
Submitted:
26 June 2023
Posted:
27 June 2023
You are already at the latest version
Abstract
Keywords: chronic lymphocytic leukemia; older patient, Bruton tyrosine kinase, BCL2, cost-effectiveness Bruton tyrosine kinase inhibitors (BTKi) and the BCL2 inhibitor venetoclax, with or without the anti CD20 monoclonal antibody Obinutuzumab, represent the preferred options for the first-line therapy of CLL because they are more effective and may improve quality of life. However, pa-tient’s inclusion criteria were heterogeneous across trials designed for older patients and the identification of CLL-specific parameters identifying unfit patients at risk of developing drug-specific adverse events are required to guide treatment choice. Due to inclusion/exclusion criteria in trials, higher discontinuation rates with BTKi were reported in real-world studies and registry analyses provided useful information on factors predicting for earlier discontinuation in a real-world setting. Though targeted agents were shown to be cost-effective treatments in high-income countries, the out-of-pocket expenses may limit accessibility to these drugs and the overall expenditure for new drugs in CLL is projected to increase substantially posing an issue for sustainability. This being said, the choice of a finite duration treatment based on venetoclax containing regimens or treatment until progression with BTKi is today possible in high- income countries and the therapy choice drivers are represented by coexisting medical conditions rather than age, by patient expectations, logistics and sustainability.
Keywords:
chronic lymphocytic leukemia
; older patient
; ibrutinib
; acalabrutinib
; zanubrutinib
; venetoclax
; sustainabiity
1. Introduction
Chronic lymphocytic leukemia (CLL) is one of the most frequent type of leukemia, representing 1% of all cancer cases [1]. The reported incidence is 4.7 cases per 100,000 and the probability of developing CLL during lifetime is of 0.6%, with an estimated number of CLL patients living in United Stated in 2020 of 207,463 [1]. In 2023, 18,740 new CLL were diagnosed in the U.S. with 4,490 deaths [2]. Median age at diagnosis is around 70 years, with the highest percentage of new cases among people aged 65-74 [1] and an estimate 10-year prevalence of 49.8 people per 100,000 inhabitants was reported in the U.K. [3]. Five-year relative survival continuously increased during the past decades [4], with a 5-year relative survival of 88% [1]. Considering the increasing life expectancy of the general population in many countries and the advances in treatment, it is reasonable to predict that the incidence and prevalence of CLL will increase [5].
While for decades the mainstay of CLL treatment was represented by chemotherapy [6], in 2010 the chemoimmunotherapy (CIT) regimen fludarabine, cyclophosphamide and the anti CD20 monoclonal antibody (MoAb) rituximab (FCR) was shown to improve overall survival (OS) and progression free survival (PFS) in fit patients as compared with chemotherapy [7]. Furthermore, durable responses were observed with FCR in up to 2/3 cases with favorable genetic profile, i.e., mutated configuration of the immunoglobulin heavy chain gene (IGHV) and absence of 11q- and TP53 aberrations [8,9]. While FCR became standard of care in young patients, older patients, who are frequently affected by coexistent medical conditions were shown to benefit from CIT regimens combining an anti CD20 MoAb with chlorambucil or bendamustine [10,11,12].
More recently, the treatment of CLL dramatically changed following the demonstration of a significant PFS advantage with Bruton tyrosine kinase inhibitors (BTKi) or with the of BCL-2 inhibitor venetoclax in combination with anti CD20 MoAb as compared with CIT [13,14,15,16]. However, while in young patients the BTK inhibitor ibrutinib was shown to produce an OS advantage over FCR [13] there is no documented OS advantage with these new agents as compared with CIT in the elderly patient.
In this review we summarized and discussed existing evidence on the usage of targeted agents in older patients requiring first line treatment with particular reference to i) the definition of older patient, ii) the efficacy of targeted agents in this patient population and, iii) the cost-effectiveness of targeted therapy.
2. Literature Search
A literature search was performed to identify studies evaluating the role of targeted agents in the upfront treatment of CLL, covering three areas: clinical trial, real world data and cost effectiveness.
We used PubMed as search engine, using MeSH controlled vocabulary as follows: (("Leukemia, Lymphocytic, Chronic, B-Cell"[Mesh]) AND ("ibrutinib" [Supplementary Concept] OR "acalabrutinib" [Supplementary Concept] OR "zanubrutinib" [Supplementary Concept] OR "venetoclax" [Supplementary Concept]). Citations were restricted using PubMed age filter (65+ years) and 458 citations were retrieved, spanning a period from Oct 2012 to March 2023. The manuscripts included in our analysis fulfilled the following inclusion criteria: i) english language; ii) full text paper available; iiia) phase 3 clinical trial or iiib) real world study or iiic) cost effectiveness studies; iv) first-line therapy of CLL; v) elderly or unfit patient population. Paper reporting efficacy data on CIT were excluded. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [17] were used to report the manuscript selection process (Fig 1; supplementary material).
3. The Older Patient
Physiological age is determined not only by chronological age but also by the functional status of each patient, which may take into account the fitness status, as assessed by the presence and severity of comorbidities and organ function and by a comprehensive geriatric assessment (CGA) [18]. Therefore, age is not “per se” a criterion for the choice of the intensity of a given treatment in CLL. Indeed, a cumulative illness Rating Scale (CIRS) score ≥ 6 [19], and/or a creatinine clearance (CrCl) ≤ 70 ml/min were adopted to identify unfit patients to be enrolled in clinical trials of the German Cooperative Study Group (GCLLSG) [20], whereas in other trials an age cut-off ≥65 years, or the presence of existing medical conditions were adopted as main inclusion criteria [15,21,22,23,24]. Thus, the definition of older patient ineligible to fludarabine-based regimen in CLL was heterogeneous across published clinical trials and the impact of coexisting medical conditions or CGA may represent more appropriate tools than age to identify patients eligible to intensive treatment.
3.1. The Impact of Comorbidities
The number of coexisting medical conditions in patients with cancer increases with age, and at CLL diagnosis up to 93% of patients has at least one comorbidity [25]. Patients in the 65-74 year-range carry a median of 3.6 comorbidities [26]. Comorbidities can be quantified with various scores such as the Cumulative Illness Rating Scale (CIRS) [19], Carlson Comorbidity Index (CCI) [27], and the National Cancer Institute (NCI) Comorbidity Index [28].
A CIRS score ≥ 6 at diagnosis was found to be associated with shorter OS independent of CLL-IPI in a cohort of 335 untreated CLL patients treated at a single institution [29]. Interestingly, a retrospective analysis of the Danish CLL register demonstrated that comorbidities at diagnosis were associated with CLL-related mortality at multivariable analysis, with 38% of comorbid patients having died from CLL related causes at a median follow up of 3.3 years [30]. In a prospective US cohort study [25], the impact of comorbidities on mortality was assessed in 1143 patients with newly diagnosed CLL. After a median follow up of 6 years, 225 patients (20%) died and the causes of death were: CLL progression in 46% of the cases, comorbid health conditions in 27%, infection in 8% and or other cancers in 19%. At multivariate analysis, however, CCI score was significantly associated with non CLL-specific mortality and not with CLL-related mortality. The younger age of the US cohort vs the Danish cohort (63 Vs 71 years) may account for this observation. Because CLL or its complications are the leading causes of mortality regardless of CCI score or the number of comorbidities, CLL directed therapies that can be used on elderly and comorbid patients are needed [25,30].
The role of comorbidities as a prognostic factor was evaluated not only in newly diagnosed patients but also at time of treatment. At time of progression requiring treatment with CIT, a simplified, CLL-specific comorbidity index was shown to correlate with survival in CLL [31]. For patients treated with ibrutinib, CIRS score appeared to have a negative impact on OS in 145 patients (80% relapsed/refractory) evaluated retrospectively by Gordon et al. [32], whereas in a similar series including 712 patients (75% relapsed/refractory), CIRS score was predictive of shorter EFS and PFS but not of OS [33].
Appling a machine-learning algorithm in a CLL patient cohort, the most important comorbidities were identified in order to generate the CLL comorbidity index (CLL-CI), which represents a simplified and more specific comorbidity score [34]. The CLL-CI stratified the patients into 3 risk groups based on vascular, endocrine and gastrointestinal comorbidities at time of treatment initiation. The favorable, intermediate and high-risk groups were associated with statistically significant differences in terms of EFS and OS. The CCI-CI was applied at the time of diagnosis and at the time of first line treatment in a large cohort of CLL patient of the Danish CLL register. In this analysis the authors were able to demonstrate that CLL-CI was independently predictive of TTFT, EFS and OS from diagnosis and was associated with shorter EFS and OS from time of first therapy [35].
3.2. The Impact of CGA
CGA represents an accurate evaluation of physiological age [18]. CGA explores multiple domains, including the functional status, physical health, social and environmental issues, and psychological health [36]. Although there is an association between PS and CGA, the latter appears an independent factor, capable of adding information on the functional status of elderly patients with cancer, including patients with a good PS [37].
Applying the CGA to 75 older patients enrolled in the CLL9 trial, 19%, 63%, 49% and 36% of the patients were shown to have an impairment of instrumental activities of daily living (IADLs), physical performance, cognitive ability or high burden of comorbidity, respectively [38]. Interestingly, decreased physical and cognitive capacity were predictive of decreased survival.
Because CGA requires a multidisciplinary team and specific assessment tools it is a time-consuming procedure, rarely used in clinical practice and in CLL clinical trials. That being said, it is worth noting that CGA may be useful to predict treatment tolerance, OS and health care utilization, such as hospitalization and emergency room visits [36]. Moreover, CGA can be assessed not only before treatment but also multiple times in a longitudinal way, thus enabling the treating physician to understand how the patient is tolerating treatment and which domains are most affected by therapy. Thus CGA may guide the supportive intervention, such as physical therapist, dietician, and psychologist [36].
Bonanad et al. developed the Geriatric Assessment in Hematology (GAH) which represents a simplified assessment of CGA [39]. The GHA scale was specifically designed for the evaluation of older subjects with different hematological malignancies, 33% of whom were affected by CLL. Interestingly, the mean time to complete the scale was only 12 minutes [39] and the GAH scale was validated by additional studies [40].
Interestingly, a planned analysis of the Alliance trial [21] evaluated the significance of CGA in a population of CLL patients treated upfront with CIT or Ibrutinib+/- Rituximab, showing that the domains of social activity and nutritional status were significantly associated with PFS and/or OS, regardless of treatment received. However, no domain was associated the probability to develop high-grade toxicity or treatment discontinuation were enrolled in this trial, moreover the assessment of some domains was underrepresented (eg. cognitive impairment) [41].
These data show that, in general, the assessment of comorbidities and CGA may assist the clinician to tailor the intensity of treatment to the need of the older patient and that refinement of the tools that assist the clinician in determining the fitness status and tolerability of novel agents represent an area of important investigation [41].
4. Data from Trials
Despite CLL is a disease of the elderly with a median age at onset around 70 years, the majority of published clinical trials until 2010 enrolled patients with a median age between 58 and 64 years [42]. The need of clinical trials specifically designed for older patients was recognized and the CLL5 trial showed that purine analog fludarabine was not superior to chlorambucil in older patients [43]. While bendamustine with the anti CD20 monoclonal antibody rituximab (BR) was shown to be an effective treatment in fit patients >65 years [11] and guidelines for the usage of bendamustine in CLL were published [12], the CLL 11 trial was specifically designed for elderly and unfit patients. In this randomized phase 3 study, single agent chlorambucil was compared with chlorambucil associated with the anti CD20 monoclonal antibody rituximab or the second generation anti CD20 obinutuzumab [10]. Chlorambucil plus obitutuzumab (Chlor+O) produced a significant PFS advantage as compared with the chlorambucil and rituximab. Furthermore, 37.7% of the patients who received chlorambucil and obinutuzumab attained an undetectable minimal residual disease in the peripheral blood and experienced prolonged PFS, especially in those cases with a favorable genetic profile, i.e., with a mutated configuration of the immunoglobulin gene [10]. Thus, the combination of Chlor+O or the BR regimen became standard treatment regimens for older patients [44].
Following the demonstration of an excellent activity in relapsed/refractory CLL [45,46] targeted agents revolutionized the treatment of CLL, including patients with genetically defined high-risk disease [47,48]. Therefore several randomized phase 3 trials were designed to test the efficacy of targeted agents as compared with standard CIT in treatment-naïve older patients. A summary of salient data for these trials is presented and discussed here.
4.1. Bruton Tyrosine Kinase Inhibitors
Five randomized trials showed the superiority of the BTKi ibrutinib, acalabrutinib and zanubrutinib as compared with chemo(immuno)therapy in previously untreated older patients. The salient efficacy data at the time of the primary pre-planned analyses in these trials are summarized in Table 1 and the incidence of adverse events of clinical interest are reported in Table 2.

Table 1.
Results of phase-3 clinical trials comparing the BTKi Ibrutinib, acalabrutinib and zanubrutinib or venetoclax-containing regimens versus standard chemo(immuno)therapy in older patients.
Table 1.
Results of phase-3 clinical trials comparing the BTKi Ibrutinib, acalabrutinib and zanubrutinib or venetoclax-containing regimens versus standard chemo(immuno)therapy in older patients.
|
N. of Patients |
Median Age | Median Follow-Up (months) | % TP53 Aberrations | PFS | OS | Reference | |
| BTKi vs comparator | |||||||
| IBR vs. CHLOR | 269 | Median age 72–73 yr | 18.4 | 0% | 18-months PFS: IBR 90%; Chlor 52% | 2-yr OS: IBR 98%, Chlor 85% |
50 |
| IBR vs. IBR+R vs BR. |
547 | 71 y | 38 | 10% | 2-yr PFS: IBR 87%; IBR+R 88%; BR 74% | 2-yr OS: IBR 90%, IBR+R 94%, BR 95% |
21 |
| IBR+O vs CHLOR+O | 229 | 70-72 | 31.3 | 16%/20% | 30-month PFS: IBR+O 77%; CHLOR +O 16% | 30-month OS: IBR+O 86%; CHLOR+O 85% | 105 |
| ACALA+O, ACALA, CHLOR+O |
535 | Median age 70 yr | 28.3 | 9% | 2-yr PFS: ACALA 87%; ACALA+O 93%; CHLOR+O 47% | 2-yr OS: ACALA 95%; ACALA+O 95%; CHOLOR+O 92% |
24 |
| ZANU, BR | 479 | Median age 70 yr, |
26.2 | 0% | 24-mo PFS: ZANU 85.5%; BR 69.5% | 24-mo OS: ZANU 94.3%, BR 94.6% |
15 |
| Venetoclax containing regimen vs comparator | |||||||
| V+O vs. CHLOR+O | 432 | 72–74 | 28.1 |
11.1% |
24-mo PFS: VO (88.2%) CHLOR+O: 64.1% |
24-mo OS: VO 91.8% CHLOR+O 93.3% |
20 |
| IBR+V vs CHLOR+O |
211 | 71 |
27.7 | 4.3% | 30-mo PFS: IBRU+V 80.5% CHLOR+O 35.8% |
NR | 23 |
IBR: Ibrutinib; R: rituximab; CHLOR: Chlorambucil; O: obinutuzumab; ACALA: Acalabrutinib; ZANU: zanubrutinib; V: Venetoclax; NR: not reported.
Table 2.
Grade ≥3 adverse events of clinical interest with BTKi in phase-3 clinical trials comparing standard chemo(immuno)therapy and BTKi in older patients.
Table 2.
Grade ≥3 adverse events of clinical interest with BTKi in phase-3 clinical trials comparing standard chemo(immuno)therapy and BTKi in older patients.
| Trial | Median Follow-Up (months) | Afib(*) | Hypertension | Bleeding | Arthralgia | Reference |
| Resonate-2 | 18.4 | IBRU *6%/1.5% CHLOR 0.7% | IBRU 4% CHLOR 0% |
IBRU 4% CHLOR 2% | IBRU 16%** CHLOR 7% |
106 |
| Alliance |
38 | IBR *17%/9%; IBR+R *14%/6% BR 3%/3% |
IBR 29%, IBR+R 34% BR 15% |
IBR 2% IBR+R 4% BR 0% |
NR | 21 |
| iLLUMINATE | 31.3 | IBRU+O *12%/5% CHLOR+O 0% | IBRU+O 4% CHLOR+O 4% |
NR | IBRU+O 1% CHLOR+O 0% |
105 |
| ACAL+O, ACAL, CHLOR+O |
28.3 | A *4% A+O *3% CHLOR+O: *1% |
A 2% A+O 3% |
A 2% A+O 2% |
A 0.6%; A+O 1.1% |
24 |
| SEQUOIA | 26.2 | ZANU *3% BR *3% |
ZANU 6% BR 5% | ZANU 3.5% BR 1.5% |
ZANU 1% BR 0.5% |
15 |
(*) all grades/grade ≥3; ** all grades.
Updated results with longer follow-up were published for these studies. In the RESONATE-2 trial, 269 patients 65 years of age or older were randomized to receive ibrutinib or the chemotherapy agent chlorambucil. Patients with del17p were excluded. At an extended median follow-up of 7.4 years [49], the experimental arm showed an increased 7-year PFS of 59% vs 9% [HR 0.154; 95% CI (0.108-0.220)] and an OS benefit despite crossover to ibrutinib at progression in the chlorambucil arm, with a median OS not reached vs 89 months [HR 0.453, 95% CI (0.276–0.743)]. The benefit of ibrutinib was consistent across all subgroups and there was no significant difference in PFS in the ibrutinib arm in patients <70 or ≥70 years. Ibrutinib was well tolerated, with a median duration of treatment of 74 months and 42% of patients on ibrutinib with up to 8 years of follow-up. The most frequent all-grade adverse events (AEs) with ibrutinib were diarrhea (50%), cough (37%), and fatigue (37%). Most of the ibrutinib associated AEs decreased over time, with the exception of hypertension, which showed prevalence rates of 25%, 23%, and 25% of patients in years 5-6, 6-7, and 7-8, respectively [49]. Grade ≥3 atrial fibrillation (AFib), grade 3 major hemorrhage and cardiac fatal events occurred respectively in 6%, 7% and 3% of patients in the experimental arm [49]. Grade ≥3 infections with ibrutinib occurred in 23% of patients at a median follow-up of 29 months [50]. Ibrutinib was discontinued because of AEs in 24% of patients and 23% required a dose reduction because of AEs. Noteworthy, greater quality of life (QOL) improvements were recorded with ibrutinib as compared with chlorambucil in Functional Assessment of Chronic Illness Therapy-Fatigue. However clinically meaningful improvements, though occurring more frequently with ibrutinib than chlorambucil, did not reach statistical significance [50].
The Alliance trial (A041202) randomized 547 untreated CLL older patients (65 years of age or older) to receive ibrutinib (I), ibrutinib with rituximab (I+R) or BR [21]. Patients with del(17p) were included. With a median follow-up of 55 months [51], the estimated 48-month PFS was 76% in both I containing arms as compared with 47% in the BR arm and 48-month OS estimates were 85% in the I arm, 86% in I+R and 84%, BR arms. Adverse events of clinical interest with ibrutinib included all grade Afib in 19% of the patients as compared with 6% in the BR arm. All grade hypertension was recorded in 73% of the patients on ibrutinib and in 54% of the patients on BR. Interestingly the AE score was higher in the CIT arm for the first 6 cycles than in the ibrutinib containing arms, whereas it was lower with BR when comparing the entire duration of assessment. This observation should be interpreted with caution because only unsolicited, treatment-related grade 1–2 and all-cause grade 3–4 AEs were captured for patients in observation after BR [52].
The iLLUMINATE trial compared ibrutinib plus obinutuzumab (I+O) to Chlor+O, in 229 patients older than 65 years, or younger with comorbidities as assessed by a CIRS score≥6 [22]. A clear PFS advantage was documented in the I+O arm as compared with the Chlor+O arm, with an estimated 42-month PFS of 74% Vs 33% and with a 75% reduction in the risk of disease progression or death (HR 0.25; 95% CI: 0.16-0.39; p<0.0001). Interestingly, a significant PFS advantage in the I+O arm was also noted among patients with a favorable immunogenetic profile, i.e., with a mutated status of the immunoglobulin heavy chain gene (M-IGHV) (HR: 0.20; 95% CI: 0.07-0.59). Moreover patient with or without TP53 aberration (del17p or TP53 mutation) had a similar PFS (HR 0.9) in the experimental arm [22].
Acalabrutinib is a second generation BTKi, characterized by a greater specificity for BTK with fewer off-target effects [53].
ELEVATE-TN is a phase III randomized trial that enrolled 535 untreated patients ≥65 years or younger with creatinine clearance of 30–69 mL/min or CIRS >6 [24]. The experimental arms were acalabrutinib with obinutuzumab (A+O) or without (A) and the control arm was Chlor+O. At a median follow up of 46.9 months [14] a PFS of 87%, 78% and 25% was reported in the A+O, A and Chlor+O arms, respectively. The addition of obinutuzumab to acalabrutinib was associated with a significant prolongation of PFS as compared with A alone (p=0.0296). In the subgroup of patients with TP53 aberration (del17p and/or TP53 mutation) the estimated 4-year PFS was 75% in both acalabrutinib containing arms. IGHV mutational status was not predictive of an inferior PFS in patients treated with A and A+O. Median OS was not reached in all treatment arms and no survival advantage was observed in the experimental arms as compared with the CIT arm. Acalabrutinib-containing arms were associated with a higher incidence of all-grade headache, diarrhea, fatigue, arthralgia, cough, and upper respiratory tract infection. At a 4-year follow-up, grade ≥3 infections occurred in 23.6% patients in the A+O arm, in 16.2% patients in the A arm and in 8.3% in the Chlor+O arm. The incidence of any grade AFib and hypertension was 3.9%/7.9% and 6.1%/7.3% in patients exposed to A+O and A, respectively, as compared with a 0.6%/4.1% in the Chol+O arm. Although cross-trial comparisons should be interpreted with caution it is worth noting that these data on the incidence of cardiovascular events with acalabrutinib compare favorably with those reported in ibrutinib trials and that a head-to head comparison of acalabrutinib and ibrutinib in the relapsed/refractory setting showed a better tolerability profile in the acalabrutinib arm [54]. At a 4-year follow-up, SPM, including non-melanoma skin cancer were reported in 15.7%, 13% and 4.1% of patients respectively treated with A+O, A and Chlor+O [14].
Zanubrutinib is a second generation BTKi, that was tested in treatment naïve CLL in the SEQUOIA trial [15]. Patients enrolled were older (>65 years) or younger with comorbidities (CIRS >6, creatinine clearance <70 mL/min, history of severe or frequent infections which rendered them unsuitable for FCR [15]. Patients without del17p were randomized to receive zanubrutinib (group A) or BR (group B), while patients with del17p were enrolled in the non-randomized group C.
In 479 patients randomized to zanubrutinib or BR the ORR was 95% Vs 85% respectively. The experimental arm showed a significant prolongation of the 24-month PFS (85.5% Vs 69.5%) and a PFS advantage in the subgroup of M-IGHV became apparent in a recent updated report with median follow-up of 43.7 months [55]. Median OS was not reached in both groups. Grade ≥3 AE and discontinuations due to AE were reported more frequently in the BR arm than in the zanubrutinib arm (79.7%/13.7% Vs 52.5%/ 8.3%). A 5% and 14.2 incidence of major bleeding and hypertension were reported in the zanubrutinib arm at a median follow-up of 26.2 months and, interestingly, any grade Afib was reported in 3% of the cases in the zanubrutinib arm and in the BR arm [15].
In group C, 109 patients with del17p and a median age of 70 (range 66–74) were treated with zanubrutinib single agent. The ORR was 94.5%. The estimated PFS at 18-month was 88.6%, with an OS of 95.1%. Safety data were consistent with those reported in previous studies of zanubrutinib. Clinically relevant AEs were AFib in 2.8% of patients, major bleeding in 5.6% with no central nervous system events [56]. Other cancers were reported in 13%, 9% and 22% of patients in group A, B and C; it is worth noting that in group C 10.8% of cancer were basal cell carcinoma of the skin [15].
4.2. The BCL-2 Inhibitor Venetoclax
BCL-2, a negative regulator of the mitochondrial pathway of apoptosis, was found to be upregulated in CLL as a consequence of chromosome 13q deletion causing loss of the negative regulatory miRNA-15a/16-1 [57]. Venetoclax is the first BCL2 inhibitor and was approved by FDA and EMA for the treatment of CLL following the publication of studies that showed its efficacy in CLL with 17p- [58], in relapsed/refractory CLL [59] and in treatment naïve CLL [20].
The CLL 14 study is a phase III trial that enrolled 432 previously untreated patients with a median age of 72 years. The patients had coexisting comorbidities as defined by CIRS >6 and/or CrCl <70 mL/min [20]. The patients were randomized to receive venetoclax and obinutuzumab (V+O) or Chlor+O. A higher ORR was obtained with V+O (84.7%, including 49.5% CR) as compared with Chlor+O (71.2% including 48.1% CR) [16]. At a median follow-up of 65.4 months PFS was longer in V+O arm than in the Chlor+O arm ([HR] 0.35 [95% CI 0.26–0.46]) and the estimated PFS rate at 5 years after randomization was 62.6% after V+O and 27.0% after Chlor+O [60]. The PFS benefit provided by venetoclax was independent from IGHV mutational status and TP53 disruption. Interestingly, a longer PFS was observed with V+O as compared with Chlor+O both in the IGHV unmutated subset (HR 0.25; 95% CI, 0.17 to 0.37; P<.0001) and in the IGHV mutated subset (HR 0.36;95% CI, 0.19 to 0.68; P = .002) [16]. However, it is worth noting that PFS in both arms was shorter in high-risk subsets, as defined by TP53 disruption and IGHV unmutated. No significant difference in OS was detected at last follow up [60].
Fixed duration therapy with V+O and Chlor+ O produced deep responses with undetectable minimal residual disease (MRD), which represents a prognostic factor predictive for a longer for progression-free survival (PFS) [10,61].
In CLL 14 MRD was measured in peripheral blood (PB) and bone marrow (BM) by an allele-specific oligonucleotide polymerase chain reaction (ASO-PCR), with a cutoff for undetectable MRD (uMRD) at 10−4 [16]. A higher percentage of patients attained an uMRD in PB at the end of treatment (EoT) in the V+O arm (75%) than in the Chlor+O arm (35.2%, P<0.001). Likewise, a higher fraction of patients was shown to attain uMRD in the BM in the V+O arm (56.9%) as compared with the Chlo+O arm (17.1%) (P<0.001). The duration of uMRD status was longer in the V+O arm than in the Chlor+O arm, with a median time to reach a detectable MRD at 10-2 of 1,259 days vs 233 days (P <.0001). Interestingly, univariate and multivariate analysis for MRD conversion by NGS from <10-4 at the end of treatment to ≥10-4 in the whole cohort showed that age ≥75 years had no impact on the duration of uMRD [16].
Treatment discontinuation due to AEs occurred in 16.0% and 15.4% of patients in the V+O arm and Chlor+O arm, respectively [16]. The most common grade≥ 3 AEs was neutropenia, 52.8% in former arm vs 48.1 in latter arm. With grade ≥ 3 infection rate of 17.5% with the V+O arm and a 15.0% rate with the Chlor+O arm, the treatment proved to be well tolerated in this elderly patient population which showed a non-significant increase in the incidence of SPM in the V+O arm (12.7%) as compared with the Chlor+O arm (7.5%) (p=0.074) [60]. A summary of AE of clinical interest with venetoclax containing regimens is shown in Table 3.
Table 3.
Grade ≥3 adverse events of clinical interest with venetoclax containing regimes in phase-3 clinical trials in older patients.
Table 3.
Grade ≥3 adverse events of clinical interest with venetoclax containing regimes in phase-3 clinical trials in older patients.
| Trial | Median Follow-Up (months) |
Infusion Related Reactions |
Tumor Lysis Syndrome | Neutropenia | Infections | Afib* | Reference |
| CLL14 | 28.1 | V+O 9% Chlor+O 10.3% |
V+O 0.5% Chlor+O 1.9% |
V+O 52.8% Chlor+O 48.1% |
V+O 17.5% Chlor+O 15.0% | NA | 20 |
| GLOW | 27.7 | NA | Ibr+V 0% Chlor+O 5.7% |
Ibr+V 34.9% Chlor+O 49.5% |
Ibr+V 12.3% Chlor+O 8.6% |
Ibr+V^ 14%/6% Chlor+O 1.9%0% |
23 |
(*) all grades/grade ≥3; ** all grade; IBR: Ibrutinib; CHLOR Chlorambucil; O: obinutuzumab; V: Venetoclax; Afib: atrial fibrillation; NA: not applicable; ^ Four sudden deaths, all in patients with a high comorbidities and ECOG PS of 2.
A prespecified secondary endpoint of CLL14 was represented by the evaluation of health-related QOL and the burden of CLL-specific symptom severity, based on the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30) and the MD Anderson Symptom Inventory (MDASI) with the CLL module (MDASI-CLL). In the V+O arm a relevant improvement of general health status and QOL was recorded at cycle 3, whereas improvement was delayed until cycle 8 with Chlor+O. CLL related symptoms (measured with MDASI-CLL) were similar between the two arms and they remained low during treatment and follow up. The authors concluded that treatment with venetoclax-obinutuzumab was associated with an earlier improvement compared to control arm and that no negative signals on QOL with the V+O regimen were observed [62].
4.3. Combination Therapy
Ibrutinib and venetoclax exert a preferential anti-leukemic activity in different anatomic compartments. Ibrutinib induces a rapid shrinkage of lymphadenopathy, while venetoclax leads to a rapid clearance of peripheral blood. In ex vivo model of CLL, Pin Lu et al., demonstrated that ibrutinib inactivated a subpopulation of CLL cells more frequently encountered in the proliferation centers of the lymph nodes, whereas venetoclax was able to induce the cell death of resting CLL cells especially in peripheral blood [63]. Moreover, BTK inhibition was shown to enhance mitochondrial BCL2 dependence of CLL cells, favoring the killing by venetoclax [64]. Based on these biologic data, trials combining a BTKi and venetoclax were designed, showing high efficacy of this combination in all age groups [23,65,66,67].
In the GLOW trial, that included older patients (>65 years) and/or patients with comorbidities, i.e., with CIRS>6 or creatinine clearance <70 mL/min) [23], 210 untreated CLL patients were randomized to receive 3 months of lead-in ibrutinib followed by 12 months of ibrutinib and venetoclax (I+V) or Chlor+O (6 cycles). Patients with TP53 disruption were excluded. A similar ORR was observed (86.8% with I+V and 84.8% with Chlor+O), but CR rates were higher with I+V (38.7% Vs 11.4%). Interestingly, uMRD at end of treatment was observed in the PB and BM in the I+V arm (54.7% and 51.9%, respectively). With a median follow-up of 27.7 months, PFS was longer with for I+V than with Chlor+O (hazard ratio, 0.216; 95% confidence interval 0.131-0.357; P<.001), with an estimated 24-month PFS rate of 84.4% with I+V vs 44.1% with Chlor+O. The PFS advantage was evident across all the specified subgroups, including patients ≥65 years. With a median follow up of 34.1 months, OS was not significantly different in the two arms.
AE events of clinical interest with I+V are summarized in Table 3. The overall incidence of grade≥3 AEs was similar in the 2 arms (75.5% and 69.5% of patients in the I+V arm and Chlor+O arm, respectively). The administration of 3 cycles of ibrutinib prior to venetoclax reduced the number of patients at high risk of tumor lysis syndrome (TLS) (1.9% vs 24.5% at baseline) and no case of TLS occurred in the I+V arm. SPM were reported in 7.5% and 9.5% of patients treated respectively in the I+V and Chlor+O arms. The overall number of deaths at the primary analysis was similar for the two arms, however I+V was associated with four cardiac/sudden deaths that occurred in patients with higher CIRS and ECOG PS score, underlining the importance of a complete cardiologic assessment before ibrutinib based treatment [23].
5. Real World Evidence
Real-world evidence (RWE) is based on real-world data (RWD) collected from a variety of sources such as electronic health records, medical claims, databases, registries, or patient-generated data [68]. RWD can in-form on the population of patient not included in clinical trial which represents >95% of patients with a neo-plasia in the U.S. [69].
RWE uses similar endpoints as in randomized clinical trials (RCT), with OS, time to next treatment (TTNT)) and time to treatment discontinuation (TTD) representing objective measure of efficacy in observational studies [70]. That being said, it is noteworthy that RWD must be interpreted with caution due to possible selection bi-as, as in clinical practice treatment selection is almost always based on individual patient’s characteristics at baseline [71].
Over the last years, RWD on novel agents in CLL highlighted significant difference between patients treated in RCT and those treated in the everyday practice. Treatment discontinuation rates were higher in real world analyses than in RTC, whereas no major difference in terms of OS were noted, including patient treated with a reduced-dose or a time-limited therapy [72,73].
Goyal et al. [74] conducted one of the larger population-based retrospective cohort study. Among 7,965 Med-icare patients treated for CLL, they were able to analyze 2033 patients treated with first line ibrutinib, with a median age of 75 years and a CCI score of 4.6. At a median follow up of 19 months, median OS was not reached. Ibrutinib treated patients experienced more thrombocytopenia, bleeding, atrial fibrillation, pneumo-nia and renal failure than patients treated chemo(immuno) therapy regimens for CLL. Moreover 85.6% of ibru-tinib treated patients experienced grade ≥ 3 AEs and overall these data show that there is considerable sus-ceptibility to AEs in Medicare patients with CLL in the U.S. Interestingly, 2190 patients treated with first line ibrutinib were analyzed using a nationwide U.S. electronic health record-derived database. TTNT with ibrutinib was not significantly different in patient with high-risk cardiovascular profile, with a TTD in all patients of 15.7 months, as compared with 11.7 and 13.7 months in patients with high AF risk and in high stroke risk, respec-tively [75].
Mato et al. [76] analyzed data from an health electronic health record−derived database in the US and report-ed outcomes in 1,069 patients with a median age of 69 years treated in the U.S. with first line ibrutinib and found a median time to treatment discontinuation (TTD) of 38.6 months (95% CI: 33.4-42.9) and a shorter OS in patients with del(17p) than in patients without (57.7 months vs. not reached; P=0.0006).
In an unbiased nationwide survey of 747 patients with 17p-/TP53 deletion and with a median age of 71 years (range 32-95) treated upfront with ibrutinib, an estimated treatment persistence rate of 63.4% (95% CI 60.0%-67.0%) and survival rate of 82.6% (95% CI 79.9%-85.4%) were recorded at 24 months. A higher risk of treat-ment discontinuation was found to be associated with age, ECOG-PS and pre-existing heart disease. ECOG≥1, age≥70 years and male sex were associated with an increased risk of death [77]. Interestingly single hit or double hit TP53 aberrations had no impact on TTD and OS in subgroup of 496 patients (66.4% of the total population) with similar clinicobiologic characteristics as the entire cohort. In the Italian CLL campus group report that included 100 treatment naïve CLL patients with TP53 disruption treated with ibrutinib the 36-month PFS and OS rates were 75% and 87% respectively. Male gender, double hit TP53 disruption, lack of response and CIRS>6 were associated with a decreased OS. [78].
RWD were also reported to compare the efficacy of first line ibrutinib and CIT. Cuneo et al. performed a matched-adjusted indirect comparison between a European cohort of unfit CLL patients treated with BR (157 patients) and a US cohort of 162 patients ≥65 years treated with ibrutinib, excluding patients with del(17p)/TP53 aberrations [79]. Ibrutinib was associated with a significant prolongation of PFS but not of OS. In patients with advanced stage disease there was also a trend for OS prolongation in favor of ibrutinib co-hort.
An indirect comparison of CIT with Chlor+O and ibrutinib was performed with the Italian CLL campus network [80]. Patients with TP53 disruption were excluded. The cohort of Chlor+O treated patients had a higher CIRS score, worse renal function and a higher rate of M-IGHV. ORR were similar (87% for Chlor+O and 86% for ib-rutinib), but the Chlor+O group had more CR and uMRD rate. The 30 month PFS rate (93% Vs 68%; p = 0.0061) and TTNT (97% Vs 88%, p = 0.0043) were significantly longer with ibrutinib. After a propensity score matched analysis, that was performed to balance differences between treatment groups, the PFS and TTNT advantage in favor of ibrutinib was maintained, whereas no OS advantage was observed. In the Chlor+O group a higher incidence of AE than in the ibrutinib group was recorded, with 2.98 vs. 1.68 AE/month of treatment/person observed.
6. Cost Effectiveness
Over the last 10 years, concerns were raised on the sustainability of the expenditures for new drugs in hematology even in high-income countries. The average price of drugs appears to increase over the time [81] and the usage of oral targeted therapies in the United States was estimated to cause a 590% increase of the annual cost of therapy in CLL with respect to the CIT era [82]. Medicare spending in the U.S. from 2004 to 2020 for oral drugs in CLL increased from 254 million to 3.7 billion dollars due to the growing number of beneficiaries and to the rising costs for a 30-day supply of the first-in-class BTKi ibrutinib [83]. The rising costs of medicines increase the total out-of-pocket expense for many patients, with possible negative impact on adherence to treatment, potentially undermining the effectiveness of therapy [84]. Interestingly, a significant proportion of U.S. patients chose the lower-cost medicine when presented with a choice between 2 medicines and their out-of-pocket cost [85]. Clearly, the trend of unaffordable drug prices demand action to define fair prices of new drugs to guarantee effective treatment to as many patients as possible. Initiatives for assessing the value of cancer treatment and price negotiation were recently reviewed along with possible initiatives by oncologists and health systems to mitigate the financial burden in CLL [86,87]. In some countries the willingness to pay (WTP) for a new drug based on its efficacy as assessed by the incremental cost-effectiveness ratios (ICERs) was defined. ICER represent the difference in cost between 2 different treatments divided by the difference in their effect in terms of quality-adjusted life years (QALY) gained by the new treatment compared with the standard of care. One QALY equates to one year in perfect health and represents a single number that can be compared across different types of treatments [86].
Independent studies that assessed ICERs and QALY in previously untreated CLL were performed for the first-in-class BTKi ibrutinib, for acalabrutinib, for V+O and for the combination ibrutinib and venetoclax. The results of cost effectiveness analyses conducted by health-policy institutions or by non-sponsored teams of university researchers are summarized in Table 4. These data consistently show that finite duration treatment with V+O or with Ibrutinib combined with venetoclax and continuous treatment with acalabrutinib represent cost effective option as compared with most comparators for first line treatment of CLL in several countries, independent of disease characteristics. Noteworthy confidential discount were applied in the UK and the BTKi ibrutinib may be cost effective only after a significant reduction of the cost of treatment in the U.S.
Table 4.
Cost-effectiveness analyses of target agents in first line treatment of CLL.
|
Source/Country/ Reference |
WTP/QALY | Treatment | Comparator | Target Population | ICER | Comments | Cost Effective |
| NICE/U.K/107 | £20,000 to £30,000 | V+O | ibrutinib | 17p- | £549,699 saved per QALY lost* | V+O results in cost saving of £199,622 and QALY loss of 0.363* | YES^ |
| Chlor+O | Unsuitable for FCR/BR | NR | Dominant effect V+O vs Chlor+O° (more effective and less costly) | YES^ | |||
| FR/BR | Suitable for FCR/BR | £47,494 vs FCR £67,445 vs BR per QALY gained | ICERs varied widely if the upper and lower bounds of the PFS and OS HR-CI were applied. | NO | |||
| Dutch National Health Care Institute/ Holland / 108 |
50,000 EUR | V+O | Chlor+O | non-fit patients, uIGHV§ | incremental QALYs of 1.14 and cost saving 159,276 € | Dominant effect (more effective and less costly). Negotiation of prices recommended | YES |
| non-fit patients, mIGHV§ | NR | V+O cost saving despite limited availability of data | YES | ||||
| Erasmus University Rotterdam/Holland/ 109 | 20, 000 EUR | V+O | Chlor+O | all patients | 1.25 QALYs gained; 62,316 € saved | The sensitivity analyses demonstrated the robustness of these results | YES |
| Stanford University/ USA/110 |
150,000 USD | Ibrutinib | Chlor+O | CLL without 17p- | $189,000 per QALY gained | A reduction of $20 400 per year would be required to reach the WTP of 150,000 USD | NO# |
| Erasmus University Rotterdam/UK /111 | £20,000 to £30,000 | Ibrutinib | Chlor+O | CLL | £75,648 per QALY gained | An adequate discount on ibrutinib is required to make it cost-effective as per the UK thresholds | NO# |
| NICE/UK/112 | Acalabrutinib | Chlor+O | CLL unsuitable for FRC/BR, including 17p- | <£30,000 per QALY gained | Considering confidential discounts | YES | |
| NICE/UK/113 | £20,000 to £30,000 | ibrutinib and venetoclax |
FRC/BR | CLL suitable for FRC/BR, including 17p- | <£30,000 per QALY gained | Considering confidential discounts | YES |
| Chlor+O and V+O | unsuitable for FRC/ BR, including 17p- | <£30,000 per QALY gained | Dominant effect vs Chlo+O° | YES | |||
| Acalabrutinib and Ibrutinib | NR | Cost saving and a small QALY loss compared with acalabrutinib and ibrutinib | YES |
WTP/QALY: Willingness to pay threshold per QALY gain; V+O: venetoclax and obinutuzumab; Chlor+O: chlorambu-cil and obinutuzumab; NR: not reported; uIGHV: unmutated Ig gene, mIGHV: mutated Ig gene; HR: hazard ratio * When a drug is less effective and less costly than its comparator, the higher the ICER, the more cost effective a treatment becomes; °Dominant effect:more effective and less costly ^Provided that the companies provide the drugs according to the commercial arrangements; § CLL with 17p-/TP53 mutated not included in the assessment; #unless a discount on ibrutinib is applied.
A company-sponsored probabilistic analysis showed that at a willingness to pay of $50,000/QALY gained in Canada, VEN+O has the greatest probability of being cost effective as compared with Chlor+O, BR, ibrutinib and acalabrutinib [88]. Likewise, acalabrutinib monotherapy showed a 59% to 73% probability of being cost-effective vs Chlor+O at a $100,000-to-150,000/QALY gained in the US in a company-sponsored analysis [89]. An investigator-initiated study funded by an unrestricted research grant from a company showed that a willingness to pay of EUR 23,600-35,600 per QALY, fixed duration therapy with VEN+O was cost-effective with respect to Chlor+O, whereas the comparison of ibrutinib vs Ven+O yielded substantially increased incremental cost of over a lifetime horizon, with an ICER of €302,156/QALY [90].
Overall these analyses are reassuring for the cost-effectiveness of target therapy according to the WTP by high income countries and clearly support the need to take action to negotiate fair prices, especially for continuous treatment [91]. This process is especially important for CLL, the prevalence of which is expected to increase due the efficacy of new agents and to the rising median age of the population in several countries [5,92,93].
7. Conclusions and Future Directions
The introduction of targeted agent revolutionized the approach to the treatment of CLL regardless of risk factors and age. Indeed, BTKi and venetoclax with or without the anti CD20 monoclonal antibody obinutuzumab were convincingly shown to represent effective agents and, according to recent guidelines or expert opinion papers, they represent the preferred options for the first-line therapy of CLL [44,94,95,96]. That being said, it is important to recall that a survival advantage over CIT has not been documented so far in older patients [97], in part due to the effectiveness of novel agents as first salvage regimens [98]. Furthermore, novel prognostic factors in the era of novel agents represent an area of intense investigation [99,100,101,102].
Four issues discussed in this review are relevant in the everyday practice and need to be put in perspective.
- (a)
- The interpretation of the excellent results reported in studies designed for older patients should be interpreted bearing in mind that inclusion criteria were heterogeneous across trials, some investigators having adopted a 65-year age cut-off and others having used renal dis-function and a high cumulative illness rating scale defined for geriatric patients as inclusion criteria. In view of the widespread adoption of targeted agents, the identification of CLL-specific parameters identifying unfit patients would be highly desirable to tailor the intensity of treatment to the characteristics of each patient, with special reference to the capability to predict the onset of drug specific adverse events, i.e., cardiovascular toxicity and bleeding with BTKi, tumor lysis syndrome, infusion reactions and neutropenia with venetoclax and obinutuzumab.
- (b)
- Heterogeneous inclusion criteria and some notable exclusion criteria in clinical studies limit the transferability of the efficacy data to the everyday practice. Higher discontinuation rates with BTKi were reported in real world studies [73] and the analysis of data from registries [76], or unbiased databases with 100% capture of the patient population treated with an anti-CLL drug outside of clinical trials are of utmost importance to identify factors predicting for earlier discontinuation in a real-world setting [77]
- (c)
- QOL is a very important issue in older patients and, interestingly, fixed duration treatment with V+O produced an earlier improvement compared to CIT [16]. BTK inhibitors may improve QOL as compared with chlorambucil and were shown to reduce the burden of AE during the first 6 months of treatment, as compared with the BR regimen [52]. The results of QOL assessment are awaited for second generation BTKi, which appear to be better tolerated than the first-in- class agent ibrutinib [54,103]
- (d)
- Recent independent pharmacoeconomic analyses showed that targeted agents represented a cost-effective use of health system resources in high income countries, under confidential agreements on discounted price. Most importantly, targeted agents appeared to be dominant i.e., more effective and less costly than CIT in some analyses, as summarized in table 4. Fixed duration treatment with targeted may be expected to result in significant cost reductions in a recent analysis [104].
However, it is noteworthy that the overall expenditure for new drugs in CLL is projected to increase substantially posing the issue of sustainability. Furthermore, out of-pocket expenses may limit accessibility to these drugs and actions need to be undertaken by regulatory agencies to negotiate fair prices.
Thus personalized treatment of the older patient with CLL is today possible and the choice of a finite duration approach based on venetoclax containing regimens or treatment until progression with BTKi should be discussed with every patient, taking into considerations coexisting medical conditions, logistics and sustainability, as summarized in Figure 1.
Author Contributions
Conceptualization: AC and GMR,: literature search: AU; writing original draft manuscript: AU. All the authors reviewed the manuscript for important intellectual content and contributed to preparation of the final version All authors have read, approved and agreed to the published version of the manuscript.”
Funding
Work in the Authors laboratories was supported by FAR 2021-2023 University of Ferrara, PRIN MIUR,
AIL-FE, and by Beat Leukemia Onlus.
Conflicts of Interest
AC received honoraria for participation to speakers’ boureau and advisory board from Abbvie, Astra Zeneca, Beigene, Janssen Lilly; GMR received honoraria for participation to speakers’ bureau and advisory board from Abbvie, Astra Zeneca, Janssen. The other authors declare no conflict of interest.
References
- National Cancer Institute. Chronic Lymphocytic Leukemia - Cancer Stat Facts. Available online: https://seer.cancer.gov/statfacts/html/clyl.html (accessed on 15 May 2023).
- Siegel, R. L.; Miller, K. D.; Wagle, N. S.; Jemal, A. Cancer Statistics, 2023. CA: A Cancer Journal for Clinicians 2023, 73 (1), 17–48. [CrossRef]
- Haematological Malignancy Research Network. Available online: https://hmrn.org/statistics/prevalence (accessed on 15 May 2023).
- van der Straten, L.; Maas, C. C. H. M.; Levin, M.-D.; Visser, O.; Posthuma, E. F. M.; Doorduijn, J. K.; Langerak, A. W.; Kater, A. P.; Dinmohamed, A. G. Long-Term Trends in the Loss in Expectation of Life after a Diagnosis of Chronic Lymphocytic Leukemia: A Population-Based Study in the Netherlands, 1989–2018. Blood Cancer Journal 2022, 12 (4). [CrossRef]
- Chen, Q.; Jain, N.; Ayer, T.; Wierda, W. G.; Flowers, C. R.; O’Brien, S. M.; Keating, M. J.; Kantarjian, H. M.; Chhatwal, J. Economic Burden of Chronic Lymphocytic Leukemia in the Era of Oral Targeted Therapies in the United States. Journal of Clinical Oncology 2017, 35(2), 166–174. [Google Scholar] [CrossRef]
- Cuneo, A.; Cavazzini, F.; Ciccone, M.; Daghia, G.; Sofritti, O.; Saccenti, E.; Negrini, M.; Rigolin, G. M. Modern Treatment in Chronic Lymphocytic Leukemia: Impact on Survival and Efficacy in High-Risk Subgroups. Cancer Medicine 2014, 3(3), 555–564. [Google Scholar] [CrossRef]
- Hallek, M.; Fischer, K.; Fingerle-Rowson, G.; Fink, A. M.; Busch, R.; Mayer, J.; Hensel, M.; Hopfinger, G.; Hess, G.; von Grünhagen, U.; Bergmann, M.; Catalano, J.; Zinzani, P. L.; Caligaris-Cappio, F.; Seymour, J. F.; Berrebi, A.; Jäger, U.; Cazin, B.; Trneny, M.; Westermann, A. Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with Chronic Lymphocytic Leukaemia: A Randomised, Open-Label, Phase 3 Trial. Lancet 2010, 376(9747), 1164–1174. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P. A.; Tam, C. S.; OBrien, S. M.; Wierda, W. G.; Stingo, F.; Plunkett, W.; Smith, S. C.; Kantarjian, H. M.; Freireich, E. J.; Keating, M. J. Fludarabine, Cyclophosphamide, and Rituximab Treatment Achieves Long-Term Disease-Free Survival in IGHV-Mutated Chronic Lymphocytic Leukemia. Blood 2015, 127(3), 303–309. [Google Scholar] [CrossRef] [PubMed]
- Rossi, D.; Terzi-di-Bergamo, L.; De Paoli, L.; Cerri, M.; Ghilardi, G.; Chiarenza, A.; Bulian, P.; Visco, C.; Mauro, F. R.; Morabito, F.; Cortelezzi, A.; Zaja, F.; Forconi, F.; Laurenti, L.; Del Giudice, I.; Gentile, M.; Vincelli, I.; Motta, M.; Coscia, M.; Rigolin, G. M. Molecular Prediction of Durable Remission after First-Line Fludarabine-Cyclophosphamide-Rituximab in Chronic Lymphocytic Leukemia. Blood 2015, 126(16), 1921–1924. [Google Scholar] [CrossRef] [PubMed]
- Goede, V.; Fischer, K.; Busch, R.; Engelke, A.; Eichhorst, B.; Wendtner, C. M.; Chagorova, T.; de la Serna, J.; Dilhuydy, M.-S.; Illmer, T.; Opat, S.; Owen, C. J.; Samoylova, O.; Kreuzer, K.-A.; Stilgenbauer, S.; Döhner, H.; Langerak, A. W.; Ritgen, M.; Kneba, M.; Asikanius, E. Obinutuzumab plus Chlorambucil in Patients with CLL and Coexisting Conditions. New England Journal of Medicine 2014, 370(12), 1101–1110. [Google Scholar] [CrossRef]
- Fischer, K.; Cramer, P.; Busch, R.; Böttcher, S.; Bahlo, J.; Schubert, J.; Pflüger, K. H.; Schott, S.; Goede, V.; Isfort, S.; von Tresckow, J.; Fink, A.-M.; Bühler, A.; Winkler, D.; Kreuzer, K.-A.; Staib, P.; Ritgen, M.; Kneba, M.; Döhner, H.; Eichhorst, B. F. Bendamustine in Combination with Rituximab for Previously Untreated Patients with Chronic Lymphocytic Leukemia: A Multicenter Phase II Trial of the German Chronic Lymphocytic Leukemia Study Group. Journal of Clinical Oncology 2012, 30(26), 3209–3216. [Google Scholar] [CrossRef]
- Cuneo, A.; Marchetti, M.; Barosi, G.; Billio, A.; Brugiatelli, M.; Ciolli, S.; Laurenti, L.; Mauro, F. R.; Molica, S.; Montillo, M.; Zinzani, P.; Tura, S. Appropriate Use of Bendamustine in First-Line Therapy of Chronic Lymphocytic Leukemia. Recommendations from SIE, SIES, GITMO Group. Leukemia Research 2014, 38 (11), 1269–1277. [CrossRef]
- Shanafelt, T. D.; Wang, X. V.; Hanson, C. A.; Paietta, E. M.; O’Brien, S.; Barrientos, J. C.; Jelinek, D. F.; Braggio, E.; Leis, J. F.; Zhang, C. (Christine); Coutre, S. E.; Barr, P. M.; Cashen, A. F.; Mato, A. R.; Singh, A. K.; Mullane, M. P.; Little, R. F.; Erba, H. P.; Stone, R. M.; Litzow, M. R. Long-Term Outcomes for Ibrutinib-Rituximab and Chemoimmunotherapy in CLL: Updated Results of the E1912 Trial. Blood 2022. [CrossRef]
- Sharman, J. P.; Egyed, M.; Jurczak, W.; Skarbnik, A.; Pagel, J. M.; Flinn, I. W.; Kamdar, M.; Munir, T.; Walewska, R.; Corbett, G.; Fogliatto, L. M.; Herishanu, Y.; Banerji, V.; Coutre, S.; Follows, G.; Walker, P.; Karlsson, K.; Ghia, P.; Janssens, A.; Cymbalista, F. Efficacy and Safety in a 4-Year Follow-up of the ELEVATE-TN Study Comparing Acalabrutinib with or without Obinutuzumab versus Obinutuzumab plus Chlorambucil in Treatment-Naïve Chronic Lymphocytic Leukemia. Leukemia 2022. [CrossRef]
- Tam, C. S.; Brown, J. R.; Kahl, B. S.; Ghia, P.; Giannopoulos, K.; Jurczak, W.; Šimkovič, M.; Shadman, M.; Österborg, A.; Laurenti, L.; Walker, P.; Opat, S.; Chan, H.; Ciepluch, H.; Greil, R.; Tani, M.; Trněný, M.; Brander, D. M.; Flinn, I. W.; Grosicki, S. Zanubrutinib versus Bendamustine and Rituximab in Untreated Chronic Lymphocytic Leukaemia and Small Lymphocytic Lymphoma (SEQUOIA): A Randomised, Controlled, Phase 3 Trial. The Lancet Oncology 2022, 23(8), 1031–1043. [Google Scholar] [CrossRef]
- Al-Sawaf, O.; Zhang, C.; Lu, T.; Liao, M. Z.; Panchal, A.; Robrecht, S.; Ching, T.; Tandon, M.; Fink, A.-M.; Tausch, E.; Schneider, C.; Ritgen, M.; Böttcher, S.; Kreuzer, K.-A.; Chyla, B.; Miles, D.; Wendtner, C.-M.; Eichhorst, B.; Stilgenbauer, S.; Jiang, Y. Minimal Residual Disease Dynamics after Venetoclax-Obinutuzumab Treatment: Extended Off-Treatment Follow-up from the Randomized CLL14 Study. Journal of Clinical Oncology 2021, 39(36), 4049–4060. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L. A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Systematic Reviews 2015, 4 (1). [CrossRef]
- Shanafelt, T. Treatment of Older Patients with Chronic Lymphocytic Leukemia: Key Questions and Current Answers. Hematology 2013, 2013(1), 158–167. [Google Scholar] [CrossRef] [PubMed]
- Linn, B. S.; Linn, M. W.; Gurel, L. CUMULATIVE ILLNESS RATING SCALE. Journal of the American Geriatrics Society 1968, 16(5), 622–626. [Google Scholar] [CrossRef]
- Fischer, K.; Al-Sawaf, O.; Bahlo, J.; Fink, A.-M.; Tandon, M.; Dixon, M.; Robrecht, S.; Warburton, S.; Humphrey, K.; Samoylova, O.; Liberati, A. M.; Pinilla-Ibarz, J.; Opat, S.; Sivcheva, L.; Le Dû, K.; Fogliatto, L. M.; Niemann, C. U.; Weinkove, R.; Robinson, S.; Kipps, T. J. Venetoclax and Obinutuzumab in Patients with CLL and Coexisting Conditions. New England Journal of Medicine 2019, 380(23), 2225–2236. [Google Scholar] [CrossRef]
- Woyach, J. A.; Ruppert, A. S.; Heerema, N. A.; Zhao, W.; Booth, A. M.; Ding, W.; Bartlett, N. L.; Brander, D. M.; Barr, P. M.; Rogers, K. A.; Parikh, S. A.; Coutre, S.; Hurria, A.; Brown, J. R.; Lozanski, G.; Blachly, J. S.; Ozer, H. G.; Major-Elechi, B.; Fruth, B.; Nattam, S. Ibrutinib Regimens versus Chemoimmunotherapy in Older Patients with Untreated CLL. New England Journal of Medicine 2018, 379(26), 2517–2528. [Google Scholar] [CrossRef]
- Moreno, C.; Greil, R.; Demirkan, F.; Tedeschi, A.; Anz, B.; Larratt, L.; Simkovic, M.; Novak, J.; Strugov, V.; Gill, D.; Gribben, J. G.; Kwei, K.; Dai, S.; Hsu, E.; Dean, J. P.; Flinn, I. W. First-Line Treatment of Chronic Lymphocytic Leukemia with Ibrutinib plus Obinutuzumab versus Chlorambucil plus Obinutuzumab: Final Analysis of the Randomized, Phase 3 ILLUMINATE Trial. Haematologica 2022. [CrossRef]
- Kater, A. P.; Owen, C.; Moreno, C.; Follows, G.; Munir, T.; Levin, M.-D.; Benjamini, O.; Janssens, A.; Osterborg, A.; Robak, T.; Simkovic, M.; Stevens, D.; Voloshin, S.; Vorobyev, V.; Ysebaert, L.; Qin, R.; Steele, A. J.; Schuier, N.; Baeten, K.; Caces, D. B. Fixed-Duration Ibrutinib-Venetoclax in Patients with Chronic Lymphocytic Leukemia and Comorbidities. NEJM Evidence 2022. [CrossRef]
- Sharman, J. P.; Egyed, M.; Jurczak, W.; Skarbnik, A.; Pagel, J. M.; Flinn, I. W.; Kamdar, M.; Munir, T.; Walewska, R.; Corbett, G.; Fogliatto, L. M.; Herishanu, Y.; Banerji, V.; Coutre, S.; Follows, G.; Walker, P.; Karlsson, K.; Ghia, P.; Janssens, A.; Cymbalista, F. Acalabrutinib with or without Obinutuzumab versus Chlorambucil and Obinutuzumab for Treatment-Naive Chronic Lymphocytic Leukaemia (ELEVATE-TN): A Randomised, Controlled, Phase 3 Trial. The Lancet 2020, 395(10232), 1278–1291. [Google Scholar] [CrossRef]
- Strati, P.; Parikh, S. A.; Chaffee, K. G.; Kay, N. E.; Call, T. G.; Achenbach, S. J.; Cerhan, J. R.; Slager, S. L.; Shanafelt, T. D. Relationship between Co-Morbidities at Diagnosis, Survival and Ultimate Cause of Death in Patients with Chronic Lymphocytic Leukaemia (CLL): A Prospective Cohort Study. British Journal of Haematology 2017, 178(3), 394–402. [Google Scholar] [CrossRef] [PubMed]
- Yancik, R. Cancer Burden in the Aged: An Epidemiologic and Demographic Overview. Cancer 1997, 80(7), 1273–1283. [Google Scholar] [CrossRef]
- Charlson, M. E.; Pompei, P.; Ales, K. L.; MacKenzie, C. Ronald. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. Journal of Chronic Diseases 1987, 40 (5), 373–383. [CrossRef]
- Yancik, R.; Wesley, M. N.; Ries, L. A. G.; Havlik, R. J.; Long, S.; Edwards, B. K.; Yates, J. W. Comorbidity and Age as Predictors of Risk for Early Mortality of Male and Female Colon Carcinoma Patients. Cancer 1998, 82(11), 2123–2134. [Google Scholar] [CrossRef]
- Rigolin, G. M.; Cavallari, M.; Quaglia, F. M.; Formigaro, L.; Lista, E.; Urso, A.; Guardalben, E.; Liberatore, C.; Faraci, D.; Saccenti, E.; Bassi, C.; Lupini, L.; Bardi, M. A.; Volta, E.; Tammiso, E.; Melandri, A.; Negrini, M.; Cavazzini, F.; Cuneo, A. In CLL, Comorbidities and the Complex Karyotype Are Associated with an Inferior Outcome Independently of CLL-IPI. Blood 2017, 129(26), 3495–3498. [Google Scholar] [CrossRef] [PubMed]
- Rotbain, E. C.; Niemann, C. U.; Rostgaard, K.; da Cunha-Bang, C.; Hjalgrim, H.; Frederiksen, H. Mapping Comorbidity in Chronic Lymphocytic Leukemia: Impact of Individual Comorbidities on Treatment, Mortality, and Causes of Death. Leukemia 2021, 35(9), 2570–2580. [Google Scholar] [CrossRef] [PubMed]
- Manda, S.; James, S.; Wang, R.; Krishnan, R.; Danilov, A. V. Impact of Comorbidities on Treatment Outcomes in Chronic Lymphocytic Leukemia: A Retrospective Analysis. Blood 2014, 124(21), 1312–1312. [Google Scholar] [CrossRef]
- Gordon, M. J.; Churnetski, M.; Alqahtani, H.; Rivera, X.; Kittai, A.; Amrock, S. M.; James, S.; Hoff, S.; Manda, S.; Spurgeon, S. E.; Choi, M.; Cohen, J. B.; Persky, D.; Danilov, A. V. Comorbidities Predict Inferior Outcomes in Chronic Lymphocytic Leukemia Treated with Ibrutinib. Cancer 2018, 124(15), 3192–3200. [Google Scholar] [CrossRef]
- Tedeschi, A.; Frustaci, A. M.; Mauro, F. R.; Chiarenza, A.; Coscia, M.; Ciolli, S.; Reda, G.; Laurenti, L.; Varettoni, M.; Murru, R.; Baratè, C.; Sportoletti, P.; Greco, A.; Borella, C.; Rossi, V.; Deodato, M.; Biagi, A.; Curto Pelle, A.; Lapietra, G.; Vitale, C. Do Age, Fitness and Concomitant Medications Influence Management and Outcomes of CLL Patients Treated with Ibrutinib? Blood 2020, 136 (Supplement 1), 54–55. [Google Scholar] [CrossRef]
- Gordon, M. J.; Kaempf, A.; Sitlinger, A.; Shouse, G.; Mei, M.; Brander, D. M.; Salous, T.; Hill, B. T.; Alqahtani, H.; Choi, M.; Churnetski, M. C.; Cohen, J. B.; Stephens, D. M.; Siddiqi, T.; Rivera, X.; Persky, D.; Wisniewski, P.; Patel, K.; Shadman, M.; Park, B. The Chronic Lymphocytic Leukemia Comorbidity Index (CLL-CI): A Three-Factor Comorbidity Model. Clinical Cancer Research 2021, 27(17), 4814–4824. [Google Scholar] [CrossRef] [PubMed]
- Rotbain, E. C.; Gordon, M. J.; Vainer, N.; Frederiksen, H.; Hjalgrim, H.; Danilov, A. V.; Niemann, C. U. The CLL Comorbidity Index in a Population-Based Cohort: A Tool for Clinical Care and Research. Blood Advances 2022, 6(8), 2701–2706. [Google Scholar] [CrossRef]
- Klepin, H. D. Ready for Prime Time: Role for Geriatric Assessment to Improve Quality of Care in Hematology Practice. Blood 2019, 134(23), 2005–2012. [Google Scholar] [CrossRef]
- Repetto, L.; Fratino, L.; Audisio, R. A.; Venturino, A.; Gianni, W.; Vercelli, M.; Parodi, S.; Dal Lago, D.; Gioia, F.; Monfardini, S.; Aapro, M. S.; Serraino, D.; Zagonel, V. Comprehensive Geriatric Assessment Adds Information to Eastern Cooperative Oncology Group Performance Status in Elderly Cancer Patients: An Italian Group for Geriatric Oncology Study. Journal of Clinical Oncology 2002, 20(2), 494–502. [Google Scholar] [CrossRef]
- Goede, V.; Bahlo, J.; Chataline, V.; Eichhorst, B.; Dürig, J.; Stilgenbauer, S.; Kolb, G.; Honecker, F.; Wedding, U.; Hallek, M. Evaluation of Geriatric Assessment in Patients with Chronic Lymphocytic Leu-kemia: Results of the CLL9 Trial of the German CLL Study Group. Leukemia & Lymphoma 2015, 57 (4), 789–796. [CrossRef]
- Bonanad, S.; De la Rubia, J.; Gironella, M.; Pérez Persona, E.; González, B.; Fernández Lago, C.; Arnan, M.; Zudaire, M.; Hernández Rivas, J. A.; Soler, A.; Marrero, C.; Olivier, C.; Altés, A.; Valcárcel, D.; Hernández, M. T.; Oiartzabal, I.; Fernández Ordoño, R.; Arnao, M.; Esquerra, A.; Sarrá, J. Development and Psychometric Validation of a Brief Comprehensive Health Status Assessment Scale in Older Patients with Hematological Malignancies: The GAH Scale. Journal of Geriatric Oncology 2015, 6(5), 353–361. [Google Scholar] [CrossRef] [PubMed]
- de la Rubia, J.; González, B.; Cruz-Jentoft, A. J.; Iglesias, L.; Jarque, I.; Persona, E. P.; Lluch, R.; Marrero, C.; Zudaire, M.; Gironella, M.; Hernández-Rivas, J. Á.; Arnan, M.; Olivier, C.; Encinas, C.; Soler, J. A.; Payer, Á. R.; Casado, A.; Fernández, P.; Vilanova, D.; Bonanad, S. Geriatric Assessment in Hematology Scale Predicts Treatment Tolerability in Older Patients Diagnosed with Hematological Malignancies: The RETROGAH Study. Journal of Geriatric Oncology 2022, 101401. [Google Scholar] [CrossRef] [PubMed]
- <b>41. </b>P. Connor, Johnson; Woyach, J. A.; Ulrich, A.; Marcotte, V.; Nipp, R. D.; Lage, D. E.; Nelson, A. M.; Newcomb, R. A.; Rice, J.; Lavoie, M. W.; Ritchie, C. S.; Bartlett, N.; Stephens, D. M.; Ding, W.; Owen, C.; Stone, R.; Ruppert, A. S.; Mandrekar, S. J.; Byrd, J. C. P. Connor Johnson; Woyach, J. A.; Ulrich, A.; Marcotte, V.; Nipp, R. D.; Lage, D. E.; Nelson, A. M.; Newcomb, R. A.; Rice, J.; Lavoie, M. W.; Ritchie, C. S.; Bartlett, N.; Stephens, D. M.; Ding, W.; Owen, C.; Stone, R.; Ruppert, A. S.; Mandrekar, S. J.; Byrd, J. C.; Areej El-Jawahri. Geriatric Assessment Measures Are Predictive of Outcomes in Chronic Lymphocytic Leukemia. J Geriatr Oncol. 2023, 14 (6), 101538–101538. [CrossRef]
- Woyach, J. A. Making Clinical Trials Work for Older Patients with Chronic Lymphocytic Leukemia. Journal of Geriatric Oncology 2020, 11(1), 17–18. [Google Scholar] [CrossRef] [PubMed]
- Eichhorst, B. F.; Busch, R.; Stilgenbauer, S.; Stauch, M.; Bergmann, M. A.; Ritgen, M.; Kranzhöfer, N.; Rohrberg, R.; Söling, U.; Burkhard, O.; Westermann, A.; Goede, V.; Schweighofer, C. D.; Fischer, K.; Fink, A.-M.; Wendtner, C. M.; Brittinger, G.; Döhner, H.; Emmerich, B.; Hallek, M. First-Line Therapy with Fludarabine Compared with Chlorambucil Does Not Result in a Major Benefit for Elderly Patients with Advanced Chronic Lymphocytic Leukemia. Blood 2009, 114(16), 3382–3391. [Google Scholar] [CrossRef]
- Hallek, M.; Al-Sawaf, O. Chronic Lymphocytic Leukemia: 2022 Update on Diagnostic and Therapeutic Procedures. American Journal of Hematology 2021, 96(12), 1679–1705. [Google Scholar] [CrossRef]
- Byrd, J. C.; Brown, J. R.; O’Brien, S.; Barrientos, J. C.; Kay, N. E.; Reddy, N. M.; Coutre, S.; Tam, C. S.; Mulligan, S. P.; Jaeger, U.; Devereux, S.; Barr, P. M.; Furman, R. R.; Kipps, T. J.; Cymbalista, F.; Pocock, C.; Thornton, P.; Caligaris-Cappio, F.; Robak, T.; Delgado, J. Ibrutinib versus Ofatumumab in Previously Treated Chronic Lymphoid Leukemia. New England Journal of Medicine 2014, 371(3), 213–223. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A. W.; Davids, M. S.; Pagel, J. M.; Kahl, B. S.; Puvvada, S. D.; Gerecitano, J. F.; Kipps, T. J.; Anderson, M. A.; Brown, J. R.; Gressick, L.; Wong, S.; Dunbar, M.; Zhu, M.; Desai, M. B.; Cerri, E.; Heitner Enschede, S.; Humerickhouse, R. A.; Wierda, W. G.; Seymour, J. F. Targeting BCL2 with Venetoclax in Relapsed Chronic Lymphocytic Leukemia. New England Journal of Medicine 2016, 374(4), 311–322. [Google Scholar] [CrossRef]
- O’Brien, S.; Jones, J. A.; Coutre, S. E.; Mato, A. R.; Hillmen, P.; Tam, C.; Österborg, A.; Siddiqi, T.; Thirman, M. J.; Furman, R. R.; Ilhan, O.; Keating, M. J.; Call, T. G.; Brown, J. R.; Stevens-Brogan, M.; Li, Y.; Clow, F.; James, D. F.; Chu, A. D.; Hallek, M. Ibrutinib for Patients with Relapsed or Refractory Chronic Lymphocytic Leukaemia with 17p Deletion (RESONATE-17): A Phase 2, Open-Label, Multicentre Study. The Lancet Oncology 2016, 17(10), 1409–1418. [Google Scholar] [CrossRef]
- Stilgenbauer, S.; Eichhorst, B.; Schetelig, J.; Hillmen, P.; Seymour, J. F.; Coutre, S.; Jurczak, W.; Mulligan, S. P.; Schuh, A.; Assouline, S.; Wendtner, C.-M.; Roberts, A. W.; Davids, M. S.; Bloehdorn, J.; Munir, T.; Böttcher, S.; Zhou, L.; Salem, A. H.; Desai, M.; Chyla, B. Venetoclax for Patients with Chronic Lymphocytic Leukemia with 17p Deletion: Results from the Full Population of a Phase II Pivotal Trial. Journal of Clinical Oncology 2018, 36(19), 1973–1980. [Google Scholar] [CrossRef]
- Barr, P. M.; Owen, C.; Robak, T.; Tedeschi, A.; Bairey, O.; Burger, J. A.; Hillmen, P.; Coutre, S. E.; Dearden, C.; Grosicki, S.; McCarthy, H.; Li, J.-Y.; Offner, F.; Moreno, C.; Zhou, C.; Hsu, E.; Szoke, A.; Kipps, T. J.; Ghia, P. Up to 8-Year Follow-up from RESONATE-2: First-Line Ibrutinib Treatment for Patients with Chronic Lymphocytic Leukemia. Blood Advances 2022, 6(11), 3440–3450. [Google Scholar] [CrossRef] [PubMed]
- Barr, P. M.; Robak, T.; Owen, C.; Tedeschi, A. ; Osnat Bairey; Bartlett, N. L., Burger, J. A., Hillmen, P., Coutre, S., Devereux, S., Grosicki, S., McCarthy, H. O., Li, J., Simpson, D., Offner, F., Moreno, C., Zhou, C., Styles, L., James, D. F., Eds.; Kipps, T. J. Sustained Efficacy and Detailed Clinical Follow-up of First-Line Ibrutinib Treatment in Older Patients with Chronic Lymphocytic Leukemia: Extended Phase 3 Results from RESONATE-2. Haematologica 2018, 103 (9), 1502–1510. [Google Scholar] [CrossRef]
- Woyach, J. A.; Ruppert, A. S.; Heerema, N. A.; Zhao, W.; Booth, A. M.; Ding, W.; Bartlett, N. L.; Brander, D. M.; Barr, P. M.; Rogers, K. A.; Parikh, S. A.; Coutre, S.; Lozanski, G. ; Sreenivasa Nattam; Larson, R. A.; Erba, H. P.; Litzow, M. R.; Blachly, J. S.; Owen, C.; Kuzma, C. S. Long-Term Results of Alliance A041202 Show Continued Advantage of Ibrutinib-Based Regimens Compared with Bendamustine plus Rituximab (BR) Chemoimmunotherapy. 2021, 138 (Supplement 1), 639–639. [CrossRef]
- Ruppert, A. S.; Booth, A. M.; Ding, W.; Bartlett, N. L.; Brander, D. M.; Coutre, S.; Brown, J. R. ; Sreenivasa Nattam; Larson, R. A., Erba, H. P., Litzow, M. R., Owen, C., Kuzma, C. S., Abramson, J. S., Little, R. F., Smith, S. T., Stone, R., Byrd, J. C., Mandrekar, S. J., Eds.; Woyach, J. A. Adverse Event Burden in Older Patients with CLL Receiving Bendamustine plus Rituximab or Ibrutinib Regimens: Alliance A041202. Leukemia 2021, 35 (10), 2854–2861. [Google Scholar] [CrossRef]
- Wu, J.; Zhang, M.; Liu, D. Acalabrutinib (ACP-196): A Selective Second-Generation BTK Inhibitor. Journal of Hematology & Oncology 2016, 9 (1). [CrossRef]
- Byrd, J. C.; Hillmen, P.; Ghia, P.; Kater, A. P.; Chanan-Khan, A.; Furman, R. R.; O’Brien, S.; Yenerel, M. N.; Illés, A.; Kay, N.; Garcia-Marco, J. A.; Mato, A.; Pinilla-Ibarz, J.; Seymour, J. F.; Lepretre, S.; Stilgenbauer, S.; Robak, T.; Rothbaum, W.; Izumi, R.; Hamdy, A. Acalabrutinib versus Ibrutinib in Previously Treated Chronic Lymphocytic Leukemia: Results of the First Randomized Phase III Trial. Journal of Clinical Oncology 2021, 39(31), 3441–3452. [Google Scholar] [CrossRef]
- Munir, T.; Shadman, M.; Robak, T.; Brown, J.; Kahl, B.; Ghia, P.; Giannopoulos, K.; Simkovic, M.; Österberg, A.; Laurenti, L.; Walker, P.; Opat, S.; Ciepluch, H.; Greil, R.; Hanna, M.; Tani, M.; Trneny, M.; Brander, D. M.; Flinn, I. W.; Grosicki, S.; Verner, E.; Tedeschi, T.; De Guibert, S.; Tumyan, G.; Laribi, K.; Garcia Marco, J. A.; Li, J.; Tian, T.; Ramakrishnan, V.; Liu, Y.; Szeto, A.; Paik, J.; Cohen, A.; Tam, C.; Jurczak, W. ZANUBRUTINIB (ZANU) VS BENDAMUSTINE + RITUXIMAB (BR) IN PATIENTS (PTS) WITH TREATMENT-NAÏVE CHRONIC LYMPHOCYTIC LEUKEMIA/SMALL LYMPHOCYTIC LYMPHOMA (CLL/SLL): EXTENDED FOLLOW-UP OF THE SEQUOIA STUDY. 8 June 2023; -11. [Google Scholar]
- Tam, C. S.; Robak, T.; Ghia, P.; Kahl, B. S.; Walker, P.; Janowski, W.; Simpson, D.; Shadman, M.; Ganly, P. S.; Laurenti, L.; Opat, S.; Tani, M.; Ciepluch, H.; Verner, E.; Šimkovič, M.; Österborg, A.; Trněný, M.; Tedeschi, A.; Paik, J. C.; Kuwahara, S. B. Zanubrutinib Monotherapy for Patients with Treatment-Naïve Chronic Lymphocytic Leukemia and 17p Deletion. Haematologica 2020, 106(9), 2354–2363. [Google Scholar] [CrossRef]
- Kapoor, I.; Bodo, J.; Hill, B. T.; Hsi, E. D.; Almasan, A. Targeting BCL-2 in B-Cell Malignancies and Overcoming Therapeutic Resistance. Cell Death & Disease 2020, 11 (11). [CrossRef]
- Stilgenbauer, S.; Eichhorst, B.; Schetelig, J.; Coutre, S.; Seymour, J. F.; Munir, T.; Puvvada, S. D.; Wendtner, C.-M.; Roberts, A. W.; Jurczak, W.; Mulligan, S. P.; Böttcher, S.; Mobasher, M.; Zhu, M.; Desai, M.; Chyla, B.; Verdugo, M.; Enschede, S. H.; Cerri, E.; Humerickhouse, R. Venetoclax in Relapsed or Refractory Chronic Lymphocytic Leukaemia with 17p Deletion: A Multicentre, Open-Label, Phase 2 Study. The Lancet Oncology 2016, 17(6), 768–778. [Google Scholar] [CrossRef] [PubMed]
- Seymour, J. F.; Kipps, T. J.; Eichhorst, B.; Hillmen, P.; D’Rozario, J.; Assouline, S.; Owen, C.; Gerecitano, J.; Robak, T.; De la Serna, J.; Jaeger, U.; Cartron, G.; Montillo, M.; Humerickhouse, R.; Punnoose, E. A.; Li, Y.; Boyer, M.; Humphrey, K.; Mobasher, M.; Kater, A. P. Venetoclax–Rituximab in Relapsed or Refractory Chronic Lymphocytic Leukemia. New England Journal of Medicine 2018, 378(12), 1107–1120. [Google Scholar] [CrossRef] [PubMed]
- <b>60. </b>Othman, Al-Sawaf; Zhang, C.; Hyun Yong, Jin; Robrecht, S.; Choi, Y.; Balasubramanian, S.; Kotak, A.; Yi Meng, Chang; Anna Maria, Fink; Tausch, E.; Schneider, C.; Matthias, Ritgen; Kreuzer, K.-A.; Chyla, B.; Paulson, J.; Pallasch, C. P.; Frenzel, L. P.; Peifer, M.; Eichhorst, B.; Stilgenbauer, S. Othman Al-Sawaf; Zhang, C.; Hyun Yong Jin; Robrecht, S.; Choi, Y.; Balasubramanian, S.; Kotak, A.; Yi Meng Chang; Anna Maria Fink; Tausch, E.; Schneider, C.; Matthias Ritgen; Kreuzer, K.-A.; Chyla, B.; Paulson, J.; Pallasch, C. P.; Frenzel, L. P.; Peifer, M.; Eichhorst, B.; Stilgenbauer, S. Transcriptomic Profiles and 5-Year Results from the Randomized CLL14 Study of Venetoclax plus Obinutuzumab versus Chlorambucil plus Obinutuzumab in Chronic Lymphocytic Leukemia. 2023, 14 (1). [CrossRef]
- Thompson, M.; Brander, D.; Nabhan, C.; Mato, A. Minimal Residual Disease in Chronic Lymphocytic Leukemia in the Era of Novel Agents. JAMA Oncology 2018, 4(3), 394. [Google Scholar] [CrossRef]
- Al-Sawaf, O.; Gentile, B.; Devine, J.; Zhang, C.; Sail, K.; Tandon, M.; Fink, A.; Kutsch, N.; Wendtner, C.; Eichhorst, B.; Hallek, M.; Fischer, K. Health-Related Quality of Life with Fixed-Duration Venetoclax-Obinutuzumab for Previously Untreated Chronic Lymphocytic Leukemia: Results from the Randomized, Phase 3 CLL14 Trial. American Journal of Hematology 2021, 96(9), 1112–1119. [Google Scholar] [CrossRef]
- Lu, P.; Wang, S.; Franzen, C. A.; Venkataraman, G.; McClure, R.; Li, L.; Wu, W.; Niu, N.; Sukhanova, M.; Pei, J.; Baldwin, D. A.; Nejati, R.; Wasik, M. A.; Khan, N.; Tu, Y.; Gao, J.; Chen, Y.; Ma, S.; Larson, R. A.; Wang, Y. L. Ibrutinib and Venetoclax Target Distinct Subpopulations of CLL Cells: Implication for Resid-ual Disease Eradication. Blood Cancer Journal 2021, 11 (2). [CrossRef]
- Deng, J.; Isik, E.; Fernandes, S. M.; Brown, J. R.; Letai, A.; Davids, M. S. Bruton’s Tyrosine Kinase Inhibition Increases BCL-2 Dependence and Enhances Sensitivity to Venetoclax in Chronic Lymphocytic Leukemia. Leukemia 2017, 31(10), 2075–2084. [Google Scholar] [CrossRef]
- Jain, N.; Keating, M.; Thompson, P.; Ferrajoli, A.; Burger, J.; Borthakur, G.; Takahashi, K.; Estrov, Z.; Fowler, N.; Kadia, T.; Konopleva, M.; Alvarado, Y.; Yilmaz, M.; DiNardo, C.; Bose, P.; Ohanian, M.; Pemmaraju, N.; Jabbour, E.; Sasaki, K.; Kanagal-Shamanna, R. Ibrutinib and Venetoclax for First-Line Treatment of CLL. New England Journal of Medicine 2019, 380(22), 2095–2103. [Google Scholar] [CrossRef] [PubMed]
- Wierda, W. G.; Allan, J. N.; Siddiqi, T.; Kipps, T. J.; Opat, S.; Tedeschi, A.; Badoux, X. C.; Kuss, B. J.; Jackson, S.; Moreno, C.; Jacobs, R.; Pagel, J. M.; Flinn, I.; Pak, Y.; Zhou, C.; Szafer-Glusman, E.; Ninomoto, J.; Dean, J. P.; James, D. F.; Ghia, P. Ibrutinib plus Venetoclax for First-Line Treatment of Chronic Lymphocytic Leukemia: Primary Analysis Results from the Minimal Residual Disease Cohort of the Randomized Phase II CAPTIVATE Study. Journal of Clinical Oncology 2021, 39(34), 3853–3865. [Google Scholar] [CrossRef]
- Tam, C. S.; Allan, J. N.; Siddiqi, T.; Kipps, T. J.; Jacobs, R.; Opat, S.; Barr, P. M.; Tedeschi, A.; Trentin, L.; Bannerji, R.; Jackson, S.; Kuss, B. J.; Moreno, C.; Szafer-Glusman, E.; Russell, K.; Zhou, C.; Ninomoto, J.; Dean, J. P.; Wierda, W. G.; Ghia, P. Fixed-Duration Ibrutinib plus Venetoclax for First-Line Treatment of CLL: Primary Analysis of the CAPTIVATE FD Cohort. Blood 2022, 139(22), 3278–3289. [Google Scholar] [CrossRef]
- Marchetti, M.; Vitale, C.; Rigolin, G. M.; Vasile, A.; Visentin, A.; Scarfò, L.; Coscia, M.; Cuneo, A. Old and New Drugs for Chronic Lymphocytic Leukemia: Lights and Shadows of Real-World Evidence. Journal of Clinical Medicine 2022, 11(8), 2076. [Google Scholar] [CrossRef]
- El-Galaly, T. C.; Cheah, C. Y.; Villa, D. Real World Data as a Key Element in Precision Medicine for Lymphoid Malignancies: Potentials and Pitfalls. British Journal of Haematology 2019, 186(3), 409–419. [Google Scholar] [CrossRef] [PubMed]
- Ibrutinib for Relapsed/Refractory Chronic Lymphocytic Leukemia: A UK and Ireland Analysis of Outcomes in 315 Patients. Haematologica 2016, 101(12), 1563–1572. [CrossRef]
- Karim, S.; Booth, C. M. Effectiveness in the Absence of Efficacy: Cautionary Tales from Real-World Ev-idence. Journal of Clinical Oncology 2019, 37(13), 1047–1050. [Google Scholar] [CrossRef] [PubMed]
- Islam, P.; Mato, A. R. Utilizing Real-World Evidence (RWE) to Improve Care in Chronic Lymphocytic Leukemia: Challenges and Opportunities. Current Hematologic Malignancy Reports 2020. [CrossRef]
- Ghia, P.; Cuneo, A. Ibrutinib in the Real World Patient: Many Lights and Some Shades. Haematologica 2016, 101(12), 1448–1450. [Google Scholar] [CrossRef] [PubMed]
- Goyal, R. K.; Nagar, S. P.; Kabadi, S. M.; Le, H.; Davis, K. L.; Kaye, J. A. Overall Survival, Adverse Events, and Economic Burden in Patients with Chronic Lymphocytic Leukemia Receiving Systemic Therapy: Real-World Evidence from the Medicare Population. Cancer Medicine 2021, 10(8), 2690–2702. [Google Scholar] [CrossRef]
- Narezkina, A.; Akhter, N.; Lu, X.; Emond, B.; Panjabi, S.; Forbes, S. P.; Hilts, A.; Liu, S.; Lafeuille, M.-H.; Lefebvre, P.; Huang, Q.; Choi, M. Real-World Persistence and Time to next Treatment with Ibrutinib in Patients with Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Including Patients at High Risk for Atrial Fibrillation or Stroke. Clinical Lymphoma Myeloma and Leukemia 2022, 22(11), e959–e971. [Google Scholar] [CrossRef]
- Mato, A. R.; Tang, B.; Azmi, S.; Yang, K.; Zhang, X.; Stern, J. C.; Hedrick, E.; Huang, J.-S.; Sharman, J. P. A Clinical Practice Comparison of Patients with Chronic Lymphocytic Leukemia with and without Deletion 17p Receiving First-Line Treatment with Ibrutinib. 2022, 107 (11), 2630–2640. [CrossRef]
- Rigolin, G.M.; Olimpieri, P. P.; Summa, V.; Celant, S.; Scarfò, L.; Tognolo, L. ; Maria Pia Ballardini; Urso, A.; Sessa, M.; Gambara, S.; Cura, F.; Fortini, M.; Ghia, P.; Cuneo, A.; Russo, P. Outcomes in Patients with Chronic Lymphocytic Leukemia and TP53 Aberration Who Received First Line Ibrutinib: A Nationwide Registry Study from the Italian Medicines Agency. Blood Cancer Journal. 2023. [CrossRef]
- Visentin, A.; Mauro, F. R.; Cibien, F.; Vitale, C.; Reda, G.; Fresa, A.; Ciolli, S.; Pietrasanta, D.; Marchetti, M.; Murru, R.; Gentile, M.; Rigolin, G. M.; Quaglia, F. M.; Scarfò, L.; Sportoletti, P.; Pravato, S.; Piazza, F.; Coscia, M.; Laurenti, L.; Molica, S. Continuous Treatment with Ibrutinib in 100 Untreated Patients with TP 53 Disrupted Chronic Lymphocytic Leukemia: A Real-Life Campus CLL Study. American Journal of Hematology 2021, 97 (3). [CrossRef]
- Cuneo, A.; Mato, A. R.; Rigolin, G. M.; Piciocchi, A.; Gentile, M.; Laurenti, L.; Allan, J. N.; Pagel, J. M.; Brander, D. M.; Hill, B. T.; Winter, A.; Lamanna, N.; Tam, C. S.; Jacobs, R.; Lansigan, F.; Barr, P. M.; Shadman, M.; Skarbnik, A. P.; Pu, J. J.; Sehgal, A. R. Efficacy of Bendamustine and Rituximab in Unfit Patients with Previously Untreated Chronic Lymphocytic Leukemia. Indirect Comparison with Ibrutinib in a Real-World Setting. A GIMEMA-ERIC and US Study. Cancer Medicine 2020, 9 (22), 8468–8479. [CrossRef]
- Visentin, A.; Mauro, F. R.; Catania, G.; Fresa, A.; Vitale, C.; Sanna, A.; Mattiello, V.; Cibien, F.; Sporto-letti, P.; Gentile, M.; Rigolin, G. M.; Quaglia, F. M.; Murru, R.; Gozzetti, A.; Molica, S.; Marchetti, M.; Pravato, S.; Angotzi, F.; Cellini, A.; Scarfò, L. Obinutuzumab plus Chlorambucil versus Ibrutinib in Pre-viously Untreated Chronic Lymphocytic Leukemia Patients without TP53 Disruptions: A Real-Life CLL Campus Study. Frontiers in Oncology 2022, 12. [Google Scholar] [CrossRef]
- Green, T.; Bron, D.; Chomienne, C.; de Wit, T. D.; de Haas, F.; Engert, A.; Hagenbeek, A.; Jäger, U.; MacIntyre, E.; Muckenthaler, M. U.; Smand, C.; Sonneveld, P. Costs of Haematological Disease High and Rising. The Lancet Haematology 2016, 3(8), e353–e354. [Google Scholar] [CrossRef]
- Chen, Q.; Jain, N.; Ayer, T.; Wierda, W. G.; Flowers, C. R.; O’Brien, S. M.; Keating, M. J.; Kantarjian, H. M.; Chhatwal, J. Economic Burden of Chronic Lymphocytic Leukemia in the Era of Oral Targeted Therapies in the United States. Journal of Clinical Oncology 2017, 35(2), 166–174. [Google Scholar] [CrossRef]
- Scheffer Cliff, E. R.; Kesselheim, A. S.; Rome, B. N.; Feldman, W. B. Trends in Medicare Spending on Oral Drugs for Chronic Lymphocytic Leukemia from 2014 to 2020. JAMA network open 2023, 6(4), e237467–e237467. [Google Scholar] [CrossRef]
- Shanafelt, T. D.; Borah, B. J.; Finnes, H. D.; Rabe, K. G.; Ding, W.; Leis, J. F. ; Asher Chanan-Khan; Parikh, S. A.; Slager, S. L.; Kay, N. E.; Call, T. G. Impact of Ibrutinib and Idelalisib on the Pharmaceutical Cost of Treating Chronic Lymphocytic Leukemia at the Individual and Societal Levels. J. Oncol. Pract. 2015, 11 (3), 252–258. [CrossRef]
- Mansfield, C.; Masaquel, A.; Sutphin, J.; Weiss, E.; Gutierrez, M.; Wilson, J.; Boeri, M.; Li, J.; Reyes, C. Patients’ Priorities in Selecting Chronic Lymphocytic Leukemia Treatments. Blood Advances 2017, 1(24), 2176–2185. [Google Scholar] [CrossRef] [PubMed]
- Cuneo, A.; Cavazzini, F.; Cavallari, M.; Foà, R. ; Gian Matteo Rigolin. Optimal Management of Chronic Lymphocytic Leukemia and Economic Constraints. Cancer J 2021 Jul-Aug;27(4):320-327. [CrossRef]
- Khan HM, Ramsey S, Shankaran V. Financial Toxicity in Cancer Care: Implications for Clinical Care and Potential Practice Solutions. J Clin Oncol. 2023 Jun 1;41(16):3051-3058. [CrossRef] [PubMed]
- Chatterjee, A. ; van; Goeree, R.; Owen, C.; A.C. Desbois; Barakat, S.; Manzoor, B. S.; Kavita Sail. A Probabilistic Cost-Effectiveness Analysis of Venetoclax and Obinutuzumab as a First-Line Therapy in Chronic Lymphocytic Leukemia in Canada. Pharmacoecon. Open 2023 Mar;7(2):199-216. [CrossRef]
- Munir, T.; Genovez, V.; Genestier, V.; Ryan, K. ; Bengt Liljas; Priyanka Gaitonde. Cost-Effectiveness of Acalabrutinib Regimens in Treatment-Naïve Chronic Lymphocytic Leukemia in the United States. Expert. Rev. Pharmacoecon. Outcomes Res. 2023 Jun;23(5):579-589. [CrossRef]
- Slot M, Niemann CU., Ehlers LH., Rotbain EC. Cost-effectiveness of targeted treatment vs chemoimmunotherapy in treatment-naïve unfit CLL without TP53 aberrations. Blood Adv. 2023 [Epub ahead of print]. 15 May. [PubMed]
- Vokinger, K. N.; Hwang, T. J.; Grischott, T.; Reichert, S.; Tibau, A.; Rosemann, T.; Kesselheim, A. S. Prices and Clinical Benefit of Cancer Drugs in the USA and Europe: A Cost–Benefit Analysis. The Lancet Oncology 2020, 21(5), 664–670. [Google Scholar] [CrossRef] [PubMed]
- United Nations. World Population Prospects 2022, available at https://population.un. (accessed on 15 May 2023)1829.
- Eurostat statistics explained. Available at https://ec.europa.eu/eurostat/statistics-explained/SEPDF/cache/80393. (accessed on 15 May 2023).
- Wierda, W. G.; Brown, J.; Abramson, J. S.; Awan, F.; Bilgrami, S. F.; Bociek, G.; Brander, D.; Chanan-Khan, A. A.; Coutre, S. E.; Davis, R. S.; Eradat, H.; Fletcher, C. D.; Gaballa, S.; Ghobadi, A.; Hamid, M. S.; Hernandez-Ilizaliturri, F.; Hill, B.; Kaesberg, P.; Kamdar, M.; Kaplan, L. D. NCCN Guidelines® Insights: Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma, Version 3. 2022. Journal of the National Comprehensive Cancer Network 2022, 20(6), 622–634. [Google Scholar] [CrossRef] [PubMed]
- Eichhorst, B.; Robak, T.; Montserrat, E.; Ghia, P.; Niemann, C. U.; Kater, A. P.; Gregor, M.; Cymbalista, F.; Buske, C.; Hillmen, P.; Hallek, M.; Mey, U. Chronic Lymphocytic Leukaemia: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Annals of Oncology 2021, 32(1), 23–33. [Google Scholar] [CrossRef]
- Ahn, I. E.; Brown, J. R. Selecting Initial Therapy in CLL. Hematology Am Soc Hematol Educ Program. 2022;2022(1):323-328. [CrossRef]
- Kim, M. S.; Prasad, V. Front-Line Chronic Lymphocytic Leukemia: The Role of Chemoimmunotherapy. Am. J Hematol. 2023, 98(4), 560-561. https://10.1002/ajh. 2686. [Google Scholar]
- Brown, J. R. Relapsed CLL: Sequencing, Combinations, and Novel Agents. Hematology Am. Soc. Hematol. Educ. Program. 2018, 2018, 1, 248–255. [Google Scholar] [CrossRef]
- Kittai, AS. : Miller, C.; Goldstein, D.; Huang, Y;. Abruzzo, LV;. Beckwith, K,; Bhat, SA.; Bond DA, Grever, MR.; Heerema, NA.; Rogers, KA.; Ruppert, AS.; Byrd.; JC, Woyach, JA. The impact of increasing karyotypic complexity and evolution on survival in patients with CLL treated with ibrutinib. Blood. 2021, 138(23):2372-2382.
- Mauro, F. R.; Paoloni, F.; Molica, S.; Reda, G.; Trentin, L.; Sportoletti, P.; Marchetti, M.; Pietrasanta, D.; Marasca, R.; Gaidano, G.; Coscia, M.; Stelitano, C.; Mannina, D.; Di Renzo, N.; Ilariucci, F.; Liberati, A. M.; Orsucci, L.; Re, F.; Tani, M.; Musuraca, G. Efficacy of Front-Line Ibrutinib and Rituximab Combination and the Impact of Treatment Discontinuation in Unfit Patients with Chronic Lymphocytic Leukemia: Results of the Gimema LLC1114 Study. Cancers 2021, 14(1), 207. [Google Scholar] [CrossRef]
- Rigolin, G. M.; Del Giudice, I.; Bardi, A.; Melandri, A.; García-Jacobo, R. E.; Cura, F.; Raponi, S.; Ilari, C.; Cafforio, L.; Piciocchi, A.; Arena, V.; Reda, G.; Albano, F.; Molica, S.; Sportoletti, P.; Trentin, L.; Marchetti, M.; Nanni, M.; Peragine, N.; Mariglia, P. Complex Karyotype in Unfit Patients with CLL Treated with Ibrutinib and Rituximab: The GIMEMA LLC1114 Phase 2 Study. Blood 2021, 138(25), 2727–2730. [Google Scholar] [CrossRef]
- Fürstenau, M.; Thus, YJ.; Robrecht, S. ; Mellink, CHM.; van der Kevie-Kersemaekers, AF.; Dubois, J.; von Tresckow, J.; Patz, M.; Gregor, M.; Thornton, P.; Staber, PB.; Tadmor, T.; Levin, MD.; da Cunha-Bang, C.; Schneider, C.; Poulsen, CB.; Illmer, T,; Schöttker, B.; Janssens, A.; Christiansen, I.; Noesslinger, T.; Baumann, M.; Hebart, H.; Gaska, T.; Regelink, J.; Dompeling, EC.; Lindstrom, V.; Juliusson, G,; Widmer, AA.; Goede, JS.; Goldschmidt, N,; Simon, F,; De Silva, N.; Fink, AM,; Fischer, K.; Wendtner. CM.; Ritgen, M.; Brüggemann, M.; Tausch, E.; Spaargaren, M.; Eldering, E.; Stilgenbauer, S.; Niemann, CU.; Hallek, M.; Eichhorst, B.; Kreuzer, KA.; Kater, AP. High karyotypic complexity is an independent prognostic factor in patients with CLL treated with venetoclax combinations. Blood. 2023 :blood.2023019634. 12 May; ahead of print. [CrossRef] [PubMed]
- Brown, J. R.; Eichhorst, B.; Hillmen, P.; Jurczak, W.; Kaźmierczak, M.; Lamanna, N.; O’Brien, S. M.; Tam, C. S.; Qiu, L.; Zhou, K.; Simkovic, M.; Mayer, J.; Gillespie-Twardy, A.; Ferrajoli, A.; Ganly, P. S.; Weinkove, R.; Grosicki, S.; Mital, A.; Robak, T.; Osterborg, A. Zanubrutinib or Ibrutinib in Relapsed or Refractory Chronic Lymphocytic Leukemia. New England Journal of Medicine 2023, 388(4), 319–332. [Google Scholar] [CrossRef]
- Lachaine, J.; Guinan, K.; Aw, A.; Banerji, V.; Fleury, I.; Owen, C. Impact of Fixed-Duration Oral Targeted Therapies on the Economic Burden of Chronic Lymphocytic Leukemia in Canada. Current Oncology 2023, 30(5), 4483–4498. [Google Scholar] [CrossRef]
- Moreno, C.; Greil, R.; Demirkan, F.; Tedeschi, A.; Anz, B.; Larratt, L.; Simkovic, M.; Samoilova, O.; Novak, J.; Ben-Yehuda, D.; Strugov, V.; Gill, D.; Gribben, J. G.; Hsu, E.; Lih, C.-J.; Zhou, C.; Clow, F.; James, D. F.; Styles, L.; Flinn, I. W. Ibrutinib plus Obinutuzumab versus Chlorambucil plus Obinutuzumab in First-Line Treatment of Chronic Lymphocytic Leukaemia (ILLUMINATE): A Multicentre, Randomised, Open-Label, Phase 3 Trial. The Lancet Oncology 2019, 20(1), 43–56. [Google Scholar] [CrossRef] [PubMed]
- Burger, J. A.; Tedeschi, A.; Barr, P. M.; Robak, T.; Owen, C.; Ghia, P.; Bairey, O.; Hillmen, P.; Bartlett, N. L.; Li, J.; Simpson, D.; Grosicki, S.; Devereux, S.; McCarthy, H.; Coutre, S.; Quach, H.; Gaidano, G.; Maslyak, Z.; Stevens, D. A.; Janssens, A. Ibrutinib as Initial Therapy for Patients with Chronic Lymphocytic Leukemia. New England Journal of Medicine 2015, 373(25), 2425–2437. [Google Scholar] [CrossRef]
- The National Institute for Health and Care Excellence. Evidence-based recommendations on venetoclax (Venclyxto) with obinutuzumab for untreated chronic lymphocytic leukaemia in adults Available online:. Available online: www.nice.org.uk/guidance/ta663 (accessed on 15 May 2023).
- Zorginstituut Nederland. Available online: https://english.zorginstituutnederland.nl/publications/reports/2020/11/16/venetoclax-venclyxto (accessed on 15 May 2023).
- Do, N.; Thielen, F. Cost-Effectiveness of Venetoclax plus Obinutuzumab versus Chlorambucil plus Obinutuzumab for the First-Line Treatment of Adult Patients with Chronic Lymphocytic Leukemia – an Extended Societal View. Value in Health 2022. [CrossRef]
- Barnes, J. I.; Divi, V.; Begaye, A.; Wong, R.; Coutre, S.; Owens, D. K.; Goldhaber-Fiebert, J. D. Cost-Effectiveness of Ibrutinib as First-Line Therapy for Chronic Lymphocytic Leukemia in Older Adults without Deletion 17p. Blood Advances 2018, 2(15), 1946–1956. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R.; Redekop, W. K. Cost-Effectiveness of Ibrutinib Compared with Obinutuzumab with Chlorambucil in Untreated Chronic Lymphocytic Leukemia Patients with Comorbidities in the United Kingdom. Clinical Lymphoma Myeloma and Leukemia 2018, 18(2), e131–e142. [Google Scholar] [CrossRef] [PubMed]
- The National Institute for Health and Care Excellence. Acalabrutinib for treating chronic lymphocytic leukaemia. Available online: https://www.nice.org.uk/guidance/TA689/chapter/1-Recommendations (accessed on 15 May 2023).
- The National Institute for Health and Care Excellence. Ibrutinib with venetoclax for untreated chronic lymphocytic leukaemia. Available online: https://www.nice.org.uk/guidance/TA891/chapter/1-Recommendations (accessed on 15 May 2023).
Figure 1.
Therapy choice drivers in older patients with CLL.
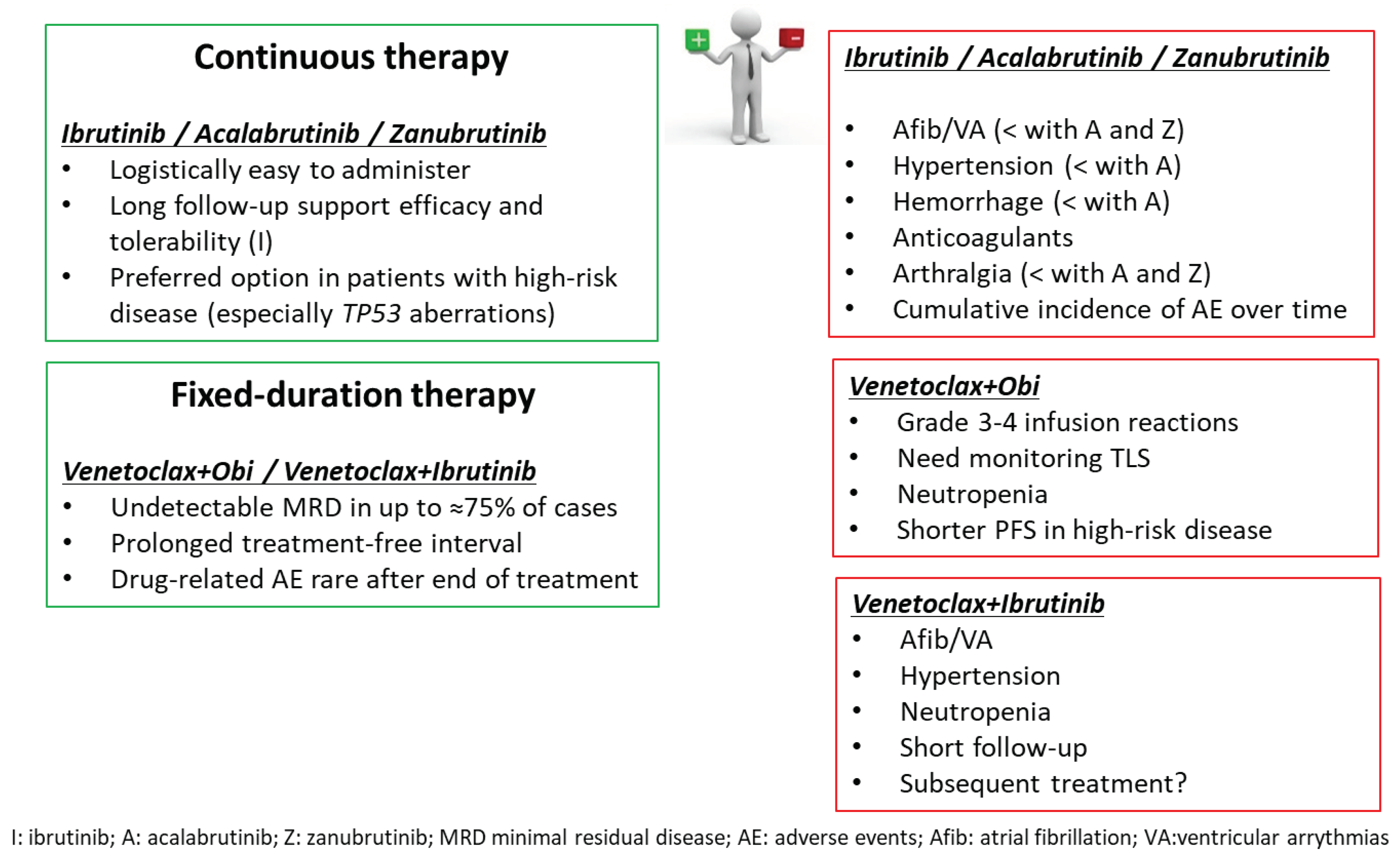
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



