
Submitted:
15 June 2023
Posted:
16 June 2023
You are already at the latest version
Abstract
Background: Myeloid sarcoma (MS), also known as granulocytic sarcoma or chloroma, is a rare disease entity characterized by the emergence of an extramedullary tumour which may be antecedent, coexisting or manifest secondarily to an ongoing malignancy of lymphoid origin. Owing to its low prevalence, scientific reports addressing this matter comprise mainly retrospective studies with a limited number of participants, rather low-quality research and only few case reports. Despite MS’s rarity, the need for enhancing diagnostic tools and refinement of therapeutic regimens is broadly recognised among physicians.
Case summary: In this case series, we present the clinical histories of two patients diagnosed with MS. The former (Case 1) exhibited MS of the sternum alongside chronic myeloid leukemia (CML), while in case of the latter (Case 2) MS was the initial manifestation of a current acute myeloid leukemia (AML). Regardless of treatment institution comprising chemotherapy (CHTH) and radiotherapy (RT), the patient afflicted by CML did eventually pass due to cardiorespiratory insufficiency secondary to an infection, whereas the second one is in clinical remission up to this date, that is 16 months since MS had been diagnosed. Furthermore, a comprehensive analysis of previously reported cases was conducted which involves MS in patients with AML and CML.
Conclusion: The objective of this report is to emphasize the heterogeneity among the clinical manifestations of MS, to underline the relevance of histopathological and molecular diagnostic tools in opting for the appropriate therapy and that, in spite of it occurring rather uncommonly, physicians should think of MS in presence of pathological masses in patients under risk of hematological malignancies.
Keywords:
myeloid sarcoma
; acute myeloid leukemia
; chronic myeloid leukemia
; chloroma
; granulocytic sarcoma
; case report
1. Introduction
According to WHO, MS presents as a distinctive tissue-based manifestation of AML, transformed myelodysplastic syndrome (MDS), MDS/myeloprofilerative neoplasms (MPN), or MPN [1]. However, there have been reports in which MS ensued without bone marrow (BM) involvement, in which case it is called isolated myeloid sarcoma [2]. Cases of newly occurring myeloid sarcoma should undergo a thorough investigation that includes cytogenetic and molecular analyses to ensure accurate classification and effective treatment planning. Approximately 70% of patients exhibit concordant molecular alterations in both myeloid sarcoma and concurrent bone marrow disease, implying a potential origin from a shared hematopoietic stem cell or precursor [3,4]. In some individuals with a morphologically normal BM, relevant gene mutations can be still detected, indicating the presence of a low-level clonal myeloid disease or clonal hematopoiesis within the bone marrow [3,5]. It has been found that there is a prevalence of males over females in patients affected by MS, of whom approximately 9% are at risk of developing AML or CML [6]. Due to its rarity and lack of prospective and randomised controlled studies, data concerning the prognosis is conflicting, and there is no consensus on the treatment. In addition to that, MS is a source of significant diagnostic burden, which results in frequent misdiagnosis with various malignancies, such as Non-Hodgkin’s Lymphoma (NHL), small round cell tumours, or thymoma, which significantly delays treatment institution [7]. MS can be interpreted variously, depending on its time of arising in regard to that of AML or CML. If it presents primarily or concomitantly, MS may be seen as a manifestation of an ongoing haematological malignancy outside of the BM. However, if it is secondary, it could be a sign of disease progression and development of resistance to therapy. As for the applied regimen, it is worth mentioning that it could undergo modifications over time because of mutations that may appear as the disease progresses. As a result, the initially administered medications become ineffective. Through an in-depth analysis of our cases and studies concerning MS in patients with AML or CML, we sought to provide further insight into both the diagnostic and therapeutic approaches for the management of patients afflicted by MS, and emphasise the fundamental role played by molecular testing in opting for the adequate, most efficacious therapy. Moreover, we explore whether MS occurs rather primarily or secondarily to myeloid malignancies, the most frequently affected sites, and how its arising may influence our proceedings.
2. Materials and Methods
We confirm that patients provided informed consent for both the procedures itself and the publication of the resulting data. To gather relevant information, an extensive literature search was conducted, encompassing publications up until June 2023. Various combinations of keywords, such as myeloid sarcoma, AML, CML, chloroma, and granulocytoma, were utilized. The search embraced databases, including PubMed, UpToDate, and Scopus. As a result, 54 papers were specifically selected for inclusion in our manuscript, as they closely relate to our study. Articles written in English language were included, while articles written in other languages were ruled out.
3. Case 1
A 71-year-old man was admitted to our clinic to assess a growing mass in the area of the sternum, 6 months following the diagnosis of CML treated with imatinib (based on a medical interview, the patient had not brought documentation). A thorax computed tomography (CT) scan revealed a pathological mass located in the soft tissues on the right side of the chest. Furthermore, a positron emission tomography (PET) confirmed its presence, besides disclosing segmental lysis and involvement of the manubrium of the sternum. (Figure 2) Blood testing showed moderate normocytic anemia, lymphopenia, a low reticulocyte count, and high LDH and D-dimer levels. In view of the clinical picture, a sample for pathology assessment was collected. (Figure 1) Microscopic examination revealed fibrous connective tissue covered by an infiltrate of cells with acidophilic cytoplasm and signs of angioinvasion. Immunohistochemical (IH) staining was positive for the following markers: CD45, CD34, CD117, CD15, MPO, Ki-67, CK Pan, and negative for CD3, CD20, PAX5, CD138, MUM1, S100, CD30. BM biopsy excluded its involvement. Hence, a diagnosis of CML blast crisis in the form of MS was made. At that time, BCR-ABL1 kinase domain sequencing revealed no mutations which may have resulted in kinase inhibitor resistance. Upon receiving the results of RQ-PCR testing showing b3a2 (p210) transcript levels of 5,891 (IS) corresponding to the absence of major molecular response (MMR), the patient was qualified for conformal radiotherapy (24 Gy in 12 fractions) in conjunction with dasatinib 140 mg/day.
In the following months, a major response to treatment was noticed both clinically, manifesting as a loss of tumor volume, and molecularly, as p210 transcript levels dropped below the threshold of deep molecular response (MR4). Nevertheless, the patient developed skin lesions and pleural effusion, which was confirmed by diagnostic imaging. 5 months following therapy institution, BCR-ABL1 p210 transcripts reached a level of 1,45 (IS). Further scrutiny revealed the presence of the T315I (c.944C>T) mutation, thus explaining the cause of disease progression and development of resistance to dasatinib. The patient was then qualified for being treated with ponatinib (45 mg/day), resulting in clinical and laboratory improvement, as 1 month into the new regimen p210 transcript level dropped, yet not below the MMR threshold. Due to a persistent presence of pleural effusion, flow cytometry upon sample collection was carried out, showing the presence of blasts positive for CD15, CD65, CD13, CD34, CD117, HLA-DR, CD33, CD38, CD7, and negative for CD19, and MPO. Furthermore, 50% of the blast cells have shown altered signaling for the ABL1 and BCR genes, of which:
- 43% had 4 fusion signals, 1 red signal for ABL1 (9q34) and 1 green for BCR (22q11);
- 4% had 3 fusion signals, 1 red signal for ABL1 (9q34) and 1 green for BCR (22q11);
- 3% had 2 fusion signals, 1 red signal for ABL1 (9q34) and 1 green for BCR (22q11).
In the context of the cytogenetic testing performed upon diagnosis, this result is proof of clonal evolution and disease progression. Correspondingly, a regimen consisting of DA 3+7 (daunorubicin 60 mg/m2 days 1-3, Ara-C 100 mg/m2 days 1-7) and ponatinib 45 mg/day was administered, leading to the patient reaching once more MR4 in RQ-PCR testing, with a concurrent resolution of dyspnea which was present at the moment of admission.
After 2 more months, disease progression was revealed by RQ-PCR, CT, BM biopsy, and the evolution of skin lesions. BCR-ABL1 kinase domain sequencing ruled out the presence of mutations, including T315I. Despite a satisfying response to reinduction chemotherapy following the FLAG-IDA protocol (fludarabine 30 mg/m2, Ara-C 2 g/m2 for 5 days, idarubicin 10 mg/m2 for 3 days, and G-CSF 5 µg/kg days 1-5 and until neutrophil recovery), the patient unfortunately died, having subsequently suffered from neutropenia and respiratory tract infection leading to cardiorespiratory insufficiency. The results of BCR-ABL kinase domain sequencing have been presented in Figure 3.
4. Case 2
A 50-year-old male patient arrived at our hospital’s Hematology Department with a yet uncertain diagnosis, owing to an ambiguous result of histopathological analysis of a mediastinal tumor sample. The first and only symptom was reported to be noticed a little over 1 month prior to the admission to our ward, and it consisted of an enlargement of the neck’s circumference. A thorax CT scan was carried out by a different clinic, revealing a mass located in the anterior mediastinum compressing the superior vena cava. Subsequently, the patient was referred to our hospital’s Department of Thoracic Surgery with symptoms of superior vena cava syndrome which were managed with dexamethasone. Then, tumour sampling was performed, whose first analysis resulted inconclusive, and he was transferred to our Department.
Laboratory testing showed moderate normocytic anemia with elevated LDH and D-dimer levels. As for the following diagnostic measures, we opted for PET-CT and BM biopsy. (Figure 5) The former confirmed the presence of a mass in the anterior mediastinum with no signs of liver, spleen, BM, or lymphonodal involvement, while the latter revealed two blast populations, of which the first was positive for Tdt+, CD34, CD33, CD123, CD38, CD7, HLA-DR, 45dim, and negative for CD117, while the second one resulted positive for Tdt, CD34, CD33, CD123, CD38, CD7, 45dim, and negative for HLA-DR and CD117. Further scrutiny comprising BM’s cytogenetic testing found the presence of chromosome 21 trisomy, while cerebrospinal fluid examination ruled out central nervous system involvement. A revision of the formerly collected tumor sample proved that the patient suffered from MS, and IH staining confirmed the cooccurrence of the same process both in the BM and anterior mediastinum. (Figure 4) According to the clinical picture, a diagnosis of MS as the primary manifestation of a coexisting AML was made.
Due to an initial refusal of therapy, the patient was administered treatment following the DAC protocol (daunorubicin 60 mg/m2 days 1-3, cladribin 5 mg/m2 days 1-5, Ara-C 200 mg/m2 days 1-7) 1 month after the diagnosis had been made. Despite a reduction in tumor volume and a lowering of blasts’ percentage in the BM, complete remission (CR) was not achieved. Therefore, we opted for a FLAG-IDA reinduction protocol (G-CSF 0,48 mg days 1-7, Ara-C 2 g/m2 days 2-6, fludarabine 30 mg/m2 days 2-6, idarubicin 8 mg/m2 days 4-6) concomitantly with gemtuzumab ozogamicin (GO) (5 mg i.v. in day 1) resulting from a considerable expression of the CD33 antigen on the surface of blast cells, and conformal radiotherapy (24 Gy in 12 fractions). The patient tolerated the regimen well, achieved CR, and was eligible for allogeneic peripheral blood stem cell transplantation (allo-PBSCT). Allo-PBSCT was delayed due to a gastrointestinal Salmonella spp. infection, which resolved upon therapy within a few days. Transplantation from a matched unrelated donor with Bu4Cy2Thymoglobuline conditioning was performed 8 months following the diagnosis with an unremarkable post-transplantation period.
Currently, at 8 months after allo-MUD-SCT and 16 months since the diagnosis was made, the patient remains in CR with minimal residual changes in PET-CT imaging (Figure 3B), chimerism levels ranging 99,54%-100%, and no viral reactivations being observed.
4. Discussion
MS is frequently associated with CML or AML [1], and occasionally it can be their first manifestation, preceding the diagnosis of an ongoing myeloid malignancy [53]. In a clinical setting, it may result challenging to think of MS owing to its rarity and uncharacteristic clinical appearance. Histological examination and IH staining are two essential modalities, which in case of MS usually reveal positive for MPO, CD34, and c-kit. In both of our patients they had a fundamental role in making the diagnosis and ascertaining whether the extramedullary neoplasm corresponded histologically to the process in the BM.
To the best of our knowledge, a total of 51 cases of MS in patients with AML or CML have been reported up to date considering English-language literature, which we presented in Table 1. Of these 51 cases, 7 of them concerned patients with CML, suggesting that MS occurs more frequently in the course of AML. The male to female ratio was 1:0,96. In terms of time MS’s time of arising, 18 cases were primary, 21 were secondary, and 12 - concomitant. Interestingly, every MS in CML was secondary, while in AML we can notice a prevalence of primary MS (n=18) over secondary (n=16) and cooccurring ones (n=12). Some of the most commonly affected sites were breast (n=4), lymph nodes (n=4), stomach (n=3), and the retro-orbital space (n=3). Bone involvement was observed in a total of 6 patients, and it included the temporal bone, maxilla, femur, thoracic spine and twice the cranial base. With respect to therapy, CHTH was by far the most utilized approach (n=31), in some instances in conjunction with surgical treatment (n=7). It was also the most effective therapeutic approach, achieving CR in 15/31 cases. RT was employed in 12 patients, of whom 9 received concomitant CHTH; its effectiveness was scarce, with CR achieved in only 3/12 cases. A less common, yet promising approach is allo-SCT, which was employed in 1/7 cases in MS with CML, and in 9/44 with MS and AML. CR was achieved in 5/10 cases including the one with CML, with an average follow-up period of 2,1 years ranging from 6 months to 5 years. An unusual method called microtransplantation was instituted by Zhang et al. [21] comprising HLA-mismatched G-CSF-mobilized donor peripheral blood stem-cell infusions following CHTH, with no graft-vs-host disease prophylaxis [54]. DP was observed in 19/51 cases, while PR was reported in 6/51. 19/51 patients succumbed, with an average follow-up period of 0,56 year, ranging from 10 days to 3 years.
Considering the information retrieved from the found articles and our case series, we reached a few conclusions. Based on available literature, it seems that patients with MS occurring in patients affected by AML are significantly more numerous than those with CML. Despite a claimed prevalence of MS in males over females of 1.2:1 [6], we discovered it to be closer to 1:1, at least in what concerns cases with coexisting AML or CML. An interesting finding is that considering the cited articles and our Case 1 patient, MS arised secondarily to CML in every instance, which strongly suggests that in the vast majority of patients with CML MS will manifest secondarily rather than primarily. In the Case 2 patient, MS’s manifestation preceded briefly the AML diagnosis, which is in line with the available data, where MS most frequently was primary to AML. As for the affected site, our cases present two extremely rare ones, as we found just one previous report of a patient suffering from mediastinal MS, and there have been none of MS of the sternum. Finally, it seems that the most frequently administered therapy was CHTH with concomitant RT in some instances, and surgical treatment if the mass results particularly pronounced and symptomatic. An approach to be considered is allo-SCT. Evidence coming from the analysed studies and our Case 2 patient, who is currently in CR 8 months after transplantation, suggests that allo-SCT can be seen as an effective, potentially curable treatment method. The inclusion of TKIs in patients suffering from MS with CML is reasonable, yet following BCR-ABL kinase domain sequencing in search of mutations that could potentially rule out some TKIs groups due to inefficacy. Whenever the TKI-based regimen loses its efficaciousness, we have to take into account that a BCR-ABL mutation might have occurred in course of the disease. However, it is important to note that MS can progress independently from the achievement of molecular response, manifesting as a growth of the tumour.
We are aware that due to very limited evidence we cannot provide enough proof supporting a particular therapy or diagnostic pathway that could be considered the gold standard. Due to a scarce prevalence of MS, no randomised controlled trials can be carried out. Consequently, case reports are of major value to physicians, providing resourceful data on MS’s clinical course in the context of instituted therapeutic approaches.
Supplementary Materials
not applicable.
Author Contributions
U.G., J.D. provided conceptualization; U.G., J.D. designed the methodology and performed validation; J.D. provided formal analysis; J.P., J.M., A.B. were responsible for investigation; J.P., J.M., A.B. performed data curation; U.G., M.S. provided writing and original draft preparation; J.D, K.Z., M.S. was in charge of supervision; U.G., A.B. were responsible for project administration; K.Z. provided histopathological expertise. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
not applicable.
Acknowledgments
not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
CARE Checklist (2016) statement
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to it.
References
- Khoury, J.D.; Solary, E.; Abla, O.; Akkari, Y.; Alaggio, R.; Apperley, J.F.; Bejar, R.; Berti, E.; Busque, L.; Chan, J.K.C.; et al. The 5th Edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia 2022 36:7 2022, 36, 1703–1719. [Google Scholar] [CrossRef]
- Goyal, G.; Bartley, A.C.; Patnaik, M.M.; Litzow, M.R.; Al-Kali, A.; Go, R.S. Clinical Features and Outcomes of Extramedullary Myeloid Sarcoma in the United States: Analysis Using a National Data Set. Blood Cancer J 2017, 7. [Google Scholar] [CrossRef]
- Werstein, B.; Dunlap, J.; Cascio, M.J.; Ohgami, R.S.; Fan, G.; Press, R.; Raess, P.W. Molecular Discordance between Myeloid Sarcomas and Concurrent Bone Marrows Occurs in Actionable Genes and Is Associated with Worse Overall Survival. J Mol Diagn 2020, 22, 338–345. [Google Scholar] [CrossRef]
- Greenland, N.Y.; Van Ziffle, J.A.; Liu, Y.C.; Qi, Z.; Prakash, S.; Wang, L. Genomic Analysis in Myeloid Sarcoma and Comparison with Paired Acute Myeloid Leukemia. Hum Pathol 2021, 108, 76–83. [Google Scholar] [CrossRef]
- Engel, N.W.; Reinert, J.; Borchert, N.M.; Panagiota, V.; Gabdoulline, R.; Thol, F.; Heuser, M.; Fiedler, W. Newly Diagnosed Isolated Myeloid Sarcoma-Paired NGS Panel Analysis of Extramedullary Tumor and Bone Marrow. Ann Hematol 2021, 100, 499–503. [Google Scholar] [CrossRef]
- Almond, L.M.; Charalampakis, M.; Ford, S.J.; Gourevitch, D.; Desai, A. Myeloid Sarcoma: Presentation, Diagnosis, and Treatment. Clin Lymphoma Myeloma Leuk 2017, 17, 263–267. [Google Scholar] [CrossRef]
- Yilmaz, A.F.; Saydam, G.; Sahin, F.; Baran, Y. Granulocytic Sarcoma: A Systematic Review. Am J Blood Res 2013, 3, 265. [Google Scholar]
- Nanote, V.A.; Mahajan, O.A.; Gaidhane, S.A.; Parve, S.D.; Raut, L. Chronic Myeloid Leukemia: Chronic Phase Presenting as Extramedullary Presentation. Cureus 2022, 14. [Google Scholar] [CrossRef]
- Ali, E.A.; Abu-Tineh, M.; Abdelrazek, M.; Petkar, M.; Karzoun, M.; Subahi, E.A.; Szabados, L.; Yassin, M.A. Myeloid Sarcoma Mimicking Dental Abscess in a Patient with Chronic Myeloid Leukemia: Diagnostic and Therapeutic Dilemma. Case Rep Oncol 2022, 15, 755–761. [Google Scholar] [CrossRef]
- Han, S.; Li, Y.; Niu, T.; Wang, X.; Li, Z.; Ren, X.; Gao, J. Granulocytic Sarcoma Causing Long Spinal Cord Compression: Case Report and Literature Review. J Spinal Cord Med 2022, 45, 481–485. [Google Scholar] [CrossRef]
- Zhang, Y.; Swoboda, D.M.; Grover, A.; Nodzon, L.; Zhang, L.; Pinilla-Ibarz, J. T315I-Mutated Myeloid Sarcoma. Leuk Res Rep 2019, 12. [Google Scholar] [CrossRef]
- Palejwala, A.H.; O’Connor, K. P.; Shi, H.; Villeneuve, L.; Scordino, T.; Glenn, C.A. Chronic Myeloid Leukemia Manifested as Myeloid Sarcoma: Review of Literature and Case Report. J Clin Neurosci 2019, 64, 269–276. [Google Scholar] [CrossRef]
- AI, D.; LIU, W.; LU, G.; PATEL, K.P.; CHEN, Z. Extramedullary Blast Crisis as Initial Presentation in Chronic Myeloid Leukemia with the E1a2 BCR-ABL1 Transcript: A Case Report. Mol Clin Oncol 2015, 3, 1319–1322. [Google Scholar] [CrossRef]
- Kwatra, K.S.; Prabhakar, B.R.; Arora, Y. Bilateral Granulocytic Sarcoma (Chloroma) of the Breast in CML in Blast Crisis: A Case Report. Indian J Pathol Microbiol 2004, 47, 66–68. [Google Scholar]
- Amiraian, D.; McDonough, M.; Geiger, X. Bilateral Myeloid Sarcoma of the Breast: A Case Report With Radiological and Pathological Correlation. Cureus 2022, 14. [Google Scholar] [CrossRef]
- Mullen, C.; Beverstock, S.; Roddie, H.; Campbell, V.L.; Al-Qsous, W. Myeloid Sarcoma of Uterine Cervix: A Case Report with Review of the Literature. Gynecol Oncol Rep 2022, 39, 100931. [Google Scholar] [CrossRef]
- Park, J.H.; Son, Y.; Hyon, J.Y.; Lee, J.Y.; Jeon, H.S. Relapsed Acute Myeloid Leukemia Presenting as Conjunctival Myeloid Sarcoma: A Case Report. BMC Ophthalmol 2022, 22. [Google Scholar] [CrossRef] [PubMed]
- Athukuri, P.; Khan, A.B.; Gadot, R.; Haque, M.; Lee, S.; Gallagher, K.K.; Mims, M.P.; Rivero, G.A.; Barbieri, A.; Patel, A.J.; et al. Myeloid Sarcoma of the Skull Base: A Case Report and Systematic Literature Review. Surg Neurol Int 2022, 13. [Google Scholar] [CrossRef]
- Taminishi-Katsuragawa, Y.; Shimura, Y.; Inoue, Y.; Matsumura-Kimoto, Y.; Tsukamoto, T.; Mizutani, S.; Kobayashi, T.; Takeda-Miyata, N.; Nishimura, A.; Takatsuka, K.; et al. Gastric Myeloid Sarcoma Mimicking a Scirrhous Gastric Cancer. Intern Med 2022, 61, 1231–1235. [Google Scholar] [CrossRef]
- Asawa, P.; Vusqa, U.; Vashistha, K.; Din, M.T.U.; Karna, R.; Chen, F.; Dutton, N.; Samhouri, Y.; Fazal, S. Polyserositis as a Unique Presentation of Isolated Myeloid Sarcoma: A Case Report. Anticancer Res 2022, 42, 3595–3599. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wang, S.; Wang, F.; Shen, Q.; Jia, Y. Microtransplantation for Myeloid Sarcoma: Two Case Reports. Leuk Res Rep 2022, 17, 100326. [Google Scholar] [CrossRef] [PubMed]
- Tuna, R.; Karaman, S.; Oktar, T.; Anak, S.; Doğan, Ö.; Ünüvar, A.; Tuğcu, D.; Bayramoğlu, Z.; Kılıç, S.Ç.; Çelik, A.İ.; et al. Bladder Granulocytic Sarcoma in a Child: Case Report and Literature Review. Turk J Pediatr 2022, 64, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Jiang, Y. Granulocytic Sarcoma of Cervix: A Rare Case Report. Medicine 2022, 101, E29419. [Google Scholar] [CrossRef] [PubMed]
- Shash, H.A.; Khairy, A.M. Successful Treatment of Pediatric Acute Myeloid Leukemia Presenting with Hyperbilirubinemia Secondary to Myeloid Sarcoma: A Case Report. Children (Basel) 2022, 9. [Google Scholar] [CrossRef]
- Wang, V.; Van Perre, K.; Pu, L.; Liu, Y.; Wang, J.; Choo, E.; Moyers, J.; Cao, H.; Lau, E. Concurrent Epstein Barr Virus-Associated Smooth Muscle Tumor and Myeloid Sarcoma of the Liver and Acute Myeloid Leukemia in a Patient Post Kidney Transplant: A Case Report and Review of the Literature. J Gastrointest Oncol 2022, 13, 3329–3335. [Google Scholar] [CrossRef]
- Cross, A.; Chajewski, O.S.; Rutland, C.; Smith, K.; Woodham, P.; Skipper, D.; Lindsey, K.G. Myeloid Sarcoma Diagnosed on Pleural Effusion Cytology: A Case Report and Literature Review. Diagn Cytopathol 2021, 49, E316–E319. [Google Scholar] [CrossRef]
- Gosavi, A.Y.; Puranik, A.; Agrawal, A.; Purandare, N.C.; Shah, S.; Rangarajan, V.; Thomas, A. Myeloid Sarcoma of the Prostatic Tissue Diagnosed on 18F-FDG PET/CT in Treated Case of Acute Myeloid Leukemia. Indian J Nucl Med 2021, 36, 193. [Google Scholar] [CrossRef]
- Huang, C.; Fei, S.; Yao, J.; Chen, P.; Luo, J.; Wang, Y.; Li, J.; Wang, W. Breast Myeloid Sarcoma Presenting as a Palpable Breast Lump after Allogeneic Stem Cell Transplantation for Acute Myelomonocytic Leukemia: A Rare Case Report. World J Surg Oncol 2021, 19. [Google Scholar] [CrossRef]
- Wu, K.; Zhang, X.; Zhang, B. Myeloid Sarcoma of the Pancreas: A Case Report and Literature Review. Medicine 2021, 100, E24913. [Google Scholar] [CrossRef]
- Thomson, A.; Timm, B.; Nazaretian, S.; Liodakis, P.; Bolton, D. Rare Presentation of Isolated Bilateral Testicular Myeloid Sarcoma: A Case Report. Urol Case Rep 2021, 36. [Google Scholar] [CrossRef]
- Liu, R.; Du, J.; Gao, L.; Liu, Y.; Liu, S. Myeloid Sarcoma of the Nasal Cavity in a 15-Month-Old Child: A Case Report. Medicine 2020, 99, e21119. [Google Scholar] [CrossRef]
- Hernández, E.M.P.; Vázquez, L.A.Z.; Herevia, A.E.J.; Ugarte, D.H.; Moreno, E.O. Intestinal Chloroma. Cureus 2020, 12. [Google Scholar] [CrossRef]
- Sun, X.; Rong, X.; Nie, H.; Yan, X. Isolated Retro-Orbital Granulocytic Sarcoma Relapse of Acute Myeloid Leukemia after Allogeneic Hematopoietic Stem Cell Transplantation: A Case Report. Eur J Ophthalmol 2020, 32, NP94–NP98. [Google Scholar] [CrossRef]
- Slusarenko da Silva, Y.; Naclério-Homem, M. da G. Myeloid Sarcoma on the Temporal Region before the Onset of the Acute Myeloid Leukemia: An Extremely Rare Case Report. Oral Maxillofac Surg 2020, 24, 251–254. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Sonia, F.; Hamadani, S.M.; Abbas, S.A. A Rare Case of Acute Cord Compression From Spinal Myeloid Sarcoma: A Complication of Acute Myeloid Leukemia. Cureus 2020, 12. [Google Scholar] [CrossRef]
- Pi, Y.; Wang, B.; Wang, L.; Ren, H. Polyserositis as a Primary Clinical Manifestation of CD7+ Acute Myelogenous Leukemia with Myeloid Sarcoma: A Case Report. Medicine 2020, 99, E23615. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Dadu, T.; Bhalla, V.P.; Malhotra, V. Myeloid Sarcoma of Bile Ducts Presenting as Obstructive Jaundice - A Case Report. Indian J Pathol Microbiol 2019, 62, 602–604. [Google Scholar] [CrossRef]
- Marwah, N.; Bhutani, N.; Budhwar, A.; Sen, R. Isolated Myeloid Sarcoma of the Temporal Bone: As the First Clinical Manifestation of Acute Myeloid Leukemia in a Patient of down’s Syndrome. Int J Surg Case Rep 2019, 58, 77–80. [Google Scholar] [CrossRef]
- Almalki, A.M.J.; Alotaibi, F.A.; Jabr, H.F.; Mastan, A.R. Unilateral Proptosis As An Initial Sign Of Acute Myeloid Leukemia In A Child: A Case Report. Int Med Case Rep J 2019, 12, 319–323. [Google Scholar] [CrossRef]
- Abdelnabi, M.H.; Almaghraby, A.; Saleh, Y.; ElSharkawy, E. Cardiac Chloroma or Cardiac Myeloid Sarcoma: Case Report. Echocardiography 2019, 36, 1594–1595. [Google Scholar] [CrossRef]
- Bubulac, L.; Bardaş, A.; Popa, D.C.; Didona Vasilache, E.; Ionescu, B.O.; Coriu, D.; Varady, Z.; Dobrea, C.-M. Breast Myeloid Sarcoma after Allogeneic Stem Cell Transplantation for Acute Myelomonocytic Leukemia-Case Report. Rom J Morphol Embryol 2019, 707–711. [Google Scholar] [CrossRef]
- Feng, Y.; Zhang, L.; Cheng, N.; Lai, W.; Chen, Y.; Liu, J. A Case of Granulocytic Sarcoma of the Lung in Acute Myeloid Leukemia. Clin Lab 2019, 65, 1355–1359. [Google Scholar] [CrossRef]
- Nguyen, R.; Sayar, H. Primary Myeloid Sarcoma of the Prostate: A Case Report and Literature Review. Case Rep Hematol 2018, 2018, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Khaja, M.; Omesh, T.; Niazi, M.; Shaikh, D.; Mudunuru, S.A.; Reyes, O.A.; Malik, S. Co-Occurrence of Myeloid Sarcoma of the Lymph Node and Acute Monocytic Myeloid Leukemia: A Case Report and Literature Review. Case Rep Oncol 2018, 11, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Siraj, F.; Kaur, M.; Dalal, V.; Khanna, A.; Khan, A.A. Myeloid Sarcoma: A Report of Four Cases at Unusual Sites. Ger Med Sci 2017, 15. [Google Scholar] [CrossRef]
- Huang, B.; You, P.; Zhu, P.; Du, Z.; Wu, B.; Xu, X.; Chen, Z. Isolated Duodenal Myeloid Sarcoma Associated with the CBFβ/MYH11 Fusion Gene Followed by Acute Myeloid Leukemia Progression: A Case Report and Literature Review. Oncol Lett 2014, 8, 1261. [Google Scholar] [CrossRef] [PubMed]
- Kini, S.; Amarapurkar, A.; Balasubramanian, M. Small Intestinal Obstruction with Intussusception Due to Acute Myeloid Leukemia: A Case Report. Case Rep Gastrointest Med 2012, 2012, 1–3. [Google Scholar] [CrossRef]
- Cash, T.; Becton, D.; Mian, A. Cardiac Myeloid Sarcoma: A Case Report and Review of Literature. J Pediatr Hematol Oncol 2011, 33. [Google Scholar] [CrossRef]
- Gadage, V.; Zutshi, G.; Menon, S.; Shet, T.; Gupta, S. Gastric Myeloid Sarcoma--a Report of Two Cases Addressing Diagnostic Issues. Indian J Pathol Microbiol 2011, 54, 832–835. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.H.; Zhang, R.; Li, Y. Granulocytic Sarcoma of Abdomen in Acute Myeloid Leukemia Patient with Inv(16) and t(6;17) Abnormal Chromosome: Case Report and Review of Literature. Leuk Res 2010, 34, 958–961. [Google Scholar] [CrossRef]
- Skeete, D.H.A.; Cesar-Rittenberg, P.; Jong, R.; Murray, S.K.; Colgan, T.J. Myeloid Sarcoma of the Vagina: A Report of 2 Cases. J Low Genit Tract Dis 2010, 14, 136–141. [Google Scholar] [CrossRef]
- Mneimneh, W.S.; Bonte, H.; Bernheim, A.; Martin, A. Myeloid Sarcoma of the Prostate Revealed by Urinary Retention: A Case Report. BMJ Case Rep 2009, 2009. [Google Scholar] [CrossRef] [PubMed]
- Shallis, R.M.; Gale, R.P.; Lazarus, H.M.; Roberts, K.B.; Xu, M.L.; Seropian, S.E.; Gore, S.D.; Podoltsev, N.A. Myeloid Sarcoma, Chloroma, or Extramedullary Acute Myeloid Leukemia Tumor: A Tale of Misnomers, Controversy and the Unresolved. Blood Rev 2021, 47. [Google Scholar] [CrossRef]
- Guo, M.; Chao, N.J.; Li, J.Y.; Rizzieri, D.A.; Sun, Q.Y.; Mohrbacher, A.; Krakow, E.F.; Sun, W.J.; Shen, X.L.; Zhan, X.R.; et al. HLA-Mismatched Microtransplant in Older Patients Newly Diagnosed With Acute Myeloid Leukemia: Results From the Microtransplantation Interest Group. JAMA Oncol 2018, 4, 54. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A - diffuse proliferation of pleomorphic blasts with irregular nuclear membrane. HE 400x magnification. B - Strong CD34 expression. CD34 stain 400x magnification.
Figure 1.
A - diffuse proliferation of pleomorphic blasts with irregular nuclear membrane. HE 400x magnification. B - Strong CD34 expression. CD34 stain 400x magnification.
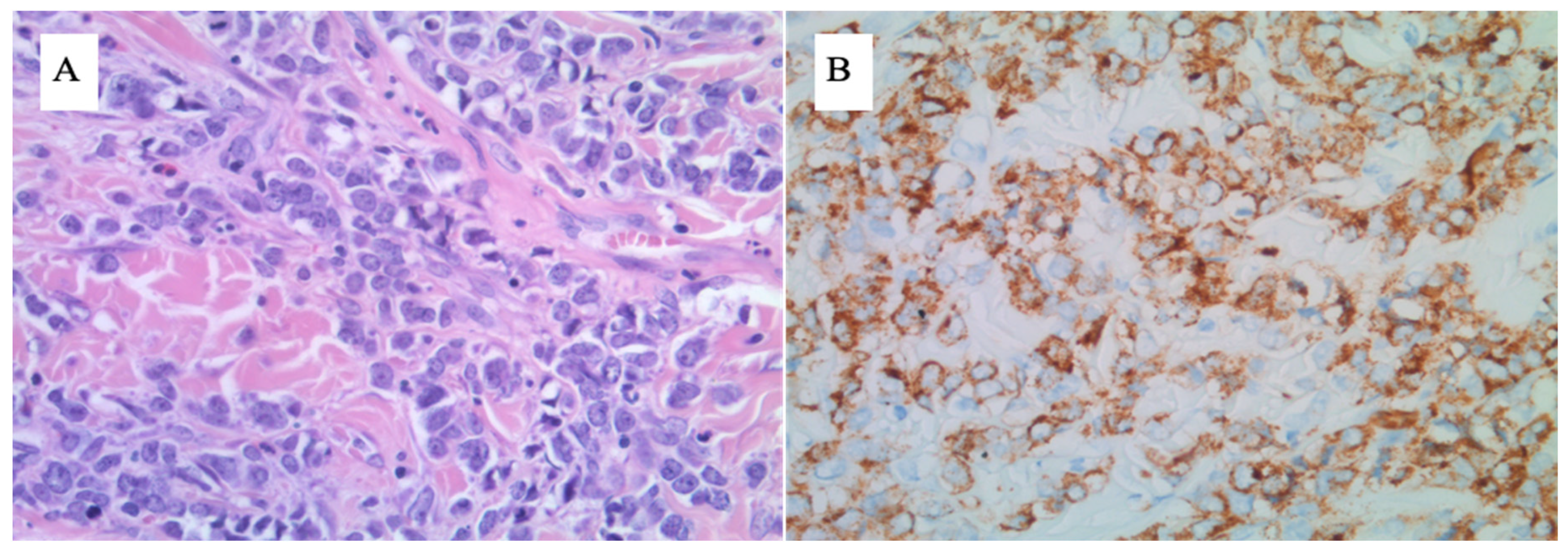
Figure 2.
Comparison of PET-CT scans upon diagnosis (A) and the best result achieved after treatment institution (B) related to Case 1.
Figure 2.
Comparison of PET-CT scans upon diagnosis (A) and the best result achieved after treatment institution (B) related to Case 1.
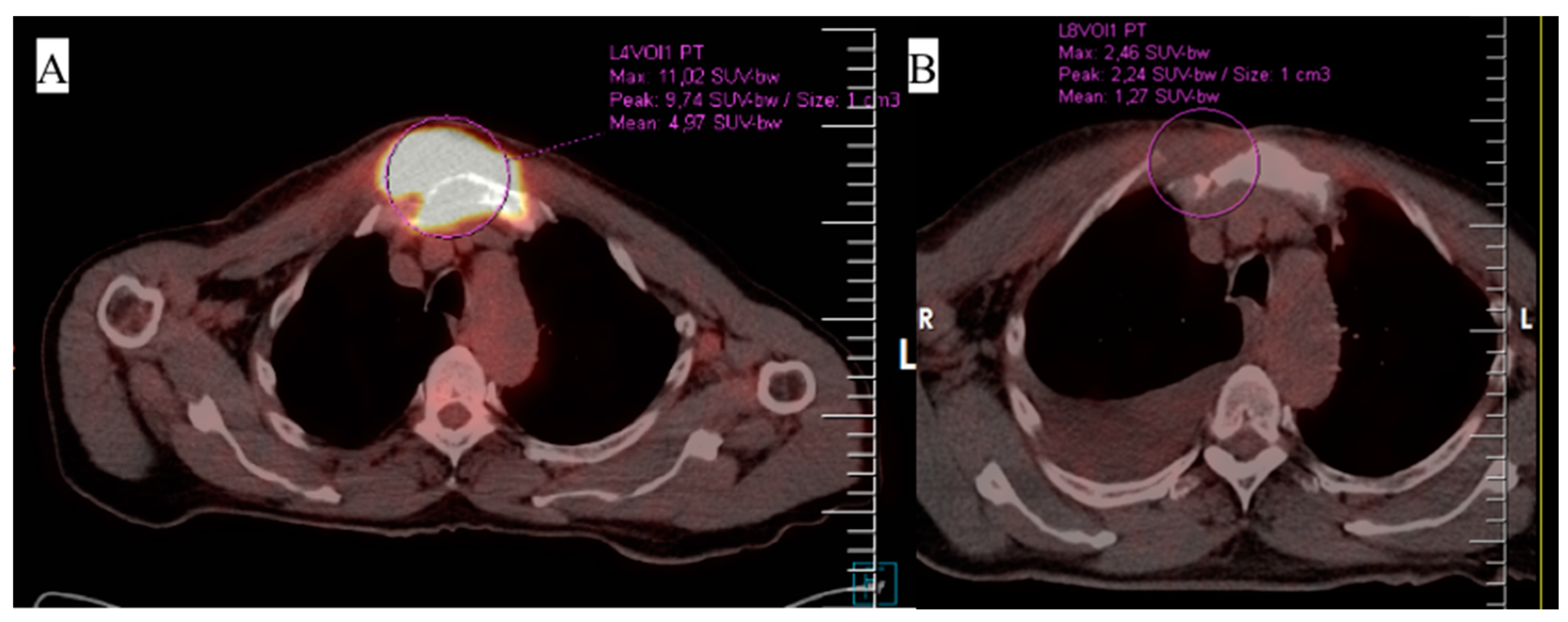
Figure 3.
Results of BCR-ABL1 kinase domain sequencing related to Case 1. Samples were collected from peripheral blood unless otherwise indicated. The blue line represents the MMR threshold, while the green one - MR4. Note: the patient has been administered dasatinib since 17.02.2022, ponatinib since 17.08.2022, and CHTH following the DA 3+7 protocol between 08-14.10.2022.
Figure 3.
Results of BCR-ABL1 kinase domain sequencing related to Case 1. Samples were collected from peripheral blood unless otherwise indicated. The blue line represents the MMR threshold, while the green one - MR4. Note: the patient has been administered dasatinib since 17.02.2022, ponatinib since 17.08.2022, and CHTH following the DA 3+7 protocol between 08-14.10.2022.
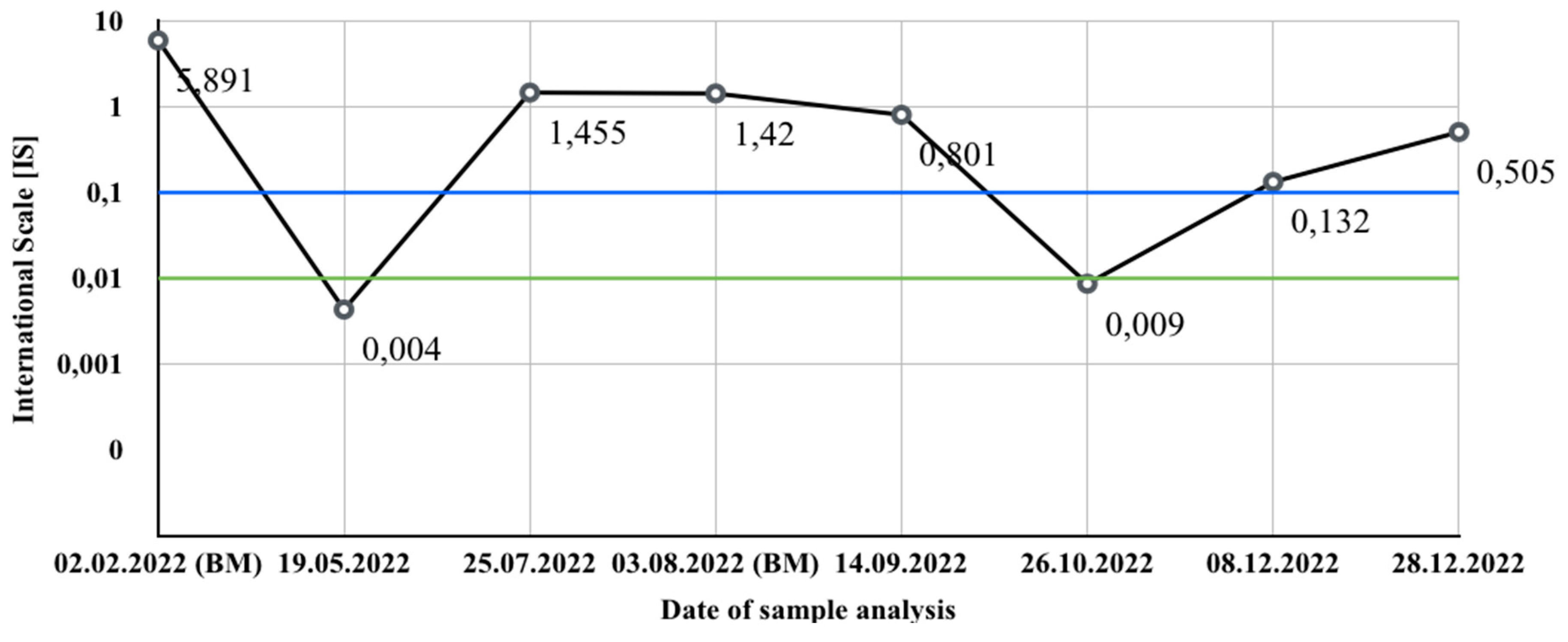
Figure 4.
A - diffuse infiltrate composed of monomorphic medium-sized blasts. Note strong crush artifact. HE 400x magnification. B - most cells weakly express CD79a. CD79a stain 400x magnification.
Figure 4.
A - diffuse infiltrate composed of monomorphic medium-sized blasts. Note strong crush artifact. HE 400x magnification. B - most cells weakly express CD79a. CD79a stain 400x magnification.
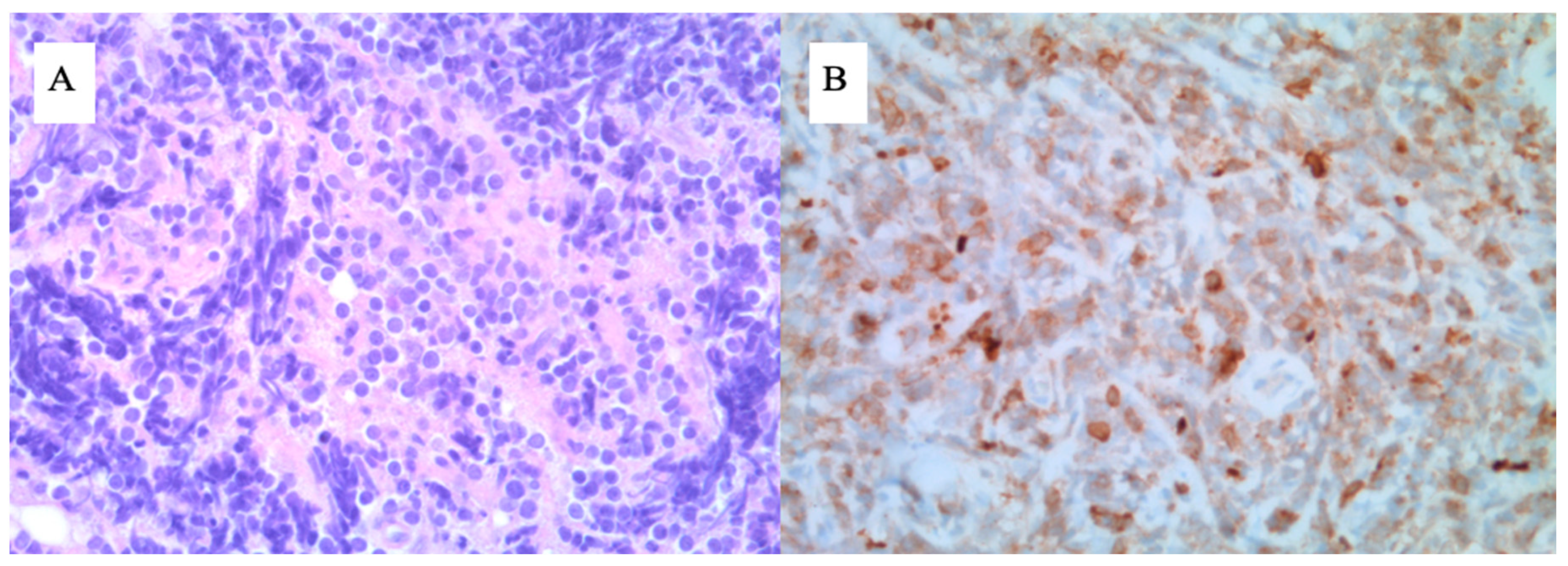
Figure 5.
Comparison of PET-CT scans upon diagnosis (A) and the best result achieved after treatment institution (B) related to Case 2.
Figure 5.
Comparison of PET-CT scans upon diagnosis (A) and the best result achieved after treatment institution (B) related to Case 2.
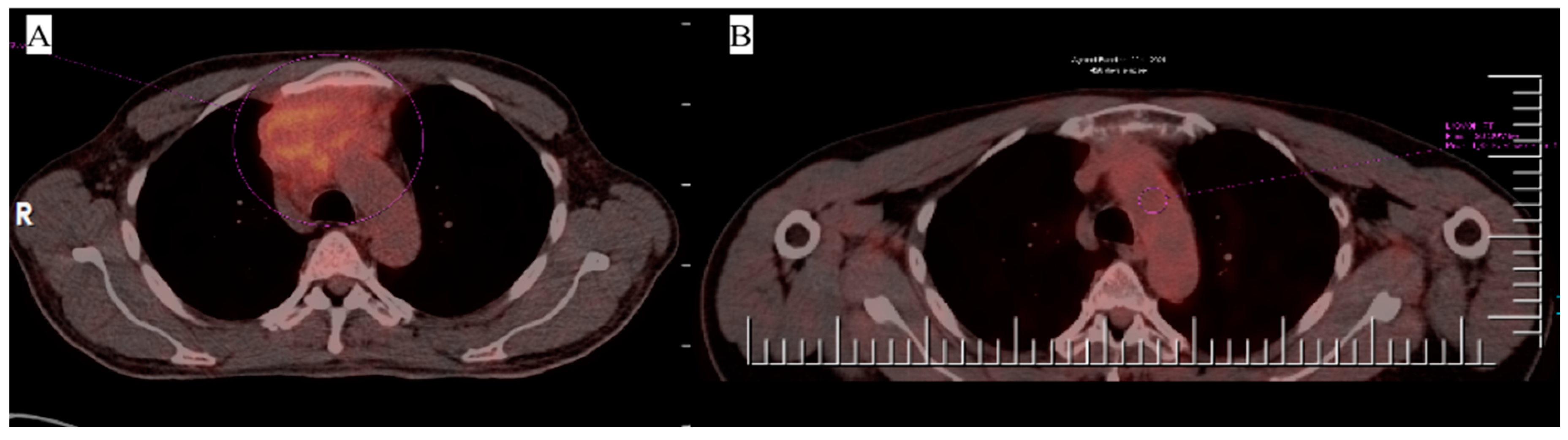

Table 1.
Case reports of patients affected by MS with myeloid malignancy.
| Year | Author | Age | Sex | Malignancy | Occurrence of MS in relation to leukemia | Location | Follow-up period | Patient status (dead/alive) | Therapy for MS | Clinical outcome of MS |
|---|---|---|---|---|---|---|---|---|---|---|
| 2022 | Nanote et al. [8] | 69 | F | CML | Secondary | Parotid gland | NR | alive | CHTH | NR |
| 2022 | Ali et al. [9] | 26 | M | CML | Secondary | Maxilla | NR | alive | CRT | PR |
| 2020 | Han et al. [10] | 37 | M | CML | Secondary | Spinal canal | 1 year | alive | Surgical, CHTH | CR |
| 2019 | Zhang et al. [11] | 21 | M | CML | Secondary | Femur | NR | alive | CHTH | NR |
| 2019 | Palejwala et al. [12] | 50 | F | CML | Secondary | Frontal lobe | 1 month | alive | Surgical, CRT | PR |
| 2015 | Ai et al. [13] | 23 | F | CML | Secondary | Lymph nodes | 4 years | alive | CHTH, allo-SCT MRD | CR |
| 2004 | Kwatra et al. [14] | 35 | F | CML | Secondary | Breast | N/a | N/a | N/a | N/a |
| 2022 | Amiraian et al. [15] | 63 | F | AML | Secondary | Breast | NR | dead | None (passed before therapy) | DP |
| 2022 | Mullen et al. [16] | 26 | F | AML | Primary | Uterine cervix | 18 months | alive | CHTH, allo-SCT MRD | CR |
| 2022 | Park et al. [17] | 50 | M | AML | Secondary | Conjuctiva | 3 years | alive | CRT, allo-SCT | CR |
| 2022 | Athukuri et al. [18] | 30 | M | AML | Secondary | Cranial base | 8 months | alive | Surgical, CHTH | PR |
| 2022 | Taminishi-Katsuragawa et al. [19] | 66 | M | AML | Concomitant | Stomach | NR | alive | CHTH | CR |
| 2022 | Asawa et al. [20] | 20 | M | AML | Primary | Upper lobe of the left lung, Mediastinum | 6 months | alive | CHTH, allo-SCT | CR |
| 2022 | Zhang et al. [21] | 38 | F | AML | Primary | Lymph nodes | 5,5 years | alive | CHTH, microtransplantation[54] | DP |
| 2022 | Zhang et al. [21] | 26 | F | AML | Concomitant | Cranial base, parapharyngeal space | 6 years | alive | CHTH, microtransplantation[54] | CR |
| 2022 | Tuna et al. [22] | 12 | F | AML | Concomitant | Bladder | 5 years | alive | CRT, surgical, allo-SCT MUD | CR |
| 2022 | Ye et al. [23] | 45 | F | AML | Primary | Uterine cervix | 1 year | alive | Surgical, CHTH | CR |
| 2022 | Shash et al. [24] | 4 | M | AML | Primary | Retroperitoneum | 4 years | alive | CHTH | CR |
| 2022 | Wang et al. [25] | 23 | F | AML | Concomitant | Liver | NR | dead | CHTH | CR |
| 2021 | Cross et al. [26] | 45 | M | AML | Primary | Heart, Pancreas | NR | alive | CHTH | PR |
| 2021 | Gosavi et al. [27] | 27 | M | AML | Secondary | Prostate | 6 months | dead | CRT, allo-SCT | DP |
| 2021 | Huang et al. [28] | 34 | F | AML | Secondary | Breast | 1 year | dead | CHTH, allo-SCT MMRD | DP |
| 2021 | Wu et al. [29] | 32 | F | AML | Secondary | Pancreas | NR | alive | CHTH | PR |
| 2021 | Thomson et al. [30] | 67 | M | AML | Primary | Testicles | NR | alive | CHTH | CR |
| 2020 | Liu et al. [31] | 15 months | M | AML | Primary | Nasal cavity | 2 years | alive | Surgical, CHTH | CR |
| 2020 | Hernández et al. [32] | 22 | F | AML | Concomitant | Intestine | 12 days | dead | Surgical | DP |
| 2020 | Sun et al. [33] | 37 | M | AML | Secondary | Retro-orbital space | 6 months | dead | RT, allo-SCT | DP |
| 2020 | Slusarenko da Silva et al. [34] | 29 | M | AML | Primary | Temporal region | N/a | N/a | N/a | N/a |
| 2020 | Kumar et al. [35] | 64 | F | AML | Secondary | Thoracic spine | NR | dead | CRT | DP |
| 2020 | Pi et al. [36] | 30 | F | AML | Concomitant | Lymph node | 4 months | dead | CHTH | DP |
| 2019 | Agarwal et al. [37] | 72 | F | AML | Primary | Bile ducts | 2 months | dead | Surgical | DP |
| 2019 | Marwah et al. [38] | 2 | M | AML | Primary | Temporal bone | NR | alive | CHTH | CR |
| 2019 | Almalki et al. [39] | 1 | M | AML | Concomitant | Retro-orbital space | NR | alive | CHTH | N/a |
| 2019 | Abdelnabi et al. [40] | 70 | M | AML | Secondary | Left cardiac ventricle | NR | dead | CRT | DP |
| 2019 | Bubulac et al. [41] | 30 | F | AML | Secondary | Breast | 3 years | dead | CRT, allo-SCT MRD | DP |
| 2019 | Feng et al. [42] | 56 | M | AML | Secondary | Lung | N/a | N/a | CHTH | CR |
| 2018 | Nguyen et al. [43] | 73 | M | AML | Primary | Prostate | NR | alive | Surgical, CHTH | PR |
| 2018 | Khaja et al. [44] | 29 | F | AML | Concomitant | Lymph node | NR | alive | CHTH | NR |
| 2017 | Siraj et al. [45] | 38 | M | AML | Primary | Nasal cavity | NR | N/a | CHTH | N/a |
| 2017 | Siraj et al. [45] | 11 | M | AML | Primary | Retro-orbital space | 18 months | alive | CRT | CR |
| 2017 | Siraj et al. [45] | 49 | M | AML | Primary | Brain | 6 months | dead | Surgical, CHTH | DP |
| 2017 | Siraj et al. [45] | 52 | M | AML | Secondary | Peritoneum | NR | NR | NR | NR |
| 2014 | Huang et al. [46] | 58 | F | AML | Primary | Duodenum | NR | alive | CHTH | CR |
| 2012 | Kini et al. [47] | 25 | M | AML | Concomitant | Gastrointestinal tract | 10 days | dead | Surgical | DP |
| 2011 | Cash et al. [48] | 24 | F | AML | Secondary | Heart | NR | dead | CHTH, allo-SCT | DP |
| 2011 | Gadage et al. [49] | 35 | M | AML | Concomitant | Stomach | 10 months | dead | CHTH | DP |
| 2011 | Gadage et al. [49] | 25 | M | AML | Primary | Stomach | 15 days | dead | Surgical | DP |
| 2010 | Zhang et al. [50] | 16 | M | AML | Concomitant | Abdomen | NR | alive | CHTH | CR |
| 2010 | Skeete et al. [51] | 77 | F | AML | Primary | Vagina | 5 months | dead | RT | DP |
| 2010 | Skeete et al. [51] | 36 | F | AML | Secondary | Vagina | 5 months | dead | RT | DP |
| 2009 | Mneimneh et al. [52] | 65 | M | AML | Concomitant | Prostate | 3 weeks | dead | Surgical, CHTH | DP |
Abbreviations: CHTH - chemotherapy, CRT - chemoradiotherapy, RT - radiotherapy, allo-SCT - allogeneic stem cell transplantation, MUD - matched unrelated donor, MRD - matched related donor, MMRD - mismatched related donor, DP - disease progression, CR - complete remission, PR - partial response, N/a - not available, NR - not reported.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



