
Submitted:
13 June 2023
Posted:
14 June 2023
You are already at the latest version
Abstract
Left ventricular (LV) remodeling is a dynamic process which is characterized by abnormal LV wall thickness and altered myocardial geometry, and it is considered as a negative prognostic factor in both heart failure with reduced eject fraction (HFrEF) and heart failure with preserved eject fraction (HFpEF). Hypertension, type 2 diabetes (T2D) and obesity are strongly correlated with the development and the progression of LV remodeling, LV hypertrophy and LV systolic and/or diastolic dysfunction. Indeed, the beneficial impact of exercise training on primary and secondary prevention of cardiovascular disease (CVD) has been well-established. Recent studies highlight that exercise training enhances functional capacity, muscle strength and endurance, cardiac function and cardiac-related biomarkers, among patients with established coronary artery disease (CAD) or HF, thus improving substantially their cardiovascular prognosis, survival rates and needs for rehospitalization. Therefore, in this review article, we discuss the evidence of LV remodeling in patients with cardiometabolic risk factors, such as hypertension, T2D, obesity, and also highlight the current studies evaluating the effect of exercise training on LV remodeling in these patients.
Keywords:
exercise
; diabetes
; obesity
; hypertension
; ventricular remodeling
; heart failure
1. Introduction
It is estimated that more than 26 million adults suffer from heart failure (HF) worldwide, with the prevalence rates to grow rapidly [1]. According to current literature, 35-50% of patients with HF experience frequent rehospitalizations within 6 months of discharge, thus deteriorating their prognosis and incurring billions in costs [2]. Left ventricular hypertrophy (LVH) seems to be one of the leading cause of death worldwide and is characterized by increased left ventricular (LV) mass and cardiomyocyte hypertrophy [3]. Hypertension, type 2 diabetes (T2D), chronic kidney disease and aortic stenosis are considered major risk factors for LVH [4,5]. Furthermore, LVH has been associated with increased risk for LV dysfunction, HF, arrythmias, stroke and sudden cardiac death [3].
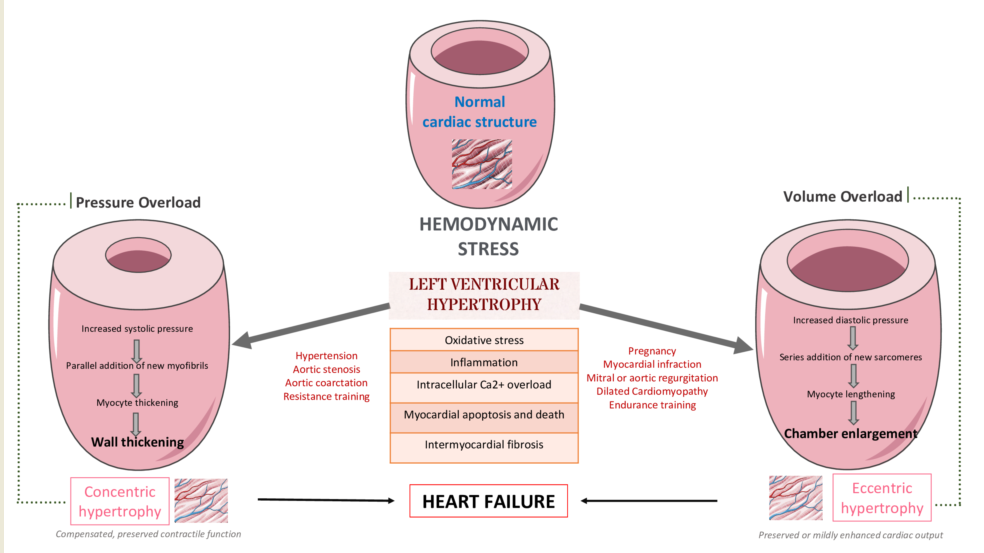
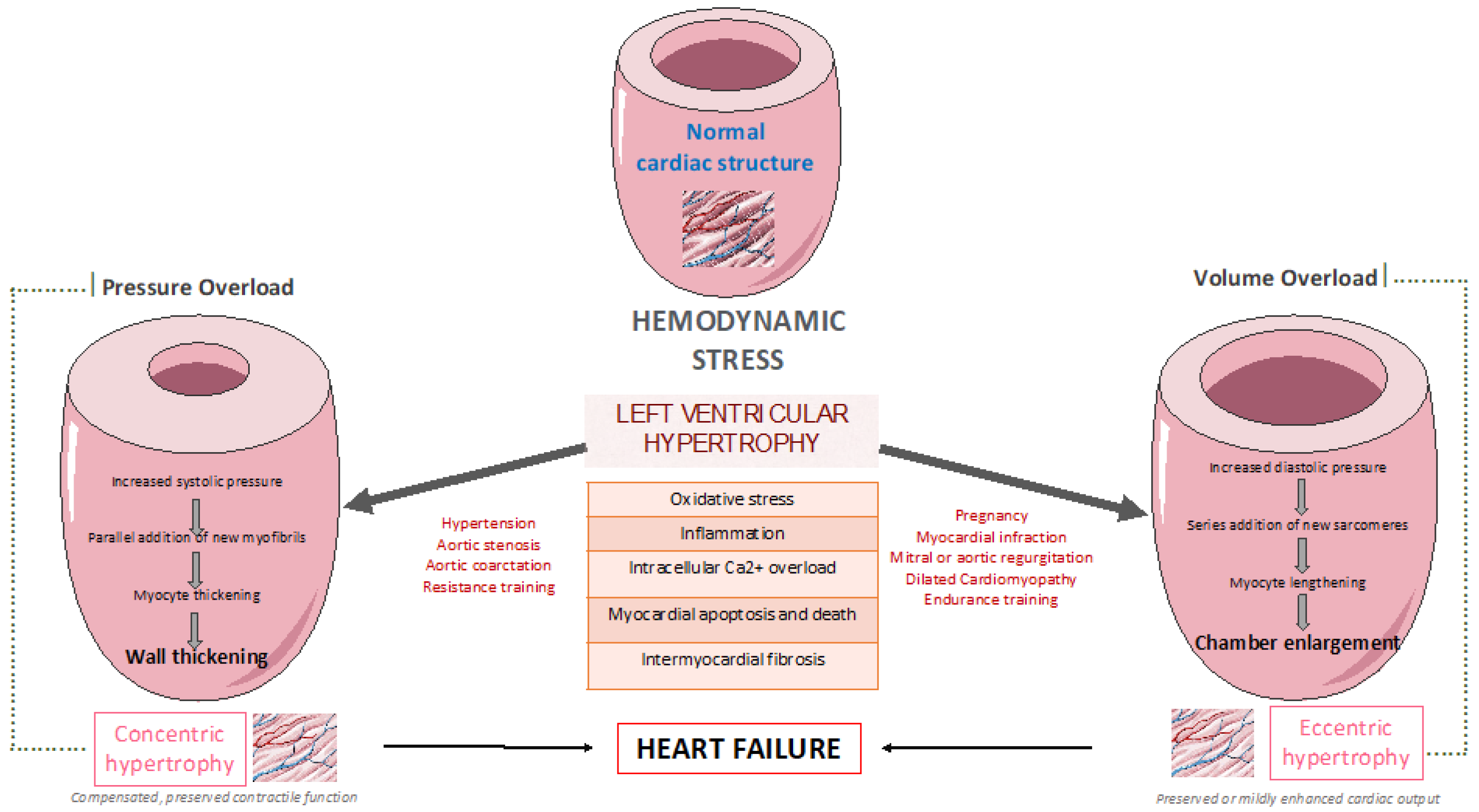
LV remodeling is a dynamic process which is characterized by abnormal LV wall thickness and altered myocardial geometry, and it is considered as a negative prognostic factor in both heart failure with reduced eject fraction (HFrEF) and heart failure with preserved eject fraction (HFpEF). In more details, obesity and hypertension cause increase in systemic pressure, afterload and wall stress, thus leading to the development of LVH [6,7]. Up to 60% of patients with hypertension may present with signs of increased LV mass on echocardiography [8]. Mild to moderate hypertension and LVH is commonly accompanied by varying degree of impaired LV diastolic filling with normal or mild increased systolic performance at rest, as well as diminished coronary vasodilator capacity [9]. Nevertheless, LVH might evolve to overt systolic and diastolic dysfunction, thus leading to the development and progression of HFrEF or HFpEF, respectively, as presented in Figure 1.
Plenty complex and multifactorial mechanisms resulting in transcriptional, signaling, structural and electrophysiological changes are involved in this process of LV remodeling [10]. More specifically, oxidative stress and altered intracellular calcium metabolism provoke cardiomyocyte hypertrophy, thus resulting in impaired contraction and relaxation, as well as increased risk for fatal ventricular arrythmias and sudden cardiac death [11,12]. Of note, interstitial and replacement fibrosis play a pivotal role in the progression of LV remodeling [8].
On the one hand, LVH regression seems to limit LVH-related adverse clinical outcomes and improve patient prognosis [13]. On the other hand, the beneficial impact of exercise training on primary and secondary prevention of plenty clinical conditions such as cardiovascular disease (CVD), T2D, as well as obesity has been well-established so far [14]. Recent studies highlight that exercise training enhances functional capacity, muscle strength and endurance, cardiac function and cardiac-related biomarkers, among patients with established coronary artery disease (CAD) [15] or HF [16], thus improving substantially their cardiovascular prognosis, survival rates and needs for rehospitalization [17].
In this review article, we discuss the evidence of LV remodelling among patients with cardiometabolic risk factors, such as hypertension, T2D, obesity and we also focus on current studies evaluating the effect of exercise training on LV remodeling in these patients.
2. LV remodelling pattern among patients with cardiometabolic risk factors
2.1. Athlete’s heart
Exercise training typically increases heart rate and blood pressure, leading to specific cardiac changes among healthy individuals, especially the highly trained athletes[18]. This condition should be differentiated from hypertension-induced cardiac maladaptation and LVH, thus it is further discussed below. “Athlete’s heart” is characterized by eccentric LVH, especially among elite athletes, and those participating in endurance and resistance training programs, whereas the related functional and structural changes occur parallel with exercise training, as an adaptation to intensive and chronic hemodynamic overload [19]. Therefore, LVH might be a physiological adaptation to strenuous physical exercise, as observed in athletes, whereas it is generally benign. However, it strongly correlated with the type of exercise [20]. Dynamic exercise, such as running and swimming, causes volume overload, whereas static exercise such a weightlifting, increases pressure load [19]. Aerobic exercise programs induce normally cardiac remodeling characterized by increased right ventricular (RV) and LV chamber dimensions and wall thickness, increased left atrial (LA) cavity size along with normal systolic and diastolic function, although resistance training increases mildly LV thickness, with no effect on LV chamber size [19]. The increase in LV wall thickness and LA cavity is even greater in master endurance athletes [21]. LV wall thickness may exceed the normal upper limits of 13 to 15 mm [22] up to 16mm in elite male athletes [23]. Of note, exercise programs combining both aerobic and anaerobic types of activities, such as prolonged cycling, rowing, and swimming result in mixed structural and functional cardiac adaptations and these athletes experience the most increase in LV mass [24].
Interestingly, it has been reported that athletes may have a 15-20% increase in LV wall thickness, a 10% increase in LV cavity size and a 24% increase in RV cavity size [25]. LV thickness up to 15mm is commonly apparent in most athletes, while the most thickened region is the anterior portion of the ventricular septum [26]. Morphologic adaptation to training in athletes enlarges the cavity size to an end-diastolic diameter ≥55 mm [6]. Nevertheless, “athlete’s heart” differentiates from hypertension-induced cardiac maladaptation and LVH. The overall pattern of LVH in “athlete’s heart” seems to be symmetric and homogenous [27]. However, athletes with LVH do not have impaired left ventricular ejection fraction (LVEF) or any evidence of systolic or diastolic dysfunction. Therefore, chronic exercise-mediated cardiac adaptations observed in athletes are considered to be normal hemodynamic responses, which do not correlate with increased risk of diastolic or systolic dysfunction, arrythmias, or adverse prognosis, whereas they regress gradually, when there is exercise restriction [28]. Moreover, cardiac dimensions, LV hypertrophy and LA dilatation generally regress to normal values after a period of detraining and deconditioning, which can take up to several years in longtime athletes [29]. However, an increase in LV mass, LV cavity size and LA diameter might be persistent up to 50% of endurance athletes even after 3 years of detraining [29].
2.2. Hypertensive heart disease
Chronic hemodynamic overload in hypertension provokes major structural and functional changes leading to LVH. In more details, chronically increase blood pressure cause LV pressure overload, thus increasing LV workload and resulting in LVH [6]. This clinical condition is characterized by hypertrophy of existing cardiomyocytes, addition of sarcomeres, increased deposition of collagen and extracellular matrix, leading to an increase in ventricular mass [30]. Typical echocardiographic structural findings, including concentric remodeling, concentric hypertrophy or even a combination of concentric and eccentric hypertrophy, along with increased LV wall thickness, LV diastolic and systolic dimensions, have been described. Functional changes cause activation of sympathetic and renin-angiotensin-aldosterone system, thus increasing myocardial wall stress and leading to detrimental systolic and diastolic dysfunction. At the later stages, impaired ventricular contractility and systolic HF may present [31]. Interestingly, healthy individuals, who do not exceed blood pressure levels above 150mmHg during exercise, do not stimulate cardiac remodeling, and as a result they are less likely to develop LVH [6]. So far, European Society of Hypertension along with European Society of Cardiology have announced recommendations for LVH evaluation based on electrocardiogram and echocardiogram findings. Although ECG is a low-cost and widely used method, echocardiogram is the most preferred method for assessing LV size and function [32].
2.3. Diabetic cardiomyopathy
T2D is a systemic disease with detrimental macro and micro-vascular complications. Patients with T2D have a 2.5-fold increased risk to develop HF, independently of age or concomitant comorbidities such as CAD and dyslipidemia [33,34], whereas these patients represent the one third of HF population in clinical trials [35]. The term of “diabetic myocardiopathy” is a clinical condition characterized by impairments in cardiac structure and function independent of the macrovascular complications of diabetes (including hypertension, CAD and atherosclerosis) [36,37]. Of note, cardiac dysfunction commonly remains clinically silent and as a result underdiagnosed until the latest stages of the disease, whereas almost 50% of asymptomatic, normotensive patients with T2D and good glycemic control demonstrate a degree of cardiac dysfunction [38].
Diabetes-induced LV diastolic dysfunction caused by prolonged and delayed LV filling and relaxation, often is presented in the absence of concomitant impairments in LV systolic function [39,40]. Moreover, diabetes-induced abnormal collagen deposition, cardiomyocyte hypertrophy and cardiomyocyte loss via myocardial cell death pathways resulting in cardiac fibrosis and hypertrophy has been described in both animal and human studies [41,42,43,44]. Furthermore, coronary microvascular hypoperfusion as characterized by impairment in coronary flow reserve, and myocardial blood flow, with increased coronary resistance, have been also reported among patients with T2D [45]. Complex pathophysiological pathways including oxidative stress, inflammation, impaired Ca2+ metabolism, mitochondrial and metabolic dysfunction, endoplasmic reticulum stress, along with alterations to insulin sensitivity and signaling, gene regulation, neurohumoral activation and cardiac cell death seem to be the main contributors to the development and progress of diabetic cardiomyopathy [46,47].
2.4. Obesity-related cardiomyopathy
Obesity is a multifactorial metabolic disorder characterized by a heterogeneous complex of biological, socioeconomic and environmental factors leading to adverse health outcomes [48,49]. According to recent epidemiological data, it is estimated that more than 603 million adults suffer already from obesity worldwide, whereas prevalence rates grow rapidly [50]. Obesity has been strongly correlated with the presence of T2D, hypertension and various lipid disorders such as triglyceridemia, low levels of high-density lipoprotein, increased levels of small dense low lipoprotein and apoprotein B, thus increasing the cardiovascular risk [51,52]. Especially, central, visceral obesity is a pivotal cardiovascular risk factor [53]. Pericardial and epicardial adipose tissue seem to be also a main contributor for CVD [54]. Obesity-induced insulin resistance, hyperinsulinemia, endothelial dysfunction, lipid accumulation, chronic low-grade systematic inflammation, oxidative stress and prothrombotic status seems to be the main pathophysiological pathways leading to the development and progression of CVD [54,55].
Obesity is associated with atherosclerosis, abnormalities in the coronary microvasculature and as a result increased risk for CAD [56,57]. Furthermore, excess adipose tissue accumulation leads to major hemodynamic changes, including increased blood volume and blood pressure, cardiac output, as well as myocardial wall stress [58]. Moreover, ectopic pericardial and epicardial fat induces myocardial fat accumulation, resulting in local inflammation, macrophage infiltration, cytokine gene expression, thus leading to subsequent myocardial fibrosis, and cardiomyocytes hypertrophy. Of note, concentric LV remodeling and LVH, right ventricular dilatation and right ventricular dysfunction have been reported among patients with obesity [54]. Considering that patients with obesity present impaired systolic and diastolic cardiac function, they are more likely to develop HF [59]. Interestingly, obese patients have a 56% higher risk of developing HFpEF [60].
3. The effect of exercise training on left ventricular remodelling among patients with cardiometabolic risk factors
3.1. In patients with hypertension
According to current literature, exercise training leads to substantial reduction in resting systolic and diastolic blood pressure, as well as in LVH among hypertensive patients [61,62], as presented in Table 1. Additionally, recent studies indicate that moderate and regular physical activity reduces significantly total peripheral resistance [63,64]. Exercise-mediated hemodynamic changes include also increased cardiac output along with redistribution of blood flow to muscular territories [65]. So far, there is evidence that exercise training may reduce LV hypertrophy in parallel with systolic and diastolic blood pressure improvement [66].
Turner et al. were from the first to report that that exercise training may induce regression of LVH and LV concentric remodeling among patients with mild or moderate hypertension [67]. In more details, exercise training improved aerobic efficacy by 16% and decreased substantially systolic and diastolic blood pressure, LV wall thickness, as well as LV mass index. Of note, LVH regression was mainly attributed to the reduction of the systolic blood pressure [67]. Indeed, the evidence that exercise training improves significantly systolic and diastolic blood pressure among patients with mild or moderate hypertension is well documented so far [68,69].
Furthermore, low-fit individuals with hypertension seem to have higher LV mass index when compared to the moderate and high-fit individuals [62]. In this randomized controlled trial, 16 weeks of aerobic exercise led to a substantial regression of LV mass and thickness of the interventricular septum, which were mainly attributed to linear reduction in systolic and diastolic blood pressure [62]. Similarly, regular exercise training results in lowering blood pressure, LV mass index, as well as exercise capacity among patients with borderline or mild hypertension [66]. Εxercise-mediated decreased posterior wall and intraventricular septal thickness are also found in hypertensive patients [70]. Moreover, there is also evidence that 1-MET increase in workload offers a 42% reduction in the risk of LVH [71]. Of note, regular physical activity seems to prevent the development of LVH among hypertensive patients at stage 1 [72]. More specifically, patients in physically active group were less likely to develop LVH when compared to those following a sedentary lifestyle, after a median follow-up of 8.3 years.
3.2. In patients with type 2 diabetes
So far, there is evidence that exercise training may improve both LV systolic and diastolic function in patients with diabetes, resulting in favorable changes in stroke volume, LVEF, end-systolic volumes, as well as LV filling [73]. Both endurance and combined endurance and resistance exercise training beneficially affect cardiovascular parameters among patients with T2D [74]. According to a randomized clinical trial, high intensity intermittent training (HIIT) seems to improve substantially cardiac function and structure among patients with T2D, resulting finally in a positive cardiac remodeling [75]. In more details, this type of 12-month exercise interventional program ameliorated both LV mass and systolic function when compared to standard care. Of note, these changes were accompanied by modest improvements in glycemic control.
Furthermore, Otten et al. reported that supervised exercise training (3weeks/hour) along with paleolithic diet (based on vegetables, fruits, berries, nuts, seafood, eggs, fish and lean meat with a high restriction of dairy products, cereals, legumes, refined fats, added sugar and salt) resulted in favorable metabolic and cardiac changes with a decrease in triglycerides levels and LV mass to end-diastolic volume ratio and an increase in LVEDV and stroke volume, among overweight and obese patients with T2D [76]. Similarly, exercise training seems also to improve diastolic function among patients with T2D. In a randomized clinical trial, a 12-week supervised aerobic exercise training program improved diastolic function in the absence of any major effects on LV remodeling, perfusion, or aortic stiffening, among asymptomatic young patients with T2D [77]. Interestingly, exercise-mediated favorable changes in LV remodeling index seems to be the best predictor of improvement in LV diastolic function after the lifestyle intervention program including increased physical activity among patients with T2D and CAD [78].
3.3. In patients with type obesity
Physical activity improves LVH among patients with obesity and hypertension. In more details, higher physical activity was associated with a reduction in LV mass index and an improvement in LVH, as well as cardiac biomarkers such as N-terminal pro-atrial natriuretic peptide (NT-pro BNP) and mid-regional sequence of pro-A-type natriuretic peptide (MR pro-ANP) [79]. Similarly, a decrease in triglycerides levels and LV mass to end-diastolic volume ratio and an increase in LVEDV and stroke volume, are reported among overweight and obese patients with T2D who participated in supervised exercise training programs [76]. Of note, the beneficial effects of exercise training on the reduction on LV mass are apparent regardless of whether the obese patients are normotensive or hypertensive. More specifically, Himeno et al. reported that mild exercise along with mild hypocaloric intake resulted in significant weight and LV mass reduction among obese patients, after a 12-week intervention period [80]. Indeed, LV mass was significantly decreased among obese patients regardless the presence of hypertension or not, whereas significant changes were found in the systolic, diastolic, and mean blood pressure. These data provide evidence that exercise-mediated reduction in LV mass is not only attributed to reduction in blood pressure and weight loss, but also to further mechanisms such as improved cardiac autonomous function [81], myocardial metabolism and metabolic flexibility, as well as reduced LV stiffness [82].
Main studies evaluating the effect of exercise training on LV remodeling in patients with cardiometabolic risk factors, such as hypertension, T2D, and obesity are summarized below in Table 1.

Table 1.
Main studies evaluating the effect of exercise training on LV remodeling in patients with cardiometabolic risk factors, such as hypertension, type 2 diabetes, and obesity.
Table 1.
Main studies evaluating the effect of exercise training on LV remodeling in patients with cardiometabolic risk factors, such as hypertension, type 2 diabetes, and obesity.
| Author | Type of study | Patient Characteristics | Main findings |
|---|---|---|---|
| Zanettini et al. [61] | Prospective cohort study | ∙14 sedentary patients with untreated diastolic BP (90-104 mmHg) ∙12-week supervised exercise program |
∙Exercise-mediated increase in aerobic fitness significantly reduced resting systolic and diastolic BP, mean systolic and diastolic 24-hour BP, as well as LV mass index. |
| Kokkinos et al. [62] | Randomized controlled trial | ∙46 male patients with severe hypertension ∙35-76 years of age ∙16 or 32-week exercise program plus antihypertensive medication or antihypertensive medication alone |
∙Diastolic BP decreased in the patients who exercised, whereas it increased slightly, in those who did not exercise. ∙Thickness of interventricular septum, LV mass, and mass index decreased significantly only in the patients who exercised. |
| Turner et al. [67] | Prospective cohort study | ∙11 patients with mild to moderate hypertension vs 7 sedentary hypertensive patients as controls ∙65.5± 1.2 vs 68.5±1 years of age ∙6.8±3.8- month exercise program |
∙Exercise training decreased systolic and diastolic BP, LV wall thickness and mass, as well as wall thickness-to-radius. ∙Only the reduction in resting systolic BP was correlated significantly with the regression of concentric remodeling. |
| Pitsavos et al. [66] | Randomized controlled trial | ∙40 patients with borderline to mild hypertension ∙53±7 years of age ∙16-week exercise aerobic program or standard care |
∙Systolic and diastolic BP, as well as heart rate were significantly lower in the exercise group compared to the control group. ∙LV mass index decreased significantly only in the exercise group. |
| Palatini et al. [72] | Prospective cohort study | ∙454 patients with stage 1 hypertension ∙33.1±8.4 years of age ∙median follow-up of 8.3 years |
∙Physically active groups were less likely to develop LVH than sedentary group. ∙BP declined in physically active patients and slightly increased in the sedentary peers. |
| Cassidy et al. [75]C | Randomized controlled trial | ∙28 patients with type 2 diabetes ∙61±9 vs 59±9 years of age ∙12-week HIIT or standard care |
∙HIIT improved LV wall mass and stroke volume. ∙Early diastolic filling rates increased, and peak torsion decreased in the treatment group. |
| Otten et al. [76] | Randomized controlled trial | ∙22 overweight and obese subjects with type 2 diabetes ∙61(58–66) vs 59(52–64) years of age ∙12-week PD-EX vs PD and standard care |
∙Significant decreases in LV mass to EDV ratio was observed in the PD-EX group. ∙LVEDV and stroke volume increased significantly only in the PD-EX group. |
| Gulsin et al. [77] | Randomized controlled trial | ∙87 patients with type 2 diabetes and 36 matched controls ∙50.5±6.5 vs 48.6±6.2 years of age ∙12-week supervised aerobic exercise training vs low-energy MRP diet vs routine care |
∙Supervised aerobic exercise training program improved diastolic function in the absence of any major effects on LV remodeling, perfusion, or aortic stiffening. ∙MRP resulted in weight loss, and improved blood pressure, glycemia, LV mass/volume, and aortic stiffness but not diastolic function. |
| Kamimura et al. [79] | Retrospective cohort study | ∙1,300 African Americans with preserved LVEF (>50%) ∙63 (57, 69) years of age ∙physical activity was calculated as 3*heavy activity hours + 2*moderate activity hours + slight activity hours/day |
∙Higher physical activity index was independently associated with lower LV mass. ∙Higher physical activity index was associated with lower LV mass index more in obese or hypertensive participants compared with non-obese or non-hypertensive participants. |
| Himeno et al. [80] | Prospective cohort study | ∙11 obese and hypertensive patients and 11 obese and normotensive patients ∙37±11 vs 35±7 years of age ∙12-week weight-reduction program consisted of mild exercise and mild hypocaloric intake |
∙Systolic, diastolic, and mean BP were significantly reduced only in the hypertensive group. ∙LV mas was significantly reduced both among hypertensive and normotensive obese patients. |
3.4. In patients with coronary artery disease
LV remodeling following acute myocardial infraction (AMI) is a complex process characterized by fibroblast proliferation, collagen deposition, scar formation, as well as ventricular expansion, resulting in LV dysfunction and HF, thus negatively affecting long-term prognosis in these patients [83,84]. The beneficial effect of exercise training on cardiovascular mortality and morbidity, functional capacity and quality of life in patients with AMI is quite well documented so far [85]. Plenty studies demonstrate that exercise training affects favorably LVH and LV remodeling. Interestingly, exercise training might reverse LVH to normal status or at least undergoing concentric remodeling [86]. Moreover, there is evidence that training, especially aerobic, improves LVEF, decreases end-diastolic volume (EDV) and end-systolic volume (ESV) [87,88]. According to a large meta-analysis, exercise training leads to an increase in LVEF, as well as reduction in ESV and EDV in clinically stable post-MI patients [89]. Of note, the greatest benefits in LVEF, ESV and EDV are occurring when exercise training starts earlier following MI and lasts longer than 3 months, with each week of training delay to require one additional month of training to achieve the same level of improvement in LV remodeling and the comparable reduction in volumes. Moreover, a decrease in plasma NT-pro-BNP and increase in peak early mitral flow velocity have been also observed post-training [87,88,90]. Moreover, there is evidence that systematic exercise and participation in cardiac rehabilitation programs may significantly improve the cardiorespiratory function, exercise ability, and quality of life in patients with ischemic and nonobstructive coronary arteries (INOCA) [91]. Nevertheless, prolong endurance exercise training seems to have detrimental effect on LV systolic and diastolic function.
The beneficial effect of exercise on LV remodeling and cardiopulmonary rehabilitation in LV dysfunction among post-MI patients is also verified by Zhang et al. In this large meta-analysis, it was reported that the greatest benefit of exercise on LV remodeling and cardiopulmonary capacity rehabilitation, as assessed by peak oxygen uptake (VO2), was observed, when exercise was initiated in the acute phase after MI, without an increase in the incidence of MACEs [92]. Indeed, during the healing phase after acute MI, the beneficial effects of exercise training on LVEF, LVESD and peak VO2 weakened compared to the acute phase. Even HIIT seems to improve exercise capacity and quality of life without any detrimental effects on LV remodeling [89,93]. These data imply that secondary prevention along with cardiac rehabilitation programs should be early initiated to achieve the maximal anti-remodeling benefit.
3.5. In patients with heart failure
Obesity and physical inactivity are considered major lifestyle risk factors for the development and progression of HFpEF [94]. Indeed, low fitness has been associated with a great risk of HFpEF than HFrEF [95], whereas patients with HFpEF demonstrate impaired peak VO2 and cardiorespiratory fitness (CRF), which encompass exercise intolerance, when compared to healthy individuals, deteriorating substantially their prognosis [96].
Physical activity and fitness diminish substantially the risk of developing HF, and improve cardiovascular prognosis among patients with established HF [97,98]. Interestingly, for every 1-MET improvement in functional capacity, the risk of HF is reduced by 17% [99]. Participation in exercise-based cardiac rehabilitation programs seems to increase exercise capacity up to 25%, improves New Yor Heart Association (NYHA) functional status, as well as LV remodeling and hypertrophy [100]. Of note, there is evidence that the beneficial effect of training programs on symptoms, CRF, left ventricular diastolic and systolic function, as well as quality of life and HF-related hospitalizations are also apparent among patients with HFpEF and HFrEF [101,102,103,104,105]. Moreover, it is also reported that even endurance training reverses adverse cardiac remodeling, and reduces ESV and EDV, thus improving both systolic and diastolic dysfunction in patients with HFrEF [106]. Similarly, high-intensity training affects beneficially exercise capacity and quality of life, with no detrimental changes in LV remodeling among patients with HFrEF [107]. As a result, patients with higher levels of physical activity experience less adverse cardiac events [108].
According to current literature, exercise training has been associated with a substantial improvement in LV diastolic function, [95,98]. Moreover, it has been reported that exercise reduces LV volumes, which are surrogate markers of LV concentric remodeling or LVH, in patients with HFpEF, whereas exercise training is also correlated with improved measures of CRF. These data demonstrate the pathophysiologic role of LV concentric remodeling contributing to impaired CRF and exercise intolerance in patients with HFpEF and imply that the exercise-meditated improvement in LV remodeling may improve CRF in patients with HFpEF, thus providing novel therapeutical implications [109].
4. Pathophysiological mechanisms of exercise-mediated favorable cardiovascular outcomes
One possible explanation for the favorable effect of exercise training on LV remodeling is the reduction in blood pressure [110]. Afterload reduction to LV mediated by lowering blood pressure has been proposed as a possible mechanism leading to regression of LVH and concentric remodeling [67,111]. Additionally, favorable effects of exercise training on cardiovascular system are mainly attributed to changes in vascular function, cardiac energy metabolism, autonomic balance, including improvement in endothelial dysfunction, arterial and LV stiffness, myocyte calcium handling, mitochondrial function, systolic and diastolic wall stress, cardiac output, and oxygen extraction in the active skeletal muscles. Moreover, increased vasculogenesis though activation of endothelial progenitor cells, ameliorates ischemia and reperfusion injury [64,65,112,113,114,115,116]. Exercise modifies shear stress conditions and modulates further the bioavailability of endothelial nitric oxide (NO), which limits oxidative burden, thus promoting vasodilation and improving vascular endothelial function [64]. Specifically, improvement of endothelium-dependent relaxation is mainly regulated by decreased NO scavenging by reactive oxygen species (ROS) and increased vascular NO production and release.
Furthermore, exercise is related to decreased chronic, low-grade inflammation, increasing the release of anti-inflammatory peptides and reducing the production of pro-inflammatory cytokines [117]. Moreover, exercise-mediated reduction of myocardial collage has been also described [118]. So, another possible mechanism of exercise-mediated improvement in LV dysfunction is the upregulation of miRNA-29, which has been associated with a drop in collagen gene expression [119]. Moreover, exercise training reduces total peripheral resistance [63], increases parasympathetic activity and restores arterial baroreflex sensitivity (BRS) [120], thus ameliorating LVEF and heart rate variability [121]. Nevertheless, plenty pathophysiological mechanism responsible for exercise-mediated regression of LVH remain still unclear.
5. Recommendations and new perspectives
According to 2019 American College of Cardiology (ACC) in collaboration with (AHA) Guideline on the Primary Prevention of CVD, in general, healthy individuals should undergo at least 150 minutes/week of accumulated moderate-intensity physical activity. Otherwise, 75 minutes/week of vigorous-intensity physical activity to reduce the risk of atherosclerotic CVD [122]. In total agreement to previous recommendations, European Society of Cardiology (ESC) highlights that additional benefit is achieved by doubling the previous exercise duration, with multiple sessions of exercise carried out throughout the week [123,124]. More specifically, hypertensive patients should be advised to participate in at least 30 min of moderate- intensity dynamic aerobic exercise (walking, jogging, cycling, or swimming) on 5–7 days per week [125]. Performance of resistance (and especially isometric) exercise on 2-3 days per week can also be advised. However, patients, who are unable to perform the recommended and desirable regular physical activity, should be encouraged to participate in training programs even below the target goal, considering that the exercise-mediated benefit for the cardiovascular system still remains. Therefore, healthcare professionals should offer patient-focused counseling, encourage their patients to participate in well-organized supervised training programs and help them to optimize their physical activity status, considering the favorable effect of exercise on cardiometabolic risk factors and LVH regression [122].
The European Association of Preventive Cardiology Exercise Prescription in Everyday Practice and Rehabilitative Training (EXPERT) tool is an interactive, digital training and support system, which aims to help sports medicine specialists, family physicians, cardiologists, and other medical specialties, to prescribe clinically effective and medically safe exercise training programs among patients with established CVD or cardiometabolic risk factors [126]. In further detail, this website application will analyze patient characteristics, the presence of CVD or cardiometabolic risk factors, contaminant medication or other clinically relevant medical information, so as to generate the most suitable exercise training program for each patient, discouraging certain types of exercise and providing personalized safety advice. Of note, individualized recommendations regarding exercise training intensity, frequency, duration, type, session, as well as additional exercise training modalities will be offered to the patient [126].
6. Conclusions
Improving exercise capacity and optimizing safety of cardiorespiratory programs play a pivotal role in promoting cardiovascular health. Exercise training enhances functional capacity, muscle strength and endurance, cardiac function and cardiac-related biomarkers, as well as quality of life, thus improving substantially cardiovascular prognosis. Exercise training exerts beneficial changes to LV remodeling, thus improving cardiac function and structure among patients with cardiometabolic risk factors. These favorable effects are mainly attributed to positive hemodynamic changes in vascular function, cardiac energy metabolism, and autonomic balance. Therefore, a comprehensive and more personalized approach should be taking into account based on the individual behavioral habits and wishes, cardiovascular profile and needs. It is of major importance that guided, detailed and personalized exercise prescription should be offered by all physicians so as to achieve better treatment, as well as health outcomes.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet Lond Engl 2015, 385, 117–171. [Google Scholar] [CrossRef]
- Gupta A, Fonarow GC. The Hospital Readmissions Reduction Program-learning from failure of a healthcare policy. Eur J Heart Fail 2018, 20, 1169–1174. [Google Scholar] [CrossRef]
- Lorell BH, Carabello BA. Left ventricular hypertrophy: pathogenesis, detection, and prognosis. Circulation 2000, 102, 470–479. [Google Scholar] [CrossRef]
- Stein EJ, Fearon WF, Elmariah S, et al. Left Ventricular Hypertrophy and Biomarkers of Cardiac Damage and Stress in Aortic Stenosis. J Am Heart Assoc 2022, 11, e023466. [Google Scholar] [CrossRef]
- Rader F, Sachdev E, Arsanjani R, et al. Left ventricular hypertrophy in valvular aortic stenosis: mechanisms and clinical implications. Am J Med 2015, 128, 344–352. [Google Scholar] [CrossRef]
- Lovic D, Narayan P, Pittaras A, et al. Left ventricular hypertrophy in athletes and hypertensive patients. J Clin Hypertens 2017, 19, 413–417. [Google Scholar] [CrossRef]
- Gupta S, Berry JD, Ayers CR, et al. Association of Health Aging and Body Composition (ABC) Heart Failure score with cardiac structural and functional abnormalities in young individuals. Am Heart J 2010, 159, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Devereux RB, Casale PN, Hammond IW, et al. Echocardiographic detection of pressure-overload left ventricular hypertrophy: effect of criteria and patient population. J Clin Hypertens 1987, 3, 66–78. [Google Scholar]
- Polese A, De Cesare N, Montorsi P, et al. Upward shift of the lower range of coronary flow autoregulation in hypertensive patients with hypertrophy of the left ventricle. Circulation 1991, 83, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Burchfield JS, Xie M, Hill JA. Pathological ventricular remodeling: mechanisms: part 1 of 2. Circulation 2013, 128, 388–400. [Google Scholar] [CrossRef] [PubMed]
- Nakamura M, Sadoshima J. Mechanisms of physiological and pathological cardiac hypertrophy. Nat Rev Cardiol 2018, 15, 387–407. [Google Scholar] [CrossRef]
- Parati G, Esler M. The human sympathetic nervous system: its relevance in hypertension and heart failure. Eur Heart J 2012, 33, 1058–1066. [Google Scholar] [CrossRef]
- Levy D, Garrison RJ, Savage DD, et al. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med 1990, 322, 1561–1566. [Google Scholar] [CrossRef]
- Dimitriadis K, Bletsa E, Lazarou E, et al. A Narrative Review on Exercise and Cardiovascular Events: “Primum Non Nocere”. Heart Mind 2022, 6, 127. [Google Scholar] [CrossRef]
- Rauch B, Davos CH, Doherty P, et al. The prognostic effect of cardiac rehabilitation in the era of acute revascularisation and statin therapy: A systematic review and meta-analysis of randomized and non-randomized studies – The Cardiac Rehabilitation Outcome Study (CROS). Eur J Prev Cardiol 2016, 23, 1914–1939. [Google Scholar] [CrossRef] [PubMed]
- Lewinter C, Doherty P, Gale CP, et al. Exercise-based cardiac rehabilitation in patients with heart failure: a meta-analysis of randomised controlled trials between 1999 and 2013. Eur J Prev Cardiol 2015, 22, 1504–1512. [Google Scholar] [CrossRef] [PubMed]
- Smart N, Marwick TH. Exercise training for patients with heart failure: a systematic review of factors that improve mortality and morbidity. Am J Med 2004, 116, 693–706. [Google Scholar] [CrossRef] [PubMed]
- Coates AM, Cheung CP, Currie KD, et al. Cardiac Remodeling in Elite Aquatic Sport Athletes. Clin J Sport Med 2022, 32, e485–e491. [Google Scholar] [CrossRef] [PubMed]
- Lazzeroni D, Rimoldi O, Camici PG. From Left Ventricular Hypertrophy to Dysfunction and Failure. Circ J Off J Jpn Circ Soc 2016, 80, 555–564. [Google Scholar]
- Albaeni A, Davis JW, Ahmad M. Echocardiographic evaluation of the Athlete’s heart. Echocardiography 2021, 38, 1002–1016. [Google Scholar] [CrossRef] [PubMed]
- Merghani A, Maestrini V, Rosmini S, et al. Prevalence of Subclinical Coronary Artery Disease in Masters Endurance Athletes With a Low Atherosclerotic Risk Profile. Circulation 2017, 136, 126–137. [Google Scholar] [CrossRef]
- Pelliccia A, Maron BJ, Spataro A, et al. The upper limit of physiologic cardiac hypertrophy in highly trained elite athletes. N Engl J Med 1991, 324, 295–301. [Google Scholar] [CrossRef]
- Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA 2003, 289, 2560–2572. [Google Scholar] [CrossRef]
- Maron BJ, Pelliccia A. The heart of trained athletes: cardiac remodeling and the risks of sports, including sudden death. Circulation 2006, 114, 1633–1644. [Google Scholar] [CrossRef]
- Maron, BJ. Structural features of the athlete heart as defined by echocardiography. J Am Coll Cardiol 1986, 7, 190–203. [Google Scholar] [CrossRef]
- Augustine DX, Howard L. Left Ventricular Hypertrophy in Athletes: Differentiating Physiology From Pathology. Curr Treat Options Cardiovasc Med 2018, 20, 96. [Google Scholar] [CrossRef]
- Go AS, Mozaffarian D, Roger VL, et al. Heart Disease and Stroke Statistics—2014 Update: A Report From the American Heart Association. Circulation; 129. Epub ahead of print 21 January 2014. [CrossRef]
- Lattanzi F, Di Bello V, Picano E, et al. Normal ultrasonic myocardial reflectivity in athletes with increased left ventricular mass. A tissue characterization study. Circulation 1992, 85, 1828–1834. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia A, Maron BJ, De Luca R, et al. Remodeling of Left Ventricular Hypertrophy in Elite Athletes After Long-Term Deconditioning. Circulation 2002, 105, 944–949. [Google Scholar] [CrossRef] [PubMed]
- Gosse P, Cremer A, Vircoulon M, et al. Prognostic value of the extent of left ventricular hypertrophy and its evolution in the hypertensive patient. J Hypertens 2012, 30, 2403–2409. [Google Scholar] [CrossRef]
- Drazner, MH. The Progression of Hypertensive Heart Disease. Circulation 2011, 123, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2013, 34, 2159–2219. [Google Scholar] [CrossRef]
- Ohkuma T, Komorita Y, Peters SAE, et al. Diabetes as a risk factor for heart failure in women and men: a systematic review and meta-analysis of 47 cohorts including 12 million individuals. Diabetologia 2019, 62, 1550–1560. [Google Scholar] [CrossRef] [PubMed]
- Gulsin GS, Swarbrick DJ, Hunt WH, et al. Relation of Aortic Stiffness to Left Ventricular Remodeling in Younger Adults With Type 2 Diabetes. Diabetes 2018, 67, 1395–1400. [Google Scholar] [CrossRef] [PubMed]
- Matsue Y, Suzuki M, Nakamura R, et al. Prevalence and prognostic implications of pre-diabetic state in patients with heart failure. Circ J Off J Jpn Circ Soc 2011, 75, 2833–2839. [Google Scholar]
- Miki T, Yuda S, Kouzu H, et al. Diabetic cardiomyopathy: pathophysiology and clinical features. Heart Fail Rev 2013, 18, 149–166. [Google Scholar] [CrossRef] [PubMed]
- Marwick TH, Ritchie R, Shaw JE, et al. Implications of Underlying Mechanisms for the Recognition and Management of Diabetic Cardiomyopathy. J Am Coll Cardiol 2018, 71, 339–351. [Google Scholar] [CrossRef] [PubMed]
- Boyer JK, Thanigaraj S, Schechtman KB, et al. Prevalence of ventricular diastolic dysfunction in asymptomatic, normotensive patients with diabetes mellitus. Am J Cardiol 2004, 93, 870–875. [Google Scholar] [CrossRef]
- Zabalgoitia M, Ismaeil MF, Anderson L, et al. Prevalence of diastolic dysfunction in normotensive, asymptomatic patients with well-controlled type 2 diabetes mellitus. Am J Cardiol 2001, 87, 320–323. [Google Scholar] [CrossRef]
- Nagueh SF, Smiseth OA, Appleton CP, et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 2016, 17, 1321–1360. [Google Scholar] [CrossRef]
- Dawson A, Morris AD, Struthers AD. The epidemiology of left ventricular hypertrophy in type 2 diabetes mellitus. Diabetologia 2005, 48, 1971–1979. [Google Scholar] [CrossRef]
- Huynh K, McMullen JR, Julius TL, et al. Cardiac-specific IGF-1 receptor transgenic expression protects against cardiac fibrosis and diastolic dysfunction in a mouse model of diabetic cardiomyopathy. Diabetes 2010, 59, 1512–1520. [Google Scholar] [CrossRef] [PubMed]
- Bowden MA, Tesch GH, Julius TL, et al. Earlier onset of diabesity-Induced adverse cardiac remodeling in female compared to male mice. Obes Silver Spring Md 2015, 23, 1166–1177. [Google Scholar] [CrossRef] [PubMed]
- Shimizu M, Umeda K, Sugihara N, et al. Collagen remodelling in myocardia of patients with diabetes. J Clin Pathol 1993, 46, 32–36. [Google Scholar] [CrossRef]
- Di Carli MF, Janisse J, Grunberger G, et al. Role of chronic hyperglycemia in the pathogenesis of coronary microvascular dysfunction in diabetes. J Am Coll Cardiol 2003, 41, 1387–1393. [Google Scholar] [CrossRef]
- Huynh K, Bernardo BC, McMullen JR, et al. Diabetic cardiomyopathy: mechanisms and new treatment strategies targeting antioxidant signaling pathways. Pharmacol Ther 2014, 142, 375–415. [Google Scholar] [CrossRef] [PubMed]
- Ritchie RH, Abel ED. Basic Mechanisms of Diabetic Heart Disease. Circ Res 2020, 126, 1501–1525. [Google Scholar] [CrossRef]
- Jastreboff AM, Kotz CM, Kahan S, et al. Obesity as a Disease: The Obesity Society 2018 Position Statement. Obes Silver Spring Md 2019, 27, 7–9. [Google Scholar] [CrossRef]
- Gordon-Larsen P, Heymsfield SB. Obesity as a Disease, Not a Behavior. Circulation 2018, 137, 1543–1545. [Google Scholar] [CrossRef]
- GBD 2015 Obesity Collaborators, Afshin A, Forouzanfar MH, et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N Engl J Med 2017, 377, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Katta N, Loethen T, Lavie CJ, et al. Obesity and Coronary Heart Disease: Epidemiology, Pathology, and Coronary Artery Imaging. Curr Probl Cardiol 2021, 46, 100655. [Google Scholar] [CrossRef] [PubMed]
- Koliaki C, Liatis S, Kokkinos A. Obesity and cardiovascular disease: revisiting an old relationship. Metabolism 2019, 92, 98–107. [Google Scholar] [CrossRef]
- Després J-P. Body fat distribution and risk of cardiovascular disease: an update. Circulation 2012, 126, 1301–1313. [Google Scholar] [CrossRef] [PubMed]
- Powell-Wiley TM, Poirier P, Burke LE, et al. Obesity and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar]
- Bastien M, Poirier P, Lemieux I, et al. Overview of epidemiology and contribution of obesity to cardiovascular disease. Prog Cardiovasc Dis 2014, 56, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Taqueti VR, Di Carli MF. Coronary Microvascular Disease Pathogenic Mechanisms and Therapeutic Options: JACC State-of-the-Art Review. J Am Coll Cardiol 2018, 72, 2625–2641. [Google Scholar] [CrossRef]
- Bogers RP, Bemelmans WJE, Hoogenveen RT, et al. Association of overweight with increased risk of coronary heart disease partly independent of blood pressure and cholesterol levels: a meta-analysis of 21 cohort studies including more than 300 000 persons. Arch Intern Med 2007, 167, 1720–1728. [Google Scholar] [CrossRef]
- Csige I, Ujvárosy D, Szabó Z, et al. The Impact of Obesity on the Cardiovascular System. J Diabetes Res 2018, 2018, 3407306. [Google Scholar]
- Neeland IJ, Gupta S, Ayers CR, et al. Relation of regional fat distribution to left ventricular structure and function. Circ Cardiovasc Imaging 2013, 6, 800–807. [Google Scholar] [CrossRef]
- Pandey A, LaMonte M, Klein L, et al. Relationship Between Physical Activity, Body Mass Index, and Risk of Heart Failure. J Am Coll Cardiol 2017, 69, 1129–1142. [Google Scholar] [CrossRef]
- Zanettini R, Bettega D, Agostoni O, et al. Exercise Training in Mild Hypertension: Effects on Blood Pressure, Left Ventricular Mass and Coagulation Factor VII and Fibrinogen. Cardiology 1997, 88, 468–473. [Google Scholar] [CrossRef]
- Kokkinos PF, Narayan P, Colleran JA, et al. Effects of Regular Exercise on Blood Pressure and Left Ventricular Hypertrophy in African-American Men with Severe Hypertension. N Engl J Med 1995, 333, 1462–1467. [Google Scholar] [CrossRef]
- Korsager Larsen M, Matchkov VV. Hypertension and physical exercise: The role of oxidative stress. Med Kaunas Lith 2016, 52, 19–27. [Google Scholar]
- Vona M, Rossi A, Capodaglio P, et al. Impact of physical training and detraining on endothelium-dependent vasodilation in patients with recent acute myocardial infarction. Am Heart J 2004, 147, 1039–1046. [Google Scholar] [CrossRef] [PubMed]
- Gielen S, Schuler G, Adams V. Cardiovascular Effects of Exercise Training: Molecular Mechanisms. Circulation 2010, 122, 1221–1238. [Google Scholar] [CrossRef] [PubMed]
- Pitsavos C, Chrysohoou C, Koutroumbi M, et al. The impact of moderate aerobic physical training on left ventricular mass, exercise capacity and blood pressure response during treadmill testing in borderline and mildly hypertensive males. Hell J Cardiol HJC Hell Kardiologike Epitheorese 2011, 52, 6–14. [Google Scholar]
- Turner MJ, Spina RJ, Kohrt WM, et al. Effect of endurance exercise training on left ventricular size and remodeling in older adults with hypertension. J Gerontol A Biol Sci Med Sci 2000, 55, M245–M251. [Google Scholar] [CrossRef] [PubMed]
- Seals DR, Reiling MJ. Effect of regular exercise on 24-hour arterial pressure in older hypertensive humans. Hypertens Dallas Tex 1979 1991, 18, 583–592. [Google Scholar]
- Hagberg JM, Montain SJ, Martin WH, et al. Effect of exercise training in 60- to 69-year-old persons with essential hypertension. Am J Cardiol 1989, 64, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Lou M, Zong X-F, Wang L-L. Curative treatment of hypertension by physical exercise. Eur Rev Med Pharmacol Sci 2017, 21, 3320–3326. [Google Scholar]
- Kokkinos P, Pittaras A, Narayan P, et al. Exercise Capacity and Blood Pressure Associations With Left Ventricular Mass in Prehypertensive Individuals. Hypertension 2007, 49, 55–61. [Google Scholar] [CrossRef]
- Palatini P, Visentin P, Dorigatti F, et al. Regular physical activity prevents development of left ventricular hypertrophy in hypertension. Eur Heart J 2009, 30, 225–232. [Google Scholar]
- Gusso S, Pinto T, Baldi JC, et al. Exercise Training Improves but Does Not Normalize Left Ventricular Systolic and Diastolic Function in Adolescents With Type 1 Diabetes. Diabetes Care 2017, 40, 1264–1272. [Google Scholar] [CrossRef] [PubMed]
- Verboven M, Van Ryckeghem L, Belkhouribchia J, et al. Effect of Exercise Intervention on Cardiac Function in Type 2 Diabetes Mellitus: A Systematic Review. Sports Med Auckl NZ 2019, 49, 255–268. [Google Scholar] [CrossRef] [PubMed]
- Cassidy S, Thoma C, Hallsworth K, et al. High intensity intermittent exercise improves cardiac structure and function and reduces liver fat in patients with type 2 diabetes: a randomised controlled trial. Diabetologia 2016, 59, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Otten J, Andersson J, Ståhl J, et al. Exercise Training Adds Cardiometabolic Benefits of a Paleolithic Diet in Type 2 Diabetes Mellitus. J Am Heart Assoc 2019, 8, e010634. [Google Scholar] [CrossRef] [PubMed]
- Gulsin GS, Swarbrick DJ, Athithan L, et al. Effects of Low-Energy Diet or Exercise on Cardiovascular Function in Working-Age Adults With Type 2 Diabetes: A Prospective, Randomized, Open-Label, Blinded End Point Trial. Diabetes Care 2020, 43, 1300–1310. [Google Scholar] [CrossRef]
- Piché M-E, Poirier P, Marette A, et al. Benefits of 1-Year Lifestyle Modification Program on Exercise Capacity and Diastolic Function Among Coronary Artery Disease Men With and Without Type 2 Diabetes. Metab Syndr Relat Disord 2019, 17, 149–159. [Google Scholar] [CrossRef]
- Kamimura D, Loprinzi PD, Wang W, et al. Physical Activity Is Associated With Reduced Left Ventricular Mass in Obese and Hypertensive African Americans. Am J Hypertens 2017, 30, 617–623. [Google Scholar] [CrossRef]
- Himeno E, Nishino K, Nakashima Y, et al. Weight reduction regresses left ventricular mass regardless of blood pressure level in obese subjects. Am Heart J 1996, 131, 313–319. [Google Scholar] [CrossRef]
- Voulgari C, Pagoni S, Vinik A, et al. Exercise improves cardiac autonomic function in obesity and diabetes. Metabolism 2013, 62, 609–621. [Google Scholar] [CrossRef]
- Carbone S, Del Buono MG, Ozemek C, et al. Obesity, risk of diabetes and role of physical activity, exercise training and cardiorespiratory fitness. Prog Cardiovasc Dis 2019, 62, 327–333. [Google Scholar] [CrossRef]
- Pfeffer MA, Braunwald E. Ventricular remodeling after myocardial infarction. Experimental observations and clinical implications. Circulation 1990, 81, 1161–1172. [Google Scholar] [CrossRef] [PubMed]
- Cohn JN, Ferrari R, Sharpe N. Cardiac remodeling--concepts and clinical implications: a consensus paper from an international forum on cardiac remodeling. Behalf of an International Forum on Cardiac Remodeling. J Am Coll Cardiol 2000, 35, 569–582. [Google Scholar] [CrossRef] [PubMed]
- Taylor RS, Brown A, Ebrahim S, et al. Exercise-based rehabilitation for patients with coronary heart disease: systematic review and meta-analysis of randomized controlled trials. Am J Med 2004, 116, 682–692. [Google Scholar] [CrossRef] [PubMed]
- Koren MJ, Devereux RB. Mechanism, effects, and reversal of left ventricular hypertrophy in hypertension. Curr Opin Nephrol Hypertens 1993, 2, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Giallauria F, Cirillo P, Lucci R, et al. Left ventricular remodelling in patients with moderate systolic dysfunction after myocardial infarction: favourable effects of exercise training and predictive role of N -terminal pro-brain natriuretic peptide. Eur J Cardiovasc Prev Rehabil 2008, 15, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Giallauria F, Galizia G, Lucci R, et al. Favourable effects of exercise-based Cardiac Rehabilitation after acute myocardial infarction on left atrial remodeling. Int J Cardiol 2009, 136, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Haykowsky M, Scott J, Esch B, et al. A Meta-analysis of the effects of Exercise Training on Left Ventricular Remodeling Following Myocardial Infarction: Start early and go longer for greatest exercise benefits on remodeling. Trials 2011, 12, 92. [Google Scholar] [CrossRef] [PubMed]
- Giallauria F, Lorenzo AD, Pilerci F, et al. Reduction of N terminal-pro-brain (B-type) natriuretic peptide levels with exercise-based cardiac rehabilitation in patients with left ventricular dysfunction after myocardial infarction. Eur J Cardiovasc Prev Rehabil 2006, 13, 625–632. [Google Scholar] [CrossRef]
- Wen Y, Zhang X, Lan W, et al. Effects of Cardiac Rehabilitation on Cardiac Function and Quality of Life in Patients with Ischemic Nonobstructive Coronary Artery Disease and Diabetes Mellitus. BioMed Res Int 2022, 2022, 1–5. [Google Scholar]
- Zhang Y-M, Lu Y, Tang Y, et al. The effects of different initiation time of exercise training on left ventricular remodeling and cardiopulmonary rehabilitation in patients with left ventricular dysfunction after myocardial infarction. Disabil Rehabil 2016, 38, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Wisløff U, Støylen A, Loennechen JP, et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: a randomized study. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef] [PubMed]
- Pandey A, LaMonte M, Klein L, et al. Relationship Between Physical Activity, Body Mass Index, and Risk of Heart Failure. J Am Coll Cardiol 2017, 69, 1129–1142. [Google Scholar] [CrossRef] [PubMed]
- Pandey A, Allen NB, Ayers C, et al. Fitness in Young Adulthood and Long-Term Cardiac Structure and Function. JACC Heart Fail 2017, 5, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Kitzman DW, Nicklas B, Kraus WE, et al. Skeletal muscle abnormalities and exercise intolerance in older patients with heart failure and preserved ejection fraction. Am J Physiol Heart Circ Physiol 2014, 306, H1364–H1370. [Google Scholar] [CrossRef] [PubMed]
- Horwich TB, Fonarow GC, Clark AL. Obesity and the Obesity Paradox in Heart Failure. Prog Cardiovasc Dis 2018, 61, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Pandey A, Cornwell WK, Willis B, et al. Body Mass Index and Cardiorespiratory Fitness in Mid-Life and Risk of Heart Failure Hospitalization in Older Age. JACC Heart Fail 2017, 5, 367–374. [Google Scholar] [CrossRef]
- Pandey A, Patel M, Gao A, et al. Changes in mid-life fitness predicts heart failure risk at a later age independent of interval development of cardiac and noncardiac risk factors: The Cooper Center Longitudinal Study. Am Heart J 2015, 169, 290–297.e1. [Google Scholar] [CrossRef]
- Heran BS, Chen JM, Ebrahim S, et al. Exercise-based cardiac rehabilitation for coronary heart disease. In: The Cochrane Collaboration (ed) Cochrane Database of Systematic Reviews. Chichester, UK: John Wiley & Sons, Ltd, p. CD001800.pub2.
- Pandey A, Parashar A, Kumbhani DJ, et al. Exercise Training in Patients With Heart Failure and Preserved Ejection Fraction: Meta-Analysis of Randomized Control Trials. Circ Heart Fail 2015, 8, 33–40. [Google Scholar] [CrossRef]
- Davies EJ, Moxham T, Rees K, et al. Exercise training for systolic heart failure: Cochrane systematic review and meta-analysis. Eur J Heart Fail 2010, 12, 706–715. [Google Scholar] [CrossRef]
- Edwards JJ, O’Driscoll JM. Exercise Training in Heart failure with Preserved and Reduced Ejection Fraction: A Systematic Review and Meta-Analysis. Sports Med - Open 2022, 8, 76. [Google Scholar] [CrossRef] [PubMed]
- O’Connor CM, Whellan DJ, Lee KL, et al. Efficacy and Safety of Exercise Training in Patients With Chronic Heart Failure: HF-ACTION Randomized Controlled Trial. JAMA 2009, 301, 1439. [Google Scholar] [CrossRef] [PubMed]
- van Tol BAF, Huijsmans RJ, Kroon DW, et al. Effects of exercise training on cardiac performance, exercise capacity and quality of life in patients with heart failure: A meta-analysis. Eur J Heart Fail 2006, 8, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Sandri M, Kozarez I, Adams V, et al. Age-related effects of exercise training on diastolic function in heart failure with reduced ejection fraction: The Leipzig Exercise Intervention in Chronic Heart Failure and Aging (LEICA) Diastolic Dysfunction Study. Eur Heart J 2012, 33, 1758–1768. [Google Scholar] [CrossRef] [PubMed]
- Haykowsky MJ, Timmons MP, Kruger C, et al. Meta-analysis of aerobic interval training on exercise capacity and systolic function in patients with heart failure and reduced ejection fractions. Am J Cardiol 2013, 111, 1466–1469. [Google Scholar] [CrossRef]
- Hegde SM, Claggett B, Shah AM, et al. Physical Activity and Prognosis in the TOPCAT Trial (Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist). Circulation 2017, 136, 982–992. [Google Scholar] [CrossRef]
- Heizer J, Carbone S, Billingsley HE, et al. Left ventricular concentric remodeling and impaired cardiorespiratory fitness in patients with heart failure and preserved ejection fraction. Minerva Cardiol Angiol. Epub ahead of print September 2020. [CrossRef]
- Whelton SP, Chin A, Xin X, et al. Effect of aerobic exercise on blood pressure: a meta-analysis of randomized, controlled trials. Ann Intern Med 2002, 136, 493–503. [Google Scholar] [CrossRef]
- Sadoshima J, Izumo S. The cellular and molecular response of cardiac myocytes to mechanical stress. Annu Rev Physiol 1997, 59, 551–571. [Google Scholar] [CrossRef]
- Pearson MJ, Smart NA. Effect of exercise training on endothelial function in heart failure patients: A systematic review meta-analysis. Int J Cardiol 2017, 231, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Siasos G, Athanasiou D, Terzis G, et al. Acute effects of different types of aerobic exercise on endothelial function and arterial stiffness. Eur J Prev Cardiol 2016, 23, 1565–1572. [Google Scholar] [CrossRef] [PubMed]
- Ehsani AA, Biello DR, Schultz J, et al. Improvement of left ventricular contractile function by exercise training in patients with coronary artery disease. Circulation 1986, 74, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Belardinelli R, Georgiou D, Ginzton L, et al. Effects of Moderate Exercise Training on Thallium Uptake and Contractile Response to Low-Dose Dobutamine of Dysfunctional Myocardium in Patients With Ischemic Cardiomyopathy. Circulation 1998, 97, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Brehm M, Picard F, Ebner P, et al. Effects of exercise training on mobilization and functional activity of blood-derived progenitor cells in patients with acute myocardial infarction. Eur J Med Res 2009, 14, 393. [Google Scholar] [CrossRef] [PubMed]
- Febbraio MA, Pedersen BK. Muscle-derived interleukin-6: mechanisms for activation and possible biological roles. FASEB J 2002, 16, 1335–1347. [Google Scholar] [CrossRef]
- Thomas DP, McCormick RJ, Zimmerman SD, et al. Aging- and training-induced alterations in collagen characteristics of rat left ventricle and papillary muscle. Am J Physiol 1992, 263, H778–H783. [Google Scholar]
- Melo SFS, Fernandes T, Baraúna VG, et al. Expression of MicroRNA-29 and Collagen in Cardiac Muscle after Swimming Training in Myocardial-Infarcted Rats. Cell Physiol Biochem 2014, 33, 657–669. [Google Scholar] [CrossRef] [PubMed]
- Martinez DG, Nicolau JC, Lage RL, et al. Effects of Long-Term Exercise Training on Autonomic Control in Myocardial Infarction Patients. Hypertension 2011, 58, 1049–1056. [Google Scholar] [CrossRef]
- Malfatto G, Facchini M, Bragato R, et al. Short and long term effects of exercise training on the tonic autonomic modulation of heart rate variability after myocardial infarction. Eur Heart J 1996, 17, 532–538. [Google Scholar] [CrossRef]
- Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e563–e595. [Google Scholar]
- Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J 2016, 37, 2315–2381. [Google Scholar]
- Pelliccia A, Sharma S, Gati S, et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J 2021, 42, 17–96. [Google Scholar] [CrossRef] [PubMed]
- Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Hansen D, Dendale P, Coninx K, et al. The European Association of Preventive Cardiology Exercise Prescription in Everyday Practice and Rehabilitative Training (EXPERT) tool: A digital training and decision support system for optimized exercise prescription in cardiovascular disease. Concept, definitions and construction methodology. Eur J Prev Cardiol 2017, 24, 1017–1031. [Google Scholar]
Figure 1.
The pathway from left ventricular hypertrophy to heart failure.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



