
Submitted:
12 June 2023
Posted:
13 June 2023
You are already at the latest version
Abstract
The effects of statin use for primary prevention in reducing mortality among older adults in Asian populations are unknown. This study aimed to determine whether use of statins for primary prevention was associated with a decreased risk of all-cause mortality in a Japanese older adult population. A regional, population-based, longitudinal cohort study was conducted using the Shizuoka Kokuho Database (SKDB). Data were compared between the statin-treated group and a non-statin-treated (control) group using the inverse probability of treatment weighting (IPTW) method. In the SKDB cohort aged ≥65 years, new statin use was associated with a decreased risk of all-cause mortality (hazard ratio, 0.40; 95% confidence interval [CI], 0.33–0.48) after IPTW adjustment. The risk difference for mortality at 5 years in the statin-treated group (7.9%) compared with that in the control group (92.1%) was 0.05 (95% CI, 0.04–0.06), and the number needed to treat was 21.20 (95% CI, 18.10–24.70). In conclusion, statin use for primary prevention in older adults may reduce the risk of all-cause mortality in the population without atherosclerotic disease. Furthermore, statin use for primary prevention is feasible in patients aged 75 to <85 years and in patients with comorbidities such as diabetes, or dementia.
Keywords:
Health service needs
; statins
; mortality
; population
; primary prevention
; subgroups
1. Introduction
Cardiovascular and cerebrovascular diseases are the leading causes of death among older adults. In particular, atherosclerotic cardiovascular disease shows increasing incidence and prevalence with age and is a major cause of death, quality of life deterioration, and increased healthcare costs [1]. Atherosclerosis is caused by risk factors such as dyslipidemia, diabetes, hypertension, smoking, and lack of exercise. High low-density lipoprotein (LDL)-cholesterol level is an important risk factor for atherosclerosis development [2].
Statins are drugs that lower cholesterol levels in the blood and are widely used to treat dyslipidemia and familial hypercholesterolemia [3]. Decreases in LDL-cholesterol following statin therapy were shown to reduce the risk of atherosclerotic cardiovascular diseases such as myocardial infarction [4,5]. In populations with atherosclerotic disease, the effectiveness of statin therapy was independent of age [6].
Large-scale data analyses in US have shown that statin therapy for primary prevention effectively reduces mortality in late stage elderly and that the effectiveness of the therapy differs among subgroups [7]. However, the effects in Asian populations are unknown because almost all population are white and black in this study and this study is lack inspection data which affects survival such as anemia, hemoglobin A1c, and cholesterols level. The present study aimed to determine whether the use of statin for primary prevention is associated with a reduced risk of all-cause mortality in a population of older Japanese adults, as well as to identify any subgroups whom statin therapy may be particularly effective in reducing mortality.
2. Materials and Methods
2.1. Data source
The SKDB is a longitudinal dataset covering the whole of Shizuoka Prefecture in Japan and contains the receipt records for more than 2 million residents [8]. It has been used as a data source in several studies [9,10,11]. The SKDB contains information on injuries and diseases, medical receipts, nursing care levels, and health checkup results. In addition to basic information such as age and sex, it is possible to obtain information for disease names based on International Classification of Diseases 10th Revision (ICD-10) codes, prescription drug statuses, medical receipts, blood tests, and medical interview responses provided in health checkups [8]. The first date of an individual’s observation period in the SKDB was defined as their enrollment in the National Health Insurance or Late-Stage Senior Citizen’s Insurance or the start date of the SKDB (April 1, 2012), whichever was later. The end date of the observation period was defined as their withdrawal from the insurance or September 30, 2020, whichever was earlier.
2.2. Study design and population
The study was an in-database cohort study that used data from the SKDB and conducted analyses with a new-user design [12]. The date of the first statin prescription was defined as the index date for the statin-treated group and the date of the first medical checkup was defined as the index date for the non-statin-treated (control) group. Data for comorbidities and prescribed drugs were obtained retrospectively over the previous year. The statin-treated group had the closest health checkup information before the first prescription. Among the registered cases in the SKDB, patients who were aged ≥65 years at the index date and who received health checkup information were included in the study. Patients who were prescribed statins during the 1-year baseline period and patients with a history of myocardial infarction, cerebrovascular disease, or peripheral vascular disease were excluded.
Patients who were prescribed statins for >150 days within 1 year during the observation period were included in the statin-treated group. Patients who were prescribed statins for <150 days were excluded from the analysis population. An intention-to-treat approach was applied, assuming that exposure to statins remained constant during the follow-up period. Statins were reported to require approximately 1.5 to 3 years to affect all-cause mortality [13], and their prescription for people with very short life expectancy is not recommended [14]. Therefore, to exclude selection bias, patients with an observation period of <1 year were excluded from the analysis population, regardless of whether they were in the statin-treated group or the control group. A flowchart of the participant selection for the study is shown in Figure 1.
2.3. Outcome and confounder candidates
The primary outcome was the time to all-cause mortality recorded in the SKDB. The covariates examined were: age, sex, body mass index (BMI), smoking status, alcohol consumption, physical activity, health consciousness, estimated glomerular filtration rate (eGFR), hemoglobin A1c (HbA1c), LDL-cholesterol, cancer, liver disease, alcohol dependence, diabetes, hypertension, hemiplegia or other neurological disorders, chronic kidney disease, peptic ulcer disease, chronic obstructive pulmonary disease, depression, hyperlipidemia, sleep apnea and anemia. Additional variables specific to older adults included frailty, arthritis, dementia, fatigue, and gait abnormalities. The covariates for medications were: angiotensin-converting enzyme (ACE) inhibitors, alpha-blockers, angiotensin II receptor blockers, beta-blockers, calcium channel blockers, diuretics, and lipid-lowering agents other than statins. Current smoking, alcohol consumption, physical activity, and health consciousness were examined by referring to the responses in the questionnaires used in the annual health checkups. The ICD-10 disease codes are listed in Supplementary Table S1. All these covariates were used in the adjusted analysis as confounders.
2.4. Statistical analysis
Frequencies and percentages were calculated for continuous and categorical variables. Propensity scores [15] were estimated using logistic regression models with all confounder candidates predetermined by the literature and consultation with physicians to predict the probability that individuals would be assigned to the statin-treated group. Inverse probability of treatment weighting (IPTW) was employed to adjust for confounding factors related to statin use and outcomes, and the average treatment effect (ATE) of statin use was calculated [15]. A problem arises when the propensity score is exceptionally close to 1 or 0, because the weights for IPTW become extreme [16]. In the present study, we addressed this issue by trimming cases with stabilized IPTW and extreme propensity score weights [16]. Specifically, the analysis was limited to populations with propensity scores ranging from the bottom 2.5% of propensity scores in the statin group to the top 2.5% of propensity scores in the control group. The standardized mean difference (SMD) was used to compare the distribution of baseline characteristics between the two groups before and after adjustment. If the absolute value of the SMD was <10%, the balance between the treatment groups was considered sufficient [17].
Hazard ratios (HRs) and 95% confidence intervals (CIs) for mortality were estimated using a weighted Cox proportional hazards model. To measure the treatment effectiveness of statins, we calculated the risk difference for all-cause mortality at 5 years between the statin-treated group and the control group. The number needed to treat (NNT) was calculated from the reciprocal of the risk difference [17]. In addition, the bootstrap method with resampling performed 2000 times was employed to calculate the 95% CI of the risk difference.
In the secondary analysis, subgroup analyses were performed according to age (65 years to ≥85 years in 10-year increments), sex, smoking status, BMI, LDL-cholesterol, diabetes, dementia, and rheumatic diseases. For each subgroup, the ATE was estimated using the same covariates employed for the whole population analysis to adjust for confounding factors related to statin use and outcomes. Despite the possibility of an increasing type I error due to multiple comparisons in the statistical testing, adjustments for multiple testing were not performed, because of the exploratory aspect of the study.
As a sensitivity analysis to determine whether potential unmeasured confounders could affect the primary outcome, E-values were calculated to quantify the magnitude of unmeasured confounders that might negate the observed association between statin use and incidence of all-cause mortality [18,19]. This study did not use the imputation method for missing values. A value of p<0.05 (two-sided) was considered statistically significant. SAS version 9.4 (SAS Institute, Cary, NC) was used for statistical analyses.
2.5. Ethics
All information on the study participants was anonymized before analysis [8]. The study underwent ethical review and received approval from the Ethics Committee at Shizuoka Graduate University of Public Health. (SGUPH_2021_001_029).
3. Results
3.1. Demographics of participants
The analysis population was 210,052 patients, after excluding patients who met the exclusion criteria from the total SKDB cohort (Figure 1). The statin-treated group contained 16,691 individuals (7.9%) and had 530 deaths during the observation period with a median (maximum) of 6.06 (7.50) years. The control group contained 193,361 individuals (92.1%) and had 18,456 deaths. Before IPTW adjustment, the statin-treated group had a higher proportion of patients aged 65 to <75 years than the control group. The statin-treated group also had a higher proportion of women, a higher LDL-cholesterol level, higher prevalence of hypertension and hyperlipidemia, and higher prescription rates of angiotensin II receptor blockers, beta-blockers, calcium channel blockers, and lipid-lowering medications other than statins. After IPTW adjustment for patient background characteristics, the results showed a good balance between the groups for all covariates (Table 1).
3.2. Effectiveness of statin therapy for survival
The HR for mortality in the statin-treated group compared with that in the control group in the overall population before IPTW adjustment was 0.29 (95% CI, 0.26–0.31). After IPTW adjustment, there was a reduction in mortality in the statin-treated group (HR, 0.40; 95% CI, 0.33–0.48). The patient background characteristics in each group after IPTW adjustment are shown in Table 1. The risk difference for mortality at 5 years in the statin-treated group compared with that in the control group was 0.05 (95% CI, 0.04–0.06), and the NNT was 21.20 (95% CI, 18.10–24.70). A longer time to all-cause mortality was observed in the statin-treated group than in the control group. In the assessment for the magnitude of the effect of unmeasured confounders, the E-value was 4.44, with 3.59 as the lower value of the 95% CI.
3.3. Subgroup Analyses
The subgroup analyses showed significant effects of statin therapy on mortality for all subgroups, except BMI ≥30 kg/m2. When the NNT was used as the index, in patients aged 75 to <85 years, male sex, non-smoker status, BMI <18.5 kg/m2, and presence of diabetes, rheumatic diseases, or dementia tended to make statins more effective (Table 2). The risk differences for all-cause mortality at 5 years between the statin-treated group and the control group stratified by age, sex, current smoker status, BMI, LDL-cholesterol, diabetes, rheumatic disease, and dementia are shown in Figure 2. Detailed results can be found in Supplemental Table S2.
4. Discussion
In the present population aged ≥65 years without atherosclerotic cerebrovascular disease at baseline, administration of statins was associated with a lower risk of all-cause mortality. Furthermore, the subgroup analyses based on the NNT showed that the effectiveness of statin therapy was associated with age 75 to <85 years, male sex, non-smoker status, BMI <18.5 kg/m2, and presence of diabetes, or dementia.
Several randomized controlled trials showed reduced risks of death and cardiovascular events using statins on older adults [20,21,22,23,24]. Meta-analyses also indicated that statins were associated with a reduction in all-cause mortality compared with placebo [4,5,25,26]. Similarly, observational studies on the effectiveness of statins in older adults demonstrated reductions in the risks of all-cause mortality and cardiovascular events [7,27,28,29]. Based on the results of the present study and the previous concordant results, statin therapy as primary prevention for older adults may reduce the risk of all-cause mortality.
The United States Preventive Services Task Force stated that the current evidence was insufficient to assess the balance between the benefits and harms of initiating statin therapy for the primary prevention of cardiovascular events and death in adults aged ≥76 years [30]. In the present study, administration of statins was associated with a lower risk of all-cause mortality in patients aged 75 to <85 years (HR, 0.42; 95% CI, 0.31–0.57). And based on the measurements of the risk difference and NNT, the treatment effect was greater compared to patients aged 65 to <75 years (NNT: 44.64, 95% CI, 39.18-54.57 vs. NNT, 14.78, 95% CI, 11.75–22.39). These findings may reflect the multifaceted effects include the suppression of inflammation and decreasing oxidative stress of statin administration in patients aged 75 to <85 years and its main purpose of reducing cardiovascular events Pleiotropic Effects of Statins [31].
Obesity is suggested to be one of the characteristics of low response to statin therapy (<15% reduction in LDL) [32]. Moreover, obese patients (BMI > 30) showed atherosclerotic progression despite optimized statin therapy [33]. However, an observational study conducted in Korea showed that the effectiveness of statin therapy in reducing all-cause mortality was not dependent on the level of obesity [34]. The present analysis did not confirm any benefit of statin therapy in reducing all-cause mortality in the population with BMI ≥30 kg/m2 (p=0.41). The effectiveness of statin administration for primary prevention is unclear for people aged ≥65 years who have BMI ≥30 kg/m2. Meanwhile, the lowest NNT was calculated for people with BMI <18.5 kg/m2 (NNT, 12.02; 95% CI, 8.97–25.33). Therefore, the effectiveness of statin administration may be recommended for older adults without excessive overweight.
Statin treatment in older people with or without diabetes can be beneficial. A Spanish database study reported that statin therapy was not associated with a reduction in the risk of all-cause mortality in a population aged ≥75 years without diabetes mellitus, but did reduce the risk of all-cause mortality in patients with diabetes mellitus aged up to 85 years [27]. A US database study reported that the effects of statin therapy on the risks of all-cause and cardiovascular mortality were reduced in a population aged ≥75 years without a history of atherosclerotic cardiovascular disease, even for people without a history of diabetes mellitus [7]. The present study showed the efficacy of statin treatment for reducing all-cause mortality in adults aged ≥65 years with or without diabetes and not limited to healthy populations. However, patients with a history of atherosclerotic myocardial infarction or cerebrovascular disease were excluded. Meanwhile, when the NNT was used as the effect measure, the all-cause mortality reduction was greater in patients with diabetes than in patients without diabetes (NNT: 12.78, 95% CI, 9.66–20.96 vs. 22.14, 95% CI, 18.85–26.45; Table 2). Thus, the benefit of statin therapy for healthy older adults without diabetes can be relatively small. Nevertheless, statin therapy for older adults with or without diabetes may be beneficial.
Several observational studies demonstrated that statin therapy reduced all-cause mortality in patients with rheumatic diseases [40,41,42], consistent with the results of the present study. Statins were also found to reduce the risk of all-cause mortality in a population with dementia [43]. The present study supports the preventive effect of statins on patients with rheumatic disease and dementia those aged ≥65 years.
To create a cohort of older adults that reflects typical clinical practice, the present study did not exclude participants with comorbidities such as tumors, diabetes, dementia, rheumatic diseases, and renal diseases, which are risk factors for all-cause mortality. Moreover, statins are generally prescribed for the treatment of hyperlipidemia to prevent cardiovascular events [3], and other multifaceted effects include the suppression of inflammation and decreasing oxidative stress [31]. In the subgroup analyses in the present study, statin therapy reduced all-cause mortality particularly in patients with comorbidities such as diabetes, or dementia. These findings suggest that statins may have a multifaceted effect on the above diseases and patient conditions.
4.2. Strengths
The study used a large-scale dataset called the SKDB, which provided a sufficient sample size and ensured the inclusion of participants with various backgrounds. In general, it has been pointed out that only small numbers of older adults can be recruited for clinical trials that examine the effects of drugs, and therefore sufficient evidence may not be available [44]. For older adults, who are often excluded from clinical trials because of comorbidities such as tumors and dementia or a high risk of cardiovascular events, the present study helps to examine the effect of statin therapy based on data used in daily medical practice. Another strength of the study is the use of a new-user design to reduce confounding effects and immortal bias through a propensity score analysis. A further strength is that the study provides an easy-to-understand effect size for each subgroup by calculating not only the HR but also the risk difference and the NNT as indices for the effects of statin administration on the risk of all-cause mortality.
4.3. Limitations
First, unmeasured confounders may remain. Because the E-value for the HR was 4.44, we believe that the results of the study have some reliability in the absence of unmeasured confounding factors that affect both statin administration and all-cause mortality by more than 4.44-fold. Second, we used explanatory variables included in the SKDB, but could not examine essential variables such as family history, socioeconomic status, and non-statin medication status. In addition, we were unable to adjust for covariates that may lead patients to abandon prescriptions, such as a history of adverse drug reactions, including aspiration pneumonia and rhabdomyolysis. Third, the analysis was focused on populations with propensity scores ranging from the bottom 2.5% of propensity scores in the statin group to the top 2.5% of propensity scores in the control group. Therefore, the analysis may have been conducted on a population with a high likelihood of being prescribed statins. Fourth, there was the possibility of an increased type I error due to multiple testing. Therefore, the results of the subgroup analyses in the study should be interpreted in an exploratory manner.
Fifth, the definition of the statins administered included both standard statins and potent statins and did not distinguish between these types in the exposure groups. Furthermore, the exact amounts of statins prescribed were not recorded, making it impossible to evaluate the capacity-response relationship. It has been reported that approximately 1.5 to 3 years of treatment is required before an effect of statin therapy in reducing all-cause mortality can be expected [13]. Furthermore, randomized controlled trials in countries outside of Japan showed that discontinuation of statins in patients with a life expectancy of ≤1 year was safe, improved patient quality of life, and reduced medical costs [14]. In the present study, statin exposure was defined as >150 days of continuous administration within 1 year of the observation period. Sixth, the outcome in the study was all-cause mortality, but analysis by causes of death was not possible because the causes of death could not be determined based on the characteristics of the database used. Seventh, while the present study demonstrated the benefits of statin therapy, the risks of adverse events and associated medical costs were not analyzed. These further analyses need to be conducted to allow the decision-making for statin use to be based on risk-benefit considerations. Finally, since this population was exclusively Japanese, our results may not be generalizable to other ethnic groups.
5. Conclusions
In a population aged ≥65 years without atherosclerotic cerebrovascular disease at baseline, administration of statins was associated with a significantly lower risk of all-cause mortality. The subgroup analyses further showed that statin use was associated with a lower risk of all-cause mortality, particularly in patients aged 75 to <85 years and patients with comorbidities such as diabetes, or dementia.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
DF wrote the draft of the manuscript and performed the statistical analyses. DF and EN interpreted the data. DF, HK, AM, KS, HS and EN contributed to critical revision of the manuscript. All authors have read and approved the final version of the manuscript.
Funding
The Shizuoka Graduate University of Public Health conducts research projects on public health under contract with Shizuoka Prefecture, including the present study.
Institutional Review Board Statement
The study underwent ethical review and received approval from the Ethics Committee at Shizuoka Graduate University of Public Health. (SGUPH_2021_001_029).
Informed Consent Statement
Informed consent was waived due to the retrospective nature of the study.
Data Availability Statement
Based on a data use agreement with regional insurers in Shizuoka Prefecture, the authors cannot make the analyzed data accessible to readers.
Acknowledgments
For the drug code searches, a database from the Japan Pharmaceutical Information Center was used. The authors thank Alison Sherwin, PhD, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef]
- White, J.; Swerdlow, D.I.; Preiss, D.; Fairhurst-Hunter, Z.; Keating, B.J.; Asselbergs, F.W.; Sattar, N.; Humphries, S.E.; Hingorani, A.D.; Holmes, M.V. Association of Lipid Fractions With Risks for Coronary Artery Disease and Diabetes. JAMA Cardiol 2016, 1, 692–699. [Google Scholar] [CrossRef]
- Vrecer, M.; Turk, S.; Drinovec, J.; Mrhar, A. Use of Statins in Primary and Secondary Prevention of Coronary Heart Disease and Ischemic Stroke. Meta-Analysis of Randomized Trials. Int. J. Clin. Pharmacol. Ther. 2003, 41, 567–577. [Google Scholar] [CrossRef]
- Cholesterol Treatment Trialists’ (CTT) Collaborators; Mihaylova, B. ; Emberson, J.; Blackwell, L.; Keech, A.; Simes, J.; Barnes, E.H.; Voysey, M.; Gray, A.; Collins, R.; et al. The Effects of Lowering LDL Cholesterol with Statin Therapy in People at Low Risk of Vascular Disease: Meta-Analysis of Individual Data from 27 Randomised Trials. Lancet 2012, 380, 581–590. [Google Scholar]
- Gencer, B.; Marston, N.A.; Im, K.; Cannon, C.P.; Sever, P.; Keech, A.; Braunwald, E.; Giugliano, R.P.; Sabatine, M.S. Efficacy and Safety of Lowering LDL Cholesterol in Older Patients: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Lancet 2020, 396, 1637–1643. [Google Scholar] [CrossRef] [PubMed]
- Cholesterol Treatment Trialists’ Collaboration Efficacy and Safety of Statin Therapy in Older People: A Meta-Analysis of Individual Participant Data from 28 Randomised Controlled Trials. Lancet 2019, 393, 407–415. [CrossRef] [PubMed]
- Orkaby, A.R.; Driver, J.A.; Ho, Y.-L.; Lu, B.; Costa, L.; Honerlaw, J.; Galloway, A.; Vassy, J.L.; Forman, D.E.; Gaziano, J.M.; et al. Association of Statin Use With All-Cause and Cardiovascular Mortality in US Veterans 75 Years and Older. JAMA 2020, 324, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Nakatani, E.; Tabara, Y.; Sato, Y.; Tsuchiya, A.; Miyachi, Y. Data Resource Profile of Shizuoka Kokuho Database (SKDB) Using Integrated Health- and Care-Insurance Claims and Health Checkups: The Shizuoka Study. J. Epidemiol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Saito, K.; Sato, Y.; Nakatani, E.; Kaneda, H.; Yamamoto, S.; Miyachi, Y.; Itoh, H. Statin Exposure and Pancreatic Cancer Incidence: A Japanese Regional Population-Based Cohort Study, the Shizuoka Study. Cancer Prev. Res. 2021, 14, 863–872. [Google Scholar] [CrossRef] [PubMed]
- Shimada, K.; Yamamoto, H.; Nakatani, E.; Kumamaru, H.; Nishimura, S.; Ichihara, N.; Hirahara, N.; Mori, K.; Kotani, M.; Miyachi, Y.; et al. Real-World Evidence of the Incidence of and Risk Factors for Type 1 Diabetes Mellitus and Hypothyroidism as Immune-Related Adverse Events Associated With Programmed Cell Death-1 Inhibitors. Endocr. Pract. 2021, 27, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Kohsaka, S.; Kumamaru, H.; Nishimura, S.; Shoji, S.; Nakatani, E.; Ichihara, N.; Yamamoto, H.; Miyachi, Y.; Miyata, H. Incidence of Adverse Cardiovascular Events in Type 2 Diabetes Mellitus Patients after Initiation of Glucose-Lowering Agents: A Population-Based Community Study from the Shizuoka Kokuho Database. J. Diabetes Investig. 2021, 12, 1452–1461. [Google Scholar] [CrossRef]
- Ray, W.A. Evaluating Medication Effects Outside of Clinical Trials: New-User Designs. Am. J. Epidemiol. 2003, 158, 915–920. [Google Scholar] [CrossRef]
- Holmes, H.M.; Min, L.C.; Yee, M.; Varadhan, R.; Basran, J.; Dale, W.; Boyd, C.M. Rationalizing Prescribing for Older Patients with Multimorbidity: Considering Time to Benefit. Drugs Aging 2013, 30, 655–666. [Google Scholar] [CrossRef]
- Kutner, J.S.; Blatchford, P.J.; Taylor, D.H., Jr; Ritchie, C.S.; Bull, J.H.; Fairclough, D.L.; Hanson, L.C.; LeBlanc, T.W.; Samsa, G.P.; Wolf, S.; et al. Safety and Benefit of Discontinuing Statin Therapy in the Setting of Advanced, Life-Limiting Illness: A Randomized Clinical Trial. JAMA Intern. Med. 2015, 175, 691–700. [Google Scholar] [CrossRef]
- Rosenbaum, P.R.; Rubin, D.B. The Central Role of the Propensity Score in Observational Studies for Causal Effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Austin, P.C.; Stuart, E.A. Moving towards Best Practice When Using Inverse Probability of Treatment Weighting (IPTW) Using the Propensity Score to Estimate Causal Treatment Effects in Observational Studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef]
- Austin, P.C. Absolute Risk Reductions and Numbers Needed to Treat Can Be Obtained from Adjusted Survival Models for Time-to-Event Outcomes. J. Clin. Epidemiol. 2010, 63, 46–55. [Google Scholar] [CrossRef]
- VanderWeele, T.J.; Ding, P. Sensitivity Analysis in Observational Research: Introducing the E-Value. Ann. Intern. Med. 2017, 167, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Mathur, M.B.; Ding, P.; Riddell, C.A.; VanderWeele, T.J. Web Site and R Package for Computing E-Values. Epidemiology 2018, 29, e45–e47. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, J.; Blauw, G.J.; Murphy, M.B.; Bollen, E.L.E.M.; Buckley, B.M.; Cobbe, S.M.; Ford, I.; Gaw, A.; Hyland, M.; Jukema, J.W.; et al. Pravastatin in Elderly Individuals at Risk of Vascular Disease (PROSPER): A Randomised Controlled Trial. Lancet 2002, 360, 1623–1630. [Google Scholar] [CrossRef] [PubMed]
- Everett, B.M.; Glynn, R.J.; MacFadyen, J.G.; Ridker, P.M. Rosuvastatin in the Prevention of Stroke among Men and Women with Elevated Levels of C-Reactive Protein: Justification for the Use of Statins in Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER). Circulation 2010, 121, 143–150. [Google Scholar] [CrossRef]
- Downs, J.R.; Clearfield, M.; Weis, S.; Whitney, E.; Shapiro, D.R.; Beere, P.A.; Langendorfer, A.; Stein, E.A.; Kruyer, W.; Gotto, A.M. , Jr Primary Prevention of Acute Coronary Events with Lovastatin in Men and Women with Average Cholesterol Levels: Results of AFCAPS/TexCAPS. Air Force/Texas Coronary Atherosclerosis Prevention Study. JAMA 1998, 279, 1615–1622. [Google Scholar] [CrossRef]
- Nakamura, H.; Arakawa, K.; Itakura, H.; Kitabatake, A.; Goto, Y.; Toyota, T.; Nakaya, N.; Nishimoto, S.; Muranaka, M.; Yamamoto, A.; et al. Primary Prevention of Cardiovascular Disease with Pravastatin in Japan (MEGA Study): A Prospective Randomised Controlled Trial. Lancet 2006, 368, 1155–1163. [Google Scholar] [CrossRef]
- Heart Protection Study Collaborative Group MRC/BHF Heart Protection Study of Cholesterol Lowering with Simvastatin in 20,536 High-Risk Individuals: A Randomised Placebo-Controlled Trial. Lancet 2002, 360, 7–22. [CrossRef] [PubMed]
- Roberts, C.G.P.; Guallar, E.; Rodriguez, A. Efficacy and Safety of Statin Monotherapy in Older Adults: A Meta-Analysis. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 879–887. [Google Scholar] [CrossRef]
- Cholesterol Treatment Trialists’ (CTT) Collaboration; Fulcher, J. ; O’Connell, R.; Voysey, M.; Emberson, J.; Blackwell, L.; Mihaylova, B.; Simes, J.; Collins, R.; Kirby, A.; et al. Efficacy and Safety of LDL-Lowering Therapy among Men and Women: Meta-Analysis of Individual Data from 174,000 Participants in 27 Randomised Trials. Lancet 2015, 385, 1397–1405. [Google Scholar]
- Ramos, R.; Comas-Cufí, M.; Martí-Lluch, R.; Balló, E.; Ponjoan, A.; Alves-Cabratosa, L.; Blanch, J.; Marrugat, J.; Elosua, R.; Grau, M.; et al. Statins for Primary Prevention of Cardiovascular Events and Mortality in Old and Very Old Adults with and without Type 2 Diabetes: Retrospective Cohort Study. BMJ 2018, 362, k3359. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Lee, C.J.; Shim, C.-Y.; Kim, J.-S.; Kim, B.-K.; Park, S.; Chang, H.-J.; Hong, G.-R.; Ko, Y.-G.; Kang, S.-M.; et al. Statin and Clinical Outcomes of Primary Prevention in Individuals Aged >75 Years: The SCOPE-75 Study. Atherosclerosis 2019, 284, 31–36. [Google Scholar] [CrossRef]
- Jun, J.E.; Cho, I.-J.; Han, K.; Jeong, I.-K.; Ahn, K.J.; Chung, H.Y.; Hwang, Y.-C. Statins for Primary Prevention in Adults Aged 75 Years and Older: A Nationwide Population-Based Case-Control Study. Atherosclerosis 2019, 283, 28–34. [Google Scholar] [CrossRef]
- Stone, N.J.; Greenland, P.; Grundy, S.M. Statin Usage in Primary Prevention-Comparing the USPSTF Recommendations With the AHA/ACC/Multisociety Guidelines. JAMA Cardiol 2022. [Google Scholar] [CrossRef] [PubMed]
- Liao, J.K.; Laufs, U. Pleiotropic Effects of Statins. Annu. Rev. Pharmacol. Toxicol. 2005, 45, 89–118. [Google Scholar] [CrossRef]
- Kataoka, Y.; St John, J.; Wolski, K.; Uno, K.; Puri, R.; Tuzcu, E.M.; Nissen, S.E.; Nicholls, S.J. Atheroma Progression in Hyporesponders to Statin Therapy. Arterioscler. Thromb. Vasc. Biol. 2015, 35, 990–995. [Google Scholar] [CrossRef] [PubMed]
- Sandfort, V.; Lai, S.; Ahlman, M.A.; Mallek, M.; Liu, S.; Sibley, C.T.; Turkbey, E.B.; Lima, J.A.C.; Bluemke, D.A. Obesity Is Associated With Progression of Atherosclerosis During Statin Treatment. J. Am. Heart Assoc. 2016, 5. [Google Scholar] [CrossRef] [PubMed]
- Won, K.-B.; Hur, S.-H.; Nam, C.-W.; Ann, S.H.; Park, G.-M.; Lee, S.-G.; Kim, H.-E.; Cho, Y.-K.; Yoon, H.-J.; Park, H.-S.; et al. Evaluation of the Impact of Statin Therapy on the Obesity Paradox in Patients with Acute Myocardial Infarction: A Propensity Score Matching Analysis from the Korea Acute Myocardial Infarction Registry. Medicine 2017, 96, e7180. [Google Scholar] [CrossRef] [PubMed]
- Winter, J.E.; MacInnis, R.J.; Wattanapenpaiboon, N.; Nowson, C.A. BMI and All-Cause Mortality in Older Adults: A Meta-Analysis. Am. J. Clin. Nutr. 2014, 99, 875–890. [Google Scholar] [CrossRef] [PubMed]
- Donini, L.M.; Savina, C.; Gennaro, E.; De Felice, M.R.; Rosano, A.; Pandolfo, M.M.; Del Balzo, V.; Cannella, C.; Ritz, P.; Chumlea, W.C. A Systematic Review of the Literature Concerning the Relationship between Obesity and Mortality in the Elderly. J. Nutr. Health Aging 2012, 16, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Fontaine, K.R.; McCubrey, R.; Mehta, T.; Pajewski, N.M.; Keith, S.W.; Bangalore, S.S.; Crespo, C.J.; Allison, D.B. Body Mass Index and Mortality Rate among Hispanic Adults: A Pooled Analysis of Multiple Epidemiologic Data Sets. Int. J. Obes. 2012, 36, 1121–1126. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Association of All-Cause Mortality with Overweight and Obesity Using Standard Body Mass Index Categories: A Systematic Review and Meta-Analysis. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef]
- Yamazaki, K.; Suzuki, E.; Yorifuji, T.; Tsuda, T.; Ohta, T.; Ishikawa-Takata, K.; Doi, H. Is There an Obesity Paradox in the Japanese Elderly Population? A Community-Based Cohort Study of 13 280 Men and Women. Geriatr. Gerontol. Int. 2017, 17, 1257–1264. [Google Scholar] [CrossRef]
- Ozen, G.; Dell’Aniello, S.; Pedro, S.; Michaud, K.; Suissa, S. Reduction of Cardiovascular Disease and Mortality versus Risk of New Onset Diabetes with Statin Use in Patients with Rheumatoid Arthritis. Arthritis Care Res. 2022. [Google Scholar] [CrossRef]
- Chhibber, A.; Hansen, S.; Biskupiak, J. Statin Use and Mortality in Rheumatoid Arthritis: An Incident User Cohort Study. J Manag Care Spec Pharm 2021, 27, 296–305. [Google Scholar] [CrossRef]
- Schoenfeld, S.R.; Lu, L.; Rai, S.K.; Seeger, J.D.; Zhang, Y.; Choi, H.K. Statin Use and Mortality in Rheumatoid Arthritis: A General Population-Based Cohort Study. Ann. Rheum. Dis. 2016, 75, 1315–1320. [Google Scholar] [CrossRef] [PubMed]
- Petek, B.; Xu, H.; Villa-Lopez, M.; Winblad, B.; Kramberger, M.G.; Eriksdotter, M.; Garcia-Ptacek, S. Statins, Risk of Death and Ischemic Stroke in Patients with Dementia: A Registry-Based Observational Cohort Study. Curr. Alzheimer Res. 2020, 17, 881–892. [Google Scholar] [CrossRef] [PubMed]
- Cherubini, A.; Oristrell, J.; Pla, X.; Ruggiero, C.; Ferretti, R.; Diestre, G.; Clarfield, A.M.; Crome, P.; Hertogh, C.; Lesauskaite, V.; et al. The Persistent Exclusion of Older Patients from Ongoing Clinical Trials Regarding Heart Failure. Arch. Intern. Med. 2011, 171, 550–556. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
After patients who met the exclusion criteria were excluded from the total SKDB cohort, the analysis population was 210,052 patients. The number of patients in the statin-treated group was 16,691 (7.9%), and there were 530 deaths. The number of patients in the non-statin-treated (control) group was 193,361 (92.1%), and there were 18,456 deaths. SKDB, Shizuoka Kokuho database.
Figure 1.
After patients who met the exclusion criteria were excluded from the total SKDB cohort, the analysis population was 210,052 patients. The number of patients in the statin-treated group was 16,691 (7.9%), and there were 530 deaths. The number of patients in the non-statin-treated (control) group was 193,361 (92.1%), and there were 18,456 deaths. SKDB, Shizuoka Kokuho database.
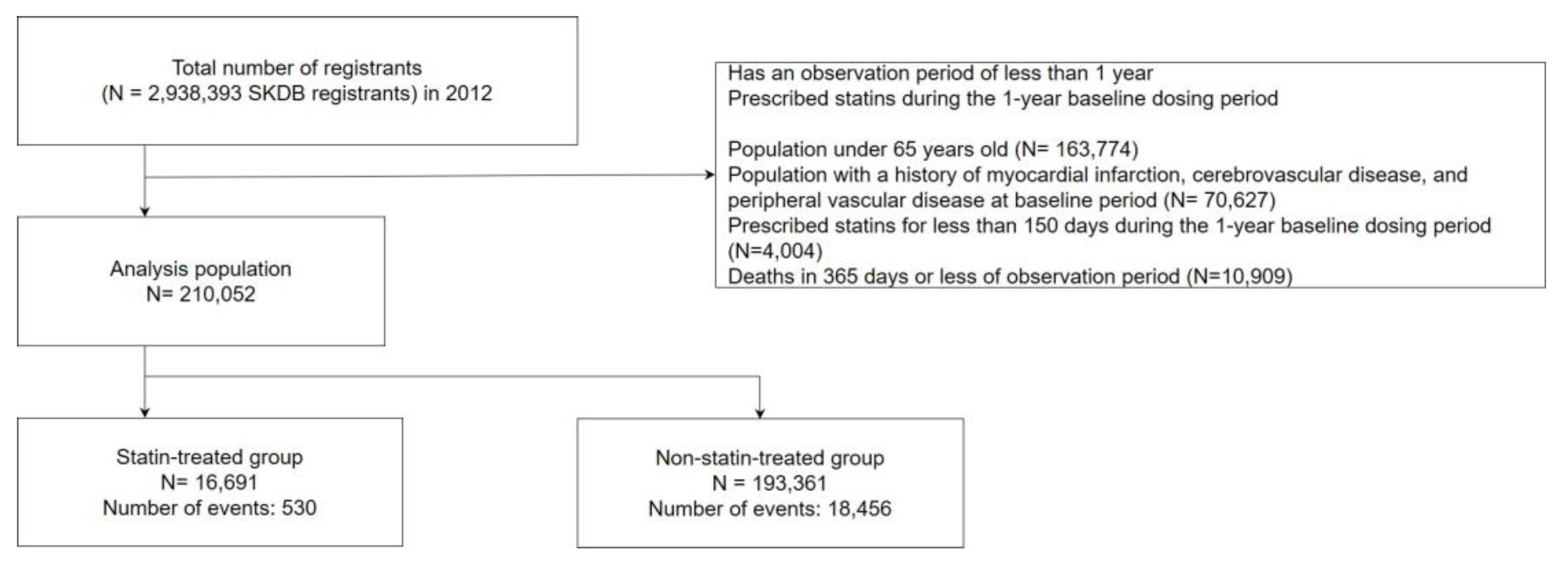
Figure 2.
The forest plots show the risk differences for all-cause mortality between the statin-treated group and the control group for each subgroup at 5 years of follow-up. RD, risk difference; CI, confidence interval; BMI: body mass index; LDL: low-density lipoprotein.
Figure 2.
The forest plots show the risk differences for all-cause mortality between the statin-treated group and the control group for each subgroup at 5 years of follow-up. RD, risk difference; CI, confidence interval; BMI: body mass index; LDL: low-density lipoprotein.
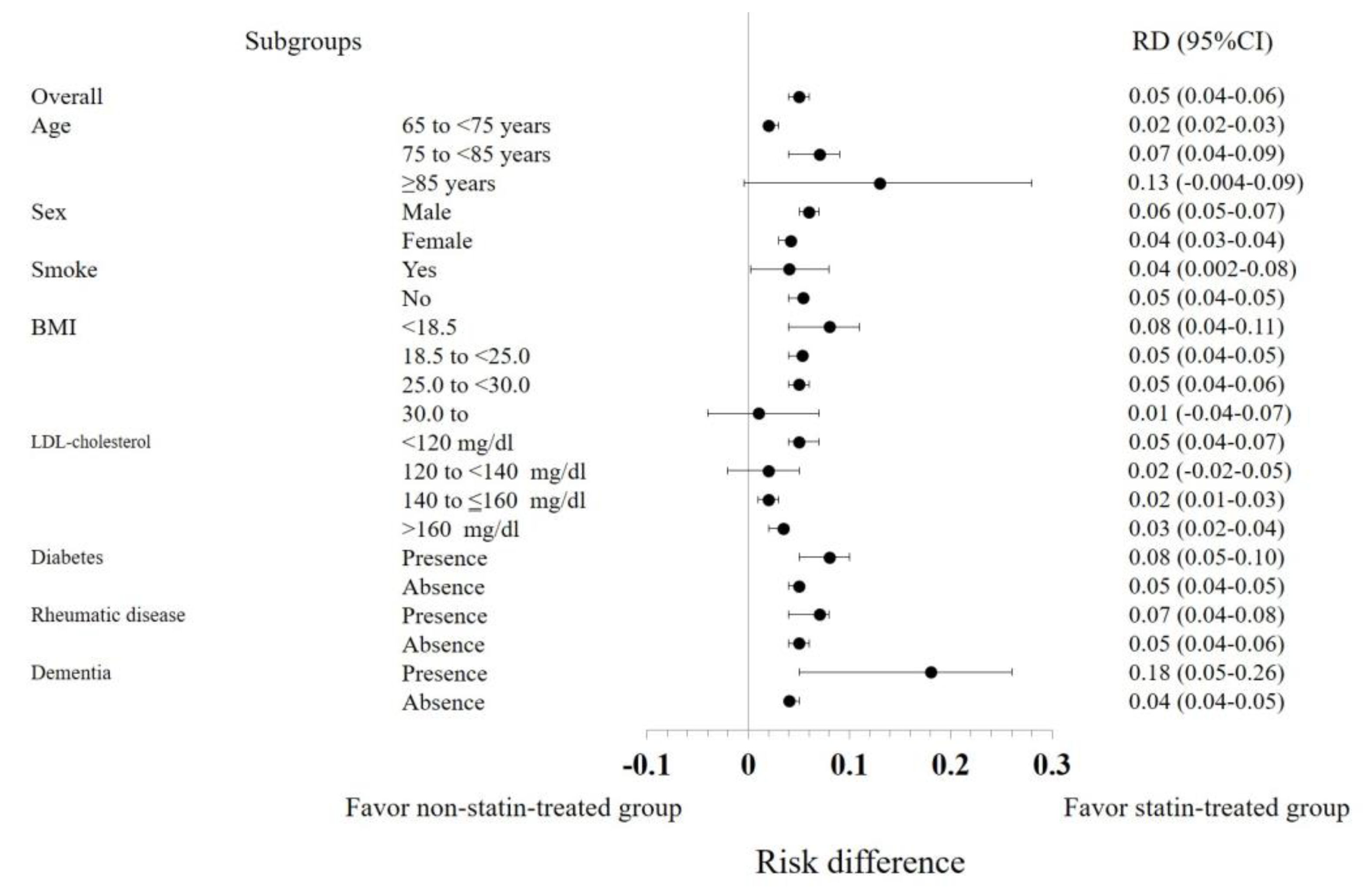

Table 1.
Demographics of participants, before and after adjustment by the inverse probability of treatment-weighted (IPTW) method.
Table 1.
Demographics of participants, before and after adjustment by the inverse probability of treatment-weighted (IPTW) method.
| Variable | Category | Before adjustment | After adjustment | ||||
|---|---|---|---|---|---|---|---|
| statin-exposure | statin-non-exposure | SMD | statin-exposure | statin-non-exposure | SMD | ||
| (n=16,691) | (n=193,361) | (n=2,753) | (n=31,466) | ||||
| Age | 65-<75 | 12637 (75.7) | 121013 (62.6) | 0.33 | 1826.95 (66.4) | 20965.04 (66.6) | 0.04 |
| 75-<85 | 3667 (22.0) | 57563 (29.8) | 0.33 | 740.26 (26.9) | 8484.53 (27.0) | 0.04 | |
| ≥85 | 387 (2.3) | 14785 (7.6) | 0.33 | 185.83 (6.8) | 2016.64 (6.4) | 0.04 | |
| Sex | Men | 5884 (35.3) | 94368 (48.8) | -0.28 | 1176.54 (42.7) | 13756.10 (43.7) | -0.02 |
| Current smoker | Yes | 1441 (8.6) | 19694 (10.2) | -0.05 | 223.79 (8.1) | 2912.78 (9.3) | -0.04 |
| BMI | <18.5 | 1114 (6.7) | 21748 (11.3) | 0.15 | 216.59 (7.9) | 2602.25 (8.3) | 0.06 |
| 18.5 to <25.0 | 12044 (72.3) | 136537 (70.8) | 0.15 | 1902.15 (69.1) | 21933.86 (69.7) | 0.06 | |
| 25.0 to <30.0 | 3216 (19.3) | 31488 (16.3) | 0.15 | 560.53 (20.4) | 6182.11 (19.6) | 0.06 | |
| 30.0 to | 292 (1.8) | 3137 (1.6) | 0.15 | 73.77 (2.7) | 747.99 (2.4) | 0.06 | |
| Missing number | 25 | 451 | 0.15 | 0.00 | 0.00 | 0.00 | |
| Alcohol intake | <40 g/day | 13794 (96.0) | 151595 (93.5) | -0.11 | 2588.07 (94.0) | 29500.87 (93.8) | -0.01 |
| ≥40 g/day | 569 (4.0) | 10543 (6.5) | -0.11 | 164.98 (6.0) | 1965.34 (6.2) | -0.01 | |
| Missing number | 2328 | 31223 | -0.11 | 0.00 | 0.00 | 0.00 | |
| With exercise habits* | Yes | 6577 (47.2) | 72654 (46.4) | 0.02 | 1305.5 (47.4) | 14517.14 (46.1) | 0.02 |
| Missing number | 2747 | 36699 | 0.02 | 0.00 | 0.00 | 0.00 | |
| Health conscience† | Low | 7816 (56.8) | 95792 (62.1) | 0.11 | 1571.89 (57.1) | 18653.94 (59.3) | 0.07 |
| Intermediate | 1926 (14.0) | 16976 (11.0) | 0.11 | 339.46 (12.3) | 4004.75 (12.7) | 0.07 | |
| High | 4018 (29.2) | 41529 (26.9) | 0.11 | 841.70 (30.6) | 8807.52 (28.0) | 0.07 | |
| Missing number | 2931 | 39064 | 0.11 | 0.00 | 0.00 | 0.00 | |
| eGFR | >60 | 11369 (71.0) | 130944 (71.3) | 0.14 | 1855.67 (67.4) | 21362.33 (67.9) | 0.04 |
| >45,<=60 | 3962 (24.7) | 43519 (23.7) | 0.14 | 718.25 (26.1) | 8117.45 (25.8) | 0.04 | |
| >30,<=45 | 605 (3.8) | 7821 (4.3) | 0.14 | 151.58 (5.5) | 1691.87 (5.4) | 0.04 | |
| <=30 | 74 (0.5) | 1319 (0.7) | 0.14 | 27.55 (1.0) | 294.56 (0.9) | 0.04 | |
| Missing number | 681 | 9758 | 0.14 | 0.00 | 0.00 | 0.00 | |
| HbA1c | <6.5 | 14891 (90.5) | 164986 (87.4) | 0.14 | 2308.38 (83.8) | 26261.23 (83.5) | 0.08 |
| <7,6.5≥ | 771 (4.7) | 13923 (7.4) | 0.14 | 257.19 (9.3) | 2876.13 (9.1) | 0.08 | |
| <7.5,7≥ | 324 (2.0) | 4960 (2.6) | 0.14 | 98.04 (3.6) | 1180.08 (3.8) | 0.08 | |
| <8,7.5≥ | 163 (1.0) | 1931 (1.0) | 0.14 | 40.51 (1.5) | 498.82 (1.6) | 0.08 | |
| ≥8 | 302 (1.8) | 2970 (1.6) | 0.14 | 48.91 (1.8) | 649.93 (2.1) | 0.08 | |
| Missing number | 240 | 4591 | 0.14 | 0.00 | 0.00 | 0.00 | |
| LDL | <120 | 1548 (9.3) | 86789 (44.9) | 1.18 | 940.52 (34.2) | 10587.78 (33.6) | 0.04 |
| 120<-139 | 2953 (17.8) | 54297 (28.1) | 1.18 | 842.02 (30.6) | 9612.41 (30.5) | 0.04 | |
| 140<-160 | 5015 (30.3) | 34876 (18.1) | 1.18 | 689.34 (25.0) | 7489.79 (23.8) | 0.04 | |
| >160 | 7061 (42.6) | 17238 (8.9) | 1.18 | 281.18 (10.2) | 3776.23 (12.0) | 0.04 | |
| Missing number | 114 | 161 | 1.18 | 0.00 | 0.00 | 0.00 | |
| Any malignancy‡ | Presence | 1422 (8.5) | 17222 (8.9) | -0.01 | 316.73 (11.5) | 3110.49 (9.9) | 0.05 |
| Liver disease | Presence | 2187 (13.1) | 23427 (12.1) | 0.03 | 616.01 (22.4) | 6971.22 (22.2) | 0.01 |
| Hypertension | Presence | 9712 (58.2) | 83181 (43.0) | 0.31 | 1770.22 (64.3) | 19118.98 (60.8) | 0.07 |
| Diabetes | Presence | 807 (4.8) | 6651 (3.4) | 0.07 | 180.37 (6.6) | 1978.72 (6.3) | 0.01 |
| Rheumatic disease | Presence | 466 (2.8) | 5330 (2.8) | 0.00 | 110.94 (4.0) | 1152.58 (3.7) | 0.02 |
| Dementia | Presence | 323 (1.9) | 4527 (2.3) | -0.03 | 74.60 (2.7) | 758.89 (2.4) | 0.02 |
| Renal disease | Presence | 537 (3.2) | 3529 (1.7) | 0.10 | 95.31 (3.5) | 940.35 (3.0) | 0.03 |
| Peptic ulcer disease | Presence | 2328 (13.9) | 26015 (13.5) | 0.01 | 513.61 (18.7) | 5605.58 (17.8) | 0.02 |
| Alcohol abuse | Presence | 58 (0.3) | 908 (0.5) | -0.02 | 17.88 (0.6) | 253.18 (0.8) | -0.19 |
| Anemia | Presence | 739 (4.4) | 9310 (4.8) | -0.02 | 186.85 (6.8) | 1944.47 (6.2) | 0.02 |
| Depression | Presence | 729 (4.4) | 6991 (3.6) | 0.04 | 146.84 (5.3) | 1592.70 (5.1) | 0.01 |
| Hemiplegia or paraplegia | Presence | 21 (0.1) | 241 (0.1) | 0.00 | 3.25 (0.1) | 49.10 (0.2) | -0.01 |
| Fatigue | Presence | 128 (0.8) | 1351 (0.7) | 0.01 | 35.59 (1.3) | 312.13 (1.0) | 0.03 |
| Gait Abnormality or difficulty walking | Presence | 45 (0.3) | 643 (0.3) | -0.01 | 13.47 (0.5) | 113.23 (0.4) | 0.02 |
| Hyperlipidemia | Presence | 16189 (97.0) | 38352 (19.8) | 2.52 | 2542.36 (92.3) | 28498.23 (90.6) | 0.06 |
| Sleep Apnea | Presence | 104 (0.6) | 977 (0.5) | 0.02 | 18.98 (0.7) | 248.64 (0.8) | -0.01 |
| COPD | Presence | 889 (5.3) | 11165 (5.8) | -0.02 | 204.44 (7.4) | 2311.47 (7.3) | 0.00 |
| ACE inhibitor | Presence | 517 (3.1) | 4618 (2.4) | 0.04 | 108.80 (4.0) | 1099.75 (3.5) | 0.02 |
| α-Blocker | Presence | 1157 (6.9) | 15573 (8.1) | -0.04 | 261.47 (9.5) | 2869.89 (9.1) | 0.01 |
| Angiotensin receptor blocker | Presence | 5045 (30.2) | 44749 (23.1) | 0.16 | 926.70 (33.7) | 10306.97 (32.8) | 0.02 |
| β-Blocker | Presence | 1670 (10.0) | 12253 (6.3) | 0.13 | 274.17 (10.0) | 2801.00 (8.9) | 0.04 |
| Calcium channel blocker | Presence | 6814 (40.8) | 59300 (30.7) | 0.21 | 1216.87 (44.2) | 13327.32 (42.4) | 0.04 |
| Diuretics | Presence | 1257 (7.5) | 12965 (6.7) | 0.03 | 245.17 (8.9) | 2676.15 (8.5) | 0.01 |
| Non-statin lipid-lowering drug | Presence | 2181 (13.1) | 11370 (5.9) | 0.25 | 606.60 (22.0) | 6655.94 (21.2) | 0.02 |
BMI: body mass index, COPD: chronic obstructive pulmonary disease, ACE: angiotensin-converting enzyme, SMD: Standardized mean difference. *With exercise habits is the answer to the question “Are you in the habit of doing exercise to sweat lightly for over 30 minutes a time, two times weekly, for over a year?”. Answers are obtained in yes/no form. †Health conscience is the answer to the question “Do you want to improve your life habits of eating and exercising?” choosing from the following "1 Don't want", "2 Do want", "3 Want to improve in near future (within a month) and began to start", "4 Already trying to improve (less than 6 months)", "5 Already trying to improve (over 6 months)". And the answer interpreted 1, 2 as low, 3 as Intermediate, 4, 5 as High. ‡Any malignancy, including lymphoma and leukemia, and malignant neoplasm of skin.
Table 2.
Association between statin use, all-cause mortality, after adjustment by the inverse probability of treatment-weighted (IPTW) method. CI: confidence interval, HR: hazard ratio, NNT: number needed to treat, RD: risk difference, RR: risk ratio.
Table 2.
Association between statin use, all-cause mortality, after adjustment by the inverse probability of treatment-weighted (IPTW) method. CI: confidence interval, HR: hazard ratio, NNT: number needed to treat, RD: risk difference, RR: risk ratio.
| Variable | Category | Number of cases after adjustment | Number of statin group | Cox regression analysis in adjusted population | RR | RD | RD 95% CI | NNT | NNT 95% CI | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-value | ||||||||||||
| Overall population | - | 34,219 | 2,753 | 0.40 | 0.33 | 0.48 | <.0001 | 0.31 | 0.05 | 0.04 | 0.06 | 21.20 | 18.10 | 24.70 |
| Age | 65 to <75 years | 21,479 | 2,062 | 0.30 | 0.20 | 0.44 | <.0001 | 0.22 | 0.02 | 0.02 | 0.03 | 44.64 | 39.18 | 54.57 |
| 75 to <85 years | 10,284 | 613 | 0.42 | 0.31 | 0.57 | <.0001 | 0.37 | 0.07 | 0.04 | 0.09 | 14.78 | 11.75 | 22.39 | |
| ≥85 years | 3,011 | 75 | 0.59 | 0.37 | 0.93 | 0.02 | 0.55 | 0.13 | -0.004 | 0.28 | 7.63 | 3.63 | -244.3 | |
| Sex | Men | 17,643 | 1,027 | 0.35 | 0.26 | 0.48 | <.0001 | 0.25 | 0.06 | 0.05 | 0.07 | 15.68 | 13.45 | 19.21 |
| Current smoker | No | 30,474 | 2,535 | 0.38 | 0.31 | 0.47 | <.0001 | 0.29 | 0.05 | 0.04 | 0.05 | 20.95 | 18.34 | 24.42 |
| BMI | <18.5 | 2,847 | 133 | 0.23 | 0.10 | 0.55 | 0.0008 | 0.27 | 0.08 | 0.04 | 0.11 | 12.02 | 8.97 | 25.33 |
| ≥30.0 | 798 | 71 | 0.64 | 0.22 | 1.83 | 0.41 | 0.77 | 0.01 | -0.04 | 0.07 | 73.34 | 13.55 | -22.85 | |
| LDL cholesterol | <120 mg/dl | 27,956 | 436 | 0.57 | 0.37 | 0.86 | 0.008 | 0.20 | 0.05 | 0.04 | 0.07 | 20.34 | 14.62 | 23.46 |
| 140 to ≤160 mg/dl | 8,781 | 1,132 | 0.47 | 0.34 | 0.66 | <.0001 | 0.53 | 0.02 | 0.01 | 0.03 | 45.42 | 31.91 | 75.48 | |
| >160 mg/dl | 7,223 | 2,134 | 0.51 | 0.39 | 0.67 | <.0001 | 0.36 | 0.03 | 0.02 | 0.04 | 34.19 | 25.29 | 51.32 | |
| Diabetes | Yes | 2,223 | 239 | 0.31 | 0.16 | 0.58 | 0.0002 | 0.25 | 0.08 | 0.05 | 0.10 | 12.78 | 9.66 | 20.96 |
| No | 31,225 | 2,516 | 0.41 | 0.34 | 0.50 | <.0001 | 0.32 | 0.05 | 0.04 | 0.05 | 22.14 | 18.85 | 26.45 | |
| Rheumatic disease | Yes | 1,350 | 118 | 0.40 | 0.17 | 0.97 | 0.04 | 0.11 | 0.07 | 0.04 | 0.08 | 14.75 | 12.11 | 24.07 |
| Dementia | Yes | 861 | 60 | 0.35 | 0.19 | 0.67 | 0.0015 | 0.42 | 0.18 | 0.05 | 0.26 | 5.69 | 3.83 | 18.81 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



