
Submitted:
06 June 2023
Posted:
07 June 2023
You are already at the latest version
Abstract
Systemic lupus erythematosus (SLE), the prototype of systemic autoimmune diseases is characterized by extreme heterogeneity with a variable clinical course. Renal involvement may be observed and affects the outcome. Hydroxychloroquine is the cornerstone of lupus treatment. Conventional immunosuppressive therapy includes corticosteroids, methotrexate, azathioprine, cyclosporine and tacrolimus. Cyclophosphamide and mycophenolate mofetil may also be used. However, despite conventional immunosuppressive treatment flares occur and broad immunosuppression is accompanied by multiple side effects. Flare occurrence, target organ involvement, side effects of broad immunosuppression, increased knowledge of the pathogenetic mechanisms involved in SLE pathogenesis as well as the availability of biologic agents has led to the application of biologic agents in SLE management. Biologic agents targeting various pathogenetic paths have been applied. B cell targeting agents have been used successfully. Belimumab, a B cell targeting agent has been approved for the treatment of SLE. Rituximab, an anti-CD20 targeting agent is also used in SLE. Anifrolumab, an interferon I receptor targeting agent has beneficial effects on SLE. In conclusion, biologic treatment is applied in SLE and should be further evaluated with the aim of a good treatment response and a significant improvement in quality of life.
Keywords:
systemic lupus erythematosus
; treatment
; hydroxychloroquine
; corticosteroids
; biologic agents
; belimumab
; rituximab
; anifrolumab
; tocilizumab
; baricitinib
1. Introduction
Systemic lupus erythematosus (SLE), the prototype of autoimmune diseases, is a highly heterogenous disease, affects all organ systems and has an unpredictable course [1]. Its course ranges from mild to severe fatal disease [2]. Women within the reproductive period are mainly affected [3]. Females originating from Africa or Asia are frequently affected and may exhibit severe disease manifestations [3]. SLE treatment is the focus of scientific research as biologic agents and small molecules enter management of the disease [4].
SLE follows a variable and unpredictable course [5]. It can be chronic or follow a relapsing remitting course. The disease may present with serious musculoskeletal, cardiovascular and ocular manifestations [6]. Many of those are disease manifestations or may be due to the application of corticosteroids for disease management [7]. In 2014 the principle “treat to target” was introduced into the treatment strategy of SLE [8]. Flares, target organ involvement, refractory disease, adverse effects of conventional immunosuppressive agents, better understanding of molecular pathogenesis of SLE as well as the availability of biologic agents led to the application of biologic agents and small molecules in SLE treatment [9,10]. New biologic agents are in development for the management of SLE with various molecular therapeutic targets. Hydroxychloroquine is the standard mainstay treatment of SLE and it is recommended by EULAR for patients with symptoms but without major organ lesions [11]. Corticosteroids are administered for the treatment of SLE, but they induce broad immunosuppression and their use is accompanied by side effects. Hence, it has been proposed that glucocorticoid use should be limited to the shortest possible time and the lower dose possible. For patients who do not respond to hydroxychloroquine and glucocorticoid dosage cannot be reduced azathioprine and methotrexate are recommended. For patients with severe organ lesions and high disease activity the use of immunosuppressive agents, pulse cyclophosphamide and mycophenolate mofetil may be applied along with hydroxychloroquine as standard treatment. As standard immunosuppressive treatment is non-specific biologic agents have been developed and several others are in development with the aim to achieve targeted immunomodulation, disease remission and improved quality of life. Belimumab, an anti-B cell biologic has been approved for the management of SLE. Rituximab, an anti-CD20 antibody targeting B lymphocytes is also used in severe SLE. Anifrolumab, an interferon I receptor antagonist, is applied successfully in the treatment of SLE. In the present review, the therapeutic management and the introduction of biologic agents and small molecules in SLE treatment along with recent progress and new horizons in the matter will be discussed.
2. Methods
All articles published in PubMed regarding treatment in SLE in a period from 2000 to 2022 were reviewed. Articles reviewed included clinical trials and reviews. The search was limited to articles in the English language. After elimination of duplicates eligible articles were read and evaluated (Figure 1). The search methodology was that of the PRISMA 2020 flow chart [12].
3. Systemic lupus erythematosus treatment
3.1. Antimalarials
Hydroxychloroquine, an antimalarial, when taken by soldiers during the Second World War for the prevention of malaria was shown to improve musculoskeletal complaints. Hence, it was applied in the treatment of rheumatic conditions. Hydroxychloroquine is now considered standard of care treatment of SLE as it was shown to significantly reduce mortality in all ethnic groups [13,14,15], unless there are contraindications to it [16,17]. It is applied in discoid lupus and SLE [18]. Hydroxychloroquine modulates the immune response by modulating macrophage and other antigen presenting cell function [19,20] and by blocking Toll-like receptors on dendritic cells [21]. Hydroxychloroquine prevents lupus flares, increases survival in all populations groups and decreases lupus activity in pregnancy without adverse effects on the fetus [22]. Hydroxychloroquine may also prevent irreversible organ damage, bone destruction and thrombosis [23]. Hydroxychloroquine reduces disease activity in SLE, improves lipid levels and prevents subclinical atherosclerosis [24]. The antimalarial agent also improves glucose metabolism [25]. If attention is paid to dosage, antimalarial toxicity is mild, does not occur frequently and is usually reversible. Ruiz-Irastorza et al. declared that hydroxychloroquine is a cornerstone in the treatment of lupus patients and that its administration should last for all disease duration [26]. Discontinuation of hydroxychloroquine is performed when retinopathy is suspected or documented and may improve the electroretinogram in cases of suspected retinopathy [27].
3.2. Glucocorticoids
Glucocorticoids are used in SLE in large bolus doses and small doses as maintenance treatment [28] to reduce disease activity and disease burden accumulation. They act by a genomic pathway, involving a transrepressive and transactivating mode of action on the cell nucleus and by a non-genomic pathway29. However, they induce broad immunosuppression and their use is accompanied by side effects. Therefore, it has been suggested that their use should be limited in time and dose as much as possible [30,31].
3.3. Azathioprine
3.4. Methotrexate
If low dose glucocorticoids do not control the disease, methotrexate may be applied as an immunosuppressive agent and contributes to steroid sparing [34,35]. Methotrexate has an antifolate mechanism of action [36]. It is indicated in lupus patients who display an inadequate response to hydroxychloroquine and in patients with cutaneous and articular involvement37, without renal disease. Methotrexate enters cells through a folate transporter [35]. Once within the cell, methotrexate as monoglutamate forms polyglutamates, a more potent drug form which inhibit various enzymes leading to increased adenosine levels [38], decreased production of ammonium and H2O2 and decreased synthesis of purines, methionine and DNA. Adenosine is a molecule with anti-inflammatory effects [39]. Methotrexate is administered in moderate or severe lupus, which does not respond to hydroxycholoroquine with the aim of steroid sparing. It has been shown to reduce disease activity in lupus patients as well as to allow reduction of glucocorticoid dosage [40] and to be beneficial in patients with articular and cutaneous involvement [41]. It is teratogenic and it should be withdrawn before conception [42].
3.5. Mycophenolate mofetil
Mycophenolate mofetil (MMF) inhibits inosine 5-monophosphate dehydrogenase thereby inhibiting the synthesis of guanine. Thus, B cells, T cells and fibroblasts are decreased. MMF also reduces transforming growth factor β and fibronectin synthesis thereby exhibiting antifibrotic effects [43]. MMF inhibits expression of cell adhesion molecules thereby interfering with the recruitment of lymphocytes and monocytes in sites of inflammation. It may also induce T cell apoptosis [44]. The first trial in lupus with MMF was performed in 2000. Thereafter MMF became a standard drug for the treatment of lupus nephritis [45]. It is also used in non-renal lupus. Good quality studies performed in patients with lupus nephritis have proven that MMF is equivalent to iv cyclophosphamide and equivalent or superior to azathioprine during maintenance treatment [46,47,48,49,50]. Beneficial effects of MMF are observed in patients with hematological involvement, refractory cutaneous manifestations and arthritis. MMF is less toxic than cyclophosphamide. It displays gastrointestinal side effects, suppresses the bone marrow, and increases the risk of infection. Long-term cancer risk is raised due to its immunosuppressive action. It should be said that there are subgroups of patients with specific susceptibility to the agent, such as an Asian subgroup which is extremely sensitive to MMF if combined with high-dose glucocorticoids [51,52,53]. In African Americans in high risk for the development of renal involvement MMF effectively prevents exacerbation of renal lupus [54].
3.6. Cyclophosphamide
Cyclophosphamide is an alkylating drug which acts on DNA and leads to the death of activated lymphocytes while simultaneously it has a protective effect on glomeruli [55,56]. Cyclophosphamide displays side effects such as leukopenia, an increased infection risk, bladder toxicity and an increased cancer risk [57]. Cyclophosphamide may be applied as induction therapy for flares or target organ involvement [53,58]. Thereafter, it is replaced by other conventional immunosuppressive drugs to achieve maintenance treatment.
3.7. Calcineurin inhibitors
Calcineurin inhibitors tacrolimus and cyclosporine have been applied as immunosuppressives in organ transplantation. They modulate the immune response mainly by inhibiting T cell activation. Additionally, they reduce albuminuria and preserve renal function [59]. In SLE without renal involvement cyclosporine contributes to lowering steroid dosage, reduced disease activity and flare prevention [60] by modulating T cell function [61,62]. Tacrolimus is administered combined with MMF and steroids as induction therapy in renal lupus with beneficial effects [63,64,65]. It is also used successfully in refractory lupus nephritis [66]. However, serious adverse events are observed such as infections and diabetic metabolic derangement. Cyclosporine is also successfully applied in non- responsive to treatment lupus nephritis, with main adverse events observed tremor and hypertension [66]. Voclosporin is a new calcineurin inhibitor which has been approved for the treatment of lupus nephritis [67,68]. Voclosporin co-administered with MMF and low dose steroids led to more patients achieving a complete renal response as opposed to the combination of MMF with steroids [69].
3.8. Intravenous immunoglobulin
Therapeutic intravenous immunoglobulin (IVIg) is a product which contains human multi-specific immunoglobulin G. IVIg has been used successfully in lupus patients leading to a reduction of disease activity [70]. IVIg was shown to be effective for various manifestations in SLE. It was shown to be effective for renal disease in SLE, as well as target organ manifestations such as thrombocytopenia, refractory neuropsychiatric lupus [71] and lupus myocarditis [72]. IVIg may act via various mechanisms including the inhibition of autoreactive B lymphocytes [73]. IVIg is a safe and beneficial mode of treatment for patients with SLE [74] who are resistant to or deny other types of treatment.
4. Biologic treatment in systemic lupus erythematosus
Flare occurrence, target organ involvement, inadequate response of some SLE patients to conventional immunosuppressive treatment and the side effects of broad immunosuppressives as well as the increasing and deeper study of disease pathogenesis have led to the application of biologic agents in SLE treatment [9]. Agents targeting various pathogenetic paths have been applied and others are being studied [9,28]. In particular, B cell targeting agents, interferon targeting agents, TNFa inhibitors and other biologic agents are investigated.
Biologic drugs which are in use with beneficial effects in SLE are rituximab [75,76,77] and belimumab [78,79,80,81]. The use of rituximab followed by belimumab is also investigated [82,83]. Other B cell targeting biologic agents are also studied [84]. A variety of biologic drugs targeting various molecular pathways have been introduced in treatment schedules for SLE with refractoriness or intolerance to standard of care treatment [85] (Figure 2). The aim of the introduction of biologics into SLE treatment is the induction of disease remission and the establishment of self-tolerance [86,87]. This aim has not yet been reached. Further research and deeper understanding of disease heterogeneity and molecular mechanisms involved in SLE pathogenesis may lead to the development of agents targeting specific pathogenetic pathways which may be efficacious in specific groups of SLE patients [85].
4.1. B cell targeted treatment
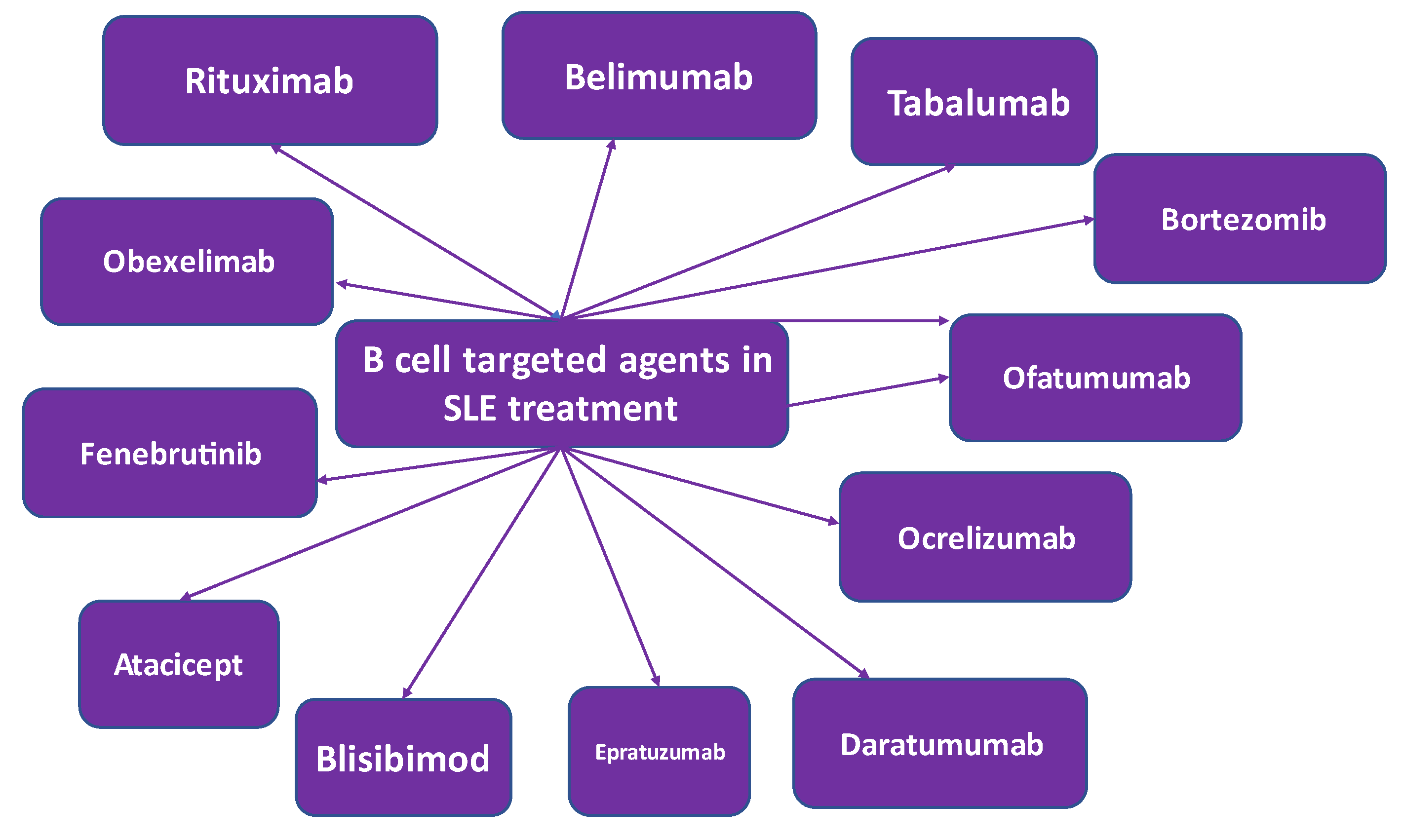
SLE pathophysiology is characterized by B cell involvement [88,89]. Therefore, various therapeutic strategies targeting the B cell have been applied [90,91]. B lymphocytes are involved in antibody dependent and antibody independent mechanisms in SLE pathogenesis. Autoantibodies are produced by B cells which are self-reacting thereby triggering an inflammatory response. In health B cells produce protective antibodies [92]. In SLE autoantibodies are produced which are involved in triggering an inflammatory response via multiple mechanisms including the induction of cytokine and interferon production by innate immune cells [93]. This immune mechanism is perturbed in SLE patients and is further deranged by abnormal functioning of other immune cells [94]. Treatment methods have been developed and are in development which target the B cell [90,91] (Figure 3). Agents involved in growth, activation or proliferation of B cells are treatment targets. Additionally, molecules expressed by B cell subpopulations have been discovered which if targeted may lead to their depletion, anergy and apoptosis [78,95,96,97,98].
An aim in the management of SLE is steroid withdrawal, as it is accompanied by broad immunosuppression and is fraught with side effects [30]. To this end the use of targeted immunosuppression has been attempted and has been found to improve outcome, for some but not all patients and for some but not all agents applied [28,99]. B cells express various cell surface antigens depending on the stage of maturation. B cells, mature and immature express CD20 and CD22 which are B cell surface antigens. These surface antigens are not expressed by plasma cells. It has been suggested that SLE treatment failure in patients administered agents targeting B-cell surface antigens, may be due plasma cells which do not express CD20. This led to the application of alternative B cell targets like B lymphocyte stimulator (BlyS), known as B cell activating factor BAFF and proliferating inducing ligand (APRIL), which are members of the TNF cytokine group and are applied as targets in the treatment of SLE. Elevated BlyS levels are found in the circulation in lupus patients and are associated with disease activity. These data led to the identification of BlyS as a target for SLE treatment. Intracellular signaling molecules involved in B cell activation include Bruton’s tyrosine kinase. Inhibition of Bruton’s tyrosine kinase is investigated in SLE therapy [100,101]. A proteasome inhibitor which specifically inhibits B cell differentiation, is also studied and works via a toxic effect on plasma cells.
4.1.1. Rituximab
Rituximab is a B cell depleting anti-CD20 monoclonal antibody applied as a B cell targeted treatment. Rituximab depletes CD20-positive B cells, however it spares stem cells and plasma cells as they do not express the CD20 molecule [102,103]. Rituximab depletes B cells by antibody-dependent and complement mediated cytotoxicity [104]. It induces B cell apoptosis and reduces proliferation. Rituximab may be used to treat refractory SLE with renal and neuropsychiatric manifestations [105,106,107]. In a comprehensive review rituximab was shown to induce a significant improvement in systemic manifestations in >90% of lupus cases [108]. Rituximab has not yet been approved by the FDA for SLE treatment, as some trials failed to achieve their primary endpoints109.
Rituximab has been evaluated in the treatment of SLE in the randomized controlled trials, EXPLORER and Lupus Nephritis Assessment trial. Rituximab was found to be effective in refractory SLE [110,111], safe and effective in non-renal SLE [111] and effective in refractory neuropsychiatric SLE [112]. Rituximab reduces disease activity, immunologic parameters and contributs to lowering the steroid dosage. It is beneficial in the treatment of arthritis and thrombocytopenia. In comparison to MMF and cyclophosphamide it was shown to be equally effective in renal disease in lupus [113]. Incomplete B cell depletion is observed as CD20 is not expressed by early B cells and plasma cells [114]. Rituximab normalizes B cell subsets in SLE patients [105]. Early on it was thought that complete B cell depletion might bring about a better outcome for SLE [105]. However, SLE flares were observed after repeated rituximab administration. Flares were attributed to elevated circulating CD257 (BLyS) levels and increased anti-dsDNA levels [115,116]. Hence, it was proposed that rituximab administration acting via B cell depletion might have paradoxically increased CD257 levels thereby leading to higher SLE activity [114]. Rituximab B cell depletion paradoxically induced peripheral B cell reconstitution and an increase in plasmablasts, which may lead to T helper cell stimulation, autoantibody production and an augmentation in disease activity [114]. Thereafter, rituximab is contemplated for introduction in the management of lupus nephritis only after failure of conventional immunosuppressants or in relapses of lupus nephritis [117]. Despite that, a study with rituximab indicated complete response of renal lupus [118].
4.1.2. Belimumab
Belimumab is a fully humanized monoclonal antibody against BlyS. It has been administered in clinical trials intravenously and subcutaneously. Belimumab was approved by the FDA for the treatment of seropositive, moderate SLE. Two international clinical trials [78,119] in autoantibody-positive adult patients with active SLE evaluated belimumab. SLE patients were randomized to receive either belimumab or placebo in addition to standard-of-care treatment. Both trials achieved their primary endpoints, demonstrated reduced SLE disease activity and flares. Analysis of these trials documented that the rate of lupus disease flares, serologic activity and steroid dosage were significantly reduced while quality of life was improved by belimumab plus standard of care SLE therapy [120]. Belimumab applied subcutaneously also displayed good efficacy as it decreased disease flares and enabled steroid sparing. Belimumab has also been approved by the FDA for the treatment of autoantibody positive moderate SLE in children. Belimumab is an anti-CD257 monoclonal antibody and was the first agent to be approved by the FDA for SLE over a period of time of more than 50 years [121,122,123,124,125,126,127,128]. Belimumab should be contemplated in lupus patients without renal involvement responding inadequately to hydroxychloroquine, glucocorticoids and immunosuppressants [129]. A better response is observed in patients with cutaneous and musculoskeletal involvement. Belimumab has been shown to decrease albuminuria and improve neuropsychiatric manifestations in lupus [130]. In lupus nephritis patients belimumab led to a primary efficacy renal response and complete renal response [119]. Belimumab lowered the risk of a death related to kidney involvement. The sequential use of rituximab followed by belimumab has also been attempted in several trials [131,132], as well as the concurrent use of belimumab and rituximab, with promising results [133], showing a possible synergistic effect [82].
4.1.3. Tabalumab
Tabalumab, is a monoclonal antibody against soluble and membrane-bound BlyS [134]. Tabalumab was tested in two phase III trials, namely ILLUMINATE-1 and ILLUMINATE-2 in adult patients with moderate to severe SLE without kidney involvement [96,134]. ILLUMINATE-1 did not meet the primary efficacy endpoint in the tamalumab arm, as opposed to ILLUMINATE-2 in which the SRI_5 response was met, in the cohort receiving tabalumab 120 mg twice monthly. Depression was observed in some patients on tabalumab and some patients attempted suicide.
4.1.4. Atacicept
Atacicept is an antagonist of BlyS and APRIL mediated B cell activation. It is a fused protein of the TACI (transmembrane activator calcium moderator and cyclophilin ligand interactor) and IgG, which binds to both Blys and APRIL. As both BlyS and APRIL have been found to be increased in SLE patients, it was suggested that the dual blockade by atacicept might be more effective than BlyS blocking [97]. Atacicept was tested in a phase II b study in SLE patients [135]. However, it did not meet the primary endpoint of the trial in any of its arms, although in a secondary analysis of patients with active disease atacicept was found to meet primary endpoints and to decrease flare risk. However, deaths due to alveolar hemorrhage in the context of pneumonia were noted in the atacicept arm of the trial.
4.1.5. Blisibimod
Blisibimod is a moiety which inhibits BlyS and displays characteristics of a peptide and an antibody. It was tested in a phase II trial in SLE and did not meet the primary efficacy endpoint of SRI-5 response [136]. A beneficial treatment effect was observed in SLE patients with high disease activity, where it appeared to be effective in lowering the steroid dosage [137]. The drug appeared to be well tolerated with no serious reported adverse events and no deaths in the treatment arms.
4.1.6. Epratuzumab
Epratuzumab is a monoclonal antibody against CD22. It binds to CD22 thereby inhibiting B cell activation [138,139]. CD22 is a molecule which is expressed on mature B cells, not on plasma cells or memory B cells and acts as an inhibitory co-receptor of the B cell receptor and modulates B cell activation and migration. A failure in medication supply led to the premature termination of epratuzumab phase II and III trials. Consequently, 2 phase III clinical studies, namely EMBODY-1 and EMBODY-2, indicated initial rapid improvement in SLE patients but they did not achieve their primary efficacy endpoint [140].
4.1.7. Daratumumab
Daratumumab is a monoclonal antibody against CD38, a molecule expressed on plasmablasts [141]. CD38 is expressed on plasmablasts, CD19+ mature B cells and plasmacytoid dendritic cells in lupus patients. Daratumumab has been administered to two female patients with lupus nephritis and autoimmune hemolytic anemia not responding to immunosuppression [142]. Patients were administered belimumab after the unsuccessful administration of daratumumab.
4.1.8. Ocrelizumab
Ocrelizumab is a fully humanized monoclonal antibody against CD20 with higher antibody dependent complement and lower complement dependent cytotoxicity effects as compared to rituximab in SLE patients [143]. Ocrelizumab is successfully used in relapsing remitting and primary progressive multiple sclerosis [144]. Ocrelizumab was tested in patients with lupus nephritis with beneficial effects but it displayed a high rate of serious infections [145].
4.1.9. Obinutuzumab
Obinutuzumab, a novel humanized type II glycoengineered anti-CD20 antibody, is a B-cell targeting treatment which may be administered in SLE patients [141,146]. Studies performed in vitro indicated that obinutuzumab may induce higher B cell cytotoxicity as compared to rituximab in SLE [146,147]. Thereafter, it was suggested that in lupus patients not responding to rituximab obinutuzumab might be a choice [148].
4.1.10. Ofatumumab
Ofatumumab is a fully humanized anti-CD20 monoclonal antibody. It has been applied as a B cell-depleting agent which may be used in patients with SLE intolerant to rituximab, i.e., in patients who develop infusion reactions to rituximab [149,150]. It induces antibody and complement dependent cytotoxicity in B lymphocytes expressing CD20. Ofatumumab exhibits potency in B cells lysis, which stems from its ability to bind with high affinity to the short extracellular part of the CD20 molecule and its slow release from the target molecule. Ofatumumab has been used in an SLE patient with low complement levels combined with fresh frozen plasma [151]. Lupus patients intolerant to rituximab infusion may be administered ofatumumab [149]. It is well accepted and may represent an alternative B cell targeted treatment in SLE.
4.1.11. Obexelimab
Obexelimab is a humanized anti-CD19 monoclonal antibody targeting FcgRIIb, which is a reversible B-cell inhibitor [141]. CD-19 is a cell surface molecule found on B cells, plasmablasts and plasma cells [152]. It was hypothesized that targeting CD19 could lead to a significant B and plasma cell depletion of B cells in lupus patients. Obexelimab was tested in a phase II randomized trial in moderately active lupus patients. However, it did not meet its primary end point and further studies were not conducted.
4.1.12. Bruton’s Tyrosine Kinase-Targeted Treatment
Currently, B-cell signaling is a target for B-cell treatment in SLE. Tyrosine kinases, in particular Bruton’s tyrosine kinase, acts as an intracellular molecule essential for the development, survival and activation of B cells. Bruton’s tyrosine kinase is involved in antigen presentation, B-cell differentiation and production of autoantibodies in SLE [153]. In experimental animal models, Bruton’s tyrosine kinase inhibition was shown to have beneficial effects in SLE [154].
In a phase II trial fenebrutinib, an oral highly selective inhibitor of Bruton’s tyrosine kinase, was tested in moderate to severe SLE in addition to standard of care treatment [101]. The trial did not meet its primary endpoint, however beneficial effects of fenebrutinib in SLE were observed. Ibrutinib, another irreversible tyrosine kinase selective inhibitor was tested in lupus nephritis mouse models [155].
4.1.13. Proteasome Inhibitors
CD-20 negative cells may be source of treatment failures with CD-20 targeting agents. CD-20 negative cells may be targeted by inhibiting the proteasome. Proteasome inhibition leads to accumulation of defective immunoglobulin chains, induces stress in the endoplasmic reticulum leading to plasma cell apoptosis [156]. Bortezomib is a proteasome inhibitor which has been tested in animal models of lupus [157]. Bortezomib was also tested in SLE patients. Bortezomib was tested in severe refractory lupus nephritis [158] and exhibited good results in SLE [156,159]. However, severe side effects observed led to the idea that it might be used only as salvage treatment for refractory lupus patients. Thus, bortezomib may be used in SLE patients with very active disease, who have been already treated with rituximab.
4.1.14. Rigerimod
Rigerimod is a peptide which blocks antigen presentation to T cells by reducing the stability of MHC molecules thereby inhibiting B cell function. Rigerimod has been applied in lupus patients with encouraging results [160].
4.2. Interferon inhibitors
4.2.1. Sifalimumab
Interferons (IFNs) are immunostimulatory cytokines divided in three categoris, type I, II and III [161]. IFNα is a type I IFN which is abundant and has been studied in depth. The role of interferons in the pathogenesis of SLE has been extensively studied and has been proved [162]. Sifalimumab is a fully human monoclonal antibody against IFN-α subtypes and has shown a beneficial effect in a phase IIb clinical trial in SLE [163].
4.2.2. Anifrolumab
Type I IFN may be implicated in the pathogenesis of SLE. A gain-of -function genetic mutation in type I IFN pathway may be associated with a higher risk of SLE [164]. In the period before the clinical presentation of SLE high type I IFN and SLE autoantibodies have been observed. Patients with established SLE and evidence of high type I IFN may have more active disease and lupus nephritis or other severe manifestations. As reiterated previously within this review, there is a need for new therapeutic modalities in SLE, as existing therapeutic agents have adverse effects. Type I IFNs are mediated by type I IFN-α/β/ω receptor, known as IFNAR. Anifrolumab, a fully human immunoglobulin G1k antibody which binds IFNAR, a type I interferon receptor antagonist, showed good results in patients suffering from scleroderma. As similarities have been observed in the type I IFN response between scleroderma and SLE, anifrolumab was tested in patients with SLE. The MUSE (MEDI-546 in Uncontrolled Systemic Lupus) trial was implemented to assess the safety and efficacy of anifrolumab. This trial was followed by the phase 3 trials TULIP-1 (Treatment of Uncontrolled Lupus via the Interferon Pathway-10) and TULIP-2 (Treatment of Uncontrolled Lupus via the Interferon Pathway-2) [165]. These trials led to the approval of anifrolumab by the FDA for moderate to severe SLE, excluding patients with lupus nephritis or central nervous system involvement [166]. It was also approved by EMA during 2022, as additional treatment for adult patients with moderate to severe SLE, despite conventional treatment. The MUSE trial showed positive effects in its primary end point. The TULIP-2 trial reached also its primary endpoint. The most significant adverse effect of anifrolumab was herpes zoster.
4.4. Interleukin inhibitors
4.4.1. Tocilizumab
Tocilizumab, is a humanized monoclonal antibody against interleukin-6 receptor [167] which has been mainly used in the treatment of rheumatoid arthritis [168] and is also applied in giant cell arteritis [169]. Tocilizumab has been also used in patients with severe infections from the SARS-CoV-2 virus [170]. Tocilizumab has been applied to treat refractory hemolytic anemia in an SLE patient [171]. It has also been used in an adolescent patient with SLE and a pleural effusion [172]. It has also been used successfully in SLE patients with persistent high grade fever, resistant to treatment with antibiotics and corticosteroids [173]. Tocilizumab administration has been shown to have beneficial effects in lupus patients with arthritis [174]. However, neutropenia and risk of infection are factors limiting its use in SLE.
4.4.2. Secukinumab
Secukinumab is a monoclonal antibody which binds to interleukin 17A. It is used in ankylosing spondylitis, psoriasis and psoriatic arthritis [175,176,177]. T-helper 17 cells are thought to be involved in the pathogenesis of SLE [178]. Secukinumab has been administered to a female patient with psoriasis and refractory lupus nephritis with beneficial effects [179]. Secukinumab is evaluated in the treatment of active lupus nephritis [180].
4.5. JAK inhibitors
4.5.1. Baricitinib
Baricitinib, an oral selective Janus kinase inhibitor has been approved for the treatment of rheumatoid arthritis [181]. Baricitinib has been evaluated in active SLE not responding to standard of care treatment. Resolution of arthritis and rash was observed [182]. However, a high rate of infections was found. A program for the application of baricitinib in the management of SLE was stopped as no efficacy was observed.
5. Therapeutic strategies for the management of SLE
In 2014 the treat to target principle was introduced in the strategy for the therapeutic management of SLE [8]. In 2019 the EULAR recommendations based on evidence and expert opinion for the management of SLE were updated [183]. It was concluded that hydroxychloroquine should be administered to all lupus patients. In lupus flares bolus doses of glucocorticoids should be administered. During maintenance treatment glucocorticoids should be minimized and if possible withdrawn. Initiation of immunomodulatory agents can aid in tapering or withdrawal of glucocorticoids. However, despite conventional immunosuppressive treatment flares of the disease occur and some patients may not respond to it. Flares, unresponsive patients, target organ involvement, the observation of side effects, the deeper knowledge of pathogenetic paths in SLE and the availability of biologic agents has enabled the introduction of biologic agents and small molecules in the treatment of SLE. B cell targeting agents have been introduced with success. Rituximab may be used in renal and non-renal SLE. Belimumab has been approved for the treatment of SLE. The sequential use of rituximab followed by belimumab has also been tried in refractory cases. In 2023 the Study Group of Autoimmune Diseases of the Portuguese Society of Internal Medicine issued recommendations for the off-label use of biologic agents and small molecules in SLE [9]. They suggested that in SLE patients with very active disease, ie SLEDAI >20 or BILAG 3A’s, severe hemolytic anemia or severe thrombocytopenia, severe kidney disease (stage IV), severe CNS disease the use of rituximab is recommended as first line therapy. In patients with very active disease, severe kidney disease and severe CNS disease the sequential use of rituximab followed by belimumab may be applied. In patients with persistently active disease for at least one year with flares or very active disease rituximab is recommended in rituximab naïve cases as second line therapy, baricitinib or tocilizumab may be used if arthritis predominates as second line. In lupus patients with severe kidney disease rituximab is recommended in rituximab naïve patients as second line therapy, sequential use of rituximab and belimumab may be used in refractory cases as second line treatment. In patients with very active disease the sequential use of rituximab followed by belimumab may be applied in rituximab naïve patients as second line treatment. In these patients with very active disease bortezomib may be considered in multi-refractory cases as second line treatment. In patients with hemolytic anemia or thrombocytopenia rituximab is recommended and bortezomib may be considered in multi-refractoriness. For moderate or severe CNS disease rituximab is recommended in rituximab naïve cases as second line treatment and the sequential use of rituximab followed by belimumab may be considered in refractory cases as second line treatment.
6. Conclusion
In conclusion, hydroxychloroquine and glucocorticoids are standard of care in the therapeutic management of SLE. When flares occur, conventional immunosuppressive agents are added. Refractory disease, target organ involvement, flare recurrence, adverse events of conventional immunosuppressive agents and further understanding of molecular SLE pathogenesis have led to the introduction of biologic agents and small molecules in SLE treatment with the aim to improve disease activity, outcome and quality of life. The introduction of rituximab and belimumab, biologic agents targeting the B cell, have opened a new era in SLE management and have extended the therapeutic spectrum in all subgroups of lupus patients. New biologic agents and small molecules targeting various pathogenetic paths are in development. Although significant progress has been achieved in SLE treatment, more work is needed to incorporate further therapeutic developments in SLE treatment and to ensure improved quality of life in SLE patients.
Author Contributions
Conceptualization, P.A. and L.A.; methodology, P. A and L.A.; investigation, P.A and L.A.; resources, P.A. and L.A.; draft preparation, P.A. and L.A.; writing—review and editing, P.A. and L.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rúa-Figueroa Fernández de Larrinoa, I. What is new in systemic lupus erythematosus. Reumatol Clin. 2015, 11, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Ocampo-Piraquive V, Nieto-Aristizábal I, Cañas CA, Tobón GJ. Mortality in systemic lupus erythematosus: causes, predictors and interventions. Expert Rev Clin Immunol. 2018, 14, 1043–1053. [Google Scholar] [CrossRef]
- Pons-Estel GJ, Ugarte-Gil MF, Alarcón GS. Epidemiology of systemic lupus erythematosus. Expert Rev Clin Immunol. 2017, 13, 799–814. [Google Scholar] [CrossRef] [PubMed]
- Dörner T, Furie R. Novel paradigms in systemic lupus erythematosus. Lancet. 2019, 393, 2344–2358. [Google Scholar] [CrossRef] [PubMed]
- Lisnevskaia L, Murphy G, Isenberg D. Systemic lupus erythematosus. Lancet. 2014, 384, 1878–1888. [Google Scholar] [CrossRef] [PubMed]
- Fortuna G, Brennan MT. Systemic lupus erythematosus: epidemiology, pathophysiology, manifestations, and management. Dent Clin North Am. 2013, 57, 631–655. [Google Scholar] [CrossRef]
- Ginzler EM, Aranow C. Prevention and treatment of adverse effects of corticosteroids in systemic lupus erythematosus. Baillieres Clin Rheumatol. 1998, 12, 495–510. [Google Scholar] [CrossRef]
- van Vollenhoven RF, Mosca M, Bertsias G, et al. Treat-to-target in systemic lupus erythematosus: recommendations from an international task force. Ann Rheum Dis. 2014, 73, 958–967. [Google Scholar] [CrossRef]
- Marinho A, Delgado Alves J, Fortuna J, et al. Biological therapy in systemic lupus erythematosus, antiphospholipid syndrome, and Sjögren’s syndrome: evidence- and practice-based guidance. Front Immunol. 2023, 14, 1117699. [Google Scholar] [CrossRef] [PubMed]
- Aringer M, Burkhardt H, Burmester GR, et al. Current state of evidence on ‘off-label’ therapeutic options for systemic lupus erythematosus, including biological immunosuppressive agents, in Germany, Austria and Switzerland--a consensus report. Lupus. 2012, 21, 386–401. [Google Scholar] [CrossRef] [PubMed]
- Bertsias GK, Tektonidou M, Amoura Z, et al. Joint European League Against Rheumatism and European Renal Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of adult and paediatric lupus nephritis. Ann Rheum Dis. 2012, 71, 1771–1782. [Google Scholar] [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Bmj. 2021, 372, n71. [Google Scholar] [CrossRef]
- A randomized study of the effect of withdrawing hydroxychloroquine sulfate in systemic lupus erythematosus. N Engl J Med. 1991, 324, 150–154. [CrossRef]
- Alarcón GS, McGwin G, Bertoli AM, et al. Effect of hydroxychloroquine on the survival of patients with systemic lupus erythematosus: data from LUMINA, a multiethnic US cohort (LUMINA L). Ann Rheum Dis. 2007, 66, 1168–1172. [Google Scholar] [CrossRef]
- Shinjo SK, Bonfá E, Wojdyla D, et al. Antimalarial treatment may have a time-dependent effect on lupus survival: data from a multinational Latin American inception cohort. Arthritis Rheum. 2010, 62, 855–862. [Google Scholar] [CrossRef]
- Rainsford KD, Parke AL, Clifford-Rashotte M, Kean WF. Therapy and pharmacological properties of hydroxychloroquine and chloroquine in treatment of systemic lupus erythematosus, rheumatoid arthritis and related diseases. Inflammopharmacology. 2015, 23, 231–269. [Google Scholar] [CrossRef]
- James JA, Kim-Howard XR, Bruner BF, et al. Hydroxychloroquine sulfate treatment is associated with later onset of systemic lupus erythematosus. Lupus. 2007, 16, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Fischer-Betz R, Schneider M. [Antimalarials. A treatment option for every lupus patient!?]. Z Rheumatol. 2009, 68, 584–586. [Google Scholar] [CrossRef]
- Fox, RI. Mechanism of action of hydroxychloroquine as an antirheumatic drug. Semin Arthritis Rheum. 1993, 23 (Suppl. 1), 82–91. [Google Scholar] [CrossRef] [PubMed]
- Fox, R. Anti-malarial drugs: possible mechanisms of action in autoimmune disease and prospects for drug development. Lupus. 1996, 5 (Suppl. 1), S4–S10. [Google Scholar] [CrossRef] [PubMed]
- Schrezenmeier E, Dörner T. Mechanisms of action of hydroxychloroquine and chloroquine: implications for rheumatology. Nat Rev Rheumatol. 2020, 16, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Irastorza G, Ramos-Casals M, Brito-Zeron P, Khamashta MA. Clinical efficacy and side effects of antimalarials in systemic lupus erythematosus: a systematic review. Ann Rheum Dis. 2010, 69, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Petri, M. Use of hydroxychloroquine to prevent thrombosis in systemic lupus erythematosus and in antiphospholipid antibody-positive patients. Curr Rheumatol Rep. 2011, 13, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Floris A, Piga M, Mangoni AA, Bortoluzzi A, Erre GL, Cauli A. Protective Effects of Hydroxychloroquine against Accelerated Atherosclerosis in Systemic Lupus Erythematosus. Mediators Inflamm. 2018, 2018, 3424136. [Google Scholar] [CrossRef]
- Penn SK, Kao AH, Schott LL, et al. Hydroxychloroquine and glycemia in women with rheumatoid arthritis and systemic lupus erythematosus. J Rheumatol. 2010, 37, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Irastorza G, Khamashta MA. Hydroxychloroquine: the cornerstone of lupus therapy. Lupus. 2008, 4, 271–273. [Google Scholar]
- Adamptey B, Rudnisky CJ, MacDonald IM. Effect of stopping hydroxychloroquine therapy on the multifocal electroretinogram in patients with rheumatic disorders. Can J Ophthalmol. 2020, 55, 38–44. [Google Scholar] [CrossRef]
- Tanaka, Y. State-of-the-art treatment of systemic lupus erythematosus. Int J Rheum Dis. 2020, 23, 465–471. [Google Scholar] [CrossRef]
- Porta S, Danza A, Arias Saavedra M, et al. Glucocorticoids in Systemic Lupus Erythematosus. Ten Questions and Some Issues. J Clin Med. 2020, 9, 2709. [Google Scholar] [CrossRef]
- Fava A, Petri M. Systemic lupus erythematosus: Diagnosis and clinical management. J Autoimmun. 2019, 96, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Petri, M. Long-term outcomes in lupus. Am J Manag Care. 2001, 7 (Suppl. 16), S480–S485. [Google Scholar]
- Jaryal A, Vikrant S. Current status of lupus nephritis. Indian J Med Res. 2017, 145, 167–178. [Google Scholar] [CrossRef]
- Saavedra M, Sánchez A, Morales S, Ángeles U, Jara LJ. Azathioprine during pregnancy in systemic lupus erythematosus patients is not associated with poor fetal outcome. Clin Rheumatol. 2015, 34, 1211–1216. [Google Scholar] [CrossRef]
- Fortin PR, Abrahamowicz M, Ferland D, Lacaille D, Smith CD, Zummer M. Steroid-sparing effects of methotrexate in systemic lupus erythematosus: a double-blind, randomized, placebo-controlled trial. Arthritis Rheum. 2008, 59, 1796–1804. [Google Scholar] [CrossRef] [PubMed]
- Muangchan C, van Vollenhoven RF, Bernatsky SR, et al. Treatment Algorithms in Systemic Lupus Erythematosus. Arthritis Care Res (Hoboken). 2015, 67, 1237–1245. [Google Scholar] [CrossRef] [PubMed]
- Maksimovic V, Pavlovic-Popovic Z, Vukmirovic S, et al. Molecular mechanism of action and pharmacokinetic properties of methotrexate. Mol Biol Rep. 2020, 47, 4699–4708. [Google Scholar] [CrossRef] [PubMed]
- Islam MN, Hossain M, Haq SA, Alam MN, Ten Klooster PM, Rasker JJ. Efficacy and safety of methotrexate in articular and cutaneous manifestations of systemic lupus erythematosus. Int J Rheum Dis. 2012, 15, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Cronstein BN, Aune TM. Methotrexate and its mechanisms of action in inflammatory arthritis. Nat Rev Rheumatol. 2020, 16, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Cipriani P, Ruscitti P, Carubbi F, Liakouli V, Giacomelli R. Methotrexate: an old new drug in autoimmune disease. Expert Rev Clin Immunol. 2014, 10, 1519–1530. [Google Scholar] [CrossRef] [PubMed]
- Sakthiswary R, Suresh E. Methotrexate in systemic lupus erythematosus: a systematic review of its efficacy. Lupus. 2014, 23, 225–235. [Google Scholar] [CrossRef]
- Bertsias G, Ioannidis JP, Boletis J, et al. EULAR recommendations for the management of systemic lupus erythematosus. Report of a Task Force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics. Ann Rheum Dis. 2008, 67, 195–205. [Google Scholar] [CrossRef]
- Vroom F, de Walle HE, van de Laar MA, Brouwers JR, de Jong-van den Berg LT. Disease-modifying antirheumatic drugs in pregnancy: current status and implications for the future. Drug Saf. 2006, 29, 845–863. [Google Scholar] [CrossRef]
- Broen JCA, van Laar JM. Mycophenolate mofetil, azathioprine and tacrolimus: mechanisms in rheumatology. Nat Rev Rheumatol. 2020, 16, 167–178. [Google Scholar] [CrossRef]
- Olech E, Merrill JT. Mycophenolate mofetil for lupus nephritis. Expert Rev Clin Immunol. 2008, 4, 313–319. [Google Scholar] [CrossRef]
- Walsh M, James M, Jayne D, Tonelli M, Manns BJ, Hemmelgarn BR. Mycophenolate mofetil for induction therapy of lupus nephritis: a systematic review and meta-analysis. Clin J Am Soc Nephrol. 2007, 2, 968–975. [Google Scholar] [CrossRef]
- Morris HK, Canetta PA, Appel GB. Impact of the ALMS and MAINTAIN trials on the management of lupus nephritis. Nephrol Dial Transplant. 2013, 28, 1371–1376. [Google Scholar] [CrossRef]
- Sinclair A, Appel G, Dooley MA, et al. Mycophenolate mofetil as induction and maintenance therapy for lupus nephritis: rationale and protocol for the randomized, controlled Aspreva Lupus Management Study (ALMS). Lupus. 2007, 16, 972–980. [Google Scholar] [CrossRef] [PubMed]
- Houssiau FA, D’Cruz D, Sangle S, et al. Azathioprine versus mycophenolate mofetil for long-term immunosuppression in lupus nephritis: results from the MAINTAIN Nephritis Trial. Ann Rheum Dis. 2010, 69, 2083–2089. [Google Scholar] [CrossRef] [PubMed]
- Stoenoiu MS, Aydin S, Tektonidou M, et al. Repeat kidney biopsies fail to detect differences between azathioprine and mycophenolate mofetil maintenance therapy for lupus nephritis: data from the MAINTAIN Nephritis Trial. Nephrol Dial Transplant. 2012, 27, 1924–1930. [Google Scholar] [CrossRef] [PubMed]
- Ginzler EM, Wofsy D, Isenberg D, Gordon C, Lisk L, Dooley MA. Nonrenal disease activity following mycophenolate mofetil or intravenous cyclophosphamide as induction treatment for lupus nephritis: findings in a multicenter, prospective, randomized, open-label, parallel-group clinical trial. Arthritis Rheum. 2010, 62, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Mok, CC. Mycophenolate mofetil for non-renal manifestations of systemic lupus erythematosus: a systematic review. Scand J Rheumatol. 2007, 36, 329–337. [Google Scholar] [CrossRef]
- Appel GB, Contreras G, Dooley MA, et al. Mycophenolate mofetil versus cyclophosphamide for induction treatment of lupus nephritis. J Am Soc Nephrol. 2009, 20, 1103–1112. [Google Scholar] [CrossRef] [PubMed]
- Houssiau FA, Vasconcelos C, D’Cruz D, et al. The 10-year follow-up data of the Euro-Lupus Nephritis Trial comparing low-dose and high-dose intravenous cyclophosphamide. Ann Rheum Dis. 2010, 69, 61–64. [Google Scholar] [CrossRef]
- Yap DY, Chan TM. Lupus Nephritis in Asia: Clinical Features and Management. Kidney Dis (Basel). 2015, 1, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Hurd ER, Ziff M. The mechanism of action of cyclophosphamide on the nephritis of (NZB x NZW)F1 hybrid mice. Clin Exp Immunol. 1977, 29, 132–139. [Google Scholar]
- Fassbinder T, Saunders U, Mickholz E, et al. Differential effects of cyclophosphamide and mycophenolate mofetil on cellular and serological parameters in patients with systemic lupus erythematosus. Arthritis Res Ther. 2015, 17, 92. [Google Scholar] [CrossRef]
- Martin F, Lauwerys B, Lefèbvre C, Devogelaer JP, Houssiau FA. Side-effects of intravenous cyclophosphamide pulse therapy. Lupus. 1997, 6, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Houssiau FA, Vasconcelos C, D’Cruz D, et al. Immunosuppressive therapy in lupus nephritis: the Euro-Lupus Nephritis Trial, a randomized trial of low-dose versus high-dose intravenous cyclophosphamide. Arthritis Rheum. 2002, 46, 2121–2131. [Google Scholar] [CrossRef]
- Faul C, Donnelly M, Merscher-Gomez S, et al. The actin cytoskeleton of kidney podocytes is a direct target of the antiproteinuric effect of cyclosporine A. Nat Med. 2008, 14, 931–938. [Google Scholar] [CrossRef]
- Pego-Reigosa JM, Cobo-Ibáñez T, Calvo-Alén J, et al. Efficacy and safety of nonbiologic immunosuppressants in the treatment of nonrenal systemic lupus erythematosus: a systematic review. Arthritis Care Res (Hoboken). 2013, 65, 1775–1785. [Google Scholar] [CrossRef]
- Schreiber SL, Crabtree GR. The mechanism of action of cyclosporin A and FK506. Immunol Today. 1992, 13, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Russell G, Graveley R, Seid J, al-Humidan AK, Skjodt H. Mechanisms of action of cyclosporine and effects on connective tissues. Semin Arthritis Rheum. 1992, 21 (Suppl. 3), 16–22. [Google Scholar] [CrossRef] [PubMed]
- Mok, CC. Towards new avenues in the management of lupus glomerulonephritis. Nat Rev Rheumatol. 2016, 12, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Bao H, Liu ZH, Xie HL, Hu WX, Zhang HT, Li LS. Successful treatment of class V+IV lupus nephritis with multitarget therapy. J Am Soc Nephrol. 2008, 19, 2001–2010. [Google Scholar] [CrossRef] [PubMed]
- Liu Z, Zhang H, Xing C, et al. Multitarget therapy for induction treatment of lupus nephritis: a randomized trial. Ann Intern Med. 2015, 162, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Kronbichler A, Brezina B, Gauckler P, Quintana LF, Jayne DRW. Refractory lupus nephritis: When, why and how to treat. Autoimmun Rev. 2019, 18, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Rovin BH, Solomons N, Pendergraft WF, 3rd, et al. A randomized, controlled double-blind study comparing the efficacy and safety of dose-ranging voclosporin with placebo in achieving remission in patients with active lupus nephritis. Kidney Int. 2019, 95, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Parodis I, Houssiau FA. From sequential to combination and personalised therapy in lupus nephritis: moving towards a paradigm shift? Ann Rheum Dis. 2022, 81, 15–19. [Google Scholar] [CrossRef]
- Rovin BH, Teng YKO, Ginzler EM, et al. Efficacy and safety of voclosporin versus placebo for lupus nephritis (AURORA 1): a double-blind, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet. 2021, 397, 2070–2080. [Google Scholar] [CrossRef]
- Sakthiswary R, D’Cruz D. Intravenous immunoglobulin in the therapeutic armamentarium of systemic lupus erythematosus: a systematic review and meta-analysis. Medicine (Baltimore). 2014, 93, e86. [Google Scholar] [CrossRef]
- Magro-Checa C, Zirkzee EJ, Huizinga TW, Steup-Beekman GM. Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives. Drugs. 2016, 76, 459–483. [Google Scholar] [CrossRef]
- Suri V, Varma S, Joshi K, Malhotra P, Kumari S, Jain S. Lupus myocarditis: marked improvement in cardiac function after intravenous immunoglobulin therapy. Rheumatol Int. 2010, 30, 1503–1505. [Google Scholar] [CrossRef]
- Zandman-Goddard G, Blank M, Shoenfeld Y. Intravenous immunoglobulins in systemic lupus erythematosus: from the bench to the bedside. Lupus. 2009, 18, 884–888. [Google Scholar] [CrossRef]
- Zandman-Goddard G, Levy Y, Shoenfeld Y. Intravenous immunoglobulin therapy and systemic lupus erythematosus. Clin Rev Allergy Immunol. 2005, 29, 219–228. [Google Scholar] [CrossRef]
- Merrill JT, Neuwelt CM, Wallace DJ, et al. Efficacy and safety of rituximab in moderately-to-severely active systemic lupus erythematosus: the randomized, double-blind, phase II/III systemic lupus erythematosus evaluation of rituximab trial. Arthritis Rheum. 2010, 62, 222–233. [Google Scholar] [CrossRef] [PubMed]
- Pirone C, Mendoza-Pinto C, van der Windt DA, Parker B, M OS, Bruce IN. Predictive and prognostic factors influencing outcomes of rituximab therapy in systemic lupus erythematosus (SLE): A systematic review. Semin Arthritis Rheum. 2017, 47, 384–396. [Google Scholar] [CrossRef] [PubMed]
- Iwata S, Saito K, Hirata S, et al. Efficacy and safety of anti-CD20 antibody rituximab for patients with refractory systemic lupus erythematosus. Lupus. 2018, 27, 802–811. [Google Scholar] [CrossRef] [PubMed]
- Navarra SV, Guzmán RM, Gallacher AE, et al. Efficacy and safety of belimumab in patients with active systemic lupus erythematosus: a randomised, placebo-controlled, phase 3 trial. Lancet. 2011, 377, 721–731. [Google Scholar] [CrossRef]
- Blair HA, Duggan ST. Belimumab: A Review in Systemic Lupus Erythematosus. Drugs. 2018, 78, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Poh YJ, Baptista B, D’Cruz DP. Subcutaneous and intravenous belimumab in the treatment of systemic lupus erythematosus: a review of data on subcutaneous and intravenous administration. Expert Rev Clin Immunol. 2017, 13, 925–938. [Google Scholar] [CrossRef] [PubMed]
- Wallace DJ, Ginzler EM, Merrill JT, et al. Safety and Efficacy of Belimumab Plus Standard Therapy for Up to Thirteen Years in Patients With Systemic Lupus Erythematosus. Arthritis Rheumatol. 2019, 71, 1125–1134. [Google Scholar] [CrossRef]
- Kraaij T, Kamerling SWA, de Rooij ENM, et al. The NET-effect of combining rituximab with belimumab in severe systemic lupus erythematosus. J Autoimmun. 2018, 91, 45–54. [Google Scholar] [CrossRef]
- Gualtierotti R, Borghi MO, Gerosa M, et al. Successful sequential therapy with rituximab and belimumab in patients with active systemic lupus erythematosus: a case series. Clin Exp Rheumatol. Jul- 2018, 36, 643–647. [Google Scholar]
- Lee WS, Amengual O. B cells targeting therapy in the management of systemic lupus erythematosus. Immunol Med. 2020, 43, 16–35. [Google Scholar] [CrossRef] [PubMed]
- Davis LS, Reimold AM. Research and therapeutics-traditional and emerging therapies in systemic lupus erythematosus. Rheumatology (Oxford). 2017, 56 (suppl. 1), i100–i113. [Google Scholar] [CrossRef] [PubMed]
- Magro, R. Biological therapies and their clinical impact in the treatment of systemic lupus erythematosus. Ther Adv Musculoskelet Dis. 2019, 11, 1759720x19874309. [Google Scholar] [CrossRef] [PubMed]
- Samotij D, Reich A. Biologics in the Treatment of Lupus Erythematosus: A Critical Literature Review. Biomed Res Int. 2019, 2019, 8142368. [Google Scholar] [CrossRef]
- Ma K, Du W, Wang X, et al. Multiple Functions of B Cells in the Pathogenesis of Systemic Lupus Erythematosus. Int J Mol Sci. 2019, 20, 6021. [Google Scholar] [CrossRef] [PubMed]
- Möckel T, Basta F, Weinmann-Menke J, Schwarting A. B cell activating factor (BAFF): Structure, functions, autoimmunity and clinical implications in Systemic Lupus Erythematosus (SLE). Autoimmun Rev. 2021, 20, 102736. [Google Scholar] [CrossRef] [PubMed]
- Arbitman L, Furie R, Vashistha H. B cell-targeted therapies in systemic lupus erythematosus. J Autoimmun. 2022, 132, 102873. [Google Scholar] [CrossRef]
- Samy E, Wax S, Huard B, Hess H, Schneider P. Targeting BAFF and APRIL in systemic lupus erythematosus and other antibody-associated diseases. Int Rev Immunol. 2017, 36, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Chen C, Laidlaw BJ. Development and function of tissue-resident memory B cells. Adv Immunol. 2022, 155, 1–38. [Google Scholar] [CrossRef]
- Sabahi R, Anolik JH. B-cell-targeted therapy for systemic lupus erythematosus. Drugs. 2006, 66, 1933–1948. [Google Scholar] [CrossRef] [PubMed]
- Yap DYH, Chan TM. B Cell Abnormalities in Systemic Lupus Erythematosus and Lupus Nephritis-Role in Pathogenesis and Effect of Immunosuppressive Treatments. Int J Mol Sci. 2019, 20, 6231. [Google Scholar] [CrossRef] [PubMed]
- Furie R, Petri M, Zamani O, et al. A phase III, randomized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients with systemic lupus erythematosus. Arthritis Rheum. 2011, 63, 3918–3930. [Google Scholar] [CrossRef] [PubMed]
- Merrill JT, van Vollenhoven RF, Buyon JP, et al. Efficacy and safety of subcutaneous tabalumab, a monoclonal antibody to B-cell activating factor, in patients with systemic lupus erythematosus: results from ILLUMINATE-2, a 52-week, phase III, multicentre, randomised, double-blind, placebo-controlled study. Ann Rheum Dis. 2016, 75, 332–340. [Google Scholar] [CrossRef]
- Isenberg D, Gordon C, Licu D, Copt S, Rossi CP, Wofsy D. Efficacy and safety of atacicept for prevention of flares in patients with moderate-to-severe systemic lupus erythematosus (SLE): 52-week data (APRIL-SLE randomised trial). Ann Rheum Dis. 2015, 74, 2006–2015. [Google Scholar] [CrossRef]
- Merrill JT, Shanahan WR, Scheinberg M, Kalunian KC, Wofsy D, Martin RS. Phase III trial results with blisibimod, a selective inhibitor of B-cell activating factor, in subjects with systemic lupus erythematosus (SLE): results from a randomised, double-blind, placebo-controlled trial. Ann Rheum Dis. 2018, 77, 883–889. [Google Scholar] [CrossRef]
- Lazar S, Kahlenberg JM. Systemic Lupus Erythematosus: New Diagnostic and Therapeutic Approaches. Annu Rev Med. 2023, 74, 339–352. [Google Scholar] [CrossRef]
- Jiang Y, Cheng Y, Ma S, et al. Systemic lupus erythematosus-complicating immune thrombocytopenia: From pathogenesis to treatment. J Autoimmun. 2022, 132, 102887. [Google Scholar] [CrossRef]
- Isenberg D, Furie R, Jones NS, et al. Efficacy, Safety, and Pharmacodynamic Effects of the Bruton’s Tyrosine Kinase Inhibitor Fenebrutinib (GDC-0853) in Systemic Lupus Erythematosus: Results of a Phase II, Randomized, Double-Blind, Placebo-Controlled Trial. Arthritis Rheumatol. 2021, 73, 1835–1846. [Google Scholar] [CrossRef]
- Cerny T, Borisch B, Introna M, Johnson P, Rose AL. Mechanism of action of rituximab. Anticancer Drugs. 2002, 13 (Suppl 2), S3–S10. [Google Scholar] [CrossRef]
- McDonald V, Leandro M. Rituximab in non-haematological disorders of adults and its mode of action. Br J Haematol. 2009, 146, 233–246. [Google Scholar] [CrossRef] [PubMed]
- Weiner, GJ. Rituximab: mechanism of action. Semin Hematol. 2010, 47, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Sanz I, Lee FE. B cells as therapeutic targets in SLE. Nat Rev Rheumatol. 2010, 6, 326–337. [Google Scholar] [CrossRef] [PubMed]
- Sanz, I. Systemic lupus erythematosus: Extent and patterns of off-label use of rituximab for SLE. Nat Rev Rheumatol. 2016, 12, 700–702. [Google Scholar] [CrossRef] [PubMed]
- Wang CR, Tsai YS, Li WT. Lupus myocarditis receiving the rituximab therapy-a monocentric retrospective study. Clin Rheumatol. 2018, 37, 1701–1707. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Casals M, Soto MJ, Cuadrado MJ, Khamashta MA. Rituximab in systemic lupus erythematosus: A systematic review of off-label use in 188 cases. Lupus. 2009, 18, 767–776. [Google Scholar] [CrossRef] [PubMed]
- Gunnarsson I, Jonsdottir T. Rituximab treatment in lupus nephritis--where do we stand? Lupus. 2013, 22, 381–389. [Google Scholar] [CrossRef]
- Witt M, Grunke M, Proft F, et al. Clinical outcomes and safety of rituximab treatment for patients with systemic lupus erythematosus (SLE) - results from a nationwide cohort in Germany (GRAID). Lupus. 2013, 22, 1142–1149. [Google Scholar] [CrossRef]
- Cobo-Ibáñez T, Loza-Santamaría E, Pego-Reigosa JM, et al. Efficacy and safety of rituximab in the treatment of non-renal systemic lupus erythematosus: a systematic review. Semin Arthritis Rheum. 2014, 44, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Tokunaga M, Saito K, Kawabata D, et al. Efficacy of rituximab (anti-CD20) for refractory systemic lupus erythematosus involving the central nervous system. Ann Rheum Dis. 2007, 66, 470–475. [Google Scholar] [CrossRef]
- Moroni G, Raffiotta F, Trezzi B, et al. Rituximab vs mycophenolate and vs cyclophosphamide pulses for induction therapy of active lupus nephritis: a clinical observational study. Rheumatology (Oxford). 2014, 53, 1570–1577. [Google Scholar] [CrossRef] [PubMed]
- Ehrenstein MR, Wing C. The BAFFling effects of rituximab in lupus: danger ahead? Nat Rev Rheumatol. 2016, 12, 367–372. [Google Scholar] [CrossRef]
- Lazarus MN, Turner-Stokes T, Chavele KM, Isenberg DA, Ehrenstein MR. B-cell numbers and phenotype at clinical relapse following rituximab therapy differ in SLE patients according to anti-dsDNA antibody levels. Rheumatology (Oxford). 2012, 51, 1208–1215. [Google Scholar] [CrossRef]
- Carter LM, Isenberg DA, Ehrenstein MR. Elevated serum BAFF levels are associated with rising anti-double-stranded DNA antibody levels and disease flare following B cell depletion therapy in systemic lupus erythematosus. Arthritis Rheum. 2013, 65, 2672–2679. [Google Scholar] [CrossRef]
- Díaz-Lagares C, Croca S, Sangle S, et al. Efficacy of rituximab in 164 patients with biopsy-proven lupus nephritis: pooled data from European cohorts. Autoimmun Rev. 2012, 11, 357–364. [Google Scholar] [CrossRef]
- Gomez Mendez LM, Cascino MD, Garg J, et al. Peripheral Blood B Cell Depletion after Rituximab and Complete Response in Lupus Nephritis. Clin J Am Soc Nephrol. 2018, 13, 1502–1509. [Google Scholar] [CrossRef]
- Furie R, Rovin BH, Houssiau F, et al. Two-Year, Randomized, Controlled Trial of Belimumab in Lupus Nephritis. N Engl J Med. 2020, 383, 1117–1128. [Google Scholar] [CrossRef]
- van Vollenhoven RF, Petri MA, Cervera R, et al. Belimumab in the treatment of systemic lupus erythematosus: high disease activity predictors of response. Ann Rheum Dis. 2012, 71, 1343–1349. [Google Scholar] [CrossRef]
- Stohl, W. Future prospects in biologic therapy for systemic lupus erythematosus. Nat Rev Rheumatol. 2013, 9, 705–720. [Google Scholar] [CrossRef]
- Morais SA, Vilas-Boas A, Isenberg DA. B-cell survival factors in autoimmune rheumatic disorders. Ther Adv Musculoskelet Dis. 2015, 7, 122–151. [Google Scholar] [CrossRef]
- Vilas-Boas A, Morais SA, Isenberg DA. Belimumab in systemic lupus erythematosus. RMD Open. 2015, 1, e000011. [Google Scholar] [CrossRef]
- Naradikian MS, Perate AR, Cancro MP. BAFF receptors and ligands create independent homeostatic niches for B cell subsets. Curr Opin Immunol. 2015, 34, 126–129. [Google Scholar] [CrossRef]
- Vincent FB, Morand EF, Schneider P, Mackay F. The BAFF/APRIL system in SLE pathogenesis. Nat Rev Rheumatol. 2014, 10, 365–373. [Google Scholar] [CrossRef]
- Dillon SR, Harder B, Lewis KB, et al. B-lymphocyte stimulator/a proliferation-inducing ligand heterotrimers are elevated in the sera of patients with autoimmune disease and are neutralized by atacicept and B-cell maturation antigen-immunoglobulin. Arthritis Res Ther. 2010, 12, R48. [Google Scholar] [CrossRef]
- Roschke V, Sosnovtseva S, Ward CD, et al. BLyS and APRIL form biologically active heterotrimers that are expressed in patients with systemic immune-based rheumatic diseases. J Immunol. 2002, 169, 4314–4321. [Google Scholar] [CrossRef]
- Stohl, W. Systemic lupus erythematosus and its ABCs (APRIL/BLyS complexes). Arthritis Res Ther. 2010, 2, 111. [Google Scholar] [CrossRef] [PubMed]
- Guerreiro Castro S, Isenberg DA. Belimumab in systemic lupus erythematosus (SLE): evidence-to-date and clinical usefulness. Ther Adv Musculoskelet Dis. 2017, 9, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Plüß M, Tampe B, Niebusch N, Zeisberg M, Müller GA, Korsten P. Clinical Efficacy of Routinely Administered Belimumab on Proteinuria and Neuropsychiatric Lupus. Front Med (Lausanne). 2020, 7, 222. [Google Scholar] [CrossRef]
- Shipa M, Embleton-Thirsk A, Parvaz M, et al. Effectiveness of Belimumab After Rituximab in Systemic Lupus Erythematosus : A Randomized Controlled Trial. Ann Intern Med. 2021, 174, 1647–1657. [Google Scholar] [CrossRef] [PubMed]
- Petricca L, Gigante MR, Paglionico A, et al. Rituximab Followed by Belimumab Controls Severe Lupus Nephritis and Bullous Pemphigoid in Systemic Lupus Erythematosus Refractory to Several Combination Therapies. Front Med (Lausanne). 2020, 7, 553075. [Google Scholar] [CrossRef]
- Kraaij T, Arends EJ, van Dam LS, et al. Long-term effects of combined B-cell immunomodulation with rituximab and belimumab in severe, refractory systemic lupus erythematosus: 2-year results. Nephrol Dial Transplant. 2021, 36, 1474–1483. [Google Scholar] [CrossRef] [PubMed]
- Isenberg DA, Petri M, Kalunian K, et al. Efficacy and safety of subcutaneous tabalumab in patients with systemic lupus erythematosus: results from ILLUMINATE-1, a 52-week, phase III, multicentre, randomised, double-blind, placebo-controlled study. Ann Rheum Dis. 2016, 75, 323–331. [Google Scholar] [CrossRef]
- Merrill JT, Wallace DJ, Wax S, et al. Efficacy and Safety of Atacicept in Patients With Systemic Lupus Erythematosus: Results of a Twenty-Four-Week, Multicenter, Randomized, Double-Blind, Placebo-Controlled, Parallel-Arm, Phase IIb Study. Arthritis Rheumatol. 2018, 70, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Petri MA, Martin RS, Scheinberg MA, Furie RA. Assessments of fatigue and disease activity in patients with systemic lupus erythematosus enrolled in the Phase 2 clinical trial with blisibimod. Lupus. 2017, 26, 27–37. [Google Scholar] [CrossRef]
- Lenert A, Niewold TB, Lenert P. Spotlight on blisibimod and its potential in the treatment of systemic lupus erythematosus: evidence to date. Drug Des Devel Ther. 2017, 11, 747–757. [Google Scholar] [CrossRef]
- Geh D, Gordon C. Epratuzumab for the treatment of systemic lupus erythematosus. Expert Rev Clin Immunol. 2018, 14, 245–258. [Google Scholar] [CrossRef]
- Wallace DJ, Goldenberg DM. Epratuzumab for systemic lupus erythematosus. Lupus. 2013, 22, 400–405. [Google Scholar] [CrossRef]
- Gottenberg JE, Dörner T, Bootsma H, et al. Efficacy of Epratuzumab, an Anti-CD22 Monoclonal IgG Antibody, in Systemic Lupus Erythematosus Patients With Associated Sjögren’s Syndrome: Post Hoc Analyses From the EMBODY Trials. Arthritis Rheumatol. 2018, 70, 763–773. [Google Scholar] [CrossRef]
- Bag-Ozbek A, Hui-Yuen JS. Emerging B-Cell Therapies in Systemic Lupus Erythematosus. Ther Clin Risk Manag. 2021, 17, 39–54. [Google Scholar] [CrossRef] [PubMed]
- Ostendorf L, Burns M, Durek P, et al. Targeting CD38 with Daratumumab in Refractory Systemic Lupus Erythematosus. N Engl J Med. 2020, 383, 1149–1155. [Google Scholar] [CrossRef] [PubMed]
- Oon S, Huq M, Godfrey T, Nikpour M. Systematic review, and meta-analysis of steroid-sparing effect, of biologic agents in randomized, placebo-controlled phase 3 trials for systemic lupus erythematosus. Semin Arthritis Rheum. 2018, 48, 221–239. [Google Scholar] [CrossRef] [PubMed]
- Lamb, YN. Ocrelizumab: A Review in Multiple Sclerosis. Drugs. 2022, 82, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Mysler EF, Spindler AJ, Guzman R, et al. Efficacy and safety of ocrelizumab in active proliferative lupus nephritis: results from a randomized, double-blind, phase III study. Arthritis Rheum. 2013, 65, 2368–2379. [Google Scholar] [CrossRef]
- Reddy V, Klein C, Isenberg DA, et al. Obinutuzumab induces superior B-cell cytotoxicity to rituximab in rheumatoid arthritis and systemic lupus erythematosus patient samples. Rheumatology (Oxford). 2017, 56, 1227–1237. [Google Scholar] [CrossRef]
- Reddy V, Dahal LN, Cragg MS, Leandro M. Optimising B-cell depletion in autoimmune disease: is obinutuzumab the answer? Drug Discov Today. 2016, 21, 1330–1338. [Google Scholar] [CrossRef]
- Hassan SU, Md Yusof MY, Emery P, Dass S, Vital EM. Biologic Sequencing in Systemic Lupus Erythematosus: After Secondary Non-response to Rituximab, Switching to Humanised Anti-CD20 Agent Is More Effective Than Belimumab. Front Med (Lausanne). 2020, 7, 498. [Google Scholar] [CrossRef]
- Masoud S, McAdoo SP, Bedi R, Cairns TD, Lightstone L. Ofatumumab for B cell depletion in patients with systemic lupus erythematosus who are allergic to rituximab. Rheumatology (Oxford). 2018, 57, 1156–1161. [Google Scholar] [CrossRef]
- Sanford M, McCormack PL. Ofatumumab. Drugs. 2010, 70, 1013–1019. [Google Scholar] [CrossRef]
- Speth F, Hinze C, Häfner R. Combination of ofatumumab and fresh frozen plasma in hypocomplementemic systemic lupus erythematosus: a case report. Lupus. 2018, 27, 1395–1396. [Google Scholar] [CrossRef]
- Chu SY, Pong E, Bonzon C, et al. Inhibition of B cell activation following in vivo co-engagement of B cell antigen receptor and Fcγ receptor IIb in non-autoimmune-prone and SLE-prone mice. J Transl Autoimmun. 2021, 4, 100075. [Google Scholar] [CrossRef] [PubMed]
- Satterthwaite, AB. Bruton’s Tyrosine Kinase, a Component of B Cell Signaling Pathways, Has Multiple Roles in the Pathogenesis of Lupus. Front Immunol. 2017, 8, 1986. [Google Scholar] [CrossRef] [PubMed]
- Garg N, Padron EJ, Rammohan KW, Goodman CF. Bruton’s Tyrosine Kinase Inhibitors: The Next Frontier of B-Cell-Targeted Therapies for Cancer, Autoimmune Disorders, and Multiple Sclerosis. J Clin Med. 2022, 11, 6139. [Google Scholar] [CrossRef] [PubMed]
- Rozkiewicz D, Hermanowicz JM, Kwiatkowska I, Krupa A, Pawlak D. Bruton’s Tyrosine Kinase Inhibitors (BTKIs): Review of Preclinical Studies and Evaluation of Clinical Trials. Molecules. 2023, 28, 2400. [Google Scholar] [CrossRef]
- Alexander T, Sarfert R, Klotsche J, et al. The proteasome inhibitior bortezomib depletes plasma cells and ameliorates clinical manifestations of refractory systemic lupus erythematosus. Ann Rheum Dis. 2015, 74, 1474–1478. [Google Scholar] [CrossRef] [PubMed]
- Tan CRC, Abdul-Majeed S, Cael B, Barta SK. Clinical Pharmacokinetics and Pharmacodynamics of Bortezomib. Clin Pharmacokinet. 2019, 58, 157–168. [Google Scholar] [CrossRef]
- Segarra A, Arredondo KV, Jaramillo J, et al. Efficacy and safety of bortezomib in refractory lupus nephritis: a single-center experience. Lupus. 2020, 29, 118–125. [Google Scholar] [CrossRef]
- Walhelm T, Gunnarsson I, Heijke R, et al. Clinical Experience of Proteasome Inhibitor Bortezomib Regarding Efficacy and Safety in Severe Systemic Lupus Erythematosus: A Nationwide Study. Front Immunol. 2021, 12, 756941. [Google Scholar] [CrossRef]
- Zimmer R, Scherbarth HR, Rillo OL, Gomez-Reino JJ, Muller S. Lupuzor/P140 peptide in patients with systemic lupus erythematosus: a randomised, double-blind, placebo-controlled phase IIb clinical trial. Ann Rheum Dis. 2013, 72, 1830–1835. [Google Scholar] [CrossRef]
- Schneider WM, Chevillotte MD, Rice CM. Interferon-stimulated genes: a complex web of host defenses. Annu Rev Immunol. 2014, 32, 513–45. [Google Scholar] [CrossRef]
- Rönnblom, L. The importance of the type I interferon system in autoimmunity. Clin Exp Rheumatol. 2016, 34 (Suppl. 98), 21–24. [Google Scholar]
- Khamashta M, Merrill JT, Werth VP, et al. Sifalimumab, an anti-interferon-α monoclonal antibody, in moderate to severe systemic lupus erythematosus: a randomised, double-blind, placebo-controlled study. Ann Rheum Dis. 2016, 75, 1909–1916. [Google Scholar] [CrossRef]
- Pellerin A, Yasuda K, Cohen-Bucay A, et al. Monoallelic IRF5 deficiency in B cells prevents murine lupus. JCI Insight. 2021, 6. [Google Scholar] [CrossRef]
- Morand EF, Trasieva T, Berglind A, Illei GG, Tummala R. Lupus Low Disease Activity State (LLDAS) attainment discriminates responders in a systemic lupus erythematosus trial: post-hoc analysis of the Phase IIb MUSE trial of anifrolumab. Ann Rheum Dis. 2018, 77, 706–713. [Google Scholar] [CrossRef]
- Deeks ED. Anifrolumab: First Approval. Drugs. 2021, 81, 1795–1802. [Google Scholar] [CrossRef]
- Sheppard M, Laskou F, Stapleton PP, Hadavi S, Dasgupta B. Tocilizumab (Actemra). Hum Vaccin Immunother. 2017, 13, 1972–1988. [Google Scholar] [CrossRef] [PubMed]
- Scott, LJ. Tocilizumab: A Review in Rheumatoid Arthritis. Drugs. 2017, 77, 1865–1879. [Google Scholar] [CrossRef] [PubMed]
- Stone JH, Tuckwell K, Dimonaco S, et al. Trial of Tocilizumab in Giant-Cell Arteritis. N Engl J Med. 2017, 377, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Somers EC, Eschenauer GA, Troost JP, et al. Tocilizumab for Treatment of Mechanically Ventilated Patients With COVID-19. Clin Infect Dis. 2021, 73, e445–e454. [Google Scholar] [CrossRef] [PubMed]
- García-Hernández FJ, González-León R, Castillo-Palma MJ, Ocaña-Medina C, Sánchez-Román J. Tocilizumab for treating refractory haemolytic anaemia in a patient with systemic lupus erythematosus. Rheumatology (Oxford). 2012, 10, 1918–1919. [Google Scholar]
- De Matteis A, Sacco E, Celani C, et al. Tocilizumab for massive refractory pleural effusion in an adolescent with systemic lupus erythematosus. Pediatr Rheumatol Online J. 2021, 19, 144. [Google Scholar] [CrossRef]
- Chaoyi M, Shrestha B, Hui L, Qiujin D, Ping F. Tocilizumab therapy for persistent high-grade fever in systemic lupus erythematosus: two cases and a literature review. J Int Med Res. 2022, 50, 3000605221088558. [Google Scholar] [CrossRef]
- Jüptner M, Zeuner R, Schreiber S, Laudes M, Schröder JO. Successful application of belimumab in two patients with systemic lupus erythematosus experiencing a flare during tocilizumab treatment. Lupus. 2014, 23, 428–430. [Google Scholar] [CrossRef] [PubMed]
- Blair, HA. Secukinumab: A Review in Ankylosing Spondylitis. Drugs. 2019, 79, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Blair, HA. Secukinumab: A Review in Psoriatic Arthritis. Drugs. 2021, 81, 483–494. [Google Scholar] [CrossRef] [PubMed]
- Langley RG, Elewski BE, Lebwohl M, et al. Secukinumab in plaque psoriasis--results of two phase 3 trials. N Engl J Med. 2014, 371, 326–338. [Google Scholar] [CrossRef] [PubMed]
- Pan HF, Ye DQ, Li XP. Type 17 T-helper cells might be a promising therapeutic target for systemic lupus erythematosus. Nat Clin Pract Rheumatol. 2008, 4, 352–353. [Google Scholar] [CrossRef] [PubMed]
- Satoh Y, Nakano K, Yoshinari H, et al. A case of refractory lupus nephritis complicated by psoriasis vulgaris that was controlled with secukinumab. Lupus. 2018, 27, 1202–1206. [Google Scholar] [CrossRef] [PubMed]
- Petrić M, Radić M. Is Th17-Targeted Therapy Effective in Systemic Lupus Erythematosus? Curr Issues Mol Biol. 2023, 45, 4331–4343. [Google Scholar] [CrossRef] [PubMed]
- Wang F, Sun L, Wang S, et al. Efficacy and Safety of Tofacitinib, Baricitinib, and Upadacitinib for Rheumatoid Arthritis: A Systematic Review and Meta-Analysis. Mayo Clin Proc. 2020, 95, 1404–1419. [Google Scholar] [CrossRef] [PubMed]
- Yuan K, Huang G, Sang X, Xu A. Baricitinib for systemic lupus erythematosus. Lancet. 2019, 393, 402. [Google Scholar] [CrossRef]
- Fanouriakis A, Kostopoulou M, Alunno A, et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann Rheum Dis. 2019, 78, 736–745. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Search method based on the PRISMA flow diagram for identifying studies regarding biological treatment in SLE.
Figure 1.
Search method based on the PRISMA flow diagram for identifying studies regarding biological treatment in SLE.
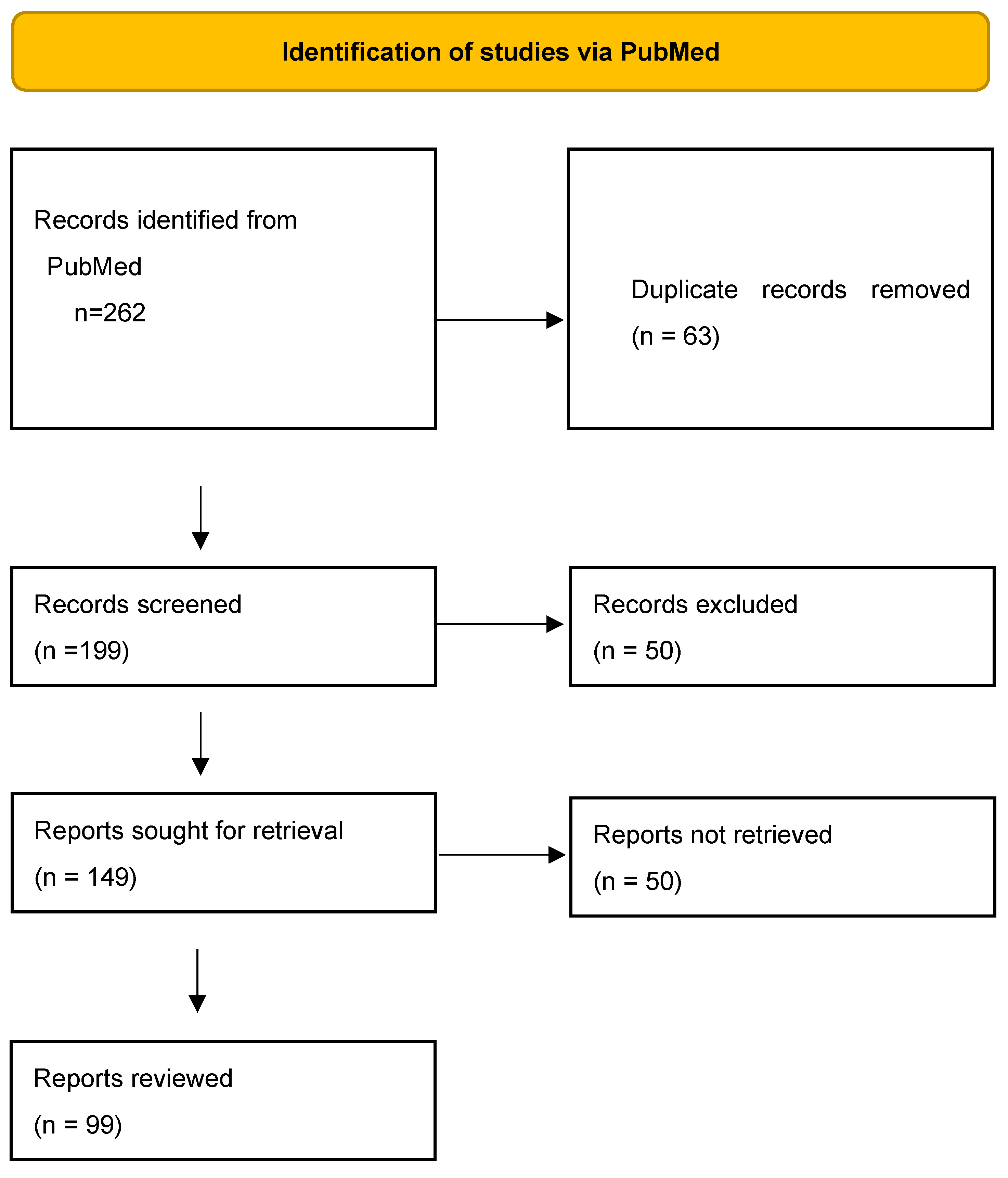
Figure 2.
Biologic agents and small molecules in the treatment of systemic lupus erythematosus (SLE).
Figure 2.
Biologic agents and small molecules in the treatment of systemic lupus erythematosus (SLE).
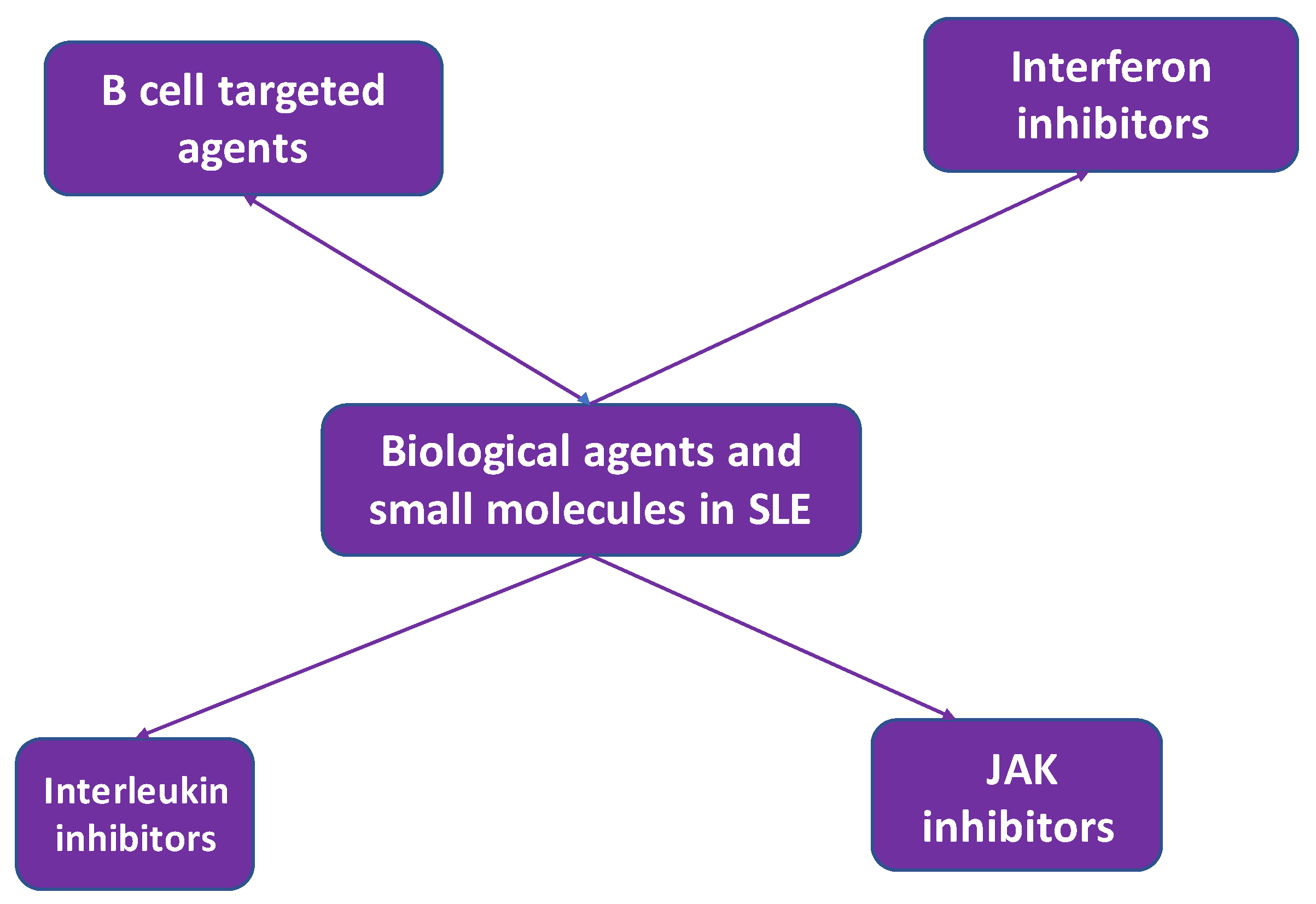
Figure 3.
B cell targeted biologic agents in the treatment of systemic lupus erythematosus (SLE).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



