
Submitted:
30 June 2023
Posted:
30 June 2023
You are already at the latest version
Abstract
Background: Malnutrition in oesophageal and pharyngeal cancer patients constitutes a common and serious concern, which significantly reduces patients’ prognosis. Cancers of the oesophagus and the pharynx can considerably impair feeding in patients, resulting in severe undernutrition. This is a scoping review which aims to critically summarize and scrutinize the current clinical evidence on the use and prognostic role of diverse nutritional assessment tools on the prognosis of patients with oesophageal and pharyngeal cancers. Methods: PubMed, Scopus, Web of Science and Google Scholar databases were comprehensively explored utilizing relative keywords to detect clinical studies that investigate whether nutritional status may affect disease prognosis. Results: Several assessment tools have evaluated and highlighted the prognostic role of nutritional status on patients’ survival and disease complications in both oesophageal and pharyngeal cancers. Regarding oesophageal cancer, CONUT, PNI, PG-SGA and NRS-2002 are more commonly used, while albumin is also frequently evaluated. Regarding pharyngeal cancers, fewer studies are currently available. PNI has been evaluated and its significance as a factor for shorter overall survival, distant metastasis-free survival, progression-free survival, and locoregional recurrence-free has been highlighted. Comprehensive Nutritional Index has also been evaluated with positive results, as well as NRS 2002, GPS, and body weight status. However, there is currently a lack of studies with adequate female patients. There is also a significant lack of well-designed prospective studies with well-organized methodology. Conclusion: Nutritional status may significantly affect disease progression and patients’ survival, highlighting the importance of a good nutritional status in patients with oesophageal and pharyngeal cancers. Further large-scaled and well-designed prospective clinical studies are strongly recommended to verify the potential beneficial effects of nutritional status in patients with oesophageal and pharyngeal cancers.
Keywords:
nutritional assessment
; oesophageal cancer
; pharyngeal cancer
; prognosis
; survival
; nutritional status
; diagnosis
; malnutrition
; chemotherapy
; radiotherapy
1. Introduction
Cancer is one of the most common causes of death, accounting for 1 in 6 deaths worldwide, according to the World Health Organization (WHO) [1]. According to the International Agency for Research on Cancer (IARC), cancer of the oesophagus ac-counted for 3.1% (604,100) of new cases, and 5.5% (544,076) of deaths worldwide in 2020 [1]. In the meantime, 98,412 new cases of oropharyngeal cancers, and 133,354 new cases of nasopharyngeal cancers were diagnosed, while 48,143 and 80,008 deaths were accounted due to oropharyngeal and nasopharyngeal cancers, respectively [1].
Around one-third of cancer deaths are caused by the following lifestyle choices: high Body Mass Index (BMI), low fruit and vegetable intake, low levels of physical activity, smoking and alcohol. Smoking is considered to be the most important risk factor for cancer, causing 20% of cancer deaths and around 70% of lung cancer deaths in the world [2,3]. Genetic and environ-mental factors influence cancer risk and development. Hereditary genetic mutations (germ-line mutations) are non-modifiable risk factors but can be found via genetic testing. It is estimated that only about 2-3% cancers diagnosed are linked to an inherited mutated gene [3,4]. Epigenetic mutations are the result of the interaction between a person's genetic factors and 3 categories of external agents, including physical carcinogens (ultraviolet and ionizing radiation), chemical carcinogens (asbestos, components of tobacco smoke, aflatoxin and arsenic), and biological carcinogens (infections from certain viruses, bacteria or parasites) [2,4]
Malnutrition constitutes a frequent finding in cancer patients, even at the time of diagnosis. Its prevalence ranges from 31% to 87%, and depends on the tumor stage, histopathological type, treatment, and the individual patient [2,3]. Weight decline commonly arises due to enhanced energy requirements, low energy intake and/or di-minished nutrients’ absorption. In carcinoma patients, undernutrition could be ascribed to several factors. Inflammation and catabolism related with tumor development and progression can lead to muscle atrophy and body weight decrease, while tumor gastrointestinal blockage can diminish food intake and absorption, as dysphagia, pain, and vomiting could be triggered [4]. In addition, the side effects of anticancer medication, including anorexia, early satiety, nausea, vomiting, oral and intestinal mucositis with dysphagia, diarrhoea, haemorrhoids, anal fissures, and alterations in smell and taste disturb not only the whole energy intake, but also the nutrients’ absorption, affecting negatively nutritional status. The poor mental health status of cancer patients is also able to influence their energy intake, as well [5].
Malnutrition in head and neck cancers is a common and serious concern, with dysphagia severely impairing patients’ nutritional status [6]. Malnutrition is also considered as a crucial risk factor for a low compliance to chemotherapy and radiotherapy and finally for the oncologic outcome [7,8,9]. Cancers of the oesophagus and the pharynx can impair feeding in patients, and lead to undernutrition [7,8,9]. Nutrition impact symptoms negatively influence cancer patients beyond the acute phase of cancer therapy [10,11]. These symptoms are linked with reduced nutrition and quality of life. Notably, 23.8-48.9% of patients with oral cancers are diagnosed with malnutrition [10,11], while the rates for oesophageal cancer patients reach 79% [9].
Nutritional assessment is important in order to prevent and manage malnutrition [12], whilst nutritional status acts as a prognostic factor for disease progression [13]. A substantial concern regarding malnutrition is under-diagnosis [14], in spite of the fact that nutritional status screening is recommended to be accomplished at diagnosis [12]. Moreover, body composition analysis can decrease the risk of treatment toxicity, shorter time to tumor progression, poorer outcomes of surgery, physical impairment, and shorter survival [15], while BMI alone cannot distinguish fat mass from fat-free mass and cannot consider weight loss [16].
In view of the above considerations, this scoping review aims to critically summarize and scrutinize the existing clinical evidence on the use of diverse nutritional assessment tools on the survival and disease progression of patients with oesophageal and pharyngeal cancers.
2. Methods
This is a scoping review that aims to map the literature concerning the impact of nutritional status in disease progression and prognosis in patients with oesophageal or pharyngeal cancers and provide an opportunity to identify key concepts, gaps in the research, and types and sources of evidence to inform practice, policymaking, and research on this topic. Peer-reviewed journal papers were included if they were: published between the periods of 2000 and 2023, written in English, involved only clinical human studies, and described a measure for burden of treatment, e.g., including single measurements, measuring and/or incorporating one or two dimensions of burden of treatment.
Quantitative, qualitative, and mixed-method studies were included to consider different aspects of measuring treatment burden. A comprehensive search of the existing international literature was carried out in the most accurate scientific databases, e.g., PubMed, Scopus, Web of Science, and Google Scholar, applying effective and characteristic keywords like nutrition, nutritional assessment, nutritional status, nutritional tools, cancer, oesophageal cancer, pharyngeal cancer, cancer progression, patients’ prognosis, survival, clinical studies, etc. The search was supplemented with the scanning of reference lists of relevant reviews and hand-searching key journals, commentaries, editorials, and abstracts in congress proceedings. The retrieved surveys were additionally comprehensively checked for related studies quoted in their text.
The search strategies were drafted by an experienced librarian and further refined through team discussion by all authors. The final search results were exported into EndNote, and duplicates were re-moved by a library technician [Constantinos Gryparis]. All authors acted as reviewers. To increase consistency among reviewers, all reviewers screened all the retrieved publications, discussed the results, and amended the screening and data extraction manual before beginning screening for this review. Six reviewers working in pairs sequentially evaluated the titles, abstracts, and then full text of all publications identified by our searches for potentially relevant publications. We resolved disagreements on study selection and data extraction by consensus and discussion with all the authors/reviewers, if needed.
A data charting form was jointly developed by two reviewers (S.K.P. and C.G.) to determine which variables to extract. The two reviewers independently charted the data, discussed the results, and continuously updated the data-charting form in an iterative process. Where we identified a systematic review, we counted the number of studies included in the review that potentially met our inclusion criteria and noted how many studies had been missed by our search. Inclusion criteria were any prospective, cross-sectional, descriptive, pilot, or case-report clinical studies conducted on Caucasian individuals. In vitro and in vivo animal studies were excluded. Papers were excluded if they did not fit into the conceptual framework of the study. Only studies assessing the impact of nutrition status on disease progression and prognosis in patients with oesophageal or pharyngeal cancers were included.
Clinical studies that included patients with simultaneously other types of cancer in other organs of the human body beyond oesophagus and pharynx were excluded. The findings were selected based on relevance, and the most relevant ones were chosen and mentioned below according to the PRISMA flow diagram depicted in Figure 1. We examined emerging evidence concerning whether a good nutritional status may ameliorate patients’ prognosis and disease symptomatology, slowing down simultaneously disease progression, to help map the literature on this specific topic that may inform future research and systematic reviews on this issue.
3. Results and Discussion
3.1. Oesophageal cancer
Oesophageal cancer is a disease with poor prognosis, due to the increased preva-lence of malnutrition and cachexia in patients with the disease [17], which is prevalent in patients with obesity, as well [18]. Although the prognostic significance of the nutri-tional status does not mean exclusion from treatment [19], the need for timely nutri-tional assessment is important, as interventions for the treatment of malnutrition can improve survival [20]. Several nutritional assessment tools have been used in studies, and shown prognostic potential [21,22]. Table 1 includes all clinical studies evaluating the use of the prognostic role of diverse nutritional assessment tools on the survival of patients with oesophageal carcinoma.
A plethora of recent surveys have investigated the prognostic importance of “Controlling Nutritional Status” (CONUT) scoring on oesophageal carcinoma and shown that CONUT score may be an independent prognosticator of overall and dis-ease-specific survival in patients undergone oesophagectomy [23]. More to the point, in a recent retrospective survey of 69 patients with advanced oesophageal carcinoma treated with immune checkpoint inhibitor, CONUT score was an independent prognosticator for overall survival and progression-free survival [24]. The retrospective survey of Hirahara et al. (2018) also confirmed that the CONUT scoring is an independent prognosticator for cancer-specific survival in patients aged < 70 years old that undergo curative surgery [25]. Further retrospective studies highlight that the CONUT score can predict malnutrition and act as a prognosticator of overall and dis-ease-specific survival in patients treated with surgery [26,27]. A retrospective study was performed on 352 patients undergone elective esophagectomy with lymphadenectomy for esophageal cancer, which were assigned to three groupings based on the CONUT assessment [26]. Malnourished patients exhibited a considerably elevated prevalence of any morbidity, serious morbidities, and surgical site infections. Hospitalization of malnourished patients was found substantially extended. In multivariate analysis, moderate or severe malnutrition was an independent risk factor for any morbidity and serious morbidities [26]. Another retrospective study by the same research group was conducted on 373 patients undergone 3-incision esophagectomy with 2- or 3-field lymphadenectomy due to esophageal carcinoma [27]. This study showed that malnourished patients underwent a considerably elevated incidence of reoperation and a greater tendency of lung morbidities. CONUT score was able to predict malnutrition and acted as a prognosticator of overall and disease-specific patients’ survival [27]. Regarding recurrence, a recent retrospective study using CONUT score, with a cut-off point of 3, found that patients underwent neoadjuvant immunochemotherapy with high CONUT were more likely to relapse, while those with a reduced CONUT scoring exhibited a favorable disease-free survival after one year [28]. Moreover, vessel invasion, postoperative pneumonia, advanced ypT, cTNM and ypTNM stage were substantially related to patients scoring high CONUT values [28].
Prognostic Nutritional Index (PNI) score has been applied in a few recent studies with oesophageal carcinoma patients. In fact, PNI was used in a study group of 337 patients, with those with a low PNI (<45) having shorter overall survival than those with high PNI score [29]. Interestingly, PNI was considerably related with tumor-infiltrating lymphocytes (TILs) state and CD8-positive cell count, supporting evidence that nutritional status and systemic immune competency could affect patients’ survival via local immune response [29]. A recent study on 407 patients who under-went curative oesophagectomy showed that low PNI < 48.33 was an independent prognosticator for overall survival, being also associated with high prevalence of postoperative complications. [30]. In a smaller study with 32 patients with oesophageal squamous cell carcinoma who experienced salvage oesophagectomy showed that PNI, with a cut-off point at 45, was an independent preoperative prognosticator for overall survival [31]. After adjustment for patients’ age, clinical response, and pre-operative PNI, yet PNI was not a prognosticator for disease-specific survival [31]. Nakatani et al. (2017) explored the prognostic significance of PNI in 66 patients under-gone neoadjuvant chemotherapy and applied as a cut-off point the PNI score of 45, like the aforementioned studies [32]. Preoperative PNI was recognized as an independent prognosticator for shorter overall and relapse-free survival, yet pre-chemotherapy PNI was not an independent predictor of overall and relapse-free survival [32]. In the sur-vey by Wang et al. (2018), PNI was identified as a prognosticator for overall survival, but not for progression-free survival, distant metastasis-free survival, or local regional recurrence-free survival [33]. Concerning patients at risk of malnutrition, the average hospitalization of nutritionally supported patients was significantly shorter, and the average hospitalization costs were lower than those without nutritional support [33].
Patient-Generated Subjective Global Assessment (PG-SGA) is another tool that has been explored in oesophageal carcinoma patients. Movahed at al. (2020) followed 71 newly diagnosed patients for one year. At 12 months, mortality was related with decreased BMI after chemo-radiotherapy, baseline PG-SGA score, weight decline, low BMI (<18.5 kg/m2) and decreased mid upper arm circumference (MUAC) [34]. Furthermore, Chen et al. (2021) found that PG-SGA had prognostic role on survival in 340 newly diagnosed patients with oesophageal squamous cell cancer at stages T2 to T4 or regional lymph node metastasis [35]. A high PG-SGA score (>3) at diagnosis, indicative of malnutrition, was correlated with a greater probability of presenting organ metastasis and shorter patients’ survival. In addition to this, survival after surgery was longer for well-nourished patients [34]. It is important to note that cut-off points may differ in different studies, which may confuse clinicians [34,36].
Song et al. (2017) followed 202 patients with unresectable locally advanced oesophageal carcinoma (stages 3 and 4) who were treated with definitive concurrent chemoradiotherapy. Nutrition Risk Screening (NRS)-2002 score with a cut-off point at ≥3 was used to assess malnutrition at treatment initiation [37]. NRS-2002 score was identified as an independent prognosticator for the response to chemoradiotherapy, overall patients’ survival and progression-free patients’ survival [37]. The study of Noh et al. (2022) with 274 patients (stages 1 to 3) undergone direct surgery for oesophageal squamous cell carcinoma, showed that after a median follow-up of 55 months, overall survival was lower and post-operative complications were more common in the group with an elevated NRS 2002 scoring [38]. NRS-2002 was also evaluated in the study by Wang et al. (2018) in 97 oesophageal cancer patients treated with chemoradiotherapy. Baseline NRS-2002 (cut-off point = 3) score was an independent prognosticator of overall survival, but not for progression-free survival, dis-tant metastasis-free survival, or local regional recurrence-free survival [39].
Cox et al. (2016) found that Nutritional Risk Index (NRI) less than 100 was a predictor of malnutrition in oesophageal carcinoma patients [20]. In fact, Clavier et al. (2014) studied the prognostic factors for survival and causes of therapy interruption after definitive chemoradiotherapy for oesophageal carcinoma [40]. Among other fac-tors, they examined the role of NRI in 143 patients with squamous cell carcinoma and adenocarcinoma of the oesophagus. NRI greater >97.5 and Performance Status (PS) of zero (PS=0) were independent prognosticators of 3-year and 5-year disease-free survival and median, 3-year and 5-year overall survival [40]. Geriatric Nutritional Risk Index (GNRI) has also been assessed and was substantially related with shorter overall survival and cancer-specific survival amongst esophageal squamous cell carcinoma patients, with the recent meta-analysis by Fan et al. (2022) determining that low GNRI may be correlated with shorter overall and cancer-specific patients’ survival [41].
Other surveys have investigated the impact of PS, weight loss and serum albumin levels as predictors of survival. Zemanova et al. (2012) in their retrospective study examined the influence of clinical and nutritional factors on overall survival and time to disease progression in 107 oesophageal carcinoma patients received neo-adjuvant chemoradiotherapy and undergone surgery [42]. Measures of PS, body weight changes prior to and across chemoradiotherapy, dysphagia, nutritional support, and serum albumin were included. Decreased PS, severe dysphagia, demand for nasogastric tube insertion, more than average pre-treatment weight decline, weight decrease above 5% across treatment, and serum albumin ≤35g/l prior to or next to chemoradiotherapy im-plied a poor prognosis [42]. Serum albumin concentrations, nasogastric tube insertion and pretreatment weight decline were independent prognosticators for overall patients’ survival, while serum albumin levels next to chemoradiotherapy and nasogastric tube insertion were identified as prognosticators for time to progression [42]. Additionally, Hamai et al. (2013) in their retrospective survey examined potential prognosticators in the management of locally advanced oesophageal carcinoma with adjacent organ invasion and investigated the outcomes in 74 patients [43]. Younger patients’ age (<60 years) and elevated pre-treatment hemoglobin (≥13 g/dl) were independent predictors of favorable therapeutic outcomes, and elevated pre-treatment se-rum albumin (≥3.5 g/dl) was an independent prognostic factor for longer survival [43]. Similarly, Di Fiore et al. (2007) documented that serum albumin > 35 g/L was the only independent predictive factor of complete treatment response, while BMI > 18 kg/m2, along with dysphagia Atkinson score < 2, dose of radiotherapy > 50 Grays and complete response to chemoradiotherapy were independent prognosticators of favorable patients’ survival [44].
In another study, conducted by Harada et al. (2015), the impact of sarcopenia on the survival of oesophageal squamous cell carcinoma patients followed surgical resection or definitive CRT was examined [45]. Skeletal muscle mass was measured utilizing computed tomography scans. Sarcopenia was not considerably related with overall patients’ survival. Nevertheless, in patients without lymph node invasion, sarcopenia was associated with worse prognosis, suggesting that it may function as a probable biomarker for recognizing patients to present an unfavorable outcome [45]. Zemanova et al. (2014) also evaluated the impact of nutritional, genetic, and inflammatory factors in the pathophysiology of squamous cell oesophageal carcinoma in 42 men, received a multimodal regimen of simultaneous neoadjuvant chemoradiotherapy, followed by surgery [46]. In univariate analysis, elevated serum adiponectin was associated with worse overall patients’ survival, while elevated serum albumin, and cholesterol were associated with favorable overall patients’ survival [46].
As far as short-term outcomes and complications are concerned, further studies have been undertaken. In 100 patients with oesophageal cancer, baseline PG-SGA score over 9 points was independently associated with radiation oesophagitis [47]. Regarding post-operative complications, studies have shown that greater body weight loss, low albumin levels and low GNRI were predictors for major complications [48], while high NRS-2002 score [38] and low PNI [30] were also associated with frequent postoperative complications. Furthermore, Hikage et al. (2019) retrospectively evaluated 141 oesophageal cancer patients who were treated with neoadjuvant chemotherapy post radical oesophagectomy and found that preoperative CONUT score could predict malnutrition 14 days after oesophagectomy [49]. Further studies have also highlighted the prognostic value of CONUT for short-term post-operative complications after oesophagectomy [26,50].
3.2. Pharyngeal cancer
Several nutritional assessment tools have been used to investigate the prognostic impact of nutritional status on pharyngeal cancers as described in Table 2. The recent retrospective study by Wu et al. (2022) highlighted the fact that several markers of nutritional status and assessment tools have prognostic value for pharyngeal cancers [51]. More to the point, BMI, hemoglobin, albumin, PNI, NRI and Hemoglobin, Albu-min, Lymphocyte, and Platelet (HALP) scores were of value in this clinical setting [51].
Low PNI was recognized as a significant predictor of shorter overall survival, organ metastasis-free survival, progression-free survival, and locoregional recurrence-free survival in patients with nasopharyngeal cancer [52], and a prognostic factor of survival and recurrence free survival in patients with oesophageal squamous cell carcinoma [53]. Other recent studies have agreed with these findings. Topkan et al. (2021) recently showed that low baseline PNI (cut-off point at 51) was an independent prognosticator for overall survival, cancer-specific survival, locoregional progression-free survival, organ metastasis-free survival, and progression-free survival in 154 patients with locoregionally advanced nasopharyngeal carcinoma receiving concurrent chemoradiotherapy [54]. The negative effect of the low PNI was also remained at 10-year time point [54]. Additionally, PNI < 51 was substantially related with greater rates of weight decrease >5% during the previous 6 months compared to PNI < 51 group [54]. Moreover, PNI was evaluated in the current survey by Küçükarda et al. (2022), in 107 non-metastatic nasopharyngeal cancer patients, who were assessed before and after treatment [55]. PNI at both time periods was an independent prognosticator for overall patients’ survival, while pre-treatment PNI with a cut-off point of ≤50.65 was associated with worse loco-regional recurrence-free survival, and organ metastasis-free survival [55]. Moreover, after chemoradiotherapy for advanced cancer (stage 3 and 4) of the oral cavity, oropharynx, and hypopharynx, low PNI was associated with toxicity and toxic death, as well as with T categorization and advanced tumor stage. Patients presenting decreased PNI were less probable to accept concurrent chemoradiotherapy, needed also more frequently tube feeding support [56]. Regarding hypopharyngeal squamous cell carcinoma, high PNI at a cut-off point of 52 was an independent prognosticator for better overall, progression-free, locoregional recurrence-free survival and distant metastasis-free survival, in 123 patients at all stages of the disease, of whom 16.3% were at stage 3 and 69.1% at stage 4 [57].
CNI, which takes into account BMI, typical body weight percentage, hemoglobin and albumin concentrations, and total lymphocyte count, was evaluated in 359 newly diagnosed nasopharyngeal carcinoma patients receiving intensity-modulated radiation therapy (IMRT), and it was shown that decreased CNI was an independent prognosticator of overall survival [58]. The CNI was relatively modest in patients with III-IV clinical tumor stage and those receiving induction chemotherapy plus simultaneous chemotherapy. After IMRT, lower CNI score was associated with poorer quality of life [58]. Similarly, in stage 3 and 4 elderly cancer patients with nasopharyngeal cancer, who underwent radiotherapy, CNI was used to assess the prognostic role of nutritional status, and it was found that CNI was an independent prognosticator for survival and disease-free survival [59]. In the same survey, PNI and NRI were also assessed with similar results [59].
Su et al. (2020) investigated the prognostic impact of modified Nutrition Index (m-NI) on treatment toxicity and survival in 187 nasopharyngeal cancer patients who had a normal nutrition before treatment. Severe nutritional impairment during IMRT, which was assessed as a reduction in m-NI score of ≥ 50%, was an independent prognosticator for overall patients’ survival and oral mucositis [60]. Similarly, the recent survey by Song et al. (2023) demonstrated that malnutrition before radiotherapy, assessed via m-NI, was a predictor of short-term clinical complications such as severe dysgeusia, oral mucositis, dysphagia, and xerostomia next to radiotherapy for nasopharyngeal cancer, which in turn worsen patients’ nutritional status [61]. Regarding overall survival, the prospective study by Hong et al. (2017) on 323 nasopharyngeal cancer patients undergone intensity-modulated radiotherapy indicated that the m-NI was a substantial prognosticator for 1-, 3-, and 5-year overall survival in this patient group [62].
Furthermore, NRS-2002 was evaluated by Peng et al. (2018) in nasopharyngeal carcinoma patients, utilizing a big-data intelligence database platform and detected 3232 patients [63]. Patients presenting NRS2002 ≤3 vs >3 exhibited considerably different 5-year disease-free survival, overall survival, organ metastasis-free survival and locoregional relapse-free survival [63]. This survey used a different cut-off point for the NRS-2002. The European Society for Clinical Nutrition and Metabolism (ESPEN) recommended ≥3 score to be the cut-off for nutritional impairment, not >3 [63]. Other tools that have been utilized are the Glasgow Prognostic Score (GPS) and the Neutrophil-Lymphocyte Ratio (NLR) in locally advanced hypopharyngeal squamous cell carcinoma patients undergone pharyngo-laryngo-cervical esophagectomy, reconstructed by jejunal graft [64]. Poor PS according to GPS, and high NLR (cut off point at ≥5) were recognized as independent prognosticators of poor survival, while elevated pre-operative GPS was a risk factor for post-operative complications [64].
Weight status (percentage ideal body weight) and albumin were evaluated in a group of 512 patients with nasopharyngeal carcinoma receiving radiotherapy [65]. Both parameters were independent prognosticators for overall patients’ survival, while pre-treatment body weight at <90% of the ideal body weight was correlated with worse overall survival and organ metastasis-free survival [65]. However, Bozec et al. (2015) failed to find significant relationships between nutritional status and clinical outcomes in locally advanced (stage 3 and 4) cancer patients, of whom 11,3% had lost significant weight (>10%) and 32% needed enteral nutrition [66]. Only WHO PS and minimum weight loss were significant independent prognostic factors for complications during radiotherapy [66]. The explanation for this finding may be the relatively low prevalence of malnutrition in the study group, as pre-treatment malnutrition rates in this patient group was 19-45% [67].
4. Conclusions
Malnutrition in cancer patients is one of the most prominent factors in the evolution and mortality of such patients and cancer cachexia significantly increases the risk of mortality. To reduce the incidence of malnutrition, it is strongly recommended to establish an effective and systematic nutritional intervention, which should be personalized according to the specific characteristics of cancer patients. For this purpose, validated and accurate nutritional assessment tools and specific indicators have been developed to determine the patient's condition. At this time, there are currently several nutritional assessment tools, which used independently of the type of cancer. This is a significant and remarkable gap of the international literatures since each type of cancer has different histopathological disease progression, and prognostic characteristics. Notably, this is very noticeable in our study on oesophageal and pharyngeal cancers where different nutritional assessment tools were used even in the case of only one type of cancer.
Regarding oesophageal cancer, nutritional status has been identified as a significant prognostic factor of survival, and short-term treatment complications. Several tools have been evaluated around the world, with CONUT, PNI, PG-SGA and NRS-2002 being more common in the literature, while albumin is also frequently evaluated regarding clinical outcomes. Recent meta-analyses have also indicated that sarcopenia may be used as a significant factor for worse survival [68], while GNRI and PNI can also be used as prognostic factors of survival in oesophageal squamous cell carcinoma [41,53].
As far as pharyngeal cancers are concerned, fewer studies are currently available. PNI has been evaluated and its significance as a potential factor for shorter overall patients’ survival, organ metastasis-free survival, progression-free survival, and locoregional recurrence-free has been highlighted. CNI has also been investigated with positive results, as well as NRS 2002 and GPS. Regarding weight status, most studies do agree that weight loss may be considered as a prognosticator for survival, which is necessary for nutritional support across the therapy.
It should be noticed that most studies are observational and retrospective, and are comprised mainly by men, with women being the minority of the study populations. In this aspect, recall bias should be taken into consideration, while causality effect cannot be supported. Hence, further prospective, large-scaled, well-designed clinical surveys that will examine the prognostic impact of nutritional status and studies that evaluate the impact of improving the nutritional status on survival and clinical outcomes are strongly recommended. Last but not least, the lack of studies that focus on female patients is of great importance, as gender differences may be present [69].
The currently available studies in these patient groups regarding the prognostic impact of nutritional status on disease progression and survival outcomes strongly highlight the significance of maintaining a good nutritional status and/or intervening, in order to support patients, and improve their nutritional status [70,71,72]. The nutritional assessment tools that have been utilized and evaluated are easy to perform and are currently used in the routine clinical setting. However, there is a strong demand to investigate which nutritional assessment tool is more suitable and effective for each cancer type separately, and thus future clinical studies are recommended to systematically focus on this direction.
Author Contributions
Conceptualization, M.T.; N.T.; and C.G.; methodology, E.P(Evmorfia Psara).; C.T.; and M.S.; formal analysis, S.K.P.; E.P. (Eleni Pavlidou); N.K.; investigation, E.P.(Evmorfia Psara); A.-L.P.; and M.M.; resources, C.T.; M.S.; E.P. (Eleni Pavlidou); A.S.; and M.M.; data curation, E.P. (Evmorfia Psara); S.K.P.; M.T.; and N.T.; writing—original draft preparation, E.P.(Evmorfia Psara); C.T.; and C.G.; writing—review and editing, C.G.; visualization, S.K.P.; M.T.; N.T.,; and C.G.; supervision, C.G.; project administration, C.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data of the study are available upon request to the corresponding author.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today. Lyon: International Agency for Research on Cancer; 2020. 20 December. Available online: https://gco.iarc.fr/today (accessed on December 2022).
- Dewys, W.D.; Begg, C.; Lavin, P.T.; Band, P.R.; Bennett, J.M.; Bertino, J.R.; Cohen, M.H.; Douglass, H.O.Jr.; Engstrom, P.F.; Ezdinli, E.Z.; et al. Prognostic effect of weight loss prior to chemotherapy in cancer patients. Eastern Cooperative Oncology Group. Am. J. Med. 1980, 69, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Argilés, J.M. Cancer-associated malnutrition. Eur. J. Oncol. Nurs. 2005, 9, S39–S50. [Google Scholar] [CrossRef] [PubMed]
- Laviano, A. , Preziosa, I.; Fanelli, F.R. Cancer and Nutritional Status. In Nutrition and Cancer, C. Shaw (Ed.): Nutrition and cancer. Wiley-Blackwell Publishing Ltd, Oxford 2011. [Google Scholar] [CrossRef]
- Santarpia, L., Contaldo; Pasanisi, F. Nutritional screening and early treatment of malnutrition in cancer patients. J. Cachexia Sarcopenia Muscle 2011, 2, 27–35. [Google Scholar] [CrossRef]
- Cristofaro, M.G.; Barca, I.; Ferragina, F.; Novembre, D.; Ferro, Y.; Pujia, R.; Montalcini, T. The health risks of dysphagia for patients with head and neck cancer: a multicentre prospective observational study. J. Transl. Med. 2021, 19, 472. [Google Scholar] [CrossRef] [PubMed]
- Martin-Harris, B.; McFarland, D.; Hill, E.G.; Strange, C.B.; Focht, K.L.; Wan, Z.; Blair, J.; McGrattan, K. Respiratory-swallow training in patients with head and neck cancer. Arch. Phys. Med. Rehabil. 2015, 96, 885–893. [Google Scholar] [CrossRef]
- Bressan, V.; Stevanin, S.; Bianchi, M.; Aleo, G.; Bagnasco, A.; Sasso, L. The effects of swallowing disorders, dysgeusia, oral mucositis and xerostomia on nutritional status, oral intake and weight loss in head and neck cancer patients: A systematic review. Cancer Treat. Rev. 2016, 45, 105–119. [Google Scholar] [CrossRef]
- Jordan, T.; Mastnak, D.M.; Palamar, N.; Kozjek, N.R. Nutritional Therapy for Patients with Esophageal Cancer. Nutr. Cancer 2018, 70, 23–29. [Google Scholar] [CrossRef]
- Bossi, P.; Delrio, P.; Mascheroni, A.; Zanetti, M. The Spectrum of Malnutrition/Cachexia/Sarcopenia in Oncology According to Different Cancer Types and Settings: A Narrative Review. Nutrients 2021, 13, 1980. [Google Scholar] [CrossRef]
- Bossi, P.; De Luca, R.; Ciani, O.; D'Angelo, E.; Caccialanza, R. Malnutrition management in oncology: An expert view on controversial issues and future perspectives. Front. Oncol. 2022, 12, 910770. [Google Scholar] [CrossRef]
- Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Fearon, K.; Hütterer, E.; Isenring, E.; Kaasa, S.; Krznaric, Z.; Laird, B, Larsson, M. ; Laviano, A.; Mühlebach, S.; Muscaritoli, M.; Oldervoll, L.; Ravasco, P.; Solheim, T.; Strasser, F.; de van der Schueren, M.; Preiser, J.C. ESPEN guidelines on nutrition in cancer patients. Clin. Nutr. 2017, 36, 11–48. [Google Scholar] [CrossRef]
- Mantzorou, M.; Koutelidakis, A.; Theocharis, S.; Giaginis, C. Clinical Value of Nutritional Status in Cancer: What is its Impact and how it Affects Disease Progression and Prognosis? Nutr. Cancer 2017, 69, 1151–1176. [Google Scholar] [CrossRef] [PubMed]
- Attar, A.; Malka, D.; Sabaté, J.M.; Bonnetain, F.; Lecomte, T.; Aparicio, T.; Locher, C.; Laharie, D.; Ezenfis, J.; Taieb, J. Malnutrition is high and underestimated during chemotherapy in gastrointestinal cancer: an AGEO prospective cross-sectional multicenter study. Nutr. Cancer 2012, 64, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.; Cushen, S.J.; Orsso, C.E.; Ryan, A.M. Sarcopenia and cachexia in the era of obesity: clinical and nutritional impact. Proc. Nutr. Soc. 2016, 75, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Ozorio, G.A.; Barão, K.; Forones, N.M. Cachexia Stage, Patient-Generated Subjective Global Assessment, Phase Angle, and Handgrip Strength in Patients with Gastrointestinal Cancer. Nutr. Cancer 2017, 69, 772–779. [Google Scholar] [CrossRef]
- Anandavadivelan, P. , Lagergren, P. Cachexia in patients with oesophageal cancer. Nat. Rev. Clin. Oncol. 2006, 13, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Ryan, A. M.; Rowley, S.P.; Healy, L.A.; Flood, P.M.; Ravi, N.; Reynolds, J.V. Post-oesophagectomy early enteral nutrition via a needle catheter jejunostomy: 8-year experience at a specialist unit. Clin. Nutr. 2006, 25, 386–393. [Google Scholar] [CrossRef]
- Grotenhuis, B.A.; Wijnhoven, B.P.; Grüne, F.; van Bommel, J.; Tilanus, H.W.; van Lanschot, J.J. Preoperative risk assessment and prevention of complications in patients with esophageal cancer. J. Surg. Oncol. 2010, 101, 270–278. [Google Scholar] [CrossRef]
- Cox, S.; Powell, C.; Carter, B.; Hurt, C.; Mukherjee, S.; Crosby, T.D. Role of nutritional status and intervention in oesophageal cancer treated with definitive chemoradiotherapy: outcomes from SCOPE1. Br. J. Cancer 2016, 115, 172–177. [Google Scholar] [CrossRef]
- Wang, P.Y.; Chen, X.K.; Liu, Q.; Xu, L.; Zhang, R.X.; Liu, X.B.; Li, Y. Application of four nutritional risk indexes in perioperative management for esophageal cancer patients. J. Cancer Res. Clin. Oncol. 2021, 147, 3099–3111. [Google Scholar] [CrossRef]
- Chen, M.F.; Hsieh, C.C.; Chen, P.T.; Lu, M.S. Role of Nutritional Status in the Treatment Outcome for Esophageal Squamous Cell Carcinoma. Nutrients 2021, 13, 2997. [Google Scholar] [CrossRef]
- Takagi, K.; Buettner, S.; Ijzermans, J.N.M.; Wijnhoven, B.P.L. Systematic Review on the Controlling Nutritional Status (CONUT) Score in Patients Undergoing Esophagectomy for Esophageal Cancer. Anticancer Res. 2020, 40, 5343–5349. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.; Cheng, Q.; Ma, Y.; Wu, C.; Zhang, X.; Ma, Q.; He, L.; Li, Q.; Tao, J. Prognostic Effect of the Controlling Nutritional Status Score in Patients With Esophageal Cancer Treated With Immune Checkpoint Inhibitor. J. Immunother. 2022, 45, 415–422. [Google Scholar] [CrossRef]
- Hirahara, N.; Matsubara, T.; Hayashi, H.; Takai, K.; Nakada, S.; Tajima, Y. Prognostic Importance of Controlling Nutritional Status in Patients Undergoing Curative Thoracoscopic Esophagectomy for Esophageal Cancer. Am. J. Ther. 2018, 25, e524–e532. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, N.; Baba, Y.; Shigaki, H.; Harada, K.; Iwatsuki, M.; Kurashige, J.; Sakamoto, Y.; Miyamoto, Y.; Ishimoto, T.; Kosumi, K.; et al. Preoperative Nutritional Assessment by Controlling Nutritional Status (CONUT) is Useful to estimate Postoperative Morbidity After Esophagectomy for Esophageal Cancer. World J. Surg. 2016, 40, 1910–1917. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, N.; Harada, K.; Baba, Y.; Kosumi, K.; Iwatsuki, M.; Kinoshita, K.; Nakamura, K.; Sakamoto, Y.; Miyamoto, Y.; Karashima, R.; et al. Preoperative controlling nutritional status (CONUT) is useful to estimate the prognosis after esophagectomy for esophageal cancer. Langenbecks Arch. Surg. 2017, 402, 333–341. [Google Scholar] [CrossRef]
- Feng, J.; Wang, L.; Yang, X.; Chen, Q.; Cheng, X. The usefulness of pretreatment controlling nutritional status score for predicting recurrence in patients with esophageal squamous cell carcinoma undergoing neoadjuvant immunochemotherapy: A real-world study. Front. Immunol. 2022, 13, 1015365. [Google Scholar] [CrossRef]
- Okadome, K.; Baba, Y.; Yagi, T.; Kiyozumi, Y.; Ishimoto, T.; Iwatsuki, M.; Miyamoto, Y.; Yoshida, N.; Watanabe, M.; Baba, H. Prognostic Nutritional Index, Tumor-infiltrating Lymphocytes, and Prognosis in Patients with Esophageal Cancer. Ann. Surg. 2020, 271, 693–700. [Google Scholar] [CrossRef]
- Qi, Q.; Song, Q.; Cheng, Y.; Wang, N. Prognostic Significance of Preoperative Prognostic Nutritional Index for Overall Survival and Postoperative Complications in Esophageal Cancer Patients. Cancer Manag. Res. 2021, 13, 8585–8597. [Google Scholar] [CrossRef]
- Sakai, M.; Sohda, M. ; Miyazaki, T.; Yoshida, T.; Kumakura, Y.; Honjo, H.; Hara, K.; Ozawa, D.; Suzuki, S.; Tanaka, N.; Yokobori, T.; Kuwano, H. Association of Preoperative Nutritional Status with Prognosis in Patients with Esophageal Cancer Undergoing Salvage Esophagectomy. Anticancer Res. 2018, 38, 933–938. [Google Scholar] [CrossRef]
- Nakatani, M.; Migita, K.; Matsumoto, S.; Wakatsuki, K.; Ito, M.; Nakade, H.; Kunishige, T.; Kitano, M.; Kanehiro, H. Prognostic significance of the prognostic nutritional index in esophageal cancer patients undergoing neoadjuvant chemotherapy. Dis. Esophagus. 2017, 30, 1–7. [Google Scholar] [CrossRef]
- Wang, R.; Cai, H.; Li, Y.; Chen, C.; Cui, Y. Impact Exerted by Nutritional Risk Screening on Clinical Outcome of Patients with Esophageal Cancer. Biomed. Res. Int. 2018, 2018, 7894084. [Google Scholar] [CrossRef] [PubMed]
- Movahed, S.; Norouzy, A.; Ghanbari-Motlagh, A.; Eslami, S.; Khadem-Rezaiyan, M.; Emadzadeh, M.; Nematy, M.; Ghayour-Mobarhan, M.; Varshoee Tabrizi, F.; Bozzetti, F.; Seilanian Toussi, M. Nutritional Status in Patients with Esophageal Cancer Receiving Chemoradiation and Assessing the Efficacy of Usual Care for Nutritional Managements. Asian Pac. J. Cancer Prev. 2020, 21, 2315–2323. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.B.; Liu, D.T.; Chen, Y.P. The Impact of Preoperative Nutritional Status on the Survival of Patients With Esophageal Squamous Cell Carcinoma. Front. Surg. 2021, 8, 752792. [Google Scholar] [CrossRef]
- Cao, Y.; Han, D.; Zhou, X.; Han, Y.; Zhang, Y.; Li, H. Effects of preoperative nutrition on postoperative outcomes in esophageal cancer: a systematic review and meta-analysis. Dis. Esophagus. 2022, 35, doab028. [Google Scholar] [CrossRef] [PubMed]
- Song, T.; Wan, Q.; Yu, W. ; Li, J.; Lu, S.; Xie, C.; Wang, H.; Fang, M. Pretreatment nutritional risk scores and performance status are prognostic factors in esophageal cancer patients treated with definitive chemoradiotherapy. Oncotarget 2017, 8, 98974–98984. [Google Scholar] [CrossRef]
- Noh, J.H.; Na, H.K.; Kim, Y.H.; Song, H.J.; Kim, H.R.; Choi, K.D.; Lee, G.H.; Jung, H.Y. Influence of Preoperative Nutritional Status on Patients Who Undergo Upfront Surgery for Esophageal Squamous Cell Carcinoma. Nutr. Cancer 2022, 74, 2910–2919. [Google Scholar] [CrossRef]
- Wang, J.; Yu, B.; Ye, Y.; Shen, J.; Ding, N.; Tang, H.; Xu, Y.; Song, L.; Zhu, Z.; Chen, Y.; Xie, S.; Chen, M. Predictive Value of Nutritional Risk Screening 2002 and Prognostic Nutritional Index for Esophageal Cancer Patients Undergoing Definitive Radiochemotherapy. Nutr. Cancer 2018, 70, 879–885. [Google Scholar] [CrossRef]
- Clavier, J.B.; Antoni, D.; Atlani, D.; Ben Abdelghani, M.; Schumacher, C.; Dufour, P.; Kurtz, J.E.; Noel, G. Baseline nutritional status is prognostic factor after definitive radiochemotherapy for esophageal cancer. Dis. Esophagus 2014, 27, 560–567. [Google Scholar] [CrossRef]
- Fan H, Ma W, Fu Y, Yi T, Tian J. Association of Geriatric Nutritional Risk Index with Survival Outcomes in Patients with Esophageal Squamous Cell Carcinoma: A Meta-Analysis. Nutr. Cancer 2022, 74, 2796–2802. [Google Scholar] [CrossRef]
- Zemanova, M.; Novak, F.; Vitek, P.; Pazdro, A.; Smejkal, M.; Pazdrova, G.; Petruzelka, L. Outcomes of patients with oesophageal cancer treated with preoperative chemoradiotherapy, followed by tumor resection: influence of nutritional factors. J. BUON 2012, 17, 310–316. [Google Scholar]
- Hamai, Y.; Hihara, J.; Emi, M.; Taomoto, J.; Aoki, Y.; Kishimoto, I.; Ibuki, Y.; Okada, M. Treatment outcomes and prognostic factors for thoracic esophageal cancer with clinical evidence of adjacent organ invasion. Anticancer Res. 2013, 33, 3495–3502. [Google Scholar] [PubMed]
- Di Fiore, F.; Lecleire, S.; Pop, D.; Rigal, O.; Hamidou, H.; Paillot, B.; Ducrotté, P.; Lerebours, E.; Michel, P. Baseline nutritional status is predictive of response to treatment and survival in patients treated by definitive chemoradiotherapy for a locally advanced esophageal cancer. Am. J. Gastroenterol. 2007, 102, 2557–2563. [Google Scholar] [CrossRef] [PubMed]
- Harada, K.; Ida, S.; Baba, Y.; Ishimoto, T.; Kosumi, K.; Tokunaga, R.; Izumi, D.; Ohuchi, M.; Nakamura, K.; Kiyozumi, Y.; Imamura, Y.; Iwatsuki, M.; Iwagami, S.; Miyamoto, Y.; Sakamoto, Y.; Yoshida, N.; Watanabe, M.; Baba, H. Prognostic and clinical impact of sarcopenia in esophageal squamous cell carcinoma. Dis. Esophagus 2016, 29, 627–633. [Google Scholar] [CrossRef]
- Zemanová, M.; Staňková, B.; Ušiakova, Z.; Tvrzická, E.; Pazdro, A.; Petruželka, L.; Zeman, M. Serum adiponectin relates to shortened overall survival in men with squamous cell esophageal cancer treated with preoperative concurrent chemoradiotherapy: a pilot study. Med. Sci. Monit. 2014, 20, 2351–2357. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Zhang, W.; Zhang, T.; Chen, X.; Zhao, J.; Zeng, Y.; Chen, Y.; Wei, X.; Lei, T.; Wang, P.; et al. Baseline nutritional status could be a predictor for radiation esophagitis in esophageal cancer patients undergoing radiotherapy. Ann. Transl. Med. 2020, 8, 1148. [Google Scholar] [CrossRef] [PubMed]
- Lidoriki, I.; Mylonas, K.S.; Syllaios, A.; Vergadis, C.; Stratigopoulou, P.; Marinos, G.; Mastoraki, A.; Karavokyros, I.; Schizas, D. The Impact of Nutritional and Functional Status on Postoperative Outcomes following Esophageal Cancer Surgery. Nutr. Cancer 2022, 74, 2846–2858. [Google Scholar] [CrossRef]
- Hikage, M.; Taniyama, Y.; Sakurai, T.; Sato, C.; Takaya, K.; Okamoto, H.; Konno, T.; Ujiie, N.; Naitoh, T.; Unno, M.; Kamei, T. The Influence of the Perioperative Nutritional Status on the Survival Outcomes for Esophageal Cancer Patients with Neoadjuvant Chemotherapy. Ann. Surg. Oncol. 2019, 26, 4744–4753. [Google Scholar] [CrossRef]
- Horinouchi, T.; Yoshida, N.; Harada, K.; Eto, K.; Sawayama, H.; Iwatsuki, M.; Iwagami, S.; Baba, Y.; Miyamoto, Y.; Baba, H. A retrospective study of preoperative malnutrition based on the Controlling Nutritional Status score as an associated marker for short-term outcomes after open and minimally invasive esophagectomy for esophageal cancer. Langenbecks Arch. Surg. 2022, 407, 3367–3375. [Google Scholar] [CrossRef]
- Wu, C.Y.; Lin, Y.H.; Lo, W.C.; Cheng, P.C.; Hsu, W.L.; Chen, Y.C.; Shueng, P.W.; Hsieh, C.H.; Liao, L.J. Nutritional status at diagnosis is prognostic for pharyngeal cancer patients: a retrospective study. Eur. Arch. Otorhinolaryngol. 2022, 279, 3671–3678. [Google Scholar] [CrossRef]
- Tu, X.; Ren, J.; Zhao, Y. Prognostic value of prognostic nutritional index in nasopharyngeal carcinoma: A meta-analysis containing 4511 patients. Oral Oncol. 2020, 110, 104991. [Google Scholar] [CrossRef]
- Li, P.; Wang, X.; Lai, Y.; Zhou, K.; Tang, Y.; Che, G. The prognostic value of pre-treatment prognostic nutritional index in esophageal squamous cell carcinoma: A meta-analysis. Medicine (Baltimore) 2019, 98, e15280. [Google Scholar] [CrossRef] [PubMed]
- Topkan, E.; Yucel Ekici, N.; Ozdemir, Y.; Besen, A.A.; Mertsoylu, H.; Sezer, A.; Selek, U. Baseline Low Prognostic Nutritional Index Predicts Poor Survival in Locally Advanced Nasopharyngeal Carcinomas Treated With Radical Concurrent Chemoradiotherapy. Ear. Nose Throat J. 2021, 100, NP69–NP76. [Google Scholar] [CrossRef]
- Küçükarda, A.; Erdoğan, B.; Gökyer, A.; Sayın, S.; Gökmen, İ.; Özcan, E.; Hacıoğlu, M.B.; Uzunoğlu, S.; Çiçin, İ. Prognostic nutritional index and its dynamics after curative treatment are independent prognostic factors on survival in non-metastatic nasopharyngeal carcinoma. Support Care Cancer 2022, 30, 2131–2139. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.H.; Hsieh, J.C.; Yeh, K.Y.; Chen, E.Y.; Yang, S.W.; Huang, J.S.; Lai, C.H.; Wu, T.H.; Huang, Y.M.; Chang, Y.S.; Chou, W.C.; Wang, C.H. Prognostic nutritional index relevance in chemoradiotherapy for advanced oral cavity, oropharyngeal and hypopharyngeal cancer. Asia Pac. J. Clin. Nutr. 2018, 27, 996–1001. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.L.; Oei, R.W.; Kong, F.F.; Du, C.R.; Zhai, R.P.; Ji, Q.H.; Hu, C.S.; Ying, H.M. The prognostic value of preoperative prognostic nutritional index in patients with hypopharyngeal squamous cell carcinoma: a retrospective study. J. Transl. Med. 2018, 16, 12. [Google Scholar] [CrossRef]
- Deng, J.; He, Y.; Sun, X.S.; Li, J.M.; Xin, M.Z.; Li, W.Q.; Li, Z.X.; Nie, S.; Wang, C.; Li, Y.Z.; et al. Mai, H.Q. Construction of a comprehensive nutritional index and its correlation with quality of life and survival in patients with nasopharyngeal carcinoma undergoing IMRT: A prospective study. Oral Oncol. 2019, 98, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Duan, Y.Y.; Deng, J.; Su, D.F.; Li, W.Q.; Han, Y.; Li, Z.X.; Huan, X.Z.; Zhu, S.H.; Yang, Q.L.; Hu, W.; Xin, M.Z.; Tang, L.Q.; Mai, H.Q.; Fan, Y.Y.; He, Y. Construction of a comprehensive nutritional index and comparison of its prognostic performance with the PNI and NRI for survival in older patients with nasopharyngeal carcinoma: a retrospective study. Support Care Cancer 2021, 29, 5371–5381. [Google Scholar] [CrossRef]
- Su, L.; Lin, Q.; Li, R.; Hua, Y.; Zhang, H.; Song, X.; Ye, J.; Zhang, W.; Hong, J. Prognostic value of nutritional impairment on treatment-related toxicity and survival in patients with nasopharyngeal carcinoma taking normal nutrition before radiotherapy. Head Neck 2020, 42, 3580–3589. [Google Scholar] [CrossRef]
- Song, X.; Su, L.; Lin, Q.; Liu, S.; Zhang, W.; Hong, J. Effect of nutritional status before radiotherapy on radiation-induced acute toxicities in patients with nasopharyngeal carcinoma. Head Neck 2023, 45, 620–628. [Google Scholar] [CrossRef]
- Hong, J.S.; Hua, Y.J.; Su, L.; Zhang, H.R.; Lv, W.L.; Chen, X.Y.; Tian, J.; Zhang, W.J. Modified-Nutrition Index is a Significant Prognostic Factor for the Overall Survival of the Nasopharyngeal Carcinoma Patients who Undergo Intensity-modulated Radiotherapy. Nutr. Cancer 2017, 69, 1011–1018. [Google Scholar] [CrossRef]
- Peng, H, Chen, B. B.; Tang, L.L.; Chen, L.; Li, W.F.; Zhang, Y.; Mao, Y,P,; Sun, Y.; Liu, L.Z.; Tian, L.; Guo, Y.; Ma, J. Prognostic value of nutritional risk screening 2002 scale in nasopharyngeal carcinoma: A large-scale cohort study. Cancer Sci. 2018, 109, 1909–1919. [Google Scholar] [CrossRef] [PubMed]
- Ikeguchi, M. Glasgow prognostic score and neutrophil-lymphocyte ratio are good prognostic indicators after radical neck dissection for advanced squamous cell carcinoma in the hypopharynx. Langenbecks Arch. Surg. 2016, 401, 861–866. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Gao, J.; Liu, Z.G.; Tao, Y.L.; Xu, B.Q.; Tu, Z.W.; Zhang, X.P.; Zeng, M.S.; Xia, Y.F. Influence of pretreatment ideal body weight percentile and albumin on prognosis of nasopharyngeal carcinoma: Long-term outcomes of 512 patients from a single institution. Head Neck 2014, 36, 660–666. [Google Scholar] [CrossRef]
- Bozec, A.; Benezery, K.; Chamorey, E, Ettaiche, M. ; Vandersteen, C.; Dassonville, O.; Poissonnet, G.; Riss, J.C.; Hannoun-Lévi, J.M.; Chand, M.E.; Leysalle, A.; Saada, E.; Sudaka, A.; Haudebourg, J.; Hebert, C.; Falewee, M.N.; Demard, F.; Santini, J.; Peyrade F. Nutritional status and feeding-tube placement in patients with locally advanced hypopharyngeal cancer included in an induction chemotherapy-based larynx preservation program. Eur. Arch. Otorhinolaryngol. 2016, 273, 2681–2687. [Google Scholar] [CrossRef] [PubMed]
- Jager-Wittenaar H, Dijkstra PU, Vissink A, van Oort RP, van der Laan BF, Roodenburg JL. Malnutrition in patients treated for oral or oropharyngeal cancer--prevalence and relationship with oral symptoms: an explorative study. Support Care Cancer 2011, 19, 1675–1683. [Google Scholar] [CrossRef]
- Jogiat, U.M.; Sasewich, H.; Turner, S.R.; Baracos, V.; Eurich, D.T.; Filafilo, H.; Bédard, E.L.R. Sarcopenia Determined by Skeletal Muscle Index Predicts Overall Survival, Disease-free Survival, and Postoperative Complications in Resectable Esophageal Cancer: A Systematic Review and Meta-analysis. Ann. Surg. 2022, 276, e311–e318. [Google Scholar] [CrossRef]
- Leoncini, E.; Vukovic, V.; Cadoni, G.; Giraldi, L.; Pastorino, R.; Arzani, D.; Petrelli, L.; Wünsch-Filho, V.; Toporcov, T.N.; Moyses, R.A.; et al. Tumour stage and gender predict recurrence and second primary malignancies in head and neck cancer: a multicentre study within the INHANCE consortium. Eur. J. Epidemiol. 2018, 33, 1205–1218. [Google Scholar] [CrossRef]
- Ravasco, P.; Monteiro Grillo, I.; Camilo, M. Cancer wasting and quality of life react to early individualized nutritional counselling! Clin Nutr. 2007, 26, 7–15. [Google Scholar] [CrossRef]
- Ravasco, P. Nutrition in Cancer Patients. J. Clin. Med. 2019, 8, 1211. [Google Scholar] [CrossRef]
- Cao, J.; Xu, H.; Li, W.; Guo, Z.; Lin, Y.; Shi, Y.; Hu, W.; Ba, Y.; Li, S.; Li, Z.; et al. Investigation on Nutrition Status and Clinical Outcome of Common Cancers (INSCOC) Group, Chinese Society of Nutritional Oncology. Nutritional assessment and risk factors associated to malnutrition in patients with esophageal cancer. Curr. Probl. Cancer 2021, 45, 100638. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flow diagram.
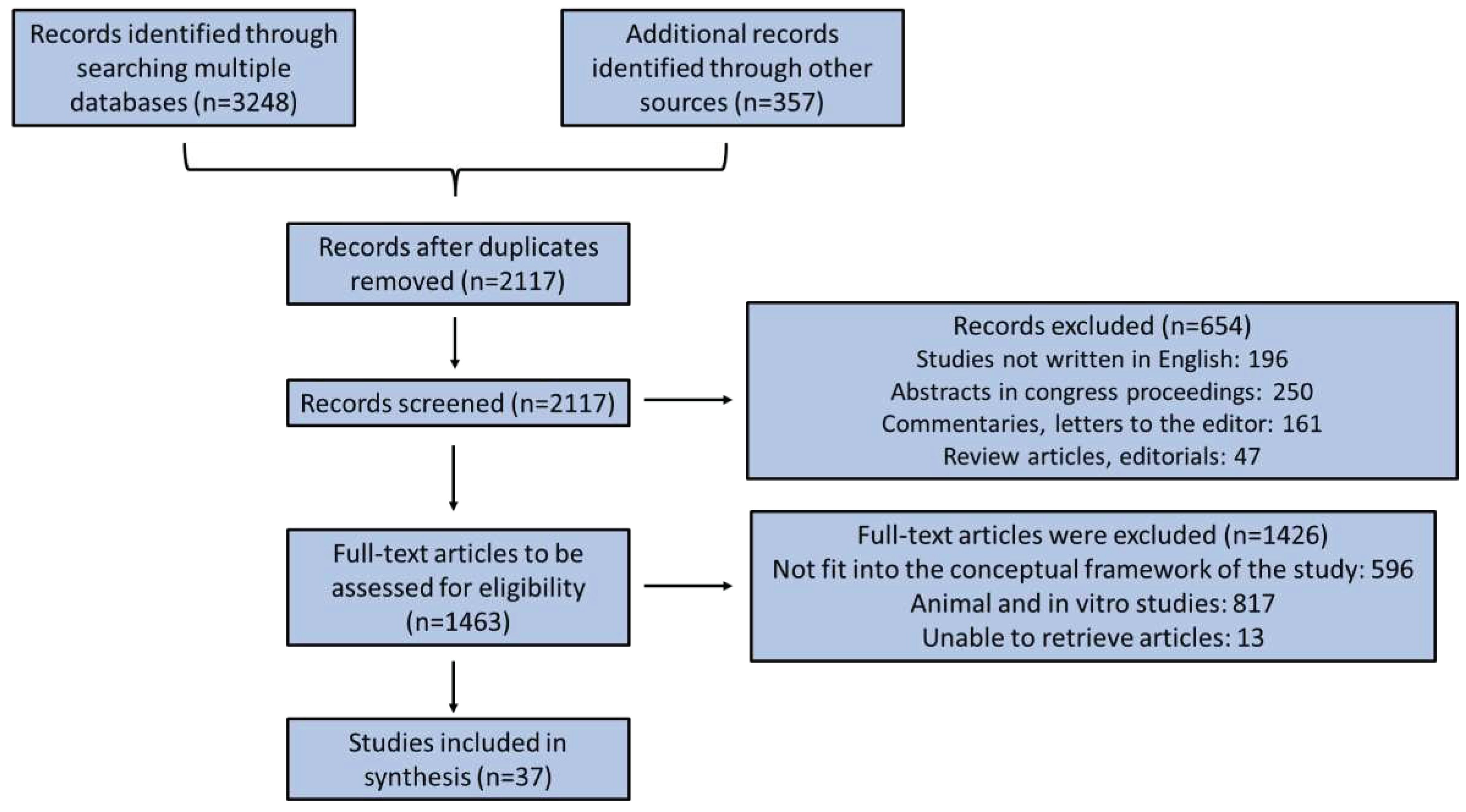

Table 1.
Studies regarding oesophageal carcinoma and the prognostic role of nutritional status.
| Number of patients and cancer type | Assessment tool | Results | Reference |
|---|---|---|---|
| 258 patients randomly assigned to definitive chemoradiotherapy (dCRT) +/- cetuximab | NRI | Baseline NRI<100 predicted worse overall survival. | Cox 2016 [20] |
| Retrospective study on 69 advanced oesophageal carcinoma patients, aged 18-80 years, treated with Immune Checkpoint Inhibitor (ICI) | CONUT | CONUT score (cut-off point =1) was an independent prognosticator for overall survival and progression-free survival in patients undergoing ICI. | Chang 2022 [24] |
| Retrospective study of 148 patients with oesophageal squamous cell carcinoma who underwent potentially curative esophagectomy (complete resection) | CONUT | CONUT score was an independent prognosticator for cancer-specific survival in patients aged < 70 years old. | Hirahara 2018 [25] |
| Retrospective study of 352 patients who underwent elective oesophagectomy with lymphadenectomy for oesophageal carcinoma | CONUT | Malnourished patients had a substantial greater prevalence of any morbidity, serious morbidities, and surgical site infection. Hospitalization of malnourished patients was considerably longer. Moderate or severe malnutrition was an independent risk factor for any morbidity and serious morbidities. | Yoshida 2016 [26] |
| Retrospective study of 373 patients who underwent three-incision oesophagectomy with 2- or 3-field lymphadenectomy for oesophageal carcinoma | CONUT | CONUT score was able to predict malnutrition and acted as a prognosticator of overall and disease-specific survival in patients undergone surgery. | Yoshida 2017 [27] |
| 216 patients with oesophageal squamous cell carcinoma, receiving neoadjuvant immunochemotherapy | CONUT | ↑CONUT score (cut-off point=3): ↑risk of relapse. CONUT score: independent prognosticator for disease-free survival at one year. |
Feng 2022 [28] |
| Database of 337 curatively resected oesophageal cancers | PNI | ↓PNI led to considerably poorer overall survival in both univariate and multivariate analysis. | Okadome 2020 [29] |
| Retrospective study of 407 oesophageal carcinoma patients who underwent esophagectomy | PNI | Multivariable analysis identified PNI as an independent prognosticator for overall survival and post-operative complications. | Qi 2021 [30] |
| retrospective study with 32 patients with oesophageal squamous cell carcinoma who underwent salvage oesophagectomy | PNI | PNI (cut-off point=45) was an independent prognostic preoperative factor for overall survival after adjustment for age, clinical response, and preoperative PNI. PNI was not a prognosticator for disease-specific survival. |
Sakai 2018 [31] |
| 66 squamous cell oesophageal carcinoma patients undergoing neoadjuvant chemotherapy | PNI | The mean pre-treatment and preoperative PNI were 50.2 ± 5.7 and 48.1 ± 4.7, respectively. PNI decreased following chemotherapy in 66.7% patients. Pre-chemotherapy PNI and preoperative PNI were considerably correlated with the overall survival and relapse-free survival rates. In multivariate analysis, only preoperative PNI was an independent prognosticator for worse overall and relapse-free survival. |
Nakatani 2017 [33] |
| 97 esophageal carcinoma patients earlier cured with definitive chemo-radiotherapy (CRT) | PNI | ↑Baseline PNI or PNI at the end of CRT (≥45) was related with better 2-year overall survival. PNI was a prognosticator for overall, but not for progression-free survival, organ metastasis-free survival, or local regional recurrence-free survival post CRT. | Wang 2018 [33] |
| 71 newly diagnosed patients followed for 1 year | PG-SGA | 1 year mortality was considerably associated with reduced BMI after CRT, primary PG-SGA score, weight loss, BMI<18.5, MUAC, physical performance, living in rural or urban areas, and addiction. | Movahed 2020 [34] |
| Retrospective study on 340 esophageal-squamous cell carcinoma patients who completed curative treatment | PG-SGA | Well-nourished patients benefited from surgery. Malnutrition was associated with worse prognosis, regarding metastases and survival. |
Chen 2021 [35] |
| 202 patients with unresectable locally advanced oesophageal carcinoma (stages 3 and 4) who were treated with definitive concurrent chemoradiotherapy | NRS-2002 | NRS-2002 score (cut-off point ≥3) (was an independent prognosticator for the response to chemoradiotherapy, overall survival and progression-free survival. | Song 2017 [37] |
| 274 patients (stages 1 to 3, median age 63 years) undergone direct surgery for oesophageal squamous cell carcinoma, with a median follow-up of 55 months | NRS-2002 | Overall survival rates were shorter in the NRS 2002 group with elevated scores. A high NRS 2002 score was related with more frequent postoperative complications. | Noh 2022 [38] |
| 97 oesophageal carcinoma patients treated with CRT | NRS-2002 | NRS-2002 score 3 at baseline was associated with better 2-year overall survival than NRS-2002 score ≥4. NRS-2002 score at baseline was an independent risk factor for prognosis. |
Wang 2018 [39] |
| Retrospective study with 143 patients with oesophageal squamous cell carcinoma and adenocarcinoma followed for 20.8 months | NRI | Overall Survival: NRI > 97.5 and PS = 0 were independent predictive factors. Disease-free survival: NRI > 97.5 and PS = 0 were independent predictive factors. |
Clavier 2014 [40] |
| Meta-analysis of 8 retrospective studies with 1460 oesophageal squamous cell carcinoma patients | GNRI | Low GNRI was correlated with shorter overall and cancer-specific survival. | Fan 2022 [41] |
| Retrospective study on 107 esophageal carcinoma patients cured with neoadjuvant CRT and surgery | Weight status, Performance statusAlbumin | Low PS, serious dysphagia, above-average pre-treatment weight decline, weight decrease >5% throughout CRT, and serum albumin ≤ 35 g/l prior to or next to CRT implied shorter survival times. Serum albumin concentrations, nasogastric tube insertion and pretreatment body weight decline were independent prognosticators for overall survival. Serum albumin concentrations, along with nasogastric tube insertion after CRT was prognostic factor for time to progression. |
Zemanova 2012 [42] |
| Retrospective study on 74 patients with locally advanced esophageal carcinoma with adjacent organ invasion | AlbuminandHemoglobin | Younger age (<60 years) and hemoglobin ≥13 g/dl were independent predictors of favorable treatment outcome.Pre-treatment higher serum albumin (≥3.5 g/dl) was an independent favorable predictor of patients’ survival. | Hamai 2013 [43] |
| Retrospective study on 105 non-metastatic patients with a locally advanced oesophageal carcinoma cured with definitive CRT | Albumin | Serum albumin > 35 g/L was the only independent predictive factor of complete therapy response. Independent prognostic factors of survival were BMI > 18 Kg/m2, dysphagia Atkinson score <2, dose of RT > 50 Grays and CR to CRT were independent prognosticators of favorable patients’ survival. |
Di Fiore 2007 [44] |
| Retrospective study on 325 oesophageal squamous cell carcinoma patients (256 surgical and 69 dCRT cases) | Sarcopenia | Sarcopenia substantially lowered the overall survival of patients without lymph node metastasis, but not in patients presenting lymph involvement. | Harada 2015 [45] |
| Retrospective study on 42 patients, treated with a multimodal regimen of simultaneous neoadjuvant CRT, followed by surgery. | AdiponectinSerum albumin, and Cholesterol | In univariate analysis, elevated serum adiponectin was linked with poorer overall survival, while elevated serum albumin, and cholesterol were associated with favorable overall survival. In multivariate analysis, only a tendency for negative serum adiponectin relationship with the overall survival was noted. | Zemanova 2014 [46] |
| Retrospective study on 100 patients with oesophageal carcinoma cured with definitive chemoradiotherapy, preoperative chemoradiation and definitive radiotherapy | PG-SGABMI%Weight loss in 3 months Albumin Hemoglobin CRP GPS | PG-SGA score ≥9 was recognized as an independent predictor of radiation oesophagitis. | Dong 2020 [47] |
| 70 patients with oesophageal and gastroesophageal junction carcinoma who underwent oesophagectomy | GNRIAlbuminMuscle mass%weight loss | Albumin and GNRI were decreased in patients developing severe complications compared to patients without postoperative complications. Major complications were related with ↑%weight loss and with ↓ handgrip strength. Albumin and poor muscle mass were considerably correlated with anastomotic leakage occurrence. |
Lidoriki 2022 [48] |
| Retrospective study on 141 oesophageal carcinoma patients undergone neoadjuvant chemotherapy after radical oesophagectomy | CONUTPNI | In multivariate analysis, malnutrition 14 days after surgery according to CONUT and ↓PNI before surgery were identified as independent prognosticators of overall patients’ survival. | Hikage 2019 [49] |
| c674 patients who underwent three-incision oesophagectomy for oesophageal carcinoma | CONUT | Malnutrition according to CONUT was an independent risk factor for severe, respiratory, and cardiovascular morbidities after surgical operation. | Horinouchi 2022 [50] |
Table 2.
Studies regarding pharyngeal cancers and the prognostic role of nutritional status.
| Number of patients and cancer type | Assessment tool | Results | Author, date |
|---|---|---|---|
| 319 pharyngeal cancer patients with nasopharyngeal carcinoma, oropharyngeal carcinoma and hypopharyngeal carcinoma | BMI, hemoglobin, albumin, PNI, NRI, HALP | HALP score was an independent factor for overall survival after adjusting for sex, age, tumor site, clinical stage, and BMI. PNI was the most important independent factor for overall and cancer-specific survival. |
Wu 2022 [51] |
| Meta-analysis of 10 studies with 4511 patients with nasopharyngeal carcinoma | PNI | Patients with decreased PNI exhibited a worse overall, distant metastasis-free, progression-free and locoregional recurrence-free survival. Subgroup analysis: ↓ PNI was a significant prognostic factor for overall and distant metastasis-free survival. |
Tu 2020 [52] |
| 154 patients presenting locoregionally advanced nasopharyngeal cancer treated with concurrent chemoradiotherapy | PNI | ↓ baseline PNI (cut-off point=51) is an independent prognosticator for overall, cancer-specific, locoregional progression-free, organ metastasis-free, and progression-free survival. | Topkan 2021 [54] |
| 107 non-metastatic nasopharyngeal carcinoma patients | PNI | Pre- and post-treatment PNI were independent predictors for overall survival. | Küçükarda 2022 [55] |
| 143 patients presenting stage III, IVA, and IVB pharyngeal cancers who were treated with concurrent chemoradiotherapy | PNI | Patients with ↓ PNI had higher likelihoods of grade 3/4 hematological toxicities, sepsis and toxic death. Patients with ↓ PNI were less probable to tolerate concurrent chemoradiotherapy, even when they treated with a considerably lower dosage of cisplatin, showing a decreased completion rate of planned radiotherapy, or a longer overall radiotherapy treatment time. |
Chang 2018 [56] |
| 123 hypopharyngeal squamous cell carcinoma patients treated with radical surgery | PNI | ↑ preoperative PNI was an independent prognosticator for better overall, progression-free, locoregional recurrence-free and organ metastasis-free survival. | Ye 2018 [57] |
| 359 newly diagnosed nasopharyngeal cancer patients undergoing intensity-modulated radiation therapy | CNI | CNI decreased after therapy. CNI was an independent prognosticator of overall survival. |
Deng 2019 [58] |
| Retrospective study with 309 older nasopharyngeal carcinoma patients | CNI | CNI was an independent prognosticator of overall and disease-free survival. Kaplan-Meier analysis indicated that reduced CNI was correlated with unfavorable overall and disease-free survival. |
Duan 2021 [59] |
| 187 nasopharyngeal cancer patients who had a normal nutrition before treatment | modified Nutrition Index (m-NI) | Severe nutritional impairment, assessed as a reduction in m-NI score ≥50%, was an independent prognosticator for overall survival and an independent risk factor for grade ≥2 oral mucositis. | Su 2020 [60] |
| 228 nasopharyngeal cancer patients with NPC treated with intensity-modulated radiotherapy | modified Nutrition Index |
m-NI ≤6 was a risk factor for xerostomia, oral mucositis, dysgeusia and dysphagia. Total score of radiation-induced acute toxicities of malnourished patients was considerably greater compared to that of patients with normal nutrition. |
Song 2023 [61] |
| 323 patients with nasopharyngeal carcinoma undergoing intensity-modulated radiotherapy | modified Nutrition Index |
The 1-, 3-, and 5-year overall survival rates between malnutrition and normal nutrition groups assessed by m-NI were 93.0% vs. 96.9%, 76.4% vs. 82.8%, and 61.8% vs. 77.1%, respectively. Regression analysis indicated that m-NI was an independent prognosticator for overall survival. |
Hong 2017 [62] |
| 3232 nasopharyngeal carcinoma patients from big-data database | NRS-2002 | NRS2002 ≤3 vs >3 had significantly different 5-year disease-free, overall, distant metastasis-free and locoregional relapse-free survival. | Peng 2018 [63] |
| 59 patients presenting clinical stage III and IV hypopharyngeal squamous cell carcinoma who underwent pharyngo-laryngo-cervical esophagectomy with definitive tracheostomy followed by free jejunal graft reconstruction. | GPSNLR | ↑ GPS (1 or 2) and ↑NLR (≥5) were independent unfavorable prognosticators for 5-year overall survival. | Ikeguchi 2016 [64] |
| Prospective survey on 512 patients with nasopharyngeal carcinoma undergone radical RT | Weight status (ideal body weight, IBW)Albumin | Prior to radiotherapy, IBW% <90% was associated with shorter overall and organ metastasis-free survival. Albumin ≤43.0 g/L was related to shorter overall and metastasis-free survival. |
Li 2014 [65] |
| 53 patients presenting locally advanced hypopharyngeal carcinoma (stage 3 and 4) assigned to an induction chemotherapy (ICT)-based larynx preservation program without prophylactic feeding-tube placement | Weight loss | Maximum weight loss was considerably correlated with a greater probability of enteral tube feeding during treatment and a higher likelihood of complications during radiotherapy. | Bozec 2016 [66] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



