
Submitted:
01 June 2023
Posted:
02 June 2023
You are already at the latest version
Abstract
Type 2 diabetes mellitus may be complicated with chronic complications including diabetic neuropathy (DN). Timely diagnosis is crucial in treatment and maybe reversal of this complication. C reactive protein to albumin ratio (CAR) is considered as a marker of inflammation in various diseases that characterized with acute or chronic inflammation. Since diabetic neuropathy and type 2 diabetes mellitus are also associated with chronic, low grade inflammation, we aimed to study CAR levels of type 2 diabetic subjects with diabetic neuropathy and to compare to those in patients without diabetic neuropathy. Type 2 diabetic patients presented to our institutional outpatient clinics were divided into two according to the presence of DN. Subjects with DN were listed as DN group and others were as non-DN group. Characteristics and laboratory data, including CAR, in DN and non-DN groups were compared. Median CAR of the DN and non-DN groups were 2,19 (0,2-49)% and 0,56 (0,02-5,8)%, respectively (p<0.001). CAR was significantly and positively correlated with age (r=0.15, p<0.001), weight (r=0.19, p=0.01), BMI (r=0.11, p=0.03), waist circumference (r=0.10, p=0.046), fasting plasma glucose (r=0.14, p=0.004), serum creatinine (r=0.25, p<0.001), triglyceride (r=0.17, p<0.001), and LDL-cholesterol (r=0.13, p=0.001) levels. Moreover, CAR was inversely correlated with eGFR levels (r=-0.16, p<0.001). The sensitivity and specificity of CAR (when higher than 1,02%) in predicting diabetic neuropathy were 78% and 73%, respectively (AUC: 0.84, p<0.001, 95% CI: 0,82-0,87). Moreover, high CAR level was an independent risk factor of diabetic neuropathy (p<0.001, OR: 1.34, 95% CI: 0.48-1.62). In conclusion, elevated CAR levels could be considered as a marker of diabetic neuropathy.
Keywords:
type 2 diabetes mellitus
; diabetic neuropathy
; inflammation
; C reactive protein to albumin ratio
1. Introduction
Type 2 Diabetes mellitus is associated with insulin resistance and chronic hyperglycemia. It is by far the most common type of diabetes mellitus and it constitutes 90-95% of all diabetic patients [1]. Insulin is an essential hormone that produced in beta cells in the pancreas. Insulin facilitates glucose intake of the cells from blood, where it is utilized for energy production or stored as glycogen. Resistance to insulin action in target tissues may result in hyperinsulinism, which eventually progress to impaired secretion of the hormone. Development of type 2 diabetes mellitus, probably the most common metabolic condition, is either caused by deteriorated response of peripheral tisues to insulin or defective secretion of insulin from pancreatic β-cells. Insulin is also an essential hormone in the metabolism of fats and proteins. Therefore, insulin deficiency or insulin resistance leads to hyperglycemia, hyperlipidemia and other laboratory and clinical manifestation of diabetes mellitus. Yet, most of the patients are asymptomatic at presentation and are diagnosed by the presence of hyperglycemia in the routine laboratory evaluation and subsequent tests. The rate of type 2 diabetes mellitus diagnosis is increased and the rate of symptomatic disease decreased with efforts to diagnose type 2 diabetes mellitus earlier through screening tests [2]. Injury of major organs and systems, including cardiovascular diseases, diabetic kidney injury, diabetic foot ulcers, diabetic retinopathy, and diabetic neuropathy may occur when hyperglycemia persists in diabetic subjects [3]. Unfortunately, most of the diabetic patients have at least one of these macrovascular or microvascular complications of the disease and of those, cardiovascular events are the leading cause of mortality in diabetic population [4]. However, if appropriate management of diabetes is provided, these serious complications can be delayed or completely avoided [5].
Type 2 diabetes mellitus is usually accompanied by other conditions such as hypertension, dyslipidemia, and central obesity. Thus, it can be considered as a part of Syndrome X or so called metabolic syndrome [6]. Processes of insulin production and secretion are controlled strictly, since the balance of blood glucose depend mainly to release and action of insulin. Metabolic imbalance which could progress to type 2 diabetes mellitus may be driven by any defects in these processes [7].
Recent researches have focused on the role of inflammation as a link between obesity, atherosclerosis, and type 2 diabetes mellitus [8]. Commonly used inflammatory markers including C-reactive protein (CRP), IL-6, plasminogen activator inhibitor-1 (PAI-1), and tumor necrosis factor-alpha (TNF-alpha) were reported to be associated with incidence of type 2 diabetes mellitus [9]. In addition, chemokines or so called chemotactic pro-inflammatory cytokines [10], white blood cell count in blood [11], and adipokines (the inflammatory factors released from adipose tissue) [12], were also observed to stimulate inflammatory activity in subjects with insulin resistance. Studies on these inflammatory cytokines found that is subject have shown that serum levels of the cytokines are reduced by intensive lifestyle interventions [13]. Anti-diabetic drugs such as thiazolidinediones and lipid-lowering agents such as statins have additional therapeutic benefits due to their anti-inflammatory actions [14]. Moreover, a lower incidence of diabetes has been noted in subjects with psoriasis or rheumatoid arthritis, who are on anti-inflammatory and disease-modifying anti-rheumatic drugs compared to those using other medicines [15].
Long-term intracellular hyperglycemia leads to complications mainly arising from the kidneys, eyes and nervous system by disrupting the microvascular structure. It is estimated that up to 25% of patients have already developed one or more diabetic complications at the time of initial diagnosis of type 2 diabetes mellitus [3]. Hence screening for the disease has great importance in sake of establishing the diagnosis as early as possible. One of these complications is diabetic neuropathy which is the most frequently seen type of peripheral neuropathies in developed countries [16].
Diabetic neuropathy is one of the most common complications of diabetes that can lead to pain, loss of sensation, and limb amputation, hence impair the quality of life [17]. Diabetic neuropathy has a complex pathophysiology and it affects both components (autonomic and somatic) of the nervous system. Neuropathic pain, tingling, paraesthesia, numbness and burning feeling is characterized symptoms of diabetic neuropathy. These symptoms mainly occur in toes, feet, or legs. The complication has been defined as a peripheral nerve disorder that may develop due to genetic, traumatic, toxic, metabolic or infectious factors in diabetic subjects. Nearly half of the population with type 2 diabetes mellitus suffer from diabetic neuropathy and the estimated number of the diabetic subjects with this complication by the year 2045 is 350 million [18]. Underlying mechanisms of diabetic neuropathy development is not fully clear and often complex and related with multiple factors. Some of these factors are metabolic disturbance especially blood glucose alterations, inflammation, involvement of reactive oxygen species, polyol pathway, diacylglycerol/protein kinase C pathway, dysfunction in the endothelium, overproduction and accumulation of advanced glycosylation products, and deteriorated regulation of neurothropic proteins [19]. The inflammation in the nerve cells is triggered by advanced glycosylation end products via activation of nuclear factor kappa beta, interleukins, nitric oxide synthase, and tumor necrosis factor- alpha [20]. In diabetic neuropathy, this inflammation at the cellular level causes other inflammatory cells to come to the area, causing the inflammatory cytokines they secrete to turn the environment into a place of fire. Within the nerve cells, ischemia and hypoxia develop, resulting in mitochondrial dysfunction and excessive production of reactive oxygen species [21].
The polyol aldose reductase pathway is one of the bypass metabolic pathways of glucose and is activated due to high blood glucose. In this pathway, aldose reductase enhances production of sorbitol from glucose and sorbitol dehydrogenase converts sorbitol to fructose [22]. Fructokinase enzyme is absent in neural tissues, therefore, fructose accumulates in neural cells. On the other hand, sorbitol slowly spreads around and it also accumulates in these cells. Elevated levels of intracellular fructose and sorbitol promote increased osmotic pressure in neural cell membranes which deteriorates inositol and taurine balance of the neural cells [23]. Inositol takes part in detoxification of free oxygen species and moreover, involves in phospholipid metabolism. Reactive oxygen radicals cannot be scavenged adequately when inositol levels are depleted, thus, conduction of the nerve is decelerated due to decreased activity of Na/K ATPase [23]. On the other hand, increased levels of glucose in blood block the inositol transport into nerve cells. As a result, nerve cells lose a lot of the inositol they have. Not only depletion of inositol but also reduction of taurine contributes to the diabetic neuropathy in patients with type 2 diabetes mellitus. Taurine is an anti-oxidant and transmitter of neural tissues which also involves in calcium regulation in cellular level. Neural cells swell, degenerate and even become necrotic when taurine levels decrease which all together cause diabetic peripheral neuropathy [24]. Another molecule that involve in neuropathy in diabetic subjects is nicotinamide adenine dinucleotide phosphate, which is reduced to the biochemical reactions that convert glucose to sorbitol. Conversion of glutathione disulfide to glutathione is limited and activity of nitric oxide synthase is inhibited because of the reduced cellular levels of nicotinamide adenine dinucleotide phosphate. Finally, free radicals cannot be removed properly from the micro-environment and production of reactive oxygen species is increased [23]. Another biochemical reaction that involves in neural damage in patients with type 2 diabetes mellitus is catalyzed by succinate dehydrogenase. Nicotinamide adenine dinucleotide is converted to its reduced form (NADH) by this enzyme and formation of superoxide takes place in the mitochondria, which increase oxidative stress within the cell [25]. As a result, these pathways cause a decrease in the redox capacity of nerve cells and cell damage due to both the consumption of glutathione and the production of reactive oxygen derivatives.
Diabetic neuropathy is also one of the leading causes of morbidity related to the type 2 diabetes mellitus. Complications related with diabetic foot including infection, ulceration, ischemia, gangrene and amputation are usually occur because of diabetic neuropathy as a precipitating factor [26]. Both diabetic neuropathy and related complications that mentioned above reduces the quality of life of the diabetic patients and impose a great socioeconomic burden on healthcare systems [26]. Annual cost of the diabetic subjects with diabetic neuropathy is 2 to 4 times higher than the diabetic patients without neuropathy [27]. It increases the risk of diabetic foot ulcers and limb amputations. Therefore, yearly examination and evaluation for diabetic neuropathy is recommended in diabetic population. In addition to routine physical examination, monofilament and tuning fork tests are used in neuropathy assessment. Moreover, electrophysiological findings obtained by standard electromyography (EMG) are used in the diagnosis of diabetic neuropathy. Abnormalities in nerve conduction tests are often the first concrete sign of this diabetic microvascular complication. First signs of neuropathy after the onset of hyperglycemia include dysfunctions such as decreased sensory nerve and motor nerve conduction velocities, increased sensitivity to pain and painful response to even normal stimuli. If autonomic neuropathy is suspected, extensive examination of the systems should be performed. Tight glycemic regulation should be ensured to prevent disease progression right after the establishment of diabetic peripheral neuropathy diagnosis. The benefit of maintaining glycemic control to prevent the progression of neuropathy is prominent in the patients with type 1 diabetes mellitus, however, no benefit was obvious in subjects with type 2 diabetes mellitus [28]. There are studies indicating that axonopathy, demyelination, nerve degeneration and sensitivity to pain decrease as the disease progresses.
Although the mechanisms that cause diabetic neuropathy have been well-established, the effective treatment method of this complication is not fully understood. Current treatment of diabetic neuropathy focused on symptomatic relief since there is no specific treatment option for this complication [29]. Hence, establishing the diagnosis as early as possible following with strict glucose control remains the only effective strategy for diabetic neuropathy.
These accumulating evidences suggest that diabetic peripheral neuropathy is associated with increased burden of inflammation. On the other hand, a novel inflammatory marker, C-reactive protein to serum albumin ratio (CAR) has been introduced as anew and promising marker of inflammatory conditions and as a diagnostic and prognostic marker of various diseases. For example, the CARE TIME study showed that elevated levels of CAR could be a marker of diabetic nephropathy in type 2 diabetes mellitus [30]. Moreover, CAR is considered as a diagnostic marker in colorectal carcinoma [31], and pancreas malignancy [32], and as a prognostic marker in sepsis [33]. All of these conditions are associated with inflammation as diabetic neuropathy is. However, to the best of our knowledge, CAR levels have not been studied in type 2 diabetes mellitus patients with diabetic neuropathy.
In present study, we aimed to observe CAR levels in diabetic neuropathy subjects and to compare to those in diabetic patients without diabetic neuropathy.
2. Materials and Methods
Patients with type 2 diabetes mellitus that treated in outpatients internal medicine clinics of Abant Izzet Baysal University Hospital were enrolled to the present retrospective analysis. Patients with active infection, inflammatory disease, advanced liver disease, cancer, and pregnancy were excluded from the study. The subjects receiving anti-inflammatory drugs were also excluded. Study population was divided into two according to the presence of diabetic neuropathy; diabetic patients with DN (DN group) and diabetic subjects without DN (non-DN group). The diagnosis of diabetic neuropathy was based on the recommendations of the Toronto Diabetic Neuropathy Expert Group [34].
Age, sex, body weight, height, duration of type 2 diabetes mellitus, systolic and diastolic blood pressures, smoking and drinking habits of the study cohort recorded from institutional computerized database and from the files of the patients. Presence of diabetic nephropathy and retinopathy were also recorded. A body mass index (BMI) was calculated by division of weight (kg) by the square of height (m).
Laboratory parameters including blood leukocyte count, hemoglobin, hematocrit, platelet count, fasting glucose, glycated hemoglobin (HbA1c), blood urea, creatinine, estimated glomerular filtration rate (eGFR), serum uric acid, liver function tests (aspartate [AST] and alanine [ALT] transaminases), total, LDL and HDL cholesterol levels, plasma triglyceride, C-reactive protein and albumin, were also obtained and recorded. A CAR value was calculated by division of C-reactive protein by serum albumin. General characteristics and laboratory parameters of the DN and non-DN groups were compared.
Statistics
Statistical software (SPSS 16.0 for Windows, IBM Co. Chicago, IL, USA) was used in statistical analyses of the study variables. Distribution skewness of the study variables were held with Kolmogorov Smirnov test. The variables that fit into normal distribution were expressed as means and standard deviations while the variables with skewed distribution were expressed as medians (min-max). Categorical variables were expressed as numbers and percentages. Comparison of the variables with normal distribution was conducted with independent samples t test while the comparison of the variables with skewed distribution was held with Mann Whitney u test. Chi-square test w sued in comparison of categorical variables among study groups. Correlations between CAR and other study variables were analyzed with Person’s correlation analysis test. CAR’s sensitivity and specificity in showing DN were analyzed with ROC analysis test. Logistic regression analysis (independent variables; age, BMI, diabetes duration, fasting plasma glucose, HbA1c, serum creatinine, LDL-cholesterol and CAR) was conducted to find out independent risk factors for diabetic neuropathy. It is considered as statistically significant when the p value is lower than 0.05 thresholds.
3. Results
Study cohort was consisted with 697 diabetic individuals; 266 in DN and 431 in non-DN groups. Mean age of the DN and non-DN groups were 60 ± 10 years and 56 ± 11 years, respectively. Age was not statistically different between the study groups (p=0.11). 172 (65%) the subjects in DN group was women and 94 (35%) of them were men, while 219 (56%) of the participants in non-DN group were women and 212 (44%) of them were men. There was no statistically significant difference between DN and non-DN groups in term of gender (p=0.06).
Body weight (p=0.6), waist circumference (p=0.56), systolic blood pressure (p=0.17) and diastolic blood pressure (p=0.07) of the DN and non-DN groups were not statistically different. However, body mass index of the DN group (31,1 [17-46,3] kg/m2) was significantly greater than the BMI of the non-DN group (30,8 [19-55,4] kg/m2), (p=0.02). Table 1 summarizes the general characteristics of the DN and non-DN groups.
Blood leukocyte count (p=0.33), hemoglobin (p=0.16), hematocrit (p=0.27), platelet count (p=0.35), aspartate transaminase (p=0.68), alanine transaminase (p=0.65), blood urea (p=0.14), eGFR (p=0.057), serum uric acid (p=0.07), total cholesterol (p=0.14), triglyceride (p=0.36), and HDL-cholesterol (p=0.1) levels of the DN and non-DN groups were not statistically different. On the other hand, C-reactive protein (p<0.001), serum albumin (p=0.01), fasting plasma glucose (p<0.001), HbA1c (p=0.001), serum creatinine (p=0.049), and LDL-cholesterol (p=0.03) levels of the DN group was significantly higher than those of the non-DN group. Table 2 shows the laboratory data of the DN and non-DN groups.
Median CAR of the DN and non-DN groups were 2,19 (0,2-49)% and 0,56 (0,02-5,8)%, respectively. CAR was significantly elevated in DN group compared to the CAR of the subjects in non-DN group (p<0.001).
Smoking (p=0.27) and drinking alcohol (p=0.44) rates were not significantly different among DN and non-DN groups. However, the rate of diabetic retinopathy (p<0.001) and diabetic nephropathy (p<0.001) were higher in subjects in DN group compared to the patients in non-DN group.
Correlation tests revealed that CAR was significantly and positively correlated with age (r=0.15, p<0.001), weight (r=0.19, p=0.01), BMI (r=0.11, p=0.03), waist circumference (r=0.10, p=0.046), fasting plasma glucose (r=0.14, p=0.004), serum creatinine (r=0.25, p<0.001), triglyceride (r=0.17, p<0.001), and LDL-cholesterol (r=0.13, p=0.001) levels. Moreover, CAR was inversely correlated with eGFR levels (r=-0.16, p<0.001).
In receiver operative characteristics (ROC) curve analysis, the sensitivity and specificity of CAR (when higher than 1,02%) in predicting diabetic neuropathy were 78% and 73%, respectively (AUC: 0.84, p<0.001, 95% CI: 0,82-0,87). Figure 1 shows the ROC curve of CAR in detecting diabetic neuropathy.
Logistic regression analysis was performed to find out whether CAR was an independent risk factor of diabetic neuropathy (also taking into account BMI, diabetes duration, fasting plasma glucose, HbA1c, serum creatinine and LDL-cholesterol levels). High CAR level appeared as an independent risk factor of diabetic neuropathy (p<0.001, OR: 1.34, 95% CI: 0.48-1.62).
4. Discussion
Present study showed several important results; (a) patients with DN have higher CAR levels compared to the diabetic patients without DN, (b) there are significant correlation between CAR and markers of poor diabetic outcome in patients with type 2 diabetes mellitus, (c) CAR have considerably high sensitivity and specificity in detecting diabetic neuropathy, and (d) increased CAR level is an independent risk factor for diabetic neuropathy (a unit increase in CAR increase the odds of diabetic neuropathy by 34%).
The body mass index level of the DN group was greater than the BMI level of the non-DN group in present study. Accordingly, there are similar works in literature that found elevated BMI in diabetic subjects with neuropathy. For example a study by Smith et al. studied 218 subjects and found that obesity was a risk factor for development of diabetic neuropathy [35]. A more recent work by Callaghan et al. reported that obesity was an important risk factor for diabetic neuropathy in subjects with diabetes mellitus [36]. Another report from Africa showed that patients with diabetic neuropathy were more likely to have higher body mass index compared to the diabetic subjects without neuropathy [37]. Not only body mass index, but also other indexes of obesity are found to be related with neuropathy in diabetic patients. For instance, a study from Korea revealed that besides body mass index, waist circumference, whole body fat and visceral fat mass were higher in patients with diabetic neuropathy compared to those without diabetic neuropathy [38].
Duration of diabetes mellitus was another factor that associated with diabetic neuropathy in present study. An Indian study including 336 diabetic subjects revealed that duration of diabetes was associated with the presence of diabetic neuropathy [39]. A recent meta-analysis on more than 12000 diabetic patients found that duration of diabetes was significantly associated with increased risk of diabetic polyneuropathy [40]. These data suggest that increased disease duration is associated with increased neuropathy risk in diabetic population. In accordance with the literature knowledge, present study showed that duration of diabetes was significantly longer in DN group compared to that in non-DN group.
Fasting plasma glucose is an important factor in development of neuropathy in diabetic patients. Poor control of diabetes mellitus which result in high blood glucose levels increases the risk of diabetic polyneuropathy. In contrast, authors reported that enhancement of blood glucose control could prevent the development of diabetic neuropathy [28]. Fluctuations in blood glucose levels in diabetic subjects have negative effects on development and progression of diabetic polyneuropathy, according to the study by Oyibo et al. [41]. Not only diabetic subjects but also patients with prediabetes are at risk of neuropathy. The rate of impaired glucose tolerance have been reported to be increased in individuals with peripheral neuropathy [42]. Moreover, not only impaired tolerance of glucose, but also metabolic syndrome rates were increased in subjects with symmetric peripheral neuropathy [43]. In line with literature knowledge, in present study, we reported higher blood fasting glucose levels in patients with diabetic neuropathy compared to the subjects without diabetic neuropathy.
Diabetic neuropathy is closely associated with HbA1c in type 2 diabetes mellitus patients. Variability in glycated hemoglobin levels was suggested to be correlated with the presence of diabetic neuropathy in diabetic population [44]. Similarly, studies in different populations were linked diabetic neuropathy to the increased levels of HbA1c [45]. In addition, extensive control of glucose by reducing HbA1c to target levels in a short interval result in amelioration of neuropathy in diabetic subjects [46]. However, there are conflicting studies in literature, too. A recent study by Casedei et al. concluded that HbA1c was a valuable marker of diabetes mellitus but its role in the diagnosis of diabetic neuropathy should be elucidated more in the following studies with larger cohort [47]. Present study, in which higher HbA1c levels were detected in patients with diabetic neuropathy compared to the patients without diabetic neuropathy, supports the previous studies in the literature claiming that elevated HbA1c increases the risk of diabetic neuropathy.
The difference among DN and non-DN groups in term of serum creatinine levels was slightly significant while the difference in eGFR was slightly insignificant in present work. The CARE TIME study found increased rate of diabetic neuropathy in subjects with diabetic kidney disease and higher levels of serum creatinine were noted in those subjects [30]. Another study in literature which involved 100 subjects revealed that serum creatinine levels of the patients with diabetic microvascular complications were significantly higher than that of the diabetic subjects without microvascular complications [48]. Thus, we can claim that our results were consistent with the literature knowledge.
Plasma LDL-cholesterol levels of the DN group were greater than the LDL of non-DN group in present report. There are studies with similar results in the literature. Tesfaye et al. reported that elevated LDL-cholesterol was associated with increased diabetic neuropathy risk in diabetic subjects [49]. Subsequently, Andersen et al.’s study confirmed the results of the previous studies by reporting high diabetic neuropathy risk in diabetic patients with elevated LDL-cholesterol [50]. Furthermore, a recent meta-analysis that studied more than 30000 subjects revealed that patients with high LDL-cholesterol were at increased risk of diabetic neuropathy [51]. However, there are also conflicting reports in the literature about the role of LDL-cholesterol in diabetic neuropathy. A Danish study in 2019 reported that increased LDL-cholesterol was not associated with high risk of diabetic neuropathy [52]. The results of present study support the studies suggested that high LDL-cholesterol increases the risk of diabetic neuropathy. However, we could not report any statistical difference in plasma triglyceride levels of the subjects with or without diabetic neuropathy.
Serum C-reactive protein is the prototype and most commonly used marker of inflammation. On the other hand, serum albumin is considered as a negative acute phase marker since it is reduced during infections and inflammatory conditions. Combined use of these two indices, CAR has been studied in various conditions. Previously, the CARE TIME study reported that elevated CAR levels were associated with diabetic kidney injury [30]. The role of CAR has been studied in malignant conditions, too. A recent work suggested that CAR was superior than other indexes in predicting the outcome of the subjects with colorectal carcinoma [53]. In addition, CAR was introduced as a prognostic indicator of survival in patients with non-small cell lung cancer [54]. Interestingly, a meta-analysis suggested that CAR was useful in predicting outcome after treatment in patients with various types of cancer [55]. Infectious diseases are also characterized with high CAR levels. Authors suggested CAR as a useful marker of prognosis and disease severity in Covid-19 cases [56]. In geriatric population with sepsis, elevated CAR was associated with 28 day mortality [57]. CAR was also studied in rheumatologic conditions. In 2019, elevated CAR levels were proposed as a marker of disease activity in Takayasu arteritis [58]. In another study, CAR has been reported to have high sensitivity and specificity in predicting ANCA associated vasculitis [59]. Recent studies investigated its role in surgical procedures. For example, CAR was useful in risk stratification of patients whom received trans-catheter edge to edge mitral valve repair [60]. Moreover, higher CAR in patients undergoing surgery higher rate of mechanical ventilation needed in postoperative period [61]. Behera et al. studied CAR levels in patients with pancreatitis and found that CAR was an independent predictor of mortality in those patients [62]. All of these conditions are associated with inflammatory burden as diabetic neuropathy is. Thus, our results showing increased CAR levels in diabetic neuropathy appear to be compatible with the literature.
We can emphasize the presence of several limitations in the present study. Relatively small study population and retrospective design of the work are main limitations that prevent globalization of the results of the present work. Moreover, single center nature of the study makes the third limitation. However, to the best of our knowledge, this is the first work in the literature that reported association between CAR and diabetic neuropathy.
5. Conclusions
In summary, elevated CAR levels could be considered as a marker of diabetic neuropathy and warrant prompt evaluation in patients with type 2 diabetes mellitus. CAR can be a valuable additional diagnostic tool in this aspect due to its inexpensive and easy to assess nature.
Author Contributions
G.A. performed all the works related to this study.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (approval date: 11st of April, 2023; approval number: 2023/105,).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data regarding to this work is available by corresponding author on reasonable requests.
Conflicts of Interest
The author declares no conflict of interest.
References
- Tripathi, B.K.; Srivastava, A.K. Diabetes mellitus: complications and therapeutics. Med Sci Monit 2006, 12, Ra130–147. [Google Scholar]
- Pottie, K.; Jaramillo, A.; Lewin, G.; Dickinson, J.; Bell, N.; Brauer, P.; Dunfield, L.; Joffres, M.; Singh, H.; Tonelli, M. Recommendations on screening for type 2 diabetes in adults. CMAJ 2012, 184, 1687–1696. [Google Scholar] [CrossRef]
- Faselis, C.; Katsimardou, A.; Imprialos, K.; Deligkaris, P.; Kallistratos, M.; Dimitriadis, K. Microvascular Complications of Type 2 Diabetes Mellitus. Curr Vasc Pharmacol 2020, 18, 117–124. [Google Scholar] [CrossRef]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol 2018, 14, 88–98. [Google Scholar] [CrossRef]
- Stolar, M. Glycemic control and complications in type 2 diabetes mellitus. Am J Med 2010, 123, S3–11. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Galicia-Garcia, U.; Benito-Vicente, A.; Jebari, S.; Larrea-Sebal, A.; Siddiqi, H.; Uribe, K.B.; Ostolaza, H.; Martín, C. Pathophysiology of Type 2 Diabetes Mellitus. Int J Mol Sci 2020, 21. [Google Scholar] [CrossRef] [PubMed]
- Vandanmagsar, B.; Youm, Y.H.; Ravussin, A.; Galgani, J.E.; Stadler, K.; Mynatt, R.L.; Ravussin, E.; Stephens, J.M.; Dixit, V.D. The NLRP3 inflammasome instigates obesity-induced inflammation and insulin resistance. Nat Med 2011, 17, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, A.D.; Manson, J.E.; Rifai, N.; Buring, J.E.; Ridker, P.M. C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. JAMA 2001, 286, 327–334. [Google Scholar] [CrossRef]
- Chavey, C.; Lazennec, G.; Lagarrigue, S.; Clapé, C.; Iankova, I.; Teyssier, J.; Annicotte, J.S.; Schmidt, J.; Mataki, C.; Yamamoto, H.; et al. CXC ligand 5 is an adipose-tissue derived factor that links obesity to insulin resistance. Cell Metab 2009, 9, 339–349. [Google Scholar] [CrossRef]
- Vozarova, B.; Weyer, C.; Lindsay, R.S.; Pratley, R.E.; Bogardus, C.; Tataranni, P.A. High white blood cell count is associated with a worsening of insulin sensitivity and predicts the development of type 2 diabetes. Diabetes 2002, 51, 455–461. [Google Scholar] [CrossRef]
- Jaganathan, R.; Ravindran, R.; Dhanasekaran, S. Emerging Role of Adipocytokines in Type 2 Diabetes as Mediators of Insulin Resistance and Cardiovascular Disease. Can J Diabetes 2018, 42, 446–456.e441. [Google Scholar] [CrossRef]
- Haffner, S.; Temprosa, M.; Crandall, J.; Fowler, S.; Goldberg, R.; Horton, E.; Marcovina, S.; Mather, K.; Orchard, T.; Ratner, R.; et al. Intensive lifestyle intervention or metformin on inflammation and coagulation in participants with impaired glucose tolerance. Diabetes 2005, 54, 1566–1572. [Google Scholar] [CrossRef]
- Muhlestein, J.B.; May, H.T.; Jensen, J.R.; Horne, B.D.; Lanman, R.B.; Lavasani, F.; Wolfert, R.L.; Pearson, R.R.; Yannicelli, H.D.; Anderson, J.L. The reduction of inflammatory biomarkers by statin, fibrate, and combination therapy among diabetic patients with mixed dyslipidemia: the DIACOR (Diabetes and Combined Lipid Therapy Regimen) study. J Am Coll Cardiol 2006, 48, 396–401. [Google Scholar] [CrossRef]
- Solomon, D.H.; Massarotti, E.; Garg, R.; Liu, J.; Canning, C.; Schneeweiss, S. Association between disease-modifying antirheumatic drugs and diabetes risk in patients with rheumatoid arthritis and psoriasis. JAMA 2011, 305, 2525–2531. [Google Scholar] [CrossRef] [PubMed]
- Dyck, P.J.; Kratz, K.M.; Karnes, J.L.; Litchy, W.J.; Klein, R.; Pach, J.M.; Wilson, D.M.; O’Brien, P.C.; Melton, L.J., 3rd; Service, F.J. The prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population-based cohort: the Rochester Diabetic Neuropathy Study. Neurology 1993, 43, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Calcutt, N.A. Diabetic neuropathy and neuropathic pain: a (con)fusion of pathogenic mechanisms? Pain 2020, 161, S65–s86. [Google Scholar] [CrossRef] [PubMed]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res Clin Pract 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Demir, S.; Nawroth, P.P.; Herzig, S.; Ekim Üstünel, B. Emerging Targets in Type 2 Diabetes and Diabetic Complications. Adv Sci (Weinh) 2021, 8, e2100275. [Google Scholar] [CrossRef] [PubMed]
- Rendra, E.; Riabov, V.; Mossel, D.M.; Sevastyanova, T.; Harmsen, M.C.; Kzhyshkowska, J. Reactive oxygen species (ROS) in macrophage activation and function in diabetes. Immunobiology 2019, 224, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, K.; Martin, D.P.; Schmelzer, J.D.; Mitsui, Y.; Low, P.A. Pro- and anti-inflammatory cytokine gene expression in rat sciatic nerve chronic constriction injury model of neuropathic pain. Exp Neurol 2001, 169, 386–391. [Google Scholar] [CrossRef]
- Braswell, K.; Dickey, C.A.; Jinwal, U.K. A commentary on: Modulating molecular chaperones improves sensory fiber recovery and mitochondrial function in diabetic peripheral neuropathy. Exp Neurol 2013, 241, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Román-Pintos, L.M.; Villegas-Rivera, G.; Rodríguez-Carrizalez, A.D.; Miranda-Díaz, A.G.; Cardona-Muñoz, E.G. Diabetic Polyneuropathy in Type 2 Diabetes Mellitus: Inflammation, Oxidative Stress, and Mitochondrial Function. J Diabetes Res 2016, 2016, 3425617. [Google Scholar] [CrossRef]
- Tahrani, A.A.; Askwith, T.; Stevens, M.J. Emerging drugs for diabetic neuropathy. Expert Opin Emerg Drugs 2010, 15, 661–683. [Google Scholar] [CrossRef] [PubMed]
- Thakur, S.; Gupta, S.K.; Ali, V.; Singh, P.; Verma, M. Aldose Reductase: a cause and a potential target for the treatment of diabetic complications. Arch Pharm Res 2021, 44, 655–667. [Google Scholar] [CrossRef]
- Sloan, G.; Alam, U.; Selvarajah, D.; Tesfaye, S. The Treatment of Painful Diabetic Neuropathy. Curr Diabetes Rev 2022, 18, e070721194556. [Google Scholar] [CrossRef]
- Sadosky, A.; Mardekian, J.; Parsons, B.; Hopps, M.; Bienen, E.J.; Markman, J. Healthcare utilization and costs in diabetes relative to the clinical spectrum of painful diabetic peripheral neuropathy. J Diabetes Complications 2015, 29, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, B.C.; Little, A.A.; Feldman, E.L.; Hughes, R.A. Enhanced glucose control for preventing and treating diabetic neuropathy. Cochrane Database Syst Rev 2012, 6, Cd007543. [Google Scholar] [CrossRef]
- Khdour, M.R. Treatment of diabetic peripheral neuropathy: a review. J Pharm Pharmacol 2020, 72, 863–872. [Google Scholar] [CrossRef]
- Bilgin, S.; Kurtkulagi, O.; Atak Tel, B.M.; Duman, T.T.; Kahveci, G.; Khalid, A.; Aktas, G. Does C-reactive protein to serum Albumin Ratio correlate with diabEtic nephropathy in patients with Type 2 dIabetes MEllitus? The CARE TIME study. Prim Care Diabetes 2021, 15, 1071–1074. [Google Scholar] [CrossRef]
- Ishizuka, M.; Nagata, H.; Takagi, K.; Iwasaki, Y.; Shibuya, N.; Kubota, K. Clinical Significance of the C-Reactive Protein to Albumin Ratio for Survival After Surgery for Colorectal Cancer. Ann Surg Oncol 2016, 23, 900–907. [Google Scholar] [CrossRef]
- Haruki, K.; Shiba, H.; Shirai, Y.; Horiuchi, T.; Iwase, R.; Fujiwara, Y.; Furukawa, K.; Misawa, T.; Yanaga, K. The C-reactive Protein to Albumin Ratio Predicts Long-Term Outcomes in Patients with Pancreatic Cancer After Pancreatic Resection. World J Surg 2016, 40, 2254–2260. [Google Scholar] [CrossRef]
- Deng, T.B.; Zhang, J.; Zhou, Y.Z.; Li, W.M. The prognostic value of C-reactive protein to albumin ratio in patients with lung cancer. Medicine (Baltimore) 2018, 97, e13505. [Google Scholar] [CrossRef]
- Tesfaye, S.; Boulton, A.J.; Dyck, P.J.; Freeman, R.; Horowitz, M.; Kempler, P.; Lauria, G.; Malik, R.A.; Spallone, V.; Vinik, A.; et al. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care 2010, 33, 2285–2293. [Google Scholar] [CrossRef]
- Smith, A.G.; Singleton, J.R. Obesity and hyperlipidemia are risk factors for early diabetic neuropathy. J Diabetes Complications 2013, 27, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Callaghan, B.C.; Gallagher, G.; Fridman, V.; Feldman, E.L. Diabetic neuropathy: what does the future hold? Diabetologia 2020, 63, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Amour, A.A.; Chamba, N.; Kayandabila, J.; Lyaruu, I.A.; Marieke, D.; Shao, E.R.; Howlett, W. Prevalence, Patterns, and Factors Associated with Peripheral Neuropathies among Diabetic Patients at Tertiary Hospital in the Kilimanjaro Region: Descriptive Cross-Sectional Study from North-Eastern Tanzania. Int J Endocrinol 2019, 2019, 5404781. [Google Scholar] [CrossRef] [PubMed]
- Oh, T.J.; Lee, J.E.; Choi, S.H.; Jang, H.C. Association between Body Fat and Diabetic Peripheral Neuropathy in Middle-Aged Adults with Type 2 Diabetes Mellitus: A Preliminary Report. J Obes Metab Syndr 2019, 28, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Darivemula, S.; Nagoor, K.; Patan, S.K.; Reddy, N.B.; Deepthi, C.S.; Chittooru, C.S. Prevalence and Its Associated Determinants of Diabetic Peripheral Neuropathy (DPN) in Individuals Having Type-2 Diabetes Mellitus in Rural South India. Indian J Community Med 2019, 44, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Xu, Y.; An, M.; Zeng, Q. The risk factors for diabetic peripheral neuropathy: A meta-analysis. PLoS One 2019, 14, e0212574. [Google Scholar] [CrossRef] [PubMed]
- Oyibo, S.O.; Prasad, Y.D.; Jackson, N.J.; Jude, E.B.; Boulton, A.J. The relationship between blood glucose excursions and painful diabetic peripheral neuropathy: a pilot study. Diabet Med 2002, 19, 870–873. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.G.; Singleton, J.R. Impaired glucose tolerance and neuropathy. Neurologist 2008, 14, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.G. Impaired glucose tolerance and metabolic syndrome in idiopathic neuropathy. J Peripher Nerv Syst 2012, 17 Suppl 2, 15–21. [Google Scholar] [CrossRef]
- Su, J.B.; Zhao, L.H.; Zhang, X.L.; Cai, H.L.; Huang, H.Y.; Xu, F.; Chen, T.; Wang, X.Q. HbA1c variability and diabetic peripheral neuropathy in type 2 diabetic patients. Cardiovasc Diabetol 2018, 17, 47. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.; Sarkar, M.; Mahbub, I.; Islam, S. A study on peripheral neuropathy and its related risk factors associated with hba1c levels. Journal of Bio-Science 2021, 29, 123-138.
- Ishibashi, F.; Taniguchi, M.; Kosaka, A.; Uetake, H.; Tavakoli, M. Improvement in Neuropathy Outcomes With Normalizing HbA(1c) in Patients With Type 2 Diabetes. Diabetes Care 2019, 42, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Casadei, G.; Filippini, M.; Brognara, L. Glycated Hemoglobin (HbA1c) as a Biomarker for Diabetic Foot Peripheral Neuropathy. Diseases 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Kocak, M.Z.; Aktas, G.; Atak, B.M.; Duman, T.T.; Yis, O.M.; Erkus, E.; Savli, H. Is Neuregulin-4 a predictive marker of microvascular complications in type 2 diabetes mellitus? Eur J Clin Invest 2020, 50, e13206. [Google Scholar] [CrossRef] [PubMed]
- Tesfaye, S.; Chaturvedi, N.; Eaton, S.E.; Ward, J.D.; Manes, C.; Ionescu-Tirgoviste, C.; Witte, D.R.; Fuller, J.H. Vascular risk factors and diabetic neuropathy. N Engl J Med 2005, 352, 341–350. [Google Scholar] [CrossRef]
- Andersen, S.T.; Witte, D.R.; Dalsgaard, E.M.; Andersen, H.; Nawroth, P.; Fleming, T.; Jensen, T.M.; Finnerup, N.B.; Jensen, T.S.; Lauritzen, T.; et al. Risk Factors for Incident Diabetic Polyneuropathy in a Cohort With Screen-Detected Type 2 Diabetes Followed for 13 Years: ADDITION-Denmark. Diabetes Care 2018, 41, 1068–1075. [Google Scholar] [CrossRef]
- Cai, Z.; Yang, Y.; Zhang, J. A systematic review and meta-analysis of the serum lipid profile in prediction of diabetic neuropathy. Sci Rep 2021, 11, 499. [Google Scholar] [CrossRef]
- Emanuelsson, F.; Nordestgaard, B.G.; Tybjærg-Hansen, A.; Benn, M. Impact of LDL Cholesterol on Microvascular Versus Macrovascular Disease: A Mendelian Randomization Study. J Am Coll Cardiol 2019, 74, 1465–1476. [Google Scholar] [CrossRef]
- Kudou, K.; Hasuda, H.; Tsuda, Y.; Kusumoto, E.; Uehara, H.; Yoshida, R.; Koga, T.; Yamashita, Y.I.; Sakaguchi, Y.; Kusumoto, T. Prognostic significance of a novel index score based on the inflammation-based prognostic scores of patients with colorectal cancer. J Gastroenterol Hepatol 2023. [Google Scholar] [CrossRef]
- Yang, J.R.; Xu, J.Y.; Chen, G.C.; Yu, N.; Yang, J.; Zeng, D.X.; Gu, M.J.; Li, D.P.; Zhang, Y.S.; Qin, L.Q. Post-diagnostic C-reactive protein and albumin predict survival in Chinese patients with non-small cell lung cancer: a prospective cohort study. Sci Rep 2019, 9, 8143. [Google Scholar] [CrossRef]
- Dai, M.; Wu, W. Prognostic role of C-reactive protein to albumin ratio in cancer patients treated with immune checkpoint inhibitors: a meta-analysis. Front Oncol 2023, 13, 1148786. [Google Scholar] [CrossRef]
- El-Shabrawy, M.; Alsadik, M.E.; El-Shafei, M.; Abdelmoaty, A.A.; Alazzouni, A.S.; Esawy, M.M.; Shabana, M.A. Interleukin-6 and C-reactive protein/albumin ratio as predictors of COVID-19 severity and mortality. Egyptian J Bronchol 2021, 15, 1–7. [Google Scholar] [CrossRef]
- Cha, K.; Choi, S.P.; Kim, S.H.; Oh, S.H. Prognostic value of ambulation ability with albumin and C-reactive protein to predict 28-day mortality in elderly sepsis patients: a retrospective multicentre registry-based study. BMC Geriatr 2022, 22, 661. [Google Scholar] [CrossRef] [PubMed]
- Seringec Akkececi, N.; Yildirim Cetin, G.; Gogebakan, H.; Acipayam, C. The C-Reactive Protein/Albumin Ratio and Complete Blood Count Parameters as Indicators of Disease Activity in Patients with Takayasu Arteritis. Med Sci Monit 2019, 25, 1401–1409. [Google Scholar] [CrossRef] [PubMed]
- Atas, D.B.; Sahin, G.K.; Şengül, Ş.; Kaya, B.; Paydaş, S.; Alibaz-Oner, F.; Direskeneli, H.; Tuglular, S.; Asicioglu, E. C-Reactive Protein to Albumin Ratio is Associated with Disease Activity in Anti-Neutrophil Cytoplasmic Antibody Associated Vasculitis. Mediterr J Rheumatol 2023, 34, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Koell, B.; Ludwig, S.; Weimann, J.; Waldschmidt, L.; Schirmer, J.; Reichenspurner, H.; Blankenberg, S.; Conradi, L.; Schofer, N.; Kalbacher, D. C-Reactive Protein to Albumin Ratio offers superior risk prediction in patients undergoing mitral valve edge-to-edge repair: a comparison to established surgical risk scores. Eur Heart J 2022, 43, ehac544.1641. [Google Scholar] [CrossRef]
- Tharavath, V.; Rao, P.B.; Nayak, S.; Panda, A.; Bandyopadhyay, D.; Pati, S. Preoperative C-reactive protein - Albumin ratio as a predictor of requirement for postoperative mechanical ventilation after non-cardiac surgery under general anaesthesia: A prospective observational study (HICARV). Indian J Anaesth 2023, 67, 262–268. [Google Scholar] [CrossRef]
- Behera, M.; Mishra, D.; Sahu, M.; Nittala, R.; Singh, A.; Pati, G.; Agarwal, S.; Narayan, J. C-reactive protein/albumin and ferritin as predictive markers for severity and mortality in patients with acute pancreatitis. Gastroenterology Rev 2022, 17, 1–7. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
ROC curve of CAR in detecting diabetic neuropathy.
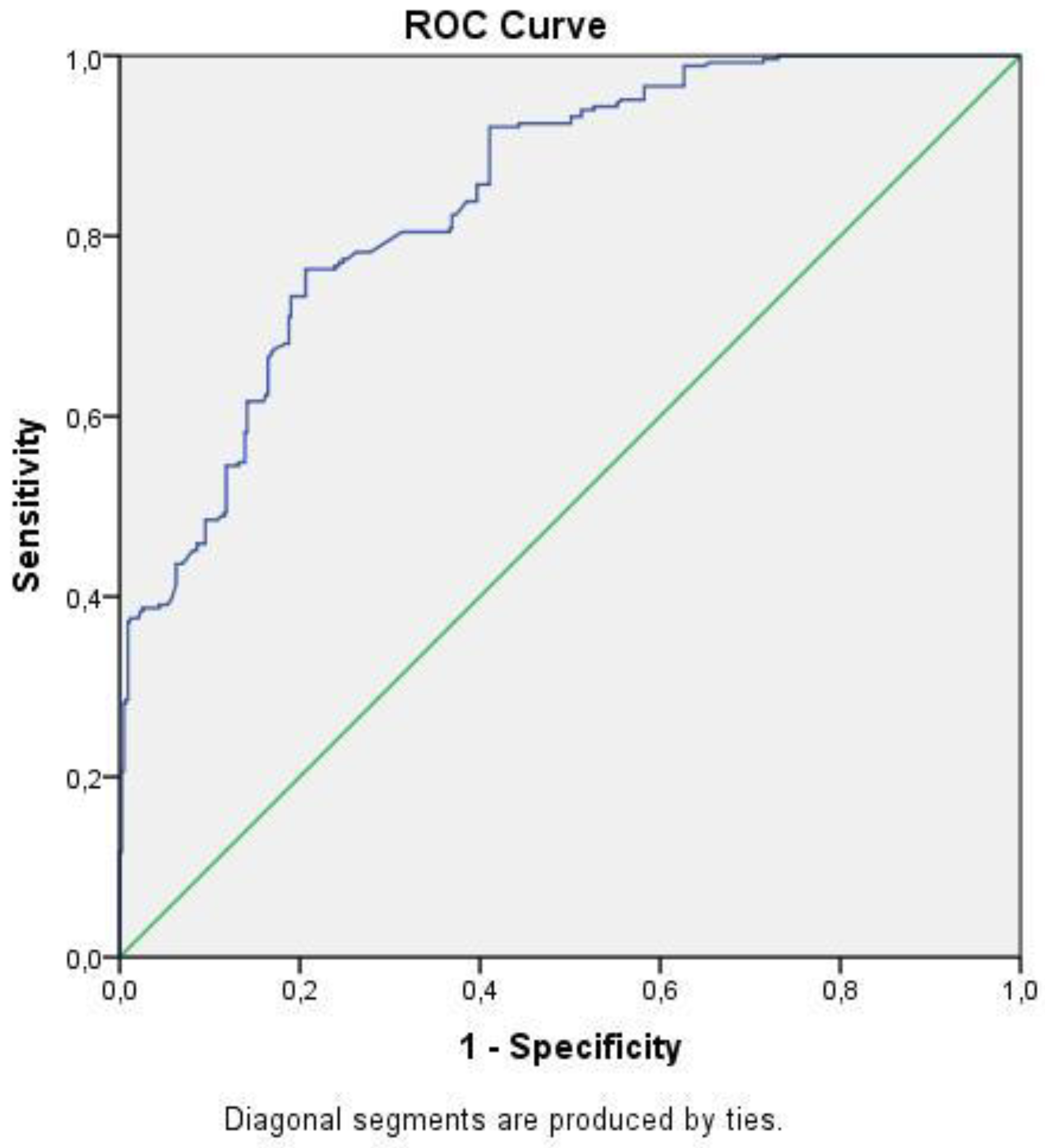

Table 1.
General characteristics of the DN and non-DN groups.
| DN group | Non-DN group | p | ||
|---|---|---|---|---|
| Gender | Women (n, (%)) | 172 (65%) | 219 (56%) | 0.06 |
| Men (n, (%)) | 94 (35%) | 212 (44%) | ||
| Mean ± Standard Deviation | ||||
| Age (years) | 60 ± 10 | 56 ± 11 | 0.11 | |
| Median (min.-max.) | ||||
| Weight (kg) | 82 (48-120) | 83 (46-150) | 0.6 | |
| Waist circumference (cm) | 105 (75-132) | 105 (78-160) | 0.56 | |
| BMI (kg/m2) | 31,1 (17-46,3) | 30,8 (19-55,4) | 0.02 | |
| Diabetes duration (years) | 6 (1-24) | 3 (1-20) | <0.001 | |
| Systolic blood pressure (mmHg) | 128 (90-180) | 130 (90-200) | 0.17 | |
| Diastolic blood pressure (mmHg) | 75 (50-110) | 80 (50-110) | 0.07 | |
Abbreviations: BMI; body mass index.
Table 2.
Laboratory parameters of the DN and non-DN groups.
| DN group | Non-DN group | p | |
|---|---|---|---|
| Mean ± Standard Deviation | |||
| leukocyte count (k/mm3) | 6,9 ± 2 | 6,8 ± 2,3 | 0.33 |
| Hemoglobin (g/dL) | 13,1 ± 1,6 | 13,5 ± 1,7 | 0.16 |
| Hematocrit (%) | 39 ± 4 | 40 ± 5 | 0.27 |
| platelet count (k/mm3) | 262 ± 36 | 256 ± 34 | 0.35 |
| aspartate transaminase (U/L) | 24 ± 9 | 28 ± 10 | 0.68 |
| alanine transaminase (U/L) | 23 ± 11 | 22 ± 12 | 0.65 |
| Median (min.-max.) | |||
| C-reactive protein (mg/L) | 9,5 (1-250) | 2,2 (0,1-26,1) | <0.001 |
| Serum albumin (g/dL) | 4,3 (2,8-5,3) | 4,4 (2,9-5,6) | 0.01 |
| Fasting plasma glucose (mg/dL) | 8,3 (4,9-16,5) | 7,7 (5,1-17,2) | <0.001 |
| HbA1c (%) | 177 (66-565) | 147 (65-514) | 0.001 |
| Blood urea (mg/dL) | 34 (17-222) | 32 (13-258) | 0.14 |
| Serum creatinine (mg/dL) | 0,83 (0,59-3,41) | 0,8 (0,39-3,93) | 0.049 |
| eGFR (%) | 99,5 (15,3-185) | 99,8 (15,8-181) | 0.057 |
| Serum uric acid (mg/dL) | 5,6 (1,8-10,4) | 5,5 (2,4-13,6) | 0.07 |
| Triglyceride (mg/dL) | 153 (47-850) | 151 (50-856) | 0.36 |
| Total cholesteroö (mg/dL) | 187 (52-318) | 200 (50-378) | 0.14 |
| LDL-cholesterol (mg/dL) | 132 (21-200) | 114 (29-244) | 0.03 |
| HDL-cholesterol (mg/dL) | 46 (13-87) | 44 (17-92) | 0.1 |
| CAR (%) | 2,19 (0,2-49) | 0,56 (0,02-5,8) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



