
Submitted:
21 June 2023
Posted:
21 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The COVID-19 pandemic has expanded globally and caused serious consequence in both health system and the economy. MPV is one of two oral antivirals for COVID-19 with mild-to-moderate symptoms that have received FDA approval so far. This study aims to evaluate the cost-utility of using MPV in COVID-19 treatment. To compare the utility costs of MPV and non-MPV treatments for COVID-19 patients, we used a decision tree model. Data on clinical efficacy, cost, and quality of life were gathered from previous studies. The incremental effective cost ratio (ICER) calculated based on costs incurred and quality-adjusted life years (QALY), was considered as primary out-come. The total cost of MPV treatment and not using MPV was 15,362,516 VND (618 USD) and 15,771,262 VND (634 USD), respectively. The estimated QALY with using-MPV was 28.33, while without MPV was 19.72. The ICER was dominant, resulting in savings of 47,453 VND/QALY (1.9 USD). MPV is a cost-effective medication used to treat COVID-19. In mild-to-moderate COVID-19 patients, MPV considerably lowers costs and improves quality of life. However, several clinical factors of the drug still need to be taken into account.
Keywords:
Cost-utility
; Covid-19
; Molnupiravir
; Vietnam
; Utility
1. Introduction
A global pandemic caused by the coronavirus that first emerged in China 2019 has had a significant impact on both the health system and the entire world economy [1]. With the outbreak of the new Corona virus (COVID-19) originating from Wuhan City, Hubei Province of China, the rapid spread of the disease in the community, regionally and internationally has occurred with the exponential increase in the number of cases and deaths. On January 30th, 2020, the Director-General (DG) of World Health Organization (WHO) declared the COVID-19 outbreak a public health emergency of international concern (PHEIC) under the International Health Regulations (IHR) (2005) [2].
Globally, there are now nearly 2.3 million new cases and nearly 15,000 deaths from Covid-19 recorded in the past 28 days (April 24th - May 21st, 2023). There were 21% and 17% reductions respectively in the number of cases and deaths recorded 28 days earlier (March 27th - April 23rd, 2023). The epidemic situation at the world level is different, with an increase in reported cases in the Africa and Western Pacific Region and an increase in deaths in Africa, the Americas, Southeast Asia, and the Western Pacific Region. As of May 21st, 2023, more than 766 million confirmed cases and more than 6.9 million deaths have been reported globally [3,4].
In Southeast Asia, more than 146,000 new cases and 1143 new deaths were reported, a 31% decrease in incidence and a 61% decrease in death compared to the previous 28 days. Six of the 10 countries for which data are available reported an increase in new cases of 20% or more, with the highest rate of increase recorded in Myanmar (3685 vs 276 new cases; +1235%), Thailand Lan (8498 vs 1858 new cases; +357%), and Timor-Leste (16 vs four new cases; +300%). The highest number of new cases and deaths were reported from Indonesia (38 150 new cases; 13.9 new cases per 100 000; +92% - 497 new deaths; <1 new deaths per 100 000; +172%) and Thailand (8498 new cases; 12.2 new cases per 100 000; +357% - 106 new deaths; <1 new deaths per 100 000; +783%) [3,4].
In Vietnam, the cumulative incidence from April 2021 to May 31th, 2023 recorded 11,612,608 cases, including 43,206 deaths (PFC 0.4%) in 63 provinces/cities city [5]. The five provinces/cities with the highest number of cases include: Hanoi (1,647,706 cases, 1,238 deaths, PFC 0.08%); HCMC (627,587 cases, 20,476 deaths, PFC 3.31%); Hai Phong (537,931 cases, 138 deaths, PFC 0.03%), Nghe An (502,017 cases, 145 deaths, PFC 0.03%) and Bac Giang (391,356 cases, 93 deaths, PFC 0. 02%). The Omicron variant remains the most worrying variant, accounting for 82.7% of the variants that have appeared in Vietnam when reported to the global reporting platform (GISAID), since it was first recorded. recognized in the country in December 2021 (5,966 out of 7,211 sequences) [3,5].
On February 24th, 2020, WHO officially named SARS-CoV-2 as the cause of a pandemic that has the potential to spread globally [6].The outbreak of SARS-CoV-2 makes it the third coronavirus-related pandemic of the twenty-first century, following the occurrences of severe acute respiratory distress syndrome (SARS-CoV) in 2002 and Middle East respiratory syndrome (MERS-CoV) in 2012 [7]. SARS-CoV-2 is the 7th member of the Coronavirus family capable of infecting humans [8]. Since the virus is highly contagious, close contact and droplets may be important channels for human-to-human transmission. It is linked to respiratory diseases such as severe pneumonia and acute respiratory distress syndrome (ARDS) [9]. The extensive destruction of CoVid-19 pandemic is regarded to be equivalent to 1894 plague (12 million deaths) and the 1918-A (H1N1) influenza pandemic (50 million deaths) [7]. As of November 2022, there has been more than 600 million infections and more than 6 million deaths nationwide [3]. Although the mortality rate of the SARS-CoV-2 strain is lower than previous corona pandemics, it has an exceptionally high rate of spread along with the continuous emergence of new strains [10]. In addition to beta/gamma strains that have just been updated, Omicron strains are threatening to start a new round of another large-scale epidemic [11]. Vaccine development is constrained by the constant emergence of variant strains and significant vaccine reluctance gradually [12].
Therefore, the repurposing of pharmaceuticals is anticipated to reverse the pandemic's situation [12]. Drug repositioning or drug repurposing is defined as a different strategy to discover new applications for a previously approved drug to treat disease aside from its primary indication [10]. This reduces cost and expedites the drug development because the drug has been proven medication safety and pharmacokinetic profiling [10]. Because of that, research on broad-spectrum antiviral medications is given priority since they can both prevent and treat human pathogenic viruses that could result in epidemics in the future [12].
An enzyme known as RNA-dependent RNA polymerase (RdRp) is necessary for the single-stranded, gram-positive SARS-CoV-2 virus to replicate in host cells. As a result, numerous antiviral medications focus on this protein to prevent viral replication [12]. The first RdRp inhibitor licensed by the FDA to treat infections brought on by SARS-CoV-2 is Remdesivir. However, Remdesivir is given intravenously, necessitating a medical team's presence, making it inconvenient for non-hospitalized objects [12].
According to a comparative analysis on RdRp inhibition, molnupiravir was reported to have the strongest effect among the anti-viral drugs, including Entacavir, Favipiravir, Peniciclovir, Remdesivir, Ribavirin, Tenofovir [12]. Therefore, the reuse of molnupiravir has attracted attention in the treatment of Covid-19 recently [10]. Molnupiravir also known as β-d-N4-hydroxycytidine-5′-isopropyl ester (NHC) - has been shown to be effective against RNA viruses in influenza, SARS, and Ebola [3]. Molnupiravir is one of only two oral antiviral agents to be urgently approved by the FDA for the treatment of COVID-19 in mild-to-moderate non-hospitalized patients, and at risk of severe progression by December 2021 [13]. Compared with RDS, oral administration of MPV makes it easier for patients to access treatment.
In environments with limited vaccination coverage at the beginning stage, MPV is particularly advantageous at the prophylactic level [10]. Result from clinical trials carried out in 20 countries, which focuses on non-hospitalized individual with mild-to-moderate condition, indicates that using molnupiravir in the early stages of illness mitigates viral load and mortality by up to 30% [14]. Vietnam is one of many countries licensed to circulate molnupiravir [15]. According to the press releases on COVID-19 status on 8th November 2022, Vietnam recorded a total of more than 11 million infections, ranking 13/230 among countries. Additionally, Vietnam's overall fatality rate in Asia came in at 7/49 ( ranked third in ASEAN) [16].
On the other hand, the majority of those with an infection are mild to moderate [17], thus taking oral antivirals is viewed as a suitable preventative approach to balance off the overburdening health care system [17]. However, certain factors such as cost and effectiveness still need further investigation to make sure the use of MPV is appropriate economically [14]. This study aims to estimate the cost of utility of using molnupiravir in mild-to-moderate Covid-19 patients treatment in Vietnam.
2. Materials and Methods
2.1. Study Design
The decision tree model was used to compare the cost utility of treatments for COVID-19 patients with MPV and without MPV in societal perspective. The input comprises adult patients diagnosed with mild-to-moderate COVID-19, who was not hospitalized and had at least one risk factor that could lead to severe progression to hospitalization or death. The study treatment follow-up time was 29 days. All the costs and results were modified with a 3% discount rate based on WHO recommendation. Ultimately, the results are determined through ICER comparison [18,19,20]. It is calculated based on the basis of costs incurred and quality-adjusted life years. Also, the willingness to pay threshold is applied according to WHO recommendations for low- and middle-income countries. In Vietnam, the willingness to pay threshold was not established, so Gross Domestic Product (GDP) of Vietnam was used as the willingness to pay threshold [18,19,20].
2.2. Economic Model
A decision tree model is built based on illness progression. In each option with and without using MPV, there were 3 progressions: recovery, hospitalization, and death. When patients were admitted to hospitals, they received treatment. In the hospitalization, patients were followed up based on two progressions: recovery and death. Patients can move between two different health stages depending on the transition probabilities for the distinct time period. To develop this decision model in this research, we reviewed previous economic evaluation researches on molnupiravir treatment [21,22]. After that, we conducted consultation with local clinical experts and specialized persons, who are conducted COVID-19 treatment in Vietnam to validate model. In order to portray crucial parameters on the model, data were gathered based on assessments of clinical efficacy and economic efficacy, then reviewed and calculated. Consequently, using a decision tree is an easy, practical, and convenient way to visualize the data and calculate costs and efficacy as shown Figure 1.
This model also has a couple assumptions to reduce uncertainty factors that can be affected to model: (1) Patients in this model were diagnosed with mild-to-moderate COVID-19; (2) The COVID-19 treatment did not include complication and co-mobility disease. So, the cost of treatment did not include complication treatment costs and co-mobility treatment costs. (3) The post-Covid treatment symptoms and its treatment cost were not included in the model.
2.3. Cost Variables
The study was designed based on society approaches. The costs include direct medical costs (MPV drugs, hospitalization costs, COVID-19 diagnostic tests), non-medical direct costs (meals, transportation costs of patients and relatives) and indirect costs (opportunity costs lost due to job-related loss of patients and relatives during the treatment period) in the three stages involve before treatment, during the treatment and recovery after treatment. These costs were collected and averaged per day per patient. The costs then will be adjusted to the amount of days required for each stage in order to acquire official non-medical direct cost parameters, serving calculation on the model. Based on Vietnamese State Bank report, all costs were adjusted and presented as US$ in 2022 values using the consumer price index [23].
2.4. Clinical Variables
The probability transmissions were reviewed in previous studies. Mortality and hospitalization rates were obtained from the randomized controlled trial by Jayk Bernal et al. [24] using the transition probabilities, starting from the input: group of patients with positive COVID-19 to recovery, hospitalization and death stage corresponding in the two intervention group. Mortality from the randomized trial by Arribas et al. [25] was used as transition probabilities from the stage of hospitalization to death in MPV-treated patients. In a retrospective study by Andrea Carta et al. [26], mortality was used as the transition probabilities from hospital admission to death in the non-MPV group.
2.5. Health Outcomes
Health outcomes are presented as quality-adjusted life years (QALYs). QALY is calculated by multiplying utility score and life year gained value (LYG). Utility score collecting directly from the overview needs to the reasonable whether using MPV or not. In some circumstances which utility cannot be determined directly from the overview, it then can be calculated using related QALY and LYG.
2.6. Uncertainty Analysis
This study uses one-way sensitivity analysis and probabilistic sensitivity analysis. Sensitivity analysis allows analyzing the influence of data on the model's results, indicating the relationship of input and output factors when the factors were changed in their ±20% valuable change. The one-way sensitivity analysis is displayed through Tornado diagram to compare the impact of different one-way analyses. The probabilistic sensitivity analysis is presented as a cost-effectiveness diagram. The graph is built based on two input variables including incremental costs and incremental QALYs, and the outputs are the ICER distribution points. The probabilistic sensitivity based on Monte Carlo simulation for 1000 times was used to analyze the variability of ICER in case all parameters were varied together simultaneously.

Table 1.
Input parameters of model.
| Parameter description | Value | Distribution | Mean | SE | Reference |
|---|---|---|---|---|---|
| Transitional probability abilities | |||||
| Probability patients received molnupiravir treatment | 0.5036 | Beta | Fischer et al., 2021, Mahase et al., 2021, Jayk Bernal et al., 2021 [24,27,28] | ||
| Probability patients received non-molnupiravir treatment | 0.4964 | Beta | |||
| Probability of recovery using molnupiravir | 0.9323 | Beta | |||
| Probability of hospitalization using molnupiravir | 0.0663 | Beta | |||
| Probability of death using molnupiravir | 0.0014 | Beta | |||
| Probability of hospitalization and recovery using molnupiravir | 0.9444 | Beta | Arribas et al., 2021 [25] | ||
| Probability of hospitalization and death using molnupiravir | 0.0556 | Beta | |||
| Probability of recovery using non-molnupiravir | 0.9027 | Beta | Fischer et al., 2021, Mahase et al., 2021, Jayk Bernal et al., 2021 [24,27,28] | ||
| Probability of hospitalization using non-molnupiravir | 0.0844 | Beta | |||
| Probability of death using non-molnupiravir | 0.0129 | Beta | |||
| Probability of hospitalization and recovery using non-molnupiravir | 0.8516 | Beta | |||
| Probability of hospitalization and death using non-molnupiravir | 0.1484 | Beta | Carta et al., 2021 [26] | ||
| Resource cost parameter | |||||
| Direct medical care cost | |||||
| Direct medical care cost of molnupiravir | 10.83 | Gamma | Sheet Additional information | ||
| Direct medical care cost of hospitalization | 1,476.36 | Gamma | Sheet Additional information Carta et al., 2021 [26] |
||
| Direct medical care cost of quick test | 5.52 | Gamma | Sheet Additional information | ||
| Direct medical care cost of PCR test | 29.53 | Gamma | 14/2019/TT-BYT [29] | ||
| Direct medical care cost of subclinical | 130.41 | Gamma | |||
| Direct non-medical care cost | |||||
| Direct non-medical care cost of eating and drinking for patient (1 day) | 2.31 | Gamma | Thuy et al., 2013 [30] | ||
| Direct non-medical care cost of eating and drinking for caregiver (1 day) | 0.92 | Gamma | |||
| Direct non-medical care cost of moving for patient (1 day) | 0.38 | Gamma | |||
| Direct non-medical care cost of moving for caregiver (1 day) | 0.57 | Gamma | |||
| Direct non-medical care cost of another thing (1 day) | 1.51 | Gamma | |||
| Indirect cost | |||||
| Indirect cost of the patient's opportunity cost (1 day) | 9.44 | Gamma | |||
| Indirect cost of the caregiver's opportunity cost (1 day) | 9.44 | Gamma | |||
| Total cost | |||||
| Total treatment cost of recovery with using molnupiravir | 489.00 | Gamma | Calculation | ||
| Total treatment cost of hospitalization with using molnupiravir | 2,119.78 | Gamma | |||
| Total treatment cost of hospitalization and recovery with using molnupiravir | 344.19 | Gamma | |||
| Total treatment cost of recovery without using molnupiravir | 478.17 | Gamma | |||
| Total treatment cost of hospitalization without using molnupiravir | 2,108.95 | Gamma | |||
| Total treatment cost of hospitalization and recovery without using molnupiravir | 344.19 | Gamma | |||
| Utility parameter | |||||
| Utility of patients using molnupiravir with recovery (mild-moderate) | 0.8900 | ||||
| Utility of patients using molnupiravir with hospitalization and recovery | 0.8900 | Sheinson et al., 2021 [31] | |||
| Utility of patients using non-molnupiravir with recovery | 0.6200 | ||||
| Utility of patients using non-molnupiravir with hospitalization and recovery | 0.7870 | Calculation | |||
| Life-years gained of using antiviral drug | 12.9610 | Sheinson et al., 2021 [31] | |||
| Quality adjusted life years of using antiviral drug | 10.2280 | ||||
| Life-years gained of non-using antiviral drug | 12.4320 | ||||
| Quality adjusted life years of non-using antiviral drug | 9.7900 | ||||
| Discounting rate for course | 3% | WHO | |||
| Discounting rate for outcomes | 3% | ||||
3. Results
3.1. Base Case Analysis
The total cost for patients getting molnupiravir was US$ 617.96, whereas the cost for those not receiving it was US$ 634.40. The LYG between the two interventions was similar, but Utility score in the MPV-treated group (0.89) was higher compared to the non-MPV users (0.62). It can be concluded that the use of molnupiravir in treatment improves the quality of life (QALYs) of Covid-19 patients.
After determining the effectiveness and cost, the findings showed that utilizing MPV not only reduced expenses (saving US$ 16.44) but also improved quality of life in COVID-19 patients. According to estimates, individuals who received MPV in therapy had 8.61 QALYs higher than those who did not.
The ICER coefficient shows that molnupiravir is very cost effective when compared to Vietnam's GDP 3,694.02 USD (2021) [32].
Table 2.
Total costs, QALYs and ICER in base case analysis.
| Content | MPV | Non-MPV |
|---|---|---|
| Utility | 0.89 | 0.62 |
| LYG | 32.00 | 32.00 |
| QALYs | 28.33 | 19.72 |
| Incremental QALYs | 8.6137 | |
| Costs | 617.96 | 634.40 |
| Incremental Costs | -16.44 | |
| ICER | -1.91 | |
* 1 USD = 24,860 VND [23]
3.2. Uncertainty Analysis
One-way sensitivity analysis is shown in Figure 2 as a tornado diagram with the change of factors. The most significant influences on model outputs were made by non-medical direct costs (-10.13% to 15.14% change in ICER) and patients' utility (-11.53% to 7.91% change in ICER), whereas direct medical expenses (-1.11% to 1.81% change in ICER) had the least impact. The remaining factors that contributed to the model’s result include medication expenses, transportation costs, food costs, hospitalization costs, and testing costs.
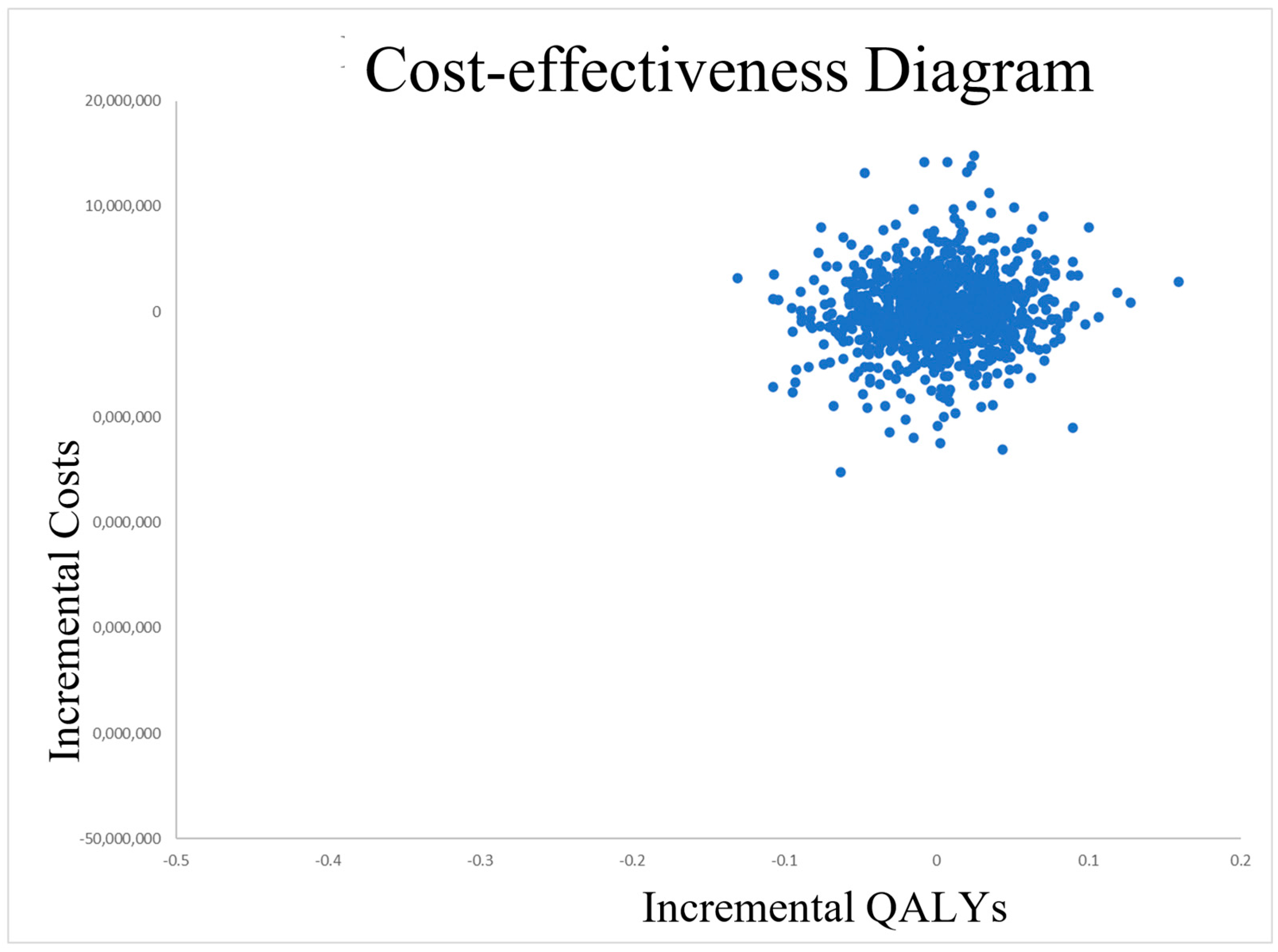
On the other hand, the incremental costs and incremental QALYs are used as the inputs for the two-way sensitivity analysis, and the ICER distribution points are the outputs. The distribution results are presented in the form of scatter plots (Figure 3). The distribution locations are largely concentrated in the southeast quadrant, as shown by the cost-effectiveness graphic. Additionally, the distribution points have minor data dispersion and cluster around a position that is somewhat near to the study's ICER value. This suggests using MPV is more effective and less money-consuming than treatment without MPV.
4. Discussion
The study outcome demonstrates that MPV is clinically effective in treating COVID-19 individuals with mild-to-moderate symptoms. MPV helped to reduce hospitalization rates, risk of death, and improve illness status. Hospitalization and mortality rates for MPV-treated patients were 0.0663 and 0.0014, respectively, compared to 0.0844 and 0.0129 for non-MPV users. Given that the study participants had at least one risk factor that might cause a serious illness requiring hospitalization or even death, MPV did lower the hospitalization rate 1.3-fold and mortality rate significantly with 9.2-fold. On the other hand, MPV contributed to a 21.45% reduction in hospital admissions along with 89.15% reduction in mortality. Furthermore, a 30.42% decrease in overall hospitalization rate and mortality rate showed that MPV offered great benefits for the treatment of mild-to-moderate COVID-19 patients as well as for the medical team and other healthcare workers. Hospitalized patients' recovery and death rates were 0.9444 and 0.0556 in the MPV-using group, respectively, indicating an increase of 1.1-fold and a drop of 2.7-fold compared to the placebo group, which had reported rates of 0.8516 and 0.1484 respectively. The outcome proved that MPV is helpful in lowering hospitalization and mortality in COVID-19 patients with mild- to-moderate symptoms.
The total utility cost of the using molnupiravir groups (US$ 617.96) was lower than that of the non-using molnupiravir groups (US$ 634.40), suggesting a clinical effect in mild-to-moderate COVID-19 infections. As a result, MPV helps society and the patient save money by lowering the potential that the sickness will get worse and require hospitalization. Noticeably, since MPV helps to lower the hospitalization rate, it also helps to lessen the financial burden on patients and their families as the cost in hospitalized groups is significantly higher than that in non-hospitalized ones. It was observed that there was no significant gap in the overall cost of treatment in the two intervention groups. The cost of molnupiravir ($10.83) is what makes the difference. By spending just one day's worth of the typical salary or more, patients can maximize their chances of saving on hospitalization costs, which can account for more than 60% of a Vietnamese individual's annual income.
The direct non-medical cost was believed to have the biggest impact on our study’s result. The percentage change in ICER value affected by this factor is 8.65 times higher compared to the direct medical costs. The expense of moving to the hospital and other variables could be the cause of the increase in non-medical direct costs. Also, the rise in direct medical costs and treatment costs alone may result in the discontinuation of therapeutic procedures ultimately, due to patient’s inability to afford full treatment. To help patients cope with the burden of direct non-medical charges, the government could consider building new hospitals, particularly in rural locations distant from urban centers. This will lower travel expenses and make it simpler for patients to access healthcare. Consequently, it is possible to decrease the number of patients who must discontinue treatment and prevent the patient's condition from getting worse in the future. Additionally, the inclusion of MPV in health insurance will make it simpler for patients to get MPV therapy and lessens financial worries.
According to the study's findings, patients who used MPV had significantly better post-recovery conditions than those who didn't, having a utility of 0.89 and 0.62, respectively. Regarding hospital admission, patients receiving MPV treatment were thought to feel more at ease and better than groups not receiving MPV treatment. One may assert that MPV not only demonstrates clinical efficacy and lowers treatment costs, but also improves the quality-adjusted life years (QALYs) of COVID-19 patients with mild-to-moderate symptoms.
After calculation, the ICER obtained is -1.91 USD/QALY. Comparing the MPV-using group to those who did not use MPV, the result reveals a decrease in utility costs and an improvement in treatment efficacy. Furthermore, the ICER value indicates that utilizing MPV to treat patients with mild-to-moderate COVID-19 results in savings of $1.91 for each QALY attained. When compared with Vietnam's willingness to pay as determined by GDP, the value of ICER < 1 GDP (3,694.02 USD – 2021) [32] suggests that the drug is very cost-effectiveness.
The results of this study are consistent with the cost-effectiveness studies of molnupiravir in the US [21] and South Korea [22], both showing that molnupiravir is cost-effectiveness in treating mild and moderate COVID-19 patients and, the group of patients showing high efficiency in treatment is the elderly group. The study also showed a similarity in the therapeutic effect of molnupiravir where hospitalization was significantly reduced and recovery probability also increased significantly compared with the group without using molnupiravir [21,22]. Because of many complications from Corona virus, so all studies were not included complications, adverse events and post-COVID in model calculations [21,22].
However, our study still has a couple limitations. (1) molnupiravir is the first oral antiviral to be included in the treatment guidelines for COVID-19. Because this is a new drug, there is very little data on its safety and efficacy on COVID-19 treatment. (2) We did not include side effects and adverse events (ADRs), complications and post-COVID. This, in turn, can reduce the quality of life and increase costs. (3) Noticeably, there hasn't yet been any clinical research on MPV done in Vietnam. Thus, the data for the statistics utilized in this article—including utility score, patient mortality, hospitalization rates, recovery rates, and other expense information—was acquired from sources in different nations and National COVID-19 report. As a result, the findings might not be universally representative of Vietnamese people. (4) In this study, we did not declare the variant of COVID-19, so the efficacy and safety in patients may be changed.
5. Conclusions
This is first research in Vietnam when estimated the cost-effectiveness of using molnupiravir in COVID-19 treatment. It is dominant to use molnupiravir in Vietnam to treat people with mild-to-moderate COVID-19 infections. As a result, decision-makers should consider including molnupiravir on the Vietnam Health Insurance Drug List to reduce cost of treatment of patients. Utilizing MPV is advised while controlling COVID-19. However, various clinically relevant drug-related factors still need to be evaluated. As the previous mentioned, this is the first new oral antiviral drug, there is limited data on safety and efficacy. Therefore, when administering drugs to patients, active safety monitoring is required, along with other strategies to minimize potential harm. Because of these concerns and data gaps, molnupiravir should only be given to non-severe COVID-19 patients at high risk of hospitalization, typically those who have not been vaccinated against COVID-19, older adults, immunocompromised and chronically ill.
References
- Tu, Y.-F.; Chien, C.-S.; Yarmishyn, A.A.; Lin, Y.-Y.; Luo, Y.-H.; Lin, Y.-T.; Lai, W.-Y.; Yang, D.-M.; Chou, S.-J.; Yang, Y.-P.; et al. A Review Of SARS-Cov-2 And The Ongoing Clinical Trials. International Journal Of Molecular Sciences 2020, 21, 2657. [Google Scholar] [CrossRef] [PubMed]
- WHO. COVID-19 Situation Reports. 2019. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 7 November 2022).
- WHO. COVID-19 Weekly Epidemiological Update; 25 May 2023, 2023. 25 May.
- Vietnam, W. Viet Nam COVID-19 Situation Report #109; 2023.
- Wu, Z.; Harrich, D.; Li, Z.; Hu, D.; Li, D. The Unique Features Of SARS-Cov-2 Transmission: Comparison With SARS-Cov, MERS-Cov And 2009 H1N1 Pandemic Influenza Virus. Reviews In Medical Virology 2020, 31, e2171. [Google Scholar] [CrossRef]
- Kai-Wang, K.; Sridhar, S.; Chiu, K.H.-Y.; Hung, D.L.-L.; Li, X.; Hung, I.F.-N.; Tam, A.R.; Chung, T.W.-H.; Chan, J.F.-W.; Zhang, A.J.-X.; et al. Lessons Learned 1 Year After SARS-Cov-2 Emergence Leading To COVID-19 Pandemic. Emerging Microbes & Infections 2021, 10, 507–535. [Google Scholar]
- Wang, Y.; Wang, Y.; Chen, Y.; Qin, Q. Unique Epidemiological And Clinical Features Of The Emerging 2019 Novel Coronavirus Pneumonia (COVID-19) Implicate Special Control Measures. Journal Of Medical Virology 2020, 92, 568–576. [Google Scholar] [CrossRef] [PubMed]
- Bchetnia, M.; Girard, C.; Duchaine, C.; Laprise, C. The Outbreak Of The Novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-Cov-2): A Review Of The Current Global Status. Journal Of Infection And Public Health 2020, 13, 1601–1610. [Google Scholar] [CrossRef]
- Yip, A.J.W.; Low, Z.Y.; Chow, V.T.K.; Lal, S.K. Repurposing Molnupiravir For COVID-19: The Mechanisms Of Antiviral Activity. Viruses 2022, 14, 1345. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Chen, Y.; Lu, X.; Zhang, W.; Fang, W.; Yuan, L.; Wang, X. An Update On Inhibitors Targeting RNA-Dependent RNA Polymerase For COVID-19 Treatment: Promises And Challenges. Biochemical Pharmacology 2022, 205, 115279. [Google Scholar] [CrossRef]
- Masyeni, S.; Iqhrammullah, M.; Frediansyah, A.; Nainu, F.; Tallei, T.; Emran, T.B.; Ophinni, Y.; Dhama, K.; Harapan, H. Molnupiravir: A Lethal Mutagenic Drug Against Rapidly Mutating Severe Acute Respiratory Syndrome Coronavirus 2—A Narrative Review. Journal Of Medical Virology 2022, 94, 3006–3016. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.K.H.; Au, I.C.H.; Lau, K.T.K.; Lau, E.H.Y.; Cowling, B.J.; Leung, G.M. Real-World Effectiveness Of Early Molnupiravir Or Nirmatrelvir–Ritonavir In Hospitalised Patients With COVID-19 Without Supplemental Oxygen Requirement On Admission During Hong Kong's Omicron BA.2 Wave: A Retrospective Cohort Study. The Lancet Infectious Diseases 2022, 22, 1681–1693. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.K.H.; Au, I.C.H.; Lau, K.T.K.; Lau, E.H.Y.; Cowling, B.J.; Leung, G.M. Real-World Effectiveness Of Molnupiravir And Nirmatrelvir Plus Ritonavir Against Mortality, Hospitalisation, And In-Hospital Outcomes Among Community-Dwelling, Ambulatory Patients With Confirmed SARS-Cov-2 Infection During The Omicron Wave In Hong Kong: An Observational Study. The Lancet 2022, 400, 1213–1222. [Google Scholar]
- Vietnam, M. One more domestically generic produced drug Molnupiravir to treat COVID-19 has been granted a certificate of circulation in Vietnam. Available online: https://moh.gov.vn/thong-tin-chi-dao-dieu-hanh/-/asset_publisher/DOHhlnDN87WZ/content/them-1-thuoc-molnupiravir-ieu-tri-covid-19-san-xuat-trong-nuoc-uoc-cap-giay-ang-ky-luu-hanh-tai-viet-nam?inheritRedirect=false (accessed on 7 November 2022).
- Vietnam, M. Newsletter on COVID-19 prevention and control of the Ministry of Health on August 11th. Available online: https://moh.gov.vn/tin-tong-hop/-/asset_publisher/k206Q9qkZOqn/content/ban-tin-phong-chong-dich-covid-19-cua-bo-y-te-ngay-8-11?inheritRedirect=false&redirect=https%3A%2F%2Fmoh.gov.vn%3A443%2Ftin-tong-hop%3Fp_p_id%3D101_INSTANCE_k206Q9qkZOqn%26p_p_lifecycle%3D0%26p_p_state%3Dnormal%26p_p_mode%3Dview%26p_p_col_id%3Drow-3-column-2%26p_p_col_pos%3D1%26p_p_col_count%3D2 (accessed on 7 November 2022).
- Jo, Y.; Kim, S.B.; Radnaabaatar, M.; Huh, K.; Yoo, J.-H.; Peck, K.R.; Park, H.; Jung, J. Model-Based Cost-Effectiveness Analysis Of Oral Antivirals Against SARS-Cov-2 In Korea. Epidemiology And Health 2022, 44, e2022034. [Google Scholar] [CrossRef] [PubMed]
- WHO. Cost-effectiveness thresholds. 2012.
- WHO. MAKING CHOICES IN HEALTH: WHO GUIDE TO COST-EFFECTIVENESS ANALYSIS. Available online: https://apps.who.int/iris/bitstream/handle/10665/42699/9241546018.pdf;jsessionid=6A5719658CC4ADCE9ECF39BFB22A260C?sequence=1.
- WHO. New cost-effectiveness updates from WHO-CHOICE. Available online: https://www.who.int/news-room/feature-stories/detail/new-cost-effectiveness-updates-from-who-choice.
- Goswami, H.; Alsumali, A.; Jiang, Y.; Schindler, M.; Duke, E.R.; Cohen, J.; Briggs, A.; Puenpatom, A. Cost-Effectiveness Analysis of Molnupiravir Versus Best Supportive Care for the Treatment of Outpatient COVID-19 in Adults in the US. Pharmacoeconomics 2022, 40, 699–714. [Google Scholar] [CrossRef] [PubMed]
- Jo, Y.; Kim, S.B.; Radnaabaatar, M.; Huh, K.; Yoo, J.H.; Peck, K.R.; Park, H.; Jung, J. Model-based cost-effectiveness analysis of oral antivirals against SARS-CoV-2 in Korea. Epidemiol Health 2022, 44, e2022034. [Google Scholar] [CrossRef] [PubMed]
- Vietnam, T.S.B.o. Reference exchange rate at the State Bank of Vietnam 2022. Available online: https://sbv.gov.vn/TyGia/faces/TyGia.jspx?_afrLoop=4216357552103891&_afrWindowMode=0&_adf.ctrl-state=owrk6r3t8_4 (accessed on 12 November 2022).
- Bernal, A.J.; Silva, M.M.G.d.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Reyes, V.D.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of Covid-19 in Nonhospitalized Patients. N Engl J Med 2022, 386, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Arribas, J.R.; Bhagani, S.; Lobo, S.M.; Khaertynova, I.; Mateu, L.; Fishchuk, R.; Park, W.Y.; Hussein, K.; Kim, S.W.; Ghosn, J.; et al. Randomized Trial of Molnupiravir or Placebo in Patients Hospitalized with Covid-19. NEJM Evidence 2021, 1, 9. [Google Scholar] [CrossRef]
- Carta, A.; Conversano, C. Cost utility analysis of Remdesivir and Dexamethasone treatment for hospitalised COVID-19 patients - a hypothetical study. BMC Health Serv Res 2021, 21, 986. [Google Scholar] [CrossRef] [PubMed]
- Fischer, W.A.; Eron, J.J., Jr.; Holman, W.; Cohen, M.S.; Fang, L.; Szewczyk, L.J.; Sheahan, T.P.; Baric, R.; Mollan, K.R.; Wolfe, C.R.; et al. A phase 2a clinical trial of molnupiravir in patients with COVID-19 shows accelerated SARS-CoV-2 RNA clearance and elimination of infectious virus. Sci Transl Med 2022, 14, eabl7430. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. Covid-19: Molnupiravir reduces risk of hospital admission or death by 50% in patients at risk, MSD reports. BMJ 2021, 375, n2422. [Google Scholar] [CrossRef] [PubMed]
- Vietnam, M. Circular 14/2019/TT-BYT. Ha Noi, 2019.
- THUY, N.T.B.; PHU, V.X.; ANH, N.Q. Direct medical care cost and non-medical care cost of patients with diabetes in the endocrinology department, hospital Thanh Nhan – Hanoi, 2013. Y HỌC THỰC HÀNH 2013, 893, 8. [Google Scholar]
- Sheinson, D.; Dang, J.; Shah, A.; Meng, Y.; Elsea, D.; Kowal, S. A Cost-Effectiveness Framework for COVID-19 Treatments for Hospitalized Patients in the United States. Adv Ther 2021, 38, 1811–1831. [Google Scholar] [CrossRef] [PubMed]
- IBRD. GDP per capita (current US$) - Vietnam 2021. Available online: https://data.worldbank.org/country/vietnam (accessed on 11 November 2022).
Figure 1.
Decision tree model of using molnupiravir and non-molnupiravir for COVID-19 patients in Vietnam.
Figure 1.
Decision tree model of using molnupiravir and non-molnupiravir for COVID-19 patients in Vietnam.
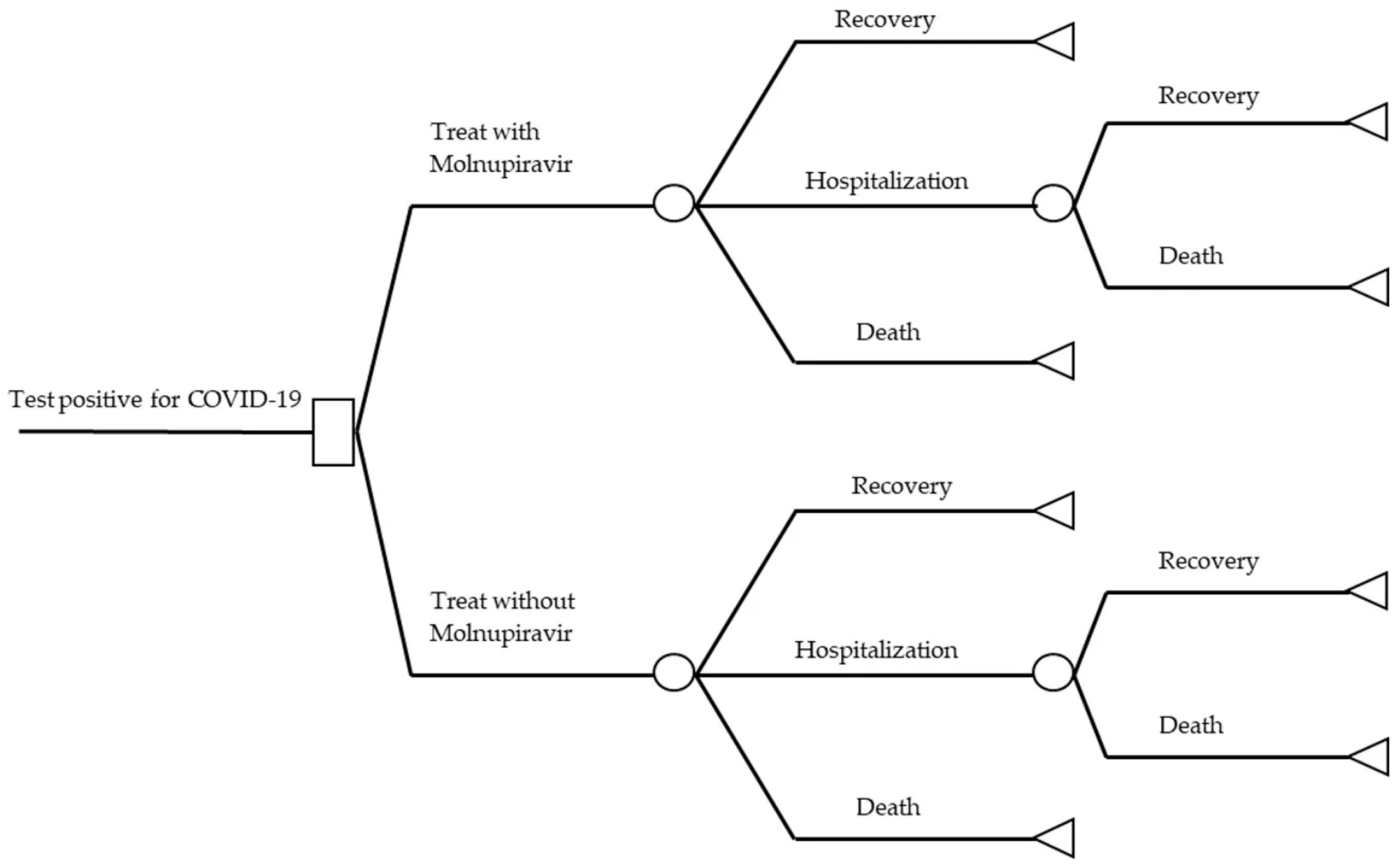
Figure 2.
Tornado model.
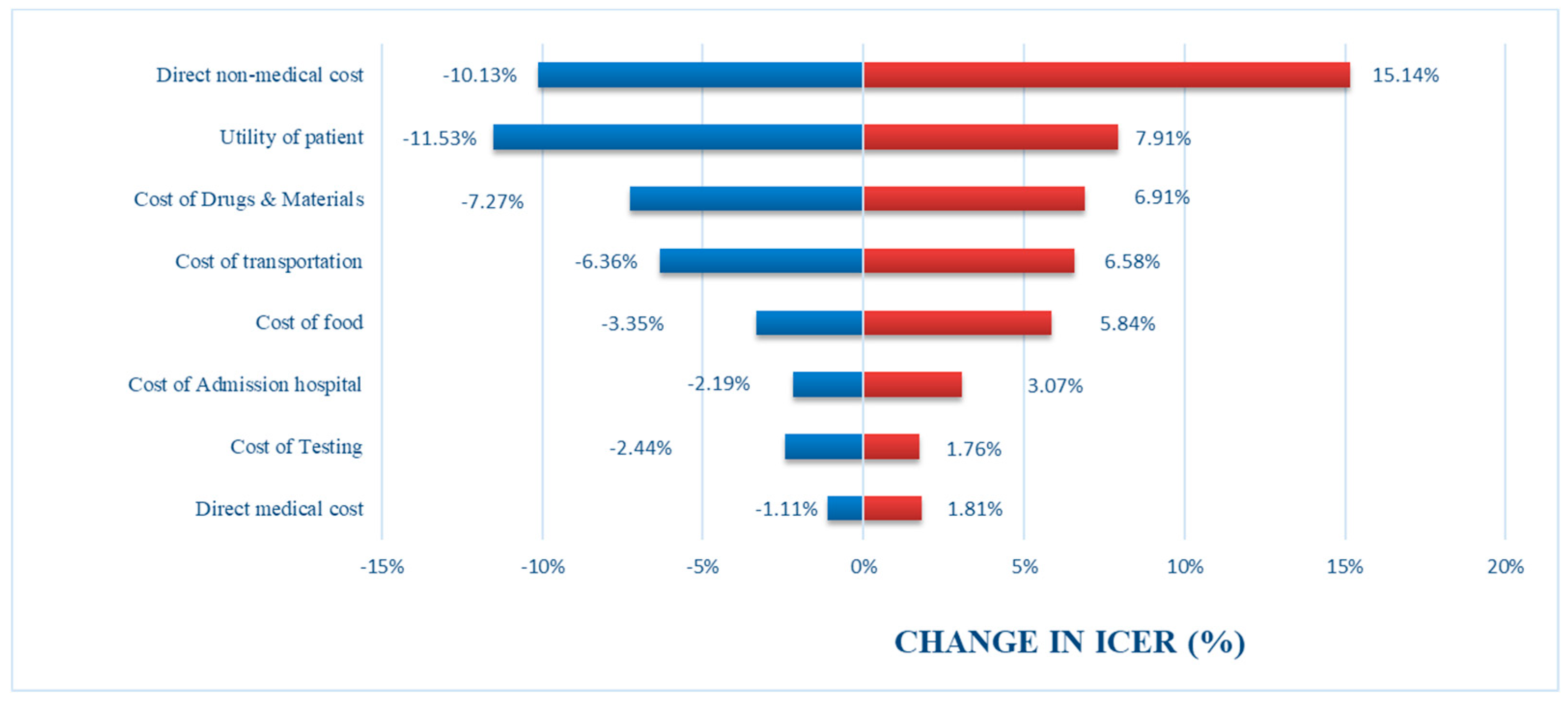
Figure 3.
Cost-effectiveness diagram.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



