
Submitted:
28 June 2023
Posted:
29 June 2023
You are already at the latest version
Abstract
The increased emergence of multidrug-resistant Helicobacter pylori influences the prevention of stomach cancer. Zingiber officinale is a plant usually used in folk medicine to treat a variety of diseases involving infections, nausea, vomiting, peptic ulcer, dyspepsia, and inflammation. This study was conducted to evaluate the ability of Z. officinale extract to combat resistant H. pylori. The disc diffusion, microdilution, and microplate assays were performed to evaluate the susceptibility to antibiotics, and the antibacterial and antibiofilm activities of the Z. officinale extracts. Using the checkerboard method, the combined effects of the gentamicin and Z. officinale extract were investigated. In addition, anti-inflammatory activity and GC-MS analysis were determined by the modified protocol. According to the findings, H. pylori isolates exhibited resistance rates of 56.33, 50.0, and 45.85 for metronidazole, gentamicin, and tetracycline, respectively. The methanolic extract of Z. officinale had the strongest effectiveness against resistant H. pylori isolates with MIC of 20.0 to 50.0 µg/ml against both H. pylori isolates and the stranded strain NCTC 11637. Z. officinale extract suppress the biofilm formed by H. pylori isolates with a percentage of 92.96% at 50.0µg/ml, compared with 97.19% for gentamicin at the same concentration. According to FICI values, combination of methanolic Z. officinale extract to gentamicin increases bacterial sensitivity to such drugs. Moreover, the Z. officinale extract exhibits strong anti-inflammatory activity. The GC-MS analysis of Z. officinale extract exhibits 17 different chemical compounds. Conclusions: The Z. officinale extract contain the anti-inflammatory compound gingerol as the main constituent which inhibits the growth of H. pylori and its biofilm, are a promising natural therapeutic alternative or enhance antibiotics activity
Keywords:
H. pylori
; antibiotics resistant
; Z. officinale antibacterial
; biofilm suppression
; anti-inflammatory
; GC-MS
1. Introduction
The gastrointestinal tract, particularly the stomach, is colonized by H. pylori [1]. H. pylori is one of the most common causes of human infection, especially in developing countries, where it affects more than 80% of the population. [2]. An infection with H. pylori typically persists for the rest of one's life. This bacterium has also been related to mucosa-associated lymphoid tissue (MALT) lymphoma, peptic ulcer, chronic gastritis, and gastric cancer. [3-6]. Despite the fact that the majority of H. pylori infections are asymptomatic, those who are infected are at a significant risk of developing the aforementioned illnesses. H. pylori was categorized as a human carcinogen category I by the World Health Organization International Agency for Research on Cancer in 1994. [7]. Flagella, biofilm, outer membrane proteins (OMPs) catalase, mucinase, lipase, urease, proteases, and phospholipase), vacuolating cytotoxin A (VacA), cytotoxin-associated gene antigen (CagA), and induced contact of the epithelium A (IceA), among others, are virulence factors that control the pathogenicity of H. pylori [1, 7]. Several studies have shown that H. pylori strains have the potential to form biofilms in human stomach mucosa both in vitro and in vivo. [8-12]. Amoxicillin, clarithromycin, or amoxicillin and metronidazole are the two antibiotics used in the H. pylori treatment regimen, together with a proton pump inhibitor. Due to the emergence of drug-resistant strains, standard treatment was unable to completely eradicate H. pylori [1, 12]. The formation of biofilms modifies the outer membrane proteins associated with antibiotic resistance, and elevating proteinase K levels alters clarithromycin resistance, according to findings by Hathroubi et al. [13]. Moreover, eDNA in biofilms stimulates microbial adhesion, prevents the diffusion of antibiotics, and chelates cations. [14]. Some extracellular enzymes in the biofilm deactivate antibiotics [15]. The rapid emergence of multi-drug H. pylori is a strong reason to search for a new approach to eradicating it [16]. In comparison to treatments derived from chemical sources, using plant extracts for the therapeutic treatment of multi-drug resistant H. pylori has benefits. This approach was preferred because, as compared to those developed from chemical sources, these therapeutics had less toxicological and pharmacological side effects. In an attempt to decrease the toxicity of synthetic drugs, researchers in a wide range of disciplines, including gastroenterology and bacteriology, have focused a great deal of emphasis on the pharmacological actions of natural products against H. pylori [17, 18]. So, several studies have examined plant compounds that have gastroprotective and anti-H. pylori activity. [1, 19, 20]. Zingiber officinale, which belongs to the Zingiberaceae family, has grown in popularity as a complementary medicine in many parts of the world. The methanol extracts of Zingiber officinale prevent the growth of 19 H. pylori strains in vitro with a MIC range of 6.25 to 50 µg/ml. Most H. pylori strains are inhibited by gingerols, an active fraction with a MIC range of 0.78 -12.5 µg/ml and significant activity against CagA positive bacteria [21]. Moreover, Ohno et al. (2003) shown that plant essential oils can inhibit H. pylori isolates from clinical samples and the ATCC strain [22]. An infection with H. pylori activates many pro-inflammatory signals. This reaction contributes to the pathophysiology of a number of gastrointestinal illnesses. To treat stomach disease caused by H. pylori infection, the inflammatory response must be under control. Strong anti-inflammatory properties and an ability to stop the release of cytokines that induce inflammation are included in the Zingiber officinale extract. [23]. The use of combination therapy has several benefits, including the ability to treat mixed infections and infections caused by a specific causal organism, as well as to enhance antimicrobial activity, reduce the need for continuous antibiotic administration, and stop the formation of bacteria that are resistant to several drugs [18]. The current work aimed to identify the main bioactive components of Zingiber officinale methanolic extracts and explore its antibacterial, antibiofilm, the ability to enhance antibiotics activity and anti-inflammatory actions against resistant H. pylori.
2. Materials and Methods
2.1. Zingiber officinale
Zingiber officinale rhizomes were obtained from the local market in Cairo, Egypt, in 2022. The rhizomes of Z. officinale were washed with distilled water, after drying at room temperature. After drying, the rhizomes of Z. officinale are cut into small parts and ground to powder using an electrical blender.
2.1.1. Extract of Z. officinale (ZO) preparation
Ten grams of powdered Z. officinale were mixed with 100 ml of methanol (Sigma-Aldrich, St. Louis, USA) to generate the methanol extract, which was then allowed to soak for 24 hours at room temperature. Throughout the time spent soaking, the extracts were filtered using Whatman No. 1 filter paper, and the filtrate was then evaporated at 50 °C under decreased pressure in a vacuum evaporator. The extracts were kept in opaque vials and frozen at -10 oC until further research.
2.2. Antibiotic susceptibility of H. pylori isolates
Seventy-six H. pylori isolates previously identified and the reference strain NCTC 11637 were grown at 37 oC in Mueller-Hinton broth (MH) medium (Oxoid, UK) supplemented with 5% horse blood until they reached the exponential phase. The turbidity of bacterial growth was measured using a spectrophotometer set at 620 nm and examined every 30 minutes to identify the exponential phase. The inoculum density in each bacterial solution was then adjusted to 0.5 McFarland Standard (1.5 X 106 CFU/ml) in sterile saline (0.84% NaCl). Antibiotic susceptibility testing of H. pylori isolates was performed using the disc diffusion technique, as described in the Clinical and Laboratory Standards Institute (CLSI 2020) guidelines (M7-A5) [24]. In brief, 50µl of the bacterial suspension at the above-mentioned turbidity concentration were inoculated onto (MH) agar medium enriched with 5% horse blood. Antibiotic discs representing different classes of antibiotics (antibiotics panel were ciprofloxacin 5μg/ml, levofloxacin 5μg/ml gentamicin 10μg/ml, neomycin 30μg/ml, clarithromycin 15μg/ml, erythromycin 15μg/ml, tetracycline 30μg/ml, amoxicillin 25μg/ml, metronidazole 5μg/ml and amoxicillin/clavulanic acid 20/10μg/ml), were gently loaded on the prepared plates using sterile forceps. Then, they were incubated for 24 h under microaerophilic conditions (10% CO2, 5% O2, and 85% N2) using a gas pack system (Mitsubishi, Japan) at 37°C. The diameter of the inhibition zone was measured in millimeters (mm), compared with the standard zone diameter given in the protocol chart. It can be determined whether the bacterial isolate is resistant, intermediate, or susceptible to the tested antibiotics.
2.3.1. Anti H. pylori activity of (ZO) extract
Zingiber officinale extract were investigated for antibacterial activity against resistant H. pylori isolates and H. pylori NCTC 11637. One hundred microliters of bacterial growth (1.5 x106 CFU/ml) were inoculated into Muller Hinton Blood Agar (MHBA) medium. Paper discs (8mm) were saturated with 50µl of crude extract containing 10 mg of (ZO) in DMSO per ml. The saturated paper discs were plated on the surface of the inoculated MHBA plate, and a control antibiotic, gentamicin paper discs containing 25 g/ml, was used on the same plates. The plates were incubated at 37 °C for 48 hours under microaerophilic conditions (10% CO2, 5% O2, and 85% N2) using a gas pack system (Mitsubishi, Japan), and the diameter of the inhibitory zone was estimated with (mm). This experiment was performed in three replicates [25].
2.3.2. Determination of minimum inhibitory concentrations (MICs) of (ZO) extract
The microbroth dilution technique was used to evaluate the MIC of the methanolic extract (ZO) against H. pylori isolates and standard strain NCTC 11637 using gentamicin (HiMedia Laboratories Pvt. Ltd., India) as an antibacterial control. In each well of a 96-well microplate, gentamicin and a methanolic extract of (ZO) were coated in twofold serial dilutions. A saline suspension of the test strain was added to each well, and the cultures were incubated at 35 °C for 3 days in a microaerophilic atmosphere (10% CO2, 5% O2, and 85% N2). Z. officinale extract was investigated at concentrations ranging from 0.0, 5.0, 10.0, 15.0, 20.0, 25.0, 30.0, 35.0, 40.0, 45.0, 50.0, 55.0, and 60.0 µg/ml, and gentamicin was started at 0.30, 0.613, 1.25, 2.5, 5.0, 10.0, 20.0, 40.0, and 80.0 g/ml. The experiment was performed according to the criteria of the CLSI 2020 guidelines (M7-A5) [24, 26]. Wells containing a negative control (medium + ZO) extract or gentamicin at the tested concentrations) were performed to determine the differences in optical density (OD) at 630 nm. MIC was defined as the lowest concentration of the Z. officinale extract or gentamycin that can inhibit the visible growth of bacteria.
2.3. Checkerboard assay
Checkerboard is a technique used to determine the synergistic effect between gentamicin and ZO extract. Using the broth microdilution method, two-dimensional checkerboard serial dilutions were carried out, with the concentration of gentamicin decreasing vertically and the concentration of the of (ZO) decreasing horizontally. The previously made stock solution was diluted with Mueller-Hinton broth. Gentamicin concentrations started at 1/ 128 MIC in the rows, and (ZO) concentrations started at 1/ 128 MIC in the columns. At a density of 106 (CFU)/ml/well, bacterial isolates were inoculated. and the plate was incubated for 24 hours at 37°C. A positive control well included only media with bacteria inoculated and no gentamicin /(ZO) combinations. The negative control wells contained only medium containing the used combinations with no bacteria inoculated. By comparing the growth of tested bacteria in the wells with the positive and negative controls, the MIC for the antibacterial agents was identified. Spectrophotometer was analyzed the optical density (OD) of the microplate at 620 nm. To determine the correlation between gentamicin and (ZO), fractional inhibitory concentration index (FICI) was determined with the formula [18].
where, FIC gentamicin = (MIC of gentamicin in the presence of ZO)/ (MIC of gentamicin alone) and FICZO = (MIC of ZO in the presence of gentamicin)/ (MIC of ZO alone).
FICI = FIC gentamycin + FICZO
Then, the interpretation ranges were applied to the FICI value. (Synergy ≤ 0.5, additive > 0.5 and ≤ 1.0, Indifference > 1 and ≤ 4.0, and Antagonism > 4.0)
2.4. Antibiofilm activity of methanolic extract Z. officinale
The ability of Z. officinale methanolic extracts to inhibit biofilm formation by H. pylori isolates at concentrations of 25 and 50µg/ml and using gentamicin as a control at the same concentrations were assessed using microtiter plate assays. In brief, 0.5 McFarland turbidity was adjusted from previous 24-hour cultures of each isolate to a 100-fold dilution using TBS (Liofilchem, Italy). Then, 100μl of this dilution was inoculated in triplicate on a 96-well flat-bottomed polystyrene plate (China) and incubated for 24 h at 37°C. Each well had its contents removed, and phosphate-buffered saline was used to repeatedly wash the wells (PBS). The plate was then air-dried after a 15-minute methanol fixing procedure. Each well was stained with 100μl of 1% crystal violet solution in water and incubated at room temperature for 30 min. Afterward, the stain was solubilized by 100μl of glacial acetic acid (GAA) (33%), plates were washed with distilled water three times, and then they were dried. The optical density (OD) of each well was read at 570 nm using an enzyme-linked immunosorbent assay (ELISA) reader. Based on the OD average values, the results of the biofilm formation were interpreted as follows; (OD≤ODC) = negative (non-biofilm formation), ODC optical density of control; (ODC≤ OD≤2ODC) = weak biofilm formation, (2ODC≤OD≤4ODC) = moderate biofilm formation; and (4ODC≤OD) = strong biofilm formation [27].
2.5. Anti-inflammatory assay by human RBCs
Using a human red blood cell (HRBC) technique, the anti-inflammatory activity of Z. officinale extract were examined. An equal volume of Alsever solution (consisting of 0.8% sodium citrate, 2% dextrose, 0.42% sodium chloride, and 0.5% citric acid) was added to the blood of a healthy human volunteer who had abstained from using non-steroidal anti-inflammatory drugs (NSAIDS) for the two weeks before the study began. The mixture was then centrifuged at 3,000 rpm. After being iso-saline washed from the precipitated cells, a 10% suspension was made. Deionized water was used to prepare different extract concentrations, including 4, 8, 16, and 32 µg/ml. To each concentration, 1 ml of phosphate buffer, 2 ml of hypo-saline, and 0.5 ml of HRBC solution were added. After a 30-minute incubation period at 37 °C, they conducted a 20-minute centrifugation at 3,000 rpm. Spectrophotometrically determine the supernatant's hemoglobin concentration at 560 nm [28]. The following equation was used to calculate the inhibition percentage.
2.6. Identification of chemicals that constitute Z. officinale extract by GC-MS
Gas chromatography-mass spectrometry (GC-MS) was used to evaluate, count, and identify the main active components in Z. officinale extract, with a few minor adjustments according to El-Sherbiny et al [29].
2.7. Statistical analysis
Using the statistical package-extended Minitab 18 software and Microsoft Excel 365, the data were computed as the mean ±SD value.
3. Results
3.1. Antibiotics profile of H. pylori isolates
Of the 76 previously identified H. pylori isolates and the reference strain, NCTC 11637 was investigated for antibiotic susceptibility using disc diffusion techniques. The findings demonstrate that H. pylori isolates are resistant to metronidazole, gentamicin, and tetracycline with 56.33%, 50.0%, and 45.85%, respectively. The antibiotics with the highest activity against those isolates were amoxicillin-clavulanate and ciprofloxacin, with ratio sensitivity of 73.36% and 58.95%, respectively. While the standard strain was shown to be susceptible to all antibiotics tested as shown in Table 1. H. pylori rapidly develops resistance to one treatment and requires combination therapy with different antibiotics. The combination therapy used in the treatment program should be chosen based on the country's predicted national drug resistance rates [1]. Globally, resistance to metronidazole and clarithromycin has grown over the past several years, lowering the efficacy of conventional first-line treatment regimens and raising the number of treatment failures brought on by drug-resistant H. pylori [30]. A significant number of isolates (73.9%) were previously demonstrated to be resistant to metronidazole, which was followed by amoxicillin (54.3%), clarithromycin (47.8%), ciprofloxacin (13.3%), and tetracycline (4.3%), according to Rasheed et al. [31]. Additionally, a study of antibiotic susceptibility by Tan and colleagues [32] in 2018 on 34 H. pylori strains revealed metronidazole resistance as the most frequent antibiotic resistance (79.4%), followed by clarithromycin (70.6%) and ciprofloxacin (42.9%). Among macrolides, including gentamicin, clarithromycin has been employed in front-line regimens for H. pylori eradication given its two pharmacokinetic features in the stomach, acid stability and amelioration absorption in the gastric mucus layer [33]. By reversibly binding to the peptidyl transferase loop of the 23S ribosomal RNA's domain V in the bacterial cell, macrolides inhibit protein synthesis and have antibacterial effects. Overall, point mutations in domain V of the 23S rRNA gene are the main cause of clarithromycin resistance in H. pylori, [34]. Tetracyclines have been used in a variety of regimens to eradicate H. pylori. The several Tet protein homologs mediate the molecular mechanisms causing H. pylori tetracycline resistance. Despite the fact that H. pylori encodes numerous assumed PBPs and -lactamase-like proteins, it causes amoxicillin resistance mainly by decreasing the binding affinity to a specific PBP without generating significant -lactamase activity [33]. Fluoroquinolones (moxifloxacin, levofloxacin, and ciprofloxacin) have been used as an alternative first- and second-line H. pylori eradication treatment. These antibiotics have a bactericidal effect by inhibiting two key bacterial type II topoisomerases, topoisomerase IV, and DNA gyrase, which modify the chromosomal supercoiling necessary for DNA synthesis, transcription, and cell division [35]. Bacterial resistance to fluoroquinolones is commonly caused by three distinct but non-exclusive mechanisms: target-mediated resistance caused by mutated topoisomerase IV or DNA gyrase, plasmid-mediated resistance caused by plasmids encoding DNA mimics that compete with natural drug targets; enzymes that lower antibiotic activity through acetylation and efflux systems; and chromosome-mediated resistance caused by altered antibiotic uptake and intrinsic efflux systems [33]. H. pylori, which is naturally absent of these genes, fluoroquinolone resistance is due to target-mediated mechanisms attributed to mutations in single or dual gyrA and gyrB genes encoding Gyr subunits A and B [36].
3.2. Antibacterial activity and minimum inhibitory concentration of Z. officinale extract
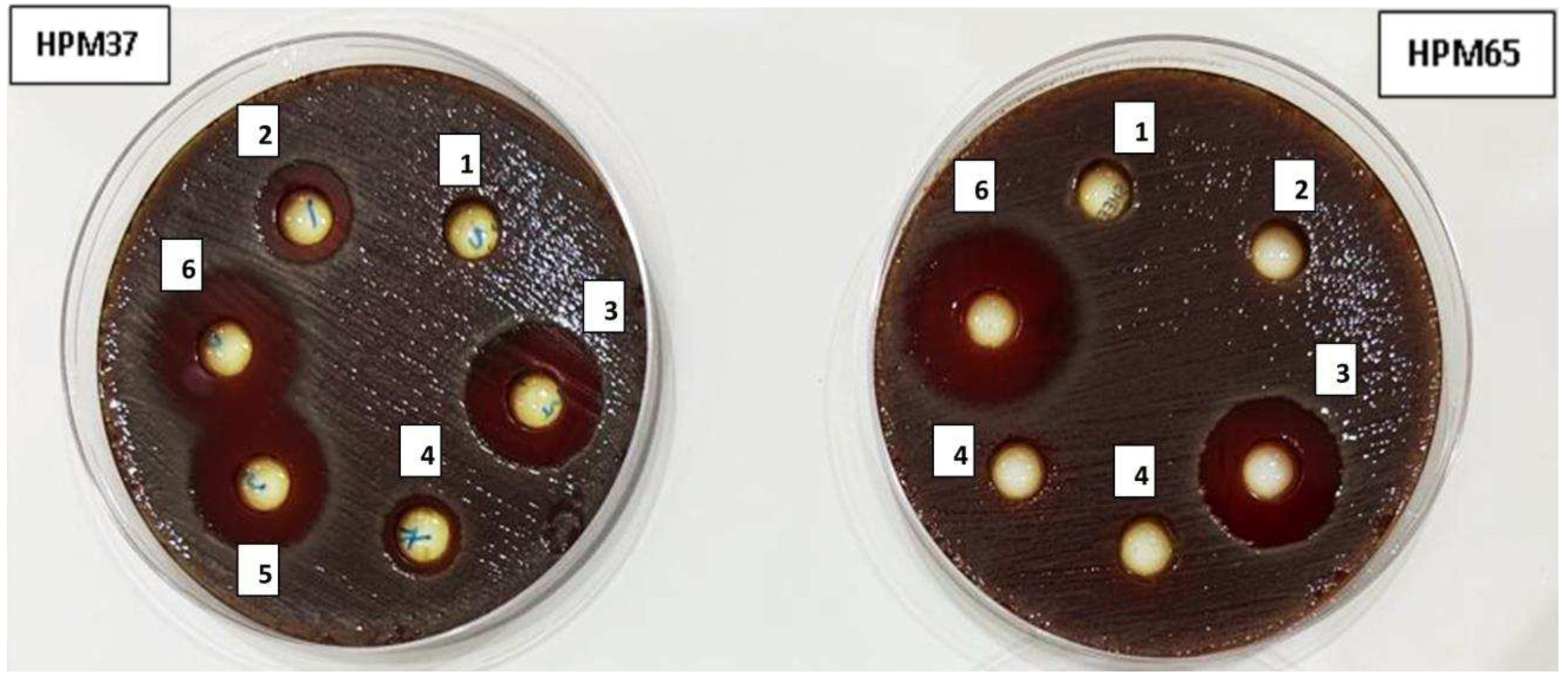
To assess the antibacterial activity of Z. officinale extract against H. pylori isolates and standard strain NCTC 11637 using a disc diffusion assay. The results showed that Z. officinale extract possesses potential antibacterial activity, with a mean ± SD imbibition zone ranging from 10±03 to 24±04 mm against both H. pylori isolates and standard strain NCTC 11637 are comparable with gentamicin 22±0.04 against standard strain NCTC 11637 as shown in Table 2. Several studies reported the antibacterial activity of Z. officinale extract against different bacterial strains isolated from clinical samples and standard strains [37-39]. Also, many studies [21, 40, 41] found Z. officinale extract to have antibacterial activity against H. pylori. In this study, the minimum inhibitory concentration of Z. officinale against resistant H. pylori isolates and the standard strain ranged from 20 to 48 µg/ml as shown in Table 3. These findings are consistent with those of Mahady et al. [21] found that a crude methanol extract of Z. officinale suppressed the growth of 14 clinical isolates of H. pylori, four CagA+ strains, and the ATCC-43504 strain, with a MIC of 50.0 µg/ml. Moreover, Azadi et al. [42] found that the ethanolic Z. officinale extract had a MIC of 58 µg/ml against the H. pylori CagA+ strain and that a combination of Z. officinale and cinnamon extract downregulated the CagA gene level by 1.94 times. According to Chakotiya et al. [38], Z. officinale extract changes the permeability and efflux activity of bacterial cells.
Figure 1.
Antibacterial activity of gentamycin (1), amoxicillin (2), ciprofloxacin (3), Dimethyl sulfoxide (DMSO) (4), amoxicillin-clavulanate r (5), Z. officinale extract (6) against resistant H. pylori isolates (HPM37 and HPM 65) and H. pylori NCTC 11637.
Figure 1.
Antibacterial activity of gentamycin (1), amoxicillin (2), ciprofloxacin (3), Dimethyl sulfoxide (DMSO) (4), amoxicillin-clavulanate r (5), Z. officinale extract (6) against resistant H. pylori isolates (HPM37 and HPM 65) and H. pylori NCTC 11637.
3.3. Synergistic effect of gentamicin combination with Z. officinale extract against resistant H. pylori isolate HPM72
In checkerboard technique, the interactions between gentamicin and ZO extract against resistant H. pylori isolate HPM72 exhibited thirty-eight treatments causing inhibition of resistant H. pylori isolate HPM72. A synergistic effect was considered when gentamicin and ZO extract combination showed FICI value ≤ 0.5, this case was observed with only eleven combinations at different ratios (0.25+0.25, 0.25+0.125, 0.25+0.062, 0.25+0.03, 0.125+0.25, 0.125+0.125, 0.125+0.062, 0.062+0.25, 0.031+0.2, 0.015+0.25 and 0.007+0.25 (µg/µg)/ml of gentamicin and ZO extract, respectively). Also, there were fourteen combinations with FICI ranged from 1.007 to 1.5 meaning additive effects. On the other hand, one combination showed an indifferent effect where the FICI 2 (µg/µg)/ml of gentamicin and ZO extract. Through these interactions, the MIC of gentamicin was reduced from 42 µg /ml to 0.125 µg (336-fold) while the MIC of ZO extract was reduced 33 µg /ml to 0.062µg (532-times). The FIC indexes for the tested combinations and their interpretations are presented in Table 4. Combination therapy has many advantages, including treating mixed infections, infections brought on by a particular causative organism, increasing antimicrobial activity, avoiding the need for prolonged antibiotic use, and preventing the emergence of multidrug-resistant bacteria. Combination therapy is the most frequently recommended empirical treatment for bacterial infections in intensive care units [18]. The MIC values against drug-resistant P. aeruginosa and clinical isolates of multidrug resistant Staphylococcus aureus were dramatically reduced when various antibiotics were combined with crude extracts of several plants [18,43]. Infections brought on by resistant bacterial stains can be treated more effectively when gentamicin and plant extract are combined, according to research done with Khameneh et al [44]. The efflux pumps appear to be inhibited by secondary plant compounds through competitive and non-competitive inhibition or by lowering the expression of the efflux genes. Due to the concentration and persistence of antibiotics in the bacteria, herbal extracts are therefore likely to prevent bacterial resistance to antibiotics. Moreover, Z. officinale extract possesses significant nephroprotective activity which is induced by gentamicin [45].
3.3. Antibiofilm activity of Z. officinale extract
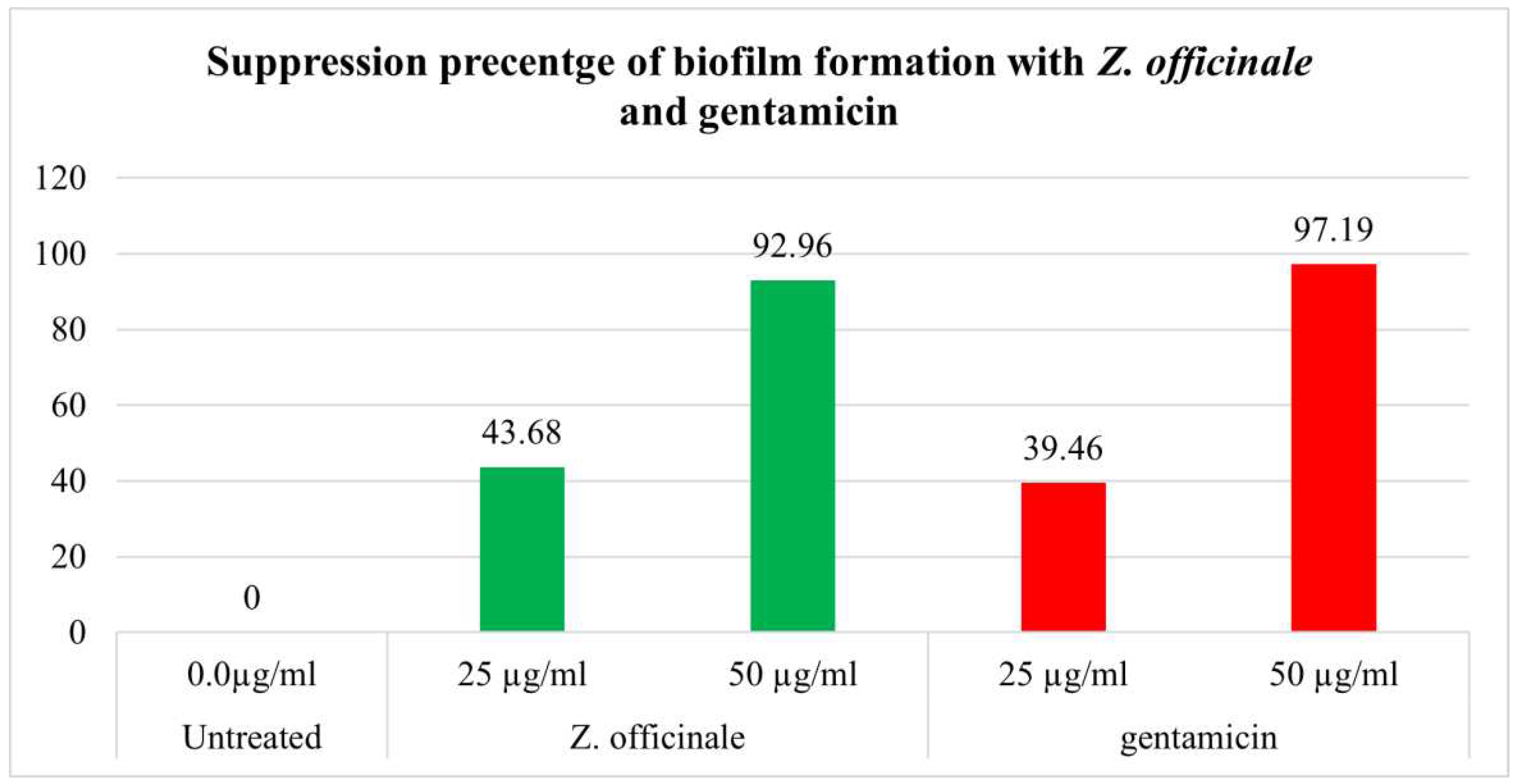
In this investigation, H. pylori isolates formed biofilm with different degrees (93.36%), with the moderate degree being the most common. The antibiofilm efficacy of methanolic extracts of Z. officinale in vitro suppressed biofilm formation to various degrees in bacterial isolates at concentrations of 25 and 50 µg/ml compared to gentamicin as the control at the same concentrations Table 5. As shown in the Figure 1, the highest reduction of biofilm formation by Z. officinale extract was seen at 50 µg/ml (92.96%). Antibiotic resistance is a result of the structural features of the biofilm and its bacterial constituents. A complex phenomenon, biofilm-related drug resistance may be greatly influenced by biofilms. Biofilms and related infections can be treated with antibiotics, sanitizers, and germicidal chemicals. When compared to their planktonic stage, bacteria that live in biofilms exhibit a 10-1000-fold increase in drug resistance, particularly antibiotic resistance [46]. According to studies by Hoyle et al., bacteria in dispersed biofilms are 15 times more sensitive to the antibiotic tobramycin than bacteria in intact biofilms [47]. Numerous studies have revealed the ability of Z. officinale extract to inhibit biofilm formation in various bacterial strain isolates from clinical samples. [48-50]. According to Kim et al. [50], Z. officinale extract reduces the synthesis of exopolysaccharide in bacterial stains that develop biofilm. H. pylori, which forms biofilms, may play an essential role in antibiotic resistance in clinical settings. Additionally, while the fecal-oral pathway is thought to be the primary mode of transmission for H. pylori, there is evidence that biofilm-forming strains growing on surface-exposed water may provide another route for infection transmission [51]. Moreover, H. pylori can transform into dormant cells known as coccoid forms, for which much higher MICs of different antibiotics are required to achieve bactericidal action [52]. Coccoid development may further exacerbate MDR due to an ultrastructural alteration in the cell membrane and metabolic pathways that reduce antibiotic target exposure and antibiotic penetration. [53].
Figure 2.
Percentage of biofilm suppression with Z. officinale and gentamicin.
3.4. Anti-inflammatory activity of Z. officinale extract
The anti-inflammatory activity of Z. officinale extract was demonstrated in vitro, with the inhibition percentage of red blood cell membrane stabilization increasing from 49.83% to 61.47% at a concentration of 4 to 32µg/ml, comparable to 63.72% to 71.43% as an inhibition percentage of the positive control (sodium diclofenac) at the same concentration, as shown in Table 6. Z. officinale has long been used as an anti-inflammatory, and some of its constituents have been shown to have anti-inflammatory properties. [54]. Because of the limiting of cyclooxygenase and cyclooxygenase, Z. officinale extract can decrease prostaglandin formation and have the same pharmacological action as non-steroidal anti-inflammatory medications (NSAIDs) [55]. Z. officinale also possesses anti-inflammatory properties that help to reduce gingival bleeding [49]. Moreover, Z. officinale extract decreased the production of IL-1b, IL-6, IL-8, and TNF-a from LPS-stimulated human PBMCs in the fight against H. pylori infection. [56].
3.5. Chemical Composition of Z. officinale extract
Table 7 and Figure 2 indicated that GC-MS screening of Z. officinale methanolic extraction identified approximately 17 distinct chemicals. gingerol (45.05%), zingiberene (16.05%), and thymol (10.50%) were the primary principal chemicals. Elbashir et al. [57] revealed that gingerol is the primary principal detected component (43%) in the ethanolic extraction of Z. officinale, followed by zingiberene (14%). Z. officinale from the eastern portion of Nigeria had gingerol at peak 12 and ricinoleic acid towards the end. [58]. GC-MS screening of methanol extract of Z. officinale from India, detected zingiberene, AR-curcumene, α-bergamotene, gingerol, zingerone, caryophyllene and ç-elemene [59]. Gingerols extracted from Z. officinale suppress the development of H. pylori Cag A+ strains [21]. Geraniol, another active component in Z. officinale, has numerous pharmacological properties, including antibacterial action against Helicobacter pylori, anti-inflammatory, and anti-ulcer properties [40]. Gingerol inhibits tumor promotion in mouse skin, inhibits neoplastic transformation and AP-1 stimulation in mouse epidermal JB6 cells treated with epidermal growth factor, inhibits human cancer cell proliferation by inducing apoptosis, and prevents pulmonary metastasis in mice implanted with B16F10 melanoma cells [21].
5. Conclusions
Based on our findings, Z. officinale exhibits potent antibacterial and antibiofilm properties against H. pylori resistance, as well as anti-inflammatory activity. As a result, we suggest utilizing Z. officinale extract to combat H. pylori infection by developing regimens for H. pylori eradication and inflammation.
Author Contributions
G.M.S. Conceptualization, writing-original draft preparation, investigation, supervision; M. K. M. B. Conceptualization and investigation; S.A.M Conceptualization. Writing review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
Not available.
Institutional Review Board Statement
In this section, you should add the Institutional Review Board Statement and approval number, if relevant to your study. You might choose to exclude this statement if the study did not require ethical approval. Please note that the Editorial Office might ask you for further information. Please add “The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of NAME OF INSTITUTE (protocol code XXX and date of approval).” for studies involving humans. OR “The animal study protocol was approved by the Institutional Review Board (or Ethics Committee) of NAME OF INSTITUTE (protocol code XXX and date of approval).” for studies involving animals. OR “Ethical review and approval were waived for this study due to REASON (please provide a detailed justification).” OR “Not applicable” for studies not involving humans or animals.
Informed Consent Statement
Not applicablee.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author has no conflicts of interest that are concerned with this article.
References
- El-Sherbiny GM, Mahmoud KM. A review – plant essential oils active against Helicobacter pylori. J. Essent. Oil Res. 34:3, 203-215, 2022. [CrossRef]
- Dunn BE, Cohen H, Blaser MJ. “Helicobacter pylori,” Clinical Microbiology Reviews, 10(4) 720–741, 1997.
- Blaser MJ, “Helicobacter pylori: its role in disease,” Clinical Infectious Diseases, vol. 15, no. 3, pp. 386–393, 1992. [CrossRef]
- Graham DY, “Campylobacter pylori and peptic ulcer disease,” Gastroenterology, vol. 96, no. 2, supplement 2, pp. 615–625, 1989. [CrossRef]
- Parsonnet J., Friedman G.D, Vandersteen DP, et al., “Helicobacter pylori infection and the risk of gastric carcinoma,” The New England Journal of Medicine, vol. 325, no. 16, pp. 1127–1131, 1991. [CrossRef]
- Wotherspoon C, Doglioni C, Diss TC. et al., “Regression of primary low-grade-B-cell gastric lymphoma of mucosa associated lymphoid tissue type after eradication of Helicobacter pylori,” The Lancet, vol. 342, no. 8871, pp. 575–577, 1993. [CrossRef]
- International Agency for Research on Cancer (IARC) 1994 and World Health Organization, “Schistosomes, liver flukes, and Helicobacter pylori,” in Monographs on the Evaluation of Carcinogenic Risks.
- Bonifácio B.V., Ramos A.S., Silva P.B., Taís M.B., Antimicrobial activity of natural products against Helicobacter pylori: a review. Annals of Clinical Microbiology and Antimicrobials, 13, 54 (2014). [CrossRef]
- Stark R. M., Gerwig G. J., Pitman R. S. et al., “Biofilm formation by Helicobacter pylori,” Letters in Applied Microbiology, vol. 28, no. 2, pp. 121–126, 1999. [CrossRef]
- Cole S. P., Harwood J., Lee R., She R., Guiney D. G., “Characterization of monospecies biofilm formation by Helicobacter pylori,” Journal of Bacteriology, vol. 186, no. 10, pp. 3124–3132, 2004. [CrossRef]
- Cellini L., Grande R., Campli E. et al., “Characterization of a Helicobacter pylori environmental strain,” Journal of Applied Microbiology, vol. 105, no. 3, pp. 761–769, 2008. [CrossRef]
- Hou. C., Yin F., Wang S., Zhao A., Li Y., Liu Y., Helicobacter pylori Biofilm-Related Drug Resistance and New Developments in Its Anti-Biofilm Agents Infection and Drug Resistance 2022:15 1561–1571. [CrossRef]
- Hathroubi S, Zerebinski J, Clarke A, Ottemann KM. Helicobacter pylori biofilm confers antibiotic tolerance in part via a protein-dependent mechanism. Antibiotics. 2020;9(6). [CrossRef]
- Okshevsky M, Meyer RL. The role of extracellular DNA in the establishment, maintenance and perpetuation of bacterial biofilms. Crit Rev Microbiol. 2015;41(3):341–352. [CrossRef]
- Ma JF, Hager PW, Howell ML, Phibbs PV, Hassett DJ. Cloning and characterization of the Pseudomonas aeruginosa zwf gene encoding glucose-6-phosphate dehydrogenase, an enzyme important in resistance to methyl viologen (paraquat). J Bacteriol. 1998;180(7):1741–1749. [CrossRef]
- Hsu, D.C. Wu, W.C. Chen, H.H. Tseng, H.C. Yu, H. M. Wang, S.S. Kao, K.H. Lai, A. Chen and F.W. Tsay, Randomized controlled trial comparing 7-day triple, 10-day sequential, and 7-day concomitant therapies for Helicobacter pylori infection. Antimicrobial Agents and Chemotherapy, 58(10), 5936–5942 (2014). [CrossRef]
- Bonifácio B.V., Dos Santos Ramos M.A., Da Silva P.B., et al., Antimicrobial activity of natural products against Helicobacter pylori: a review. Annals of Clinical Microbiology and Antimicrobials, 13(54), (2014). [CrossRef]
- Sharaf MH, El-Sherbiny GM, Moghannem SA, et al. New combination approaches to combat methicillin-resistant Staphylococcus aureus (MRSA). Sci Rep. 2021a;11(1):1–16. [CrossRef]
- Vale F.F. and Oleastro M., Overview of the phytomedicine approach against Helicobacter pylori. World Journal of Gastroenterology, 20(19), 5594–5609 (2014). [CrossRef]
- Wang Y.C., Medicinal plant activity on Helicobacter pylori-related diseases. World Journal of Gastroenterology, 20(30), 10368–10382 (2014). [CrossRef]
- Mahady G.B., PendlandS.L, YunG.S., Lu Z., Stoia A.Ginger (Zingiber officinale Roscoe) and the Gingerols Inhibit the Growth of Cag A+ Strains of Helicobacter pylori Anticancer Res. 2003 ; 23(0): 3699–3702.
- Ohno T., Kita M., Yamaoka Y., Imamura S., Yamamoto T., Mitsufuji S., Kodoma K., Kashima T., Imanishi, J. Antimicrobial activity of essential oils against Helicobacter pylori. Helicobacter, 8(3), 207–215 (2003). [CrossRef]
- Song MY, Lee DY, Park SY, Seo AA, Hwang JS., Heo SH, Kim EH Steamed Ginger Extract Exerts Anti-inflammatory Effects in Helicobacter pylori-infected Gastric Epithelial Cells through Inhibition of NF-κB. J Cancer Prev. 2021 30;26(4):289-297. [CrossRef]
- Clinical and Laboratory Standards Institute (CLSI) 2020 guidelines (M7-A5).
- Parekh, J., Chanda, S., 2007. Antibacterial and phytochemical studies on twelve species of Indian medicinal plants. Afr. J. Biomed. Res. 10: 175–181. [CrossRef]
- Foda A.M., Kalaba M.H., El-Sherbiny G.M., Moghannem S.A., El-Fakharany E.M. Antibacterial activity of essential oils for combating colistin-resistant bacteria Expert Rev. Anti-Infect. Ther., 20 (2022), pp. 1351-1364. [CrossRef]
- Kodori M., Nikmanesh B., Hakimi H., Ghalavand Z, Antibiotic Susceptibility and Biofilm Formation of Bacterial Isolates Derived from Pediatric Patients with Cystic Fibrosis from Tehran, Iran Archives of Razi Institute, Vol. 76, No. 2 (2021) 397-406. [CrossRef]
- Rahman H, Eswaraiah MC, Dutta A (2015) In-vitro anti-inflammatory and anti-arthritic activity of Oryza sativa Var. joha rice (an aromatic indigenous rice of Assam). Am Eurasian J Agric Environ Sci 15(1):115–121.
- El-Sherbiny GM, Gazelly AM, Sharaf MH. Moghannemm SA, Shehata M. .Ismail MKA, .El-Hawary AS, Exploitation of the antibacterial, antibiofilm and antioxidant activities of Salvadora persica (Miswak) extract Journal of Bioresources and Bioproducts 2022. [CrossRef]
- Thung I., Aramin H., Vavinskaya V., Gupta S., Park J. Y., Crowe S.E., Valasek M.A., Review article: the global emergence of Helicobacter pylori antibiotic resistance. Alimentary Pharmacology & Therapeutics, 43(4), 514–533 (2016).
- Rasheed F, Campbel BJ, Alfizah, H, Varro A, Zahra R, Yamaoka Y, Mark D, Pritchard Analysis of Clinical Isolates of Helicobacter pylori in Pakistan Reveals High Degrees of Pathogenicity and High Frequencies of Antibiotic Resistance. Helicobacter (2014) 19: 387–399. [CrossRef]
- Tan B., Yang JC, Young, C.L. et al. Helicobacter pylori Antimicrobial Susceptibility Testing-Guided Salvage Therapy in the USA: A Real Life Experience. Dig Dis Sci 63, 437–445 (2018). [CrossRef]
- Tshibangu-Kabamba, E., Yamaoka, Y. Helicobacter pylori infection and antibiotic resistance — from biology to clinical implications. Nat Rev Gastroenterol Hepatol 18, 613–629 (2021). [CrossRef]
- Gaynor M., Mankin, A. S. Macrolide antibiotics: binding site, mechanism of action, resistance. Curr. Top. Med. Chem. 3, 949–960 (2003). [CrossRef]
- Correia, S., Poeta, P., Hébraud, M., Capelo, J. L. & Igrejas, G. Mechanisms of quinolone action and resistance: where do we stand? J. Med. Microbiol. 66, 551–559 (2017). [CrossRef]
- Mori H., Suzuki H., Matsuzaki J., Masaoka T., Kanai T. Acquisition of double mutation in gyrA caused high resistance to sitafloxacin in Helicobacter pylori after unsuccessful eradication with sitafloxacin-containing regimens. United European Gastroenterol. J. 6, 391–397 (2018). [CrossRef]
- EL-Sherbiny GM. Antimicrobial Susceptibility of Bacteria Detected from the Root Canal Infection (Before and After) Root-Filled Teeth: An in Vitro Study International Journal of Dental Sciences and Research, 2015, Vol. 3, No. 1, 4-9.
- Chakotiya A S., Tanwar A., Narula A., Sharma RK, Zingiber officinale: Its antibacterial activity on Pseudomonas aeruginosa and mode of action evaluated by flow cytometry Microbial Pathogenesis 107, 2017, 254-260. [CrossRef]
- Jing Y, Cheng W, Ma Y, Zhang Y, Li M, Zheng Y, Zhang D and Wu L (2022) Structural Characterization, Antioxidant and Antibacterial Activities of a Novel Polysaccharide From Zingiber officinale and Its Application in Synthesis of Silver Nanoparticles. Front. Nutr. 9:917094. [CrossRef]
- Bhattamisra SK., Yean VL., Lee CK, Kuean CH, Candasamy M, Liew YK, Sahu PS Protective activity of geraniol against acetic acid and Helicobacter pylori- induced gastric ulcers in rats. Journal of Traditional and Complementary Medicine 9 (2019) 206e214. [CrossRef]
- Song MY, Lee DY, Park SY, Seo SA, Jeong-Seung Hwang JS, Heo AH, Kim EH, Steamed Ginger Extract Exerts Anti-inflammatory Effects in Helicobacter pylori-infected Gastric Epithelial Cells through Inhibition of NF-B. J Cancer Prev 26(4):289-297, 2021. [CrossRef]
- Azadi M, Ebrahimi A, Khaledi A, Esmaeili D, Study of inhibitory effects of the mixture of cinnamon and ginger extracts on cagA gene expression of Helicobacter pylori by Real-Time RT-PCR technique Gene Reports 17 (2019) 100493. [CrossRef]
- Fatemi, N., Sharifmoghadam, M.R., Bahreini, M. et al. Antibacterial and Synergistic Effects of Herbal Extracts in Combination with Amikacin and Imipenem Against Multidrug-Resistant Isolates of Acinetobacter. Curr Microbiol 77, 1959–1967 (2020). [CrossRef]
- Khameneh B, Iranshahy M, Ghandadi M, Ghoochi Atashbeyk D, Fazly Bazzaz BS, Iranshahi M (2015) Investigation of the antibacterial activity and efflux pump inhibitory effect of co-loaded piperine and gentamicin nanoliposomes in methicillin-resistant Staphylococcus aureus. Drug Dev Ind Pharm 41:989–994. [CrossRef]
- Lakshmi B.V. S; Sudhakar M. Protective Effect of Zingiber officinale on Gentamicin-Induced Nephrotoxicity in Rats International Journal of Pharmacology 2010; 6(1), 58-62.
- Sharma, S.; Mohler, J.; Mahajan, S.D.; Schwartz, S.A.; Bruggemann, L.; Aalinkeel, R. Microbial Biofilm: A Review on Formation, Infection, Antibiotic Resistance, Control Measures, and Innovative Treatment. Microorganisms 2023, 11, 1614. [CrossRef]
- Hoyle, B.D.; Wong, C.K.; Costerton, J.W. Disparate efficacy of tobramycin on Ca(2+)-, Mg(2+)-, and HEPES-treated Pseudomonas aeruginosa biofilms. Can. J. Microbiol. 1992, 38, 1214–1218. [. [CrossRef]
- Aghazadeh M, Bialvaei AZ, Aghazadeh M, Kabiri F, Saliani N, Mehdi Yousefi M, et al. Survey of the Antibiofilm and Antimicrobial Effects of Zingiber officinale (in Vitro Study) Jundishapur J Microbiol. 2016 February; 9(2): e30167.
- Faria TRB, Furletti-Goes VF, Franzini CM, et al Anti-inflammatory and antimicrobial effects of Zingiber officinale mouthwash on patients with fixed orthodontic appliances American Journal of Orthodontics and Dentofacial Orthopedics 159(1), 2021, 21-29. [CrossRef]
- Kim H-S, Park H-D (2013) Ginger Extract Inhibits Biofilm Formation by Pseudomonas aeruginosa PA14. PLoS ONE 8(9): e76106. [CrossRef]
- Mackay W., Gribbon L., Barer M. Reid D. Biofilms in drinking water systems: a possible reservoir for Helicobacter pylori. J. Appl. Microbiol. 85, 52S–59S (1998). [CrossRef]
- Sarem M., Corti, R. Role of Helicobacter pylori coccoid forms in infection and recrudescence. Gastroenterol. Hepatol. 39, 28–35 (2016). [CrossRef]
- Kadkhodaei, S., Siavoshi, F. & Akbari Noghabi, K. Mucoid and coccoid Helicobacter pylori with fast growth and antibiotic resistance. Helicobacter 25, e12678 (2020). [CrossRef]
- Ali BH, Blunden G, Tanira MO and Nemmar A: Some phytochemical, pharmacological and toxicological properties of ginger (Zingiber officinale roscoe): a review of recent research. Food and Chemical Toxicology 2008; 46(2): 409-20. [CrossRef]
- Charlier C., Michaux C, Dual inhibition of cyclooxygenase-2 (COX-2) and 5-lipoxygenase (5-LOX) as a new strategy to provide safer non-steroidal anti-inflammatory drugs. European Journal of Medicinal Chemistry 2003; 38(7): 645-59. [CrossRef]
- Grzanna R, Lindmark L and Frondoza CG: Ginger--an herbal medicinal product with broad anti-inflammatory actions. J Med Food 2005; 8(2): 125-32. [CrossRef]
- Elbashir DMM, Kehail MAA, Mohamed AIA, Ali AEH, Phytochemistry and GC-MS Screening and Biocidal Potentiality of Ginger (Zingiber officinale) Rhizome against Mosquito’s Larvae International Journal of Science and Research Archive, 2021, 03(02), 090–096. [CrossRef]
- Chinonye II, Oze RN, Lynda OU, Nkwoada A, Adanma AU. Phytochemical and GC/MS Analysis of the Rhizome of Zingiber officinale Plant Grown in Eastern Part of Nigeria. African Journal of Biology and Medical Research. 2018; 1(1): 43-54.
- Choudhari SS, Kareppa BM. Identification of Bioactive Compounds of Z. Officinale Roscoe Rhizomes through Gas Chromatography and Mass Spectrometry. Intern. J. Pharmac. Res. and Development. 2013; 5(8): 16 – 20.
Figure 2.
GC-MS analysis of Z. officinale methanolic extraction.
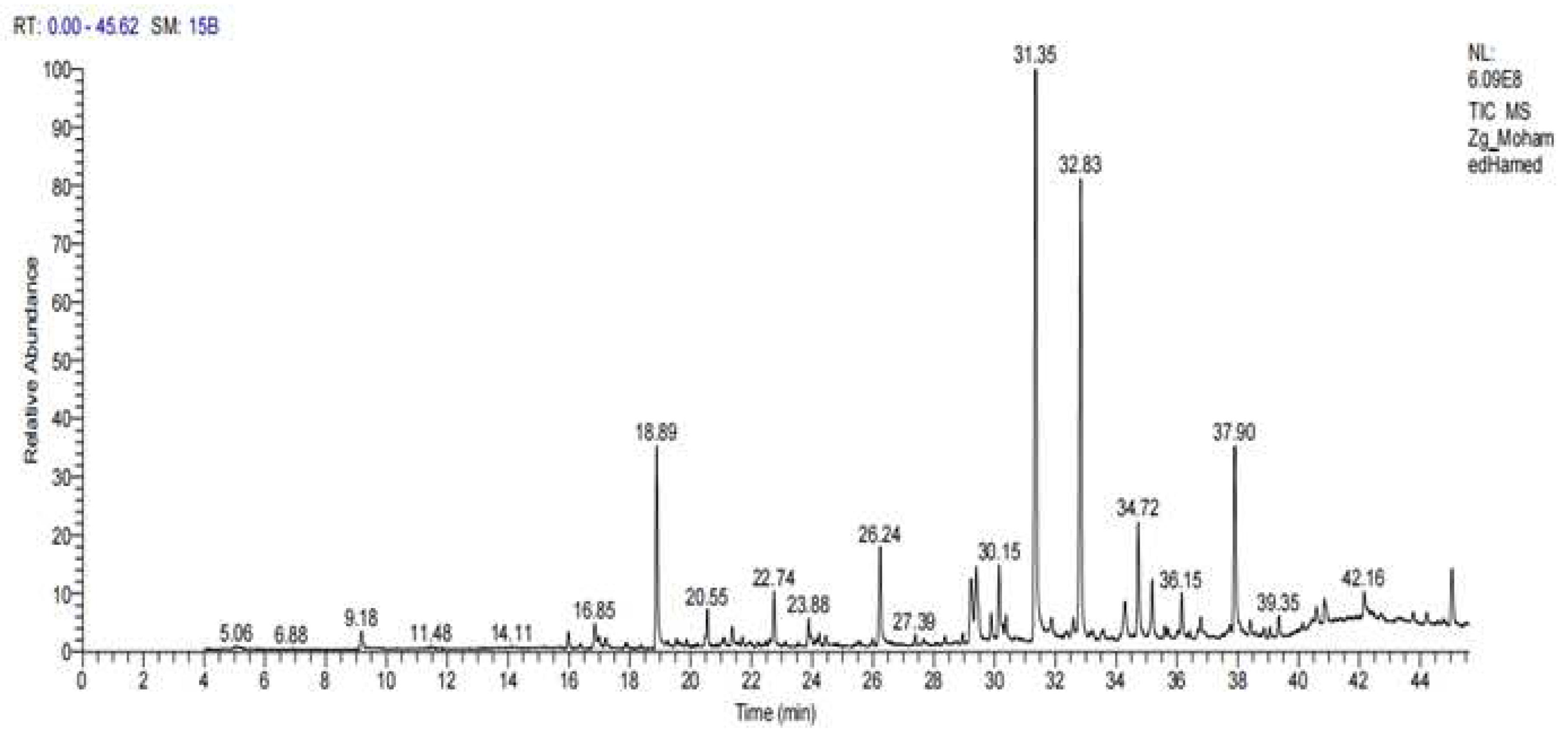

Table 1.
Antibiotics susceptibility among 76 H. pylori isolates.
| Class of antibiotics and mode of action | Antibiotic |
Potency (µg/disk) |
Antibiotics Susceptibility | Ref. normal value zone diameter breakpoints |
Ref. normal value H. pylori NCTC 11637 |
||||
| S. N (%) | I. N (%) | R. N (%) | S | I | R | ||||
| Inhibition of bacterial nucleic acid synthesis | |||||||||
| Fluoroquinolone | Ciprofloxacin | 5 | 45 (58.95) | 0(0.0) | 31 (40.61) | ≥ 21 | 16-20 | ≤ 15 | 22.40 |
| Quinolone | Levofloxacin | 5 | 39(51.09) | 9(11.79) | 28 (36.68) | ≥ 17 | 13–16 | ˂12 | 20.0 |
| Inhibition of bacterial protein synthesis | |||||||||
| Aminoglycosides | Gentamicin | 10 | 22 (28.82) | 16(20.96) | 38 (50.0) | ≥ 15 | 13-14 | ≤ 12 | 19.70 |
| Neomycin | 30 | 16(20.96) | 27(35.37) | 33 (43.23) | 21.0 | ||||
| Macrolides | Erythromycin | 15 | 30(39.30) | 12(15.72) | 34 (44.54) | ≥ 23 | 14-22 | ≤ 13 | 20.50 |
| Clarithromycin | 15 | 37 (48.47) | 9(11.79) | 30(39.30) | ≥21 | 15-20 | ≤14 | 21-70 | |
| Tetracyclines | Tetracycline | 30 | 19(24.89) | 22 (28.82) | 35 (45.85) | ≥ 19 | 15-18 | ≤ 14 | 23-80 |
| Inhibitors of bacterial cell wall synthesis | |||||||||
| Amoxicillin | 25 | 43 (56.33) | 8(10.48) | 25 (32.75) | ≥ 13 | 11-12 | ≤ 10 | 24.30 | |
| Penicillin combination | Amoxicillin-clavulanate | 20/10 | 56 (73.36) | 2(2.62.) | 18 (23.58) | ˃19 | - | ˂20 | 26.30 |
| Metabolic antagonism | |||||||||
| Nitroimidazoles | Metronidazole | 5 | 15(19.65) | 18 (23.58) | 43 (56.33) | ˃21 | 16-21 | ˂16 | 18.70 |
S = Sensitive, I = Intermediate, R = Resistance.
Table 2.
Antibacterial activity of methanolic Z. officinale extract against twenty-fiver MDR H. pylori isolates and NCTC 11637.
Table 2.
Antibacterial activity of methanolic Z. officinale extract against twenty-fiver MDR H. pylori isolates and NCTC 11637.
| No | Strains code | Mean of inhibition zone diameter (mm ± SD) | No | Strains code | Mean of inhibition zone diameter (mm ± SD) | ||
|---|---|---|---|---|---|---|---|
| Z. officinale extract | Gentamicin | Z. officinale extract | Gentamicin | ||||
| 1 | HPM4 | 14±00 | 0.0 | 14 | HPM48 | 12±05 | 0.0 |
| 2 | HPM7 | 13±09 | 0.0 | 15 | HPM51 | 15±20 | 0.0 |
| 3 | HPM9 | 12±05 | 0.0 | 16 | HPM54 | 24±04 | 0.0 |
| 4 | HPM12 | 11±05 | 0.0 | 17 | HPM57 | 14±06 | 0.0 |
| 5 | HPM15 | 15±09 | 0.0 | 18 | HPM62 | 12±04 | 0.0 |
| 6 | HPM16 | 13±03 | 0.0 | 19 | HPM63 | 13±06 | 0.0 |
| 7 | HPM19 | 15±00 | 0.0 | 20 | HPM65 | 16±00 | 0.0 |
| 8 | HPM26 | 12±04 | 0.0 | 21 | HPM66 | 11±04 | 0.0 |
| 9 | HPM37 | 16±00 | 0.0 | 22 | HPM70 | 10±03 | 0.0 |
| 10 | HPM44 | 11±06 | 0.0 | 23 | HPM72 | 12±07 | 0.0 |
| 11 | HPM48 | 15±08 | 0.0 | 24 | HPM73 | 14±08 | 0.0 |
| 12 | HPM52 | 12±00 | 0.0 | 25 | HPM75 | 15±08 | 0.0 |
| 13 | HPM56 | 14±06 | 0.0 | 26 | H. pylori NCTC 11637 | 17±06 | 20±04 |
Table 3.
MIC of Zingiber officinale extracted against resistant H. pylori species.
| No | Strains code | Minimum inhibitory concentration (μg/ml) | No | Strains code | Minimum inhibitory concentration (μg/ml) |
|---|---|---|---|---|---|
| Z. officinale extract | Z. officinale extract | ||||
| 1 | HPM4 | 25.0 | 14 | HPM48 | 39.0 |
| 2 | HPM7 | 27.0 | 15 | HPM51 | 28.0 |
| 3 | HPM9 | 22.0 | 16 | HPM54 | 23.0 |
| 4 | HPM12 | 25.0 | 17 | HPM57 | 29.0 |
| 5 | HPM15 | 29.0 | 18 | HPM62 | 38.0 |
| 6 | HPM16 | 32.0 | 19 | HPM63 | 50.0 |
| 7 | HPM19 | 22.0 | 20 | HPM65 | 27.0 |
| 8 | HPM26 | 23.0 | 21 | HPM66 | 33.0 |
| 9 | HPM37 | 33.0 | 22 | HPM70 | 46.0 |
| 10 | HPM44 | 26.0 | 23 | HPM72 | 42.0 |
| 11 | HPM48 | 35.0 | 24 | HPM73 | 35.0 |
| 12 | HPM52 | 37.0 | 25 | HPM75 | 48.0 |
| 13 | HPM56 | 44.0 | 26 | H. pylori NCTC 11637 | 20.0 |
Table 4.
Synergistic effect of gentamicin and ZO extract against resistant H. pylori HPM72.
| No | MIC Gentamicin + MIC ZO extract |
Gentamicin + ZO extract (µg/ml) | FICI Gentamicin + FICI ZO extract | FICI | interpretation | MIC Gentamicin + MIC ZO extract |
|---|---|---|---|---|---|---|
| 1 | MIC+MIC | 42+33 | 1+1 | 2 | Indifference | MIC+MIC |
| 2 | MIC+1/2MIC | 42+16.5 | 1+0.5 | 1.5 | additive | MIC+1/2MIC |
| 3 | MIC+1/4MIC | 42+8,25 | 1+0.25 | 1.25 | additive | MIC+1/4MIC |
| 4 | MIC+1/8MIC | 42+4.13 | 1+0.125 | 1.125 | additive | MIC+1/8MIC |
| 5 | MIC+1/16MIC | 42+2.06 | 1+0.062 | 1.062 | additive | MIC+1/16MIC |
| 6 | MIC+1/32MIC | 42+1.03 | 1+0.031 | 1.031 | additive | MIC+1/32MIC |
| 7 | MIC+1/64MIC | 42+0,51 | 1+0.015 | 1.015 | additive | MIC+1/64MIC |
| 8 | MIC+1/128MIC | 42+0.25 | 1+0.007 | 1.007 | additive | MIC+1/128MIC |
| 9 | 1/2MIC+MIC | 21+33 | 0.5+1 | 1.5 | additive | 1/2MIC+MIC |
| 10 | 1/2MIC+1/2MIC | 21+16,5 | 0.5+0.5 | 1 | partial synergy | 1/2MIC+1/2MIC |
| 11 | 1/2MIC+1/4MIC | 21+8,25 | 0.5+0.25 | 0.75 | partial synergy | 1/2MIC+1/4MIC |
| 12 | 1/2MIC+1/8MIC | 21+4.13 | 0.5+0.125 | 0.625 | partial synergy | 1/2MIC+1/8MIC |
| 13 | 1/2MIC+1/16MIC | 21+2.06 | 0.5+0.062 | 0.562 | partial synergy | 1/2MIC+1/16MIC |
| 14 | 1/2MIC+1/32MIC | 21+1.03 | 0.5+0.031 | 0.531 | partial synergy | 1/2MIC+1/32MIC |
| 15 | 1/2MIC+1/64MIC | 21+0,51 | 0.5+0.015 | 0.515 | partial synergy | 1/2MIC+1/64MIC |
| 16 | 1/4MIC+MIC | 10.5+33 | 0.25+1 | 1.25 | additive | 1/4MIC+MIC |
| 17 | 1/4MIC+1/2MIC | 10.5+16.5 | 0.25+0.5 | 0.75 | partial synergy | 1/4MIC+1/2MIC |
| 18 | 1/4MIC+1/4MIC | 10.5+8.25 | 0.25+0.25 | 0.5 | synergy | 1/4MIC+1/4MIC |
| 19 | 1/4MIC+1/8MIC | 10.5+4.13 | 0.25+0.125 | 0.375 | synergy | 1/4MIC+1/8MIC |
| 20 | 1/4MIC+1/16MIC | 10.5+2.06 | 0.25+0.062 | 0.312 | synergy | 1/4MIC+1/16MIC |
| 21 | 1/4MIC+1/32MIC | 10.5+1.03 | 0.25+0.031 | 0.281 | synergy | 1/4MIC+1/32MIC |
| 22 | 1/8MIC+MIC | 5.25+33 | 0.125+1 | 1.125 | additive | 1/8MIC+MIC |
| 23 | 1/8MIC+1/2MIC | 5.25+16.5 | 0.125+0.5 | 0.625 | partial synergy | 1/8MIC+1/2MIC |
| 24 | 1/8MIC+1/4MIC | 5.25+8.25 | 0.125+0.25 | 0.375 | synergy | 1/8MIC+1/4MIC |
| 25 | 1/8MIC+1/8MIC | 5.25+4.14 | 0.125+0.125 | 0.25 | synergy | 1/8MIC+1/8MIC |
| 26 | 1/8MIC+1/16MIC | 5.25+2.06 | 0.125+0.062 | 0.187 | synergy | 1/8MIC+1/16MIC |
| 27 | 1/16MIC+MIC | 2.62+33 | 0.062+1 | 1.062 | additive | 1/16MIC+MIC |
| 28 | 1/16MIC+1/2MIC | 2.62+16.5 | 0.062+0.5 | 0.562 | partial synergy | 1/16MIC+1/2MIC |
| 29 | 1/16MIC+1/4MIC | 2.62+8.25 | 0.062+0.25 | 0.312 | synergy | 1/16MIC+1/4MIC |
| 30 | 1/32MIC+MIC | 1.31+33 | 0.031+1 | 1.031 | additive | 1/32MIC+MIC |
| 31 | 1/32MIC+1/2MIC | 1.31+16.5 | 0.031+0.5 | 0.531 | partial synergy | 1/32MIC+1/2MIC |
| 32 | 1/32MIC+1/4MIC | 1.31+8.25 | 0.031+0.25 | 0.281 | synergy | 1/32MIC+1/4MIC |
| 33 | 1/64MIC+MIC | 0.65+33 | 0.015+1 | 1.015 | additive | 1/64MIC+MIC |
| 34 | 1/64MIC+1/2MIC | 0.65+16.5 | 0.015+0.5 | 0.515 | partial synergy | 1/64MIC+1/2MIC |
| 35 | 1/64MIC+1/4MIC | 0.65+8.25 | 0.015+0.25 | 0.265 | synergy | 1/64MIC+1/4MIC |
| 36 | 1/128MIC+MIC | 0.22+33 | 0.007+1 | 1.007 | additive | 1/128MIC+MIC |
| 37 | 1/128MIC+1/2MIC | 0.32+16.5 | 0.007+0.5 | 0.507 | partial synergy | 1/128MIC+1/2MIC |
| 38 | 1/128MIC+1/4MIC | 0.32+8.25 | 0.007+0.25 | 0.257 | synergy | 1/128MIC+1/4MIC |
Table 5.
Detection of biofilm 76 H. pylori isolates before and after treatment with Z. officinale and gentamicin.
Table 5.
Detection of biofilm 76 H. pylori isolates before and after treatment with Z. officinale and gentamicin.
| Treatment | Number of bacterial isolates biofilm formation (%) | Degree (%) | |||
|---|---|---|---|---|---|
| Weak (%) | Moderate (%) | Strong (%) | |||
| Untreated | 0.0 µg/ml | 71(93.36) | 23.93 | 60.54 | 15.48 |
| Z. officinale | 25 µg/ml | 40(52.6) | 30.0 | 45.0 | 25.0 |
| 50 µg/ml | 5(6.31) | 0.0 | 40.0 | 60.0 | |
| Gentamicin | 25 µg/ml | 43(56.54) | 25.57 | 44.17 | 30.22 |
| 50 µg/ml | 2(2.63) | 0.0 | 100 | 0.0 | |
Table 6.
Assessment of anti-inflammatory activity of Z. officinale extract.
| Treatment | Concentration (μg/ml) | Absorbance 560 nm | Percentage inhibition |
|---|---|---|---|
| Control | 0.0 | 1.246 | 0.0 |
| Z. officinale | 4 | 0.625 | 49.83% |
| 8 | 0.536 | 56.68% | |
| 16 | 0.501 | 59.79% | |
| 32 | 0.480 | 61.47% | |
| Sodium diclofenac | 4 | 0.452 | 63.72% |
| 8 | 0.405 | 67.49% | |
| 16 | 0.384 | 69.18% | |
| 32 | 0.357 | 71.43% |
Table 7.
Chemical profile of Zingiber officinale extract by GC-MS.
| Peak | Rotation Time | Contents % | Compound name | Molecular Formula | Molecular weight |
|---|---|---|---|---|---|
| 1 | 9.18 | 0.68 | Decanal | C10H20O | 156 |
| 2 | 16.85 | 0.98 | Dodecanamine, N, N-dimethyl- | C14H31N | 213 |
| 3 | 18.89 | 10.50 | Thymol | C10H14O | 150 |
| 4 | 20.55 | 3.26 | Phenol, 2-methyl-5-(1-methylethyl)- Carvacrol | C10H14O | 150 |
| 5 | 22.74 | 2.32 | Eugenol | C10H12O2 | 166 |
| 6 | 23.88 | 0.47 | Alpha-terpineol | C10H20O | 156 |
| 7 | 26.24 | 2.14 | Butanedioic acid, 2,3-bis(acetyloxy) | C8H14O8 | 182 |
| 8 | 27. 39 | 0.76 | Benzenediamine, 2,5-dimethoxy-alpha | C12H17NO2 | 207 |
| 8 | 30. 15 | 655 | Shogaol | C19H28O3 | 304 |
| 10 | 31.35 | 45.05 | Gingerol | C17H28O4 | 246 |
| 12 | 32.83 | 16.05 | Zingiberene | C15H27 | 207 |
| 13 | 34.72 | 3.44 | Beta-bisabolene | C15H22 | 200 |
| 14 | 36.15 | 2.26 | E-11-hexadecenoic acid, ethyl ester | C18H34O2 | 282 |
| 15 | 37.90 | 6.69 | Cyclohexane, 3-(1,5-dimethyl-4-hexenyl)- | C15H24 | 204 |
| 16 | 39.35. | 1.25 | Farnesyl acetone | C18H27O | 269 |
| 17 | 42.16 | 1.26 | Desoxo-9x-hydroxy-7-ketoingol 3,8,9,12-tetraacetate | C28H38O10 | 534 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



