
Submitted:
29 May 2023
Posted:
30 May 2023
You are already at the latest version
Abstract
: Glaucoma is the most common cause of blindness, which significantly reduces quality of life. Most glaucoma cases are primary glaucoma; nevertheless, many patients suffer from glaucoma caused by drugs, such as corticosteroids. A comprehensive review of the risks associated with corticosteroid-induced glaucoma is limited. Therefore, we used the Japanese Adverse Drug Event Reporting Database (JADER) published by the Pharmaceuticals and Medical Devices Agency (PMDA) to analyze the risk factors associated with glaucoma and the trends and characteristics of corticosteroid-induced glaucoma. We did not find sex or age differences associated with the onset of glaucoma. Hierarchical clustering and principal component analysis revealed that triamcinolone acetonide and betamethasone sodium phosphate, which are used around the eyes in Japan, are more likely to induce intraocular pressure (IOP) elevation compared with other corticosteroids. Increased IOP is a direct cause of glaucoma. Based on these findings, it may be necessary to limit or avoid the use of these corticosteroids.
Keywords:
glaucoma
; corticosteroids
; intraocular pressure
; Japanese Adverse Drug Event Report
; spontaneous reporting system
; volcano plot
; hierarchical clustering
; principal component analysis
1. Introduction
In Japan, the most common cause of visually impairment among people over 60 years old is glaucoma (28.6%) [1], which glaucoma has increased in recent years. Visual impairment significantly decreases patient quality of life. There are a wide variety of glaucoma types, but secondary glaucoma caused by diseases (including systemic diseases) and drugs has been reported along with primary glaucoma. According to the Tajimi Study, the prevalence of confirmed total glaucoma cases over the age of 40 is 5.0% (95%CI, 4.2–5.8), whereas secondary glaucoma, which is a rare type, accounts for 0.3% (95%CI, 0.13–0.51) of the confirmed cases [2,3].
Drug-induced glaucoma is primarily caused by corticosteroids. Adrenergic agonists, cholinergics, and anticholinergics can induce glaucoma; however, it is rare and the underlying mechanism is different from that of corticosteroids [4]. The use of corticosteroids induces IOP elevation, which increases the risk of developing glaucoma. People with elevated IOP caused by corticosteroid use are known as corticosteroid responders. There are individual differences in IOP elevation. In the normal population, approximately 61%–63% are nonresponders to corticosteroids, exhibiting IOP elevations <5 mmHg, 33% exhibit a moderate increase in IOP (6–15 mmHg), and 4%–6% are high responders to corticosteroids (IOP elevation >15 mmHg). Furthermore, children under the age of 10 show marked IOP elevation caused by corticosteroids [5].
Several clinical trials have demonstrated that corticosteroids induce glaucoma; however, a comprehensive analysis of glaucoma-inducing tendencies by corticosteroid type has not been conducted. Therefore, using the Japanese Adverse Drug Event Report database (JADER), a database of spontaneous reports of suspected side effects published by the Pharmaceuticals and Medical Devices Agency (PMDA), we analyzed the risk of glaucoma caused by corticosteroids and its characteristics.
2. Results
2.1. Preparing Data Tables for Analysis
Figure 1 shows a flowchart for creating a data table for analysis. The data were generated from a DRUG table (6,097,229 records), a REAC table (1,280,060 tables), and a DEMO table (872,822 records) from JADER. We removed cured glaucoma patients, eliminated three duplicate tables, and combined them, resulting in 5,601,557 records in a final data table. The data table for analysis included 3,611 and 259,428 records for glaucoma and corticosteroid-related cases, respectively.
Duplicate data in the DRUG, REAC, and DEMO tables were deleted. Three tables were combined using identification numbers. Patients taking glaucoma medications were removed from the analysis.
2.2. Relevance of Glaucoma to Patient Characteristics
Table 1 shows the characteristics of patients with glaucoma. In the glaucoma patient group, we did not detect any association with sex or age.
2.3. Relationship Between Glaucoma and Drugs
Figure 2 shows the association of glaucoma with drug use. Drugs plotted in the upper right tend to induce glaucoma. The labeled drugs are corticosteroids.
The X-axis shows the natural logarithm of the reported odds ratio (lnROR). The Y-axis shows the reciprocal of the common logarithm for the p-value of the Fisher’s exact test [-log(p-value)]. RORs were calculated using a crosstabulation table. The dotted line on the Y-axis represents a p-value of 0.05. The color of the plot represents the number of reported adverse events. The common logarithm of the total number of reported times is shown in red to blue.
2.4. Hierarchical Clustering of Glaucoma-Inducing Corticosteroids
Figure 3 shows the dendrogram generated by hierarchical clustering resulting in two clusters.
Table 2 shows the number of corticosteroid reports used for hierarchical clustering.
The dendrogram shows the relationship between 14 corticosteroids and 5 glaucoma-related side effects. The color map shows the correlation between the variables.
2.5. Principal Component Analysis of Glaucoma-Induced Corticosteroids
Figure 4 shows the results of principal component analysis. The contribution of the principal components was 84.1% for principal component 1 and 9.82% for principal component 2. We created a scattergram using principal components 1 and 2. We then visualized the relationship between glaucoma-related adverse events and each principal component representing each adverse event as a loading vector. The X-axis represents principal component 1, which was positively correlated with the ROR. The Y-axis represents principal component 2, ocular hypertension (0.48487) and intraocular pressure increased (0.20892) exhibited a positive correlation. Normal tension glaucoma (−0.38005), angle-closure glaucoma (−0.25989), and glaucoma (−0.01468) showed a negative correlation.
Principal component score plot (a) showing the relationship between corticosteroids and each principal component. Each plot represents a corticosteroid. The color of each plot represents classification by hierarchical clustering. Principal component loading plot (b) shows the relationship between glaucoma-related adverse events and each principal component. Each loading vector represents an adverse event.
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
3. Discussion
3.1. Glaucoma and Characteristics of the Patient
In this study, we observed no significant differences in glaucoma based on sex. Malclès et al. found that men have a 2.24-fold increased risk of IOP elevation with corticosteroid administration compared with women (Multivariate Analysis, 95%CI: 1.38–3.63, p-value <0.001) [6]. On the other hand, the Rotterdam study showed that the earlier the age of menopause (i.e., the shorter the duration of exposure to female hormones), the higher the risk of open-angle glaucoma [7]. The results of the two previous studies differ from those obtained in the present study. Both previous studies are epidemiological studies of primary glaucoma. Because JADER is a large database of adverse drug reaction reports, registered glaucoma is an adverse event resulting from drug treatment. In other words, unlike primary glaucoma, drug-induced glaucoma may not show significant sex differences.
The present study also revealed that there was no difference between the two groups at either age 70 and over or age 40 and over. Choi et al. reported that the rate of IOP elevation after an intravitreal injection of dexamethasone, a type of corticosteroid, was 42.9% for those aged 30 years or younger, 35.3% for those aged 31–40 years, 28.3% for those aged 41–50 years, 14.9% for those aged 51–60 years, 12.2% for those aged 61–70 years, 8.4% for those aged 71–80 years, and 9.1% for those aged 81–90 years. The incidence of IOP elevation was reported to increase with younger age [8]. In addition, age below 30 years is a risk factor for IOP elevation, according to Parekh et al [9]. In contrast, Garbe et al. showed that the administration of oral corticosteroids to elderly patients was associated with a 1.41-fold (95%CI, 1.22–1.63) increased risk of IOP elevation or open-angle glaucoma compared with the untreated group [10]. Thus, different results have been reported in previous studies. We believe that the reason for this discrepancy is the insufficient number of subjects enrolled in these clinical studies; however, the large database analysis used in this study did not show statistically significant differences in age despite the extremely large number of subjects.
3.2. Glaucoma and Corticosteroids
Corticosteroids are well-known drugs that cause glaucoma [11]. Therefore, the analysis in the present study focused on corticosteroids. Of the 47 corticosteroids in clinical use as prescription drugs in Japan (excluding combination drugs and discontinued products, only those reported to JADER) [12], 28 were plotted on the upper right in the volcano plot [-log(p-value) >1.3 and lnROR >0]. Thus, it was estimated that these corticosteroids tended to induce glaucoma significantly (Figure 2). Corticosteroids, which are associated with a low number of glaucoma reports, are a confounding factor and do not provide the differences in characteristics between corticosteroids that we would expect to observe and that tend to induce glaucoma.
Corticosteroid-induced glaucoma has symptoms similar to primary open-angle glaucoma [13]. Although open-angle glaucoma is the most common type of glaucoma among the Japanese population, only 42 cases of open-angle glaucoma were reported in JADER. The Lowest Level Term of the Preferred Term "Glaucoma” includes “corticosteroid glaucoma,” “steroid-induced glaucoma,” “secondary glaucoma,” etc. In other words, corticosteroid-induced glaucoma is not reported by type, but is registered collectively as the Preferred Term “glaucoma.” Therefore, contrary to the expectation that open-angle glaucoma would be the most frequently reported type of corticosteroid-induced glaucoma, we presumed that there were fewer reports of open-angle glaucoma.
Hierarchical clustering, which groups similar data, divided corticosteroids into three clusters based on Preferred Terms related to glaucoma (Figure 3). The cluster (red) that exhibited a strong correlation with all five glaucoma-related Preferred Terms included three corticosteroids (diflucortolone valerate, fluorometholone, and triamcinolone acetonide). The cluster showing a relatively weak correlation (green) included seven corticosteroids (clobetasol propionate, hydrocortisone acetate, fluticasone propionate, betamethasone sodium phosphate, difluprednate, betamethasone, methylprednisolone). Four corticosteroids (dexamethasone, dexamethasone sodium phosphate, prednisolone, and methylprednisolone sodium succinate) that showed a weak correlation (blue) all had more than 10,000 records (Table 2). Based on these results, a principal component analysis was performed to further clarify the characteristics of each corticosteroid.
Principal component analysis may be used to summarize and visualize the bias of explanatory variables [14]. Color coding based on the three clusters obtained in the hierarchical cluster analysis indicated a correlation with principal component 1. Furthermore, principal component 1 was strongly correlated with lnROR, indicating that it is readily induced for glaucoma (Figure 4. In contrast, principal component 2 in Figure 4(b), which shows the principal component loadings, was plotted in the positive direction for ocular hypertension and intraocular pressure increased, and in the negative direction for glaucoma, angle-closure glaucoma, and normal tension glaucoma. Both ocular hypertension and intraocular pressure increased are Preferred Terms, indicating a condition of IOP elevation. Glaucoma may be caused by IOP elevation [15], but not all glaucoma cases are necessarily associated with IOP elevation [16]. Therefore, principal component 2 may indicate a simple induction of IOP elevation. Figure 4(a) shows the score plot. This indicates corticosteroids with high values for principal component 1, which indicates easy induction, and positive values for principal component 2, which indicates IOP elevation associated with triamcinolone acetonide and betamethasone sodium phosphate. These two corticosteroids were presumed to readily induce IOP elevation. Triamcinolone acetonide is the only corticosteroid administered intravitreously in Japan for vitreous visualization during vitrectomy and for the reduction of macular edema, such as diabetic macular edema. The intravitreal injection of triamcinolone acetonide readily induces IOP elevation. Roth et al. found that in eyes injected with intravitreous triamcinolone acetonide (929 eyes in 841 patients), the incidence of IOP elevation above 21 mmHg two years after injection was 44.6% (95% CI, 41%–50%) [17]. Betamethasone sodium phosphate is used in Japan as an eye, ear, and nose drop. Topical administration of corticosteroids, such as eye drops, is associated with a higher risk of glaucoma compared with systemic administration [18]. The results of the present study support this clinical finding. Corticosteroids with high values for principal component 1 and negative values for principal component 2 included clobetasol propionate, diflucortolone valerate, difluprednate, hydrocortisone acetate, fluorometholone, and fluticasone propionate. These corticosteroids are associated with a smaller tendency to induce IOP elevation compared with other corticosteroids. Fluorometholone is an eye drop, fluticasone propionate is a nasal drop, and the others are transdermal drugs, such as ointments and creams. Transdermal drugs, even in the periocular area, have a low risk of causing glaucoma when administered over short periods [19], which is consistent with the present findings. We found that corticosteroids may have different rates of side effects depending on the method of administration. This may lead to the development of new methods, such as changing the route of administration to avoid glaucoma and IOP elevation in patients requiring treatment with corticosteroids.
3.3. Limitations
There are several limitations to this study. First, we there are limitations with respect to the database used. Because this database contains information on adverse reactions based on spontaneous reports, cases are limited to those that are recognized as adverse reactions. Specifically, mild side effects may occur occasionally, whereas severe side effects may be frequent. This is known as reporting bias, a characteristic of self-reporting databases [20]. In this study, the total number of patients who used corticosteroids could not be ascertained, so an accurate assessment of the adverse events was not possible. Therefore, we tried to increase the usefulness of the analysis by setting a filter for the number of reports and avoiding easy p-value and ROR comparisons. Second, some JADER data were incomplete and may contain blank cells, such as missing values or incorrectly entered letters or numbers. When missing values for sex and age were found, they were removed and addressed. Third, when multiple drugs are administered, it is difficult to identify the specific cause of adverse events. Although fatal adverse events registered in JADER are confirmed by PMDA, other adverse events are based on the reporter's judgment and may include not only actual adverse events, but also questionable adverse events. Nonetheless, JADER is the largest database of voluntary reports for adverse drug reactions in Japan. Adverse drug reaction information obtained from JADER is expected to reflect pharmacological and pharmacokinetic properties and prescribing and usage conditions. Therefore, JADER is an excellent tool for understanding adverse drug reactions and may be used across several research areas.
4. Materials and Methods
4.1. Database(JADER)
JADER is an adverse drug reaction database published by PMDA that summarizes suspected adverse drug reactions reported by manufacturers, distributors, or medical institutions. The data used in the present study was downloaded from the PMDA website [21], ranging from April 1, 2004 to June 30, 2022. Since this study used anonymized data from the open-access database, it was exempt from the requirements for ethical approval and informed consent by the Ethics Committee of Meiji Pharmaceutical University.
4.2. Drugs to Be Analyzed and Adverse Event Terms
The drugs analyzed were corticosteroids, which are currently used clinically in Japan. Combination drugs were excluded from the analysis [12]. Glaucoma was defined by MedDRA/J version 25.0 [22]. Of the 47 narrow scope terms of Standardized MedDRA Queries (Table 3), the Preferred Terms (20) excluding congenital, traumatic, postoperative, and surgical terms were analyzed (Table 4).
4.3. Creation of a Data Table for Analysis
The analysis was performed using the DRUG, REAC, and DEMO tables of JADER. Three operations were performed using these tables. First, when ";" was included in the route, date, dose, dosage unit, and several divided doses in DRUG, the lines were stacked for each";.” Second, when “;” was included in the reporter information in the DEMO, the lines were stacked for each “;.” Third, if the drug name was a combination drug, the rows were stacked by the “・” in the name. The completed tables were used for analysis. Duplicate data were deleted in each of the three tables and joined by identification number. Patients taking glaucoma medications were removed from the data tables.
4.4. Glaucoma and Characteristics of the Patients
The Tajimi Study represents an epidemiological study of glaucoma conducted among people aged 40 years or older living in Tajimi City, Gifu Prefecture, Japan. The results indicated that 5.0% (95%CI, 4.2–5.8) of those aged 40 years or older had glaucoma [2,3]. Therefore, an analysis was conducted in two separate segments: age 40, which is generally considered to have a sharply increased risk of glaucoma, and age 65 and older, defined as elderly by the World Health Organization (in the 70s fore age-specific reporting in JADER). Age was grouped by age group. Elderly people in their 70s, 80s, and 90s and elderly people were defined as “age 70 and older.” In addition, individuals in their 40s, 50s, 60s, 70s, 80s, 90s, and the elderly were defined as “age 40 and older.” Adults and unknown subjects were not included in the analysis. They were further divided into two groups according to the presence or absence of glaucoma, and a p-value was calculated using a bivariate relationship to examine the presence of a significant difference. The p-value was calculated using Fisher’s exact test. The analysis was performed only on data that did not contain missing values.
4.5. Glaucoma and Corticosteroids
The association between 47 corticosteroids and glaucoma was analyzed. The risk of glaucoma on corticosteroids was assessed using the ROR and Fisher’s exact test. First, a crosstabulation table (Table 5) was created, in which cells with 0 cannot be calculated. If the cell value is small, the estimation becomes unstable. Therefore, 0.5 was added to all cells as a correction (the Haldane correction) [23]. Drugs with an ROR of 1 or higher and a p-value of less than 0.05 in Fisher's exact test were considered glaucoma-inducing corticosteroids [24]. Next, to visualize adverse events, a scatterplot containing ROR and p-values was created. This scatterplot used ROR as the natural logarithm (lnROR) and the p-value obtained from Fisher's exact test as the common logarithm of the reciprocal. Scatterplots corresponding to volcano plots and are often used to visualize gene expression trends [25,26].
A crosstabulation table consisting of reports with the suspected medicine, all other reports, reports of glaucoma, and reports of nonglaucoma.
4.6. Hierarchical Clustering
Of the 47 corticosteroids (Table 3), only 14 reported in 100 or more cases and 10 or more reported glaucoma cases were included. In addition, only five Preferred Terms for glaucoma were included in 50 or more reported Preferred Terms. We calculated the ROR from the crosstabulation table, converted the resulting ROR to the natural logarithm, and performed hierarchical clustering to objectively classify them. The Ward method based on Euclidean distance with loads from five Preferred Terms was used [27].
4.7. Principal Component Analysis
Similar to hierarchical clustering, only 14 corticosteroids reported in 100 or more cases and 10 or more reported glaucoma cases were included and only 5 Preferred Terms with 50 or more reports were included. The ROR was calculated from the crosstabulation table (Figure 3.) and it was converted to a natural logarithm. Principal component analysis was performed using the covariance matrix and focused on principal components 1 and 2.
4.8. Statistical Analysis
Statistical analysis was performed using JMP Pro16 software (SAS Institute Inc., Cary, NC, USA). The level of statistical significance was set at 0.05.
5. Conclusions
Analysis of JADER data revealed a trend in corticosteroids that cause glaucoma, a rare side effect. All corticosteroids for which effective values were obtained in JADER were shown to induce glaucoma. Furthermore, different types of corticosteroids exhibited different inducing IOP elevations, which can cause glaucoma. Triamcinolone acetonide and betamethasone phosphate sodium had a high tendency to cause IOP elevation. We anticipate that the results of this study will contribute to improved risk management for drug-induced glaucoma patients.
Author Contributions
Conceptualization, Y.U.; Methodology, Y.U.; Software, Y.U.; Validation, A.K. and Y.U.; Formal Analysis, A.K. and Y.U.; Investigation, A.K. and Y.U.; Resources, A.K. and Y.U.; Data Curation, A.K. and Y.U.; Writing – Original Draft Preparation, A.K.; Writing – Review & Editing, A.K. and Y.U.; Visualization, A.K. and Y.U.; Supervision, Y.U.; Project Administration, Y.U.; Funding Acquisition, Y.U. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is contained within the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Morizane, Y; Morimoto, N; Fujiwara, A; Kawasaki, R; Yamashita, H; Ogura, Y; Shiraga, F. Incidence and causes of visual impairment in Japan: the first nation-wide complete enumeration survey of newly certified visually impaired individuals. Jpn J Ophthalmol 2019, 63, 26–33. [Google Scholar] [CrossRef]
- Iwase, A; Suzuki, Y; Araie, M; Yamamoto, T; Abe, H; Shirato, S; Kuwayama, Y; Mishima, HK; Shimizu, H; Tomita, G; et al. The prevalence of primary open-angle glaucoma in Japanese: the Tajimi Study. Ophthalmology 2004, 111, 1641–1648. [Google Scholar] [CrossRef]
- Yamamoto, T; Iwase, A; Araie, M; Suzuki, Y; Abe, H; Shirato, S; Kuwayama, Y; Mishima, HK; Shimizu, H; Tomita, G; et al. The Tajimi Study Group, Japan Glaucoma Society. The Tajimi Study report 2: prevalence of primary angle closure and secondary glaucoma in a Japanese population. Ophthalmology 2005, 112, 1661–1669. [Google Scholar] [CrossRef]
- Tripathi, RC; Tripathi, BJ; Haggerty, C. Drug-induced glaucomas: mechanism and management. Drug Saf 2003, 26, 749–767. [Google Scholar] [CrossRef]
- Razeghinejad, MR; Katz, LJ. Steroid-induced iatrogenic glaucoma. Ophthal Res 2012, 47, 66–80. [Google Scholar] [CrossRef]
- Malclès, A; Dot, C; Voirin, N; Vié, AL; Agard, É; Bellocq, D; Denis, P; Kodjikian, L Safety of intravitreal dexamethasone implant (OZURDEX): the SAFODEX study. Incidence and risk factors of ocular hypertension. Retina 2017, 37, 1352–1359. [Google Scholar] [CrossRef]
- Hulsman, CA; Westendorp, IC; Ramrattan, RS; Wolfs, RC; Witteman, JC; Vingerling, JR; Hofman, A; de Jong, PT. Is open-angle glaucoma associated with early menopause? The Rotterdam study. Am J Epidemiol 2001, 154, 138–144. [Google Scholar] [CrossRef]
- Choi, W; Park, SE; Kang, HG; Byeon, SH; Kim, SS; Koh, HJ; Lee, S; Seong, GJ; Kim, CY; Kim, M. Intraocular pressure change after injection of intravitreal dexamethasone (Ozurdex) implant in Korean patients. Br J Ophthalmol 2019, 103, 1380–1387. [Google Scholar] [CrossRef]
- Parekh, A; Srivastava, S; Bena, J; Albini, T; Nguyen, QD; Goldstein, DA. Risk factors associated with intraocular pressure increase in patients with uveitis treated with the fluocinolone acetonide implant. JAMA Ophthalmol 2015, 133, 568–573. [Google Scholar] [CrossRef]
- Garbe, E; LeLorier, J; Boivin, JF; Suissa, S. Risk of ocular hypertension or open-angle glaucoma in elderly patients on oral glucocorticoids. Lancet 1997, 350, 979–982. [Google Scholar] [CrossRef]
- Kersey, JP; Broadway, DC. Corticosteroid-induced glaucoma: a review of the literature. Eye (Lond) 2006, 20, 407–416. [Google Scholar] [CrossRef]
- Today’s Drug Therapy in 2022, 44th ed. ; Kazuyuki, S; Shinichi, K, Koji, I, Yasushi, I., Eds.; Nankodo: Tokyo, Japan, 2022; ISBN 978-4-524-23211-6. [Google Scholar]
- Clark, AF; Wilson, K; de Kater, AW; Allingham, RR; McCartney, MD. Dexamethasone-induced ocular hypertension in perfusion-cultured human eyes. Invest Ophthalmol Vis Sci 1995, 36, 478–489. [Google Scholar]
- Jolliffe, IT. Principal Component Analysis, 2nd ed.; Springer: New York, NY, USA, 2002; ISBN 978-0-387-95442-4. [Google Scholar]
- Weinreb, RN; Khaw, PT. Primary open-angle glaucoma. Lancet 2004, 363, 1711–1720. [Google Scholar] [CrossRef]
- Wiggs, JL; Pasquale, LR. Genetics of glaucoma. Hum Mol Genet 2017, 26, R21–R27. [Google Scholar] [CrossRef]
- Roth, DB; Verma, V; Realini, T; Prenner, JL; Feuer, WJ; Fechtner, RD. Long-term incidence and timing of intraocular hypertension after intravitreal triamcinolone acetonide injection. Ophthalmology 2009, 116, 455–460. [Google Scholar] [CrossRef]
- Sihota, R; Konkal, VL; Dada, T; Agarwal, HC; Singh, R. Prospective, long-term evaluation of steroid-induced glaucoma. Eye (Lond) 2008, 22, 26–30. [Google Scholar] [CrossRef]
- Roberti, G; Oddone, F; Agnifili, L; Katsanos, A; Michelessi, M; Mastropasqua, L; Quaranta, L; Riva, I; Tanga, L; Manni, G. Steroid-induced glaucoma: epidemiology, pathophysiology, and clinical management. Surv Ophthalmol 2020, 65, 458–472. [Google Scholar] [CrossRef]
- Maeda, R. JADER from pharmacovigilance point of view. Jpn J Pharmacoepidemiol 2014, 19, 51–56. [Google Scholar]
- Pharmaceutical and Medical Devices Agency. Available online: https://www.pmda.go.jp/safety/info-services/drugs/adr-info/suspected-adr/0005.html (accessed on 12 April 2023).
- MedDRA Japanese Maintenance Organization. Available online: https://www.jmo.pmrj.jp/ (accessed on 12 April 2023).
- Greenland, S; Schwartzbaum, JA; Finkle WD. Problems due to small samples and sparse data in conditional logistic regression analysis. Am J Epidemiol 2000, 151, 531–539. [Google Scholar]
- Van Puijenbroek, EP; Bate, A; Leufkens, HGM; Lindquist, M; Orre, R; Egberts, AC. A Comparison of measures of disproportionality for signal detection in spontaneous reporting systems for adverse drug reactions. Pharmacoepidemiol. Drug. Saf. 2002, 11, 3–10. [Google Scholar]
- Chen, JJ; Wang, SJ; Tsai, CA; Lin, CJ. Selection of differentially expressed genes in microarray data analysis. Pharmacogenomics J. 2007, 7, 212–220. [Google Scholar]
- Okunaka, M; Kano, D; Matsui, R; Kawasaki, T; Uesawa, Y. Comprehensive analysis of chemotherapeutic agents that induce infectious neutropenia. Pharmaceuticals 2021, 14, 681. [Google Scholar] [CrossRef]
- Everitt, BS; Landau, S; Leese, M; Stahl, D. Cluster Analysis, 5th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2011; ISBN 978-0-470-74991-3. [Google Scholar]
Figure 1.
Flowchart for the construction of the data analysis tables.
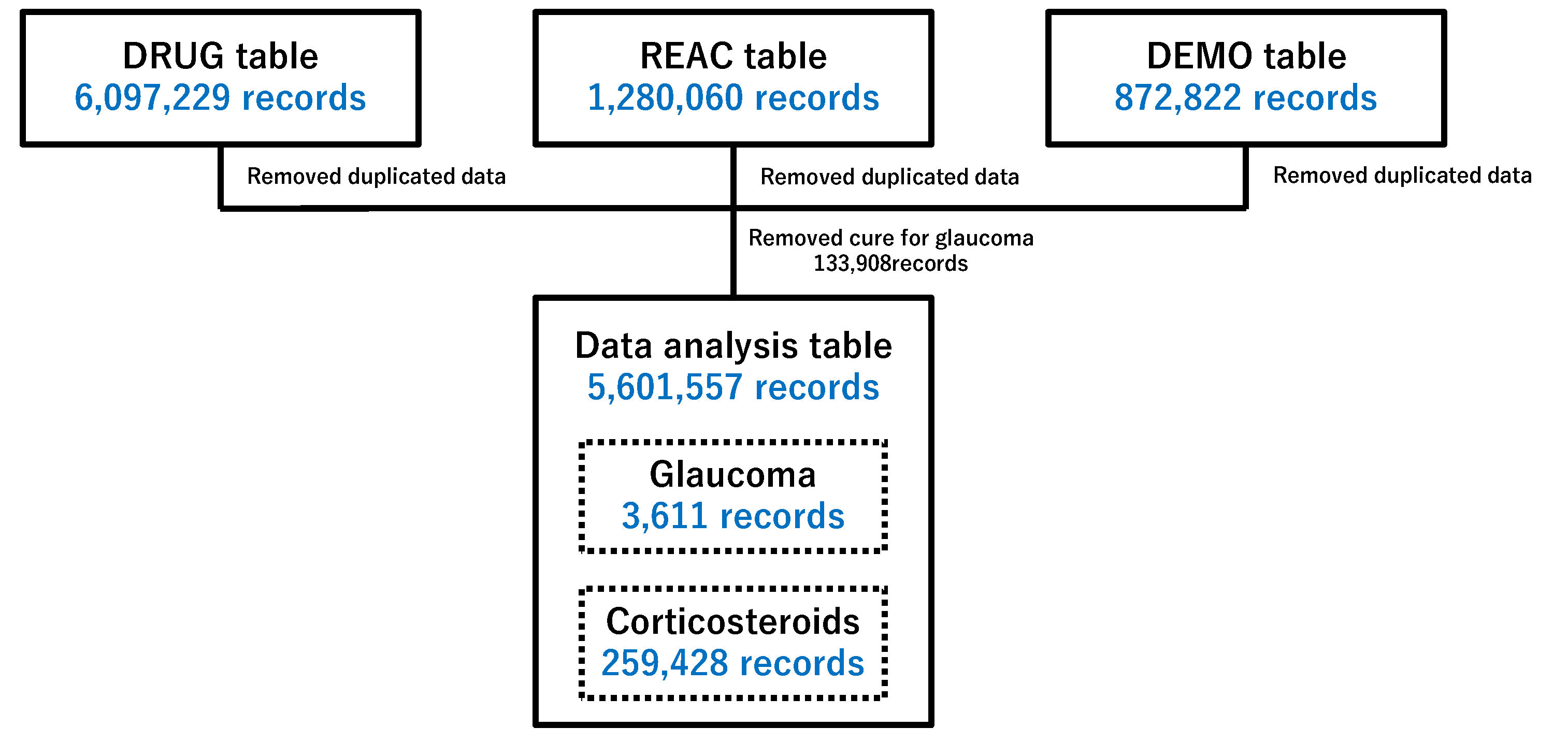
Figure 2.
Drugs associated with glaucoma.
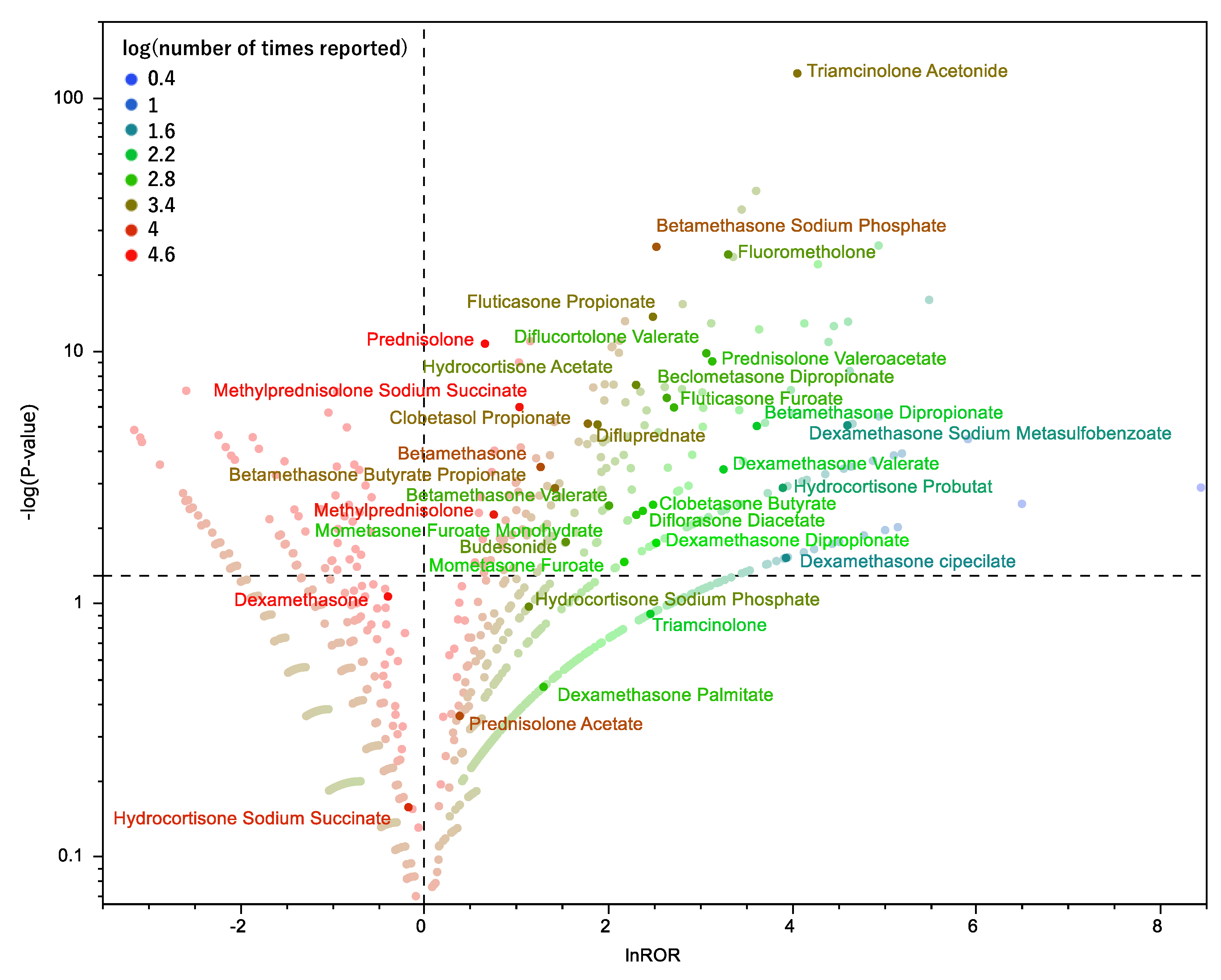
Figure 3.
Classification of corticosteroids associated with glaucoma using hierarchical clustering.
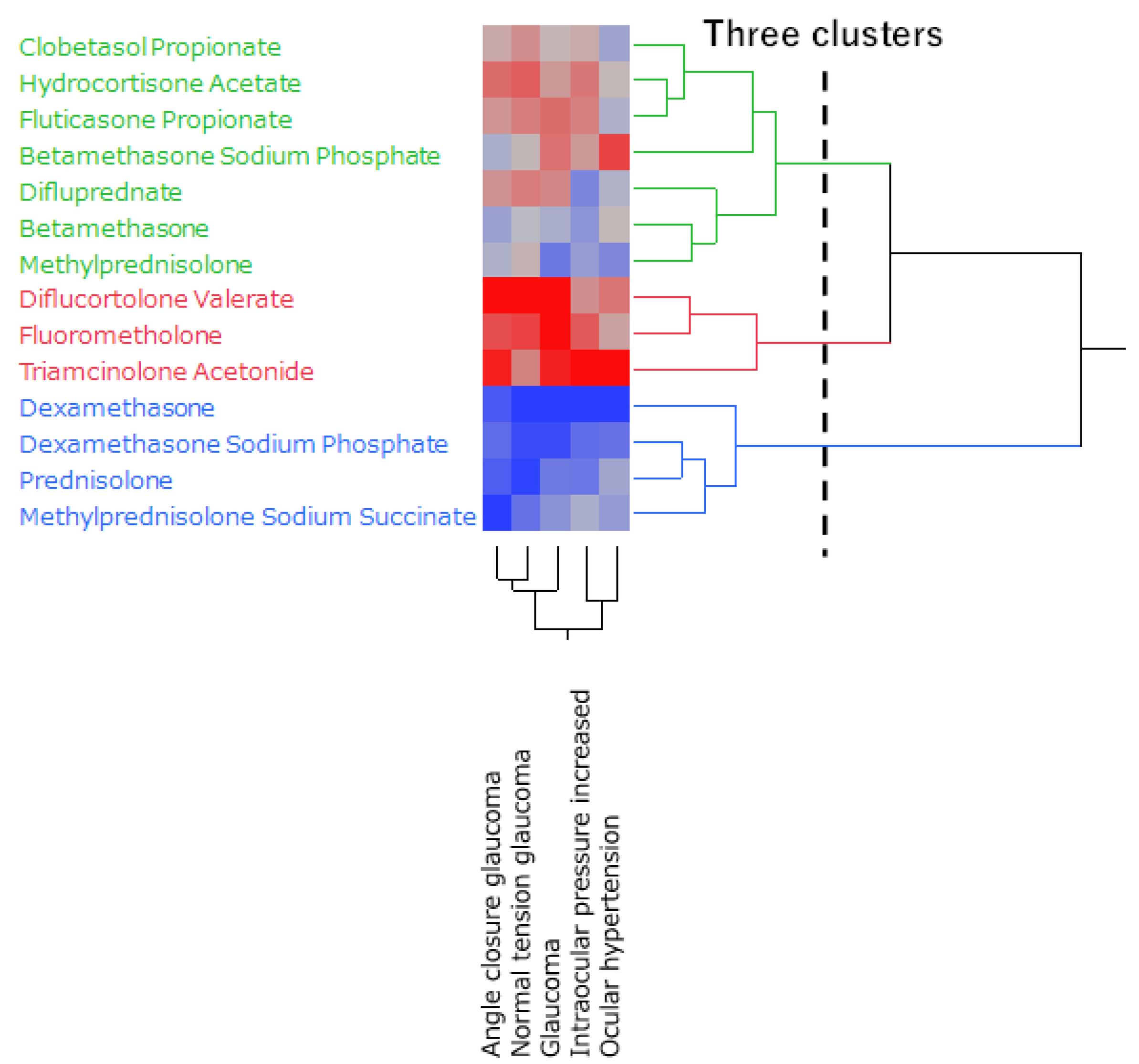
Figure 4.
Association between glaucoma and corticosteroids using principal component analysis.
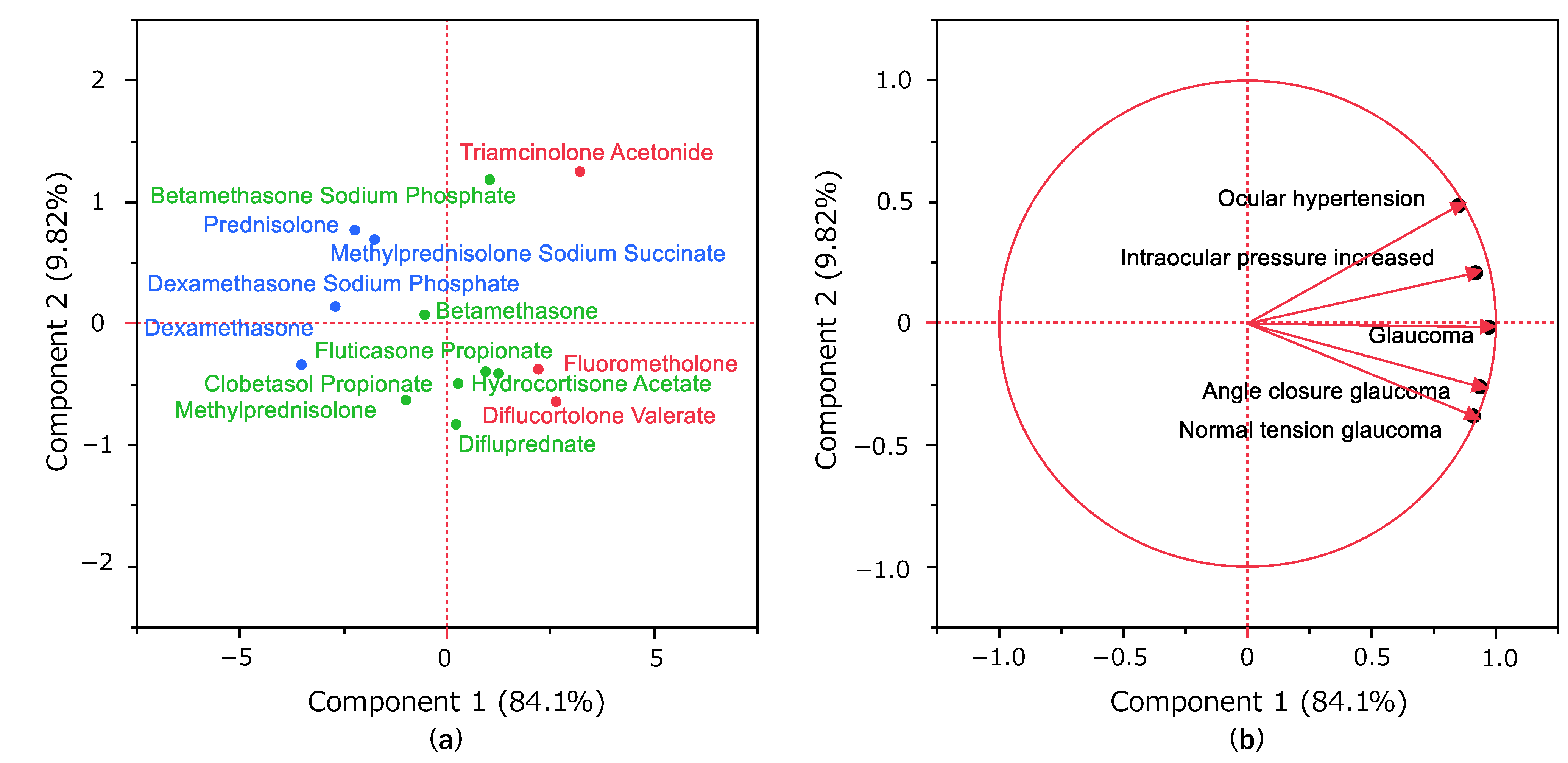

Table 1.
Characteristics of glaucoma and nonglaucoma patients.
| Patients | Glaucoma (1,405) | Nonglaucoma (1,288,906) | p-Value (Fisher's exact test) |
|
|---|---|---|---|---|
| Sex | Male | 653/1,347 | 599,030/1,209,010 | 0.445 |
| Female | 694/1,347 | 609,980/1,209,010 | ||
| Age | ≧70 years old | 436/1,145 | 468,717/1,170,976 | 0.184 |
| <70 years old | 709/1,145 | 702,259/1,170,976 | ||
| ≧40 years old | 949/1,145 | 960,658/1,170,976 | 0.488 | |
| <40 years old | 196/1,145 | 210,318/1,170,976 |
Table 2.
The number of times reported corticosteroids used for hierarchical clustering.
| Corticosteroids | Number of Times Reported |
|---|---|
| Clobetasol propionate | 3023 |
| Diflucortolone Valerate | 768 |
| Difluprednate | 2485 |
| Dexamethasone | 37816 |
| Dexamethasone Sodium Phosphate | 30523 |
| Triamcinolone Acetonide | 2693 |
| Hydrocortisone Butyrate | 1794 |
| Fluorometholone | 1366 |
| Fluticasone Propionate | 2543 |
| prednisolone | 107943 |
| betamethasone | 5483 |
| Betamethasone Sodium Phosphate | 4604 |
| Methylprednisolone Sodium Succinate | 17429 |
Table 3.
Analysis of 47 corticosteroids.
| Corticosteroids | |
|---|---|
| Alclometasone Dipropionate | Amcinonide |
| Beclometasone Dipropionate | Betamethasone |
| Betamethasone Butyrate Propionate | Betamethasone Dipropionate |
| Betamethasone Sodium Phosphate | Betamethasone Valerate |
| Budesonide | Ciclesonide |
| Clobetasol Propionate | Clobetasone Butyrate |
| Cortisone Acetate | Deprodone Propionate |
| Dexamethasone | Dexamethasone cipecilate |
| Dexamethasone Dipropionate | Dexamethasone Palmitate |
| Dexamethasone Sodium Metasulfobenzoate | Dexamethasone Sodium Phosphate |
| Dexamethasone Valerate | Diflorasone Diacetate |
| Diflucortolone Valerate | Difluprednate |
| Fludrocortisone Acetate | Fludroxycortide |
| Fluocinolone Acetonide | Fluocinonide |
| Fluorometholone | Fluticasone Furoate |
| Fluticasone Propionate | Hydrocortisone Acetate |
| Hydrocortisone Probutat | Hydrocortisone Sodium Phosphate |
| Hydrocortisone Sodium Succinate | Methylprednisolone |
| Methylprednisolone Acetate | Methylprednisolone Sodium Succinate |
| Mometasone Furoate | Mometasone Furoate Monohydrate |
| Prednisolone | Prednisolone Acetate |
| Prednisolone Sodium Phosphate | Prednisolone Sodium Succinate |
| Prednisolone Valeroacetate | Triamcinolone |
| Triamcinolone Acetonide | |
Table 4.
Analysis of 20 Preferred Terms (MedDRA/J version 25.0).
| Preferred Terms | Number of reports |
|---|---|
| Acute myopia | 0 |
| Angle-closure glaucoma | 507 |
| Aphakic glaucoma | 0 |
| Borderline glaucoma | 0 |
| Diabetic glaucoma | 0 |
| Exfoliation glaucoma | 1 |
| Fundoscopy abnormal | 21 |
| Glaucoma | 1790 |
| Glaucoma drug therapy | 0 |
| Glaucomatocyclitic crises | 16 |
| Glaucomatous optic disc atrophy | 1 |
| Gonioscopy abnormal | 0 |
| Halo vision | 0 |
| Intraocular pressure fluctuation | 2 |
| Intraocular pressure increased | 838 |
| Intraocular pressure test abnormal | 1 |
| Loss of visual contrast sensitivity | 1 |
| Malignant glaucoma | 4 |
| Normal tension glaucoma | 52 |
| Ocular hypertension | 272 |
| Open-angle glaucoma | 41 |
| Optic discs blurred | 1 |
| The optical nerve cup/disc ratio increased | 0 |
| Optic nerve cupping | 40 |
| Phacolytic glaucoma | 0 |
| Pigmentary glaucoma | 0 |
| Pseudophakic glaucoma | 0 |
| Pupillary light reflex tests abnormal | 7 |
| Slit-lamp tests abnormal | 0 |
| Uveitic glaucoma | 1 |
| Uveitis-glaucoma-hyphaema syndrome | 0 |
| The visualVisual field tests abnormal | 15 |
Table 5.
A crosstabulation table and ROR formulas.
| Glaucoma | Nonglaucoma | |
|---|---|---|
| Reports with the suspected medicine | a | b |
| All other reports | c | d |
ROR (Reporting Odds Ratio) = (a/b)/(c/d) = ad/bc.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



