
Submitted:
15 June 2023
Posted:
15 June 2023
You are already at the latest version
Abstract
We sought to evaluate the effects of non-surgical periodontal treatment (NSPT) on periodontal clinical parameters, systemic blood pressure (BP) and plasma levels of systemic inflammation markers in patients with combined refractory arterial hypertension (RAH) and stage III grade B periodontitis. Twenty-seven participants with RAH and periodontitis received NSPT. The analyzed clinical parameters were probing depth (PD), clinical attachment level (CAL), bleeding on probing (BOP), and plaque index (PI). An assessment was performed for systemic BP, complete blood count, coagulogram, creatinine measurement, C-reactive protein (CRP), glycated hemoglobin, cholesterol, glutamic oxaloacetic transaminase, glutamate pyruvic transaminase, waist-hip ratio, and body mass index. In the follow-up period, twenty-two patients were evaluated at baseline and after 90 and 180 days. The data were submitted to statistical analysis (α=0.05%). As expected, the clinical results showed a significant improvement in the percentages of PI, BOP, PD and CAL, which were statistically significant at 90 and 180 days (p<0.0001). Importantly, NSPT significantly reduced the blood level of CRP (p<0.02). However, no significant reduction in BP parameters was noted in the evaluated follow-up periods. NSPT, despite the benefits in periodontal clinical parameters, reduced the plasma level of CRP but not the BP in patients with combined RAH and periodontitis.
Keywords:
periodontitis
; periodontal disease
; hypertension
; dental scaling
; clinical trial
1. Introduction
Arterial hypertension (AH), a complex multifactorial clinical condition, is characterized by an elevation of blood pressure at levels ≥ 140 and 90 mmHg [1]. It is estimated that 31.1% of the global population are diagnosed with AH [2]. Cardiovascular diseases (CVD) have persisted as the leading causes of death worldwide and significantly contribute to loss of health and excess health system costs [3]. High systolic blood pressure (SBP) rests the foremost changeable risk factor globally for attributable cardiovascular deaths, accounting for 11.3 million deaths overall in 2021 [4]. To date, the mechanisms that can fully explain the increase in blood pressure (BP) is not totally elucidated [5]. Refractory arterial hypertension (RAH) is defined as an increase in BP in patients using three or more antihypertensive medications, including diuretics [6].
Periodontitis is a multifactorial chronic inflammatory disease associated with a dysbiotic biofilm and characterized by the progressive destruction of supporting periodontal tissues [7]. Dysbiosis results from inflammation-mediated microbial succession in periodontitis, in which disease-related species appear over time in the periodontal pocket [8]. Periodontitis is one of the most common chronic inflammatory conditions with a prevalence rate around 50% [9], in which the prevalence of its severe form account for 11% of the global population, affecting approximately 734 million people worldwide [10]. Periodontitis is considered the sixth most common epidemic disease globally [11], and the leading cause for teeth loss in the adult population [12]. Moreover, periodontitis has been considered as a risk factor for other chronic inflammatory diseases, such as cardiovascular inflammation and endothelial dysfunction [13, 14], rheumatoid arthritis [15, 16], and diabetes mellitus [17, 18] . Therefore, if a causal relationship could be shown, periodontitis would be associated with an increasing overall burden of hypertension and other non-communicable chronic diseases, and oral health assessment and management of oral inflammation could have an essential role in preventing hypertension and its complications [11]. Despite the current understanding regarding the effect of periodontitis on RAH, the nature of this association is still poorly understood.
Several cohort studies have associated periodontitis with hypertension [19, 20], while others have pointed to the relationship between periodontitis and the risk of AH [21-23]. In a recent systematic review, Munoz Aguilera et al. (2020) have suggested a linear association between periodontitis and the risk of AH showing that periodontitis diagnosis increased likelihood of AH occurrence (OR = 1.68). Patients with periodontitis exhibited higher mean of SBP and diastolic blood pressure (DBP) when compared with non-periodontitis patients in prospective studies. Of importance, 5 out 12 interventional studies confirmed a reduction in blood pressure levels following periodontal therapy, ranging from 3 to 12.5 mmHg of SBP and from 0 to 10 mmHg of DBP [24]. These findings parallel observation made by previous studies showing that patients subjected to non-surgical periodontal treatment (NSPT) showed improved periodontal clinical parameters and reduced plasma levels of inflammatory markers [25-28].
Vidal et al. (2011) found that periodontitis is a risk indicator for hypertensive patients, and there are indications that systemic inflammation is associated with both conditions [29]. A recent study tested the association of periodontal inflammation and bleeding on probing (BOP) using the NHANES III database [30]. Compared to no inflammation, severe periodontal inflammation and gingival bleeding were associated with 43% and 32% higher odds of high/uncontrolled BP (≥130/80 mmHg), and with higher SBP by approximately 4 and 5 mmHg, respectively. They concluded that local inflammation might contribute to the inflammatory burden to mediate this association.
Since there is still limited evidence suggesting that successful NSPT can improve systemic BP post-treatment in RAH patients [25-27], we hypothesize that NSPT in RAH patients would enhance the control of BP and a reduction in the plasma levels of systemic inflammatory markers. Therefore, the objective of this study was to clinically evaluate the effect of NSPT on clinical periodontal parameters, systemic BP and the plasma levels of systemic inflammation markers in patients with RAH and stage III, grade B periodontitis.
2. Materials and Methods
2.1. Study Population
A prospective, interventional cohort clinical study was developed and performed in a single-center with follow-ups of 90 and 180 days. The study was carried out between August 2019 and May 2021. This study was approved by the Human Research Ethics Committee of the Dentistry School of Araçatuba (CAAE 14338819.5.0000.5420) and was registered with the Brazilian Registry of Clinical Trials (Registration Number: RBR-9d78qy). The report follows the rules of the TREND Statement.
2.2. Participants
To be included in this study, participants had to meet the following inclusion criteria: a diagnosis of stages III and/or IV, grade B periodontitis [7] and be diagnosed with RAH ≥140mmHg and 90 mmHg for five years, using three or more antihypertensive medications [6].
Exclusion criteria were defined as: smokers or former smokers; individuals with anemia; active cancer; blood disorders; pregnancy; chronic kidney disease; type II diabetes mellitus (HbA1c>7.0); bacterial endocarditis [26]; having received some type of periodontal therapy in the last 6 months; current use of medication like antibiotics or anti-inflammatories; systemic conditions that affect periodontal progression or treatment [26]; individuals undergoing chemotherapy or head and neck radiotherapy; medical disorders that required antibiotic prophylaxis or that could influence treatment response; as well as alcoholism and illicit drug use.
The participants were recruited among patients at the Periodontics Clinic of the Araçatuba School of Dentistry - UNESP. First, they completed a full questionnaire about their general and oral health to assess whether they met the inclusion criteria. If positive, a clinical assessment was accompanied.
2.3. Primary and Secondary Clinical Outcomes
The primary outcomes evaluated in this study were the percentage of sites with clinical attachment level (CAL) gains and a reduction in the number of sites with probing depth (PD) ≥5 mm, the clinical parameters of PD, BOP, and plaque index (PI). The secondary outcomes evaluated in this study were BP and systemic inflammatory markers.
The clinical examination of all participants was performed by a single calibrated examiner (JVSR) at baseline and 90 and 180 days post-treatment. In the clinical examination, the visible PI (present or absent) was registered at the six sites of all teeth in the oral cavity. PD, BOP (present or absent) and CAL examinations were also performed at all six sites of each tooth in the oral cavity. These clinical parameters were obtained using a millimeter periodontal probe (PCPUNC-15, Hu-Friedy, Chicago, IL, USA).
2.4. Blood Pressure Analysis
In addition to the previous medical diagnosis of RAH, the BP of each participant was obtained through measurement with a non-invasive digital electronic sphygmomanometer (Digital Automatic Arm Blood Pressure Monitor - Omron), validated and calibrated. The BP measurement was performed by explaining the procedure and keeping the participants at rest for three to five minutes in a calm environment before verification. They were instructed not to talk during the measurement and not to have a full bladder. The examiner also asked about any physical exercise practiced less than sixty minutes before the measurement and ingestion of alcohol, coffee or food less than thirty minutes before BP measurement. The measurement was performed with the participant seated, legs uncrossed and feet flat on the floor, back leaning and with the arm positioned at heart level and supported with the palm facing up, clothes not constricting the upper arms. Measurements were taken on both arms, twice with a one-minute interval between each measurement, after which the highest value was used [1]. In addition, information was obtained about medications and dosages to control AH or other associated systemic diseases.
2.5. Bodyweight Analysis
Participants underwent analysis of the Waist-Hip Relationship (WHR = waist [cm] ÷ hip [cm]) using a tape measure, considering limit values for men and women at 0.85 and 0.90, respectively [31]. Furthermore, body mass index (BMI) values were obtained using anthropometric scale (digital anthropometric scale 200kg/100g, Welmy), through the values of weight (kg) and height (m), using the calculation BMI=Weight [Kg] / height2[m2] [32].
2.6. Blood Analysis
A specialized clinical analysis laboratory collected peripheral blood samples 7 days before the clinical evaluations. The requested tests were: Complete blood count, coagulogram, C-reactive protein (CRP), fasting and estimated blood glucose, glycated hemoglobin (HbA1c), total cholesterol, oxalacetic glutamic transaminase (OGT), pyruvic glutamic transaminase (PGT) and creatinine. The determination of positive CRP was characterized by levels equal to or above 6 mg/l, with indices below that threshold considered negative [33]. The above exams were requested at baseline and the 90 and 180 days follow-ups.
2.7. Experimental Design and Treatment Protocol
Fifteen days before treatment, the clinical periodontal examinations were performed (baseline), in which the parameters of PD, CAL, PI and BOP were noted. Immediately after this procedure, participants received detailed information about the etiology of periodontal disease and oral hygiene instructions (OHI), including toothbrushes, dental floss and interproximal brushes as needed. This instruction was repeated at each visit.
The initial treatment of periodontitis consists of the NSPT of subgingival instrumentation (SI) in combination with OHI [34]. The participants underwent an SI session of 1.5 hours, using Gracey and McCall manual curettes (Hu-Friedy Chicago, IL, USA), in line with the recommendations of the Guideline for Clinical Practice [34]. The SI procedures were performed by a single and experienced periodontist (JVSR).
One week after SI, all participants were visually inspected to assess possible undesirable signs and symptoms. Subsequently, follow-ups took place after 90 and 180 days, during which clinical exams were performed and laboratory tests requested, following the same parameters as in the initial exams. In these reassessments, supragingival plaque control and OHI were given according to each participant’s needs [26, 28].
2.8. Statistical Analysis
Sample Calculation
Based on previous studies [26, 28], sample size was calculated (Biostat 5.0, Mamirauá Institute, AM, Brazil) with a test power of 80% and the significance level set at 5%, to recognize a significant difference of 1 mm in PD. Considering a possible loss of 20%, the inclusion of 27 participants was recommended.
The demographic data, periodontal clinical parameters, complementary exams obtained from blood tests, physical exams and BP were submitted to descriptive and analytical statistical analysis using software package (GraphPad Prism versão 8.3.4, San Diego, CA, USA). The data showed a normal distribution after the normality test (Shapiro-Wilk). Periodontal clinical variables, blood tests, and physical and BP data were compared between periods (baseline, 90 and 180 days) and presented as means and standard deviation (SD). The data were then submitted to the ANOVA test, followed by Tukey’s posthoc test. The categorical variable CRP was compared using the chi-square test. All analyses were performed at a significance level of 5%.
A linear regression analysis was performed with the help of STATA 12.0 for Windows (Statistics/Data Analysis, Stata Corporation, College Station, TX, USA) to evaluate the effects of the different periods on the periodontal clinical parameters, biochemical and physical exams, and the BP parameters. Logistic regression analysis was then performed to evaluate the effect of different periods on periodontal clinical parameters (BoP, CAL ≥6 mm) and SBP and DBP. The results were binary (presence or not): (i) severity of the periodontal disease, with a predominance of deep pockets (CAL ≥6 mm or BOP ≥30% of the evaluated sites) [35]; or (ii) changes in BP levels (SBP ≥140 mmHg or DBP ≥90 mmHg) [1].
3. Results
3.1. Examiner Calibration
In the pre-experimental period, the examiner’s calibration procedures were performed through a clinical periodontal evaluation of 6 participants. PD and CAL parameters were obtained on two separate occasions (7-day intervals). Data were tabulated and submitted to the Kappa agreement test [36]. The obtained value of 0.88 is representative of a significant intra-examiner agreement.
3.2. Participants sample
Following the initial screening, 129 participants were recruited (Figure 1). Of these, 102 were excluded because did not meet the inclusion criteria. The remaining 27 patients were enrolled in the study presenting with RAH and stages III and IV grade B periodontitis.
Thirteen men and fourteen women aged 45 to 71 years underwent NSPT and were individually informed about the nature of the study and signed an informed consent form. During the follow-ups visit, five participants were excluded due to antibiotic use (2) and non-attendance at follow-ups (3). Thus, the final assessment in 90 and 180 days consisted of 22 participants (Figure 1).
Table 1 presents the demographic characteristics of the 22 participants who make up the study’s final sample, 10 men (45.45%) and 12 women (54.55%) with a mean age of 59.9 years. No statistically significant difference was observed in the distribution between men and women.
The antihypertensive drugs most used by the participants were Losartan (63.3%) and Atenolol (15.40%). Regarding diuretics, 45.45% of the participants used Hydrochlorothiazide, and 22.72% used Furosemide. Regarding anticoagulants, 18.18% used the drug Acetyl Salicylic Acid. To reduce blood cholesterol levels, 45.45% of the participants used simvastatin, and for glycemic control, 18.18% used Metformin.
3.3. Clinical Parameters
Regarding periodontal clinical parameters, there was no significant difference in the number of teeth between the evaluated periods. In the analysis of %PI, BOP, PD ≤4 mm, PD ≥5 mm, and CAL ≤3 mm, there was a statistically significant reduction at 90 and 180 days compared to baseline. Comparing the percentage of sites with a CAL of 4-5 mm (p=0.11) and CAL ≥6 mm (p=0.59), no significant difference between the evaluated periods was found (Table 2).
Table 3 presents the linear regression analysis of individuals in the different periods analyzed after NSPT (90 and 180 days) to verify its effect on the study variables. Similar to what is presented in Table 2, the main significant results were found in the periodontal clinical parameters, i.e. PI, BOP, PD ≥5 mm and CAL ≥6 mm presenting an inversely proportional decrease as the follow-up time increased. However, there was an increase in the percentage of sites with PD ≤4 mm, per evaluation periods, confirming the improvement of deep periodontal pockets after NSPT.
Table 4 presents the logistic regression analysis between the different periods. To categorize periodontitis according to the severity of gingival tissue inflammation, the subjects were divided according to the presence of BOP in ≥30% of the evaluated sites or the severity with a presence of CAL≥ 5 mm (Iwasaki et al., 2019). It was observed that for both the baseline versus 90 days and baseline versus 180 days comparisons, individuals were less likely to present BOP in ≥30% of sites (OR 0.02, 95% CI 0.002- 0.29, p=0.001; OR 0.05, 95%CI 0.009-0.26, p=0.000, respectively). Regarding CAL≥6 mm, no significant differences were found at 90 days (OR 0.54, CI 95%: 0.18–1.68, p=0.28), or 180 days (OR 0.61, CI 95%: 0.19–1.94, p=0.41).
3.4. Blood Pressure
In the analysis of systemic BP parameters, no statistically significant differences were observed in any variable (p>0.05). No significant reductions were observed at 90 and 180 days, when compared to baseline, in the data of SBP (p=0.28), DBP (p=0.39), mean arterial pressure (MAP; p=0.08) and differential pressure (p=0.09; Table 2). Statistically significant differences were not observed in systemic BP parameters in the different evaluated periods in the linear regression analysis (Table 3).
To assess systemic BP parameters, the participants were divided according to the changes found, SBP ≥140 mmHg or DBP ≥90 mmHg (Williams et al., 2018), but no statistically significant differences were found in SBP at 90 days (OR 0 .48, 95% CI: 0.15-1.61, p=0.24) and 180 days (OR 0.83, 95% CI: 0.26-2.65, p=0.75), or in the DBP at 90 days (OR 1.17, CI 95%: 0.34-1.02, p=0.79) and 180 days (OR 1.97, CI 95%: 0.59-6.63, p =0.27; Table 4).
3.5. Blood Analysis
All blood count and coagulogram parameters were within normal ranges (data not shown). The test results for HbA1c, fasting blood glucose, estimated blood glucose, total cholesterol, creatinine, OGT and PGT showed no statistically significant reduction in any follow-up period compared to the baseline (Table 2). In the categorical comparison between the periods, it was observed that after NSPT, there was a significant reduction in the inflammatory marker CRP (p=0.02; Table 2). Statistically significant differences were not observed in the blood biomarker exams in the different evaluated periods in the linear regression analysis (Table 3).
3.6. Bodyweight
The outcomes of physical examinations remained constant in all periods, without any significant differences in the data for waist-hip ratio (p=0.59) and BMI (p=0.98) between the evaluation periods (Table 2). Similar to what is presented in Table 2, statistically significant differences were not observed in physical exams in the different evaluated periods in the linear regression analysis (Table 3). This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
4. Discussion
The results of this prospective clinical study showed that NSPT reduced the systemic levels of CRP but did not result in any positive effect regarding the BP levels in patients with combined periodontitis and RAH. Similar to periodontitis, diabetes and hypertension share common risk factors (aging, smoking and unfavorable socioeconomic status). Thus, residual confounders can affect the degree of these associations. Importantly, this connection may also be driven by an association between BP changes and other undetected sources or chronic infections [24]. Periodontitis and hypertension are related to chronic immune dysfunction brought by periodontal inflammation [37].
Good periodontal health may be associated with better BP control during antihypertensive treatment [38]. The effects of NSPT in hypertensive individuals have been reported in a few studies [26-28, 39]. In our study, the NSPT of individuals with RAH proved to be beneficial during the 90 and 180-day evaluations. SI and OHI led to a significant reduction of PI, PD, BOP and deep pockets after 90 and 180 days. These residual pockets are an essential indicator of periodontitis persistence and a heightened risk of periodontal disease progression, which requires a repetition of NSPT or surgical treatment [40]. In the present study, a CAL gain was also observed in sites with CAL ≤3 mm in the 90 and 180 days periods, compared to the baseline. Such findings confirm that NSPT promotes significant improvements in periodontal clinical parameters [41].
In the logistic regression analysis, aimed at the categorization of periodontal disease according to its severity, it can be observed that at both assessment points, patients had lower chances of ≥30% sites with BOP (OR 0.02, 95%CI 0.002-0.29, p=0.00). These finds indicate that NSPT decreases the chances of generalized gingival inflammation in all experimental periods.
The identification of periodontitis as a possible risk factor for hypertension can be explained by some mechanisms [24]. Periodontitis is related to systemic inflammation, and its mediators include CRP, interleukin 6 (IL-6) and tumour necrosis factor-alpha (TNF-α), which can affect the endothelial function. Clinical evidence has shown that periodontitis affects the whole-body endothelial function, which may, in turn, affect hypertension [13, 14]. An experimental study in animals has demonstrated that the immune response to the common periodontal pathogen Porphyromonas gingivalis can cause elevated blood pressure, vascular inflammation and endothelial dysfunction [42].
CRP is elevated in hypertensive patients, being one of the determinants of systemic inflammation caused by AH [43]. Furthermore, periodontitis increases the levels of local and systemic inflammatory markers, in addition to causing changes in the neutrophil function. The latter disrupts the regulatory balance by reducing nitric oxide and induces increased IL-6, TNF-α and blood CRP levels [44]. This generates vascular changes and endothelial cell dysfunction [44]. Interestingly, the categorical variable CRP showed a statistically significant reduction in individuals with RAH at 90 and 180 days after NSPT. However, other studies have not observed a significant reduction in the plasma levels of inflammatory markers [45] in patients with periodontitis or healthy individuals [46]. Therefore, NSPT, leading to reduced clinical and systemic infection and inflammation, seems to improve endothelial function in patients with RAH.
The effects of periodontal treatment on the plasma levels of inflammatory markers are described in the literature. Some studies have shown that plasma and/or serum levels of IL-6, fibrinogen, CRP, other proteins and interleukins decrease after NSPT in individuals with CVD [47], coronary artery disease [48], in normotensive and hypertensive individuals [49], and in individuals with RAH [26, 28]. The evaluation periods varied between 1 and 6 months after periodontal treatment in the studies mentioned above.
Regarding the biochemical tests for total cholesterol, creatinine, OGT, and PGT after NSPT, it was observed that NSPT did not result in any beneficial effect. Furthermore, NSPT did not influence the levels of HbA1c, estimated glycemia and fasting glycemia in individuals with RAH. Some studies have demonstrated an improvement in the control of HbA1c levels in diabetic patients following NSPT [50, 51]. Therefore, these results demonstrated that other factors should be considered, such as the use of medicines to control blood glucose, dietary habits and physical exercise.
Our study did not show statistically significant reductions in the physical examinations of WHR and BMI after NSPT in individuals with RAH. The literature has indicated that obesity plays a role in developing AH and CVDs [52]. Some studies found an association between BMI and AH, which indicates that obese patients are at a higher risk of developing AH [53]. A significant association between SBP and BMI has also been observed in hypertensive individuals [32]. This higher rate of obesity may be related to one of the risk factors for the development of non-communicable diseases like AH and type 2 diabetes mellitus [54]. In addition, it can be observed that participants of this study with RAH were obese and, presented a high cardiac risk factor.
Subgingival periodontal bacteria levels were directly correlate with SBP and DBP and the prevalence of hypertension [55]. Another study demonstrated that systemic exposure to periodontal bacteria is related to hypertension [38]. Studies that evaluated the effect of NSPT on systemic BP are controversial [22, 25-28, 48, 49, 56]. Some studies have demonstrated a BP improvement after NSPT [25-27], whereas other studies did not show such improvements [28, 48, 49, 56]. In the present study, in the analysis of systemic BP variables, no significant reductions were observed after NSPT at 90 and 180 days compared to baseline.
Recent meta-analyses have shown that regular aerobic and aquatic exercises can significantly reduce SBP [57]. Pietropaoli et al. (2018) demonstrated in a clinical study that a combination of lifestyle adjustments and periodontal therapy could help control BP. Given these facts, it can be noted that other individual factors like antihypertensive drugs, lifestyle, or diet can interfere with systemic BP control in addition to the treatment of chronic inflammatory diseases. Such findings restate the limitation of the inference that periodontal treatment can directly or indirectly influence the control of AH [38]
This prospective interventional clinical study possesses some important caveats. One is the impossibility of controlling variables that can affect the control of systemic AH, such as changes in the use of antihypertensive drugs, diet or the individual’s emotional state. The present study was carried out during the Covid-19 pandemic, which may have significantly influenced the control of patients’ systemic BP due to the effects of stress, changes in eating and dietary habits, use of medication, a lack of medical control and a decrease in physical activity [58]. Finally, the lower number of patients included in this study is also a limitation of the experimental desing. Therefore, prospective clinical studies with a significant number of participants to perform a global follow-up of AH patients and to observe the benefits of NSPT in reducing the serum levels of inflammatory markers and systemic BP in individuals with RAH and long-term periodontitis are warranted.
5. Conclusions
Within the limits of this study, it can be concluded that NSPT effectively improved periodontal clinical parameters and reduced the plasma level of CRP but did not interfere with systemic BP parameters in individuals with combined stages III periodontitis and RAH.
Author Contributions
Conceptualization: JVSR, VGG and LHT; Methodology: JVSR, MMC, JPSF, RACR, TC, RSM, CMF, VGG and LHT; Formal analysis and investigation: JVSR, MMC, JPSF, RACR, RSM and TC; Writing - original draft preparation: JVSR, RSM and TC; Writing - review and editing: JVSR, MMC, JPSF, RACR, TC, RSM, CMF, VGG and LHT; Funding acquisition: VGG and LHT; Resources: CMF, VGG and LHT; Supervision: VGG and LHT.
Funding
This work has been carried out through funding by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brazil (CAPES), in the scope of Programa CAPES/Print - Funding code: 001(Process: 88887.194785/2018-00).
Institutional Review Board Statement
The study was conducted after obtaining ethical approval from the Human Research Ethics Committee of the Dentistry School of Araçatuba (CAAE 14338819.5.0000.5420). This study was registered in the Brazilian Registry of Clinical Trials (Registration Number: RBR-9d78qy). It was also performed in accordance with the principles of the modified Helsinki code for human clinical studies, as revised in 2013. The report follows the rules of the TREND Statement. Written informed consent was obtained from each participant.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.”.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Acknowledgments
The authors would like to thank the Periodontics Department at the Araçatuba School of Dentistry and the Center for Dental Assistance to Persons with Disabilities (CAOE) at the São Paulo State University UNESP.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Czopek, A.; Moorhouse, R.; Guyonnet, L.; Farrah, T.; Lenoir, O.; Owen, E.; van Bragt, J.; Costello, H.M.; Menolascina, F.; Baudrie, V.; et al. A novel role for myeloid endothelin-B receptors in hypertension. Eur. Hear. J. 2019, 40, 768–784. [Google Scholar] [CrossRef]
- Pimenta, E.; Gaddam, K.K.; Oparil, S. Mechanisms and Treatment of Resistant Hypertension. J. Clin. Hypertens. 2008, 10, 239–244. [Google Scholar] [CrossRef]
- Roth GA, Mensah GA and Fuster V. The Global Burden of Cardiovascular Diseases and Risks: A Compass for Global Action. J Am Coll Cardiol. 2020, 76, 2980–2981. [CrossRef]
- Razo, C.; Welgan, C.A.; Johnson, C.O.; McLaughlin, S.A.; Iannucci, V.; Rodgers, A.; Wang, N.; LeGrand, K.E.; Sorensen, R.J.D.; He, J.; et al. Effects of elevated systolic blood pressure on ischemic heart disease: a Burden of Proof study. Nat. Med. 2022, 28, 2056–2065. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.T.; Stefanescu, A.; He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef]
- Papapanou PN, Sanz M, Buduneli N, et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol. 2018, 45 Suppl 20, S162–S170.
- Van Dyke, T.E.; Bartold, P.M.; Reynolds, E.C. The Nexus Between Periodontal Inflammation and Dysbiosis. Front. Immunol. 2020, 11, 511. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Jepsen, S.; Jin, L.; Otomo-Corgel, J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: A call for global action. J. Clin. Periodontol. 2017, 44, 456–462. [Google Scholar] [CrossRef]
- Richards, D. Review finds that severe periodontitis affects 11% of the world population. Evidence-Based Dent. 2014, 15, 70–1. [Google Scholar] [CrossRef]
- Masi, S.; D’aiuto, F.; Deanfield, J. Cardiovascular prevention starts from your mouth. Eur. Hear. J. 2019, 40, 1146–1148. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Chavakis, T.; Lambris, J.D. Current understanding of periodontal disease pathogenesis and targets for host-modulation therapy. Periodontology 2000 2020, 84, 14–34. [Google Scholar] [CrossRef]
- Tonetti, M.S.; D’Aiuto, F.; Nibali, L.; Donald, A.; Storry, C.; Parkar, M.; Suvan, J.; Hingorani, A.D.; Vallance, P.; Deanfield, J. Treatment of Periodontitis and Endothelial Function. New Engl. J. Med. 2007, 356, 911–920. [Google Scholar] [CrossRef]
- D’Aiuto, F.; Gkranias, N.; Bhowruth, D.; Khan, T.; Orlandi, M.; Suvan, J.; Masi, S.; Tsakos, G.; Hurel, S.; Hingorani, A.D.; et al. Systemic effects of periodontitis treatment in patients with type 2 diabetes: a 12 month, single-centre, investigator-masked, randomised trial. Lancet Diabetes Endocrinol. 2018, 6, 954–965. [Google Scholar] [CrossRef]
- de Molon RS, Rossa C, Jr., Thurlings RM, et al. Linkage of Periodontitis and Rheumatoid Arthritis: Current Evidence and Potential Biological Interactions. Int J Mol Sci. 2019, 20.
- Gonzalez-Febles J and Sanz, M. Periodontitis and rheumatoid arthritis: What have we learned about their connection and their treatment? Periodontol 2000. 2021, 87, 181–203. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J.; Borgnakke, W.S. Diabetes as a potential risk for periodontitis: association studies. Periodontology 2000 2020, 83, 40–45. [Google Scholar] [CrossRef]
- Nibali, L.; Gkranias, N.; Mainas, G.; Di Pino, A. Periodontitis and implant complications in diabetes. Periodontology 2000 2022, 90, 88–105. [Google Scholar] [CrossRef]
- Morita, T.; Yamazaki, Y.; Fujiharu, C.; Ishii, T.; Seto, M.; Nishinoue, N.; Sasaki, Y.; Nakai, K.; Tanaka, H.; Kawato, T.; et al. Association Between the Duration of Periodontitis and Increased Cardiometabolic Risk Factors: A 9-Year Cohort Study. Metab. Syndr. Relat. Disord. 2016, 14, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Lee JH, Oh JY, Youk TM, et al. Association between periodontal disease and non-communicable diseases: A 12-year longitudinal health-examinee cohort study in South Korea. Medicine (Baltimore) 2017, 96, e7398. [CrossRef]
- Martin-Cabezas, R.; Seelam, N.; Petit, C.; Agossa, K.; Gaertner, S.; Tenenbaum, H.; Davideau, J.-L.; Huck, O. Association between periodontitis and arterial hypertension: A systematic review and meta-analysis. Am. Hear. J. 2016, 180, 98–112. [Google Scholar] [CrossRef]
- Czesnikiewicz-Guzik, M.; Osmenda, G.; Siedlinski, M.; Nosalski, R.; Pelka, P.; Nowakowski, D.; Wilk, G.; Mikolajczyk, T.P.; Schramm-Luc, A.; Furtak, A.; et al. Causal association between periodontitis and hypertension: evidence from Mendelian randomization and a randomized controlled trial of non-surgical periodontal therapy. Eur. Hear. J. 2019, 40, 3459–3470. [Google Scholar] [CrossRef]
- Del Pinto R, Pietropaoli D, Munoz-Aguilera E, et al. Periodontitis and Hypertension: Is the Association Causal? High Blood Press Cardiovasc Prev. 2020, 27, 281–289. [CrossRef] [PubMed]
- Munoz Aguilera E, Suvan J, Buti J, et al. Periodontitis is associated with hypertension: a systematic review and meta-analysis. Cardiovasc Res. 2020, 116, 28–39. [CrossRef] [PubMed]
- D’Aiuto, F.; Parkar, M.; Nibali, L.; Suvan, J.; Lessem, J.; Tonetti, M.S. Periodontal infections cause changes in traditional and novel cardiovascular risk factors: Results from a randomized controlled clinical trial. Am. Hear. J. 2006, 151, 977–984. [Google Scholar] [CrossRef] [PubMed]
- Vidal, F.; Cordovil, I.; Figueredo, C.M.S.; Fischer, R.G. Non-surgical periodontal treatment reduces cardiovascular risk in refractory hypertensive patients: a pilot study. J. Clin. Periodontol. 2013, 40, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Escobar Arregoces FM, Del Hierro Rada M, Saenz Martinez MJ, et al. Systemic inflammatory response to non-surgical treatment in hypertensive patients with periodontal infection. Medicine (Baltimore) 2021, 100, e24951. [CrossRef] [PubMed]
- Vidal, F.; Figueredo, C.M.S.; Cordovil, I.; Fischer, R.G. Periodontal Therapy Reduces Plasma Levels of Interleukin-6, C-Reactive Protein, and Fibrinogen in Patients With Severe Periodontitis and Refractory Arterial Hypertension. J. Periodontol. 2009, 80, 786–791. [Google Scholar] [CrossRef] [PubMed]
- Vidal, F.; Figueredo, C.; Cordovil, I.; Fischer, R. Higher prevalence of periodontitis in patients with refractory arterial hypertension: a case–control study. Oral Dis. 2011, 17, 560–563. [Google Scholar] [CrossRef] [PubMed]
- Pietropaoli, D.; Del Pinto, R.; Ferri, C.; Marzo, G.; Giannoni, M.; Ortu, E.; Monaco, A. Association between periodontal inflammation and hypertension using periodontal inflamed surface area and bleeding on probing. J. Clin. Periodontol. 2019, 47, 160–172. [Google Scholar] [CrossRef]
- Cao Q, Yu S, Xiong W, et al. Waist-hip ratio as a predictor of myocardial infarction risk: A systematic review and meta-analysis. Medicine (Baltimore) 2018, 97, e11639. [CrossRef]
- Paddmanabhan, P.; Gita, B.; Chandrasekaran, S. Association between chronic periodontitis and hypertension in South Indian population: A cross-sectional study. J. Pharm. Bioallied Sci. 2015, 7, 543–S547. [Google Scholar] [CrossRef]
- Kablak-Ziembicka A, Przewlocki T, Sokolowski A, et al. Carotid intima-media thickness, hs-CRP and TNF-alpha are independently associated with cardiovascular event risk in patients with atherosclerotic occlusive disease. Atherosclerosis. 2011, 214, 185–190. [CrossRef]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Berglundh, T.; Sculean, A.; Tonetti, M.S.; Consultants, E.W.P.A.M.; Consultants, T.E.W.P.A.M.; et al. Treatment of stage I–III periodontitis—The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47, 4–60. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki M, Kimura Y, Ogawa H, et al. Periodontitis, periodontal inflammation, and mild cognitive impairment: A 5-year cohort study. J Periodontal Res. 2019, 54, 233–240. [CrossRef] [PubMed]
- Theodoro, L.H.; Lopes, A.B.; Nuernberg, M.A.A.; Cláudio, M.M.; Miessi, D.M.J.; Alves, M.L.F.; Duque, C.; Mombelli, A.; Garcia, V.G. Comparison of repeated applications of aPDT with amoxicillin and metronidazole in the treatment of chronic periodontitis: A short-term study. J. Photochem. Photobiol. B: Biol. 2017, 174, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Hosadurga, R.; Soe, H.H.K.; Lim, A.T.P.; Adl, A.; Mathew, M. Association between tooth loss and hypertension: A cross-sectional study. J. Fam. Med. Prim. Care 2020, 9, 925–932. [Google Scholar] [CrossRef]
- Pietropaoli, D.; Del Pinto, R.; Ferri, C.; Wright, J.T., Jr.; Giannoni, M.; Ortu, E.; Monaco, A. Poor Oral Health and Blood Pressure Control Among US Hypertensive Adults. Hypertension 2018, 72, 1365–1373. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, A.B.; Razan, K.K.; Raed, A.D.M. Effect of surgical and non-surgical periodontal debridement on vascular thrombotic markers in hypertensives. J. Indian Soc. Periodontol. 2013, 17, 324–9. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A.; Almaghlouth, A.; Cionca, N.; Courvoisier, D.S.; Giannopoulou, C. Differential Benefits of Amoxicillin–Metronidazole in Different Phases of Periodontal Therapy in a Randomized Controlled Crossover Clinical Trial. J. Periodontol. 2015, 86, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Cobb, C.M. Clinical significance of non-surgical periodontal therapy: an evidence-based perspective of scaling and root planing. J. Clin. Periodontol. 2002, 29 (Suppl. 2), 22–32. [Google Scholar] [CrossRef]
- Czesnikiewicz-Guzik, M.; Nosalski, R.; Mikolajczyk, T.P.; Vidler, F.; Dohnal, T.; Dembowska, E.; Graham, D.; Harrison, D.G.; Guzik, T.J. Th1-type immune responses to Porphyromonas gingivalis antigens exacerbate angiotensin II-dependent hypertension and vascular dysfunction. Br. J. Pharmacol. 2018, 176, 1922–1931. [Google Scholar] [CrossRef]
- Yuan, M.; Wang, B.; Tan, S. Mecobalamin and early functional outcomes of ischemic stroke patients with H-type hypertension. Front. Public Heal. 2018, 64, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Munoz Aguilera E, Leira Y, Miro Catalina Q, et al. Is systemic inflammation a missing link between periodontitis and hypertension? Results from two large population-based surveys. J Intern Med. 2021, 289, 532–546. [CrossRef]
- Ide, M.; McPartlin, D.; Coward, P.; Crook, M.; Lumb, P.; Wilson, R. Effect of treatment of chronic periodontitis on levels of serum markers of acute-phase inflammatory and vascular responses. J. Clin. Periodontol. 2003, 30, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, K.; Honda, T.; Oda, T.; Ueki-Maruyama, K.; Nakajima, T.; Yoshie, H.; Seymour, G.J. Effect of periodontal treatment on the C-reactive protein and proinflammatory cytokine levels in Japanese periodontitis patients. J. Periodontal Res. 2004, 40, 53–58. [Google Scholar] [CrossRef]
- D’Isidoro, O.; Perrotti, V.; Hui, W.L.; Piattelli, A.; Iaculli, F.; Quaranta, A. The impact of non-surgical therapy of periodontal disease on surrogate markers for cardiovascular disease: A literature review. Am J Dent. 2019, 32, 191–200. [Google Scholar] [PubMed]
- Higashi, Y.; Goto, C.; Hidaka, T.; Soga, J.; Nakamura, S.; Fujii, Y.; Hata, T.; Idei, N.; Fujimura, N.; Chayama, K.; et al. Oral infection-inflammatory pathway, periodontitis, is a risk factor for endothelial dysfunction in patients with coronary artery disease. Atherosclerosis 2009, 206, 604–610. [Google Scholar] [CrossRef]
- Higashi, Y.; Goto, C.; Jitsuiki, D.; Umemura, T.; Nishioka, K.; Hidaka, T.; Takemoto, H.; Nakamura, S.; Soga, J.; Chayama, K.; et al. Periodontal Infection Is Associated With Endothelial Dysfunction in Healthy Subjects and Hypertensive Patients. Hypertension 2008, 51, 446–453. [Google Scholar] [CrossRef]
- Jain, A.; Jain, A.; Gupta, J.; Bansal, D.; Sood, S.; Gupta, S. Effect of scaling and root planing as monotherapy on glycemic control in patients of Type 2 diabetes with chronic periodontitis: A systematic review and meta-analysis. J. Indian Soc. Periodontol. 2019, 23, 303–310. [Google Scholar] [CrossRef]
- Baeza, M.; Morales, A.; Cisterna, C.; Cavalla, F.; Jara, G.; Isamitt, Y.; Pino, P.; Gamonal, J. Effect of periodontal treatment in patients with periodontitis and diabetes: systematic review and meta-analysis. J. Appl. Oral Sci. 2020, 28, e20190248. [Google Scholar] [CrossRef]
- Alpert, M.A.; Omran, J.; Mehra, A.; Ardhanari, S. Impact of Obesity and Weight Loss on Cardiac Performance and Morphology in Adults. Prog. Cardiovasc. Dis. 2014, 56, 391–400. [Google Scholar] [CrossRef]
- Zhao, D.; Qi, Y.; Zheng, Z.; Wang, Y.; Zhang, X.-Y.; Li, H.-J.; Liu, H.-H.; Zhang, X.-T.; Du, J.; Liu, J. Dietary factors associated with hypertension. Nat. Rev. Cardiol. 2011, 8, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Sanz M, Del Castillo AM, Jepsen S, et al. Periodontitis and Cardiovascular Diseases. Consensus Report. Glob Heart. 2020, 15, 1. [CrossRef]
- Desvarieux, M.; Demmer, R.T.; Jacobs, D.R.; Rundek, T., Jr.; Boden-Albala, B.; Sacco, R.L.; Papapanou, P.N. Periodontal bacteria and hypertension: the oral infections and vascular disease epidemiology study (INVEST). J. Hypertens. 2010, 28, 1413–1421. [Google Scholar] [CrossRef]
- Graziani, F.; Cei, S.; Tonetti, M.; Paolantonio, M.; Serio, R.; Sammartino, G.; Gabriele, M.; D’Aiuto, F. Systemic inflammation following non-surgical and surgical periodontal therapy. J. Clin. Periodontol. 2010, 37, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, Y.; Nogami, Y. The effect of regular aquatic exercise on blood pressure: A meta-analysis of randomized controlled trials. Eur. J. Prev. Cardiol. 2017, 25, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Munekawa, C.; Hosomi, Y.; Hashimoto, Y.; Okamura, T.; Takahashi, F.; Kawano, R.; Nakajima, H.; Osaka, T.; Okada, H.; Majima, S.; et al. Effect of coronavirus disease 2019 pandemic on the lifestyle and glycemic control in patients with type 2 diabetes: a cross-section and retrospective cohort study. Endocr. J. 2021, 68, 201–210. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of the study.
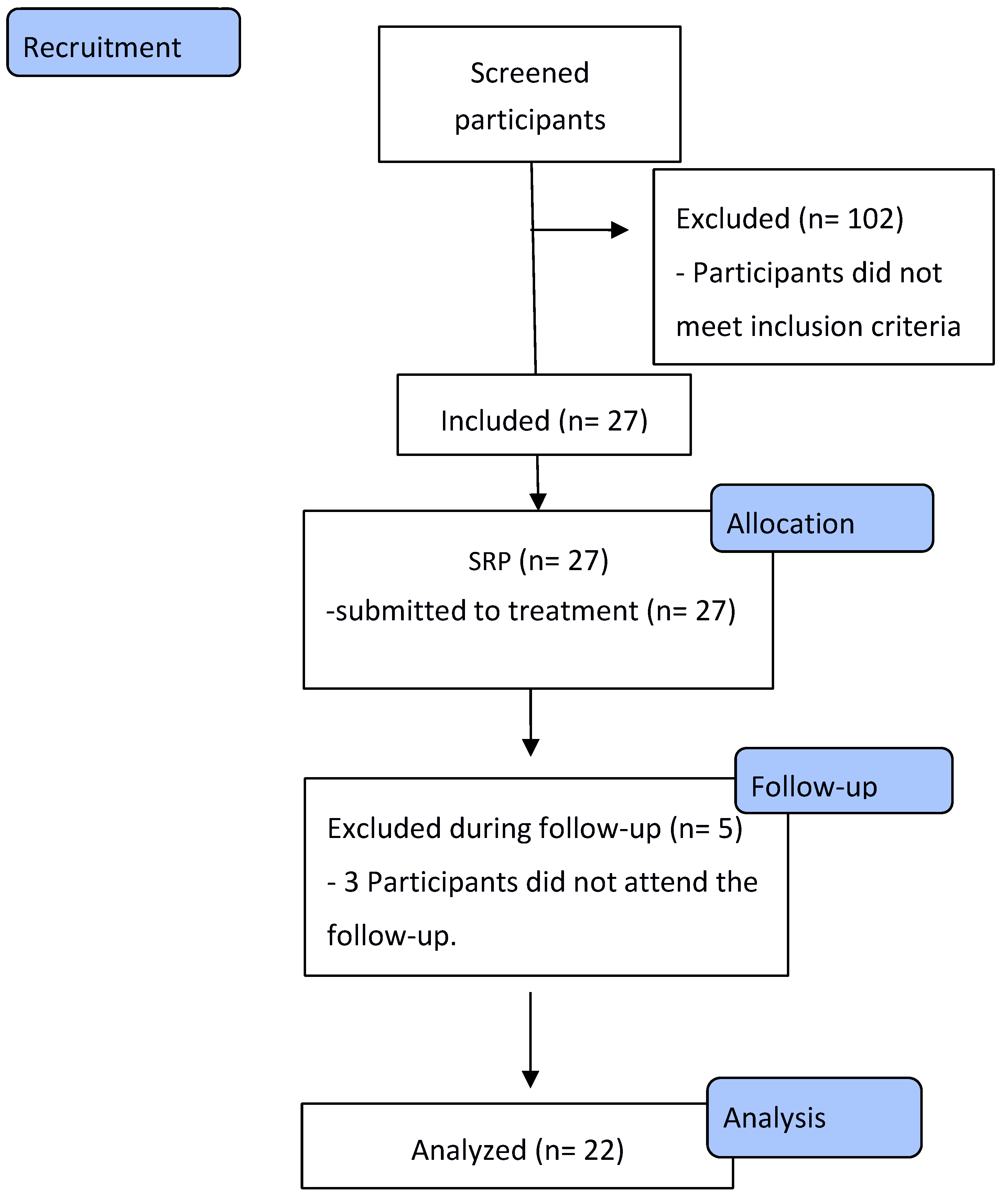

Table 1.
Demographic characteristics of the studied sample.
| Demographic characteristics | n= 22 |
|---|---|
| Age - mean (SD) | 59.9 (±8.2) |
| Sex – n, (%) | |
| Men | 10 (45.45%) |
| Women | 12 (54.55%) |
Table 2.
Comparison of periodontal clinical variables, results of biochemical tests and blood pressure parameters evaluated in the different evaluation periods.
Table 2.
Comparison of periodontal clinical variables, results of biochemical tests and blood pressure parameters evaluated in the different evaluation periods.
| Evaluated variables | Baseline n=22 |
90 days n=22 |
180 days n=22 |
p-value |
|---|---|---|---|---|
| Periodontal Clinical Parameters - Mean (SD) | ||||
| N° teeth | 22.9 (± 4.1) | 22.9 (± 4.1) | 22.8 (±4.0) | 0.99 |
| PI (% of the sites) | 35.7 (±26.2)a | 16.0 (±9.6)b | 19.8 (±16.5)b | <0.0025 |
| BOP (% of the sites) | 0.39 (±0.18) a | 0.29 (±0.09) b | 0.17 (±0.08) )b | <0.0001 |
| PD ≤4 mm (% of the sites) | 94.1 (±5.74)a | 99.1 (±1.42)b | 99.13 (±1.61)b | <0.0001 |
| PD ≥5 mm (% of the sites) | 5.89 (±5.74)a | 0.87 (±1.42) b | 0.87 (±1.61) b | <0.0001 |
| CAL ≤3 mm (% of the sites) | 6.05 (±5.37)a | 0.89 (±1.45)b | 0.96 (±1.75)b | <0.0001 |
| CAL 4-5 mm(% of the sites) | 65.1 (±20.14) | 74.29 (±18.56) | 74.62 (±18.39) | 0.1172 |
| CAL ≥6 mm (% of the sites) | 28.85(±17.38 | 24.81 (±18.59) | 24.42 (±17.63) | 0.5968 |
| Biochemical and physical exams – Mean (SD) | ||||
| HbA1c (%) | 5.78 (±0.52) | 5.83 (±0.44) | 5.73 (±0.52) | 0.7296 |
| Fasting glucose (mg/dL) | 103.3(±14.89) | 106.0 (±14.20) | 107.0 (±13.12) | 0.6814 |
| Estimated glucose (mg/dL) | 116.9(±16.34) | 114.0 (±13.15) | 114.9 (±13.65) | 0.8091 |
| Total cholesterol(mg/dL) | 178.1(±40.07) | 195.5 (±47.94) | 171.2 (±29.41) | 0.2478 |
| Creatinine (mg/dL) | 0.94 (±0.32) | 0.94 (±0.26) | 0.97 (±0.35) | 0.9222 |
| PGT (U/l) | 23.55 (±9.26) | 22.66 (±7.75) | 2196 (±8.67) | 0.8321 |
| OGT (U/l) | 25.10 (±8.77) | 23.24 (±6.67) | 25.27 (±7.36) | 0.8929 |
| Waist hip ratio (cm) | 0.97 (±0.08) | 0.97 (±0.09) | 0.95 (±0.06) | 0.5930 |
| BMI (Kg/m2) | 29.41 (±4.61) | 29.66 (±4.62) | 29.53(±5.21) | 0.9823 |
| C-reactive Protein n, (%) | ||||
| Positive | 5 | 0 | 1 | 0.0213 |
| Negative | 17 | 22 | 21 | |
| Blood pressure parameters - Mean (DP) | ||||
| SBP (mmHg) | 139.6(±15.24) | 132.9 (±15.46) | 136.2 (±10.61) | 0.2878 |
| DBP (mmHg) | 79.50(±12.35) | 77.45 (±17.65) | 83.14 (±9.54) | 0.3912 |
| MBP (mmHg) | 109.5(±11.23) | 103.8 (±10.83) | 109.7(±6.29) | 0.0861 |
| Differential pressure (mmHg) | 60.09(±16.28) | 50.14 (±13.62) | 52.95 (±15.41) | 0.0924 |
Abbreviations: SD= standard deviation, PI= plaque index, BOP= bleeding on probing, PD= probing depth, CAL= clinical attachment level, HbA1C= glycated hemoglobin, PGT= pyruvic glutamic transaminase, OGT= oxalacetic glutamic transaminase, BMI= body mass index, SBP= systolic blood pressure, DBP= diastolic blood pressure, MBP= mean blood pressure. Bold font= p<0.05, a,b,c = different letter means statistically significant difference between groups (p<0.05). Categorical (C-reactive protein) intergroup comparison was performed using the chi-square test. Other parameters were analyzed using the ANOVA test of repeated measures with Tukey’s post-tests.
Table 3.
Linear regression analysis of subjects to assess the effects of different time periods on clinical periodontal parameters, biochemical and physical examinations and blood pressure parameters.
Table 3.
Linear regression analysis of subjects to assess the effects of different time periods on clinical periodontal parameters, biochemical and physical examinations and blood pressure parameters.
| Periodontal Clinical Parameters | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PI | BOP | PD≤4mm | PD≥5mm | CAL≤3mm | CAL≥6mm | |||||||
| β (95% CI) | p-value | β (95% CI) | p-value | β (95% CI) | p-value | β (95% CI) | p-value | β (95% CI) | p-value | β (95% CI) | p-value | |
| 90 days | -0.007(-0.01- -0.001) | 0.021 | -1.80(-2.46- -1.13) | 0.0001 | 0.05(0.02 -0.08) | 0.001 | -0.05(-0.08 - -0.03) | 0.0001 | -0.06(-0.09 - -0.03) | 0.0001 | -0.003(-0.01 -0005) | 0.41 |
| 180 days | -0.008(-0.01 - -0.001) | 0.021 | -1.81(-2.47 - -1.14) | 0.0001 | 0.05(0.03 -0.08) | 0.001 | -0.05(-0.07 - -0.03) | 0.0001 | -0.06(-0.09 - -0.03) | 0.0001 | -0.003(-0.02 -0005) | 0.40 |
| Biochemical exams | ||||||||||||
| HbA 1c | Fasting glucose | Total Cholesterol | C reactive protein | PGT | OCT | |||||||
| 90 days | -0.05(-0.36 – 0.24) | 0.73 | 0.004(-0.006 – 0.02) | 0.39 | -0.001(-0.006 – 0.003) | 0.58 | -0.38(-0.82 0.05) | 0.08 | -0.005(-0.03 -0.01) | 0.56 | 0.0007(-0.2 – 0.21) | 0.94 |
| 180 days | -0.05(-0.36 – 0.25) | 0.73 | 0.005(-0.007 – 0.02) | 0.40 | -0.002(-0.007 – 0.004) | 0.58 | -0.39(-0.82 0.05) | 0.08 | -0.005(-0.03 -0.01) | 0.56 | 0.0007(-0.19 – 0.20) | 0.95 |
| Physical Exams and Blood Pressure Parameters | ||||||||||||
| Hip/Waist ratio | MIB | SBP | DBP | MBP | Differential pressure | |||||||
| 90 days | -0.96(-3.01 -1.06) | 0.34 | 0.001(-0.03 – 0.03) | 0.93 | -0.002(-0.12 -0.009) | 0.79 | 0.008(-0.003 -0.20) | 0.15 | 0.004(-0.009 -0.018) | 0.53 | -0.007(-0.02 – 0.003) | 0.14 |
| 180 days | -0.97(-3.01 -1.06) | 0.34 | 0.001(-0.03 – 0.04) | 0.93 | -0.001(-0.12 -0.009) | 0.74 | 0.008(-0.003 -0.20) | 0.15 | 0.004(-0.009 -0.018) | 0.53 | -0.007(-0.01 – 0.001) | 0.14 |
Abbreviations: PI= plaque index, BOP= bleeding on probing, PD= probing depth, CAL= clinical attachment level, HbA1C= glycated hemoglobin, PGT= pyruvic glutamic transaminase, OGT= oxalacetic glutamic transaminase, BMI= body mass index, SBP= systolic blood pressure, DBP= diastolic blood pressure, MBP= mean blood pressure. Bold font= p<0.05.
Table 4.
Logistic regression of participant at different follow-up times, associated with periodontal and blood pressure parameters.
Table 4.
Logistic regression of participant at different follow-up times, associated with periodontal and blood pressure parameters.
| . | Time 1 | Time 2 | ||
| OR (95% CI) | p-value | OR (95% CI) | p-value | |
| BOP (% of sites) | ||||
| <30 % | Ref | Ref | ||
| ≥30 % | 0.02 (0.002 – 0.29) | 0.001 | 0.05 (0.009 – 0.26) | 0.000 |
| CAL ≥6 mm (% of sites) | ||||
| <30 % | Ref | Ref | ||
| ≥30 % | 0.54 (0.18 – 1.68) | 0.28 | 0.61 (0.19 – 1.94) | 0.41 |
| SBP (mmHg) | ||||
| <140 | Ref | Ref | ||
| ≥140 | 0.48 (0.15-1.61) | 0.24 | 0.83 (0.26 – 2.65) | 0.75 |
| DBP (mmHg) | ||||
| <90 | Ref | Ref | ||
| ≥90 | 1.17 (0.34-1.02) | 0.79 | 1.97 (0.59 – 6.63) | 0.27 |
Abbreviations: Time 1= baseline versus 90 days; Time 2= baseline versus 180 days, OR= odds ratio, CI= confidence interval, BOP= bleeding on probing, CAL= clinical attachment level, SBP= systolic blood pressure, DBP= diastolic blood pressure, Bold font= p<0 .05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



