
Submitted:
29 June 2023
Posted:
04 July 2023
You are already at the latest version
Abstract
In healthy humans, taste sensitivity varies widely, influencing food selection and nutritional status. Chemosensory reductions have been associated with numerous pathological disorders or pharmacological interventions. Reliable psychophysical methods are crucial resources to analyze the taste function during routine clinical assessment. However, in the daily clinical routine, they are often considered to be too time-consuming. We used the Supervised Learning (SL) regression method to analyze with high precision the overall taste status of healthy controls (HC) and patients with chemosensory loss and to characterize the combination of responses that best can predict the overall taste status of two groups. Random Forest regressor allowed us to achieve our objective. The analysis of the order of importance and impact of each parameter on the prediction of overall taste status in the two groups showed that salty (low concentration) and sour (high concentration) stimuli specifically characterized healthy subjects, while bitter (high concentration) and astringent (high concentration) stimuli identified patients with chemosensory loss. The identification of these distinctions appears to be of interest to the health system since they may allow the use of specific stimuli during routine clinical assessments of taste function reducing the commitment in terms of time and costs.
Keywords:
general taste status
; taste loss
; supervised learning regression
; random forest regressor
1. Introduction
Taste sensitivity is known to have a great physiological variability among the healthy human population. This diversity drives food acceptance and selection and affects nutritional status. At the same time, numerous disorders and pharmacological interventions may cause taste dysfunction, described as the pathological decrease of sensitivity (hypogeusia), or the rare complete taste loss (ageusia). Depending on definitions, hypogeusia can be found in 5% of the population within the age range of 5-89 years [1]. The number of individuals with taste disorders increases with age [2,3,4,5,6], reaching up to 15% among the US population over 57 years [7].
Taste loss diminishes not only the ability to detect noxious or unhealthy substances, but a loss of taste reduces the joy of consuming tasty foods and, consequently, the pleasures of social eating. Thus, depressive symptoms are commonly detected in patients with chemosensory disorders [8,9] with a frequency of such symptoms in patients suffering from gustatory disorders ranging from 25 to 36% [10,11]. These symptoms become even more frequent in patients with ageusia or qualitative disorders [8].
In healthy adults, another factor associated with a decline in gustatory sensitivity is an increasing body mass index (BMI) [12], supporting the idea that taste disorders facilitate the consumption of high-caloric foods. Specifically, the threshold for salty was higher [13,14], and the identification for salty, umami, and bitter was lower [15] in subjects with high BMI. However, results concerning sweet taste are contradictory: some found a direct correlation between higher glucose sensitivity and the predisposition for developing obesity and diabetes [16,17], while in some other cases, no differences in sweet sensitivity between healthy and obese subjects were observed [18,19]. Importantly, an increased ability to identify sweet taste was found after bariatric surgery in parallel with a significant reduction of weight [20].
Sensitivity to the bitterness of 6-n-propylthyouracil (PROP) and phenylthiocarbamide (PTC) also predicts the perception of the other taste qualities [21,22,23], chemical irritants [24], and astringent foods [25,26,27] and, for these reasons, it is considered a marker for inter-individual differences in general taste sensitivity. Several studies reported that individuals with a strong bitter perception of PROP/PTC bitterness have a higher sensitivity (super-tasters) to other taste stimuli compared to individuals with the non-sensitive (non-tasters) phenotype [28,29,30]. PROP sensitivity was also positively correlated with health status [31,32,33,34], but negatively correlated with BMI [35,36]. Additionally, Essick and coauthors showed that super-tasters had higher spatial resolution acuity in the tongue than non-tasters using an elegant identification test with 3D-printed letters of the alphabet [37].
Reliable methods for assessing taste perception in patients are crucial resources to define the degree of impairment in patients expressing an altered perception. Most of these methods, although easy to administer, are lengthy procedures in which patients have to maintain focus, and require a significant commitment from the health personnel. Hence, the Seven-iTT was recently proposed for routine clinical assessment of gustatory and somatosensory functions including astringency and spiciness [38]. Mastinu and coauthors showed that sweet was the most correctly identified taste sensation, followed by salty, bitter and sour and that patients with taste impairments had lower identification scores for astringency (dryness sensation) and spiciness (burning sensation). These correlations addressed the tight connection between gustatory and somatosensory perceptions at a peripheral level [39,40] that might fail after skull base surgery [41,42]. On the other hand, these results suggest that taste perception, and even more so dysfunction, is complex and governed by numerous factors.
In the present study, we analyzed with high precision the taste function of healthy controls (HC) and patients with chemosensory loss, using a supervised learning (SL) approach that provides real-time decision-making. We applied the SL regression method with different algorithms. The algorithms were targeted to obtain the most precise prediction on the taste function of subjects of the two groups. To this aim, we assessed the intensity ratings for a low and a high concentration of each of the six stimuli representative of sweet, sour, salty, bitter, astringent and spicy. The mean value calculated for each subject was termed as “overall taste status” and was used as the target of the algorithms. As inputs for the algorithms, we used a structured set of data consisting of the sensory, clinical, and anthropometric parameters that had been determined in the subjects of our previous study [38]. We aimed at establishing which combination of parameters best predicts the taste function of healthy controls or taste dysfunction of patients with chemosensory loss.
2. Materials and Methods
2.1. Subjects
One-hundred fifty-three individuals aged 18 to 81 years (38.3 ±14.3 years; 103 females) have been recruited at the Department of Otorhinolaryngology of the TU Dresden from February 2021 to January 2022. Of these, 51 were patients of the Smell and Taste Clinic who self-reported a chemosensory dysfunction. The remaining study sample comprised 102 healthy controls as a reference group. For the purpose of this cross-sectional study, patients were enrolled regardless the etiology of the taste dysfunction, or their smoking habits. Exclusion criteria were: pregnancy, allergy to substances used in the present study, unmedicated hypo/hyperthyreosis, uncontrolled diabetes mellitus, renal dysfunction, and significant cardiovascular issues. Informed written consent was obtained from all participants prior to their inclusion in the study. The research protocol was approved by the Ethics Review Board at the University Clinic of the Technische Universität Dresden, application number BO-EK-25012021.
2.2. Experimental Procedure
The experimental procedure took place in a single session from February 2021 to January 2022. Subjects were requested to abstain from drinking (except water), eating, and using chewing gum or oral care products for at least 1 h prior to testing. Their taste sensitivity of the four primary qualities (sweet, sour, salty, bitter) and sensations of astringency and spiciness were assessed as described below. Before the session, participants’ health status was ascertained with a detailed medical history. Weight (kg) and height (m) were recorded in order to calculate the subjects’ BMI (kg/m2). Additionally, all participants were screened for depression using the 5-item World Health Organization Well-Being Index (WHO-5) [43,44]. The questionnaire consists of five positively phrased items concerning being in good spirits, feeling relaxed, having energy, waking up fresh and rested, and being interested in things. Each of the five items is rated on a 6-point Likert scale from 0 to 5. The theoretical raw score ranges from 0 to 25. A high score in the WHO-5 indicates a high level of well-being, while a score below 13 indicates poor well-being [43,44]. They were also asked to indicate their liking for eating spicy food.
Authors had no access to information that could identify individual participants during or after data collection.
2.3. Sensory measurements
All taste measurements were performed using the same “taste strips” that are used in the validated “Taste Strip Test” (TST, Burghart Company, Wedel, Germany) [45,46]. Taste strips used in the assessments consisted of filter papers impregnated with two concentrations of stimuli representative of four basic taste qualities (sweet, sour, salty, bitter) and of sensations of astringency and spiciness. Taste qualities were presented in a semi-randomized order, with trigeminal stimuli at last because of their lingering sensations. Before every new testing, participants were asked to rinse their mouth with tap water. The evaluation did not include umami sensation due to the low familiarity in the European population [47].
The following two concentrations (one low and one high) for each stimulus were used: 0.4 and 0.05 g/mL sucrose; 0.3 and 0.05 g/mL citric acid; 0.25 and 0.016 g/mL sodium chloride; 0.006 and 0.0004 g/mL quinine hydrochloride; 0.1 and 0.2 g/mL tannin; 2.47x10-5 and 2.47x10-4 g/mL capsaicin. After placing each filter paper on the tongue, each subject had to evaluate the perceived intensity for each stimulus using a visual analog scale from 0 to 5 (0 = no taste at all, 5 = extremely strong taste). The ratings of the perceived taste intensity for the two concentrations of each stimulus were called: sweet_low_int and sweet_high_int, sour_low_int and sour_high_int, salty_low_int and salty_high_int, bitter_low_int and bitter_high_int, astring_low_int and astring_high_int, hot_low_int and hot_high_int. The overall taste status, which is the target of regressor model, was calculated in each subject as the mean value of intensity ratings for the low and the high concentration of the six stimuli (score_lowhigh_capsadstr_int1). Subjects also had to identify the taste quality he/she of each stimulus by choosing from a list of six possible answers (sweet, sour, salty, bitter, astringency and hot) in a forced choice procedure [45]. Each correct answer was rated 1, the number of correctly identified tastes was summed up in the total taste score (score_lowhigh_capsadstr1) whose maximum values was 12. The scores of the correct answer for the two concentrations of each stimulus were called as follows: salty_low_taste_correct; salty_high_taste_correct; sweet_low_taste_correct; sweet_high_taste_correct; sour_low_taste_correct; sour_high_taste_correct; bitter_low_taste_correct; bitter_high_taste_correct; hot_low_taste_correct; hot_high_taste_correct; astring_low_taste_correct; astring_high_taste_correct.
2.4. Supervised Learning
The automatic prediction of the overall taste status of healthy controls and patients with chemosensory loss was carried out from January 2022 to October 2022 by SL algorithms exploiting the subjects’ parameters that were presented in the data model as predictive variables (features). We used the SL regressors because they are specific to predict continuous outcomes such as the overall taste status of subjects [48]. The SL regressors learned and created automatic regressor models that evaluated the differences among subjects and returned, with high precision, a prediction of the value of the overall taste status in healthy controls or patients with chemosensory loss subjects. The following algorithms were used: Logistic Regression, Random Forest regressor, and CatBoost regressor. During training, the different algorithms learn the hidden patterns in the structured dataset, then they take new unforeseen inputs (test dataset) to predict the value of the target (the overall taste status). To archive our aim (to analyze the overall taste status of healthy controls and patients with chemosensory loss and individuate specific stimulus or their combination that best can predict the overall taste status of two groups) was necessary to apply the regressor model separately to the dataset of healthy controls and patients with chemosensory loss. Therefore, we performed two SL regressor experiments: experiment 1 included healthy controls (n = 102) and experiment 2 included patients with chemosensory loss (n = 51).
The interpretation of the results of the Random Forest regressor model have been performed by using Shapley Additive exPlanations (SHAP)[49] which is a game-theoretic method that allows to link the importance of each feature with its effect. SHAP returns a specific plot for each Random Forest regressor experiment representing the impact of each feature in that experiment.
The following data processing operations, which are a crucial phase in the performance of an SL project, were applied:
- The definition of correlations between numerical parameters and those between each numerical feature and the target, which were a fundamental step to understand the data structure, were also considered to include a feature in the data set (Figure 1).
- Choice of features that are used by the algorithm as predictive variables of the target: the set of parameters most suitable for our case study was selected as features by expert researchers in taste physiology and an ML engineer, based on their domain knowledge, from a database of the sensory, clinical, and demographic parameters [50]. In addition, since two features strongly correlated with each other have almost the same effect on the dependent variable, one of them has been dropped to reduce the noise that can impact algorithm performance [51]. Specifically, the sum of the scores of the correct answer for the two concentrations of salty, sweet, sour, bitter, hot and astringency, the sum of the scores of the correct answers for the two concentrations of salty, sweet, sour and bitter, and the intensity ratings for the two concentrations of salty, sweet, sour and bitter strongly correlated with each other. The first summated variable that include evaluations of all stimuli was selected, the latter two were excluded.
- Handling of missing values: every line of the subject that represents lacking information in some column was eliminated.
- Elimination of duplicate values. In fifty-eight subjects of the group of controls all sensory measurements were repeated twice. The column relative to these measures repeated, and those of the overall taste status and total taste score calculated in these subjects (twenty-nine columns in total) have been eliminated from the data set.
- Converting the dataset's content into a language that an algorithm can understand: this included the One Hot Encoding which encodes categorical data into numerical data and the normalization of the numerical data which consisted in transforming a real range of numerical values in a range between 0 to 1.
After data processing operations that included the remotion of all non-significant and correlated features, we increased the parameters of numbers of estimators, maximum of depth of the SL regressors. Moreover, we used 3-fold Cross-Validation, which mixes and splits data into two groups (training data, 66.66% and test data, 33.33%) for three times using different subsets of data each time.
The evaluation of the performance of the algorithms was found by metrics, such as Mean Absolute Percentage Error (MAPE) and Mean Squared Error (MSE) that assesses the differences between the observed and predicted values. In particular, MAPE represents the error percentage of predicted values, while MSE represents the average of the summation of the squared difference between the actual output value and the predicted output value. The overall behavior of our regressors was evaluated by the automatic optimization of their hyperparameters by Grid Search Algorithm successively.
2.5. Statistical Analysis
Fisher’s Exact Test was used to analyze differences, between healthy controls and patients with chemosensory loss, with regard to the frequency of correct answers for the two concentrations of each stimulus, gender, and like to eat spicy. T test was used to compare differences, between healthy controls and patients with chemosensory loss, in age, BMI, depression, taste intensity ratings for each stimulus and total taste score. Statistical analyses were conducted using STATISTICA for WINDOWS (version 7; StatSoft Inc, Tulsa, OK, USA). P values < 0.05 were considered significant. P values of T test were adjusted by Bonferroni correction (adjusted P = P / number of groups being compared) (P values < 0.0031 were considered significant).
3. Results
Value means ± SD or frequencies of the sensory, clinical, and anthropometric parameters determined in healthy controls and patients with chemosensory loss are shown in Table 1. T-test adjusted by Bonferroni correction showed that the ratings of the taste intensity in response to the low concentrations of each stimulus and the high concentration of sweet, sour and astringency, as well as the total taste score, of healthy controls, were higher than that of patients with chemosensory loss (p ≤ 0.0006). Depression level was higher in patients with chemosensory loss than in healthy controls (p < 0.0001). The number of correct answers for the low concentrations of salty, bitter, hot, and astringency and the high concentration of sweet, sour, and astringency and the number of subjects who like to eat spicy was higher in healthy controls than in patients with chemosensory loss (χ2 ≥ 4.79; p ≤ 0.041; Fisher’s test). No differences in the ratings of the taste intensity in response to the high concentrations of salty, bitter and hot, age, BMI, gender, or in the number of correct answers for low concentrations of sweet and sour, and high concentrations of salty, bitter and hot were found between the two groups (p > 0.05).
The metrics of evaluation of the performance of the algorithms, MAPE and MSE, which measure the accuracy of a forecast system, showed that the random forest regressor was the best algorithm to predict the values of the overall taste status with high precision. The scatterplots showing experimental values vs predicted values of the overall taste status obtained with the random forest regressor in healthy controls and patients with chemosensory loss are shown in Figure 2. The values of MSE, which evaluates how estimated values are close to experimental values, were 0.019 and 0.014 in the two groups. Besides, the MAPE values, which represent the error percentage of predicted values, were 4.55%, and 8.40% in healthy controls and patients with chemosensory loss, respectively.
The Random Forest regressor allowed us to determine the order of importance and the contribution of the sensory, clinical, and anthropometric features on the prediction of overall taste status in the two groups, and the interpretation by SHAP algorithm allowed us to obtain an overview of their impact on the prediction.
Specifically, the rating of the perceived taste intensity for the low concentration of salt was the most important feature for the learning of model in healthy controls and its contribution on the prediction of the overall taste status, estimated as the average impact on the model, was 0.079 (Figure 3A). This feature was followed in order of importance from the second to the tenth by: the intensity rating for the high concentration of sour, for the low concentration of bitter, for the high concentration of sweet, for the high concentration of bitter, for the low concentration of hot, for the high concentration of salty, for the low concentration of astringency, the total taste score and the intensity rating for the low concentration of sweet. It is interesting to note that depression status was a significant feature (sixteen in importance order). These features had an average impact on the model lower than 0.057. The link between features’ importance and features’ effect on the overall status of the healthy controls is shown in the SHAP summary plot (Figure 3B). The plot highlights that high estimated values (pink) of the rating of the perceived taste intensity for the low concentration of salt and for the high concentration of sour had a strong and positive impact to make a prediction of high values of overall taste status and low estimated values (blue) of these features strongly pushed the model prediction towards low values of the overall taste status. The mean of the positive impacts of these two features were 0.052 and 0.040, while that of the negative impacts were -0.155 and -0.106. High estimated values (pink) of the successive eight features had a positive impact (≤ 0.057) to make a prediction of high values of overall taste status, medium values (violet) impacted the model to make a prediction of medium values of the overall taste status and low estimated values (blue) of these features pushed the model prediction towards low values of the overall taste status (negative impact ≤ -0.069).
The features’ importance in facilitating the learning of the Random Forest regressor to predict the overall taste status, and an overview of how the most important features impact it to make a prediction in patients with chemosensory loss are shown in Figure 4. In this case, the rating of the perceived taste intensity for the high concentration of bitter and for the high concentration of astringency were the first two most important features for the model to predict the overall taste status of this group, giving a similar contribution on the model prediction of the overall taste status, the average impacts were 0.105 and 0.100 (Figure 4A). These were followed in order of importance from the third to the tenth by: the total taste status, the intensity rating for the low concentration of salty, for the high concentration of sweet, for the low concentration of bitter, for the low concentration of sweet, for the high concentrations of sour, for the high concentration of salty and for the low concentration of sour. These features had an average impact on the model lower than 0.077. SHAP summary plot highlights that high estimated values (pink) of the rating of the perceived taste intensity for the high concentration of bitter and for the high concentration of astringency had a strong and positive impact to make a prediction of high values of overall taste status and low estimated values (blue) of these features strongly pushed the model prediction towards low values of the overall taste status (Figure 4B). The mean of the positive impacts of these two features were 0.085 and 0.096, while that of the negative impacts were -0.134 and -0.105. High estimated values (pink) of the successive eight features had a positive impact (≤ 0.098) to make a prediction of high values of overall taste status, medium (violet) and low values (blue) estimated values of these features impacted the model to make a prediction of medium and low values of the overall taste status (negative impact ≤ -0.105).
The error percentage of predicted values of the overall taste status (MAPE values) calculated in the datasets of the two groups by using as inputs for the algorithm only the most important feature for the two groups (the intensity rating for the low concentration of salt in healthy subjects and high concentration of bitter in patients), was 12.35%, and 17.94% in healthy controls and patients with chemosensory loss, respectively. When the second important features were also included in the model (high concentration of sour for healthy subjects and high concentration of astringency for patients), the error percentage of predicted values of the overall taste status was 11.05%, and 17.16% in healthy controls and patients with chemosensory loss, respectively.
4. Discussion
This project used the SL regression method to establish which combination of sensory, clinical, and anthropometric parameters best predicts the overall taste status of healthy controls or that of patients with chemosensory loss. The subjects included as patients with chemosensory loss have been selected based on what they reported. The values of the sensory parameters, which were used as predictive variables of the overall taste status, as well as the correlation between them and the target, confirm that they showed a lower taste sensitivity compared to the subjects of the group of control. The low taste sensitivity of these subjects was linked to their higher depression status according to what was already reported [8].
The Random Forest regressor was the best model to deeply understand differences among subjects and obtain, with high precision, the value of the overall taste status of subjects. Moreover, the Random Forest regressor allowed us to establish each parameter’s impact on prediction, identifying the combination of the biological parameters that could best predict the overall taste status of healthy subjects or that of patients with chemosensory loss. The performance of our approach was tested by the metrics of evaluation, MAPE and MSE, which allowed us to verify that the estimated values by the Random Forest regressor were strictly close to experimental values with an error percentage of 4.55%, and 8.40% in healthy controls and patients with chemosensory loss, respectively.
The Random Forest regressor allowed us also to achieve the order of importance of each feature on the prediction of the overall taste status of subjects of the two groups. The regressor identified the rating of the perceived taste intensity for the low concentration of salt to be the most important parameter in healthy subjects, while the rating of the perceived taste intensity for the high concentration of bitter was the most significant in patients with chemosensory loss. Moreover, the interpretation of the linking between parameters’ importance and parameter’ effect showed that high estimated values of the perceived intensity for the low concentration of salt had a strong and positive impact to predict high values of overall taste status in healthy subjects. On the other hand, high estimated values of the rating of the perceived taste intensity for the high concentration of bitter had a strong and positive impact to predict high values of overall taste status in patients with chemosensory loss. Low values of these two parameters strongly pushed the model prediction towards low values of the overall taste status in both groups. The fact that the most important parameter to predict the overall taste status in healthy controls was the rating of the perceived intensity for the low concentration of salt is not surprising, as we can see from experimental values shown in Table 1, the low concentration of salt evoked the highest response compared to the low concentrations of other stimuli and a high percentage of subjects (85.3%) recognized it correctly. The rating of the perceived taste intensity for the high concentration of bitter, which was the most important feature in patients with chemosensory loss, was correctly recognized by 76.5 % of patients. The bitter taste was an important stimulus also in healthy controls, third in importance order at low concentration, it was correctly recognized by 61.8% of subjects. The difference in the importance of bitter taste that we found in the two groups may be explained by possible genetic differences between the two groups. In our pilot study we found that, differently from healthy controls, in patients with taste disorders, a taster haplotype in the gene coding for bitter TAS2R38 receptor is not sufficient to exhibit high responses, suggesting that the genetic constitution may represent a risk factor for the development of taste disorders [52]. Besides, based on the results that suggested the TAS2R38 pathway as an immune response target [33,53], patients with the non-taster haplotype, who show lower responsiveness, could have a higher susceptibility to oropharyngeal infections, which may contribute to their chemosensory loss.
The second most important parameter in learning the model in healthy controls was the perceived intensity rating for high concentration of sour, it was the stimulus that evoked the highest response and 91.2 % of subjects correctly recognized it. High estimated values had a positive impact to predict high values of overall taste status, while low estimated values strongly pushed the model prediction towards low values of the overall taste status. Less important was the importance and impact that sour had on the prediction of the overall taste status in patients with chemosensory loss, in which was the eighth feature in importance order suggesting that the impact of sour on taste function may be more important in subjects that have not pathologies that determine chemosensory loss.
The second most important parameter in learning the model in the patients with chemosensory loss was the perceived intensity rating of the for high concentration of astringency, which strongly impacted the prediction of the overall status of this group in a way equivalent to what was done by the most important feature, the high concentration of bitter (the values of their contribution on the model prediction were 0.105 and 0.100). Less important was the contribution and impact that astringency (eighth in important order at low concentration and eleventh at high concentration) had on the prediction of the overall taste status in healthy subjects, in which low estimated values pushed the model prediction towards low values of the target. These results allow us to speculate that the impact of astringency on taste function could be more important in subjects with low sensitivity. This result deserves to be further investigated in future studies.
It is interesting to note that the performance of our model applied in the datasets of the healthy controls and that of patients by using as inputs for the algorithm only the most important features for the two groups, allowed us to verify that the estimated values were strictly close to experimental values with an error percentage of 12.35% and 17.95%. By including in the model also the second important features as the predictive variables, the error percentage of predicted values of the overall taste status decreased of 1.3% and 0.79%, in healthy controls and patients, respectively.
5. Conclusions
In conclusion, our results indicated that the Random Forest regressor is a reliable strategy to analyze taste function, by exploiting a structured dataset consisting of sensory, clinical, and anthropometric parameters previously determined in the participants [38], as inputs for the algorithm. Furthermore, the proposed approach, which provides real-time decision-making, allowed us to identify with high precision different stimuli and their combination that best can predict the overall taste status in the two groups. The low concentration of salt and high concentration of sour were specific for healthy subjects, while the high concentration of bitter and high concentration of astringency stimuli were the most indicative ones for pathological taste disorders. These four stimuli strongly impacted the model prediction mostly in the subjects where evoked low responses (the impact values were two-fold increase with respect to those of the other stimuli), suggesting that a low response to these stimuli characterizes taste dysfunction.
Identifying these combinations of stimuli as the most critical to efficiently assess gustatory function of healthy subjects and patients with chemosensory loss could simplify testing especially during routine clinical examinations (e.g., annual physical exams), and therefore reduce the health system commitment in terms of time and costs.
Author Contributions
Conceptualization, T.H. and I.T.B.; methodology, L.C.N., Ma.Ma. T.G. and A.W.; software, L.C.N.; formal analysis, L.C.N. and Me.Me.; investigation, Ma.Ma. T.G. and A.W.; data curation, L.C.N. and Me.Me; writing—original draft preparation, I.T.B.; writing—review and editing, L.C.N., Ma.Ma., Me.Me., and T.H.; supervision, T.H. and I.T.B.; project administration, T.H., Me.Me. and I.T.B.; funding acquisition, T.H. and Me.Me. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by EXU-transcelerator B3 grant, TU Dresden to T.H. and by Fondazione Sardegna, Italy to Me.Me.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board at the University Clinic of the Technische Universität Dresden, application number BO-EK-25012021.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All datasets and code presented in this study are freely available in Github at the link: https://github.com/lala-sudo/SCORE_LOW_HIGH_CAPSADSTR_INTENSITYW
Acknowledgments
We would like to thank Masha Niv for her invaluable help with project. We also thank Ilyas Chaoua for its supervising the SL method.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Welge-Lüssen, A.; Dörig, P.; Wolfensberger, M.; Krone, F.; Hummel, T. A study about the frequency of taste disorders. J Neurol 2011, 258, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Doty, R.L. Age-related deficits in taste and smell. Otolaryngol. Clin. North Am. 2018, 51, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Mojet, J.; Christ-Hazelhof, E.; Heidema, J. Taste perception with age: generic or specific losses in threshold sensitivity to the five basic tastes? Chem. Senses 2001, 26, 845–860. [Google Scholar] [CrossRef]
- Mojet, J.; Heidema, J.; Christ-Hazelhof, E. Taste perception with age: generic or specific losses in supra-threshold intensities of five taste qualities? Chem Senses 2003, 28, 397–413. [Google Scholar] [CrossRef] [PubMed]
- Doty, R.L.; Heidt, J.M.; MacGillivray, M.R.; Dsouza, M.; Tracey, E.H.; Mirza, N.; Bigelow, D. Influences of age, tongue region, and chorda tympani nerve sectioning on signal detection measures of lingual taste sensitivity. Physiol Behav 2016, 155, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, S.S. Taste and smell losses in normal aging and disease. JAMA 1997, 278, 1357–1362. [Google Scholar] [CrossRef]
- Boesveldt, S.; Lindau, S.T.; McClintock, M.K.; Hummel, T.; Lundstrom, J.N. Gustatory and olfactory dysfunction in older adults: a national probability study. Rhinology 2011, 49, 324–330. [Google Scholar] [CrossRef]
- Chen, B.; Benzien, C.; Faria, V.; Ning, Y.; Cuevas, M.; Linke, J.; Croy, I.; Haehner, A.; Hummel, T. Symptoms of Depression in Patients with Chemosensory Disorders. ORL J Otorhinolaryngol Relat Spec 2021, 83, 135–143. [Google Scholar] [CrossRef]
- Croy, I.; Negoias, S.; Novakova, L.; Landis, B.N.; Hummel, T. Learning about the Functions of the Olfactory System from People without a Sense of Smell. Plos One 2012, 7, e33365. [Google Scholar] [CrossRef]
- Walliczek-Dworschak, U.; Schops, F.; Feron, G.; Brignot, H.; Hahner, A.; Hummel, T. Differences in the Density of Fungiform Papillae and Composition of Saliva in Patients With Taste Disorders Compared to Healthy Controls. Chem Senses 2017, 42, 699–708. [Google Scholar] [CrossRef]
- Deems, D.A.; Doty, R.L.; Settle, R.G.; Moore-Gillon, V.; Shaman, P.; Mester, A.F.; Kimmelman, C.P.; Brightman, V.J.; Snow, J.B., Jr. Smell and taste disorders, a study of 750 patients from the University of Pennsylvania Smell and Taste Center. Arch Otolaryngol Head Neck Surg 1991, 117, 519–528. [Google Scholar] [CrossRef]
- Tepper, B.J.; Banni, S.; Melis, M.; Crnjar, R.; Tomassini Barbarossa, I. Genetic sensitivity to the bitter taste of 6-n-propylthiouracil (PROP) and its association with physiological mechanisms controlling body mass index (BMI). Nutrients 2014, 6, 3363–3381. [Google Scholar] [CrossRef] [PubMed]
- Skrandies, W.; Zschieschang, R. Olfactory and gustatory functions and its relation to body weight. Physiol Behav 2015, 142, 1–4. [Google Scholar] [CrossRef]
- Park, D.C.; Yeo, J.H.; Ryu, I.Y.; Kim, S.H.; Jung, J.; Yeo, S.G. Differences in taste detection thresholds between normal-weight and obese young adults. Acta Oto-Laryngol 2015, 135, 478–483. [Google Scholar] [CrossRef]
- Overberg, J.; Hummel, T.; Krude, H.; Wiegand, S. Differences in taste sensitivity between obese and non-obese children and adolescents. Arch. Dis. Child. 2012, 97, 1048–1052. [Google Scholar] [CrossRef] [PubMed]
- Pasquet, P.; Frelut, M.L.; Simmen, B.; Hladik, C.M.; Monneuse, M.O. Taste perception in massively obese and in non-obese adolescents. Int J Pediatr Obes 2007, 2, 242–248. [Google Scholar] [CrossRef]
- Kumari, B.G.; Kumar, Z.N. Evaluation of sweet taste sensitivity in type-II Diabetes Mellitus patients. IJCBR 2020, 10–12. [Google Scholar] [CrossRef]
- Anderson, G.H. Sugars, sweetness, and food intake. Am J Clin Nutr 1995, 62, 195S–201S; discussion 201S-202S. [Google Scholar] [CrossRef]
- Simchen, U.; Koebnick, C.; Hoyer, S.; Issanchou, S.; Zunft, H.J. Odour and taste sensitivity is associated with body weight and extent of misreporting of body weight. European journal of clinical nutrition 2006, 60, 698–705. [Google Scholar] [CrossRef] [PubMed]
- Melis, M.; Pintus, S.; Mastinu, M.; Fantola, G.; Moroni, R.; Pepino, M.Y.; Barbarossa, I.T. Changes of Taste, Smell and Eating Behavior in Patients Undergoing Bariatric Surgery: Associations with PROP Phenotypes and Polymorphisms in the Odorant-Binding Protein OBPIIa and CD36 Receptor Genes. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Dinehart, M.E.; Hayes, J.E.; Bartoshuk, L.M.; Lanier, S.L.; Duffy, V.B. Bitter taste markers explain variability in vegetable sweetness, bitterness, and intake. Physiol. Behav. 2006, 87, 304–313. [Google Scholar] [PubMed]
- Tepper, B.J. Nutritional implications of genetic taste variation: the role of PROP sensitivity and other taste phenotypes. Annu. Rev. Nutr. 2008, 28, 367–388. [Google Scholar] [PubMed]
- Hayes, J.E.; Duffy, V.B. Revisiting sugar-fat mixtures: sweetness and creaminess vary with phenotypic markers of oral sensation. Chem. Senses 2007, 32, 225–236. [Google Scholar]
- Duffy, V.B.; Davidson, A.C.; Kidd, J.R.; Kidd, K.K.; Speed, W.C.; Pakstis, A.J.; Reed, D.R.; Snyder, D.J.; Bartoshuk, L.M. Bitter Receptor Gene (TAS2R38), 6-n-Propylthiouracil (PROP) Bitterness and Alcohol Intake. Alcohol. Clin. Exp. Res. 2004, 28, 1629–1637. [Google Scholar] [CrossRef]
- Melis, M.; Yousaf, N.Y.; Mattes, M.Z.; Cabras, T.; Messana, I.; Crnjar, R.; Tomassini Barbarossa, I.; Tepper, B.J. Sensory perception of and salivary protein response to astringency as a function of the 6-n-propylthioural (PROP) bitter-taste phenotype. Physiol. Behav. 2017, 173, 163–173. [Google Scholar] [PubMed]
- Yousaf, N.Y.; Melis, M.; Mastinu, M.; Contini, C.; Cabras, T.; Tomassini Barbarossa, I.; Tepper, B.J. Time Course of Salivary Protein Responses to Cranberry-Derived Polyphenol Exposure as a Function of PROP Taster Status. Nutrients 2020, 12, 2878. [Google Scholar] [CrossRef] [PubMed]
- Yousaf, N.Y.; Tepper, B.J. The Effects of Cranberry Polyphenol Extract (CPE) Supplementation on Astringency and Flavor Perception as a Function of PROP Taster Status and Other Individual Factors. Int J Env Res Pub He 2022, 19, 11995. [Google Scholar] [CrossRef]
- Bartoshuk, L.M.; Fast, K.; Karrer, T.A.; Marino, S.; Price, R.A.; Reed, D.A. PROP supertasters and the perception of sweetness and bitterness. Chem. Senses 1992, 17, 594. [Google Scholar]
- Bartoshuk, L.M.; Rifkin, B.; Marks, L.E.; Hooper, J.E. Bitterness of KCl and benzoate: related to genetic status for sensitivity to PTC/PROP. Chem. Senses 1988, 13, 517–528. [Google Scholar] [CrossRef]
- Gent, J.; Bartoshuk, L. Sweetness of sucrose, neohesperidin dihydrochalcone, and saccharin is related to genetic ability to taste the bitter substance 6-n-propylthiouracil. Chem. Senses 1983, 7, 265–272. [Google Scholar] [CrossRef]
- Whissell-Buechy, D. Effects of age and sex on taste sensitivity to phenylthiocarbamide (PTC) in the Berkeley Guidance sample. Chem. Senses 1990, 15, 39–57. [Google Scholar]
- Melis, M.; Errigo, A.; Crnjar, R.; Pes, G.M.; Tomassini Barbarossa, I. TAS2R38 bitter taste receptor and attainment of exceptional longevity. Sci. Rep. 2019, 9, 18047. [Google Scholar] [PubMed]
- Lee, R.J.; Cohen, N.A. Role of the bitter taste receptor T2R38 in upper respiratory infection and chronic rhinosinusitis. Curr. Opin. Allergy Clin. Immunol. 2015, 15, 14–20. [Google Scholar]
- Cossu, G.; Melis, M.; Sarchioto, M.; Melis, M.; Melis, M.; Morelli, M.; Tomassini Barbarossa, I. 6-n-propylthiouracil taste disruption and TAS2R38 nontasting form in Parkinson's disease. Mov. Disord. 2018, 33, 1331–1339. [Google Scholar]
- Tepper, B.J.; Koelliker, Y.; Zhao, L.; Ullrich, N.V.; Lanzara, C.; d'Adamo, P.; Ferrara, A.; Ulivi, S.; Esposito, L.; Gasparini, P. Variation in the bitter-taste receptor gene TAS2R38, and adiposity in a genetically isolated population in Southern Italy. Obesity 2008, 16, 2289–2295. [Google Scholar]
- Lumeng, J.C.; Cardinal, T.M.; Sitto, J.R.; Kannan, S. Ability to taste 6-n-propylthiouracil and BMI in low-income preschool-aged children. Obesity 2008, 16, 1522–1528. [Google Scholar] [PubMed]
- Essick, G.K.; Chopra, A.; Guest, S.; McGlone, F. Lingual tactile acuity, taste perception, and the density and diameter of fungiform papillae in female subjects. Physiol Behav 2003, 80, 289–302. [Google Scholar]
- Mastinu, M.; Pieniak, M.; Wolf, A.; Green, T.; Hähner, A.; Niv, M.Y.; Hummel, T. A Simple Taste Test for Clinical Assessment of Taste and Oral Somatosensory Function—The “Seven-iTT”. Life 2023, 13, 59. [Google Scholar]
- Bangcuyo, R.G.; Simons, C.T. Lingual tactile sensitivity: effect of age group, sex, and fungiform papillae density. Exp Brain Res 2017, 235, 2679–2688. [Google Scholar]
- Bogdanov, V.; Reinhard, J.; McGlone, F.; Haehner, A.; Simons, C.T.; Hummel, T. Oral Somatosensory Sensitivity in Patients With Taste Disturbance. Laryngoscope 2021, 131, 2572–2577. [Google Scholar]
- Matsumoto, S.; Osawa, K.; Hirose, Y.; Nakayama, M.; Wada, T.; Matsuda, M.; Akutsu, H.; Ii, R.; Koizumi, H.; Okano, Y.; et al. Objective evaluation of gustatory function after surgery for vestibular schwannoma: A pilot study. Auris Nasus Larynx 2022, 49, 183–187. [Google Scholar]
- Podlesek, D.; Chao, Y.T.; Weitkamp, F.; Schackert, G.; Hummel, T. Trigeminal Sensory Neuropathy Predicts Chemosensory Dysfunction After Skull Base Surgery. Operative neurosurgery (Hagerstown, Md.), 2022. [Google Scholar]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: a systematic review of the literature. Psychotherapy and psychosomatics 2015, 84, 167–176. [Google Scholar]
- World Health Organization. Regional Office for, E. Wellbeing measures in primary health care/the DepCare Project: report on a WHO meeting: Stockholm, Sweden, 12–13 February 1998; World Health Organization. Regional Office for Europe: Copenhagen, 1998 1998. [Google Scholar]
- Landis, B.N.; Welge-Luessen, A.; Bramerson, A.; Bende, M.; Mueller, C.A.; Nordin, S.; Hummel, T. "Taste Strips" - a rapid, lateralized, gustatory bedside identification test based on impregnated filter papers. J. Neurol. 2009, 256, 242–248. [Google Scholar]
- Mueller, C.; Kallert, S.; Renner, B.; Stiassny, K.; Temmel, A.F.; Hummel, T.; Kobal, G. Quantitative assessment of gustatory function in a clinical context using impregnated "taste strips". Rhinology 2003, 41, 2–6. [Google Scholar]
- Maria Paola, C.; Antti, K.; Eileen, H.; Federico, B.; Thomas, H.; Emilia, I. A cross-cultural survey of umami familiarity in European countries. Food Qual Prefer 2019, 74, 172–178. [Google Scholar]
- Sidey-Gibbons, J.A.M.; Sidey-Gibbons, C.J. Machine learning in medicine: a practical introduction. BMC medical research methodology 2019, 19, 64. [Google Scholar]
- Lundberg, S.M.; Lee, S.-I. A Unified Approach to Interpreting Model Predictions. Nips'17, 2017; 4768–4777. [Google Scholar]
- Yousef, M.; Kumar, A.; Bakir-Gungor, B. Application of Biological Domain Knowledge Based Feature Selection on Gene Expression Data. Entropy 2021, 23. [Google Scholar] [CrossRef]
- Yu, L.; Liu, H. Feature Selection for High-Dimensional Data: A Fast Correlation-Based Filter Solution; 2003; Volume 2, pp. 856–863.
- Melis, M.; Grzeschuchna, L.; Sollai, G.; Hummel, T.; Tomassini Barbarossa, I. Taste disorders are partly genetically determined: Role of the TAS2R38 gene, a pilot study. Laryngoscope 2019. [Google Scholar]
- Lee, R.J.; Xiong, G.; Kofonow, J.M.; Chen, B.; Lysenko, A.; Jiang, P.; Abraham, V.; Doghramji, L.; Adappa, N.D.; Palmer, J.N.; et al. T2R38 taste receptor polymorphisms underlie susceptibility to upper respiratory infection. J. Clin. Invest. 2012, 122, 4145–4159. [Google Scholar]
Figure 1.
Linear correlation analysis between the numerical features of the dataset and those between numerical features and the target. The bar color on the right side on the Y axis represents the value of linear correlation between features. P values are indicated inside each square and derived from Pearson’s coefficient analysis
Figure 1.
Linear correlation analysis between the numerical features of the dataset and those between numerical features and the target. The bar color on the right side on the Y axis represents the value of linear correlation between features. P values are indicated inside each square and derived from Pearson’s coefficient analysis
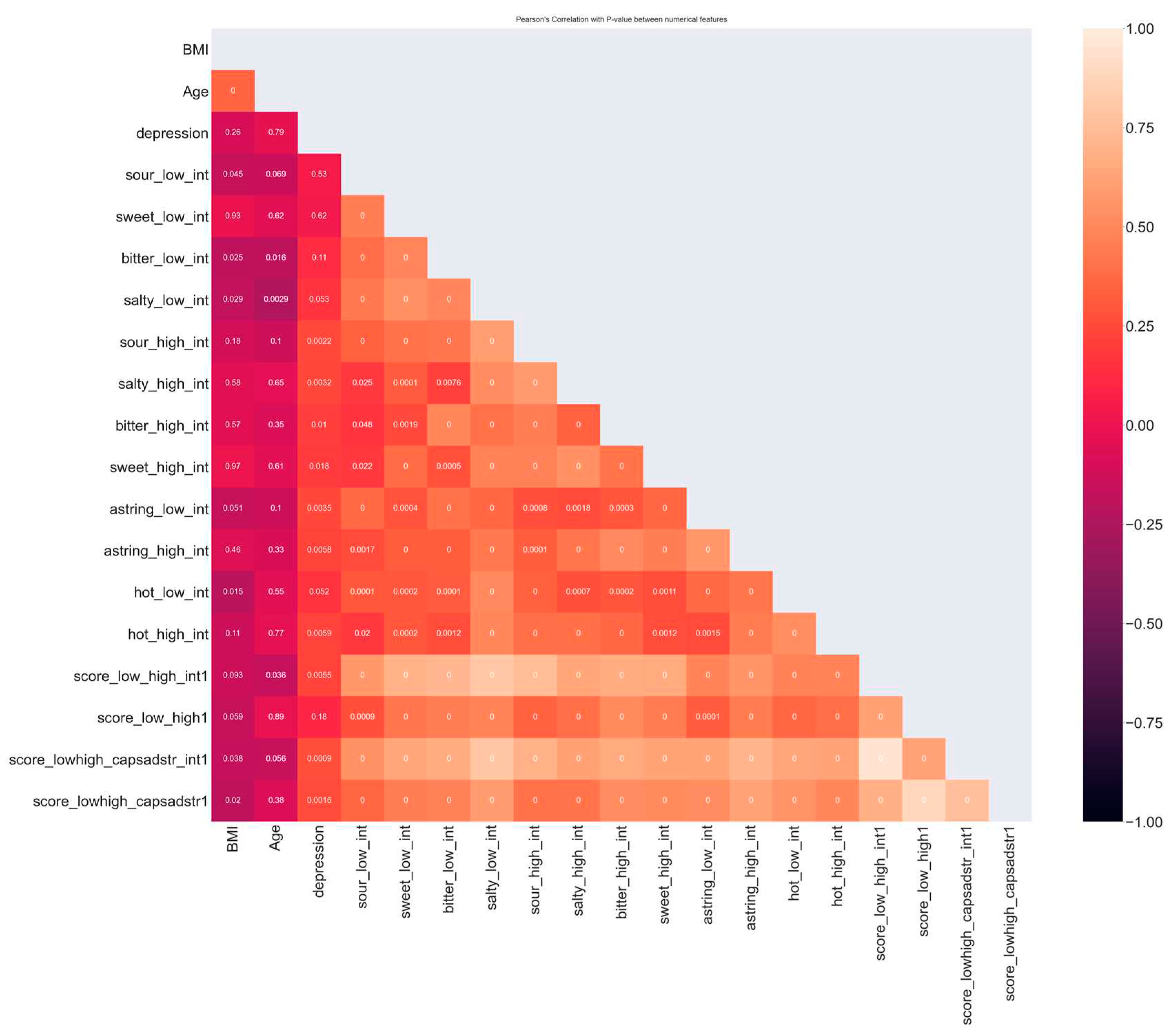
Figure 2.
Scatterplots of experimental values vs predicted values of the overall status obtained with the random forest regressor in healthy controls (n = 102) (A) and in patients with chemosensory loss (n =51) (B).
Figure 2.
Scatterplots of experimental values vs predicted values of the overall status obtained with the random forest regressor in healthy controls (n = 102) (A) and in patients with chemosensory loss (n =51) (B).
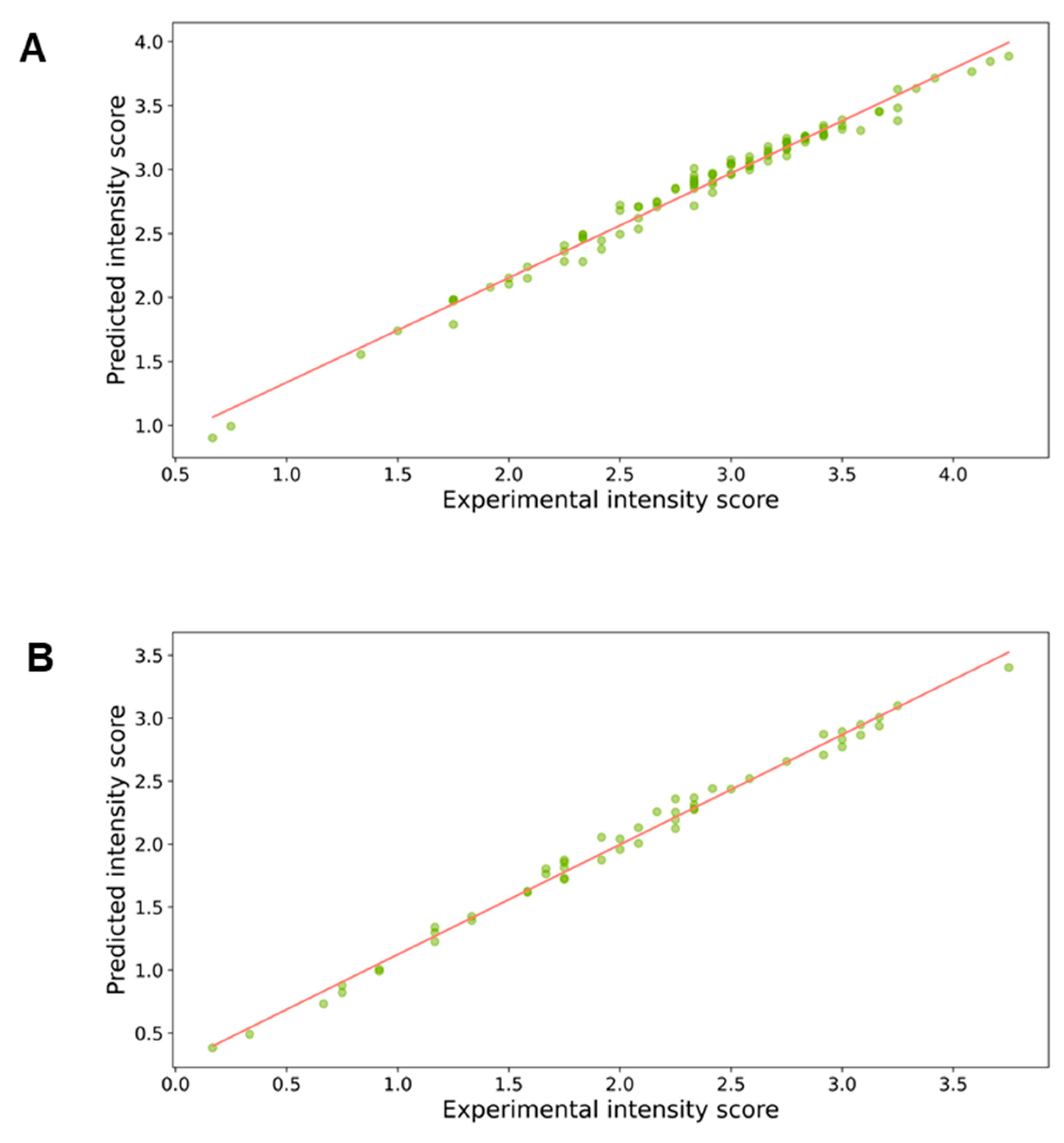
Figure 3.
Importance and impact of the sensory, clinical, and anthropometric features on the overall taste status prediction determined with Random Forest regressor in healthy controls. Importance of features in the learning of model to understand the overall taste status (A). The Y axis represents the order of the features’ importance, while the average impact on the model output is represented in the X axis. The SHAP summary plot in the healthy controls (B). The left-hand side of the Y-axis represents the descending order of importance; the X-axis represents the SHAP value i.e., the impact on the output model. The color represents the feature value: high values have a pink color, while low values have a blue one. Numbers indicated for each line represent the mean of the positive impact values and the negative impact of each feature.
Figure 3.
Importance and impact of the sensory, clinical, and anthropometric features on the overall taste status prediction determined with Random Forest regressor in healthy controls. Importance of features in the learning of model to understand the overall taste status (A). The Y axis represents the order of the features’ importance, while the average impact on the model output is represented in the X axis. The SHAP summary plot in the healthy controls (B). The left-hand side of the Y-axis represents the descending order of importance; the X-axis represents the SHAP value i.e., the impact on the output model. The color represents the feature value: high values have a pink color, while low values have a blue one. Numbers indicated for each line represent the mean of the positive impact values and the negative impact of each feature.
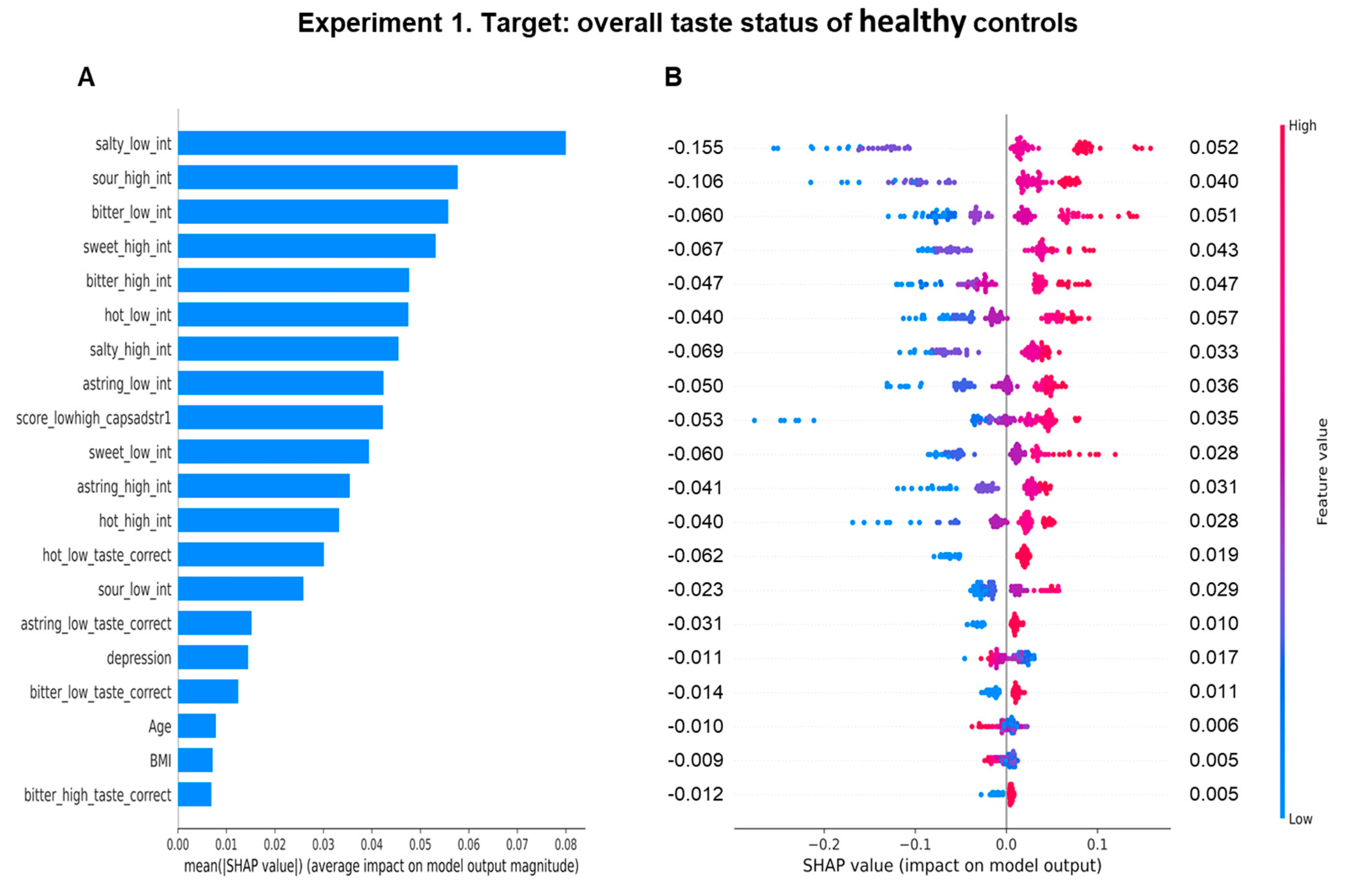
Figure 4.
Importance and impact of the sensory, clinical, and anthropometric features on the overall taste status prediction determined with Random Forest regressor in patients with chemosensory loss. Importance of features in the training model to understand the overall taste status (A). The Y axis represents the order of the features’ importance, while the average impact on the model output is represented in the X axis. The SHAP summary plot in patients with chemosensory loss (B). The left-hand side of the Y-axis represents the descending order of importance; the X-axis represents the SHAP value i.e., the impact on the output model. The color represents the feature value: high values have a pink color, while low values have a blue one. Numbers indicated for each line represent the mean of the positive impact values and the negative impact of each feature.
Figure 4.
Importance and impact of the sensory, clinical, and anthropometric features on the overall taste status prediction determined with Random Forest regressor in patients with chemosensory loss. Importance of features in the training model to understand the overall taste status (A). The Y axis represents the order of the features’ importance, while the average impact on the model output is represented in the X axis. The SHAP summary plot in patients with chemosensory loss (B). The left-hand side of the Y-axis represents the descending order of importance; the X-axis represents the SHAP value i.e., the impact on the output model. The color represents the feature value: high values have a pink color, while low values have a blue one. Numbers indicated for each line represent the mean of the positive impact values and the negative impact of each feature.
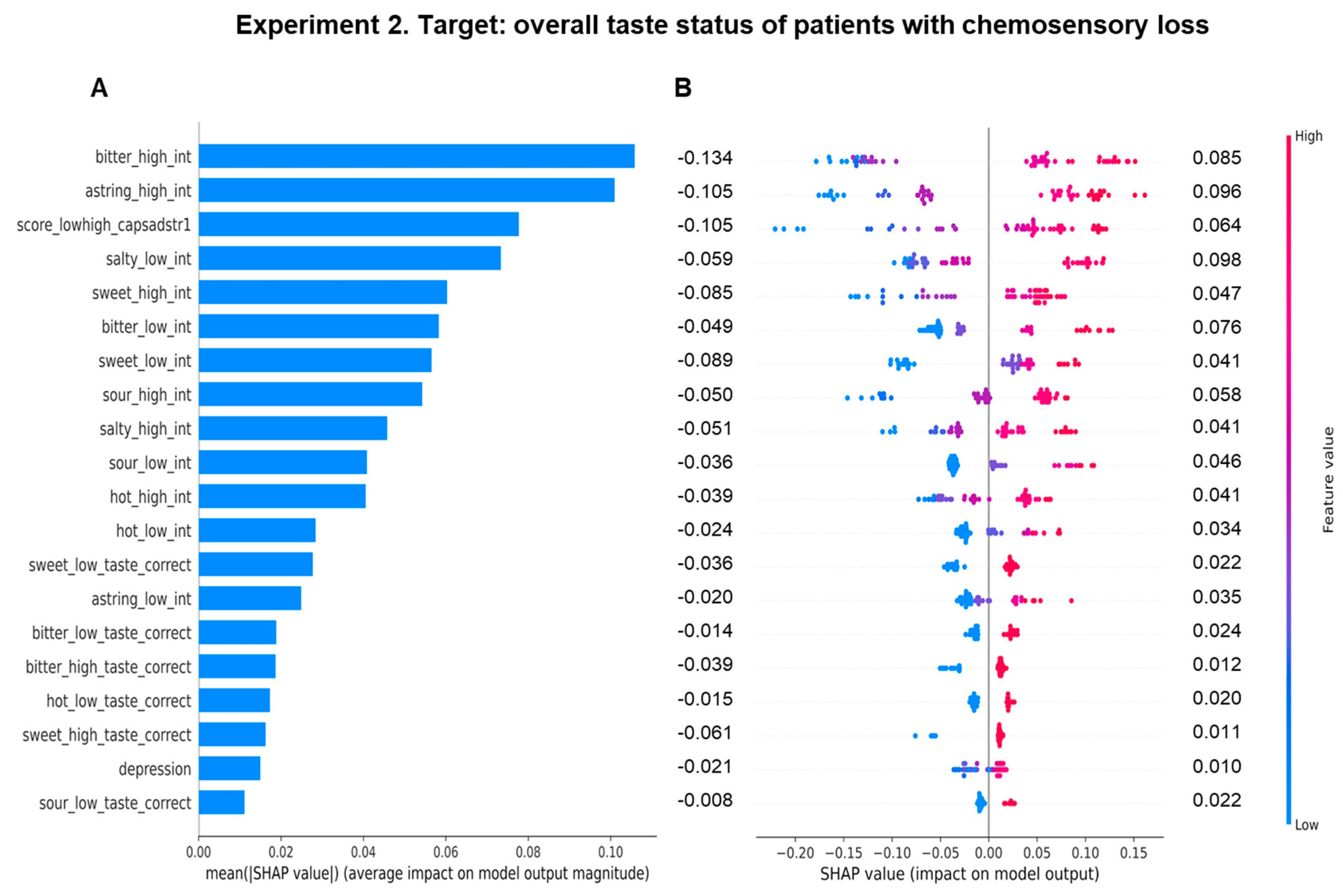

Table 1.
Sensory, clinical, and anthropometric parameters of healthy controls and patients with chemosensory loss.
Table 1.
Sensory, clinical, and anthropometric parameters of healthy controls and patients with chemosensory loss.
| Features | Healthy Controls (n = 102) | Patients with chemosensory loss (n = 51) | p-value |
|---|---|---|---|
| Numerical type | |||
| astring_low_int | 2.24 ± 1.32 | 0.84 ± 1.10* | < 0.0001 |
| bitter_low_int | 2.40 ± 1.49 | 1.06 ± 1.26* | < 0.0001 |
| hot_low_int | 2.04 ± 1.30 | 0.84 ± 1.24* | < 0.0001 |
| salty_low_int | 3.03 ± 1.07 | 1.92 ± 1.18* | < 0.0001 |
| astring_high_int | 3.53 ± 1.09 | 2.43 ± 1.43* | < 0.0001 |
| score_lowhigh_capsadstr1 | 9.37 ± 1.92 | 7.18 ± 2.47* | < 0.0001 |
| sour_high_int | 3.90 ± 0.85 | 3.27 ± 1.05* | 0.0001 |
| sweet_low_int | 1.99 ± 1.18 | 1.22 ± 1.14* | 0.0002 |
| sweet_high_int | 3.58 ± 0.89 | 2.90 ± 1.38* | 0.0003 |
| sour low int | 1.37 ± 1.22 | 0.68 ± 0.97* | 0.0006 |
| bitter_high_int | 3.15 ± 1.43 | 2.57 ± 1.43 | 0.018 |
| hot_high_int | 3.54 ± 1.16 | 3.04 ± 1.33 | 0.018 |
| salty_high_int | 3.79 ± 0.89 | 3.45 ± 1.27 | 0.054 |
| depression | 17.15 ± 3.62 | 14.14 ± 5.18* | < 0.0001 |
| BMI (kg/m2) | 23.66 ± 4.02 | 25.61 ± 5.55 | 0.014 |
| Age (y) | 36.70 ± 14.43 | 40.45 ± 12.62 | 0.116 |
| Categorial type | |||
| astring_low_taste_correct/non (n) | 78/24 | 15/36# | < 0.0001 |
| astring_high_taste_correct/non (n) | 86/16 | 24/27# | <0.0001 |
| hot_low_taste_correct/non (n) | 77/25 | 18/33# | <0.0001 |
| salty_low_taste_correct/non (n) | 87/15 | 33/18# | 0.0039 |
| sour_high_taste_correct/non (n) | 93/9 | 36/15# | 0.0014 |
| bitter_low_taste_correct/non (n) | 63/39 | 22/29# | 0.0221 |
| sweet_high_taste_correct/non (n) | 100/2 | 46/5# | 0.0415 |
| sour_low_taste_correct/non (n) | 32/70 | 10/41 | 0.0877 |
| sweet_low_taste_correct/non (n) | 72/30 | 32/19 | 0.2122 |
| hot_high_taste_correct/non (n) | 97/5 | 46/5 | 0.2061 |
| bitter_high_taste_correct/non (n) | 77/25 | 39/12 | 0.531 |
| salty_high_taste_correct/non (n) | 90/12 | 45/6 | 0.596 |
| Like_to_eat_spicy/non (n) | 66/36 | 23/28# | 0.016 |
| sex_f1_m2 (women/men; n) | 65/37 | 36/15 | 0.255 |
Values are means ± SD, or number correct answers, or number of subjects. Body Mass Index, BMI; significant differences in mean values between healthy controls and patients with chemosensory loss are indicated by * (p ≤ 0.0006; T test adjusted by Bonferroni correction), while differences in frequency distribution are indicated by # (p < 0.041; Fisher's method).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



