.Z.; Sallum, E.A. Treatment of dehiscence-type defects with collagen matrix and/or enamel matrix derivative: Histomorphometric study in minipigs. J Periodontol 2020, 91, 967–974. [Google Scholar] [CrossRef]
- Chambrone, L.; Pini Prato, G.P. Clinical insights about the evolution of root coverage procedures: The flap, the graft, and the surgery. J Periodontol 2019, 90, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, E.L.; Roberts, J.L.; Moseley, R.; Griffiths, P.C.; Thomas, D.W. Evaluation of the physical and biological properties of hyaluronan and hyaluronan fragments. Int J Pharm 2011, 420, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Meyer, K.; Palmer, J.W. THE POLYSACCHARIDE OF THE VITREOUS HUMOR. The Journal of biological chemistry 1934, 107, 629–634. [Google Scholar] [CrossRef]
- Fraser, J.R.; Laurent, T.C.; Laurent, U.B. Hyaluronan: its nature, distribution, functions and turnover. J Intern Med 1997, 242, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Laurent, T.C.; Fraser, J.R. Hyaluronan. Faseb j 1992, 6, 2397–2404. [Google Scholar] [CrossRef]
- Pirnazar, P.; Wolinsky, L.; Nachnani, S.; Haake, S.; Pilloni, A.; Bernard, G.W. Bacteriostatic effects of hyaluronic acid. J Periodontol 1999, 70, 370–374. [Google Scholar] [CrossRef]
- Fallacara, A.; Baldini, E.; Manfredini, S.; Vertuani, S. Hyaluronic Acid in the Third Millennium. Polymers (Basel) 2018, 10. [Google Scholar] [CrossRef]
- Dahiya, P.; Kamal, R. Hyaluronic Acid: a boon in periodontal therapy. N Am J Med Sci 2013, 5, 309–315. [Google Scholar] [CrossRef]
- Prato, G.P.; Rotundo, R.; Magnani, C.; Soranzo, C.; Muzzi, L.; Cairo, F. An autologous cell hyaluronic acid graft technique for gingival augmentation: a case series. J Periodontol 2003, 74, 262–267. [Google Scholar] [CrossRef]
- Casale, M.; Moffa, A.; Vella, P.; Sabatino, L.; Capuano, F.; Salvinelli, B.; Lopez, M.A.; Carinci, F.; Salvinelli, F. Hyaluronic acid: Perspectives in dentistry. A systematic review. Int J Immunopathol Pharmacol 2016, 29, 572–582. [Google Scholar] [CrossRef]
- Pilloni, A.; Schmidlin, P.R.; Sahrmann, P.; Sculean, A.; Rojas, M.A. Effectiveness of adjunctive hyaluronic acid application in coronally advanced flap in Miller class I single gingival recession sites: a randomized controlled clinical trial. Clinical oral investigations 2019, 23, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Srinivas, M.; Pai, J.; Suragimath, G.; Prasad, K.; Polepalle, T. Efficacy of hyaluronic acid (hyaluronan) in root coverage procedures as an adjunct to coronally advanced flap in Millers Class I recession: A clinical study. J Indian Soc Periodontol 2014, 18, 746–750. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O'Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Stern, C.; Aromataris, E.; Lockwood, C.; Jordan, Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med Res Methodol 2018, 18, 5. [Google Scholar] [CrossRef] [PubMed]
- Bateson, M. Systematic Reviews to Support Evidence-Based Medicine: How to Review and Apply Findings of Healthcare Research. Postgraduate Medical Journal 2004, 80, 123. [Google Scholar]
- Al-Ardah, A.J.; AlHelal, A.; Proussaefs, P.; AlBader, B.; Al Humaidan, A.A.; Lozada, J. Managing Titanium Mesh Exposure With Partial Removal of the Exposed Site: A Case Series Study. J Oral Implantol 2017, 43, 482–490. [Google Scholar] [CrossRef]
- Nandanwar, J.; Bhongade, M.; Puri, S.; Dhadse, P.; Datir, M.; Kasatwar, A. Comparison of effectiveness of hyaluronic acid in combination with polylactic acid/polyglycolic acid membrane and subepithelial connective tissue graft for the treatment of multiple gingival recession defects in human: A clinical study. Journal of Datta Meghe Institute of Medical Sciences University 2018, 13, 48–53. [Google Scholar] [CrossRef]
- Pilloni, A.; Schmidlin, P.R.; Sahrmann, P.; Sculean, A.; Rojas, M.A. Effectiveness of adjunctive hyaluronic acid application in coronally advanced flap in Miller class I single gingival recession sites: a randomized controlled clinical trial. Clin Oral Investig 2019, 23, 1133–1141. [Google Scholar] [CrossRef]
- Lanzrein, C.; Guldener, K.; Imber, J.C.; Katsaros, C.; Stähli, A.; Sculean, A. Treatment of multiple adjacent recessions with the modified coronally advanced tunnel or laterally closed tunnel in conjunction with cross-linked hyaluronic acid and subepithelial connective tissue graft: a report of 15 cases. Quintessence Int 2020, 51, 710–719. [Google Scholar] [CrossRef]
- Guldener, K.; Lanzrein, C.; Eliezer, M.; Katsaros, C.; Stähli, A.; Sculean, A. Treatment of single mandibular recessions with the modified coronally advanced tunnel or laterally closed tunnel, hyaluronic acid, and subepithelial connective tissue graft: a report of 12 cases. Quintessence International 2020, 51, 456–463. [Google Scholar] [CrossRef]
- Baldi, C.; Pini-Prato, G.; Pagliaro, U.; Nieri, M.; Saletta, D.; Muzzi, L.; Cortellini, P. Coronally advanced flap procedure for root coverage. Is flap thickness a relevant predictor to achieve root coverage? A 19-case series. J Periodontol 1999, 70, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; Stefanini, M.; Ganz, S.; Mazzotti, C.; Mounssif, I.; Marzadori, M. Coronally Advanced Flap with Different Designs in the Treatment of Gingival Recession: A Comparative Controlled Randomized Clinical Trial. Int J Periodontics Restorative Dent 2016, 36, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Cosgarea, R.; Stähli, A.; Katsaros, C.; Arweiler, N.B.; Brecx, M.; Deppe, H. The modified coronally advanced tunnel combined with an enamel matrix derivative and subepithelial connective tissue graft for the treatment of isolated mandibular Miller Class I and II gingival recessions: a report of 16 cases. Quintessence Int 2014, 45, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Allen, E.P. The Laterally Closed Tunnel for the Treatment of Deep Isolated Mandibular Recessions: Surgical Technique and a Report of 24 Cases. Int J Periodontics Restorative Dent 2018, 38, 479–487. [Google Scholar] [CrossRef] [PubMed]
- West, D.C.; Hampson, I.N.; Arnold, F.; Kumar, S. Angiogenesis induced by degradation products of hyaluronic acid. Science 1985, 228, 1324–1326. [Google Scholar] [CrossRef] [PubMed]
- Scully, M.F.; Kakkar, V.V.; Goodwin, C.A.; O'Regan, M. Inhibition of fibrinolytic activity by hyaluronan and its alcohol ester derivatives. Thromb Res 1995, 78, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Trombelli, L.; Simonelli, A.; Pramstraller, M.; Guarnelli, M.E.; Fabbri, C.; Maietti, E.; Farina, R. Clinical efficacy of a chlorhexidine-based mouthrinse containing hyaluronic acid and an antidiscoloration system in patients undergoing flap surgery: A triple-blind, parallel-arm, randomized controlled trial. Int J Dent Hyg 2018, 16, 541–552. [Google Scholar] [CrossRef]
- Vänttinen, E.; Viljanto, J. Tensile strength of new connective tissue formed in pretreated viscose cellulose implants. Ann Med Exp Biol Fenn 1965, 43, 257–259. [Google Scholar]
- Pilloni, A.; Bernard, G.W. The effect of hyaluronan on mouse intramembranous osteogenesis in vitro. Cell Tissue Res 1998, 294, 323–333. [Google Scholar] [CrossRef]
- Pilloni, A.; Rimondini, L.; De Luca, M.; Bernard, G.W. Effect of hyaluronan on calcification-nodule formation from human periodontal ligament cell culture. J Appl Biomater Biomech 2003, 1, 84–90. [Google Scholar]
- Wikesjö, U.M.; Selvig, K.A. Periodontal wound healing and regeneration. Periodontol 2000 1999, 19, 21–39. [Google Scholar] [CrossRef] [PubMed]
- Johannsen, A.; Tellefsen, M.; Wikesjö, U.; Johannsen, G. Local delivery of hyaluronan as an adjunct to scaling and root planing in the treatment of chronic periodontitis. J Periodontol 2009, 80, 1493–1497. [Google Scholar] [CrossRef] [PubMed]
- Jentsch, H.; Pomowski, R.; Kundt, G.; Göcke, R. Treatment of gingivitis with hyaluronan. J Clin Periodontol 2003, 30, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Ficho, A.C.; de Souza Faloni, A.P.; Pennisi, P.R.C.; Borges, L.G.F.; de Macedo Bernadino, Í.; Paranhos, L.R.; Queiroz, T.P.; Santos, P.L. Is interdental papilla filling using hyaluronic acid a stable approach to treat black triangles? A systematic review. J Esthet Restor Dent 2021, 33, 458–465. [Google Scholar] [CrossRef]
- Ballini, A.; Cantore, S.; Capodiferro, S.; Grassi, F.R. Esterified hyaluronic acid and autologous bone in the surgical correction of the infra-bone defects. Int J Med Sci 2009, 6, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Kediege, S.D.; Gupta, A.; Jain, K. Evaluation of gengigel® application in the management of furcation with coronally advanced flap through surgical re-entry-a split mouth clinical study. Journal of Clinical and Diagnostic Research 2017, 11, ZC27–ZC32. [Google Scholar] [CrossRef] [PubMed]
- Ibraheem, W.; Jedaiba, W.H.; Alnami, A.M.; Hussain Baiti, L.A.; Ali Manqari, S.M.; Bhati, A.; Almarghlani, A.; Assaggaf, M. Efficacy of hyaluronic acid gel and spray in healing of extraction wound: a randomized controlled study. Eur Rev Med Pharmacol Sci 2022, 26, 3444–3449. [Google Scholar] [CrossRef] [PubMed]
- Stähli, A.; Duong, H.Y.; Imber, J.C.; Roccuzzo, A.; Salvi, G.E.; Katsaros, C.; Ramseier, C.A.; Sculean, A. Recession coverage using the modified coronally advanced tunnel and connective tissue graft with or without enamel matrix derivative: 5-year results of a randomised clinical trial. Clin Oral Investig 2022, 1–9. [Google Scholar] [CrossRef]
- Górski, B.; Szerszeń, M.; Kaczyński, T. Effect of 24% EDTA root conditioning on the outcome of modified coronally advanced tunnel technique with subepithelial connective tissue graft for the treatment of multiple gingival recessions: a randomized clinical trial. Clin Oral Investig 2022, 26, 1761–1772. [Google Scholar] [CrossRef]
- Rasperini, G.; Acunzo, R.; Limiroli, E. Decision Making in Gingival Recession Treatment: Scientific Evidence and Clinical Experience. Clin Adv Periodontics 2011, 1, 41–52. [Google Scholar] [CrossRef]
- Pini Prato, G.; Pagliaro, U.; Baldi, C.; Nieri, M.; Saletta, D.; Cairo, F.; Cortellini, P. Coronally advanced flap procedure for root coverage. Flap with tension versus flap without tension: a randomized controlled clinical study. J Periodontol 2000, 71, 188–201. [Google Scholar] [CrossRef] [PubMed]
- Pini-Prato, G.; Baldi, C.; Pagliaro, U.; Nieri, M.; Saletta, D.; Rotundo, R.; Cortellini, P. Coronally advanced flap procedure for root coverage. Treatment of root surface: root planning versus polishing. J Periodontol 1999, 70, 1064–1076. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Lindhe, J. Clinical Periodontology and Implant Dentistry, 2 Volume Set; Wiley: 2015.
- Chambrone, L.; Tatakis, D.N. Periodontal soft tissue root coverage procedures: a systematic review from the AAP Regeneration Workshop. J Periodontol 2015, 86, S8–51. [Google Scholar] [CrossRef]
- Cairo, F.; Nieri, M.; Pagliaro, U. Efficacy of periodontal plastic surgery procedures in the treatment of localized facial gingival recessions. A systematic review. J Clin Periodontol 2014, 41 Suppl 15, S44–62. [Google Scholar] [CrossRef]
- Chambrone, L.; Lima, L.A.; Pustiglioni, F.E.; Chambrone, L.A. Systematic review of periodontal plastic surgery in the treatment of multiple recession-type defects. J Can Dent Assoc 2009, 75, 203a–203f. [Google Scholar] [PubMed]
- Chambrone, L.; Sukekava, F.; Araújo, M.G.; Pustiglioni, F.E.; Chambrone, L.A.; Lima, L.A. Root-coverage procedures for the treatment of localized recession-type defects: a Cochrane systematic review. J Periodontol 2010, 81, 452–478. [Google Scholar] [CrossRef] [PubMed]
- Pini Prato, G.P.; Baldi, C.; Nieri, M.; Franseschi, D.; Cortellini, P.; Clauser, C.; Rotundo, R.; Muzzi, L. Coronally advanced flap: the post-surgical position of the gingival margin is an important factor for achieving complete root coverage. J Periodontol 2005, 76, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Saletta, D.; Pini Prato, G.; Pagliaro, U.; Baldi, C.; Mauri, M.; Nieri, M. Coronally advanced flap procedure: is the interdental papilla a prognostic factor for root coverage? J Periodontol 2001, 72, 760–766. [Google Scholar] [CrossRef]
- Hwang, D.; Wang, H.L. Flap thickness as a predictor of root coverage: a systematic review. J Periodontol 2006, 77, 1625–1634. [Google Scholar] [CrossRef]
- Al-Khateeb, R.; Olszewska-Czyz, I. Biological molecules in dental applications: hyaluronic acid as a companion biomaterial for diverse dental applications. Heliyon 2020, 6, e03722. [Google Scholar] [CrossRef]
- Liu, H.; Yin, Y.; Yao, K.; Ma, D.; Cui, L.; Cao, Y. Influence of the concentrations of hyaluronic acid on the properties and biocompatibility of Cs-Gel-HA membranes. Biomaterials 2004, 25, 3523–3530. [Google Scholar] [CrossRef] [PubMed]
- Castellanos, A.; de la Rosa, M.; de la Garza, M.; Caffesse, R.G. Enamel matrix derivative and coronal flaps to cover marginal tissue recessions. J Periodontol 2006, 77, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Dias, A.T.; de Menezes, C.C.; Kahn, S.; Fischer, R.G.; da Silva Figueredo, C.M.; Fernandes, G.V.d.O. Gingival recession treatment with enamel matrix derivative associated with coronally advanced flap and subepithelial connective tissue graft: a split-mouth randomized controlled clinical trial with molecular evaluation. Clinical Oral Investigations 2022, 26, 1453–1463. [Google Scholar] [CrossRef] [PubMed]
- Miron, R.J.; Caluseru, O.M.; Guillemette, V.; Zhang, Y.; Gemperli, A.C.; Chandad, F.; Sculean, A. Influence of enamel matrix derivative on cells at different maturation stages of differentiation. PLoS One 2013, 8, e71008. [Google Scholar] [CrossRef] [PubMed]
- Pini-Prato, G.P.; Cairo, F.; Nieri, M.; Franceschi, D.; Rotundo, R.; Cortellini, P. Coronally advanced flap versus connective tissue graft in the treatment of multiple gingival recessions: a split-mouth study with a 5-year follow-up. J Clin Periodontol 2010, 37, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, S.; Özener, H.; Doğan, B.; Kuru, B. Effect of topically applied hyaluronic acid on pain and palatal epithelial wound healing: An examiner-masked, randomized, controlled clinical trial. J Periodontol 2018, 89, 36–45. [Google Scholar] [CrossRef]
- Cairo, F.; Rotundo, R.; Miller, P.D.; Pini Prato, G.P. Root coverage esthetic score: a system to evaluate the esthetic outcome of the treatment of gingival recession through evaluation of clinical cases. J Periodontol 2009, 80, 705–710. [Google Scholar] [CrossRef]
- Rotundo, R.; Nieri, M.; Mori, M.; Clauser, C.; Prato, G.P. Aesthetic perception after root coverage procedure. J Clin Periodontol 2008, 35, 705–712. [Google Scholar] [CrossRef]
- Roccuzzo, M.; Bunino, M.; Needleman, I.; Sanz, M. Periodontal plastic surgery for treatment of localized gingival recessions: a systematic review. J Clin Periodontol 2002, 29 Suppl 3, 178-194; discussion 195-176. 3. [CrossRef]
Figure 1.
Selection strategy.
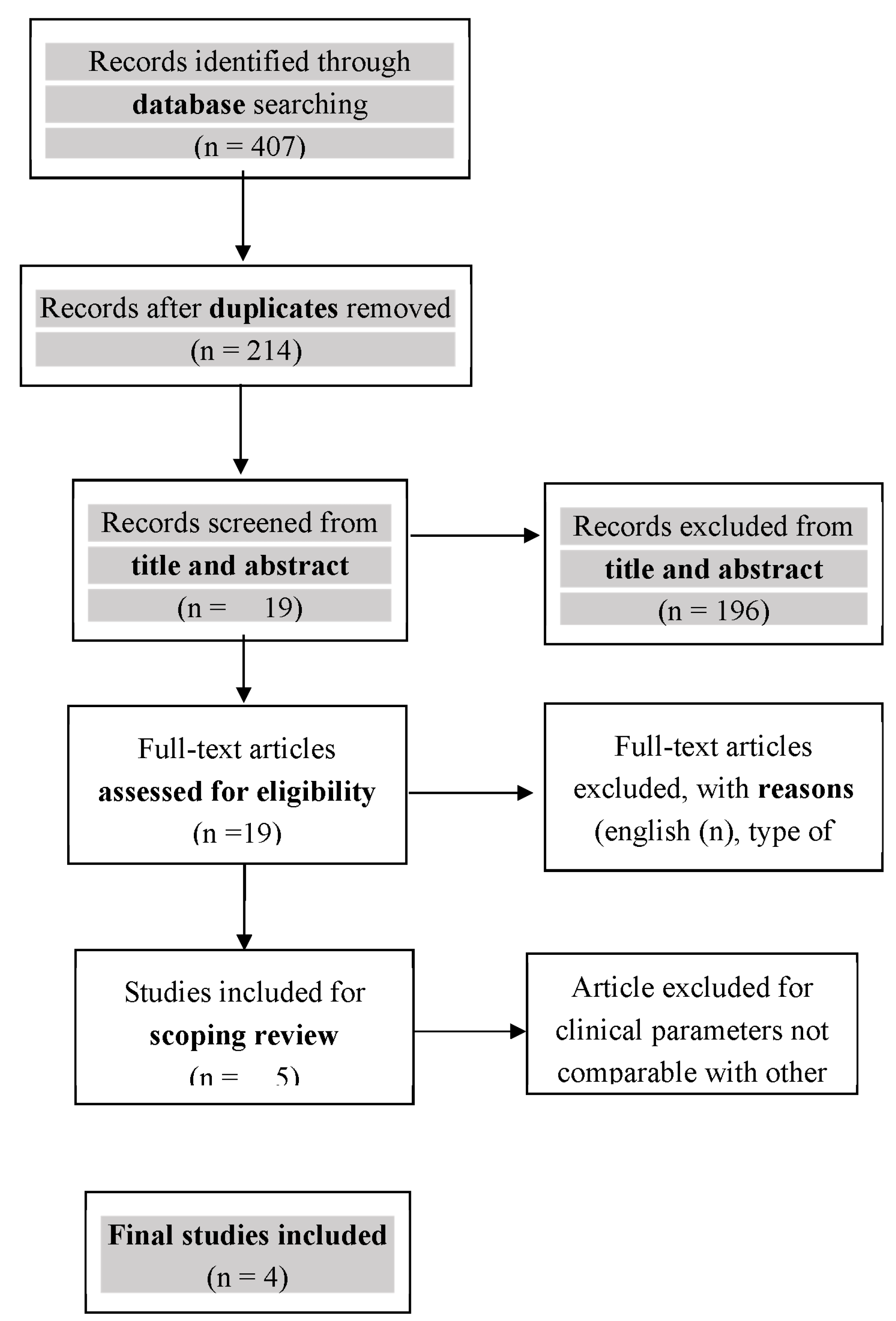

Table 1.
Summary of results.
| Article | Design | Recession type | Single/multiple | HA | Surgical technique | Test | Control | Outcome | Follow up |
|---|---|---|---|---|---|---|---|---|---|
| 2014 Kumar |
RCT split (7M – 3F) 10 20 rec |
RT1 | Single | Hyaluronic acid (Gengigel 0.2% gel which is 0.2% hyaluronan gel marketed by Ricerfarma pharmaceuticals, Milan, Italy) | CAF | CAF+HA GEL (10) |
CAF (1 0) |
RD, PD, CAL | 1, 3, 6, 12, 24 Weeks |
| 2017 Pilloni |
RCT (M – F) 30 |
RT1 | Single | 1,6% cross-linked HA, 0.2% linear HA (Hyadent BG, Regedent) | CAF | CAF+HA (15) | CAF (15) | RD, PD, CAL, KT, CRC, MRC, VAS | 18 mounths |
| 2020 Guldener | CASE SERIES 12 |
RT1 | Single | 1,6% cross-linked HA, 0.2% linear HA (Hyadent BG, Regedent) | MCAT+sCTG +HA LCT+sCTG +HA |
- | - | RD, PD, CAL, KT, CRC, MRC | range 6 to 30 months |
| 2020 Lanzrein | CASE SERIES 15 |
RT1 and RT2 | Multiple | 1,6% cross-linked HA, 0.2% linear HA (Hyadent BG, Regedent) | MCAT+sCTG+HA LCT+sCTG+HA |
- | - | RD, PD, CAL, KT, CRC, MRC, RES | range 6 to 33 months |
RT Recession Type. HA hyaluronic acid. CAF coronally advanced flap. sCTG,subepithelial connective tissue graft. MCAT Modified Coronally Advanced Tunnel. LCT Laterally Closed Tunnel. RD Recession Depth. PD Probing Depth. CAL Clinical Attachment Level. MRC Mean Root Coverage. CRC Complete Root Coverage. KT Keratinized Tissue. RES Root Coverage Esthetic Score. VAS Visual Analog Scale.
Table 2.
Summary of results.
| FU | RD | PD | CAL | MRC | CRC | ||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow up | Baseline | Follow up | Baseline | Follow up | Follow up | Follow up | ||
| Kumar 2014 | 24 weeks | Test: 3.20 mm | Test: 1.10 mm | Test: 1.80 mm | Test: 1.70 mm | Test: 5 mm | Test: 2.80 mm | Test: 68,3% | Test: 40% |
| Control: 2.90 mm | Control: 1.00 mm | Control: 2.00 mm | Control: 2.00 mm | Control: 4.90 mm | Control: 3.00 mm | Control:61,6% | Control: 20% | ||
|
Pilloni 2017 |
18 months |
Test: 3.0[1.0] mm | Test: 0.0[0.0] mm | Test: 1.0[0.0] mm | Test: 1.0[1.0] mm | Test:4.0[1.0] mm | Test: 1.0[0.0] mm | Test: 93,8% | Test: 80% |
| Control:3.0[1.0] mm | Control:1.0[1.0] mm | Control:1.0[0.0] mm | Control:2.0[1.0] mm | Control:4.0[1.0] mm | Control:2.0[0.0] mm | Control: 73,1% | Control: 30% | ||
|
Guldener 2020 |
6±33 months | 4.6[0.9]mm | 0.5[0.6] mm | 1.8[0.9]mm | 1.3[0.5] | 6.4 mm | 1.8[0.5] | 96.09%. | 50% |
|
Lanzrein 2020 |
6±30 months | 3.3[0.8]mm | 0.8[1.0] mm | 1.3[0.5]mm | 1.5[0.5] mm | 4.6 mm | 2.3 mm | 85.1% | 20% |
FU Last Follow Up. RD Recession depth. PD probing depth. CAL Clinical Attachment Level. MRC mean root coverage. CRC complete root coverage.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



