
Submitted:
16 June 2023
Posted:
19 June 2023
You are already at the latest version
Abstract
Adiposity is associated with adverse health conditions such as obesity, cardiovascular disease and type 2 diabetes. The combination of resistance exercise and creatine supplementation has been shown to decrease body fat % in adults ≥ 50 years of age. However, the effects in adults < 50 years of age is unknown. To address this limitation, we systematically reviewed the literature and performed several meta-analyses comparing studies that included resistance exercise and creatine supplementation to resistance exercise and placebo. Twelve studies were included involving 266 participants. Adults (< 50 years of age) that supplemented with creatine and performed resistance exercise experienced a significant reduction in body fat % (-1.19%, p=0.006) and a non-significant reduction in absolute fat mass (-0.09 kg, p=0.88). Collectively, the combination of resistance exercise and creatine supplementation produces a very small reduction in body fat % in adults < 50 years of age.
Keywords:
body composition
; ergogenic aids
; adipose tissue
; strength training
1. Introduction
There is a significant increase in the prevalence of adiposity in young adults [1] which could lead to the development of adverse health conditions such as obesity, cardiovascular disease and type 2 diabetes later in life [2,3]. From an overall health and longevity perspective, lifestyle interventions that help regulate fat mass are likely important for promoting a healthier metabolic phenotype over time [4,5].
A recent systematic review and meta-analysis involving over 800 healthy adults (≥ 19 years) showed that resistance exercise (≥ 4 times per week for up to 2 years) decreased fat mass by 0.55 kg (95% CI: -0.75 to -0.34; p<0.0001) and body fat % by 1.46% (95% CI: -1.78 to -1.14; p<0.0001) over time [6]. These changes may be related to the stimulating effects of resistance exercise on resting metabolic rate [7], excess post oxygen consumption [8] and circulating levels of non-esterified fatty acids and by decreasing the respiratory quotient (indicating increased adipocyte lipolysis and/or intramuscular triglyceride oxidation) [9]. In addition to resistance exercise, supplementing with creatine (methylguanidine acetic acid) may lead to greater reductions in fat mass over time compared to resistance exercise alone. We previously performed a meta-analysis showing that healthy older adults (n=609; 19 studies; ≥ 50 years) who supplemented with creatine (≥ 2 grams/day) and performed resistance exercise (2-3 times/week for up to 1 year) experienced a significant reduction in body fat % (0.55%; CI: -1.08 to -0.03; p=0.04) and a non-significant decrease in fat mass (-0.50 kg; 95% CI: -1.15 to 0.15; p=0.13) compared to resistance exercise alone [10]. While no mechanisms were determined in this analysis, creatine has the ability to influence whole-body energy expenditure, adipocyte metabolism, thermogenesis, fat bioenergetics and body fat accumulation [10,11,12,13,14]. However, the generalizability of these findings may be limited because older adults have a high degree of variability in their responsiveness to resistance exercise and creatine supplementation.
Individual studies examining the efficacy of creatine supplementation and resistance exercise on measures of body fat in healthy younger adults (< 50 years) indicate that creatine has no meaningful effect on fat mass [15]. Interestingly, in children (n=9) suffering from cancer (acute lymphoblastic leukemia), creatine significantly reduced body fat % over time (p<0.05) [15]. A limitation of individual studies is that it is typically difficult to obtain adequate statistical power to detect small differences between creatine and placebo over time due to small sample sizes. Combining studies into a meta-analysis helps overcome this limitation by assessing a large cohort of individuals. However, the meta-analytic effects of resistance exercise and creatine supplementation in adults < 50 years of age is unknown. This is important to determine because a common belief held by many exercising individuals is that creatine supplementation increases fat mass over time [15]. Therefore, the purpose of this systematic review and meta-analysis was to determine the effects of resistance exercise and creatine supplementation on measures of fat mass (i.e., absolute and body fat %) in adults < 50 years of age, while accounting for several associated variables, including creatine dose and duration, and health status.
2. Materials and Methods
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) standards were followed to conduct this systematic review and meta-analysis [16] and the protocol was registered in the PROSPERO (International Prospective Register of Systematic Reviews) database (CRD:42023416700).
2.1. Search Strategy
From the inception to April 2023, two separate reviewers (K.P. and F.R.) searched PubMed, Scopus, Web of Science, and the Cochrane library, using the following keywords: "creatine supplementation" OR “creatine” OR "creatine monohydrate" AND "body fat*" OR "body composition". The following inclusion criteria was used: (1) studies had to be randomized controlled trials (RCTs); (2) mean age of participants <50 years; (3) intervention group was receiving creatine monohydrate and the comparator group was receiving placebo; (4) evaluation of fat mass was performed via dual x-ray absorptiometry (DXA), bioelectrical impedance (BIA), hydrodensitometry, magnetic resonance imaging (MRI), computed tomography (CT) scan, or air displacement plethysmography (Bod Pod); and (5) a minimum study duration of 4 weeks. Studies were excluded if: (1) they were not RCTs; (2) had no full text; or (3) had subjects with any kind of dietary restrictions (i.e., vegans/vegetarians).
2.2. Data Extraction and Risk of Bias
Data was independently extracted by two investigators (K.P. and F.R.). Name of the first author, publication date, country of origin, study design, participant age, sex, and health status, sample size, outcomes assessed, dose and duration of creatine supplementation, fat mass assessment tool, and dietary intake assessment, were among the information that was extracted. A third investigator (D.G.C.) settled disagreements between the authors. Version 2 of the Cochrane risk-of-bias 2 instrument for randomized trials (RoB2) was used to evaluate the quality of the included studies, and it was reviewed by two independent reviewers (K.P. and S.C.F.). Appraisal of risk of bias using the RoB2 tool included the assessment of the following domains of bias in RCTs: (1) randomization process, (2) deviations from intended interventions, (3) missing outcome data, (4) measurement of the outcome, and (5) selection of the reported result. Study quality was categorized as either low risk of bias, considerable concerns, or high risk of bias using the RoB2 tool rating system.
2.3. Statistical Analysis
The mean differences between groups were calculated by comparing changes in outcomes from baseline to follow-up, treating quantitative data as continuous measurements. Standardized mean differences were employed when measurement units were inconsistent (e.g., body fat % changes mixed with absolute body fat kilogram changes) and could not be changed to the units needed for the analyses. The inverse-variance approach and the random-effects model were used to determine statistical significance. Standard deviations and missing data for any changes between baseline and follow-up outcome data were determined by deriving a correlation coefficient of 0.5, considering that a value of standard deviation change from baseline derived from an included study was not provided.
Utilizing the overlap of their 95% confidence intervals (CIs) and expressing the results as a measurement of Cochran's Q (χ2 test) and I2, statistical heterogeneity of outcome measurements across included studies was evaluated. Low heterogeneity was considered when I2 levels were <50%, moderate heterogeneity between 50% to 74.9%, and high heterogeneity ≥75%. Subgroup analyses based on age (<40 years vs 41-49 years), sex (males only vs females only vs mixed sexes), fat mass assessment tool (DXA vs. BIA vs. Hydrodensitometry vs. Bod Pod), body mass index (BMI) (<25 kg/m2 vs. ≥25 kg/m2), creatine monohydrate duration (< 8 weeks vs ≥ 8 weeks) and dose (≤ 5 g/d vs > 5 g/d) were performed. Additionally, sensitivity analyses were performed to evaluate the robustness of reported statistical results by discounting the effects of lack of dietary intake assessment, participants with comorbidities, and studies with increased risk of bias. The meta-analyses were synthesized using Cochrane’s Review Manager (RevMan 5.4.1) software.
3. Results
3.1. Literature Search
In the initial literature search, 3028 publications were found. Of these, 486 duplicate publications were eliminated, leaving 2542 distinct publications from which, 2134 were deemed ineligible and another 376 publications were not retrieved due to irrelevant study designs and outcomes of interest. In total, 32 RCTs investigating the effects of creatine monohydrate on body fat in adults aged <50 years were found. After further examination of the remaining publications five of these used skinfold calipers for the measurement of body fat, four used creatine monohydrate in the absence of resistance training, three had a short-term treatment duration (<4 weeks), two used the Siri equation to quantify body fat, one had inadequate data, one used endurance training, one used high intensity interval training, and three did not have a standardized resistance training protocol. Overall, 12 RCTs were included in this systematic review and meta-analysis (Figure 1) involving 266 participants (130 in the creatine monohydrate and resistance exercise group and 133 in the placebo and resistance exercise group). A detailed description of the included studies is depicted in Table 1.
3.2. Creatine Supplementation and Body Fat Changes
Our main analysis showed that creatine supplementation did not significantly impact changes in absolute fat mass (kg) over time (k = 7; MD = -0.09; 95%CI, -1.20 – 1.03; I2 = 0%; P = 0.88) (Figure 2). However, creatine did produce a significant reduction in body fat % over time (k = 10; MD = -1.19; 95% CI, -2.03 – -0.34; I2 = 0%; P = 0.006) (Figure 3).
Subgroup analysis based on age (<40 years vs. 41-49 years) showed that creatine supplementation did not influence fat mass more than placebo (<40 years: SMD = -0.18; 95%CI, -0.44 – 0.08; I2 = 0%; P = 0.18 vs. 41-49 years: SMD = -0.05; 95%CI, -0.73 – 0.63; P = 0.88) (Figure S1). Similar results were found with regards to fat mass assessment tool (DXA: SMD = -0.13; 95%CI, -0.46 – 0.20; I2 = 0%; P = 0.44 vs. BIA: SMD = -0.27; 95%CI, -0.99 – 0.45; P = 0.47 vs. hydrodensitometry: SMD = -0.17; 95%CI, -0.62 – 0.29; I2 = 0%; P = 0.47 vs. Bod Pod: SMD = -0.26; 95%CI, -1.35 – 0.84; P = 0.65) (Figure S2), BMI (<25 kg/m2: SMD = -0.14; 95%CI, -0.45 – 0.16; I2 = 0%; P = 0.36 vs. ≥25 kg/m2: SMD = -0.20; 95%CI, -0.61 – 0.22; I2 = 6%; P = 0.35) (Figure S3), sex (Females only: SMD = 0.08; 95%CI, -0.69 – 0.85; P = 0.84 vs. Males only: SMD = -0.19; 95%CI, -0.45 – 0.08; I2 = 0%; P = 0.17 vs. Mixed: SMD = -0.26; 95%CI, -1.35 – 0.84; P = 0.65) (Figure S4), creatine dose (<5 g: SMD = -0.12; 95%CI, -0.43 – 0.18; I2 = 0%; P = 0.43 vs. ≥5 g: SMD = -0.24; 95%CI, -0.65 – 0.17; I2 = 2%; P = 0.26) (Figure S5), and duration of supplementation (<8 weeks: SMD = -0.08; 95%CI, -0.41 – 0.25; I2 = 0%; P = 0.63 vs. ≥8 weeks: SMD = -0.28; 95%CI, -0.69 – 0.13; I2 = 20%; P = 0.18) (Figure S6).
Sensitivity analysis excluding participants with health conditions (Healthy participants: SMD = -0.18; 95%CI, -0.44 – 0.08; I2 = 0%; P = 0.18 vs. Unhealthy participants: SMD = -0.05; 95%CI, -0.73 – 0.63; P = 0.88) (Figure S7), studies that did not assess for dietary intake (Assessment: SMD = -0.20; 95%CI, -0.52 – 0.11; I2 = 0%; P = 0.20 vs. No assessment: SMD = -0.10; 95%CI, -0.49 – 0.29; I2 = 0%; P = 0.61) (Figure S8), and studies with increased risk of bias (SMD = -0.19; 95%CI, -0.45 – 0.08; I2 = 0%; P = 0.17) (Figure S9), did not alter any of the findings.
3.3. Risk of Bias Assessment
Four of the studies were classified as having a low risk of bias [17,18,19,20], six studies had a moderate risk [21,22,23,24,25,26], while two studies had a high risk of bias [27,28]. These concerns primarily arose due to the absence of specific details regarding randomization procedures or treatment allocation, considering that two studies did not report whether the participants were randomized [27,28]. Lastly, in one study, the supplement was provided in a single-blind fashion [26]. A detailed description of the risk of bias assessment is depicted in Figure 4.
4. Discussion
This is the first meta-analysis to examine the efficacy of resistance exercise and creatine supplementation on measures of fat mass in adults < 50 years of age. Results showed that the combination of resistance exercise and creatine supplementation (≥ 4 weeks) significantly reduced body fat % by 1.19% (p=0.006) and also led to a small, non-significant reduction in absolute fat mass (-0.09 kg; p=0.88) compared to resistance exercise alone. Variables such as age (< 40 years: p=0.18; 41-49 years: p=0.88), sex (females only: p=0.84; males only: p=0.17; females and males combined: p=0.65), fat mass assessment tool (p=0.36 to 0.65), creatine dosage (< 5 grams: p=0.43; ≥ 5 grams: p=0.26) and duration of creatine supplementation (< 8 weeks: p=0.63; ≥ 8 weeks: p=0.18) did not alter these findings (p>0.05)..
These reductions in fat mass from resistance exercise and creatine supplementation in adults < 50 years are compatible to our previous meta-analysis findings in adults ≥ 50 years (absolute fat mass: -0.50 kg; p=013; body fat %: -0.55; p=0.04) using similar inclusion criteria. Collectively, results across meta-analyses indicate that the combination of resistance exercise and creatine supplementation produces a very small reduction in body fat % in adults ≥ 18 years. These findings refute the common belief held by many exercising individuals that creatine supplementation increases fat mass over time [15].
From a population health perspective, the combination of resistance exercise and creatine supplementation may have some (albeit very small) application for helping attenuate global obesity rates and escalating healthcare costs. According to the 2023 World Obesity Atlas report [29], over 4 billion people will be diagnosed with obesity by the year 2035, costing almost $4 trillion annually. Obesity also contributes to other adverse conditions such as stroke, heart disease, type 2 diabetes, and different types of cancer [30], putting substantial strain on the global healthcare system.
Mechanistically, the small reduction in body fat % from creatine may be related to its involvement in adipose tissue metabolism and whole-body energy expenditure [11,14]. There are two major types of adipose tissue, white adipose tissue (WAT) and brown adipose tissue (BAT) [31]. Traditionally, WAT is purported to store energy and BAT plays a critical role in non-shivering thermogenesis through both independent and dependent effects of uncoupling protein-1 (UCP-1) [11]. However, there is a growing body of evidence that WAT is not inert and can be altered to simulate the phenotypical and functional characteristics of BAT [31], through a process known as “browning” [32]. This process activates beige adipocytes residing in WAT depots [32]. Due to the quantity of WAT an individual possess, activation of this type of adipose tissue may play an important role in thermoregulation and has the potential to significantly increases daily whole-body energy expenditure [31]. Therefore, increasing properties of WAT could lead to decreases in fat mass over time. In Sprague-Dawley rats (16 male, 16 female), creatine supplementation (2.5 g/L, 5 g/L, 10 g/L that corresponds to ~2.5, 4.7, and 9.0 g/day in an average 70 kg human) for 8 weeks significantly increased WAT mitochondrial markers (COXIV, PDH-E1 α) and that these mitochondrial markers respond in a sex and depot specific manner [31]. For example, in inguinal WAT the female rats had significantly elevated increases in COXIV, PDH-E1 α, and cytochrome C protein content, while in the male rats, gonadal WAT specific increases in COXIV and PDH-E1 α protein content were increased [31]. Furthermore, in transgenic mice lacking either the adipose tissue creatine transporter (Adipo-CrT knockout) or the ability to endogenously synthesize creatine (Adipo-Gatm knockout) both leading to low total creatine levels, had significant reductions in beige adipose tissue oxidative metabolism and whole-body energy expenditure resulting in an increase in fat mass compared to control mice [13,14]. Others has shown that a reduction in creatine in beige adipose tissue impairs energy expenditure and adipose metabolic rate in mice [11,33]. In examining the effects of creatine supplementation (20 g/day for 5 days followed by 5g/day for 51 days) in adults with total cholesterol levels > 200 mg/dL, Earnest et al. [34] showed that creatine significantly reduced plasma triglyceride levels by 23% over time.
Beyond these potential direct mechanisms, creatine supplementation may indirectly have a favorable effect on fat mass through its positive effect on lean tissue mass and muscle accretion. Several meta-analyses have been performed collectively showing that the combination of creatine supplementation and resistance exercise increases measures of whole-body lean tissue mass by ~1.37 kg compared to placebo and resistance exercise [35,36,37,38,39]. Furthermore, Burke et al. [40] performed a systematic review and meta-analysis involving 10 studies and found significant improvements in direct measures of limb muscle hypertrophy (0.10-0.16 cm; as measured using ultrasound and peripheral quantitative computed tomography [pQCT]) in the upper- and lower-body from creatine supplementation and resistance exercise compared to resistance exercise and placebo. Interestingly, the lone study that used pQCT showed that creatine supplementation (52 weeks) increased lower-limb muscle density (Δ +0.83 ± 1.15 mg·cm-3; p = 0.016) compared to placebo (Δ -0.16 ± 1.56 mg·cm-3). Mechanistically, these lean tissue mass and muscle improvements may be related to creatine increasing cellular hydration status, high-energy phosphate metabolism (phosphocreatine content and recovery), glycogen synthesis, satellite cell proliferation and activity, growth factor production and expression (i.e., insulin-like growth factor-1), myogenic transcription factor expression (Myf5, Mrf4, MyoD, myogenin), protein kinases downstream in the mammalian target of rapamycin (mTOR) signaling pathway which are involved in translation and decreasing measures of inflammation, oxidative stress (reactive oxygen species) and protein catabolism (whole-body leucine oxidation, urinary excretion of 3-methylhistidine) [36]. The significant increases in whole-body lean tissue mass, limb muscle hypertrophy and muscle density from creatine supplementation may increase energy expenditure which could reduce fat mass over time [41]. Our results indirectly support this notion as there was a statistically significant reduction in body fat % with only a small, non-significant change, in fat mass over time. Unfortunately, the mechanistic effects of creatine, with and without resistance exercise, in healthy adults (≥ 18 years) is unknown.
5. Conclusions
In adults < 50 years of age, the combination of resistance exercise and creatine supplementation results in a significant reduction in body fat % (1.19%, p=0.006) and non-significant reduction in fat mass (-0.09 kg, p=0.88) compared to resistance exercise alone.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, D.G.C., S.C.F., K.P; methodology, D.G.C., S.C.F. K.P, F.R; validation, S.C.F, K.P.; formal analysis, S.C.F., K.P. writing—original draft preparation, all authors; writing—review and editing, all authors.
Funding
This research received no external funding .
Institutional Review Board Statement
Not applicable .
Informed Consent Statement
Not applicable .
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
S.C.F. previously served as a scientific advisor for a company that sold creatine ; has received creatine donations for scientific studies ; and sells creatine education resources. D.G.C. has conducted industry sponsored research involving creatine supplementation and received creatine donations for scientific studies and travel support for presentations involving creatine supplementation at scientific conferences. In addition, D.G.C. serves on the Scientific Advisory Board for Alzchem (a company that manufactures creatine) and as an expert witness/consultant in legal cases involving creatine supplementation. B.C. has received grants and contracts to conduct research on dietary supplements ; has served as a paid consultant for industry; has received honoraria for speaking at conferences and writing lay articles about sports nutrition ingredients and topics; and has served as an expert witness on behalf of the plaintiff and defense in cases involving dietary supplements. S.M.O. serves on the Scientific Advisory Board for Alzchem (a company that manufactures creatine). SMO owns patent “Sports Supplements Based on Liquid Creatine” at European Patent Office (WO2019150323 A1), and active patent application “Synergistic Creatine” at UK Intellectual Property Office (GB2012773.4). SMO has served as a speaker at Abbott Nutrition, a consultant of Allied Beverages Adriatic and IMLEK, and has received research funding related to creatine from the Serbian Ministry of Education, Science, and Technological Development, Provincial Secretariat for Higher Education and Scientific Research, AlzChem GmbH, KW Pfannenschmidt GmbH, ThermoLife International LLC, and Hueston Hennigan LLP. K.P and F.R. declare no conflicts.
References
- Souza, N.A.B.; Rimes-Dias, K.A.; Costa, J.C.; Canella, D.S. Weight Gain and Change in Body Mass Index after Age 20 in the Brazilian Population and Associated Sociodemographic Factors: Data from the National Health Survey. Int. J. Environ. Res. Public Health 2022, 19. [Google Scholar] [CrossRef]
- Frank, A.P.; De Souza Santos, R.; Palmer, B.F.; Clegg, D.J. Determinants of body fat distribution in humans may provide insight about obesity-related health risks. J. Lipid Res. 2019, 60, 1710–1719. [Google Scholar] [CrossRef]
- Simmonds, M.; Llewellyn, A.; Owen, C.G.; Woolacott, N. Predicting adult obesity from childhood obesity: a systematic review and meta-analysis. Obes. Rev. 2016, 17, 95–107. [Google Scholar] [CrossRef]
- Jakicic, J.M.; Powell, K.E.; Campbell, W.W.; Dipietro, L.; Pate, R.R.; Pescatello, L.S.; Collins, K.A.; Bloodgood, B.; Piercy, K.L. Physical Activity and the Prevention of Weight Gain in Adults: A Systematic Review. Med. Sci. Sports Exerc. 2019, 51, 1262–1269. [Google Scholar] [CrossRef]
- Fruh, S.; Williams, S.; Hayes, K.; Hauff, C.; Hudson, G.M.; Sittig, S.; Graves, R.J.; Hall, H.; Barinas, J. A practical approach to obesity prevention: Healthy home habits. J. Am. Assoc. Nurse Pract. 2021, 33, 1055–1065. [Google Scholar] [CrossRef] [PubMed]
- Wewege, M.A.; Desai, I.; Honey, C.; Coorie, B.; Jones, M.D.; Clifford, B.K.; Leake, H.B.; Hagstrom, A.D. The Effect of Resistance Training in Healthy Adults on Body Fat Percentage, Fat Mass and Visceral Fat: A Systematic Review and Meta-Analysis. Sports Med. 2022, 52, 287–300. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie-Shalders, K.; Kelly, J.T.; So, D.; Coffey, V.G.; Byrne, N.M. The effect of exercise interventions on resting metabolic rate: A systematic review and meta-analysis. J. Sports Sci. 2020, 38, 1635–1649. [Google Scholar] [CrossRef] [PubMed]
- Schuenke, M.D.; Mikat, R.P.; McBride, J.M. Effect of an acute period of resistance exercise on excess post-exercise oxygen consumption: implications for body mass management. Eur. J. Appl. Physiol. 2002, 86, 411–417. [Google Scholar] [CrossRef]
- Vechetti, I.J.; Peck, B.D.; Wen, Y.; Walton, R.G.; Valentino, T.R.; Alimov, A.P.; Dungan, C.M.; Van Pelt, D.W.; von Walden, F.; Alkner, B.; et al. Mechanical overload-induced muscle-derived extracellular vesicles promote adipose tissue lipolysis. FASEB J. 2021, 35. [Google Scholar] [CrossRef]
- Forbes, S.; Candow, D.; Krentz, J.; Roberts, M.; Young, K. Changes in Fat Mass Following Creatine Supplementation and Resistance Training in Adults ≥50 Years of Age: A Meta-Analysis. J. Funct. Morphol. Kinesiol. 2019, 4. [Google Scholar] [CrossRef]
- Kazak, L.; Chouchani, E.T.; Jedrychowski, M.P.; Erickson, B.K.; Shinoda, K.; Cohen, P.; Vetrivelan, R.; Lu, G.Z.; Laznik-Bogoslavski, D.; Hasenfuss, S.C.; et al. A creatine-driven substrate cycle enhances energy expenditure and thermogenesis in beige fat. Cell 2015, 163, 643–655. [Google Scholar] [CrossRef]
- Kazak, L.; Cohen, P. Creatine metabolism: energy homeostasis, immunity and cancer biology. Nat. Rev. Endocrinol. 2020, 16, 421–436. [Google Scholar] [CrossRef] [PubMed]
- Kazak, L.; Chouchani, E.T.; Lu, G.Z.; Jedrychowski, M.P.; Bare, C.J.; Mina, A.I.; Kumari, M.; Zhang, S.; Vuckovic, I.; Laznik-Bogoslavski, D.; et al. Genetic Depletion of Adipocyte Creatine Metabolism Inhibits Diet-Induced Thermogenesis and Drives Obesity. Cell Metab. 2017, 26, 660–671.e3. [Google Scholar] [CrossRef] [PubMed]
- Kazak, L.; Rahbani, J.F.; Samborska, B.; Lu, G.Z.; Jedrychowski, M.P.; Lajoie, M.; Zhang, S.; Ramsay, L.A.; Dou, F.Y.; Tenen, D.; et al. Ablation of adipocyte creatine transport impairs thermogenesis and causes diet-induced obesity. Nat. Metab. 2019, 1, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Antonio, J.; Candow, D.G.; Forbes, S.C.; Gualano, B.; Jagim, A.R.; Kreider, R.B.; Rawson, E.S.; Smith-Ryan, A.E.; VanDusseldorp, T.A.; Willoughby, D.S.; et al. Common questions and misconceptions about creatine supplementation: what does the scientific evidence really show? J. Int. Soc. Sports Nutr. 2021, 18, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, T.; Syrotuik, D. Effects of creatine monohydrate supplementation on body composition and strength indices in experienced resistance trained women. J. strength Cond. Res. 2006, 20, 939–946. [Google Scholar] [CrossRef]
- Pakulak, A.; Candow, D.G.; Totosy de Zepetnek, J.; Forbes, S.C.; Basta, D. Effects of Creatine and Caffeine Supplementation During Resistance Training on Body Composition, Strength, Endurance, Rating of Perceived Exertion and Fatigue in Trained Young Adults. J. Diet. Suppl. 2022, 19, 587–602. [Google Scholar] [CrossRef]
- Hoffman, J.; Ratamess, N.; Kang, J.; Mangine, G.; Faigenbaum, A.; Stout, J. Effect of creatine and beta-alanine supplementation on performance and endocrine responses in strength/power athletes. Int. J. Sport Nutr. Exerc. Metab. 2006, 16, 430–446. [Google Scholar] [CrossRef]
- Sakkas, G.K.; Mulligan, K.; DaSilva, M.; Doyle, J.W.; Khatami, H.; Schleich, T.; Kent-Braun, J.A.; Schambelan, M. Creatine fails to augment the benefits from resistance training in patients with HIV infection: a randomized, double-blind, placebo-controlled study. PLoS One 2009, 4. [Google Scholar] [CrossRef]
- Arciero, P.J.; Hannibal, N.S.; Nindl, B.C.; Gentile, C.L.; Hamed, J.; Vukovich, M.D. Comparison of creatine ingestion and resistance training on energy expenditure and limb blood flow. Metab. - Clin. Exp. 2001, 50, 1429–1434. [Google Scholar] [CrossRef]
- Bemben, M.G.; Bemben, D.A.; Loftiss, D.D.; Knehans, A.W. Creatine supplementation during resistance training in college football athletes. Med. Sci. Sports Exerc. 2001, 33, 1667–1673. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.C.; Fang, C.C.; Lee, Y.H.; Yang, M.T.; Chan, K.H. Effects of 4-Week Creatine Supplementation Combined with Complex Training on Muscle Damage and Sport Performance. Nutrients 2018, 10. [Google Scholar] [CrossRef]
- Kreider, R.; Ferreira, M.; Wilson, M.; Grindstaff, P.; Plisk, S.; Reinardy, J.; Cantler, E.; Almada, A. Effects of creatine supplementation on body composition, strength, and sprint performance. Med. Sci. Sports Exerc. 1998, 30, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Volek, J.S.; Ratamess, N.A.; Rubin, M.R.; Gómez, A.L.; French, D.N.; McGuigan, M.M.; Scheett, T.P.; Sharman, M.J.; Häkkinen, K.; Kraemer, W.J. The effects of creatine supplementation on muscular performance and body composition responses to short-term resistance training overreaching. Eur. J. Appl. Physiol. 2004, 91, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Wilder, N.; Deivert, R.G.; Hagerman, F.; Gilders, R. The Effects of Low-Dose Creatine Supplementation Versus Creatine Loading in Collegiate Football Players. J. Athl. Train. 2001, 36, 124. [Google Scholar]
- Becque, M.D.; Lochmann, J.D.; Melrose, D.R. Effects of oral creatine supplementation on muscular strength and body composition. Med. Sci. Sports Exerc. 2000, 32, 654–658. [Google Scholar] [CrossRef] [PubMed]
- Kutz, M.; Gunter, M. Creatine monohydrate supplementation on body weight and percent body fat. J. Strength Cond. Res. 2003, 17, 817–821. [Google Scholar]
- WOF Obesity Atlas 2023 | World Obesity Federation Global Obesity Observatory. Available online: https://data.worldobesity.org/publications/?cat=19 (accessed on May 24, 2023).
- Wannamethee, S.G.; Atkins, J.L. Muscle loss and obesity: the health implications of sarcopenia and sarcopenic obesity. Proc. Nutr. Soc. 2015, 74, 405–412. [Google Scholar] [CrossRef]
- Ryan, C.R.; Finch, M.S.; Dunham, T.C.; Murphy, J.E.; Roy, B.D.; Macpherson, R.E.K. Creatine Monohydrate Supplementation Increases White Adipose Tissue Mitochondrial Markers in Male and Female Rats in a Depot Specific Manner. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Chang, E.; Varghese, M.; Singer, K. Gender and Sex Differences in Adipose Tissue. Curr. Diab. Rep. 2018, 18. [Google Scholar] [CrossRef] [PubMed]
- Wakatsuki, T.; Hirata, F.; Ohno, H.; Yamamoto, M.; Sato, Y.; Ohira, Y. Thermogenic responses to high-energy phosphate contents and/or hindlimb suspension in rats. Jpn. J. Physiol. 1996, 46, 171–175. [Google Scholar] [CrossRef]
- Earnest, C.P.; Almada, A.L.; Mitchell, T.L. High-performance capillary electrophoresis-pure creatine monohydrate reduces blood lipids in men and women. Clin. Sci. (Lond). 1996, 91, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Forbes, S.C.; Candow, D.G.; Ostojic, S.M.; Roberts, M.D.; Chilibeck, P.D. Meta-analysis examining the importance of creatine ingestion strategies on lean tissue mass and strength in older adults. 2021. [Google Scholar] [CrossRef]
- Chilibeck, P.D.; Kaviani, M.; Candow, D.G.; Zello, G.A. Effect of creatine supplementation during resistance training on lean tissue mass and muscular strength in older adults: a meta-analysis. Open Access J. Sport. Med. 2017, 8, 226. [Google Scholar] [CrossRef] [PubMed]
- Delpino, F.M.; Figueiredo, L.M.; Forbes, S.C.; Candow, D.G.; Santos, H.O. Influence of age, sex, and type of exercise on the efficacy of creatine supplementation on lean body mass: A systematic review and meta-analysis of randomized clinical trials. Nutrition 2022, 103–104, 111791. [Google Scholar] [CrossRef]
- Candow, D.G.; Chilibeck, P.D.; Forbes, S.C. Creatine supplementation and aging musculoskeletal health. Endocrine 2014, 45, 354–361. [Google Scholar] [CrossRef]
- Devries, M.C.; Phillips, S.M. Creatine supplementation during resistance training in older adults - A meta-analysis. Med. Sci. Sports Exerc. 2014, 46, 1194–1203. [Google Scholar] [CrossRef]
- Burke, R.; Piñero, A.; Coleman, M.; Mohan, A.; Sapuppo, M.; Augustin, F.; Aragon, A.A.; Candow, D.G.; Forbes, S.C.; Swinton, P.; et al. The Effects of Creatine Supplementation Combined with Resistance Training on Regional Measures of Muscle Hypertrophy: A Systematic Review with Meta-Analysis. Nutrients 2023, 15, 2116. [Google Scholar] [CrossRef]
- Westerterp, K.R. Control of energy expenditure in humans. Eur. J. Clin. Nutr. 2017 713 2016, 71, 340–344. [Google Scholar] [CrossRef]
- Dos Santos, E.E.P.; de Araújo, R.C.; Candow, D.G.; Forbes, S.C.; Guijo, J.A.; de Almeida Santana, C.C.; Do Prado, W.L.; Botero, J.P. Efficacy of Creatine Supplementation Combined with Resistance Training on Muscle Strength and Muscle Mass in Older Females: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3757. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Study selection flow chart.
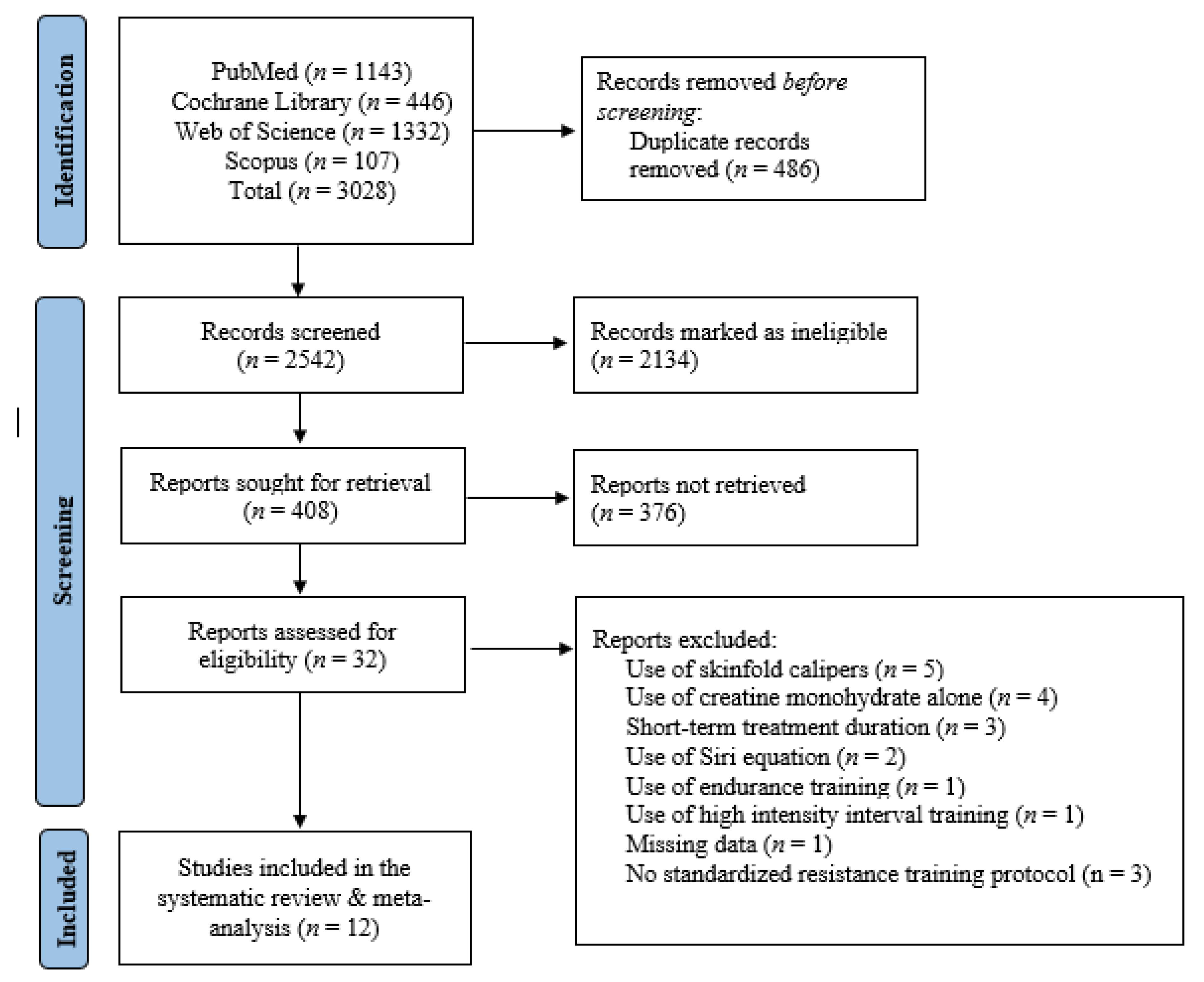
Figure 2.
Forest plots for changes in absolute fat mass (kg).
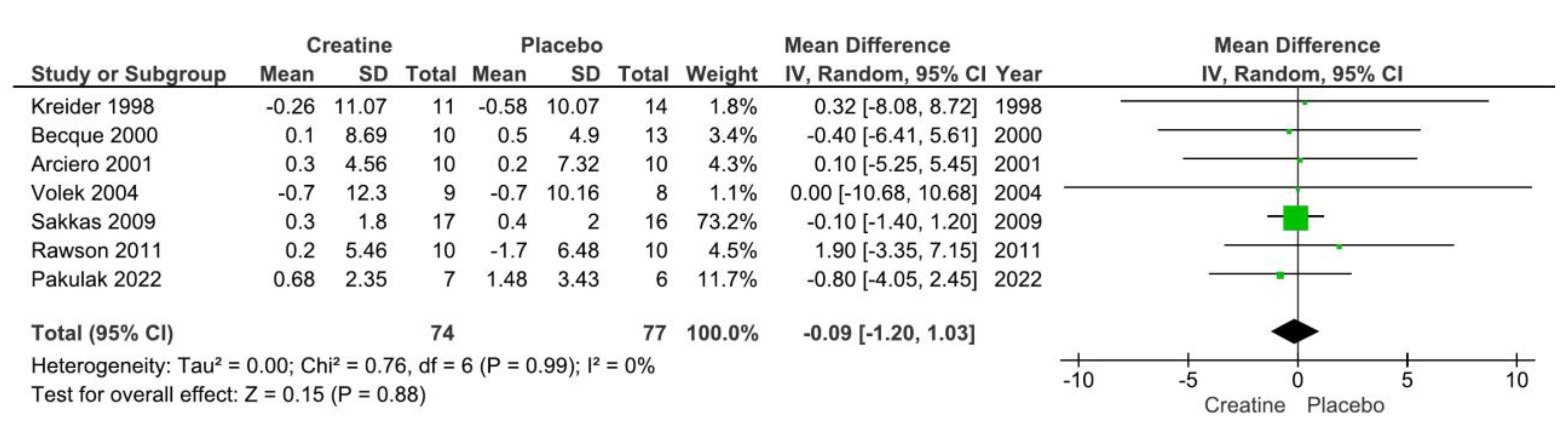
Figure 3.
Forest plot for changes in body fat %.
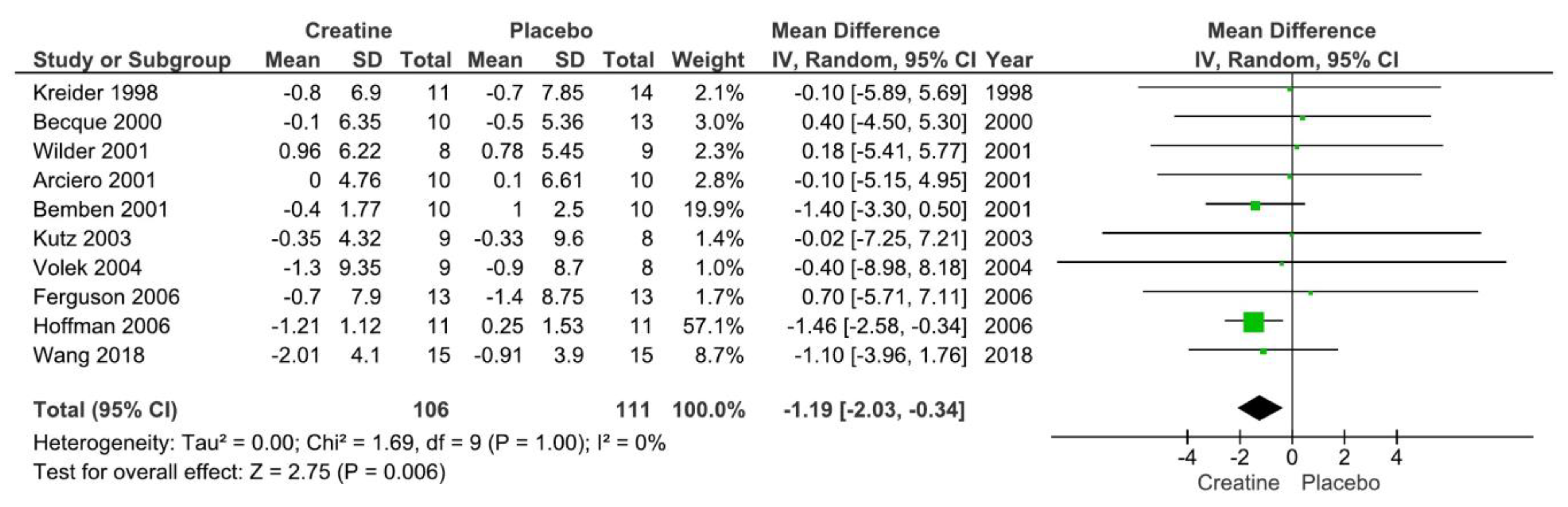
Figure 4.
Risk of bias assessment.
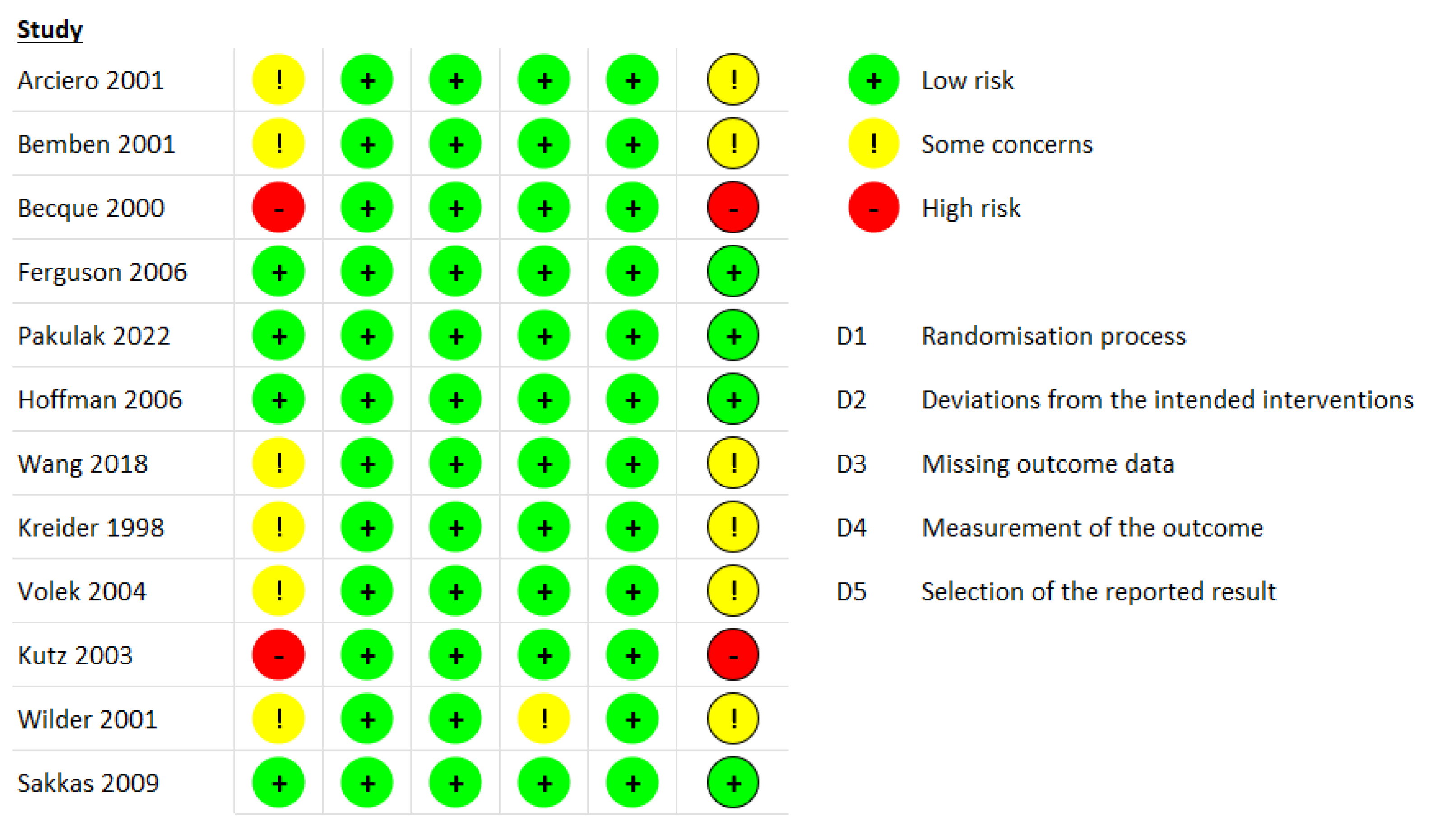

Table 1.
Summary of study characteristics.
| First Author, Year | Population | Supplement Dose | Fat MassTool | Duration | RT Protocol | Result | |
|---|---|---|---|---|---|---|---|
| Arciero et al. 2001 | N=30; Healthy males (21±3 y | CR: 20 g/day (5 g 4 x daily) for 5 days and then 10 g/day (5 g 2 x daily) for the remainder; PLA: same dosing as CR (dextrose) | DEXA | 28 days | RT 3x/wk; 2 sets of 10 @ 70% 1RM and 1 set performed to failure. | CR ↑ body mass, FFM, and RMR. ↔ fat mass or %BF. | |
| Becque et al. 2000 | N=23; healthy males with at least 1 y weight training experience (CR: n=10; PLA: n=13); Age: 21.5±2.7 y | CR: 20 g/day (5 g 4 x daily) for 5 days and then 2 g/day for the remainder; PLA: same dosing as CR (sucrose). | hydrodensitometry | 6 weeks | RT 2/wk (arm flexor: preacher curl). | CR ↑ body mass, FFM. ↔ fat mass or %BF. | |
| Bemben et al. 2001 | N=25 NCAA Division 1 football athletes; (PLA: n=8; CR: n=9; Control: n=8). Age: 18-22 y | CR: 20 g/d (4 equal doses) for 5 d followed by 5 g/d; PLA: same dose (sodium phosphate) | hydrodensitometry | 9 weeks | RT 4/wk split routine. | CR ↑ LBM, body mass. ↔ on %BF. | |
| Ferguson and Syrotuik 2006 | N=26 healthy recreationally strength trained women Age: 18-35 y | CR: 0.3 g/kg/d for 7 days and then 0.03 g/kg/d for the remainder or PLA | DEXA | 10 weeks | RT 4x/wks split routine. | ↔ between groups for LBM, fat mass, %BF, or total body mass. | |
| Hoffman et al. 2006 | N=33 male strength power athletes. Age: not reported | CR: 10.5 g/day or PLA: Dextrose | DEXA | 10 weeks | RT 4x/wks split routine. | ↔ between groups for LBM, fat mass, %BF, or total body mass. | |
| Kreider et al. 1998 | N=25 NCAA Division 1 football athletes. Age: 19.9±0.3 y | CR: 15.75 g/day or PLA | DEXA | 28 days | RT: 4x/wk + agility/sprint training 3x/wk | CR ↑ body mass and LBM; ↔ fat mass or %BF | |
| Kutz and Gunter 2003 | N=17 active males. Age: 22.9±4.9 y. | CR: 30 g/day for 2 weeks followed by 15 g/day for the remainder or PLA (dextrose) | hydrodensitometry | 4 weeks | RT: 2x/wk lower body only | CR ↑ body mass and TBW; ↔ %BF | |
| Pakulak et al. 2022 | N=28 resistance trained males and females (CR: n=7; PLA: n=6). Age: 18-38 y. | CR: 0.1 g/kg/d or PLA (maltodextrin) | air displacement plethysmography | 6 weeks | RT: 5-6x/wk split routine | ↔ FFM, fat mass, body mass | |
| Sakkas et al. 2009 | N=40 HIV-positive men | CR: 20 g/day for 5 days followed by 4.8 g/d for the remainder or PLA | DEXA | 14 weeks | RT: 3x/wk | CR ↑ body mass and LBM; ↔ fat mass | |
| Volek et al. 2003 | N=17 healthy males; 21±3 y | CR: 0.3 g/kg/d for 7 days followed by 0.05 g/kg/d for the remainder or PLA (cellulose) | DEXA | 4 weeks | RT: 5x/wk | CR ↑ body mass and LBM (trend); ↔ fat mass, %BF | |
| Wang et al. 2018 | N=30 males athletes (baseball, basketball, tchoukball); age: 20±2 y. | CR: 20 g/day for 6 days followed by 2 g/d for the remainder or PLA (cellulose) | Bioelectrical impedance analysis | 4 weeks | RT: Complex training including heavy resistance training and plyometrics 3x/wk. | ↔ %BF, body mass or FFM. There was a main effect of time for %BF | |
| Wilder et al. 2001 | N=25 division 1A collegiate football players; age: 20±2 y | CR: 20 g/day for 6 days followed by 5 g/d for the remainder or 3 g/day or PLA (cellulose) | hydrodensitometry | 4 weeks | RT: Complex training including heavy resistance training and plyometrics 3x/wk. | ↔ %BF, FFM. | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



