
Submitted:
29 June 2023
Posted:
03 July 2023
You are already at the latest version
Abstract
Background: Globally, about 3.5 billion people are affected by intestinal parasitic infections (IPIs). This study aimed to investigate the effects of IPIs on intestinal wall thickness and its potential association with hypertension in different genders. Methods: A total of 108 subjects, including 83 consecutive patients with symptomatic and laboratory-confirmed IPIs (male = 48; female = 35) and 25 healthy controls (male = 10; female = 15), were recruited. B-mode ultrasound grayscale and color images of the duodenum and colon were obtained with and without water contrast. Results: Patients with IPIs had a tendency towards greater duodenal wall thickness (DUOTHICK = 0.88 ± 0.73 cm) compared to controls (0.595 ± 0.089 cm), p = 0.056. Patients with IPIs also had significantly greater ascending colon wall thickness (ASCTHICK = 1.076 ± 0.29 cm) and descending colon wall thickness (DSCTHICK = 1.175 ± 0.366 cm) compared to controls (ASCTHICK = 0.6015 ± 0.1607 cm, DSCTHICK = 0.6223 ± 0.135 cm), p < 0.05. Men over 50 years had greater DSCTHICK (1.25 ± 0.434 cm) than post-menopausal women (0.986 ± 0.389 cm), p < 0.05. DSCTHICK significantly predicted diastolic blood pressure (β = -0.295, p < .05) and blood sodium level (β = -0.300, p < .05). Conclusion: We demonstrated the effects of IPIs on the intestinal microbiome causing intestinal wall cytoskeletal dysfunction, which led to the development of a "leaky gut syndrome."
Keywords:
Intestinal Microbiome
; Gut Microbiota
; Parasites
; Ultrasound
INTRODUCTION
Globally, about 3.5 billion people are affected by intestinal parasitic infections (IPIs) [1]. Approximately 450 million people develop severe morbidity, and over 200 million die from IPIs, the majority of whom are children. According to the World Health Organization (WHO), there were 800–1000 million Ascaris lumbricoides, 700–900 million Hookworm infections, 500 million Trichuris trichuria, 200 million Giardia lamblia, and 500 million Entamoeba histolytica/dispar cases worldwide [2,3,4,5,6,7,8,9]. In Nigeria, the spatial distribution of helminthic infections (Ascaris lumbricoides, hookworm, Trichuris trichiura, S. stercoralis, Taenia sp, S. mansoni, Enterobius vermicularis, and Hymenolopis nana) across the six geopolitical zones of Nigeria has been identified [10]. The prevalence of intestinal helminths in Nigeria has not declined since the 1970s. Ascaris lumbricoides was the most prevalent helminth in the South-western (21%) and South-southern (13%) Nigeria. Hookworm was the most prevalent helminthic infection in the South-eastern (19%) Nigeria. On the other hand, there were multiple infections in Northern Nigeria (25% in North-central and 19% in the North-east and North-west, respectively). There was a high prevalence of Taenia sp and Schistosoma mansoni infections in the North-east and North-west of Nigeria (8% and 6%, respectively) [10]. In Owerri West Local Government Area in Imo State, South-eastern Nigeria, the prevalence of soil-transmitted helminths was 35.43% in primary school pupils [11]. In Owerri Municipal LGA, the overall prevalence of helminths was 58% among children in day-care centers [12].
The role of the human intestinal microbiome in health and disease has gained significant attention in recent years. Some investigators have suggested that the intestinal microbiome may differ between men and women. The divergence in the intestinal microbiome observed between men and women may be related to the gender differences observed in the prevalence of hypertension, metabolic, and intestinal inflammatory diseases. Some have suggested that gender differences may be influenced by the grade of obesity [13]. There are clearly gender differences in cardiovascular disease. Women experience cardiovascular events at an older age, and at any age, women, on average, have less atherosclerotic plaque than men [13]. Furthermore, men and women are known to have gender-specific differences in their immune system and intestinal microbiome composition [14].
Several cross-sectional studies in humans have shown an association between the intestinal microbiome and hypertension [15,16,17,18,19,20,21,22,23,24]. Globally, there are estimated 1.28 billion adults aged 30–79 years with hypertension. Over 75% of patients with hypertension live in low- and middle-income countries. In Nigeria, the prevalence of hypertension increased from 8.2% in 1990 to 32.5% in 2020 [25], and others have suggested a prevalence of hypertension as high as 38% [26]. There is a gender difference in the prevalence of hypertension. The prevalence of hypertension was higher among men up to the age of 50 years; beyond that, in every age group, females experienced higher rates [27]. In Nigeria, in most studies, the prevalence of hypertension was higher in men than in women [28].
It is of interest to explore, if there is a causal link between the high prevalence rates of IPIs and hypertension in Nigerians. If so, could the effective treatment of IPIs in early childhood and adulthood lower the incidence of hypertension in elderly Nigerians?
The IPIs cause intestinal cytoskeletal dysfunction, which in turn facilitates dysbiosis of the intestinal microbiome [29]. The causal relationship between dysbiosis and hypertension remains inconclusive. The specific mechanism by which intestinal microbiome affects the progression of hypertension is unclear. It is therefore of interest, to investigate the interaction between intestinal cytoskeletal dysfunction and hypertension. It has been postulated that, there are key mechanisms regulating the effects of intestinal microbiome in hypertension [30]. It was proposed that, intestinal dysbiosis leads to disruption of the nervous system, renal function, intestinal short chain fatty acids (SCFAs), immune system, increase in lipopolysaccharide (LPS) production and intestinal permeability, thereby aggravating the progression of hypertension [30].
Recently, we applied ultrasound duodenography and colonography to demonstrate that IPI-induced intestinal wall thickening with rearrangement of the cytoskeleton, caused malfunction of the glucose transporter system which resulted in Type 2 diabetes mellitus (T2DM) [29]. The inflammatory processes associated with IPIs lead to increased intestinal wall thickness, which could be measured as a surrogate marker for intestinal cytoskeletal dysfunction, using high-frequency ultrasound duodenography and colonography [29,31,32,33].
The purpose of the present work is to investigate gender differences between the interaction of intestinal cytoskeletal dysfunction and hypertension. We postulate a theory based on our earlier hypothesis, that, due to the effects of IPIs causing intestinal wall cytoskeletal dysfunction, the intestinal wall becomes ‘leaky’ to the microbiome, sugar, salts, other metabolites, and causing dysbalance of the sympathetic nervous system [34], which in turn, exacerbates the risk of hypertension, metabolic and intestinal inflammatory diseases. Moreover, increased sympathetic tone has been linked with elevated inflammation both systemically and in the intestine [35], which could contribute to the vascular gastrointestinal leakage [36]. Furthermore, we propose innovative ways of ‘sealing the leak’ on the intestinal wall by using emerging stem cell therapy and estrogen antagonists [37].
METHODS
In this study, 108 participants were recruited, including 83 consecutive patients (male = 48; female = 35) with symptomatic and laboratory confirmed IPIs and 25 healthy controls (male = 10; female = 15). The male mean ± standard deviation [SD] age was 47.9 ± 16.4 years, and the female mean ± SD age was 51.4 ± 15.95 years. A standardized questionnaire was used to collect clinical symptoms and disease history, including the onset and duration of illness. Qualitative and quantitative aspects of the illness, including the intensity and periodicity of abdominal pain, were recorded. The body mass index (BMI), fasting blood sugar (FBS), systolic and diastolic blood pressure, blood sodium, and potassium levels were also monitored.
The patient population was classified based on the onset and duration of illness at presentation into three groups: acute, subacute, and chronic. Exposure to contaminated food or water was recorded for each subject. Patients with parasitic infections who presented with rectal bleeding underwent colonoscopy to exclude colorectal cancer. Patients with a history of alcoholism, ulcerative colitis, major gastrointestinal diseases such as polyposis, collagen vascular diseases, pancreatic diseases, liver diseases, Crohn’s disease, tropical sprue, colon cancer, and diverticulitis were excluded from the study. The institutional human research ethics review board approved the protocol.
Laboratory Tests:
The laboratory stool test involved the microscopic detection of IPIs in fecal smears of three individual specimens or duodenal aspirates. Wet preparations of stool samples were examined by two parasitologists, and any discrepancies were resolved by a third parasitologist who was not involved in the initial evaluation [29,31,32,33]. The quantitative evaluation of IPIs in stool samples was based on the count per high power field (hpf) of view. In follow-up studies of the control group, a negative stool test or reduced count of trophozoites per hpf was used as an indicator of recovery. Patients underwent a comprehensive panel of standard laboratory blood tests, including measurements of complete blood count, liver and kidney function, lipid profile, and glucose levels.
High-Frequency Ultrasound Duodenography and Colonography
The high-frequency ultrasound duodenography and colonography protocol was described in detail elsewhere [29,31,33]. Briefly, traditional abdominal ultrasound examinations were performed using B mode and color flow Doppler ultrasonography with a low-frequency transducer (2.5 MHz) of a phased array transducer (S4 probe) of a duplex color flow Doppler ultrasound system (Agilent HP/Philips SONOS 5500, Philips Medical Systems, Cambridge, MA, USA) [29]. The abdominal ultrasound scan examined the internal organs, including the liver, gall bladder, spleen, pancreas, duodenum, colon, and kidneys in all subjects [29,31,33]. The ultrasound examination applied color flow Doppler to examine the localization of lesions in relation to vessels [29]. The ultrasound examination was used to detect the existence of co-morbid conditions [29].
The high-frequency ultrasound duodenography and colonography examination preceded the result of stool analysis. All ultrasound scans were performed with and without water contrast after overnight fasting (for at least 16 h) using the scanning procedure described in detail elsewhere [31,33]. The water contrast imaging was performed by having the subjects take at least 1 L of water before the examination [31,33]. The subject was placed in the supine horizontal, left posterior oblique, and left lateral decubitus positions using the intercostal and subcostal approaches [31,33].
All measurements and grading of echogenicity were performed by a single trained sonographer using built-in software. Measurements were taken between peristaltic waves. The measurements of the duodenum (duodenometrics), ascending and descending colon (colonometrics) were performed with the water contrast image [31,33]. The measurement endpoints for intestinal cytoskeleton dysfunction were the wall thickness [31,33]. The duodenometric measurement of the duodenal wall thickness (DUOTHICK) was measured between two mucosal folds of Kerckring [31,33], from the surface of the moderately echogenic mucosa, through the hyperechoic submucosa and hypoechoic muscularis to the hyperechoic serosa layer. Similarly, the colonometric measurement of the ascending colon wall thickness (ASCTHICK) and descending colon wall thickness (DSCTHICK) were taken between two haustra across all three layers of the wall [31,33].
The lesion in each subject was characterized by location, wall thickness, echogenicity of intestinal wall tissue, presence or absence of flattening or loss of duodenal folds and/or colonic haustration, presence or absence of hyperechoic floating foci (HFF) demonstrating chaotic and/or bulk motility, presence or absence of perilesional tissue echogenicity, and type of colonic peristalsis [29,31,33]. The IPIs lesions were due to the presence of protozoa and/or helminths [29]. The helminthic parasites were visible macroscopic organisms which were demonstrated as hyperechoic curvilinear foci (HCF) with serpentine motility [31]. The protozoan parasites were microscopic lesions that were visible due to their presence on echogenic floaters. The floaters used by flagellates (e.g. Giardia lamblia) or ciliated parasites demonstrated chaotic motility defined as sonographically observed rapid floatation movements in all directions by HFF, between peristaltic waves. On the other hand, floaters used by amebic lesions demonstrated bulk motility defined as sonographically observed slow floatation movements of HFF in mainly one direction, between peristaltic waves.
Anti-Parasitic Treatment
The treatment regimen for protozoal infections consisted of intravenous infusion of metronidazole (500 mg in 100 mL) or oral administration of one tablet (500 mg) or two tablets (250 mg) three times daily for 10 days [29]. The treatment regimen for helminthiasis consisted of oral administration of albendazole (400 mg) twice daily for 3 days [29].
Blood Pressure Classification
The classification of blood pressure followed the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure [38].
Statistical analysis
Statistical analysis was performed using descriptive, t-test statistics, regression and analysis of variance (ANOVA) for group comparison with the software package IBM SPSS Statistics for Windows, version 28.0.1.1. (15) (IBM Corp., Armonk, N. Y., USA). Mean values were reported as mean ± SD. The level of statistical significance was set at p < 0.05
RESULTS
Patients with IPIs exhibited various symptoms, including abdominal pain, especially in the right upper quadrant, flatulence, nausea, vomiting, borborygmi, perceived weight loss, occasional constipation or diarrhea. The stool analysis of patients with IPIs revealed the presence of multiple microorganisms, including E. histolytica, E. coli, G. lamblia, A. lumbricoides, hookworm, T. trichiura, and Taenia species. In contrast, healthy individuals did not exhibit any symptoms.
General Effects
A one-way ANOVA was conducted to investigate the impact of parasites on various dependent variables, such as age, BMI, FBS, SBP, DBP and blood sodium levels (Na+). The results revealed that there was no significant difference in age between patients with parasites (mean age = 50 ± 16.4 years) and the control group (mean age = 47 ± 15.7 years), p = NS. Patients with parasites had a statistically higher BMI (mean = 28.98 ± 7.43) than the control group (mean = 24.68 ± 7.2), F (1,96) = 5.78, p < 0.05. However, there was no gender-related difference between men and women with regards to BMI, FBS, SBP, DBP, and Na+.
To investigate the impact of IPIs on intestinal wall thickness, a one-way ANOVA was conducted to compare the effects of chronic parasitic infection on patients and control subjects using the dependent variables DUOTHICK, ASCTHICK, and DSCTHICK. The results showed that patients with parasites had a tendency towards a statistically significant difference in DUOTHICK (mean = 0.88 ± 0.73 cm) compared to controls (mean = 0.595 ± 0.089 cm), F(1,104) = 3.73, p = 0.056. There was a significant difference in ASCTHICK between patients with chronic parasites (mean = 1.076 ± 0.29 cm) and the control group (mean = 0.6015 ± 0.1607 cm), F (1,105) = 59.4, p < 0.001. Similarly, there was a significant difference in DSCTHICK between patients with chronic parasites (mean = 1.175 ± 0.366 cm) and the control group (mean = 0.6223 ± 0.135 cm), F(1,97) = 49.97, p < 0.001.
To investigate the impact of gender in patients with chronic parasitic lesions aged over 50 years, a one-way ANOVA was conducted. The results showed that in men, the thickness of the descending colon (DSCTHICK = 1.25 ± 0.434 cm) was greater than that in post-menopausal women (DSCTHICK = 0.986 ± 0.389 cm), F(1,49) = 5.5, p < 0.05. However, there was no significant gender-related difference in other parts of the intestine (DUOTHICK and ASCTHICK). Moreover, in patients younger than 50 years, there was no significant difference in the thickness of the descending colon wall between men (DSCTHICK = 0.965 ± 0.439 cm) and pre-menopausal women (AGE < 50 years) (DSCTHICK = 1.068 ± 0.342 cm), p = NS.
To investigate the relationship between intestinal wall thickening of the descending colon and diastolic blood pressure, a linear regression model was used. It quantified the relationship between the predictor variable DSCTHICK and the response variable DBP in patients with chronic parasitic lesions. Simple linear regression was used to test if DSCTHICK significantly predicted DBP. The fitted regression model was: DBP = 100.822 - 12.367*(DSCTHICK). The overall regression was statistically significant (adjusted R2 = 0.075, F(1, 74) = 7.055, p < .05). It was found that the intestinal wall thickness of the descending colon significantly predicted the diastolic blood pressure (β = -0.295, p < .05). However, the intestinal wall thickness of the descending colon did not predict the systolic blood pressure (p = NS).
To investigate the association between intestinal wall thickness of the descending colon in patients with parasitic lesions and blood sodium levels, a linear regression model was used. Simple linear regression was performed to test if DSCTHICK significantly predicted Na+ level in blood. The fitted regression model was: Na+ = 193.367 - 29.77*(DSCTHICK). The overall regression was statistically significant (adjusted R2 = 0.077, F(1, 73) = 7.197, p < .05). It was observed that intestinal wall thickening of the descending colon significantly predicted the blood sodium level (β = -0.300, p < .05).
Moreover, we explored the relationship between intestinal wall thickness of the duodenum (DUO), ascending colon (ASC), and descending colon (DSC) in men with parasitic infections and blood sodium levels. A multiple linear regression model was employed to test if predictors DUOTHICK, ASCTHICK, and DSCTHICK significantly predicted the response of Na+. The overall regression was statistically significant (adjusted R2 = 0.179, F(3,39) = 4.047, p < 0.05). It was discovered that the predictor DUOTHICK significantly predicted the response of Na+ level (β = -0.295, p < 0.05). Similarly, the predictor DSCTHICK significantly predicted the response of Na+ level (β = -0.387, p < 0.05). However, the predictor ASCTHICK did not significantly predict the response of Na+ blood level (β = -0.578, p = NS).
A 48-year-old male presented with hematochezia, abdominal pain, constipation, persistent flatulence, borborygmi, and lactose intolerance. The symptoms began two years ago when he abruptly noticed hematochezia. He consumes fresh garden eggs (Solanum aethiopicum) and African star apple (Chrysophyllum albidum), which might have exposed him to parasites present in soil contaminated with human waste in the environment. Laboratory tests showed a hematocrit of 42%, hemoglobin of 14.1 g, a white blood cell count of 3,500/mm3, an ESR of 11 mm/hr, a clotting time of 10 minutes, a platelet count of 185,000/mm3, a prothrombin time of 26 seconds, hypernatremia (sodium of 166 mEq/L), chloride of 92 mEq/L, potassium of 6 mEq/L, and calcium of 10.8 mg/dL. Liver function tests showed normal alanine transaminase (ALT) of 8 IU/L, aspartate transaminase (AST) of 7 IU/L, and conjugated bilirubin (CB) of 0.21 mg/dL, but raised total bilirubin (TB) of 0.62 mg/dL. The D-dimer was normal at 478 g/L. Colonoscopy did not reveal any growths (polyposis) or cancer. There were no major bleeding sites or inflammation. The internal hemorrhoidal complexes were engorged circumferentially and some had shallow ulcerations. The posterior hemorrhoid bundle had grade 1 hemorrhoids that bleed but do not prolapse.
The thickness of the duodenal wall was measured pre-treatment (DUOTHICK of 0.663 cm), but post-treatment, the thickness had reduced (DUOTHICK of 0.32 cm). Similarly, in the ascending colon, the pre-treatment wall thickness was measured (ASCTHICK of 1.02 cm), but after treatment, the thickness had reduced (ASCTHICK of 0.663 cm).
Before treatment, the ultrasound image of the descending colon [Figure 1A] showed changes in echoanatomy, with increased wall thickness (DSCTHICK = 1.64 cm) [Figure 1A, marked with double white star], decreased wall echogenicity, and rearrangement of the tri-layer wall structure. There was also haustral unfolding and occasional HFF with chaotic motility [Figure 1A, marked with white arrowhead]. However, after ten days of treatment, the post-treatment ultrasound image of the descending colon [Figure 1B] showed increased echogenicity of the walls and haustra, and the wall thickness had reduced (DSCTHICK of 0.82 cm) [Figure 1B, marked with double white star]. The follow-up post-treatment ultrasound image [Figure 1C] taken three months later showed a slight increase in wall thickness (DSCTHICK of 0.943 cm). Nevertheless, there was a remarkable change in wall echogenicity with a normal tri-layer wall arrangement, showing hyperechoic mucosa and submucosa layers, hypoechoic muscularis layer, and hyperechoic serosa layer.
The pre-treatment ultrasound image of the sigmoid colon (Figure 2A) revealed many HFF with chaotic motility (white arrowhead in Figure 1A) and increased echogenicity and wall thickness (SIGMOID of 0.69 cm). The patient had persistent rectal bleeding. However, in the post-treatment image taken 3 months later (Figure 2B), there was no more rectal bleeding or HFF. The wall thickness (SIGMOID of 0.443 cm) and echogenicity had significantly decreased.
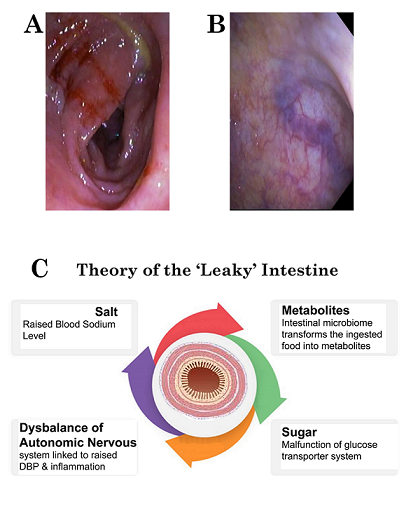
The pre-treatment images [Figure 3 A-B], obtained during colonoscopy, show bleeding sites [Figure 3A] in the descending colon. The mucosal and submucosal layers of the descending colon exhibit abnormally tortuous engorged veins (angiodysplasia). The patients were followed up for at least three months, during which significant improvements were observed in clinical presentation and control ultrasound and stool tests. In cases where complaints and control tests suggested incomplete clearance of IPIs, a repeat regimen using metronidazole and albendazole was administered.
DISCUSSION
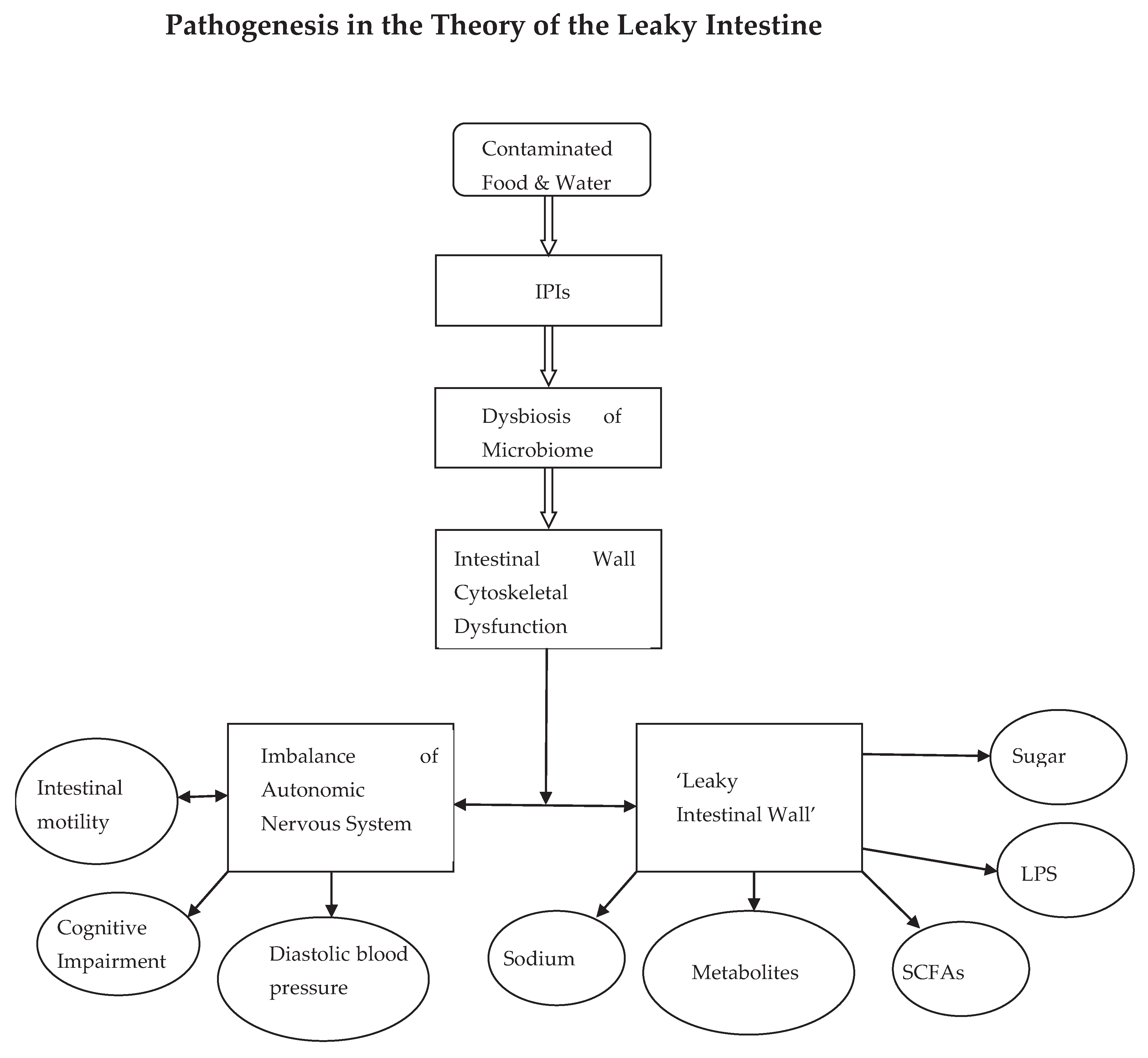
Our findings suggest that patients were exposed to contaminated food and water, which led to infection with IPIs. The IPIs, in turn, caused dysbiosis of the intestinal microbiome, and the accompanying inflammatory processes led to dysfunction of the cytoskeleton of the intestinal wall. The cytoskeletal dysfunction creates a neuromuscular mismatch leading to autonomic nervous system dysbalance with local effects on intestinal motility and general effects on diastolic blood pressure. The increase in sympathetic activity may be implicated in both initiating and sustaining the diastolic blood pressure elevatio. The autonomic innervation of the small and large intestine is supplied by extrinsic sympathetic and parasympathetic fibers. The innervation of the colon depends on embryological origin [39]. The ascending colon and proximal two-thirds of the transverse colon, which derive from the midgut, receive their sympathetic, parasympathetic, and sensory supply via nerves from the superior mesenteric plexus. On the other hand, the distal one-third of the transverse colon, descending colon, and sigmoid colon receive their sympathetic, parasympathetic, and sensory supply via nerves from the inferior mesenteric plexus. The parasympathetic innervation derives from the pelvic splanchnic nerves, while the sympathetic innervation is received via the lumbar splanchnic nerves.
The results demonstrate changes in the macroscopic echoanatomy of the intestinal wall, depicting rearrangement of the cytoskeleton and its transformation in the post-treatment period. The latter suggests that the effects of IPIs on cytoskeletal dysfunction disrupt the electrogenic mechanism in the well-ordered colonic intestinal epithelium. There is increased intestinal permeability for absorption of sodium salt and water, especially in the descending colon. The cumulative effects of the IPI-induced rearrangement of the colonic wall cytoskeleton could lead to raised sodium levels, short-chain fatty acids (SCFAs), lipopolysaccharides (LPS), sugar, and other metabolites [29,30]. The sequence of events could be summarized in the steps depicted in Figure 3 C-D. The cumulative effects of IPIs on the intestinal wall result in a "leaky intestine." Hence, we suggest a theory of the "Leaky Intestine" due to the effects of IPIs and intestinal microbiome. The main pathogenetic steps are outlined in the schematic diagram (Figure 4).
The transformative changes in wall echogenicity from pre-treatment to post-treatment effects suggest increased blood flow leading to tissue regeneration of the intestinal wall cytoskeleton. These processes of tissue regeneration result in the "sealing of the leak of the intestinal wall." This may point to a role for innovative stem cell therapy for "sealing of the intestinal wall." Moreover, investigators have suggested the use of mesenchymal stem cell (MSC) therapy to manage inflammatory bowel disease (IBD), mainly by dampening inflammation, regulating immune disorders, and promoting mucosal tissue repair [37,43,44]. We are not aware of the use of MSC after serious IPIs, but an exploratory study may be helpful.
The role of gender may offer some clues to potential new treatment drugs for sealing the leaky intestine. There was no difference in descending colon wall thickness in men and women younger than 50 years. However, in those older than 50 years, in men, the intestinal wall thickness was much greater than in post-menopausal women (>50 years). In other words, in post-menopausal women with low levels of circulating estrogen/progesterone, there was reduced intestinal wall thickness and intestinal cytoskeletal dysfunction, hence "sealing the leak." On the other hand, in men, there was no difference, which would suggest that testosterone levels had no such effects. It is known that estrogen is immunoenhancing, while testosterone is immunosuppressive [39]. One plausible explanation is that in premenopausal women, the estrogen immunoenhancing effect up-regulates immune response within the intestinal brush-border region, leading to deposition of immune complexes that result in intestinal wall thickening. In the postmenopausal period, the reduced effects of estrogen result in lesser intestinal wall thickness. On the other hand, some have suggested that the intestinal microbiome regulates estrogens through secretion of β-glucuronidase, an enzyme that deconjugates estrogens into their active forms. Infection with IPIs impairs this process through dysbiosis of the intestinal microbiome, characterized by lower microbial diversity. The decrease in deconjugation results in a reduction of circulating estrogens. The alteration in circulating estrogens may contribute to the development of conditions related to obesity, metabolic syndrome, cancer, endometrial hyperplasia, endometriosis, polycystic ovary syndrome, fertility, cardiovascular disease (CVD), and cognitive function [40].
It could be presumed that modulation of the microbiome composition subsequently impacts the metabolic profile, and vice versa, and has been shown to alleviate many of the estrogen-modulated disease states [40]. The aforementioned may suggest that, estrogen antagonists, for example, tamoxifen, may be a potential drug treatment candidate for "sealing the leak" of the intestine [40]. Moreover, some investigators have demonstrated the antimicrobial activity of tamoxifen metabolites against multidrug-resistant (MDR) Acinetobacter baumannii and Escherichia coli, and it may be a potential alternative for the treatment of infections caused by these two pathogens [41].
Conversely, others have suggested that female mice mount a natural killer T (NKT) cell–dependent fast and vigorous immune response that controls the parasite load and inhibits the development of amebic liver abscess (ALA), whereas in males, an immunopathologic process dominates the immune process. Thus, it has been shown that dexamethasone treatment prevents male hamsters from developing ALA [42].
In conclusion, we demonstrated the effects of IPIs on the intestinal microbiome and the development of a "leaky intestine." The IPIs lead to dysbiosis of the intestinal microbiome, which causes dysfunction of the cytoskeleton of the intestinal wall. This creates a neuromuscular mismatch, leading to autonomic nervous system dysbalance with local effects on intestinal peristalsis and general effects on diastolic blood pressure. The cumulative effects of IPI-induced rearrangement of the colonic wall cytoskeleton could lead to raised sodium levels, short-chain fatty acids (SCFAs), lipopolysaccharides (LPS), sugar, and other metabolites. The ensuing condition is associated with a plethora of symptoms presenting as a syndrome complex that could be best described as the ‘leaky gut syndrome’. The main pathogenetic steps are outlined in the schematic diagram. The transformative changes in wall echogenicity from pre-treatment to post-treatment effects suggest increased blood flow leading to tissue regeneration of the intestinal wall cytoskeleton. We suggest a role for innovative stem cell therapy for "sealing the leak" in the intestinal wall [37,43]. Furthermore, the role of gender may offer some clues to potential new treatment drugs for sealing the leaky intestine [45,46,47,48].
Funding
This research received no funding.
Conflicts of interest
There are no conflicts of interest.
References
- WHO. Conquering, Suffering and Enriching Humanity Report of an Informal Consultation. 2000.
- Olubunmi, O. Parasites of Man and Animals: Concept publication limited. 2013.
- Vandenberg O, Van Laethem Y, Souayah H, Kutane WT, Van Gool T. Improvement of routine diagnosis of intestinal parasites with multiple sampling and SAF-fixative in the triple-feces-test. Gastroenterology Belg. 2006; 69: 361-366.
- 4. Mehraj V, Hatcher J, Akhtar S, Rafique G, Beg A. Prevalence and Factors Associated with Intestinal Parasitic Infection among Children in an Urban Slum of Karachi. PLoS ONE 2008; 3(11): e3680. [CrossRef]
- Ahmed T, Khanum H, Uddin MS, Barua P, Arju T, Kabir M, Haque R. Entameoba Histolytica, Giardia Lamblia and Cryptosporidium spp. infection in children in an urban slum area of Bangladesh Bio res. Comm. 2016; 2: 175-181.
- World Health Organization. Prevention and control of intestinal parasitic infections: Report of a WHO Expert Committee [meeting held in Geneva from 3 to 7 March 1986]. World Health Organization; 1987.
- Abate A, Kibret B, Bekalu E, Abera S, Teklu T, Yalew A; et al. Cross-sectional study on the prevalence of intestinal parasites and associated risk factors in Teda Health Centre, Northwest Ethiopia. International Scholarly Research Notices. 2013;2013. [CrossRef]
- Ayelgn M, Worku L, Ferede G, Wondimeneh Y. A 5 year retrospective analysis of common intestinal parasites at Poly Health Center, Gondar, Northwest Ethiopia. BMC research notes. 2019;12(1):697. [CrossRef]
- Norhayati M, Fatmah M, Yusof S, Edariah A. Intestinal parasitic infections in man: A review. Medical Journal of Malaysia. 2003;58(2):296–305.
- Funso-Aina OI, Chineke HN, Adogu PO. A Review of Prevalence and Pattern of Intestinal Parasites in Nigeria (2006-2015). European Journal of Medical and Health Sciences. 2020;2(1). [CrossRef]
- Ogonaka IA, Nwoke BEB, Ukaga GN. Prevalence of Soil Transmitted Helminthes among Primary School Pupils in Owerri West Local Government Area in Imo State, Nigeria. Parasitol Public Health Soc Niger. 2011;27:92.
- Opara KN, Nwoke EA, Abanobico-Onwuliri COE, Iwuala C, Amadi AN. Intestinal parasites among children in day-care centres in Owerri metropolis Nigeria. Niger J Parasitol. 2010;31(1):45-49.
- Ahmed S, Spence JD. Sex differences in the intestinal microbiome: Interactions with risk factors for atherosclerosis and cardiovascular disease. Biol Sex Differ. 2021;12(1):35. [CrossRef]
- Fransen F, van Beek AA, Borghuis T, Meijer B, Hugenholtz F, van der Gaast-de Jongh C; et al. The Impact of Gut Microbiota on Gender-Specific Differences in Immunity. Front Immunol. 2017;8:754. [CrossRef]
- Dan X, Mushi Z, Baili W, Han L, Enqi W, Huanhu Z; et al. Differential analysis of hypertension-associated intestinal microbiota. Int J Med Sci. 2019;16:872–881. [CrossRef]
- de la Cuesta-Zuluaga J, Mueller NT, Alvarez-Quintero R, Velasquez-Mejia EP, Sierra JA, Corrales-Agudelo V; et al. Higher fecal short-chain fatty acid levels are associated with gut microbiome dysbiosis, obesity, hypertension and cardiometabolic disease risk factors. Nutrients. 2018;11(1):51. [CrossRef]
- Li J, Zhao F, Wang Y, Chen J, Tao J, Tian G; et al. Gut microbiota dysbiosis contributes to the development of hypertension. Microbiome. 2017;5(1):14. [CrossRef]
- Sun S, Lulla A, Sioda M, Winglee K, Wu MC, Jacobs DR; et al. Gut microbiota composition and blood pressure. Hypertension. 2019;73(5):998-1006. [CrossRef]
- Verhaar BJH, Collard D, Prodan A, Levels JHM, Zwinderman AH, Bäckhed F; et al. Associations between gut microbiota, faecal short-chain fatty acids, and blood pressure across ethnic groups: The HELIUS study. Eur Heart J. 2020;41(44):4259-4267. [CrossRef]
- Yan Q, Gu Y, Li X, Yang W, Jia L, Chen C; et al. Alterations of the gut microbiome in hypertension. Front Cell Infect Microbiol. 2017;7:381. [CrossRef]
- Yang T, Santisteban MM, Rodriguez V, Li E, Ahmari N; et al. Gut dysbiosis is linked to hypertension. Hypertension. 2015;65:1331–1340. [CrossRef]
- Kim S, Goel R, Kumar A, Qi Y, Lobaton G, Hosaka K; et al. Imbalance of gut microbiome and intestinal epithelial barrier dysfunction in patients with high blood pressure. Clin Sci (Lond). 2018;132:701–718. [CrossRef]
- Huart J, Leenders J, Taminiau B, Descy J, Saint-Remy A, Daube G; et al. Gut microbiota and fecal levels of short-chain fatty acids differ upon 24-hour blood pressure levels in men. Hypertension. 2019;74:1005–1013. [CrossRef]
- Jackson MA, Verdi S, Maxan ME, Shin CM, Zierer J, Bowyer RCE, Martin T, Williams FMK, Menni C, Bell JT; et al. Gut microbiota associations with common diseases and prescription medications in a population-based cohort. Nat Commun. 2018;9:2655. [CrossRef]
- Adeloye D, Owolabi EO, Ojji DB, Auta A, Dewan MT, Olanrewaju TO; et al. Prevalence, awareness, treatment, and control of hypertension in Nigeria in 1995 and 2020: A systematic analysis of current evidence. J Clin Hypertens. 2021;23:963–977. [CrossRef]
- Odili A, Chori B, Danladi B, Nwakile P, Okoye I, Abdullah U; et al. Prevalence, Awareness, Treatment and Control of Hypertension in Nigeria: Data from a Nationwide Survey 2017. Glob Heart. 2020. [CrossRef]
- Mohanty P, Patnaik L, Nayak G; et al. Gender difference in prevalence of hypertension among Indians across various age-groups: A report from multiple nationally representative samples. BMC Public Health. 2022;22:1524. [CrossRef]
- 28. Akinlua JT, Meakin R, Umar AM, Freemantle N. Current Prevalence Pattern of Hypertension in Nigeria: A Systematic Review. PLoS ONE 2015;10(10):e0140021. [CrossRef]
- Njemanze PC, Darlington CC, Onuchukwu JE, Ukeje NE, Amadi A, Mgbenu CU; et al. Intestinal parasitic infection-induced intestinal wall cytoskeleton dysfunction in diabetes mellitus. Niger J Gen Pract. 2022;20:29-35. [CrossRef]
- Sun, D. , Xiang H., Yan J., He L. Intestinal microbiota: A promising therapeutic target for hypertension. Front Cardiovasc Med. 2022 Nov 15;9:970036. PMID: 36457803; PMCID: PMC9705378. [CrossRef]
- Njemanze, P.C. , Njemanze J., Skelton A., Akudo A., Akagha O., Chukwu A.A ; et al. High-frequency ultrasound imaging of the duodenum and colon in patients with symptomatic giardiasis in comparison to amebiasis and healthy subjects. J Gastroenterol Hepatol 2008;23:e34-42. [CrossRef]
- Njemanze, P.C. , Njemanze J.T., Ofoegbu C.C., Darlington C.C., Nneke E., Onweni J.A.; et al. High-frequency ultrasound imaging of the intestine in normal subjects and patients with intestinal parasites. In: Ali Abdo Gamie S, Mahmoud Foda E, editors. Essentials of Abdominal Ultrasound. London: IntechOpen; 2019; pp. 91–105. [Google Scholar] [CrossRef]
- Njemanze, P.C. , Njemanze J.T., Ofoegbu C.C., Nneke E., Onweni I.A., Ejiogu U.V.; et al. Technical notes on high-frequency ultrasound duodenography and colonography imaging of giardial lesions. Niger J Gen Pract 2021;19:54-60.
- Zubcevic, J. , Richards E.M., Yang T., Kim S., Sumners C., Pepine C.J.; et al. Impaired Autonomic Nervous System-Microbiome Circuit in Hypertension. Circ Res. 2019 Jun 21;125(1):104-116. PMID: 31219753; PMCID: PMC6588177. [CrossRef]
- Straub, R. , Wiest R., Strauch U., Harle P., Schölmerich J. The role of the sympathetic nervous system in intestinal inflammation. Gut 2006;55(11):1640–649. [CrossRef]
- Jeong, J. , Kim K., Lim D., Kim K., Kim H., Lee S.; et al. Microvasculature remodeling in the mouse lower gut during inflammaging. Sci Rep 2017;7:39848. [CrossRef]
- Liu, A. , Wang X., Liang X., Wang W., Li C., Qian J., Zhang X. Human umbilical cord mesenchymal stem cells regulate immunoglobulin a secretion and remodel the diversification of intestinal microbiota to improve colitis. Front Cell Infect Microbiol. 2022 Sep 2;12:960208. [CrossRef]
- National High Blood Pressure Education Program. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Bethesda (MD): National Heart, Lung, and Blood Institute (US); 2004 Aug. Classification of Blood Pressure. Available from: https://www.ncbi.nlm.nih.gov/books/NBK9633/.
- Taneja, V. Sex hormones determine immune response. Front Immunol. 2018; 9:1931. [CrossRef]
- Baker JM, Al-Nakkash L, Herbst-Kralovetz MM. Estrogen-gut microbiome axis: Physiological and clinical implications. Maturitas. 2017 Sep;103:45-53. [CrossRef]
- Miró-Canturri A, Ayerbe-Algaba R, Vila-Domínguez A, Jiménez-Mejías ME, Pachón J, Smani Y. Repurposing of the Tamoxifen Metabolites to Combat Infections by Multidrug-Resistant Gram-Negative Bacilli. Antibiotics (Basel). 2021 Mar 22;10(3):336. [CrossRef]
- Quintanar-Quintanar ME, Jarillo-Luna A, Rivera-Aguilar V; et al. Immunosuppressive treatment inhibits the development of amebic liver abscesses in hamsters. Med Sci Monit. 2004;10(11):BR317-24.
- Koppula S, Kumar H. More than a pore: The therapeutic potential of stem cells for neurological disorders. Cell Tissue Res. 2019 Jan;375(1):11-24.
- Fujita T, Kishimoto K, Kato Y; et al. Sympathetic nervous system regulates adipocyte proliferation by modulating bone marrow mesenchymal stem cell niche through β2-adrenergic receptor. Nat Commun. 2015 Jun 22;6:8281. [CrossRef]
- Fasano, A. Leaky gut and autoimmune diseases. Clin Rev Allergy Immunol. 2012 Feb;42(1):71-8. [CrossRef]
- Mu Q, Kirby J, Reilly CM, Luo XM. Leaky gut as a danger signal for autoimmune diseases. Front Immunol. 2017;8:598. [CrossRef]
- Bischoff SC, Barbara G, Buurman W, Ockhuizen T, Schulzke JD, Serino M, Tilg H, Watson A, Wells JM. Intestinal permeability - a new target for disease prevention and therapy. BMC Gastroenterol. 2014 Dec 19;14:189. [CrossRef]
- Hollander, D. Intestinal permeability, leaky gut, and intestinal disorders. Curr Gastroenterol Rep. 1999 Oct;1(5):410-6. [CrossRef]
Figure 1.
A-C show the pre-treatment image (Figure 1A), post-treatment image taken after 10 days (Figure 1B), and follow-up post-treatment image taken 3 months later (Figure 1C) with white star markers indicating wall thickness.
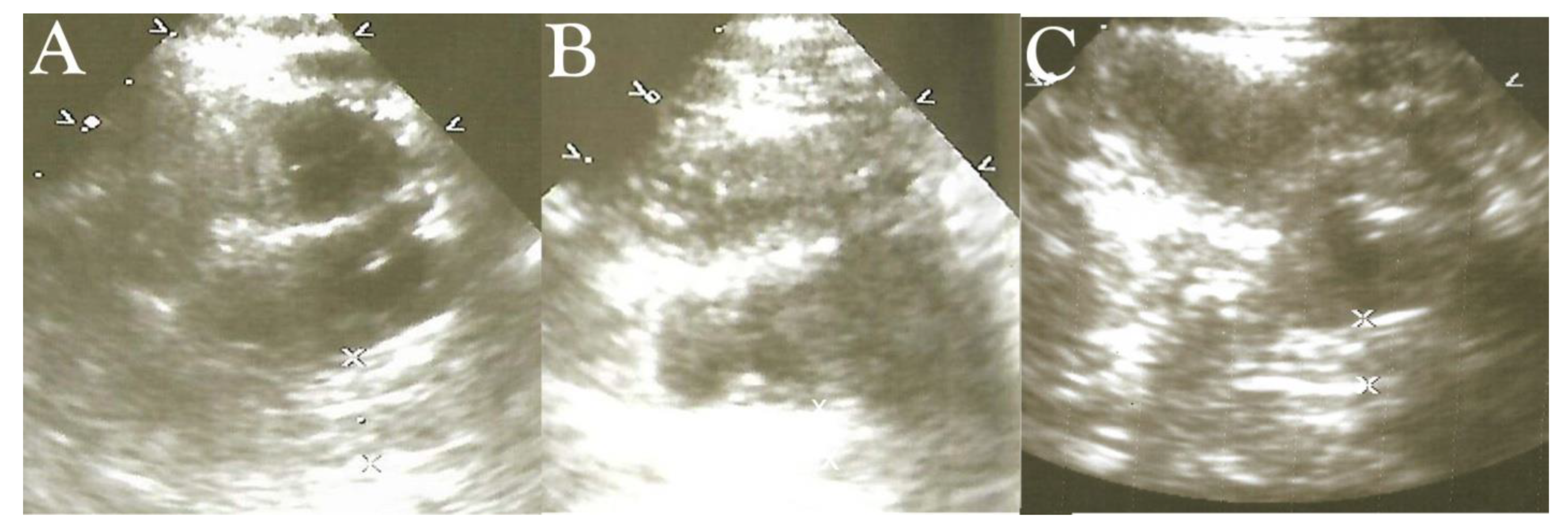
Figure 2.
(A-B) displays the pre-treatment image [Figure 2A] of the sigmoid colon and rectum with abundant HFF (black arrowhead), highly echogenic increased wall thickness. The post-treatment image [Figure 2B] reveals reduced wall thickness and echogenicity and absent HFF in the sigmoid colon (black arrowhead).
Figure 2.
(A-B) displays the pre-treatment image [Figure 2A] of the sigmoid colon and rectum with abundant HFF (black arrowhead), highly echogenic increased wall thickness. The post-treatment image [Figure 2B] reveals reduced wall thickness and echogenicity and absent HFF in the sigmoid colon (black arrowhead).
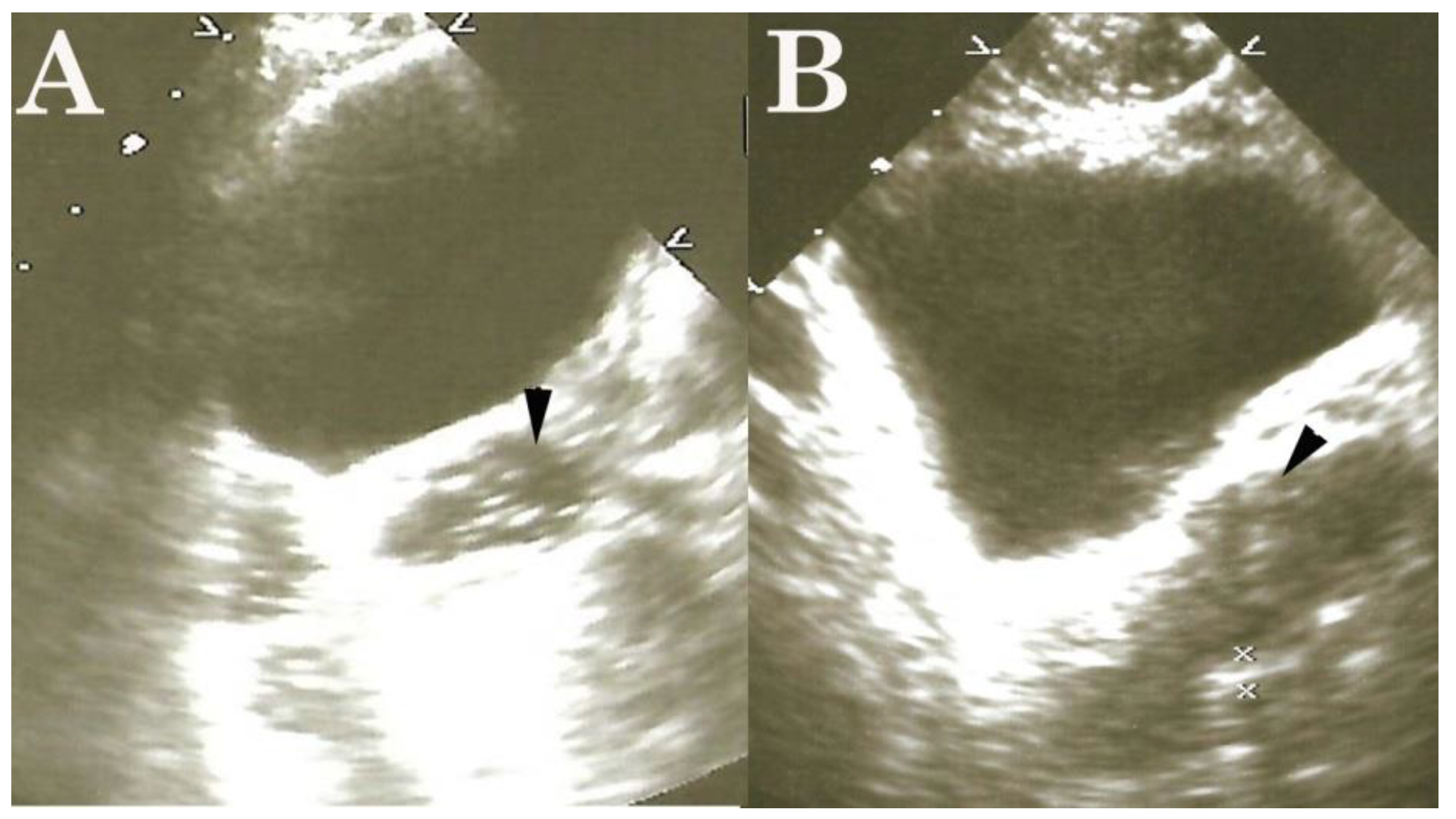
Figure 3.
(A-C) shows the pre-treatment images [Figure 3 A-B], obtained during colonoscopy, show bleeding sites [Figure 3A] in the descending colon. Figure 3C summarizes the sequence of events implicated in the ‘leaky intestine’.
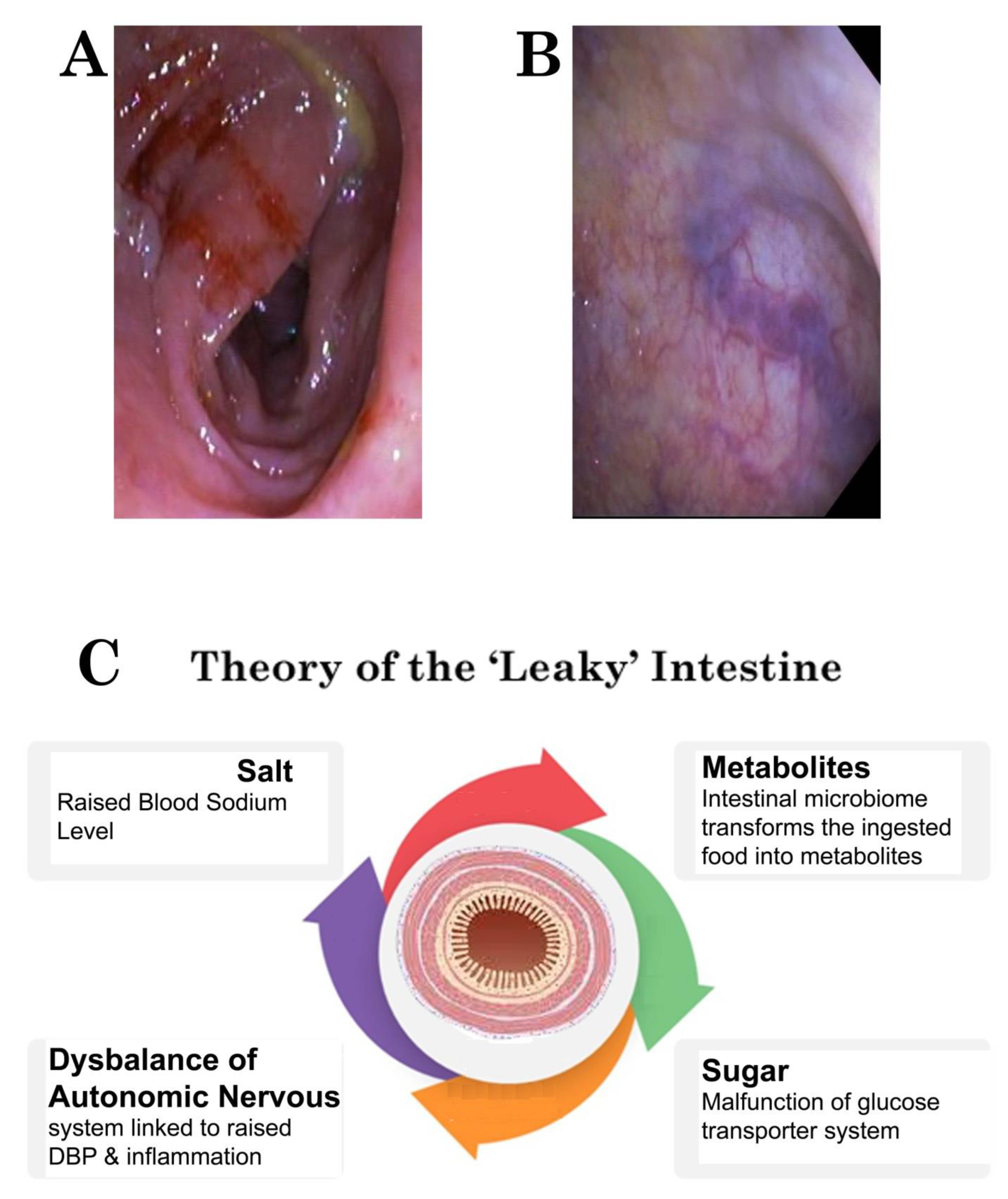
Figure 4.
shows the pathogenetic steps implicated in the development of a ‘leaky intestine’.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



