
Submitted:
03 July 2023
Posted:
04 July 2023
You are already at the latest version
Abstract
The aim of this study was to measure the effects on 3D active cervical Range of Motion (ACROM) and perceived pain of a n elastic taping (ET) application in the cervical area. Thirty participants (n: 22M and 8F, age 35.4±4.4 years; body height 173.1±8.4 cm; body mass 73.5±12.8 kg) for the study group (SG) and twenty subjects (n: 11M and 9F, age 32.6±3.9 years; body height 174.9±10.9 cm; body mass 71.2±12.9 kg) for the control group (CG) were recruited. All subjects were symptomatic for neck and cervical pain in baseline condition. Each group performed on ACROM test and the perceived pain on neck basing as Numerical Rating Scale (NRS 0-10, a.u.): at the baseline (T0); after 20' from ET application (T1); after three days of wearing the ET application (T2). Between T0 and T1 an ET was applied on the cervical area of the SG participants. Statistical analysis did not show any significant change in CG in any measurement session for ACROM and neck pain parameters. Conversely, the SG showed significant improvements for ACROM rotation left (T0 64.8 ± 7.7° - T2 76.0 ± 11.1° p < 0.000) and right (T0 66.0 ± 11.9° - T2 74.2 ± 9.6° p < 0.000); lateral inclination left (T0 37.5 ± 6.9° - T2 40.6 ± 10.8° p < 0.000) and right (T0 36.5 ± 7.9° - T2 40.9 ± 5.2° p < 0.000); flexion posterior (T0 47.0 ± 12.9° - T2 55.1 ± 12.3° p < 0.001) and anterior (T0 55.0 ± 3.6° - T2 62.9 ± 12.0° p < 0.006). A significant decrease was measure also in SG for pain NRS between T0 and T2 (T0 7.5 ± 1.0° - T1 5.5 ± 1.4 - T2 1.4 ± 1.5° p < 0.000). In conclusion, the results of this study underline the usefulness of a bilateral and symmetrical ET cervical application in terms to enhance multiplanar ACROM and to reduce subjective self-perceived cervical pain when it is needed. These findings can be applied for managing musculoskeletal health of different kind of individuals.
Keywords:
Cervical ROM
; elastic taping
; neck pain
; kinesiology
; 3D motion analysis
1. Introduction
The cervical spine, consisting of seven vertebras, is known for its exceptional mobility within the spinal column. It plays a crucial role in facilitating multiplanar movements of the head in space. Specifically, the motion of the cervical spine and head complex can be categorized into right-left rotation, lateral inclination, and posterior and anterior flexion [1]. These movements can be performed individually on a single anatomical plane or in a three-dimensional and multiplanar manner, depending on the functional demands of the environment.
Given these unique characteristics, preserving the physiological active range of motion (ACROM) of the cervical spine becomes a significant challenge in daily life, particularly in sports and various activities, as it contributes to maintaining optimal health [2,3]. Numerous factors can impede and restrict the ACROM, including traumatic injuries, repetitive movements, occupational practices, prolonged postures, head positioning, and other factors [4,5,6,7,8]. Diminished ACROM can have various detrimental effects on the musculoskeletal system, affecting the use of the eyes, other spinal segments, shoulder mobility, and more. Additionally, a reduced ACROM is a common observation among individuals experiencing neck pain [9,10,11,12,13].
In light of this context, two primary considerations arise: 1) the need for a comprehensive evaluation of ACROM, and 2) the implementation of effective strategies to enhance it.
Regarding ACROM assessment, professionals have the option to conduct tests with or without devices [14]. Qualitative analyses without devices are cost-effective and straightforward, but there is no change to compare data over time [15]. Within the realm of instrument-based evaluation, various solutions exist, including video analysis and 3D motion capture systems. However, these methods are more suited for analyzing posture and complex movements in specific contexts [16,17,18]. As a result, the most commonly utilized and practical approach involves the use of inertial sensors [3,19,20,21,22].
These tools enable professionals to accurately measure ACROM in a convenient and efficient manner, without causing discomfort to the subjects. Typically, an inertial sensor is positioned on the subject's forehead and moves in conjunction with the head, capturing angles and range of motion during active movements [19,20,21,22].
Turning to strategies for preserving and improving ACROM, multiple approaches can be considered, such as reducing screen time, minimizing sedentary behavior, receiving massages, engaging in targeted exercises, utilizing cupping techniques, and employing elastic taping [23,24,25,26,27]. Among these solutions, elastic taping (ET) possesses a distinctive characteristic: it can be worn directly on the skin for an extended period, continuously working 24 hours a day and adapting to the subject's movements until removal. This unique characteristic makes ET a valuable and practical tool not only for sports and athletes [28,29], but also for individuals in their daily lives.
Based on current knowledge, the effectiveness of ET applications in reducing neck pain and improving ACROM has been demonstrated [30,31,32]. However, there is a lack of data on the immediate and short-term effects of a single bilateral and symmetrical ET application worn for three days by video terminal workers experiencing neck pain and restricted ACROM. It is reasonable to hypothesize that wearing the same ET application for three days can have beneficial effects on cervical pain and ACROM outcomes in video terminal workers. Therefore, the objective of this research was to assess the immediate and short-term impact of a single bilateral and symmetrical ET application on self-perceived pain and multiplanar motion of the cervical spine, as measured using an inertial sensor.
2. Materials and Methods
2.1. Design and Participants
This study utilized a short-term longitudinal small-cohort design with repeated measures. The participants were recruited from employees of a call center located in the south of Italy. Voluntary participation was sought, and specific selection criteria were applied, including: 1) individuals experiencing chronic and recurrent self-perceived musculoskeletal cervical pain, and 2) individuals working as video terminal operators.
A total of 60 participants were recruited and randomly assigned to either the study group (SG) or the control group (CG), ensuring a balanced distribution. However, 10 participants dropped out during the course of the study, resulting in a final sample size of 50 participants who completed the experiment (Figure 1). The SG comprised 30 participants (n: 22M and 8F, age 35.4 ± 4.4 years; body height 173.1 ± 8.4 cm; body mass 73.5 ± 12.8 kg), while the CG included 20 participants (n: 11M and 9F, 32.6 ± 3.9 years; body height 174.9 ± 10.9 cm; body mass 71.2 ± 12.9 kg). A power analysis was performed, indicating that a sample size of 20 and 30 subjects per group respectively would provide 80% power, with a 5% error probability and an effect size of 0.55. Prior to the intervention phase, all participants were thoroughly informed about the study and provided voluntary consent. Privacy criteria were also strictly adhered to. The study received approval from the Ovidius University of Constanta, Number 78, dated 27th January 2023, in accordance with the principles outlined in the Helsinki Declaration.
2.2. Instrumentation
The assessment of multiplanar ACROM was conducted using an inertial sensor (Moover®, Sensor Medica, Guidonia-RM, Italy) positioned in the middle of the forehead and secured with an elastic band (Figure 2).
To ensure the accuracy and validity of the inertial sensor, a preliminary comparison was made using a six 3-dimensional camera optoelectronic system (SMART DX, BTS Bioengineering, Garbagnate Milanese, Italy), which served as the gold standard. A convenience sample of nineteen subjects participated in this trial, performing ACROM tests using the inertial sensor with a passive reflective marker attached to it. The data obtained from the Moover® sensor did not show any statistically significant differences when compared to the 3D kinematic data. Further details can be found in Appendix A.
Self-perceived cervical pain was evaluated using a Numerical Rating Scale (NRS, 0-10), with 0 representing the absence of pain and 10 indicating the highest level of sustainable pain.
For the ET application, two personalized strips of Taping Elastico® (ATS, Arezzo - AR, Italy) were used for each subject in the SG. The application procedures are described in the subsequent section.
2.3. Procedure and Data Collection
The testing procedures were conducted in a dedicated room within the participants’ working place, maintaining a mean temperature of 19 °C and a mean relative humidity of 52%. To minimize the potential influence of circadian effects, each subject underwent testing at the same time of day, as is customary in laboratory procedures of this nature [33,34,35]. The study consisted of three test sessions (T0-T1-T2), with a preliminary familiarization session conducted one week prior to the start of the protocol to provide instructions to the participants. T0 served as the baseline assessment, T1 as the acute assessment taken 20 minutes after the application of the ET on the cervical area, and T2 as the short-term assessment conducted after three days of wearing the ET application (Figure 3). T0 and T1 assessments were performed on the same day. Both SG and CG underwent the three test sessions in the same order. The CG received no intervention between T0 and T1, as well as between T1 and T2.
Each test session (T0-T1-T2) consisted of two evaluations performed in the following sequence: 1) assessment of perceived cervical pain using a 0-10 Numerical Rating Scale (NRS), and 2) measurement of ACROM using an inertial sensor.
The NRS was printed on a white paper, and each subject marked an "X" on the score corresponding to their self-perceived pain in the cervical area.
The assessment of multiplanar ACROM involved measuring angular motions in three directions: right-left rotation on the transversal plane, right-left lateral inclination on the frontal plane, and posterior-anterior flexion on the sagittal plane (Figure 4). Each test included a total of 14 movements, with 7 repetitions performed for each direction (right-left and posterior-anterior). The maximum and minimum values were excluded, and the average value was calculated.
The ET application was administered by a skilled operator immediately after T0. The same operator applied the ET for all subjects in the study group (SG). The ET application followed the Taping Elastico® Method (ATS, Arezzo, Italy) and was applied symmetrically on both sides of the cervical area [36]. A strip of tape was cut in a "Y" shape, with the anchor applied to the skin at the level of the acromion, and the two tails directed towards the base of the head. One tail followed the upper trapezius direction on the lateral portion of the neck, while the other was applied to the posterior portion (Figure 5). During the application, participants inclined their heads to the opposite side, stretching the skin. The ET was applied with zero tension, aiming to create convolutions when the head was in a neutral position. The ET application was bilateral and symmetrical.
After the ET application, participants in the SG waited for 20 minutes while wearing the application before proceeding to the next test session (T1). The control group (CG) observed the same time between T0 and T1 without any intervention. Participants in the SG continued to wear the ET for three days during their daily activities. They were instructed to be cautious during dressing and washing to minimize the possibility of dislodging the ET. No instances of detachment were reported until T2. On the third day, one hour prior to the final test session (T2), the operator removed the ET.
2.4. Statistical Analysis
The normality of the data was assessed using the Shapiro-Wilk's test. As the data followed a normal distribution, parametric tests were employed for the analysis. Differences at baseline were tested with a t-test for independent samples. A mixed ANOVA design (Time x Group) for repeated measures with Bonferroni correction was used to compare the post-hoc effects. Effect sizes (partial eta squared, ) were also calculated to facilitate interpretation of the results, with values of 0.01, 0.06, and above 0.15 indicating small, medium, and large effect sizes, respectively. The significance level was set at p = 0.05, and the statistical analysis was performed using SPSS (SPSS Inc., Chicago, IL, USA).
3. Results
The statistical analysis revealed no significant differences between SG and CG at T0 for any of the parameters measured. A Time x Group significant interaction was measured for all the ACROM directions as well as for self-perceived pain; indicating that the changes in ROM and pain over time are not the same across the two groups (Table 1).
The CG did not exhibit any significant differences in any parameter at any time point. However, the SG demonstrated a significant increase in all ACROM values at T2 compared to T0 (Table 2). Additionally, self-perceived pain in the cervical area was significantly lower at T2 compared to T0. Significant differences were also observed between T0 and T1, as well as between T1 and T2. Table 2 provides a detailed overview of the results.
The ET application resulted in increased ACROM in all directions after three days of wearing. However, significant increases were observed specifically in left rotation and anterior flexion even after just 20 minutes of wearing. Additionally, when comparing the measurements taken at T1 and T2, all ACROM directions, except for posterior flexion, showed a significant increase (Figure 6).
Furthermore, the self-perceived cervical pain exhibited a significant decrease both after 20 minutes and after three days of wearing the ET application. Notably, there was also a significant difference in pain levels between T1 and T2 (Figure 7).
4. Discussion
The primary objective of this study was to evaluate the immediate and short-term impact of an ET application to the cervical area on self-perceived pain and multiplanar motion of the cervical spine, as assessed using an inertial sensor. The novelty of this investigation lies in examining the short-term effects of a bilateral and symmetrical ET application on ACROM. Additionally, investigating the effects of ET on pain is of great interest to healthcare professionals, given the chronic nature of cervical pain and its substantial societal costs [37,38,39]. Moreover, cervical pain is recognized as one of the leading causes of global disability, placing it among the top five contributors [40].
Previous research conducted by Erdoğanoğlu et al. [30] with a similar study design demonstrated that wearing an ET application for 24 hours resulted in a significant reduction in neck pain and improved ACROM. However, it is important to note that this previous study only included symptomatic individuals with cervical pain and lacked a control group, and the observed effects were limited to a 24-hour timeframe. In contrast, the present study also included symptomatic individuals but incorporated a control group and extended the measurement period by two days using a single ET application. This represents a significant advancement in the scientific evidence supporting the application of ET. Another study by Alahmari et al. [31] investigated the effects of ET application for more than three days, extending up to seven days, but employed a different application technique and did not measure ACROM. Additionally, Ay et al. [32] demonstrated the effectiveness of five ET applications over a two-weeks period in reducing neck pain and improving ACROM. While their study employed a similar ET application method to our research, the ET shape, location, and unilateral application differed.
The findings of the present study align with previous literature, supporting the immediate effects of ET on perceived pain and ACROM. Particularly noteworthy is the significant reduction in perceived pain after 20 minutes of ET application in the SG (7.5 ± 1.0 and 5.5 ± 1.4 at T0 and T1, respectively, p < 0.000). Moreover in the same time span, there was a significant increase in ACROM for left rotation (64.8 ± 7.7° and 70.4 ± 12.5° at T0 and T1, respectively, p = 0.041) and anterior flexion (55.0 ± 3.6° and 61.7 ± 12.8° at T0 and T1, respectively, p = 0.007). These immediate improvements in anterior flexion and pain reduction confirm the positive effects of ET application. It is well recognized that individuals with cervical pain and disorders often experience limitations in anterior flexion, making these findings particularly relevant [9,10,11,12,13].
From a practical and professional standpoint, the most notable finding of this study is undeniably the short-term effect observed after three days of using a single bilateral ET application. It is widely acknowledged that ET applications cannot be worn for extended periods due to factors such as personal hygiene practices, perspiration, and clothing changes. Consequently, it is common practice among healthcare professionals to remove and replace the ET application every three or four days [32,36]. The results of this study validate these procedural recommendations, demonstrating a substantial effect lasting for three days with a single ET application, without the need for removal and replacement.
For each direction of ACROM, a significant average improvement of 15% was observed between T0 and T2. Particularly noteworthy were the higher relative improvements observed in two specific directions: left rotation (64.8 ± 7.7° and 76.0 ± 11.1° at T0 and T2, respectively, p < 0.001) and posterior flexion (47.0 ± 12.9° and 55.1 ± 12.3° at T0 and T2, respectively, p < 0.001). These directions demonstrated a remarkable 17% increase in ACROM following three days of ET application. Furthermore, self-perceived pain exhibited a substantial average decrease of -81% between T0 and T2 (7.5 ± 1.0 and 1.4 ± 1.5, p < 0.001, respectively).
One crucial aspect that deserves discussion in this paper is the different approach employed in this research compared to previous studies. While previous studies applied tension to the ET [30,31], with one exception that used a similar application method but a different placement and shape [32], in this study, the ET was applied without tension while stretching the skin during application (by inclining the head on the opposite side). This technique allowed for the formation of skin convolutions when the head and neck were in a neutral position. It is important to note that the two methods of application (with tension and without tension) differ significantly in terms of the pressure exerted on the skin. Although skin convolutions are thought to enhance local blood flow, the available data do not strongly support this claim [41,42,43]. While there are various studies on lower back pain that indicate no significant effects or differences between elastic taping applications with or without convolutions [44,45], there is a lack of similar data for the cervical area; except for the research conducted by Ay et al. [32]. They demonstrated that both convoluted and non-convoluted ET applications are effective in reducing neck pain and improving ACROM. Thus, the present study can be considered one of the first to use a bilateral and symmetrical ET application on the cervical area for three consecutive days, assessing its effects on self-perceived pain and ACROM. It is intriguing to hypothesize how two vastly different methods of ET (with tension and without tension) can yield similar results in terms of pain relief and cervical motion. A plausible explanation can be found in the existing literature, which suggests that the actual effect of ET can be attributed to both the direct contact itself and the pressure gradient generated between the taping and the surrounding skin area [46]. This idea is based on the findings of Pamuk et al. [47], which discuss the effects of ET on the underlying tissues, both at the immediate application site and in more distant regions. However, it should be noted that the latter explanation remains a hypothesis, and further research is required to elucidate this phenomenon.
Limitations
Like any scientific study, this study also has certain limitations that need to be acknowledged. One notable limitation is the inability to conduct additional test sessions following a three-day washout period of ET. Consequently, the findings of this paper are specific to the immediate and short-term effects of ET, and information regarding its longer-term effects is currently unavailable. Future research should aim to replicate the study protocol while incorporating a fourth and fifth test session to assess changes in self-perceived pain and multiplanar ACROM after ET removal. Since the restoration of muscle function is considered essential in the treatment of cervical spine disorders [15], it would be highly valuable to investigate further whether ET application can be regarded as beneficial for muscle function restoration.
5. Conclusions
Inertial sensors can be considered a suitable tool for proper measurement of multiplanar motion of cervical spine (ACROM). In summary, the results of this study underline the usefulness of a bilateral and symmetrical ET cervical application in terms to enhance multiplanar ACROM and to reduce subjective self-perceived cervical pain when it is needed. These results can find practical applications in various fields, from managing musculoskeletal health of computer workers to high-level sports.
Author Contributions
Conceptualization, L.R. and T.P.; methodology, L.R.; software, L.R. and P. B.; validation, J.P.; formal analysis, L.R.; investigation, T.P.; resources, A.L. and G.M.M.; data curation, L.R.; writing—original draft preparation, L.R.; writing—review and editing, L.R. and J.P.; visualization, G.M.M.; supervision, J.P.; project administration, L.R. A.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Ovidius University of Constanta (n. 78, January 27, 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Acknowledgments
The Authors are grateful to FGP s.r.l. (Dossobuono, Verona, Italy) for the possibility to use the biomechanics laboratory in which the validation of the inertial sensors was performed using the six 3-dimensional cameras optoelectronic system.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
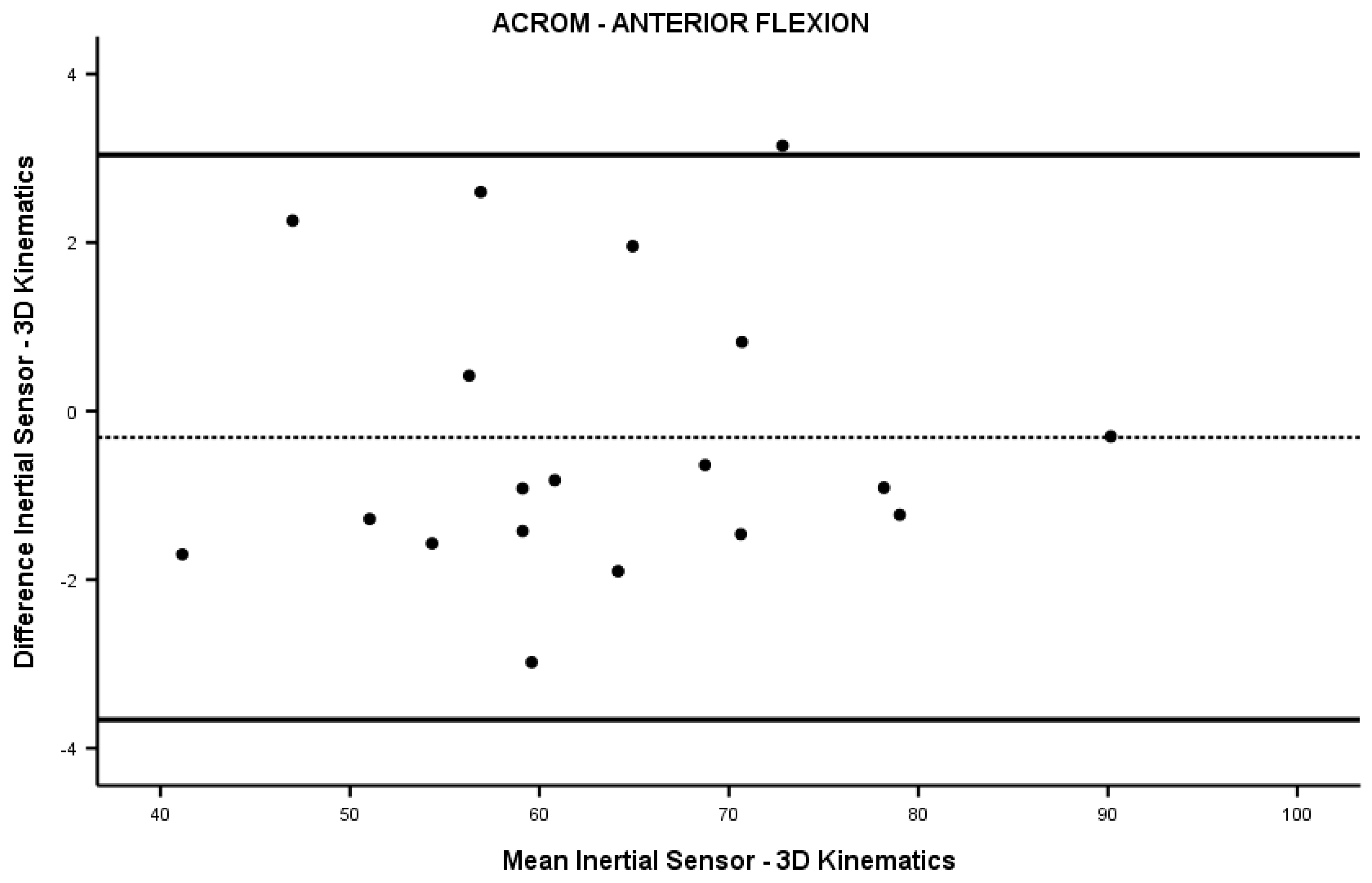
The Appendix A contains the data referred to the test session conducted to validate the Moover® inertial sensor in comparison to the 3D kinematics system. Table A1 presents a summary of the data obtained from the convenience sample. Table A2 provides the statistical analysis, while Figure A1, Figure A2, Figure A3, Figure A4, Figure A5 and Figure A6 depict the Bland-Altman graphs for each tested direction. These findings contribute to the assessment of the accuracy and validity of the inertial sensor in measuring multiplanar ACROM.

Table A1.
Anthropometric of the sample (11M; 8 F).
| Variables | Mean (SD) |
|---|---|
| Age (years) | 36.4 (7.3) |
| Body Height (cm) | 172.5 (7.8) |
| Body Mass (kg) | 73.3 (19.3) |
Table A2.
Statistical comparison of the ACROM inertial sensor angular measures vs 3D kinematics.
| Parameter | Inertial sensor Mean (SD) |
3D Kinematics Mean (SD) |
Z score | p value |
|---|---|---|---|---|
| Right rotation (°) | 72.1 (11.7) | 74.5 (11.6) | -0.818 | 0.414 |
| Left rotation (°) | 75.9 (8.5) | 76.8 (9.2) | -0.336 | 0.737 |
| Right lateral inclination (°) | 44.0 (7.9) | 46.2 (10.0) | -0.744 | 0.457 |
| Left lateral inclination (°) | 44.9 (7.2) | 45.0 (6.4) | -0.248 | 0.804 |
| Posterior flexion (°) | 59.0 (10.0) | 59.5 (10.9) | -0.044 | 0.965 |
| Anterior flexion (°) | 63.2 (12.0) | 63.6 (11.9) | -0.248 | 0.804 |
Due to the sample numerosity a Mann-Whitney test was used to compare the data collected with the two measurement systems. No significant differences were measured in ACROM between the two measuring systems in any tested direction.
Figure A1.
Bland-Altman graph for ACROM right rotation.
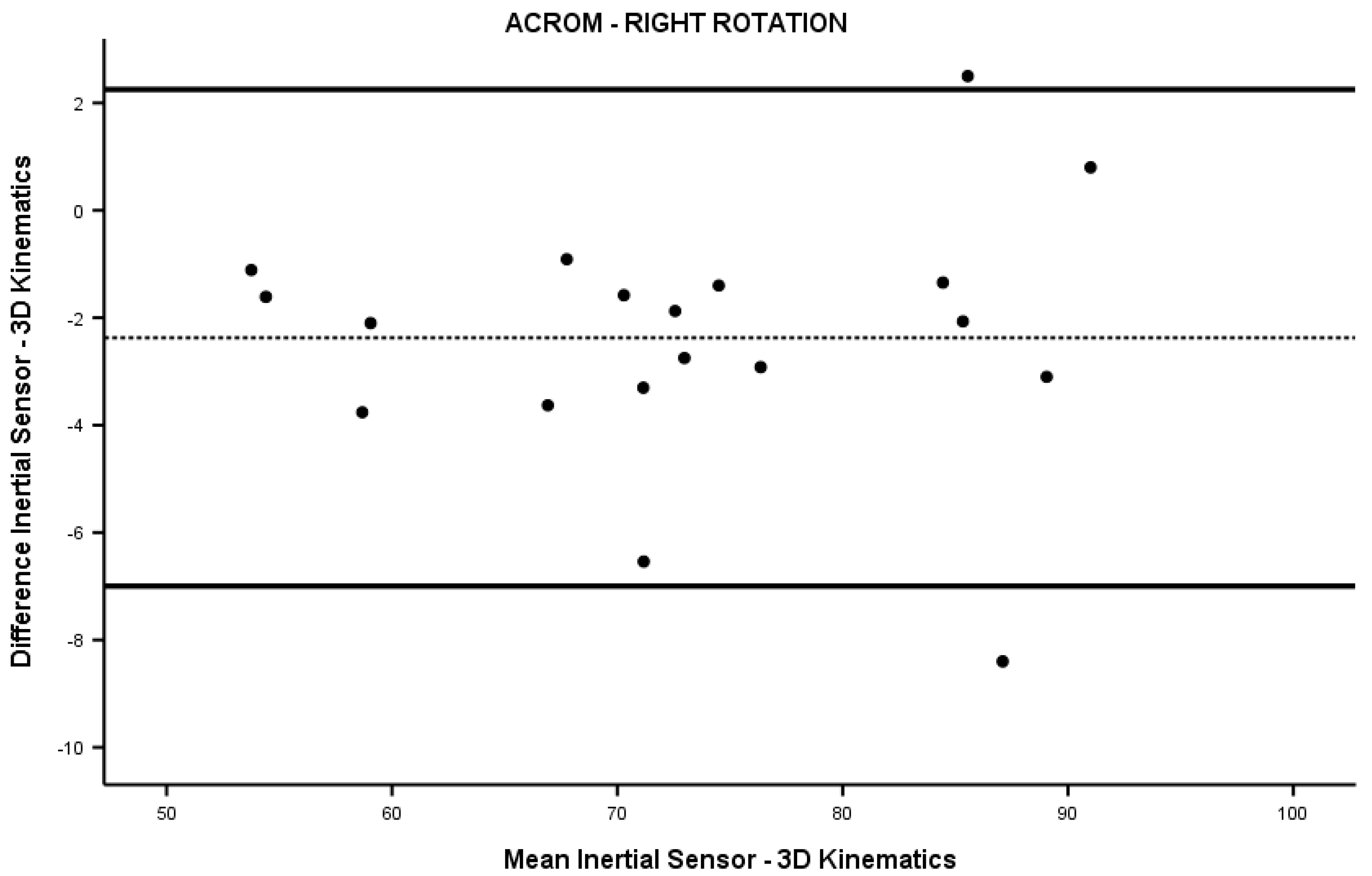
Figure A2.
Bland-Altman graph for ACROM left rotation.
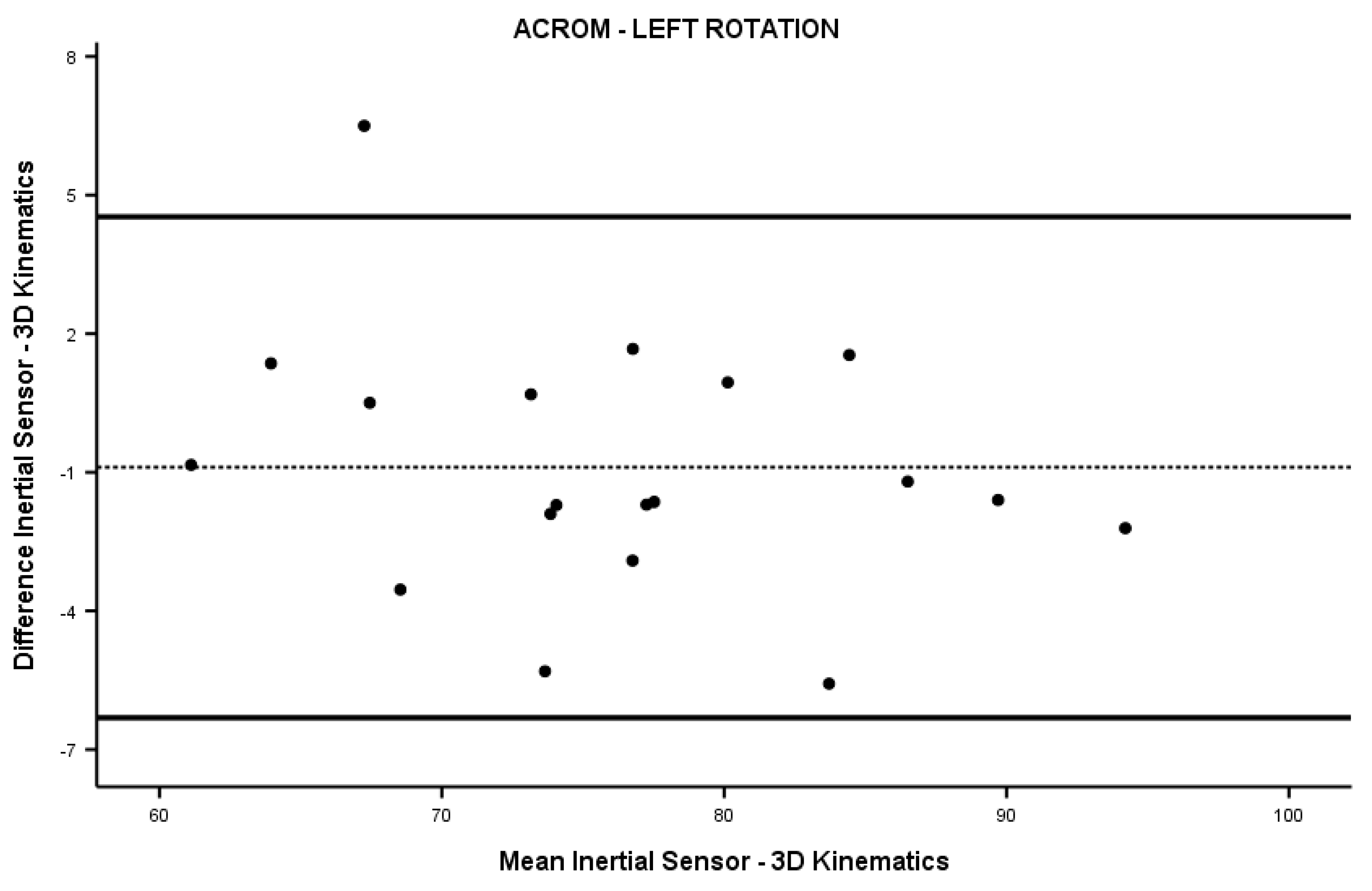
Figure A3.
Bland-Altman graph for ACROM right lateral inclination.
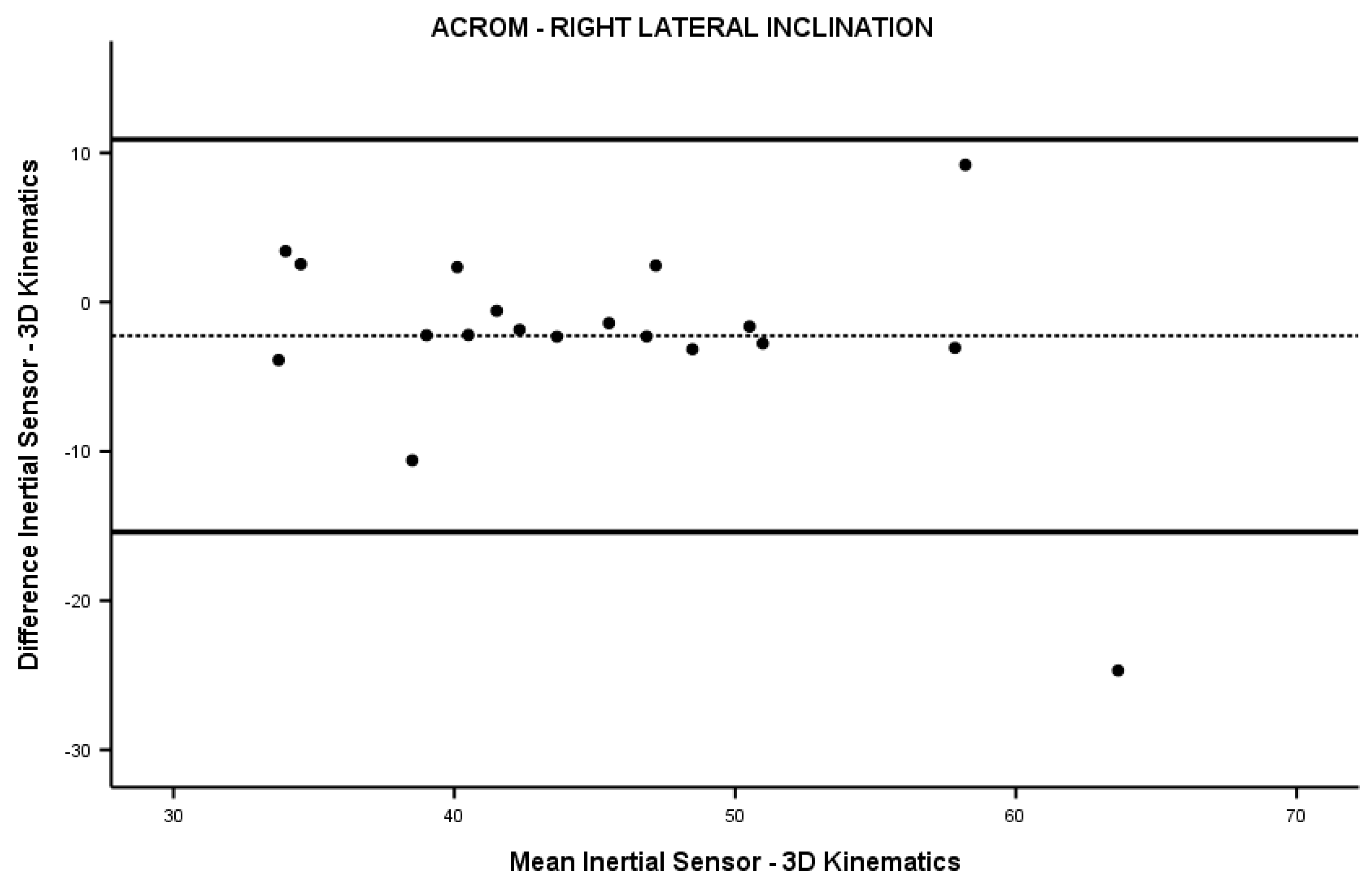
Figure A4.
Bland-Altman graph for ACROM left lateral inclination.
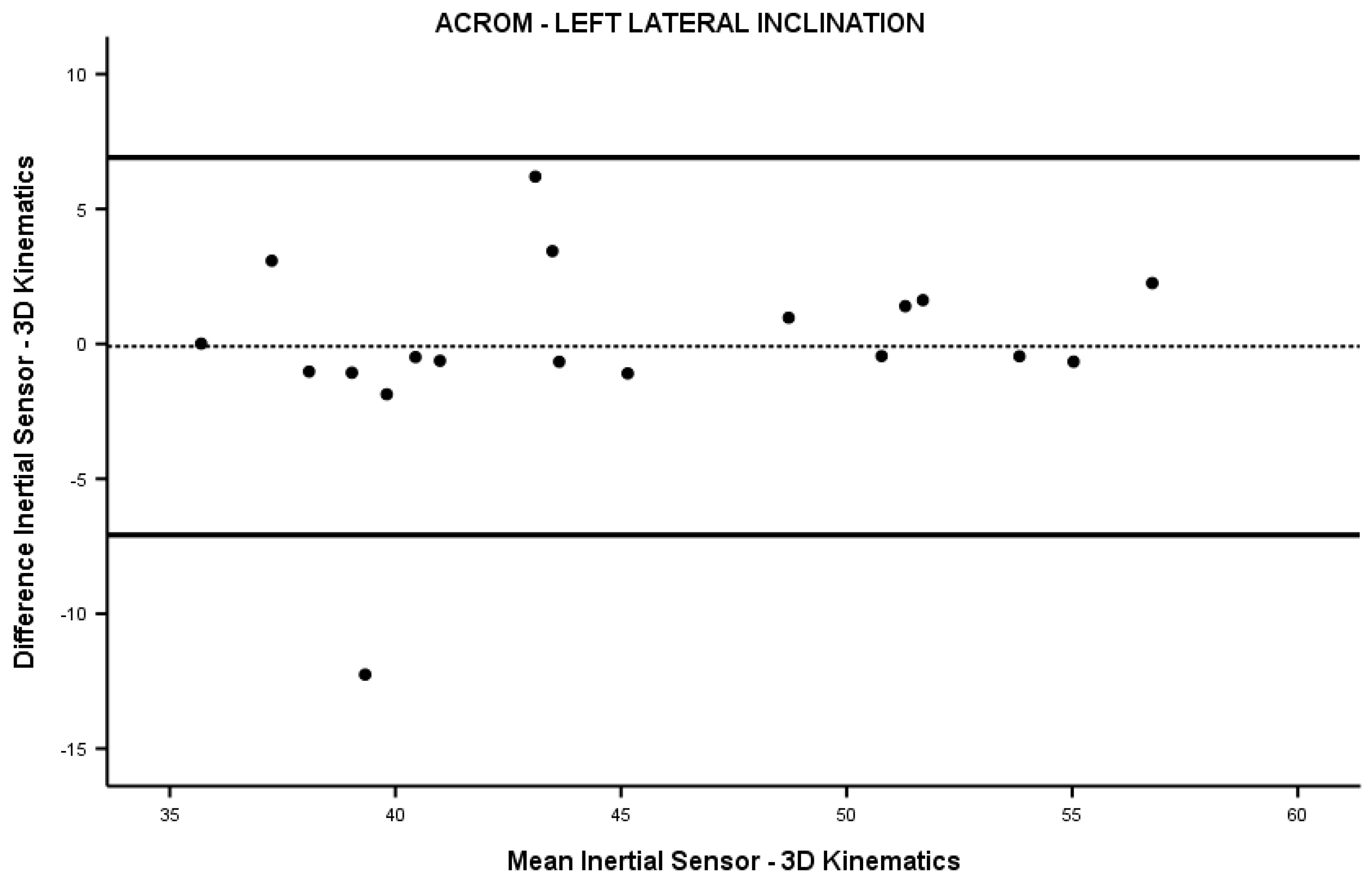
Figure A5.
Bland-Altman graph for ACROM posterior flexion.
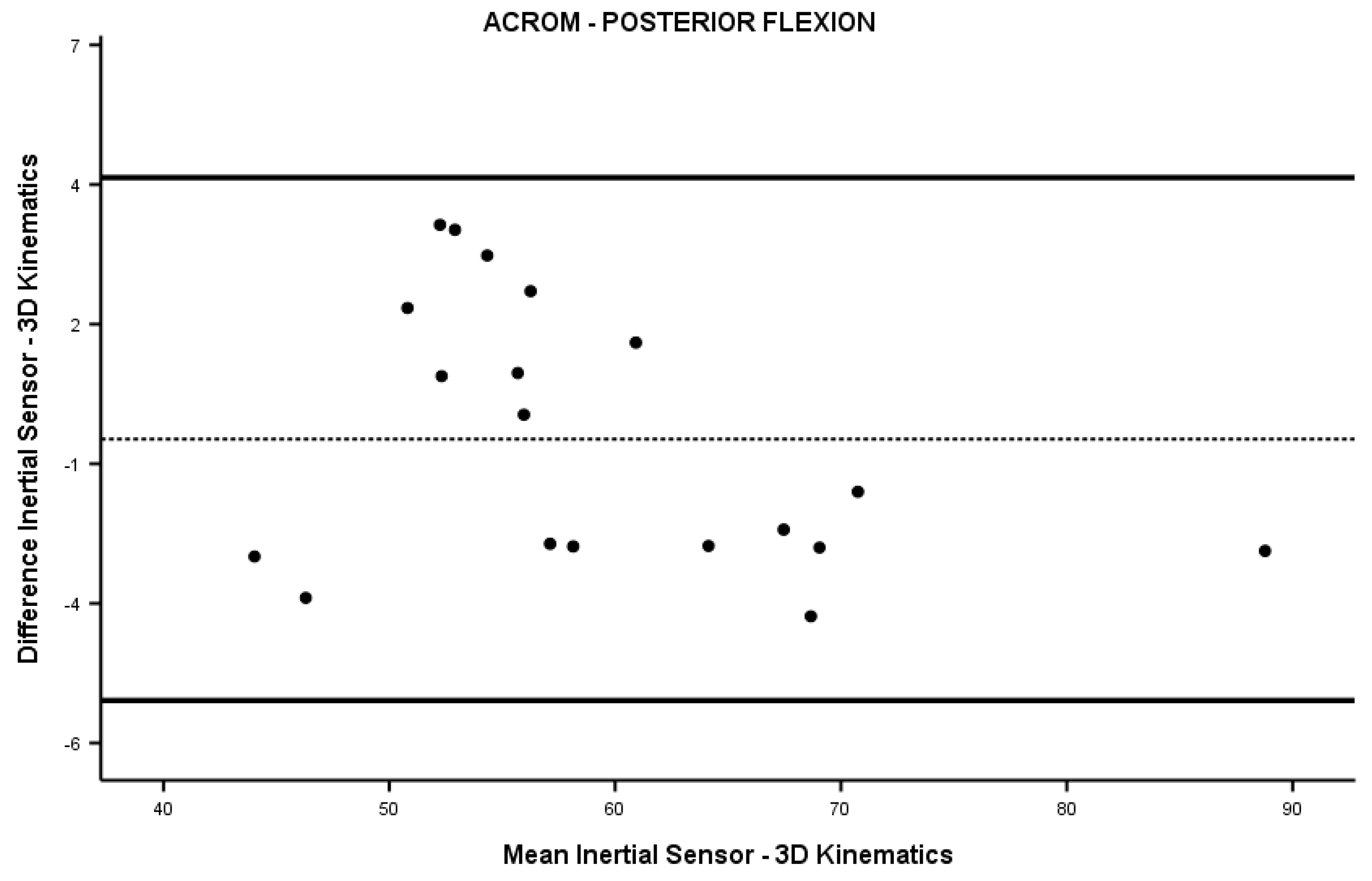
Figure A6.
Bland-Altman graph for ACROM anterior flexion.
References
- Bogduk, N.; Mercer, S. Biomechanics of the Cervical Spine. I: Normal Kinematics. Clin Biomech (Bristol, Avon) 2000, 15, 633–648. [Google Scholar] [CrossRef]
- Shugg, J.A.J.; Jackson, C.D.; Dickey, J.P. Cervical Spine Rotation and Range of Motion: Pilot Measurements during Driving. Traffic Inj Prev 2011, 12, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Thoomes-de Graaf, M.; Thoomes, E.; Fernández-de-las-Peñas, C.; Plaza-Manzano, G.; Cleland, J.A. Normative Values of Cervical Range of Motion for Both Children and Adults: A Systematic Review. Musculoskelet Sci Pract 2020, 49. [Google Scholar] [CrossRef] [PubMed]
- Dowdell, J.; Kim, J.; Overley, S.; Hecht, A. Biomechanics and Common Mechanisms of Injury of the Cervical Spine. Handb Clin Neurol 2018, 158, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.J.; Han, H.Y.; Cheon, S.H.; Park, S.H.; Yong, M.S. The Effect of Forward Head Posture on Muscle Activity during Neck Protraction and Retraction. J Phys Ther Sci 2015, 27, 977–979. [Google Scholar] [CrossRef]
- Cheon, S.H.; Park, S.H. Changes in Neck and Upper Trunk Muscle Activities According to the Angle of Movement of the Neck in Subjects with Forward Head Posture. J Phys Ther Sci 2017, 29, 191–193. [Google Scholar] [CrossRef] [PubMed]
- Gareiss, L.; Krumm, A.; Otte, A. [On Biomechanics of the Cervical Spine When Using a Smartphone]. MMW Fortschr Med 2020, 162, 10–14. [Google Scholar] [CrossRef]
- Johnston, V.; Jull, G.; Souvlis, T.; Jimmieson, N.L. Neck Movement and Muscle Activity Characteristics in Female Office Workers with Neck Pain. Spine (Phila Pa 1976) 2008, 33, 555–563. [Google Scholar] [CrossRef]
- Hagen, K.B.; Harms-Ringdahl, K.; Enger, N.O.; Hedenstad, R.; Morten, H. Relationship between Subjective Neck Disorders and Cervical Spine Mobility and Motion-Related Pain in Male Machine Operators. Spine (Phila Pa 1976) 1997, 22, 1501–1507. [Google Scholar] [CrossRef]
- Jordan, A.; Mehlsen, J.; Ostergaard, K. A comparison of physical characteristics between patients seeking treatment for neck pain and age-matched healthy people. J Manipulative Physiol Ther 1997, 20, 468–475. [Google Scholar]
- Woodhouse, A.; Vasseljen, O. Altered Motor Control Patterns in Whiplash and Chronic Neck Pain. BMC Musculoskelet Disord 2008, 9. [Google Scholar] [CrossRef] [PubMed]
- Stenneberg, M.S.; Rood, M.; de Bie, R.; Schmitt, M.A.; Cattrysse, E.; Scholten-Peeters, G.G. To What Degree Does Active Cervical Range of Motion Differ Between Patients With Neck Pain, Patients With Whiplash, and Those Without Neck Pain? A Systematic Review and Meta-Analysis. Arch Phys Med Rehabil 2017, 98, 1407–1434. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Nicholson, L.L.; Adams, R.D. Neck Muscle Endurance, Self-Report, and Range of Motion Data from Subjects with Treated and Untreated Neck Pain. J Manipulative Physiol Ther 2005, 28, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.A.; McCarthy, C.J.; Chorti, A.; Cooke, M.W.; Gates, S. A Systematic Review of Reliability and Validity Studies of Methods for Measuring Active and Passive Cervical Range of Motion. J Manipulative Physiol Ther 2010, 33, 138–155. [Google Scholar] [CrossRef]
- Jull, G.A.; O’Leary, S.P.; Falla, D.L. Clinical Assessment of the Deep Cervical Flexor Muscles: The Craniocervical Flexion Test. J Manipulative Physiol Ther 2008, 31, 525–533. [Google Scholar] [CrossRef]
- Belli, G.; Toselli, S.; Mauro, M.; Maietta Latessa, P.; Russo, L. Relation between Photogrammetry and Spinal Mouse for Sagittal Imbalance Assessment in Adolescents with Thoracic Kyphosis. J Funct Morphol Kinesiol 2023, 8, 68. [Google Scholar] [CrossRef]
- Russo, L.; Belli, G.; Di Blasio, A.; Lupu, E.; Larion, A.; Fischetti, F.; Montagnani, E.; Di Biase Arrivabene, P.; De Angelis, M. The Impact of Nordic Walking Pole Length on Gait Kinematic Parameters. J Funct Morphol Kinesiol 2023, 8, 50. [Google Scholar] [CrossRef]
- Di Giminiani, R.; Di Lorenzo, D.; La Greca, S.; Russo, L.; Masedu, F.; Totaro, R.; Padua, E. Angle-Angle Diagrams in the Assessment of Locomotion in Persons with Multiple Sclerosis: A Preliminary Study. Applied Sciences 2022, Vol. 12, Page 7223 2022, 12, 7223. [Google Scholar] [CrossRef]
- Raya, R.; Garcia-Carmona, R.; Sanchez, C.; Urendes, E.; Ramirez, O.; Martin, A.; Otero, A. An Inexpensive and Easy to Use Cervical Range of Motion Measurement Solution Using Inertial Sensors. Sensors (Basel) 2018, 18. [Google Scholar] [CrossRef]
- Elizagaray-García, I.; Gil-Martínez, A.; Navarro-Fernández, G.; Navarro-Moreno, A.R.; Sánchez-De-toro-hernández, J.; Díaz-De-terán, J.; Lerma-Lara, S. Inter, Intra-Examiner Reliability and Validity of Inertial Sensors to Measure the Active Cervical Range of Motion in Patients with Primary Headache. EXCLI J 2021, 20, 879–893. [Google Scholar] [CrossRef]
- Russo, L.; Giustino, V.; Toscano, R.E.; Secolo, G.; Secolo, I.; Iovane, A.; Messina, G. Can Tongue Position and Cervical ROM Affect Postural Oscillations? A Pilot and Preliminary Study. Journal of Human Sport and Exercise 2020, 15, S840–S847. [Google Scholar] [CrossRef]
- Theobald, P.S.; Jones, M.D.; Williams, J.M. Do Inertial Sensors Represent a Viable Method to Reliably Measure Cervical Spine Range of Motion? Man Ther 2012, 17, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Wood, S.; Fryer, G.; Tan, L.L.F.; Cleary, C. Dry Cupping for Musculoskeletal Pain and Range of Motion: A Systematic Review and Meta-Analysis. J Bodyw Mov Ther 2020, 24, 503–518. [Google Scholar] [CrossRef]
- Saavedra-Hernández, M.; Castro-Sánchez, A.M.; Arroyo-Morales, M.; Cleland, J.A.; Lara-Palomo, I.C.; Fernández-De-Las-Peñas, C. Short-Term Effects of Kinesio Taping versus Cervical Thrust Manipulation in Patients with Mechanical Neck Pain: A Randomized Clinical Trial. J Orthop Sports Phys Ther 2012, 42, 724–730. [Google Scholar] [CrossRef]
- Xiong, J.; Zhang, Z.; Zhang, Z.; Ma, Y.; Li, Z.; Chen, Y.; Liu, Q.; Liao, W. Short-Term Effects of Kinesio Taping Combined with Cervical Muscles Multi-Angle Isometric Training in Patients with Cervical Spondylosis. BMC Musculoskelet Disord 2023, 24. [Google Scholar] [CrossRef]
- Šiško, P.K.; Videmšek, M.; Karpljuk, D. The Effect of a Corporate Chair Massage Program on Musculoskeletal Discomfort and Joint Range of Motion in Office Workers. J Altern Complement Med 2011, 17, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Tsauo, J.Y.; Lee, H.Y.; Hsu, J.H.; Chen, C.Y.; Chen, C.J. Physical Exercise and Health Education for Neck and Shoulder Complaints among Sedentary Workers. J Rehabil Med 2004, 36, 253–257. [Google Scholar] [CrossRef]
- Williams, S.; Whatman, C.; Hume, P.A.; Sheerin, K. Kinesio Taping in Treatment and Prevention of Sports Injuries: A Meta-Analysis of the Evidence for Its Effectiveness. Sports Med 2012, 42, 153–164. [Google Scholar] [CrossRef]
- Russo, L.; Bartolucci, P.; Ardigò, L.P.; Padulo, J.; Pausic, J.; Iacono, A. Dello An Exploratory Study on the Acute Effects of Proprioceptive Exercise and/or Neuromuscular Taping on Balance Performance. Asian Journal of Sports Medicine 2018 9:2 2018, 9, 63020. [Google Scholar] [CrossRef]
- Erdoğanoğlu, Y.; Bayraklı, B. Short-Term Changes in Chronic Neck Pain After the Use of Elastic Adhesive Tape. J Chiropr Med 2021, 20, 70–76. [Google Scholar] [CrossRef]
- Alahmari, K.A.; Reddy, R.S.; Tedla, J.S.; Samuel, P.S.; Kakaraparthi, V.N.; Rengaramanujam, K.; Ahmed, I. The Effect of Kinesio Taping on Cervical Proprioception in Athletes with Mechanical Neck Pain-a Placebo-Controlled Trial. BMC Musculoskelet Disord 2020, 21. [Google Scholar] [CrossRef] [PubMed]
- Ay, S.; Konak, H.E.; Evcik, D.; Kibar, S. The Effectiveness of Kinesio Taping on Pain and Disability in Cervical Myofascial Pain Syndrome. Rev Bras Reumatol 2017, 57, 93–99. [Google Scholar] [CrossRef]
- Russo, L.; Montagnani, E.; Pietrantuono, D.; D’Angona, F.; Fratini, T.; Di Giminiani, R.; Palermi, S.; Ceccarini, F.; Migliaccio, G.M.; Lupu, E.; et al. Self-Myofascial Release of the Foot Plantar Surface: The Effects of a Single Exercise Session on the Posterior Muscular Chain Flexibility after One Hour. Int J Environ Res Public Health 2023, 20. [Google Scholar] [CrossRef] [PubMed]
- Russo, L.; Di Capua, R.; Arnone, B.; Borrelli, M.; Coppola, R.; Esposito, F.; Padulo, J. Shoes and Insoles: The Influence on Motor Tasks Related to Walking Gait Variability and Stability. Int J Environ Res Public Health 2020, 17, 1–12. [Google Scholar] [CrossRef]
- Russo, L.; D'Eramo, U.; Padulo, J.; Foti, C.; Schiffer, R.; Scoppa, F. Day-time effect on postural stability in young sportsmen. Muscles Ligaments Tendons J, 2015; 5, 38–42. [Google Scholar] [CrossRef]
- Russo, L.; Bartolucci, P. Taping Elastico® Applicazioni in Chinesiologia; ATS—Giacomo Catalani Editore: Arezzo, Italy, 2018. [Google Scholar]
- Korthals-de Bos, I.B.C.; Hoving, J.L.; Van Tulder, M.W.; Rutten-van Mölken, M.P.M.H.; Adèr, H.J.; De Vet, H.C.W.; Koes, B.W.; Vondeling, H.; Bouter, L.M. Cost Effectiveness of Physiotherapy, Manual Therapy, and General Practitioner Care for Neck Pain: Economic Evaluation alongside a Randomised Controlled Trial. BMJ 2003, 326, 911–914. [Google Scholar] [CrossRef]
- Driessen, M.T.; Lin, C.W.C.; Van Tulder, M.W. Cost-Effectiveness of Conservative Treatments for Neck Pain: A Systematic Review on Economic Evaluations. Eur Spine J 2012, 21, 1441–1450. [Google Scholar] [CrossRef]
- Aboagye, E.; Lilje, S.; Bengtsson, C.; Peterson, A.; Persson, U.; Skillgate, E. Manual Therapy versus Advice to Stay Active for Nonspecific Back and/or Neck Pain: A Cost-Effectiveness Analysis. Chiropr Man Therap 2022, 30. [Google Scholar] [CrossRef]
- Hoy, D.; March, L.; Woolf, A.; Blyth, F.; Brooks, P.; Smith, E.; Vos, T.; Jan, B.; Blore, J.; Murray, C.; et al. The Global Burden of Neck Pain: Estimates from the Global Burden of Disease 2010 Study. Ann Rheum Dis 2014, 73, 1309–1315. [Google Scholar] [CrossRef]
- Yang, J.M.; Lee, J.H. Is Kinesio Taping to Generate Skin Convolutions Effective for Increasing Local Blood Circulation? Med Sci Monit 2018, 24, 288–293. [Google Scholar] [CrossRef]
- Craighead, D.H.; Shank, S.W.; Volz, K.M.; Alexander, L.M. Kinesiology Tape Modestly Increases Skin Blood Flow Regardless of Tape Application Technique. J Perform Health Res, 1, https://www.scilit.net/article/e1fb961c060ad0d85a412149b7b4488f.
- Banerjee, G.; Briggs, M.; Johnson, M.I. The Immediate Effects of Kinesiology Taping on Cutaneous Blood Flow in Healthy Humans under Resting Conditions: A Randomised Controlled Repeated-Measures Laboratory Study. PLoS One 2020, 15. [Google Scholar] [CrossRef]
- Parreira, P. do C.S.; Costa, L. da C.M.; Takahashi, R.; Junior, L.C.H.; Junior, M.A.Ô. da L.; Silva, T.M. da; Costa, L.O.P. Kinesio Taping to Generate Skin Convolutions Is Not Better than Sham Taping for People with Chronic Non-Specific Low Back Pain: A Randomised Trial. J Physiother 2014, 60, 90–96. [Google Scholar] [CrossRef]
- Araujo, A.C.; do Carmo Silva Parreira, P.; Junior, L.C.H.; da Silva, T.M.; da Luz Junior, M.A.; da Cunha Menezes Costa, L.; Pena Costa, L.O. Medium Term Effects of Kinesio Taping in Patients with Chronic Non-Specific Low Back Pain: A Randomized Controlled Trial. Physiotherapy 2018, 104, 149–151. [Google Scholar] [CrossRef]
- Vercelli, S.; Colombo, C.; Tolosa, F.; Moriondo, A.; Bravini, E.; Ferriero, G.; Francesco, S. The Effects of Kinesio Taping on the Color Intensity of Superficial Skin Hematomas: A Pilot Study. Phys Ther Sport 2017, 23, 156–161. [Google Scholar] [CrossRef]
- Pamuk, U.; Yucesoy, C.A. MRI Analyses Show That Kinesio Taping Affects Much More than Just the Targeted Superficial Tissues and Causes Heterogeneous Deformations within the Whole Limb. J Biomech 2015, 48, 4262–4270. [Google Scholar] [CrossRef]
Figure 1.
Participants’ distribution into groups.
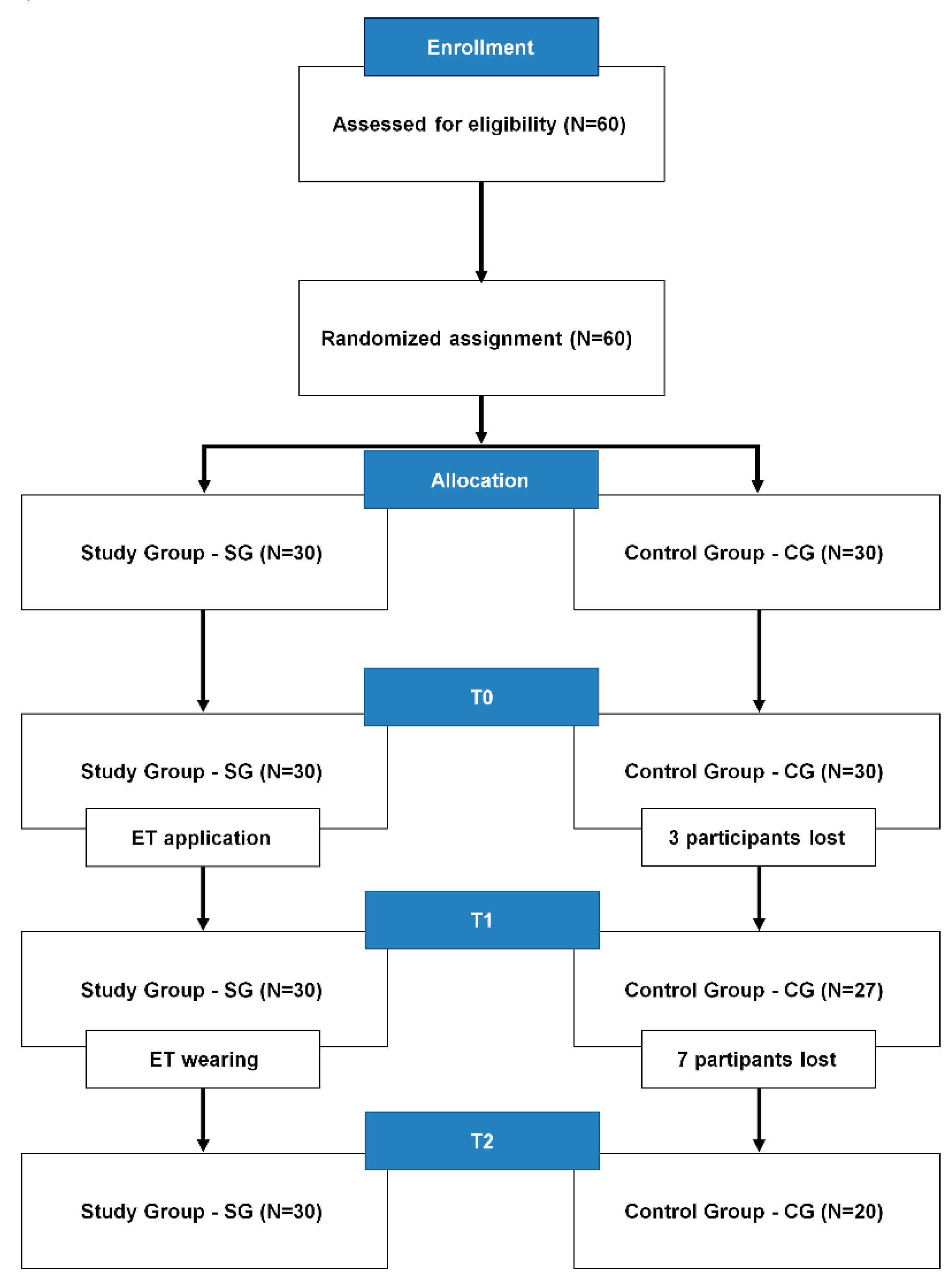
Figure 2.
Placement of the inertial sensor on the forehead for measuring of the multiplanar ACROM.

Figure 3.
Graphical description of procedures and study timeline.
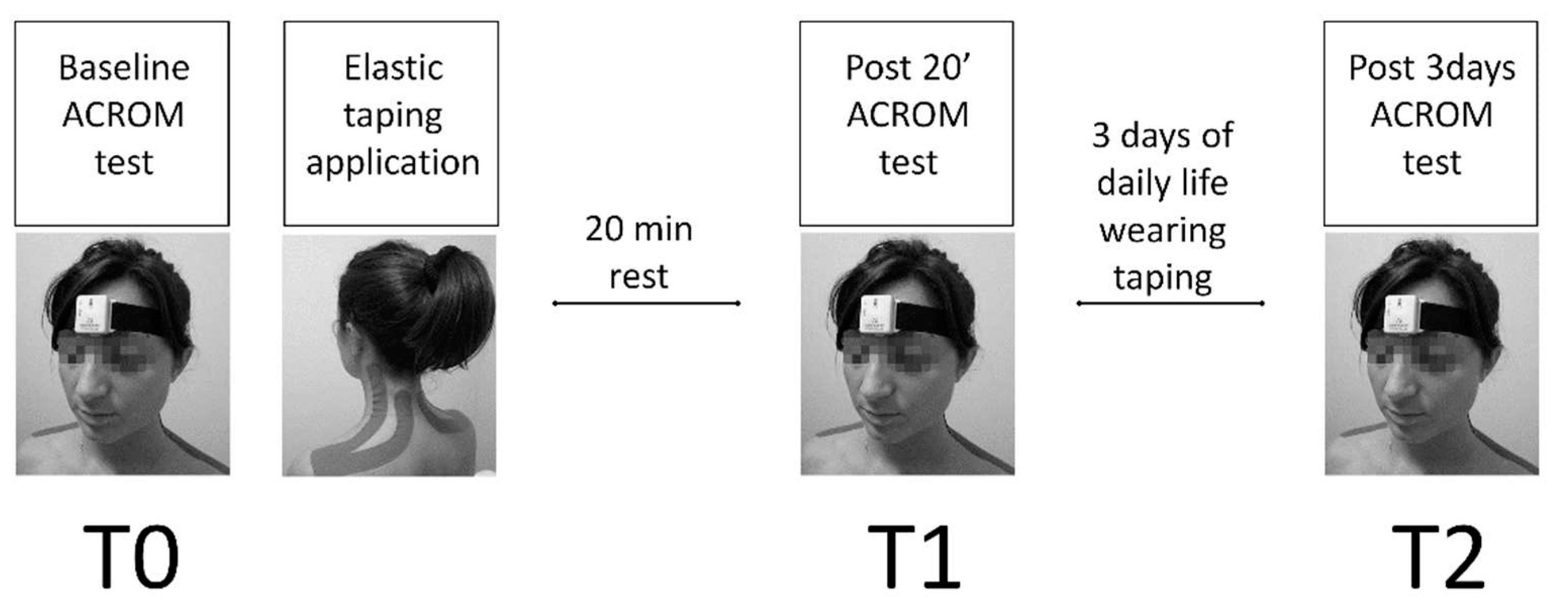
Figure 4.
ACROM directions and anatomical planes tested using the inertial sensor. A: right-left rotation on the transversal plane; B: right-left lateral inclination on the frontal plane; C: posterior-anterior flexion on the sagittal plane.
Figure 4.
ACROM directions and anatomical planes tested using the inertial sensor. A: right-left rotation on the transversal plane; B: right-left lateral inclination on the frontal plane; C: posterior-anterior flexion on the sagittal plane.

Figure 5.
ET application following the Taping Elastico® Method. It is possible to distinguish the convolutions of the two tails, typical of a zero-tension application with the aim to reduce compression of the underlying tissues.
Figure 5.
ET application following the Taping Elastico® Method. It is possible to distinguish the convolutions of the two tails, typical of a zero-tension application with the aim to reduce compression of the underlying tissues.

Figure 6.
ACROM modifications over the time in the six tested directions for SG (solid line) and CG (dotted line). “*” - Significant difference between T0 and T1. “#” - Significant difference between T0 and T2. “§” - Significant difference between T1 and T2.
Figure 6.
ACROM modifications over the time in the six tested directions for SG (solid line) and CG (dotted line). “*” - Significant difference between T0 and T1. “#” - Significant difference between T0 and T2. “§” - Significant difference between T1 and T2.
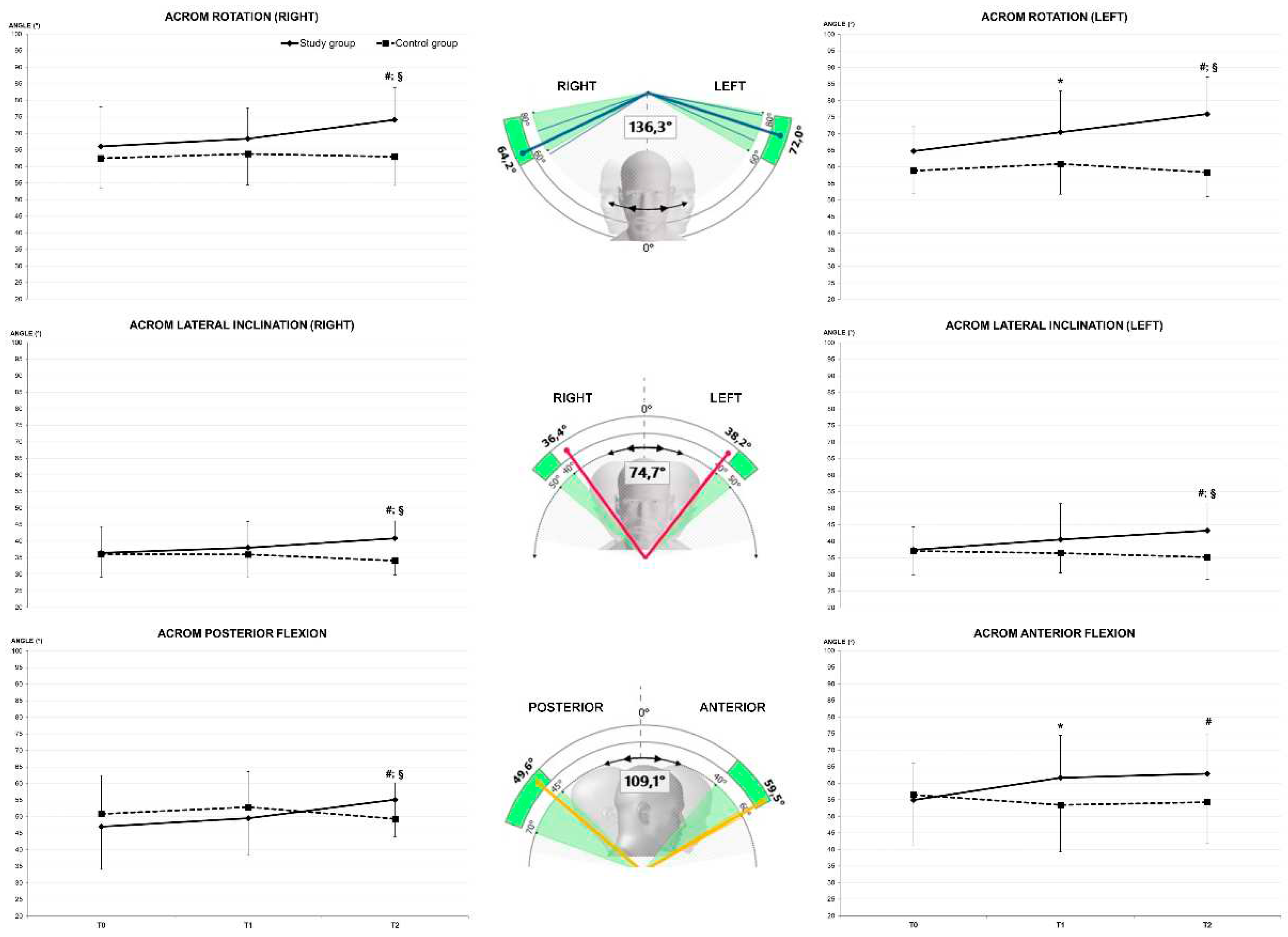
Figure 7.
Numerical Rating Scale of self-perceived cervical pain modifications over the time for SG (solid line) and CG (dotted line). “*” - Significant difference between T0 and T1. “#” - Significant difference between T0 and T2. “§” - Significant difference between T1 and T2.
Figure 7.
Numerical Rating Scale of self-perceived cervical pain modifications over the time for SG (solid line) and CG (dotted line). “*” - Significant difference between T0 and T1. “#” - Significant difference between T0 and T2. “§” - Significant difference between T1 and T2.
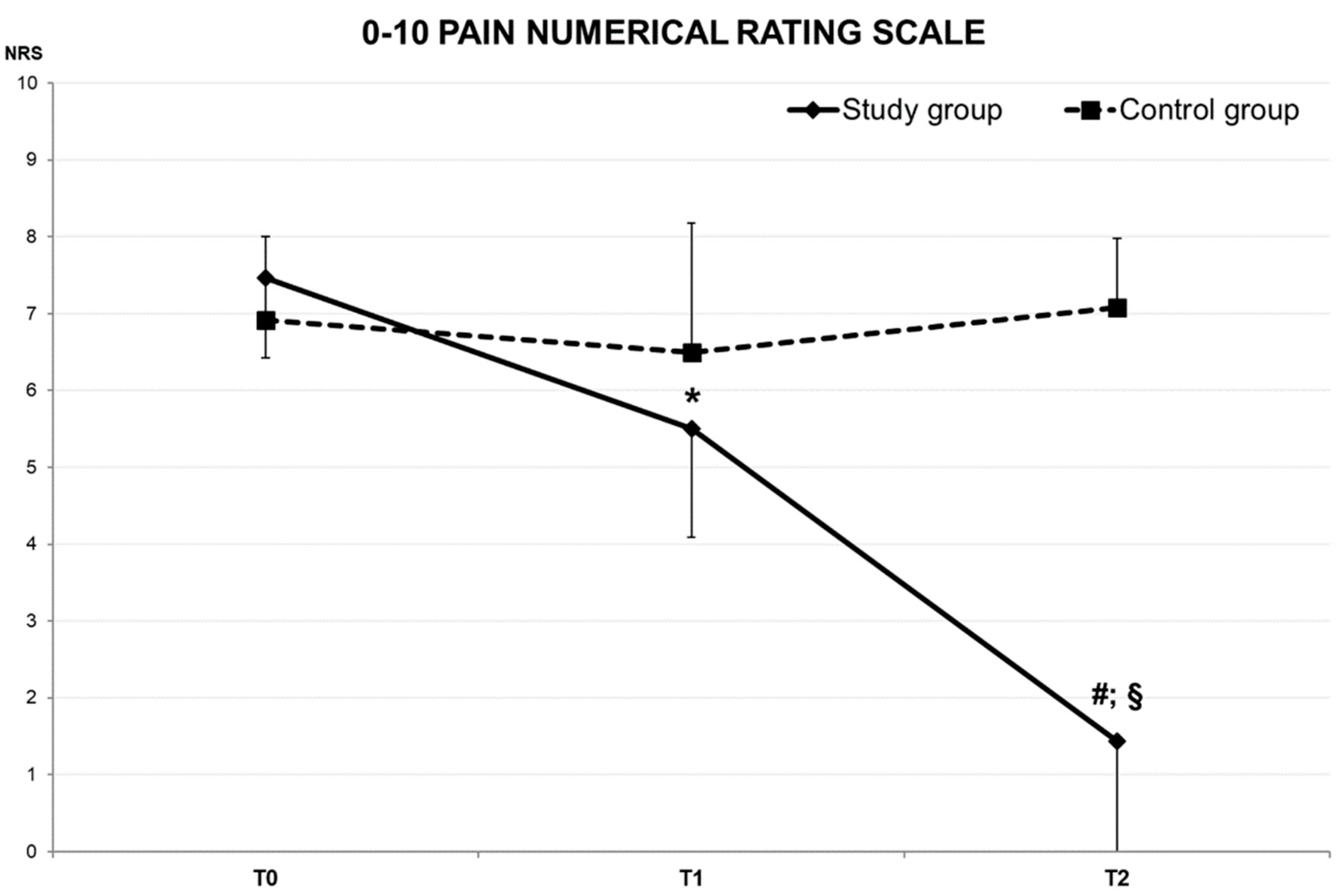
Table 1.
Results of the mixed ANOVA Time x Group interaction.
| Parameter | F | p Value |
|---|---|---|
| ACROM right rotation (°) | 3.764 | 0.027 |
| ACROM left rotation (°) | 8.034 | 0.001 |
| ACROM right lateral inclination (°) | 10.400 | 0.000 |
| ACROM left lateral inclination (°) | 7.537 | 0.001 |
| ACROM posterior flexion (°) | 7.435 | 0.001 |
| ACROM anterior flexion (°) | 5.708 | 0.005 |
| Pain (A.U.) | 113.111 | 0.000 |
Table 2.
Results of the experiment for SG and CG.
| Parameter | T0 | T1 | T2 | p Value | ||
|---|---|---|---|---|---|---|
| Study Group (SG) | ACROM right rotation (°) | 66.0 ± 11.9 | 68.4 ± 9.3 | 74.2 ± 9.6 #§ | 0.432 | 0.000 |
| ACROM left rotation (°) | 64.8 ± 7.7 | 70.4 ± 12.5 * | 76.0 ± 11.1 #§ | 0.599 | 0.000 | |
| ACROM right lateral inclination (°) | 36.5 ± 7.9 | 38.0 ± 7.9 | 40.9 ± 5.2 #§ | 0.452 | 0.000 | |
| ACROM left lateral inclination (°) | 37.5 ± 6.9 | 40.6 ± 10.8 | 43.2 ± 8.0 #§ | 0.554 | 0.000 | |
| ACROM posterior flexion (°) | 47.0 ± 12.9 | 49.6 ± 11.3 | 55.1 ± 11.3 #§ | 0.360 | 0.000 | |
| ACROM anterior flexion (°) | 55.0 ± 3.6 | 61.7 ± 12.8 * | 62.9 ± 12.0 # | 0.288 | 0.002 | |
| Pain (A.U.) | 7.5 ± 1.0 | 5.5 ± 1.4 * | 1.4 ± 1.5 #§ | 0.945 | 0.000 | |
| Control Group (CG) | ACROM right rotation (°) | 62.5 ± 9.1 | 63.8 ± 9.3 | 63.0 ± 8.7 | 0.017 | 0.569 |
| ACROM left rotation (°) | 58.8 ± 7.0 | 60.9 ± 9.2 | 58.4 ± 7.5 | 0.012 | 0.630 | |
| ACROM right lateral inclination (°) | 36.0 ± 7.0 | 36.0 ± 6.7 | 34.1 ± 4.2 | 0.094 | 0.175 | |
| ACROM left lateral inclination (°) | 37.1 ± 7.1 | 36.4 ± 6.0 | 35.2 ± 6.6 | 0.009 | 0.675 | |
| ACROM posterior flexion (°) | 50.9 ± 11.6 | 52.9 ± 10.7 | 49.3 ± 10.8 | 0.049 | 0.337 | |
| ACROM anterior flexion (°) | 56.5 ± 15.2 | 53.4 ± 14.1 | 54.3 ± 12.5 | 0.081 | 0.211 | |
| Pain (a.u.) | 6.9 ± 1.1 | 6.5 ± 1.7 | 7.1 ± 0.9 | 0.056 | 0.438 |
ACROM —Active Cervical Range of Motion. T0—baseline test session. T1—Test session after 20’ of wearing ET application. T2—Test session after three days of wearing ET application. “*” - Significant difference between T0 and T1. “#” - Significant difference between T0 and T2. “§” - Significant difference between T1 and T2. .
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



