Submitted:
25 June 2023
Posted:
27 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: The Covid-19 pandemic abruptly disrupted global healthcare systems, necessitating rapid adaptations. This study evaluates the impact on health systems and services in the aftermath of the first wave in the Indian context. It analyses the disruptions, adaptive measures, and changes made, as well as the challenges faced by healthcare providers and seekers. Valuable insights from this study will enhance the resilience and preparedness of healthcare systems for future challenges. Methods: The eligible studies included primary studies conducted in the Indian context that explore the impact of COVID-19 on health services provision, utilisation, and the well-being of healthcare providers and seekers. Electronic searches were conducted in six databases: PubMed, MEDLINE, Embase, Global Health, CINAHL, and the WHO database on COVID-19. The results were analysed using detailed narrative synthesis. Results: The review includes 38 articles, incorporating a total of 22,502 subjects. There has been a substantial impact on health service provision, particularly in outpatient departments (OPD) (n=19) and elective services (n=16), while emergency services continued at sub-optimal levels (n=20). Various adaptations and changes were implemented in precautionary measures, protocols, staff allocation and training, usage of personal protective equipment (PPE), preoperative, operative, and postoperative measures, as well as physical infrastructure and resources. Depression and stress (n=14), fear of contracting the infection (n=6), stigmatisation (n=5), and financial repercussions (n=5) significantly affected the mental health of healthcare providers, and healthcare seekers also faced significant challenges (n=11). Conclusion: The study reveals COVID-19's substantial impact on health services. The healthcare system responded by quickly adjusting staff management, resource allocation, and infection prevention measures. The study also highlights the mental health challenges faced by healthcare providers and the concerns of healthcare seekers regarding delays and suboptimal care. Looking ahead, the findings underscore the importance of preparedness for future pandemics, including improved healthcare infrastructure, resource optimisation, and comprehensive protocols. Lessons learned from COVID-19 should inform strategies to mitigate disruptions and ensure the well-being of healthcare providers and seekers in future outbreaks.
Keywords:
health system
; health services
; outpatient department (OPD)
; elective health services
; emergency health services
; Personal Protective Equipment (PPE)
; health care providers
1. Introduction
The COVID-19 pandemic has posed unprecedented challenges to healthcare systems, healthcare providers, and communities worldwide, including India. At the peak of the outbreak, healthcare services in hospitals, clinics, and healthcare centres faced immense strain, with a rapid and significant increase in patient care demands. Balancing the provision of care for COVID-19 patients while ensuring continued treatment for individuals with other medical conditions presented a complex planning challenge.
While several primary studies have examined the impact of COVID-19 on the health system and its stakeholders, there is a need for a systematic appraisal and critique of these studies, particularly focusing on the peak of the outbreak. This review aims to consolidate the available literature to gain a comprehensive understanding of the health system's response and assess the impact of the pandemic on healthcare services, healthcare providers, and healthcare seekers across various clinical areas and facilities during the peak of the COVID-19 outbreak. The review aims to achieve the following objectives:
- Assess the impact of COVID-19 on the provision, utilisation, and availability of health services
- Understand the health system’s response – adaptations, interventions and efforts for continuity and resumption of services
- Evaluate the implications of COVID-19 and its response on individuals – Health care providers and health care seekers
2. Materials and Methods
The review is registered with PROSPERO (International Prospective Register of systematic reviews) at the National Institute for Health Research and Centre for Reviews and Dissemination (CRD) at the University of York (registration number CRD42020227327). Design and reporting were conducted per the PRISMA Statement [1].
2.1. Inclusion criteria
- ▪
- Studies conducted exclusively within the Indian context, from the onset of Covid-19 to its first peak and in its aftermath until December 15th, 2020
- ▪
- Primary studies of any research design
- ▪
- Studies evaluating the impact of COVID-19 on the provision, utilisation, and availability of health services
- ▪
- Studies exploring the health system’s response in terms of adaptations, interventions and efforts made in different types of health facilities for maintaining the continuity of services
- ▪
- Studies examining the impact of the pandemic on individuals – health care providers, individuals with acute and chronic diseases
2.2. Exclusion criteria
- ▪
- Studies on pandemics other than COVID-19
- ▪
- Studies that are not primary (like reviews, reports, policy briefs, commentary etc.)
- ▪
- Global/multi-country studies with India just as one of the settings and studies not conducted in the Indian context.
- ▪
- Studies evaluating aetiology, pathophysiology, histopathology, serology or laboratory examination of COVID-19, clinical trials, or vaccine development.
- ▪
- Studies that are not written in English
2.3. Search strategy
We utilised the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [1] to conduct a search of electronic databases. We electronically searched six databases, namely PubMed, MEDLINE, Embase, Global Health, CINAHL, and the WHO database on COVID-19, to identify primary studies employing quantitative, qualitative, and mixed methods. The search was limited to primary studies published in English until December 15th 2020. Our search approach employed a combination of Medical Subject Headings (MeSH), free-text terms, and word variants related to COVID-19, the health system, health services, communities, and community facilitators in the Indian context. In addition to the electronic databases, we also conducted a search on Google Scholar for relevant primary studies. Furthermore, we performed a snowball search to identify references from relevant papers. Detailed search strategies were developed for each electronic database.
2.4. Data extraction (selection and coding)
The results of all literature searches were imported into the Mendeley reference management software. Duplicate records were identified and removed using the software, and the remaining unique records were then imported into Covidence, a web-based systematic review software package developed by Veritas Health Innovation.
Firstly, two authors independently screened the titles and abstracts of the retrieved records against the predefined inclusion and exclusion criteria. Secondly, all studies that met the inclusion criteria underwent a thorough full-text screening process by the two authors independently. Any disagreements were resolved through discussions or, if necessary, involving an independent reviewer.
In addition, a hand search was conducted by reviewing the reference lists of relevant papers to identify any additional studies for inclusion. Furthermore, all the screened articles underwent a further relevance check.
The data extraction process involved two reviewers extracting data from the included studies into Excel using a predefined and pilot-tested data collection form.
2.5. Data items
The following general information was extracted from the included articles and organised into a table: author name(s), publishing journal, study objectives, study design, outcome measures, and findings related to the availability, provision, and delivery of health services mentioned in the studies, adaptations and changes in the health system, efforts undertaken, impact on healthcare providers, as well as the impact on the health, livelihood, and disease progression among individuals and communities.
2.6. Outcomes
Given the anticipated heterogeneity in the impact of COVID-19 on the health system and its different components and stakeholders, we included studies that reported a range of outcomes. Specifically, we included studies that examined the effects on at least one of the primary outcomes, with or without the secondary outcomes listed below:
2.6.1. Primary
-
Health services for varied health conditions:
- ▪
-
Changes in the provision, utilisation, or availability of:
- ○
- Outpatient department (OPD)
- ○
- Elective health services
- ○
- Emergency health services
pertaining to reproductive, maternal, and child health services, non-communicable diseases (cancer, cardiovascular diseases, diabetes, etc.), and other general or specific health conditions (orthopaedic, ophthalmic, neurological, etc.).
- 2.
-
Health system response to COVID-19:
- ▪
-
Efforts and adaptations made in:
- ○
- General precautionary and infection prevention measures
- ○
- Protocols and guidelines
- ○
- Staff allocation, management, and training
- ○
- Personal Protective Equipment (PPE)
- ○
- Physical infrastructure and resources.
2.6.2. Secondary
-
Mental/psychological health of health care providers:
- ▪
- Depression, anxiety, and burnout
- ▪
- Fear of infecting themselves and transmitting it to family members,
- ▪
- Financial repercussions
- General health or disease conditions of health care seekers/individuals
2.7. Critical appraisal – quality assessment
Two reviewers (A.S.C., A.N.) appraised the included studies using two tools - the CASP (Critical appraisal skills programme) checklist for qualitative (observational) studies and AXIS critical appraisal tool for cross sectional studies/surveys. Both tools have been adapted for use in this review. The reviewers utilised the checklists to evaluate each included study's design, conduct, and analysis, with a focus on addressing potential biases.
Any discrepancies in ratings between the two reviewers were thoroughly discussed, and consensus was reached for each checklist item. The quality appraisal was not a criterion for study inclusion; therefore, no studies were excluded based on the results of the appraisal.
2.8. Data analysis
Due to the heterogeneity of the studies, a detailed narrative synthesis was employed to analyse and interpret the data based on the outcome measures. This approach enabled us to thoroughly examine and comprehend the data, taking into account its diverse nature. The narrative synthesis played a crucial role in identifying patterns and trends within the findings. By utilising this method, we gained valuable insights from the varied studies without compromising their heterogeneity.
3. Results
3.1. Screening and inclusion of studies
From the screening of five databases—PubMed, MEDLINE, Global Health, EMBASE, CINAHL, and WHO COVID-19 Global literature on coronavirus disease—we identified 1477 records (Figure 1). Additionally, 74 records were retrieved and added from other sources, such as Google Scholar and references in the citations. After removing duplicates, 1271 records were retained. Subsequently, 526 studies were selected based on the initial screening of abstracts. The full text of these 526 articles was assessed for eligibility criteria, resulting in 121 articles. Of these, 38 articles were included for narrative analysis, while 83 were excluded for not meeting the eligibility criteria.
3.2. Narrative analysis
The review comprises a total of 38 primary studies (Table 1) with a collective participant count of 22,502. These studies consist of 21 cross-sectional surveys, 16 observational studies, and 1 mixed-method study combining survey and observational approaches. They were conducted in diverse settings, including clinics, hospitals, and primary healthcare or community health centres.
The participants involved in these studies encompassed healthcare providers, including surgeons, doctors, nurses, and frontline workers, as well as healthcare seekers, specifically patients. The findings derived from these studies have been meticulously analysed, interpreted, and categorised based on specific thematic areas.
3.2.1. Impact of COVID 19 and turn of events on provision, availability, and utilisation of health services
- a)
- Outpatient department (OPD) services
OPD services were described in 19 studies [2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20], involving 11,890 healthcare stakeholders. These studies covered various fields such as oncology, neurosurgery, ophthalmology, maternal health, primary health care, general surgery, orthopaedics, and palliative care. All 19 studies reported a significant reduction in OPD services during the lockdown phase (March-May 2020), which persisted for several months thereafter. On further studying analytically, the reduction in these OPD services was statistically significant (p <0.05 or <0.01) as reported in two studies [7,14]. Another study reported a staggering 97% decrease in OPD visits compared to the corresponding period in 2019 [15].
Among the OPD clinics at Primary Health Care sites, the greatest reduction was observed in noncommunicable diseases (NCDs) and immunisation clinics, while ANC services experienced lesser disruptions. General OPDs were the least affected [6]. Several included studies also reported the presence of screening OPDs, where incoming patients were assessed for COVID-19-related symptoms, travel history, and underwent thermal screening and/or subsequent COVID-19 testing [2,3,5,15,16].
- b)
- Elective services
Elective procedures are described in 16 studies [2,3,4,7,8,9,10,11,14,15,16,22,23,24,25,26], involving a total of 9,268 subjects. These studies consistently report a significant impact on elective procedures across various areas of healthcare services, with procedures either being completely halted, significantly reduced, or deferred.
For instance, several studies focus on cancer care, all indicating a noteworthy decline, deferral, or even cessation of elective oncological procedures [3,9,10,25,26]. These procedures include radiotherapy [9,26], surgery, chemotherapy [9], tumour boards [26], and nutritionist consultations [26]. In cases where appropriate, such as advanced cases, deferrals were made to manage cancer through neoadjuvant chemotherapy [3,26].
Orthopaedics also experienced a similar trend, with the majority of elective surgeries being halted [23]. Many orthopaedic surgeons limited their practice to performing only essential trauma surgeries (62%) or ceased surgeries altogether (35%) during this period. Likewise, 93% of general surgical practices ceased all elective surgical procedures [7].
There was a significant decrease in vitreoretinal ophthalmological surgeries [24], with many of them being postponed [15]. Neurosurgery also witnessed a sharp decline, with approximately 70% fewer surgeries performed (P=0.000)[14].
In the realm of maternal health services, a substantial 45% decrease in the number of deliveries was reported compared to pre-COVID-19 times, and this decline was statistically significant (P<0.001) [8]. Furthermore, there were notable delays in service provision [16].
When it comes to cardiovascular diseases, there was a notable reduction in STEMI admissions by 67% during the lockdown period compared to the pre-COVID period. The reduction in NSTEMI cases was even more significant, reaching 93% within the same timeframe [22].
- c)
- Emergency services
Emergency services are the subject of 20 studies [2,3,4,5,7,8,9,10,12,14,15,16,18,20,21,24,25,26,27,28] involving 12,850 healthcare stakeholders. These services encompass various areas such as ophthalmology, maternal health, non-communicable diseases (including cardiovascular diseases, diabetes, and kidney diseases), neurosurgery, orthopaedics, injuries/trauma, and general surgical practice.
Overall, the majority of healthcare providers and institutions continued to deliver emergency and urgent services, taking necessary precautions and adapting protocols and techniques accordingly. However, the provision and utilisation of these services were found to be impacted and altered due to challenges related to accessibility, transportation difficulties, infrastructural changes, resource constraints, and concerns arising from the lockdown. Consequently, these factors resulted in suboptimal medical care in life-threatening emergencies.Top of FormBottom of FormTop of FormBottom of Form
The altered pattern and adaptations are described in several studies in different clinical areas. In ophthalmological services [4], trauma cases accounted for the majority (51.9%), and a significant portion of doctors (83%) focused solely on emergency cases. Notably, there was a sharp 60% increase in home-related trauma cases during the lockdown, particularly among children.
In the realm of cardiovascular diseases [22], there was an upsurge in acute coronary syndrome (ACS) patients presenting with delayed symptoms and mechanical complications. Similarly, in the context of diabetes [18], only a small percentage of individuals experiencing severe hyperglycaemia and recurrent hypoglycaemia received emergency consultations or services.
Renal diseases witnessed a decline in the number of available dialysis stations and patients, both in the public and private sectors [20]. In cancer care, a significant proportion of respondents (69 - 92%) continued to provide treatment for advanced-stage emergency gynaecological cancers [10,25], employing modified approaches according to institutional protocols [25]. There has been an increase in the volume of maternal and obstetric emergencies due to factors such as the reduced number of antenatal visits, delays in accessing services (due to travel restrictions), and waiting until the last moment due to infection fears [8]. In orthopaedics, approximately 21% had even ceased emergency surgeries entirely, and a significant number of surgeons were exclusively performing unavoidable emergency trauma surgeries (62%)[23].
3.2.2. Health system’s response – adaptations and efforts for resumption of health care services
- a)
- General precautionary and infection prevention measures
Ten studies [3,5,6,13,14,15,16,18,24,29] involving 5,911 healthcare providers/seekers examined general precautionary and infection prevention measures. Several of these studies [3,5,13,15,16,24] highlight the widespread implementation of essential measures, including initial screening at entry, mandatory mask-wearing, and limitations on the number of attendants.
In addition to these measures, various efforts were implemented at several study sites [3,5,13,15,18,24] to ensure safety and hygiene. These efforts included providing hand sanitisers at accessible locations and displaying audio-visual notices at regular intervals to promote hand washing, mask usage, and adherence to social distancing norms. Furthermore, standing spaces were marked to maintain physical distance, adequately spaced sitting areas were designated, and surfaces were regularly sanitised.
Healthcare providers were reported to diligently implement infection prevention measures and take necessary precautions while delivering services. These included frequent hand sanitisation using alcohol-based sanitisers, utilising N95 masks, face shields, or safety goggles, wearing disposable gowns and gloves, layering double gowns when needed, and employing dedicated ICUs for suspected COVID-19 cases [3,5,13,14,18,29].
While these general precautionary measures were generally adhered to in most hospitals, they were significantly compromised at numerous primary healthcare centres [6]. For example, at 12 of these centres, the patient queuing capacity averaged 14.1 individuals, with efforts made to maintain minimal physical distancing. Furthermore, airborne infection control measures were absent in 76% of the sites, and 24% of the sites lacked adequate handwashing facilities for patients.
- b)
- Protocol and guidelines
To guide the operations, healthcare centres, hospitals, and clinics implemented various guidelines and protocols. The adoption and adherence to these diverse protocols and guidelines are discussed in ten studies [3,7,9,10,14,15,16,20,25,28], encompassing 8,355 participants. Some institutions formulated or modified their guidelines based on existing literature and guidelines, while others followed state, national, or international guidelines.
For example, in an oncological study, it was found that a significant majority of institutes (69%) were adhering to institutional guidelines, while the remaining institutes were following state or alternative guidelines [10]. Another oncological study [25] revealed that the majority of surveyed surgeons (75%) followed institutional or national guidelines, while the rest (25%) adhered to international guidelines. This considerable heterogeneity in the adoption and adherence to guidelines and protocols was further confirmed by a survey conducted by Prasad et al. in 19 major hospitals, which reported variations among facilities in terms of adhering to the guidelines issued by the Ministry of Health and Family Welfare (MoHFW) and the Indian Council of Medical Research (ICMR), with some institutions using their own protocols [20].
Within 3-4 months of the pandemic (May-June 2020), the majority of healthcare facilities had implemented protocols for reopening services in the "new normal" situation [14]. However, despite the availability of these protocols and guidelines, a significant proportion (60%) of healthcare providers expressed a lack of scientific evidence supporting the guidelines [25]. This absence of specific protocols also contributed to the stress experienced by healthcare workers, highlighting the urgent need for evidence-based protocols [14]. For example, a significant majority (71.5%) of surgeons expressed the explicit need for guidelines addressing safety measures for future surgical practices and providing solutions to mitigate the aftereffects of the pandemic [7].
- c)
- Staff allocation, management, and training
Fifteen (n=15) studies [2,3,6,9,12,14,15,16,18,19,20,24,29,30,31], involving 10,247 healthcare stakeholders provide valuable insights into staff allocation, training, and management during the peak of the pandemic. These studies shed light on the various measures implemented to enhance the efficiency of human resources and prevent the transmission of infection.
To effectively respond to the crisis, healthcare facilities established initiatives such as creating a dedicated COVID-19 action group, implementing staff rotation with different teams working in shifts, or dividing the workforce into separate groups for COVID-19 and non-COVID patients [3,9,19]. Some studies also highlighted the adoption of reduced staffing strategies to preserve the workforce and prevent fatigue in hospitals and clinics [2,14,15,24]. Additionally, all out-station leaves of healthcare workers were suspended to prevent community spread and ensure the maximum availability of the workforce [2]. Staff members arriving from areas declared as containment zones were granted paid leaves to mitigate the risk of cross-infection. Furthermore, operation theatres were observed to operate with minimal staff, organised into teams or shifts [24].
However, despite these measures, instances of human resource constraints were reported, particularly when older or pregnant staff members were relieved from high-risk duties [30]. The existing staff faced the challenge of balancing their time between designing and implementing new interventions and providing essential care.
The implementation of infection prevention guidelines also led to the further quarantining of staff, which contributed to reduced availability of personnel at any given time. Both private and public healthcare providers underwent adequate quarantine measures in cases of incidental exposure or if they were working in isolation wards or had any form of exposure to COVID-19 [3,9,12,16,18,19,20,24,29]. In order to ensure preparedness and adherence to protocols, mandatory trainings were conducted for all staff and doctors at healthcare institutions. These trainings covered various aspects such as infection control, sanitisation, proper usage of personal protective equipment (PPE), and the correct donning and doffing procedures for PPE. Several studies highlighted the importance of these trainings in effectively managing COVID-19 patients and following established protocols [5,6,9,16,18,30].
- d)
- Personal Protective Equipment (PPE)
The use and challenges related to Personal Protective Equipment (PPE) are discussed in 21 studies included in this analysis [2,3,4,5,6,7,8,9,10,11,12,13,14,15,20,21,25,29,30,31,32], involving 14,544 participants. According to these studies, a significant number of healthcare providers (HCPs) utilised appropriate PPE [3,4,5,7,9,13,15,25,29] during consultations, surgeries, and other healthcare services. While the use of PPE became widespread, specific instances, predicaments, and challenges emerged.
A common-sense, rationed approach to using resources like PPE during a pandemic of this magnitude is being followed cautiously in India and worldwide. Most practitioners felt that complete PPE needed to be reserved for workers dealing with high-risk patients [25]. While this seems to be a reasonable approach, many argue that primary care providers are also known to be at an increased risk, especially during epidemics. If the allocation of PPE limits the provision of N95 masks to only those HCPs directly involved in the management of confirmed COVID-19 cases [25], HCPs in resource-constrained settings working in enclosed small spaces without adequate ventilation and likely overcrowded, are rendered highly vulnerable to COVID-19 in the absence of adequate PPE provision. PPE suits, N-95 masks, and surgical masks were available at only 27%, 50% and 39% of primary health care sites, respectively. Besides this, the unavailability and short supply of adequate quality PPE were rife issues, as reported in a plethora of included studies [6,10,12,20,21,29,32].
Several other studies have shed light on the challenges associated with donning PPE, especially during surgical procedures, such as the occurrence of eyewear/face shield misting and the discomfort caused by extreme heat and dehydration [16]. Additionally, disinfecting PPE in settings with limited resources and space has proven to be a challenge [30]. A significant number of respondents (85%) indicated that the maximum tolerable duration for wearing PPE ranged from 1 to 4 hours [21].
- e)
- Preoperative/OT/post-operative measures
Thirteen studies [2,3,4,7,9,10,14,19,21,24,25,26,33] provide insights into preoperative, intraoperative, and postoperative measures, involving a total of 3,814 participants. Several studies consistently emphasised the necessity of COVID testing for all preoperative patients, ensuring that only those testing negative for the virus proceeded with surgeries [2,19,21]. However, at the onset of the pandemic, there was significant uncertainty and scepticism surrounding preoperative procedures. For instance, an early study [4] revealed that the majority of clinicians (63%) were uncertain about the appropriate course of action and were eagerly awaiting guidelines regarding preoperative screening. Another study [10] highlighted a similar predicament during the initial phase, as the recommendations by the Government of India did not initially allow for preoperative COVID-19 testing, making it challenging to make decisions regarding surgery based on COVID-19 status. This ambiguity surrounding preoperative testing and procedures was widely observed during the early stages of the pandemic.
In addition to preoperative testing, certain institutions implemented changes in their surgical strategies and techniques. For instance, an ophthalmological study reported modifications in their operation theatre (OT) sterilisation protocol [24]. Furthermore, some surgeons adopted the use of a "heads-up" 3D visualisation system during vitreoretinal surgery to increase the distance between the surgeon and the patient, thereby minimising the risk of exposure. Additionally, in several settings, strict precautions were taken upon admitting patients, allowing only one attendant [3,14,19]. In the field of oncology, studies highlighted the use of neoadjuvant chemotherapy as an alternative to upfront surgery, which deviated from the standard of care but served as a viable option when resources were constrained during the pandemic [3,9,25,26,33].
In addition to preoperative testing, certain institutions implemented changes in their surgical strategies and techniques. For instance, an ophthalmological study reported modifications in their operation theatre (OT) sterilisation protocol [24]. Furthermore, some surgeons adopted the use of a "heads-up" 3D visualisation system during vitreoretinal surgery to increase the distance between the surgeon and the patient, thereby minimising the risk of exposure. Additionally, in several settings, strict precautions were taken upon admitting patients, allowing only one attendant [3,14,19]. In the field of oncology, studies highlighted the use of neoadjuvant chemotherapy as an alternative to upfront surgery, which deviated from the standard of care but served as a viable option when resources were constrained during the pandemic [3,9,25,26,33].
- f)
- Physical infrastructure and resources
Seven studies [3,6,9,14,16,20,30] involving 4,024 subjects have documented modifications in infrastructure and resources. These changes aimed to establish COVID-safe environments in buildings, wards, operating rooms (ORs), and other facilities. Examples of these adaptations included allocating a separate building for managing COVID-19 patients [3,16], employing engineering controls like physical barriers, curtains, or partitions [14,16], establishing distinct entrances for patients and healthcare providers, creating dedicated spaces for COVID-suspects (holding areas), designating separate areas for donning and doffing PPE. Furthermore, efforts were made to maintain a minimum distance of 1.5 meters between beds and ensure proper ventilation and air conditioning in wards, ICUs, operating rooms, and other areas [16]. Even in resource-limited healthcare settings, various modifications have been made to existing infrastructure [30]. These include allocating waiting areas and designated hand wash zones, shifting consultation rooms to open spaces, and implementing visual triage to screen patients for COVID-19. Isolated fever clinics were also established to provide specialised care.
Besides these adaptations, several changes were made in the processes. For instance, surgical procedures in operating rooms were spaced out with sufficient time intervals to ensure proper sterilisation [9]. Solutions were implemented to cohort COVID-positive patients or suspected cases, including the creation of isolation rooms and dedicated shifts [20]. Furthermore, adjustments were made to resources, such as increasing the hospital's oxygen capacity and procuring respiratory support devices [16], in response to the increased demand for oxygen during the COVID-19 pandemic.
3.2.3. Impact of pandemic on healthcare providers and individuals/communities
- a)
- Impact on health care providers
- ▪
- Depression, stress, anxiety, and burnout in health care providers
Fourteen studies [3,4,6,9,11,12,14,21,29,30,31,32,34,35] examined the mental health status of healthcare providers (HCPs), involving 8,568 participants. These studies revealed a significant prevalence of pandemic-related stress and burnout among HCPs. Approximately 33% to 35% of HCPs [29,35] experienced depression, surpassing the prevalence of 10% for common mental disorders in the general population of India [35]. A specific study [30] conducted on frontline workers in slums depicted the emotional toll of working in precarious conditions that filled these workers with uncertainties. Factors contributing to stress and anxiety among healthcare providers included a lack of confidence in effectively segregating patients, concerns about the availability of adequate PPE, working fully clad in PPE for long hours, and insufficient administrative support from institutions [6,21,30,32].
- ▪
- Fear of contracting infection and carrying it at home
The fear of contracting and transmitting the infection has been addressed in six studies [3,4,30,31,32,35], involving 6,176 participants. Among HCPs caring for COVID-19 patients, approximately 55% expressed fear of contracting the infection themselves, while an even higher percentage (67%) feared transmitting it to their families [31]. In the study conducted by Wilson et al. [32], a significant majority of HCPs (78%) across ten states and one union territory expressed serious concerns about infecting their friends or family members. Similarly, healthcare workers serving in the community health division of a hospital and working in a large slum [30], emphasised the primary concern of transmitting the infection to vulnerable family members, such as the elderly, immune-compromised individuals, or those with chronic medical conditions. Depression among HCPs has also been identified as a consequence of their fear of transmitting the infection to their families in studies conducted by Khanna et al. [35] and Wilson et al. [32].
- ▪
- Stigmatisation
Stigmatisation targeting healthcare providers (HCPs) has been documented in five studies [9,29,30,31,35], involving 5,173 participants (Table 1). A significant proportion of HCPs in a comprehensive survey (26.6%) reported feeling unwelcome in their communities [31]. The studies conducted in both community and hospital settings [9,29,30] highlighted that healthcare workers were perceived as carriers of infection and often faced ostracisation from friends, neighbours, and society as a self-protective measure This stigmatisation had negative impacts on the mental well-being of HCPs, leading to feelings of depression, stress, and anxiety [29,31,35].
- ▪
- Financial impact
The adverse impact of the pandemic on the financial status of healthcare practitioners is documented in five studies [3,7,23,32,35], involving 3,489 participants. A survey conducted on 433 healthcare providers in ten states and one Union Territory of India revealed that a significant majority (82%) of healthcare providers experienced financial harm due to the pandemic [32]. Over 70% of the healthcare providers reported a decrease of more than 50% in their monthly income [6]. The financial burden caused by the pandemic was more pronounced among private practitioners and those with multiple affiliations, compared to those in government jobs (P = 0.000) [7,32]. Furthermore, approximately 28% to 33% of respondents who owned hospitals anticipated a monthly financial liability of $30,000 or expected their income to decline by more than 90%. Surgeons with more years of practice, specifically those with 20 to 30 years or more than 30 years of experience, were particularly affected compared to their younger counterparts [23].Top of FormBottom of Form
- b)
- Effect of pandemic on healthcare seekers
Eleven studies [5,8,9,17,19,28,33,36,37,38,39] involving 5,611 participants examined the effects of the pandemic on the physical and mental health of individuals. These studies highlighted various impacts on disease progression, disease status, lifestyle factors such as physical activity and diet, and medication adherence.
For instance, among diabetic patients, there was an observed increase in missed insulin doses (27%) [17], irregular blood glucose monitoring (28%-39%)[17,36] reduced engagement in regular physical activities ( (37%) [17], and decreased compliance with dietary guidelines (17%) [17] etc. These factors resulted in elevated average blood glucose and HbA1c levels, a higher incidence of hyperglycaemic episodes (37%), and an increased rate of hospitalisations (8%) [17]. Regarding cancer patients, they encountered challenges such as limited availability of chemotherapy slots (56%), long waiting hours despite scheduled appointments (22%), postponed surgeries (14%) and tumour board meetings (20%), delays in teleconsultations (42%) and nutritionist advice (89%), and unavailability of chemotherapy medications (22%) among others [19,33].
Widespread fear was observed among patients [2,19,33,39] due to the heightened risk of infection associated with their existing conditions and concerns about the worsening of their underlying diseases due to delayed or suboptimal treatment. A large majority of respondents also faced significant transportation challenges arising from strict lockdown conditions [5,9,13].
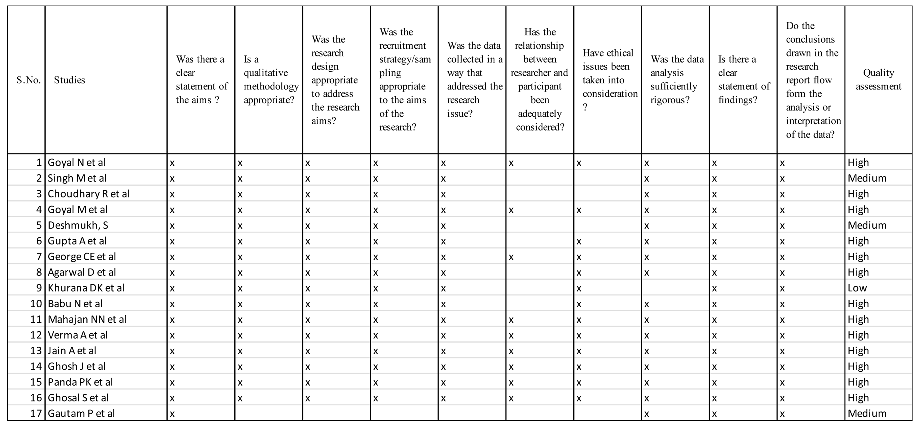
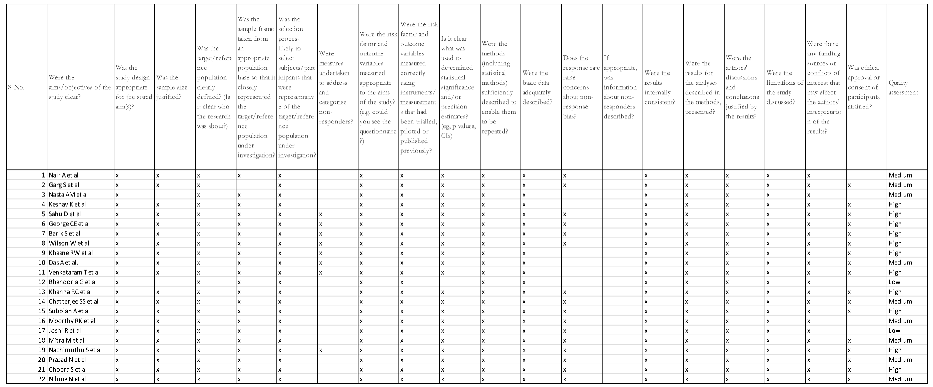
3.3. Quality appraisal of included studies
The quality of the primary studies included in this review is assessed using two tools: the CASP (Critical appraisal skills programme) checklist for qualitative (observational) studies and AXIS critical Appraisal tool for cross sectional Studies. Both tools have been adapted for use in this review.
Among the 16 observational studies, the overall quality ranges from high to low. Specifically, 13 studies are rated as high quality, 3 studies are considered to be of moderate quality, and 1 study is assessed as low quality. Similarly, among the 21 cross-sectional surveys, the overall quality varies from high to low (Appendix 1a). Of these surveys, 11 are classified as high quality, 9 are deemed to be of moderate quality, and 2 are evaluated as low quality (Appendix 1b). In addition, there is one mixed-method qualitative study that incorporates both observational methodology and cross-sectional survey components. This study undergoes assessment using both tools and is determined to be of high quality.
4. Discussion
This review examines the impact of COVID-19 on health services and the health system's response in India during the first wave and its aftermath. It explores the initial stumbling and disruption of the system, highlighting sudden and urgent instances of imbalance, resource strain, and coordination challenges. It also sheds light on subsequent adaptations and efforts that were made with a sense of urgency to effectively address COVID-19 while at the same time striving to maintain and deliver essential health services. The review offers valuable lessons for future preparedness and identifies areas for improvement in building a resilient healthcare system capable of managing similar sudden and unprecedented crises.
This review is based on primary studies conducted in different Indian health care settings to keep the analysis based on robust research and first-hand evidence.
Consistent findings across multiple studies included in this review indicate a significant reduction in outpatient department (OPD) services during the initial lockdown phase and subsequent months. Notably, noncommunicable diseases (NCDs) and immunisation clinics were particularly affected, while general OPDs experienced relatively fewer disruptions. Elective procedures across diverse healthcare areas were either completely halted or significantly scaled back, leading to delays and postponements in treatment. Despite these challenges, emergency services persevered, albeit with difficulties in accessibility, transport, and resource constraints.
These findings align with a comprehensive survey conducted by the World Health Organisation (WHO) across 155 countries during a similar time frame, which highlighted severe interruptions in prevention and treatment services for non-communicable diseases (NCDs) as countries transitioned from sporadic cases to community transmission of the coronavirus [40].
A comprehensive systematic review conducted in multi-country settings [41] during that time further substantiates our findings, revealing a significant reduction in healthcare utilisation across various populations and countries. This reduction was particularly pronounced among individuals with less severe illnesses, in line with our observation of disrupted elective and essential services for less severe conditions, which experienced substantial declines. Conversely, emergency services for severe illnesses persisted, albeit with necessary adaptations. Furthermore, a study [42] conducted in the United States provides additional support for these findings, demonstrating a marked decrease in medical admissions during the COVID-19 outbreak in March and April 2020 across diverse patient groups. The study also emphasises the significance of long-term research to fully understand the implications of avoiding hospitalisation during the pandemic on patients' mortality, morbidity, and quality of life, a consideration extensively discussed and observed in the included studies of this review.
In addition to evaluating the impact on health services, our study sheds light on the level of preparedness and various adaptations undertaken by healthcare facilities, encompassing staff management, resource allocation, and infrastructure modifications. These findings from our review are consistent with studies conducted in different settings and geographies during this phase of the pandemic. For instance, a study in Ireland found that healthcare infrastructures were reconfigured to facilitate the pandemic response, including the construction of structures to separate patients and the strengthening of triage systems [43]. Similarly, an analysis of datasets and literature reviews in England showed that hospitals implemented interventions to manage patient admissions and increase resource availability, including the cancellation of elective surgeries and the deployment of additional medical personnel [44]. Likewise, a National Survey conducted in the US reported comparable adaptations such as the establishment of dedicated respiratory isolation units, expanded use of inpatient telehealth, and strategies to minimise room entry [45]. These consistent findings highlight the similar efforts made to address the challenges posed by the pandemic across various healthcare settings.
Furthermore, the aforementioned survey [45], a large-scale study conducted in nursing homes across the US [46], and a prospective observational cohort study [47] conducted in both the UK and the US focusing on frontline healthcare workers, all highlighted the concerning insufficiency of personal protective equipment (PPE) and the widespread practice of reusing PPE. These findings closely align with the conclusions drawn from our review, emphasising the critical shortage of PPE and the desperate need to reuse it.
Another significant finding of our study is the prevalence of pandemic-related stress and burnout among healthcare providers (HCPs). HCPs, (including doctors, nurses, paramedics, and administrative staff), who cared for COVID-19 patients, feared contracting and transmitting the infection to their families. Similar findings have emerged in other studies conducted in diverse multi-country settings. For instance, an observational cohort multicentre study in acute hospital settings in the South-East of Ireland [48] highlighted the scarcity of research focusing on mental health issues during the pandemic and found a notable prevalence of psychological distress among HCPs in those settings. On similar lines, a systematic review during the time in selected Asian countries [49] examined viral epidemic outbreak studies and concluded that the prevalence of anxiety, depression, acute and PTSD, and burnout was high during and after outbreaks; with problems having a long-lasting effect on the mental health of HCPs.
Furthermore, our study observed instances of stigmatisation against HCPs, which is consistent with the statement released by the International Committee of the Red Cross (ICRC) [50], reporting over 600 incidents of violence, harassment, or stigmatisation targeting healthcare providers, patients, and medical infrastructure in relation to the COVID-19 pandemic.
While the review highlights the research and evidence-based picture of the challenges posed by the pandemic and the response to it, it is crucial to acknowledge the inherent limitations within the primary studies included. These studies were conducted during the early stages of the pandemic, necessitating careful consideration of the spatial and temporal aspects of the findings. Extrapolating the review's findings to a different time period or phase of the pandemic may contradict them and limit their generalisability. Furthermore, the contextual nature of the findings within Indian settings prevents their direct applicability to other countries.
The majority of the studies aimed to assess changes in the status of health services across different health conditions and levels, considering the immense and sudden pressures faced by the health system. Due to the rapidly evolving situation, limited attention was given to meticulous sample selection methods and research study design. Consequently, all the studies relied on cross-sectional surveys with purposefully selected samples. While this approach may have compromised the robustness of the evidence collected, it effectively captured the sudden impact of the pandemic on various health services, especially when timely evidence was crucial for interventions. Additionally, the study faced other limitations, including the inability to conduct a meta-analysis due to significant heterogeneity in the included studies, the potential exclusion of important data sources such as studies with smaller sample sizes, reports, and subjectivity in our outcome assessments.
5. Conclusions
In conclusion, this study sheds light on the profound and sudden impact of COVID-19 on health services during the initial wave, resulting in disruptive effects on OPD and elective services and raising concerns about suboptimal emergency care. The healthcare system promptly responded by implementing quick and possible adaptations in staff management, resource allocation, and infection prevention. These valuable findings and insights provide essential knowledge to enhance our understanding of the necessary measures, approaches, and level of preparedness required to build resilient health systems. Incorporating these insights into future strategies will ensure that the health system is well-prepared and resilient in effectively addressing similar crises proactively.
Furthermore, the study underscores the significant toll on the mental health and well-being of healthcare providers, who endured unparalleled challenges and resource constraints. It also illuminates the widespread concerns and fears amongst healthcare seekers, particularly regarding the worsening of their underlying diseases or conditions due to significant delays, formidable barriers, and suboptimal services for diagnosis, treatment, and follow-up.
To mount an effective response to future similar emergencies, it is imperative to prioritise the readiness and preparedness of the health system. This involves adopting agile and efficient strategies to strengthen healthcare infrastructure, optimise resource allocation, and implement comprehensive protocols. Timely public health campaigns that address the concerns of healthcare seekers in such emergencies and the implementation of supportive organisational measures for healthcare providers are vital. By placing emphasis on these aspects, we can proactively enhance the resilience of the health system, ensuring improved outcomes in times of crisis.
Supplementary Materials
The protocol registered on PROSPERO can be downloaded at: - https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=227327
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualisation, A.S.C., K.S., R.B. and S.K.; methodology, A.S.C., K.S., R.B. and S.K. software, A.S.C., A.N.; validation, K.S., R.B. and S.K.; formal analysis, A.S.C., A.N.; investigation, A.S.C., A.N.; resources, K.S., R.B. and S.K.; data curation, A.S.C. A.N.; writing—original draft preparation, A.S.C.; writing—review and editing, A.S.C., K.S., R.B. and S.K; visualisation, A.S.C., A.N.; supervision, A.S.C., K.S., R.B. and S.K.; project administration, A.S.C., K.S., R.B. and S.K.; funding acquisition, A.S.C, K.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Asian Development Bank (47354-003)
Institutional Review Board Statement
This review is a part of research approved by Human Research Ethics Committee—Ethics committee of Delhi - Sigma-IRB (Institutional Review Board)-IRB Approved date/number—14.12.2020/10044/IRB/D/20-21.
Informed Consent Statement
Not applicable
Data Availability Statement
The data used in this review are derived from published literature and publicly available sources. No additional data sets were generated or analysed specifically for this review. All references and sources cited in this review are provided for transparency and accessibility.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Appendix A.1. Quality appraisal of observational studies using adapted CASP checklist
Appendix A.2. Quality appraisal of cross-sectional surveys using adapted JBI tool
References
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Goyal, N.; Venkataram, T.; Singh, V.; Chaturvedi, J. Collateral Damage Caused by COVID-19: Change in Volume and Spectrum of Neurosurgery Patients. J Clin Neurosci 2020, 80, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Gautam, P.; Gandhi, V.; Naik, S.; Mane, A.; Kanitkar, G.; Hegde, S.; Deshmukh, S. Cancer Care in a Western Indian Tertiary Centre during the Pandemic: Surgeon’s Perspective. J Surg Oncol 2020, 122, 1525–1533. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.G.; Gandhi, R.A.; Natarajan, S. Effect of COVID-19 Related Lockdown on Ophthalmic Practice and Patient Care in India: Results of a Survey. Indian J Ophthalmol 2020, 68, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Sanghavi, P.; Patel, B.; Umrania, R.; Chishi, K.; Ghoghari, M. Experience of Palliative Care Services at Tertiary Comprehensive Cancer Centre during COVID-19 Lockdown Phase: An Analytical Original Study. Indian J Palliat Care 2020, 26, S27–S30. [Google Scholar] [CrossRef] [PubMed]
- Garg, S.; Basu, S.; Rustagi, R.; Borle, A. Primary Health Care Facility Preparedness for Outpatient Service Provision During the COVID-19 Pandemic in India: Cross-Sectional Study. JMIR Public Health Surveill 2020, 6, e19927. [Google Scholar] [CrossRef]
- Nasta, A.M.; Goel, R.; Kanagavel, M.; Easwaramoorthy, S. Impact of COVID-19 on General Surgical Practice in India. Indian J Surg 2020, 82, 259–263. [Google Scholar] [CrossRef]
- Goyal, M.; Singh, P.; Singh, K.; Shekhar, S.; Agrawal, N.; Misra, S. The Effect of the COVID-19 Pandemic on Maternal Health Due to Delay in Seeking Health Care: Experience from a Tertiary Centre. Int J Gynaecol Obstet 2021, 152, 231–235. [Google Scholar] [CrossRef]
- Deshmukh, S.; Naik, S.; Zade, B.; Patwa, R.; Gawande, J.; Watgaonkar, R.; Wagh, S.; Deshmukh, S.; Gautam, P.; Gandhi, V.; et al. Impact of the Pandemic on Cancer Care: Lessons Learnt from a Rural Cancer Centre in the First 3 Months. J Surg Oncol 2020, 122, 831–838. [Google Scholar] [CrossRef]
- Gupta, A.; Arora, V.; Nair, D.; Agrawal, N.; Su, Y.-X.; Holsinger, F.C.; Chan, J.Y.K. Status and Strategies for the Management of Head and Neck Cancer during COVID-19 Pandemic: Indian Scenario. Head Neck 2020, 42, 1460–1465. [Google Scholar] [CrossRef]
- Sahu, D.; Agrawal, T.; Rathod, V.; Bagaria, V. Impact of COVID 19 Lockdown on Orthopaedic Surgeons in India: A Survey. J Clin Orthop Trauma 2020, 11, S283–S290. [Google Scholar] [CrossRef] [PubMed]
- Barik, S.; Paul, S.; Kandwal, P. Insight into the Changing Patterns in Clinical and Academic Activities of the Orthopedic Residents during COVID-19 Pandemic: A Cross-Sectional Survey. Knee Surg Sports Traumatol Arthrosc 2020, 28, 3087–3093. [Google Scholar] [CrossRef] [PubMed]
- Khurana, D.K.; Raheja, S.G.; Dayal, M.; Pande, D.; Ganapathy, U. COVID 19: The New Normal in the Clinic: Overcoming Challenges in Palliative Care. Indian J Palliat Care 2020, 26, S81–S85. [Google Scholar] [CrossRef] [PubMed]
- Venkataram, T.; Goyal, N.; Dash, C.; Chandra, P.P.; Chaturvedi, J.; Raheja, A.; Singla, R.; Sardhara, J.; Singh, B.; Gupta, R. Impact of the COVID-19 Pandemic on Neurosurgical Practice in India: Results of an Anonymized National Survey. Neurol India 2020, 68, 595–602. [Google Scholar] [CrossRef]
- Babu, N.; Kohli, P.; Mishra, C.; Sen, S.; Arthur, D.; Chhablani, D.; Baliga, G.; Ramasamy, K. To Evaluate the Effect of COVID-19 Pandemic and National Lockdown on Patient Care at a Tertiary-Care Ophthalmology Institute. Indian J Ophthalmol 2020, 68, 1540–1544. [Google Scholar] [CrossRef]
- Mahajan, N.N.; Pednekar, R.; Patil, S.R.; Subramanyam, A.A.; Rathi, S.; Malik, S.; Mohite, S.C.; Shinde, G.; Joshi, M.; Kumbhar, P.; et al. Preparedness, Administrative Challenges for Establishing Obstetric Services, and Experience of Delivering over 400 Women at a Tertiary Care COVID-19 Hospital in India. Int J Gynaecol Obstet 2020, 151, 188–196. [Google Scholar] [CrossRef]
- Verma, A.; Rajput, R.; Verma, S.; Balania, V.K.B.; Jangra, B. Impact of Lockdown in COVID 19 on Glycemic Control in Patients with Type 1 Diabetes Mellitus. Diabetes Metab Syndr 2020, 14, 1213–1216. [Google Scholar] [CrossRef]
- Joshi, R.; Atal, S.; Fatima, Z.; Balakrishnan, S.; Sharma, S.; Joshi, A. Diabetes Care during COVID-19 Lockdown at a Tertiary Care Centre in India. Diabetes Res Clin Pract 2020, 166, 108316. [Google Scholar] [CrossRef]
- Mitra, M.; Basu, M. A Study on Challenges to Health Care Delivery Faced by Cancer Patients in India During the COVID-19 Pandemic. J Prim Care Community Health 2020, 11, 2150132720942705. [Google Scholar] [CrossRef]
- Prasad, N.; Bhatt, M.; Agarwal, S.K.; Kohli, H.S.; Gopalakrishnan, N.; Fernando, E.; Sahay, M.; Rajapurkar, M.; Chowdhary, A.R.; Rathi, M.; et al. The Adverse Effect of COVID Pandemic on the Care of Patients With Kidney Diseases in India. Kidney Int Rep 2020, 5, 1545–1550. [Google Scholar] [CrossRef]
- Moorthy, R.K.; Rajshekhar, V. Impact of COVID-19 Pandemic on Neurosurgical Practice in India: A Survey on Personal Protective Equipment Usage, Testing, and Perceptions on Disease Transmission. Neurol India 2020, 68, 1133–1138. [Google Scholar] [CrossRef] [PubMed]
- Rahul Choudhary; Dinesh Gautam; Rohit Mathur; Dinesh Choudhary Management of Cardiovascular Emergencies during the COVID-19 Pandemic. Emerg Med J 2020, 37, 778. [CrossRef]
- Keshav, K.; Kumar, A.; Sharma, P.; Baghel, A.; Mishra, P.; Huda, N. How Much Has COVID-19 Pandemic Affected Indian Orthopaedic Practice? Results of an Online Survey. Indian J Orthop 2020, 54, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, D.; Chawla, R.; Varshney, T.; Shaikh, N.; Chandra, P.; Kumar, A. Managing Vitreoretinal Surgeries during COVID-19 Lockdown in India: Experiences and Future Implications. Indian Journal of Ophthalmology 2020, 68, 2126–2130. [Google Scholar] [CrossRef] [PubMed]
- Bhandoria, G.; Shylasree, T.S.; Bhandarkar, P.; Ahuja, V.; Maheshwari, A.; Sekhon, R.; Somashekhar, S.P. Impact of COVID-19 Pandemic on Gynecological Oncology Care: Glimpse into Association of Gynecological Oncologists of India (AGOI) Perspective. Indian J Gynecol Oncol 2020, 18, 71. [Google Scholar] [CrossRef]
- Subbian, A.; Kaur, S.; Patel, V.; Rajanbabu, A. COVID-19 and Its Impact on Gynaecologic Oncology Practice in India-Results of a Nationwide Survey. Ecancermedicalscience 2020, 14, 1067. [Google Scholar] [CrossRef]
- Panda, P.K.; Dawman, L.; Panda, P.; Sharawat, I.K. Feasibility and Effectiveness of Teleconsultation in Children with Epilepsy amidst the Ongoing COVID-19 Pandemic in a Resource-Limited Country. Seizure 2020, 81, 29–35. [Google Scholar] [CrossRef]
- Jain, A.; Goyal, V.; Varma, C. Reflection of Epidemiological Impact on Burden of Injury in Tertiary Care Centre, Pre-COVID and COVID Era: “Lockdown, a Good Fortune for Saving Life and Limb”. Indian J Surg 2021, 83, 139–143. [Google Scholar] [CrossRef]
- Chatterjee, S.S.; Bhattacharyya, R.; Bhattacharyya, S.; Gupta, S.; Das, S.; Banerjee, B.B. Attitude, Practice, Behavior, and Mental Health Impact of COVID-19 on Doctors. Indian J Psychiatry 2020, 62, 257–265. [Google Scholar] [CrossRef]
- George, C.E.; Inbaraj, L.R.; Rajukutty, S.; de Witte, L.P. Challenges, Experience and Coping of Health Professionals in Delivering Healthcare in an Urban Slum in India during the First 40 Days of COVID-19 Crisis: A Mixed Method Study. BMJ Open 2020, 10, e042171. [Google Scholar] [CrossRef]
- Khasne, R.W.; Dhakulkar, B.S.; Mahajan, H.C.; Kulkarni, A.P. Burnout among Healthcare Workers during COVID-19 Pandemic in India: Results of a Questionnaire-Based Survey. Indian J Crit Care Med 2020, 24, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Wilson, W.; Raj, J.P.; Rao, S.; Ghiya, M.; Nedungalaparambil, N.M.; Mundra, H.; Mathew, R. Prevalence and Predictors of Stress, Anxiety, and Depression among Healthcare Workers Managing COVID-19 Pandemic in India: A Nationwide Observational Study. Indian J Psychol Med 2020, 42, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, J.; Ganguly, S.; Mondal, D.; Pandey, P.; Dabkara, D.; Biswas, B. Perspective of Oncology Patients During COVID-19 Pandemic: A Prospective Observational Study From India. JCO Glob Oncol 2020, 6, 844–851. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Sil, A.; Jaiswal, S.; Rajeev, R.; Thole, A.; Jafferany, M.; Ali, S.N. A Study to Evaluate Depression and Perceived Stress Among Frontline Indian Doctors Combating the COVID-19 Pandemic. Prim Care Companion CNS Disord 2020, 22, 20m02716. [Google Scholar] [CrossRef] [PubMed]
- Khanna, R.C.; Honavar, S.G.; Metla, A.L.; Bhattacharya, A.; Maulik, P.K. Psychological Impact of COVID-19 on Ophthalmologists-in-Training and Practising Ophthalmologists in India. Indian J Ophthalmol 2020, 68, 994–998. [Google Scholar] [CrossRef] [PubMed]
- Nachimuthu, S.; Vijayalakshmi, R.; Sudha, M.; Viswanathan, V. Coping with Diabetes during the COVID - 19 Lockdown in India: Results of an Online Pilot Survey. Diabetes Metab Syndr 2020, 14, 579–582. [Google Scholar] [CrossRef]
- Ghosal, S.; Arora, B.; Dutta, K.; Ghosh, A.; Sinha, B.; Misra, A. Increase in the Risk of Type 2 Diabetes during Lockdown for the COVID19 Pandemic in India: A Cohort Analysis. Diabetes Metab Syndr 2020, 14, 949–952. [Google Scholar] [CrossRef]
- Nilima, N.; Kaushik, S.; Tiwary, B.; Pandey, P.K. Psycho-Social Factors Associated with the Nationwide Lockdown in India during COVID- 19 Pandemic. Clin Epidemiol Glob Health 2021, 9, 47–52. [Google Scholar] [CrossRef]
- Chopra, S.; Ranjan, P.; Singh, V.; Kumar, S.; Arora, M.; Hasan, M.S.; Kasiraj, R.; Suryansh; Kaur, D. ; Vikram, N.K.; et al. Impact of COVID-19 on Lifestyle-Related Behaviours- a Cross-Sectional Audit of Responses from Nine Hundred and Ninety-Five Participants from India. Diabetes Metab Syndr 2020, 14, 2021–2030. [Google Scholar] [CrossRef]
- World Health Organisation. COVID-19 Significantly Impacts Health Services for Noncommunicable Diseases. Available online: https://www.who.int/news/item/01-06-2020-covid-19-significantly-impacts-health-services-for-noncommunicable-diseases.
- Ray Moynihan; Sharon Sanders; Zoe A Michaleff; Anna Mae Scott; Justin Clark; Emma J To; Mark Jones; Eliza Kitchener; Melissa Fox; Minna Johansson; et al. Impact of COVID-19 Pandemic on Utilisation of Healthcare Services: A Systematic Review. BMJ Open 2021, 11, e045343. [Google Scholar] [CrossRef]
- Birkmeyer, J.D.; Barnato, A.; Birkmeyer, N.; Bessler, R.; Skinner, J. The Impact Of The COVID-19 Pandemic On Hospital Admissions In The United States. Health Aff (Millwood) 2020, 39, 2010–2017. [Google Scholar] [CrossRef]
- Conlon, C.; McDonnell, T.; Barrett, M.; Cummins, F.; Deasy, C.; Hensey, C.; McAuliffe, E.; Nicholson, E. The Impact of the COVID-19 Pandemic on Child Health and the Provision of Care in Paediatric Emergency Departments: A Qualitative Study of Frontline Emergency Care Staff. BMC Health Services Research 2021, 21, 279. [Google Scholar] [CrossRef]
- McCabe, R.; Schmit, N.; Christen, P.; D’Aeth, J.C.; Løchen, A.; Rizmie, D.; Nayagam, S.; Miraldo, M.; Aylin, P.; Bottle, A.; et al. Adapting Hospital Capacity to Meet Changing Demands during the COVID-19 Pandemic. BMC Medicine 2020, 18, 329. [Google Scholar] [CrossRef]
- Auerbach, A.; O’Leary, K.J.; Greysen, S.R.; Harrison, J.D.; Kripalani, S.; Ruhnke, G.W.; Vasilevskis, E.E.; Maselli, J.; Fang, M.C.; Herzig, S.J.; et al. Hospital Ward Adaptation During the COVID-19 Pandemic: A National Survey of Academic Medical Centres. J Hosp Med 2020, 15, 483–488. [Google Scholar] [CrossRef]
- McGarry, B.E.; Grabowski, D.C.; Barnett, M.L. Severe Staffing And Personal Protective Equipment Shortages Faced By Nursing Homes During The COVID-19 Pandemic. Health Aff (Millwood) 2020, 39, 1812–1821. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.-G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.-H.; et al. Risk of COVID-19 among Front-Line Health-Care Workers and the General Community: A Prospective Cohort Study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Ali, S.; Maguire, S.; Marks, E.; Doyle, M.; Sheehy, C. Psychological Impact of the COVID-19 Pandemic on Healthcare Workers at Acute Hospital Settings in the South-East of Ireland: An Observational Cohort Multicentre Study. BMJ Open 2020, 10, e042930. [Google Scholar] [CrossRef]
- Serrano-Ripoll, M.J.; Meneses-Echavez, J.F.; Ricci-Cabello, I.; Fraile-Navarro, D.; Fiol-deRoque, M.A.; Pastor-Moreno, G.; Castro, A.; Ruiz-Pérez, I.; Zamanillo Campos, R.; Gonçalves-Bradley, D.C. Impact of Viral Epidemic Outbreaks on Mental Health of Healthcare Workers: A Rapid Systematic Review and Meta-Analysis. J Affect Disord 2020, 277, 347–357. [Google Scholar] [CrossRef]
- Devi, S. COVID-19 Exacerbates Violence against Health Workers. The Lancet 2020, 396, 658. [Google Scholar] [CrossRef]
Figure 1.
PRISMA Flow diagram.
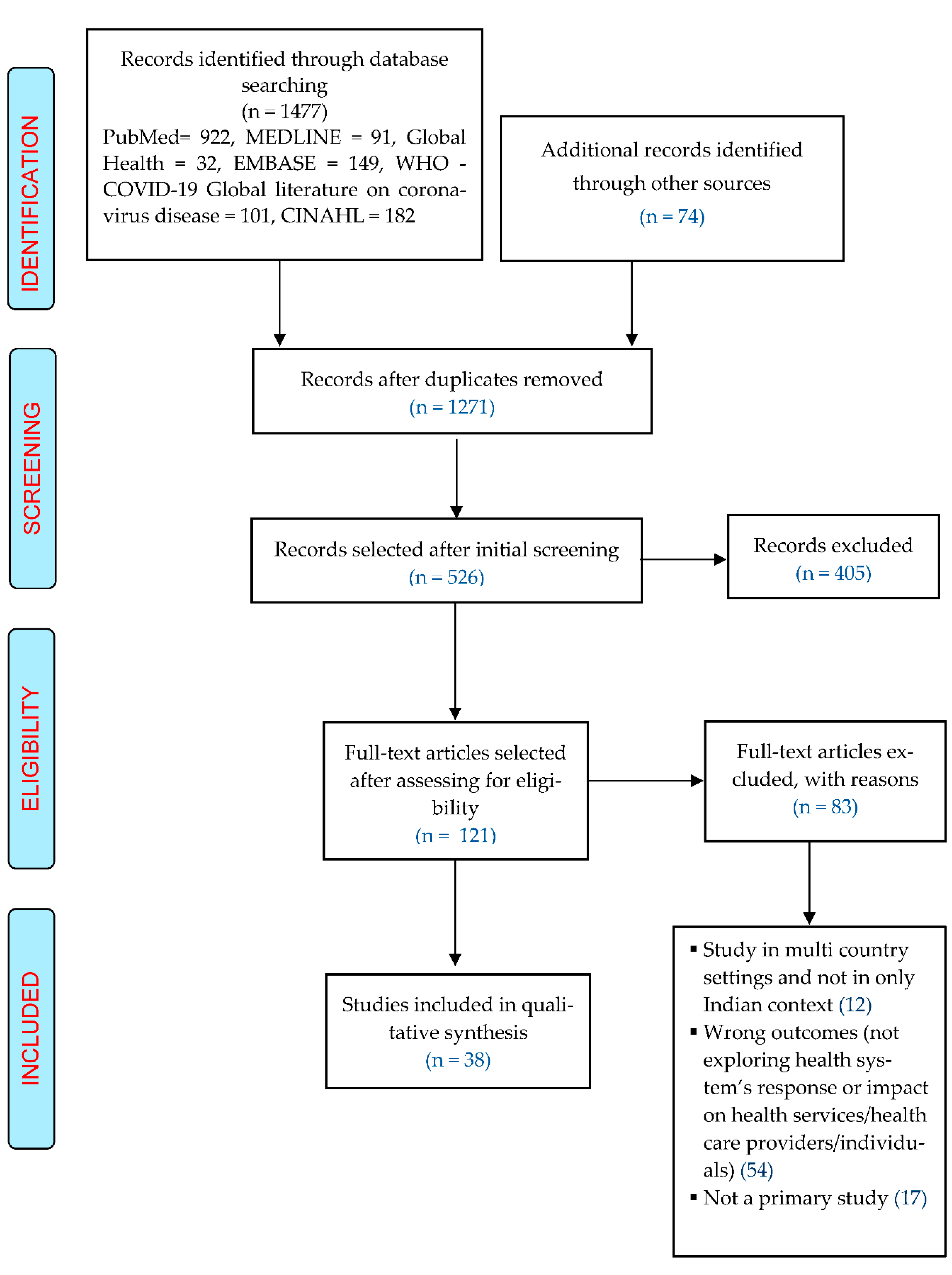

Table 1.
Characteristics of included studies.
| S.no. | Author | Area of work | Participants | No. of Participants | Setting/context |
|---|---|---|---|---|---|
| Gautam P et al | Cancer care | Onco-surgeons | 15 | A tertiary care centre, Pune | |
| Goyal N et al | Neurosurgery | Patients operated under the Department of Neurosurgery since the onset of pandemic | 164 | The Department of Neurosurgery, All India Institute of Medical Sciences, Uttarakhand institute | |
| Nair A et al | Ophthalmic practice | Ophthalmologists | 1260 | Online survey of ophthalmologists from Private clinics, ophthalmic institutes, corporate/multi-specialty hospitals, government/municipal hospitals, freelancing surgeons | |
| Singh M et al | Palliative Cancer care | Patients availing palliative care service | 1161 | Department of pain and palliative medicine in a tertiary comprehensive Cancer centre, Gujarat. | |
| Garg S et al | Primary health care | Supervisors and managers of primary health care facilities | 51 | Primary health care facilities attached to medical colleges and institutions anywhere in India, either in the government or private setting. | |
| Nasta AM et al | General Surgical practice | Surgeons (members of Indian Association of Gastro-intestinal Endo-surgeons -IAGES) | 153 | Online survey of members of Indian Association of Gastro-intestinal Endo-surgeons (IAGES) | |
| Choudhary R et al | Cardiovascular emergencies | Patients presenting with cardiovascular emergencies | 289 | Four tertiary regional emergency departments in western India | |
| Goyal M et al | Maternal health | Pregnant women | 633 | Department of Obstetrics and Gynaecology at All India Institute of Medical Sciences, Jodhpur | |
| Deshmukh, S | Cancer | Cancer patients who underwent surgery, CT, and RT | 553 | A charitable cancer hospital, Pune | |
| Keshav K et al | Orthopaedic Practice | Practicing orthopaedic surgeons | 533 | Online nationwide survey | |
| Gupta A et al | Head and neck cancer | Head and neck health care stakeholders | 16 | Major head and neck health care facilities across India | |
| Sahu D et al | Orthopaedic surgery | Orthopaedic surgeons | 611 | Online nationwide survey | |
| George CE et al | Healthcare services in a large slum | A healthcare team of doctors, nurses, paramedical and support staff. | 87 | Community Health Division, Bangalore Baptist Hospital, Bangalore | |
| Agarwal D et al | Ophthalmology | Patients of vitreoretinal surgery | 86 | A government tertiary eye care hospital | |
| Barik S et al | Orthopaedic | Orthopaedic residents | 158 | Seven tertiary care centres in North India | |
| Khurana DK et al | Patient volume, infection prevention measures | All patients coming to the clinic and inpatient referrals. | 108 | Pain and palliative care unit at a tertiary care hospital | |
| Wilson W et al | Stress, depression, anxiety | HCPs (doctors & nurses) directly involved in the triage, screening, diagnosing, and treatment of COVID-19 patients and suspects. | 433 | Online survey - Ten states and one union territory | |
| Khasne RW et al | Burnout/stress | All HCPs (doctors, nurses, paramedics) looking after COVID-19 patients. | 2026 | Nationwide online survey | |
| Das A et al. | Burnout, stress, workload | Frontline doctors involved in clinical services in OPDs, designated COVID-19 wards, screening blocks, fever clinics, and intensive care units | 422 | Tertiary care hospitals in India | |
| Venkataram T et al | PPE, preoperative testing, burnout | Practising neurosurgeons | 201 | Online nationwide survey | |
| Bhandoria G et al | Guidelines, service, teleconsultation | Gynaecological oncologists | 567 | The Association of Gynaecological Oncologists of India (AGOI). | |
| Babu N et al | Procedures, precautions | Patients presenting to the hospital during COVID-19 lockdown | 3434 | Tertiary care dedicated ophthalmic hospital in Tamil Nadu | |
| Khanna RC et al | Stress and fear | Ophthalmologists and ophthalmology trainees | 2355 | Online nationwide survey | |
| Chatterjee SS et al | Stress and anxiety | Doctors | 152 | Online survey - West Bengal | |
| Subbian A et al | Patient volumes, surgical load, and changes in practice protocols | Healthcare professionals involved in the care of gynaecologic cancer patients | 153 | National online survey | |
| Mahajan NN et al | Protocols,measures, preparedness | Obstetric patients | 600 | Multispecialty tertiary care centre in Mumbai | |
| Moorthy RK et al | PPE use, precautions, change in practices | Neurosurgeons | 244 | Online survey of members of the Neurological Society of India | |
| Verma A et al | Patients health, clinical,behavioural risk factors | Patients with T1DM | 52 | Tertiary care teaching hospital |
|
| Joshi R et al | Patients health, clinical, behavioural risk factors | Individuals with diabetes who needed the follow up consultation | 103 | Telemedicine facility of All India Institute of Medical Sciences Bhopal | |
| Jain A et al | Patients/injuries | Trauma victims presented to trauma centre. | 299 | A tertiary care hospital with level 1 trauma centre and a multidisciplinary 600-bed public hospital in Delhi NCR | |
| Mitra M et al | Patient challenges | Cancer patients in different stages of treatment and follow-up | 100 | A 600-bed multispecialty hospital | |
| Ghosh J et al | Patients’ concerns | All patients age ≥ 18 years who are actively undergoing systemic therapy for solid malignancies |
302 | Department of Medical Oncology | |
| Panda PK et al | Telemedicine/young patients | Caregivers of children suffering from neurological disorders | 153 | Pediatric Neurology Division, All India Institute of Medical Sciences, Rishikesh | |
| Nachimuthu S et al | Adherence to medicine, diet, physical activity | Diabetic patients | 100 | A diabetes speciality hospital in Chennai | |
| Prasad N et al | Patient volume and services/procedures | Director or the heads of the departments | 2517 | 26 public sector tertiary care teaching institutes and private sector corporate hospitals | |
| 36. | Ghosal S et al | Individual health/patient concerns | Non-diabetic household members of T2D patients | 100 | Tertiary care diabetes centre |
| 37. | Chopra S et al | Lifestyle related behaviours | Adults age ≥ 18 years | 995 | Nationwide online survey |
| 38. | Nilima N et al | Community/individual health | People from all the states | 1316 | Nationwide online survey |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



