
Submitted:
19 June 2023
Posted:
19 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The severe respiratory distress syndrome (SRDS) has been a significant clinical issue in modern respiratory medicine. Its role in COVID-19 pandemic is not well defined. Outside-the-hospital SRDS is usually community-acquired septic pneumonia; however, in-hospitals incidences are complicated by co-infections. While SRDS is genetically selected in European and African origins, these are not clear in Middle East, particularly in COVID-19 backgrounds. There is a severe paucity in high quality data on correlations between COVID-19, ARDS, co-infectome, and patient demographics. We have conducted a comprehensive investigation on 298 patients for associations of SRDS, coinfections, and patient demographics on COVID-19 patients’ outcomes. Of these, 9.4% (n=28) had SRDS, and the rest (90.6%) had not. 54% of those with SRDS died while 84% survived; SRDS fatality was highly significant (Chi-square test P-value = 0.00000246). Irrespective of gender, the age of patients was significantly associated with SRDS (72.9 +/-8.9) compared to those without it (56.2 +/-15.1). However, there was no significant difference neither in the age of admitted patients before COVID-19 (58.5 +/-15.3) and during COVID-19 (57.2 +/-15.5) nor in the gender and COVID-19 fatality (Fisher Exact test 2-sided 1.000, 1-sided .546) ruling out that SRDS age-specificity were selected by virus susceptibility. A 100% of SRDS patients without bacterial co-infections survived while only 25% of those with co- infectome did not; this association was highly significant (P value= 0.00041). Co-infections alone without underlying SRDS was also associated with high fatality among patients (P value= 0.00000000076). Almost all COVID-19 patients without co-infectome (99.2%) survived while 28% of those with bacterial co-infection died. The major bacterial pathogens that potentially predisposed to SRDS, were Acinetobacter baumannii, and Escherichia coli either alone or in a mixed infection with Klebsiella pneumoniae were predominant species identified during SRDS attack. Thus, Gram-negative co-infectome potentially induced fatal SRDS aggravating COVID-19 outcome. These findings have significant clinical implications in specific differential diagnosis of SRDS syndromes for subsequent empiric therapy and patient management strategies. Future vertical investigation for similar mechanisms of cytokine-induced SRDS by Gram negative pathogens is imperative since hypervirulent strains are rapidly circulating in the region. The study is limited by a single center study confined to Ha’il hospitals; large scale investigation in major national hospitals would gain more insights.
Keywords:
SRDS
; Co-infections
; COVID-19 fatality
; co-evolution of virulence
1. Introduction
The acute or severe respiratory distress syndrome (SRDS) has been regarded as a significant clinical issue in respiratory medicine ever since it was first described, over five decades ago [1]. Poor oxygenation, pulmonary infiltrates, and an early onset are the hallmarks of the SRDS (this form will be used hereafter to mean both SRDS and ARDS), a life-threatening illness that affects seriously ill patients. The ratio of the patient’s oxygen saturation in arterial blood (PaO2) to the oxygen content of inspired air is used to define SRDS (FiO2). The PaO2/FiO2 ratio for these patients is under 300. The Berlin definition of SRDS [2] was modified in 2012 where the term “acute lung injury” was excluded. Few effective therapy approaches exist to treat SRDS, which has a significant fatality rate [3,4]. A number of studies have found more severe reductions in lung compliance and less responsiveness to positive end-expiratory pressure (PEEP) when the SRDS was caused by a pulmonary process as opposed to an extrapulmonary precipitant, such as sepsis, raising doubts about the validity of the assumption that different inciting events cause a similar pattern of lung injury and similar clinical features [5,6,7]. Therefore, it is not clear what are the mechanism(s) and pre-disposing factors involved in ARDS and particularly, how it is stimulated during COVID-19. To understand these mechanisms and how SRDS is triggered during the course of SARS-CoV-2 infection , it has become imperative to understand the rates and frequencies of SRDS before and after COVID-19 pandemic. This is particularly relevant in the context of co-infections that aggravate the disease.
The epidemiology of SRDS is important in understanding different mechanisms of its evolution. Since its first description by Ashbaugh et al.[1] in 1967, the SRDS has been widely recognized as a major clinical problem worldwide with high morbidity and mortality burdens [8,9,10]. Although the recent Berlin definition [2] is probably much better than previous ones, there is still a high variability in both epidemiology and clinical outcomes in diverse healthcare settings [11]. In fact, the incidence of SRDS ranges from 1.5 cases per 100 000 [11] to nearly 79 cases per 100 000 [11] with European countries reporting a lower incidence than USA [12]. Moreover, studies from Brazil reported incidence rates ranging from 1.8 to 31 per 100 000 [13,14].
Although the overall survival rate is increasing [15,16], the in-hospital mortality rate varies significantly across a number of observational studies [8,9,13,15,16,17,18]. This might be accounted for by variations in risk factors, diagnostic accessibility, awareness of SRDS, and some selection biases impacting clinical trials [19]. The incidence of SRDS was recently assessed across 459 intensive care units (ICUs) in 50 countries as part of a major worldwide observational research (the LUNG SAFE trial) [20]. Any patient included in the trial was selected using a computer algorithm based on the Berlin criteria [2] in order to evaluate the clinical recognition of SRDS in accordance with the most recent definition, and the diagnosis provided by the attending physicians was then compared. The SRDS occurred in 10.4% of overall ICU admissions and in 23.4% of patients requiring mechanical ventilation among 4499 patients who developed acute hypoxemic respiratory failure. In comparison to South America, Asia, and Africa, higher incidence rates were found in North America, Oceania, and Europe. According to the Berlin criteria, 30.0% of patients had mild SRDS, 46.6% had moderate, and the remaining 23.4% had severe SRDS. Only 34% of patients had clinical evidence of SRDS on day 1 and 60.2% had it by the end of their ICU stay, although clinical evidence of SRDS was frequently delayed and less common in mild cases than in severe ones [20]. The LUNG SAFE trial’s adjunctive therapies and ventilator management were among its secondary endpoints, the use of optimal mechanical ventilation was low, and even adjunctive treatments were underutilized for ARDS patients [21,22,23]. Thus, the severity of SRDS worsened in 19% of patients, in-hospital mortality was 40%, and fatality increased concurrently with higher driving pressure reaching 46% severe SRDS [20].
There are over 60 probable predisposing risk factors for SARS-CoV-2 induced SRDS; the most frequent are different types of pneumonias. The majority of SRDS incidences, however, are due to a small number of prevalent causes [24,25,26,27,28]. The most frequent and widely studies aetiologies are pneumonia (40 %), sepsis (32 %), and aspiration (9%) as reported on 107 patients in a medical intensive care unit [29]. There are some known risk factors that are prone to stimulate SRDS indirectly. These include pneumonia as the most common cause outside-the-hospital SRDS [30]. in the form of community-acquired pneumonia. Its alarming rates of increasing mortality of up to 25% triggered high concern of clinicians and public healthy practicians globally. Streptococcus pneumoniae [31]. Legionella pneumophila, Pneumocystis jirovecii, Staphylococcus aureus, enteric gram-negative organisms, and several respiratory viruses are examples of common pathogens [32,33]. The percentage likelihood of particular infectious aetiologies may also fluctuate depending on the local presence of particular microorganisms (eg, high prevalence of SARS-CoV-2 during the COVID-19 pandemic and subsequent surges). Additionally, nosocomial pneumonias can develop into SRDS. The most frequently mentioned pathogens include Staphylococcus aureus, Pseudomonas aeruginosa, and other enteric gram-negative bacteria. Although methicillin-resistant Staphylococcus aureus (MRSA) has been linked to nosocomial pneumonia in some publications, MRSA has also been implicated in cases of community-acquired pneumonia (CAP). Community-acquired MRSA (CA-MRSA) pneumonia is thought to be the major etiology in the past decade. However, these rates are entirely dependent on local profiles of circulating strains which record much high rates in most countries. Intensive care unit admission and in-patient mortality were more severe clinical outcomes for patients with CA-MRSA pneumonia than for those with pneumococcal CAP [34]. According to some studies, the fatality rate for CA-MRSA pneumonia might range from 56% to 63% [35,36]. The pathogenicity of Panton-Valentine leukocidin (PVL) is frequently linked to CA-MRSA strains [37]. Extensive lung necrosis, multilobular infiltrates, leucopenia, hemoptysis, and sepsis are symptoms of CAP caused by MRSA bearing the PVL gene, therefore increases the mortality rate [38,39].
The second most common trigger of SRDS is sepsis [40,41,42,43]. Every time SRDS manifests in a patient, sepsis is the first etiology to be taken into consideration. Community-acquired pneumonia (CAP) is a most severe infection in communities and/or extended home-cares worldwide due to the septic necrotizing pneumonia [44,45,46,47]. Staphylococcus aureus hospital pulmonary sepsis has been postulated to correlate with SRDS for years until a recent study confirmed the MRSA direct involvement and the role of FTY720 S-phosphonate in endothelial cell protection [48]. Estimated 30 million cases of lung sepsis annually have led to more than eight million deaths, i.e.,15–30% in high-income countries and 50% or higher in low-and middle-income countries [49]. It becomes critically serious when pvl-positive S. aureus (CA-MRSA lineage) are involved in SRDS conditions. More importantly, clinical management is particularly challenging when the etiologic scenarios in SRDS and superantigenic CA-MRSA pneumonias are further complicated by similar respiratory Covid-19 and/or skin monkeypox syndromes. For these reasons, rapid differential diagnosis of pneumonia cases is imperative for successful clinical management strategies. Thus, multi-point surveillance of S. aureus lineages including MRSA and PVL- positive S. aureus in nosocomial setting is important for control of necrotizing pneumonia, SRDS, and early recognition of potential aggravation by monkeypox or Covid-19. Data is limited in these new aspects of COVID-19 complicated bacterial infections. In recent years, with the increase in global population dynamics a significant increase in community associated lung infections have occurred globally. Despite the remarkable progress made in advancing healthcare systems, pneumonia associated to lung sepsis remains a burdensome in global public health [50,51]. Furthermore, the high complexity and costs associated to lung care complicates cases leading to high morbidity and mortality. Particularly, the clinical and economic burden of CAP is staggering, far-reaching, and expected to increase as new antibiotic resistance mechanisms emerge while the world’s population ages [52]. In the US alone, the annual hospitalization rate for CAP is more than USD$ 2.6 million, ranking second only to childbirth for hospital admissions [available at: https://www.hcup-us.ahrq.gov/db/nation/nis/NIS_Introduction_2017.jsp] accessed May 24 2022, the Agency for Healthcare Research and Quality National: regional estimates on hospital use for all patients from the HCUP National Inpatient Survey (NIS 2017)]. Therefore, a leading cause of death worldwide is sepsis especially when developed as a dysregulated immune response to infectious pneumonia [53,54]. The potential risk of S. aureus in these cases is quite high.
There have many observations in the SRDS susceptibility and mortality rates, whether due to COVID or other reasons, related to different predisposing factors in different populations. Although the prognosis is basically the same for both sexes, there are observations that men may be marginally more prone to develop SRDS than women. Less frequently do patients who are female or shorter in stature receive lung-protective ventilator tidal volumes. Female patients with severe chronic SRDS died at a greater rate than male patients. Black and Hispanic patients with SRDS showed greater fatality rates in at least one study, which appeared to be mediated by increased severity of illness. Nevertheless, black individuals may have a lower chance of having SRDS. Risk factors for SRDS also include exposure to ambient air pollutants, alcohol usage, hypoalbuminemia, chemotherapy during the past six months, and tobacco use. Thus, selective susceptibility to SRDS and COVID-19 still requires additional understanding.
COVID-19 was a main reason for SRDS during recent months and it appears to have worse outcomes than SRDS from other causes. Early studies to characterize the COVID-19 host immune response showed an immunological signature made up of high serum cytokines[55,56]. Compared to other viruses, COVID-19 and influenza are both linked to a compromised IFN-I and -III host response. However, the severity of the impairment is inversely correlated with COVID-19. In addition, age has emerged as a dominating predictor of illness severity and mortality risk, even though the precise mechanisms by which SARS-CoV-2 produces SRDS and how particular host characteristics increase the chance of developing severe disease remain unknown. Early on in the epidemic, reports from China and Italy indicated case-fatality rates of 15-20% among patients over the age of 80 compared to 1% among patients under the age of 50 [57] and concluded that COVID-19 SRDS appeared to have a worse outcome than SRDS from other causes. Patients with COVID-19 SRDS who were hospitalized in ICU experienced mortality rates ranging from 26% to 61.5%, and patients receiving mechanical ventilation experienced mortality rates ranging from 65.7% to 94%. Numerous studies have demonstrated that the pathophysiological characteristics of COVID-19 SRDS are equal to those of non-COVID-19 ARDS [56]. These findings indicate that there is a knowledge gap in these areas of research.
Thus, specific diagnosis of COVID-19-mediated, bacterial infectome-induced, or non-infectious SRDS syndromes has become imperative for clinical management of patients. These overlapping mechanisms render clinicians ponder over several scenarios involved; particularly, in cases requiring immediate interventions without laboratory aid. Diagnosis of SRDS cannot be confirmed or disproven by a single diagnostic test that adds another layer of difficulty. Furthermore, according to the Berlin definition’s expansion, it must be emphasized that SRDS is currently diagnosed only based on clinical criteria and is a syndrome rather than a particular pathologic entity until, one is specifically identified. Therefore, diagnosis of SRDS necessitates the presence of bilateral chest radiographic abnormalities and new or worsening respiratory distress for seven days or less, the inability of heart failure to fully explain the hypoxemia and radiographic infiltrates, and clinical significance of the impaired oxygenation. In contrast to earlier definitions [58], the Berlin criteria offered more precise guidance on chest radiograph patterns that are indicative of SRDS, such as bilateral opacities consistent with pulmonary oedema that can be patchy or asymmetric, and those that are not, such as isolated pleural effusions, atelectasis, or tumors. Reliance on CT pictures is challenging to distinguish COVID-19 from other types of bacterial pneumonia because the images largely overlap. While many investigations revealed a wide range of CT findings in COVID-19, there is a consensus that the presence of ground glass opacities (GGO), often with a peripheral and subpleural distribution, is the key CT characteristic of COVID-19 pneumonia. Also, the absence of centrilobular nodules and mucoid impactions makes the characteristics of COVID-19 pneumonia different [59,60,61]. In addition, there is currently a lack of pathological data on COVID-19 pneumonia, based on autopsy or biopsy results. Furthermore, for patients with severe hypoxia and those on high doses of vasoactive drugs, continuous renal replacement therapy, or other ICU procedures, obtaining a CT scan can be difficult. Moreover, CT costs money and exposes patients to ionizing radiation, which limits its repeatability [62,63]. In the Kigali update to the Berlin definition of ARDS, lung ultrasonography has been suggested as a substitute for chest radiography in settings with limited resources. However, sonographic B lines from hydrostatic pulmonary oedema are indistinguishable from those in SRDS. Combining cardiac and lung ultrasonography can be suggest a cardiogenic process, although heart failure and SRDS can coexist complicating the issue. Ultrasound visualizes primarily subpleural lung zones and can yield poor-quality images in the presence of extensive overlying soft tissue (as seen with obesity) or subcutaneous oedema [62,64,65]. Thus, for these and other several reasons, baseline association studies, such as this work, are required to lay solid foundations for rapid primary differential diagnosis of respiratory illnesses with emphasis on COVID-19- and bacterial co-infectome-induced distresses. The aim of this study was to conduct a comprehensive investigation for associations of SRDS, coinfections, and patient demographics on COVID-19 patients’ outcomes with emphasis on the potential influence of each on specific diagnosis.
2. Materials and Methods
Hospital and laboratory records on different SRDS, COVID-19, and co-infection scenarios data recorded pre-COVID-19, during COVID-19, and in COVID-19-co-infection backgrounds. Since there is no clear-cut diagnostic procedure available for one-step diagnosis of SRDS, multiple indicative criteria that usually followed including standard guidelines’ meeting definitions were collected (tests shown below). SARS-CoV-2 infection can be confirmed by positive detection of viral RNA in nasopharyngeal secretions using a specific PCR test. COVID-19 illness can be confirmed by a consistent clinical history, epidemiological contact, and a positive SARS-CoV-2 test. COVID-19 SRDS is diagnosed when a confirmed COVID-19 infection meets the Berlin 2012 ARDS diagnostic criteria: these are (i) acute hypoxaemic respiratory failure; (ii) presentation within 1 week of worsening respiratory symptoms; (iii) bilateral airspace disease on chest x-ray, computed tomography (CT) or ultrasound that is not fully explained by effusions, lobar or lung collapse, or nodules; and (iv) cardiac failure is not the primary cause of acute hypoxaemic respiratory failure. These criteria identify new or worsening respiratory symptoms, profound hypoxemia, bilateral pulmonary opacities on radiography, and inability to explain respiratory failure by cardiac failure or fluid overload. Therefore, pre-COVID SRDS is familiar; however, its association with SARS-CoV-2 viral-pneumonia and other microbial co-infections is not always successfully differentiated.
2.1. Work environment
The Ha’il University Health Research Laboratories and Health Ha’il cluster units are standard laboratory center, including Ha’il Regional Health Laboratory which is certified and accredited by the Saudi Central Board for Accreditation of Healthcare Institutions (CBAHI)-Code 2739. All patients are hospitalized at Ha’il hospitals including the King Salman Specialist Hospital (KSSH), Ha’il, Kingdom of Saudi Arabia (KSA). The KSSH hospital is a 500-bed tertiary care hospital designated to COVID-19 patients in addition to other specialized medical care services to Ha’il and all socioeconomic populations of the region. The KSSH is certified and accredited by the Saudi Central Board for Accreditation of Healthcare Institutions (CBAHI)-Ref.no. HAL/MOH/HO5/34213.
2.2. Study Designs
This is an experimental records with retrospective cross-sectional study at the King Salman Specialist Hospital (KSSH), Ha’il, Kingdom of Saudi Arabia (KSA). The hospital is a 500-bed tertiary care hospital designated to COVID-19 patients in addition to other specialized medical care services to Ha’il and all socioeconomic populations of the region. The hospital is certified and accredited by the Saudi Central Board for Accreditation of Healthcare Institutions (CBAHI) (Ref. No. HAL/MOH/HO5/34213). The KSSH has been designated to receive COVID-19 patients. A panel of experts consisting of clinical microbiologists, laboratory specialists, and clinicians reviewed the list of criteria, COVID-19-compatible clinical profiles, and test results. COVID-19 patients records were used to estimate the overall frequency of SDRS and to monitor the rates of bacterial co-infections. To study influence of individual bacteria pathogens, we mde sure no double infections or its different emerging variants, disease patterns, and isolate properties, as well as ensuring that the isolation period was the same for non-co-infected patients and co-infected patients. For ICU patients, the average stay was around two-three weeks from admission. COVID-19 diagnosis for all participating patients was confirmed by clinically compatible symptoms and by real-time reverse transcription PCR (RT-PCR) testing performed on nasopharyngeal throat swab specimens at the Ha’il Health Regional Laboratory (HHRL) for COVID-19.
2.3. Supporting examinations and tests performed for confirmation
- 2. Oxygen: Non-invasive ventilation procedures, such as supplemental oxygen in patients with signs of severe respiratory distress, or hypoxemia (i.e., SpO2 < 90%) delivered by ventilation. Initial oxygen therapy at 5 L/min and titrated to SpO2 ≥ 90%. High oxygen flows (10–15 or 50–60 L/min) is usually delivered through a face mask with a reservoir bag to reach a higher concentration of oxygen according to Borghes and Maroldi [26]66 Nava et al., 2011 [27]67 and Keenan et al., 2011 [28]68. All these protocols usually from simple to aggressive, as follows: First, a nasal canula (~4 L), then a simple facemask (~10 L), followed by a non-Rebreather mask (~15 L). If necessary, these are then followed by noninvasive medical ventilations for high flow, such as high-flow nasal canula (100 L) or Bilevel positive airway pressure (BiPAP). Often, tracheal intubation for high oxygen is required.
- Intubation: Mechanical ventilations increased difficulties with breathing or hypoxemia after using non-invasive ventilation. Invasive mechanical ventilation through an endotracheal tube or tracheostomy by an ICU expert according to the NIH NHLBI ARDS Clinical Network’s mechanical ventilation protocol card, available at: http://www.ardsnet.org/system/files/ Ventilator%20Protocol%20Card.pd (accessed on 5 December 2021).
- Records of Microbial Co-Infection or Superinfection and their antimicrobial Susceptibility Data during SRDS co-infections
Routine microbiological investigations data from SDRS cases with clinical COVID-19 co-infecting pathogens were collected. Bacterial coinfectomes (bacterial pathogens co infected with SARS-CoV-2 virus) were studied case-by-case basis during the overall evaluations. The susceptibility testing results recorded in accordance with the recommendations of the Clinical and Laboratory Standard Institute (CLSI document M100S-26)71 were used to categorize resistance classifications.
2.4. Statistical Analysis of the data
Data from different sources and experimental procedures were analyzed using Statistical Package for Social Sciences software. (IBM SPSS; Version 24 SPSS version 23.0 for Windows (SPSS, Inc., Chicago, IL, USA). The study was descriptive analysis and stratified; we presented absolute numbers, proportions, and graphical distributions. We used Fisher exact statistical, Chai tests for proportions and showed p-values where appropriate (a p-value <0.05 was considered statistically significant).
3. Results
Death rate among patients with and without SRDS
In this study, we have examined 298 patients; 9.4% (n=28) of whom had SRDS, and the rest (90.6%) had not. As shown in Figure 1, 54% of those patients with SRDS died while 84% of those without the syndrome survived. Statistical analysis of the relationship between COVID-19 case fatality in patients with underlying SRDS revealed that among COVID-19 patients, in those with SRDS, fatality incidence was highly significantly associated as indicated by the Chi-square test P-value (p value = 0.00000246). In addition, to test the notion that a specific age-range or age-group could be a potential risk factor in susceptibility to SRDS attack, we examined the ages of the target population (see Figure 2 for details). There was a significant difference in the age of patients with SRDS (72.9 +/-8.9) compared to those patients without SRDS (56.2 +/-15.1) (Figure 2 and Table 1).
To confirm whether this finding could be an age-specific susceptibility factor selected by SARS-CoV-2, we analyzed the age factor before and during COVID-19 in admitted patients; there was no significant difference in the age of admitted patients before COVID-19 (58.5 +/-15.3) and during COVID-19 (57.2 +/-15.5) (Table 2a). Similarly, we further examined the probability of the influence of gender differences in COVID-19 patients with underlying SRDS(Table 2b). However, to avoid bias in result interpretations, we first examined potential gender-based resistance to SARS-CoV-2 infection in humans. Since it has been widely established by reports and a substantial body of knowledge that women could be more likely to resistant SAR-CoV2 infection than men, we studied gender differences before and during COVID-19 pandemic. Among the study population of 298 patients, we did not find any significant association between studied patients’ gender and COVID-19 disease incidence (Table 2b; Fisher Exact test 2-sided 1.000, 1-sided .546). To avoid potential confounder, we also studied the relationships between the gender of target population and SRDS cases (Table 2c); no significant association was found (P value Exact sig 2-sided .553, Exact Sig 1-sided .307. To rule out any association between case fatality and gender, we analyzed associations between the sex of patients and death and found no significant association ( Fisher’s Exact Test 2-sided .772; 1-sided .433) and Chi square test P value .754) (Table 2d). Furthermore, the probability that SDRS predisposes to coinfection was also remote (Table 2e); (Pearson Chi-Square P value .106; Fisher’s Exact test. 2-side .114; 1-sided .077) was insignificant. However, when we reversed dependents, there was a highly significant association deaths as explained below.
In this study, we report on the significance of bacterial infections in COVID-19 patients with underlying SRDS. As shown in Figure 3, all SRDS patients who did not have bacterial co-infections along with SARS-CoV2 (100%, n=8) fortunately survived the incidence. However, only 25% of those who had bacterial infections along with the virus did not survive. This association of bacterial co-infections along with SARS-CoV-2 in SRDS patients was highly significant as determined by the Person Chi Square test value (P value= 0.00041). This finding was an overall analysis irrespective of the types of bacterial pathogens which will be examined in a separate analysis as shown below. Furthermore, in an independent investigation, and to confirm the influence of co-infections and SRDS in aggravating COVID-19 patient outcome, we examined bacterial co-infections alone without underlying SRDS on the outcome of studied patients. The case fatality of bacterial co-infection to SARS-CoV-2 among patients without SRDS indicate that there was association with a higher death rate (P value= 0.00000000076) (Figure 4). Almost all COVID-19 patients with no bacterial co-infection with the virus (99.2%) survived. However, 28% of those with bacterial co-infection did not make it. To determine the major bacterial pathogens that potentially predispose to SRDS, we investigated the associations of different infecting bacteria in SRDS cases and found that Acinetobacter baumannii, and Escherichia coli (E. coli) either alone or in a mixed infection with Klebsiella pneumoniae (K. pneumoniae) were predominant species identified during SRDS attack (Table 3).
4. Discussion
Even though 9.4% (n =28) had SRDS, this is significant for the seriousness as the outcome. Usually, SRDS incidence is fatal indicated by the fact that, out of those who had SRDS, over 50% of patients died while 84% of those without the syndrome survived. This is much higher than that reported in other countries72; however, those reported in our study were carefully monitored against several potential aggravating issues and one of the most important factors was revealed association to advanced age related SRDS (Figure 2 Table 1). Unfortunately, there is a severe paucity in high-quality data on the SRDS mechanisms affecting the two extremes of life. For instance, while SRDS post traumatic event was most common in middle-aged adults, albeit patients four years or younger and 65 years or older experienced the highest burden of ARDS related mortality where children were disproportionately affected by the incidence73. For these reasons and to adequately understand the potential confounding factors in the host-pathogen interplay, we asked several research questions and determined influence of SRDS, coinfections, and patient demographics before and after COVID-19 pandemic on patients’ outcomes (Table 2a, b, c,d,e). These included age- and gender-specificities in SRDS fatalities as well as SARS-CoV-2 selective susceptibilities in gender differences. For instance, we examined age association before and during COVID-19 in admitted patients. However, we found no significant age-related differences in COVID-19 patients and no potential gender-based resistance or susceptibility to SARS-CoV-2 infection contrary to the common belief that being a man could be a risk for the virus. This is, in part, consistent with the finding that advanced age was a factor in SARS-CoV-2 susceptibility irrespective of gender74 75. Nevertheless, recent advances support the host-specificity in the virus tropism, transmission dynamics, immune evasion, and virulence in different human population genetic structures76. These findings were critical in minimizing potential pitfalls in the accurate diagnosis and treatment of SRDS and in specifically identifying aggravations by co-infections.
Despite enormous events, the mechanisms of coinfections in aggravating COVID-19 patient outcomes with and without underlying chronic disorders have not yet been clear. In particular, accurate differential diagnosis between the cause of SRDSs whether initiated by COVID-19, bacterial infections, and/or non infectious SRDS has not been well addressed. This is of paramount importance since it directs different specific treatment strategies for each cause. In this study, we have addressed this issue in detail among the examined population where all SRDS patients (100%) without bacterial co-infections survived while 25% of those who had bacterial infections along with the virus did not. Association of bacterial co-infections in SRDS patients was highly significant (Person Chi Square test value P value= 0.00041). These finding, as much as it is significant in aggravating the disease, is an outcome of sum of several subtle mechanisms in host-pathogen interactions that necessitates investigation of each separately of one another. Therefore, from these results we attribute the lung injury due to cytokine storm provoked by a dynamics “infectome” at this stage in discussion. However, while cytokine storm is being reported77 widely in the community-acquired Staphylococcus strains (CA-MRSA) since its pandemic a decade ago, its role in Gram negatives has not yet been widely reported. To substantiate these results, stepwise investigations were necessary to confirm influence of coinfections.
In independent investigations we examined bacterial co-infections alone without underlying SRDS on the outcome of studied patients and found association with a higher death rate (P value= 0.00000000076) (Figure 4). Almost all of those without co-infection (99.2%) survived and 28% of those with bacterial co-infection died. We further determined the major bacterial pathogens that potentially predispose to SRDS and found that Acinetobacter baumannii, and Escherichia coli (E. coli) either alone or in a mixed infection with Klebsiella pneumoniae (K. pneumoniae) were predominant species identified during SRDS attacks (Table 3). This is in agreement with our previous finding that only a few selected Gram-negative pathogens were identified aggravating COVID-19 clinical profiles 78,79. While selective SARS-CoV-2 coinfection by limited pathogens became increasingly evident, their role in the development of stroke and SRDS remained unclear. This has significant clinical implications in differential diagnosis and specific empiric therapy; especially in distinguishing COVID-specific dry cough from a product one due to bacterial infections. Furthermore, SARS-CoV-2 role in stroke has been widely proposed; however, whether coinfections are involved is not fully understood. There are ample evidence for viral tropism loci leading to SRDS. The nasal olfactory bulb expresses different transcript levels in nasal partitioning ration-inspiration (NRP1), ACE2, CD147, TMPRSS2, and Furin, accounting for smell and taste losses80,81. The Higher expression levels of NRP1 in the SARS-CoV-20-infected cells of the olfactory epithelium imply a hematogenous spread - a potential route to stroke in COVID-19 patients. In addition, there are also well-established mechanisms in CA-MRSA superbug induced cytokine storm production in necrotizing pneumonia. However, future vertical investigation for similar mechanisms in these Gram negatives lung pathogenicity has become imperative since the growing outbreak by hypervirulent strains is rapidly circulating 82
Another rather more important reason for differential diagnosis to rule out bacterial co-infection in COVID-19, is the potential molecular mimicry leading to co-protections against virus infections. While other viral co-infections would potentially provide cross-protection against SARS-CoV-2 83–85, this type of cross-protection is rare in case of bacterial co-infection implying a risk of subtle bacterial virulence initiated by SARS-CoV-2. Since rare cases of cross-reactive epitomes with SARS-CoV-2 were reported for proteomes of BCG, Bordetella.pertussis, Corynebacterium .diphtheriae, Clostridium.tetani, Hemophilus.influenzae, Neisseria. meningitidis and Streptococcus.pneumoniae, 86, it implies that similar cases for Gram negatives identified in this study.
5. Conclusion
In conclusion, for the first time to best of our knowledge we report, in a comprehensive investigation, on the frequencies of associations of SRDS, coinfections, and patient demographics on COVID-19 patients’ outcomes. While SRDS and co-infections aggravated case fatality rates of COVID-19 patients either each alone or in combination, advanced age was a factor in SARS-CoV-2 susceptibility irrespective of gender. More importantly, “infectome” of A. baumannii, E. coli, and Klebsiella pneumoniae was identified in all SRDS cases and potentially might have provoked the attacks. These findings have significant clinical implications and the need for specific differential diagnosis of SRDS syndromes induced by COVID-19 and bacterial infection. This is crucial for subsequent empiric therapy and patient management strategies. Future vertical investigation for similar mechanisms of cytokine-induced SRDS by Gram negative pathogens in lung pathogenicity is imperative since the growing outbreak by hypervirulent strains is rapidly circulating 82 in the region. The study has limitations in the single center study confined to Ha’il hospitals; large scale investigation in major national hospitals would gain more insights.
Author Contributions
Conceptualization, Ahmed Alsolami and Kamaleldin Said; Data curation, Ahmed Alsolami, Khalid Farhan Alshammari, Fawwaz Alshammari, Sulaf Alhallabi, Shahad Alafnan, Safia Moussa, Abdelhafiz I. Bashir, Kareemah Alshurtan, Rana Aboras, Ehab Sogaier, Alfatih Alnajib and Kamaleldin Said; Formal analysis, Ahmed Alsolami, Khalid Farhan Alshammari, Fawwaz Alshammari, Sulaf Alhallabi, Shahad Alafnan, Safia Moussa, Abdelhafiz I. Bashir, Kareemah Alshurtan, Rana Aboras, Ehab Sogaier, Alfatih Alnajib and Kamaleldin Said; Funding acquisition, Ahmed Alsolami, Khalid Farhan Alshammari, Fawwaz Alshammari and Kamaleldin Said; Investigation, Ahmed Alsolami, Khalid Farhan Alshammari and Kamaleldin Said; Methodology, Ahmed Alsolami, Khalid Farhan Alshammari, Fawwaz Alshammari, Sulaf Alhallabi, Shahad Alafnan, Safia Moussa, Abdelhafiz I. Bashir, Kareemah Alshurtan, Rana Aboras, Ehab Sogaier, Alfatih Alnajib and Kamaleldin Said; Project administration, Ahmed Alsolami and Kamaleldin Said; Resources, Ahmed Alsolami, Khalid Farhan Alshammari, Fawwaz Alshammari, Sulaf Alhallabi, Shahad Alafnan, Safia Moussa, Abdelhafiz I. Bashir, Kareemah Alshurtan, Rana Aboras, Ehab Sogaier, Alfatih Alnajib and Kamaleldin Said; Software, Ahmed Alsolami, Khalid Farhan Alshammari, Fawwaz Alshammari, Sulaf Alhallabi, Shahad Alafnan, Safia Moussa, Abdelhafiz I. Bashir, Kareemah Alshurtan, Rana Aboras, Ehab Sogaier, Alfatih Alnajib and Kamaleldin Said; Supervision, Ahmed Alsolami and Kamaleldin Said; Validation, Ahmed Alsolami, Khalid Farhan Alshammari, Fawwaz Alshammari, Sulaf Alhallabi, Shahad Alafnan, Safia Moussa, Abdelhafiz I. Bashir, Kareemah Alshurtan, Rana Aboras, Ehab Sogaier, Alfatih Alnajib and Kamaleldin Said; Visualization, Ahmed Alsolami, Khalid Farhan Alshammari, Fawwaz Alshammari, Sulaf Alhallabi, Shahad Alafnan, Safia Moussa, Abdelhafiz I. Bashir, Kareemah Alshurtan, Rana Aboras, Ehab Sogaier, Alfatih Alnajib and Kamaleldin Said; Writing – original draft, Ahmed Alsolami and Kamaleldin Said; Writing – review & editing, Ahmed Alsolami, Khalid Farhan Alshammari, Fawwaz Alshammari, Sulaf Alhallabi, Shahad Alafnan, Safia Moussa, Abdelhafiz I. Bashir, Kareemah Alshurtan, Rana Aboras, Ehab Sogaier, Alfatih Alnajib and Kamaleldin Said.
Funding
This research project was funded by Scientific Research Deanship at the University of Ha’il- Saudi Arabia, through project number RG-21074.
Ethical approval and Institutional Review Board Statement
This project (number RG21074) has been reviewed and Approval by the Research Ethical Committee (REC) of the University of Ha’il, dated 22/11/2021 under numbers H-2021-215, File H-2020-632-16160.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
There is no additional data deposited on any other site other than those in this manuscript.
Acknowledgments
We acknowledge the University of Ha’il for the support and encouragement through the Deanship of Scientific Research.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ashbaugh, D.G.; Bigelow, D.B.; Petty, T.L.; Levine, B.E. ACUTE RESPIRATORY DISTRESS IN ADULTS. The Lancet 1967, 290, 319–323. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Gajic, O.; Dabbagh, O.; Park, P.K.; Adesanya, A.; Chang, S.Y.; Hou, P.; Anderson, H.; Hoth, J.J.; Mikkelsen, M.E.; Gentile, N.T.; et al. Early Identification of Patients at Risk of Acute Lung Injury: Evaluation of Lung Injury Prediction Score in a Multicenter Cohort Study. Am J Respir Crit Care Med 2011, 183, 462–470. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, L.; Xi, X.; Zhou, J.X. The Association Between Etiologies and Mortality in Acute Respiratory Distress Syndrome: A Multicenter Observational Cohort Study. Front Med (Lausanne) 2021, 8. [Google Scholar] [CrossRef]
- Gattinoni, L.; Pelosi, P.; Suter, P.M.; Pedoto, A.; Vercesi, P.; Lissoni, A. Acute Respiratory Distress Syndrome Caused by Pulmonary and Extrapulmonary Disease. Different Syndromes? Am J Respir Crit Care Med 1998, 158, 3–11. [Google Scholar] [CrossRef]
- Lim, C.M.; Jung, H.; Koh, Y.; Lee, J.S.; Shim, T.S.; Lee, S. do; Kim, W.S.; Kim, D.S.; Kim, W.D. Effect of Alveolar Recruitment Maneuver in Early Acute Respiratory Distress Syndrome According to Antiderecruitment Strategy, Etiological Category of Diffuse Lung Injury, and Body Position of the Patient. Crit Care Med 2003, 31, 411–418. [Google Scholar] [CrossRef]
- Tugrul, S.; Akinci, O.; Ozcan, P.E.; Ince, S.; Esen, F.; Telci, L.; Akpir, K.; Cakar, N. Effects of Sustained Inflation and Postinflation Positive End-Expiratory Pressure in Acute Respiratory Distress Syndrome: Focusing on Pulmonary and Extrapulmonary Forms. Crit Care Med 2003, 31, 738–744. [Google Scholar] [CrossRef]
- Brun-Buisson, C.; Minelli, C.; Bertolini, G.; Brazzi, L.; Pimentel, J.; Lewandowski, K.; Bion, J.; Romand, J.A.; Villar, J.; Thorsteinsson, A.; et al. Epidemiology and Outcome of Acute Lung Injury in European Intensive Care Units. Results from the ALIVE Study. Intensive Care Med 2004, 30, 51–61. [Google Scholar] [CrossRef]
- Villar, J.; Blanco, J.; Añón, J.M.; Santos-Bouza, A.; Blanch, L.; Ambrós, A.; Gandía, F.; Carriedo, D.; Mosteiro, F.; Basaldúa, S.; et al. The ALIEN Study: Incidence and Outcome of Acute Respiratory Distress Syndrome in the Era of Lung Protective Ventilation. Intensive Care Med 2011, 37, 1932–1941. [Google Scholar] [CrossRef]
- Rubenfeld, G.D.; Caldwell, E.; Peabody, E.; Weaver, J.; Martin, D.P.; Neff, M.; Stern, E.J.; Hudson, L.D. Incidence and Outcomes of Acute Lung Injury. N Engl J Med 2005, 353, 1685–1693. [Google Scholar] [CrossRef]
- Brun-Buisson, C.; Minelli, C.; Bertolini, G.; Brazzi, L.; Pimentel, J.; Lewandowski, K.; Bion, J.; Romand, J.A.; Villar, J.; Thorsteinsson, A.; et al. Epidemiology and Outcome of Acute Lung Injury in European Intensive Care Units. Results from the ALIVE Study. Intensive Care Med 2004, 30, 51–61. [Google Scholar] [CrossRef]
- Villar, J.; Blanco, J.; Kacmarek, R.M. Current Incidence and Outcome of the Acute Respiratory Distress Syndrome. Curr Opin Crit Care 2016, 22, 1–6. [Google Scholar] [CrossRef]
- Caser, E.B.; Zandonade, E.; Pereira, E.; Gama, A.M.C.; Barbas, C.S.V. Impact of Distinct Definitions of Acute Lung Injury on Its Incidence and Outcomes in Brazilian ICUs: Prospective Evaluation of 7,133 Patients*. Crit Care Med 2014, 42, 574–582. [Google Scholar] [CrossRef]
- Azevedo, L.C.P.; Park, M.; Salluh, J.I.F.; Rea-Neto, A.; Souza-Dantas, V.C.; Varaschin, P.; Oliveira, M.C.; Tierno, P.F.G.M.M.; dal-Pizzol, F.; Silva, U.V.A.; et al. Clinical Outcomes of Patients Requiring Ventilatory Support in Brazilian Intensive Care Units: A Multicenter, Prospective, Cohort Study. Crit Care 2013, 17. [Google Scholar] [CrossRef]
- Cochi, S.E.; Kempker, J.A.; Annangi, S.; Kramer, M.R.; Martin, G.S. Mortality Trends of Acute Respiratory Distress Syndrome in the United States from 1999 to 2013. Ann Am Thorac Soc 2016, 13, 1742–1751. [Google Scholar] [CrossRef]
- Erickson, S.E.; Martin, G.S.; Davis, J.L.; Matthay, M.A.; Eisner, M.D. Recent Trends in Acute Lung Injury Mortality: 1996-2005. Crit Care Med 2009, 37, 1574–1579. [Google Scholar] [CrossRef]
- Sigurdsson, M.I.; Sigvaldason, K.; Gunnarsson, T.S.; Moller, A.; Sigurdsson, G.H. Acute Respiratory Distress Syndrome: Nationwide Changes in Incidence, Treatment and Mortality over 23 Years. Acta Anaesthesiol Scand 2013, 57, 37–45. [Google Scholar] [CrossRef]
- Rubenfeld, G.D.; Caldwell, E.; Peabody, E.; Weaver, J.; Martin, D.P.; Neff, M.; Stern, E.J.; Hudson, L.D. Incidence and Outcomes of Acute Lung Injury. N Engl J Med 2005, 353, 1685–1693. [Google Scholar] [CrossRef]
- Sjoding, M.W.; Cooke, C.R.; Iwashyna, T.J.; Hofer, T.P. Acute Respiratory Distress Syndrome Measurement Error Potential Effect on Clinical Study Results. Ann Am Thorac Soc 2016, 13, 1123–1128. [Google Scholar] [CrossRef]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; van Haren, F.M.P.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef]
- Clinics, B.W.-E. M. ; 2014, undefined. Lung-Protective Ventilation Strategies and Adjunctive Treatments for the Emergency Medicine Patient with Acute Respiratory Failure. emed.theclinics.com. [CrossRef]
- Baron, R.; F1000Research, B.L.-. ; 2016, undefined. Recent Advances in Understanding and Treating ARDS. ncbi.nlm.nih.gov.
- Villar, J.; Schultz, M.J.; Kacmarek, R.M. The LUNG SAFE: A Biased Presentation of the Prevalence of ARDS! Crit Care 2016, 20. [Google Scholar] [CrossRef]
- Zaccardelli, D.S.; Pattishall, E.N. Clinical Diagnostic Criteria of the Adult Respiratory Distress Syndrome in the Intensive Care Unit. Crit Care Med 1996, 24, 247–251. [Google Scholar] [CrossRef]
- Pepe, P.E.; Potkin, R.T.; Reus, D.H.; Hudson, L.D.; Carrico, C.J. Clinical Predictors of the Adult Respiratory Distress Syndrome. Am J Surg 1982, 144, 124–130. [Google Scholar] [CrossRef]
- Hudson, L.D.; Milberg, J.A.; Anardi, D.; Maunder, R.J. Clinical Risks for Development of the Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med 1995, 151 Pt 1, 293–301. [Google Scholar] [CrossRef]
- Fowler, A.A.; Hamman, R.F.; Good, J.T.; Benson, K.N.; Baird, M.; Eberle, D.J.; Petty, T.L.; Hyers, T.M. Adult Respiratory Distress Syndrome: Risk with Common Predispositions. Ann Intern Med 1983, 98 Pt 1, 593–597. [Google Scholar] [CrossRef]
- Villar, J.; Blanco, J.; Añón, J.M.; Santos-Bouza, A.; Blanch, L.; Ambrós, A.; Gandía, F.; Carriedo, D.; Mosteiro, F.; Basaldúa, S.; et al. The ALIEN Study: Incidence and Outcome of Acute Respiratory Distress Syndrome in the Era of Lung Protective Ventilation. Intensive Care Med 2011, 37, 1932–1941. [Google Scholar] [CrossRef]
- Zilberberg, M.D.; Epstein, S.K. Acute Lung Injury in the Medical ICU: Comorbid Conditions, Age, Etiology, and Hospital Outcome. Am J Respir Crit Care Med 1998, 157 Pt 1, 1159–1164. [Google Scholar] [CrossRef]
- Baumann, W.R.; Jung, R.C.; Koss, M.; Boylen, C.T.; Navarro, L.; Sharma, O.P. Incidence and Mortality of Adult Respiratory Distress Syndrome: A Prospective Analysis from a Large Metropolitan Hospital. Crit Care Med 1986, 14, 1–4. [Google Scholar] [CrossRef]
- Mannes, G.P.; Boersma, W.G.; Baur, C.H.; Postmus, P.E. Adult Respiratory Distress Syndrome (ARDS) Due to Bacteraemic Pneumococcal Pneumonia. Eur Respir J 1991, 4, 503–504. [Google Scholar] [CrossRef]
- Pachon, J.; Prados, M.D.; Capote, F.; Cuello, J.A.; Garnacho, J.; Verano, A. Severe Community-Acquired Pneumonia. Etiology, Prognosis, and Treatment. Am Rev Respir Dis 1990, 142, 369–373. [Google Scholar] [CrossRef]
- Torres, A.; Serra-Batlles, J.; Ferrer, A.; Jimenez, P.; Celis, R.; Cobo, E.; Rodriguez-Roisin, R. Severe Community-Acquired Pneumonia. Epidemiology and Prognostic Factors. Am Rev Respir Dis 1991, 144, 312–318. [Google Scholar] [CrossRef]
- Self, W.H.; Wunderink, R.G.; Williams, D.J.; Zhu, Y.; Anderson, E.J.; Balk, R.A.; Fakhran, S.S.; Chappell, J.D.; Casimir, G.; Courtney, D.M.; et al. Staphylococcus Aureus Community-Acquired Pneumonia: Prevalence, Clinical Characteristics, and Outcomes. Clin Infect Dis 2016, 63, 300–309. [Google Scholar] [CrossRef]
- David, M.Z.; Daum, R.S. Community-Associated Methicillin-Resistant Staphylococcus Aureus: Epidemiology and Clinical Consequences of an Emerging Epidemic. Clin Microbiol Rev 2010, 23, 616–687. [Google Scholar] [CrossRef]
- Mandell, L.A.; Wunderink, R. Methicillin-Resistant Staphylococcus Aureus and Community-Acquired Pneumonia: An Evolving Relationship. Clin Infect Dis 2012, 54, 1134–1136. [Google Scholar] [CrossRef]
- Bhatta, D.R.; Cavaco, L.M.; Nath, G.; Kumar, K.; Gaur, A.; Gokhale, S.; Bhatta, D.R. Association of Panton Valentine Leukocidin (PVL) Genes with Methicillin Resistant Staphylococcus Aureus (MRSA) in Western Nepal: A Matter of Concern for Community Infections (a Hospital Based Prospective Study). BMC Infect Dis 2016, 16. [Google Scholar] [CrossRef]
- Francis, J.S.; Doherty, M.C.; Lopatin, U.; Johnston, C.P.; Sinha, G.; Ross, T.; Cai, M.; Hansel, N.N.; Perl, T.; Ticehurst, J.R.; et al. Severe Community-Onset Pneumonia in Healthy Adults Caused by Methicillin-Resistant Staphylococcus Aureus Carrying the Panton-Valentine Leukocidin Genes. Clin Infect Dis 2005, 40, 100–107. [Google Scholar] [CrossRef]
- Gillet, Y.; Issartel, B.; Vanhems, P.; Fournet, J.C.; Lina, G.; Bes, M.; Vandenesch, F.; Piémont, Y.; Brousse, N.; Floret, D.; et al. Association between Staphylococcus Aureus Strains Carrying Gene for Panton-Valentine Leukocidin and Highly Lethal Necrotising Pneumonia in Young Immunocompetent Patients. Lancet 2002, 359, 753–759. [Google Scholar] [CrossRef]
- Pepe, P.E.; Potkin, R.T.; Reus, D.H.; Hudson, L.D.; Carrico, C.J. Clinical Predictors of the Adult Respiratory Distress Syndrome. Am J Surg 1982, 144, 124–130. [Google Scholar] [CrossRef]
- Hudson, L.D.; Milberg, J.A.; Anardi, D.; Maunder, R.J. Clinical Risks for Development of the Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med 1995, 151 Pt 1, 293–301. [Google Scholar] [CrossRef]
- Doyle, R.L.; Szaflarski, N.; Modin, G.W.; Wiener-Kronish, J.P.; Matthay, M.A. Identification of Patients with Acute Lung Injury. Predictors of Mortality. Am J Respir Crit Care Med 1995, 152 Pt 1, 1818–1824. [Google Scholar] [CrossRef]
- Fein, A.M.; Lippmann, M.; Holtzman, H.; Eliraz, A.; Goldberg, S.K. The Risk Factors, Incidence, and Prognosis of ARDS Following Septicemia. Chest 1983, 83, 40–42. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Reyes, L.F.; Aliberti, S.; Restrepo, M.I. Empirical Coverage of Methicillin-Resistant Staphylococcus Aureus in Community-Acquired Pneumonia: Those Who Do Not Remember the Past Are Doomed to Repeat It. Clinical Infectious Diseases 2016, 63, 1145–1146. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Reyes, L.F.; Aliberti, S.; Restrepo, M.I. Empirical Coverage of Methicillin-Resistant Staphylococcus Aureus in Community-Acquired Pneumonia: Those Who Do Not Remember the Past Are Doomed to Repeat It. Clin Infect Dis 2016, 63, 1145–1146. [Google Scholar] [CrossRef]
- Self, W.H.; Wunderink, R.G.; Williams, D.J.; Zhu, Y.; Anderson, E.J.; Balk, R.A.; Fakhran, S.S.; Chappell, J.D.; Casimir, G.; Courtney, D.M.; et al. Staphylococcus Aureus Community-Acquired Pneumonia: Prevalence, Clinical Characteristics, and Outcomes. Clin Infect Dis 2016, 63, 300–309. [Google Scholar] [CrossRef]
- Peyrani, P.; Mandell, L.; Torres, A.; Tillotson, G.S. The Burden of Community-Acquired Bacterial Pneumonia in the Era of Antibiotic Resistance. Expert Rev Respir Med 2019, 13, 139–152. [Google Scholar] [CrossRef]
- Wang, L.; Letsiou, E.; Wang, H.; Belvitch, P.; Meliton, L.N.; Brown, M.E.; Bandela, M.; Chen, J.; Garcia, J.G.N.; Dudek, S.M. MRSA-Induced Endothelial Permeability and Acute Lung Injury Are Attenuated by FTY720 S-Phosphonate. Am J Physiol Lung Cell Mol Physiol 2022, 322, L149–L161. [Google Scholar] [CrossRef]
- Dugani, S.; Veillard, J.; Kissoon, N. Reducing the Global Burden of Sepsis. CMAJ 2017, 189, E2–E3. [Google Scholar] [CrossRef]
- Troeger, C.; Blacker, B.; Khalil, I.A.; Rao, P.C.; Cao, J.; Zimsen, S.R.M.; Albertson, S.B.; Deshpande, A.; Farag, T.; Abebe, Z.; et al. Estimates of the Global, Regional, and National Morbidity, Mortality, and Aetiologies of Lower Respiratory Infections in 195 Countries, 1990-2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis 2018, 18, 1191–1210. [Google Scholar] [CrossRef]
- Naghavi, M.; Wang, H.; Lozano, R.; Davis, A.; Liang, X.; Zhou, M.; Vollset, S.E.; Abbasoglu Ozgoren, A.; Abdalla, S.; Abd-Allah, F.; et al. Global, Regional, and National Age-Sex Specific All-Cause and Cause-Specific Mortality for 240 Causes of Death, 1990-2013: A Systematic Analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171. [Google Scholar] [CrossRef]
- McLaughlin, J.M.; Johnson, M.H.; Kagan, S.A.; Baer, S.L. Clinical and Economic Burden of Community-Acquired Pneumonia in the Veterans Health Administration, 2011: A Retrospective Cohort Study. Infection 2015, 43, 671–680. [Google Scholar] [CrossRef]
- Fernando, S.M.; Rochwerg, B.; Seely, A.J.E. Clinical Implications of the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). CMAJ 2018, 190, E1058–E1059. [Google Scholar] [CrossRef]
- Li, T.; Qian, Y.; Miao, Z.; Zheng, P.; Shi, T.; Jiang, X.; Pan, L.; Qian, F.; Yang, G.; An, H.; et al. Xuebijing Injection Alleviates Pam3CSK4-Induced Inflammatory Response and Protects Mice From Sepsis Caused by Methicillin-Resistant Staphylococcus Aureus. Front Pharmacol 2020, 11. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial Cell Infection and Endotheliitis in COVID-19. The Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. The Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Herold, S.; Becker, C.; Ridge, K.M.; Budinger, G.R.S. Influenza Virus-Induced Lung Injury: Pathogenesis and Implications for Treatment. European Respiratory Journal 2015, 45, 1463–1478. [Google Scholar] [CrossRef]
- Bernard, G.R.; Artigas, A.; Brigham, K.L.; Carlet, J.; Falke, K.; Hudson, L.; Lamy, M.; Legall, J.R.; Morris, A.; Spragg, R.; et al. The American-European Consensus Conference on ARDS. Definitions, Mechanisms, Relevant Outcomes, and Clinical Trial Coordination. https://doi.org/10.1164/ajrccm.149.3.7509706 2012, 149 (3 I), 818–824. [CrossRef]
- Bai, H.X.; Hsieh, B.; Xiong, Z.; Halsey, K.; Choi, J.W.; Tran, T.M.L.; Pan, I.; Shi, L.B.; Wang, D.C.; Mei, J.; et al. Performance of Radiologists in Differentiating COVID-19 from Viral Pneumonia on Chest CT. Radiology 2020, 296, E46–E54. [Google Scholar] [CrossRef]
- Tian, S.; Xiong, Y.; Liu, H.; Niu, L.; Guo, J.; Liao, M.; Xiao, S.Y. Pathological Study of the 2019 Novel Coronavirus Disease (COVID-19) through Postmortem Core Biopsies. Modern Pathology 2020, 33, 1007. [Google Scholar] [CrossRef]
- Hani, C.; Trieu, N.H.; Saab, I.; Dangeard, S.; Bennani, S.; Chassagnon, G.; Revel, M.P. COVID-19 Pneumonia: A Review of Typical CT Findings and Differential Diagnosis. Diagn Interv Imaging 2020, 101, 263. [Google Scholar] [CrossRef]
- Schwarz, M.I.; Albert, R.K. “Imitators” of the ARDS: Implications for Diagnosis and Treatment. Chest 2004, 125, 1530–1535. [Google Scholar] [CrossRef]
- Putman, R.K.; Hunninghake, G.M.; Dieffenbach, P.B.; Barragan-Bradford, D.; Serhan, K.; Adams, U.; Hatabu, H.; Nishino, M.; Padera, R.F.; Fredenburgh, L.E.; et al. Interstitial Lung Abnormalities Are Associated with Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med 2017, 195, 138–141. [Google Scholar] [CrossRef]
- Sekiguchi, H.; Schenck, L.A.; Horie, R.; Suzuki, J.; Lee, E.H.; McMenomy, B.P.; Chen, T.E.; Lekah, A.; Mankad, S. v.; Gajic, O. Critical Care Ultrasonography Differentiates ARDS, Pulmonary Edema, and Other Causes in the Early Course of Acute Hypoxemic Respiratory Failure. Chest 2015, 148, 912–918. [Google Scholar] [CrossRef]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International Evidence-Based Recommendations for Point-of-Care Lung Ultrasound. Intensive Care Med 2012, 38, 577–591. [Google Scholar] [CrossRef]
- Borghesi, A.; Maroldi, R. COVID-19 Outbreak in Italy: Experimental Chest X-Ray Scoring System for Quantifying and Monitoring Disease Progression. Radiol Med 2020, 125, 509–513. [Google Scholar] [CrossRef]
- Nava, S.; Schreiber, A.; Domenighetti, G. Noninvasive Ventilation for Patients with Acute Lung Injury or Acute Respiratory Distress Syndrome. Respir Care 2011, 56, 1583–1588. [Google Scholar] [CrossRef]
- Keenan, S.P.; Sinuff, T.; Burns, K.E.A.; Muscedere, J.; Kutsogiannis, J.; Mehta, S.; Cook, D.J.; Ayas, N.; Adhikari, N.K.J.; Hand, L.; et al. Clinical Practice Guidelines for the Use of Noninvasive Positive-Pressure Ventilation and Noninvasive Continuous Positive Airway Pressure in the Acute Care Setting. CMAJ 2011, 183. [Google Scholar] [CrossRef]
- Fan, B.E.; Chong, V.C.L.; Chan, S.S.W.; Lim, G.H.; Lim, K.G.E.; Tan, G.B.; Mucheli, S.S.; Kuperan, P.; Ong, K.H. Hematologic Parameters in Patients with COVID-19 Infection. Am J Hematol 2020, 95, E131–E134. [Google Scholar] [CrossRef]
- Kaushansky. Williams Hematology, 9e | AccessMedicine | McGraw Hill Medical. Williams Hematology, 9e Eds. Kenneth Kaushansky, et al. McGraw Hill, 2015. Available online: https://accessmedicine.mhmedical.com/book.aspx?bookid=1581&isMissingChapter=true (accessed on 5 December 2021).
- Patel, J. ; C., F.; I., E.G. ; J., S. ; L., J. S. ; B., L. ; M., A. J. ; M., T. ; P., R. ; R., S. S. ; et al. Performance Standards for Antimicrobial Susceptibility Testing An Informational Supplement for Global Application Developed through the Clinical and Laboratory Standards Institute Consensus Process. 26th Edition.
- Asselah, T.; Durantel, D.; Pasmant, E.; Lau, G.; Schinazi, R.F. COVID-19: Discovery, Diagnostics and Drug Development. J Hepatol 2021, 74, 168–184. [Google Scholar] [CrossRef]
- Killien, E.Y.; Mills, B.; Vavilala, M.S.; Watson, R.S.; O’Keefe, G.E.; Rivara, F.P. Association between Age and Acute Respiratory Distress Syndrome Development and Mortality Following Trauma. J Trauma Acute Care Surg 2019, 86, 844–852. [Google Scholar] [CrossRef]
- Fabião, J.; Sassi, B.; Pedrollo, E.F.; Gerchman, F.; Kramer, C.K.; Leitão, C.B.; Pinto, L.C. Why Do Men Have Worse COVID-19-Related Outcomes? A Systematic review and Meta-Analysis with Sex Adjusted for Age. Brazilian Journal of Medical and Biological Research 2022, 55. [Google Scholar] [CrossRef]
- Pachpande, V.; Senapathi, S.H.V.; Williams, K.; Chai, S.; Mandal, S.; Prabhu, S. Demographics, Comorbidities, and Laboratory Parameters in Hospitalized Patients with SARS-CoV2 Infection at a Community Hospital in Rural Pennsylvania. PLoS One 2022, 17. [Google Scholar] [CrossRef]
- Carabelli, A.M.; Peacock, T.P.; Thorne, L.G.; Harvey, W.T.; Hughes, J.; Genomics, C.-19; Consortium, U.K.; Peacock, S.J.; Barclay, W.S.; De Silva, T.I.; et al. Nature Reviews Microbiology SARS-CoV-2 Variant Biology: Immune Escape, Transmission and Fitness. Nature Reviews Microbiology | 2023, 21, 162–177. [Google Scholar] [CrossRef]
- Cao, Z.; Xu, C.; Zhang, P.; Wang, Y. Associations of Sedentary Time and Physical Activity with Adverse Health Conditions: Outcome-Wide Analyses Using Isotemporal Substitution Model. EClinicalMedicine 2022, 48. [Google Scholar] [CrossRef]
- Said, K.B.; Alsolami, A.; Alshammari, F.; Alreshidi, F.S.; Fathuldeen, A.; Alrashid, F.; Bashir, A.I.; Osman, S.; Aboras, R.; Alshammari, A.; et al. Selective COVID-19 Coinfections in Diabetic Patients with Concomitant Cardiovascular Comorbidities Are Associated with Increased Mortality. Pathogens 2022, 11, 508. [Google Scholar] [CrossRef]
- Said, K.B.; Alsolami, A.; Moussa, S.; Alfouzan, F.; Bashir, A.I.; Rashidi, M.; Aborans, R.; Taha, T.E.; Almansour, H.; Alazmi, M.; et al. COVID-19 Clinical Profiles and Fatality Rates in Hospitalized Patients Reveal Case Aggravation and Selective Co-Infection by Limited Gram-Negative Bacteria. Int J Environ Res Public Health 2022, 19, 5270. [Google Scholar] [CrossRef]
- Butowt, R.; von Bartheld, C.S. Anosmia in COVID-19: Underlying Mechanisms and Assessment of an Olfactory Route to Brain Infection. Neuroscientist 2020. [Google Scholar] [CrossRef]
- Brann, D.H.; Tsukahara, T.; Weinreb, C.; Lipovsek, M.; Van Den Berge, K.; Gong, B.; Chance, R.; Macaulay, I.C.; Chou, H.J.; Fletcher, R.B.; et al. Non-Neuronal Expression of SARS-CoV-2 Entry Genes in the Olfactory System Suggests Mechanisms Underlying COVID-19-Associated Anosmia. Sci Adv 2020, 6. [Google Scholar] [CrossRef]
- Hosoda, T.; Harada, S.; Okamoto, K.; Ishino, S.; Kaneko, M.; Suzuki, M.; Ito, R.; Mizoguchi, M. COVID-19 and Fatal Sepsis Caused by Hypervirulent Klebsiella Pneumoniae, Japan, 2020. Emerg Infect Dis 2021, 27, 556. [Google Scholar] [CrossRef]
- Boschiero, M.N.; Duarte, A.; Palamim, C.V.C.; Alvarez, A.E.; Mauch, R.M.; Marson, F.A.L. Frequency of Respiratory Pathogens Other than SARS-CoV-2 Detected during COVID-19 Testing. Diagn Microbiol Infect Dis 2022, 102, undefined. [Google Scholar] [CrossRef]
- Calcagno, A.; Ghisetti, V.; Burdino, E.; Trunfio, M.; Allice, T.; Boglione, L.; Bonora, S.; Di Perri, G. Co-Infection with Other Respiratory Pathogens in COVID-19 Patients. Clinical Microbiology and Infection 2021, 27, 297–298. [Google Scholar] [CrossRef]
- Aran, D.; Beachler, D.C.; Lanes, S.; Overhage, J.M. Prior Presumed Coronavirus Infection Reduces COVID-19 Risk: A Cohort Study. Journal of Infection 2020, 81, 923–930. [Google Scholar] [CrossRef]
- Reche, P.A. Potential Cross-Reactive Immunity to SARS-CoV-2 From Common Human Pathogens and Vaccines. Front Immunol 2020, 11. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Severe Respiratory syndrome case fatality rates among COVID-19 patients.
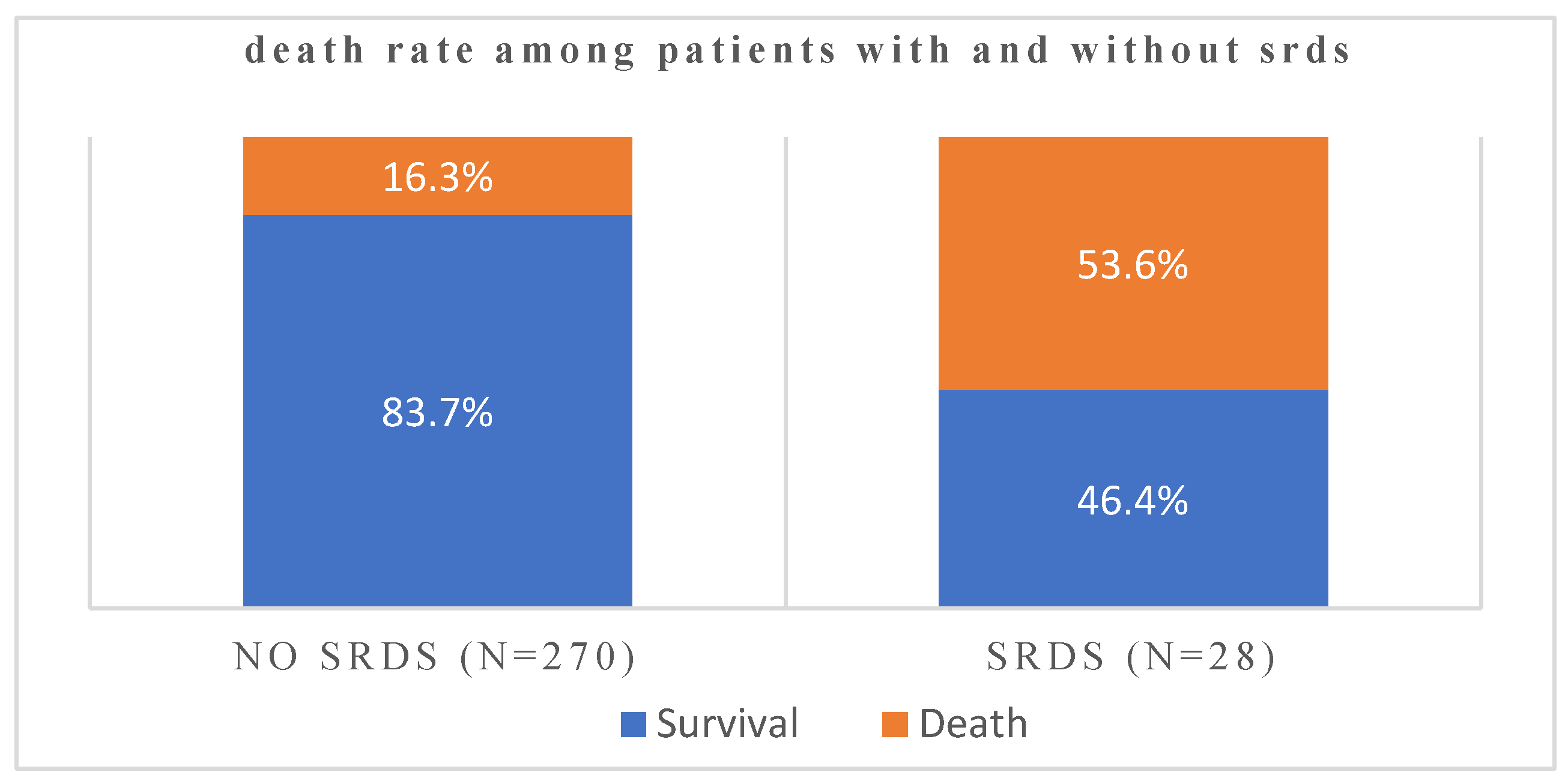
Figure 2.
Association of admitted patients’ age with SRDS incidence rates in the study population.
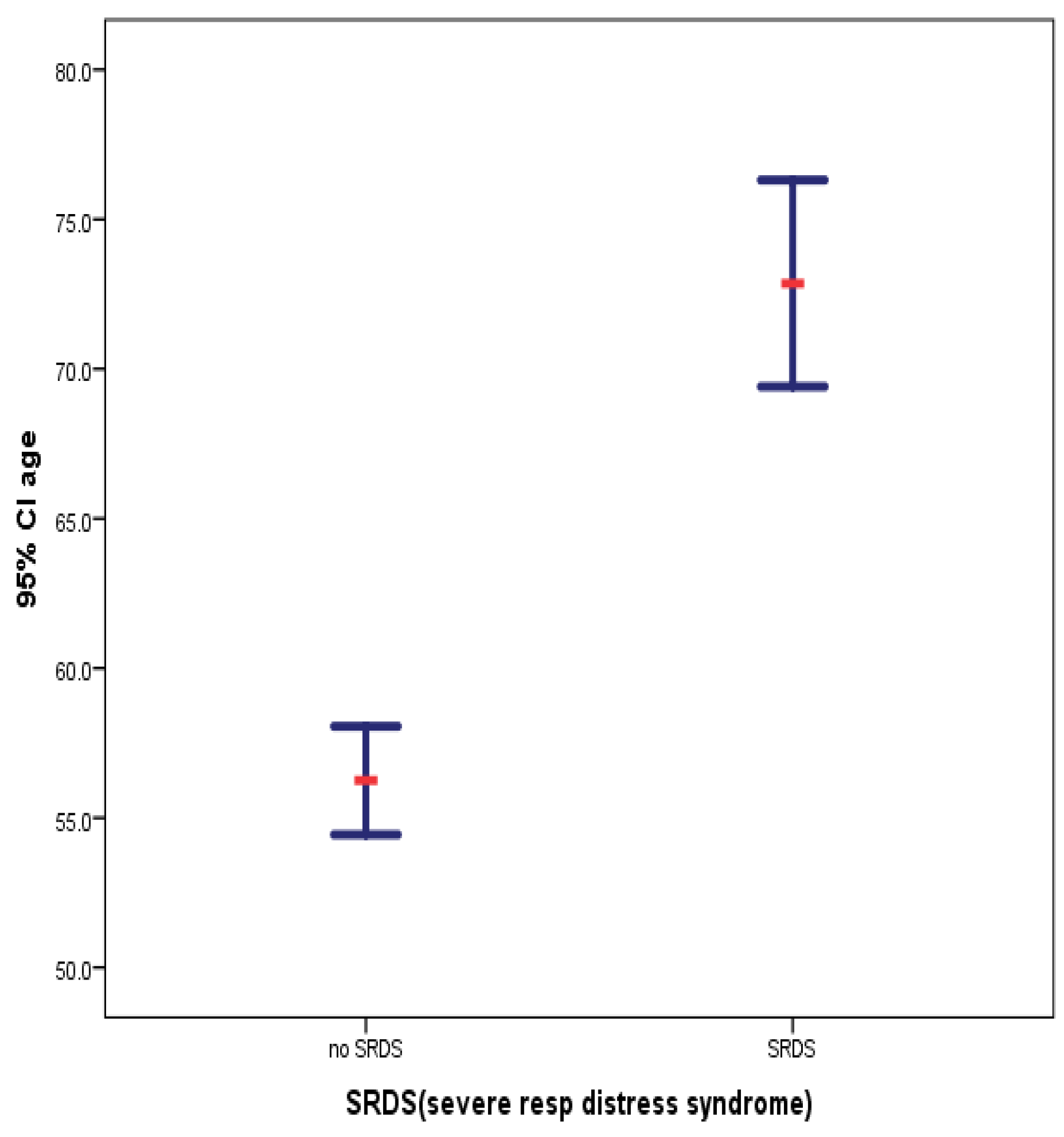
Figure 3.
Case fatality rates of COVID-19 patients with underlying Severe Distress Respiratory Syndrome with and without underlying bacterial co-infections.
Figure 3.
Case fatality rates of COVID-19 patients with underlying Severe Distress Respiratory Syndrome with and without underlying bacterial co-infections.
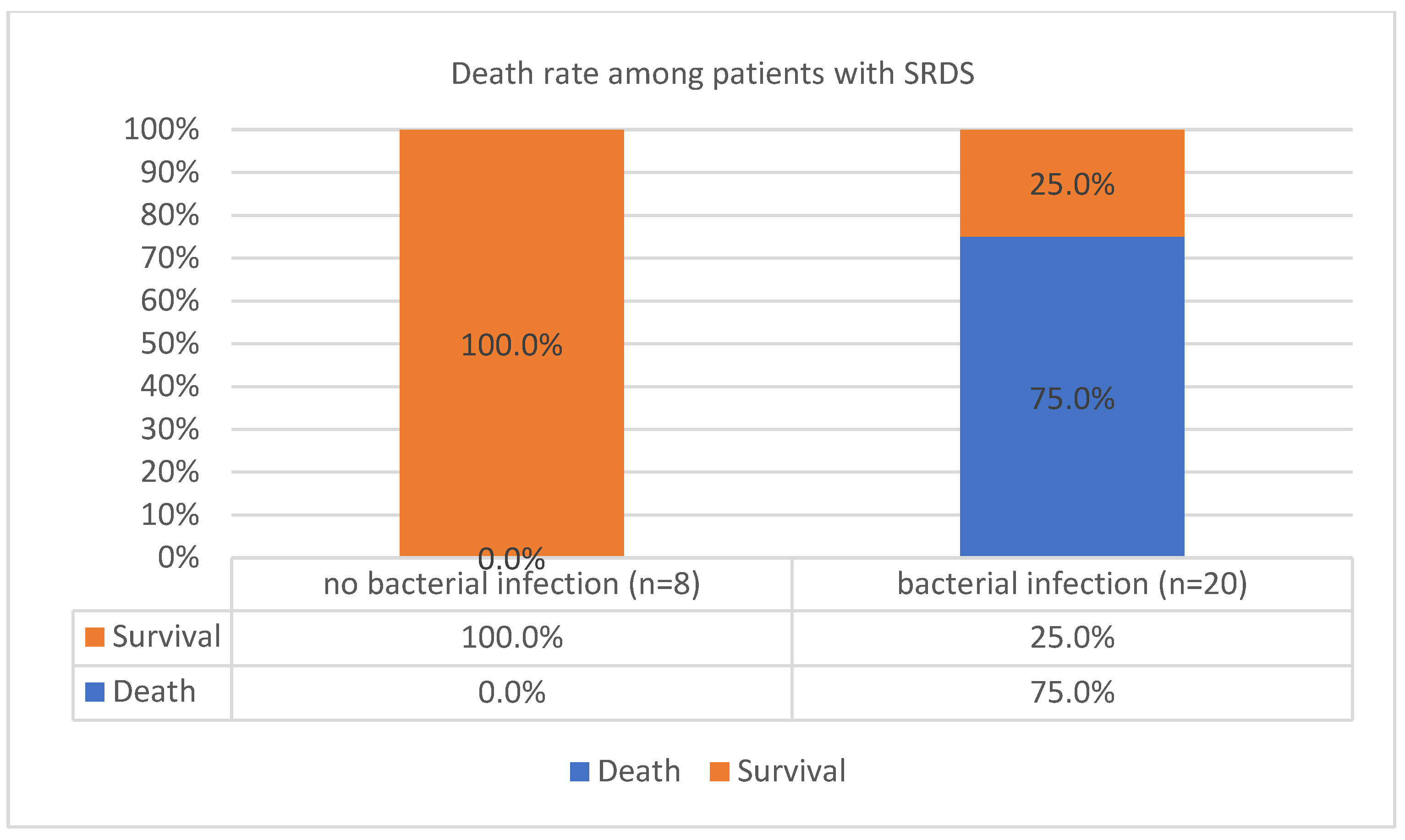
Figure 4.
Among patients without SRDS, bacterial infection is associated with a higher death rate (P value= 0.00000000076).
Figure 4.
Among patients without SRDS, bacterial infection is associated with a higher death rate (P value= 0.00000000076).
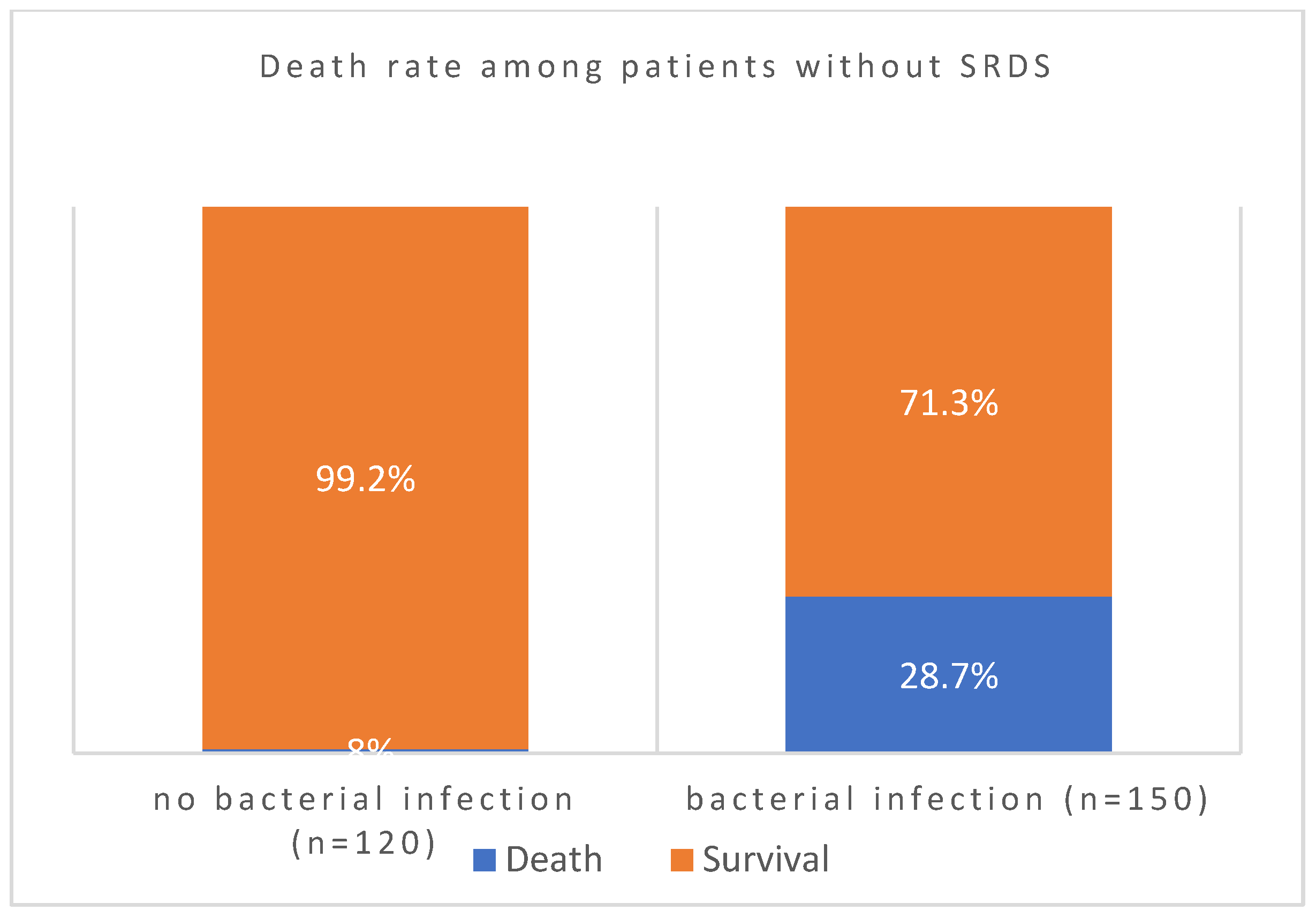

Table 1.
Age-specific difference in COVID-19 patients with and without severe resp distress syndrome.
Table 1.
Age-specific difference in COVID-19 patients with and without severe resp distress syndrome.
| SRDS(severe resp distress syndrome) | N | Mean | Std. Deviation | Std. Error Mean | |
|---|---|---|---|---|---|
| age | yes | 28 | 72.857 | 8.8974 | 1.6815 |
| no | 270 | 56.248 | 15.1019 | .9191 | |
Table 2.
(a,b,c,d,e). Comparative analysis of the diseases co-influence of SRDS, coinfections, and patient demographics before and after COVID-19 pandemic in the outcome.
Table 2.
(a,b,c,d,e). Comparative analysis of the diseases co-influence of SRDS, coinfections, and patient demographics before and after COVID-19 pandemic in the outcome.
| Group Statistics: Age profiles of patients before and after COVID-19 pandemic | |||||
|---|---|---|---|---|---|
| Group | N | Mean | Std. Deviation | Std. Error Mean | |
| age | During COVID-19 | 149 | 57.154 | 15.5058 | 1.2703 |
| Before COVID-19 | 149 | 58.463 | 15.3286 | 1.2558 | |
| a. Chi-Square Tests. Admitted patients’ gender profiles before and during the COVID-19 pandemic | |||||
| Value | df | Asymptotic Significance (2-sided) | Exact Sig. (2-sided) | Exact Sig. (1-sided) | |
| Pearson Chi-Square | .000a | 1 | 1.000 | ||
| Continuity Correctionb | 0.000 | 1 | 1.000 | ||
| Likelihood Ratio | 0.000 | 1 | 1.000 | ||
| Fisher’s Exact Test | 1.000 | .546 | |||
| N of Valid Cases | 298 | ||||
| a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 68.00. | |||||
| b. Chi-Square Tests: Analysis of the association of admitted patients’ gender and Severe Respiratory Distress Syndrome in the study population | |||||
| Value | df | Asymptotic Significance (2-sided) | Exact Sig. (2-sided) | Exact Sig. (1-sided) | |
| Pearson Chi-Square | .503a | 1 | .478 | ||
| Continuity Correctionb | .260 | 1 | .610 | ||
| Likelihood Ratio | .507 | 1 | .476 | ||
| Fisher’s Exact Test | .553 | .307 | |||
| N of Valid Cases | 298 | ||||
| a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 12.78. | |||||
| c. Chi-Square Tests: association of patients’ gender and COVID-19 fatality | |||||
| Value | df | Asymptotic Significance (2-sided) | Exact Sig. (2-sided) | Exact Sig. (1-sided) | |
| Pearson Chi-Square | .098a | 1 | .754 | ||
| Continuity Correctionb | .028 | 1 | .867 | ||
| Likelihood Ratio | .098 | 1 | .754 | ||
| Fisher’s Exact Test | .772 | .433 | |||
| N of Valid Cases | 298 | ||||
| a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 26.93. | |||||
| d. Chi-Square Tests: Whether Severe respiratory distress syndrome predisposes to coinfections | |||||
| Value | df | Asymptotic Significance (2-sided) | Exact Sig. (2-sided) | Exact Sig. (1-sided) | |
| Pearson Chi-Square | 2.609a | 1 | .106 | ||
| Continuity Correctionb | 2.001 | 1 | .157 | ||
| Likelihood Ratio | 2.714 | 1 | .099 | ||
| Fisher’s Exact Test | .114 | .077 | |||
| N of Valid Cases | 298 | ||||
| a. 0 cells (.0%) have expected count less than 5. The minimum expected count is 12.03. | |||||
Table 3.
Association of specific Gram-negative pathogens with case fatality during SRDS attack.
| Chi-Square Tests | ||||
|---|---|---|---|---|
| Value | df | Asymptotic Significance (2-sided) | Exact Sig. (2-sided) | |
| Pearson Chi-Square | 47.251a | 21 | .001 | .008 |
| Likelihood Ratio | 30.691 | 21 | .079 | .024 |
| Fisher’s Exact Test | 32.718 | .034 | ||
| N of Valid Cases | 149 | |||
| a. 38 cells (86.4%) have expected count less than 5. The minimum expected count is .11. | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



