
Submitted:
02 June 2023
Posted:
05 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
After three years of the onset of the pandemic, there is scarce evidence about how COVID-19 disease affect the female reproductive system, and consequently, the menstrual cycle. Since the common causes of secondary amenorrhea are considered as exclusion criteria in the studies about menstrual changes following SARS-CoV-2 infection, the prevalence of this event and the influencing factors in formerly menstruating women remains unknown. A retrospective observational cross-sectional study was conducted on Spanish adult women (N= 17,512), using an online survey; a subpopulation of SARS-CoV-2-infected-formerly menstruating women was included in the present analysis (n= 72). Collected data included general characteristics, medical history, and specific information about COVID-19 disease. 38.9% of the respondents experienced menstrual-related disturbances after suffering from the COVID-19 disease, unexpected vaginal bleeding being the most common (20.8%). Other alterations related with the length – “shorter” by 12.5% − and the flow − “heavier than usual” 30.3% − of the menstrual bleeding were reported. The binary logistic regression showed that being a perimenopausal woman (AOR 4.608, CI 95%, 1.018 – 20.856, p = 0.047) and having heavy menstrual bleeding (AOR 4.857, CI 95%, 1.239 – 19.031, p=0.023) are influential factors. This evidence could help health professionals to provide scientifically up-to-date information to their patients, empowering them to actively manage their reproductive health, especially in those societies where menstrual health is still a taboo.
Keywords:
SARS-CoV-2 infection
; COVID-19 disease
; women´s health
; menstrual-related disturbances
; formerly menstruating women
; secondary amenorrhea
; perimenopause
; heavy menstrual bleeding
1. Introduction
Undoubtedly, since the WHO declared the novel coronavirus SARS-CoV-2 outbreak as a global pandemic on March 2020, the life of billions of people worldwide has completely changed due to this unprecedent health crisis. To date, it is estimated that the infectious respiratory disease known as COVID-19 disease has affected 761.402.282 people, causing 6.887.000 deaths [1].
Focusing on the physiopathology, SARS-CoV-2 has been reported to trigger multisystem complications in addition to respiratory symptoms [2,3,4]. This is due to the ubiquitous expression of the membrane protein called angiotensin-converting enzyme 2 (ACE2), which is known to be the route of entry of SARS-CoV-2 virus into the host cells [5,6]; additionally, other enzymes such as the transmembrane protease serine subtype 2 (TMPRSS2) and the dipeptidyl peptidase-4 (DPP4) have been identified as co-receptors of this coronavirus during host cell entry [7]. Regarding the female reproductive system, this receptor complex is also expressed − predominantly in ovaries and regardless of the age and the ovarian reserve – [8]. As Reis et al. [9] point out, ACE2 plays a major role in the generation of angiotensin-(1-7), which stimulates ovarian follicle growth, oocyte maturation and ovulation; its precursor angiotensin II promotes vasoconstriction of the spiral arteries and consequently induces menstruation [10]. Thus, as a result of the COVID-19 disease, the altered functions of this molecular pathway and other neuroendocrine systems – e.g. hypothalamic-pituitary-gonadal (HPG) axis and hypothalamic-pituitary-adrenal (HPA) axis − may lead to menstrual cycle irregularities [7]. Additionally, the immune response resulting from the infection may also be implicated in this phenomenon, given its interaction with the endocrine system [11]. Therefore, it would be expected that SARS-CoV-2 can temporarily or even permanently impair female fertility. Unfortunately, our knowledge of the basic uterine and menstrual physiology is not enough to understand more complex processes of this kind.
Previous studies have linked viral infections with women´s reproductive health alterations [12,13,14]. Nevertheless, conflicting results have so far been achieved in relation to SARS-CoV-2 infection in menstruating women [15,16,17]. Additionally, the prevalence of menstrual-related disturbances (MRD) in formerly menstruating women (FMW) − that is, those who have secondary amenorrhea for different causes − remains unknown. Amenorrhea is defined as the absence or lack of menstrual period. Common causes of secondary amenorrhea include pregnancy, breastfeeding, menopause, contraceptives methods and gynecological conditions [18,19], most of them considered as exclusion criteria in the studies about MRD following SARS-CoV-2 infection. For this reason, the aims of this study were 1) to determine the occurrence of MRD in FMW after COVID-19 disease and 2) to analyze the factors that may be influencing this phenomenon.
2. Materials and Methods
2.1. Experimental design
A retrospective observational cross-sectional study was conducted on Spanish adult women using an online survey (Microsoft Forms®, Microsoft Corporation, Washington, USA).
2.2. Recruitment, data collection and participants
The online survey was released in December 2021 via social networks; the snowball method was applied. Thus, a total of 17,512 were recruited within 15 days; from this sample, the data pertaining to a subpopulation of FMW was selected for the present analysis (N= 72, Figure 1). The inclusion criteria were women: (i) over 18 years of age, (ii) having secondary amenorrhea for different causes, and (iii) having a diagnosis of COVID-19 disease (positive PCR test).
2.3. Survey information
A customized questionnaire based on the survey launched on April 2021 by Lee et al. [20] was designed. It was composed by 56 multiple-choice and text entry questions divided into 6 sections. Participants were asked about 1) the general characteristics of their menstrual cycles, 2) COVID-19 disease, 3) COVID-19 vaccine, 4) menstrual experiences both after the SARS-CoV-2 infection/COVID-19 vaccination in comparison with the expected period symptoms, 5) other MRD, 6) time between infection/vaccine and MRD, 7) duration of MRD, 8) side effects from each dose of the vaccine, 9) reproductive history, 10) medical history, and 11) demographics. The survey took approximately 10-15 min to complete. Variables related to COVID-19 vaccination and MRD have been excluded from the present analysis.
2.4. Statistical analysis
Participants were categorized according to the occurrence or not of MRD after COVID-19 disease. Values were expressed as mean±standard deviation for quantitative variables and number of participants and frequency (%) for qualitative ones. Chi-square and Mann-Whitney U tests were performed for qualitative and quantitative variables, respectively. Subsequently, a bivariate logistic regression analysis was performed to investigate possible associations between the occurrence of MRD following SARS-CoV-2 infection (dependent variable) and the independent variables that were significant (p<0.05) in the previous analyses. Thus, the results were presented as adjusted odds ratios (ORAs) with 95% confidence intervals (CI). The aforementioned analyses were performed using the Statistical Package for Social Sciences (SPSS v.25, IBM, New York, USA) for Windows. Statistical significance was set at p<0.05.
3. Results
3.1. Anthropometric characteristics and medical history
56.9% of the study participants (N=72, mean age 41.4 ± 11.4 years) had normal weight (mean BMI value= 27.8 ± 4.6), 19.4% had autoimmune diseases, and 27.1% had other clinical conditions. Among the causes of amenorrhea, the use of contraceptives (31.9%) and postmenopause (22.2%) were mainly reported, followed by other causes such as polycystic ovary syndrome (19.4%,), perimenopause (15.3%), and breastfeeding (11.1%). Furthermore, 31.9% of women surveyed used hormonal contraceptives for less than 10 years, 61.1% had been pregnant, and 52.8% reported having been diagnosed with a gynecological disease, being the most common polycystic ovary syndrome (18.1%), followed by heavy menstrual bleeding (18.1%), and endometriosis (11.1%) (Table 1).
3.2. Impact of COVID-19 disease on the menstrual health
As shown in table 2, most of the women with amenorrhea were diagnosed with COVID-19 in the first wave (29.2%), followed by the second (23.6%) and the fifth (20.8%); only 2.8% required hospitalization. 38.9% of the respondents experienced MRD after suffering from the COVID-19 disease, unexpected vaginal bleeding being the most common (20.8%). Other alterations related with the length – “shorter” by 12.5% − and the flow − “heavier than usual” 30.3% − of the menstrual bleeding were reported. When asked about the time between the SARS-CoV-2 infection and the occurrence of menstrual bleeding, a 20.8% of the FMW answered “more than 14 days” (20.8%); in 53.3% of cases, this event was unexpected in comparison with the probable period date. With regard to premenstrual syndrome, 56.0% of women suffered from 2 or more symptoms, including fluid retention (8.0%) and pain (4.0%). The majority of participants experiencing MRD after the infection reported that these last “until today” (27.8%).

Table 2.
COVID-19 disease and the occurrence of MRD in the study population (formerly menstruating women, N=72).
Table 2.
COVID-19 disease and the occurrence of MRD in the study population (formerly menstruating women, N=72).
| Variable | Category | Total (N=72) |
|---|---|---|
| Date of COVID-19 diagnosis (pandemic waves) | 1st wave | 21 (29.2) |
| 2nd wave | 17 (23.6) | |
| 3rd wave | 12 (16.7) | |
| 4th wave | 7 (9.7) | |
| 5th wave | 15 (20.8) | |
| Hospitalization | Yes | 2 (2.8) |
| No | 70 (97.2) | |
| MRD occurrence | Yes | 28 (38.9) |
| No | 44 (61.1) | |
| Types | Spotting | 8 (11.1) |
| Shorter menstrual cycle | 3 (4.2) | |
| Unexpected vaginal bleeding | 15 (20.8) | |
| Longer menstrual cycle | 1 (1.4) | |
| Length of menstrual bleeding | None | 45 (62.5) |
| Shorter | 9 (12.5) | |
| Unchanged | 16 (22.2) | |
| Longer | 8 (11.1) | |
| Flow of menstrual bleeding | Not applicable | 39 (54.2) |
| Lighter | 7 (21.2) | |
| Unchanged | 16 (48.5) | |
| Heavier | 10 (30.3) | |
| Time between SARS-CoV-2 infection and period/abnormal bleeding | I was menstruating when I got infected |
1 (1.4) |
| After 1-3 days | 3 (4.2) | |
| After 4-7 days | 6 (8.3) | |
| After 8-14 days | 5 (6.9) | |
| After more than 14 days | 15 (20.8) | |
| Coincidence with period date | Not applicable | 42 (58.3) |
| Yes | 9 (30.0) | |
| No | 16 (53.3) | |
| Not applicable | 5 (16.7) | |
| Premenstrual syndrome | ||
| Nº symptoms | 2 symptoms | 7 (28.0) |
| ≥3 symptoms | 7 (28.0) | |
| Types | None | 6 (24.0) |
| Fluid retention | 2 (8.0) | |
| Pain | 1 (4.0) | |
| Swelling | 0 (0.0) | |
| Thirst | 0 (0.0) | |
| Appetite | 0 (0.0) | |
| Other | 2 (2.8) | |
| Duration of MRD | 1 cycle | 4 (5.6) |
| <3 months | 3 (4.2) | |
| 3-6 months | 4 (5.6) | |
| 6-12 months | 3 (4.2) | |
| Until today | 20 (27.8) | |
| Not applicable | 38 (52.8) |
Values are expressed as: n (%). Abbreviations: BMI, Body Mass Index; IUD, Intrauterine Device; MRD, menstrual-related disturbances.
3.3. Factors associated with the occurrence or not of MRD after COVID-19 disease
Focusing on gynecological history, the comparative analysis (Table 3) revealed a significantly higher percentage of perimenopausal women in the subgroup who experienced alterations (MRD subgroup) compared to the subgroup of those who did not (n-MRD subgroup); among gynecological diseases, heavy menstrual bleeding was more frequent in the MRD subgroup. Similarly, statistically significant differences were found between subgroups in relation to the fourth pandemic wave. Furthermore, the FMW who required hospitalization belong to the MRD subgroup, being the difference between subgroups of marginal significance.
Subsequently, binary logistic regression was performed (Table 4). The analysis showed that being a perimenopausal woman (AOR 4.608, CI 95%, 1.018 – 20.856, p = 0.047) and having heavy menstrual bleeding (AOR 4.857, CI 95%, 1.239 – 19.031, p=0.023) are influential factors in the occurrence of MRD after COVID-19 infection in women with amenorrhea.
4. Discussion
COVID-19 pandemic makes it clear once again that the influence of sex and gender on human health and diseases continues nowadays to be underestimated [21]. Although it is now well established that COVID-19 exhibits gender disparities due to several biological factors, very few studies have analyzed the impact of this disease on women´s health, particularly on the female reproductive system. Based on this scarce scientific evidence available, MRD may affect 16-25% of women of childbearing age infected with SARS-CoV-2 [15,22,23]. In this subpopulation, most commonly reported disturbances were worsened premenstrual syndrome, irregular and infrequent menstruations [23], and decreased menstrual volume – regardless of the severity of the disease [15,22]. For severe hospitalized patients, prolonged menstrual cycles have been also recorded. 15 Furthermore, in a global multinational survey conducted by Davis et al. [24], approximately 30-40% of 2969 women surveyed – most 30 to 60 years old− reported post-COVID-19 menstrual/period issues, including abnormally irregular menstrual cycles (26%) and abnormally heavy periods or clotting (20%); moreover, a 3% of women in their 40s experienced early menopause. Barabás et al. [25] also observed this level of menstrual changes prevalence among infected women of the same age range. Compared with our results in FMW, these findings suggest the existence of differences in the prevalence and characteristics of the MRD between young and middle-aged women, which needs to be confirmed by further research. Moreover, although this kind of alterations seems to be of a transient nature for the majority of the study participants, the possibility that some women may also experience long-term menstrual changes cannot be excluded [22,24]. In this sense, Li et al. [15] observed that while 99% of the patients returned to their normal cycle within 1-2 months after discharge from the hospital, a 44-year-old women reported the absence of menstruation for 4 months after COVID-19 onset. In fact, the binary logistic regression performed in this study revealed that being a perimenopausal woman is influencing factor in experiencing MRD. Therefore, this also confirms that the impact of SARS-CoV-2 infection may differ throughout the different stages of a woman´s life.
As Khan et al. [23] point out, the menstrual cycle involves complex interactions between various tissues, hormones, and organ systems; thus, it can be influenced by a variety of endogenous and exogenous factors, including viral infections. In this regard, it is well established that viruses can affect the female reproductive endocrine system in different ways, as described elsewhere [26,27,28,29]. Therefore, potential direct and indirect effects of SARS-CoV-2 virus must be considered in the occurrence of menstrual changes. Systemically, the damage caused by the COVID-19 disease is suggested to be mediated by a direct viral role, pro-inflammatory immune responses, unbalanced physiological systems −e.g. renin-angiotensin-aldosterone system (RAAS) and ACE2/angiotensin-(1–7)/mitochondrial angiotensin axis, and HPG and HPA axes − and the downregulation of ACE2 expression [4,30]. This harmful context could be aggravated by local direct effects in the female reproductive system, as the tissue damage and the subsequent inflammation leading by the entry into the cell host via the receptor complex ACE2/TMPRSS2/DPP4, with undetermined consequences on menstrual physiology [16,31]. At this point, it should be remembered that estrogens are well known to act in a coordinated way with immune system and metabolism [4,21,31]. Particularly, estradiol has been suggested to play a protective role in COVID-19 through different pathways, including the RAAS system, the anti-inflammatory and anti-viral responses, the upregulation of endolysosomal degradation pathways and changes in the expression of several molecules involved in the virus entry, such as the components of the above-mentioned receptor complex and furin [31,32]. Therefore, the abnormal sex-hormone secretion derived from the SARS-CoV-2 infection, may also alter the immune-neuro-endocrine network. Nevertheless, evidence remains equivocal as conflicting results have been published. Whereas Li et al. [15] conclude that the average sex hormone concentrations and the ovarian reserve did not significantly change in those COVID-19 women of child-bearing age who experienced self-resolve menstrual changes, Ding et al. [16] point out that female COVID-19 patients probably have an ovarian injury, with a poor ovarian reserve of decreased anti-Müllerian hormone and reproductive endocrine disorder of aberrant sex hormone levels, especially high testosterone and prolactin. On the basis of the above, the question arises if the prevalence and the characteristics of menstrual disturbances could be subject to the fluctuation of the hormone levels in the different stages not only of the menstrual cycle, but also of a woman´s life – in other words, her age −. This assumption may also explain the reported differences for primary COVID-19 outcomes according to the menstrual status and the use of contraceptives [33,34]. In fact, our results from the binary logistic regression support these findings, pointing out perimenopause as an influencing factor in the occurrence of MRD in FMW. Taking into account that this transition phase is mainly characterized by lower circulating estradiol levels, it is supposed that the resulting dampened immune response – e.g. the increased levels of the pro-inflammatory cytokines such as IL-6, IL-1β, and TNF-α – and the downregulation of autophagy and the altered expression of ACE2, TMPRSS2, DPP4 and furin [31,32] could underly the increased risk of experience this unexpected event. Conversely, high estrogen levels and consequently the increased estrogen receptor (ER) signaling, may prevent further respiratory complications in SARS-CoV-2-infected pregnant women [34,35]. For this reason, estrogen supplementation has been proposed as a therapeutic approach to reduce the severity of the COVID-19 disease [35,36]. Furthermore, for authors such as Mateus et al. [37], not only estrogen but sex hormones all together might justify the differences between genders and age rates, which makes sense given the opposite effects of testosterone on immune response and virus clearance, in comparison with estradiol [31,32].
On the other hand, other concurrent factors must not be discarded in the prevalence of MRD following SARS-CoV-2 infection in FMW. Firstly, comorbidities may increase the risk of suffer from systemic complications, and hence menstrual changes. In this sense, Li et al. [15] reported that severely ill patients, which had more comorbidities – particularly diabetes, hepatic disease and malignant tumors − and complications than mildly ill ones, were more prone to experience menstrual cycle prolongation; on the contrary, Ding et al. [16] did not observe any differences according to the clinical and gynecological history of the participants. However, the low rate of hospitalization in our study and others [22,24,25] and the marginal significance found between subgroups makes it difficult to draw any conclusion about this issue. According to Suba [35], pre-existing chronic diseases associated with insulin resistant status – e.g. cardiovascular diseases, type-2 diabetes, chronic obstructive pulmonary disease, chronic kidney disease and cancer − aggravate the outcome of COVID-19 infection; insulin resistance, in turn, is associated with a deficient ER signaling and, therefore, with a dysregulated immune response. It should be remembered that HPG axis can be affected by different severe acute illness, leading to decreased levels of progesterone and estrogens [38]. In addition, different degree of ACE2 deficiency are related with some of the above-mentioned diseases [39]. Moreover, regarding gynecological disorders, our results showed that heavy menstrual bleeding may be an influencing factor in the occurrence of menstrual disturbances. In this case, the unbalance between estrogens and progesterone levels may be underlie this unexpected event [40,41], leading to the physiological dysfunctions previously described. Overall, it is worth considering whether the endocrine disorder observed in female COVID-19 patients are consequence of systemic effects rather than local ones. In this sense, Ding et al. [16] point out that the ovarian injury observed in their research must also be linked to nervous system injuries and pituitary dysfunction. However, there are conflicting results about the SARS-CoV-2 neuroinvasion [42]. Finally, stress-associated neuroendocrine-immune mechanisms should also be considered in the occurrence of menstrual disturbances during the pandemic [21,22,25]. In fact, hospitalization itself can be a stressful situation that can induce menstrual abnormalities [10]. Furthermore, as pointed by Barabás et al. [25] the great psychological burden caused by the COVID-19 pandemic on society, with the subsequent increasing levels of depression, may also underlie the menstrual irregularities. Epidemiology shows that women in reproductive age are nearly twice as likely as men to develop major depression [43]. In this condition, the increased levels of the main stress hormone cortisol inhibit the secretion of gonadotropin releasing hormone, which governs the menstrual cycle [25]. Nevertheless, the potential role of mental health in this phenomenon remains controversial and needs to be further investigated. Several other intrinsic and extrinsic factors such as genetics, sociodemographic, culture and lifestyle must also be taken into account [22,25,39,44].
This is one of the few studies conducted worldwide to focus on the impact of COVID-19 disease on the menstrual health of women with secondary amenorrhea, as well as on the potential influence of health-related factors. Although the sample was small and the different subgroups of secondary amenorrhea were not assessed independently, our findings offer a reasonable starting point for future studies. The experimental design could have influenced the detection of significant differences, and therefore causal relationships cannot be properly determined. The risk of recall bias or self-selection must also be considered. Nevertheless, this and other similar survey-based studies have provided insight into different aspects of the menstrual changes following COVID-19 infection/vaccination, when official reports did not yet reflect it. As in similar studies, our findings here might not be applicable to other countries than Spain, due to some of the above-mentioned reasons. Taking into account all of the above, we agree that a longitudinal and multinational study could help to establish the cause-effect relationship and to clarify the factors influencing the occurrence of menstrual alterations after COVID-19 disease.
5. Conclusions
Menstrual disturbances in formerly menstruating women following COVID-19 disease tend to appear more in perimenopause, probably due to the hypersensitivity of the gonadal hormonal axis around this stage of a woman´s life. The lack of scientific evidence on different aspects of women’s health, as a consequence of the predominant androcentrism in modern medicine, continues to cause this type of phenomenon to be underestimated or directly ignored, in a so-called gender bias [45]. Therefore, increasing research efforts on this novel field would contribute directly to the achievement of the WHO´s Sustainable Development Goals 3 “Good Health and Well-being” and 5 “Gender equality” [46]. Furthermore, such evidence could help health professionals to provide scientifically up-to-date information to their patients, empowering them to choose the best option for their reproductive decisions, especially in those societies where menstrual health is still a taboo.
Author Contributions
MG and MA have contributed to this manuscript equally. Conceptualization: CC, ABR, MA; Methodology: CC, ABR, MA; Investigation: MG, CC, ABR; Visualization: CC, ABR; Supervision: CC, ABR; Writing—original draft: MG, CC; Writing—review & editing: MG, CC, ABR, MA.
Funding
This work was supported by the Regional Government of Extremadura-ERDF funds under Grant BBB021- GR21042; Dermofarm S.A. under research agreement with the University of Extremadura (ref. 431/22). Neither the government agency nor the sponsoring company have played a role in the study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of University of Extremadura (ref. 180/2021).
Informed Consent Statement
An informed consent was only obtained from those who agree to be contacted via email by the research group for additional data collection.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical restrictions.
Acknowledgments
The research team would like to thank all the participants who have collaborated in the study in an unselfish manner.
Conflicts of Interest
Authors declare that they have no competing interests.
References
- World Health Organization (WHO). WHO Coronavirus (COVID-19) Dashboard. https://covid19.who.int.
- Guan W-J, Zheng-yi N, Yu H, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 2020, 382, 1708–1720. [CrossRef]
- Majumder J, Minko T. Recent Developments on Therapeutic and Diagnostic Approaches for COVID-19. AAPS J 2021, 23. [CrossRef]
- Kirtipal N, Kumar S, Dubey SK, et al. Understanding on the possible routes for SARS CoV-2 invasion via ACE2 in the host linked with multiple organs damage. Infect Genet Evol 2022, 99, 105254. [CrossRef]
- Zhou P, Yang XL, Wang XG, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [CrossRef]
- Ni W, Yang X, Yang D, et al. Role of angiotensin-converting enzyme 2 (ACE2) in COVID-19. Crit Care 2020, 24, 422. [CrossRef]
- Bechmann N, Maccio U, Kotb R. , et al. COVID-19 Infections in Gonads: Consequences on Fertility? Horm Metab Res 2022, 54, 549–555. [CrossRef]
- Wu M, Ma L, Xue L, et al. Co-expression of the SARS-CoV-2 entry molecules ACE2 and TMPRSS2 in human ovaries: Identification of cell types and trends with age. Genomics 2021, 113, 3449–3460. [CrossRef]
- Reis FM, Reis AM. Angiotensin-converting enzyme 2 (ACE2), angiotensin-(1-7) and Mas receptor in gonadal and reproductive functions. Clin Sci 2020, 134, 2929–2941. [CrossRef]
- Carp-Veliscu A, Mehedintu C, Frincu F, et al. The Effects of SARS-CoV-2 Infection on Female Fertility: A Review of the Literature. Int J Environ Res Public Health 2022, 19, 984. [CrossRef]
- Male, V. Menstrual changes after covid-19 vaccination. BMJ 2021, 374:n2211. [CrossRef]
- Schoenbaum EE, Hartel D, Lo Y, et al. HIV infection, drug use, and onset of natural menopause. Clin Infect Dis 2005, 41, 1517–24. [CrossRef]
- Giakoumelou S, Wheelhouse N, Cuschieri K, Entrican G, Howie SE, Horne AW. The role of infection in miscarriage. Hum Reprod Update 2016, 22, 116–33. [CrossRef]
- Kurmanova AM, Kurmanova GM, Lokshin VN. Reproductive dysfunctions in viral hepatitis. Gynecol Endocrinol 2016, 32(sup2):37-40. [CrossRef]
- Li K, Chen G, Hou H, et al. Analysis of sex hormones and menstruation in COVID-19 women of child-bearing age. Reprod Biomed Online 2021, 42, 260–267. [CrossRef]
- Ding T, Wang T, Zhang J et al. Analysis of ovarian injury associated with COVID-19 disease in reproductive-aged women in Wuhan, China: an observational study. Front Med (Lausanne) 2021, 8, 635255. [CrossRef]
- Wang, M. , Yang, Q., Ren, X., Hu, J., Li, Z., Long, R., Xi, Q., Zhu, L., Jin, L. Investigating the impact of asymptomatic or mild SARS-CoV-2 infection on female fertility and in vitro fertilization outcomes: a retrospective cohort study. EClinicalMedicine 2021, 38: 101013. [CrossRef]
- Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), “Amenorrhea” (United States Government, 2021, https://www.nichd.nih.gov/health/topics/amenorrhea).
- Lord M, Sahni M. “Secondary Amenorrhea” in StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing (2022). https://www.ncbi.nlm.nih.gov/ books/NBK431055.
- Lee KMN, Junkins EJ, Luo C, Fatima UA, Cox ML, Clancy KBH. Investigating trends in those who experience menstrual bleeding changes after SARS-CoV-2 vaccination. Sci Adv 2022, 8, eabm7201. [CrossRef]
- Spini A, Giudice V, Brancaleone V, Morgese MG, De Francia S, Filippelli A, et al. Sex-tailored pharmacology and COVID-19: Next steps towards appropriateness and health equity. Pharmacol Res 2021, 173, 105848. [CrossRef]
- Amer AA, Amer SA, Alrufaidi KM, Abd-Elatif EE, Alafandi BZ, Yousif DA, et al. Menstrual changes after COVID-19 vaccination and/or SARS-CoV-2 infection and their demographic, mood, and lifestyle determinants in Arab women of childbearing age. Front Reprod Health 2022, 4, 927211. [CrossRef]
- Khan SM, Shilen A, Heslin KM, Ishimwe P, Allen AM, Jacobs ET al. SARS-CoV-2 infection and subsequent changes in the menstrual cycle among participants in the Arizona CoVHORT study. Am J Obstet Gynecol 2022, 226, 270–273. [CrossRef]
- Davis HE, Assaf GS, McCorkell L, Wei H, Low RJ, Re'em Y, et al. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [CrossRef]
- Barabás K, Makkai B, Farkas N, Horváth HR, Nagy Z, Váradi K, et al. Influence of COVID-19 pandemic and vaccination on the menstrual cycle: A retrospective study in Hungary. Front Endocrinol (Lausanne) 2022, 13: 974788. [CrossRef]
- Schoenbaum EE, Hartel D, Lo Y, et al. HIV infection, drug use, and onset of natural menopause. Clin Infect Dis 2005, 41, 1517–24. [CrossRef]
- Kallio ER, Helle H, Koskela E, Mappes T, Vapalahti O. Age-related effects of chronic hantavirus infection on female host fecundity. J Anim Ecol 2015, 84: 1264–1272. [CrossRef]
- Kurmanova AM, Kurmanova GM, Lokshin VN. Reproductive dysfunctions in viral hepatitis. Gynecol Endocrinol 2016, 32(sup2):37-40. [CrossRef]
- Giakoumelou S, Wheelhouse N, Cuschieri K, Entrican G, Howie SE, Horne AW. The role of infection in miscarriage. Hum Reprod Update 2016, 22, 116–33. [CrossRef]
- Ni W, Yang X, Yang D, Bao J, Li R, Xiao Y, et al. Role of angiotensin-converting enzyme 2 (ACE2) in COVID-19. Crit Care 2020, 24, 422. [CrossRef]
- Ho JQ, Sepand MR, Bigdelou B, Shekarian T, Esfandyarpour R, Chauhan P, et al. The immune response to COVID-19: Does sex matter? Immunology 2022, 166, 429–443. [CrossRef]
- Khan, N. Possible protective role of 17β-estradiol against COVID-19. J Allergy Infect Dis 2020, 1, 38–48. [Google Scholar] [CrossRef]
- Ding T, Zhang J, Wang T, Cui P, Chen Z, Jiang J, et al. Potential Influence of Menstrual Status and Sex Hormones on Female Severe Acute Respiratory Syndrome Coronavirus 2 Infection: A Cross-sectional Multicenter Study in Wuhan, China. Clin Infect Dis. 2021, 72, e240–e248. [CrossRef]
- Costeira R, Lee KA, Murray B, Christiansen C, Castillo-Fernandez J, Ni Lochlainn M, et al. Estrogen and COVID-19 symptoms: Associations in women from the COVID Symptom Study. PLoS One 2021, 16, e0257051. [CrossRef]
- Seeland U, Coluzzi F, Simmaco M, Mura C, Bourne PE, Heiland M, et al. Evidence for treatment with estradiol for women with SARS-CoV-2 infection. BMC Med 2020, 18, 369. [CrossRef]
- Suba, Z. Prevention and therapy of COVID-19 via exogenous estrogen treatment for both male and female patients. J Pharm Sci 2020, 23, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Mateus D, Sebastião AI, Carrascal MA, Carmo AD, Matos AM, Cruz MT. Crosstalk between estrogen, dendritic cells, and SARS-CoV-2 infection. Rev Med Virol 2022, 32, e2290. [CrossRef]
- Madjunkov M, Dviri M, Librach C. A comprehensive review of the impact of COVID-19 on human reproductive biology, assisted reproduction care and pregnancy: a Canadian perspective. J Ovarian Res 2020, 13, 140. [CrossRef]
- Salamanna F, Maglio M, Landini MP, Fini M. Body Localization of ACE-2: On the Trail of the Keyhole of SARS-CoV-2. Front Med (Lausanne) 2020, 7, 594495. [CrossRef]
- Sweet MG, Schmidt-Dalton TA, Weiss PM, Madsen KP. Evaluation and management of abnormal uterine bleeding in premenopausal women. Am Fam Physician 2012, 85, 35–43.
- Ray S, Ray A. Non-surgical interventions for treating heavy menstrual bleeding (menorrhagia) in women with bleeding disorders. Cochrane Database Syst Rev 2016, 11, CD010338. [CrossRef]
- Taga A, Lauria G. COVID-19 and the peripheral nervous system. A 2-year review from the pandemic to the vaccine era. J Peripher Nerv Syst 2022, 27, 4–30. [CrossRef]
- Albert, PR. Why is depression more prevalent in women? J Psychiatry Neurosci 2015, 40, 219–21. [Google Scholar] [CrossRef]
- Cherenack EM, Salazar AS, Nogueira NF, Raccamarich P, Rodriguez VJ, Mantero AM, et al. Infection with SARS-CoV-2 is associated with menstrual irregularities among women of reproductive age. PLoS One. 2022, 17, e0276131. [CrossRef]
- Scully EP, Haverfield J, Ursin RL, Tannenbaum C, Klein SL. Considering how biological sex impacts immune responses and COVID-19 outcomes. Nat Rev Immunol. 2020, 20, 442–447. [CrossRef]
- Word Health Organization (WHO). “The Sustainable Development Goals Report 2022” (2021, https://unstats.un.org/sdgs/report/2022/The-Sustainable-Development-Goals-Report-2022.pdf).
Figure 1.
STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) flow diagram.
Figure 1.
STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) flow diagram.
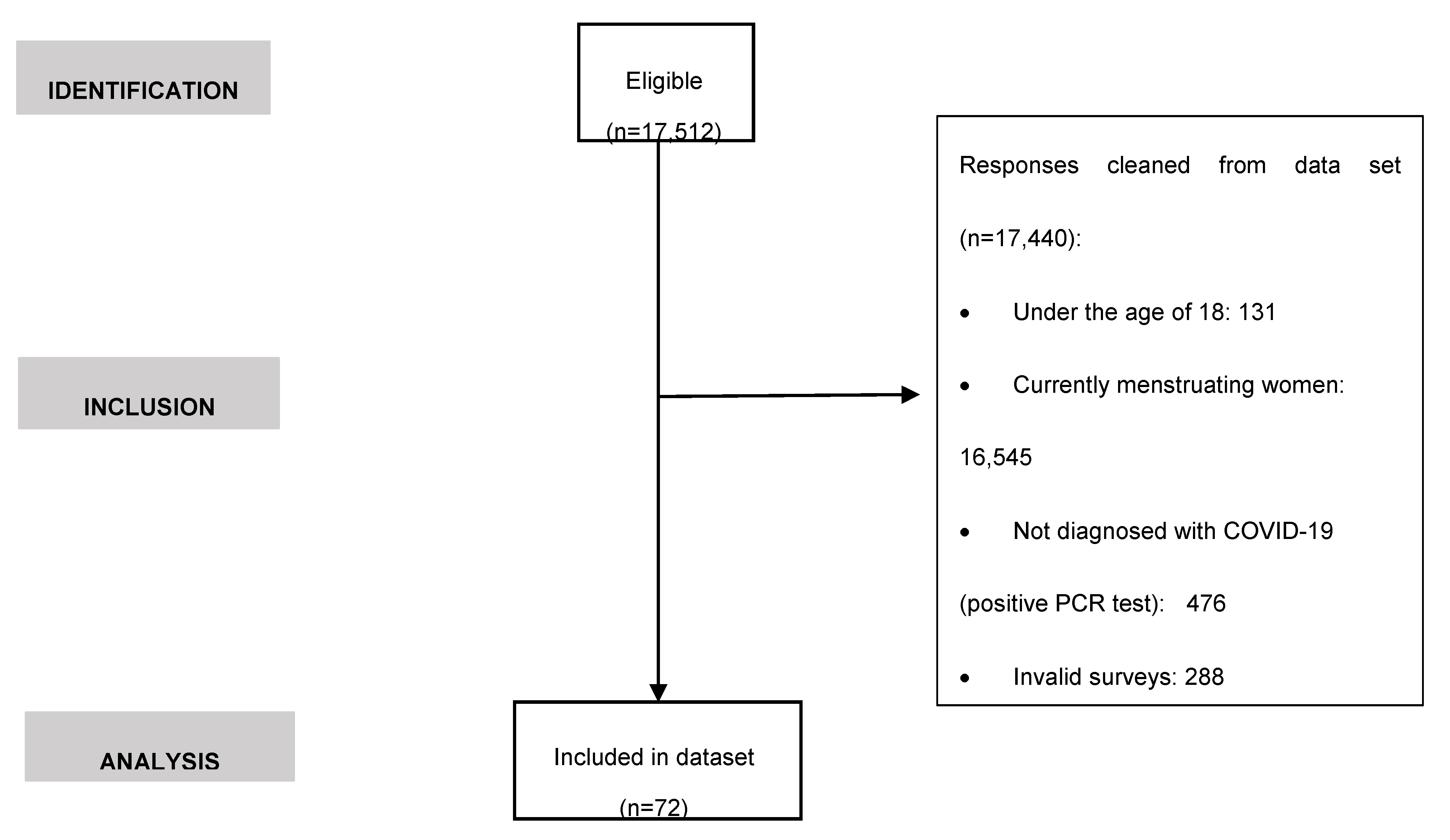
Table 1.
Anthropometric characteristics and medical history of the study population (formerly menstruating women, N=72).
Table 1.
Anthropometric characteristics and medical history of the study population (formerly menstruating women, N=72).
| Variable | Category | Total (N=27) | |
|---|---|---|---|
| Age (years) a | - | 41.4±11.4 | |
| Weight (kg) a | - | 66.5±13.2 | |
| Height (cm) a | - | 163.7±6.0 | |
| BMI a, b | - | 27.8±4.6 | |
| Underweight | 5 (6.9) | ||
| Normal weight | 41 (56.9) | ||
| Pre-obesity/overweight | 13 (18.1) | ||
| Obesity I | 12 (16.7) | ||
| Obesity II | 0 (0.0) | ||
| Obesity III | 1 (1.4) | ||
| Medical history b | |||
| Autoimmune diseases | Diagnosis | Yes | 14 (19.4) |
| No | 58 (19.4) | ||
| Comorbidity | Yes | 1 (7.1) | |
| No | 13 (92.9) | ||
| Types | Thyroid | 6 (8.3) | |
| Gastrointestinal | 3 (4.2) | ||
| Other | 3 (4.2) | ||
| Dermatological | 2 (2.8) | ||
| Rheumatic/articular | 2 (2.8) | ||
| Other clinical conditions | Diagnosis | Yes | 19 (27.1) |
| No | 51 (72.9) | ||
| Comorbidity | Yes | 5 (23.8) | |
| No | 16 (76.2) | ||
| Types | Other | 6 (8.3) | |
| Gynecological | 4 (5.6) | ||
| Cancer | 3 (4.2) | ||
| HPV | 3 (4.2) | ||
| Cardiovascular | 2 (2.8) | ||
| Gastrointestinal | 2 (2.8) | ||
| Neurological/mental | 1 (1.4) | ||
| Respiratory | 1 (1.4) | ||
| Rheumatic/articular | 1 (1.4) | ||
| Thyroid | 1 (1.4) | ||
| Dermatological | 0 (0.0) | ||
| Allergies | Diagnosis | Yes | 26 (36.1) |
| No | 46 (63.9) | ||
| Gynecological history a, b | |||
| Age 1st menstruation |
- | 12.8±1.4 | |
| Amenorrhea | Causes | Contraceptives | 23 (31.9) |
| Postmenopause | 16 (22.2) | ||
| Other | 14 (19.4) | ||
| Perimenopause | 16 (22.2) | ||
| Breastfeeding | 8 (11.1) | ||
| Current/ past use of contraceptives | Time of use | <10 years | 23 (31.9) |
| Types | >10 years | 6 (8.3) | |
| None | 43 (59.7) | ||
| Hormonal | 23 (31.9) | ||
| IUD (nonhormonal) | 6 (8.3) | ||
| Reproduction | Have you ever been pregnant? | Yes | 44 (61.1) |
| Nº pregnancies | No | 28 (38.9) | |
| 0-2 | 60 (83.3) | ||
| >2 | 16 (16.7) | ||
| Nº children | 0-2 | 68 (94.4) | |
| >2 | 4 (5.6) | ||
| Diseases | Diagnosis | Yes | 38 (52.8) |
| No | 34 (47.2) | ||
| Comorbidity | Yes | 7 (18.4) | |
| No | 34 (47.2) | ||
| Types | PCOS | 13 (18.1) | |
| EndometriosisHeavy menstrual bleeding | 8 (11.1)13(18.1) | ||
| Other | 8 (11.1) | ||
| Fibroids | 4 (5.6) | ||
| Menorrhagia | 1 (1.4) | ||
| Adenomyosis | 0 (0.0) | ||
| Uterine bleeding | 0 (0.0) |
Values are expressed as: a mean±standard deviation; b n (%). Abbreviations: IDU, Intrauterine Device; BMI, Body Mass Index; PCOS, Polycystic Ovary Syndrome; HPV, Human Papillomavirus.
Table 3.
Differences in the study variables according the occurrence or not of MRD after suffering from COVID-19 disease in the study population (formerly menstruating women, N=72).
Table 3.
Differences in the study variables according the occurrence or not of MRD after suffering from COVID-19 disease in the study population (formerly menstruating women, N=72).
| Subgroup | ||||||
|---|---|---|---|---|---|---|
| Variable | Category | n-MRD (n=44) |
MRD (n=28) |
X2 | p-value | |
| Age (years)a | 41.4±12.3 | 41.5±9.9 | - | 0.954 | ||
| Weight (kg)a | - | 66.1±13.8 | 67.0±12.5 | - | 0.785 | |
| Height (cm)a | - | 163.6±6.5 | 163.8±5.3 | - | 0.889 | |
| BMI a,b | - | 24.7±5.0 | 24.9±4.1 | - | 0.768 | |
| Underweight | 3 (6.8) | 2 (7.1) | 0.683 | |||
| Normal weight | 27 (61.4) | 14 (50.0) | ||||
| Pre-obesity/ overweight | 6 (13.6) | 7 (25.0) | ||||
| Obesity I | 7 (15.9) | 5 (17.9) | ||||
| Obesity II | 0 (0.0) | 0 (0.0) | ||||
| Obesity III | 1 (2.3) | 0 (0.0) | ||||
| Medical history b | ||||||
| Autoimmune diseases | Types | Dermatological | 1 (2.3) | 1 (3.6) | 0.107 | 0.744 |
| Gastrointestinal | 1 (2.3) | 2 (7.1) | 1.016 | 0.313 | ||
| Rheumatics/ articular | 1 (2.3) | 1 (3.6) | 0.107 | 0.744 | ||
| Other | 3 (6.8) | 0 (0.0) | 1.992 | 0.158 | ||
| Thyroid | 3 (6.8) | 3 (10.7) | 0.340 | 0.560 | ||
| Other clinical conditions | Types | Cardiovascular | 1 (2.3) | 1 (3.6) | 0.107 | 0.744 |
| Cancer | 2 (4.5) | 1 (3.6) | 0.041 | 0.840 | ||
| Dermatological | 0 (0.0) | 0 (0.0) | ||||
| Gastrointestinal | 2 (4.5) | 0 (0.0) | 1.309 | 0.253 | ||
| Gynecological | 3 (6.8) | 1 (3.6) | 0.344 | 0.558 | ||
| Neurological/ mental | 1 (2.3) | 0 (0.0) | 0.645 | 0.422 | ||
| Other | 4 (9.1) | 2 (7.1) | 0.085 | 0.711 | ||
| Respiratory | 0 (0.0) | 1 (3.6) | 1.594 | 0.207 | ||
| Rheumatic/ articular | 0 (0.0) | 1 (3.6) | 1.594 | 0.207 | ||
| Thyroid | 1 (2.3) | 0 (0.0) | 0.645 | 0.422 | ||
| HPV | 1 (2.3) | 2 (7.1) | 1.016 | 0.313 | ||
| Allergies | - | 31 (70.5) | 13 (29.5) | 2.114 | 0.146 | |
| Gynecological history a,b | ||||||
| Age 1st menstruation | - | 12.7±14 | 12.8±1.4 | 0.921 | ||
| Contraceptives | Time of use | <10 years | 12 (27.3) | 11 (39.3) | 1.810 | 0.405 |
| >10 years | 3 (6.8) | 3 (10.7) | ||||
| Types | None | 29 (65.9) | 14 (50.0) | 2.511 | 0.285 | |
| Hormonal | 11 (25.0) | 12 (42.9) | ||||
| IUD (nonhormonal) | 4 (9.1) | 2 (7.1) | ||||
| Reproduction | Have you ever been pregnant? | Yes | 27 (61.4) | 17 (60.7) | 0.003 | 0.956 |
| No | 17 (38.6) | 11 (39.3) | ||||
| Nº pregnancies | 0-2 | 37 (84.1) | 23 (82.1) | 0.047 | 0.29 | |
| > 2 | 7 (15.9) | 5 (17.9) | ||||
| Nº children | 0-2 | 40 (90.9) | 28 (100.0) | 2.695 | 0.101 | |
| > 2 | 4 (9.1) | 0 (0.0) | ||||
| Amenorrhea | Types | Perimenopause | 3 (6.8) | 8 (28.6) * | 6.809 | 0.033 |
| Postmenopause | 12 (27.3) | 4 (14.3) | ||||
| Other | 29 (65.9) | 16 (57.1) | ||||
| Diseases | Types | Adenomyosis | 0 (0.0) | 0 (0.0) | ||
| Endometriosis | 3 (6.8) | 5 (17.9) | 2.111 | 0.146 | ||
| Fibroids | 2 (4.5) | 2 (7.1) | 0.220 | 0.639 | ||
| Menorrhagia | 0 (0.0) | 1 (3.6) | 1.594 | 0.207 | ||
| Other | 5 (11.4) | 3 (10.7) | 0.007 | 0.932 | ||
| Heavy menstrual bleeding | 4 (9.1) | 9 (32.1) * | 6.146 | 0.013 | ||
| Uterine bleeding | 0(0.0) | 0(0.0) | ||||
| PCOS | 8 (18.2) | 5 (17.9) | 0.001 | 0.972 | ||
| COVID-19 | ||||||
| Date of COVID-19 diagnosis (pandemic waves) |
1st wave | 15 (34.1) | 6 (21.4) | 10.378 | 0.035 | |
| 2nd wave | 9 (20.5) | 8 (28.6) | ||||
| 3rd wave | 10 (22.7) | 2 (7.1) | ||||
| 4th wave | 1 (2.3) | 6 (21.4) * | ||||
| 5th wave | 9 (20.5) | 6 (21.4) | ||||
| Hospitalization | Yes | 0 (0.0) | 2 (7.1) | 3.233 | 0.072 | |
| No | 44 (100.0) | 26 (92.9) |
Values are expressed as: a mean ± standard deviation; b n (%). *p<0.05 vs. subgroup n-MRD. Abbreviations: BMI, Body Mass Index; IDU, Intrauterine Device; MRD: menstrual-related disturbances subgroup; n-MRD: non-menstrual-related disturbances subgroup; PCOS, Polycystic Ovary Syndrome; HPV, Human Papillomavirus.
Table 4.
Factors associated with the occurrence of MRD after suffering from COVID-19 disease (formerly menstruating women, N=72): binary logistic regression.
Table 4.
Factors associated with the occurrence of MRD after suffering from COVID-19 disease (formerly menstruating women, N=72): binary logistic regression.
| Subgroup MRD (n=28) | |||
|---|---|---|---|
| Variable | Category | AOR(CI95%) | p-value |
| Amenorrhea | Perimenopause | 4.608(1.018-20.856) | 0.047 |
| Postmenopause | 0.541(0.139-2.103) | 0.375 | |
| Other | 1 | ||
| Gynecological history | |||
| Heavy menstrual bleeding | Yes | 4.857(1.239-19.031) | 0.023 |
| No | 1 |
Note: Reference group: Do not experience changes COVID-19 disease-related. AOR: adjusted odd ratio; CI 95%: confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



