
Submitted:
30 June 2023
Posted:
30 June 2023
You are already at the latest version
Abstract
The incidence of carbapenem-resistant Enterobacteriaceae (CRE) has been increasing considerably annually since being first reported in 2008. Gyeonggi Province has the largest number of healthcare facilities in South Korea, which contribute to its regional vulnerability to CRE infections. Thus, there is a need to obtain up to date information on the occurrence of CRE infections in the Gyeonggi Province to take corrective measures. Therefore, in this study, we aimed to investigate the overall trends of CRE occurrence in Gyeonggi Province over the past 4 years and the epidemiological characteristics of CRE-related mortality. Patients admitted to a healthcare facility in Gyeonggi Province from January 2018 to December 2021 with positive blood cultures to CRE were included in the study and investigated. Additionally, the risk factors for CRE-related death were determined using data from CRE-positive patients who died within 30 days of last blood sampling. Older adults aged 70 and over accounted for the highest percentage of both survivors and non-survivors with CRE bacteremia. The number of non-survivors was higher in tertiary hospitals and among patients in intensive care unit. There were no significant differences in the mortality risk according to the use of antibiotics. Moreover, non-survivors were predominant among patients with hypertension, malignant tumor, and those having two or more underlying diseases. Klebsiella pneumoniae was the most common CRE strain in both survivors and non-survivors. Among the survivors, carbapenemase-producing Enterobacteriaceae was detected in 151 cases (71.2%) and 49 cases (23.1%) in the KPC and NDM groups, respectively. Among the non-survivors, it was detected in 25 cases (86.2%) and 5 cases (17.2%) in the KPC and NDM groups, respectively. The endemicity of CRE in South Korea has been proposed for several years; our results have suggested endemicity of CRE in the Gyeonggi Province. Despite the strengthened infection control policies in healthcare facilities during the pandemic, there has been an increasing trend in the isolation of CRE strains in South Korean long-term care hospitals and hospitals within Gyeonggi Province. Factors such as history of hospitalization and underlying diseases have been identified as risk factors for CRE-related deaths. However, to address this issue strictly, it is important to establish infection control infrastructure tailored based on each type of healthcare facility, and elaborate specific government support measures, accordingly.
Keywords:
carbapenem-resistant Enterobacteriaceae (CRE)
; carbapenemase-producing Enterobacteriaceae (CPE)
; death toll
; epidemiologic characteristic
1. INTRODUCTION
The increasing prevalence of infections caused by bacteria that produce carbapenemases has been recognized as a global public health threat [1,2]. While carbapenems are considered the “last resort” for the treatment of multidrug-resistant Gram-negative bacterial infections, the growing incidence of antimicrobial resistance has necessitated a greater use of carbapenems, thereby increasing the prevalence of carbapenem-resistant Enterobacteriaceae (CRE) [3,4]. Over the past 4 years, 45,436 cases of CRE infection have been reported in South Korea, and the number of reported cases and reporting healthcare facilities has continuously increased [3]. In South Korea, since the first report in 2008, the frequency of CRE infections has increased rapidly every year. In December 2010, CRE infection was designated as a legal infectious disease and controlled by a sentinel surveillance system. The domestic outbreak in 2015–2016 was followed by a switch to a mandatory surveillance system in June 2017 for monitoring, patient management, and outbreak response [5]. With the recent increase in reports of CRE epidemics in healthcare facilities and the very high incidence and fatality rates [6,7,8,9,10], especially in CRE epidemics in long-term care facilities wherein the mortality rate is higher than in other healthcare facilities the importance of CRE is being further emphasized [7,11].
Since CRE is transmitted through direct or indirect contact with infected patients, pathogen carriers, or through contaminated instruments, items, or environmental surfaces, infection control in healthcare facilities is crucial for disease prevention [12,13,14]. Although the scope and intensity of recommendations for the prevention and management of CRE epidemics are diverse, early detection of CRE and active CRE monitoring are recommended for high-risk groups, showing risk factors for transmission during hospitalization [12,14,15], and screening should also be performed before or during hospitalization in healthcare facilities [15].
Most patients with CRE infections are simple carriers and do not receive treatment; however, many patients show resistance to various classes of antibiotics, making clinical treatment difficult. CRE mainly causes urinary tract infections as well as various infections such as gastroenteritis, pneumonia, and sepsis. In addition, it affects patient prognosis and is associated with a high mortality rate of 40–50% [16].
According to the national healthcare facility standard data (as of October 2022) obtained from facilities that can accommodate more than 30 patients, Gyeonggi-do contains the largest number of healthcare facilities in South Korea (877/4644, 18%), including 328 of the 1,525 long-term care facilities nationwide; highlighting the regional characteristics that make it more vulnerable to CRE infections, and thus requiring major management. Therefore, in this study, we analyzed the cases of CRE-bacteremia between January 2018 and December 2021 in Gyeonggi-do and examined the factors affecting CRE-related deaths in these cases. These findings are expected to clarify the epidemiological characteristics of CRE-related deaths and present the basis for countermeasures against infectious diseases and managing CRE infections in South Korea.
2. RESULTS
2.1. Demographic and clinical characteristics
Table 1 presents the data for the sex, age, hospitalization history, and healthcare institutions of CRE-bacteremia from 2018 to 2021 and classified by survival and death. The 454 reported cases in which CRE strains were isolated from blood cultures included 57 deaths (35 males and 22 females; sex ratio, 1.6:1). The survivors included 216 males and 181 females (sex ratio, 1.2:1). The median age was 72 (range, 50–97) years among those who died and 71 years (range, 0–96) years among those who survived, which included a very young survivor (0 years of age; infant). In comparisons based on age, the deaths were higher than that of survivors in the 30s, 40s, 50s, and 90s, and the survivors were higher in the 60s, 70s, and 80s.
Although CRE was sometimes identified during outpatient or home nursing care, survivors’ hospitalization rate was higher (92.2% for survivors and 80.7% for deaths). In contrast, the intensive care unit (ICU) admission rate was higher among deceased cases (26.3% in deceased cases and 25.4% in survivors). Also, the percentage of cases confirmed through outpatient visits and home nursing was higher among deceased cases (7.0% for deceased cases and 4.5% for survivors).
In analyses based on the type of healthcare institution, CRE reports were received from tertiary hospitals, general hospitals, long-term care facilities, and hospitals. Tertiary hospitals accounted for the highest proportion of deaths (27/57 deaths, 47.4%), followed by general hospitals (25 deaths, 43.9%), long-term care facilities (4 deaths, 7.0%), and hospitals (1 death, 1.7%). When examining the distribution of deaths by type of healthcare facility and year, the percentage of reported cases from general hospitals was the highest in all 4 years, while the number of reported cases in tertiary hospitals was high in 2020 but decreased in 2021. Long-term care facilities and hospitals showed the same pattern in 2019 and 2020 but with an increasing trend in 2021. The proportion of survivors was the highest in general hospitals (211/397 cases, 53.1%), followed by tertiary hospitals (146 cases, 36.8%), long-term care facilities (32 cases, 8.1%), and hospitals (8 cases, 2.0%). The distribution of cases by healthcare facility type and year (Figure 1 and Figure 2) showed that in long-term care facilities, general hospitals, and tertiary general hospitals, the number of CRE reports increased in 2020 and subsequently decreased from 2021, whereas in hospitals, it decreased from 2020 onwards.
The distribution of CRE infection survivors and CRE-related deaths in healthcare facilities in Gyeonggi-do revealed that the number of CRE infection survivors in hospitals gradually decreased in 2020. In long-term care facilities, the number of survivors increased in 2020 and showed the same trend in 2021; in general hospitals and tertiary hospitals, the number of survivors increased in 2020 and then decreased again from 2021. No CRE-related deaths were reported from hospitals in 2019, 2020, 2021, and from long-term care facilities in 2021. In general hospitals and tertiary hospitals, the number of deaths increased in 2020 with a similar trend in the number of survivors but decreased again in 2021. Antibiotic usage was higher among survivors, with a history of antibiotic usage reported for 40.6% of the survivors and 29.8% of the deaths; however, mortality risk did not differ significantly with the usage of antibiotics (Table 1).
Since information on underlying diseases was collected only for those who tested positive for carbapenemase-producing Enterobacteriaceae (CPE), this information was obtained for 214 patients reported as showing positive results for CPE among 454 cases (Table 2).
The underlying diseases identified in the CPE infection report were primarily categorized as follows: diabetes, stroke, renal failure, dialysis, chronic obstructive pulmonary disease, immunosuppressive drug administration, liver disease, and cancer, while other underlying diseases were categorized as others. Among the 214 patients whose underlying disease information was collected, underlying diseases were more frequently found in deceased patients than in survivors (186/397 [46.9%] survivors vs. 28/57 [46.9%] deaths). Among the eight underlying diseases, diabetes accounted for the highest proportion of survivors (35.5%, 66 cases), followed by malignant tumors (29.0%, 54 cases) and hypertension (26.9%, 50 cases). In contrast, malignant tumors were the most frequent underlying diseases in deaths (57.1%), followed by diabetes (32.1%, 9 cases) and stroke (14.3%, 4 cases). Except for hypertension and malignancy, none of the other underlying diseases showed differences in incidence between the survivors and the patients who died. In our analysis of the risk factors for death in relation to underlying disease by ORs, hypertension showed β = 1.575 and an odds ratio (OR) of 4.83 (95% confidence interval, 1.045–22.328), indicating that the odds of death in patients with hypertension were 4.83 times higher than that in those without hypertension.
2.2. CRE occurrence distribution by strains and digestive enzymes
From 2018 to 2021, a total of 454 cases of CRE-bacteremia and reported to all 43 public health centers in Gyeonggi-do (Table 3).
After excluding 15 cases in which the causative strains were not reported, Klebsiella pneumoniae comprised the largest proportion of cases in both survivors (230 cases, 59.6%) and deceased patients (37 cases, 69.8%). A total of 241 cases (53.1%) were CPE-positive. Of the 213 cases in which CPE-related information was not entered, 18 were because the confirmation test was not performed due to negative CPE results, whereas 10 were due to input errors. Of the 29 deaths among the 241 CPE-positive cases, 25 (86.2%) showed Klebsiella pneumoniae carbapenemase (KPC), and five (17.2%) showed New Delhi metallo-β-lactamase (NDM) in analyses of degradation enzymes. Among the survivors, 151 cases (71.2%) showed KPC, 49 (23.1%) showed NDM, and 11 (5.2%) showed oxacillinase (OXA) in the same pattern as among the deaths (Table 4).
The distribution of occurrence by region for each strain over 4 years confirmed similar patterns in the survivors and deaths, and K. pneumoniae, E. coli, and Enterobacter strains were identified in areas where general hospitals and tertiary healthcare facilities were concentrated (Figure 3).
3. DISCUSSION
In our analysis of CRE-bacteremia and reported from 2018 to 2021 at healthcare facilities in the Gyeonggi-do province, patients aged ≥70 comprised the largest proportions of both survivors and deaths. Since most patients were confirmed to be inpatients, hospitalization history was a risk factor for CRE-related mortality (Table 1). Since the need for critical care treatment and the possibility of hospitalization increased with age, these findings were consistent with the results of several previous studies in which the risk factors for acquiring antibiotic-resistant bacteria included a history of hospitalization in an ICU and a prolonged hospitalization period [16].
In analyses based on the type of healthcare facility, the proportion of survivors was high in secondary hospitals, but the proportion of deaths was high in tertiary hospitals (Table 1). These results can be interpreted in two ways. First, when critically ill patients were transferred from long-term care facilities and secondary hospitals to tertiary hospitals, CRE carriers were identified in a pre-hospitalization screening and classified as external infections in some cases, thereby being excluded from reporting. Second, some cases were related to risk factors for CRE colonization, such as invasive treatment and a long-term ICU stay [17]. Since critically ill patients account for a larger proportion of the cases in tertiary hospitals than in secondary hospitals and long-term care facilities, they are more likely to undergo invasive procedures such as mechanical ventilation and catheter insertion, which are known risk factors for death due to CRE infection. Although a history of antibiotic use was not a significant risk factor for death, 40.6% of survivors had a history of antibiotic use, suggesting that said use may emerge as a risk factor for mortality in the future. In previous studies, the use of antibiotics such as cephalosporins, β-lactams or β-lactam/β-lactamase inhibitors, aminoglycosides, fluoroquinolones, and glycopeptides were reported as a risk factor for CRE colonization [18,19,20,21,22].
In our analysis of underlying diseases (Table 2), diabetes was the most frequent underlying disease among survivors (66 cases, 35.5%). Consistent with the results of this study, diabetes is known to increase the risk of bloodstream infection as well as CRE infections [19,23]. In contrast, malignant tumors were the most frequent underlying diseases among the patients who died (16 cases, 57.1%). Although these results were not consistent with those of a previous study [20], in which underlying diseases related to immunosuppressed conditions, such as malignant tumors and the use of immunosuppressive drugs, were not risk factors for death, among the underlying diseases in the patients who died, hypertension and malignant tumors appeared to be correlated with survival. The odds of death in patients with hypertension were 4.83 times higher than those without hypertension (Table 1). Hypertension is a chronic disease that often accompanies long-term hospitalization, and malignant tumors require long-term hospitalization, suggesting that exposure to antibiotics and frequent admission to healthcare institutions may be risk factors for CRE colonization.
In our analyses of the incidence trends by strain and region (Figure 3), K. pneumoniae accounted for the largest proportion regardless of patient survival, suggesting that endemicization had already progressed in the Gyeonggi-do area. As for E. coli and Enterobacter, which accounted for the second-largest proportion after K. pneumoniae, the range of cities and counties where CRE was reported showed gradual expansion. For strains such as Citrobacter koseri, Proteus rettgeri, Serratia marcescens, and Raoultella ornithinolytica, which have been reported in fewer than 10 cases (in Gyeonggi-do, as of 2022), no investigation has been conducted in relation to outbreaks, and further investigation of individual infection routes in relevant cases may reveal epidemiological links. In evaluations of the history of exposure to antibiotics and the history of visits to healthcare facilities, which are known to increase the risk of CRE infection, the occurrence of strains was the highest in densely populated areas and in areas where tertiary hospitals and general hospitals were widely distributed.
In analyses based on degradation enzymes, KPC accounted for the largest proportion (Table 4), showing the same pattern as the overall CRE and CPE separation trend in South Korea [5]. The findings of overseas CRE surveillance studies indicate that K. pneumoniae is one of the most commonly reported CRE strains worldwide [24,25,26,27]. As for degrading enzymes, KPC has been reported to be endemic in the largest number of countries [25,26,27,28,29]. The incidence trend and disease burden indicate that KPC endemicization has already progressed in the Gyeonggi-do province.
Despite yielding a number of meaningful results, this study had some limitations. First, when analyzing the underlying disease, information on other non-parameterized chronic diseases, such as hypertension, was also entered, and unlike other variables whose input methods were standardized, this information was entered in the form of a memo, making it difficult to use for analysis. Since CRE is a healthcare-associated infection, the patient’s medical information should be collected as accurately as possible through more systematic revision and supplementation of case reports, enabling more scientific disease surveillance activities. Second, the case report form was structured such that the hospitalization and sample collection dates could be entered; however, the discharge date could not be confirmed. In addition, only the past in-hospital movement route was entered if the patient was in the hospital on the reporting date. The hospitalization period is a well-known risk factor for CRE/CPE acquisition, and its relationship could, regrettably, not be confirmed through actual data. Third, KDCA’s healthcare-associated infection control guidelines advise reporting CRE and CPE infections only when strains and enzymes are added or changed or when CRE is confirmed in blood after it is isolated from clinical samples other than blood. If the classification of the patient as a carrier of the pathogen is maintained when CRE is confirmed in clinical samples other than a blood after being first isolated from blood, additional notification is not required. Therefore, when CRE is isolated from samples such as sputum or urine, the possibility that even fecal (including rectal smear) samples have been actually collected by healthcare institutions but not reported cannot be excluded. Fourth, according to the current guidelines, cases involving CRE isolated from feces, sputum, or parts other than blood are not reported to the KDCA reporting system; therefore, the actual number of deaths in healthcare facilities may differ. In the future, reports of samples other than blood should be considered to contain data that can provide a closer analysis of the risk factors for death. Fifth, while managing the correct use of antibiotics is an important strategy for preventing multidrug-resistant bacterial infections, confirming the exact duration of antibiotic administration was difficult since only the presence and type of antibiotics administered within 3 months could be entered in the case report.
Despite these limitations, this study is meaningful in that it identified changes in the CRE occurrence trends and the epidemiological characteristics related to the deaths of patients, showing blood cultures positive for CRE/CPE based on 4-year cumulative reporting data. Since the CRE pattern change in South Korea was predicted several years ago, this study confirmed the results suggesting the CRE pattern changes and identified hospitalization history and underlying diseases as characteristics of CRE-related deaths.
For high-risk patients who are vulnerable to CRE infection due to the frequent use of antibiotics and use of multiple invasive devices in acute care hospitals, the Gyeonggi-do Center for Infectious Disease Control and Prevention conducts CRE testing upon admission to long-term care facilities [8] and enforces preemptive contact precautions before reporting the results. According to the World Health Organization guidelines [13], intensive training programs are being conducted for long-term care facility managers and infection control officials in the Gyeonggi-do province, including continuous recommendations for antibiotic use management, isolation and infection monitoring, and environmental management.
The number of CRE reports nationwide has been increasing every year, even during the COVID-19 pandemic [5,7,21]. Despite the policy to strengthen infection control in healthcare institutions during the pandemic, CRE infection cases in the long-term care facilities and hospitals in the Gyeonggi-do province increased in 2021 in this study. Thus, while struggling to respond to COVID-19, infection control officials may have also found it difficult to regularly monitor infection control in the hospital and focus on managing multidrug-resistant bacteria.
The COVID-19 pandemic has changed the healthcare system and, at least temporarily, increased the rates of healthcare-associated infections and multidrug-resistant bacteria worldwide [30,31]. A study investigating healthcare-associated infections during the COVID-19 epidemic in 53 hospitals in the United States showed a significant increase in the rates of central line-associated bloodstream infection, ventilator-associated events, and Clostridioides difficile infections in small community hospitals. In this regard, establishing a cooperative system involving the government, regional institutions, and medical systems, focusing on understanding and exploring the problems encountered by infectious disease specialists and the resource constraints faced by community hospitals, has been suggested [32]. Although the COVID-19 epidemic has passed the critical stage, maintenance of a sustainable policy to prevent healthcare-associated infections and multidrug-resistant bacteria from being neglected for new infectious diseases occurring in the future, infection control infrastructure suitable for each type of medical institution should be established, and the government’s support measures should be differentiated accordingly.
To prevent the spread of healthcare-associated infectious diseases caused by multidrug-resistant bacteria, appropriate antibiotic usage should be implemented through Antimicrobial Stewardship Programs [33], and active infection control measures, such as quarantine, contact testing, and monitoring, should be performed continuously by identifying strains at an early stage through prompt reporting. Elimination and eradication of CRE can be achieved through continuous and persistent infection control efforts by healthcare institutions, local governing bodies, and the government.
4. METHODS
4.1. Data collection
Data for this analysis were obtained through the integrated disease health management system of the Korea Disease Control and Prevention Agency (KDCA) (https://is.cdc.go.kr/). To ensure the security of surveillance data and protect personal information, identifying data other than demographic characteristics such as age or sex were discarded before analysis. Gyeonggi-do hospital status data were obtained from the public data portal (https://www.data.go.kr) used by the Ministry of Public Administration and Security. Moreover, healthcare institutions were classified into tertiary general hospitals and general hospitals, and analyzed using the current state data of Gyeonggi-do general hospitals, released by the Gyeonggi-do Health and Medical Policy Division on the website of the Gyeonggi-do Office (https://www.gg.go.kr).
4.2. Statistical analysis
This study involved a retrospective review of patient and death report data from cases in which CRE strains were isolated and reported in Gyeonggi-do over a 4-year period from 2018 to 2021. General characteristics, including the distribution of incidence by sex, age, and region, as well as overall incidence trends, were examined. Further, to determine the relationship between survival and death in relation to underlying disease and route of infection, as well as the major risk factors for healthcare-associated infection, including invasive procedures and history of hospitalization in an ICU, a chi-square test, an independent t-test, and Fisher’s exact test were conducted. Logistic regression analysis was used to analyze the ORs for correlation comparisons, with statistical significance set at P < 0.05. R version 4.2.1 and IBM SPSS version 26 were used for data analysis, and the analysis results were visualized using Tableau version 2020.4.
4.3. Definition of cases
According to the 2022 healthcare-associated infectious disease management guidelines published by KDCA, CRE-related deaths were defined as cases showing the presence of CRE, regardless of the presence of clinical symptoms, in which the patient died within 30 days after the last positive blood sample was collected. In this study, cases were defined according to the same criteria, wherein resistance to carbapenem antibiotics was defined as resistance to at least one carbapenem antibiotic, such as doripenem, imipenem, meropenem, or ertapenem, as evidenced in a culture test [34]. The test criteria for diagnosis included the isolation and identification of carbapenem-type antibiotic-resistant Enterobacteriaceae species from clinical samples through culture tests, after which the association between patient report history and pathogen report (culture test result) was also confirmed.
Author Contributions
Conceptualization: Chanhee Kim, Heeyoung Lee, Kun-hee Park. Data curation: Seung Hye Lee, Chanhee Kim. Formal analysis: Seung Hye Lee, Chanhee Kim. Investigation: Seung Hye Lee, Chanhee Kim. Methodology: Heeyoung Lee, Kun-hee Park. Project administraion: Heeyoung Lee, Kun-hee Park, Su Ha Han. Validation: Su Ha Han. Visualization: Seung Hye, Su Ha Han. Writing—original draft: Seung Hye Lee. Writing—review & editing: Su Ha Han.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
The present study was approved by the Institutional Review Board of Seoul National University Bundang Hospital (approval number: X-2212-797-901).
Informed Consent Statement
Informed consent was waived by the committee because this was a retrospective chart review study.
Data Availability Statement
The data used in this study are protected under the Personal Information Protection Act.
Acknowledgments
We would like to express our sincere gratitude to the Gyeonggi Infectious Disease Control Center and all medical institutions for their efforts on this study. Special appreciation goes to all responsible teams at Gyeonggi-do public health centers for their dedication to this epidemiological investigation. We would also like to thank Editage (www.editage.co.kr) for English language editing.
Conflicts of Interest
The authors have no potential conflicts of interest.
References
- Bonomo, R.A.; Burd, E.M.; Conly, J.; Limbago, B.M.; Poirel, L.; Segre, J.A.; Westblade, L.F. Carbapenemase-producing Organisms: A Global Scourge. Clin. Infect. Dis. 2018, 66, 1290–1297. [Google Scholar] [CrossRef]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, Research, and Development of New Antibiotics: The Who Priority List of Antibiotic Resistant Bacteria and Tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Joo, S.J.; Kim, M.K.; Shin, E.K.; Kim, J.Y.; Yoo, J.I. Molecular characteristic analysis and antimicrobial resistance of carbapenem-resistant Enterobacteriaceae (CRE) isolates in the Republic of Korea, 2017-2020. Weekly Health and Diseases 2021, 14, 3790–3804. Available online: https://www.kdca.go.kr/filepath/boardDownload.es?bid=0031&list_no=718138&seq=1.
- Park, S.H.; Kim, J.S.; Kim, H.S.; Yu, J.K.; Han, S.H.; Kang, M.J.; Chae-Kyu, H.; Sang-Me, L.; Young-Hee, O. Prevalence of Carbapenem-resistant Enterobacteriaceae in Seoul, Korea. The Korean Society for Microbiology 2020, 50, 107–116. [Google Scholar] [CrossRef]
- Go, E.B.; Ju, S.J.; Park, S.D.; Yoo, J.I.; Hwang, K.J. Distributions of Carbapenem-resistant Enterobacteriaceae (CRE) in Korea, 2018. Public Health Wkly. Rep. 2019, 12, 1977–1983. Available online: https://www.kdca.go.kr/filepath/boardDownload.es?bid=0031&list_no=711197&seq=1.
- Jeong, H.S.; Hyun, J.H. ; Lee,Y. K. Characteristics of Carbapenem-resistant Enterobacteriaceae (CRE) in the Republic of Korea, 2021. Public Health Wkly. Rep. 2022, 15, 2360–2363. Available online: https://www.kdca.go.kr/filepath/boardDownload.es?bid=0031&list_no=720486&seq=1.
- Park, J.J.; Seo, Y.B.; Lee, J.; Eom, J.S.; Song, W.; Choi, Y.K.; Kim, S.R.; Son, H.J.; Cho, N.H. Positivity of Carbapenemase-Producing Enterobacteriaceae in Patients Following Exposure Within Long-Term Care Facilities in Seoul, Korea. J. Korean Med. Sci. 2020, 35, e303. [Google Scholar] [CrossRef]
- Jung, S.W.; Park, S.S. Outbreak of Carbapenem-Resistant Enterobacteriaceae (Cre) In a Long-Term Acute Care Facility in the Republic of Korea. Infect. Control Hosp. Epidemiol. 2022, 27, 43–50. [Google Scholar]
- Lim, Y.J.; Kim, M.N.; Choi, S.H. Clearance of Carbapenemase-Producing Enterobacteriaceae (Cpe) Carriage: A Comparative Study of Ndm-1 and Kpc Cpe - Author’s Reply. Clin. Microbiol. Infect. 2019, 25, 776. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.; Choi, H.S.; Lee, J.Y.; Ryu, S.H.; Kim, S.K.; Hong, M.J.; Kwak, S.H.; Kim, H.J.; Lee, M.S.; Sung, H.; et al. Outbreak of Carbapenemase-Producing Enterobacteriaceae Associated With a Contaminated Water Dispenser and Sink Drains in the Cardiology Units of a Korean Hospital. J. Hosp. Infect. 2020, 104, 476–483. [Google Scholar] [CrossRef]
- Chen, H. Y. , Jean, S. S., Lee, Y. L., Lu, M. C., Ko, W. C., Liu, P. Y., & Hsueh, P. R. Carbapenem-Resistant Enterobacterales in Long-Term Care Facilities: A Global and Narrative Review. Frontiers in cellular and infection microbiology 2021, 11, 601968. [Google Scholar]
- Centers for Disease Control and Prevention. Facility Guidance for Control of Carbapenem-resistant Enterobacteriaceae (CRE) – November 2015 Update CRE Toolkit. Centers for Disease Control and Prevention; 2015. Available online: https://www.cdc.gov/hai/pdfs/cre/cre-guidance-508.pdf.
- Guidelines for the prevention and control of carbapenem-resistant Enterobacteriaceae, Acinetobacter baumannii and Pseudomonas aeruginosa in health care facilities. Geneva, Switzerland: World Health Organization; 2017. Available online: https://apps.who.int/iris/handle/10665/259462.
- Magiorakos, A. P. , Burns, K., Rodríguez Baño, J., Borg, M., Daikos, G., Dumpis, U.,... & Weber, J. T. Infection prevention and control measures and tools for the prevention of entry of carbapenem-resistant Enterobacteriaceae into healthcare settings: guidance from the European Centre for Disease Prevention and Control. Antimicrobial Resistance & Infection Control, 2017, 6, 1–17. [Google Scholar] [CrossRef]
- Gomides, M. D. A. , Fontes, A. M. S., Silveira, A. O. S. M., Matoso, D. C., Ferreira, A. L., & Sadoyama, G. The importance of active surveillance of carbapenem-resistant Enterobacterales (CRE) in colonization rates in critically ill patients. PloS one, 2022, 17, e0262554. [Google Scholar] [CrossRef]
- Schwartz-Neiderman, A.; Braun, T.; Fallach, N.; Schwartz, D.; Carmeli, Y.; Schechner, V. Risk Factors for Carbapenemase-Producing Carbapenem-Resistant Enterobacteriaceae (Cp-Cre) Acquisition Among Contacts of Newly Diagnosed Cp-Cre Patients. Infect. Control Hosp. Epidemiol. 2016, 37, 1219–1225. [Google Scholar] [CrossRef]
- Logan, L.K.; Weinstein, R.A. The Epidemiology of Carbapenem-Resistant Enterobacteriaceae: The Impact and Evolution of a Global Menace. J. Infect. Dis. 2017, 215, S28–S36. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.; Kim, K.H. Identification and Infection Control of Carbapenem-Resistant Enterobacterales in Intensive Care Units. Acute Critical Care 2021, 36, 175–184. [Google Scholar] [CrossRef]
- Kang, J.S.; Yi, J.; Ko, M.K.; Lee, S.O.; Lee, J.E.; Kim, K.H. Prevalence and Risk Factors of Carbapenem-Resistant Enterobacteriaceae Acquisition in an Emergency Intensive Care Unit in a Tertiary Hospital in Korea: A Case-Control Study. J Korean Med Sci 2019, 34, e140. [Google Scholar] [CrossRef]
- Jiao, Y. , Qin, Y., Liu, J., Li, Q., Dong, Y., Shang, Y., Huang, Y., & Liu, R. (2015). Risk factors for carbapenem-resistant Klebsiella pneumoniae infection/colonization and predictors of mortality: a retrospective study. Pathogens and global health, 109, 68–74. [CrossRef]
- Lee, H.J.; Choi, J.K.; Cho, S.Y.; Kim, S.H.; Park, S.H.; Choi, S.M.; Lee, D.G.; Choi, J.H.; Yoo, J.H. Carbapenem-Resistant Enterobacteriaceae: Prevalence and Risk Factors in a Single Community-Based Hospital in Korea. Infect. Chemother. 2016, 48, 166–173. [Google Scholar] [CrossRef]
- Swaminathan, M.; Sharma, S.; Poliansky Blash, S.; Patel, G.; Banach, D.B.; Phillips, M.; LaBombardi, V.; Anderson, K.F.; Kitchel, B.; Srinivasan, A.; et al. Prevalence and Risk Factors for Acquisition of Carbapenem-Resistant Enterobacteriaceae in the Setting of Endemicity. Infect. Control Hosp. Epidemiol. 2013, 34, 809–817. [Google Scholar] [CrossRef]
- Michalia, M.; Kompoti, M.; Koutsikou, A.; Paridou, A.; Giannopoulou, P.; Trikka-Graphakos, E.; Clouva-Molyvdas, P. Diabetes Mellitus Is an Independent Risk Factor for ICU-Acquired Bloodstream Infections. Intensive Care Med. 2009, 35, 448–454. [Google Scholar] [CrossRef]
- Guh, A.Y.; Bulens, S.N.; Mu, Y.; Jacob, J.T.; Reno, J.; Scott, J.; Wilson, L.E.; Vaeth, E.; Lynfield, R.; Shaw, K.M.; et al. Epidemiology of Carbapenem-resistant Enterobacteriaceae in 7 US Communities, 2012-2013. JAMA. 2015, 314, 1479–1487. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J-H. The Infinity War: How to Cope With Carbapenem-Resistant Enterobacteriaceae. J. Korean Med. Sci. 2018, 33, e255. [CrossRef]
- Zhang, Y.; Wang, Q.; Yin, Y.; Chen, H.; Jin, L.; Gu, B.; Xie, L.; Yang, C.; Ma, X.; Li, H.; et al. Epidemiology of Carbapenem-Resistant Enterobacteriaceae Infections: Report From the China CRE Network. Antimicrob. Agents Chemother. 2018, 62, e01882–17. [Google Scholar] [CrossRef]
- Suay-García, B.; Pérez-Gracia, M.T. Present and Future of Carbapenem-resistant Enterobacteriaceae (CRE) Infections. Antibiotics (Basel) 2019, 8, 122. [Google Scholar] [CrossRef] [PubMed]
- Bonomo, R.A.; Burd, E.M.; Conly, J.; Limbago, B.M.; Poirel, L.; Segre, J.A.; Westblade, L.F. Carbapenemase-Producing Organisms: A Global Scourge. Clinical Infect. Dis. 2018, 66, 1290–1297. [Google Scholar] [CrossRef]
- Kelly, A.M.; Mathema, B.; Larson, E.L. Carbapenem-Resistant Enterobacteriaceae in the Community: A Scoping Review. Int. J. Antimicrob. Agents 2017, 50, 127–134. [Google Scholar] [CrossRef]
- Fakih, M.G.; Bufalino, A.; Sturm, L.; Huang, R.H.; Ottenbacher, A.; Saake, K.; Winegar, A.; Fogel, R.; Cacchione, J. Coronavirus Disease 2019 (COVID-19) Pandemic, Central-Line-Associated Bloodstream Infection (CLABSI), and Catheter-Associated Urinary Tract Infection (CAUTI): The Urgent Need to Refocus on Hardwiring Prevention Efforts. Infect. Control Hosp. Epidemiol. 2022, 43, 26–31. [Google Scholar] [CrossRef]
- Witt, L.S.; Howard-Anderson, J.R.; Jacob, J.T.; Gottlieb, L.B. The Impact of COVID-19 on Multidrug-Resistant Organisms Causing Healthcare-Associated Infections: A Narrative Review. JAC Antimicrob. Resist. 2022, 5, 1–9. [Google Scholar] [CrossRef]
- Advani, S.D.; Sickbert-Bennett,E. ; Moehring, R.; Cromer, A.; Lokhnygina, Y.; Dodds-Ashley, E.; Kalu, I.C.; DiBiase, L.; Weber, D.J.; Anderson, D.J.; CDC Prevention Epicenters Program. The Disproportionate Impact of Coronavirus Disease 2019 (COVID-19) Pandemic on Healthcare-Associated Infections in Community Hospitals: Need for Expanding the Infectious Disease Workforce. Clin. Infect. Dis. 2023, 76, e34–e41. [Google Scholar] [CrossRef]
- French, C.E.; Coope, C.; Conway, L.; Higgins, J.P.; McCulloch, J.; Okoli, G.; Patel, B.C.; Oliver, I. Control of Carbapenemase-Producing Enterobacteriaceae Outbreaks in Acute Settings: An Evidence Review. J. Hosp. Infect. 2017, 95, 3–45. [Google Scholar] [CrossRef]
- Guideline for Healthcare-Associated Infection. North Chungcheong Province, South Korea: Korea Disease Control and Prevention Agency (KDCA); 2022. Available online: https://www.kdca.go.kr/board/board.es?mid=a20507020000&bid=0019.
Figure 1.
Healthcare institution type distribution of CRE-bacteremia Reporting cases by year, 2018-2021.
Figure 1.
Healthcare institution type distribution of CRE-bacteremia Reporting cases by year, 2018-2021.
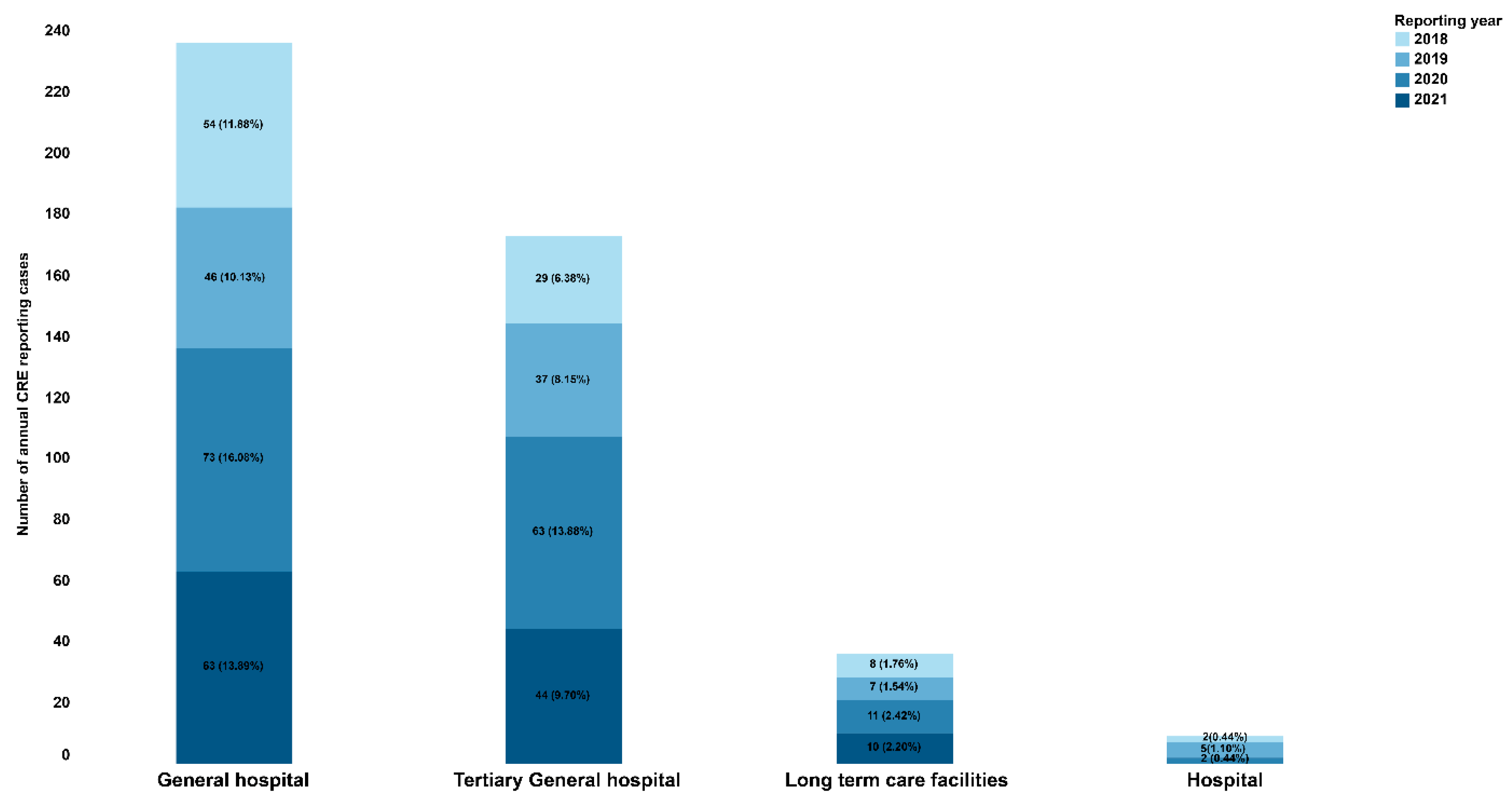
Figure 2.
Annual CRE bacteremia related survivors and deaths by healthcare facility type, 2018-2021.
Figure 2.
Annual CRE bacteremia related survivors and deaths by healthcare facility type, 2018-2021.
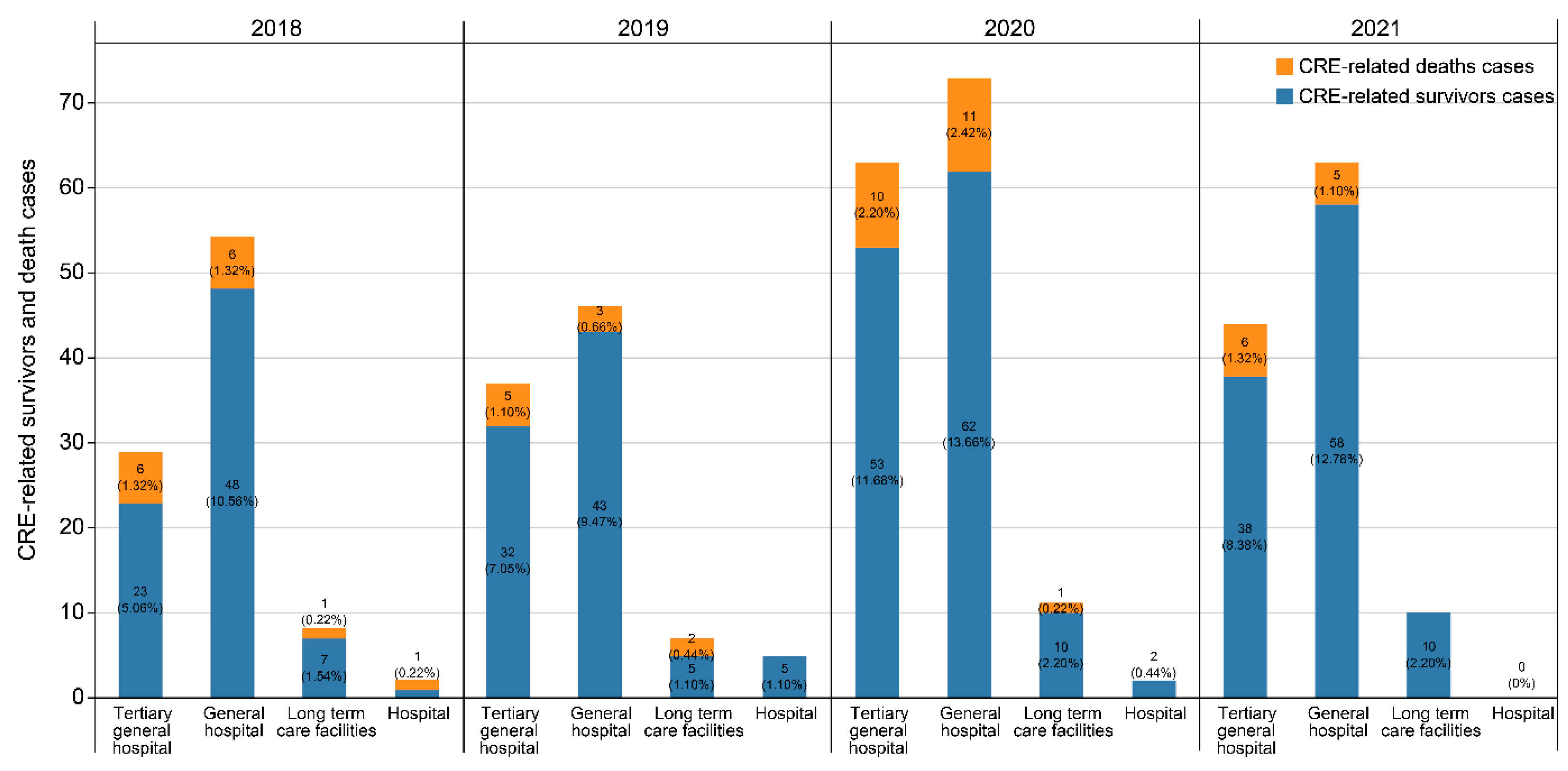
Figure 3.
Choropleth Map of CRE bacteremia in Gyeonggi Province, South Korea, 2018-2021.
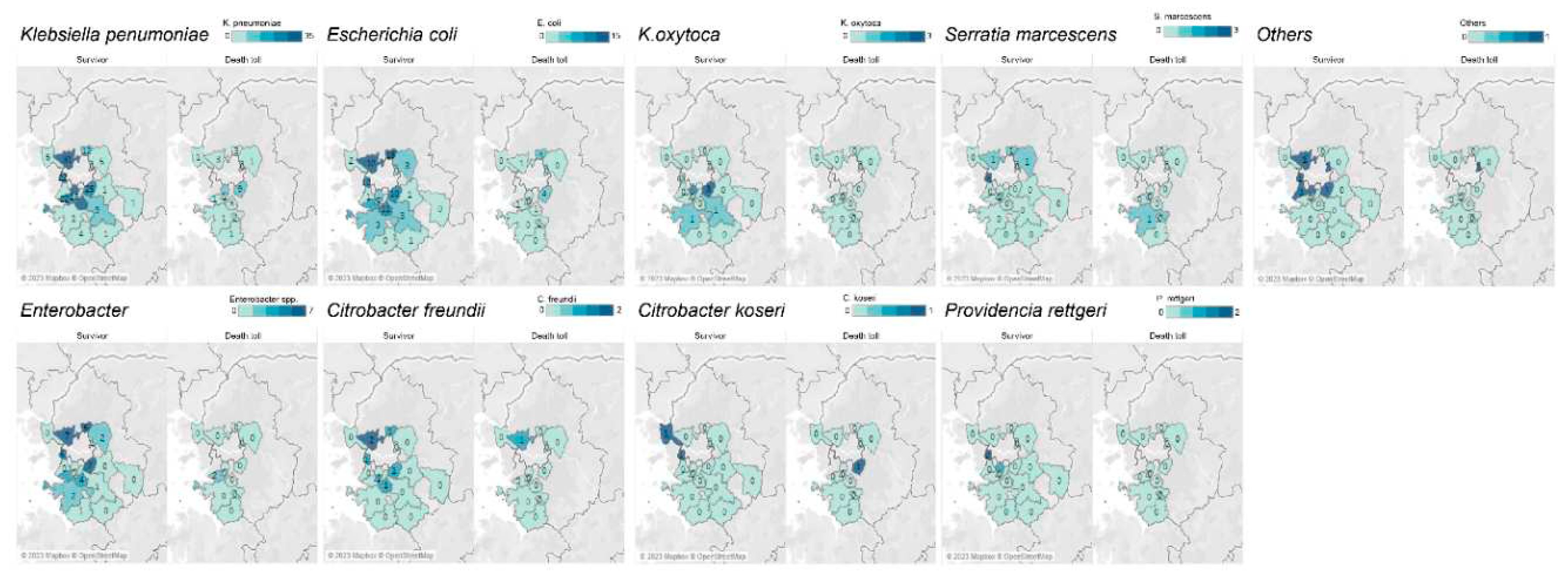

Table 1.
Demographical and clinical characteristics of CRE bacteremia, 2018 -2021.
| Survivor (n=397) | Death toll(n=57) | t or χ² | P-value | |
|---|---|---|---|---|
| N (%) | N (%) | |||
| Demographics | ||||
| Gender, Female (%) | 181 (45.6) | 22 (38.6) | 0.9867 | .3206 |
| Age, median, years (range) | 71 (0–96) | 72 (50-97) | 0.0382 | .5152 |
| Age group, years | ||||
| 0–9 | 2 (0.5) | 0 (0.0) | ||
| 10–19 | 1 (0.3) | 0 (0.0) | ||
| 20–29 | 7 (1.8) | 0 (0.0) | ||
| 30–39 | 7 (1.8) | 3 (5.3) | ||
| 40–49 | 20 (5.0) | 5 (8.8) | ||
| 50–59 | 57 (14.4) | 9 (15.8) | ||
| 60–69 | 93 (23.4) | 11 (19.3) | ||
| 70–79 | 102 (25.7) | 12 (21.1) | ||
| 80–89 | 94 (23.7) | 12 (21.1) | ||
| 90–99 | 14 (3.5) | 5 (8.8) | ||
| Clinical characteristics | ||||
| Hospitalization | 366 (92.2) | 46 (80.7) | 7.8377 | .0051 |
| Intensive care unit history | 101 (25.4) | 15 (26.3) | ||
| Visit clinics | 18 (4.5) | 4 (7.0) | ||
| Healthcare facilities | ||||
| Tertiary General hospitals | 146 (36.8) | 27 (47.4) | ||
| General hospitals | 211 (53.1) | 25 (43.9) | ||
| Lone-term care facilities | 32 (8.1) | 4 (7.0) | ||
| Antibiotics * | ||||
| Yes | 161 (40.6) | 17 (29.8) | 0.9635 | .3263 |
| Carbapenems | 92 (46.9) | 14 (49.1) | ||
| Cephalosporins | 87 (53.1) | 6 (50.9) | ||
| Fluoroquinolones | 50 (35.5) | 5 (32.1) | ||
| Aminoglycosides | 38 (26.9) | 2 (7.1) | ||
| Glycopeptides | 43 (15.1) | 6 (14.3) | ||
| Other antibiotics | 54 (29.0) | 0 (0) | ||
* multiple selection.
Table 2.
Underlying conditions of CRE bacteremia, 2018-2021.
| Survivor(n=186) | Death toll(n=28) | t or χ² | P-value | OR (95% CI) | |
|---|---|---|---|---|---|
| Underlying conditions N (%) N (%) | |||||
| Diabetes | 66 (35.5) | 9 (32.1) | 0.119 | 0.730 | 0.257 (0.422–3.743) |
| Hypertension | 50 (26.9) | 2 (7.1) | 5.155 | 0.023 | 4.830 (1.045–22.328) |
| Brain stroke | 28 (15.1) | 4 (14.3) | 1 | 1.329 (0.373–4.738) | |
| Any malignancy | 54 (29.0) | 16 (57.1) | 8.737 | 0.003 | 0.425 (0.183–0.990) |
| Renal failure | 18 (9.7) | 3 (10.7) | 0.743 | 1.444 (0.290–7.177) | |
| Liver disease | 16 (8.6) | 3 (10.7) | 0.721 | 1.252 (0.280–5.590) | |
| Chronic obstructive pulmonary disease | 4 (2.2) | 1 (3.6) | 0.508 | 0.676 (0.052–8.795) | |
| Dialysis | 8 (4.3) | 3 (10.7) | 0.161 | 0.358 (0.055–2.319) | |
| Immunosuppressantadministration | 1 (0.5) | 0 (0.0) | 1 | - | |
| More than two underlying diseases | 61 (32.8) | 14 (50.0) | 3.164 | 0.075 | 0.440 (0.188–1.033) |
| Other diseases | 83 (44.6) | 11(39.3) | 0.282 | 0.596 | 1.039 (0.380–2.842) |
OR, odds ratio; CI, confidence interval.
Table 3.
Strain of CRE bacteremia, 2018 and 2021.
| Strain | Survivor (n=386) | Death toll (n=53) |
|---|---|---|
| N (%) | N (%) | |
| Klebsiella pneumoniae | 230 (59.6) | 37 (69.8) |
| Escherichia coli | 89 (23.1) | 13 (24.5) |
| Enterobacter | 41 (10.6) | 2 (3.8) |
| Citrobacter freundii | 7 (1.8) | 1 (1.9) |
| Klebsiella oxytoca | 7 (1.8) | 0 (0.0) |
| Serratia marcescens | 7 (1.8) | 1 (1.9) |
| Citrobacter koseri | 2 (0.5) | 1 (1.9) |
| Providencia rettgeri | 3 (0.8) | 0 (0.0) |
| Multiple strain | 11 (2.8) | 3 (5.7) |
| Others | 6 (1.6) | 1 (1.9) |
Table 4.
Carbapenemase-producing CRE bacteremia, 2018-2021.
| Strain * | Survivor (n=212) | Death toll (n=29) |
|---|---|---|
| N (%) | N (%) | |
| KPC | 151 (71.2) | 25 (86.2) |
| NDM | 49 (23.1) | 5 (17.2) |
| OXA | 11 (5.2) | 0 (0.0) |
| VIM | 0 (0.0) | 0 (0.0) |
| IMP | 0 (0.0) | 0 (0.0) |
| GES | 7 (3.3) | 0 (0.0) |
KPC, Klebsiella pneumoniae carbapenemase; NDM, New Delhi metallo-β-lactamase; OXA, Oxacillinase; IMP, Imipenemase; VIM, Verona integron-encoded metallo-β-lactamase; GES, Guiana extended spectrum β-lactamase. * Multiple selection.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



