
Submitted:
20 June 2023
Posted:
21 June 2023
You are already at the latest version
Abstract
Direct laryngoscope and videolaryngoscope are the dominant endotracheal intubation tools. Styletubation technique (using a video-assisted intubating stylet) has shown its advantages regarding in short intubation time, high success rate, less stimulation, and operator’s satisfaction. The learning curve can be steep but easy to overcome if the technical pitfalls could be avoided. Conditions make styletubation challenging include secretions/blood, short/stiff neck, restricted mouth opening and cervical spine mobility, anatomical abnormalities over head and neck regions, and obesity, etc. In this clinical report, we present the effectiveness and efficiency of routine use of the styletubation for tracheal intubation in a super-super obese patient (BMI 103 kg/m2) undergoing bariatric surgery with laparoscopic sleeve gastrectomy.
Keywords:
Styletubation
; video-assisted intubating stylet
; obesity
; super-super obesity
; bariatric surgery
; laparoscopic sleeve gastrectomy
; tracheal intubation
; laryngoscopy
; videolaryngoscope
; anesthesia
; difficult airway
Introduction
Obesity, an increasing world-wide medical problem, is measured through body mass index (BMI) > 30 kg/m2 and further categorized into grade 1 (BMI 30 to < 35 kg/m2), grade 2 (BMI 35 to < 40 kg/m2), and grade 3 (BMI ≥ 40 kg/m 2). The prevalence of super obesity (SO, BMI > 50.0 kg/m2) and super-super obesity (SSO, BMI > 60 kg/m2) is also increasing during recent years. Bariatric surgery is the most effective therapy and sometimes the last resort to loose weight. Expectedly, anesthesia and peri-operative management for bariatric and non-bariatric surgeries in all categories of the obese patient populations have become a focus issue for discussion [1,2,3,4]. Among all the relevant peri-operative management, airway management in such obese populations has been extensively discussed in literatures. Airway management, particularly intubation, remains the most challenging part for intraoperative care. [5,6,7,8,9,10,11,12,13].
The severity of obesity is related to the incident of difficult airway [14], despite some contraversies [15]. The disagreement may arise from the different criteria for defining difficult intubation. Examples of the criteria to predicting difficult intubation are body mass index (BMI), neck circumference, degree of neck mobility, width of mouth opening, or any other parameters, etc [16]. Different definition for difficult airway were used, such as difficult laryngoscopy (e.g., impossible to visualize any portion of the vocal cords after multiple attempts at laryngoscopy) or difficult tracheal intubation (e.g., requires multiple attempts to intubate) [17]. Others might use intubation difficult scale (IDS) or its modified version, combined with additional parameters, to predict/identify the event of difficult airway.
Since the videolaryngoscopes (VL) were invented over two decades ago, it has been repeatedly compared with conventional direct laryngoscopes (DL). VL has been shown certain advantages over the DL including better glottic visualization, less need for alignment of the airway axes, less force and cervical spine manipulation, shorter intubation time, and perhaps higher first-pass success rate of intubation [18,19]. A plethora of literature show the advantages (e.g., easier, faster, less complications) of VL in the obese populations [20,21,22,23,24,25,26,27,28,29,30]. However, such superiority of VL over DL, regarding all the outcome parameters (e.g., speed, safety, visualization, easiness), has not been consistently confirmed in the obese patient population [31,32,33,34].
Various alternative intubation tools have been reported other than DL and VL [35]. Those tracheal intubating modalities include rigid BullardTM laryngoscope, flexible fiberoptic bronchoscope (FOB), optical stylet [36,37,38,39], or combined FOB with VL [40]. The video-assisted intubating stylet technique has recently been coined into the “styletubation”, in contrast to the concept of the conventional laryngoscopy [41]. With extensive experiences of using styletubation recently in Taiwan, clinicians found this technique useful and easy to learn. In this case report, we present our experience of applying styletubation in a super-super obese patient undergoing laparoscopic sleeve gastrectomy.
Case presentation
A 33-year-old man (height: 158 cm, weight: 258 kg, and body mass index (BMI): 103 kg/m2) was referred to our Center for Obesity & Metabolic Health, Hualien Tzu-Chi Medical Center. After entering a four-month program (medical weight loss, education, and counseling), his body weight had been successfully reduced down to 217 kg (BMI, 86.9 kg/m2), including with medication of orlistat and liraglutide. Bioelectric impedance measurement showed body composition analysis: percentage body fat 54.1%, waist 200 cm, hip 202 cm. Laparoscopic sleeve gastrectomy was scheduled. Medical history included hypertension (blood pressure 205/100 mmHg, heart rate 75 beats/min) and cellulitis over lower extremities. Losartan and amlodipine were prescribed to control high blood pressure. Pre-operative physical check-ups included: transthoracic echocardiogram revealed trivial tricuspid regurgitation, normal left ventricular motion (ejection fraction, 69%), no abnormal regional wall motion, estimated pulmonary artery pressure = 24 mmHg; pulmonary function test revealed mild obstructive lung disease; abdominal echography revealed marked fatty liver; esophagogastroduodenoscopy revealed esophagitis and gastroesophageal reflux disease; polysomnography detected moderate obstructive sleep apnea (apnea/hyponea index: 22.5/hr). Blood panel showed HbA1c 5.9% and hemoglobin 11.5 g/dL.
Pre-operative airway evaluation showed the neck circumference of 54 cm; interincisor distance 4.5 cm; sternomental distance 17 cm; thyromental distance 8 cm; Mallampati class IV (Figure 1). Observed apnea and high blood pressure and a body mass index, age, neck circumference, and gender (STOP-BANG) created a score of 7. Body weight by definition are as follows: actual BW 217 kg, ideal BW 55 kg, adjusted BW 120 kg, lean body weight 111 kg. Before induction of anesthesia, the patient was placed in the operating table, in a reverse Trendelenburg with ramp position (Figure 2). His head and torso were elevated such that his external auditory meatus and the sternal notch were approximately horizontally aligned. He received pure oxygen at a rate of 30 L/min with a nasal high flow nasal cannula for 15 min. The patient was monitored as recommended by the American Society of Anesthesiologists (ASA) standards with pulse oximetry (SpO2), capnography (ETCO2), electrocardiogram (ECG), non-invasive (NIBP) and invasive arterial blood pressure (A-line), neuromuscular blockade monitor (train-of-four, TOF), bispectral index (BIS) and density spectral array (DSA) monitor, minimally-invasive FloTrac system, cerebral oximetry , and nociception monitor (Surgical Plethysmographic Index, SPI).
Pre-induction vital signs were blood pressure, 140/78 mmHg; heart rate, 53 per minute; respiratory rate, 16 per minute; SpO2, 100%. The induction of anesthesia was started with glycopyrrolate 0.2 mg, lidocaine 50 mg, and midazolam 5 mg, followed by propofol 180 mg and rocuronium 100 mg. An airway assistant performed jaw-thrust maneuver and opened the patient’s mouth. A nasal-pharyngeal airway with a suction tube was inserted into the patient’s oropharyngeal space to clear the secretions. It also served as a guide for subsequent intubation. Tracheal intubation was performed with the styletubation technique (video-assisted intubating stylet). A standard endotracheal tube with 7.5 mm of internal diameter was used for intubation (Figure 3). The whole process was smooth (first-pass success) and swift (12 s) (Figure 4). Airway was then confirmed by the capnography and chest auscultation. The ventilator strategy and parameters were set as follows: pressure control ventilation volume guaranteed (PCV-VG) with tidal volume: 650 ml, positive end-expiratory pressure (PEEP) 7 cm H2O, respiratory rate: 14-16 breaths/min, fresh gas flow rate: 2 L/min, fraction of inspired oxygen: 60%, maintenance partial pressure of end-tidal carbon dioxide: 33-45 mmHg, and peak pressure: 28-33 mmHg.
Anesthesia was maintained with propofol (under target-controlled infusion, TCI Marsh model, Ce 2.0 μg/ml) and desflurane 4-6% (MAC 0.6-0.8, BIS 40-50). Fentanyl and rocuronium were supplemented based on the SPI and TOF values. Anesthetic and surgical procedure lasted 5 h. SPI value from the intra-operative analgesic monitoring was monitored kept around 50. During emergence phase, desflurane was stopped while dexmedetomidine was maintained at 0.2 μg/kg/h. The patient regained spontaneous breath 2 min after the injection of sugammadex (400 mg). Then, dexmedetomidine infusion was stopped and he was extubated smoothly. The patient stayed in the intensive care unit overnight. Post-operative analgesia was achieved with parecoxib (40 mg, intravenous) and transversus abdominis plane block (TAP block, 40 ml of 0.5% ropivacaine). Prophylactic use of dexamethasone was given. In ICU, the patient reported no significant pain and did not request any rescue analgesia. Since the patient had OSAS, continuous positive airway pressure (CPAP) was applied overnight, even without revealing any dyspnea, respiratory depression, or hypoxia. No post-operative pulmonary complications, e.g., respiratory depression, pneumonia, hypoxia, upper airway obstruction, were reported.
Discussion
In this case report, we present styletubation technique for tracheal intubation in a super-super obesity patient (BMI 103 kg/m2) underwent laparoscopic sleeve gastrectomy. Instead of using the conventional DL or VL, we used styletubation technique for tracheal intubation (Figure 3). The procedure of using video-assisted intubating stylet was smooth and swift, with high first-pass success (Figure 4). No significant cardiopulmonary instability (e.g., arterial desaturation, hypertension, tachycardia or bradycardia) during intubation. No soft tissue or dental injuries occurred. Although the airway team members did feel heavier mental load and stress than usual airway exercise, the end of “safe-accurate-swift” for tracheal intubation was satisfactorily achieved in such super-super obesity patient.
In general, airway operators are used to adopting either the conventional DL (with the Macintosh blade) or the VL in the obese adult patients. Although, intuitively, one would think the VL be superior over the DL in such scenario. The advantages of VL, which have been demonstrated in those proponents, include better glottic visualization, shorter intubating time, less intubation attempts, or higher intubation success rates [20,21,22,23,24,25,26,27,28,29,30]. Therefore, they proposed VL be used as the overall first-line tracheal intubation modality versus Macintosh DL in the obese patients (and perhaps for overall patient populations to be intubated). In contrast, opposite results regarding such role appeared in sporadic reports, which show either VL is slower [31,32], or both modalities allow equally quick and safe airway management [33,34].
The overall evidence to support the routine use of VL, particularly in obese patients, is sparse. No definitive study has demonstrated a clear-cut superiority for its routine use in such scenario. Much of the previous clinical comparative studies showed inconsistent results on various outcomes such as overall success rates, time to successful tracheal intubation, and number of attempts. high-risk obese patients, in comparison to normal subjects, tolerated hypoxia much less and higher risk of aspiration during tracheal intubation. Therefore both first-attempt success rate and intubation time become the most important and meaningful key performance indices among all comparators. Understandably, any intubating tools share a better glottis visualization would be advantageous for quicker successful tracheal intubation. Same true is for such application in the obese populations.

Table 1.
Comparison of laryngoscopy and styletubation on tracheal intubation in morbidly obese patients and this patient.
Table 1.
Comparison of laryngoscopy and styletubation on tracheal intubation in morbidly obese patients and this patient.
| Laryngoscopy (DL/VL) | Styletubation (VS) | |
|---|---|---|
| BMI (kg/m2) |
|
103―86.9 |
| Neck circumference (cm) | 54 | |
| Mallampati class (III/IV) |
|
IV |
| Sterno-mental distance (cm) | 17 | |
| Mouth opening width (interincisor gap) (cm) | 4.5 | |
| Upper lip bite test (II/III) |
|
II |
| Pathologically enlarged, swelled, crowding oral cavity, pharynx, or larynx | NA |
|
| OSAS | + | |
| Intubation time: (DA: > 10 min) |
12 s | |
| Operator’s subjective feeling |
|
Easy, smooth, swift |
| First-pass success rate | First-pass success | |
| Number of attempts (DA: > 2 attempts) |
1 attempt | |
| Cormack-Lehane view (III/IV) | NA (POGO 100%) | |
| De-saturation | 0 | |
| Airway injuries | 0 | |
| POST | 0 | |
| IDS score | NA | |
| DA incidence in MO | 0 |
DL: direct laryngoscopy; VL: videolaryngoscopy; VS: video-assisted intubating stylet technique; BMI: body mass index; OSAS: obstructive sleep apnea syndrome; DA: difficult airway; POST: post-operative sore throat; IDS: intubation difficulty scale; MO: morbid obesity.
It is worthy to mention that when airway operators using the conventional laryngoscopy (both DL and VL) might still encounter certain difficulties during the tracheal intubation. Such technical difficulties and pitfalls include difficult placement of the laryngoscope blade into oral cavity, injuries to the teeth or soft tissue, unable to acquire a fair three axis alignment, obstructed visualization of the glottis, and finally difficult/failed advancement of the endotracheal tube into trachea (i.e., you see that you fail) [48,49,50,51]. In contrast, as shown in this case report, styletubation with a video-assisted intubating stylet provides timely success and fulfills the ultimate goal of tracheal intubation in a super-super obese patient (i.e., swift, accurate, and safe) (Figure 3 and Figure 4). In our medical center, we have routinely and universally performed the styletubation for tracheal intubation as a daily practice since 2016 [41,52]. It is worthy to mention that such application of styletubation has also been demonstrated in various potentially difficult airway scenarios, such as limited cervical mobility, various ENT procedures, COVID-positive patients, etc [53,54,55,56,57,58].
Conclusion
Many critical issues regarding the peri-anesthesia management for super-super obese patients undergoing bariatric and non-bariatric surgeries are needed to consider and deserved challenges. For example, pre-operative optimal positioning of such patient, adequate pre-oxygenation and apneic oxygenation tactic, body weight-adjusted medication regimens, peri-operative monitoring, ventilator strategies, and post-operative care, etc. In this case report, we demonstrate the styletubation technique is applicable for tracheal intubation in a super-super obese patient undergoing bariatric surgery.
Supplementary Materials
The following supporting information can be downloaded at Preprints.org.
Author Contributions
Conceptualization, B.-G.W., H.-N.L., J.Z.Q., and A.S.; methodology, B.-G.W., H.-N.L.; validation B.-G.W., H.-N.L.; formal analysis, B.-G.W., H.-N.L.; investigation, B.-G.W., H.-N.L.; resources, H.-N.L.; data curation, B.-G.W., H.-N.L.; writing—original draft preparation, B.-G.W., H.-N.L.; writing—review and editing, J.Z.Q. and A.S.; visualization, H.-N.L.; supervision, H.-N.L.; project administration, H.-N.L.; funding acquisition, H.-N.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and was approved by REC, Hualien Tzuchi Hospital (approved letter number: CR112-0).
Informed Consent Statement
Written informed consent was obtained from all patients or their legally authorized representatives.
Data Availability Statement
Not applicable.
Acknowledgments
This work was supported by Hualien Tzuchi Hospital.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Leykin, Y.; Pellis, T.; Del Mestro, E.; Marzano, B.; Fanti, G.; Brodsky, J.B. Anesthetic management of morbidly obese and super-morbidly obese patients undergoing bariatric operations: hospital course and outcomes. Obes. Surg. 2006, 16, 1563–1569. [Google Scholar] [CrossRef]
- Gray, K.D.; Pomp, A.; Dakin, G.; Amanat, S.; Turnbull, Z.A.; Samuels, J.; Afaneh, C. Perioperative outcomes and anesthetic considerations of robotic bariatric surgery in a propensity-matched cohort of super obese and super-super obese patients. Surg. Endosc. 2018, 32, 4867–4873. [Google Scholar] [CrossRef]
- Wilkinson, K.H.; Helm, M.; Lak, K.; Higgins, R.M.; Gould, J.C.; Kindel, T.L. The risk of post-operative complications in super-super obesity compared to super obesity in accredited bariatric surgery centers. Obes. Surg. 2019, 29, 2964–2971. [Google Scholar] [CrossRef]
- Kaye, A.D.; Lingle, B.D.; Brothers, J.C.; Rodriguez, J.R.; Morris, A.G.; Greeson, E.M.; Cornett, E.M. The patient with obesity and super-super obesity: Perioperative anesthetic considerations. Saudi. J. Anaesth. 2022, 16, 332–338. [Google Scholar] [CrossRef]
- Brodsky, J.B.; Lemmens, H.J.; Brock-Utne, J.G.; Vierra, M.; Saidman, L.J. Morbid obesity and tracheal intubation. Anesth. Analg. 2002, 94, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Van Zundert, A.A.; Lee, R.A. Intubation difficulties in obese patients. Anesth. Analg. 2009, 108, 1051. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, M.S. Airway management and morbid obesity. Eur. J. Anaesthesiol. 2010, 27, 923–927. [Google Scholar] [CrossRef]
- De Jong, A.; Molinari, N.; Pouzeratte, Y.; Verzilli, D.; Chanques, G.; Jung, B.; Futier, E.; Perrigault, P.F.; Colson, P.; Capdevila, X.; Jaber, S. Difficult intubation in obese patients: incidence, risk factors, and complications in the operating theatre and in intensive care units. Br. J. Anaesth. 2015, 114, 297–306. [Google Scholar] [CrossRef]
- Petrini, F.; Di Giacinto, I.; Cataldo, R.; Esposito, C.; Pavoni, V.; Donato, P.; Trolio, A.; Merli, G.; Sorbello, M.; Pelosi, P. Obesity Task Force for the SIAARTI Airway Management Study Group. Perioperative and periprocedural airway management and respiratory safety for the obese patient: 2016 SIAARTI Consensus. Minerva Anestesiol. 2016, 82, 1314–1335. [Google Scholar] [PubMed]
- Wojcikiewicz, T.; Cousins, J.; Margarson, M. The bariatric airway. Br. J. Hosp. Med. (Lond). 2018, 79, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Moon, T.S.; Fox, P.E.; Somasundaram, A.; Minhajuddin, A.; Gonzales, M.X.; Pak, T.J.; Ogunnaike, B. The influence of morbid obesity on difficult intubation and difficult mask ventilation. J. Anesth. 2019, 33, 96–102. [Google Scholar] [CrossRef]
- Liew, W.J.; Negar, A.; Singh, P.A. Airway management in patients suffering from morbid obesity. Saudi. J. Anaesth. 2022, 16, 314–321. [Google Scholar] [CrossRef]
- Thota, B.; Jan, K.M.; Oh, M.W.; Moon, T.S. Airway management in patients with obesity. Saudi. J. Anaesth. 2022, 16, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Juvin, P.; Lavaut, E.; Dupont, H.; Lefevre, P.; Demetriou, M.; Dumoulin, J.L.; Desmonts, J.M. Difficult tracheal intubation is more common in obese than in lean patients. Anesth. Analg. 2003, 97, 595–600. [Google Scholar] [CrossRef]
- Saasouh, W.; Laffey, K.; Turan, A.; Avitsian, R.; Zura, A.; You, J.; Zimmerman, N.M.; Szarpak, L.; Sessler, D.I.; Ruetzler, K. Degree of obesity is not associated with more than one intubation attempt: a large centre experience. Br. J. Anaesth. 2018, 120, 1110–1116. [Google Scholar] [CrossRef]
- Lundstrøm, L.H.; Møller, A.M.; Rosenstock, C.; Astrup, G.; Wetterslev, J. High body mass index is a weak predictor for difficult and failed tracheal intubation: a cohort study of 91,332 consecutive patients scheduled for direct laryngoscopy registered in the Danish Anesthesia Database. Anesthesiology. 2009, 110, 266–274. [Google Scholar] [CrossRef]
- Apfelbaum, J.L.; Hagberg, C.A.; Connis, R.T.; Abdelmalak, B.B.; Agarkar, M.; Dutton, R.P.; Fiadjoe, J.E.; Greif, R.; Klock, P.A.; Mercier, D.; Myatra, S.N.; O'Sullivan, E.P.; Rosenblatt, W.H.; Sorbello, M.; Tung, A. 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 2022, 136, 31–81. [Google Scholar] [CrossRef]
- Pieters, B.M.A.; Maas, E.H.A.; Knape, J.T.A.; van Zundert, A.A.J. Videolaryngoscopy vs. direct laryngoscopy use by experienced anaesthetists in patients with known difficult airways: a systematic review and meta-analysis. Anaesthesia 2017, 72, 1532–1541. [Google Scholar] [CrossRef]
- Hansel, J.; Rogers, A.M.; Lewis, S.R.; Cook, T.M.; Smith, A.F. Videolaryngoscopy versus direct laryngoscopy for adults undergoing tracheal intubation. Cochrane Database Syst. Rev. 2022, 4, CD011136. [Google Scholar] [CrossRef]
- Marrel, J.; Blanc, C.; Frascarolo, P.; Magnusson, L. Videolaryngoscopy improves intubation condition in morbidly obese patients. Eur. J. Anaesthesiol. 2007, 24, 1045–1049. [Google Scholar] [CrossRef] [PubMed]
- Ndoko, S.K.; Amathieu, R.; Tual, L.; Polliand, C.; Kamoun, W.; El Housseini, L.; Champault, G.; Dhonneur, G. Tracheal intubation of morbidly obese patients: a randomized trial comparing performance of Macintosh and Airtraq laryngoscopes. Br. J. Anaesth. 2008, 100, 263–268. [Google Scholar] [CrossRef]
- Maassen, R.; Lee, R.; van Zundert, A.; Cooper, R. The videolaryngoscope is less traumatic than the classic laryngoscope for a difficult airway in an obese patient. J. Anesth. 2009, 23, 445–448. [Google Scholar] [CrossRef]
- Dhonneur, G,; Abdi, W.; Ndoko, S.K.; Amathieu, R.; Risk, N.; El Housseini, L.; Polliand, C.; Champault, G.; Combes, X.; Tual, L. Video-assisted versus conventional tracheal intubation in morbidly obese patients. Obes. Surg. 2009, 19, 1096–1101. [CrossRef]
- Gaszyński, T. Clinical experience with the C-Mac videolaryngoscope in morbidly obese patients. Anaesthesiol. Intensive Ther. 2014, 46, 14–16. [Google Scholar] [CrossRef] [PubMed]
- Ranieri, D. Jr.; Zinelli, F.R.; Neubauer, A.G.; Schneider, A.P.; do Nascimento, P. Jr. Preanesthetic assessment data do not influence the time for tracheal intubation with Airtraq™ video laryngoscope in obese patients. Braz. J. Anesthesiol. 2014, 64, 190–194. [Google Scholar] [CrossRef]
- Gaszyński, T. Comparison of the glottic view during video-intubation in super obese patients: a series of cases. Ther. Clin. Risk Manag. 2016, 12, 1677–1682. [Google Scholar] [CrossRef] [PubMed]
- Yumul, R.; Elvir-Lazo, O.L.; White, P.F.; Sloninsky, A.; Kaplan, M.; Kariger, R.; Naruse, R.; Parker, N.; Pham, C.; Zhang, X.; Wender, R.H. Comparison of three video laryngoscopy devices to direct laryngoscopy for intubating obese patients: a randomized controlled trial. J. Clin. Anesth. 2016, 31, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Hoshijima, H.; Denawa, Y.; Tominaga, A.; Nakamura, C.; Shiga, T.; Nagasaka, H. Videolaryngoscope versus Macintosh laryngoscope for tracheal intubation in adults with obesity: A systematic review and meta-analysis. J. Clin. Anesth. 2018, 44, 69–75. [Google Scholar] [CrossRef]
- Arslan, Z.İ.; Yörükoğlu, H.U. Tracheal intubation with the McGrath MAC X-blade videolaryngoscope in morbidly obese and nonobese patients. Turk. J. Med. Sci. 2019, 49, 1540–1546. [Google Scholar] [CrossRef]
- Brozek, T.; Bruthans, J.; Porizka, M.; Blaha, J.; Ulrichova, J.; Michalek, P. A Randomized comparison of non-channeled GlidescopeTM Titanium versus channeled KingVisionTM videolaryngoscope for orotracheal intubation in obese patients with BMI > 35 kg·m-2. Diagnostics (Basel). 2020, 10, 1024. [Google Scholar] [CrossRef]
- Andersen, L.H.; Rovsing, L.; Olsen, K.S. GlideScope videolaryngoscope vs. Macintosh direct laryngoscope for intubation of morbidly obese patients: a randomized trial. Acta Anaesthesiol. Scand. 2011, 55, 1090–1097. [Google Scholar] [CrossRef]
- Abdallah, R.; Galway, U.; You, J.; Kurz, A.; Sessler, D.I.; Doyle, D.J. A randomized comparison between the Pentax AWS video laryngoscope and the Macintosh laryngoscope in morbidly obese patients. Anesth. Analg. 2011, 113, 1082–1087. [Google Scholar] [CrossRef] [PubMed]
- Ander, F.; Magnuson, A.; Berggren, L.; Ahlstrand, R.; de Leon, A. Time-to-intubation in obese patients. A randomized study comparing direct laryngoscopy and videolaryngoscopy in experienced anesthetists. Minerva Anestesiol. 2017, 83, 906–913. [Google Scholar] [CrossRef]
- Castillo-Monzón, C.G.; Marroquín-Valz, H.A.; Fernández-Villacañas-Marín, M.; Moreno-Cascales, M.; García-Rojo, B.; Candia-Arana, C.A. Comparison of the macintosh and airtraq laryngoscopes in morbidly obese patients: a randomized and prospective study. J. Clin. Anesth. 2017, 36, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, A.; Smith, A.F.; Lewis, S.R.; Cook, T.M. Tracheal intubation with a flexible intubation scope versus other intubation techniques for obese patients requiring general anaesthesia. Cochrane Database Syst. Rev. 2014, 17, CD010320. [Google Scholar] [CrossRef] [PubMed]
- Aikins, N.L.; Ganesh, R.; Springmann, K.E.; Lunn, J.J.; Solis-Keus, J. Difficult airway management and the novice physician. J. Emerg. Trauma Shock. 2010, 3, 3,9–12. [Google Scholar] [CrossRef]
- Abdelmalak, B.B.; Bernstein, E.; Egan, C.; Abdallah, R.; You, J.; Sessler, D.I.; Doyle, D.J. GlideScope® vs flexible fibreoptic scope for elective intubation in obese patients. Anaesthesia. 2011, 66, 550–555. [Google Scholar] [CrossRef]
- Abdellatif, A.A.; Ali, M.A. GlideScope videolaryngoscope versus flexible fiberoptic bronchoscope for awake intubation of morbidly obese patient with predicted difficult intubation. Middle East J. Anaesthesiol. 2014, 22, 385–392. [Google Scholar]
- Gaszynski, T.; Pietrzyk, M.; Szewczyk, T.; Gaszynska, E. A comparison of performance of endotracheal intubation using the Levitan FPS optical stylet or Lary-Flex videolaryngoscope in morbidly obese patients. Scientific World Journal. 2014, 2014, 207591. [Google Scholar] [CrossRef]
- Chung, M.Y.; Park, B.; Seo, J.; Kim, C.J. Successful airway management with combined use of McGrath® MAC video laryngoscope and fiberoptic bronchoscope in a severe obese patient with huge goiter-a case report. Korean J. Anesthesiol. 2018, 71, 232–236. [Google Scholar] [CrossRef]
- Luk, H.N.; Qu, J.Z.; Shikani, A. Styletubation: The paradigmatic role of video-assisted intubating stylet technique for routine tracheal intubation. Asian J. Anesthesiol. 2023. Apr 20. [Google Scholar] [CrossRef]
- Gaszynski, T. Standard clinical tests for predicting difficult intubation are not useful among morbidly obese patients. Anesth. Analg. 2004, 99, 956. [Google Scholar] [CrossRef] [PubMed]
- Dixit, A.; Kulshrestha, M.; Mathews, J.J.; Bhandari, M. Are the obese difficult to intubate? Br. J. Anaesth. 2014, 112, 770–771. [Google Scholar] [CrossRef] [PubMed]
- Riad, W.; Vaez, M.N.; Raveendran, R.; Tam, A.D.; Quereshy, F.A.; Chung, F.; Wong, D.T. Neck circumference as a predictor of difficult intubation and difficult mask ventilation in morbidly obese patients: A prospective observational study. Eur. J. Anaesthesiol. 2016, 33, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Siriussawakul, A.; Limpawattana, P. A validation study of the intubation difficulty scale for obese patients. J. Clin. Anesth. 2016, 33, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Siriussawakul, A.; Maboonyanon, P.; Kueprakone, S.; Samankatiwat, S.; Komoltri, C.; Thanakiattiwibun, C. Predictive performance of a multivariable difficult intubation model for obese patients. PLoS One 2018, 13, e0203142. [Google Scholar] [CrossRef]
- Lavi, R.; Segal, D.; Ziser, A. Predicting difficult airways using the intubation difficulty scale: a study comparing obese and non-obese patients. J. Clin. Anesth. 2009, 21, 264–267. [Google Scholar] [CrossRef]
- Pieters, B.; Maassen, R.; Van Eig, E.; Maathuis, B.; Van Den Dobbelsteen, J.; Van Zundert, A. Indirect videolaryngoscopy using Macintosh blades in patients with non-anticipated difficult airways results in significantly lower forces exerted on teeth relative to classic direct laryngoscopy: a randomized crossover trial. Minerva Anestesiol. 2015, 81, 846–854. [Google Scholar]
- Kleine-Brueggeney, M.; Greif, R.; Schoettker, P.; Savoldelli, G.L.; Nabecker, S.; Theiler, L.G. Evaluation of six videolaryngoscopes in 720 patients with a simulated difficult airway: a multicentre randomized controlled trial. Br. J. Anaesth. 2016, 116, 670–679. [Google Scholar] [CrossRef]
- Aziz, M.F.; Bayman, E.O.; Van Tienderen, M.M.; Todd, M.M.; StAGE Investigator Group; Brambrink AM. Predictors of difficult videolaryngoscopy with GlideScope® or C-MAC® with D-blade: secondary analysis from a large comparative videolaryngoscopy trial. Br. J. Anaesth. 2016, 117, 118–123. [Google Scholar] [CrossRef]
- Schieren, M.; Kleinschmidt, J.; Schmutz, A.; Loop, T.; Staat, M.; Gatzweiler, K.H.; Wappler, F.; Defosse, J. Comparison of forces acting on maxillary incisors during tracheal intubation with different laryngoscopy techniques: a blinded manikin study. Anaesthesia. 2019, 74, 1563–1571. [Google Scholar] [CrossRef] [PubMed]
- Luk, H.N.; Luk, H.N.; Qu, J.Z.; Shikani, A. A paradigm shift of airway management: The role of video-assisted intubating stylet technique. In: Jessica Lovich-Sapola (Ed.), Advances in Tracheal Intubation [Working Title]. IntechOpen [Internet] London, United Kingdom. 2022. [Google Scholar] [CrossRef]
- Tsai, P.B.; Luk, H.N. Plastic sheet and video intubating stylet: A technical note. Asian J. Anesthesiol. 2021, 59, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Tsay, P.J.; Yang, C.P.; Luk, H.N.; Qu, J.Z.; Shikani, A. Video-assisted intubating stylet technique for difficult intubation: A Case Series Report. Healthcare (Basel). 2022, 10, 741. [Google Scholar] [CrossRef] [PubMed]
- Shih, T.L.; Koay, K.P.; Hu, C.Y.; Luk, H.N.; Qu, J.Z.; Shikani, A. The use of the Shikani video-assisted intubating stylet technique in patients with restricted neck mobility. Healthcare (Basel). 2022, 10, 1688. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.P.; Luk, H.N.; Qu, J.Z.; Shikani, A. The use of a video-assisted intubating stylet technique in a critically ill and contagious COVID-19 patient. Healthcare (Basel). 2022, 10, 388. [Google Scholar] [CrossRef]
- Huang, C.H.; Su, I.M.; Jhuang, B.J.; Luk, H.N.; Qu, J.Z.; Shikani, A. Video-assisted stylet intubation with a plastic sheet barrier, a safe and simple technique for tracheal intubation of COVID-19 patients. Healthcare (Basel). 2022, 10, 1105. [Google Scholar] [CrossRef]
- Jhuang, B.J.; Luk, H.N.; Qu, J.Z.; Shikani, A. Video-twin technique for airway management, combining video-intubating stylet with videolaryngoscope: A case series report and review of the literature. Healthcare (Basel). 2022, 10, 2175. [Google Scholar] [CrossRef]
Figure 1.
Pre-operative airway evaluation. A: 158 cm, weight: 258 kg, and body mass index (BMI): 103 kg/m2). B: Neck circumference 54 cm. C: The modified Mallampati classification class IV. D―G: Serial images from video naso-pharyngo-laryngoscopic examination. An omega-shaped epiglottis is noted.
Figure 1.
Pre-operative airway evaluation. A: 158 cm, weight: 258 kg, and body mass index (BMI): 103 kg/m2). B: Neck circumference 54 cm. C: The modified Mallampati classification class IV. D―G: Serial images from video naso-pharyngo-laryngoscopic examination. An omega-shaped epiglottis is noted.
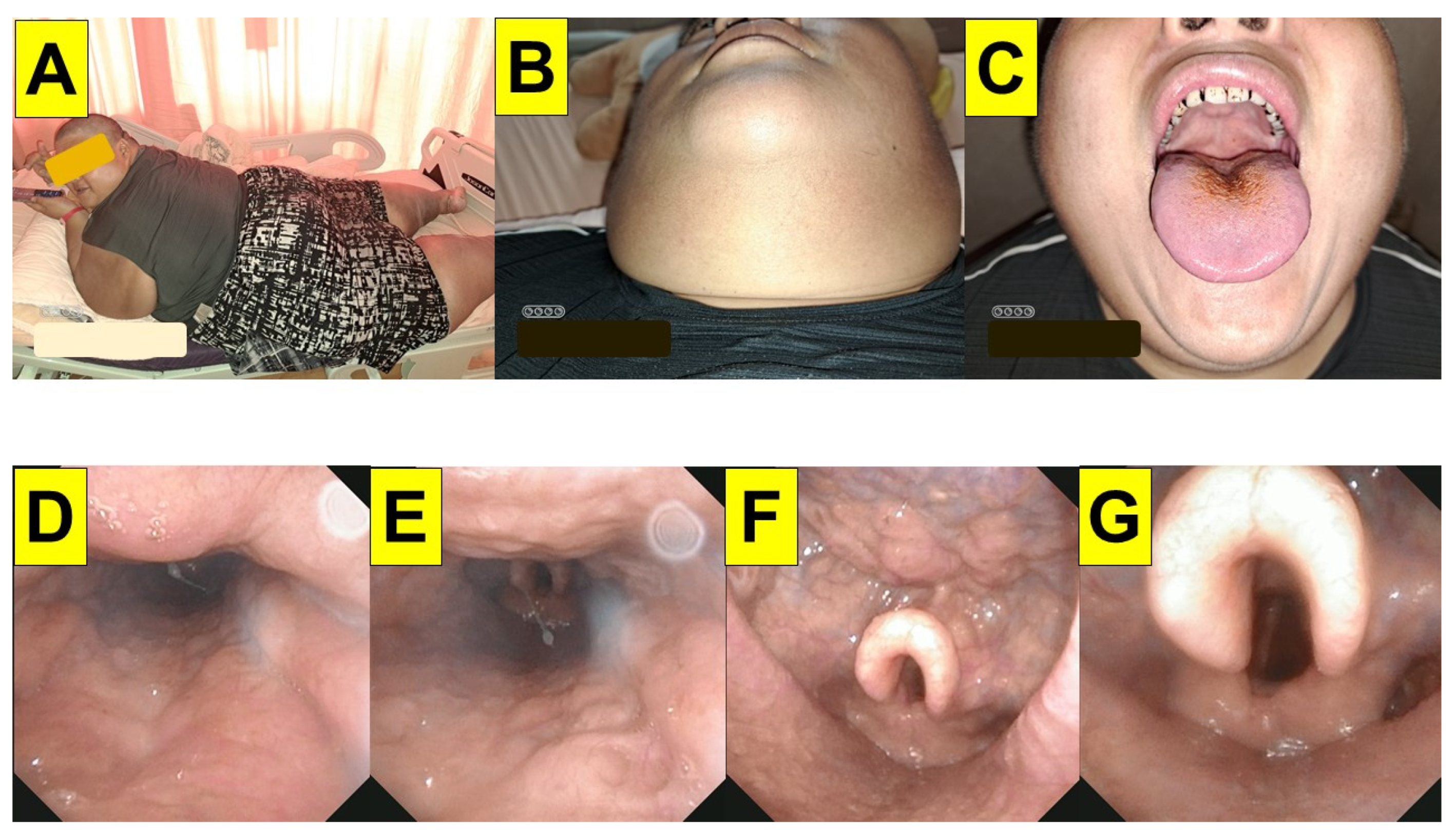
Figure 2.
Preoperative drill and planning in the operating room. A: Standing posture. B: Remained supine position on the operating table. C: The enlarged neck size with thick fat pads. D―F: Adjusting the height of the pillows and rolls under the patient to line up the ear-sternum in a ramp position. Neutral position with mouth closure (D) and opening (E). Sniff position with mouth opening (F).
Figure 2.
Preoperative drill and planning in the operating room. A: Standing posture. B: Remained supine position on the operating table. C: The enlarged neck size with thick fat pads. D―F: Adjusting the height of the pillows and rolls under the patient to line up the ear-sternum in a ramp position. Neutral position with mouth closure (D) and opening (E). Sniff position with mouth opening (F).

Figure 3.
Tracheal intubation conducted by the styletubation technique. A: Before conducting the intubation procedure, the airway assistant helped opening the patient’s mouth. A nasopharyngeal airway-flexible suction tube was applied to clear the airway. B: The airway assistant conducted jaw-thrust maneuver to lift up the patient’s mandible while keeping the airway open. C: The airway operator inserted the video intubating stylet under the guidance shown in a video monitor. D: Glottic visualization before advancing off the endotracheal tube into the patient’s trachea. .
Figure 3.
Tracheal intubation conducted by the styletubation technique. A: Before conducting the intubation procedure, the airway assistant helped opening the patient’s mouth. A nasopharyngeal airway-flexible suction tube was applied to clear the airway. B: The airway assistant conducted jaw-thrust maneuver to lift up the patient’s mandible while keeping the airway open. C: The airway operator inserted the video intubating stylet under the guidance shown in a video monitor. D: Glottic visualization before advancing off the endotracheal tube into the patient’s trachea. .
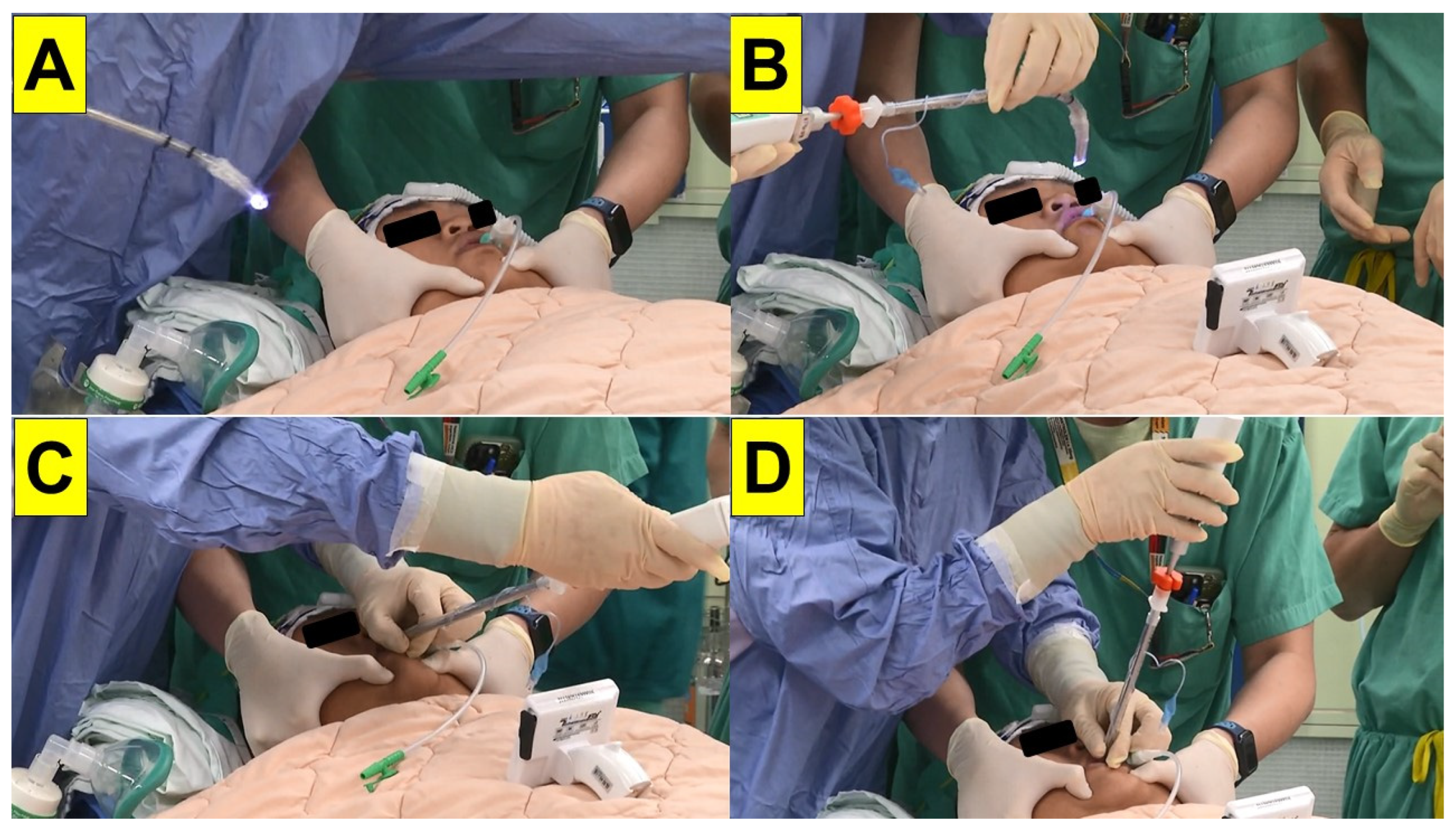
Figure 4.
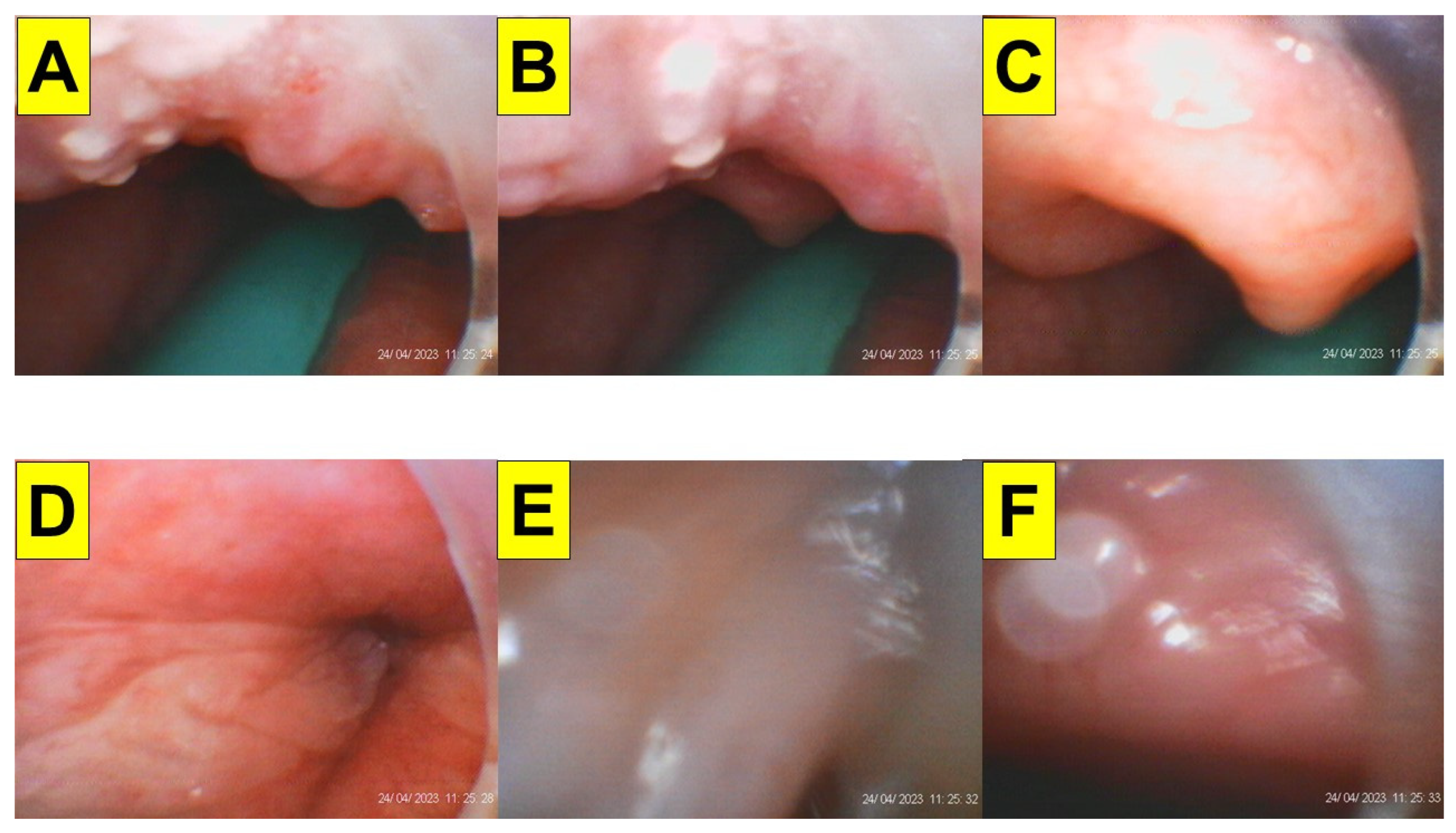
Serial images recorded during styletubation. A: A narrow oro-pharyngeal space. The green naso-pharyngeal airway can be observed. B: The omega-shape epiglottis came to sight. C: A close-up view of the omega-shaped epiglottis. D―E: Visualization of the glottis and vocal cords. F: View of the tracheal wall before advancement of the endotracheal tube into the trachea. The whole intubation process (from mouth to trachea) was 12 s and succeeded in the first attempt. Supplementary materials.
Figure 4.
Serial images recorded during styletubation. A: A narrow oro-pharyngeal space. The green naso-pharyngeal airway can be observed. B: The omega-shape epiglottis came to sight. C: A close-up view of the omega-shaped epiglottis. D―E: Visualization of the glottis and vocal cords. F: View of the tracheal wall before advancement of the endotracheal tube into the trachea. The whole intubation process (from mouth to trachea) was 12 s and succeeded in the first attempt. Supplementary materials.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



