Submitted:
12 June 2023
Posted:
13 June 2023
You are already at the latest version
Abstract
Background: Evidences on the effects of chemotherapy treatment cycles on measures of muscle, mental state, social and cognitive performance are scarce. Objective: To analyze the effects of chemotherapy cycles on muscle strength and activation, functional capacity, quality of life, fatigue and anxiety of women with breast cancer. Methods: Twenty-two women divided into a treatment group (n = 10; 46.6 ± 9.6 years) and control group (n = 12; 51.6 ± 7.0 years) participated in the study. Analysis of muscle performance, quality of life, fatigue and anxiety after the 2nd and 4th cycle of chemotherapy with anthracyclines and cyclophosphamide were performed in women with breast cancer (TRA) and compared to healthy women (CTR). Two-way ANOVA was used to compare the variance of the means and the significance level was set as p≤0.05. Results: Differences were found in the muscular activation of the vastus medialis between the groups at post time (p = 0.038), as well as in the sit and stand test in the baseline (p<0.001) and post moment (p<0.001). Functional capacity performance was different between baseline (p<0.001) and post-time (p<0.001) groups. Additionally, the TRA group worsened the quality of life in the domains of functional capacity (p<0.001) and limitation of physical aspects (p=0.002), besides presenting negative changes in fatigue. Conclusion: Anthracycline and cyclophosphamide chemotherapy cycles reduce muscular performance and affect biopsychosocial variables in women with breast cancer.
Keywords:
chemotherapy
; anthracyclines
; cyclophosphamide
; muscle strength
; quality of life
1. Introduction
Among the different types, breast cancer has a higher prevalence in women, with risk factors associated with chronic such as endocrine and reproductive diseases [1]. Breast cancer is as well as associated with lifestyle, previous pregnancy, familiar history, ethnicity, prolonged exposure to endogenous estrogens, obesity, as well as sedentary lifestyle and smoking [2,3]. Currently, the main forms of treatment involve surgery for tumor removal, chemotherapy (neoadjuvant or adjuvant), radiotherapy, hormone therapy and immunobiological agents [4].
Chemotherapy treatment has been shown to demonstrated efficiency in combating the disease, this treatment consists of cycles in which are used different combinations of medications, such as anthracyclines, cyclophosphamide and taxanes over a period between 10 and 12 weeks [5]. However, due to the toxicity of chemotherapy treatment at the cellular level, patients have side effects such as alopecia, anemia, vomiting, premature menopause, weight gain and increased fatigue, which can negatively impact the continuity of treatment [6].
In addition, some studies have shown changes in parameters related to muscle strength (MS) production resulting from the use of taxanes, as peripheral neuropathy [7], influencing overall physical fitness [8], reducing functional capacity (FC) and promoting negative changes on body composition [9,10]. Klassen et al. [11] analyzed the effects of chemotherapy treatment on muscle strength measurements in women with breast cancer using an isokinetic dynamometer, and identified a loss of up to 25% in strength responses and joint disfunction after treatment. However, due its cross-sectional design, the study did not present sufficient evidence to predict from which course of treatment the reductions in MS occur.
Chemotherapy treatment affect biopsychosocial parameters, which can be defined as subjective variables inherent to the individual's behavior in relation to external factors, by which they can change their temporary and chronic state in the biological, psychological and social spheres [12,13,14,15]. This therapy changes levels of fatigue, anxiety and quality of life [16,17,18,19,20,21], compromising the prognosis of individuals with cancer.
Despite evidence on adverse effects of chemotherapy [21], to date is unclear when this treatment begins to affect muscle strength, functional capacity and biopsychosocial responses. Therefore, the aim of the present study was to analyze the effects of anthracycline and cyclophosphamide chemotherapy cycles on MS and activation, FC, subjective perception of exertion, quality of life variables, fatigue, and anxiety.
2. Materials and Methods
Participants
The characteristics of the volunteers are described in Table 1. The sample size calculation was performed using G*power version 3.1.9. 4th software [22]. Considering an effect size of 0.6 (ES) with a power of 0.8 and significance of 0.05, a total of 20 participants (10 in each group) would be required. Therefore, 22 women were recruited, considering 10% more for possible loss. Volunteers were separated into treatment group (TRA) and control group (CTR) as described by Marques et al., [23] (n = 10 and 12, respectively).
The inclusion criteria of the volunteers for the TRA group were: to be between 30 and 70 years old; to be diagnosed with breast cancer; be between the 2nd and 3rd cycle of chemotherapy; to have medical release for physical exercise; not practicing any type of physical exercise. For the CTR group, the volunteers should: be between 30 and 70 years old; have medical clearance to perform physical exercise; not practice any kind of physical exercise and had no breast cancer diagnosis. Exclusion criteria were: hypertension; uncontrolled cardiovascular diseases; diabetes; metastasis; previous diagnosis of another type of cancer and/or orthopedic limitations that could compromise the execution of the study protocol (Figure 1).
The present study was approved by the Research Ethics Committee of the Federal University of Goiás (CAAE: 50717115.4.0000.5083), and by the Research Ethics Committee of the Clinical Hospital of the Federal University of Goiás (HC/UFG) (CAAE: 50717115.4.3001.5078) accordance with the requirement of resolution 466/12 of the National Health Council.
Experimental design
A design research was carried out adapted from an Open-label trial with no-treatment external concurrent control.
The women from TRT were assisted by physician during chemotherapy cycles, the administration of the drugs was performed every 21 days, composed of the drugs doxorubicin and epirubicin, belonging to the group of anthracycline and cyclophosphamide. The evaluations were performed between 20 and 21 days to minimize the acute effects of chemotherapy. The women in the CTR group performed only the evaluations and did not practice any type of physical exercise during the research period.
The volunteers from both groups (TRT and CTR) were submitted to the same tests. For the TRA group, the measurements occurred between the 2nd and 3rd chemotherapy cycle (QT1) and after the 4th cycle (QT4) (Figure 2).
For the CTR group, the same time interval adopted in the TRT group was used. All the visits during the evaluations period were previously and individually scheduled. At the first visit, all the volunteers signed the free and informed consent form, filled an anamnesis, and were exposed to: i) anthropometric measurements, ii) evaluation of muscle activation through electromyography, iii) functional capacity tests, and finally, they answered the quality of life questionnaires (SF-36)[24], Piper fatigue scale[25], state-trait-state anxiety inventory (STAI)[26], and this moment was called baseline. In the second visit, approximately 42 days after the baseline, the same measurements were performed.
Anthropometric measurements
Body mass was evaluated using an electronic/digital scale with accuracy of 50 grams (minimum weight 1,05kg and maximum 150 kg; Brand Lider®, model P-150M, (Araçatuba, Brazil). Height was measured by means of a professional stadiometer, with measurement field from 40 to 210 cm (Professional Sanny model ES2030; São Bernado do Campo, Brazil). With these two variables, the body mass index (BMI) was calculated, using the following equation: BMI = Body mass (kg) / Height (m²) [27].
Evaluation of muscle performance
Muscle activation and subjective perception of exertion
Miotec Medical Equipment Ltda® was used to evaluate muscle® activation. All electrode fixation procedures followed the recommendations of the International Society of Electrophysiology and Kinesiology (SIEC) and superficial electromyography for noninvasive muscle evaluation (SENIAM) [28]. The tetrapolar surface electrodes were placed in the rectus femoris (RF) and vastus medialis (VM) muscles according to SENIAM recommendations [28]. Additionally, the activation average adjusted by the activation peak in microvolts (uV) was reported.
Data were collected during the sit and stand test, a randomization was performed to choose the lower limb to fix the electrodes, in order to avoid differences in performance between dominant and non-dominant lower limbs.
The 6-20 Borg scale was used to assess the subjective perception of exertion [29], subdivided into perceptions of effort, as follows: 6 to 8 very, very light, 9 to 10 very light, 11 to 12 fairly light, 13 to 14 somewhat hard, 15 to 16 hard, 17 to 18 very hard and 19 to 20 very, very hard [30] The volunteers were asked about the perception of effort resulting from the performance of the sit and stand test.
Functional capacity and muscle strength
The muscle strength and functional capacity were performed in faculty of nutrition and health at the Federal University of Goiás. The evaluations were carried out in a room with non-slip floor, always in the morning with the same evaluator at all times. A training was previously performed by the evaluator in order to avoid vies. Were conducted these X tests:
1) Sit and stand test: In test were used, as well as the timed up and go (TUG) according to the protocol proposed by Rikli and Jones [31]. In the test of sit and stand the volunteers should sit and get up from a chair, thus completing 1 repetition.
The volunteers were verbally encouraged to complete the highest number of repetitions (score) for 30 seconds.
Statistical analysis
Parametric data are presented in mean ± standard deviation (SD), while nonparametric data are presented in median ± standard error. Data normality was tested using Shapiro-wilk test. The t-independent test was used to compare the characterization variables between groups at baseline. The two-way ANOVA (2x2) was used to compare the variance of the means between the moments. When necessary, the Bonferroni post-hoc test was used to find the differences.
Additionally, the Cohen's d effect of size [36] was calculated from the difference between groups to examine the magnitude of breast cancer treatment. The d values obtained were used to define the effect size as trivial (d <0.2), small (0.2 <d <0.5), medium (0.5 <d <0.8) and large (d> 0.8) [36].
All analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 20.0. The significance level of p≤0.05 was used.
3. Results
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
Two-way ANOVA demonstrated that muscle activation of VM in the TRT group was significantly lower compared to the CTR group at the time after (36.4 ± 2.8 uV e 46.0 ± 1.7 uV p = 0.038; d = 0.27). However, no significant differences were found in the electromyographic activity of RF in any moment (Figure 3).
Additionally, although no differences were found in the electromyographic activity of the RF, the TRT group showed lower percentage values (%) activation at all times compared to CTR (Table 2).
No significant differences were found in the subjective perception of exertion during sit and stand test between the TRT and CTR groups at baseline (10.0±2.6 au and 11.8±3.1 au, respectively) and post (11.0±2.8 au and 11.7±3.1 au, respectively), as well as between intragroup values.
However, compared to the TRT group, the CTR group performed better in the sit and stand test at baseline (17.6±3.7 reps e 29.1±4.2 reps, respectively, p<0.001; d = -0.42) and post-moment (18.5±2.6 reps e 28.5±2.4 reps, respectively, p<0.001; d = -0.42). However, no intragroup difference (Figure 4).
In addition, compared to the TRT group, the CTR group performed better in the TUG test at baseline (6.1±0.6 sec and 5.3±0.3 sec, respectively; p<0.001; d= 0.11) and post moment (TRT= 6.0±0.4 sec and CRT= 4.9 ± 0.5; p<0.001; d = 0.11), however, no intragroup differences were found (Figure 5).
The TRT group reduced the quality of life scores, specifically PF domain between baseline and post-moment [F(1;40) = 8.33; d=1.41; p = 0.006], as well as increased scores in the domain of RP [F(1;40) = 33.94; d= -0.73, p<0,001]. However, no significant changes were found in the other domains between moments and/or groups (Table 3).
From this perspective, the results related to fatigue show that a percentage part of the TRT group had moderate levels of fatigue in all domains in the baseline and post-moment, while only a small percentage of the CTR group showed similar levels only in the sensory and cognitive domains. Additionally, some volunteers from the TRT group presented severe levels of fatigue in the behavioral and affective domains (Table 4). However, the results related to A-trait and A-state anxiety were similar between groups and moments (Table 5).
4. Discussion
The aim of this study was to analyze and compare the effects of chemotherapy cycles with anthracyclines and cyclophosphamide on activation and MS, FC, effort perception, quality of life, fatigue and anxiety indicators. The results show significant differences between the groups in the muscle activation of VM, as well as in the MS evaluated by the sit and lift test and FC by the TUG test. In addition, the TRT group worsened some domains of quality of life, well as showed an increase in fatigue rates.
Despite the existence of some evidence on the possible side effects of chemotherapy treatment in MS parameters [37,38]. Our results are unprecedented in demonstrating changes in muscle activation, MS, FC and biopsychosocial parameters between chemotherapy cycles with anthracyclines and cyclophosphamide.
However, Klassen et al., [37] compared the strength levels of 255 women at different stages of chemotherapy treatment, the researchers demonstrated that women initiating chemotherapy had higher levels of MS compared to women after treatment, although no evaluations were performed between chemotherapy cycles, these findings corroborate our study by demonstrating that at some point in chemotherapy treatment there was a reduction in MS.
Interestingly, results contrary to ours were found by Marques et al., [23] when performing a comparison with women who were between the 2nd and 3rd cycle of chemotherapy with women considered healthy in MS measurements using the isokinetic device, the results did not show differences in torque measurements, as well as total work between groups. Possibly, the protocol used in isokinetics, in addition to the little functionality of the motor gesture (knee extension), may have contributed to these results.
In this sense, the differences in muscle performance found in our study in the sit and raise tests (MMII strength) and in the TUG test (FC) between the 2nd and 3rd, as well as after the 4th cycle, can be justified by the similarity of the tests with the day-to-day activities, a factor that can contribute to a better analysis of muscle performance linked to the aspect of CF when compared to isokinetic.
Additionally, the results found in the sit and raise test in the TRT group of the baseline (18,1 ± 3,5) and post moment (18,5 ± 2,6), surprisingly, are similar to the normative values of the elderly (10-22,6 repetitions) age group between 60-69 years[39], extoling the temperature of anthracycline and cyclophosphamide cycles, taking into account that the TRT group was of lower age (46,6 ± 9,6), with less exposure to the inherent factors of aging, which contribute to compromise muscle performance.
In addition, the lower results of the TRT group in the TUG test may suggest increased cardiovascular risk, Saraiva et al.,[40] found that better tug test performances, such as a decrease of 0.7 seconds in the performance of the test is associated with the increase in relative manual pressure strength, and this parameter is an important marker of mortality due to cardiovascular disease[41].
Although our study did not evaluate the relative handgrip strength, however, considering that anthracyclines and cyclophosphamide are also associated with the incidence of cardiovascular diseases[42], the difference found between the TRT and CRT groups in the TUG test probably demonstrates an indication of increased cardiovascular risk, and therefore, these findings could contribute to the use of the TUG test for this purpose or similar during chemotherapy.
Furthermore, the results of muscle activation, which is also related to muscle performance, showed a reduction in the muscle activation of the vastus medial in the TRT group after the 4th cycle, demonstrating that chemotherapy treatment with anthracyclines and cyclophosphamide may compromise the neuromuscular function of the knee extensor muscles.
Although no research has been found with analyses of muscle activation during chemotherapy treatment similar to ours, but only in other phases of treatment, such as surgical[43,44].
Our findings are important in the perspective of relating the reduction of muscle activation due to treatment, with low FC and/or MS Pio et al.,[45]demonstrated that morphological markers such as phenotype (type and proportion of fibers), architecture (muscle thickness and angle of pity) and/or muscle mechanisms (contraction and relaxation time), do not explain the reduction of FC, but neuromuscular parameters such as muscle activation, corroborating our study regarding VM activation.
However, no differences were found in the muscle activation of the rectus femoris, possibly the specificity of the sitting and lifting test may have compromised the results, since in this movement, the rectus femoris shows less request when compared to quadriceps muscles[46]. However, corroborating the research mentioned above, our VM results support that the analysis of quadriceps muscle activation may be an important assessment to be used during chemotherapy treatment in order to monitor neuromuscular factors sensitive to changes in FC.
Furthermore, the assessment of the subjective perception of exertion performed concomitantly with the sit-and-raise test, as well as EMG, did not show significant differences (classification of "relatively easy" at all times) despite the research conducted by Fernandez et al.,[47] correlate the subjective perception of exertion with central fatigue in patients diagnosed with cancer, our results suggest that chemotherapy cycles with anthracyclines and cyclophosphamide do not alter these parameters.
However, other manifestations of fatigue seem to worsen due to treatment, our findings showed that 30% of women after the 4th cycle of chemotherapy with anthracycline and cyclophosphamide presented severe levels of fatigue in the behavioral domain and 10% in the affective domain (Table 4). These results corroborate Jacobsen et al.,[48] who found that in addition to the individuals with fatigue at the beginning of treatment, they presented worsening of their condition at the end of chemotherapy.
Additionally, the percentage of women in the general mean domain of the TRT group with moderate levels of fatigue at baseline (40%), just as at the time post (50%), may be justified by several aggravating factors of cancer-related fatigue, such as increased concentration of pro-inflammatory cytosines, sleep disorders and increased cortisol[49,50].
Therefore, our findings are important in showing that fatigue problems are found after the 2nd cycle of chemotherapy, these findings may offer support for the implementation of resources aimed at controlling or reversing fatigue rates and other parameters such as anxiety.
Ferreira et al.,[51] analyzing 233 patients using an instrument different from ours to assess anxiety during treatment in different types of cancer, a prevalence of anxiety of 26.18% was found, although our study did not present "severe" levels of anxiety, between 50% and 70% of individuals in the TRT group demonstrated "moderate" levels of anxiety of the trait or state type, similar results were found in the CRT group (table 5). However, we emphasize that our findings correspond only to the period of cycles with anthracyclines and cyclophosphamide, since there is evidence suggesting problems in anxiety levels during complete treatment with association with physical inactivity, anxiolytic medication, breast swelling and/or advanced stage of the disease[52].
Despite this, Villar et al.,[52] demonstrated that anxiety levels decrease soon after the end of treatment, however, this study performed evaluations before the cycles and at the end of the complete treatment, as our results did not highlight differences between the groups, possibly anxiety is evident after anthracycline and cyclophosphamide cycles with possible decrease at the end of treatment.
In addition, Silva, Zandonade e Amorim,[53] interestingly, they found that individuals presenting "moderate" levels of anxiety similar to those of our study at the beginning of chemotherapy, develop a strategy to cope with the disease, which can negatively interfere in other variables such as quality of life, therefore, in the efficiency of treatment.
The TRT group of our study showed significant reductions in the FC domain of quality of life, in addition, the CRT group showed better baseline and post-moment scores. Although there are few studies evaluating quality of life during chemotherapy cycles in individuals with breast cancer, recent evidence presented by Klapheke et al.,[54] comparing 3 different types of cancer (cervical, ovary and uterus) demonstrated a decrease in quality of life domains similar to FC regardless of type of cancer, treatment or time of diagnosis.
However, this relationship seems to be influenced by some factors, recently Hassen et al.,[55] conducted a research in Ethiopia in order to associate several domains of quality of life with chemotherapy cycles and sociodemographic factors, curiously the domains less affected by chemotherapy cycles were those linked to physical characteristics/FC, while the most affected were linked to emotional aspects, corroborating other studies[56,57].
In this sense, the results contrary to those found in our study can be explained by the sociodemographic factors of the countries to which the research was conducted, for example, in Ethiopia, the role of women is to take care of the family, so when they get sick, suffer disorders in their usual functions and care more about the family. In addition, concerns about the future of children are common in this country and may contribute to extol emotional aspects, above physical [55], even similar results were found in poor regions of Brazil [58].
However, in addition to previous studies not performing evaluations between chemotherapy cycles, making it impossible to verify changes during treatment, they also did not verify the specific influence of aspects drugs such as anthracycline and cyclophosphamide drugs, as performed in our study, therefore, although our findings do not demonstrate changes in emotional aspects, the negative changes found in the FC domain are important to guide professionals on the use of resources in order to avoid or mitigate these changes, thus improving the quality of life of this population.
Additionally, despite the relevant findings of the present study, we can mention as a limitation the performance of evaluations only in a period of chemotherapy treatment, and it is not possible to extrapolate the results to other cycles with other drugs or different types of treatment.
5. Conclusions
Chemotherapy cycles with anthracyclines and cyclophosphamide reduced MS, FC and muscle activation performance, as well as altered some domains of fatigue and quality of life, however, no effects on anxiety were observed. These results are important because they provide information on the behavior of factors inherent to the prognosis of women with cancer due to early cycles of chemotherapy with anthracycline and cyclophosphamide, thus contributing to strategies being created aiming to improve the treatment of the disease.
Author Contributions
Conceptualization, Rafael Alves, Vitor Marques, Weder Silva and Carlos Vieira; Data curation, Rafael Alves and Fabrício Del Vecchio; Formal analysis, Rafael Alves, Vitor Marques, Weder Silva, Ruffo Junior, Anderson da Cruz, Fabrício Del Vecchio, Victor Rosa and Carlos Vieira; Methodology, Rafael Alves, Vitor Marques, Weder Silva, Ruffo Junior, Anderson da Cruz, Fabrício Del Vecchio and Carlos Vieira; Supervision, Carlos Vieira; Writing – original draft, Rafael Alves; Writing – review & editing, Vitor Marques, Weder Silva, Ruffo Junior, Anderson da Cruz, Fabrício Del Vecchio, Victor Rosa and Carlos Vieira.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and was approved by the Research Ethics Committee of the Federal University of Goiás (CAAE: 50717115.4.0000.5083), and by the Research Ethics Committee of the Hospital of Clinicals (HC/UFG) (CAAE: 50717115.4.3001.5078) accordance with the requirement of resolution 466/12 of the National Health Council.
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
TERM OF CONSENT STATEMENT
-
You are being invited to participate, as a volunteer, in the research "Effects of chemotherapy treatment on indicators of muscle strength, functional capacity and biopsychosocial aspects of women with breast cancer". The objective of this research is: To analyze the effects of chemotherapy cycles on muscle strength and activation, functional capacity, quality of life, fatigue and anxiety of women with breast cancer. The research is justified because most women in treatment have symptoms related to fatigue, quality of life and anxiety, and for many, even after treatment, these symptoms are still present. Reduced ability to work and decreased abilities to perform tasks of daily living are often accompanied by burnout and tiredness, conditions typical of cancer-related fatigue.This project will be developed in the laboratories of the Faculty of Nutrition and Health and in the University Hospital. It will take a few meetings to carry out all the necessary assessments. Each meeting will be scheduled in advance and will last close to 1 hour.At the first meeting you must sign the consent statement, as well as the following questionnaires, in random order, about quality of life, fatigue and anxiety. In addition, you will perform the functional capacity tests, and in one of them will be measured the muscle activity, through electromyography.The research will last approximately 2 months, containing two analyses on days and times to be combined with the volunteers. The times of your participation will be scheduled in advance respecting the intervals mentioned above, as well as your availability. You should be at the designated locations on the scheduled days and times and inform the researchers of any discomfort you may notice.The study does not involve expenses for you and / or companions, however if there are expenses with transportation and / or food the amounts will be reimbursed by the researchers. When necessary, the amounts will be reimbursed in the form of transportation vouchers and/or food stamps. All materials and equipment required for the tests will be provided by the researchers. This study should not be applied to people with the following conditions: those with heart disease, joint disease, respiratory problems or any contraindication to exercise.With the results of the study we will be able to obtain information about the effects of chemotherapy treatment on muscle responses, functional capacity, fatigue levels, quality of life and anxiety, defining its benefits or not the population studied, this knowledge will be useful to health professionals.The information obtained in this experiment may be used as scientific research data, and may be published and disseminated, being protected the identity of the participants. You can access your results through the responsible researcher.The responsible researcher will suspend the research immediately if he perceives any risk or damage to the participant's health, both those foreseen and those not foreseen in this term. In the unlikely physical damage resulting from participation in this study, treatment will be feasible at the nearest and most appropriate site.This project was approved by the Research Ethics Committee of the Federal University of Goiás.Your permission to participate in this research is voluntary. You will be free to deny it or to at any time give it up if you wish. You may refuse to answer any questions that cause you embarrassment. In case you agree to be part of the study, after having read and being enlightened about the above information, sign at the end of this phone, which is in two ways. One of them is yours and the other will be with the responsible researcher. All sheets must be initialed by the research volunteer or guardian and by the responsible researcher. In case of doubt or complaint, you can contact the researchers Rafael Ribeiro Alves, Vitor Alves Marques, Weder Silva, or by calling the responsible researcher Carlos Alexandre Vieira – (62) 98111-3242 or the Ethics and Research Committee of the Federal University of Goiás by phone (62) 3521-1215.Goiânia,_______de ____________ de _______________________________________________________Name / signature________________________________________________Researcher - Name / signature
Data Availability Statement
Data sharing not applicable. The data contains restrictions on sharing by researchers and cannot be made available to date.
Acknowledgments
We are grateful for the administrative support of the Federal University of Goiás and the Hospital das Clinicas, where the present research was conducted.
Conflicts of Interest
All authors declare that there is no conflict of interest.
References
- INCA. Instituto Nacional de Cancer José Alencar Gomes da Silva. Estimativa 2016: Incidência de Câncer No Brasil; 2016. doi:978-85-7318-283-5.
- Santana, silva, J. “Chorar podia emagrecer”:desejo e sacrificio na construção digital do corpo anoréxico feminino. Sociedade Brasiliera de Estudos Interdisciplinares da Comunicação 2017.
- Vieira, C.; Battaglini, C.; Ferreira-Junior, J.; Vieira, A.; Brito Vogt, M.; Freitas-Junior, R.; et al. Effects of Rest Interval on Strength Recovery in Breast Cancer Survivors. International Journal of Sports Medicine 2015, 36(07), 573–578. [CrossRef]
- Peart, O. Breast intervention and breast cancer treatment options. Radiologic technology 2015, 86(5), 535M-558M; quiz 559–562.
- Fisusi, F. A.; Akala, E. O. Drug Combinations in Breast Cancer Therapy. Pharmaceutical Nanotechnology 2019, 7(1), 3–23. [CrossRef]
- Kirjner, A.; Pinheiro, R. D. L. Interferência da Obesidade no Tratamento Quimioterápico em Mulheres com Câncer de Mama. Revista Brasileira de Cancerologia 2007, 53(3), 345–354.
- Osmani, K.; Vignes, S.; Aissi, M.; Wade, F.; Milani, P.; Lévy, B.; et al. Taxane-induced peripheral neuropathy has good long-term prognosis: A 1- to 13-year evaluation. J Neurol 2012, 249(1936–1943). [CrossRef]
- Artero, E. G.; Lee, D. C.; Ruiz, J. R.; Sui, X.; Ortega, F. B.; Church, T. S.; et al. A prospective study of muscular strength and all-cause mortality in men with hypertension. Journal of the American College of Cardiology 2011, 57(18), 1831–1837. [CrossRef]
- Prado, C. M. M.; Baracos, V. E.; McCargar, L. J.; Mourtzakis, M.; Mulder, K. E.; Reiman, T.; et al. Body composition as an independent determinant of 5-fluorouracil-based chemotherapy toxicity. Clinical Cancer Research 2007. [CrossRef]
- Jones, L. W.; Mourtzakis, M.; Peters, K. B.; Friedman, A. H.; West, M. J.; Mabe, S. K.; et al. Changes in Functional Performance Measures in Adults Undergoing Chemoradiation for Primary Malignant Glioma: A Feasibility Study. The Oncologist 2010. [CrossRef]
- Klassen, O.; Schmidt, M. E.; Ulrich, C. M.; Schneeweiss, A.; Potthoff, K.; Steindorf, K.; et al. Muscle strength in breast cancer patients receiving different treatment regimes. Journal of Cachexia, Sarcopenia and Muscle 2017. [CrossRef]
- Fayers, P. M.; Machin, D. Quality of Life: The Assessment, Analysis and Interpretation of Patient-Reported Outcomes: Second Edition; 2007. [CrossRef]
- Juniper, E. F.; Guyatt, G. H.; Epstein, R. S.; Ferrie, P. J.; Jaeschke, R.; Hiller, T. K. Evaluation of impairment of health related quality of life in asthma: Development of a questionnaire for use in clinical trials. Thorax 1992. [CrossRef]
- Bassarath, L. Conduct disorder: A biopsychosocial review. Canadian Journal of Psychiatry. 2001. [CrossRef]
- Suls, J.; Rothman, A. Evolution of the Biopsychosocial Model: Prospects and Challenges for Health Psychology. Health Psychology. 2004. [CrossRef]
- Caffo, O.; Amichetti, M.; Ferro, A.; Lucenti, A.; Valduga, F. Pain and quality of life after surgery for breast cancer. 2003, 39–48. [CrossRef]
- Galantino, M. Lou; Desai, K.; Greene, L.; Demichele, A.; Stricker, C. T.; Mao, J. J. Impact of yoga on functional outcomes in breast cancer survivors with aromatase inhibitor-associated arthralgias. Integrative Cancer Therapies 2012. [CrossRef]
- Donovan, K. A.; Jacobsen, P. B.; Andrykowski, M. A.; Winters, E. M.; Balducci, L.; Malik, U.; et al. Course of fatigue in women receiving chemotherapy and/or radiotherapy for early stage breast cancer. Journal of Pain and Symptom Management 2004. [CrossRef]
- Kilgour, R. D.; Vigano, A.; Trutschnigg, B.; Hornby, L. Cancer-related fatigue : The impact of skeletal muscle mass and strength in patients with advanced cancer. 2010, 177–185. [CrossRef]
- Taghian, N. R.; Miller, C. L.; Jammallo, L. S.; O’Toole, J.; Skolny, M. N. Lymphedema following breast cancer treatment and impact on quality of life: A review. Critical Reviews in Oncology/Hematology. 2014. [CrossRef]
- Montazeri, A. Health-related quality of life in breast cancer patients: A bibliographic review of the literature from 1974 to 2007. Journal of Experimental and Clinical Cancer Research. 2008. [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods 2007, 39(2), 175–191. [CrossRef]
- Marques, V. A.; Ferreira-Junior, J. B.; Lemos, T. V.; Moraes, R. F.; Junior, J. R. de S.; Alves, R. R.; et al. Effects of Chemotherapy Treatment on Muscle Strength, Quality of Life, Fatigue, and Anxiety in Women with Breast Cancer. International Journal of Environmental Research and Public Health 2020, 17(19), 7289. [CrossRef]
- Mosconi, P.; Cifani, S.; Crispino, S.; Fossati, R.; Apolone, G. The performance of SF-36 health survey in patients with laryngeal cancer. Head and Neck Cancer Italian Working Group. Head & neck 2000, 22(2), 175–182. [CrossRef]
- Bf, P.; Sl, D.; Mj, D.; Mc, W.; Re, S.; Sm, P. The revised Piper Fatigue Scale: Psychometric evaluation in women with breast cancer. Oncology nursing forum 1998, 25(4), 677–684.
- Biaggio, A. M. B.; Natalício, L.; Spielberger, C. D. Desenvolvimento da forma experimental em português do Inventário de Ansiedade Traço-Estado (IDATE) de Spielberger. Arquivos Brasileiros de Psicologia Aplicada 1977.
- (FAO), O. M. de la S. (OMS) y O. de las N. U. para la A. y la A.; (OMS), O. M. de la S.; (OMS), O. de las N. U. para la A. y la A. (FAO) / O. M. de la S. Segunda Conferencia Internacional sobre Nutrición Roma , 19-21 de noviembre de 2014 Documento final de la Conferencia : Declaración de Roma sobre la Nutrición. Orgaización Mundial de la Salud 2014.
- Hermens, H. J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. Journal of Electromyography and Kinesiology 2000, 10(5), 361–374. [CrossRef]
- Borg, G. Psychophysical scaling with applications in physical work and the perception of exertion. In Scandinavian Journal of Work, Environment and Health; 1990. [CrossRef]
- Borg, G. A. Psychophysical bases of perceived exertion. Medicine and science in sports and exercise 1982, 14(5), 377–381.
- Rikli, R. E.; Jones, C. J. Development and validation of a functional fitness test for community- residing older adults. Journal of Aging and Physical Activity 1999. [CrossRef]
- Swenson, K. K.; Nissen, M. J.; Henly, S. J.; Maybon, L.; Pupkes, J.; Zwicky, K.; et al. Identification of Tools to Measure Changes in Musculoskeletal Symptoms and Physical Functioning in Women With Breast Cancer Receiving Aromatase Inhibitors. Oncology Nursing Forum 2013, 40(6), 549–557. [CrossRef]
- Ciconelli, R. M.; Ferraz, M. B.; Santos, W.; Meinão, I.; Quaresma, M. R. Tradução para a língua portuguesa e validação do questionário genérico de avaliação de qualidade de vida SF-36 (Brasil SF-36). Revista Brasileira De Reumatologia. 1999, pp 143–150. doi:296502.
- Treanor, C.; Donnelly, M. A methodological review of the Short Form Health Survey 36 (SF-36) and its derivatives among breast cancer survivors. Quality of Life Research 2015, 24(2), 339–362. [CrossRef]
- Van Esch, L.; Roukema, J. A.; Van der Steeg, A. F. W.; De Vries, J. Trait anxiety predicts disease-specific health status in early-stage breast cancer patients. Quality of Life Research 2011, 20(6), 865–873. [CrossRef]
- Cohen, J. The concepts of power analysis. Statistical Power Analysis for the Behavioral Sciences. Lawrence Elbaum Associates 1988, 1–17.
- Klassen, O.; Schmidt, M. E.; Ulrich, C. M.; Schneeweiss, A.; Potthoff, K.; Steindorf, K.; et al. Muscle strength in breast cancer patients receiving different treatment regimes. Journal of cachexia, sarcopenia and muscle 2016. [CrossRef]
- Marques, V. A. Efeitos do tratamento quimioterápico sobre desempenho muscular de mulheres com câncer de mama., Universidade Federal de Goiás, 2017.
- Santos, E. C. D. O.; Galvão, L. L.; Tribess, S.; Meneguci, J.; Santos, R. G. dos; Silva, R. R.; et al. Valores normativos de força muscular em idosos. Arquivos de Ciências do Esporte 2019, 6(4). [CrossRef]
- Souza Saraiva, W.; Prestes, J.; Schwerz Funghetto, S.; Navalta, J. W.; Tibana, R. A.; da Cunha Nascimento, D. Relation Between Relative Handgrip Strength, Chronological Age and Physiological Age with Lower Functional Capacity in Older Women. Open Access Journal of Sports Medicine 2019, Volume 10, 185–190. [CrossRef]
- Lee, J. Associations Between Handgrip Strength and Disease-Specific Mortality Including Cancer, Cardiovascular, and Respiratory Diseases in Older Adults: A Meta-Analysis. Journal of Aging and Physical Activity 2019, 1–12. [CrossRef]
- McGowan, J. V.; Chung, R.; Maulik, A.; Piotrowska, I.; Walker, J. M.; Yellon, D. M. Anthracycline Chemotherapy and Cardiotoxicity. Cardiovascular Drugs and Therapy 2017. [CrossRef]
- Yang, E. J.; Kwon, Y. O. Changes in shoulder muscle activity pattern on surface electromyography after breast cancer surgery. Journal of Surgical Oncology 2018. [CrossRef]
- Perez, C.; Neves, L.; Vacari, A. luiza; Fonseca, M.; Guirro, R.; Guirro, E. Reduction in handgrip strength and electromyographic activity in women with breast cancer. Journal of Back and Musculoskeletal Rehabilitation 2017, 1(10:32), 1–6. [CrossRef]
- Pion, C. H.; Barbat-Artigas, S.; St-Jean-Pelletier, F.; Chevalier, S.; Gaudreau, P.; Gouspillou, G.; et al. Muscle strength and force development in high- and low-functioning elderly men: Influence of muscular and neural factors. Experimental Gerontology 2017, 96, 19–28. [CrossRef]
- Maeo, S.; Shan, X.; Otsuka, S.; Kanehisa, H.; Kawakami, Y. Single-joint eccentric knee extension training preferentially trains the rectus femoris within the quadriceps muscles. Translational Sports Medicine 2018. [CrossRef]
- Fernandez, C.; Firdous, S.; Jehangir, W.; Behm, B.; Mehta, Z.; Berger, A.; et al. Cancer-Related Fatigue: Perception of Effort or Task Failure? American Journal of Hospice and Palliative Medicine® 2019, 104990911984942. [CrossRef]
- Jacobsen, P. B.; Hann, D. M.; Azzarello, L. M.; Horton, J.; Balducci, L.; Lyman, G. H. Fatigue in women receiving adjuvant chemotherapy for breast cancer: Characteristics, course, and correlates. Journal of Pain and Symptom Management 1999. [CrossRef]
- Clevenger, L.; Schrepf, A.; Christensen, D.; DeGeest, K.; Bender, D.; Ahmed, A.; et al. Sleep disturbance, cytokines, and fatigue in women with ovarian cancer. Brain, Behavior, and Immunity. 2012. [CrossRef]
- Lutgendorf, S. K.; Weinrib, A. Z.; Penedo, F.; Russell, D.; DeGeest, K.; Costanzo, E. S.; et al. Interleukin-6, cortisol, and depressive symptoms in ovarian cancer patients. Journal of Clinical Oncology 2008. [CrossRef]
- Ferreira, A. S.; Bicalho, B. P.; Neves, L. F. G.; Menezes, M. T.; Silva, T. A.; Faier, T. A.; et al. Prevalência de Ansiedade e Depressão em Pacientes Oncológicos e Identificação de Variáveis Predisponentes. Revista Brasileira de Cancerologia 2019. [CrossRef]
- Villar, R. R.; Fernández, S. P.; Garea, C. C.; Pillado, M. T. S.; Barreiro, V. B.; Martín, C. G. Quality of life and anxiety in women with breast cancer before and after treatment. Revista latino-americana de enfermagem 2017. [CrossRef]
- Silva, A. V. da; Zandonade, E.; Amorim, M. H. C. Anxiety and coping in women with breast cancer in chemotherapy. Revista Latino-Americana de Enfermagem 2017. [CrossRef]
- Klapheke, A. K.; Keegan, T. H. M.; Ruskin, R.; Cress, R. D. Changes in health-related quality of life in older women after diagnosis with gynecologic cancer. Gynecologic Oncology 2019. [CrossRef]
- Hassen, A. M.; Taye, G.; Gizaw, M.; Hussien, F. M. Quality of life and associated factors among patients with breast cancer under chemotherapy at Tikur Anbessa specialized hospital, Addis Ababa, Ethiopia. PLoS ONE 2019. [CrossRef]
- Safaee, A.; Moghimi-Dehkordi, B.; Zeighami, B.; Tabatabaee, H. R.; Pourhoseingholi, M. A. Predictors of quality of life in breast cancer patients under chemotherapy. Indian Journal of Cancer 2008. [CrossRef]
- Dubashi, B.; Vidhubala, E.; Cyriac, S.; Sagar, T. Quality of life among young women with breast cancer: Study from a tertiary cancer institute in south India. Indian Journal of Cancer 2010. [CrossRef]
- Lôbo, S. A.; Fernandes, A. F. C.; Almeida, P. C. de; Carvalho, C. M. de L.; Sawada, N. O. Qualidade de vida em mulheres com neoplasias de mama em quimioterapia. Acta Paulista de Enfermagem 2014, 27(6), 554–559. [CrossRef]
Figure 1.
The flow chart of participants enrolled in the study.
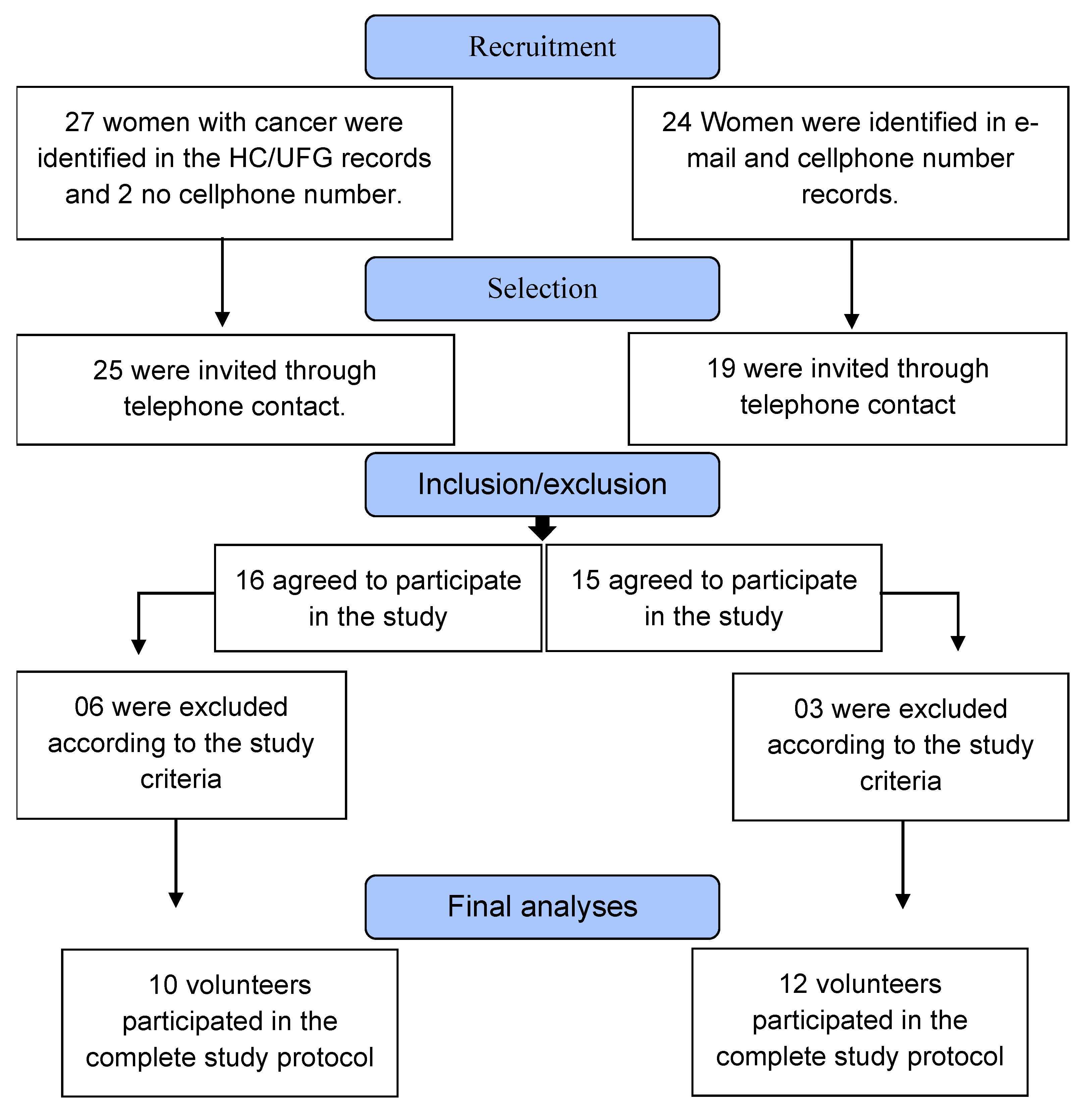
Figure 2.
Experimental design of the study; AC = anthracycline and cyclophosphamide.
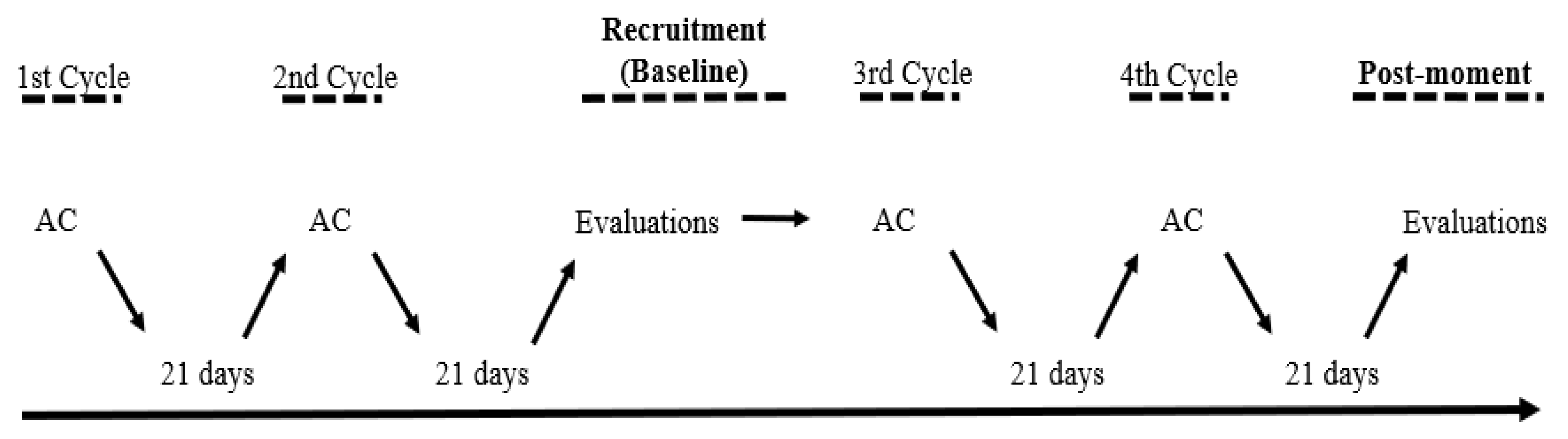
Figure 3.
Comparison of the mean EMG (%). a) = vastus medialis; b) = rectus femoris; TRT = treatment group; CTR = control group; Values are presented as median (lines) with interquartile range (boxes) ± range (minimum and maximum) and + indicates mean *p<0.05 compared to TRT.
Figure 3.
Comparison of the mean EMG (%). a) = vastus medialis; b) = rectus femoris; TRT = treatment group; CTR = control group; Values are presented as median (lines) with interquartile range (boxes) ± range (minimum and maximum) and + indicates mean *p<0.05 compared to TRT.
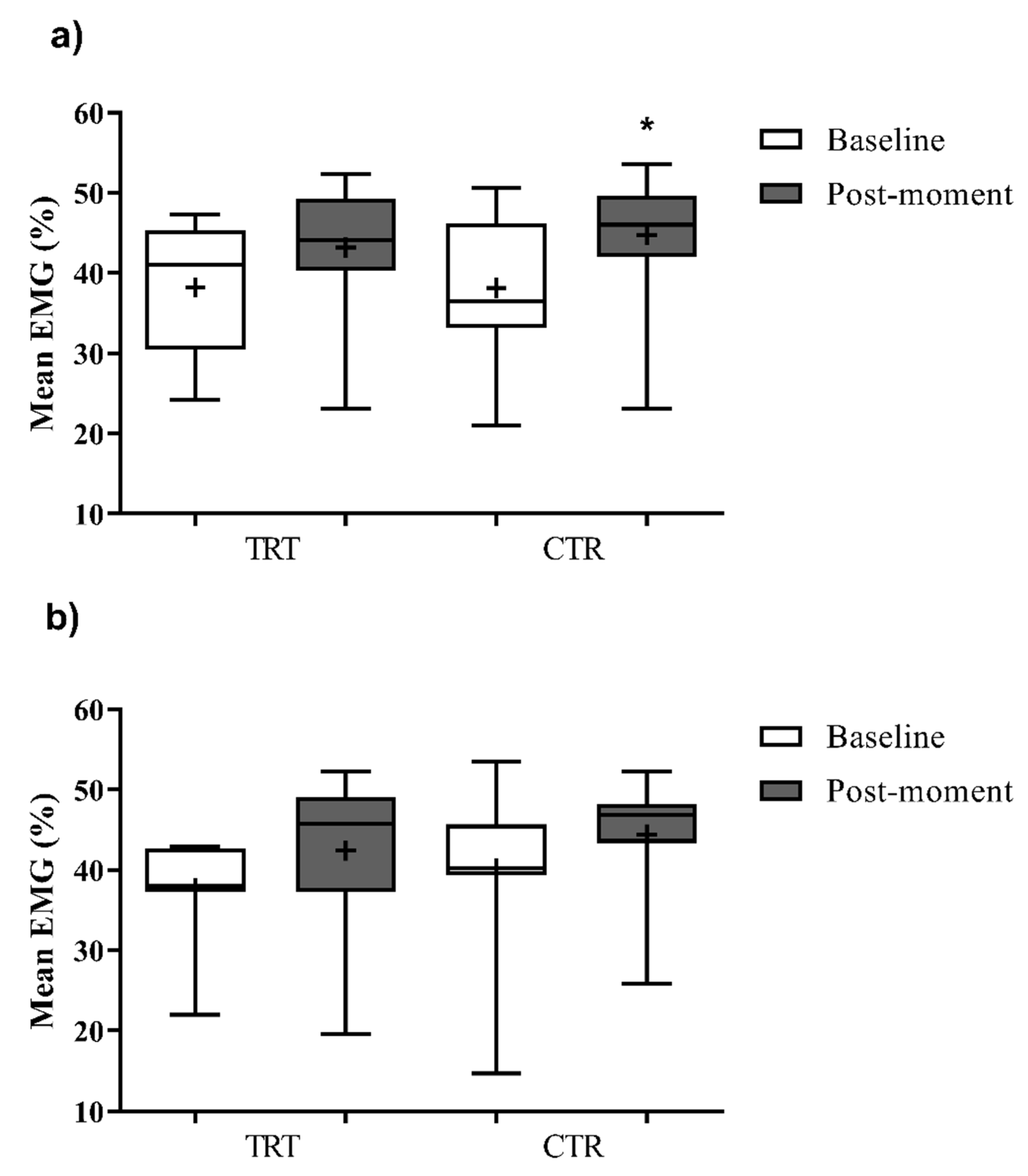
Figure 4.
Comparison of the sit and stand test.TRT= treatment group; CRT= control group; Values are presented as median (lines) with interquartile range (boxes) ± range (minimum and maximum) and + indicates mean *p<0,05 compared to TRT.
Figure 4.
Comparison of the sit and stand test.TRT= treatment group; CRT= control group; Values are presented as median (lines) with interquartile range (boxes) ± range (minimum and maximum) and + indicates mean *p<0,05 compared to TRT.
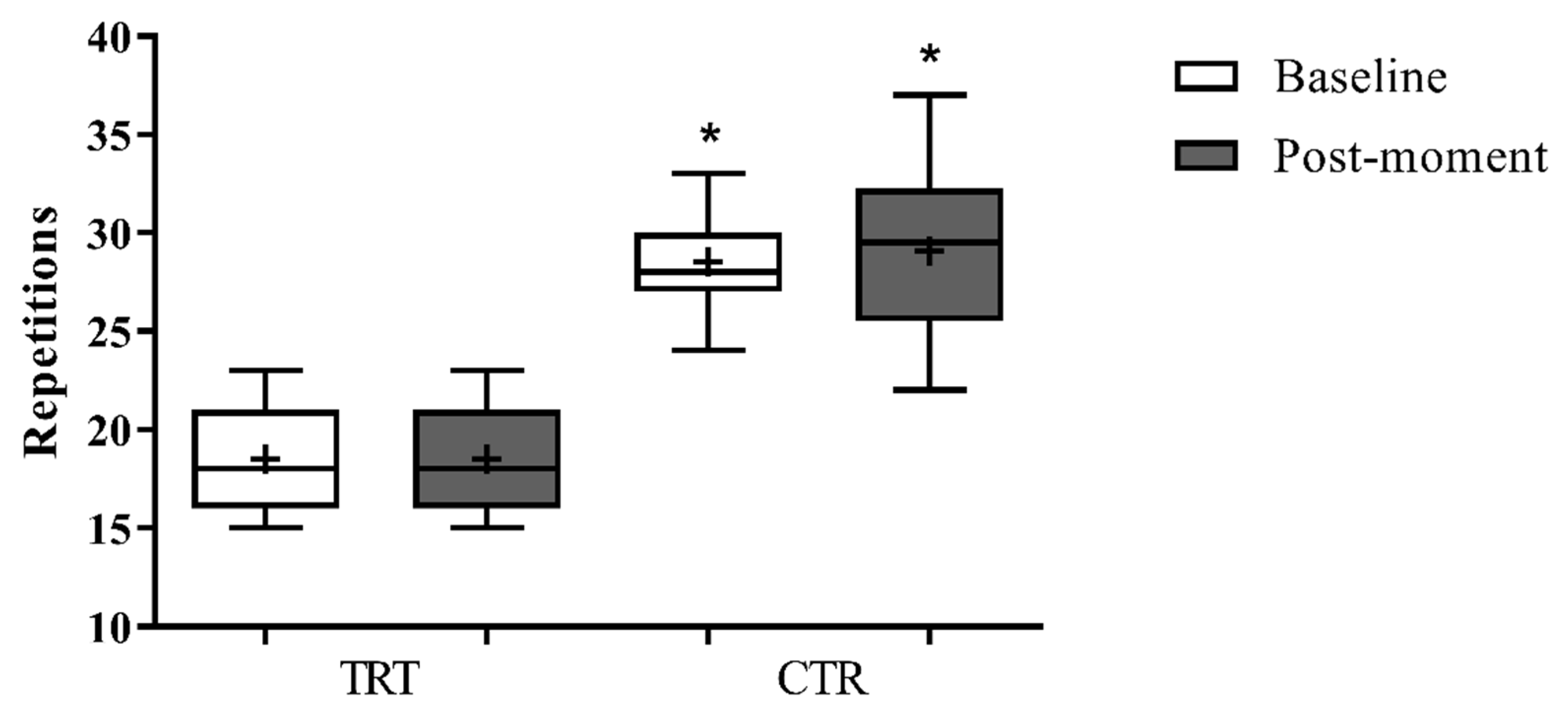
Figure 5.
Comparison of the test timed up and go. TRA = treatment group; CTR = control group; Values are presented as median (lines) with interquartile range (boxes) ± range (minimum and maximum) and + indicates mean *p<0,05 compared to TRT.
Figure 5.
Comparison of the test timed up and go. TRA = treatment group; CTR = control group; Values are presented as median (lines) with interquartile range (boxes) ± range (minimum and maximum) and + indicates mean *p<0,05 compared to TRT.
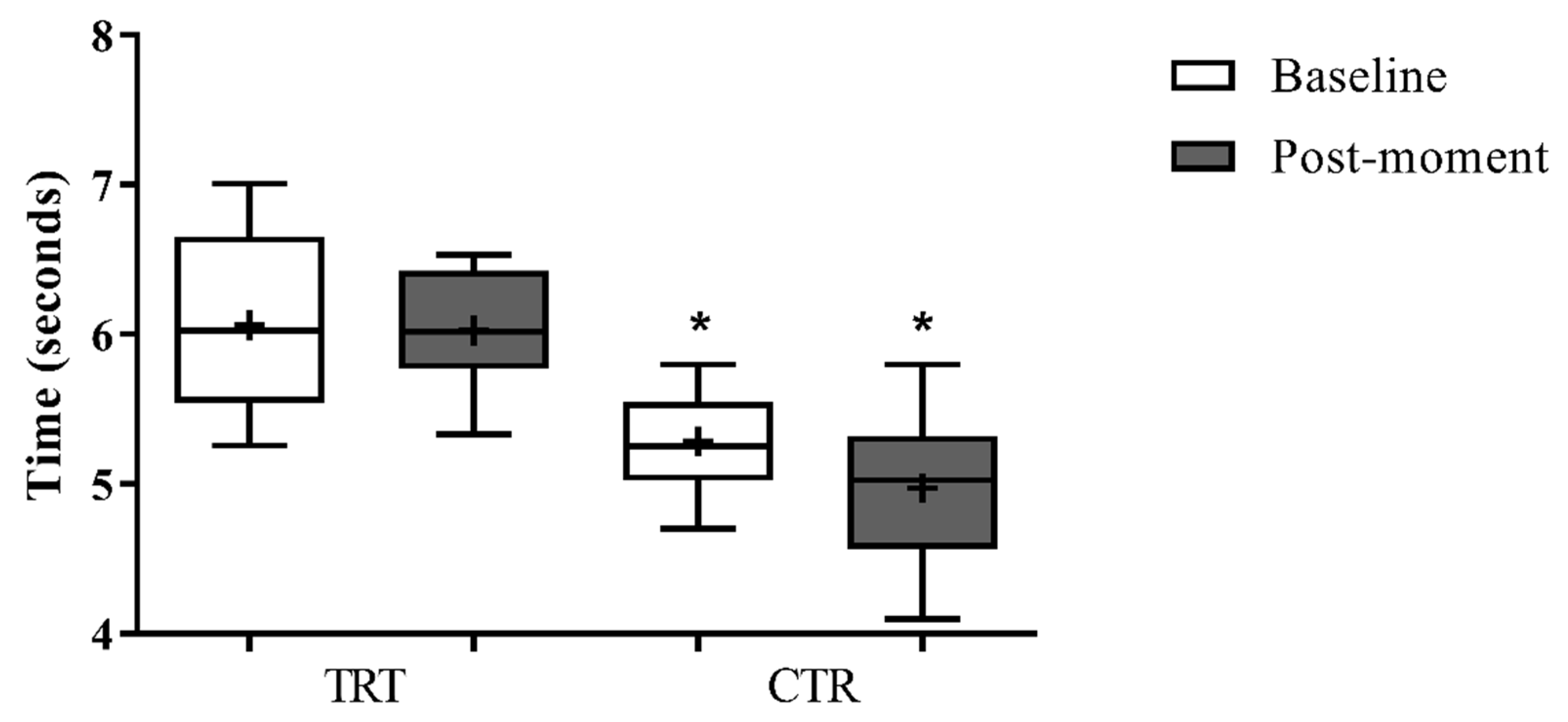

Table 1.
Characterization of volunteers.
| Groups* | Age (years) | Height (cm) | Body mass (kg) | BMI (kg/m2) | Treatment |
|---|---|---|---|---|---|
| TRT | 46.6 ± 9.6 | 1.54 ± 0.6 | 59.4 ± 5.9 | 24.9 ± 2.5 | AC |
| CTR | 51.6 ± 7.0 | 1.56 ± 0.3 | 63.3 ± 9.7 | 25.9 ± 3.7 | N/T |
TRT= Treatment group; CTR= Control group; BMI= Body mass index; AC = Anthracycline and cyclophosphamide clycles; N/T= No treatment. * t-Test showed (no) differences between groups at baseline for these variables (p<0,05).
Table 2.
Comparison EMG peak mean (uV).
| Group | Moment | ||||
|---|---|---|---|---|---|
| TRT | CTR | ||||
| Baseline | Post-moment | Baseline | Post-moment | ||
| RF | 37,7 ± 6,1 | 40,2 ± 10,2 | 42,4 ± 10,3 | 44,4 ± 7,8 | |
| VM | 38,2 ± 8,7 | 36,2 ± 13,7 | 42,4 ± 8,2 | 44,8 ± 7,8 | |
TRT = treatment group; CTR = control group; RF = rectus femoris; VM = vastus medialis.
Table 3.
Comparison Quality of life inter and intra groups.
| Variable | Group TRT (n=10) | Group CRT (n=12) |
Effect size |
p* |
|||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post-moment | p# | Baseline | Post-moment | p# | ||||
| Mean±DP | Mean±DP | Effect size | Mean±DP | Mean±DP | Group x Moment |
||||
| Quality of life | |||||||||
| Physical functioning | 77.0 ± 16.9 § | 58.7 ± 11.6 § | 0.01# | -1.26 | 88.1 ± 7.2 | 85.9 ± 10.2 | 0.65 | -0.25 | 0.03 * |
| Role physical | 12.5 ± 13.2 | 45.7 ± 45.5 | 0.02# | 0.99 | 81.4 ± 26.3 | 81.7 ± 26.3 | 0.98 | 0.01 | 0.07 |
| Bodily pain | 63.0 ± 33.7 | 57.9 ± 17.3 | 0.64 | -0.19 | 71.6 ± 24.7 | 73.5 ± 17.6 | 0.85 | 0.09 | 0.64 |
| General health | 59.8 ± 18.9 | 67.0 ± 20.1 | 0.31 | 0.37 | 72.0 ± 11.6 | 74.8 ± 12.1 | 0.66 | 0.24 | 0.65 |
| Vitality | 53.5 ± 17.1 | 64.0 ± 24.9 | 0.06 | 0.49 | 68.1 ± 13.0 | 69.0 ± 11.4 | 0.49 | 0.07 | 0.35 |
| Social functioning | 75.1 ± 22.8 | 68.3 ± 38.4 | 0.55 | -0.22 | 81.7 ± 21.6 | 85.6 ± 14.6 | 0.70 | 0.21 | 0.49 |
| Role emotional | 40.0 ± 41.0 | 44.6 ± 41.6 | 0.78 | 0.11 | 76.1 ± 35.1 | 74.3 ± 31.2 | 0.90 | -0.05 | 0.77 |
| Mental health | 66.8 ± 22.6 | 65.4 ± 23.3 | 0.86 | -0.06 | 73.0 ± 12.5 | 69.1 ± 13.0 | 0.62 | -0.31 | 0.83 |
| General status | 56.0 ± 16.3 | 59.2 ± 21.9 | 0.62 | 0.17 | 76.6 ± 9.9 | 76.7 ± 7.5 | 0.97 | 0.01 | 0.73 |
TRT= treatment group; CTR= control group; §= p < 0.05 compared to the same moment in the CRT; #= p < 0.05 compared to baseline; *=interaction between group and moment. .
Table 4.
Distribution (%) of fatigue domains baseline and post-moment.
| Domain |
Fatigue level |
Groups | |||
|---|---|---|---|---|---|
| TRT | CRT | ||||
| Baseline | Post-moment | Baseline | Post-moment | ||
| Behavioral | Absence | ------ | ------ | ------ | ------ |
| Middle | 60.0%(n=6) | 50.0%(n=5) | 100.0%(n=12) | 100.0%(n=12) | |
| Moderate | 40.0%(n=4) | 20.0%(n=2) | ------ | ------ | |
| Severe | ------ | 30.0%(n=3) | ------ | ------ | |
| Affective | Absence | ------ | ------ | ------ | ------ |
| Middle | 60.0%(n=6) | 50.0%(n=5) | 100.0%(n=12) | 100.0%(n=12) | |
| Moderate | 20.0%(n=2) | 40.0%(n=4) | ------ | ------ | |
| Severe | 20.0%(n=2) | 10.0%(n=1) | ------ | ------ | |
| Sensory | Absence | ------ | ------ | ------ | ------ |
| Middle | 70.0%(n=7) | 70.0%(n=7) | 100.0%(n=12) | 83.3%(n=7) | |
| Moderate | 30.0%(n=7) | 30.0% (n=7) | ------ | 16.7%(n=2) | |
| Severe | ------ | ------ | ------ | ------ | |
| Cognitive | Absence | ------ | ------ | ------ | ------ |
| Middle | 80.0%(n=8) | 80.0%(n=8) | 91.7%(n=11) | 100.0%(n=12) | |
| Moderate | 20.0%(n=2) | 20.0%(n=2) | 8.3%(n=1) | ------ | |
| Severe | ------ | ------ | ------ | ------ | |
| General mean | Absence | ------ | ------ | ------ | ------ |
| Middle | 60.0%(n=6) | 50.0%(n=5) | 100.0%(n=12) | 100.0%(n=12) | |
| Moderate | 40.0%(n=4) | 50.0%(n=5) | ------ | ------ | |
| Severe | ------ | ------ | ------ | ------ | |
* The data is shown as relative frequency (absolute frequency). TRT= treatment group; CRT= control group.
Table 5.
Distribution (%) of trait and state of anxiety baseline and post-moment.
| Domain |
Anxiety level |
Groups | |||
|---|---|---|---|---|---|
| TRT | CRT | ||||
| Baseline | Post-moment | Baseline | Post-moment | ||
| Trace | Low | 40.0%(n=4) | 30.0%(n=3) | 41.7%(n=5) | 33.3%(n=4) |
| Moderate | 60.0%(n=6) | 50.0%(n=5) | 58.3%(n=7) | 58.3%(n=7) | |
| High | ------ | 20.0%(n=2) | ------ | 8.3%(n=1) | |
| Severe | ------ | ------ | ------ | ------ | |
| State | Low | 40.0%(n=4) | 20.0%(n=2) | 33.3%(n=4) | 41.7%(n=5) |
| Moderate | 50.0%(n=5) | 70.0%(n=7) | 66.7%(n=8) | 50.0%(n=6) | |
| High | 10.0%(n=1) | 10.0%(n=1) | ------ | 8.3%(n=1) | |
| Severe | ------ | ------ | ------ | ------ | |
* The data is shown as relative frequency (absolute frequency).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



