
Submitted:
16 June 2023
Posted:
16 June 2023
You are already at the latest version
Abstract
Background
Some patients with mild cognitive impairment (MCI) experience gait disturbances. However, there are few reports on the relationship between gait disturbance and cognitive function in patients with MCI. Therefore, we investigated the neural correlates of gait characteristics related to cognitive dysfunction.
Methods
Eighty patients diagnosed with MCI from three dementia centres in Gangwon-do, Korea were recruited for this study. We defined MCI as a Clinical Dementia Rating global score of 0.5 or higher, with a memory domain score of 0.5 or greater. The patients were classified as having either early or late MCI based on their Mini Mental Status Examination z-scores. Multiple logistic regression analysis was performed to examine the association between the gait characteristics and cognitive impairment. Analyses included variables such as age, sex, years of education, number of comorbidities, body mass index and height.
Results
Gait velocity, step count, step length, heel-to-heel base support, swing and stance phase duration, and support time were associated with cognitive function. A decrease in gray matter volume in the right pericalcarine area was associated with gait characteristics related to cognitive dysfunction. An increase in the curvature of gray matter in the right entorhinal, right lateral orbitofrontal, right cuneus, and right and left pars opercularis areas was also associated with gait characteristics related to cognitive dysfunction.
Conclusion
Since gait impairment is an important factor in determining activities of daily living in patients with mild cognitive impairment, the evaluation of gait and cognitive functions in patients with mild cognitive impairment is important.
Keywords:
gait
; cognitive function
; mild cognitive impairment
; neural correlates
1. Introduction
Mild cognitive impairment (MCI) is a state in which cognitive decline is present but activities of daily living (ADL) are minimally affected, and independent living is possible [1]. MCI is the prodromal stage of dementia, which progresses to dementia in 10-15% of cases each year [2]. Although MCI is a disease in which cognitive decline is the main symptom of MCI, motor functions such as gait also play an important role in determining the ADL of patients with cognitive impairment [3]. In particular, because an altered gait may cause falls, it can lead to physical disability and admission to a nursing facility [4]. Additionally, falls due to gait deterioration can cause immobility, resulting in a rapid decline in cognitive function and poor prognosis in patients with cognitive impairment [5].
Patients with impaired cognitive function exhibit lower motor function when performing tasks that require cognitive function. In addition, when performing a complex task instead of a simple one, motor function deteriorates [6]. This means that gait requires cognitive functions, such as executive function and attention, rather than being a simple automated motor activity that uses minimal cognitive input [7]. Cognitive decline is caused by neuronal loss in the cerebral cortex, and the decline in cerebral cortical function due to specific brain atrophy might affect not only cognitive but also motor functions.
Therefore, we investigated altered gait characteristics and identified brain regions that affect gait in patients with MCI.
2. Methods
2.1. Participants
We prospectively recruited 80 patients with mild cognitive impairment at Chuncheon Sacred Heart Hospital between October 2020 and April 2021. The inclusion criteria were age between 40 and 100 years, a diagnosis of minor neurocognitive disorder as determined by the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-V), absence of dementia according to physicians’ judgment, and a Clinical Dementia Rating (CDR) global score of 0.5 with a memory domain score of 0.5 or greater. However, the MCI subtypes were not examined. Exclusion criteria included severe illness with an anticipated fatal outcome within three months, language barrier, deafness or blindness, and an inability to provide informed consent. The groups were classified into two groups: early-stage MCI (EMCI) showed performance on the Mini Mental Status Examination (MMSE) of less than 1.5 standard deviation (SD) below the normative mean, while late-stage MCI (LMCI) showed performance on the MMSE of more than 1.5 SD below the normative mean.
Written informed consent was obtained from each patient, and the Institutional Review Board of Chuncheon Sacred Heart Hospital approved the study protocol (IRB number: Chuncheon 2020-09-005).
2.2. Clinical assessment
We recorded demographics, including age, sex, and years of education, and measures of body composition, including height, weight, and waist circumference. We also checked the blood pressure and blood test results, including fasting glucose and total cholesterol levels. Patients completed the depression scale (Short form of Geriatric Depression Scale, SGDS), anxiety scale (Korean Geriatric Anxiety Inventory, K-GAI), quality of life scale (Geriatric Quality of Life Dementia, GQOL-D), and the Korean National Health and Nutrition Examination Survey (KNHANES). Additional medical comorbidities were checked during the clinic interviews.
2.2. Gait assessment
The GAITRite® instrumentation (CIR systems Inc., Havertown, PA) comprises an electronic walkway measuring 5.6 meters in length and 0.9 meters in width. Each patient was instructed to walk at a normal pace without a gait aid on the walkway, and each patient walked on the GAITRite pad in a single pass. The study coordinator observed each patient’s gait without any interference. For this analysis, we focused on the following gait variables: gait velocity (m/s), cadence (number of steps per minute), step time (s), step length (cm), cycle time (s), heel-to-heel (H-H) base support (cm), swing percentage of the cycle phase (%), stance percentage of the cycle phase (%), double support percent cycle phase (%), step time variability (%), and step length variability (%). Variability was expressed as the coefficient of variation, which was calculated as the standard deviation of the step time or step length divided by the mean of the step time or step length, multiplied by 100%.
2.3. MRI acquisition
Standardised T1, T2, fluid-attenuated inversion recovery (FLAIR), and three-dimensional (3D) T1-weighted images were acquired from all eligible participants at Chuncheon Sacred Heart Hospital using the same 3.0T MRI scanner (Siemens Skyra). 3D T1-weighted structural brain images were acquired using a Magnetisation Prepared Rapid Acquisition Gradient Echo (MPRAGE) sequence with the following parameters: sagittal slice thickness, 1.0 mm, no gap, repetition time (TR), 2300.0 msec, Echo Time (TE), 2.98 msec, flip angle, 9°; Inversion Time (TI) of 900msec, and imaging matrix size, 256 × 240 × 176.
2.4. Gray matter volume and Curve index measurements
3D Slicer (http://www.slicer.org, Surgical Planning Laboratory, Harvard University, Boston, MA, USA, version 4.11) and FreeSurfer (http://www.freesurfer.net, MIT Health Sciences & Technology, and Massachusetts General Hospital, USA, version 7.1.1) softwares were used to measure the volume and curve index of the gray matter for each subcortical region from the 3D T1 image data in DICOM (Digital Imaging and Communications in Medicine) format. The DICOM files were converted into NifTI (Neuroimaging Informatics Technology Initiative) format using 3D Slicer, and then reconstructed into a 2D cortical surface using the recon-all function of FreeSurfer.[8,9] The reconstruction involved several steps of the recon-all function, including motion correction, skull stripping, normalisation and transformation, white and gray matter segmentation, averaging and smoothing, parcellation of subcortical regions, and measurement of parcellation statistics. The results of the parcellation statistics provided the gray matter volume and curvature index for each of the 34 subcortical regions per hemisphere.
2.5. Statistical analysis
Baseline characteristics based on the data are presented as mean standard deviation (SD) for continuous variables and percentages for categorical variables. Differences between the EMCI and LMCI groups were confirmed using Student’s t-test for continuous variables and chi-square tests for categorical variables. The relationship between gait characteristics and the MCI stage was evaluated using multiple logistic regression analysis. We ran three regression models. In model 1, we performed a binary logistic regression analysis with each gait parameter as the determinant and the MCI stage as the outcome variable. In model 2, we performed a multiple logistic regression analysis with age, sex, years of education, and each gait parameter. In model 3, we performed a multiple logistic regression analysis with age, sex, years of education, number of comorbidities, BMI, and gait parameters.
Disease risk is expressed as odds ratios (OR) with 95% confidence interval (95% CI). Statistical significance was defined as p < 0.05. All statistical analyses were performed using SPSS version 25 software (SPSS Inc., Chicago, IL, USA).
To evaluate the topography of the gray matter related to gait characteristics, logistic regression analysis was performed on the voxel-based morphometry analysis in Python using the scikit-learn library after controlling for age, sex, year of education, number of comorbidities, BMI, and ICV. Correction for multiple comparisons was accomplished using a false discovery rate correction at a corrected probability value of 0.05. We determined that only values with a t-value of 5 or higher had a significant association; thus, only the results showing a t-value of 5 or higher are presented in the results.
3. Results
3.1. Demographics, clinical characteristics, and gait characteristics
Detailed demographic and clinical characteristics of the participants are presented in Table 1. The EMCI group had a higher proportion of females than the LMCI group. Years of education were shorter in the early MCI group than in the late MCI group. The EMCI group had a higher number of comorbidities than the LMCI group. Body mass index (BMI) was higher in the EMCI group than in the LMCI group.
Table 2 presents the gait characteristics of the participants. The LMCI group had larger H-H base support values than the EMCI group.
3.2. Association between gait characteristics and mild cognitive impairment
Table 3 shows the risk of LMCI according to gait characteristics. Patients with higher gait velocity had 0.96-fold odds of LMCI (OR 0.96, 95% CI 0.92-0.99). Step length was associated with LMCI, with a lower odds ratio for the left side (OR 0.81, 95% CI 0.71-0.91) than the right side (OR 0.86, 95% CI 0.78-0.95). H-H base support was associated with LMCI, with higher odds ratios for the left (OR 1.29, 95% CI 1.08-1.58) than the right side (OR 1.39, 95% CI 1.11-1.75). Patients with greater step length variability on the right side had 1.22-fold odds of LMCI (OR 1.22, 95% CI 1.03-1.44). A shorter swing phase, longer stance phase, and longer double support phase were also associated with LMCI.
3.3. Decreased and distorted gray matter areas associated with gait characteristics related to cognitive dysfunction
Figure 1 shows the regional areas associated with gait characteristics. A regional decrease in gray matter volume is associated with gait characteristics. Increased H-H base support is associated with the right pericalcarine area.
Regional distortion of the gray matter is also associated with gait characteristics. Slowed gait velocity was associated with an increased gray matter curvature index in the right entorhinal area. An increased step length was associated with an increased curvature index of the gray matter in the right entorhinal, right lateral orbitofrontal, right cuneus, and right pars opercularis areas. An increased step length was also associated with a decreased curvature index of the gray matter in the left pars opercularis.
4. Discussion
Slower gait velocity, shorter step length, wider H-H base support, shorter swing phase, longer stance phase, and longer double support were all associated with LMCI, as well as increased step length variability. Subsequently, we investigated the brain regions associated with these gait characteristics in relation to LMCI using MRI. We found that a decrease in gray matter volume in the left transverse temporal, left supramarginal, and right pericalcarine areas was associated with gait characteristics related to late LMCI. Additionally, an increase in the curvature of gray matter in the right entorhinal, right lateral orbitofrontal, and right pars opercularis areas was associated with gait characteristics related to LMCI.
In this study, we found that slower gait was associated with LMCI, which is consistent with the findings of previous studies suggesting that motor impairment occurs during the course of cognitive decline [10]. In previous studies, patients with MCI showed decreased motor function compared with those without cognitive impairment [11,12]. Patients with MCI were also more likely to exhibit parkinsonian features such as bradykinesia, rigidity, and gait dysfunction [13,14]. These parkinsonian features were associated with the severity of cognitive impairment [13]. However, it is not clear what causes motor function to decrease in patients with MCI. Some studies have shown that the cognitive function in a specific area is related to gait speed. A previous study found that slow gait speed was associated with lower executive function [15], and another longitudinal study reported that low memory and executive functions were related to gait speed [16]. In studies using neuroimaging studies, some researchers have reported that cerebrovascular lesions, such as periventricular white matter changes in the frontal lobe, are associated with gait disturbances in patients with MCI [12]. On the other hand, some researchers have reported that more parkinsonian features are seen in patients with MCI than in cognitively normal older adults, regardless of the vascular burden [13]. Also, in another study, temporal lobe atrophy was correlated with poor mobility, independent of cerebrovascular disease [17].
We reported that shorter step length, wider H-H base support, shorter swing phase, longer stance phase, longer double support, and increased step length variability were associated with late MCI. Since these characteristics can appear when there is a problem with balance function [18] the gait characteristics in our study suggest that MCI patients with more severe cognitive impairment had lower balance function. In a previous study, patients with MCI had decreased balance function in the eyes-open balance test but not in the eyes-closed balance test [3]. They suggested that visual information had to be processed to maintain balance with eyes open [19] but patients with MCI had a decreased ability to process visual information [20] leading to a more pronounced balance function impairment when their eyes were opened. Another study showed that impaired executive function, including attention, was associated with impaired balance in patients with cognitive impairment, and that the decrease in balance function was more pronounced with the severity of cognitive impairment [21].
Step length variability is also associated with late MCI. Similar to our findings, a previous study reported that gait variability was greater in patients with dementia [22]. There was a report that gait stability has been reported to be highly related to balance [23] and another report has suggested that it is highly related to executive function, including attention [22]. Although gait is a skilled movement, it is generally believed that no cognitive function is involved [24]. However, even for previously skilled movements, executive functions that integrate attention with motor control and input from higher cortical motor centres are required to maintain gait. Gait stability may be impaired in patients with cognitive impairment because these functions are impaired [25].
A decrease in the volume of gray matter in the right pericalcarine area was associated with gait characteristics related to LMCI. An increase in the curvature of the gray matter in the right cuneus was also associated with the gait characteristics. The pericalcarine gyrus (PCG) plays an important role in the visual networks [26]. Considering that low gait function is related to a decrease in gray matter volume in these areas, visual function seems to play an important role in maintaining gait function. Similar to this study, brain regions, such as the pericalcarine gyrus, were related to gait function in a study on the functional connectivity of brain regions related to gait function in patients with multiple sclerosis [27]. In addition, The cuneus is generally an area involved in basic visual processing, and it is also involved in locomotion. In one case report, gait dyspraxia was reported after an infarction in the right cuneus [28]. In our study, we found that an increase in the curvature index of the right cuneus was associated with a decrease in step length, which can be interpreted in the same context as previous studies.
In this study, an increase in the curvature of gray matter in the right entorhinal, right lateral orbitofrontal, and right cuneus regions was associated with gait characteristics. The entorhinal cortex is the main input and output structure of the hippocampal formation, connecting the cortex and hippocampus [29]. In a pathologic study, the pathological changes associated with Alzheimer’s disease first occurred in the entorhinal cortex, and the change started there and then spread to the hippocampus and cortex [30]. In a clinical study of the hippocampal structures, the entorhinal cortex best reflected disease progression in patients with MCI [31]. In previous studies, hippocampal volume was associated with gait and cognitive function in patients with MCI [31,32] and the entorhinal cortex itself has been associated with gait disturbance in previous studies [31]. The hippocampus and the prefrontal cortex are functionally connected through the entorhinal cortex, and the hippocampus also has a function in the integration of sensory and motor information [33]. Although our study did not show a decrease in the hippocampal volume in relation to gait characteristics, a deformity of the entorhinal cortex was observed. Since the entorhinal cortex is a region that better reflects disease progression than the entire hippocampus [31], we speculated that the deformity might occur earlier than in other regions in relation to gait disturbance in patients with MCI.
Deformities of the pars opercularis and lateral orbitofrontal areas were also observed in this study. Dysfunction of the prefrontal cortex, including the orbitofrontal cortex and the pars opercularis, plays a major role in gait dysfunction in Alzheimer’s disease (AD)?. The orbitofrontal cortex plays an important role in inhibitory control [34]. Executive-attention function, including inhibition control, is impaired in patients with prodromal AD before memory loss and is also involved in gait function [35,36]. In a previous aging study, gait function was associated with amyloid deposition in the orbitofrontal area [37]. The pars opercularis belongs to Broca’s area and is the location of the frontal part of the mirror neurons. Mirror neurons play an important role in the imitation and execution of actions. Frontal mirror neurons are known to exert greater activity during execution [38].
This study had several limitations. First, we did not classify the patients with amnestic mild cognitive impairment. Therefore, we cannot exclude the possibility that participants with degenerative pathology related to parkinsonism or vascular damage may have been present. Secondly, musculoskeletal problems affecting gait disturbances were not considered. Third, as this was a cross-sectional study, it was difficult to establish causal relationships. However, we investigated gait characteristics related to cognitive dysfunction and identified cortical areas related to gait characteristics in patients with MCI. In the future, more research is needed to determine whether the gait characteristics identified in our study will be helpful for the early detection of MCI.
Funding
This research was supported by the Memorial Foundation for Dr. Suh Succjo by Hyangseal, Korean Neurological Association (KNA-21-HS-08), National Research Foundation of Korea (NRF) grant funded by the Korean Government (NRF-2022R1A2C1011286), and Basic Science Research funded by the Korean Government(2020R1F1A1048281). This research was supported by a grant of the Korea Health Promotion R&D Project, funded by the Ministry of Health & Welfare, Republic of Korea (grant number : HS21C0000).
Data Availability
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
References
- Petersen, R.C. Mild cognitive impairment as a diagnostic entity. J Intern Med 2004, 256, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Doody, R.; Kurz, A.; Mohs, R.C.; Morris, J.C.; Rabins, P.V.; Ritchie, K.; Rossor, M.; Thal, L.; Winblad, B. Current concepts in mild cognitive impairment. Arch Neurol 2001, 58, 1985–1992. [Google Scholar] [CrossRef] [PubMed]
- Bahureksa, L.; Najafi, B.; Saleh, A.; Sabbagh, M.; Coon, D.; Mohler, M.J.; Schwenk, M. The Impact of Mild Cognitive Impairment on Gait and Balance: A Systematic Review and Meta-Analysis of Studies Using Instrumented Assessment. Gerontology 2017, 63, 67–83. [Google Scholar] [CrossRef]
- Verghese, J.; LeValley, A.; Hall, C.B.; Katz, M.J.; Ambrose, A.F.; Lipton, R.B. Epidemiology of gait disorders in community-residing older adults. J Am Geriatr Soc 2006, 54, 255–261. [Google Scholar] [CrossRef]
- Amboni, M.; Barone, P.; Hausdorff, J.M. Cognitive contributions to gait and falls: evidence and implications. Mov Disord 2013, 28, 1520–1533. [Google Scholar] [CrossRef]
- Nascimbeni, A.; Caruso, S.; Salatino, A.; Carenza, M.; Rigano, M.; Raviolo, A.; Ricci, R. Dual task-related gait changes in patients with mild cognitive impairment. Funct Neurol 2015, 30, 59–65. [Google Scholar]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. The role of executive function and attention in gait. Mov Disord 2008, 23, 329–342. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn Reson Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef]
- Dale, A.M.; Fischl, B.; Sereno, M.I. Cortical surface-based analysis. I. Segmentation and surface reconstruction. Neuroimage 1999, 9, 179–194. [Google Scholar] [CrossRef]
- Verghese, J.; Robbins, M.; Holtzer, R.; Zimmerman, M.; Wang, C.; Xue, X.; Lipton, R.B. Gait dysfunction in mild cognitive impairment syndromes. J Am Geriatr Soc 2008, 56, 1244–1251. [Google Scholar] [CrossRef]
- Kluger, A.; Gianutsos, J.G.; Golomb, J.; Ferris, S.H.; George, A.E.; Franssen, E.; Reisberg, B. Patterns of motor impairement in normal aging, mild cognitive decline, and early Alzheimer's disease. J Gerontol B Psychol Sci Soc Sci 1997, 52B, P28–39. [Google Scholar] [CrossRef] [PubMed]
- Frisoni, G.B.; Galluzzi, S.; Bresciani, L.; Zanetti, O.; Geroldi, C. Mild cognitive impairment with subcortical vascular features: clinical characteristics and outcome. J Neurol 2002, 249, 1423–1432. [Google Scholar] [CrossRef] [PubMed]
- Boyle, P.A.; Wilson, R.S.; Aggarwal, N.T.; Arvanitakis, Z.; Kelly, J.; Bienias, J.L.; Bennett, D.A. Parkinsonian signs in subjects with mild cognitive impairment. Neurology 2005, 65, 1901–1906. [Google Scholar] [CrossRef]
- Louis, E.D.; Schupf, N.; Manly, J.; Marder, K.; Tang, M.X.; Mayeux, R. Association between mild parkinsonian signs and mild cognitive impairment in a community. Neurology 2005, 64, 1157–1161. [Google Scholar] [CrossRef] [PubMed]
- McGough, E.L.; Kelly, V.E.; Logsdon, R.G.; McCurry, S.M.; Cochrane, B.B.; Engel, J.M.; Teri, L. Associations between physical performance and executive function in older adults with mild cognitive impairment: gait speed and the timed "up & go" test. Phys Ther 2011, 91, 1198–1207. [Google Scholar] [CrossRef]
- Watson, N.L.; Rosano, C.; Boudreau, R.M.; Simonsick, E.M.; Ferrucci, L.; Sutton-Tyrrell, K.; Hardy, S.E.; Atkinson, H.H.; Yaffe, K.; Satterfield, S.; et al. Executive function, memory, and gait speed decline in well-functioning older adults. J Gerontol A Biol Sci Med Sci 2010, 65, 1093–1100. [Google Scholar] [CrossRef]
- Guo, X.; Steen, B.; Matousek, M.; Andreasson, L.A.; Larsson, L.; Palsson, S.; Sundh, V.; Skoog, I. A population-based study on brain atrophy and motor performance in elderly women. J Gerontol A Biol Sci Med Sci 2001, 56, M633–637. [Google Scholar] [CrossRef]
- Marchetti, G.F.; Whitney, S.L.; Blatt, P.J.; Morris, L.O.; Vance, J.M. Temporal and spatial characteristics of gait during performance of the Dynamic Gait Index in people with and people without balance or vestibular disorders. Phys Ther 2008, 88, 640–651. [Google Scholar] [CrossRef]
- Redfern, M.S.; Jennings, J.R.; Mendelson, D.; Nebes, R.D. Perceptual inhibition is associated with sensory integration in standing postural control among older adults. J Gerontol B Psychol Sci Soc Sci 2009, 64, 569–576. [Google Scholar] [CrossRef]
- Perrochon, A.; Kemoun, G.; Dugue, B.; Berthoz, A. Cognitive Impairment Assessment through Visuospatial Memory Can Be Performed with a Modified Walking Corsi Test Using the 'Magic Carpet'. Dement Geriatr Cogn Dis Extra 2014, 4, 1–13. [Google Scholar] [CrossRef]
- Tangen, G.G.; Engedal, K.; Bergland, A.; Moger, T.A.; Mengshoel, A.M. Relationships between balance and cognition in patients with subjective cognitive impairment, mild cognitive impairment, and Alzheimer disease. Phys Ther 2014, 94, 1123–1134. [Google Scholar] [CrossRef]
- Allali, G.; Assal, F.; Kressig, R.W.; Dubost, V.; Herrmann, F.R.; Beauchet, O. Impact of impaired executive function on gait stability. Dement Geriatr Cogn Disord 2008, 26, 364–369. [Google Scholar] [CrossRef]
- Hamacher, D.; Liebl, D.; Hodl, C.; Hessler, V.; Kniewasser, C.K.; Thonnessen, T.; Zech, A. Gait Stability and Its Influencing Factors in Older Adults. Front Physiol 2018, 9, 1955. [Google Scholar] [CrossRef]
- Jahanshahi, M. Willed action and its impairments. Cogn Neuropsychol 1998, 15, 483–533. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, P.L.; Solomont, J.; Kowall, N.; Hausdorff, J.M. Influence of executive function on locomotor function: divided attention increases gait variability in Alzheimer's disease. J Am Geriatr Soc 2003, 51, 1633–1637. [Google Scholar] [CrossRef] [PubMed]
- Coppen, E.M.; Grond, J.V.; Hafkemeijer, A.; Barkey Wolf, J.J.H.; Roos, R.A.C. Structural and functional changes of the visual cortex in early Huntington's disease. Hum Brain Mapp 2018, 39, 4776–4786. [Google Scholar] [CrossRef] [PubMed]
- Bollaert, R.E.; Poe, K.; Hubbard, E.A.; Motl, R.W.; Pilutti, L.A.; Johnson, C.L.; Sutton, B.P. Associations of functional connectivity and walking performance in multiple sclerosis. Neuropsychologia 2018, 117, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Onder, H.; Buyuk, F. Gait Dyspraxia due to Right Occipital Infarct. J Mov Disord 2019, 12, 54–56. [Google Scholar] [CrossRef]
- Witter, M.P.; Doan, T.P.; Jacobsen, B.; Nilssen, E.S.; Ohara, S. Architecture of the Entorhinal Cortex A Review of Entorhinal Anatomy in Rodents with Some Comparative Notes. Front Syst Neurosci 2017, 11, 46. [Google Scholar] [CrossRef]
- Braak, H.; Braak, E. Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol 1991, 82, 239–259. [Google Scholar] [CrossRef]
- Sakurai, R.; Bartha, R.; Montero-Odasso, M. Entorhinal Cortex Volume Is Associated With Dual-Task Gait Cost Among Older Adults With MCI: Results From the Gait and Brain Study. J Gerontol A Biol Sci Med Sci 2019, 74, 698–704. [Google Scholar] [CrossRef]
- Rosso, A.L.; Verghese, J.; Metti, A.L.; Boudreau, R.M.; Aizenstein, H.J.; Kritchevsky, S.; Harris, T.; Yaffe, K.; Satterfield, S.; Studenski, S.; et al. Slowing gait and risk for cognitive impairment: The hippocampus as a shared neural substrate. Neurology 2017, 89, 336–342. [Google Scholar] [CrossRef]
- Tian, Q.; Chastan, N.; Bair, W.N.; Resnick, S.M.; Ferrucci, L.; Studenski, S.A. The brain map of gait variability in aging, cognitive impairment and dementia-A systematic review. Neurosci Biobehav Rev 2017, 74, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Bryden, D.W.; Roesch, M.R. Executive control signals in orbitofrontal cortex during response inhibition. J Neurosci 2015, 35, 3903–3914. [Google Scholar] [CrossRef] [PubMed]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The unity and diversity of executive functions and their contributions to complex "Frontal Lobe" tasks: a latent variable analysis. Cogn Psychol 2000, 41, 49–100. [Google Scholar] [CrossRef] [PubMed]
- Harrington, M.G.; Chiang, J.; Pogoda, J.M.; Gomez, M.; Thomas, K.; Marion, S.D.; Miller, K.J.; Siddarth, P.; Yi, X.; Zhou, F.; et al. Executive function changes before memory in preclinical Alzheimer's pathology: a prospective, cross-sectional, case control study. PLoS One 2013, 8, e79378. [Google Scholar] [CrossRef]
- Wennberg, A.M.V.; Savica, R.; Hagen, C.E.; Roberts, R.O.; Knopman, D.S.; Hollman, J.H.; Vemuri, P.; Jack, C.R., Jr.; Petersen, R.C.; Mielke, M.M. Cerebral Amyloid Deposition Is Associated with Gait Parameters in the Mayo Clinic Study of Aging. J Am Geriatr Soc 2017, 65, 792–799. [Google Scholar] [CrossRef]
- Iacoboni, M.; Dapretto, M. The mirror neuron system and the consequences of its dysfunction. Nat Rev Neurosci 2006, 7, 942–951. [Google Scholar] [CrossRef]
Figure 1.
Regional areas associated with gait characteristics related to cognitive dysfunction (a) Regional volume change of gray matter in the right pericalcarine area was associated with gait characteristics related to cognitive dysfunction. (b) Regional distortion of gray matter in the right entorhinal, right lateral orbitofrontal, right cuneus, right and left pars opercularis areas was associated with gait characteristics related to cognitive dysfunction. We displayed the results with a t-value >5 in the figure. Abbreviations: HH, heel to heel; rh, right; lh, left; L, left.
Figure 1.
Regional areas associated with gait characteristics related to cognitive dysfunction (a) Regional volume change of gray matter in the right pericalcarine area was associated with gait characteristics related to cognitive dysfunction. (b) Regional distortion of gray matter in the right entorhinal, right lateral orbitofrontal, right cuneus, right and left pars opercularis areas was associated with gait characteristics related to cognitive dysfunction. We displayed the results with a t-value >5 in the figure. Abbreviations: HH, heel to heel; rh, right; lh, left; L, left.
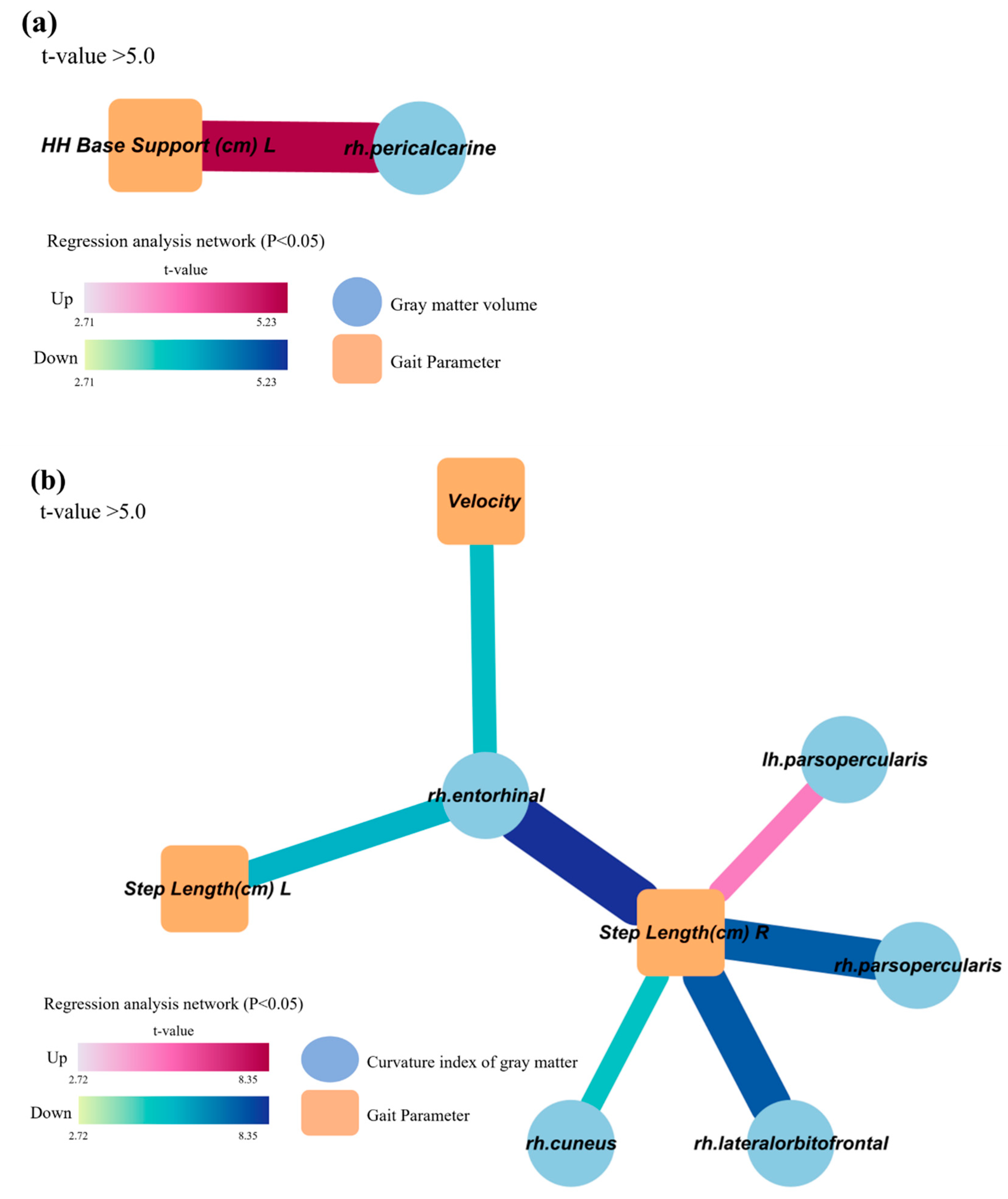

Table 1.
Demographic and clinical characteristics.
| Total (n=80) |
Early MCI (n=53) |
Late MCI (n=27) |
p value | |
| Mean age | 74.6±5.74 | 74.6±5.33 | 74.6±6.58 | 0.95 |
| Gender, female (%) | 58 (72.5) | 43 (81.1) | 15 (55.6) | 0.020 |
| Year of education | 6.88±3.980 | 5.94±4.069 | 8.72±3.114 | 0.003 |
| Number of comorbidities | 3.7±1.70 | 3.9±1.61 | 3.1±1.77 | 0.047 |
| Depression scale | 4.9±4.09 | 4.9±4.24 | 5.1±3.83 | 0.833 |
| Anxiety scale | 6.8±6.52 | 7.1±6.87 | 6.3±5.86 | 0.600 |
| QOL scale | 34.4±8.67 | 33.3±8.39 | 36.5±9.00 | 0.124 |
| Stress scale | 1.57±0.664 | 1.62±0.716 | 1.49±0.551 | 0.423 |
| Height | 156.1±8.11 | 155.4±7.98 | 157.7±8.30 | 0.232 |
| Weight | 61.0±10.92 | 61.9±11.47 | 59.3±9.72 | 0.324 |
| BMI, mean (SD) | 25.0±3.70 | 25.6±3.84 | 23.8±3.17 | 0.045 |
| Waist circumference (cm) | 87.8±10.12 | 87.6±10.39 | 88.1±9.75 | 0.825 |
| Systolic BP (mmHg) | 128.6±18.27 | 130.0±18.44 | 126.0±17.97 | 0.349 |
| Diastolic BP (mmHg) | 77.0±9.82 | 77.4±9.41 | 76.1±10.73 | 0.606 |
| Fasting glucose (mg/dL) | 108.8±26.28 | 111.3±28.44 | 104.0±21.08 | 0.240 |
| Total cholesterol (mg/dL | 162.4±32.54 | 34.0±4.67 | 30.1±5.79 | 0.913 |
Data are mean ± SD unless otherwise indicated, a Number (%), Abbreviations: QOL, quality of life; BMI, body mass index; BP, blood pressure; SD, standard deviation.
Table 2.
Gait characteristics.
| Total (n=80) |
Early MCI (n=53) |
Late MCI (n=27) |
p value | |
| Gait velocity | 93.6±20.16 | 93.9±21.48 | 90.9±17.35 | 0.404 |
| Cadence | 107.1±11.52 | 106.4±12.02 | 108.3±10.58 | 0.498 |
| Step time (sec) | ||||
| Left | 0.6±0.07 | 0.6±0.07 | 0.6±0.06 | 0.575 |
| Right | 0.6±0.07 | 0.6±0.07 | 0.6±0.05 | 0.348 |
| Step length (cm) | ||||
| Left | 51.8±8.52 | 52.9±8.60 | 49.7±8.09 | 0.111 |
| Right | 52.3±8.27 | 53.0±8.15 | 50.9±8.47 | 0.268 |
| Cycle time (sec) | ||||
| Left | 1.1±0.13 | 1.1±0.15 | 1.1±0.11 | 0.418 |
| Right | 1.1±0.13 | 1.1±0.15 | 1.1±0.11 | 0.468 |
| H-H base support (cm) | ||||
| Left | 9.0±3.12 | 8.5±3.14 | 10.1±2.82 | 0.027 |
| Right | 8.8±2.99 | 8.1±2.78 | 10.2±2.95 | 0.002 |
| Swing % of cycle | ||||
| Left | 36.8±2.28 | 36.9±2.23 | 36.7±2.42 | 0.776 |
| Right | 36.6±2.45 | 36.9±2.70 | 35.9±1.75 | 0.085 |
| Stance % of cycle | ||||
| Left | 63.2±2.28 | 63.1±2.23 | 63.3±2.42 | 0.795 |
| Right | 63.4±2.46 | 63.1±2.70 | 64.1±1.74 | 0.051 |
| Double support % of cycle | ||||
| Left | 26.4±4.20 | 26.0±4.41 | 27.2±3.72 | 0.242 |
| Right | 26.6±4.41 | 26.2±4.74 | 27.2±3.67 | 0.354 |
| Step time variability (%) | ||||
| Left | 4.1±2.77 | 4.1±2.72 | 4.2±2.91 | 0.849 |
| Right | 3.7±2.56 | 3.5±2.76 | 4.1±2.10 | 0.318 |
| Step length variability (%) | ||||
| Left | 2.4±1.65 | 2.3±1.45 | 2.6±2.00 | 0.400 |
| Right | 4.8±3.45 | 4.4±3.43 | 5.5±3.45 | 0.169 |
Table 3.
Gait parameters and odds of cognitive impairment.
| Model 1 | Model 2 | Model 3 | ||||
| OR (95% CI) | p value | OR (95% CI) | p value | OR (95% CI) | p value | |
| Gait velocity | 0.990 (0.967, 1.013) | 0.400 | 0.968 (0.940, 0.998) | 0.035 | 0.957 (0.924, 0.991) | 0.015 |
| Cadence | 1.015 (0.973, 1.057) |
0.493 | 1.008 (0.959, 1.059) |
0.763 | 1.011 (0.955, 1.069) |
0.712 |
| Step time (sec) | ||||||
| Left | 0.135 (0.000, 136.191) |
0.570 | 0.700 (0.000, 2222.031) |
0.931 | 0.896 (0.000, 8368.103) |
0.981 |
| Right | 0.025 (0.000, 53.164) |
0.347 | 0.083 (0.000, 687.854) |
0.589 | 0.069 (0.000, 2747.780) |
0.621 |
| Step length (cm) | ||||||
| Left | 0.955 (0.901, 1.011) |
0.114 | 0.878 (0.805, 0.958) |
0.003 | 0.805 (0.711, 0.912) |
0.001 |
| Right | 0.968 (0.913, 1.025) |
0.266 | 0.894 (0.822, 0.972) |
0.009 | 0.861 (0.781, 0.950) |
0.003 |
| Cycle time (sec) | ||||||
| Left | 0.213 (0.005, 8.789) |
0.415 | 0.504 (0.007, 38.928) |
0.757 | 0.567 (0.004, 83.640) |
0.824 |
| Right | 0.252 (0.006, 10.106) |
0.464 | 0.475 (0.006, 37.650) |
0.739 | 0.496 (0.003, 75.879) |
0.785 |
| H-H base support (cm) | ||||||
| Left | 1.192 (1.015, 1.400) |
0.033 | 1.167 (0.978, 1.392) |
0.087 | 1.288 (1.047, 1.584) |
0.017 |
| Right | 1.292 (1.083, 1.542) |
0.004 | 1.266 (1.040, 1.541) |
0.019 | 1.391 (1.108, 1.746) |
0.005 |
| Swing % of cycle | ||||||
| Left | 0.971 (0.792, 1.189) |
0.773 | 0.864 (0.684, 1.091) |
0.218 | 0.724 (0.541, 0.967) |
0.029 |
| Right | 0.844 (0.694, 1.027) |
0.090 | 0.716 (0.560, 0.916) |
0.008 | 0.539 (0.378, 0.768) |
0.001 |
| Stance % of cycle | ||||||
| Left | 1.028 (0.839, 1.260) |
0.792 | 1.154 (0.913, 1.458) |
0.230 | 1.377 (1.031, 1.839) |
0.030 |
| Right | 1.183 (0.973, 1.439) |
0.092 | 1.392 (1.089, 1.779) |
0.008 | 1.845 (1.298, 2.621) |
0.001 |
| Double support % of cycle | ||||||
| Left | 1.069 (0.956, 1.194) |
0.242 | 1.161 (1.014, 1.329) |
0.030 | 1.357 (1.155, 1.641) |
0.002 |
| Right | 1.051 (0.946, 1.167) |
0.352 | 1.149 (1.009, 1.308) |
0.036 | 1.354 (1.130, 1.623) |
0.001 |
| Step time variability | ||||||
| Left | 1.017 (0.860, 1.201) |
0.847 | 1.022 (0.854, 1.222) |
0.815 | 1.045 (0.844, 1.295) |
0.684 |
| Right | 1.095 (0.915, 1.311) |
0.320 | 1.147 (0.942, 1.397) |
0.173 | 1.188 (0.963, 1.465) |
0.109 |
| Step length variability | ||||||
| Left | 1.143 (0.865, 1.512) | 0.347 | 1.178 (0.863, 1.609) |
0.302 | 1.166 (0.845, 1.609) |
0.350 |
| Right | 1.098 (0.961, 1.255) | 0.170 | 1.149 (0.986, 1.339) |
0.076 | 1.215 (1.027, 1.436) |
0.023 |
Model 1: separate models associated each gait parameters with cognitive impairment; Model 2: Single model including age, sex, years of education, and each gait parameter; Model 3: Single model including age, sex, years of education, number of comorbidities, BMI, and each gait parameter.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



