
Submitted:
22 June 2023
Posted:
23 June 2023
You are already at the latest version
Abstract
Recently, two respiratory syncytial virus (RSV) vaccines based on the prefusion F (pre-F) antigen were approved in the United States. We developed and validated an enzyme-linked immunosorbent assay (ELISA)-based protocol for the practical and large-scale evaluation of RSV vaccines. Two modified pre-F proteins (DS-Cav1 and SC-TM) were produced by genetic recombination and replication using an adenoviral vector. The protocol was established by optimizing the concentrations of the coating antigen (pre-F proteins), secondary antibodies, and choice of blocking buffer. To validate the protocol, we examined its accuracy, precision, and specificity using serum samples from 150 participants across various age groups and the standard serum provided by the National Institute of Health. In the linear correlation analysis, coating concentrations of 5 and 2.5 μg/mL of DS-Cav1 and SC-TM, respectively, showed high coefficients of determination (r2 = 0.90). Concentrations of secondary antibodies (alkaline phosphatase-conjugated anti-human immunoglobulin G, diluted 1:2000) and blocking reagents (5% skim milk/PBS-T) were optimized to minimize non-specific reactions. High accuracy was observed for DS-Cav1 (r2 = 0.90) and SC-TM (r2 = 0.86). Further, both antigens showed high precision (coefficient of variation < 15%). Inhibition ELISA revealed cross-reactivity of antibodies against DS-Cav1 and SC-TM but not with the attachment protein.
Keywords:
respiratory syncytial virus
; RSV
; ELISA
; Vaccine
; Immunogenicity
1. Introduction
Respiratory syncytial virus (RSV) is a major respiratory pathogen in young children, which imposes a greater disease burden than influenza in this age group [1]. Now it is being recognized as an important pathogen in older adults and immunocompromised individuals as well, causing acute exacerbation of pre-existing cardiovascular diseases or severe pneumonia [2,3,4]. Despite its clinical importance, the treatment and prevention tools for RSV remain limited, unlike seasonal influenza for which effective antiviral drugs and vaccines are available. Therefore, the World Health Organization is committed to develop effective RSV vaccines by actively working with pharmaceutical companies [5]. As of January 2023, 22 vaccine candidates have entered clinical trials, six of which are in phase 3 [6]. Because several vaccine candidates have recently been reported to have satisfactory safety profiles and efficacy, one or more RSV vaccines are expected to be approved in the near future.
Among surface antigens of RSV, the fusion (F) protein and attachment (G) protein comprise the major immunogens, with the F protein being the preferred target of vaccines and monoclonal antibodies [7]. The F protein exists in two forms: a prefusion (pre-F) form before fusion with the host cell membrane, and a postfusion form. Despite being more immunogenic than the postfusion form, pre-F has not been used as a vaccine target because of its structural instability, a characteristic that has led to the failure of RSV vaccine development in the past [7,8]. In the last decade, the structure of the pre-F form was revealed and subsequently engineered to make it more stable, DS-Cav1 and SC-TM, being the most widely used vaccine targets [9,10].
RSV vaccine candidates are based on various platforms, making it necessary to establish a standardized immunogenicity test protocol applicable to all vaccine products. Additionally, it is desirable to examine the correlation between simple and scalable enzyme-linked immunosorbent assays (ELISA) and neutralization tests, a labor-intensive gold standard. Therefore, we developed and validated an indirect ELISA-based protocol using the two most commonly modified pre-F proteins, DS-Cav1 and SC-TM, and G protein.
2. Materials and Methods
2.1. Study Population
Anonymized blood samples were collected from a total of 150 healthy children and adults, stratified by age groups: under 5 years, 5–18 years, 19–49 years, 50–64 years, and aged 65 years and above, from February to November 2021. This study was approved by the Institutional Board of Review of Korea University Guro Hospital; IRB No. 2022GR0149, and the requirement for informed consent was waived.
2.2. Protein Construct Design, Expression, and Purification
Adeno-X 293 cells (Takara Bio Inc, Shiga, Japan) were grown in Dulbecco’s modified Eagle medium (Thermo Fisher Scientific, Waltham, MA, USA) supplemented with penicillin-streptomycin (Thermo Fisher Scientific) and 10% fetal bovine serum (FBS; Biowest, Nuaillé, France). Genes expressing the RSV A2 F protein (Genbank AC083301.1) were designed as previously reported and synthesized by Bionics (Seoul, Korea) [10,11]. All recombinant proteins were cloned into the ectodomain of the F protein with a C-terminal fold on the trimerization domain. SC-TM was designed by replacing the p27 sequence with a seven-amino acid GS-rich linker sequence and additionally replacing three amino acids (N67I, S215P, and D486N). The DS-Cav1 protein, containing four mutations (S155C, S190F, V207L, and S290C), has been previously described [9]. Each gene was cloned into the pAdenoX vector (Takara), and the linearized vectors were transfected into Adeno-X 293 cells. Proteins were purified by Ni-NTA chromatography (Thermo Fisher Scientific), and further purified by Strep-Tactin Sepharose chromatography (Iba-Life Sciences, Göttingen, Germany).
A synthetic gene encoding the RSV A2 (Genbank AC083301.1) G protein (secreted form; sG, amino acids 48 to 298) was cloned into pET28a in-frame with a C-terminal tandem 6-histidine. Recombinant G proteins were expressed in E. coli BL21(DE3) and purified by Ni-NTA chromatography (Thermo Fisher Scientific).
2.3. Development and Optimization of the ELISA-Based Protocol
The activity of the three antigens was confirmed by serial dilution and inhibition ELISA. Each antigen was fixed on the hydrophilic immunoplate, Maxibinding Plate (SPL, Pocheon, South Korea), at a concentration of 0, 1, 2.5, 5, 7.5, and 10 mcg/mL and immobilized for overnight at 4 °C. Serum samples were diluted to 1:100, 1:400, and 1:1600; phosphate buffer solution (PBS; Welgene, Gyeongsan, South Korea) was used as a negative control. The secondary antibody alkaline phosphatase-conjugated anti-human immunoglobulin G (IgG; Southern Biotech, Birmingham, AL, USA), was diluted to 1:2000, 1:4000, 1:6000, and 1:8000. Alkaline phosphatase was used as a colorimetric substrate. The optical density was measured at 405 nm (OD405) and 690 nm (OD690) using a Spectramax 190 plate reader (Molecular Devices, San Jose, CA, USA), and the value obtained by subtracting OD690 from OD405 was plotted against the titers of standardized serum provided by the National Institute of Health. The standardized curve-fit four-parameter logistic method was used to calculate antibody titers of clinical samples. Concentrations at which coating antigens and dilution factors of secondary antibodies exhibited 1) high optical density at high sample concentrations, and 2) low optical density with PBS, were chosen.
In addition, the following four blocking agents were examined to select one that minimizes non-specific antigen-antibody reactions: PBS with 0.05% Tween 20 (PBS-T); 1% bovine serum albumin (BSA)/PBS-T; 10% fetal bovine serum/PBS-T; and 5% skim milk/PBS-T. All experiments were performed in duplicate and the average values were compared. The blocking agent that exhibited the lowest optical density and highest correlation coefficient (r2) was chosen. All chemical reagents used in this study were purchased from Sigma-Aldrich (St. Louis, MO, USA).
2.4. Validation of the ELISA-Based Protocol
The accuracy, precision, and specificity of the established ELISA-based protocol were evaluated as follows:
- Accuracy: Low, medium, and high titers of National Institute of Health-provided standard serum were serially diluted 2-fold from 1:200 to 1:6,400. All experiments were performed in duplicate for each concentration. The average optical density values were plotted against the antiserum concentrations, and the r2 values were derived by correlating the calculated antibody titers against the three RSV antigens.
- Precision: One sample was used from each age group. A total of five samples was diluted 2-fold from 1:200 to 1:25,600. The experiment was performed six times for each sample concentration, and the coefficient of variation (CV) was calculated.
- Specificity: All 150 samples were adsorbed with each of the three homologous/heterologous RSV antigens (10 μg/mL of DS-Cav1, SC-TM, and G protein) for an hour with gentle shaking (300 rpm) at RT following which the antibody titers were measured. Post-adsorption titers were compared with pre-adsorption titers. Cross-reactivity was determined based on whether the antibody titers were significantly lower after adsorption. Because RSV infection is mainly prevalent in young children, and also because antibody specificity might be affected by the difference in the duration of time elapsed since the last RSV infection among the age groups studied, we investigated whether there was a difference in the antibody specificity based on age.
2.5. Correlation of Antibody Titers Determined by ELISA with Neutralizing Antibody Titers
We evaluated the correlation between antibody titers determined by ELISA and neutralizing antibody titers measured using the viral reduction neutralization test (VRNT). The VRNT was conducted on 30 samples, with six samples from each age group, and performed as follows: Hep-2 cells were seeded in a 96-well plate and cultured for 24 h at 37 °C. Sera were diluted 1/10 and inactivated at 56 °C for 30 min. RSV-RFP (RSV/A2/Kline 19 from Professor Martin ML) was diluted in PBS to a multiplicity of infection (MOI) of 2.5. 50 μL of diluted virus was mixed with 50 μL of serum sample and incubated for 1 h at 37 °C. A total of 60 µL of each virus-serum mixture was aliquoted to their designated cell-containing wells and incubated for 1.5 h at 37°C, after which the mixture was removed and incubated in 100 µL of 2% Dulbecco’s modified Eagle medium overlay solution for 24 h at 37°C. Culture medium was removed from the 96-well culture plate and well were washed with 100 µL before incubating with virus-serum mixture. After 24 h, cells were fixed with 4% paraformaldehyde for 30 min and then rinsed with PBS-T (Tween-20) wash buffer. Nuclei were stained by treating with 50 µL of 6-diaminidino-2-phenylindole solution (1:50000) for 5 min at 20°C and then washed with 100 µL PBS-T. A total of 50 µL of distilled water was added to each well before imaging the sample plates using the Operetta CLS system (PerkinElmer, USA). The neutralizing dose was determined by counting the number of infected and non-infected cells. The correlation between antibody titers against the three RSV antigens measured using our ELISA protocol and the 50% neutralization dose (VRNT50) was examined.
2.6. Statistical Analyses
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 22.0 (SPSS Korea; Seoul, Republic of Korea). For the correlation between pre-F protein concentration and OD, r2 values > 0.90 in the linear correlation analyses were considered acceptable. For precision, test conditions were considered equivalent and reproducible at a CV ≤ 20%.
3. Results
3.1. Development and Optimization of ELISA-Based Protocol
The concentration of DS-Cav1, as coating antigen, was 5 μg/mL, and the dilution factor of the secondary antibody, at which a high optical density and r2 value greater than 0.9 was obtained, was 1:2,000 (Table S1). The SC-TM and G proteins were coated at a concentration of 2.5 μg/mL and 5 μg/mL, respectively. The optimal dilution factor for the secondary antibody was 1:2,000 and 1:6,000 for SC-TM and G protein, respectively. For all three RSV antigens, 5% skim milk/PBS-T was used as the blocking reagent as it exhibited the lowest optical density and an r2 value greater than 0.9, among the four blocking agents examined (Table S2).
3.2. Validation of the ELISA-Based Protocol
High accuracy was observed for all three RSV antigens. The value of r2 was greater than 0.85 for all antisera used. Overall, the r2 values measured with the reference antiserum were 0.9045, 0.8603, and 0.9777 for DS-Cav1, SC-TM, and G protein, respectively (Table 1). The precision of CV values was estimated to be below 15% for all RSV antigens and dilution factors. The mean CV values for DS-Cav1, SC-TM, and G protein were 2.599 %, 2.737%, and 5.129%, respectively (Table 2).
Specificity was found to be high between the pre-F and G proteins, but low between the two pre-F proteins (DS-Cav1 and SC-TM). When adsorbed with a homologous antigen specific to each antibody, the anti-DS-Cav1, anti-SC-TM, and anti-G IgG titers decreased to 49.6%, 42.6%, and 24.5%, respectively (Table 3). The DS-Cav1-specific antibody titer decreased by an average of 44.3% when adsorbed with the SC-TM protein. Similarly, the titer of the SC-TM-specific antibody decreased by an average of 55.0% when adsorbed with the DS-Cav1 protein. Therefore, antibodies against DS-Cav1 and SC-TM showed cross-reactivity with SC-TM and DS-Cav1 antigens, respectively. In comparison, the DS-Cav1- and SC-TM-specific antibody titers were reduced by less than 10% after adsorption with G protein.
The differences in antibody specificity based on age group were examined. The post-adsorption anti-DS-Cav1 IgG antibody titer was found to decrease more significantly in individuals aged 65 years and above than in children aged < 5 years; anti-DS-Cav1 titers after/before adsorption with DS-Cav1, SC-TM, and G protein were 72.5%/22.6%, 68.0%/27.4%, and 106.9%/35.2%, respectively. Conversely, anti-SC-TM and anti-G protein antibody titers showed a greater decrease after adsorption in children aged < 5 years than in those aged 65 years and above. Anti-DS-Cav1 and anti-SC-TM IgG antibody titers were positively correlated (Figure 1). Although the r2 value derived from the entire study population was low (0.1742), the linear relationship became clearer when divided by age group and remained statistically significant. The correlation was strongest in individuals aged 19–49 years (r2 = 0.6552) and lowest in children aged < 5 years (r2 = 0.3879).
3.3. Correlation with Neutralizing Antibody Titers
The correlation between IgG titers and neutralizing antibody titers against the three RSV antigens was weak. The value of r2 between IgG titers and VRNT50 was 0.1449 (p = 0.526), 0.0496 (p = 0.237), and 0.2655 (p = 0.004) for DS-Cav1, SC-TM, and G protein, respectively (Figure 2). When examined based on age group, the r2 values were estimated to be in the range of 0.1158–0.4795, 0.0309–0.1437, and 0.0042–0.6080 for DS-Cav1, SC-TM, and G protein, respectively.
4. Discussion
We established an ELISA protocol using two modified pre-F proteins, DS-Cav1 and SC-TM, and G protein, which showed good accuracy and precision. Although the two types of pre-F proteins showed remarkable cross-reactivity, high specificity was observed between pre-F and G proteins in adults. There was poor correlation between IgG antibody titers and neutralizing antibody titers measured using the VRNT.
When adsorbed with G protein, the SC-TM antibody titer was barely reduced (94.9% of the pre-adsorption titer) across all age groups; however, the DS-Cav1 antibody titer was considerably reduced by 37.2% in young children aged 5-18 years. Similarly, when adsorbed with pre-F proteins, the anti-G protein antibody titer decreased by approximately 50% on average in children. Young children are repeatedly exposed to diverse respiratory viral antigens, which results in non-specific antibody responses; therefore, the proportion of antibodies with lower specificity may be higher in children than in adults. As reported previously, antibody responses to RSV infection are influenced by independent factors such as level of development of the child's immune system and the presence or absence of maternal antibodies [12]. In addition, instability of the prefusion form of the soluble DS-Cav1 pre-F protein might influence the immune response to the protein; the G protein is highly glycosylated and shows variable antigenicity among RSV strains, except for the centrally conserved domain [13,14].
The low correlation between IgG pre-F antibody titers and neutralizing antibody titers might be due to the small amounts of functional antibodies. For this study, blood samples were collected from healthy individuals when RSV was in low circulation in the community because of the COVID-19 pandemic. A higher correlation can be expected when neutralizing antibody titers and post-vaccination RSV antibody titers are measured. Further studies are warranted to validate this assay in RSV vaccine recipients.
This study had some limitations. First, neither paired acute/convalescent sera nor postvaccination sera were available. Thus, specificity and correlation analyses were limited. Second, we did not test the neutralizing activity against the two RSV strains (A and B). However, the F protein genetic sequence is highly conserved between RSV strains, in contrast to the G protein, which shows approximately 50% genetic difference between RSV A and B strains [15].
Since 2022, pre-F protein-based RSV vaccines with high efficacy in older adults and pregnant women, have been reported [16,17,18,19]. A single dose of a protein-subunit vaccine or mRNA vaccine showed an efficacy of over 80% against RSV-related lower respiratory tract diseases in adults aged 60 years and above with an acceptable safety profile during one RSV season [16,17,18]. The efficacy of the vaccine against medically-attended severe RSV-related lower respiratory tract disease in infants younger than 90 and 180 days of age has been reported to be 81.8% and 69.5%, respectively [19]. Pre-F is mainly used as the target antigen for RSV vaccines, but some companies are also developing vaccines containing the G protein, nucleocapsid, and matrix proteins to enhance cell-mediated immunity. The advent of RSV vaccines is welcome news at a time when RSV is rampant again after its transient disappearance at the onset of the COVID-19 pandemic [20,21,22]. Therefore, there is an urgent need to establish a standardized vaccine immunogenicity evaluation method. The ELISA protocol (based on two pre-F antigens and G proteins) developed and validated in this study will be helpful in evaluating vaccines that are to be introduced in the near future.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, H.S.S., J.Y.S.; Methodology, A-Y.J., H.J.J., H.S.S., J.Y.S.; Investigation, E.N. A-Y.J., K.B.A., H.J.J., M-S.P., J-Y.B., H.S.S., J.Y.S.; Validation, A-Y.J., H.J.J.; Writing - original draft, E.N., A-Y.J., H.S.S., J.Y.S.; Writing - review & editing, K.B.A., H.J.J., M-S. P., J-Y.B., H.S.S., J.Y.S.; Supervision, H.S.S., J.Y.S.
Funding
This study was funded by the grant of the Ministry of Food and Drug Safety (21172MFDS179) of South Korea.
Institutional Review Board Statement
This study was approved by the Institutional Board of Review (of Korea University Guro Hospital (IRB No. 2022GR0149).
Informed Consent Statement
Informed consent was waived due to the retrospective nature of this study and expected minimal harm to the participants.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
None.
Conflicts of Interest
None.
References
- Shi, T.; McAllister, D.A.; O'Brien, K.L.; Simoes, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: A systematic review and modelling study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; Walsh, E.E. Respiratory syncytial virus infection in adults. Clin Microbiol Rev 2000, 13, 371–384. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.; Lui, G.C.; Wong, K.T.; Li, T.C.; Tse, E.C.; Chan, J.Y.; Yu, J.; Wong, S.S.; Choi, K.W.; Wong, R.Y.; et al. High morbidity and mortality in adults hospitalized for respiratory syncytial virus infections. Clin Infect Dis 2013, 57, 1069–1077. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.G.; Noh, J.Y.; Choi, W.S.; Park, J.J.; Suh, Y.B.; Song, J.Y.; Cheong, H.J.; Kim, W.J. Clinical characteristics and disease burden of respiratory syncytial virus infection among hospitalized adults. Scientific Reports 2020, 10, 12106. [Google Scholar] [CrossRef]
- WHO. RSV Vaccine Research and Development Technology Roadmap. Available online: https://www.who.int/publications/i/item/WHO-IVB-17.12 (accessed on 19 February 2023).
- PATH. RSV Vaccine and mAb Snapshot. Available online: https://www.path.org/resources/rsv-vaccine-and-mab-snapshot/ (accessed on 19 February 2023).
- Mejias, A.; Rodríguez-Fernández, R.; Oliva, S.; Peeples, M.E.; Ramilo, O. The journey to a respiratory syncytial virus vaccine. Ann Allergy Asthma Immunol 2020, 125, 36–46. [Google Scholar] [CrossRef]
- Swanson, K.A.; Settembre, E.C.; Shaw, C.A.; Dey, A.K.; Rappuoli, R.; Mandl, C.W.; Dormitzer, P.R.; Carfi, A. Structural basis for immunization with postfusion respiratory syncytial virus fusion F glycoprotein (RSV F) to elicit high neutralizing antibody titers. Proc Natl Acad Sci U S A 2011, 108, 9619–9624. [Google Scholar] [CrossRef] [PubMed]
- McLellan, J.S.; Chen, M.; Joyce, M.G.; Sastry, M.; Stewart-Jones, G.B.; Yang, Y.; Zhang, B.; Chen, L.; Srivatsan, S.; Zheng, A.; et al. Structure-based design of a fusion glycoprotein vaccine for respiratory syncytial virus. Science 2013, 342, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Krarup, A.; Truan, D.; Furmanova-Hollenstein, P.; Bogaert, L.; Bouchier, P.; Bisschop, I.J.M.; Widjojoatmodjo, M.N.; Zahn, R.; Schuitemaker, H.; McLellan, J.S.; et al. A highly stable prefusion RSV F vaccine derived from structural analysis of the fusion mechanism. Nat Commun 2015, 6, 8143. [Google Scholar] [CrossRef] [PubMed]
- Flynn, J.A.; Durr, E.; Swoyer, R.; Cejas, P.J.; Horton, M.S.; Galli, J.D.; Cosmi, S.A.; Espeseth, A.S.; Bett, A.J.; Zhang, L. Stability Characterization of a Vaccine Antigen Based on the Respiratory Syncytial Virus Fusion Glycoprotein. PLoS One 2016, 11, e0164789. [Google Scholar] [CrossRef] [PubMed]
- Jounai, N.; Yoshioka, M.; Tozuka, M.; Inoue, K.; Oka, T.; Miyaji, K.; Ishida, K.; Kawai, N.; Ikematsu, H.; Kawakami, C.; et al. Age-Specific Profiles of Antibody Responses against Respiratory Syncytial Virus Infection. EBioMedicine 2017, 16, 124–135. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, C.-A. 2 - Vaccine immunology. In Vaccines (Sixth Edition), Plotkin, S.A., Orenstein, W.A., Offit, P.A., Eds. W.B. Saunders: London, 2013; pp. 14-32. [CrossRef]
- Cullen, L.M.; Schmidt, M.R.; Torres, G.M.; Capoferri, A.A.; Morrison, T.G. Comparison of Immune Responses to Different Versions of VLP Associated Stabilized RSV Pre-Fusion F Protein. Vaccines (Basel) 2019, 7. [Google Scholar] [CrossRef]
- Nam, H.H.; Ison, M.G. Respiratory syncytial virus infection in adults. Bmj 2019, 366, l5021. [Google Scholar] [CrossRef]
- Papi, A.; Ison, M.G.; Langley, J.M.; Lee, D.G.; Leroux-Roels, I.; Martinon-Torres, F.; Schwarz, T.F.; van Zyl-Smit, R.N.; Campora, L.; Dezutter, N.; et al. Respiratory Syncytial Virus Prefusion F Protein Vaccine in Older Adults. N Engl J Med 2023, 388, 595–608. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.E.; Pérez Marc, G.; Zareba, A.M.; Falsey, A.R.; Jiang, Q.; Patton, M.; Polack, F.P.; Llapur, C.; Doreski, P.A.; Ilangovan, K.; et al. Efficacy and Safety of a Bivalent RSV Prefusion F Vaccine in Older Adults. N Engl J Med 2023. [Google Scholar] [CrossRef] [PubMed]
- Moderna. Moderna Announces MRNA-1345, An Investigational Respiratory Syncytial Virus (RSV) Vaccine, Has Met Primary Efficacy Endpoints in Phase 3 Trial IN Older Adults. Updated Jan 17, 2023. Available online: https://investors.modernatx.com/news/news-details/2023/Moderna-Announces-mRNA-1345-an-Investigational-Respiratory-Syncytial-Virus-RSV-Vaccine-Has-Met-Primary-Efficacy-Endpoints-in-Phase-3-Trial-in-Older-Adults/default.aspx.
- Kampmann, B.; Madhi, S.A.; Munjal, I.; Simões, E.A.F.; Pahud, B.A.; Llapur, C.; Baker, J.; Pérez Marc, G.; Radley, D.; Shittu, E.; et al. Bivalent Prefusion F Vaccine in Pregnancy to Prevent RSV Illness in Infants. N Engl J Med 2023. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Kim, H.Y.; Lee, M.; Ahn, J.G.; Baek, J.Y.; Kim, M.Y.; Huh, K.; Jung, J.; Kang, J.-M. Respiratory Syncytial Virus Outbreak Without Influenza in the Second Year of the Coronavirus Disease 2019 Pandemic: A National Sentinel Surveillance in Korea, 2021–2022 Season. J Korean Med Sci 2022, 37. [Google Scholar] [CrossRef] [PubMed]
- Ujiie, M.; Tsuzuki, S.; Nakamoto, T.; Iwamoto, N. Resurgence of Respiratory Syncytial Virus Infections during COVID-19 Pandemic, Tokyo, Japan. Emerg Infect Dis 2021, 27, 2969–2970. [Google Scholar] [CrossRef] [PubMed]
- ECDC. Risk of severe pressure on healthcare systems due to RSV, flu and COVID-19 co-circulation. 2022.
Figure 1.
Correlation between anti-DS-Cav1 IgG titers and anti-SC-TM IgG titers. (A) total population, (B) aged < 5 years, (C) aged 5–18 years, (D) aged 19–49 years, (E) aged 50–64 years, and (F) aged 65 years and above.
Figure 1.
Correlation between anti-DS-Cav1 IgG titers and anti-SC-TM IgG titers. (A) total population, (B) aged < 5 years, (C) aged 5–18 years, (D) aged 19–49 years, (E) aged 50–64 years, and (F) aged 65 years and above.
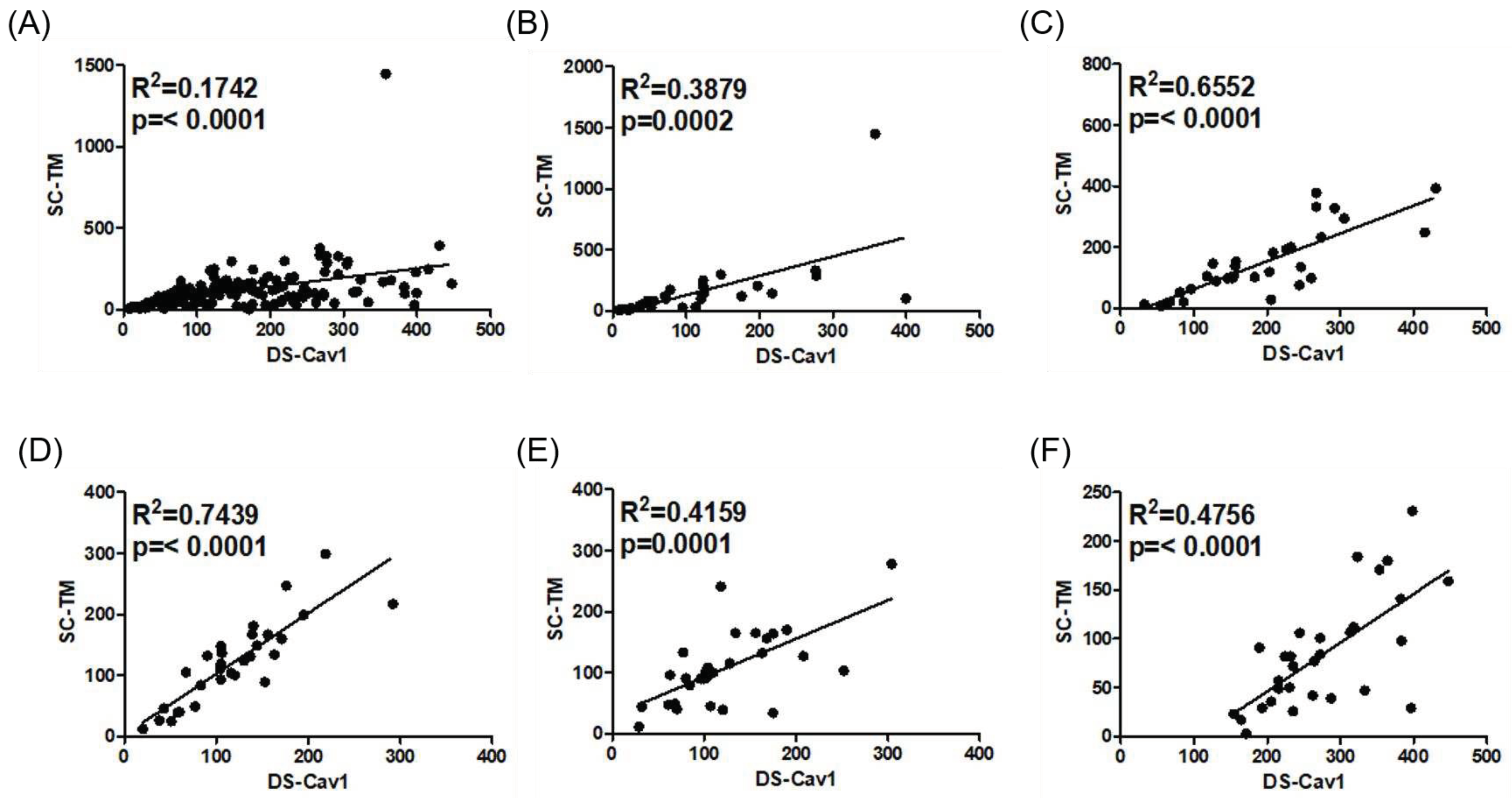
Figure 2.
Correlation between anti-DS-Cav1 IgG titers and anti-SC-TM IgG titers. (A) total population, (B) aged < 5 years, (C) aged 5–18 years, (D) aged 19–49 years, (E) aged 50–64 years, and (F) aged 65 years and above.
Figure 2.
Correlation between anti-DS-Cav1 IgG titers and anti-SC-TM IgG titers. (A) total population, (B) aged < 5 years, (C) aged 5–18 years, (D) aged 19–49 years, (E) aged 50–64 years, and (F) aged 65 years and above.
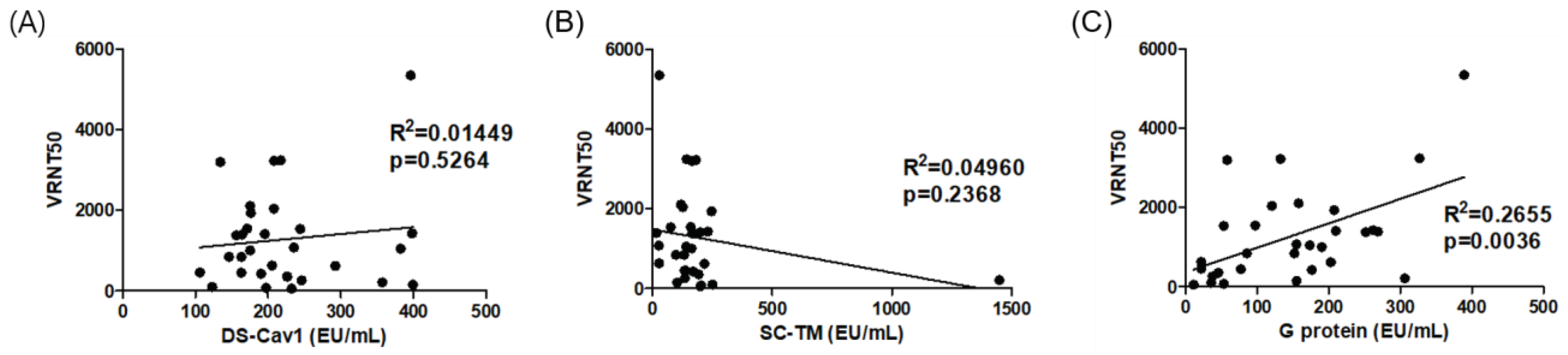

Table 1.
Accuracy (dilution linearity) of the respiratory syncytial virus (RSV) enzyme-linked immunosorbent assay (ELISA) protocol for IgG antibodies against prefusion F proteins (DS-Cav-1 and SC-TM) and G protein.
Table 1.
Accuracy (dilution linearity) of the respiratory syncytial virus (RSV) enzyme-linked immunosorbent assay (ELISA) protocol for IgG antibodies against prefusion F proteins (DS-Cav-1 and SC-TM) and G protein.
| DS-Cav1 (5 μg/ml) | |||||||
| Dilution factor | r2 | ||||||
| 1:200 | 1:400 | 1:800 | 1:1600 | 1:3200 | 1:6400 | ||
| Reference sera | 2.519 | 1.9658 | 1.4659 | 0.9846 | 0.7047 | 0.42405 | 0.9045 |
| Low titer sera | 2.2103 | 1.5678 | 1.0532 | 0.6568 | 0.46605 | 0.3265 | 0.9603 |
| Medium titer sera | 2.3991 | 1.70445 | 1.161 | 0.73195 | 0.4868 | 0.43985 | 0.9629 |
| High titer sera | 2.6452 | 2.1615 | 1.70685 | 1.21075 | 0.84935 | 0.56785 | 0.87 |
| SC-TM (2.5 μg/ml) | |||||||
| Dilution factor | R2 | ||||||
| 1:200 | 1:400 | 1:800 | 1:1600 | 1:3200 | 1:6400 | ||
| Reference sera | 2.83735 | 2.38555 | 1.8442 | 1.2892 | 0.85635 | 0.63475 | 0.8603 |
| Low titer sera | 2.34215 | 1.73725 | 1.2267 | 0.82085 | 0.4996 | 0.37665 | 0.9355 |
| Medium titer sera | 2.64995 | 2.1299 | 1.50995 | 1.037 | 0.66725 | 0.5086 | 0.9051 |
| High titer sera | 2.8413 | 2.41785 | 1.90155 | 1.34495 | 0.966 | 0.6745 | 0.8514 |
| G protein (5 μg/ml) | |||||||
| Dilution factor | R2 | ||||||
| 1:200 | 1:400 | 1:800 | 1:1600 | 1:3200 | 1:6400 | ||
| Reference sera | 1.01015 | 0.70585 | 0.4602 | 0.2764 | 0.16345 | 0.10335 | 0.9777 |
| Low titer sera | 1.14245 | 0.86765 | 0.6395 | 0.40675 | 0.2446 | 0.13945 | 0.9512 |
| Medium titer sera | 0.81455 | 0.5709 | 0.34935 | 0.2087 | 0.12385 | 0.0763 | 0.9797 |
| High titer sera | 0.97235 | 0.68775 | 0.44775 | 0.2775 | 0.1618 | 0.10215 | 0.9760 |
r2, coefficient of determination.
Table 2.
Inter-assay precision of the RSV ELISA protocol for IgG antibodies against prefusion F proteins (DS-Cav-1 and SC-TM) and G protein.
Table 2.
Inter-assay precision of the RSV ELISA protocol for IgG antibodies against prefusion F proteins (DS-Cav-1 and SC-TM) and G protein.
| Aged < 5 years | Aged 5–18 years | Aged 19–49 years | Aged 50–64 years | Aged ≥ 65 years | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Antigen | DF | OD (mean ± SD) |
CV (%) | OD (mean ± SD) |
CV (%) | OD (mean ± SD) |
CV (%) | OD (mean ± SD) |
CV (%) | OD (mean ± SD) |
CV (%) |
| DS-Cav1 | 1:200 | 1.105 ± 0.005 | 0.443 | 1.177 ± 0.020 | 1.685 | 1.230 ± 0.015 | 1.251 | 0.807 ± 0.012 | 1.505 | 1.187 ± 0.015 | 1.258 |
| 1:400 | 0.704 ± 0.009 | 1.218 | 0.894 ± 0.020 | 2.235 | 0.959 ± 0.012 | 1.247 | 0.542 ± 0.011 | 2.1 | 0.897 ± 0.021 | 2.291 | |
| 1:800 | 0.454 ± 0.010 | 2.196 | 0.690 ± 0.010 | 1.498 | 0.724 ± 0.009 | 1.223 | 0.353 ± 0.008 | 2.206 | 0.671 ± 0.014 | 2.016 | |
| 1:1600 | 0.278 ± 0.002 | 0.864 | 0.478 ± 0.012 | 2.567 | 0.514 ± 0.014 | 2.811 | 0.220 ± 0.005 | 2.241 | 0.502 ± 0.016 | 3.137 | |
| 1:3200 | 0.169 ± 0.004 | 2.623 | 0.317 ± 0.010 | 3.106 | 0.347 ± 0.012 | 3.548 | 0.138 ± 0.002 | 1.805 | 0.360 ± 0.005 | 1.414 | |
| 1:6400 | 0.108 ±0.003 | 3.046 | 0.200 ± 0.006 | 3.129 | 0.228 ± 0.007 | 2.892 | 0.090 ± 0.003 | 2.933 | 0.243 ± 0.006 | 2.506 | |
| 1:12800 | 0.072 ± 0.002 | 2.749 | 0.125 ± 0.005 | 3.881 | 0.145 ± 0.008 | 5.202 | 0.063 ± 0.002 | 3.014 | 0.159 ± 0.006 | 3.559 | |
| 1:25600 | 0.058 ± 0.002 | 3.354 | 0.088 ± 0.004 | 4.634 | 0.103 ± 0.005 | 4.526 | 0.052 ± 0.003 | 6.283 | 0.109 ± 0.004 | 3.751 | |
| SC-TM | 1:200 | 1.167 ± 0.011 | 0.982 | 1.343 ± 0.008 | 0.571 | 1.298 ± 0.027 | 2.069 | 0.962 ± 0.012 | 1.296 | 0.779 ± 0.012 | 1.567 |
| 1:400 | 0.731 ± 0.021 | 2.877 | 1.088 ± 0.014 | 1.259 | 0.983 ± 0.019 | 1.938 | 0.666 ± 0.006 | 0.918 | 0.439 ± 0.011 | 2.484 | |
| 1:800 | 0.484 ± 0.006 | 1.304 | 0.870 ± 0.020 | 2.276 | 0.728 ± 0.020 | 2.747 | 0.449 ± 0.005 | 1.004 | 0.288 ± 0.005 | 1.670 | |
| 1:1600 | 0.304 ± 0.009 | 2.857 | 0.644 ± 0.010 | 1.604 | 0.530 ± 0.008 | 1.585 | 0.291 ± 0.009 | 3.104 | 0.185 ± 0.006 | 3.237 | |
| 1:3200 | 0.188 ± 0.005 | 2.417 | 0.430 ± 0.013 | 2.980 | 0.353 ± 0.008 | 2.318 | 0.185 ± 0.007 | 3.829 | 0.121 ± 0.001 | 1.030 | |
| 1:6400 | 0.120 ± 0.007 | 6.035 | 0.273 ± 0.006 | 2.282 | 0.236 ± 0.003 | 1.061 | 0.117 ± 0.005 | 4.240 | 0.083 ± 0.001 | 1.438 | |
| 1:12800 | 0.080 ± 0.004 | 4.865 | 0.166 ± 0.006 | 3.481 | 0.151 ± 0.004 | 2.600 | 0.081 ± 0.005 | 5.856 | 0.062 ± 0.001 | 2.237 | |
| 1:25600 | 0.061 ± 0.003 | 5.454 | 0.111 ± 0.003 | 2.761 | 0.105 ± 0.003 | 3.007 | 0.062 ± 0.007 | 10.717 | 0.052 ± 0.002 | 3.524 | |
| G protein | 1:200 | 0.657 ± 0.020 | 2.987 | 0.199 ± 0.016 | 8.001 | 0.964 ± 0.032 | 3.355 | 0.746 ± 0.031 | 4.172 | 1.490 ± 0.028 | 1.904 |
| 1:400 | 0.394 ± 0.010 | 2.508 | 0.107 ± 0.010 | 9.189 | 0.600 ± 0.023 | 3.852 | 0.434 ± 0.002 | 5.154 | 1.262 ± 0.038 | 2.985 | |
| 1:800 | 0.236 ± 0.008 | 3.227 | 0.071 ± 0.007 | 9.943 | 0.430 ± 0.015 | 3.424 | 0.285 ± 0.025 | 8.754 | 1.036 ± 0.044 | 4.230 | |
| 1:1600 | 0.136 ± 0.003 | 2.274 | 0.050 ± 0.003 | 6.295 | 0.267 ± 0.009 | 3.284 | 0.170 ± 0.014 | 8.251 | 0.821 ± 0.046 | 5.596 | |
| 1:3200 | 0.086 ± 0.005 | 6.356 | 0.039 ± 0.001 | 2.807 | 0.156 ± 0.006 | 4.006 | 0.105 ± 0.008 | 8.026 | 0.579 ± 0.038 | 6.544 | |
| 1:6400 | 0.061 ± 0.003 | 4.572 | 0.035 ± 0.001 | 2.674 | 0.098 ± 0.002 | 2.385 | 0.069 ± 0.004 | 5.475 | 0.363 ± 0.034 | 9.427 | |
| 1:12800 | 0.051 ± 0.006 | 11.501 | 0.033 ± 0.001 | 2.646 | 0.065 ± 0.002 | 2.849 | 0.049 ± 0.002 | 3.124 | 0.219 ± 0.020 | 8.971 | |
| 1:25600 | 0.041 ± 0.002 | 5.743 | 0.034 ± 0.001 | 2.795 | 0.047 ± 0.002 | 3.347 | 0.040 ± 0.001 | 3.521 | 0.134 ± 0.012 | 9.003 | |
DF, dilution factor; OD, optical density; SD, standard deviation; CV, coefficient of variation.
Table 3.
Specificity of the RSV ELISA protocol after adsorption with homologous and heterologous proteins.
Table 3.
Specificity of the RSV ELISA protocol after adsorption with homologous and heterologous proteins.
| Coated protein | DS-Cav1 | SC-TM | G protein | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Inhibitor (10 μg/mL) |
None | DS-Cav1 | SC-TM | G protein | None | DS-Cav1 | SC-TM | G protein | None | DS-Cav1 | SC-TM | G protein | |
| Aged < 5 years | EU/ml | 115.0 | 83.3 | 78.2 | 122.9 | 153.3 | 35.8 | 30.8 | 113.7 | 117.3 | 53.5 | 49.2 | 22.4 |
| % | - | 72.5 | 68.0 | 106.9 | - | 23.3 | 20.1 | 74.2 | - | 45.6 | 42.0 | 19.1 | |
| Aged 5–18 years | EU/ml | 193.8 | 73.0 | 67.3 | 121.6 | 148.4 | 69.3 | 65.7 | 122.5 | 78.8 | 44.1 | 41.9 | 17.3 |
| % | - | 37.7 | 34.7 | 62.8 | - | 46.7 | 44.2 | 82.5 | - | 56.0 | 53.2 | 22.0 | |
| Aged 19–49 years | EU/ml | 118.8 | 45.2 | 60.5 | 114.0 | 121.1 | 73.4 | 60.6 | 130.7 | 101.9 | 89.0 | 77.3 | 28.2 |
| % | - | 38.1 | 51.0 | 96.0 | - | 60.6 | 50.0 | 108.0 | - | 87.4 | 75.9 | 27.6 | |
| Aged 50–64 years | EU/ml | 122.7 | 65.7 | 84.0 | 107.7 | 107.0 | 88.0 | 61.1 | 120.4 | 134.3 | 145.8 | 132.1 | 42.3 |
| % | - | 53.5 | 68.5 | 87.8 | - | 82.3 | 57.1 | 112.6 | - | 108.6 | 98.4 | 31.5 | |
| Aged ≥ 65 years | EU/ml | 113.7 | 62.2 | 75.6 | 127.2 | 84.1 | 71.4 | 43.5 | 95.2 | 165.8 | 172.4 | 157.0 | 36.1 |
| % | - | 54.7 | 66.5 | 111.9 | - | 84.8 | 51.8 | 113.2 | - | 104.0 | 94.7 | 21.8 | |
| Average | EU/ml | 132.8 | 65.9 | 73.1 | 118.7 | 122.8 | 67.6 | 52.3 | 116.5 | 119.6 | 101.0 | 91.5 | 29.3 |
| % | - | 49.6 | 55.1 | 89.4 | - | 55.0 | 42.6 | 94.9 | - | 84.4 | 76.5 | 24.5 | |
EU, ELISA unit.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



