
Submitted:
30 May 2023
Posted:
30 May 2023
You are already at the latest version
Abstract
Ultrasonography is a relevant diagnostic tool extensively used andrology of human and do-mestic animals, including dogs. The present review aimed to describe all the technologies based on ultrasound, starting with the basic B-Mode ultrasonography to the recent contrast-enhanced ultrasonography (CEUS) and the ultrasound elastography, available to assess the testicle of the dog. The principles of the different technologies and the relevant findings in normal and ab-normal testicular conditions were described and discussed. B-mode ultrasonography aims at the examination of the testis detecting focal lesions but lacks objectivization. Other technologies, such as Doppler ultrasonography, B-Flow, and CEUS allow the definition of vascular patterns, that could be measured with specific applications, such as spectral Doppler or quantitative CEUS. Finally, ultrasound elastography allows the estimation of parenchyma stiffness, in both qualitatively and quantitatively manner. Ultrasound-based technologies assist the andrology in the evaluation of the testicular function and integrity, offering valuable information to define pathological conditions that could have an impact on the health and life quality of the male dog.
Keywords:
Dog
; Testis
; Ultrasonography
; B-flow
; Doppler
; CEUS
; Sonoelastography
1. Introduction
Ultrasonographic evaluation of the reproductive tract is an important component of the andrological examination of dogs.
Ultrasonography is considered the gold standard for acute and non-acute scrotal disorders [1] because it is safe and minimally-invasive, easy- and ready-to-use, rapid to perform and interpret, and less expensive compared with other technologies (i.e., magnetic resonance, computerized tomography) [2].
Alongside conventional techniques, such as B-mode ultrasonography and Doppler-based ultrasonography, in recent years new technologies, such as contrast-enhanced ultrasonography (CEUS) and ultrasound elastography (UEl) were implemented in andrological evaluation, increasing the chances of an effective and fast diagnosis [3].
The present review aimed to describe both conventional and new ultrasound-based techniques applicable to the testis evaluation of the dog, reporting information regarding the technology, the procedure and the findings in normal testis and testicular disease.
2. Testes component evaluation by ultrasonography
2.1. Anatomy, physiology and vascularization of the testis
The two testes are the primary reproductive organs of the male [4]. They are located in the inguinal region, within the scrotum, and are oriented obliquely, with the long axis moving dorsal-caudally. The extra-abdominal position of the testes makes these organs easily accessible for ultrasonography evaluation, as well as the epididymis and the distal part of the spermatic cord [5].
The epididymis is adherent to the testis, with its head located at the testicular cranial pole, the body runs dorsal-lateral and the tail is anchored at the dorsal-caudal extremity of the testis by the short and thick proper ligament. The tail of the epididymis is in continuity with the ductus deferens, which forms the spermatic cord with the vascular compartment, moving within the inguinal canal and entering into the abdomen via the vaginal ring [5].
The testis is composed of stroma, the connective tissue framework, and the parenchyma composed of the seminiferous tubules. The stroma is made by the external tunica albuginea, from which branch septa compartmentalizing the parenchyma in lobuli [5]. The septa merge centrally in mediastinum testis a cord of connective tissue running lengthwise through the middle of the testis [5].
The large majority of the blood supply to the testis is provided by the testicular artery, while the artery of the ductus deferens serves epididymis and the deferent duct [5]. The testicular vein forms an extensive pampiniform plexus in the spermatic cord, surrounding the testicular artery, lymphatics, and nerves [5]. The testicular vessels are unusually long and tortuos, and this feature is functional to create a low temperature [6], via thermic dispersion and exchange, and low oxygen-tension environment [7], due to the low intratesticular capillary pressure, both beneficial for spermatogenesis [8].
3. Gray-scale ultrasonography
3.1. Technology and applications
Gray-scale ultrasonography was the first technique applied in the evaluation of the testis, in the early 1990s. Several authors confirmed that it is a useful tool which helps the clinician to acquire information about the health of the reproductive tract, becoming an integral component of the breeding soundness evaluation (BSE) of the dog [9,10,11,12,13] by providing fine anatomical details of the testicle and surrounding structures [14]. This reveals lesions too small or inaccessible for detection via palpation [15], albeit the ultrasonographic changes are not specific enough to identify the different types of testicular lesions [16]. Moreover, serial ultrasonographic evaluations can be very helpful in evaluating the progression of disease and response to therapy [17].
The gray-scale ultrasonography is a subjective procedure allowing qualitative evaluation of the testicular parenchyma. To overcome this limit, some authors proposed the objective estimation of the echotexture based on the pixel-intensity analysis [18]. The image display is composed of an array of picture elements (pixels), with each pixel representing a determined tissue density that is displayed in a range of shades of gray (ranging from white to black) [18]. Using the quantification of the pixel intensity in sonograms, several studies investigated the relationship between ultrasonographic appearance and semen quality in mammals [18,19,20,21,22,23] such as in human [24,25,26,27], revealing that changes in ultrasound parameters could be correlated to the percentage of morphologically normal live spermatozoa.
3.2. Examination technique
As a result of the short distance between the probe and testis, high-frequency and linear transducers should be used whenever possible, typically 7.5- to 10-MHz. The low-frequency transducers may not provide sufficient resolution to detect small lesions or subtle parenchymal changes [17].
The testicular examination is a straightforward procedure. The images can be obtained in the non-sedated dog in lateral recumbency or standing position. Clipping of the scrotal hair should be avoided: good images could be obtained by the use of copious amounts of ultrasound gel [28]. The testes should be scanned in transverse, longitudinal, and dorsal planes. A standoff pad often enhances the examination, allowing better near-field structural visualization. Alternatively, one testis may be used as a standoff to image the opposite one [17]. Both testes can often be imaged in one transverse or dorsal section, and it is helpful for direct comparison [17].
3.3. Normal findings
The canine testis is echogenic with a homogeneous, medium echo texture. The parietal and visceral tunics form a thin hyperechoic peripheral echo. The mediastinum testis is seen as an echogenic central linear structure on the midsagittal plane and as a central focal echo on a mid-transverse scan plane (Figure 1) [17].
In prepubertal dogs, the echogenicity of the testes is more hypoechoic compared with adult dogs, and the mediastinum testis can be easily identified [30]. Usually, no differences in echogenicity between the right and left testis are observed [23,30].
The tail of the epididymis is generally isoechoic compared to the testicular parenchyma (Figure 2). The tail also has a coarser echo texture than the testis. The head and body of the epididymis are nearly isoechoic with the testis. The head is cranially located, and from it, the body can be followed caudally in both sagittal and transverse planes to the tail, which is reported to be the most consistently imaged portion of the canine epididymis [17].
The testicular volume is positively correlated with total sperm count, sperm motility, sperm morphology and daily sperm production in the dog [31,32]. The estimation of testicular volume could be useful to demonstrate asymmetry or reduction since some authors reported that the testicular volume is age-related, with the maximal size reached at 6 years, followed by a progressive decrease [33]. Ultrasonography is generally considered the most accurate method for quantitative testicular volume determination [17]. Few studies have evaluated ultrasound mensuration of dog testicles, establishing its reliability in comparison with the results taken by caliper (orchidometer). Among the most common formulae used for calculating testicular volume, the formula of Lambert (volume = length x width x height x 0.71) estimates the testicular volume more accurately [31,32].
3.4. Abnormal findings
3.4.1. Intratesticular diseases
Testicular neoplasms are the most common tumours of the genital tract of male dogs [28,34,35,36,37,38,39] with a prevalence of up to 60% and an incidence that increases with age [16,40,41,42,43] and cryptorchidism [37,38,39,40,44,45,46].
The ultrasonographic features of testicular tumours are extremely variable [16]. Testicular tumours can range from circumscribed small nodules (focal tumours) to large complex masses (diffuse tumours) with heterogeneous echo-pattern and disruption of normal anatomy. Sertoli cell tumours and seminomas are usually large with mixed echogenicity, resulting sometimes in generalized testicular enlargement, while interstitial cell tumours may appear as well-defined focal hypoechoic lesions [28], but shape, margin and echogenicity do not allow differentiation between tumour types [16].
Areas of haemorrhage and necrosis may occur in all tumour types and may be seen ultrasonographically as disorganized hyperechoic and hypoechoic regions, as areas of calcification within the testicular parenchyma could be seen, appearing as hyperechoic foci producing acoustic shadowing [28].
Although testicular tumours showed a lesser ability to metastasize (<15%), early detection by ultrasonography allows the orchiectomy of the affected testis and improves the chance to maintain the fertility of the patient, especially in breeding dogs [16].
There are few reports in which dogs had been diagnosed with neoplasms of testicular origin in an extra-testicular location [47]. Few possibilities, including the presence of embryological ectopic tissue or the presence of testicular tissue transplanted during castration, are considered causal [47]. The location of the extra-testicular testicular tumours in dogs is varied and includes the spermatic cord, the inside of the scrotal skin or the site of the pre-scrotal castration incision site [47]. Most of the neoplasms were small and about 1.5 cm in diameter [35]. Their appearance, apart from their location, is undistinguishable from their intratesticular counterpart [35].
Orchitis, as the inflammation of the testis, could run acutely or chronically. Acute orchitis may have variable ultrasonographic characteristics, ranging from irregular and poorly defined anechoic areas to a diffuse patchy hypoechoic echo pattern, and focal abscessation may be evident [15,17,30]. Usually, there is an enlargement of the testis and epididymis, and fluid may accumulate between the visceral and parietal tunic within the scrotum [15,17,30,48]. Chronic orchitis is less obvious regarding ultrasonography features and may reveal hyperechoic or mixed echogenic parenchyma, with a reduction in testicular size [17]. Abscess can also occur as a chronic progression of the orchitis, and its feature is characterized by an irregular hyperechoic wall and anechoic to hypoechoic central contents [17].
Torsion of the spermatic cord is uncommon in dogs [17]. Depending on the degree of the torsion, due to the peculiar structure of testis vascularization, the consequence is the necrosis of the testis. It could be seen mainly in retained (or cryptorchid) testes [35]. Moreover, torsion of the spermatic cord in the intra-abdominal testicle was frequently reported in the presence of testicular tumours [15,17,44]. The ultrasonographic appearance of experimentally induced testicular torsion in the dog has been reported by Hricak et al.: from 15 to 60 minutes after torsion there are anatomical changes visible by ultrasound as a testicular enlargement characterized by diffusely decreased parenchymal echogenicity, and a concurrent enlargement of the epididymis and spermatic cord. The scrotal skin becomes hypoechoic and increases in thickness [49].
Testicular hypoplasia is a developmental defect of the testis, which does not reach the post-pubertal normal size. Most cases of hypoplasia are because of cryptorchidism, and in several cases are linked to the inability of the epididymis to reach the normal size too [35].
Differently from hypoplasia, testicular atrophy is used to define normally developed testis that became smaller in size, as a result of ageing [35], cryptorchidism, testicular tumour or chronic orchitis in the opposite testicle [17]. An atrophic testis typically has a normal-sized epididymis, so proportions change with increased severity.
In both testicular hypoplasia and atrophy, at the ultrasonographic examination albuginea appeared thick, and vessels are less obvious or missing. The echotexture could be variable, hypoechoic to isoechoic, or also diffusely hyperechoic depending on the cause and severity [17]. Hyperechoic foci producing acoustic shadowing could be present, reflecting parenchymal mineralization [35].
Ultrasonography is also very useful in cryptorchidism for locating and evaluating undescended testicle(s), which may be located in the abdominal cavity, inguinal canal, or in an ectopic subcutaneous location between the superficial inguinal ring and the scrotum [50]. Cryptorchid testis is usually small in size, thus testicular parenchyma could be demonstrated by detecting the hyperechoic mediastinum.
3.4.2. Extratesticular diseases
Epididymitis can occur separately or concurrently with orchitis (Figure 3), and the damage may extend to include the ductus deferens [15,17,30]. Usually, epididymitis involves the tail and sometimes the body of the epididymis; the head of the epididymis is seldom involved [51].
This may be bilateral or unilateral, and the severity varies and reflects the degree of damage, including necrosis and vascular changes. In severe acute disease, there is swelling and edema of the tail of the epididymis, with a relevant increase in size [35] with or without fluid accumulation into the vaginal cavity. Ultrasonography, by the direct visualization of the altered organs, improves the differential diagnosis of the disease causing the scrotal increase in volume [13,17,30,51].
Ultrasonography could be particularly valuable in the presence of extra-testicular (around the testicle but within the vaginal tunic) fluid accumulation. In this case, the fluid causes a scrotal enlargement, preventing the clinical discrimination between the structures involved. Types of extratesticular fluid accumulation are serum (hydrocele), blood (hematocele), pus (pyocele), or possibly urine [11,13].
Rarely epidydimal cysts, fluid accumulation as the result of epididymal canal’s occlusion, were reported in dogs [11].
Varicoceles in humans are caused by alterations in the veins of the pampiniform plexus where they become enlarged, elongated, and tortuous. On sonograms, varicoceles appear as an anechoic, tubular and serpiginous fluid collection in the region of the epididymis. Varicoceles are encountered rarely in dogs, and their ultrasonographic appearance has not been described [11].
4. Color doppler and power doppler
4.1. Technology and applications
Doppler ultrasonography has become the method of choice to evaluate the blood supply of various organs. It is one of the simplest and most precise techniques for estimating blood flow, as it combines data concerning the anatomy and dynamic flow parameters [52].
Based on how blood flow information is displayed, Doppler ultrasonography can be classified as color (color Doppler and power color Doppler) or spectral (pulsed wave—PW, continuous wave—CW), or their combination.
Color and power color Doppler are termed color Doppler due to the use of color map overlays of blood flow on real-time two-dimensional gray-scale images (Figure 4), to display information [17]. Signals from moving red blood cells are displayed in color as a function of their motion toward or away from the transducer. The amount of color saturation also indicates the relative velocity of cells.
Power color Doppler ultrasonography is more sensitive for detecting low velocities and small parenchymal vessels [17,53]. Due to the qualitative interpretation of the sonograms, color Doppler is rarely applied in experimental studies.
Quantitative blood flow analysis includes the evaluation of peak systolic velocity = PSV, end-diastolic velocity = EDV, resistance index = RI and pulsatility index = PI.
Pulsed wave and continuous wave Doppler are termed spectral Doppler, and they display quantitative information as a time-velocity waveform along y and x axes, respectively. With pulsed wave Doppler ultrasonography, sound is transmitted in pulses using the pulse-echo principle as in real-time imaging [17]. Pulsed wave is the most commonly used type of spectral Doppler because it is readily available on nearly all modern transducers and possesses depth discrimination [17]. To obtain Doppler velocity information is with continuous wave technology [54]; this Doppler ultrasonography can measure much higher flow velocities than pulsed Doppler [17].
Duplex Doppler ultrasonography refers to the simultaneous display of pulsed or continuous wave spectral Doppler tracings and B-mode images [17].
Similarly, triplex Doppler ultrasonography, involves the simultaneous use of two-dimensional ultrasound, color Doppler and pulsed Doppler, which allows the gathering of anatomical data of the vessels and functional data regarding blood flow, including its presence or absence, direction and speed [17,55].
In human medicine pulsed wave Doppler, color and power Doppler are routinely applied to asses andrology status [51,56,57,58,59,60,61,62,63,64,65,66] and to define aethiology of dyspermia [24,67], demonstrating that sperm quality and quantity are dependent on tissue perfusion [24,27,68,69,70] and proposing that the evaluation of testicular blood flow is able to predict the testicular function and, in turn, spermatogenesis [24,68,69,70].
In veterinary medicine the study of testicular vascularization was performed in the stallion [7,71,72,73,74], jackass [75], tom [76,77], bull [18,78,79], ram [21,80,81], buck [52,82], dog [48,55,83,84,85,86,87,88,89,90,91,92,93]. The results of these studies essentially confirm a relationship between testicle arterial blood flow and seminal quality both in normal and pathological conditions.
4.2. Normal findings
The peculiar vascularization of the testis allows a division of vessels into three segments: (a) supra-testicular arteries within the pampiniform plexus: the testicular artery, cremasteric artery, and deferential artery; (b) arteries within the testicular membranes: the marginal artery; and (c) intratesticular vessels: the centripetal branches and recurrent rami [89].
Characteristics of blood flow within the testicular artery assessed by pulsed wave Doppler ultrasound change depending upon the segment [87,89]. In the supra-testicular region, a biphasic waveform with a diastolic notch followed by a diastolic peak, or a monophasic waveform characterized by a slow systolic increase followed by a decreased diastolic flow, could be observed due to the vessel’s tortuous characteristics in this area. The other two regions show a low resistance flow with monophasic waveforms (Figure 5) [30]. Higher blood flow velocities are recorded within the supra-testicular region, decreasing through marginal and intra-testicular regions [30,84,87,89].
4.3. Relationship between spectral doppler measurement and dog’s semen quality
As previously mentioned, a relationship between pulsed wave Doppler measurements and semen quality has been observed in many studies, primarily in human medicine, reporting higher correlations between the values of the resistive index (RI) and peak systolic velocity (PSV) with sperm production rate scores, and considering these values as reliable indicators for spermatogenesis. These parameters are proposed in the routine clinical protocol for distinguishing various causes of dyspermia and identifying subfertile men [94].
Even in veterinary medicine, the mensuration of these indexes could be an effective tool in andrology as potential markers of seminal quality in dogs.
In the study of Zelli et al., the indexes were studied in correlation with testicular volume and semen parameters, showing that peak systolic velocity was positively correlated with testicular volume and negatively with live sperm, whilst a negative correlation existed between the resistive index and pulsatility index with total and progressive motility. Resistive index and pulsatility index were also negatively correlated with the percentage of membrane intact sperms with curled tails, while the latter was positively correlated with end diastolic velocity [93].
Moreover, in the study of Gloria et al., the blood flow parameters measured by PWD were evaluated in correlation not only with sperm attributes but also with testicular histological characteristics, confirming negative correlations between RI and PI and abnormal spermatogenesis and histological abnormalities [88].
At last, also Velasco and Ruiz proposed the ultrasonographic measurement as objective parameters to evaluate testicular function. But, because of the variability found in all the analyzed data (depending on the location of the measurement, season, species, breed and laterality), they concluded that further research is needed to determine PWD physiological parameters [95].
4.4. Abnormal findings
In testicular neoplasia power color Doppler ultrasonography is a very useful tool in assessing tumour vasculature, due to the typically high interstitial pressure in tumours and resultant low-velocity states in tumour vessels, although only a few descriptions of testicular blood flow in abnormal testes are available [96]. The Vascularity index (VI) seems that increases in solid tumours compared to those of non-neoplastic masses, as the blood flow within and around most tumours [48]. Blood flow PSV increases with the increase in size of neoplastic nodules and the spectral waveform around the lesion had a low resistance pattern with lower-middle values of PI and RI then normal [48]. None of these appearances, however, are specific for each tumour type [16,28,48].
In orchitis, testicular blood flow estimated by color Doppler, may demonstrate amplified testicular parenchymal perfusion with RI and PI increase within the testicular parenchyma [30]. However limited modifications in vascular flow could be detected in necrosis and fibrosis [48]. In this latter report, RI was significantly decreased in the inflammatory lesion, probably due to the reactive hyperemia, while it was increased in fibrotic lesions related to degenerative changes.
In dogs with torsion of the spermatic cord, the absence of perfusion to and within the twisted testis could be evidenced with color Doppler ultrasound [30,49], helping in differential diagnosis with acute orchitis [11]. In cases of incomplete torsion it may be possible to observe decreased rather than absent perfusion [30].
5. B-flow
B-Flow is a type of digitally encoded ultrasound technology specifically developed by GE Healthcare (Chicago, IL, USA) for blood flow visualization [97]. Its technical foundation is based on a combination of coded excitation and tissue equalization [97], to directly show moving blood echoes using a grayscale presentation demonstrating real-time blood movement similar to a conventional angiogram (Figure 6), along with simultaneous visualization of the surrounding anatomy [98].
In human medicine, B-flow was first applied for use in carotid artery ultrasound in vascular medicine, and more recently has been reported as valuable in the assessment of the abdomen such as hepatic vasculature and evaluation of renal perfusion [98,99,100,101]. Furthermore, several clinical studies investigated B-Flow imaging for potential applications within obstetrics and gynaecology, focusing on utilizing the technology in perinatology and fetal echocardiography [97].
Applications of B-flow have been rarely performed in animals. Its use is reported in two studies that evaluated chemically-induced mammary tumours by matching this technology with other ultrasonography techniques, reporting that B-Flow is more sensitive than power color Doppler in detecting tumour vessels [102,103].
In veterinary clinical reproduction, this technology was only focused on the evaluation of testicular neoplastic vascular patterns, concluding that patterns did not vary among the different tumour types [16].
6. Contrast enhanced ultrasonography (CEUS)
6.1. Technology and applications
Contrast enhanced ultrasonography (CEUS) was recently introduced in veterinary medicine because of its ability to quantify microvascular blood volume and blood flow of vital organs, as described in human medicine [104,105]. It is based on the intravascular injection of specific ultrasound contrast agents (USCAs) which consist of microspheres containing specific gases stabilized by an outer shell [106,107]; gases are eliminating through lungs, whereas the stabilizing components are filtered by the kidneys and eliminated by the liver [76,108,109]. Due to the reflection of echoes on gases, the intensity of the signal in gray-scale and Doppler modes is increased by 10 to 1,000 times, and it is shown meanly for 5 minutes, depending on the contrast agent used. The total duration of a CEUS evaluation is about 20 minutes, and general anaesthesia is not required [109].
Progressive inclusion of CEUS among the diagnostic tools is due to the safe, painless, fast, portable and non-irradiating nature of this technology, without nephrotoxicity. Side effects of USCAs are rare: only pain at the site of injection, nausea or vomiting were described in dogs [110]. Although high costs of the contrast material and the need for specialized ultrasonographic equipment [30], CEUS is relatively cheap when compared to computed tomography scan and magnetic resonance imaging [107,111].
Contrast enhanced ultrasonography allows the detection of several attributes of a lesion including the presence/absence of the contrast, wash-in (incoming phases), wash-out (output) and peak enhancement of CEUS in tissue, temporal behaviour, perfusion features, vascular anatomy, comparison with the surrounding tissues, and flow direction [76,107,112]. Some of them could be estimated, quantitatively in a specific region of interest (ROI) using the software integrated with the ultrasound machines [16] able to calculate peak intensity (PI), time to peak (TTP), and area under the curve (AUC). The washout (WO), as the time interval from TTP until signal intensity declined by 40% of PI, could be also calculated [16].
Over the past decades, both ultrasound contrast agents and techniques evolved rapidly, and to date this technique is used to quantify the perfusion of various deep organs, including skeletal muscle, heart, adipose tissue, kidneys, liver, and brain [104]. Some recent reports applied CEUS in human testis evaluation, investigating the different features in various pathological conditions [2,113,114,115,116].
The application of CEUS in veterinary medicine are mainly focused on the dogs about the liver and its vascularization [106,117,118,119,120,121,122], lymph nodes [119,123,124], kidneys [125,126], pancreas [127,128], eyes [129,130,131], spleen [107,132,133,134,135] and prostate [136,137,138,139,140] by studying normal and pathological aspects in order to differentiate between inflammatory, degenerative and neoplastic lesions, providing a discrimination between benign or malignant ones [96,109,141]. Some studies were also performed in cats [76,142,143]. Works about the application of CEUS in canine andrology are few and focused on chronic testicular alterations [110].
6.2. Normal findings
After injection of the contrast agent, the testicular artery branches and parenchymal perfusion had been readily observed, with a progressive opacification of the convoluted supra-testicular, marginal, and then intratesticular arteries, with flow directed towards the mediastinum testis. A progressive increase of the echogenicity of the testicular parenchyma during the vascular bed phase was observed, followed by gradual clearance of the contrast from the parenchyma during the wash-out phase. Testicular veins were also highlighted, with lower echogenicity compared to the arteries because the persistence within the vascular bed resulted in a longer wash-out than wash-in period [110]. A range of values of CEUS in normal dogs was proposed, however reference values should be used with caution due to the lack of reproductive information of healthy group and the sedation of the patients during the procedure, which could modify the physiological vascular flow.
6.3. Abnormal findings
Due to the detection of fine vascularization, CEUS is able to detect some testicular lesions not previously revealed by conventional ultrasonography, resulting particularly powerful in the assessment of testicular neoplasia [16,110]. Neoplastic lesions have been described to be better defined in the wash-in phase and tend to maintain the pattern during peak and wash-out. Thus, any specific phase is not associated with different patterns of lesional contrast enhancement over time [110].
Although some authors hypothesized to associate specific CEUS patterns to different tumour types, with controversial results [16]. Volta et al. reported the association between hypo- or iso-enhanced testicular lesions with intralesional vessels with seminomas [110], while Orlandi et al. found similar CEUS parameters in different tumour types, suggesting the inability to differentiate between testicular tumors based on contrast-enhanced pattern [16].
The CEUS pattern in non-neoplastic testicular lesions was reported in one study in the dog, in which degenerated testes, atrophic testes, testes with chronic necrotic orchitis and testes with interstitial cell hyperplasia were considered [110]. The reduced number of cases and the lack of specific lesions in different conditions reduced the application potential on this approach.
7. Ultrasound elastography
7.1. Technology and applications
Ultrasound elastography (UEl) is an ultrasonography-based technology introduced in the 1990s, which can assess the elasticity or the stiffness of the tissues [144]. This technique is based on the assumption that softer parts of tissues deform easier than the harder ones under compression, allowing an estimation of tissue elasticity [145]. Changes in the elasticity of tissue could be related to pathological modifications induced by degeneration (ageing), inflammation, and uncontrolled cell growth [144].
Elastography uses ultrasonic imaging to observe tissue shear deformation under conditions of one or both of the types of shear, currently in a real-time two-dimensional image sequence, after applying a force that is either dynamic (e. g. by thumping or vibrating) or varying so slowly that it is considered “quasi-static” (e. g. by probe palpation). The deformation may be represented in an elastogram, or as a local measurement, in one of three ways: i) tissue displacement may be detected and displayed directly, as in the method known as acoustic radiation force impulse (ARFI) imaging; ii) Tissue strain may be calculated and displayed, producing what is termed strain elastography (SE); iii) In the dynamic case only, the data may be used to record the propagation of shear-waves, which are used to calculate either a) regional values of their speed (without making images) using methods referred to herein as transient elastography (TE) and point shear-wave elastography (pSWE), or images of their speed using methods referred to herein as shear-wave elastography (SWE) which includes 2-D SWE and 3-D SWE [146,147].
Several technologies are able to evaluate qualitatively, semi-quantitatively, or quantitatively the stiffness of a tissue. In strain elastography, the deformation of the tissue is caused by the manual compression of the probe on the tissue is converted to a gray-scale image. The final result is an image, namely elastogram, in which the stiffness of the different components of the anatomical region is displayed, in real-time, on a color-coded map [148]. Due to the subjective origin of the compression, this technique could be considered qualitative. A semi-quantitative measurement was proposed to increase the objectivity of the analysis, by the calculation of the strain ratio, a value obtained by the comparison of the stiffness of the tissue under examination, estimated in a region of interest (ROI), referred to that of adjacent normal tissue in a similar-sized ROI [147].
In contrast to strain imaging, shear-wave elastography allows speed measurement of shear waves generated by the probe, allowing the quantitative estimate of tissue elasticity even in a specific range of interest (ROI) [147].
In human medicine, UEl was successfully applied in diagnostic imaging of the liver, breast, prostate, thyroid and lymph nodes, or musculoskeletal pathological conditions and it is largely used in oncology because of the ability to predict the malignancy of the lesions, even with testicular neoplasm [145,148,149,150,151,152]. In human andrology, UEl was also proposed in the examination of non-focal alterations of the testis, defining the aethiology of infertility [27,153,154].
In veterinary medicine, studies have been performed to apply UEl in canine and feline normal and pathological conditions of different organs such as the spleen, liver, kidney, and prostate [155,156,157,158], adrenal gland [159], skin [160], lymph nodes [123,161], pancreas [162], small intestine mucosa [163] and placenta [164], performing also a qualitative study even in fetal lungs and fetal liver during the final days of intrauterine development, demonstrating the changes of tissue stiffness [165]. In veterinary oncology, some authors proposed UEl as a complementary diagnostic tool to differentiate benign from malignant lesions, mainly focusing on mammary neoplasm, although giving controversial results. Preliminary studies reported that the cyto/histologic classified as benign mammary lesions are observed as deformable, whilst the malignant tissues were rigid, as like as appears in breast tumours of women [166,167]. Contrarywise, in a more recent work, malignant mammary nodular lesions showed similar stiffness compared with hyperplastic/benign neoplastic lesions [168], so further investigations on the tissue mechanical properties are necessary to optimally introduce the use of this technology in the evaluation of mammary gland tumors in the dog.
7.2. Normal findings
In normal canine testis, qualitative (Figure 7) and quantitative ultrasound elastography revealed hard, homogeneous and not pliable organs.
In agreement with the findings in the tom [169], shear velocity values were similar in animals grouped by age, suggesting a limited effect of this variable on the testicular stiffness (Figure 8) [157].
The reference values reported in this manuscript, however, should be considered with caution due to the variability of breed and weight of the males recruited, and the lack of definition of their reproductive function.
7.3. Abnormal findings
Limited information is available to date regarding the application of UEl in testicular disease of the dog. In a recent study, UEl was found able to distinguish non-neoplastic from neoplastic testicular lesions, with the latter stiffer [171]. Although the findings were not conclusive due to the limited number of animals, ultrasound elastography appeared a promising technology for the evaluation of neoplastic lesions of canine testis.
In a preliminary study on UEl in canine testicular evaluation, abnormal testes were found stiffer and inhomogeneous compared with normal testes, even though a great variability of testicular diseases was reported, making ineffective the comparison between the different conditions [170].
8. Conclusions
The present review explored the literature concerning the application of ultrasound-based technologies in the canine testis assessment. Conventional technologies, such as B-mode ultrasonography, could be effectively applied in andrological practice, but the lack of objectivization reduced the relevance in differentiating testicular disease. On the other hand, recent technologies, such as CEUS and ultrasound elastography, could expand the armamentarium for the clinicians caring for canine andrological patients but require more studies and solid results to verify their real contribution to the clinical practice.
Author Contributions
Conceptualization, A.G. and C.B.; investigation, C.B.; writing—original draft preparation, C.B.; writing—review and editing, A.G. and A.C. All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Dogra, V.S.; Gottlieb, R.H.; Oka, M.; Rubens, D.J. Sonography of the Scrotum. Radiology 2003, 227, 18–36. [Google Scholar] [CrossRef]
- Lock, G.; Schmidt, C.; Helmich, F.; Stolle, E.; Dieckmann, K.-P. Early Experience with Contrast-Enhanced Ultrasound in the Diagnosis of Testicular Masses: A Feasibility Study. Urology 2011, 77, 1049–1053. [Google Scholar] [CrossRef] [PubMed]
- De Zordo, T.; Stronegger, D.; Pallwein-Prettner, L.; Harvey, C.J.; Pinggera, G.; Jaschke, W.; Aigner, F.; Frauscher, F. Multiparametric Ultrasonography of the Testicles. Nat Rev Urol 2013, 10, 135–148. [Google Scholar] [CrossRef] [PubMed]
- Mantziaras, G. Imaging of the Male Reproductive Tract: Not so Easy as It Looks Like. Theriogenology 2020, 150, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Evans, H.E.; De Lahunta, A.; Miller, M.E. Miller’s Anatomy of the Dog; 4. ed.; Elsevier Saunders: St. Louis, Mo, 2013; ISBN 978-1-4377-0812-7. [Google Scholar]
- Kastelic, J.P.; Cook, R.B.; Coulter, G.H. Contribution of the Scrotum, Testes, and Testicular Artery to Scrotal/Testicular Thermoregulation in Bulls at Two Ambient Temperatures. Animal Reproduction Science 1997, 45, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Rodriguez, J.M.; Anel-Lopez, L.; Martín-Muñoz, P.; Álvarez, M.; Gaitskell-Phillips, G.; Anel, L.; Rodríguez-Medina, P.; Peña, F.J.; Ortega Ferrusola, C. Pulse Doppler Ultrasound as a Tool for the Diagnosis of Chronic Testicular Dysfunction in Stallions. PLoS ONE 2017, 12, e0175878. [Google Scholar] [CrossRef]
- Bergh, A.; Damber, J.-E. Vascular Controls in Testicular Physiology. In Molecular Biology of the Male Reproductive System; de Kretser, D., Ed.; Academic Press Inc., 1993; pp. 439–468 ISBN 978-0-12-209030-1.
- England Relationship between Ultrasonographic Appearance, Testicular Size, Spermatozoal Output and Testicular Lesions in the Dog. J Small Animal Practice 1991, 32, 306–311. [CrossRef]
- Johnston, G.R.; Feeney, D.A.; Johnston, S.D.; O’Brien, T.D. Ultrasonographic Features of Testicular Neoplasia in Dogs: 16 Cases (1980-1988). J Am Vet Med Assoc 1991, 198, 1779–1784. [Google Scholar] [CrossRef]
- Johnston, G.R.; Feeney, D.A.; Rivers, B.; Walter, P.A. Diagnostic Imaging of the Male Canine Reproductive Organs. Veterinary Clinics of North America: Small Animal Practice 1991, 21, 553–589. [Google Scholar] [CrossRef]
- Pugh, C.R.; Konde, L.J.; Park, R.D. Testicular Ultrasound in the Normal Dog. Veterinary Radiology 1990, 31, 195–199. [Google Scholar] [CrossRef]
- Pugh, C.R.; Konde, L.J. Sonographic Evaluation of Canine Testicular and Scrotal Abnormalities: A Review of 26 Case Histories. Veterinary Radiology 1991, 32, 243–250. [Google Scholar] [CrossRef]
- Kühn, A.L.; Scortegagna, E.; Nowitzki, K.M.; Kim, Y.H. Ultrasonography of the Scrotum in Adults. Ultrasonography 2016, 35, 180–197. [Google Scholar] [CrossRef]
- Davidson, A.P.; Baker, T.W. Reproductive Ultrasound of the Dog and Tom. Topics in Companion Animal Medicine 2009, 24, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, R.; Vallesi, E.; Boiti, C.; Polisca, A.; Bargellini, P.; Troisi, A. Characterization of Testicular Tumor Lesions in Dogs by Different Ultrasound Techniques. Animals 2022, 12, 210. [Google Scholar] [CrossRef] [PubMed]
- Mattoon, J.S.; Sellon, R.; Berry, C. Small Animal Diagnostic Ultrasound; Fourth.; Elsevier, Inc: Philadelphia, 2020; ISBN 978-0-323-53337-9. [Google Scholar]
- Arteaga, A.A.; Barth, A.D.; Brito, L.F.C. Relationship between Semen Quality and Pixel–Intensity of Testicular Ultrasonograms after Scrotal Insulation in Beef Bulls. Theriogenology 2005, 64, 408–415. [Google Scholar] [CrossRef]
- Ahmadi, B.; Lau, C.P.-S.; Giffin, J.; Santos, N.; Hahnel, A.; Raeside, J.; Christie, H.; Bartlewski, P. Suitability of Epididymal and Testicular Ultrasonography and Computerized Image Analysis for Assessment of Current and Future Semen Quality in the Ram. Exp Biol Med (Maywood) 2012, 237, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Brito, L.F.C.; Barth, A.D.; Wilde, R.E.; Kastelic, J.P. Testicular Ultrasonogram Pixel Intensity during Sexual Development and Its Relationship with Semen Quality, Sperm Production, and Quantitative Testicular Histology in Beef Bulls. Theriogenology 2012, 78, 69–76. [Google Scholar] [CrossRef]
- Carvajal-Serna, M.; Miguel-Jiménez, S.; Pérez-Pe, R.; Casao, A. Testicular Ultrasound Analysis as a Predictive Tool of Ram Sperm Quality. Biology 2022, 11, 261. [Google Scholar] [CrossRef]
- England, G.; Bright, L.; Pritchard, B.; Bowen, I.; de Souza, M.; Silva, L.; Moxon, R. Canine Reproductive Ultrasound Examination for Predicting Future Sperm Quality. Reprod Dom Anim 2017, 52, 202–207. [Google Scholar] [CrossRef]
- Moxon, R.; Bright, L.; Pritchard, B.; Bowen, I.M.; Souza, M.B. de; Silva, L.D.M. da; England, G.C.W. Digital Image Analysis of Testicular and Prostatic Ultrasonographic Echogencity and Heterogeneity in Dogs and the Relation to Semen Quality. Animal Reproduction Science 2015, 160, 112–119. [Google Scholar] [CrossRef]
- Garolla, A.; Grande, G.; Palego, P.; Canossa, A.; Caretta, N.; Di Nisio, A.; Corona, G.; Foresta, C. Central Role of Ultrasound in the Evaluation of Testicular Function and Genital Tract Obstruction in Infertile Males. Andrology 2021, 9, 1490–1498. [Google Scholar] [CrossRef]
- Moon, M.H.; Kim, S.H.; Cho, J.Y.; Seo, J.T.; Chun, Y.K. Scrotal US for Evaluation of Infertile Men with Azoospermia. Radiology 2006, 239, 168–173. [Google Scholar] [CrossRef]
- Sakamoto, H.; Ogawa, Y.; Yoshida, H. Relationship between Testicular Volume and Testicular Function: Comparison of the Prader Orchidometric and Ultrasonographic Measurements in Patients with Infertility. Asian J Andrology 2008, 10, 319–324. [Google Scholar] [CrossRef]
- Schurich, M.; Aigner, F.; Frauscher, F.; Pallwein, L. The Role of Ultrasound in Assessment of Male Fertility. European Journal of Obstetrics & Gynecology and Reproductive Biology 2009, 144, S192–S198. [Google Scholar] [CrossRef]
- Russo, M.; England, G.C.W.; Catone, G.; Marino, G. Imaging of Canine Neoplastic Reproductive Disorders. Animals 2021, 11, 1213. [Google Scholar] [CrossRef]
- Romagnoli, S.; Bonaccini, P.; Stelletta, C.; Garolla, A.; Menegazzo, M.; Foresta, C.; Mollo, A.; Milani, C.; Gelli, D. Clinical Use of Testicular Fine Needle Aspiration Cytology in Oligozoospermic and Azoospermic Dogs. Reproduction in Domestic Animals 2009, 44, 329–333. [Google Scholar] [CrossRef]
- de Souza, M.B.; Silva, L.D.M.; Moxon, R.; Russo, M.; England, G.C.W. Ultrasonography of the Prostate Gland and Testes in Dogs. In pract. 2017, 39, 21–32. [Google Scholar] [CrossRef]
- Gouletsou, P.G.; Galatos, A.D.; Leontides, L.S. Comparison between Ultrasonographic and Caliper Measurements of Testicular Volume in the Dog. Animal Reproduction Science 2008, 108, 1–12. [Google Scholar] [CrossRef]
- Paltiel, H.J.; Diamond, D.A.; Di Canzio, J.; Zurakowski, D.; Borer, J.G.; Atala, A. Testicular Volume: Comparison of Orchidometer and US Measurements in Dogs. Radiology 2002, 222, 114–119. [Google Scholar] [CrossRef]
- Mantziaras, G.; Alonge, S.; Luvoni, G.C. Ultrasonographic Study of Age-Related Changes on the Size of Prostate and Testicles in Healthy German Shepherd Dogs.; Wroclaw (Poland), 14; p. 150. 20 September.
- Cotchin, E. Testicular Neoplasms in Dogs. Journal of Comparative Pathology and Therapeutics 1960, 70, 232–IN12. [Google Scholar] [CrossRef]
- Foster, R.A. Common Lesions in the Male Reproductive Tract of Cats and Dogs. Veterinary Clinics of North America: Small Animal Practice 2012, 42, 527–545. [Google Scholar] [CrossRef]
- Grüntzig, K.; Graf, R.; Hässig, M.; Welle, M.; Meier, D.; Lott, G.; Erni, D.; Schenker, N.S.; Guscetti, F.; Boo, G.; et al. The Swiss Canine Cancer Registry: A Retrospective Study on the Occurrence of Tumours in Dogs in Switzerland from 1955 to 2008. Journal of Comparative Pathology 2015, 152, 161–171. [Google Scholar] [CrossRef]
- Lawrence, J.A.; Saba, C.F. Tumors of the Male Reproductive System. In Small Animal Clinical Oncology; Elsevier Saunders, 2013; pp. 557–571.
- Liao, A.T.; Chu, P.-Y.; Yeh, L.-S.; Lin, C.-T.; Liu, C.-H. A 12-Year Retrospective Study of Canine Testicular Tumors. J. Vet. Med. Sci. 2009, 71, 919–923. [Google Scholar] [CrossRef]
- Nascimento, H.H.L.; Santos, A. dos; Prante, A.L.; Lamego, E.C.; Tondo, L.A.S.; Flores, M.M.; Fighera, R.A.; Kommers, G.D. Testicular Tumors in 190 Dogs: Clinical, Macroscopic and Histopathological Aspects. Pesq. Vet. Bras. 2020, 40, 525–535. [Google Scholar] [CrossRef]
- Manuali, E.; Forte, C.; Porcellato, I.; Brachelente, C.; Sforna, M.; Pavone, S.; Ranciati, S.; Morgante, R.; Crescio, I.M.; Ru, G.; et al. A Five-Year Cohort Study on Testicular Tumors from a Population-Based Canine Cancer Registry in Central Italy (Umbria). Preventive Veterinary Medicine 2020, 185, 105201. [Google Scholar] [CrossRef]
- Merlo, D.F.; Rossi, L.; Pellegrino, C.; Ceppi, M.; Cardellino, U.; Capurro, C.; Ratto, A.; Sambucco, P.L.; Sestito, V.; Tanara, G.; et al. Cancer Incidence in Pet Dogs: Findings of the Animal Tumor Registry of Genoa, Italy. J Vet Intern Med 2008, 22, 976–984. [Google Scholar] [CrossRef]
- Mosier, J.E. Effect of Aging on Body Systems of the Dog. Veterinary Clinics of North America: Small Animal Practice 1989, 19, 1–12. [Google Scholar] [CrossRef]
- Santos, R.L.; Silva, C.M.; Ribeiro, A.F.C.; Serakides, R. Testicular Tumors in Dogs: Frequency and Age Distribution. Arq. Bras. Med. Vet. Zootec. 2000, 52, 25–26. [Google Scholar] [CrossRef]
- Hayes, H.M.; Wilson, G.P.; Pendergrass, T.W.; Cox, V.S. Canine Cryptorchism and Subsequent Testicular Neoplasia: Case-Control Study with Epidemiologic Update. Teratology 1985, 32, 51–56. [Google Scholar] [CrossRef]
- Khan, F.A.; Gartley, C.J.; Khanam, A. Canine Cryptorchidism: An Update. 2018.
- Memon, M.A. Common Causes of Male Dog Infertility. Theriogenology 2007, 68, 322–328. [Google Scholar] [CrossRef]
- Doxsee, A.L.; Yager, J.A.; Best, S.J.; Foster, R.A. Extratesticular Interstitial and Sertoli Cell Tumors in Previously Neutered Dogs and Cats: A Report of 17 Cases. 2006, 47. 47.
- Bigliardi, E.; Denti, L.; De Cesaris, V.; Bertocchi, M.; Di Ianni, F.; Parmigiani, E.; Bresciani, C.; Cantoni, A.M. Colour Doppler Ultrasound Imaging of Blood Flows Variations in Neoplastic and Non-Neoplastic Testicular Lesions in Dogs. Reprod Dom Anim 2019, 54, 63–71. [Google Scholar] [CrossRef]
- Hricak, H.; Lue, T.; Filly, R.A.; Alpers, C.E.; Zeineh, S.J.; Tanagho, E.A. Experimental Study of the Sonographic Diagnosis of Testicular Torsion. Journal of Ultrasound in Medicine 1983, 2, 349–356. [Google Scholar] [CrossRef]
- Felumlee, A.E.; Reichle, J.K.; Hecht, S.; Penninck, D.; Zekas, L.; Dietze Yeager, A.; Goggin, J.M.; Lowry, J. Use of Ultrasound to Locate Retained Testes in Dogs and Cats: Location of Retained Testes. Veterinary Radiology & Ultrasound 2012, 53, 581–585. [Google Scholar] [CrossRef]
- Dubinsky, T.J. Color-Flow and Power Doppler Imaging of the Testes. World J Urol 1998, 35–40. [Google Scholar] [CrossRef]
- Strina, A.; Corda, A.; Nieddu, S.; Solinas, G.; Lilliu, M.; Zedda, M.T.; Pau, S.; Ledda, S. Annual Variations in Resistive Index (RI) of Testicular Artery, Volume Measurements and Testosterone Levels in Bucks. Comp Clin Pathol 2016, 25, 409–413. [Google Scholar] [CrossRef]
- Rubin, J.M. Power Doppler. Eur Radiol 1999, 318–322. [Google Scholar] [CrossRef]
- Nelson, T.; Pretorius, D. The Doppler Signal: Where Does It Come from and What Does It Mean? American Journal of Roentgenology 1988, 151, 439–447. [Google Scholar] [CrossRef]
- de Souza, M.B.; Mota Filho, A.C.; Sousa, C.V.S.; Monteiro, C.L.B.; Carvalho, G.G.; Pinto, J.N.; Linhares, J.C.S.; Silva, L.D.M. Triplex Doppler Evaluation of the Testes in Dogs of Different Sizes. Pesq. Vet. Bras. 2014, 34, 1135–1140. [Google Scholar] [CrossRef]
- Aydos, K.; Baltaci, S.; Salih, M.; Anafarta, K.; Bedük, Y.; Gülsoy, U. Use of Color Doppler Sonography in the Evaluation of Varicoceles. Eur Urol 1993, 24, 221–225. [Google Scholar] [CrossRef]
- Gupta, A.K.; S. , S.; Shetty, S.S.; R., C. Role of High Resolution Sonography and Color Doppler Flow Imaging in the Evaluation of Scrotal Pathology. Int J Res Med Sci 2017, 5, 1499. [Google Scholar] [CrossRef]
- Horstman, W.G.; Melson, G.L.; Middleton, W.D.; Andriole, G.L. Testicular Tumors: Findings with Color Doppler US. Radiology 1992, 185, 733–737. [Google Scholar] [CrossRef]
- Jee, W.-H.; Choe, B.-Y.; Byun, J.-Y.; Shinn, K.-S.; Hwang, T.-K. Resistive Index of the Intrascrotal Artery in Scrotal Inflammatory Disease. Acta Radiol 1997, 38, 1026–1030. [Google Scholar] [CrossRef] [PubMed]
- Lee, F.T.; Winter, D.B.; Madsen, F.A.; Zagzebski, J.A.; Pozniak, M.A.; Chosy, S.G.; Scanlan, K.A. Conventional Color Doppler Velocity Sonography versus Color Doppler Energy Sonography for the Diagnosis of Acute Experimental Torsion of the Spermatic Cord. American Journal of Roentgenology 1996, 167, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Lotti, F.; Frizza, F.; Balercia, G.; Barbonetti, A.; Behre, H.M.; Calogero, A.E.; Cremers, J.; Francavilla, F.; Isidori, A.M.; Kliesch, S.; et al. The European Academy of Andrology (EAA) Ultrasound Study on Healthy, Fertile Men: An Overview on Male Genital Tract Ultrasound Reference Ranges. Andrology 2022, 10, 118–132. [Google Scholar] [CrossRef] [PubMed]
- Middleton, W.; Thorne, D.; Melson, G. Color Doppler Ultrasound of the Normal Testis. American Journal of Roentgenology 1989, 152, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Pavlica, P.; Barozzi, L. Imaging of the Acute Scrotum. European Radiology 2001, 11, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, S.A.A.; Ahmad, I.; Siddiqui, M.A.; Zaheer, S.; Ahmad, K. Role of Color Doppler Ultrasonography in Evaluation of Scrotal Swellings. 2011, 8. 8.
- Sidhu, P.S. Clinical and Imaging Features of Testicular Torsion: Role of Ultrasound. Clinical Radiology 1999, 54, 343–352. [Google Scholar] [CrossRef]
- Sriprasad, S.; Kooiman, G.G.; Muir, G.H.; Sidhu, P.S. Acute Segmental Testicular Infarction: Differentiation from Tumour Using High Frequency Colour Doppler Ultrasound. BJR 2001, 74, 965–967. [Google Scholar] [CrossRef]
- Abdulwahed, S.R.; Mohamed, E.-E.M.; Taha, E.A.; Saleh, M.A.; Abdelsalam, Y.M.; ElGanainy, E.O. Sensitivity and Specificity of Ultrasonography in Predicting Etiology of Azoospermia. Urology 2013, 81, 967–971. [Google Scholar] [CrossRef]
- Biagiotti, G.; Cavallini, G.; Modenini, F.; Vitali, G.; Gianaroli, L. Spermatogenesis and Spectral Echo-Colour Doppler Traces from the Main Testicular Artery. BJU International 2002, 90, 903–908. [Google Scholar] [CrossRef]
- Pinggera, G.-M.; Mitterberger, M.; Bartsch, G.; Strasser, H.; Gradl, J.; Aigner, F.; Pallwein, L.; Frauscher, F. Assessment of the Intratesticular Resistive Index by Colour Doppler Ultrasonography Measurements as a Predictor of Spermatogenesis. BJU Int 2008, 101, 722–726. [Google Scholar] [CrossRef] [PubMed]
- Sihag, P.; Tandon, A.; Pal, R.; Bhatt, S.; Sinha, A.; Sumbul, M. Sonography in Male Infertility: A Useful yet Underutilized Diagnostic Tool. J Ultrasound 2022, 25, 675–685. [Google Scholar] [CrossRef] [PubMed]
- Bollwein, H.; Scheibenzuber, E.; Stolla, R.; Echte, A.-F.; Sieme, H. Testicular blood flow in the stallion: variability and its relationship to sperm quality and fertility: PHK 2006, 22, 123–133. 22. [CrossRef]
- Ortega-Ferrusola, C.; Gracia-Calvo, L.; Ezquerra, J.; Pena, F. Use of Colour and Spectral Doppler Ultrasonography in Stallion Andrology. Reprod Dom Anim 2014, 49, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Pozor M., A.; McDonnell S., M. Doppler Ultrasound Measures of Testicular Blood Flow in Stallions. Theriogenology 2002, 437–440. [Google Scholar]
- Pozor, M.A.; McDonnell, S.M. Color Doppler Ultrasound Evaluation of Testicular Blood Flow in Stallions. Theriogenology 2004, 61, 799–810. [Google Scholar] [CrossRef] [PubMed]
- Gacem, S.; Papas, M.; Catalan, J.; Miró, J. Examination of Jackass (Equus Asinus) Accessory Sex Glands by B-mode Ultrasound and of Testicular Artery Blood Flow by Colour Pulsed-wave Doppler Ultrasound: Correlations with Semen Production. Reprod Dom Anim 2020, 55, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Botelho Brito, M.; Maronezi, M.C.; Uscategui, R.A.R.; Avante, M.L.; Simões, A.R.; Monteiro, F.O.B.; Feliciano, M.A.R. Metodos Ultrassonográficos Para La Evaluación de Testículos En Gatos. Rev MVZ Córdoba 2018, 23, 6888–6899. [Google Scholar] [CrossRef]
- de Brito; Feliciano, M. ; Coutinho, L.; Uscategui, R.; Simões, A.; Maronezi, M.; de Almeida, V.; Crivelaro, R.; Gasser, B.; Pavan, L.; et al. Doppler and Contrast-Enhanced Ultrasonography of Testicles in Adult Domestic Felines. Reprod Dom Anim 2015, 50, 730–734. [Google Scholar] [CrossRef]
- Gloria, A.; Carluccio, A.; Wegher, L.; Robbe, D.; Valorz, C.; Contri, A. Pulse Wave Doppler Ultrasound of Testicular Arteries and Their Relationship with Semen Characteristics in Healthy Bulls. J Animal Sci Biotechnol 2018, 9, 14. [Google Scholar] [CrossRef]
- Junior, F.A.B.; Junior, C.K.; Fávaro, P. da C.; Pereira, G.R.; Morotti, F.; Menegassi, S.R.O.; Barcellos, J.O.J.; Seneda, M.M. Effect of Breed on Testicular Blood Flow Dynamics in Bulls. Theriogenology 2018, 118, 16–21. [Google Scholar] [CrossRef]
- Elbaz, H.; Elweza, A.; Sharshar, A. Testicular Color Doppler Ultrasonography in Barki Rams. AJVS 2019, 61, 39. [Google Scholar] [CrossRef]
- Hedia M., G.; El-Belely M., S. Testicular Morphometric and Echotextural Parameters and Their Correlation with Intratesticular Blood Flow in Ossimi Ram Lambs. Large Animal Review 2021, 27, 77–82. [Google Scholar]
- Samir, H.; Nyametease, P.; Nagaoka, K.; Watanabe, G. Effect of Seasonality on Testicular Blood Flow as Determined by Color Doppler Ultrasonography and Hormonal Profiles in Shiba Goats. Animal Reproduction Science 2018, 197, 185–192. [Google Scholar] [CrossRef]
- Brito; da Rosa Filho, R. R.; Losano, J.D.A.; Vannucchi, C.I. Ageing Changes Testes and Epididymis Blood Flow without Altering Biometry and Echodensity in Dogs. Animal Reproduction Science 2021, 228, 106745. [Google Scholar] [CrossRef] [PubMed]
- Carrillo, J.; Soler, M.; Lucas, X.; Agut, A. Colour and Pulsed Doppler Ultrasonographic Study of the Canine Testis: Doppler Ultrasound Testis Dog. Reproduction in Domestic Animals 2012, 47, 655–659. [Google Scholar] [CrossRef]
- de Souza, M.B.; Barbosa, C.C.; England, G.; Mota Filho, A.C.; Sousa, C.; de Carvalho, G.G.; Silva, H.; Pinto, J.N.; Linhares, J.; Silva, L. Regional Differences of Testicular Artery Blood Flow in Post Pubertal and Pre-Pubertal Dogs. BMC Vet Res 2015, 11, 47. [Google Scholar] [CrossRef] [PubMed]
- de Souza, M.B.; England, G.C.W.; Mota Filho, A.C.; Ackermann, C.L.; Sousa, C.V.S.; de Carvalho, G.G.; Silva, H.V.R.; Pinto, J.N.; Linhares, J.C.S.; Oba, E.; et al. Semen Quality, Testicular B-Mode and Doppler Ultrasound, and Serum Testosterone Concentrations in Dogs with Established Infertility. Theriogenology 2015, 84, 805–810. [Google Scholar] [CrossRef] [PubMed]
- de Souza, M.B.; da Cunha Barbosa, C.; Pereira, B.S.; Monteiro, C.L.B.; Pinto, J.N.; Linhares, J.C.S.; da Silva, L.D.M. Doppler Velocimetric Parameters of the Testicular Artery in Healthy Dogs. Research in Veterinary Science 2014, 96, 533–536. [Google Scholar] [CrossRef]
- Gloria, A.; Di Francesco, L.; Marruchella, G.; Robbe, D.; Contri, A. Pulse-Wave Doppler Pulsatility and Resistive Indexes of the Testicular Artery Increase in Canine Testis with Abnormal Spermatogenesis. Theriogenology 2020, 158, 454–460. [Google Scholar] [CrossRef]
- Gumbsch, P.; Holzmann, A.; Gabler, C. Colour-Coded Duplex Sonography of the Testes of Dogs. Veterinary Record 2002, 151, 140–144. [Google Scholar] [CrossRef]
- Gunzel-Apel, A.-R.; Mohrke, C.; Nautrup, C.P. Colour-Coded and Pulsed Doppler Sonography of the Canine Testis, Epididymis and Prostate Gland: Physiological and Pathological Findings. Reprod Domest Anim 2001, 36, 236–240. [Google Scholar] [CrossRef]
- Lemos, H.; Dorado, J.; Hidalgo, M.; Gaivão, I.; Martins-Bessa, A. Assessment of Dog Testis Perfusion by Colour and Pulsed-Doppler Ultrasonography and Correlation With Sperm Oxidative DNA Damage. Topics in Companion Animal Medicine 2020, 41, 100452. [Google Scholar] [CrossRef] [PubMed]
- Trautwein, L.G.C.; Souza, A.K.; Martins, M.I.M. Can Testicular Artery Doppler Velocimetry Values Change According to the Measured Region in Dogs? Reprod Dom Anim 2019, 54, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Zelli, R.; Troisi, A.; Elad Ngonput, A.; Cardinali, L.; Polisca, A. Evaluation of Testicular Artery Blood Flow by Doppler Ultrasonography as a Predictor of Spermatogenesis in the Dog. Research in Veterinary Science 2013, 95, 632–637. [Google Scholar] [CrossRef]
- Samir, H.; Radwan, F.; Watanabe, G. Advances in Applications of Color Doppler Ultrasonography in the Andrological Assessment of Domestic Animals: A Review. Theriogenology 2021, 161, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Velasco, A.; Ruiz, S. New Approaches to Assess Fertility in Domestic Animals: Relationship between Arterial Blood Flow to the Testicles and Seminal Quality. Animals 2020, 11, 12. [Google Scholar] [CrossRef]
- Schärz, M.; Ohlerth, S.; Achermann, R.; Gardelle, O.; Roos, M.; Saunders, H.M.; Wergin, M.; Kaser-Hotz, B. Evaluation of Quantified Contrast-Enhanced Color and Power Doppler Ultrasonography for the Assessment of Vascularity and Perfusion of Naturally Occurring Tumors in Dogs. ajvr 2005, 66, 21–29. [Google Scholar] [CrossRef]
- Hofmann, A.G.; Mlekusch, I.; Wickenhauser, G.; Assadian, A.; Taher, F. Clinical Applications of B-Flow Ultrasound: A Scoping Review of the Literature. Diagnostics 2023, 13, 397. [Google Scholar] [CrossRef]
- Morgan, T.A.; Jha, P.; Poder, L.; Weinstein, S. Advanced Ultrasound Applications in the Assessment of Renal Transplants: Contrast-Enhanced Ultrasound, Elastography, and B-Flow. Abdom Radiol 2018, 43, 2604–2614. [Google Scholar] [CrossRef]
- Umemura, A.; Yamada, K. B-Mode Flow Imaging of the Carotid Artery. Stroke 2001, 32, 2055–2057. [Google Scholar] [CrossRef]
- Wachsberg, R.H. B-Flow, a Non-Doppler Technology for Flow Mapping: Early Experience in the Abdomen. Ultrasound Quarterly 2003, 19, 114–122. [Google Scholar] [CrossRef]
- Wachsberg, R.H. B-Flow Imaging of the Hepatic Vasculature: Correlation with Color Doppler Sonography. American Journal of Roentgenology 2007, 188, W522–W533. [Google Scholar] [CrossRef]
- Faustino-Rocha, A.I.; Silva, A.; Gabriel, J.; Teixeira-Guedes, C.I.; Lopes, C.; Gil da Costa, R.; Gama, A.; Ferreira, R.; Oliveira, P.A.; Ginja, M. Ultrasonographic, Thermographic and Histologic Evaluation of MNU-Induced Mammary Tumors in Female Sprague-Dawley Rats. Biomedicine & Pharmacotherapy 2013, 67, 771–776. [Google Scholar] [CrossRef]
- Faustino-Rocha, A.I.; Gama, A.; Oliveira, P.A.; Vanderperren, K.; Saunders, J.H.; Pires, M.J.; Ferreira, R.; Ginja, M. A Contrast-Enhanced Ultrasonographic Study About the Impact of Long-Term Exercise Training on Mammary Tumor Vascularization: Exercise Training and Mammary Tumor Vascularization. J Ultrasound Med 2017, 36, 2459–2466. [Google Scholar] [CrossRef]
- Emanuel, A.L.; Meijer, R.I.; Poelgeest, E.; Spoor, P.; Serné, E.H.; Eringa, E.C. Contrast-enhanced Ultrasound for Quantification of Tissue Perfusion in Humans. Microcirculation 2020, 27. [Google Scholar] [CrossRef] [PubMed]
- Erlichman, D.B.; Weiss, A.; Koenigsberg, M.; Stein, M.W. Contrast Enhanced Ultrasound: A Review of Radiology Applications. Clinical Imaging 2020, 60, 209–215. [Google Scholar] [CrossRef]
- Nyman, H.T.; Kristensen, A.T.; Kjelgaard-Hansen, M.; McEvoy, F.J. Contrast-Enhanced Ultrasonography in Normal Canine Liver. Evaluation of Imaging and Safety Parameters. Veterinary Radiology & Ultrasound 2005, 46, 243–250. [Google Scholar] [CrossRef]
- Canejo-Teixeira, R.; Lima, A.; Santana, A. Applications of Contrast-Enhanced Ultrasound in Splenic Studies of Dogs and Cats. Animals 2022, 12, 2104. [Google Scholar] [CrossRef]
- Correas, J.-M.; Bridal, L.; Lesavre, A.; Méjean, A.; Claudon, M.; Hélénon, O. Ultrasound Contrast Agents: Properties, Principles of Action, Tolerance, and Artifacts. Eur Radiol 2001, 11, 1316–1328. [Google Scholar] [CrossRef] [PubMed]
- Haers, H.; Saunders, J.H. Review of Clinical Characteristics and Applications of Contrast-Enhanced Ultrasonography in Dogs. Journal of the American Veterinary Medical Association 2009, 234, 460–470. [Google Scholar] [CrossRef]
- Volta, A.; Manfredi, S.; Vignoli, M.; Russo, M.; England, G.; Rossi, F.; Bigliardi, E.; Di Ianni, F.; Parmigiani, E.; Bresciani, C.; et al. Use of Contrast-Enhanced Ultrasonography in Chronic Pathologic Canine Testes. Reprod Dom Anim 2014, 49, 202–209. [Google Scholar] [CrossRef]
- Ioanitescu, E.S.; Copaci, I.; Mindrut, E.; Motoi, O.; Stanciu, A.M.; Toma, L.; Iliescu, E.L. Various Aspects of Contrast-Enhanced Ultrasonography in Splenic Lesions—a Pictorial Essay. Med Ultrason 2020, 22. [Google Scholar] [CrossRef]
- Kloth, C.; Kratzer, W.; Schmidberger, J.; Beer, M.; Clevert, D.A.; Graeter, T. Ultrasound 2020—Diagnostics & Therapy: On the Way to Multimodal Ultrasound: Contrast-Enhanced Ultrasound (CEUS), Microvascular Doppler Techniques, Fusion Imaging, Sonoelastography, Interventional Sonography. Rofo 2021, 193, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Bertolotto, M.; Derchi, L.E.; Sidhu, P.S.; Serafini, G.; Valentino, M.; Grenier, N.; Cova, M.A. Acute Segmental Testicular Infarction at Contrast-Enhanced Ultrasound: Early Features and Changes During Follow-Up. American Journal of Roentgenology 2011, 196, 834–841. [Google Scholar] [CrossRef]
- Caretta, N.; Palego, P.; Schipilliti, M.; Torino, M.; Pati, M.; Ferlin, A.; Foresta, C. Testicular Contrast Harmonic Imaging to Evaluate Intratesticular Perfusion Alterations in Patients With Varicocele. Journal of Urology 2010, 183, 263–269. [Google Scholar] [CrossRef]
- Hedayati, V.; Sellars, M.E.; Sharma, D.M.; Sidhu, P.S. Contrast-Enhanced Ultrasound in Testicular Trauma: Role in Directing Exploration, Debridement and Organ Salvage. BJR 2012, 85, e65–e68. [Google Scholar] [CrossRef] [PubMed]
- Valentino, M.; Bertolotto, M.; Derchi, L.; Bertaccini, A.; Pavlica, P.; Martorana, G.; Barozzi, L. Role of Contrast Enhanced Ultrasound in Acute Scrotal Diseases. Eur Radiol 2011, 21, 1831–1840. [Google Scholar] [CrossRef]
- Nagumo, T.; Ishigaki, K.; Yoshida, O.; Sakurai, N.; Terai, K.; Heishima, T.; Asano, K. Quantitative Analysis of Contrast-Enhanced Ultrasound Estimates Intrahepatic Portal Vascularity in Dogs with Single Extrahepatic Portosystemic Shunt. ajvr 2022, 83. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, R.T.; Iani, M.; Matheson, J.; Delaney, F.; Young, K. Contrast Harmonic Ultrasound of Spontaneous Liver Nodules in 32 Dogs. Veterinary Radiology & Ultrasound 2004, 45, 547–553. [Google Scholar] [CrossRef]
- Salwei, R.M.; O’Brien, R.T.; Matheson, J.S. Characterization of Lymphomatous Lymph Nodes in Dogs Using Contrast Harmonic and Power Doppler Ultrasound. Veterinary Radiology & Ultrasound 2005, 46, 411–416. [Google Scholar] [CrossRef]
- Tamura, M.; Ohta, H.; Nisa, K.; Osuga, T.; Sasaki, N.; Morishita, K.; Takiguchi, M. Contrast-enhanced Ultrasonography Is a Feasible Technique for Quantifying Hepatic Microvascular Perfusion in Dogs with Extrahepatic Congenital Portosystemic Shunts. Vet Radiol Ultrasound, 1269. [Google Scholar] [CrossRef]
- Wdowiak, M.; Rychlik, A.; Nieradka, R.; Nowicki, M. Contrast-Enhanced Ultrasonography (CEUS) in Canine Liver Examination. Polish Journal of Veterinary Sciences 2010, 13. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, L.E.; O’Brien, R.T.; Waller, K.R.; Zagzebski, J.A. Quantitative Contrast Harmonic Ultrasound Imaging of Normal Canine Liver. Veterinary Radiology & Ultrasound 2003, 44, 451–454. [Google Scholar] [CrossRef]
- Belotta, A.F.; Gomes, M.C.; Rocha, N.S.; Melchert, A.; Giuffrida, R.; Silva, J.P.; Mamprim, M.J. Sonography and Sonoelastography in the Detection of Malignancy in Superficial Lymph Nodes of Dogs. J Vet Intern Med 2019, 33, 1403–1413. [Google Scholar] [CrossRef]
- Gaschen, L.; Angelette, N.; Stout, R. Contrast-Enhanced Harmonic Ultrasonography of Medial Iliac Lymph Nodes in Healthy Dogs: Contrast-Enhanced Ultrasonography of Lymph Nodes. Veterinary Radiology & Ultrasound 2010, 51, 634–637. [Google Scholar] [CrossRef]
- Choi, S.-Y.; Jeong, W.-C.; Lee, Y.-W.; Choi, H.-J. Contrast Enhanced Ultrasonography of Kidney in Conscious and Anesthetized Beagle Dogs. The Journal of Veterinary Medical Science 2016, 78, 239–244. [Google Scholar] [CrossRef]
- Waller, K.R.; O’Brien, R.T.; Zagzebski, J.A. Quantitative Contrast Ultrasound Analysis of Renal Perfusion in Normal Dogs. Vet Radiol Ultrasound 2007, 48, 373–377. [Google Scholar] [CrossRef]
- Johnson-Neitman, J.L.; O’Brien, R.T.; Wallace, J.D. Quantitative Perfusion Analysis of the Pancreas and Duodenum in Healthy Dogs by Use of Contrast-Enhanced Ultrasonography. ajvr 2012, 73, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Rademacher, N.; Ohlerth, S.; Scharf, G.; Laluhova, D.; Sieber-Ruckstuhl, N.; Alt, M.; Roos, M.; Grest, P.; Kaser-Hotz, B. Contrast-Enhanced Power and Color Doppler Ultrasonography of the Pancreas in Healthy and Diseased Cats. Journal of Veterinary Internal Medicine 2008, 22, 1310–1316. [Google Scholar] [CrossRef] [PubMed]
- Blohm, K.; Hittmair, K.M.; Tichy, A.; Nell, B. Quantitative, Noninvasive Assessment of Intra- and Extraocular Perfusion by Contrast-enhanced Ultrasonography and Its Clinical Applicability in Healthy Dogs. Vet Ophthalmol 2019, 22, 767–777. [Google Scholar] [CrossRef]
- Blohm, K.; Tichy, A.; Nell, B. Clinical Utility, Dose Determination, and Safety of Ocular Contrast-enhanced Ultrasonography in Horses: A Pilot Study. Vet Ophthalmol 2020, 23, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Park, S.; Lee, D.; Cha, A.; Kim, D.; Choi, J. Contrast-Enhanced Ultrasonography for Evaluation of Blood Perfusion in Normal Canine Eyes. Vet Ophthalmol 2019, 22, 31–38. [Google Scholar] [CrossRef]
- Morabito, S.; Di Pietro, S.; Cicero, L.; Falcone, A.; Liotta, L.; Crupi, R.; Cassata, G.; Macrì, F. Impact of Region-of-Interest Size and Location on Quantitative Contrast-Enhanced Ultrasound of Canine Splenic Perfusion. BMC Vet Res 2021, 17, 271. [Google Scholar] [CrossRef]
- Nakamura, K.; Sasaki, N.; Yoshikawa, M.; Ohta, H.; Hwang, S.-J.; Mimura, T.; Yamasaki, M.; Takiguchi, M. Quantitative Contrast-Enhanced Ultrasonography of Canine Spleen. Veterinary Radiology & Ultrasound 2009, 50, 104–108. [Google Scholar] [CrossRef]
- Nakamura, K.; Sasaki, N.; Murakami, M.; Bandula Kumara, W.R.; Ohta, H.; Yamasaki, M.; Takagi, S.; Osaki, T.; Takiguchi, M. Contrast-Enhanced Ultrasonography for Characterization of Focal Splenic Lesions in Dogs: Contrast Ultrasound of Splenic Lesions. Journal of Veterinary Internal Medicine 2010, 24, 1290–1297. [Google Scholar] [CrossRef] [PubMed]
- Ohlerth, S.; Rüefli, E.; Poirier, V.; Roos, M.; Kaser-Hotz, B. Contrast Harmonic Imaging of the Normal Canine Spleen. Vet Radiol Ultrasound 2007, 48, 451–456. [Google Scholar] [CrossRef]
- Krg̈er Hagen, E.; Forsberg, F.; Liu, J.-B.; Gomella, L.G.; Aksnes, A.-K.; Merton, D.A.; Johnson, D.; Goldberg, B.B. Contrast-Enhanced Power Doppler Imaging of Normal and Decreased Blood Flow in Canine Prostates. Ultrasound in Medicine & Biology 2001, 27, 909–913. [Google Scholar] [CrossRef]
- Russo, M.; Vignoli, M.; Catone, G.; Rossi, F.; Attanasi, G.; England, G. Prostatic Perfusion in the Dog Using Contrast-Enhanced Doppler Ultrasound. Reproduction in Domestic Animals 2009, 44, 334–335. [Google Scholar] [CrossRef] [PubMed]
- Russo, M.; Vignoli, M.; England, G. B-Mode and Contrast-Enhanced Ultrasonographic Findings in Canine Prostatic Disorders. Reprod Domest Anim 2012, 47, 238–242. [Google Scholar] [CrossRef]
- Troisi, A.; Orlandi, R.; Bargellini, P.; Menchetti, L.; Borges, P.; Zelli, R.; Polisca, A. Contrast-Enhanced Ultrasonographic Characteristics of the Diseased Canine Prostate Gland. Theriogenology 2015, 84, 1423–1430. [Google Scholar] [CrossRef]
- Vignoli, M.; Russo, M.; Catone, G.; Rossi, F.; Attanasi, G.; Terragni, R.; Saunders, J.; England, G. Assessment of Vascular Perfusion Kinetics Using Contrast-Enhanced Ultrasound for the Diagnosis of Prostatic Disease in Dogs: Prostatic Perfusion Kinetics Assessed by CEUS. Reproduction in Domestic Animals 2011, 46, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Hillaert, A.; Stock, E.; Duchateau, L.; de Rooster, H.; Devriendt, N.; Vanderperren, K. B-Mode and Contrast-Enhanced Ultrasonography Aspects of Benign and Malignant Superficial Neoplasms in Dogs: A Preliminary Study. Animals 2022, 12, 2765. [Google Scholar] [CrossRef] [PubMed]
- Hillaert, A.; Stock, E.; Favril, S.; Duchateau, L.; Saunders, J.H.; Vanderperren, K. Intra- and Inter-Observer Variability of Quantitative Parameters Used in Contrast-Enhanced Ultrasound of Kidneys of Healthy Cats. Animals 2022, 12, 3557. [Google Scholar] [CrossRef] [PubMed]
- Rademacher, N.; Schur, D.; Gaschen, F.; Kearney, M.; Gaschen, L. Contrast-Enhanced Ultrasonography of the Pancreas in Healthy Dogs and in Dogs with Acute Pancreatitis: Contrast-Enhanced Ultrasound in Canine Pancreatitis. Veterinary Radiology & Ultrasound 2016, 57, 58–64. [Google Scholar] [CrossRef]
- Ophir, J.; Céspedes, I.; Ponnekanti, H.; Yazdi, Y.; Li, X. Elastography: A Quantitative Method for Imaging the Elasticity of Biological Tissues. Ultrason Imaging 1991, 13, 111–134. [Google Scholar] [CrossRef] [PubMed]
- Correas; Drakonakis, E. ; Isidori, A.M.; Hélénon, O.; Pozza, C.; Cantisani, V.; Di Leo, N.; Maghella, F.; Rubini, A.; Drudi, F.M.; et al. Update on Ultrasound Elastography: Miscellanea. Prostate, Testicle, Musculo-Skeletal. European Journal of Radiology 2013, 82, 1904–1912. [Google Scholar] [CrossRef]
- Bamber, J.; Cosgrove, D.; Dietrich, C.; Fromageau, J.; Bojunga, J.; Calliada, F.; Cantisani, V.; Correas, J.-M.; D’Onofrio, M.; Drakonaki, E.; et al. EFSUMB Guidelines and Recommendations on the Clinical Use of Ultrasound Elastography. Part 1: Basic Principles and Technology. Ultraschall in Med 2013, 34, 169–184. [Google Scholar] [CrossRef]
- Sigrist, R.M.S.; Liau, J.; Kaffas, A.E.; Chammas, M.C.; Willmann, J.K. Ultrasound Elastography: Review of Techniques and Clinical Applications. Theranostics 2017, 7, 1303–1329. [Google Scholar] [CrossRef]
- Li, Y.; Snedeker, J.G. Elastography: Modality-Specific Approaches, Clinical Applications, and Research Horizons. Skeletal Radiol 2011, 40, 389–397. [Google Scholar] [CrossRef]
- Barr, R.G. Sonographic Breast Elastography: A Primer. Journal of Ultrasound in Medicine 2012, 31, 773–783. [Google Scholar] [CrossRef]
- Itoh, A.; Ueno, E.; Tohno, E.; Kamma, H.; Takahashi, H.; Shiina, T.; Yamakawa, M.; Matsumura, T. Breast Disease: Clinical Application of US Elastography for Diagnosis. Radiology 2006, 239, 341–350. [Google Scholar] [CrossRef]
- Rouvière, O.; Melodelima, C.; Hoang Dinh, A.; Bratan, F.; Pagnoux, G.; Sanzalone, T.; Crouzet, S.; Colombel, M.; Mège-Lechevallier, F.; Souchon, R. Stiffness of Benign and Malignant Prostate Tissue Measured by Shear-Wave Elastography: A Preliminary Study. Eur Radiol 2017, 27, 1858–1866. [Google Scholar] [CrossRef]
- Goddi, A.; Sacchi, A.; Magistretti, G.; Almolla, J.; Salvadore, M. Real-Time Tissue Elastography for Testicular Lesion Assessment. Eur Radiol 2012, 22, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Muršić, M. The Role of Ultrasound Elastography in the Diagnosis of Pathologic Conditions of Testicles and Scrotum. ACC 2021. [Google Scholar] [CrossRef] [PubMed]
- Rocher, L.; Criton, A.; Gennisson, J.-L.; Izard, V.; Ferlicot, S.; Tanter, M.; Benoit, G.; Bellin, M.F.; Correas, J.-M. Testicular Shear Wave Elastography in Normal and Infertile Men: A Prospective Study on 601 Patients. Ultrasound in Medicine & Biology 2017, 43, 782–789. [Google Scholar] [CrossRef]
- Holdsworth, A.; Bradley, K.; Birch, S.; Browne, W.J.; Barberet, V. Elastography of the Normal Canine Liver, Spleen and Kidneys: Canine Elastography. Vet Radiol Ultrasound 2014, 55, 620–627. [Google Scholar] [CrossRef]
- Jeon, S.; Lee, G.; Lee, S.-K.; Kim, H.; Yu, D.; Choi, J. Ultrasonographic Elastography of the Liver, Spleen, Kidneys, and Prostate in Clinically Normal Beagle Dogs: Ultrasonographicx Elastography in Normal Dogs. Vet Radiol Ultrasound 2015, 56, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Feliciano, M.A.R.; Maronezi, M.C.; Simões, A.P.R.; Uscategui, R.R.; Maciel, G.S.; Carvalho, C.F.; Canola, J.C.; Vicente, W.R.R. Acoustic Radiation Force Impulse Elastography of Prostate and Testes of Healthy Dogs: Preliminary Results. J Small Anim Pract 2015, 56, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Cintra, C.A.; Feliciano, M.A.R.; Santos, V.J.C.; Maronezi, M.C.; Cruz, I.K.; Gasser, B.; Silva, P.; Crivellenti, L.Z.; Uscategui, R.A.R. Applicability of ARFI Elastography in the Evaluation of Canine Prostatic Alterations Detected by B-Mode and Doppler Ultrasonography. Arq. Bras. Med. Vet. Zootec. 2020, 72, 2135–2140. [Google Scholar] [CrossRef]
- Fernandez, S.; Feliciano, M.A.R.; Borin-Crivellenti, S.; Crivellenti, L.Z.; Maronezi, M.C.; Simões, A.P.R.; Silva, P.D.A.; Uscategui, R.R.; Cruz, N.R.N.; Santana, A.E.; et al. Acoustic Radiation Force Impulse (ARFI) Elastography of Adrenal Glands in Healthy Adult Dogs. Arq. Bras. Med. Vet. Zootec. 2017, 69, 340–346. [Google Scholar] [CrossRef]
- Brizzi, G.; Crepaldi, P.; Roccabianca, P.; Morabito, S.; Zini, E.; Auriemma, E.; Zanna, G. Strain Elastography for the Assessment of Skin Nodules in Dogs. Vet Dermatol 2021, 32, 272. [Google Scholar] [CrossRef]
- Favril, S.; Stock, E.; Broeckx, B.J.G.; Devriendt, N.; de Rooster, H.; Vanderperren, K. Shear Wave Elastography of Lymph Nodes in Dogs with Head and Neck Cancer: A Pilot Study. Vet Comparative Oncology 2022, 20, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.; Yang, S.; Suh, G.; Choi, J. Correlating Two-Dimensional Shear Wave Elastography of Acute Pancreatitis with Spec CPL in Dogs. J Vet Sci 2022, 23, e79. [Google Scholar] [CrossRef] [PubMed]
- Spużak, J.; Kubiak, K.; Glińska-Suchocka, K.; Jankowski, M.; Borusewicz, P.; Kubiak-Nowak, D. Accuracy of Real-Time Shear Wave Elastography in the Assessment of Normal Small Intestine Mucosa in Dogs. 2019. [CrossRef]
- Rodrigues Simões, A.P.; Cristina Maronezi, M.; Andres Ramirez Uscategui, R.; Garcia Kako Rodrigues, M.; Sitta Gomes Mariano, R.; Tavares de Almeida, V.; José Correia Santos, V.; Del Aguila da Silva, P.; Ricardo Russiano Vicente, W.; Antonio Rossi Feliciano, M. Placental ARFI Elastography and Biometry Evaluation in Bitches. Animal Reproduction Science 2020, 214, 106289. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues Simões, A.P.; Rossi Feliciano, M.A.; Maronezi, M.C.; Uscategui, R.A.R.; Bartlewski, P.M.; de Almeida, V.T.; Oh, D.; do Espírito Santo Silva, P.; da Silva, L.C.G.; Russiano Vicente, W.R. Elastographic and Echotextural Characteristics of Foetal Lungs and Liver during the Final 5 Days of Intrauterine Development in Dogs. Animal Reproduction Science 2018, 197, 170–176. [Google Scholar] [CrossRef]
- Feliciano, M.A.R.; Maronezi, M.C.; Pavan, L.; Castanheira, T.L.; Simões, A.P.R.; Carvalho, C.F.; Canola, J.C.; Vicente, W.R.R. ARFI Elastography as a Complementary Diagnostic Method for Mammary Neoplasia in Female Dogs—Preliminary Results. J Small Anim Pract 2014, 55, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Glińska-Suchocka, K.; Jankowski, M.; Kubiak, K.; Spużak, J.; Nicpon, J. Application of Shear Wave Elastography in the Diagnosis of Mammary Gland Neoplasm in Dogs. Polish Journal of Veterinary Sciences 2013, 16, 477–482. [Google Scholar] [CrossRef]
- Massimini, M.; Gloria, A.; Romanucci, M.; Della Salda, L.; Di Francesco, L.; Contri, A. Strain and Shear-Wave Elastography and Their Relationship to Histopathological Features of Canine Mammary Nodular Lesions. Veterinary Sciences 2022, 9, 506. [Google Scholar] [CrossRef]
- de Brito; Feliciano; Coutinho ARFI Elastography of Healthy Adults Felines Testes. Acta Scientiae Veterinariae 2015, 43.
- Feliciano, M.A.R.; Maronezi, M.C.; Simões, A.P.R.; Maciel, G.S.; Pavan, L.; Gasser, B.; Silva, P.; Uscategui, R.R.; Carvalho, C.F.; Canola, J.C.; et al. Acoustic Radiation Force Impulse (ARFI) Elastography of Testicular Disorders in Dogs: Preliminary Results. Arq. Bras. Med. Vet. Zootec. 2016, 68, 283–291. [Google Scholar] [CrossRef]
- Glińska-Suchocka, K.; Jankowski, M.; Kubiak, K.; Spużak, J.; Dzimira, S. Sonoelastography in Differentiation of Benign and Malignant Testicular Lesion in Dogs. 2014.
Figure 1.
Example of B-Mode ultrasonography of normal testis in the dog, in longitudinal (A) and transversal (B) scan. The hyperechoic mediastinum is visible as a band (A) or a circular area (B) within the homogeneous parenchyma.
Figure 1.
Example of B-Mode ultrasonography of normal testis in the dog, in longitudinal (A) and transversal (B) scan. The hyperechoic mediastinum is visible as a band (A) or a circular area (B) within the homogeneous parenchyma.
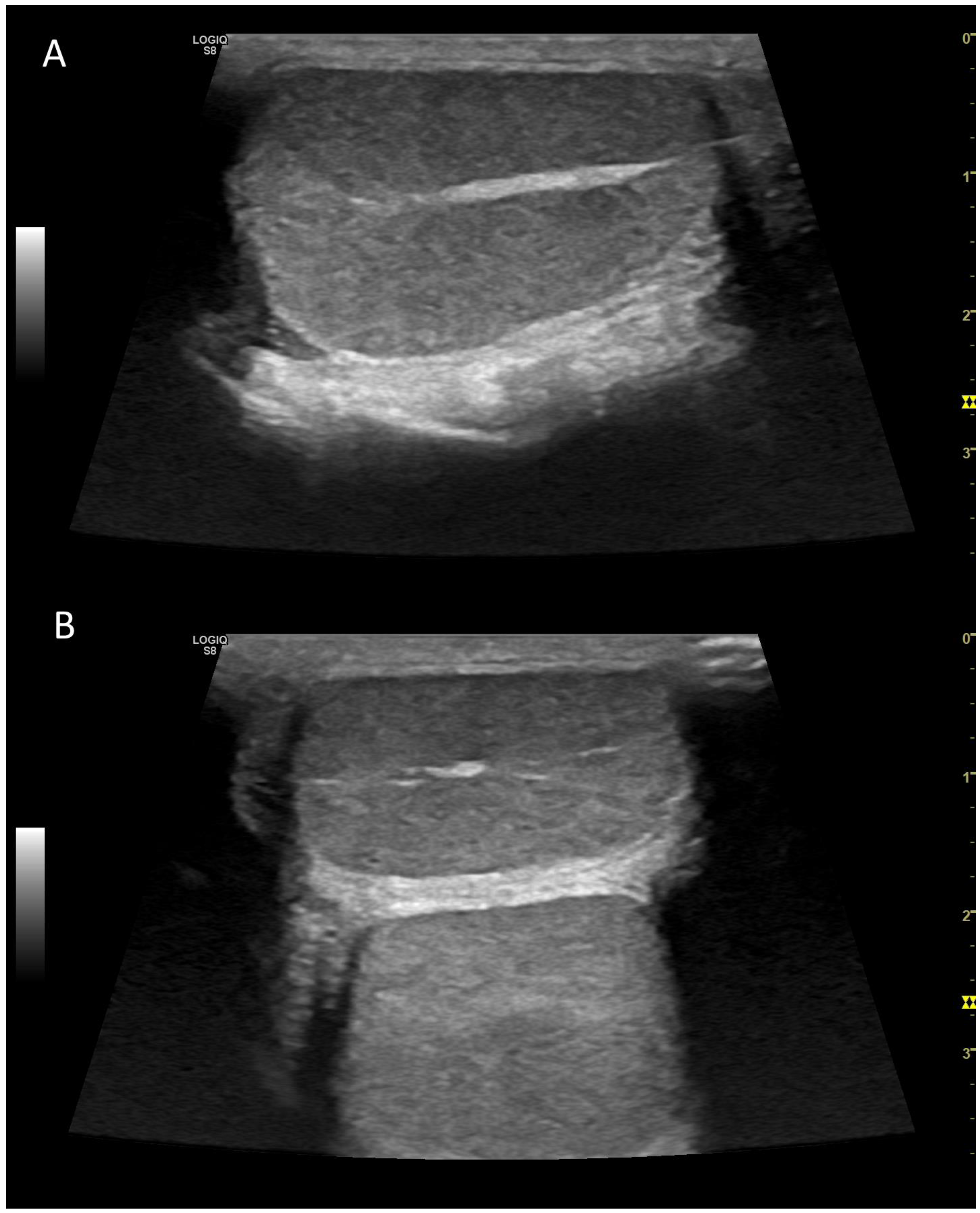
Figure 2.
Example of B-Mode ultrasonography of normal epididymis in the dog. Normal tail of the epididymis, isoechoic, could be detected on the right of the image, closely adherent to the testis (on the left).
Figure 2.
Example of B-Mode ultrasonography of normal epididymis in the dog. Normal tail of the epididymis, isoechoic, could be detected on the right of the image, closely adherent to the testis (on the left).
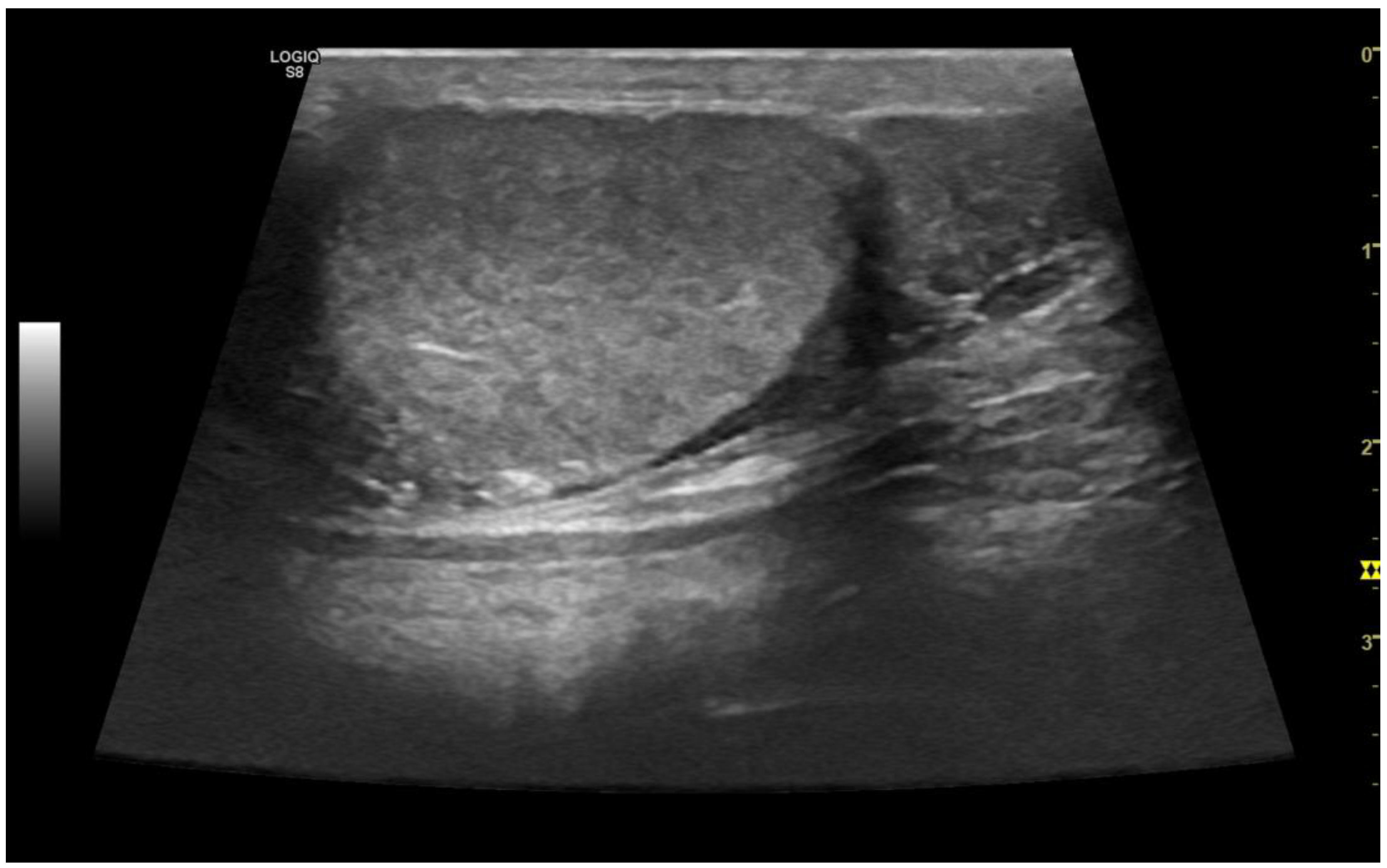
Figure 3.
A case of epididymitis, contextual with orchitis, in canine testis involving the tail of the epididymis. Note the relative hypertrophy of the tail of epididymis (on the right) compared with the correspondent testis (on the left). Both organs appeared heterogeneous, and small anechoic areas could be detected (white arrows).
Figure 3.
A case of epididymitis, contextual with orchitis, in canine testis involving the tail of the epididymis. Note the relative hypertrophy of the tail of epididymis (on the right) compared with the correspondent testis (on the left). Both organs appeared heterogeneous, and small anechoic areas could be detected (white arrows).
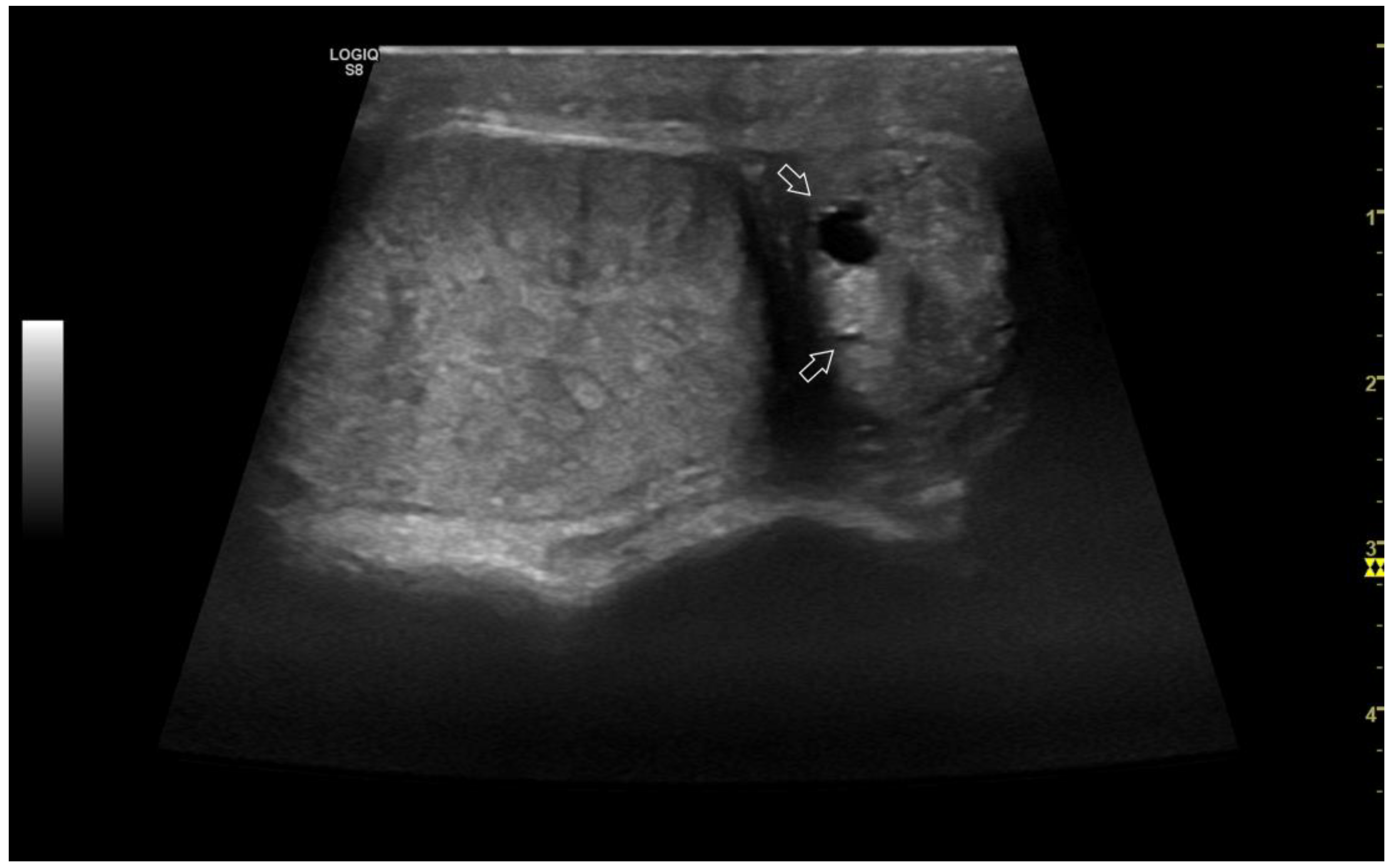
Figure 4.
Representative sonogram in color Doppler of canine testis. Note the marginal portion (black arrow) and the intratesticular branches (white arrows) of the testicular artery.
Figure 4.
Representative sonogram in color Doppler of canine testis. Note the marginal portion (black arrow) and the intratesticular branches (white arrows) of the testicular artery.
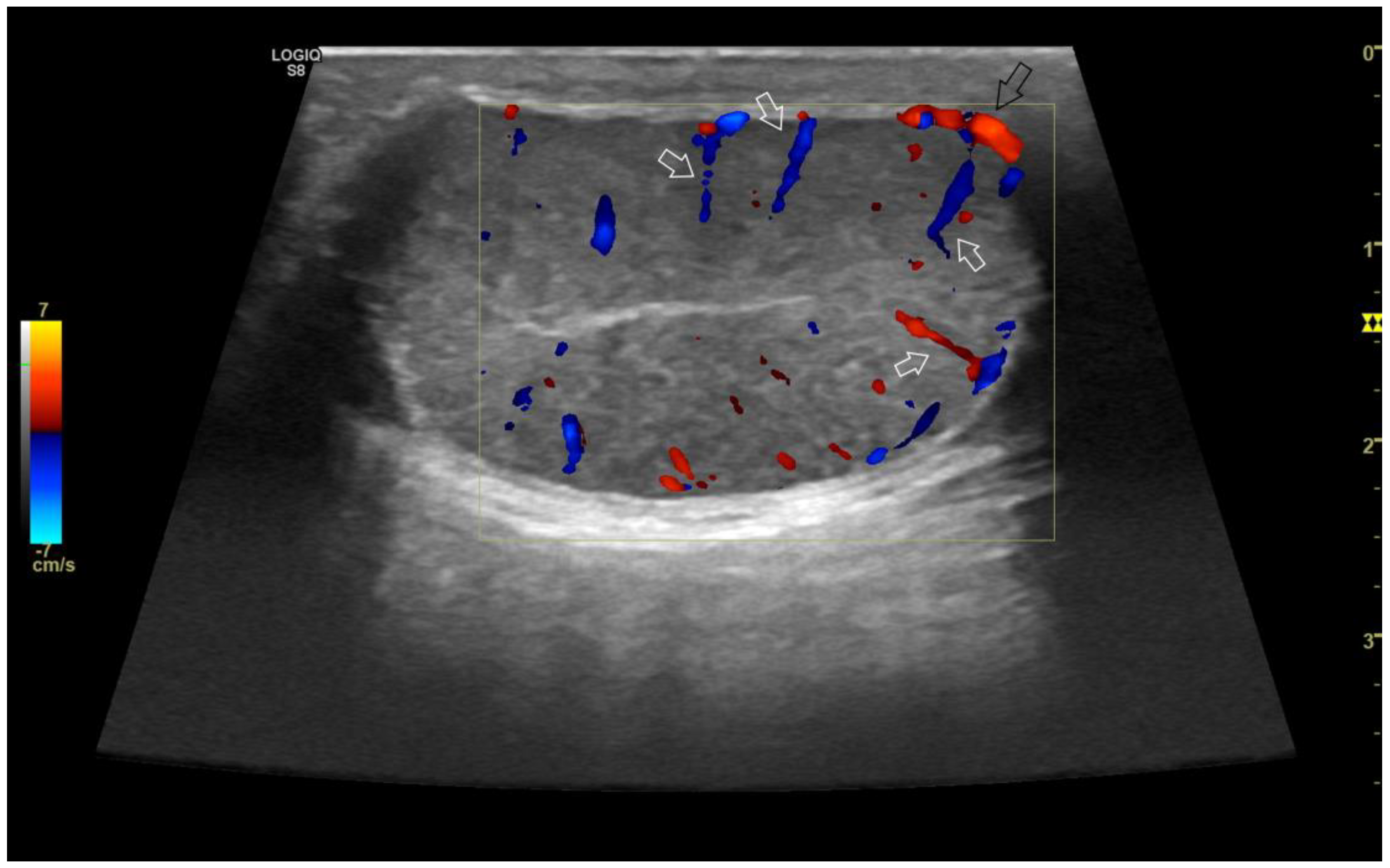
Figure 5.
Pulse wave Doppler parameters measured on the supratesticular (A) and marginal (B) portion of the testicular artery.
Figure 5.
Pulse wave Doppler parameters measured on the supratesticular (A) and marginal (B) portion of the testicular artery.
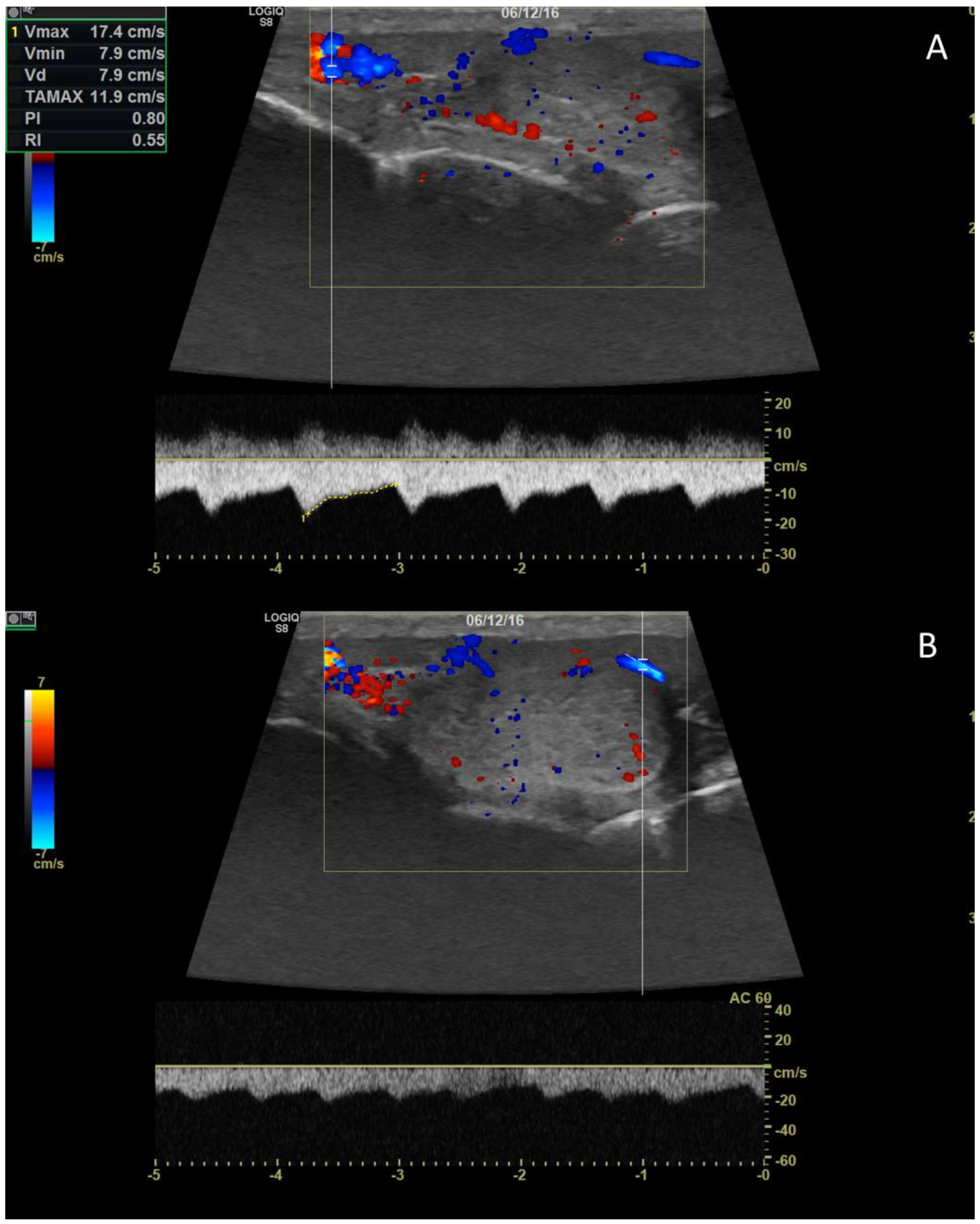
Figure 6.
Representative image of the B-Flow evaluation of canine testis.
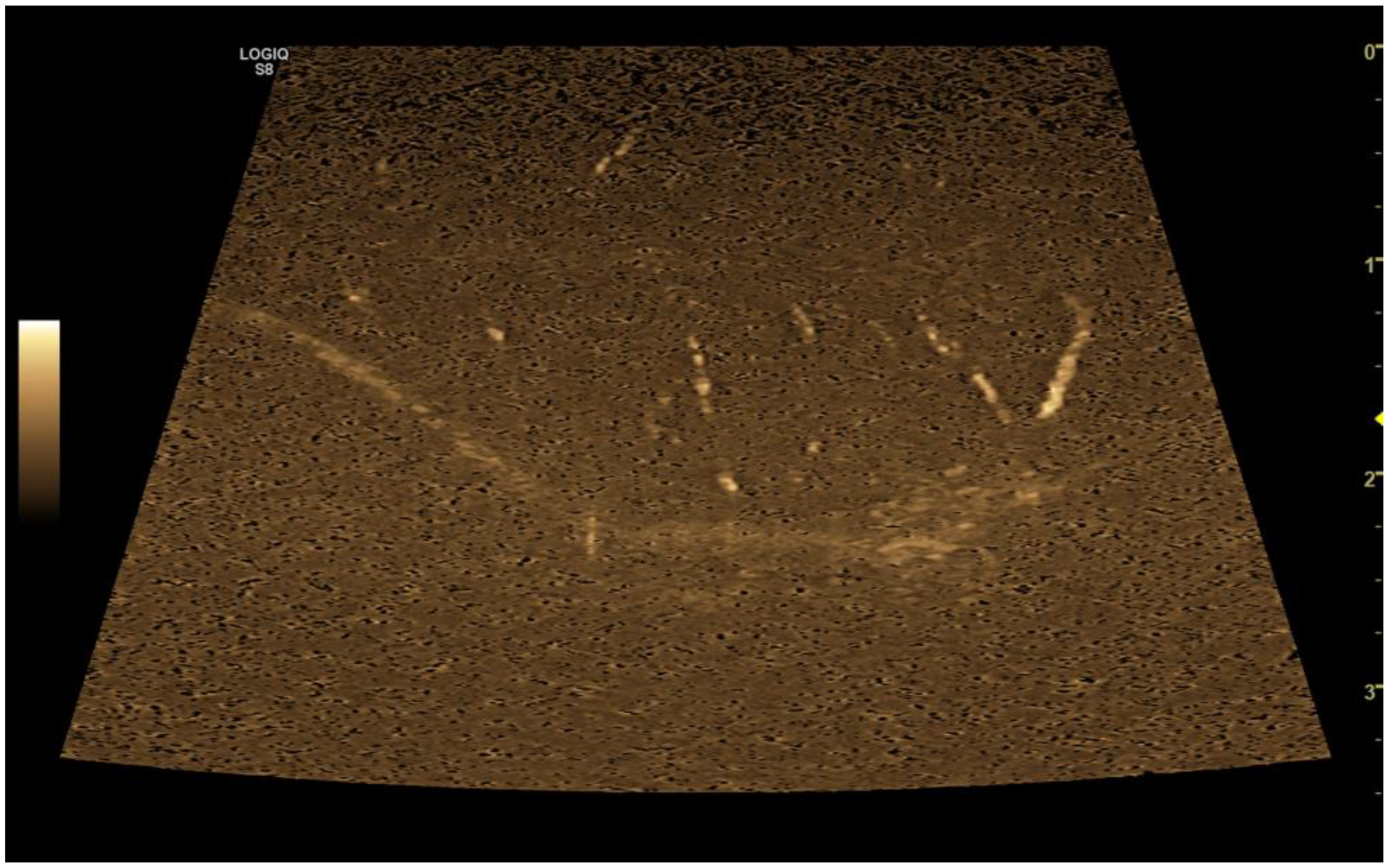
Figure 7.
Representative elastogram acquired with the qualitative strain elastography of canine testis (B) compared with B-Mode ultrasonography (A). The color scale differentiates hard (blue) and soft (red) area of the testis. The green bar in the center of the image represents the adequateness of the free-hand compression applied by the operator.
Figure 7.
Representative elastogram acquired with the qualitative strain elastography of canine testis (B) compared with B-Mode ultrasonography (A). The color scale differentiates hard (blue) and soft (red) area of the testis. The green bar in the center of the image represents the adequateness of the free-hand compression applied by the operator.
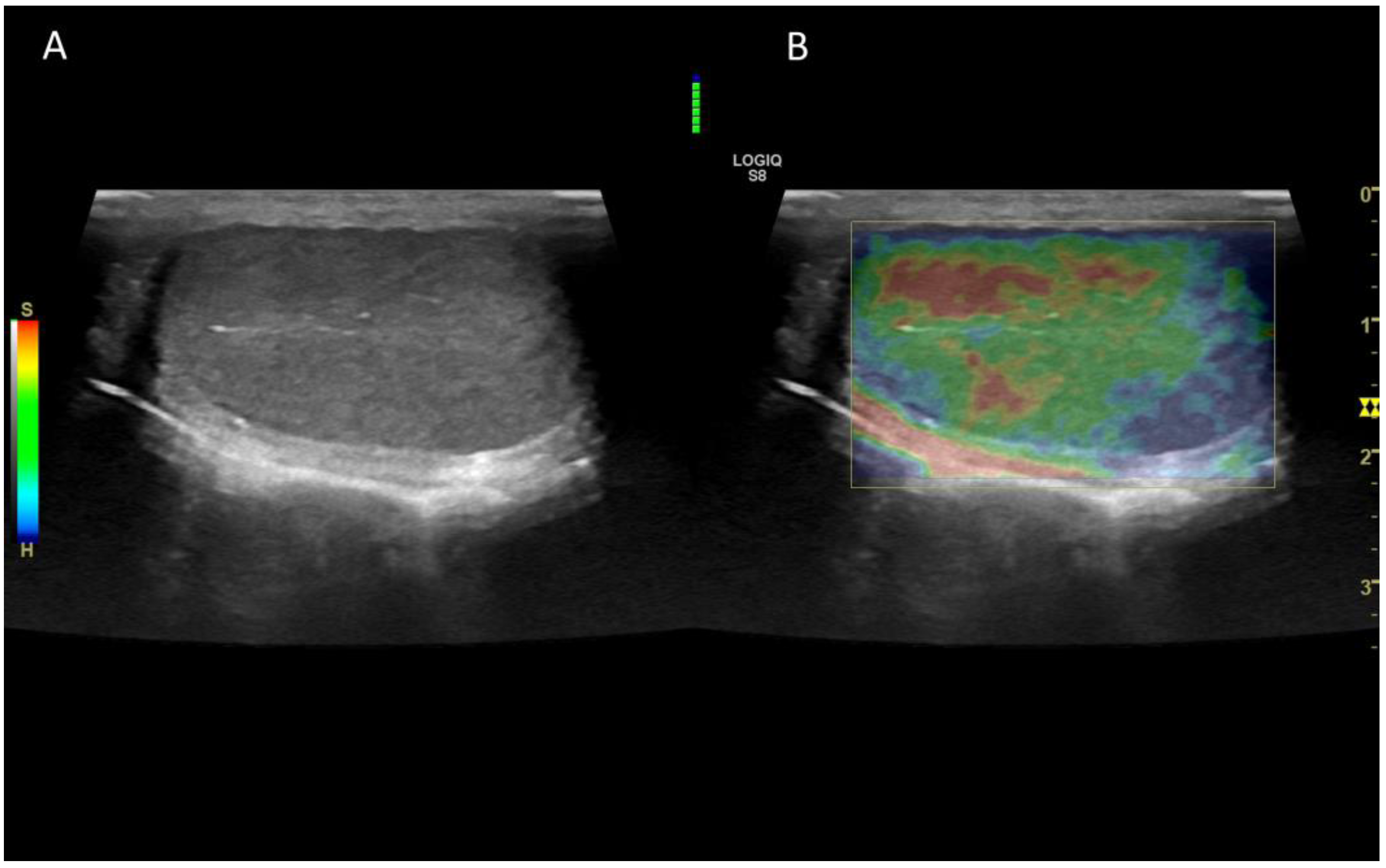
Figure 8.
Representative elastogram acquired with the quantitative shear-wave elastography of canine testis (B) compared with B-Mode ultrasonography (A). The technology is able to quantify the stiffness in objective manner.
Figure 8.
Representative elastogram acquired with the quantitative shear-wave elastography of canine testis (B) compared with B-Mode ultrasonography (A). The technology is able to quantify the stiffness in objective manner.
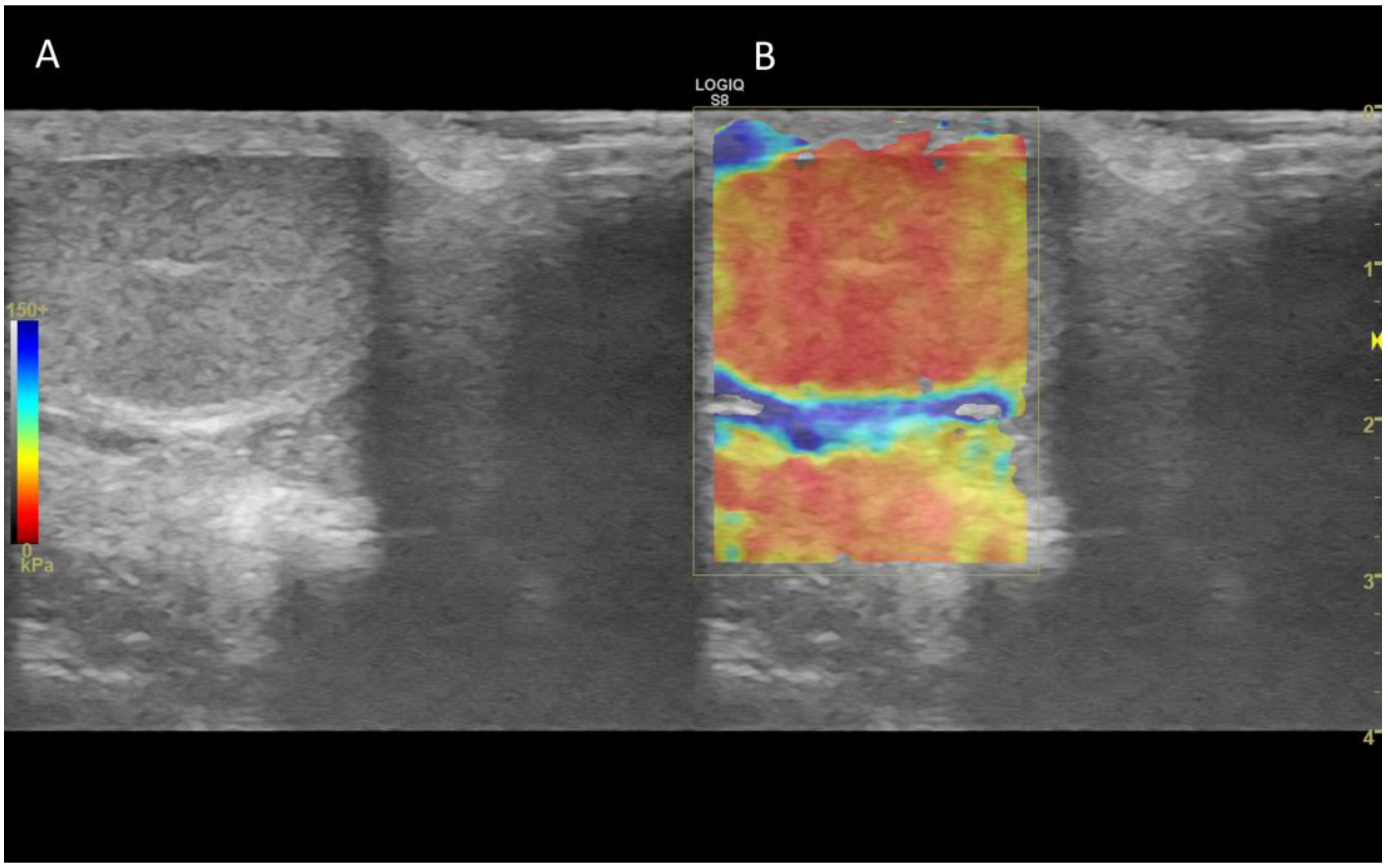
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



