
Submitted:
02 July 2023
Posted:
03 July 2023
You are already at the latest version
Abstract
(1) Background: Treatment of male stress incontinence in patients with prostate cancer treated with radical prostatectomy and adjuvant pelvic radiation is a therapeutic challenge. The efficacy and safety of the adjustable trans-obturator male system (ATOMS) in these patients is not well established, despite the general belief that outcomes are worse than in patients without radiation. (2) Methods: Retrospective multicenter study evaluating patients treated with silicone-covered scrotal port (SSP) ATOMS implant after radical prostatectomy and radiotherapy in nine different institutions between 2016 and 2022. The primary endpoint was dry patient rate, defined as pad-test ≤20 mL/day. The secondary endpoints were complication rate (defined using Clavien-Dindo classification), device removal and self-perceived satisfaction using the Patient Global Impression of Improvement (PGI-I) scale. Wilcoxon rank sum test, Fisher’s exact test and logistic regression were performed using stepwise method with a 0.15 entry and 0.1 stay criteria. (3) Results: 223 patients fulfilled criteria for inclusion, 12 (5.4%) had received salvage prostatectomy after radiation and 27 (12.1%) previous devices for stress incontinence. After ATOMS adjustment, 95 patients (42.6%) were dry and 36 (16.1%) had complications of any grade (grade I, n=20; grade II, n=11; grade III, n=5) during the first 3 months postoperatively. At a mean 36 ± 21 months follow-up the device was explanted in 26 (11.7%) patients. Regarding self-perceived satisfaction with the implant, 105 of 125 patients (84%) considered themselves satisfied (PGI-I 1 to 3). In univariate analysis dryness was associated to younger age (p=.06), primary prostatectomy (p=.08), no previous incontinence surgery (p=.02), absence of overactive bladder symptoms (p=.04), absence of bladder neck stricture (p=.001), no need of surgical revision (p=.008) and lower baseline incontinence severity (p=.0003). Multivariate analysis identified absence of surgical revision (p=.018), absence of bladder neck stricture (p=.05), primary prostatectomy (p=.07) and baseline incontinence severity (p<.0001) were independent predictors of dryness. A logistic regression model was proposed and internally validated. (4) Conclusions: ATOMS is an efficacious and safe alternative to treat male incontinence after radical prostatectomy and adjuvant radiotherapy. Factors predictive of dryness are identified in this complex scenario to allow better patient selection.
Keywords:
Adjustable Trans-Obturator Male System
; Post-prostatectomy Incontinence
; Adjuvant Radiotherapy
; Outcomes
; Satisfaction
1. Introduction
Radical prostatectomy has been the most commonly used treatment option for patients with intermediate and high-risk clinically localized prostate cancer [1]. However, despite refined surgical technique and patient selection a significant number of patients will need salvage therapy. Adjuvant radiotherapy following radical prostatectomy is frequently used in patients with adverse features such as pT3 stage, positive surgical margins or detectable PSA after prostatectomy [2,3,4]. The combination of prostatectomy plus radiation has a negative functional effect both on erection and on continence recovery [5].
Adjuvant radiotherapy may cause significant urinary and rectal toxicity, especially if high dose radiation is used [6]. Acute inflammatory disorders tend to be transitory, but late adverse effects tend to be more serious and include urinary incontinence caused by fibrotic contracted bladder and/or sphincteric damage [7]. The urethra, rhabdosphincter and or bladder neck may suffer alterations leading to impaired tissue elasticity, stricture formation and fibrotic changes with reduction of urethral mobility and consequent damage on urinary continence. A prospective study confirmed adjuvant external radiation after radical prostatectomy at a dose of 60 Gy resulted in an additional 6 % of cases with urinary incontinence compared to prostate cancer under surveillance [8]. What is more, prostate cancer surgery or transurethral resection of the prostate (TURP) after radiation increase the risk of incontinence up to five-fold [9,10].
Surgical procedures to correct persistent stress urinary incontinence after prostate cancer surgery can be more challenging when performed on irradiated tissues than on naïve ones [11]. There is also a general belief that previous irradiation compromises the effectiveness of different incontinence devices, including male slings and the Artificial Urinary Sphincter (AUS) [12,13,14].
The Master trial showed that AUS and slings offer similar rates of incontinence [15]. Although only fixed slings were used as comparator in the trial, adjustable devices like the Adjustable Trans-Obturator Male System (ATOMS) are increasingly used for the surgical correction of moderate-to-severe incontinence [16,17]. The purpose of the present study is to evaluate the effectiveness and safety of ATOMS (A.M.I. GmbH, Feldkirch, Austria) in patients with prostate cancer treated with both radical prostatectomy and radiotherapy. We also aim to describe factors that identify the population with better outcomes in this presumably unfavorable scenario, complication rate and self-perceived satisfaction with the silicone-covered scrotal port (SSP) ATOMS.
2. Materials and Methods
2.1. Study Population
A retrospective multicenter study was undertaken to evaluate the effectiveness, safety and self-reported satisfaction in patients with stress incontinence after combined radical prostatectomy and radiotherapy intervened with SSP-ATOMS between 2016 and 2021 in eleven university hospitals from Europe and Canada. The study was approved by Institutional Review Board. All patients included had persistent bothersome SUI for more than a year after radical prostatectomy refractory to pelvic floor exercises. In all cases pelvic radiotherapy and radical prostatectomy were performed before ATOMS implant and minimum follow-up after ATOMS implant was 3 months.
Bladder neck contracture was not exclusion criterium but stable urethral patency with a 17 Ch cystoscope was required. Additional local treatments of prostate cancer, severity of incontinence and patient age were not limiting factors for inclusion. The study was derived from current clinical practice. The indication for ATOMS was made by physician with the informed consent of the patient in every case.
The surgical technique for ATOMS placement followed the original description [18,19]. A 14Ch Foley catheter was placed and delicate urethral dissection without splitting bulbospongiosus muscle was performed. Careful hemostasis was always performed and drainage was not placed. When necessary, postoperative adjustment was performed in the office starting 2–3 weeks after the implantation by percutaneous injection of physiological sodium chloride solution through the SSP membrane and thereafter when required at intervals of 4 weeks until either dryness was achieved or maximum filling capacity of the system was reached.
2.2. Study Endpoints
Effectiveness and safety of SSP-ATOMS in patients with stress incontinence after prostatectomy and adjuvant pelvic radiotherapy was evaluated. The primary endpoint was dry patient rate, defined as no urine leakage or use of a single security pad with a pad-test ≤ 20 mL/day. The secondary endpoints were complication rate defined as Clavien-Dindo classification within the first three months after surgery [20], device removal rate and self-perceived satisfaction using the Patient Global Impression of Improvement (PGI-I) scale [21].
2.3. Variables Evaluated
Data analyzed included patient age at the time of ATOMS implant, time of prostatectomy, adjuvant radiation of salvage prostatectomy, additional local treatments before prostatectomy (TUR-P) or before radiotherapy (brachytherapy), former history of bladder neck stricture, intraoperative and postoperative complications, continence outcomes and self-reported satisfaction with the procedure. Patients with a 24-h pad-test ≤ 20 mL/day were considered dry. Continence was evaluated baseline before ATOMS placement and postoperatively once device adjustment was considered complete. Incontinence severity was defined according to the number of pads/day (PPD) as mild (1-2 PPD), moderate (3-5 PPD) and severe (6 or more PPD).
Pain was evaluated at discharge by the patient as a visual analogue scale (0 to 10). The number and severity of complications was registered according to Clavien-Dindo classification within the first 3 months after the implant. Late complications including device surgical revision and device removal during follow-up were also evaluated. The self-assessed PGI-I scale specified: 1 “very much better than before”; 2 “much better”; 3 “slightly better”; 4 “same”; 5 “worse”; 6 “much worse” and 7 “very much worse”. For comparison the results were pooled as 1-3 (at least better than before) vs the rest. No patient was lost to follow-up.
2.4. Statistical Analysis
Statistics were calculated as the median values, interquartile range (IQR), minimum and maximum for continuous variables, and as the frequency and percent for categorical data. Differences were calculated by the Wilcoxon test for continuous variables and the Fisher exact test for categorical variables. A p value < 0.05 was considered significant. Logistic regression was performed using a stepwise model (entry 0.15 and stay criterium 0.1) to evaluate independent variables determinant of dryness after device adjustment. The area under receiver-operating characteristic (ROC) curve for the selected model and different combinations of predictive factors was calculated. The statistical analysis was developed using Statistical Analysis System 9.3 (SAS Institute Inc., Cary, NY, USA).
3. Results
Two hundred and twenty-three consecutive patients with primary ATOMS implant for male stress incontinence after combined treatment of prostate cancer with radical prostatectomy and adjuvant radiation were included in the study. Table 1 summarizes clinical data. Median follow-up after ATOMS implant was 30 (IQR 23, range 3-96) months.
3.1. Continence and satisfaction outcomes according to incontinence severity baseline
Table 2 reveals postoperative continence and satisfaction data for the total series analyzed and also after stratification according to incontinence severity. Mean change, both in PPD and in pad-test, is expressed for the total series and for each incontinence severity group. The proportion of dry patients is inversely related to the severity of baseline incontinence (p<.0001). On the other hand, the change in PPD and in daily pad-test increases according to severity of baseline incontinence (each, p<.0001) and also the number of postoperative adjustments needed (p<.0001). Noticeably, there is not an association between baseline incontinence and self-reported satisfaction (p=.67), possibly because the proportion of patients that rate their results as better than before is very high (84% in the total series with self-reported satisfaction data).
3.2. Comparison of effectiveness between baseline and after adjustment data
Regarding our primary outcome 42.6% of the patients included in the study (95 of 223 cases) achieved dryness. Comparative distribution of incontinence severity before ATOMS implant and adjustment revealed that 36.8% of the patients (82 cases) used 1-2 pads after after adjustment, 18.4% (41 cases) used 3-5 PPD, and only 2.2% (5 cases) used ≥6 PPD (compared to baseline; Bowker simmetry test, p<.0001). Globally, 20.6% of the patients remain moderate or severe incontinence after adjustment (Figure 1).
Mean 24-h pad-count changed from 4.8 ± 2.3 (range 1-12) PPD baseline to 1.4 ± 1.6 (range 0-10) after adjustment (sign-rank test, p<.0001). Mean 24-h pad-test changed from 630 ± 386 (range 75-2000) mL baseline to 120 ± 203 (range 0-1500) mL after adjustment (sign-rank test, p<.0001) (Figure 2).
3.3. Postoperative and late complications
Intraoperative complications occurred in 2 patients (.9%), both severe intraoperative bleeding. Mean visual analogue scale for pain (from 0 to ten) was evaluated in 102 patients (45.7%) at the time of hospital discharge, with a mean ± SD of 2.2 ± 1.8 (range 0-7).
Postoperative complications within 90 days after surgery presented in 36 (16.1%) cases, one with two different complications. According to Clavien-Dindo system, 20 (9%) were grade I, 11 (4.9%) grade II and 5 (2.2%) grade III. In order of frequency the 37 complications were pain in 14 (6.3%); urinary retention, 8 (3.6%); scrotal hematoma and wound infection, 3 each (1.4%); device infection, wound dehiscence and paresthesia, 2 each (.9%); and urgency, gout and port displacement needing reposition, 1 each (.4%).
At a mean 36 ± 21 (range 3-86) months of follow-up surgical revision was performed in 29 cases (13%) and device was explanted in 26 (11.7%). The reasons for revision were persistent incontinence in 10 (4.5%); scrotal port skin erosion and pain, 6 each (2.7%); device infection, 4 (1.8%); port displacement needing reposition, 2 (.9%); and wound dehiscence, 1 (.5%).
3.4. Self-perceived satisfaction
Postoperative self-perceived satisfaction using the Patient Global Impression of Improvement (PGI-I) scale was registered in 125 patients (56%). Mean PGI-I score after adjustment compared to before ATOMS was 2.2 ± 1.2 (range 1-5). The proportion of patients with each PGI-I score is represented in Figure 3. Patients with at least better perception than before (PGI-I from 1 to 3) was registered in 84% of the cases evaluated with this tool.
3.5. Logistic regression analysis for factors predictive of dryness
Univariate analysis of factors associated with dryness (no leakage or one security PPD with ≤ 20 mL) after ATOMS adjustment were: patient age at the time of implant (unfavourable for older age; p=.06), the sequence between prostatectomy and radiation (unfavorable for salvage prostatectomy; p=.08), no previous incontinence surgery (p=.02), absence of overactive bladder symptoms baseline (p=.04), absence of bladder neck stricture (p=.001), no need of surgical revision (p=.008) and lower baseline incontinence severity (p=.0003) (Table 3).
Multivariate analysis identified that an absence of surgical revision (p=.018), absence of bladder neck stricture (p=.05), primary prostatectomy (p=.07) and baseline incontinence severity (p<.0001) were independent predictors of dryness (Table 3).
A logistic regression model for the prediction of ATOMS success (i.e.; 24-h pad-test ≥ 20 mL after ATOMS adjustment) in this population was built (Figure 4). The area under the curve for this predictive model was 79%. The model was internally validated by boootstrapping with 74.5 (95% CI 74.2-74.8) % apparent performance and 9.4 (95% CI 9.2-9.5) % expected optimism.
3.6. Nomogram to predict dryness after ATOMS adjustment
A nomogram to facilitate the prediction of dryness in patients treated with ATOMS after radical prostatectomy and radiation is proposed (Figure 5).
4. Discussion
The impact of the association of pelvic radiotherapy with radical prostatectomy on male continence after prostate cancer treatment is tremendous. According to data from the National Health and Nutrition Examination Surveys (NHANES) incontinence rate presented in 23% of men who underwent radical prostatectomy, 12% of those treated with radiotherapy and in 52% of men treated with the combination of them [22].
On the one hand, when first local treatment is prostatectomy, the use of adjuvant or salvage radiotherapy severely affects continence recovery after surgery, but the toxicity profile of immediate postoperative radiation or delayed salvage radiotherapy could be different. Clinicians are prone to postpone the use of radiotherapy to maximize continence recovery, but this could have an impact on therapeutic reduced efficacy [23,24]. The optimal radiation dose delivered after prostatectomy and fractionation could also affect continence recovery [25]. On the other hand, salvage prostatectomy after failed radiation can provide local control of disease but with 25-79% of the patients being incontinent [26].
Initially a very interesting success rate was reported with the retrourethral transobturator fixed sling in selected patients after radical prostatectomy and adjuvant radiotherapy [27]. However, soon later caution was advised in recommending a fixed sling in patients with a history of pelvic irradiation [12]. More recently severely compromised long-term functional outcomes and patient satisfaction were confirmed [28,29]. A recent systematic review and meta-analysis concluded that adjustable slings might lead to higher objective cure rates than fixed ones, but randomized controlled trials with long-term follow-up and the same definition for continence are needed [30].
Several multicenter studies identified pelvic irradiation is a factor that negatively affects the results of ATOMS [31,32,33,34,35]. Also, a systematic review and meta-analysis confirmed that the proportion of irradiated patients included in the different studies available affected reported dryness rate, thus giving a source of heterogeneity [36]. In as much, a prospective observational study confirmed that the main factors that predict development of postoperative complications after ATOMS implant were previous radiotherapy and surgery for urethral stricture [37]. However, radiation does not compromise the high self-reported satisfaction with the ATOMS [38]. Therefore, although expected outcomes with ATOMS after radiation can be compromised, the device is still an option for the correction of male stress incontinence in patients with prostate cancer treated with prostatectomy and adjuvant radiation.
This belief is partly supported by the observation that in no case reported to date the ventral compression of the ATOMS has produced urethral erosion or urethral atrophy; complications that typically occur after the circumferential periurethral placement of AUS [39]. This observation makes ATOMS device especially attractive for patients with a fragile urethra due to previously failed AUS or failed retrobulbar sling [40,41] and also for patients previously treated for urethral stricture or bladder neck contracture [42], provided of course that some residual sphincter function remains. Conversely, the risk of urethral erosion with increased surgical revision and device explant was confirmed in several studies on patients implanted AUS after radiotherapy [43,44]. Radiation and prior urethroplasty also were confirmed independent risk factors for earlier time to erosion with an AUS [45]. Mainly for this reason, the role and outcomes of AUS after pelvic irradiation remain controversial. Some series did not evidence different outcomes [46,47,48], although other studies confirmed higher risk of surgical revision and device explant [43,44]. Finally, several multicenter studies confirmed that pelvic irradiation adversely affects AUS survival for increased and earlier urethral erosion leading to device explant [11,49].
Radiation causes a variety of tissue alterations that include vascular changes, fibrosis, cellular depletions and inflammation [50]. Histopathological examination of radiated tissue demonstrated vascular loss and increased scarring in the membranous urethra and in the bladder neck, changes that may also facilitate stricture formation, thus causing confusion of the deleterious factors involved in continence status [51]. In fact, we have confirmed that in radiated patients, bladder neck stricture is a negative predictor of ATOMS results. Similarly, when evaluating the role of ATOMS in patients with previously treated urethral stricture or bladder neck contracture we identified radiation was also a confounding factor [42]. Despite the high risk of problems in the irradiated male patients with urethral fragility the AUS still remains the most frequently used option; however, the ATOMS could be an alternative to consider, especially in patients with failed previous AUS and residual sphincteric function [40,41]. In fact, recent analysis confirmed the long-term durability in the efficacy of ATOMS after radiation with 62.5% social continence after 5 years mean follow-up [52].
Overactive bladder (OAB) symptoms in irradiated patients may also be a crucial issue to evaluate postoperative efficacy of the device. There is no data to suggest that ATOMS contributes itself to development of de novo OAB; however, that did present in 5% of the cases in this series. In fact, a positive correlation between previous radiotherapy and postoperative OAB was proposed [53]. In the univariate analysis we performed lack of OAB symptoms were associated to dryness in the population evaluated, but this was not an independent factor in multivariate analysis. The same happened with the absence of bladder neck stricture and older patient age.
We confirmed that the timing between radiotherapy and radical prostatectomy has an independent impact on the results of ATOMS, with worse efficacy in patients treated first with radiation and later with salvage prostatectomy. This is a relatively infrequent situation nowadays as the favored combination of treatments is early salvage treatment would because it offers the opportunity to spare many men radiotherapy and its associated side-effects [4,5]. However, due to the characteristics of the database we used we were not able to address very important items regarding the mode of radiation, including the time between surgery and radiation, total dose and fractionation. All these factors contribute to the prediction of continence recovery [24,25,55], and could also have an influence on the success rate of ATOMS in these patients and we are sorry to recognize that they remain unstudied. Similarly, the approach used for radical prostatectomy is another missing variable, despite there is no previous report to alert it might have an influence on the results of ATOMS implant.
Also, the study is limited by the absence of a comparison group. In fact, we could not answer the really important question whether combined prostatectomy and radiation implies worse results after ATOMS implant and adjustment, compared to the outcomes of patients treated with radical prostatectomy alone. A study based on a larger population of patients and using propensity score matching to compare groups will serve to settle the enigma whether ATOMS performs equally or worse in patients with or w/o radiation. In this sense, we do not know either whether the security profile is impacted or not. The description of complications, revision rate and explant rate we evidenced is totally in line with that of the general population of patients with ATOMS at a similar mean follow-up [33,37,55]. Also, the reasons for surgical revision we detected in this series is very much like those in the general population [39]. As far as we know, there is no other publication centering on the description of results with ATOMS in patients with adjuvant radiation exclusively. Despite the limitations acknowledged the findings presented are encouraging to furtherly analyze the issue in multicenter studies with larger number of patients and better control of confounding variables.
In summary, total continence was achieved in 42.6% of the patients treated with adjuvant radiotherapy (65.6 % for mild incontinence, 48.3% for moderate and 24% for severe) and 84% of them self-reported as satisfied compared to their situation baseline. The logistic regression analysis we performed served to identify the variables necessary to foresee the effectiveness of ATOMS in this population. Baseline incontinence severity considering the pad-test is the most determinant variable, with patients leaking up to 5 PPS (mild and moderate incontinence) performing better. The second factor limiting efficacy is the need for surgical revision during follow-up. Pain, scrotal skin erosion and device infection are complications that may lead to surgical revision, performed in 13% of the cases at a mean 3 years follow-up. Additional predictive factors at the limit of statistical significance are bladder neck stricture and salvage prostatectomy performed after failed radiation. The nomogram built for the prediction of dryness can be a useful tool to counsel a patient in the decision to receive an ATOMS implant after prostatectomy and radiotherapy.
5. Conclusions
ATOMS can be used to correct or improve male stress incontinence in patients with a history of prostate cancer treated with the combination of prostatectomy and radiotherapy. Efficacy and safety data with this approach are in consonance with data reported from the general population, and mainly depend on the degree of baseline incontinence. Patient satisfaction with the device is also high, regardless of baseline incontinence severity. ATOMS is a very interesting option for reconstructive and functional urologists facing complex cases of male incontinence. Our experience can be useful to counsel patients with prostate cancer treated with surgery plus radiation.
Author Contributions
Conceptualization, J.C.A., A.G., C.G-E., S.S., F.Q., A.R., A.G., F.E.M., F.C. and K.R.; investigation, J.C.A., A.G., C.G-E., S.S., F.Q., A.R., A.G., F.E.M., F.C. and K.R.; data curation, J.C.A., C.T., A.G., C.G-E., S.S., F.Q., J.S., R.G., A.R., A.G., F.E.M., T.A.L., F.C. and K.R.; statistical analysis, J.C.A., C.T. and J.S.; writing—original draft preparation, J.C.A. and C.T.; writing—review and editing, J.C.A., A.G., C.G-E., S.S., F.Q., A.R., A.G., F.E.M., F.C. and K.R. All authors have read and agreed to the published version of the manuscript.
Funding
Electronic case report forms and statistical analysis were supported by Presurgy (Las Rozas, Madrid) and A.M.I. (Feldkirch, Austria). The study had no other specific funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Hospital Universitario de Getafe (A08/17).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Full data will be available upon reasonable request to corresponding author.
Acknowledgments
The authors acknowledge statistician Juan F. Dorado (PeRTICA S.L.) for statistical analysis and methodological support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chen, J.; Oromendia, C.; Halpern, J.A.; Ballman, K.V. National trends in management of localized prostate cancer: A population based analysis 2004-2013. Prostate 2018, 78, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Ganswindt, U.; Stenzl, A.; Bamberg, M.; Belka, C. Adjuvant radiotherapy for patients with locally advanced prostate cancer - a new standard? Eur. Urol. 2008, 54, 528–542. [Google Scholar] [CrossRef] [PubMed]
- Ghia, A.J.; Shrieve, D.C.; Tward, J.D. Adjuvant Radiotherapy Use and Patterns of Care Analysis for Margin-positive Prostate Adenocarcinoma with Extracapsular Extension: Postprostatectomy Adjuvant Radiotherapy: A SEER Analysis. Urology 2010, 76, 1169–1174. [Google Scholar] [CrossRef] [PubMed]
- Vale, C.L.; Fisher, D.; Kneebone, A.; Parker, C.; Pearse, M.; Richaud, P.; Sargos, P.; Sydes, M.R.; Brawley, C.; Brihoum, M.; et al. Adjuvant or early salvage radiotherapy for the treatment of localised and locally advanced prostate cancer: a prospectively planned systematic review and meta-analysis of aggregate data. Lancet 2020, 396, 1422–1431. [Google Scholar] [CrossRef] [PubMed]
- Huelster, H.L.; Laviana, A.A.; Joyce, D.D.; Huang, L.-C.; Zhao, Z.; Koyama, T.; Hoffman, K.E.; Conwill, R.; Goodman, M.; Hamilton, A.S.; et al. Radiotherapy after radical prostatectomy: Effect of timing of postprostatectomy radiation on functional outcomes. Urol. Oncol. Semin. Orig. Investig. 2020, 38, 930.e23–930.e32. [Google Scholar] [CrossRef]
- Schick, U.; Latorzeff, I.; Sargos, P. Postoperative radiotherapy in prostate cancer: Dose and volumes. Cancer Radiother. 2021, 25, 674–678. [Google Scholar] [CrossRef]
- Grise, P.; Thurman, S. Urinary Incontinence following Treatment of Localized Prostate Cancer. Cancer Control. 2001, 8, 532–539. [Google Scholar] [CrossRef]
- Van Cangh, P.J.; Richard, F.; Lorge, F.; Castille, Y.; Moxhon, A.; Opsomer, R.; De Visscher, L.; Wese, F.X.; Scaillet, P. Adjuvant radiation therapy does not cause urinary incontinence after radical prostatectomy: results of a prospective randomized study. J. Urol. 1998, 159, 164–166. [Google Scholar] [CrossRef]
- Pontes, J.E.; Montie, J.; Klein, E.; Huben, R. Salvage surgery for radiation failure in prostate cancer. Cancer 1993, 71, 976–980. [Google Scholar] [CrossRef]
- Liu, M.; Pickles, T.; Berthelet, E.; Agranovich, A.; Kwan, W.; Tyldesley, S.; McKenzie, M.; Keyes, M.; Morris, J.; Pai, H.; et al. Urinary incontinence in prostate cancer patients treated with external beam radiotherapy. Radiother. Oncol. 2005, 74, 197–201. [Google Scholar] [CrossRef]
- Mamane, J.; Sanchez, S.; Lellouch, A.G.; Gaillard, V.; Poussot, B.; Tricard, T.; Saussine, C.; Brierre, T.; Game, X.; Beraud, F.; et al. Impact of radiation therapy on artificial urinary sphincter implantation in male patients: A multicenter study. Neurourol. Urodynamics 2021, 41, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Torrey, R.; Rajeshuni, N.; Ruel, N.; Muldrew, S.; Chan, K. Radiation History Affects Continence Outcomes After AdVance Transobturator Sling Placement in Patients With Post-prostatectomy Incontinence. Urology 2013, 82, 713–717. [Google Scholar] [CrossRef] [PubMed]
- Greenwell, T.; Guillaumier, S.; Solomon, E.; Jenks, J.; Pakzad, M.; Hamid, R.; Ockrim, J.; Shah, J. Radiotherapy is associated with reduced continence outcomes following implantation of the artificial urinary sphincter in men with post-radical prostatectomy incontinence. Urol. Ann. 2017, 9, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Choi, D.; Hong, J.H.; Kim, C.-S.; Ahn, H.; Choo, M.-S. Factors contributing to treatment outcomes of post-prostatectomy incontinence surgery for the selection of the proper surgical procedure for individual patients: A single-center experience. Neurourol. Urodynamics 2018, 37, 1978–1987. [Google Scholar] [CrossRef]
- Abrams, P.; Constable, L.D.; Cooper, D.; MacLennan, G.; Drake, M.J.; Harding, C.; Mundy, A.; McCormack, K.; McDonald, A.; Norrie, J.; et al. Outcomes of a Noninferiority Randomised Controlled Trial of Surgery for Men with Urodynamic Stress Incontinence After Prostate Surgery (MASTER). Eur. Urol. 2021, 79, 812–823. [Google Scholar] [CrossRef]
- Dorado, J.F.; Angulo, J.C. Refined Nomogram Incorporating Standing Cough Test Improves Prediction of Adjustable Trans-Obturator Male System (ATOMS) Success to Treat Post-Prostatectomy Male Stress Incontinence. J. Pers. Med. 2022, 12, 94. [Google Scholar] [CrossRef]
- Téllez, C.; Szczesniewski, J.; Virseda-Chamorro, M.; Arance, I.; Angulo, J.C. Update on Adjustable Trans-Obturator Male System (ATOMS) for Male Incontinence after Prostate Cancer Surgery. Curr. Oncol. 2023, 30, 4153–4165. [Google Scholar] [CrossRef]
- Seweryn, J.; Bauer, W.; Ponholzer, A.; Schramek, P. Initial Experience and Results With a New Adjustable Transobturator Male System for the Treatment of Stress Urinary Incontinence. J. Urol. 2012, 187, 956–961. [Google Scholar] [CrossRef]
- Angulo, J.C.; Arance, I.; Esquinas, C.; Dorado, J.F.; Marcelino, J.P.; Martins, F.E. Outcome Measures of Adjustable Transobturator Male System with Pre-attached Scrotal Port for Male Stress Urinary Incontinence After Radical Prostatectomy: A Prospective Study. Adv. Ther. 2017, 34, 1173–1183. [Google Scholar] [CrossRef]
- International Surgical Outcomes Study (ISOS) group; Abbott, T. E.F.; E Greaves, K.; Patel, A.; Pearse, R.M.; Beattie, S.; Clavien, P.-A.; Demartines, N.; A Fleisher, L.; Grocott, M.; et al. Prospective observational cohort study on grading the severity of postoperative complications in global surgery research. Br. J. Surg. 2019, 106, e73–e80. [Google Scholar] [CrossRef]
- Bjelic-Radisic, V.; Ulrich, D.; Hinterholzer, S.; Reinstadler, E.; Geiss, I.; Aigmueller, T.; Tamussino, K.; Greimel, E.; Trutnovsky, G.; Austrian Urogynecology Working Group. Psychometric properties and validation of two global impression questionnaires (PGI-S, PGI-I) for stress incontinence in a German-speaking female population. Neurourol. Urodyn. 2018, 37, 1365–1371. [Google Scholar] [CrossRef]
- Daugherty, M.; Chelluri, R.; Bratslavsky, G.; Byler, T. Are we underestimating the rates of incontinence after prostate cancer treatment? Results from NHANES. Int. Urol. Nephrol. 2017, 49, 1715–1721. [Google Scholar] [CrossRef]
- Suardi, N.; Gallina, A.; Lista, G.; Gandaglia, G.; Abdollah, F.; Capitanio, U.; Dell’oglio, P.; Nini, A.; Salonia, A.; Montorsi, F.; et al. Impact of Adjuvant Radiation Therapy on Urinary Continence Recovery After Radical Prostatectomy. Eur. Urol. 2013, 65, 546–551. [Google Scholar] [CrossRef]
- Munoz, F.; Sanguineti, G.; Bresolin, A.; Cante, D.; Vavassori, V.; Waskiewicz, J.M.; Girelli, G.; Avuzzi, B.; Garibaldi, E.; Faiella, A.; et al. Predictors of Patient-Reported Incontinence at Adjuvant/Salvage Radiotherapy after Prostatectomy: Impact of Time between Surgery and Radiotherapy. Cancers 2021, 13, 3243. [Google Scholar] [CrossRef]
- Bresolin, A.; Garibaldi, E.; Faiella, A.; Cante, D.; Vavassori, V.; Waskiewicz, J.M.; Girelli, G.; Avuzzi, B.; Villa, E.; Magli, A.; et al. Predictors of 2-Year Incidence of Patient-Reported Urinary Incontinence After Post-prostatectomy Radiotherapy: Evidence of Dose and Fractionation Effects. Front. Oncol. 2020, 10, 1207. [Google Scholar] [CrossRef] [PubMed]
- Matei, D.V.; Ferro, M.; Jereczek-Fossa, B.A.; Renne, G.; Crisan, N.; Bottero, D.; Mazzarella, C.; Terracciano, D.; Autorino, R.; De Cobelli, O. Salvage Radical Prostatectomy after External Beam Radiation Therapy: A Systematic Review of Current Approaches. Urol. Int. 2015, 94, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Bauer, R.M.; Soljanik, I.; Füllhase, C.; Buchner, A.; May, F.; Stief, C.G.; Gozzi, C. Results of the AdVance Transobturator Male Sling After Radical Prostatectomy and Adjuvant Radiotherapy. Urology 2011, 77, 474–479. [Google Scholar] [CrossRef]
- Wright, H.C.; McGeagh, K.; Richter, L.A.; Hwang, J.J.; Venkatesan, K.; Pysher, A.; Koch, G.E.; Kowalczyk, K.; Bandi, G.; Marchalik, D. Transobturator sling for post-prostatectomy incontinence: radiation's effect on efficacy/satisfaction. Can J Urol. 2017, 24, 8998–9002. [Google Scholar]
- Del Favero, L.; Tasso, G.; Deruyver, Y.; Tutolo, M.; Beels, E.; Schillebeeckx, C.; De Ridder, D.; Van der Aa, F. Long-term Functional Outcomes and Patient Satisfaction After AdVance and AdVanceXP Male Sling Surgery. Eur. Urol. Focus 2022, 8, 1408–1414. [Google Scholar] [CrossRef] [PubMed]
- Meisterhofer, K.; Herzog, S.; Strini, K.A.; Sebastianelli, L.; Bauer, R.; Dalpiaz, O. Male Slings for Postprostatectomy Incontinence: A Systematic Review and Meta-analysis. Eur. Urol. Focus 2019, 6, 575–592. [Google Scholar] [CrossRef]
- Friedl, A.; Mühlstädt, S.; Zachoval, R.; Giammò, A.; Kivaranovic, D.; Rom, M.; Fornara, P.; Brössner, C. Long-term outcome of the adjustable transobturator male system (ATOMS): results of a European multicentre study. BJU Int. 2016, 119, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Angulo, J.C.; Cruz, F.; Esquinas, C.; Arance, I.; Manso, M.; Rodríguez, A.; Pereira, J.; Ojea, A.; Carballo, M.; Rabassa, M.; et al. Treatment of male stress urinary incontinence with the adjustable transobturator male system: Outcomes of a multi-center Iberian study. Neurourol. Urodynamics 2018, 37, 1458–1466. [Google Scholar] [CrossRef]
- Angulo, J.C.; Virseda-Chamorro, M.; Arance, I.; Ruiz, S.; Ojea, A.; Carballo, M.; Rodríguez, A.; Pereira, J.; Teyrouz, A.; Rebassa, M.; et al. Long-term outcome of adjustable transobturator male system for stress urinary incontinence in the Iberian multicentre study. Neurourol. Urodynamics 2020, 39, 1737–1745. [Google Scholar] [CrossRef] [PubMed]
- Giammò, A.; Ammirati, E.; Tullio, A.; Morgia, G.; Sandri, S.; Introini, C.; Canepa, G.; Timossi, L.; Rossi, C.; Mozzi, C.; et al. Implant of ATOMS® system for the treatment of postoperative male stress urinary incontinence: an Italian multicentric study. Minerva Urol. Nephrol. 2020, 72, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Redmond, E.J.; Nadeau, G.; Tu, L.-M.; Doiron, R.C.; Steele, S.S.; Herschorn, S.; Locke, J.A.; Maciejewski, C.C.; Dwyer, N.T.; Campeau, L.; et al. Multicentered Assessment of Clinical Outcomes and Factors Associated With Failure of the Adjustable TransObturator Male System (ATOMS). Urology 2020, 148, 280–286. [Google Scholar] [CrossRef]
- Esquinas, C.; Angulo, J.C. Effectiveness of Adjustable Transobturator Male System (ATOMS) to Treat Male Stress Incontinence: A Systematic Review and Meta-Analysis. Adv. Ther. 2018, 36, 426–441. [Google Scholar] [CrossRef]
- Mühlstädt, S.; Angulo, J.C.; Mohammed, N.; Schumann, A.; Fornara, P. Complications of the urinary incontinence system ATOMS: description of risk factors and how to prevent these pitfalls. World J. Urol. 2019, 38, 1795–1803. [Google Scholar] [CrossRef]
- Angulo, J.C.; Arance, I.; Ojea, A.; Carballo, M.; Rodríguez, A.; Pereira, J.; Rebassa, M.; Teyrouz, A.; Escribano, G.; Teba, F.; et al. Patient satisfaction with adjustable transobturator male system in the Iberian multicenter study. World J. Urol. 2019, 37, 2189–2197. [Google Scholar] [CrossRef]
- Angulo, J.C.; Schönburg, S.; Giammò, A.; Queissert, F.; Gonsior, A.; González-Enguita, C.; Martins, F.E.; Rourke, K.; Cruz, F. Artificial urinary sphincter or a second adjustable transobturator male system offer equivalent outcomes in patients whom required revision on the initial ATOMS device: An international multi-institutional experience. Neurourol. Urodynamics 2021, 40, 897–909. [Google Scholar] [CrossRef]
- Angulo, J.C.; Esquinas, C.; Arance, I.; Rodríguez, A.; Pereira, J.; Rabassa, M.; Teyrouz, A.; Teba, F.; Celada, G.; Marcelino, J.P.; et al. Adjustable Transobturator Male System after Failed Surgical Devices for Male Stress Urinary Incontinence: A Feasibility Study. Urol. Int. 2018, 101, 106–113. [Google Scholar] [CrossRef]
- Queissert, F.; Huesch, T.; Kretschmer, A.; Kirschner-Hermanns, R.; Pottek, T.; Olianas, R.; Friedl, A.; Homberg, R.; Pfitzenmaier, J.; Naumann, C.M.; et al. Is the Standard Artificial Urinary Sphincter AMS 800 Still a Treatment Option for the Irradiated Male Patient Presenting with a Devastated Bladder Outlet? J. Clin. Med. 2023, 12, 4002. [Google Scholar] [CrossRef] [PubMed]
- Ullate, A.; Arance, I.; Virseda-Chamorro, M.; Ruiz, S.; Szczesniewski, J.; Téllez, C.; Queissert, F.; Dorado, J.F.; Angulo, J.C. ATOMS (Adjustable Trans-Obturator Male System) in Patients with Post-Prostatectomy Incontinence and Previously Treated Urethral Stricture or Bladder Neck Contracture. J. Clin. Med. 2022, 11, 4882. [Google Scholar] [CrossRef] [PubMed]
- Manunta, A.; Guillé, F.; Patard, J.J.; Lobel, B. Artificial sphincter insertion after radiotherapy: is it worthwhile? BJU Int. 2000, 85, 490–492. [Google Scholar] [CrossRef] [PubMed]
- Ravier, E.; Fassi-Fehri, H.; Crouzet, S.; Gelet, A.; Abid, N.; Martin, X. Complications after artificial urinary sphincter implantation in patients with or without prior radiotherapy. BJU Int. 2014, 115, 300–307. [Google Scholar] [CrossRef]
- Mann, R.A.; Kasabwala, K.; Buckley, J.C.; Smith, T.G.; Westney, O.L.; Amend, G.M.; Breyer, B.N.; Erickson, B.A.; Alsikafi, N.F.; Broghammer, A.J.; et al. The “Fragile” Urethra as a Predictor of Early Artificial Urinary Sphincter Erosion. Urology 2022, 169, 233–236. [Google Scholar] [CrossRef]
- Gomha, M.A.; Boone, T.B. Artificial urinary sphincter for post-prostatectomy incontinence in men who had prior radiotherapy: a risk and outcome analysis. J. Urol. 2002, 167, 591–596. [Google Scholar] [CrossRef]
- Jhavar, S.; Swanson, G.; Deb, N.; Littlejohn, L.; Pruszynski, J.; Machen, G.; Milburn, P.; Bird, E. Durability of Artificial Urinary Sphincter With Prior Radiation Therapy. Clin. Genitourin. Cancer 2017, 15, e175–e180. [Google Scholar] [CrossRef]
- Tutolo, M.; Cornu, J.; Bauer, R.M.; Ahyai, S.; Bozzini, G.; Heesakkers, J.; Drake, M.J.; Tikkinen, K.A.; Launonen, E.; Larré, S.; et al. Efficacy and safety of artificial urinary sphincter (AUS): Results of a large multi-institutional cohort of patients with mid-term follow-up. Neurourol. Urodynamics 2018, 38, 710–718. [Google Scholar] [CrossRef]
- Kaufman, M.R.; Milam, D.F.; Johnsen, N.V.; Cleves, M.A.; Broghammer, J.A.; Brant, W.O.; Jones, L.A.; Brady, J.D.; Gross, M.S.; Henry, G.D. Prior Radiation Therapy Decreases Time to Idiopathic Erosion of Artificial Urinary Sphincter: A Multi-Institutional Analysis. J. Urol. 2018, 199, 1037–1041. [Google Scholar] [CrossRef]
- Gallet, P.; Phulpin, B.; Merlin, J.-L.; Leroux, A.; Bravetti, P.; Mecellem, H.; Tran, N.; Dolivet, G. Long-Term Alterations of Cytokines and Growth Factors Expression in Irradiated Tissues and Relation with Histological Severity Scoring. PLOS ONE 2011, 6, e29399. [Google Scholar] [CrossRef]
- Sterling, J.; Rahman, S.N.; Varghese, A.; Angulo, J.C.; Nikolavsky, D. Complications after Prostate Cancer Treatment: Pathophysiology and Repair of Post-Radiation Urethral Stricture Disease. J. Clin. Med. 2023, 12, 3950. [Google Scholar] [CrossRef]
- Giammò, A.; Ammirati, E. Long-Term Survival Rate of ATOMS Implant for Male Stress Urinary Incontinence and Management of Late Complications. J. Clin. Med. 2023, 12, 2296. [Google Scholar] [CrossRef]
- Schönburg, S.; Bauer, W.; Mohammed, N.; Brössner, C.; Fornara, P. De novo OAB After ATOMS: An Underestimated Problem or a Rare Side Effect? Front. Surg. 2019, 6. [Google Scholar] [CrossRef] [PubMed]
- Cozzarini, C.; Rancati, T.; Palorini, F.; Avuzzi, B.; Garibaldi, E.; Balestrini, D.; Cante, D.; Munoz, F.; Franco, P.; Girelli, G.; et al. Patient-reported urinary incontinence after radiotherapy for prostate cancer: Quantifying the dose–effect. Radiother. Oncol. 2017, 125, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Mühlstädt, S.; Friedl, A.; Mohammed, N.; Schumann, A.; Weigand, K.; Kawan, F.; Göllert, C.; Kahlert, C.; Theil, G.; Fischer, K.; et al. Five-year experience with the adjustable transobturator male system for the treatment of male stress urinary incontinence: a single-center evaluation. World J. Urol. 2016, 35, 145–151. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Evolution of severity of incontinence according to 24-hour pad count, before ATOMS implant and after adjustment.
Figure 1.
Evolution of severity of incontinence according to 24-hour pad count, before ATOMS implant and after adjustment.
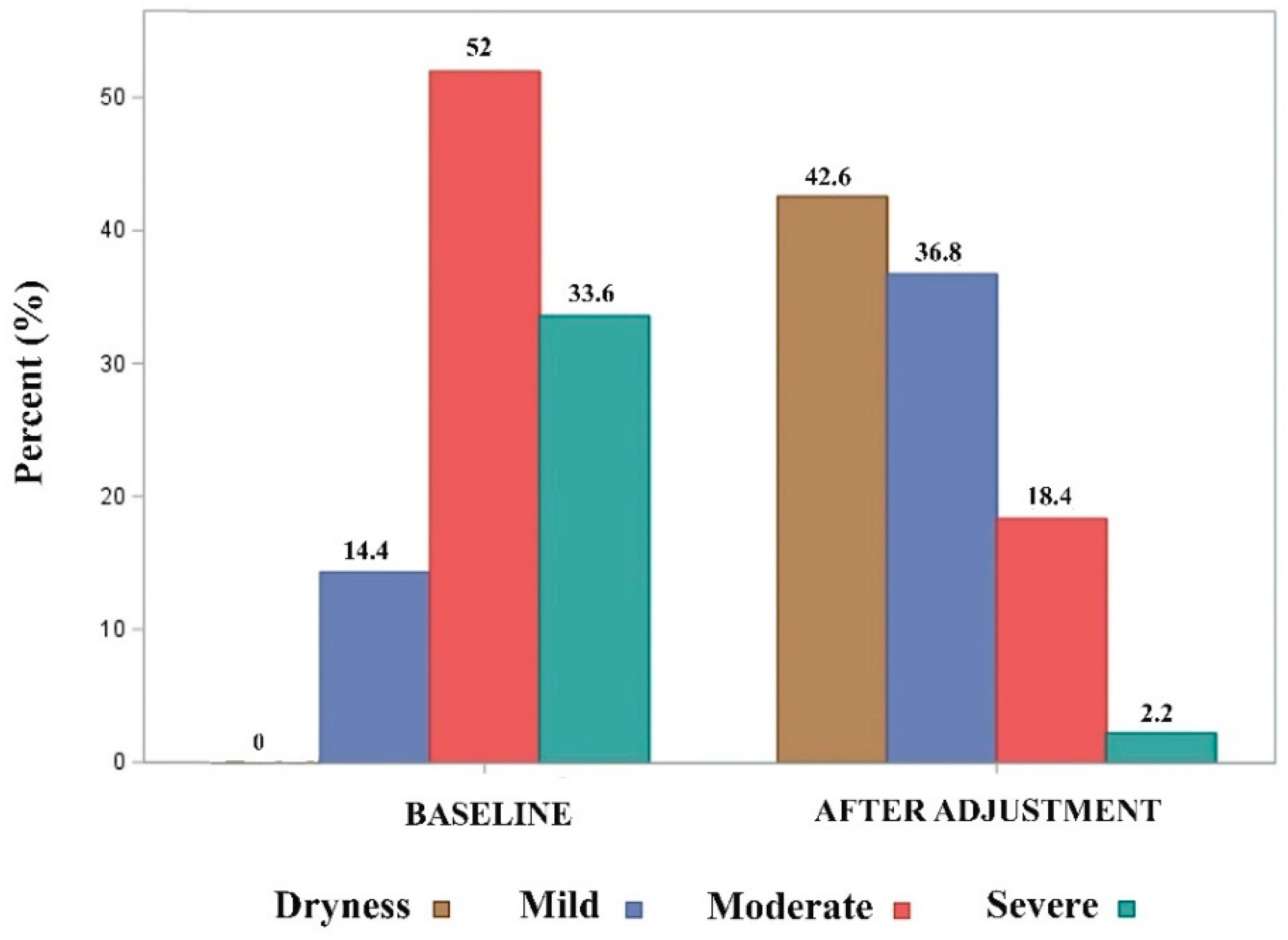
Figure 2.
(a) Evolution of 24-hour pad-count (PPD). (b) Evolution of 24-hour pad-test (mL).
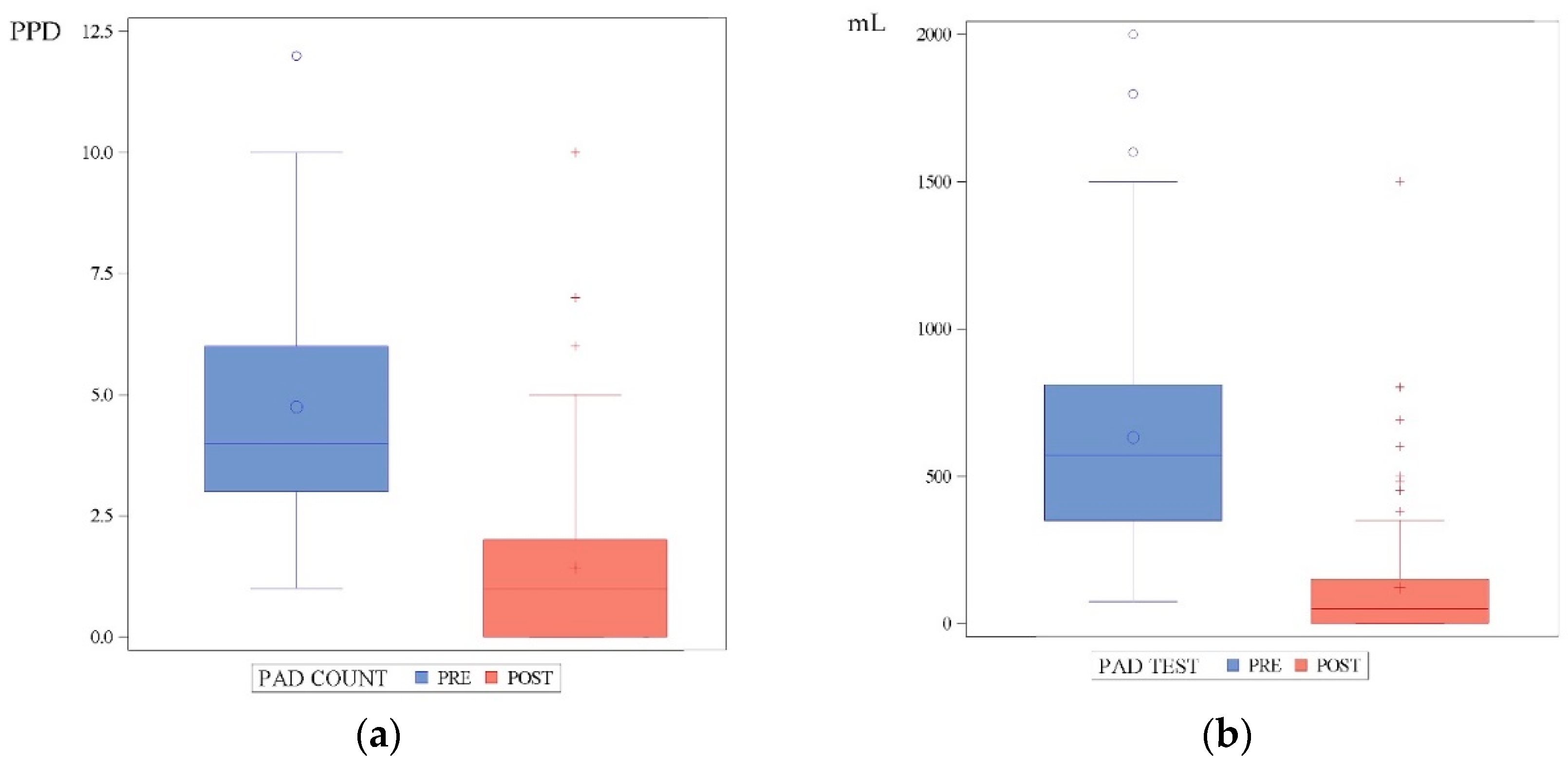
Figure 3.
Percent of each PGI-I score with ATOMS (n=125; 1, very much better; 2, much better; 3, slightly better; 4, same; 5, worse).
Figure 3.
Percent of each PGI-I score with ATOMS (n=125; 1, very much better; 2, much better; 3, slightly better; 4, same; 5, worse).
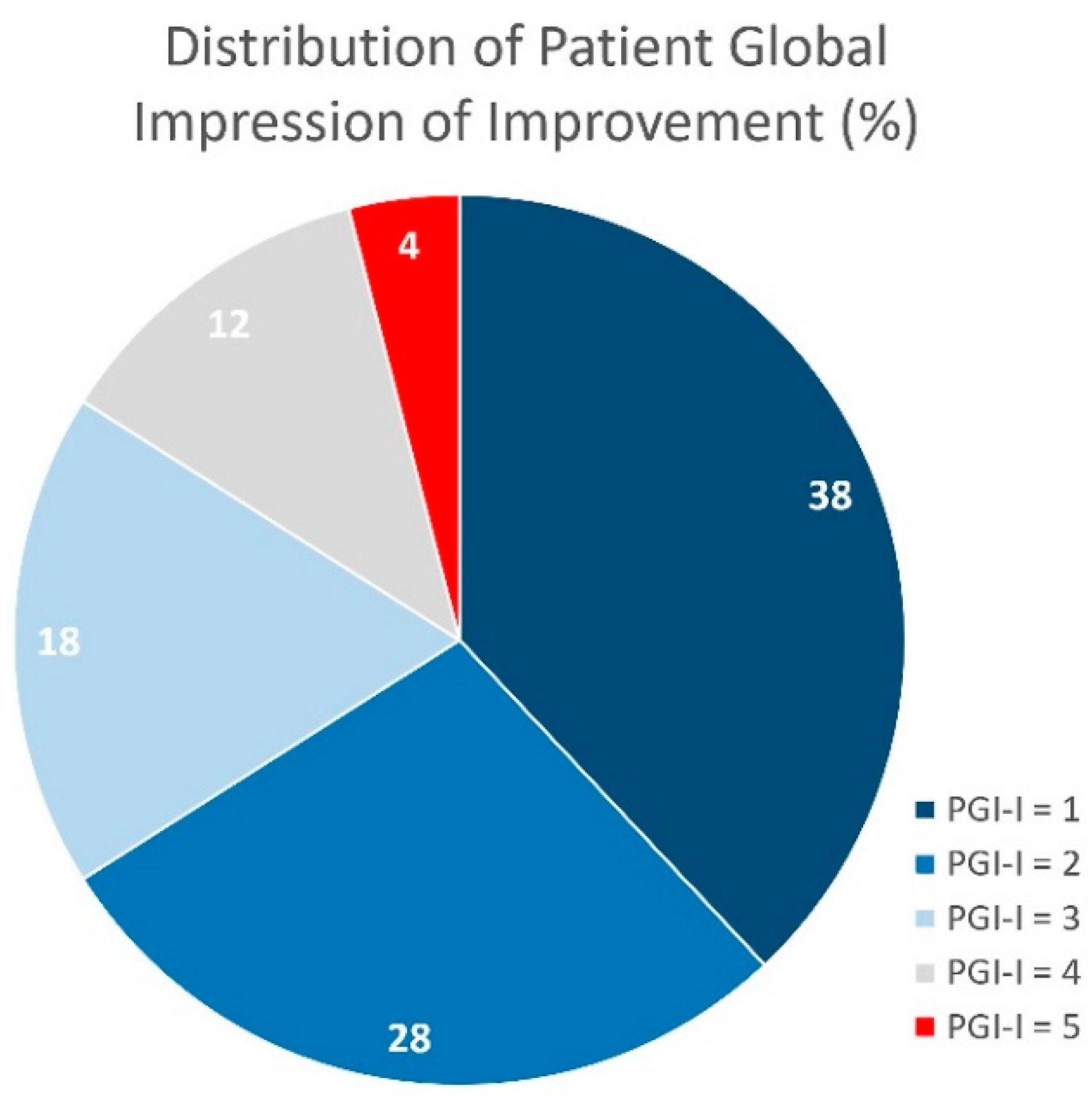
Figure 4.
Odds Ratios with 95% Confidence Limits for the independent variables identified.
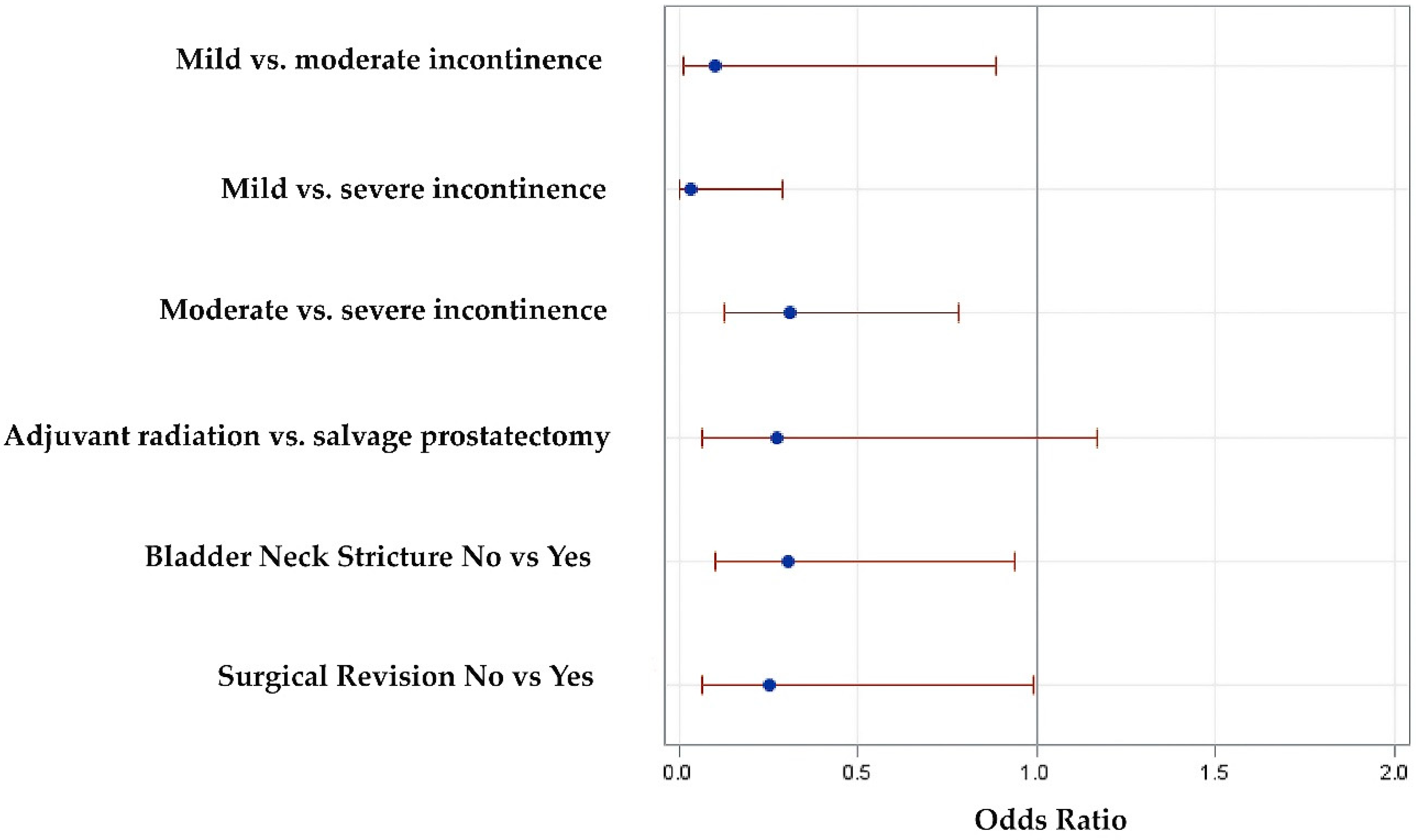
Figure 5.
Nomogram to predict dryness with ATOMS after prostatectomy and radiation.
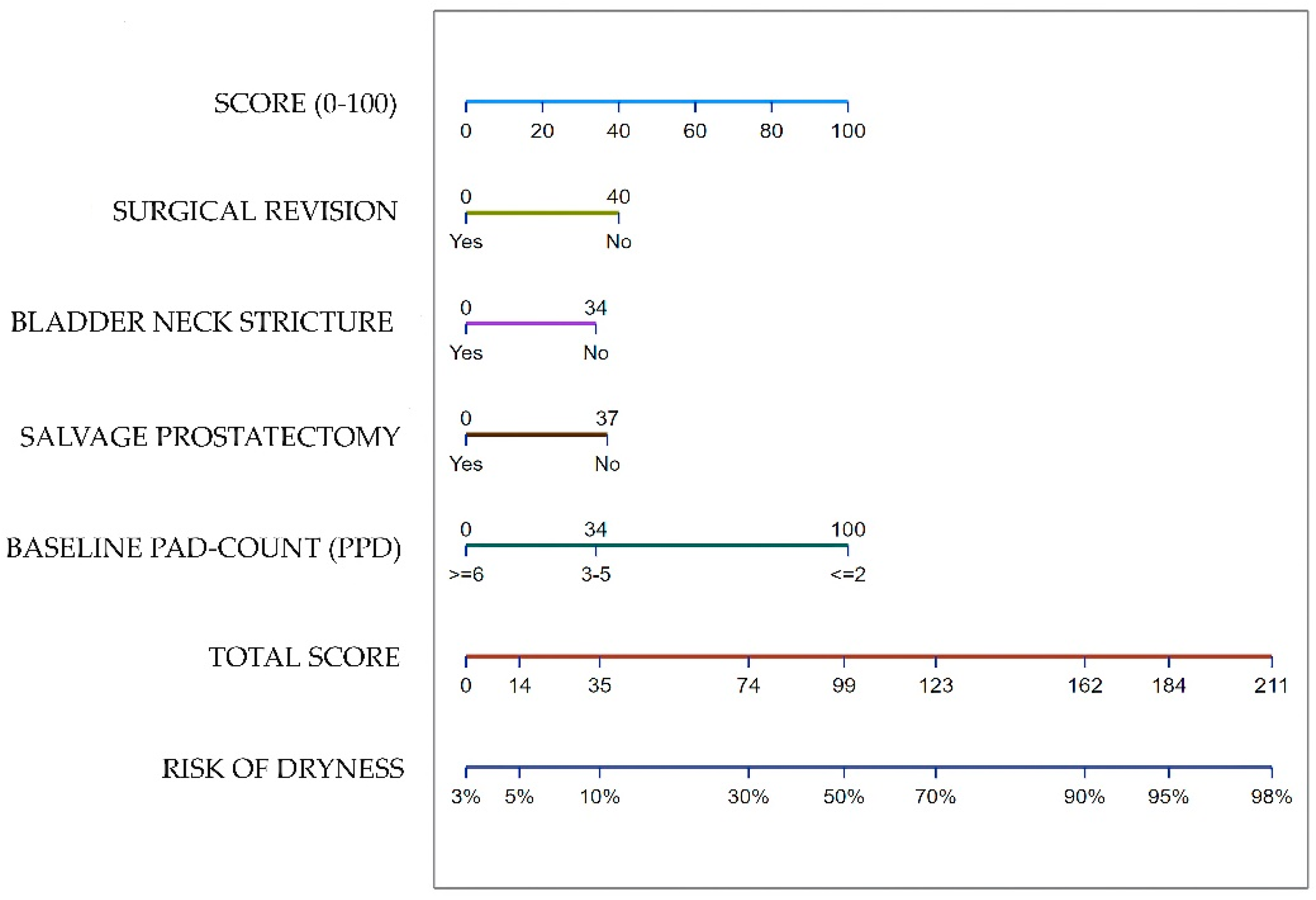

Table 1.
Preoperative, operative and postoperative data of patients included in the study.
| Variable | Total Series (n = 223) |
|---|---|
| Preoperative data | |
| Age, years, median (IQR) | 71 (11) |
| Time since prostatectomy to ATOMS, months, median (IQR) | 52 (58) |
| Previous incontinence surgery, n (%) | 27 (12.1) |
| Salvage prostatectomy, n (%) | 12 (5.4) |
| Previous TUR-P, n (%) | 8 (3.6) |
| Previous brachytherapy, n (%) | 2 (.9) |
| Androgen deprivation therapy, n (%) | 46 (20.6) |
| Bladder neck stricture, n (%) | 63 (28.2) |
| OAB symptoms, n (%) | 27 (12.1) |
| 24-h pad-count, PPD, median (IQR) | 4 (3) |
| 24-h pad-test, mL, median (IQR) (1) | 570 (460) |
| Operative data | |
| Operative time, min, median (IQR) | 62 (24) |
| Perioperative complication, n (%) | 2 (.9) |
| VAS for pain (0 – 10), median (IQR) (2) | 2 (2) |
| Postoperative data | |
| Postoperative complications (3), any grade, n (%) | 36 (16.1) |
| Grade I (3), n (%) | 20 (9) |
| Grade II (3), n (%) | 11 (4.9) |
| Grade III (3), n (%) | 5 (2.2) |
| Surgical revision, n (%) | 29 (13) |
| Device explant, n (%) | 26 (11.7) |
| De novo OAB symptoms, n (%) | 11 (4.9) |
| Total filling volume, mL, median (IQR) | 16 (11.5) |
| Number of fillings, median (IQR) | 1 (3) |
| Patients with pad-test ≤ 20 mL, n (%) | 95 (42.6) |
| 24-h pad-count, PPD, median (IQR) | 1 (2) |
| 24-h pad-test, mL, median (IQR) (4) | 50 (150) |
| PGI-I = 1 (very much better), n (%) (4) | 48 (38.4) |
| PGI-I = 2 (much better), n (%) (4) | 35 (28) |
| PGI-I = 3 (slightly better), n (%) (4) | 22 (17.6) |
| PGI-I = 4 (same), n (%) (4) | 15 (12) |
| PGI-I = 5 (worse), n (%) (4) | 5 (5) |
(1) Baseline pad-test evaluated in 125 patients. (2) Pain evaluated in 102 patients at hospital discharge, usually on day 1 after surgery; (3) According to Clavien–Dindo classification; (4) PGI-I evaluated in 125 patients; IQR, Interquartile range; PPD, pads-per-day; VAS, Visual Analogue Scale; OAB, overactive bladder; PGI-I, Patient Global Impression of Improvement.
Table 2.
Outcomes and mean change in postoperative incontinence for each incontinence severity group after ATOMS implant in patients treated with radical prostatectomy and adjunct radiation.
Table 2.
Outcomes and mean change in postoperative incontinence for each incontinence severity group after ATOMS implant in patients treated with radical prostatectomy and adjunct radiation.
| Degree of Incontinence | N (%) | Dryness (*) N (%) | Satisfaction (#) N (%) | Mean change in PPD | Mean change in pad-test (@) | Mean number of adjustments |
|---|---|---|---|---|---|---|
| Total series | 223 (100) | 95 (42.6) | 105 (84) | 3 ± 2.5 | 450 ± 400 | 3 ± 3 |
| Mild (1-2 PPD) | 32 (14.3) | 21 (65.6) | 10 (90.9) | 1.5 ± 1 | 200 ± 130 | 2.5 ± 3.5 |
| Moderate (3-5 PPD) | 116 (52) | 56 (48.3) | 52 (85.3) | 3 ± 2 | 350 ± 200 | 3 ± 3 |
| Severe (≥6 PPD) | 75 (33.7) | 18 (24) | 43 (81.1) | 5 ± 2 | 700 ± 270 | 4 ± 2 |
| P-value | <.0001 | .67 | <.0001 | <.0001 | <.0001 |
(*) 24-h pad-test <20 ml; (#) PGI-I 1-3, evaluated in 125 patients; PPD: pads/day; (@)pad-test evaluated in 125 patients.
Table 3.
Analysis of factors involved in the prediction of dryness.
| Univariate Analysis | OR | 95% CI Upper limit | 95% CI Lower limit | P value |
| Patient age <70 vs. ≥70 years | .59 | .34 | 1.01 | .06 |
| Adjuvant radiotherapy vs. salvage prostatectomy | .35 | .1 | 1.2 | .08 |
| Primary incontinence surgery | .34 | .13 | .89 | .02 |
| OAB symptoms | .37 | .14 | .96 | .04 |
| Bladder neck stricture | .35 | .18 | .67 | .001 |
| Surgical revision | .32 | .13 | .77 | .008 |
| Baseline incontinence, Mild vs. moderate | .54 | .23 | 1.25 | .0003 |
| Mild vs. severe | .21 | .09 | .50 | |
| Moderate vs. severe | .40 | .22 | .73 | |
| Multivariate Analysis | OR | 95% CI Upper limit | 95% CI Lower limit | P value |
| Surgical revision | .25 | .06 | .99 | .018 |
| Adjuvant radiotherapy vs. salvage prostatectomy | .28 | .07 | 1.17 | .07 |
| Bladder neck stricture | .3 | .1 | .94 | .05 |
| Baseline incontinence, Mild vs. moderate | .1 | .01 | .89 | <.0001 |
| Mild vs. severe | .03 | 0 | .29 | |
| Moderate vs. severe | .31 | .13 | .78 |
CI: confidence interval; OAB: overactive bladder.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



