
Submitted:
23 June 2023
Posted:
25 June 2023
You are already at the latest version
Abstract
Surface chemistry evaluation plays a crucial role in assessing the efficacy of chemical decontamination products for titanium implants. This study aimed to investigate the effectiveness of chemical decontamination solutions in cleaning a contaminated dental implant surface and to evaluate the potential of combining Pluronic gel with hydrogen peroxide (NuBone®Clean) by evaluating pellicle disruption and re-formation on implant surfaces. In addition, ensuring safety with in- vitro and human testing protocols. X-ray Photoelectron Spectroscopy (XPS) was utilized for surface analysis. All the tested gels had some effect on the surface cleanness except for PrefGel®. Among the tested chemical decontamination candidates, NuBone®Clean demonstrated effectiveness in providing a cleaner titanium surface. Furthermore, none of the tested chemical agents exhibited any cytotoxic effects, and the safety assessment showed no adverse events. The results of this study highlight the significance of conducting comprehensive evaluations, encompassing safety and efficacy, before introducing new chemical agents for dental treatments. The findings suggest that NuBone®Clean shows potential as a chemical decontamination solution for implant surfaces. However, further investigation through randomized clinical trials is necessary. By adhering to rigorous testing protocols, the development of safe and efficient chemical decontamination strategies can be advanced, benefiting patients and promoting progress in the field of implant dentistry.
Keywords:
dental implant
; acquired pellicle
; peri-implant disease
; chemical decontamination
1. Introduction
Infections associated with implants represent a worldwide health concern [1]. With the ongoing demographic shift toward an ageing population [2], the prevalence of devices such as dental, hip, and knee prostheses, joint replacements, and screws used to substitute or reinforce deteriorating bone structures is increasing. A significant challenge associated with these applications is bacterial colonisation, either during the surgical procedure or after being in function.
The surgical implantation exposes these devices to potential bacterial colonisation, originating from the patient's skin, healthcare staff, or surgical tools [3]. Once the bacteria adhere to the implant's surface, they can establish a stronghold over time, producing a viscous layer known as a biofilm [4]. This self-secreted barrier protects against the host's immune response and antibiotic treatments, contributing to the rise in antibiotic resistance [5]. In cases where the body's immune system or antibiotic treatment fails to eradicate the infection, further corrective surgeries are necessary [6], including a cleaning process of the implant. In some cases removing the implant is imperative [7].
An illustration of bacterial colonization occurring after the implant has been in use is evident in peri-implant diseases, which affect dental implants [8]. These are biofilm-driven diseases involving multiple species of microorganisms [9]. The initial step in biofilm formation on a dental implant surface is establishing a pellicle layer, providing a foundation for bacterial attachment and subsequent biofilm development [10]. Within seconds after cleaning the implant components above the bone level, an acquired pellicle forms on the exposed implant surface in the oral cavity. Bacterial adhesion and biofilm development depend on the composition and adhesion strength of the proteins adhering to the surface [11]. These proteins exhibit diversity in composition and adhesion strength, which can be influenced by numerous factors, including the surface chemistry of the material [12].
Managing peri-implant diseases poses significant challenges due to the lack of remedies specifically designed for treating the dental implant surface [13]. Titanium is the leading material for dental implants [14]; any treatment of this surface will affect the state of the surface on macroscopic, microscopic and chemical level. The aim of this study was to evaluate various chemical decontamination solutions, with evaluation of a detailed chemical characterisation of the titanium surface after using the cleaning agents. One of the remedies in this study, consisting of Pluronic and H2O2, has not yet been clinically used, this study includes the assessment of safety of this remedy through in vitro cell testing and clinical assessment. This comprehensive evaluation will allow us to understand better the cleaning agent's effects on the titanium surface and potentially pave the way for more effective treatments for peri-implantitis.
2. Materials and Methods
2.1. Preparation of titanium discs and decontamination groups
Commercially pure titanium discs, measuring 6.2 mm in diameter and 2 mm in height, were subjected to grit-blasting and acid etching in a hydrofluoric acid solution (0.2 vol.%) to replicate the rough surface characteristics of a dental implant surface, precisely resembling the OsseoSpeed® surface commercially available from Dentsply Sirona (Zürich, CH). The surface treatment protocol followed established procedures described by Lamolle et al. [15]. To ensure uniformity, all surfaces were analysed with a PLμ NEOX (Sensofar-Tech S.L., Terrassa, Spain) blue light laser profilometer and interferometer using a 50 × EPI (Nikon, Tokyo, Japan) confocal objective was used for assessing an extended topography of 2 × 2 images. Each had a viewing area of 253 μm × 190 μm at 20% overlapping. Eight images of each material were analyzed. The advanced topography software Sensomap 5.1 Plus (Sensofar-Tech S.L., Terrassa, Spain) for dimensional and surface state metrology was used to process the measured data. The following surface amplitude parameters were analyzed to ensure homogenous surfaces: average roughness (Sa), total height of the surface (St), skewness of the height distribution (Ssk), kurtosis of the height distribution (Sku) and the maximum height of summits (Sp).
Six decontamination groups were evaluated (Table 1): PrefGel® (Institut Straumann AG, Basel, Switzerland), Perisolv® (Regedent AG, Zurich, Switzerland, 3 % vol H2O2 (Sigma-Aldrich, Norway), Pluronic gel (Sigma-Aldrich, Norway), NuBone®Clean, (Corticalis AS, Oslo, Norway), and GUM® Paroex® (0.12% Chlorhexidine gluconate and 0.05 % Cetylpyridinium chloride, Sunstar Suisse, Etoy, Switzerland ).
2.2. Dental pellicle model – Pellicle formation and decontamination
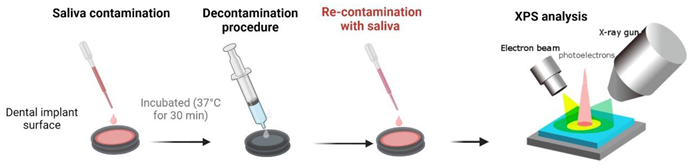
Saliva samples were collected from three healthy individuals, pooled together, and subjected to centrifugation. The prepared titanium discs were placed in 24-well plates (ThermoFisher, Waltham, US), and the pooled saliva was applied onto the disc surfaces. Following application, the discs were incubated at 37 °C for 30 minutes to facilitate the formation of a pellicle layer on the surface. It is important to note that the pellicle was not sterilised, although the presence of bacteria within it was not assessed in this study. To ensure the robustness of the experimental design, three discs were contaminated at three different time points for each decontamination group (n=9). Two sets of discs were utilised for each sample in this study phase. One set was decontaminated and subsequently analysed, while the other set was first decontaminated and then re-contaminated with the pooled saliva before analysis after re-contamination (Figure 1). The analysis methods employed were consistent for both groups of discs to assess the propensity for pellicle formation on the surface following decontamination. Discs with no treatment (pellicle formation) were employed as negative controls, while discs without pellicles were positive controls.
2.3. X-ray photoelectron spectroscopy (XPS) – analysis of chemical surface composition
The XPS analysis was conducted on an Axis UltraDLD XP spectrometer (Kratos Analytical Limited, Manchester, United Kingdom). The emission of the photoelectrons from the sample was 90° (normal to the sample surface), and the incidence angle of the X-rays was 33.3° (or 56.7° between the X-ray incidence direction and captured photoelectron emission direction). A hybrid lens mode was used with a slot aperture (analysis area of 700 x 300 µm2). Survey spectra were acquired with 80 eV pass energy between 0 eV and 1100 eV binding energy (BE), and detail spectra were recorded for O 1s, C 1s, Ti 2p, and N 1s with 40 eV pass energy. The instrument resolution was 1.1 eV for the survey scans and 0.71 eV for the detail scans for the employed settings, determined by measuring the full width at half maximum FWHM of the Ag 3d5/2 peak obtained on sputter-cleaned silver foil.
The samples were mounted on an insulating support, and low energy electrons applied for charge compensation; this combination mitigates differential charging effects due to potential insulating surface layers. Charge referencing of the spectra was based on the position of the C 1s peak attributed to aliphatic C-C/C-H bonds, set to 284.8 eV BE.
2.4. Cell culture and cytotoxicity assay
ISO 10993-5:2009 outlines the test procedures for evaluating the in vitro cytotoxicity of medical devices. It involves incubating cultured cells with a device or extracts from a device by direct contact or diffusion. In this study, a murine calvaria-derived preosteoblast cell line, MC3T3-E1 (ATCC, Manassas, VA, USA), was used to investigate the cytotoxicity of the gels. Cells were cultured in MEM alpha (A10490-01; Gibco, Waltham, MA, USA) supplemented with 15% fetal bovine serum (10270-106, Gibco), 100 U/mL penicillin and 100 µg/mL streptomycin (15140-122; Gibco) in a humidified atmosphere of 5 % CO2 at 37°C. Cells were seeded at a density of 3 x 104 cells/cm2 in culture-treated plates and allowed to settle for 48 h before treatment. To investigate the cytotoxic effects of the gels, the 1 mL gels were allowed to solidify for 10 min before an equal amount of culture medium (1 mL) was added for 24 h. The conditioned media was added to the cells. After 24 h, 50 μL media was collected, and 2% Triton X-100 (2840; J. T. Baker, Phillipsburg, NJ, USA) was added to the cells for one h to ensure optimal LDH release. Cells not exposed to Triton X-100 had the media exchanged with a new conditioned medium for an additional 24 h, after which 50 μL media was collected, and cells exposed to Triton X-100 for one h. Cells exposed to a culture medium were used as a negative control. Following the manufacturer's description, cytotoxicity was evaluated using a lactate dehydrogenase (LDH) activity kit (11644793001; Roche, Basel, Switzerland). In short, 50 μL of the collected media was mixed with 50 μL of the reaction mixture and incubated at room temperature in the dark for 30 min. The absorbance was measured at 490 nm using BioTek ELx800 Absorbance Microplate Reader (BioTek Instruments, Inc., Vermont, USA). LDH activity was measured after 24 h and 48 h. The LDH activity was compared in each well before and after Triton X-100 to evaluate the normal LDH release compared to optimal release from dead cells.
2.5. Clinical safety assessment
Pre-operative: Twelve patients were recruited to participate in the safety assessment study with an open non-comparative case series design. The Regional ethics committee approved the study, REK Sør-Øst (348696), The Norwegian Medicines Agency, NOMA (21/23242-27), and the Norwegian Centre for Research Data (NSD) approved the data handling. The ethics committee did not permit a comparison of different decontamination gels until NuBone® Clean demonstrated no adverse reactions. Consequently, no comparison was made among the different products.
Patients were included if they met the following criteria:
- Good general health
- Between 18 and 65 years of age
- Healthy oral tissues.
- At least 10 remaining teeth and/or fixed implants.
- No active oral pathologies.
- Signed Informed Consent was obtained before the start.
- Psychological appropriateness.
- Consent to complete follow-up interview.
- Patients were excluded if they met any of the following conditions:
- Not optimal general health condition
- Abscess or infection anywhere in the body at the time of study entry.
- Current pregnancy or nursing.
- Patients were excluded if they met any of the following conditions:
- Not optimal general health condition
- Abscess or infection anywhere in the body at the time of study entry.
- Current pregnancy or nursing.
- Any condition or current treatment for any condition, which in the opinion of the investigator and/or consulting physician, may constitute an unwarranted risk.
- Presence of psychological characteristics such as inappropriate attitude or motivation which, in the opinion of the investigator, are incompatible with the risks involved with the cleaning procedure and the prosthesis.
- Unwillingness to undergo a post-procedure interview.
- If, in the medical opinion of the dental professional, conditions are such that dental cleaning is deemed unsuitable for the patient.
- Intake of Non-Steroidal Anti-Inflammatory Drugs (NSAID), pain-killers or antibiotics one week before and three days after the procedure.
Two investigators conducted the safety study. One principal investigator and one clinical investigator. Preoperatively, the principal investigator provided the study candidate with comprehensive information regarding the study and presented the informed consent form, which occurred at least one week prior to the initiation of the study. In addition, the clinical investigator reviewed the signed patient information form with the patient during the pre-operative consultation to ensure that the patient understood the content and complied with the instructions.
The Pre-operative Patient History Record (CRF-1) recorded routine clinical examinations and information. The patient and study numbers were given on all Case Report Forms. An identification log was kept at the clinic. The gel in the syringe and the liquid in the vial were mixed according to the instruction. The activated cleaning gel was then applied onto the surfaces of teeth and implants to be cleaned. The gel was applied for 1 min during cleaning before removal by suction accompanied with air and water spray. Patient satisfaction and function were scored in a designated form during the postoperative follow-up interviews. Clinical assessment was done immediately after the procedure and two days after the procedure.
2.6. Statistics
Data are presented as mean with standard deviation. The groups were statistically compared using the One-Way and Two-Way ANOVA analysis parametrical test with Tukey's multiple comparison test. A probability of less than or equal to 0.05 was considered significant. All data obtained were analysed using GraphPad Prism software version 9.5 (GRAPH PAD software Inc, California, USA). All graphical representations were performed on GraphPad Prism and Biorender.
3. Results
3.1. XPS
XPS provided a detailed surface chemistry analysis on atomic level measurement both on the element and its chemical state after pellicle removal (Table 2) and re-establishment of pellicle on the dental implant surface (Table 3).
After decontamination, the carbon content was highest for PrefGel® (61.9±1.9) and Perisolv® (62.2±8.8). Individually, H2O2 and Pluronic® had distinct impacts on carbon levels, resulting in values of 50.0±2.8 and 56.5±4.0, respectively. Their combination exhibited a synergistic effect, as demonstrated by the results obtained with NuBone®Clean (38.8±1.9), giving the lowest carbon content (Table 2). After re-contamination with saliva (Table 3), H2O2 (47.6±3.3) and NuBone®Clean (48.2±2.2) had the lowest carbon content. Perisolv® had a lower carbon content after re-contamination (49.7±4.5), than after decontamination (Table 2 and Table 3).
The lowest nitrogen level was found for NuBone®Clean (2.2±0.1) after decontamination. After re-contamination none of the groups had significantly lower nitrogen content than the uncleaned control (Table 3).
The highest amount of oxygen was found on NuBone®Clean, both after decontamination (43.4±1.0) and re-contamination (33.7±1.9). Perisolv® did show a higher value after re-contamination (33.6±3.7) compared to decontamination (28.6±2.2).
Traces of silicon were found after decontamination. Other trace elements such as phosphorous, sulphur, chlorine and potassium were found in some of the groups (Table 2 and Table 3). Calcium was found elevated for NuBone®Clean and H2O2. PrefGel had the lowest calcium levels (Table 2 and Table 3). Calcium was elevated for Perisolv® after re-contamination (Table 3).
Titanium content was highest for NuBone®Clean, both after decontamination (7.9±2.2) and after re-contamination (3.6±0.9). Perisolv® did show a higher titanium content after re-contamination (2.3±1.8), than after decontamination (3.0±0.4). Table 2 and Table 3.

Table 2.
Element quantification of titanium surfaces after pellicle removal with the decontamination products (n=3), *p<0.05 versus an untreated titanium surface (i.e. surface with pellicle).
Table 2.
Element quantification of titanium surfaces after pellicle removal with the decontamination products (n=3), *p<0.05 versus an untreated titanium surface (i.e. surface with pellicle).
 |
||||||
|---|---|---|---|---|---|---|
| Elemental analysis after decontamination (atomic % ± standard deviation) | ||||||
| Element | PrefGel | Perisolv | H2O2 | Pluronic | NuBoneClean | GumPareox |
| C 1s % | 61.9±1.9 | 62.2±8.8 | 50.0±2.8* | 56.5±4.0* | 38.8±1.9* | 56.0±1.7* |
| N 1s % | 10.0±0.7 | 5.1±3.7 | 8.5±0.5 | 7.2±2.1 | 2.2±0.1* | 8.7±0.0 |
| O 1s % | 26.1±1.6* | 28.6±2.2* | 32.3±1.8 * | 30.0±1.0*,b | 43.4±1.0*b | 28.1±1.4* |
| Na 1s % | 0.9±1.3 | 0.0±0.0 | 0.0±0.0 | 0.0±0.0 | 0.0±0.0 | 0.0±0.0 |
| Si 2p % | 0.9±0.5 | 0.1±0.1, | 0.5±0.2 | 0.4±0.3 | 0.7±0.0 | 0.1±0.1 |
| P 2p % | 0.0±0.0 | 0.5±0.4 | 1.0±0.3 | 0.4±0.2 | 1.7±0.4 | 0.5±0.1 |
| S 2p % | 0.0±0.0 | 0.0±0.0 | 0.2±0.1 | 0.1±0.0 | 0.0±0.0 | 0.1±0.1 |
| Cl 2p % | 0.0±0.0 | 0.6±0.0 | 0.4±0.3 | 0.0±0.0 | 0.0±0.0 | 0.1±0.0 |
| K 2p % | 0.0±0.0 | 0.0±0.0 | 0.1±0.1 | 0.0±0.0 | 0.0±0.0 | 0.0±0.0 |
| Ca 2p % | 0.0±0.0 | 1.2±0.9 | 2.6±0.5* | 1.2±0.1 | 4.6±0.7* | 1.0±0.1 |
| Ti 2p % | 0.0±0.1 | 2.3±1.8 | 4.6±1.4* | 4.1±1.4* | 7.9±2.2* | 5.3±0.6* |
Table 3.
Element quantification of titanium surfaces after re-exposure to pellicle after applying decontamination products (n=3), x p<0.05 versus titanium surface untreated titanium surface (i.e. surface with pellicle).
Table 3.
Element quantification of titanium surfaces after re-exposure to pellicle after applying decontamination products (n=3), x p<0.05 versus titanium surface untreated titanium surface (i.e. surface with pellicle).
 | ||||||
|---|---|---|---|---|---|---|
| Elemental analysis after both decontamination and re-contaminations with saliva (atomic % ± standard deviation) | ||||||
| Element | PrefGel | Perisolv | H2O2 | Pluronic | NuBoneClean | GumPareox |
| C 1s % | 63.4±2.2 | 49.7±4.5* | 47.6±3.3* | 60.8±9.2 | 48.2±2.2* | 57.7±2.1* |
| N 1s % | 10.8±0.4 | 7.4±1.1 | 8.6±1.3 | 4.9±3.7 | 8.4±0.5 | 10.2±0.2 |
| O 1s % | 24.6±1.4* | 33.6±3.7* | 33.4±2.3* | 29.7±3.1* | 33.7±1.9* | 26.4±1.2* |
| Na 1s % | 0.0±0.0 | 0.0±0.0 | 0.0±0.0 | 0.0±0.0 | 0.0±0.0 | 0.0±0.0 |
| Si 2p % | 0.1±0.2 | 0.4±0.2 | 0.2±0.2 | 0.2±0.2 | 0.1±0.2 | 0.0±0.0 |
| P 2p % | 0.1±0.1 | 1.3±0.2* | 1.6±0.7 | 0.6±0.4 | 1.7±0.4 | 0.7±0.2 |
| S 2p % | 0.0±0.0 | 0.0±0.0 | 0.2±0.1 | 0.0±0.0 | 0.1±0.1 | 0.1±0.1 |
| Cl 2p % | 0.2±0.1 | 0.3±0.3 | 0.4±0.2 | 0.0±0.0 | 0.0±0.0 | 0.1±0.0 |
| K 2p % | 0.1±0.1 | 0.4±±0.2 | 0.6±0.6 | 0.0±0.0 | 0.0±0.0 | 0.0±0.0 |
| Ca 2p % | 0.1±0.1 | 3.0±0.4* | 2.8±0.9* | 1.2±0.6 | 3.6±0.9* | 1.7±0.4 |
| Ti 2p % | 0.5±0.6 | 3.8±2.0* | 4.7±0.3* | 2.5±1.3 | 4.1±1.4* | 3.0±0.7 |
Table 4.
Quantification of surface elements for the controls, titanium surfaces with and without pellicle (n=3).
Table 4.
Quantification of surface elements for the controls, titanium surfaces with and without pellicle (n=3).
| Controls (at % ± SD) | ||
|---|---|---|
| Element | Without Pellicle | With Pellicle |
| C 1s % | 32.1±0.5 | 73.4±3.3 |
| N 1s % | 0.9±0.1 | 6.1±0.8 |
| O 1s % | 47.6±0.5 | 17.1±1.8 |
| Na 1s % | 0.0±0.0 | 0.0±0.0 |
| Si 2p % | 0.2±0.2 | 0.0±0.0 |
| P 2p % | 0.2±0.2 | 0.4±0.1 |
| S 2p % | 0.0±0.0 | 0.4±0.1 |
| Cl 2p % | 0.1±0.2 | 0.1±0.0 |
| K 2p % | 0.0±0.1 | 2.2±0.6 |
| Ca 2p % | 0.0±0.1 | 0.1±0.1 |
| Ti 2p % | 18.7±0.3 | 0.0±0.0 |
Figure 2 shows XPS high-resolution spectra of Oxygen (O 1s) (A-B), Carbon (C 1s) (C-D), and Titanium (Ti 2p) (E-F), where the left panel are titanium surfaces after pellicle decontamination, and the right panel are titanium surfaces after re-contamination.
After decontamination, the clean control and NuBone®Clean exhibited prominent peaks at 529.7 eV BE (Figure 2 A), this peak corresponds to O2-in the TiO2 [16,17]. The other groups exhibited this peak to a smaller extent. Peak at 531.1 eV BE was prominent for PrefGel® after decontamination and can be attributed carbon oxides (-CO3) [18], this peak is visible for the different groups to a smaller extent.
After re-contamination, the peak at 529.7 was lower for NuBone®Clean than after decontamination. And still prominent for the clean control. The peak representing carbon dioxides was lower in the re-contamination for PrefGel® and similar to the other groups (Figure 2B). A peak at 532.4 was prominent for H2O2 after re-contamination, representing hydroxyl [16] or surface active oxygen in O-C groups [19]. Peaks at 531.2 for multiple groups (GumParoex®, NuBone®Clean and PrefGel®) can be attributed to C-Ti-O [20] or –OH [21].
After decontamination (Figure 2C), 284.7 to 285.2 peaks representing C-C and C-H bonds [21] were seen in all groups except the clean surface. The clean surface peaked at 284.3, which can be attributed to the C-C bond. It can be hard to differentiate C-H and C-C bonds [20]. A peak at 286.2 prominent in the NuBone®Clean group can be attributed to C-O [20]. A peak of 288 was prominent in PrefGel® and visible in all groups except for positive control, attributed to C=O [20].
After re-contamination, peaks of 284.7 to 285.2 represents C-C and C-H bonds, consistent with the findings during decontamination. A shoulder of 286.2 is more prominent for PrefGel® after re-contamination. A 288 (C=O) peak is still prominent in PrefGel® after re-contamination. Figure 2D. The controls without a pellicle exhibited the most distinct titanium 2P 3/2 and 2P ½ peaks, measured at Binding Energies (B.E) of 458.4 and 464.1, respectively [22]. The intensity of these peaks decreased with the presence of a pellicle (Figure 2E,F). In re-contamination we also see a peak at 459.1, for H2O2, attributed to TiO2; some authors attribute this to Ti-SI bonds [23].
Figure 3 shows the XPS high-resolution spectra of calcium (Ca 2p) (A-B), chlorine (Cl 2p) (C-D), and sodium (Na 1s) (E-F). Again the left panel are titanium surface after pellicle decontamination, and the right panel are titanium surface after re-contamination with pellicle. Some calcium peaks were visible for Perisolv®, H2O2, Pluronic®, GumParoex® and NuBone®Clean, whereas no Ca signal was detected from PrefGel® and the controls (Figure 3A,B). The chlorine content was too low to yield clear peaks (Figure 3C,D). Some sodium level was found for PrefGel® in both steps and for Perisolv® after decontamination (Figure 3E,F).
Figure 4 shows the quantification of C-C/C-H, O-C=O and C-O-C/C-OH, calculated from all samples of each group. For C-C/C-H state of carbon shown in Figure 4A, the highest amount was found for Perisolv® after decontamination (56±0.23). All the other groups are significantly lower than the negative control after decontamination and re-contamination. However, both of the controls have a high atomic %.
For O-C=O, NuBone®Clean was statistically significantly different from the negative control (Figure 4B) after decontamination.
C-O-C/C-OH elements were closest for NuBone®Clean to the clean control; however, the negative control also has a low value, similar to the positive control. Perisolv®, PrefGel® showed high values of these bonds. After re-contamination Pluronic® was significantly higher than the unclean control (Figure 4C).
Figure 5 shows the C=O/O-C-O and O=C-OH bonds. No significant difference was found for O=C-OH bonds (Figure 5B); for the C=O/O-C-O, differences were detected for PrefGel®, H2O2 and GumParoex® from the unclean surface. However, all mean values were above the negative controls and far from the positive controls. Perisolv® had a low value after decontamination.
3.2. Cytotoxicity
None of the tested chemical decontamination agents showed cytotoxic behaviour according to ISO 10993-5:2009 (Figure 6); however, the cytotoxic response was highest for Perisolv®, Pluronic® and GumPaerox® after 24 hrs. H2O2 and PrefGel® had the lowest LDH value. All LDH values decreased from 24 to 48 hours of exposure.
3.3. Clinical safety assessment
All 12 patients included complied with the study protocol. No signs of complications were observed during the clinical procedure, and none of the patients reported any symptoms or discomfort during the study period (Figure 8). NuBone®Clean foams, when applied (Figure 8B), were easily removed with water and air spray in combination with suction. The gingiva had normal colour upon control (Figure 8C) for all patients.
All patients reported being satisfied with the clinical procedure and had no complaints about the product. Eleven out of 12 patients gave a score of 10. One patient gave a score of 5. The mean score was 9.6, whereas the median score was 10 (Table 5).
4. Discussion
Titanium has become the material of choice for bone implants [14]. Although titanium implants have demonstrated impressive success rates in osseointegration [24,25], biofilm-induced infections remain a significant concern in implantology, especially for dental implants. Unlike orthopaedic implants, dental implants are exposed to the oral cavity, which harbours a diverse population of microorganisms capable of adhering to the implant surface. The problem arises when biofilm develops on the implant surface, which interacts with the host immune system and ultimately results in bone loss and implant failure [26]. Therefore, when cleaning a dental implant surface, the goal is to achieve a clean surface that does not attract bacterial cells while simultaneously promoting the attachment of cells crucial for peri-implant tissue regeneration [7].
The initial layer, the acquired pellicle, is crucial for biofilm formation. After cleaning implant components above the bone level, an acquired pellicle is rapidly formed on the implant surface in the oral cavity [10]. The surface chemistry of the implants significantly influences the interaction between titanium implants and the surrounding biological environment [27]. Therefore, it is crucial to evaluate the surface when assessing chemical decontamination products for treating peri-implant diseases or preserving peri-implant health. Among the products tested, Perisolv® and PrefGel® exhibited the lowest levels of titanium measured on the surface, while NuBone®Clean had the highest measured content. A higher titanium content indicates a less contaminated surface, as it is closer to the surface without a pellicle (Table 4). In addition, the titanium content in conjunction with the carbon content, showed an inverse relationship among the products (Table 2 and Table 3). This implies that the products with the highest measured titanium content, closer to the clean surface, benefit the environment surrounding the implant. In the decontamination phase, the highest content was attributed to NuBone®Clean, while in the re-contamination phase, H2O2 alone has the highest content; however, both values are close to each other. Interestingly Perisolv® had a higher content after re-contamination than after decontamination. It indicated that this product's effect is visible first when re-contaminating the surface.
NuBone®Clean also exhibited the lowest content of nitrogen on the surface after decontamination. Nitrogen is a common component in proteins [28], and the low nitrogen content observed indicates the effectiveness of surface cleaning. Interestingly, Perisolv® exhibited a lower nitrogen content after re-contamination than after decontamination, further highlighting the compound's impact after surface re-contamination. This suggests that Perisolv® remains on the surface, exerting a prolonged effect. Similarly, the calcium content on the surface followed a similar pattern, with the highest levels observed for NuBone®Clean. After re-contamination, Perisolv® showed higher calcium content than after decontamination, although still lower than NuBone®Clean. Calcium is considered beneficial as numerous calcium-binding proteins play essential roles in cellular processes [29]. Some authors have also indicated that calcium bonding to the implant surface can facilitate bone generation around implants [30]. These findings suggest that NuBone®Clean effectively reduces nitrogen content and exhibits higher calcium content on the implant surface, having potential clinical benefits in relation to surface cleaning and bone regenerating effects.
These findings have significant implications when considering early treatment of peri-implant diseases. In previous studies, Pluronic®, a polymeric hydrogel, has shown favourable effects on wound healing [31,32]. It belongs to the class of triblock copolymers, which consists of poly(ethylene oxide) (PEO) and poly(propylene oxide) (PPO) blocks arranged in a PEO-PPO-PEO structure. This helps emulsify and solubilise organic contaminants as surfactants, facilitating their removal from the titanium surface. Its use as a wound cleanser in chronic wounds with delayed healing has demonstrated positive outcomes [32]. One of the active ingredients in NuBone®Clean, hydrogen peroxide, an oxidising agent, can react with organic contaminants and also the Pluronic® hydrogel, forming new functional groups such as the O-C=O bond. The O-C=O group may be formed through the oxidation of hydroxyl groups (C-OH) in PEO and PPO blocks or from the oxidation of organic contaminants on the titanium surface. NuBone®Clean showed high values of this bond, being close to the clean control. In addition, NuBone®Clean exhibited the lowest content of C-OH and C-O-C bonds, again being closest to the clean control.
The presence of specific functional groups, such as C=O and O-C-O can affect the implant's performance and the biological response it elicits. Following exposure to saliva protein, the emergence of these carbon compounds on titanium surfaces is likely due to the adsorption and subsequent chemical reaction of these proteins on the titanium surface [33]. Saliva proteins are rich in amino acids, many containing carbonyl and ether groups. When these proteins come into contact with the titanium surface, they may undergo adsorption processes, enriching the surface with these functional groups. This can change the surface chemistry and thus influence how the implant interacts with the surrounding tissues, potentially affecting its performance and biocompatibility. Furthermore, saliva proteins may also undergo conformational changes upon interaction with the titanium surface, exposing additional functional groups initially hidden in the protein structure [34]. NuBone®Clean had the lowest overall median of C=O and O-C-O measured, being closer to a clean implant surface, indicating less contaminants on the surface. On the other hand, O-C-O groups might improve the resistance to corrosion due to their stability, providing a protective effect on the implant surface. Such conformational changes could contribute to the increase in the presence of C=O and O-C-O groups on the surface for some of the products.
Overall, the findings elucidate the advantageous effects of combining Pluronic® gel with H2O2 on pellicle structures. A safety assessment is necessary despite the potential clinical benefits of this combined effect on the pellicle. Patient safety stands dominant in the execution of dental procedures and treatments. As healthcare providers, our commitment lies in ensuring the effectiveness of our materials and strategies while preserving patient well-being. None of the tested decontamination solutions were cytotoxic.
Moreover, the clinical assessment of safety did not exhibit any adverse reactions. However, it is incumbent upon us to proceed with caution and to pursue further research before incorporating these solutions into clinical practice confidently. Studying the proteins that adhere to the implant surface remains necessary post-treatment. This investigation will provide valuable insight into whether these proteins encourage regeneration or biofilm formation. In furthering our understanding, controlled randomised clinical trials should be undertaken to evaluate this product's clinical efficacy, especially in combination with mechanical treatment modalities.
Developing new remedies for peri-implant disease treatment is urgent due to the increasing prevalence of dental implants and the subsequent rise in implant-related complications [35]. As dental practitioners, we are responsible for providing our patients with the most effective and safe treatments. However, the quest for more effective treatments should never compromise safety. We observed in this study that products like PrefGel®, typically used on root surfaces and applied to implant surfaces, did not have any beneficial effects on the implant surface. Mainly underlining the necessity for more comprehensive testing of dental biomaterials. Conclusively, our discussion underscores the necessity for larger, more extensive studies to substantiate our findings and solidify the foundation for clinical recommendations. Although our research is an encouraging pilot study in evaluating these chemical agents' safety and potential clinical benefits, we recognise the imperative of validating our findings through more comprehensive clinical trials.
5. Conclusions
In conclusion, the evaluation of surface chemistry is crucial in assessing the effectiveness of chemical decontamination products for titanium implants. Our study underscores the potential of chemical decontamination solutions in treating peri-implant disease. We have presented a potential chemical decontamination methodology that is effective against pellicle formation and is safe with limitations to the in vitro and human testing protocols. NuBone®Clean was more effective in providing a cleaner titanium surface than other tested chemical decontamination candidates. None of the tested chemical decontamination candidates had any cytotoxic effect. Furthermore, we advocate for larger studies to evaluate the safety and efficacy of these chemical agents thoroughly before they are introduced to the market. This multifaceted approach will ensure that the development and deployment of new dental treatments are safe and effective, thereby protecting patient well-being while advancing the field of dentistry.
Author Contributions
BH contributed to the conception, design, data acquisition and interpretation, performed statistical analyses, drafted, and critically revised the manuscript. SK contributed to the design, data acquisition, statistical analyses, and interpretation and critically revised the manuscript. AEA, JB Contributed to design, interpretation and critically revised the manuscript. HJH contributed to the conception, design, statistical analyses, interpretation and critically revised the manuscript. JB contributed to data acquisition, interpretation and critically revised the manuscript. SPL and JEE Contributed to the design, interpretation and critically revised the manuscript.
Funding
This study was supported by the Research Council of Norway, "MISFAITH" Grant No. 331752, "DEBRIGEL "Grant no. 332148 and Horizon Europe "BIOMATDB", Grant no. 101058779.
Data Availability Statement
Data available upon request to the corresponding author.
Acknowledgments
Martin F. Sunding, Sustainable Energy Technology, SINTEF Industry, is acknowledge for aid and great help in both conducting XPS analysis and subsequently data processing and interpretation.
Conflicts of Interest
Haugen and Lyngstadaas are inventors of the technology behind NuBoneClean (patent number: WO2011073194). The commercial rights for NuBoneClean are shared with Corticalis AS and the University of Oslo. Ellingsen, Haugen and Lyngstadaas, are shareholderof Corticalis AS.
References
- Campoccia, D.; Montanaro, L.; Arciola, C.R. The significance of infection related to orthopedic devices and issues of antibiotic resistance. Biomaterials 2006, 27, 2331–2339. [Google Scholar] [CrossRef] [PubMed]
- Grundy, E.M.; Murphy, M. Population ageing in Europe. Oxford textbook of geriatric medicine 2017, 11. [Google Scholar]
- Owens, C.D.; Stoessel, K. Surgical site infections: Epidemiology, microbiology and prevention. J Hosp Infect 2008, 70 Suppl 2, 3–10. [Google Scholar] [CrossRef]
- Donlan, R.M. Biofilms and device-associated infections. Emerg Infect Dis 2001, 7, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Stewart, P.S.; Costerton, J.W. Antibiotic resistance of bacteria in biofilms. The lancet 2001, 358, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Stevens, P.M.; Klatt, J.B. Guided growth for pathological physes: Radiographic improvement during realignment. J Pediatr Orthop 2008, 28, 632–639. [Google Scholar] [CrossRef]
- Prathapachandran, J.; Suresh, N. Management of peri-implantitis. Dental research journal 2012, 9, 516. [Google Scholar] [CrossRef]
- Lee, C.-T.; Huang, Y.-W.; Zhu, L.; Weltman, R. Prevalences of peri-implantitis and peri-implant mucositis: Systematic review and meta-analysis. J. Dent. 2017, 62, 1–12. [Google Scholar] [CrossRef]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol 2018, 89 Suppl 1, S313–S318. [Google Scholar] [CrossRef]
- Chawhuaveang, D.D.; Yu, O.Y.; Yin, I.X.; Lam, W.Y.; Mei, M.L.; Chu, C.H. Acquired salivary pellicle and oral diseases: A literature review. J Dent Sci 2021, 16, 523–529. [Google Scholar] [CrossRef]
- Länge, K.; Herold, M.; Scheideler, L.; Geis-Gerstorfer, J.; Wendel, H.P.; Gauglitz, G. Investigation of initial pellicle formation on modified titanium dioxide (TiO2) surfaces by reflectometric interference spectroscopy (RIfS) in a model system. Dent Mater 2004, 20, 814–822. [Google Scholar] [CrossRef] [PubMed]
- Sterzenbach, T.; Helbig, R.; Hannig, C.; Hannig, M. Bioadhesion in the oral cavity and approaches for biofilm management by surface modifications. Clinical oral investigations 2020, 24, 4237–4260. [Google Scholar] [CrossRef] [PubMed]
- Hussain, B.; Haugen, H.J.; Aass, A.M.; Sanz, M.; Antonoglou, G.N.; Bouchard, P.; Bozic, D.; Eickholz, P.; Jepsen, K.; Jepsen, S. Peri-Implant Health and the Knowing-Doing Gap—A Digital Survey on Procedures and Therapies. Frontiers in Dental Medicine 2021, 2, 726607. [Google Scholar] [CrossRef]
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontol 2000 2017, 73, 7–21. [Google Scholar] [CrossRef]
- Lamolle, S.F.; Monjo, M.; Rubert, M.; Haugen, H.J.; Lyngstadaas, S.P.; Ellingsen, J.E. The effect of hydrofluoric acid treatment of titanium surface on nanostructural and chemical changes and the growth of MC3T3-E1 cells. Biomaterials 2009, 30, 736–742. [Google Scholar] [CrossRef]
- Zhu, X.; Wen, G.; Liu, H.; Han, S.; Chen, S.; Kong, Q.; Feng, W. One-step hydrothermal synthesis and characterization of Cu-doped TiO 2 nanoparticles/nanobucks/nanorods with enhanced photocatalytic performance under simulated solar light. Journal of Materials Science: Materials in Electronics 2019, 30, 13826–13834. [Google Scholar] [CrossRef]
- Zhao, Z.; Zhou, Y.; Wan, W.; Wang, F.; Zhang, Q.; Lin, Y. Nanoporous TiO2/polyaniline composite films with enhanced photoelectrochemical properties. Materials Letters 2014, 130, 150–153. [Google Scholar] [CrossRef]
- Caracciolo, L.; Madec, L.; Martinez, H. XPS analysis of K-based reference compounds to allow reliable studies of solid electrolyte interphase in K-ion batteries. ACS Applied Energy Materials 2021, 4, 11693–11699. [Google Scholar] [CrossRef]
- Valencia-Alvarado, R.; De La Piedad-Beneitez, A.; López-Callejas, R.; Rodríguez-Méndez, B.; Mercado-Cabrera, A.; Peña-Eguiluz, R.; Muñoz-Castro, A.; De La Rosa-Vázquez, J. Sequential processes to produce N-TiO2 films through Rf plasmas. In Proceedings of the MATEC Web of Conferences; 2016; p. 06075. [Google Scholar] [CrossRef]
- Natu, V.; Benchakar, M.; Canaff, C.; Habrioux, A.; Celerier, S.; Barsoum, M.W. A critical analysis of the X-ray photoelectron spectra of Ti3C2Tz MXenes. Matter 2021, 4, 1224–1251. [Google Scholar] [CrossRef]
- Popov, A.A.; Tikhonowski, G.V.; Shakhov, P.V.; Popova-Kuznetsova, E.A.; Tselikov, G.I.; Romanov, R.I.; Markeev, A.M.; Klimentov, S.M.; Kabashin, A.V. Synthesis of titanium nitride nanoparticles by pulsed laser ablation in different aqueous and organic solutions. Nanomaterials 2022, 12, 1672. [Google Scholar] [CrossRef] [PubMed]
- Peña-Juárez, M.G.; Robles-Martínez, M.; Méndez-Rodríguez, K.B.; López-Esparza, R.; Pérez, E.; Gonzalez-Calderon, J.A. Role of the chemical modification of titanium dioxide surface on the interaction with silver nanoparticles and the capability to enhance antimicrobial properties of poly(lactic acid) composites. Polymer Bulletin 2021, 78, 2765–2790. [Google Scholar] [CrossRef]
- Vitanov, P.; Stefanov, P.; Harizanova, A.; Ivanova, T. XPS characterization of thin (Al2O3) x (TiO2) 1-x films deposited on silicon. In Proceedings of the Journal of Physics: Conference Series; 2008; p. 012036. [Google Scholar] [CrossRef]
- Buser, D.; Janner, S.F.; Wittneben, J.G.; Brägger, U.; Ramseier, C.A.; Salvi, G.E. 10-year survival and success rates of 511 titanium implants with a sandblasted and acid-etched surface: A retrospective study in 303 partially edentulous patients. Clinical implant dentistry and related research 2012, 14, 839–851. [Google Scholar] [CrossRef] [PubMed]
- Simão Jr, B.S.; Costa, D.D.; Cangussu, M.C.T.; Sotto-Maior, B.S.; Devita, R.L.; de Carvalho, J.J.; da Silva Brum, I. Observational Study on the Success Rate of Osseointegration: A Prospective Analysis of 15,483 Implants in a Public Health Setting. BioMed 2022, 2, 422–430. [Google Scholar] [CrossRef]
- Derks, J.; Schaller, D.; Hakansson, J.; Wennstrom, J.L.; Tomasi, C.; Berglundh, T. Peri-implantitis - onset and pattern of progression. J Clin Periodontol 2016, 43, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Guo, T.; Gulati, K.; Arora, H.; Han, P.; Fournier, B.; Ivanovski, S. Race to invade: Understanding soft tissue integration at the transmucosal region of titanium dental implants. Dent Mater 2021, 37, 816–831. [Google Scholar] [CrossRef]
- Campbell, M.K.; Farrell, S.O.; McDougal, O.M. Amino Acids and Peptides. In Biochemistry, 9th ed.; Cengage Learning: Boston, USA, 2016; pp. 60–74. [Google Scholar]
- Habibovic, P.; Barralet, J. Bioinorganics and biomaterials: Bone repair. Acta biomaterialia 2011, 7, 3013–3026. [Google Scholar] [CrossRef]
- Anitua, E.; Piñas, L.; Murias, A.; Prado, R.; Tejero, R. Effects of calcium ions on titanium surfaces for bone regeneration. Colloids and Surfaces B: Biointerfaces 2015, 130, 173–181. [Google Scholar] [CrossRef]
- Kant, V.; Gopal, A.; Kumar, D.; Gopalkrishnan, A.; Pathak, N.N.; Kurade, N.P.; Tandan, S.K.; Kumar, D. Topical pluronic F-127 gel application enhances cutaneous wound healing in rats. Acta Histochem 2014, 116, 5–13. [Google Scholar] [CrossRef]
- Percival, S.L.; Chen, R.; Mayer, D.; Salisbury, A.M. Mode of action of poloxamer-based surfactants in wound care and efficacy on biofilms. Int. Wound J. 2018, 15, 749–755. [Google Scholar] [CrossRef]
- Narendrakumar, K.; Kulkarni, M.; Addison, O.; Mazare, A.; Junkar, I.; Schmuki, P.; Sammons, R.; Iglič, A. Adherence of oral streptococci to nanostructured titanium surfaces. Dent Mater 2015, 31, 1460–1468. [Google Scholar] [CrossRef]
- Neoh, K.G.; Wang, R.; Kang, E.T. 7 - Surface nanoengineering for combating biomaterials infections. In Biomaterials and Medical Device - Associated Infections, Barnes, L., Cooper, I.R., Eds.; Woodhead Publishing: Oxford, 2015; pp. 133–161. [Google Scholar] [CrossRef]
- Astolfi, V.; Ríos-Carrasco, B.; Gil-Mur, F.J.; Ríos-Santos, J.V.; Bullón, B.; Herrero-Climent, M.; Bullón, P. Incidence of Peri-Implantitis and Relationship with Different Conditions: A Retrospective Study. Int J Environ Res Public Health 2022, 19. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Graphical illustration of how the pellicle study (top panel), in vitro (middle) and clinical study (lower panel) was performed.
Figure 1.
Graphical illustration of how the pellicle study (top panel), in vitro (middle) and clinical study (lower panel) was performed.
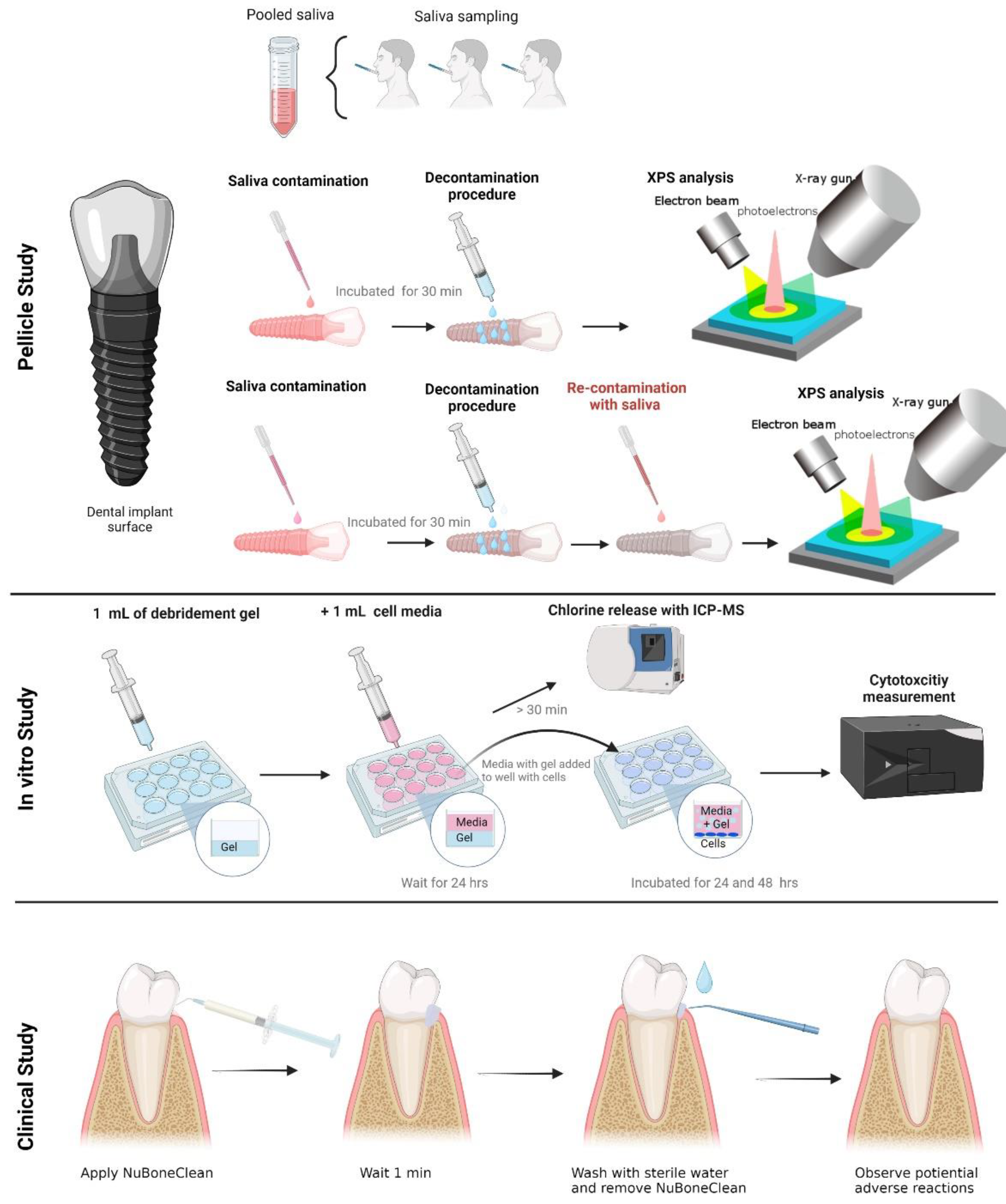
Figure 2.
XPS high-resolution spectra of Oxygen (O 1s) (A-B), Carbon (C 1s) (C-D), and Titanium (Ti 2p) (E-F). The left panel are titanium surface after pellicle decontamination, and the right panel are titanium surface after re-contamination with pellicle.
Figure 2.
XPS high-resolution spectra of Oxygen (O 1s) (A-B), Carbon (C 1s) (C-D), and Titanium (Ti 2p) (E-F). The left panel are titanium surface after pellicle decontamination, and the right panel are titanium surface after re-contamination with pellicle.
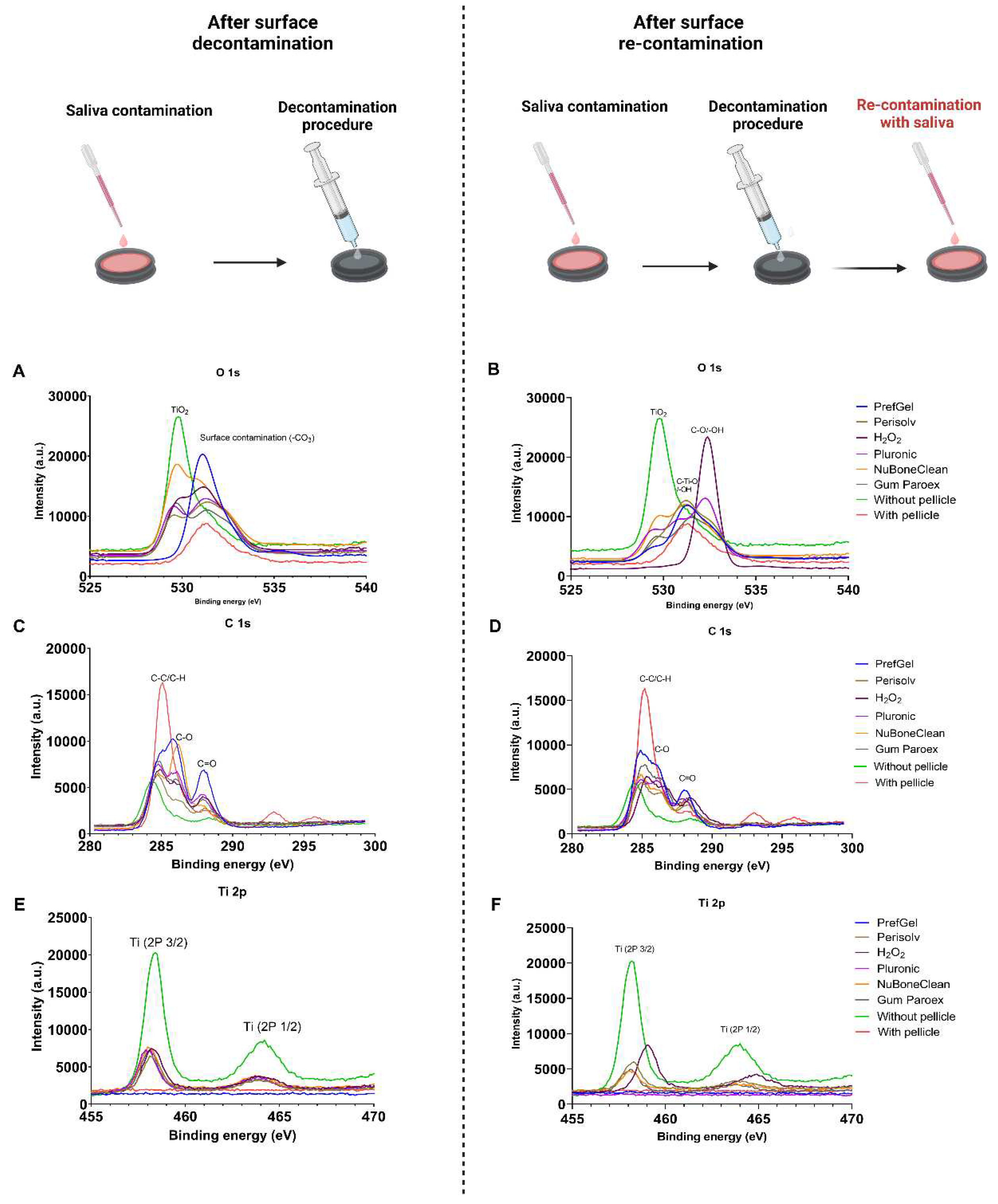
Figure 3.
XPS high-resolution spectra of calcium (Ca 1s) (A-B), chlorine (C1s) (C-D), and sodium (Na 1s) (E-F). The left panel are titanium surface after pellicle decontamination, and the right panel are titanium surface after re-contamination with pellicle.
Figure 3.
XPS high-resolution spectra of calcium (Ca 1s) (A-B), chlorine (C1s) (C-D), and sodium (Na 1s) (E-F). The left panel are titanium surface after pellicle decontamination, and the right panel are titanium surface after re-contamination with pellicle.
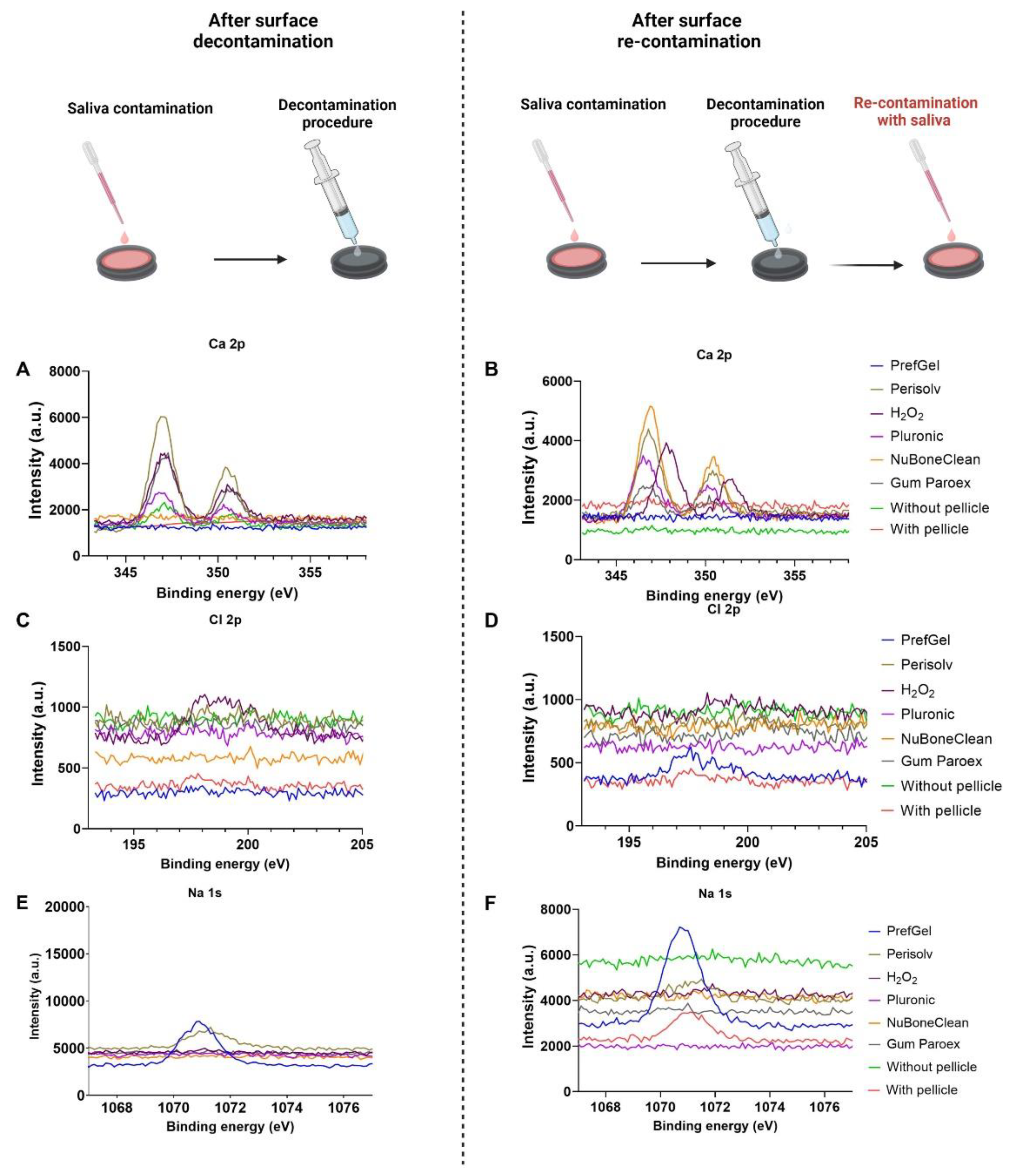
Figure 4.
Quantification of selected carbon chemical bonds (C-C/C-H, O-C=O and C-O-C/C-OH) from the XPS high-resolution spectra (n=3), *p<0.05 versus titanium surface with a pellicle.
Figure 4.
Quantification of selected carbon chemical bonds (C-C/C-H, O-C=O and C-O-C/C-OH) from the XPS high-resolution spectra (n=3), *p<0.05 versus titanium surface with a pellicle.
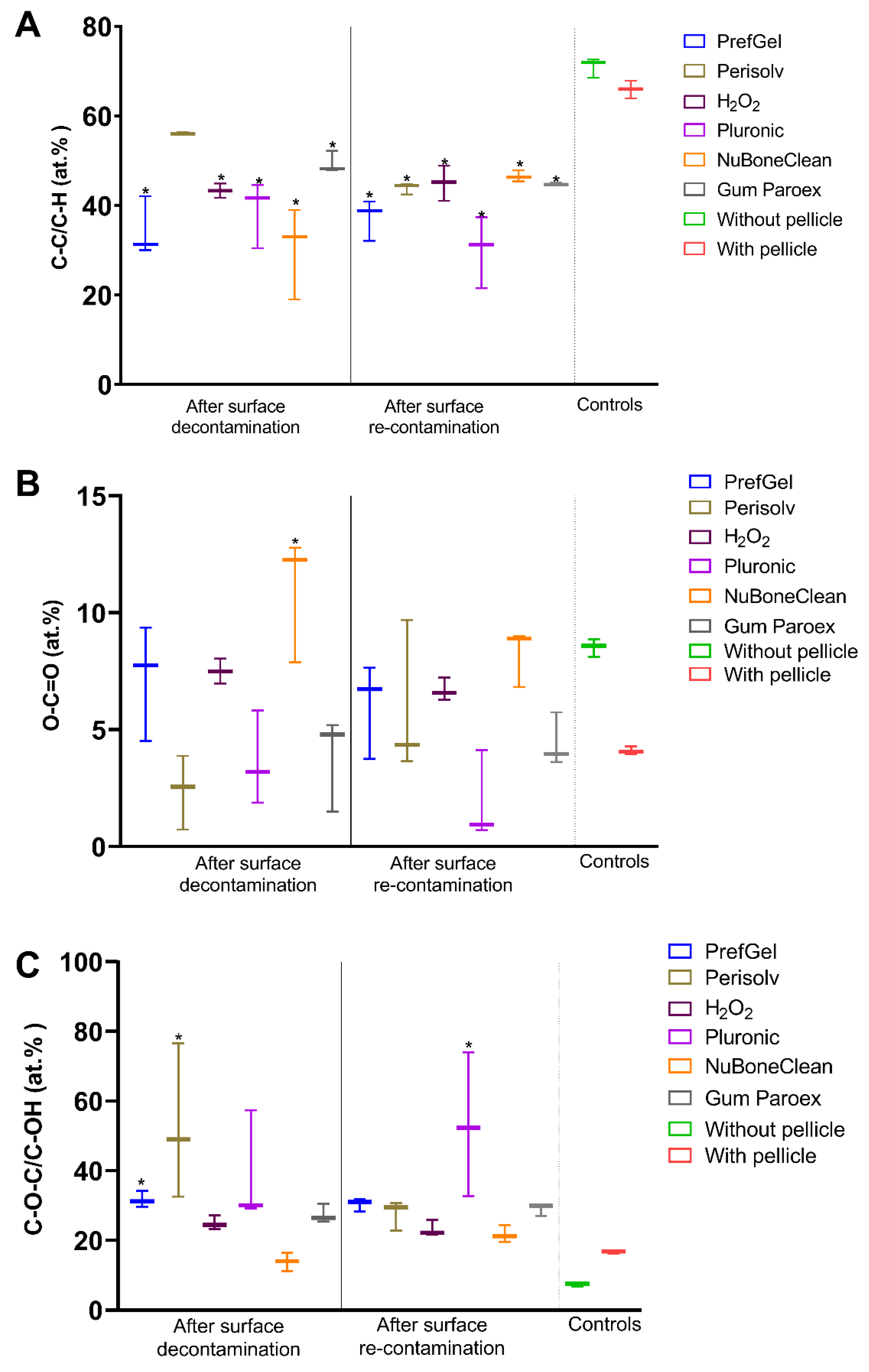
Figure 5.
Quantification of selected carbon chemical bonds (C=O/O-C-O and O=C-OH) from the XPS high-resolution spectra (n=3), *p<0.05 versus titanium surface with pellicle.
Figure 5.
Quantification of selected carbon chemical bonds (C=O/O-C-O and O=C-OH) from the XPS high-resolution spectra (n=3), *p<0.05 versus titanium surface with pellicle.
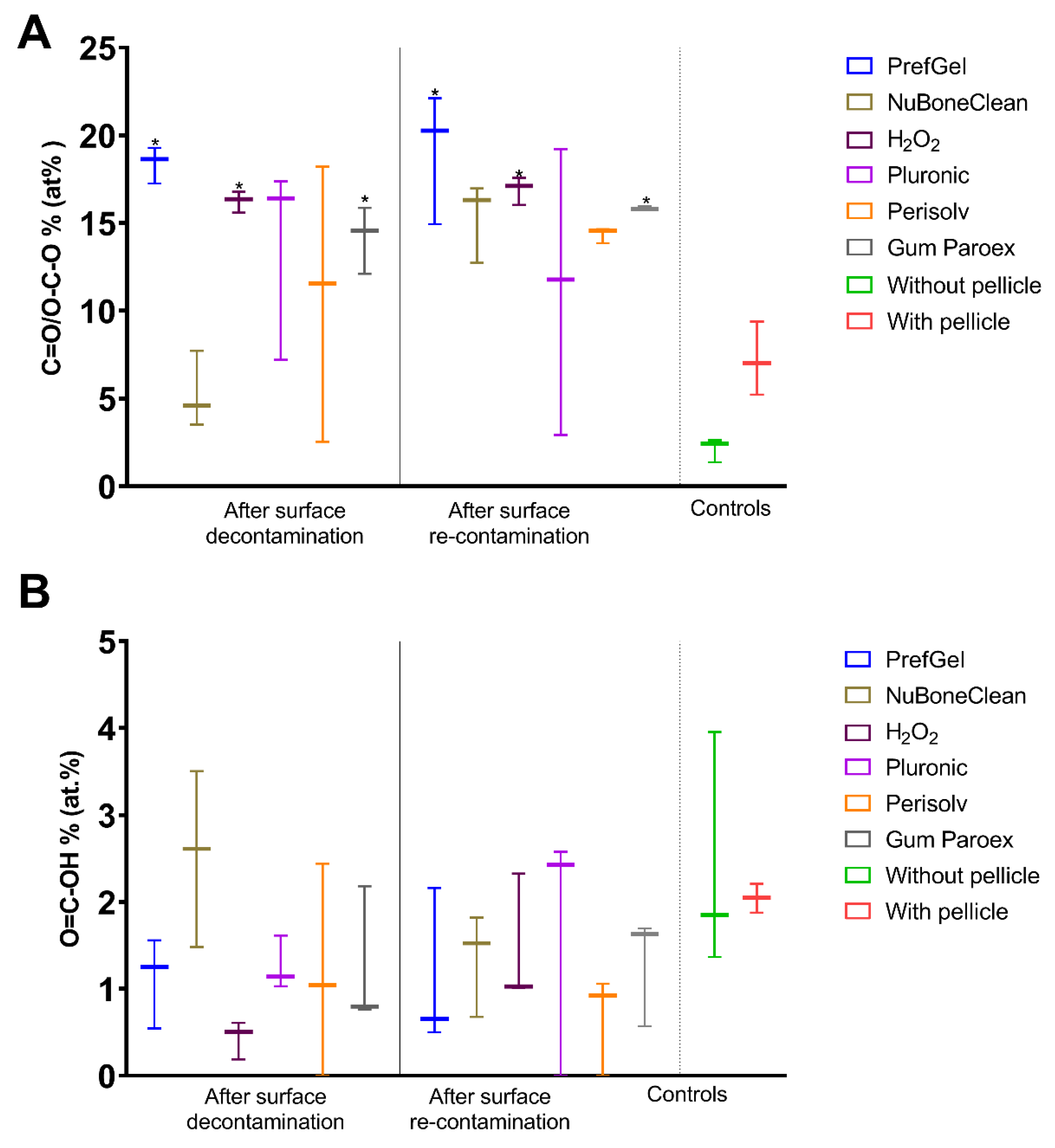
Figure 6.
LDH after 24 and 48 hours after exposure of decontamination solution to pre-osteoblastic cells, a: significantly lower than GumParoex® at 24hr, b: significantly higher than H2O2 at 24hrs, c: significantly lower than Pluronic® at 48 hrs.
Figure 6.
LDH after 24 and 48 hours after exposure of decontamination solution to pre-osteoblastic cells, a: significantly lower than GumParoex® at 24hr, b: significantly higher than H2O2 at 24hrs, c: significantly lower than Pluronic® at 48 hrs.
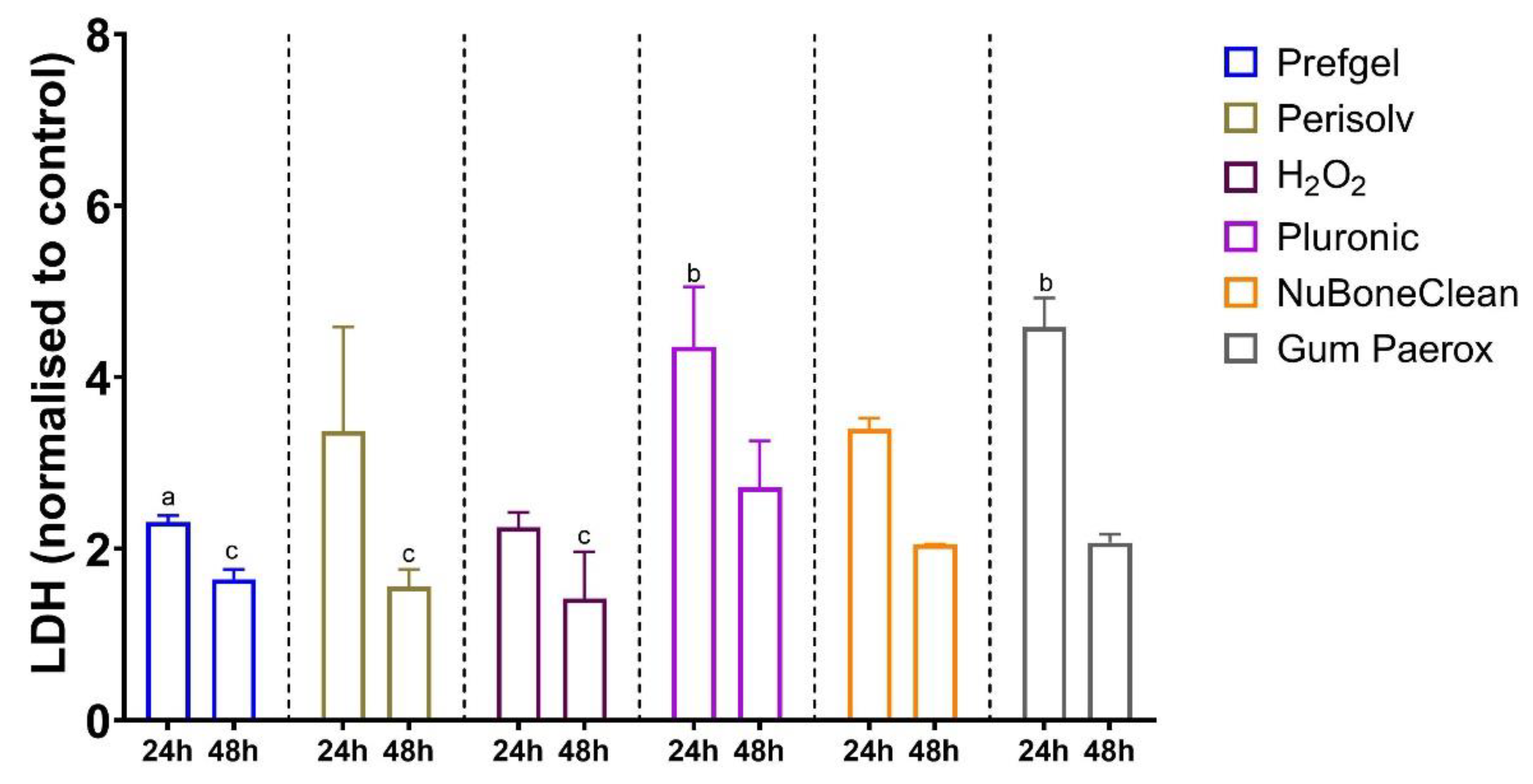
Figure 8.
Clinical experiments for detection of potential adverse reactions. A: Graphical presentation of the clinical experiment. B: After application of NuBone® Clean Advanced, C: Clinical control after two days.
Figure 8.
Clinical experiments for detection of potential adverse reactions. A: Graphical presentation of the clinical experiment. B: After application of NuBone® Clean Advanced, C: Clinical control after two days.
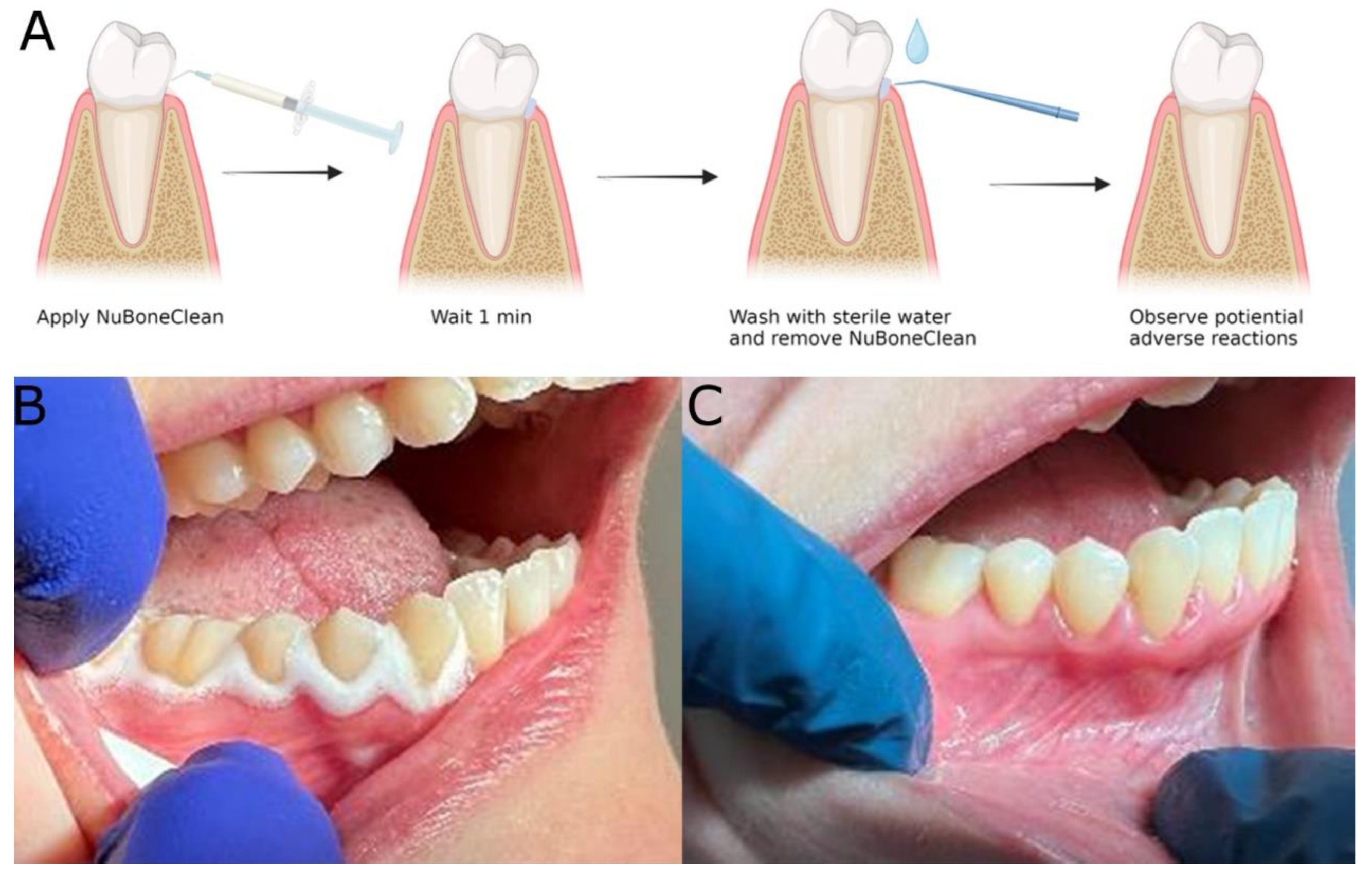
Table 1.
Decontamination products used in this study.
| Product name | Content | In clinical dental use |
|---|---|---|
| PrefGel® | 24% EDTA + hydrogel | Yes |
| Perisolv® | Sodium hypochlorite + a hydrogel | Yes |
| Hydrogenperoxide | 3% H2O2 in water | Yes |
| Pluronic® F-127 | 28 % Poloxamer in water | No |
| NuBone® Clean | 3% H2O2 + a hydrogel (poloxamer) | No |
| GUM® Paroex® | 0.12 % Chlorhexidine digluconate + 0.05 % Cetylpyridinium chloride | Yes |
Table 5.
Patient satisfaction Score.
| Patient | Patient satisfaction Score |
|---|---|
| 1 | 10 |
| 2 | 10 |
| 3 | 10 |
| 4 | 10 |
| 5 | 10 |
| 6 | 10 |
| 7 | 10 |
| 8 | 10 |
| 9 | 10 |
| 10 | 5 |
| 11 | 10 |
| 12 | 10 |
| Mean | 9.6 |
| Median | 10.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



