
Submitted:
27 June 2023
Posted:
28 June 2023
You are already at the latest version
Abstract
Nurses and paramedics play a pivotal role when Mass Casualty Incidents (MCI) occur, yet they often feel unprepared for such events. Implementation strategies for training activities, including Virtual Reality (VR) and Augmented Reality (AR) simulations, offer realistic and immersive learning experiences, enhancing skills and competencies for nursing students. The aim of this work was to investigate the adopted tools in studies on VR&AR simulations for training nursing and paramedic students in managing MCI. A scoping review was performed following the PRISMA-ScR statement, and the search strategy was conducted through five electronic databases from December 2022 to March 2023. Of 162 records identified, 27 full-text were screened and, six studies were included in this review. These studies involved students who were assigned to different training methods, including immersive VR simulation, written instruction, and traditional lecture. VR&AR and immersive simulation generally show promising evidences in enhancing practical skills and knowledge in MCI management. VR&AR showed to be promising in disaster education and preparedness training, offering different levels of immersiveness and engagement, encouraging active and experential learning. Further research is needed to determine their long-term effectiveness. The choice of training method should consider program goals, target population, and available resources.
Keywords:
nursing students
; paramedic students
; training
; virtual reality
; augmented reality
; disaster medicine
; mass casualty incidents
; competence
; self-efficacy
; learning immersion
1. Introduction
In the last decades, disasters keep cyclically, putting human life and possessions at high risk [1]. Disasters can persist for hours or months and happen without much notice [1]. Pandemics, terrorist attacks and natural disasters like tsunamis, earthquakes, and storms are recent examples of multiple casualty incidents (MCI).
Nurses and paramedics play a vital role in disaster relief globally and much have been done since their profession's inception [1,2]. These events are very stressful for frontline healthcare workers due to their workload increase, multitasking and time pressures, as well as the need to deal with horrific situations and their own anxiety, uncertainty, and worries about how such calamities will affect their homes and families [3,4]. Thus, healthcare workers frequently experience extreme physical and psychological stress that exceeds what is typically supported by basic training and the system they work within [3].
Nevertheless, there is evidence that most nurses feel not adequately prepared for a disaster in their community [1]. Disaster preparedness is defined as the capacity to adequately plan and react to a major catastrophe that strikes abruptly, with the goal of acting promptly to reduce damage and get both personal and governmental countermeasures ready [5]. To obtain and maintain an adequate level of preparation, staff and nursing students should participate in the creation, evaluation, and simulation of disaster plans as training activities [1]. In addition, the training also shows benefits in willingness to participate in disaster response, defined as an individual’s voluntary inclination to participate in it [5,6]. In fact, even though nurses play a crucial role in disaster response, not all nurses are willing to take part in it, leading to a shortage of healthcare workers in disaster situations management. However, according to the Social Cognitive Theory, which includes factors such as behavioral patterns and the person’s cognitive, affective and physiological aspects, the willingness to participate can be improved with an adequate training [7,8,9].
For this reason, the recent literature stressed out the significance of disaster preparedness education and the necessity of disaster readiness at individual, family, and nursing curriculum levels for nursing students, together with the willingness to participate in disaster response [5]. In order to achieve this purpose, the best way to develop skills and competencies is through the design of educational training programs that could be ongoing, simple to access, interesting, and realistic, exposing the learner to high-fidelity simulations [1]. Also, education for disaster preparedness should include the use of technology, such as virtual reality (VR) and augmented reality (AR), for their great potential to train healthcare professionals and students, in particular on self-efficacy, clinical reasoning capacity, learning immersion and learning satisfaction [1,10,11].
Traditional knowledge transmission is replaced by experiential learning, where knowledge construction occurs through active experimentation involving the analysis of a problem from multiple perspectives. This process is achieved by engaging in observation and reflection on the lived experience [12].
Regarding learning immersion, there is evidence that the higher the level of immersion that can be reached, the greater the effects on self-efficacy [13]. Moreover, these types of simulations are considered a financially advantageous and resource-conscious pedagogical option for nursing education [14]. For these reasons, in the last years, different typologies of VR and AR simulations were tested, adopting various tools [15].
The use of VR and AR in disaster medicine training can provide several benefits. Firstly, it can create a safe and controlled environment for the students to learn and practice their skills without putting real patients at risk. Secondly, it can enable the students to experience a wide range of disaster scenarios that they may not encounter in their clinical placements [16]. This exposure can help them develop a broad range of skills and competencies to manage various disasters. Thirdly, it can enable the students to repeat scenarios until they have mastered the skills required to manage them effectively [16]. Additionally, it can enable students to experience a wide range of disaster scenarios, which can help them develop a broad range of skills and competencies [17].
Given the breadth of today's technological offerings, numerous types of devices have been applied in the field of training for health care personnel. However, to the best of our knowledge, an overview of the tools used in MCI training is lacking.
In order to systematically map the literature available on this topic, identifying the key concepts, theories, sources of evidence, and gaps in the research, the aim of this work was to identify and analyze studies reporting VR or AR simulations regarding training for MCI among nursing and paramedic students and to investigate the adopted tools.
2. Materials and Methods
The scoping review allows researchers to identify the types of available evidence in a given field, clarify key concepts and definitions in the literature, examine how research is conducted on a certain topic or field, and identify key characteristics or factors related to a concept [18]. Thus, we conducted a scoping review, according to the PRISMA extension for scoping reviews (PRISMA-ScR) [19], and following the methodology of Arksey & O’Malley [20], along with recommendations by Levac & colleagues [21]. The review involved five steps: (1) Formulating the research question, (2) Identifying pertinent studies, (3) Selecting relevant studies, (4) Extracting and organizing data, and (5) Reviewing and summarizing the findings.
Search strategy
The PCC method (P = Population, C = Concept, C = Context) was used to define the research question: P = Nursing or Paramedic students, C = Virtual Reality or Augmented Reality simulation, C = education and training about disaster medicine. The chosen population was extended to include paramedical staff because of the possible overlap of skills between them and nursing staff in different countries. Five databases (CINAHL-Cumulative Index to Nursing and Allied Health Literature, Cochrane Library, Pubmed, Embase, Ovid Medline) were searched for papers published with no time restrictions. The adopted search string was: ("Virtual Reality" OR "Virtual Reality Exposure Therap*” OR "Augmented Reality”) AND (“Mass Casualty Incident*” OR "Disaster Medicine”). The reference lists of all included studies were hand-searched for additional relevant reports or key terms. Targeted Internet searching using Google Scholar was also examined for additional studies of interest.
Eligibility criteria
In this scoping review, papers that met the inclusion criteria were primary quantitative design studies published in peer-reviewed journals in either English or Italian language. The studies focused on nursing or paramedic students, either individually or in combination, as long as their data could be extracted from the overall data. The papers also focused on the educational or training curricula. On the other hand, papers that were excluded from the review were those that focused on students other than nursing or paramedic education, abstract-only papers, case reports, opinion papers, and books/thesis.
Studies selection
Titles and abstracts of the retrieved records were screened for eligibility by two reviewers independently. Then full texts of the remaining articles were retrieved and assessed for inclusion, and included for data extraction if reached the consensus of the authors (CEM, YL).
Data extraction
Characteristics of each study were extracted and synthetized, including: authors, year, country, aim(s), study design, sample, MCI setting, interventions, outcome(s) and measurements. Any disagreement between the authors in the data extraction was resolved by a consensus discussion to make the final decision [22]. The majority of included studies was heterogeneous in samples and measurement tools. Therefore, a convergent and sequential synthesis design was adopted [23,24] and thematic analysis was utilized to manage the extracted data [25]. The authors engaged in an iterative process of independent and repeated readings of the included studies to familiarize themselves with the data and extract meaningful information. Through an inductive analysis, the authors independently and critically examined the data, comparing similarities and differences, then synthesizing the findings [24].
3. Results
The study selection process is presented in the PRSIMA-ScR flow-chart (Figure 1), following the PRISMA-ScR checklist [19] (Supplementary materials), showing the systematic and methodological steps of this scoping review. A total of 162 potentially relevant records were identified from five databases. After the removal of duplicates (59 out of 162), 103 records were screened for eligibility based on their titles and abstracts. Following this initial screening, 25 papers were selected for further evaluation and read in detail by the authors. In addition, the authors identified 12 papers through Google Scholar and the reference lists of the included studies, two of which were also read in detail. Ultimately, six papers met the inclusion criteria and were included in this scoping review.
Study characteristics
The characteristics of the included studies are presented in Table 1.
The six papers identified, published between 2016 and 2022, utilized quantitative study designs. Specifically, the designs included a quasi-experimental (Smith et al., 2016; Smith et al., 2018; Price et al., 2018; Mills et al., 2020) [26,27,28,31], and randomized controlled trial (Shujuan et al., 2022) [29]. Two studies were conducted in the United States (Smith et al., 2016; Smith et al., 2018) [27,28], one in Spain (Price et al., 2018) [26], one in Australia (Mills et al., 2020) [31], and two in China (Shujuan et al., 2022; Hu et al., 2022) [29,30].
Findings of the qualitative synthesis
The study by Price et al. [26] assessed the efficiency of the Simple Triage and Rapid Treatment (START) protocol during the implementation of a MCI simulation scenario, and compared two different types of triage methods: VR and Clinical Simulation (CS). The VR simulation was conducted using a VR device that included a Head Mounted Display to immerse participants in the VR content, while the CS simulation used actors. The study recruited 35 voluntary participants, who were health professionals and students attending the Official Emergency and Special Care Nursing Master’s Degree program at the Catholic University of Murcia. The simulation exercises involved the performance of basic triage on 20 victims using the START protocol, including life-saving maneuvers such as opening the airway and applying hemorrhage compression.
Smith et al. (2018) [27] conducted a quasi-experimental study to assess the effectiveness of two levels of immersive Virtual Reality Simulation (VRS) in providing disaster education. A total of 172 out of 197 senior baccalaureate degree nursing students completed the study. Participants were randomly assigned to one of the three groups: (i) immersive Head Mounted Display (HDM) VRS (n=59), (ii) keyboard and mouse VRS (n=58), or (iii) a control group consisting of written instruction (n=55). All three groups completed a 30-minute web module explaining decontamination skills prior to their respective intervention.
Smith et al. (2016) [28], conducted also another similar research exploring the effects of VRS on learning outcomes and retention. Indeed, 108 senior baccalaureate students were enrolled in the quasi-experimental study and randomly assigned to two groups: the treatment group, which received VRS (n=57), and the control group, which received written instruction (n=51). Both groups watched a 25-minute web module explaining decontamination skills prior to beginning the study.
Shujuan et al. [29] conducted a randomized, controlled, single-blinded trial to evaluate the use of virtual reality (VR) disaster preparedness scenarios for nursing students. The study included 101 second-year nursing students from a tertiary program in Sichuan who were randomly allocated to two groups: a VR group (n=49) and a control group (n=52). Both groups received the usual disaster nursing course, consisting of 24 lectures and 4 skills laboratory manikin simulation sessions, while the VR group also received VR training using head-mounted displays through 12 scenarios covering topics such as earthquake, fire, triage, wound dressing, fixation, hemostasis, debridement, cardiopulmonary resuscitation, tracheal intubation, transportation, decontamination, and supportive psychological care. Participants in the VR group could choose to complete the second or third model according to their mastery, as each scenario (10-25 minutes’ duration) was developed in three models: instructing model, training model, testing model.
Mills et al. [31] conducted a study comparing the efficacy of simulation training between VR and live-scenario triage. The trial enrolled 29 second-year students attending a Bachelor’s Paramedicine Science, who were randomized to either VR or live simulation. The scenarios simulated a car chase ending with the vehicle crashing into pedestrians and a perpetrator's shooting of one police officer, two pedestrians, and himself.
In the study by Hu et al. [30], the effectiveness of a VR Mobile Game-Based Application (VR-MGBA) was compared to a traditional lecture for teaching disaster evacuation management education. The study enrolled 158 nursing students, with 78 students assigned to the game group and 80 to the lecture group. Both groups underwent the same procedures except for the intervention, with the game group completing 1-hour of basic knowledge lecture, 4-hours of VR-MGBA use, and 1-hour of learning summary. While, the lecture group completed a 6-hour lecture class. The scenarios presented to both groups were related to fire, earthquake, and first aid during evacuation.
4. Discussion
The aim of this scoping review was to provide a comprehensive overview of the adopted tools for VR or AR simulations regarding training for MCI, among nursing and paramedics students.
In fact, numerous devices have been used in the training of health care personnel, given the advances in technological development in this field. However, this aspect can be dispersive for professionals wishing to adopt such training. This paper provides an overview of VR and AR tools adopted in literature.
VR and AR represent an emerging approach, which utilizes technology to enhance the training of nursing and paramedic students in many fields including MCI.
All the included studies in this review found that VR and AR had an overall positive impact and had the potential to address the need for competency development in disaster medicine education, as suggested by Shunjuan et al. (2022), and may be more effective than other training methods, as found by Hu et al. (2022). While some studies (Price et al., 2018; Smith et al., 2018; Smith et al., 2016; Mills et al., 2020) have not demonstrated the superiority of VR and AR over traditional methods in training nursing and paramedic students, VR and AR have been shown to be more efficient (Price et al., 2018), cost-effective (Smith et al., 2018; Smith et al., 2016; Shunjuan et al., 2022; Mills et al., 2020), easy to access (Smith et al., 2018; Smith et al., 2016), and safe (Smith et al., 2018; Smith et al., 2016) for disaster medicine training.
From what emerged, there are different VR and AR devices that provide different levels of immersion and consequently determine a different level of user involvement in the immersive experience.
Desktop Virtual Reality (DVRs) are devices such as video games or video simulations, in which the user interacts with a three-dimensional world generated on a computer screen [32]. In this case, the user is not totally immersed in the virtual world and the interaction takes place through mouse, keyboard or joystick.
Devices such as fulldome and Embodied Mixed Reality Learning Environments (EMRELE) are able to increase the level of immersion thanks to the intensification of sensory stimuli coming from the virtual world or the enhancement of the embodiment experience in virtual interaction. By ensuring complete perceptual immersion and greater emotional transport, the user is able to interact through their body with objects in the virtual environment.
Finally, Immersive Virtual Reality (IVR), such as Head-Mounted Displays (HMD) and Cave Automatic Virtual Environments (CAVE), which are able to generate environments that completely surround the user and are experienced as real. Unlike other devices, these systems have some features that can totally absorb the user in the virtual experience such as: first-person navigation, dynamism of the scene, stereoscopic vision.
Usually, DVRs are used in order to stimulate the interest and attention of students towards the subject studied; fulldomes and EMRELES are mainly used in collaborative learning contexts; IVRs are mainly used in the field of e-Health and education.
Thus, increasing the level of immersion increases the level of user engagement.
As reported above, higher level of immersion are associate with higher levels of self-efficacy [13].
This is an important aspect, as self-efficacy reinforcement was identified as the most crucial component of resistance against experiencing high amounts of stress [33].
Nevertheless, there is evidence that there is a sizable gap between nurses' opinions of their own level competencies and their actual level of competencies [34].
For this reason, VR and AR training has been showed an effective way to make aware of this discrepancy [35].
Despite the potential benefits of VR and AR in disaster medicine training, there are some challenges and limitations that need to be addressed. Firstly, there is a lack of standardization in VR technology, which can affect the quality and consistency of training across different institutions [17]. Another limitation is the cost of implementing VR or AR technology and the need for technical support and expertise to develop and maintain VR simulations. This can be a challenge for institutions that do not have the resources to support such technology [17]. However, as showed by our results, there are different types of adoptable tool, resulting in different price ranges.
Strengths and limitations
To the best of our knowledge, the strength of this study lies in being the first to provide an overview of the tools and settings of VR and AR for nursing training in MCI. This study has some limitations. First, this article does not perform a critical assessment of the literature included. However, as a scoping review, the aim of this study was not to synthetize evidence, but to pool together elements and core concepts from a various body of knowledge. The literature review was performed until February 2023, exposing this work to a publication bias. Finally, the included studies were highly inhomogeneous.
5. Conclusions
Up to date, it is still challenging to state which method of delivering disaster education or preparedness training and their effectiveness within specific contexts and populations is the most effective, as each study focuses on different strategies. However, VR and AR methods have shown to potentially improve initial skills development and engagement. Furthermore, they may be a more cost-effective and efficient ways to deliver training compared to traditional methods such as lectures or written instruction, and the choice of methods and tools will depend on the specific needs and goals of the training program, the target population, and the available resources. There is an increasing need to enhance the use of VR and AR in the educational path of nursing students. Further research are needed to determine the effectiveness of different VR methods or their long-term retention of knowledge and behavioral effects.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: PRISMA-ScR checklist.
Author Contributions
Conceptualization, C.E.M. and Y.L.; methodology, C.E.M., S.B., Y.L.; investigation, C.E.M., S.B., Y.L.; resources, C.E.M., S.B., L.R. and Y.L.; writing—original draft preparation, C.E.M., S.B. and Y.L.; writing—review and editing, P.I., K.EA., C.A., C.B. and L.R.; supervision, S.B., L.R. and Y.L.; project administration, C.E.M., S.B. and Y.L.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tussing, T.E.; Chesnick, H.; Jackson, A. Disaster Preparedness: Keeping Nursing Staff and Students at the Ready. Nurs Clin North Am. 2022, 57, 599–611. [Google Scholar] [CrossRef] [PubMed]
- Labrague, L.; Hammad, K.; Gloe, D.; McEnroe-Petitte, D.; Fronda, D.; Obeidat, A.; Leocadio, M.; Cayaban, A.; Mirafuentes, E. Disaster preparedness among nurses: a systematic review of literature. Int. Nurs. Rev. 2018, 65, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Palmer, J.; Ku, M.; Wang, H.; Crosse, K.; Bennett, A.; Lee, E.; Simmons, A.; Duffy, L.; Montanaro, J.; Bazaid, K. Public health emergency and psychological distress among healthcare workers: a scoping review. BMC Public Heal. 2022, 22, 1396. [Google Scholar] [CrossRef]
- Ali, H.M.; Ranse, J.; Roiko, A.; Desha, C. Healthcare Workers’ Resilience Toolkit for Disaster Management and Climate Change Adaptation. Int. J. Environ. Res. Public Heal. 2022, 19, 12440. [Google Scholar] [CrossRef]
- Kang, J.S.; Lee, H.; Seo, J.M. Relationship Between Nursing Students' Awareness of Disaster, Preparedness for Disaster, Willingness to Participate in Disaster Response, and Disaster Nursing Competency. Disaster Med Public Health Prep. 2022, 17, e220. [Google Scholar] [CrossRef]
- Connor, S.B. When and Why Health Care Personnel Respond to a Disaster: The State of the Science. Prehospital Disaster Med. 2014, 29, 270–274. [Google Scholar] [CrossRef]
- Bandura, A. Social Cognitive Theory: An Agentic Perspective. Annu. Rev. Psychol. 2001, 52, 1–26. [Google Scholar] [CrossRef]
- Espina, E.; Teng-Calleja, M. A social cognitive approach to disaster preparedness. 2015.
- Al-Hunaishi, W.; Hoe, V.C.; Chinna, K. Factors associated with healthcare workers willingness to participate in disasters: a cross-sectional study in Sana’a, Yemen. BMJ Open 2019, 9, e030547. [Google Scholar] [CrossRef]
- Gowing JR, Walker KN, Elmer SL, Cummings EA. Disaster Preparedness among Health Professionals and Support Staff: What is Effective? An Integrative Literature Review. Prehosp Disaster Med. 2017, 32, 321–328. [Google Scholar] [CrossRef]
- Lee, H.; Han, J.-W. Development and evaluation of a virtual reality mechanical ventilation education program for nursing students. BMC Med Educ. 2022, 22, 77. [Google Scholar] [CrossRef]
- Kolb, D.A. Experiential learning : experience as the source of learning and development: Englewood Cliffs, N.J. : Prentice-Hall, [1984] ©1984; 1984.
- Makransky, G.; Borre-Gude, S.; Mayer, R.E. Motivational and cognitive benefits of training in immersive virtual reality based on multiple assessments. J. Comput. Assist. Learn. 2019, 35, 691–707. [Google Scholar] [CrossRef]
- Bumbach, M.D.; Culross, B.A.; Datta, S.K. Assessing the Financial Sustainability of High-Fidelity and Virtual Reality Simulation for Nursing Education: A Retrospective Case Analysis. Comput Inform Nurs. 2022, 40, 615–623. [Google Scholar] [CrossRef]
- Sule Biyik, B.; Nurcan, C. The Use of Virtual Reality Simulations in Nursing Education, and Patient Safety. In: Stanislaw PS, Michael SF, editors. Contemporary Topics in Patient Safety. Rijeka: IntechOpen; 2020. p. Ch. 9.
- Duan, Y.-Y.; Zhang, J.-Y.; Xie, M.; Feng, X.-B.; Xu, S.; Ye, Z.-W. Application of Virtual Reality Technology in Disaster Medicine. Curr. Med Sci. 2019, 39, 690–694. [Google Scholar] [CrossRef]
- Baniasadi, T.; Ayyoubzadeh, S.M.; Mohammadzadeh, N. Challenges and Practical Considerations in Applying Virtual Reality in Medical Education and Treatment. Oman Med J. 2020, 35, e125. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O'Brien, K.K.; Colquhoun, H.; Levac, D.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Arksey, H.; O'Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O'Brien, K.K. Scoping studies: advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Peacock, R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: audit of primary sources. BMJ 2005, 331, 1064–1065. [Google Scholar] [CrossRef]
- Hong, Q.N.; Pluye, P.; Bujold, M.; Wassef, M. Convergent and sequential synthesis designs: implications for conducting and reporting systematic reviews of qualitative and quantitative evidence. Syst. Rev. 2017, 6, 61. [Google Scholar] [CrossRef]
- Pluye, P.; Hong, Q.N. Combining the Power of Stories and the Power of Numbers: Mixed Methods Research and Mixed Studies Reviews. Annu. Rev. Public Heal. 2014, 35, 29–45. [Google Scholar] [CrossRef]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef]
- Ferrandini Price, M.; Escribano Tortosa, D.; Nieto Fernandez-Pacheco, A.; Perez Alonso, N.; Cerón Madrigal, J.J.; Melendreras-Ruiz, R.; et al. Comparative study of a simulated incident with multiple victims and immersive virtual reality. Nurse Educ Today. 2018, 71, 48–53. [Google Scholar] [CrossRef]
- Smith, S.J.; Farra, S.L.; Ulrich, D.L.; Hodgson, E.; Nicely, S.; Mickle, A. Effectiveness of Two Varying Levels of Virtual Reality Simulation. Nurs. Educ. Perspect. 2018, 39, E10–E15. [Google Scholar] [CrossRef]
- Smith, S.J.; Farra, S.; Ulrich, D.L.; Hodgson, E.; Nicely, S.; Matcham, W. Learning and Retention Using Virtual Reality in a Decontamination Simulation. Nurs. Educ. Perspect. 2016, 37, 210–214. [Google Scholar] [CrossRef]
- Shujuan, L.; Mawpin, T.; Meichan, C.; Weijun, X.; Jing, W.; Biru, L. The Use of Virtual Reality to Improve Disaster Preparedness Among Nursing Students: A Randomized Study. J. Nurs. Educ. 2022, 61, 93–96. [Google Scholar] [CrossRef]
- Hu, H.; Lai, X.; Li, H.; Nyland, J. Teaching Disaster Evacuation Management Education to Nursing Students Using Virtual Reality Mobile Game-Based Learning. CIN: Comput. Informatics, Nurs. 2022, 40, 705–710. [Google Scholar] [CrossRef]
- Mills, B.; Dykstra, P.; Hansen, S.; Miles, A.; Rankin, T.; Hopper, L.; Brook, L.; Bartlett, D. Virtual Reality Triage Training Can Provide Comparable Simulation Efficacy for Paramedicine Students Compared to Live Simulation-Based Scenarios. Prehospital Emerg. Care 2020, 24, 525–536. [Google Scholar] [CrossRef]
- Makransky, G.; Petersen, G.B. Investigating the process of learning with desktop virtual reality: A structural equation modeling approach. Comput. Educ. 2019, 134, 15–30. [Google Scholar] [CrossRef]
- Meyer, N.; Niemand, T.; Davila, A.; Kraus, S. Biting the bullet: When self-efficacy mediates the stressful effects of COVID-19 beliefs. PLoS ONE 2022, 17, e0263022. [Google Scholar]
- Fenske, C.L.; Harris, M.A.; Aebersold, M.L.; Hartman, L.S. Perception Versus Reality: A Comparative Study of the Clinical Judgment Skills of Nurses During a Simulated Activity. J. Contin. Educ. Nurs. 2013, 44, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Akdere, M.; Acheson, K.; Jiang, Y. An examination of the effectiveness of virtual reality technology for intercultural competence development. Int. J. Intercult. Relations 2021, 82, 109–120. [Google Scholar] [CrossRef]
Figure 1.
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources.
Figure 1.
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources.
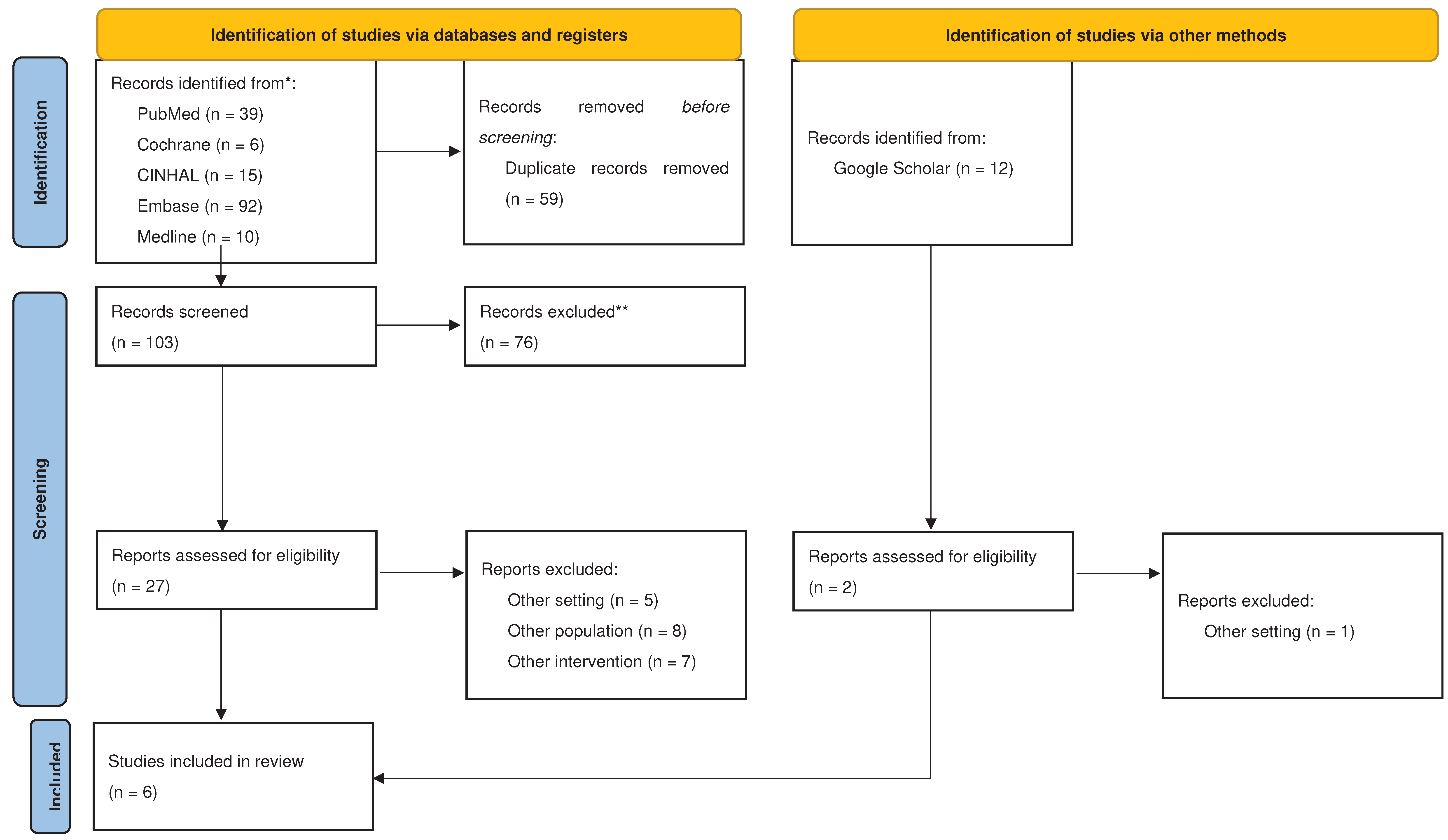

Table 1.
Included studies.
| AUTHORS and YEAR | COUNTRY | AIM(S) | STUDY DESIGN | SAMPLE | MCI SETTING | INTERVENTIONS | OUTCOME(S) | MEASUREMENTS |
|---|---|---|---|---|---|---|---|---|
| Price et al. (2018) [26] | Spain | To determine the efficiency in the execution of the START (Simple Triage and Rapid Treatment) triage, comparing VR to CS in a MCI. To compare the stress caused by the two different situations. | Quasi-experimental study | Sixtyseven students attending Official Emergency and Special Care Nursing Master’s Degree from the Catholic University of Murcia. | Performing basic triage in all the victims using the START system, including life-saving maneuvers: opening of an airway and hemorrhage compression. |
|
|
|
| Smith et al. (2018) [27] | United States | To assess two levels of immersive VR simulation to teach the skill of decontamination. | Quasi-experimental study | On a total of 197 senior baccalaureate nursing students from four Midwest campuses, 172 completed all three testing periods in the study. | Decontamination skills. |
|
|
|
| Smith et al. (2016) [28] | United States | To examine the longitudinal effects of VR simulation on learning outcomes and retention. | Quasi-experimental study | 108 students (57 were in the treatment group and 51 in the control group). | Decontamination skills. |
|
|
|
| Shujuan et al. (2022) [29] | China | To assess the impact of VR scenarios on disaster preparedness among nursing students. | A two-arm randomized controlled trial | 101 nursing students (49 in the VR group and 52 in the control group) attending the second year of a tertiary program in Sichuan, China. | Twelve highly interactive disaster scenarios:
|
|
|
|
| Hu et al. (2022) [30] | China | To explore the effectiveness of a virtual reality mobile game-based application for teaching disaster evacuation management education to nursing students. | Quasi experimental study | 158 nursing students (78 in the game group and 80 in the lecture group). | Three disaster situations: fire scenario, earthquake scenario, first aid scenario. |
|
|
|
| Mills et al. (2019) [31] | Australia | To compare the simulation efficacy of a bespoke virtual-reality MCI simulation with an equivalent live simulation scenario designed for undergraduate paramedicine students. | Quasi-experimental study | 29 students of Paramedical Science. | Car chase and shoot. |
|
|
|
Legend. CS: Clinical Simulation; DPQ: Disaster Preparedness Questionnaire; HMD: Head-Mounted Display; MCI: Mass Casualty Incident; MGBA: Mobile Game-Based Applications; NASA-TLX: National Aeronautics and Space Administration Task Load Index; SDS: Simulation Design Scale; VR: Virtual Reality.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



