
Submitted:
10 June 2023
Posted:
12 June 2023
You are already at the latest version
Abstract
Tunneled central venous catheters (CVC) are mainly considered as rescue vascular access option in dialysis but still used in about one quarter of prevalent patients worldwide as being associated with poor performances and higher risks.
Study design. In this retrospective single-center study, we aimed to report on clinical performances achieved with high-flow tunneled CVC (DualCath, DCath) and compared it with arteriovenous accesses (AVAs; AV fistula, AV graft, Thomas Shunt) in a hospital-based dialysis unit.
Methods. Sixty-eight stage 5 chronic kidney disease dialysis dependent patients (CKD5D) receiving high volume hemodiafiltration were followed-up for 30 months.
The study consisted of two phases: baseline cross-sectional and longitudinal follow-up of key performance indicators. Clinical performances consisting of effective blood flow and blood volume, recirculation, urea and ionic Kt/V and total Kt, ultrafiltration volume and percent reduction of ß2-M were measured monthly as part of quality control in our unit.
Results. At baseline, effective blood flow with DCath was close to 400 ml/min, similar to AVAs. Recirculation with DCath (7%, 6-13%) was higher than AVAs. Diffusive dialysis dose delivered with DCath (spKt and eKt/V) and convective dialysis dose achieved with DCath were slightly lower than AVAs, but still much higher than recommended by guidelines. Percent reduction of ß2-M achieved with DCath was also 4 to 10% lower than AVAs. On longitudinal follow-up, main clinical performance indicators of DCath (total Kt and total ultrafiltration volume, L/session) were maintained very stable over time and close to those achieved with AVAs.
Conclusions. As shown in this study, high-flow DualCath tunneled two single lumen silicone catheters may be used to deliver high volume hemodiafiltration in a reliable and consistent manner without compromising clinical performances. These results rely from the specific design of the two silicone cannulas and the strict adherence to best catheter practices.
Keywords:
Vascular access
; Tunneled central venous catheter
; Dialysis clinical performances
; Diffusive dialysis dose
; Convective dialysis dose
; Effective blood flow
; Recirculation
Introduction
Tunneled central venous catheters (CVC) are considered as rescue vascular access option in dialysis patients by almost all clinical practice guidelines, as being associated with higher morbidity, lower performances, and greater cost1-4. However, prevalent use of CVC in dialysis remains high, ranging almost from zero up to 50% with a median value of 25% of dialysis patients worldwide5-8. These facts tend to support the notion that CVC are still needed in the vascular access care offering 9-11 of kidney disease management since they provide an interesting option to ensure care continuity in CKD patients facing recurring vascular access problems well recognized in their last KDOQI issue2.
Intrinsic limitations of CVC are acknowledged and analyzed in various reports12,13. They belong either to the geometry of the cannulas (internal lumen diameter, length, polymer characteristics), or the catheter design (single or dual lumen, central and side holes) or to the catheter tip’s location within the venous central system (superior vena cava, right atrium)14,15. In addition, tunneled CVC bear higher risk (dysfunction, infection, thrombosis) that can be mitigated by better handling and locking solution16-19. These facts have raised several controversies in the scientific literature with pros and cons11,20-22. It is not our intent to enter this polemic, but rather to assess clinical performances delivered by means of tunneled CVC compared to arterio-venous accesses (AVA) in stage 5 chronic kidney disease (CKD5D) patients receiving high volume hemodiafiltration as mainstream treatment.
In this study, we aimed to report on clinical performances achieved with high-flow tunneled CVC (DualCath, DCath) and compared it with various AVA used at the same time in our hospital-based dialysis unit.
Material and Methods
- 1.
- Study design
This is a retrospective single-center study performed in a teaching hospital-based dialysis unit (Lapeyronie Hospital, Montpellier, France) using data extracted from patient electronic dialysis medical records. Data collection extended from October 1, 2009, to May 31, 2012 (30 months of follow-up). All data collected were part of clinical dialysis performances and quality control assessment precisely protocolized and performed monthly (first week of the month, midweek session).
The study consisted of two parts: firstly, a baseline assessment of clinical performances corresponding to a cross-sectional analysis using data of three consecutive months while patients being clustered by vascular access type (tunneled CVC, AVA); secondly, a longitudinal follow-up of clinical performances up to 30 months while patients were clustered by vascular access type.
Clinical dialysis performance indicators consisted of effective blood flow, access recirculation, urea spKt/V and dpKt/V (Daugirdas), ionic dialysance measurement (Online Clearance Measurement, OCM) from dialysis machine (OCMKt/V), total clearance delivered per session (Kt), total ultrafiltration volume (VUF) and substitution volume (VSUB) per session, albumin, Hemoglobin.
- 2.
- Patients
This study enrolled 68 stage 5 chronic kidney disease dialysis dependent patients (CKD5D) receiving high volume hemodiafiltration. Ten were incident patients (< 3 months treatment) and 58 were prevalent patients (≥3 months treatment). Some incident patients were converted during the study to arteriovenous fistula or graft access.
- 3.
- Ethics statement
The study was conducted according to the principles of the Declaration of Helsinki and in compliance with International Conference on Harmonization/Good Clinical Practice regulations. According to the French Law, the study has been registered at “Ministère de la Santé et des Solidarités” after approval by the Montpellier University Hospital’s ethics committee (Comité de Protection des Personnes Sud Méditerranée IV) with the following number DC-2008-417. All patients gave their written informed consent.
- 4.
- Vascular accesses
DualCath (DCath) is manufactured by MedComp in USA and distributed in Europe 23-26. DCath consists of two independent single lumen silicon catheters and their tubing extension adaptor are presented separately, with all material required for insertion (2 single lumen silicone cannula with their semi-rigid plastic stylets, straight tunneler, syringes, needle, sutures, large bore needles, two wire guides 50 cm, two external adaptors, two introducer-dilator catheters), packaged in a sterile tray protected by a double transparent plastic film.
DCath consists of two single lumen silicone cannulas with separate tubing extension adaptors that are docked together at the time of insertion. They present circular mark every 5 cm to precisely know length of the catheter. The intravascular cannula is made of radiopaque silicone polymer tubing (length 40 cm, inner/outer diameters 2.0/3.2 mm). The length of cannulas is adjusted at the time of insertion to patient anthropometry. As such, DCath may differ according to patient height and side of insertion: 25–27 cm and 30–32 cm for the right and left sides respectively. Six holes are disposed spirally along their distal tip. The extension or adaptor is made of 6-7 cm silicone polymer of larger diameter ending in a nylon luer-lock connection device with colored marks (blue, venous; red, artery).
- 4.1.
- DualCath Insertion
DCath insertion relies on a percutaneous method performed under local anesthesia by trained nephrologist in a clean room or theater with support of a nurse and appropriate environment and material (bed, resuscitation, light, medication, gas). Most of DCath insertions were performed under local anesthesia, sometimes with support of nitrogen dioxide gas under mask, rarely DCath insertion required general anesthesia (complex case, anxiety). Patient preparation consisted of skin washing, nonabrasive shaving and iodine disinfection (betadine) 1 hour before DCath insertion.
Choice of the central vein location depends on the anatomical condition of the patient. Vast majority of patients had DCath inserted in the right internal jugular vein, few had insertion in the left internal jugular or femoral vein as alternative options. For practical reason, vein cannulation was mainly based on landmark technique rather than guided by US mapping. Vein US mapping was mostly applied in complex cases. During the preparation of catheter insertion, landmarking of skin area and vein location was performed and drawn on skin with surgical skin marker.
Vein cannulation was performed using strictly aseptic surgical conditions, including mask, hat, sterile gown and gloves for the operator and sterile drapes covering most of patient body and leaving access to the region of interest.
DCath insertion consists usually in five main steps. In the case of right internal jugular vein cannulation, a brief description of the different steps is given here:
- The first step consists of local anesthesia in the prethoracic area and at the base of the neck region at the top of the Sedillot triangle.
- The second step consists in locating the right internal jugular vein and inserting the two silastic cannulas into the right internal jugular vein based on a percutaneous-based method using a desilet technique relying on an introducer and a vein dilator.
- The third step consists of tunnelling each cannula with a metallic tunneler advanced in the subcutaneous tissue through the cervical hole downward following the anesthetized track and exiting in the prethoracic area. Cannula is firmly attached to the tunneler with a tressed nylon suture which is then passed through tunnel with cannula. The second cannula is tunneled with the same method in a parallel subcutaneous track.
- The fourth step consists in shortening the cannulas to fit chest patient size with use of space band marks, putting on a silicone rubber collar, and then docking the external extension piece ending by luer-lock connector to the cannula. Cannula and tubing extension assembly are then rigidified by plastic stylet and pushed back with a twisting movement through the enlarged skin exit. Cannulas are then rinsed with saline and clamped with a vascular atraumatic clamp. Anchoring the two cannulas together is then performed with a subcutaneous nylon suture through the jugular neck hole. The two threads emerging from the cervical cutaneous orifice are recovered, isolated, and firmly tied together to create a bridge suture between the two cannulas (stays).
- The fifth step consists in closing skin cutaneous orifice with intradermal sutures, rinsing, locking cannulas with antithrombotic solution and capping them with Luer-lock caps.
- 4.2.
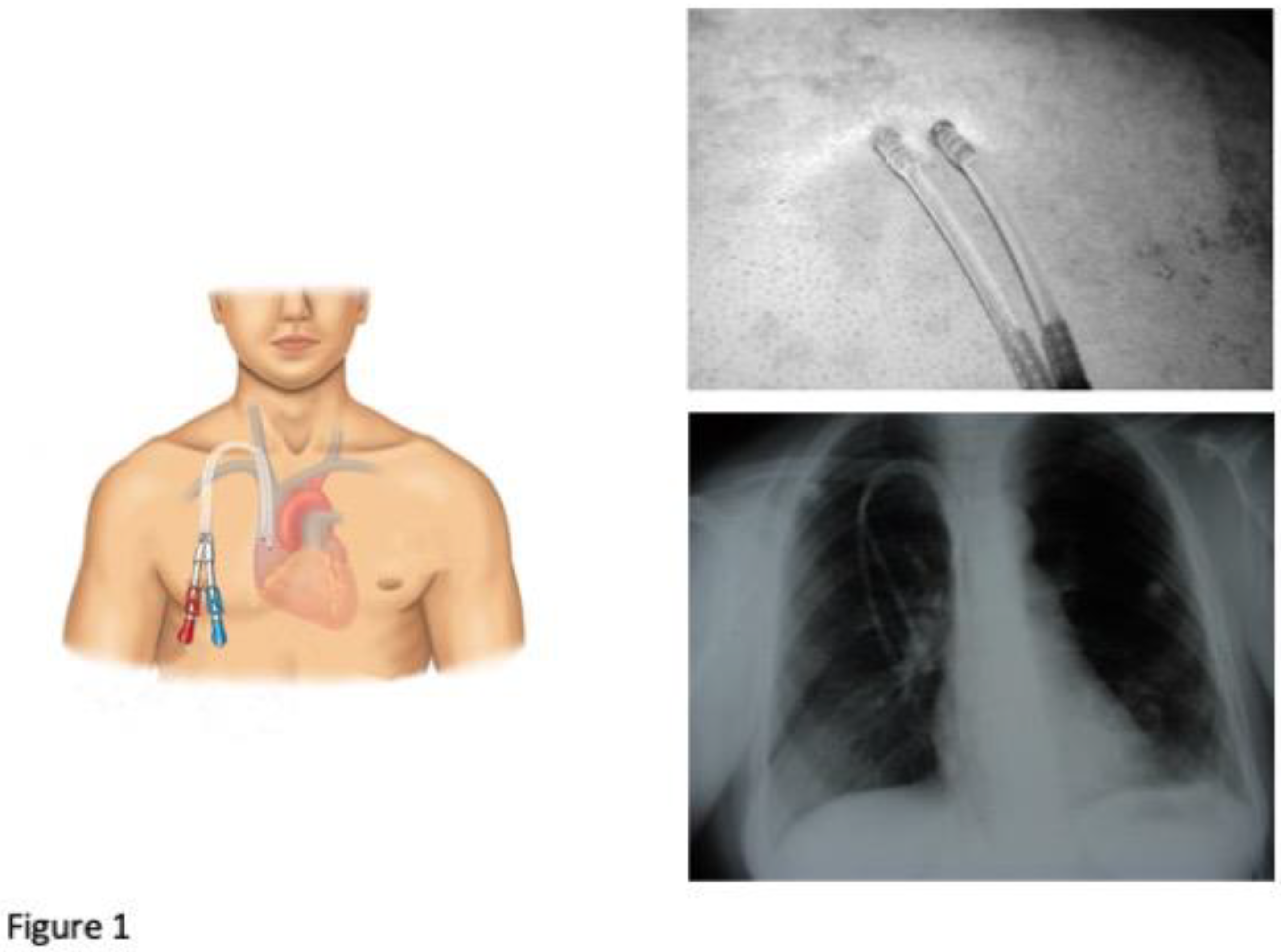
- DualCath Looking and Imaging (Figure 1)
Figure 1 presents a cartoon of the DCath inserted in the right internal jugular vein with a picture of the skin exit looking. Chest X-Ray is performed before catheter use to secure catheter position and check the lack of abnormalities or complications.
Figure 1.
Cartoon of the DCath inserted in the right internal jugular vein with a picture of the skin exit looking. Chest X-Ray is performed before catheter use to secure catheter position and check the lack of abnormalities or complications.
Figure 1.
Cartoon of the DCath inserted in the right internal jugular vein with a picture of the skin exit looking. Chest X-Ray is performed before catheter use to secure catheter position and check the lack of abnormalities or complications.
- 4.3.
- DualCath Management and Handling
DCath are used exclusively for hemodialysis purpose and any other use (i.e., IV perfusion, blood sampling) is strictly prohibited. DCath are handled by trained nurses (i.e., bearing sterile gown, mask, hat, gloves) in strictly surgical aseptic conditions (ie, sterile drape protection at time of connecting and disconnecting extracorporeal blood circuit). At the time of connection, remaining blood material and antithrombotic solution within each line of DCath is withdrawn with a 10-ml syringe and discarded. Isotonic saline (5 to 10 ml) is then flushed vigorously in each line of DCath to clean and probe resistance of DCath. Extracorporeal blood circuit is then initiated by connecting each DCath line to the corresponding blood line and blood pump is launched and brought progressively to its prescribed speed. At the time of disconnection, blood pump is stopped, and blood is flushed back and returns to patient (about 200-300 ml of saline) by means of online rinsing option alternatively on the arterial and venous side. Blood lines are disconnected, and each line of DCath is filled and locked with a mixture of saline and 0.3% citric acid solution (2.5 to 2.8 ml per catheter line).
Luer-lock cap is then screwed. DCath are wrapped in a split sterile gauze and a transparent sterile adhesive waterproof air-permeable dressing is applied and kept until next dialysis session.
- 4.4.
- Arteriovenous access management
Arteriovenous fistula or grafts are handled with particular care and strictly hygienic conditions relying on betadine as skin disinfectant, using sterile material, drape and gloves as well as mask, gown and cap for the operator at the time of access handling. Needling is performed by trained nurse with fistula needle of 15 gauges in majority of patients using laden rope method.
- 5.
- Clinical performances assessed
Baseline clinical performances consisted in six key performance indicators that included the effective blood flow (ml/min), venous pressure (mmHg), vascular access recirculation (VA.REC) (%), single pool Kt/V, double pool Kt/V and convection volume (l/session).
These indicators were measured in the six following vascular accesses: native arteriovenous fistula (AVF), arteriovenous graft (PTFE)(AVG), right femoral DCath (RFDC), right internal jugular DCath (RIJDC), left internal jugular DCath (LIJDC) and Thomas Shunt.
In addition, cumulative clinical performances comparing DCath and grouped AVA over a 30-month follow-up period were performed.
- 5.1.
- Blood flow (QB, ml/min)
Blood flow measurement was performed by means of bubble transit time on 1 meter of a calibrated segment of the arterial line27. This method is currently used in our unit and fits perfectly with Transonic data. Calculation of effective blood flow relies on the following formula:
- 5.2.
- Total blood volume processed (TBVP, L/session)
Total blood volume processed was calculated from dialysis machine as the product of the effective blood flow (QB) times treatment time (tHD) as TBVP = QB x tHD
- 5.3.
- Vascular access recirculation (VA.REC, %)
Total recirculation (T.REC) was calculated by using urea dosing issued from three blood samplings (artery (ART) and venous (VEN) sampling, then followed by a second artery sampling after 2 minutes stop of blood pump (ART+2)) as follows27,28:
T. REC = (ART+2 - ART)/(ART+2 – VEN) x 100
This method has been validated in our unit and used as standard of care for years. Results fit perfectly with recirculation obtained with Blood Thermal Monitoring device which also assesses total recirculation. When compared to Transonic data, it has been shown that 10% was coming from the cardiopulmonary bypass created by the arteriovenous bypass16,29. A 10% value of cardiopulmonary bypass was then subtracted from arteriovenous access measurements but not from tunneled central venous accesses as follows:
VA. REC = T.REC – 10 (for arteriovenous accesses only)
- Dialysis dose delivery
Dialysis dose delivery was assessed with three key indicators: firstly, the urea clearance expressed as fractional urea clearance (i.e., ureaKt/V), or its surrogate using ionic clearance (online clearance measurement, OCMKt/V)30,31 and as total urea clearance (Kt) delivered per session (i.e., liters per session) to quantify small molecules clearances30,32,33; secondly, the total ultrafiltration volume (liter per session) or convective dialytic dose used as surrogate marker of middle and large molecule clearances34; thirdly, percent reduction of ß2M (%) per session.
- 5.4
- Urea Kt/V
Urea Kt/V was calculated from pre and postdialysis blood sampling using the single-pool35 (sp) and equilibrated (e) double-pool Kt/V formula from Daugirdas36 as follows. Of note, postdialysis blood sampling was performed after reducing blood pump down to 50 ml/min for two minutes.
where WL is the weight loss during the session, BW the body weight and tHD the effective treatment time
spKt/V = - Ln (Ureapost/Ureapre – 0,008 x tHD) + (4 -3,5 x Ureapost/Ureapre) x WL/BWpost
eKt/V = spKt/V – (0,6 x spKt/V/tHD) + 0,03
- 5.5.
- Ionic dialysance and ocm Kt/V
Ionic dialysance Kt/V and ocmKt/V was measured and calculated from dialysis monitor using integrated ionic dialysance (Kocm) performed across dialysis session, effective HD machine treatment time (tHD) and total body water (V) derived from Watson formula by default.
- 5.6
- Total Kt (TKt, L/session)
Total Kt was calculated as the product of ionic clearance (Kocm) and effective treatment time (tHD) of dialysis session as TKt = Kocm x tHD
- 5.7.
- Total ultrafiltration volume (VUF, L/session)
The total ultrafiltration volume (VUF) is the sum of online substitution volume infused during the HDF session (VSUB) plus intradialytic weight loss (WL) to correct fluid overload. This indicator is used as surrogate of convective dialytic dose delivered per session34.
- 5.8.
- Percent reduction of β2-Microglobulin (PRβ2M)
Percent reduction of β2M was used as a marker of HDF efficiency as patients were receiving HDF treatment34. Postdialysis β2M was corrected for hemoconcentration using Bergstrom formula37
cor β2M = post β2M (1 + ∆BW/0.2BWpost)
where ∆BW is the difference between pre and post-treatment BW.
PRβ2M was calculated as follows:
PRβ2M = 1 – (corβ2Mpost/β2Mpre) x 100
- 5.9.
- Normalized protein catabolic rate (nPCR)
nPCR (g/kg/24h) was calculated from urea kinetic modeling using the three points method38 (pre/post and pre next dialysis session)
Blood samples were analyzed on the same day in the central laboratory of our hospital using validated autoanalyzer methods.
- 6.
- Statistics
Statistical analyses were performed using JASP Software 0.17.1 (University of AMSTERDAM). Normality and variance equality tests were made for all data, and statistical significance level was set to p <0.05 for all analyses. Continuous variables were reported as means (SD) or as medians [25-75%] depending on whether the data were normally distributed or not. Categorical variables were reported as percentages with number in parentheses. Unpaired normally distributed continuous variables were tested for difference using unpaired t-test. Unpaired non-normally distributed continuous data were analyzed using Mann-Whitney test. Pearson’s or Spearman’s test were used for correlation analyses depending on whether data were normally distributed or not, respectively.
3. Results
3.1. Patient characteristics
The cohort consisted of 27 females (age 72 [66.5-75.5] yo.) and 41 males (age 68.5 [60.0-75.0] yo.) with a dialysis vintage of 9 [2.5-30] months. Primary kidney diseases were as follows: hypertension and/or ischemic nephropathy 28 (41.2%); Diabetic kidney disease 11 (16.2%); Chronic glomerulonephritis 8 (11.8%); Toxic kidney disease 6 (8.8%); Autosomic polycystic kidney disease 4 (5.9%); Alport 1 (1.5%); Interstitial chronic nephritis uropathy 1 (1.5%); unknown 9 (13.2%). Six patients with toxic kidney disease had received an organ transplant (heart 1, liver 2, kidney 3). Main patient characteristics are given in Table 1.

Table 1.
Patient characteristics at baseline.

(BW, body weight; Vupost; Alb, albumin; Pre-alb, pre-albumin; Ht, hematocrit; TP, total protein; nPCR, normalized protein catabolic rate).
3.2. Renal replacement treatment schedule
All patients received online postdilution hemodiafiltration. Treatment schedule consisted of three sessions weekly, 4 hours in 90% of patients and 3 or 3.5 hours in the remaining 10%. Single-used hemodiafilters were made of high-flux polysulfone or polyethersulfone (FX1000, 34.4%; FX800, 59.4%; Arylane H9, 2%). Anticoagulation consisted of a single bolus injection of Fraxiparin (Nadroparin 2000-6000 IU), a low molecular weight heparin, on the venous needle or within catheter line before initiating the extracorporeal circuit. Main features of renal replacement therapy are given in Table 2.
Table 2.
Renal replacement therapy treatment schedule.

(tHD, dialysis duration; REC.VA, vascular access recirculation; Qb eff, effective blood flow; TBVP, total blood volume processed; Vinf, total infusion volume; Vuf, total ultrafiltration volume).
3.3. Baseline clinical performances (3 months)
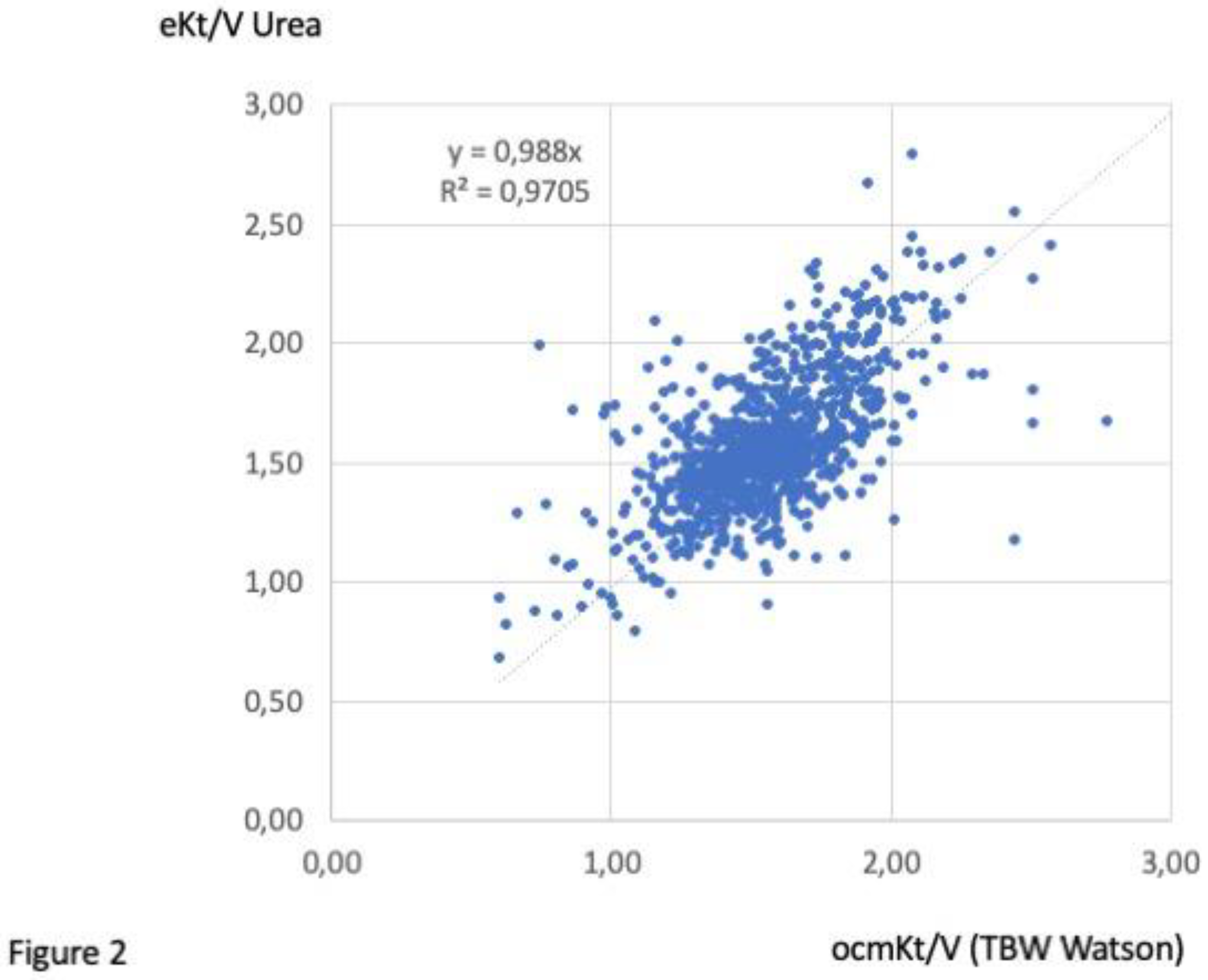
Baseline clinical performances are presented in Table 3. N stands for Number of patients given (first row) and number of measures given (second row). Median and interquartile values are given for each key performance indicator for each access type (Table 3). As shown, the effective blood flow achieved was virtually similar (400 mL/min) in each vascular access including DCath. Recirculation was significantly higher with DualCath in average 7% (6 to 13%) but higher with LIJDC. Dialysis dose delivered (Kt/V) was virtually equivalent across all vascular accesses if we account for differences in patients’ body weight and total body water. In all cases, including DCath, median value of Kt/V was superior to 1.70 (spKt/V) or 1.5 (eKt/V). Of note, we also explored the correlations between OCMKt/V and eKt/V values to confirm the validity of such routine parameters as observed in Figure 2. Convective volumes tend to be lower with DCath compared to arteriovenous accesses (AVF, AVG and TS) but still higher than 23 liters per session as recommended. Percent reduction ß2M with DCath was 4 to 10 % lower than AVF, AVG or Thomas shunt still achieving 72.6 and 75.4 percent per session.
Table 3.
Baseline clinical performances (over the first 3 months).
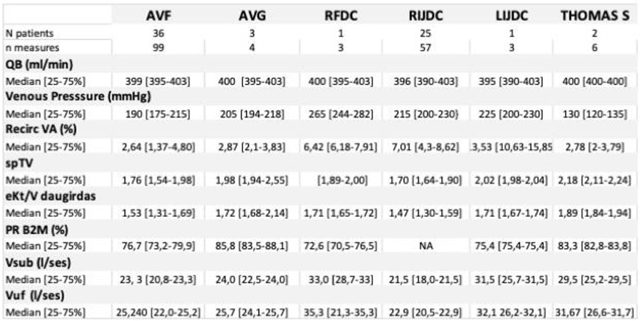
(AVF, native arteriovenous fistula; AVG, arteriovenous graft PTFE; RFDC, right femoral DualCath; RIJDC, right internal jugular DualCath; LIJDC, left internal jugular DualCath; Qb, blood flow; REC.VA, vascular access recirculation;PR, Percentage of reduction; Vsub, substitution volume; Vuf, ultrafiltration volume).
Figure 2.
Correlation between OCMKt/V and eKt/V.
3.4. Clinical performances (over a 30-month follow-up)
3.4.1. Cumulative clinical performances comparing DualCath (DCath) and grouped Arterio-Venous Accesses (AVA).
Vascular accesses are grouped as AVAs and DCath and median values of key performance indicators are presented in Table 4. As shown, patients bearing DCath tended to have a smaller body weight compared to patients treated through AVA. They also tended to have a slightly lower blood flow and a higher recirculation translating in a slightly and significantly lower dialysis dose delivered for small molecules (Kt/V and Kt) but not for convection volume (22.5 vs 25.4, NS) and percent reduction of ß2M per session (74 vs. 78%, NS). Indeed, the effective dialysis dose achieved with DCath was much higher than that recommended by best practice guidelines. This fact is confirmed by stability over time of nutritional markers such as albumin, prealbumin (transthyretin) or normalized protein catabolic rate (nPCR). CRP and fibrinogen used as indicators of inflammation were similar in all vascular access groups. Additionally, key parameter indicators of dialysis adequacy (fluid volume status, blood pressure, electrolytic control, bone mineral disorder, anemia) were maintained in target for both types of vascular access.
Table 4.
Cumulative clinical performances comparing DualCath (DCath) and grouped Arterio-Venous Accesses (AVA) (over a 30-month follow-up).
Table 4.
Cumulative clinical performances comparing DualCath (DCath) and grouped Arterio-Venous Accesses (AVA) (over a 30-month follow-up).
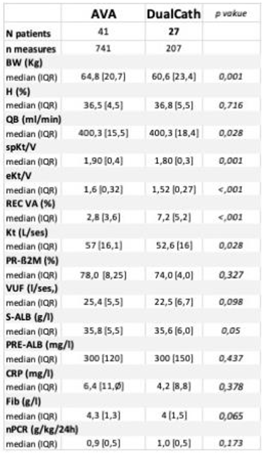
(AVA, arteriovenous access; BW, body weight; Ht, hematocrit; Qb, blood flow; REC.VA, vascular access recirculation; PR, percentage of reduction; Vuf, total ultrafiltration volume; pre-alb, pre-albumin; nPCR, normalized protein catabolic rate).
3.4.2. Longitudinal follow-up
Two main indicators of dialysis dose delivery including the effective urea clearance throughout the complete session (Figure 3) and the middle and large molecule clearance as reflected by the total ultrafiltration volume (VUF) (Figure 4) were monitored throughout the 30 months of follow-up for the two types of vascular access (AVA, Arterio-Venous Access; DC, DCath) As shown in both cases, dialysis dose delivered was maintained relatively stable over the total observational period. Small molecule clearances were slightly higher with AVA versus DCath, while total ultrafiltration volume, used in that case as a surrogate of middle molecule clearance was not different from DCath.
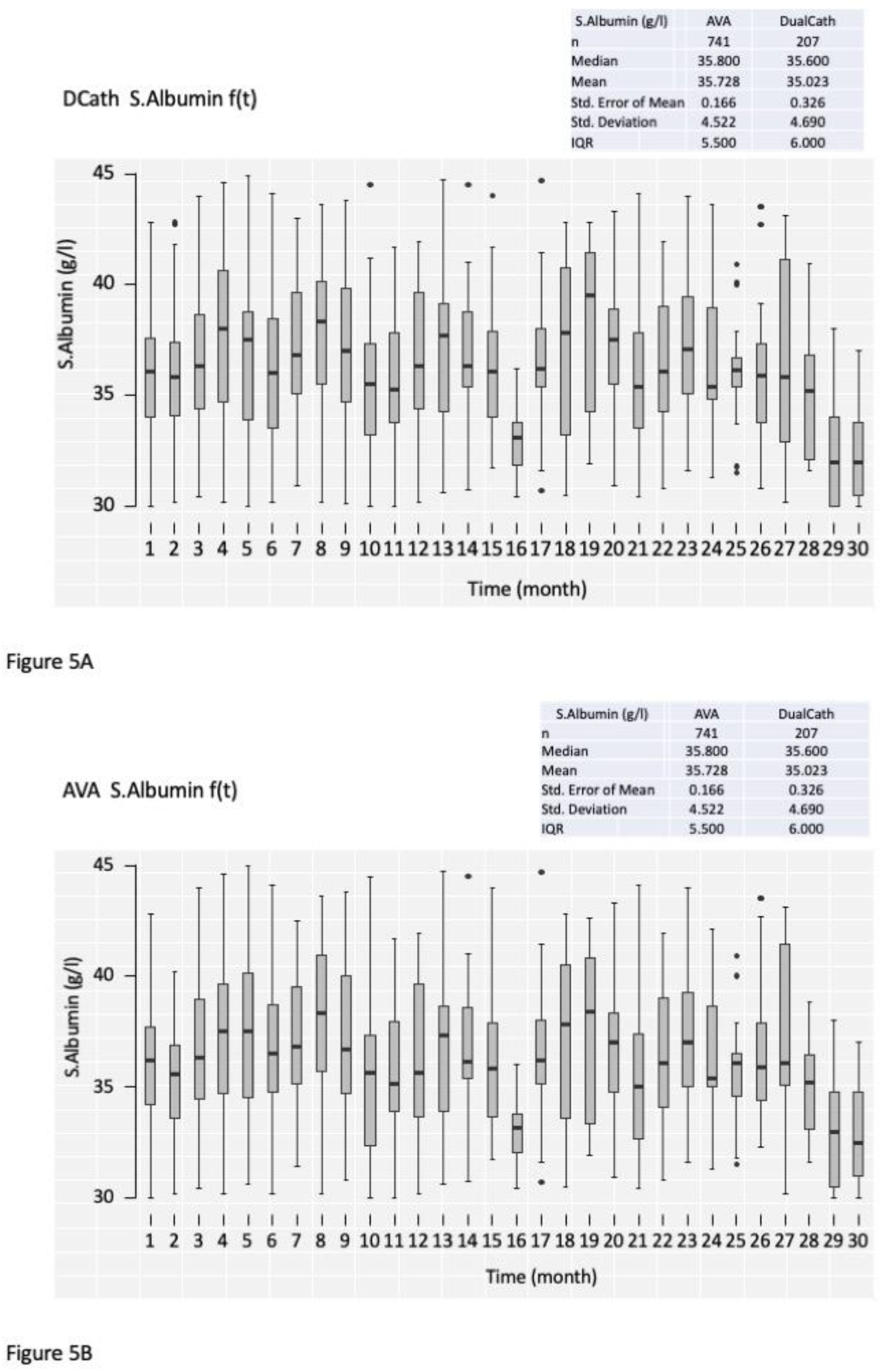
Serum albumin concentration as an integrated biomarker of dialysis adequacy and safety of the method, nutritional and inflammation status, was also monitored over the 30 months and reported in Figure 5.
Figure 3.
Effective urea clearance (dpKt, expressed in liters per session) over the 30 months of follow-up in A) DCath and B) AVA.
Figure 3.
Effective urea clearance (dpKt, expressed in liters per session) over the 30 months of follow-up in A) DCath and B) AVA.
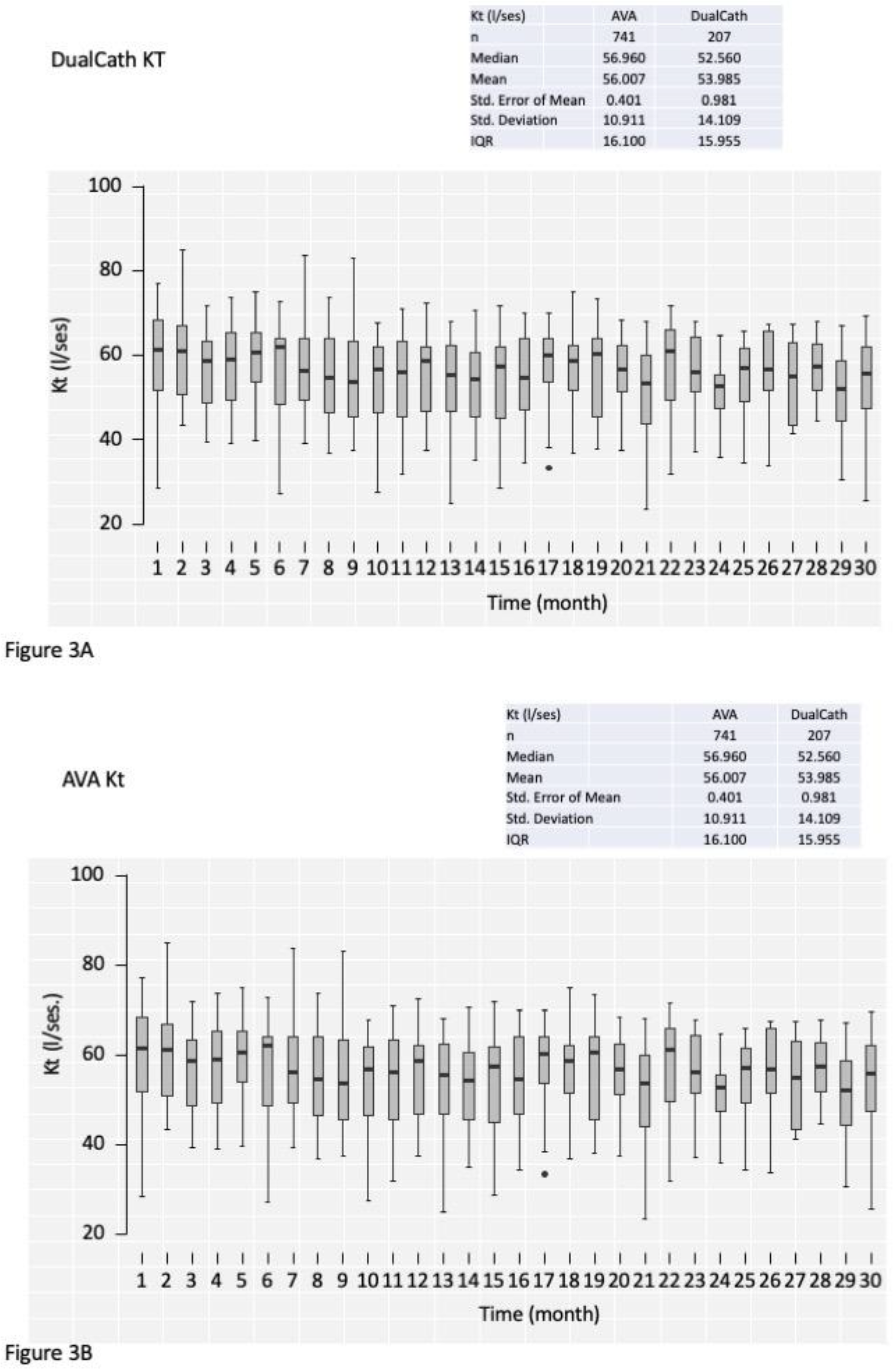
Figure 4.
Convective volume (expressed in liters per session) over the 30 months of follow-up in A) DCath and B) AVA.
Figure 4.
Convective volume (expressed in liters per session) over the 30 months of follow-up in A) DCath and B) AVA.
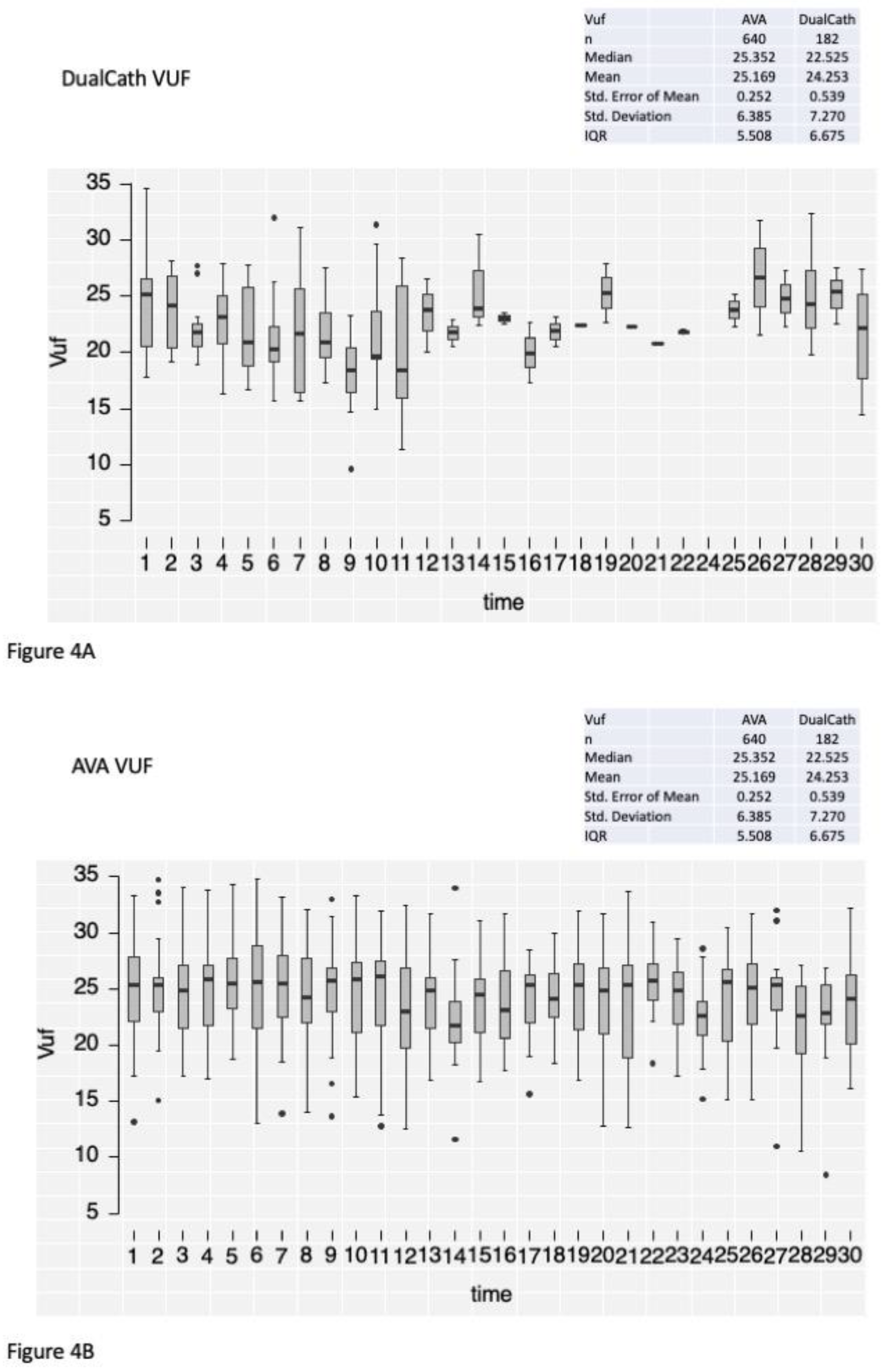
Figure 5.
Serum albumin over the 30 months of follow-up in A) DCath and B) AVA.
4. Discussion
- Main findings of our study:
In this retrospective study consisting of 68 maintenance dialysis patients, we assessed precisely clinical performances delivered throughout tunneled central venous catheters (DCath) and compared them to various arteriovenous accesses (AVA) used routinely in our dialysis facility. For this purpose, we used monthly quality control measures with 30 months followed-up. As most original finding of our study is the fact that DCath were shown to deliver high blood flow (400 ml/min) and achieved high volume hemodiafiltration on a regular basis with comparable results to AVA. As second finding, the study highlighted the fact that dialysis dose delivered, either for small sized molecules (total urea clearance) or middle-sized molecules (total ultrafiltration volume and β2M reduction rate) was almost similar with DCath and AVA, was higher than the targets recommended by clinical best practice guidelines and remained stable over time up to 30 months. The main difference relies on the fact that recirculation with DCath was significantly higher (≈7%) than AVA resulting in a total urea clearance with DCath slightly lower than AVA. Interestingly, this recirculation didn’t impact the total ultrafiltration volume which remained almost similar with DCath and AVA. In all cases, dialysis performances and key performance indicators were not affected while DCath were used as mainstream vascular access.
- Literature comparison:
This finding is in quite contrast with previous studies reporting that tunneled CVC tends to be associated with a reduction of dialysis dose delivered due to the limited blood flow and increase in vascular access recirculation, but also precluding use of high volume hemodiafiltration21,39,40. In fact, the apparent superiority of DCath compared to other tunneled central venous catheters relies on three main components: firstly, to the geometry and the design of cannulas that are specifically engineered (two independent cannulas, adjustable to patient anthropometry, with side holes at the tips) to provide high blood flow with relatively low blood flow resistance; secondly, to the careful way of inserting and positioning tips in central venous system at time of implantation, mainly at junction of superior vena cava and right atrium for internal jugular vein site, but alternatively in inferior vena cava for femoral site; thirdly, to the strict and careful catheter handling protocol consisting in using locking solutions (antithrombotic, fibrinolytic) to maintain or restore catheter flow permeability41.
Each of these components has been clearly documented in the scientific literature13. Two single cannulas made of soft silastic with adequate inner lumen (≥ 2 mm) and distal side holes tend to provide higher and more sustainable blood flow during dialysis session than double lumen semi-rigid polyurethane conventional catheters12,13,21,42. Tips positioning at the junction of superior vena cava and right atrium also tend to reduce risk of poor blood flow occurring during dialysis session due to the hypovolemia associated with the ultrafiltration43. In addition, side holes present at the tips of catheters keep lines in the core flow of the vein and prevent sucking vein walls. Higher flow achieved with side holes catheters has been challenged in some studies by thrombosis and infectious risk14,15.
Silastic cannulas made of soft rubber tend to be the most hemocompatible material reducing platelet adhesion, catheter thrombosis risk and bacterial adhesion44. This mechanistic interpretation of phenomenon has been illustrated in some catheter flow modeling studies from simulation in silico experiment45. Another important factor relies on the strict implementation of best practices catheter handling developed by nursing team46. Aside strict aseptic conditions applied to catheter handling, a new science of catheter locking solution has been developed and has been shown to be very efficient in maintaining catheter lumen patency47-50. It is not our intent to review catheter locking practices, but we refer readers interested to recent comprehensive reviews on this topic. In our unit, locking solutions have been always at the heart of catheter care practices. We moved from conventional heparin locking solution to more personalized and adaptative locking solutions involving more citrate-based solutions and/or fibrinolytic solutions guided by blood flow and/or pressure regime changes in the recent time.
- Strength and weakness of our study:
Strength of our study relies on the precise quantification and comparison of dialysis performances achieved with DCath compared to conventional arteriovenous accesses (AVF, AVG) used to deliver high volume hemodiafiltration in a relatively large number of dialysis patients followed up for 30 months. This is in clear contrast with a previous large cohort study showing that high volume HDF (>21 l) was achieved in 33% of prevalent patients51. Safety and risk assessment associated with DCath use is currently assessed in another multicenter study.
Our study has weaknesses that we want to highlight. Firstly, this is a single center study performed by well-trained physicians and nursing team dedicated to vascular access management and therefore transferability to larger centers may be questionable. Secondly, the number of patients may appear limited, but this is due to the academic hospital-based dialysis facility with large turnover of patients. Thirdly, a comparative economic evaluation between DCath and AVA was not done in this study.
- Implications for clinical practices:
As our study indicates, the use of tunneled CVC is not associated with worst vascular access scenario in dialysis patients. As such, by means of DCath, we were able to perform high volume hemodiafiltration with high blood flow in all patients for sustained period up to 30 months. This is a quite reassuring finding, since it makes possible to consider treating fragile patients (i.e., elderly, diabetic, cardiac) or patients without AVF or AVG by most efficient convective-based treatment modalities, currently high volume hemodiafiltration. In other words, tunneled central venous catheter should not be considered as a limiting factor in providing most efficient treatment modality provided the right tunneled CVC is used.
Conclusion
As shown through this study, high-flow DCath tunneled two single lumen silicone catheters may be used in dialysis-dependent chronic kidney disease patients to deliver high volume hemodiafiltration like arteriovenous accesses. Although, results obtained with DCath tended to be slightly lower than those achieved with arteriovenous accesses, they remained far above best practice guidelines, indicating that DCath were not compromising optimal clinical performances. In addition, clinical performances of DCath remained stable and achieved in a consistent manner over time. These results support the notion that design and geometry of the two silicone cannulas are optimal, and that the strict adherence to best catheter practices is clue to success in tunneled central venous catheter use.
References
- Schmidli J, Widmer MK, Basile C, et al. Editor’s Choice - Vascular Access: 2018 Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2018;55:757-818. [CrossRef]
- Lok CE, Huber TS, Lee T, et al. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. Am J Kidney Dis 2020;75:S1-s164. [CrossRef]
- Tordoir J, Canaud B, Haage P, et al. EBPG on Vascular Access. Nephrol Dial Transplant 2007;22 Suppl 2:ii88-117.
- Ravani P, Palmer SC, Oliver MJ, et al. Associations between hemodialysis access type and clinical outcomes: a systematic review. J Am Soc Nephrol 2013;24:465-73.
- Fissell RB, Fuller DS, Morgenstern H, et al. Hemodialysis patient preference for type of vascular access: variation and predictors across countries in the DOPPS. J Vasc Access 2013;14:264-72. [CrossRef]
- Pisoni RL. Vascular access use and outcomes: results from the DOPPS. Contrib Nephrol 2002:13-9.
- Pisoni RL, Young EW, Dykstra DM, et al. Vascular access use in Europe and the United States: results from the DOPPS. Kidney Int 2002;61:305-16. [CrossRef]
- Rayner HC, Besarab A, Brown WW, Disney A, Saito A, Pisoni RL. Vascular access results from the Dialysis Outcomes and Practice Patterns Study (DOPPS): performance against Kidney Disease Outcomes Quality Initiative (K/DOQI) Clinical Practice Guidelines. Am J Kidney Dis 2004;44:22-6.
- Desmeules S, Canaud B. Venous access for chronic hemodialysis: “undesirable yet unavoidable”. Artif Organs 2004;28:611-6. [CrossRef]
- Di Iorio B. Central Venous Catheters in hemodialysis: an actual conundrum without solutions. J Vasc Access 2002;3:174-6. [CrossRef]
- Sohail MA, Vachharajani TJ, Anvari E. Central Venous Catheters for Hemodialysis-the Myth and the Evidence. Kidney Int Rep 2021;6:2958-68. [CrossRef]
- Ash SR. The evolution and function of central venous catheters for dialysis. Semin Dial 2001;14:416-24.
- Ash SR. Advances in tunneled central venous catheters for dialysis: design and performance. Semin Dial 2008;21:504-15.
- Silverstein DM, Trerotola SO, Clark T, et al. Clinical and Regulatory Considerations for Central Venous Catheters for Hemodialysis. Clin J Am Soc Nephrol 2018;13:1924-32. [CrossRef]
- Tal MG, Peixoto AJ, Crowley ST, Denbow N, Eliseo D, Pollak J. Comparison of side hole versus non side hole high flow hemodialysis catheters. Hemodial Int 2006;10:63-7. [CrossRef]
- Leblanc M, Bosc JY, Paganini EP, Canaud B. Central venous dialysis catheter dysfunction. Adv Ren Replace Ther 1997;4:377-89. [CrossRef]
- McIntyre CW, Hulme LJ, Taal M, Fluck RJ. Locking of tunneled hemodialysis catheters with gentamicin and heparin. Kidney Int 2004;66:801-5. [CrossRef]
- Saxena AK, Panhotra BR. Locking hemodialysis catheters with cefotaxime instead of gentamicin to avoid potential ototoxicity. Kidney Int 2005;67:2505-6. [CrossRef]
- Stas KJ, Vanwalleghem J, De Moor B, Keuleers H. Trisodium citrate 30% vs. heparin 5% as catheter lock in the interdialytic period in twin- or double-lumen dialysis catheters for intermittent haemodialysis. Nephrol Dial Transplant 2001;16:1521-2.
- Polderman KH, Girbes AJ. Central venous catheter use. Part 1: mechanical complications. Intensive Care Med 2002;28:1-17.
- Trerotola SO, Shah H, Johnson M, et al. Randomized comparison of high-flow versus conventional hemodialysis catheters. J Vasc Interv Radiol 1999;10:1032-8. [CrossRef]
- Van Der Meersch H, De Bacquer D, Vandecasteele SJ, et al. Hemodialysis catheter design and catheter performance: a randomized controlled trial. Am J Kidney Dis 2014;64:902-8. [CrossRef]
- Canaud B, Beraud JJ, Joyeux H, Mion C. Internal jugular vein cannulation using 2 silastic catheters. A new, simple and safe long-term vascular access for extracorporeal treatment. Nephron 1986;43:133-8.
- Canaud B, Leray-Moragues H, Garred LJ, Turc-Barron C, Mion C. What is the Role of Permanent Central Vein Access in Hemodialysis Patients. Semin Dial 1996;9:397-400.
- Canaud B, Leray-Moragues H, Garrigues V, Mion C. Permanent twin catheter: a vascular access option of choice for haemodialysis in elderly patients. Nephrol Dial Transplant 1998;13 Suppl 7:82-8.
- Canaud B, Leray-Moragues H, Kerkeni N, Bosc JY, Martin K. Effective flow performances and dialysis doses delivered with permanent catheters: a 24-month comparative study of permanent catheters versus arterio-venous vascular accesses. Nephrol Dial Transplant 2002;17:1286-92.
- FA G. Hemodialysis: Technique and kinetic considerations. in The Kidney, edited by Brenner BM, Rector FC Jr, Philadelphia, WB Saunders Company, 1976 1976;Chapter 41:1673.
- Thomas M, Argiles A, Kerr PG, Canaud B, Flavier JL, Mion CM. Measurement of vascular access recirculation without contralateral venous puncture. Nephron 1992;62:224-5. [CrossRef]
- Leblanc M, Bosc JY, Vaussenat F, Maurice F, Leray-Moragues H, Canaud B. Effective blood flow and recirculation rates in internal jugular vein twin catheters: measurement by ultrasound velocity dilution. Am J Kidney Dis 1998;31:87-92. [CrossRef]
- Aslam S, Saggi SJ, Salifu M, Kossmann RJ. Online measurement of hemodialysis adequacy using effective ionic dialysance of sodium-a review of its principles, applications, benefits, and risks. Hemodial Int 2018;22:425-34.
- Kuhlmann U, Goldau R, Samadi N, et al. Accuracy and safety of online clearance monitoring based on conductivity variation. Nephrol Dial Transplant 2001;16:1053-8. [CrossRef]
- Lowrie EG, Li Z, Ofsthun N, Lazarus JM. The online measurement of hemodialysis dose (Kt): clinical outcome as a function of body surface area. Kidney Int 2005;68:1344-54. [CrossRef]
- Maduell F, Ramos R, Varas J, et al. Hemodialysis patients receiving a greater Kt dose than recommended have reduced mortality and hospitalization risk. Kidney Int 2016;90:1332-41. [CrossRef]
- Tattersall JE, Ward RA. Online haemodiafiltration: definition, dose quantification and safety revisited. Nephrol Dial Transplant 2013;28:542-50. [CrossRef]
- Daugirdas JT. Simplified equations for monitoring Kt/V, PCRn, eKt/V, and ePCRn. Adv Ren Replace Ther 1995;2:295-304. [CrossRef]
- Daugirdas JT, Schneditz D. Overestimation of hemodialysis dose depends on dialysis efficiency by regional blood flow but not by conventional two pool urea kinetic analysis. Asaio j 1995;41:M719-24. [CrossRef]
- Bergström J, Wehle B. No change in corrected beta 2-microglobulin concentration after cuprophane haemodialysis. Lancet 1987;1:628-9.
- Garred LJ, Canaud B, Argiles A, Flavier JL, Mion C. Protein catabolic rate determination from a single measurement of dialyzed urea. Asaio j 1995;41:M804-9. [CrossRef]
- Trerotola SO. Catheters: A Necessary Evil? Journal of Vascular and Interventional Radiology 2004;15:P206-P9.
- Trerotola SO, Kraus M, Shah H, et al. Randomized comparison of split tip versus step tip high-flow hemodialysis catheters. Kidney Int 2002;62:282-9. [CrossRef]
- Lok CE, Huber TS, Lee T, et al. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. Am J Kidney Dis 2020;75:S1-S164. [CrossRef]
- Power A, Hill P, Singh SK, Ashby D, Taube D, Duncan N. Comparison of Tesio and LifeCath twin permanent hemodialysis catheters: the VyTes randomized trial. J Vasc Access 2014;15:108-15. [CrossRef]
- Vesely TM. Central venous catheter tip position: a continuing controversy. J Vasc Interv Radiol 2003;14:527-34. [CrossRef]
- El Khudari H, Ozen M, Kowalczyk B, Bassuner J, Almehmi A. Hemodialysis Catheters: Update on Types, Outcomes, Designs and Complications. Semin Intervent Radiol 2022;39:90-102. [CrossRef]
- Lucas TC, Tessarolo F, Jakitsch V, et al. Blood flow in hemodialysis catheters: a numerical simulation and microscopic analysis of in vivo-formed fibrin. Artif Organs 2014;38:556-65. [CrossRef]
- Vanholder R, Canaud B, Fluck R, et al. Diagnosis, prevention and treatment of haemodialysis catheter-related bloodstream infections (CRBSI): a position statement of European Renal Best Practice (ERBP). NDT Plus 2010;3:234-46. [CrossRef]
- Jaffer Y, Selby NM, Taal MW, Fluck RJ, McIntyre CW. A meta-analysis of hemodialysis catheter locking solutions in the prevention of catheter-related infection. Am J Kidney Dis 2008;51:233-41. [CrossRef]
- Weijmer MC, Debets-Ossenkopp YJ, Van De Vondervoort FJ, ter Wee PM. Superior antimicrobial activity of trisodium citrate over heparin for catheter locking. Nephrol Dial Transplant 2002;17:2189-95.
- Weijmer MC, Kars SM, ter Wee PM. A scanning electron microscopy analysis of a spontaneous hemodialysis catheter fracture. Am J Kidney Dis 2001;38:858-61. [CrossRef]
- Weijmer MC, van den Dorpel MA, Van de Ven PJ, et al. Randomized, clinical trial comparison of trisodium citrate 30% and heparin as catheter-locking solution in hemodialysis patients. J Am Soc Nephrol 2005;16:2769-77. [CrossRef]
- Marcelli D, Scholz C, Ponce P, et al. High-volume postdilution hemodiafiltration is a feasible option in routine clinical practice. Artif Organs 2015;39:142-9. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



