Submitted:
04 July 2023
Posted:
04 July 2023
You are already at the latest version
Abstract
: Forty-nine children who started wearing cartilage conduction hearing aids (CC-HA) before elementary school graduation (including 17 cases of bilateral hearing loss and 32 cases of unilateral hearing loss) were followed up and examined. The wearing and utilization status of CC-HA, as well as the progress to date, were evaluated. In addition, 33 participants who purchased CC-Has were interviewed to assess the wearing effect. Eleven of the 17 children with bilateral hearing loss and 25 of the 32 children with unilateral hearing loss have continued using CC-HA. In terms of wearing effect, a good wearing effect was reported, even by those with one-sided hearing loss. In cases where it is difficult to wear CC-HAs stably with pasting or ear tips, it is possible to fix them stably using commercially available hair bands and eyeglass vines. In two cases, CC-HAs were worn from the age of 0. With ingenuity and appropriate educational and medical support, it is possible to wear CC-HA from infancy.
Keywords:
Atresia
; Cartilage conduction hearing aids
; Conductive hearing loss
; Infant
1. Introduction
The pathway for sound transmission to the inner ear is divided into air conduction (AC) and bone conduction (BC), and hearing aids have been broadly classified into AC and BC hearing aids. In 2004, Hosoi reported that applying vibrations to the auricular cartilage can transmit audible sounds with clarity that is similar to that of AC or BC, leading to the development of a new type of hearing aid called cartilage conduction hearing aids (CC-HAs) [1].
CC-HAs can amplify and transmit sound signals to the inner ear simply by attaching a vibration generator to the skin of the auricular cartilage [2,3]. In contrast, bone conduction hearing aids (BC-HAs) also use a vibration generator placed on the body but require strong pressure and fixation on the temporal bone [4,5,6,7,8]. Both types of hearing aids are suitable for individuals with conductive hearing loss or mixed hearing loss, who cannot wear AC-HAs, and those who have good bone conduction thresholds, such as individuals with microtia or external auditory canal atresia .
Since the release of CC-HAs, the attachment-only method has become the preferred option and has gained popularity as an alternative to BC-HAs [2,3,9,10,11,12,13,14,15], particularly in pediatric cases[16]. Since 2020, safety measures, such as battery boxes, have been fully integrated, allowing the use of the device even for children under the age of 3 years. In the case of infants, there are many opportunities to re-examine the possibility of using CC-HAs after starting from BC-HAs; however, there have been no reports of starting use from infancy. Therefore, in this study, we investigate the usage and wearing progress of CC-HAs in infants and toddlers, present cases of its application from infancy, and discuss its suitability based on the growth of children.
2. Materials and Methods
2.1. Participants
This study enrolled 49 children (17 children with bilateral hearing loss and 32 children with unilateral hearing loss), including 28 boys and 21 girls, in whom trial hearing was initiated using a CC-HA before primary school age at our hospital. The guardians/parents of these children had requested the use of a CC-HA. Trial hearing was initiated between the ages of 0 (3 months old) and 11 years in children with bilateral hearing loss and between 0 (6 months old) and 10 years in those with unilateral hearing loss. The mean age of the participants was 5.02 ± 2.71 (SD) years.
Figure 1 presents the age distribution of the participants at the time of the initiation of trial hearing. Figure 2 presents the ratios of the diagnoses of the ears fitted with CC-HA (HB-J1CC, HB-A2CC, RION Co., LTD, Tokyo, Japan).
Figure 1.
Age distribution of the participants at the time of the initiation of trial hearing. (n=49).
Figure 1.
Age distribution of the participants at the time of the initiation of trial hearing. (n=49).
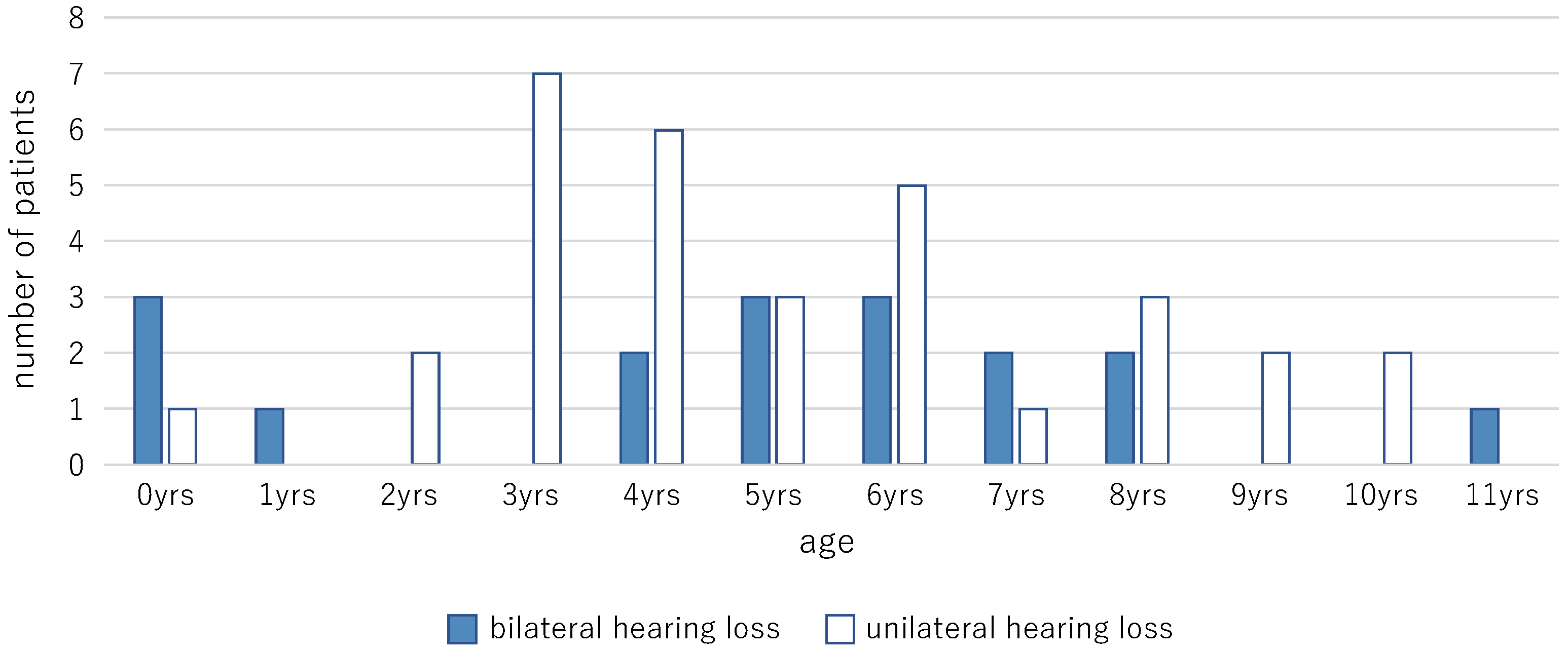
Figure 2.
Diagnoses of the fitted ears.
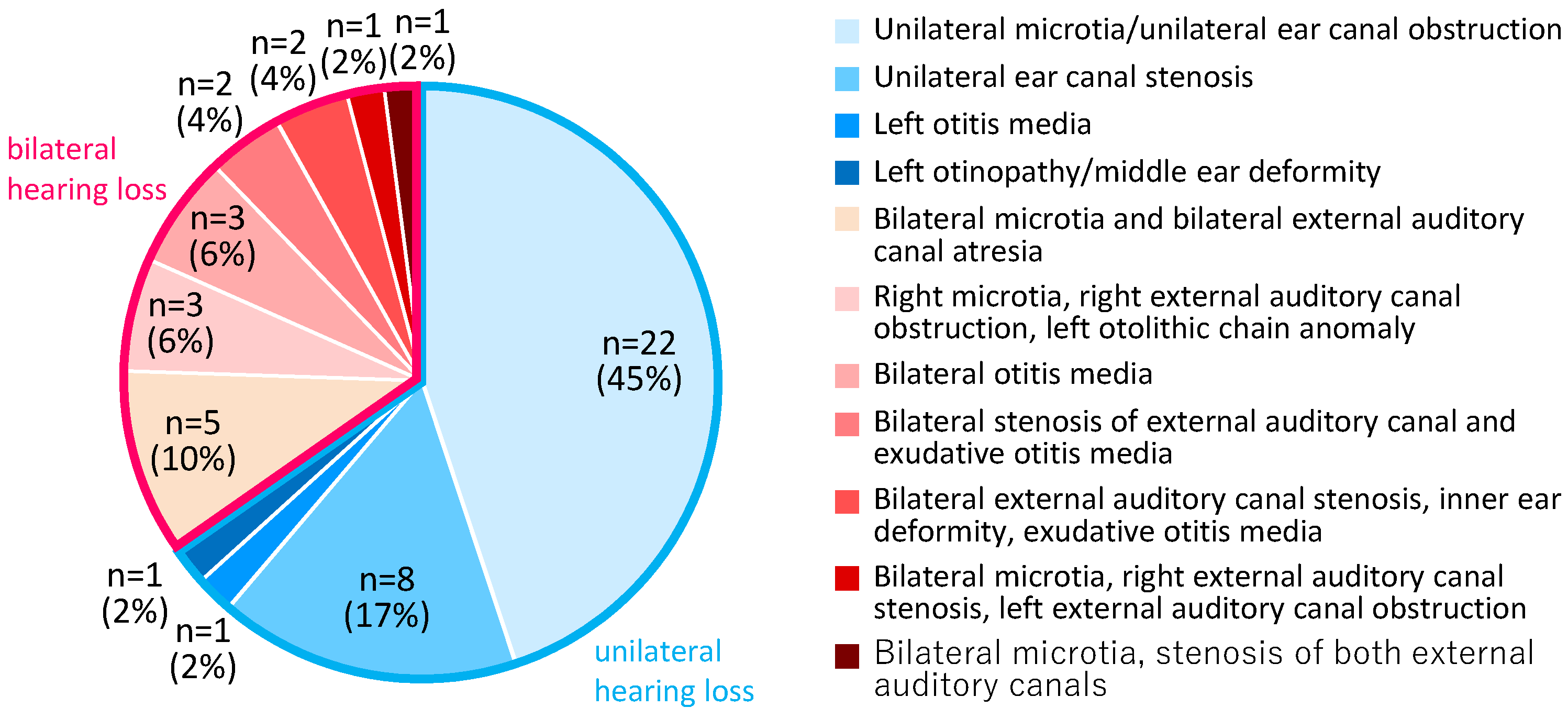
Among the participants with bilateral hearing loss, eight participants had conductive hearing loss, eight participants had mixed hearing loss, and one participant could not undergo bone conductometry. Among the participants with unilateral hearing loss, 29 participants had conductive hearing loss, one participant had mixed hearing loss, and two participants could not undergo bone conductometry. Among the participants with bilateral hearing loss, two participants had chromosome 21 trisomy, and one participant each had Treacher Collins syndrome, chromosome 18 trisomy, FOXP1 syndrome, and Primrose syndrome.
The presence of a history of hearing aid use was not observed in cases of unilateral hearing loss, and it was only observed in five out of the 17 cases of bilateral hearing loss (BC-HA: two cases at the age of 6 and 7, unilateral-AC-HA : one case at the age of 5).
2.2. Hearing Assessment
The auditory thresholds were assessed by an experienced audiologist in a standard soundproof room using a commercially available audiometer (Model AA-HI, RION Co, LTD, Tokyo, Japan). Pure tone thresholds were determined using over-ear headphones (125 Hz to 8 kHz) for the assessment of air conductance thresholds and a calibrated bone-conducting transducer (500 Hz to 4 kHz) for the assessment of bone conductance thresholds. Sound field thresholds (SF) were evaluated to assess the effects of CC-HAs. Complementary and non-complementary hearing thresholds were assessed by introducing an azimuth angle of 0° and transmitting warble tones from a loudspeaker positioned 1 m away from the participant. As CC-HAs were fitted on only one side in participants with unilateral hearing loss, masking noise was provided to the other ear through headphones such that the test tone could not be heard. The complementary hearing threshold for CC-HAs cannot be assessed accurately in participants with unilateral hearing loss; therefore, the assessment of the hearing threshold was used as the reference value. Behavioral hearing tests, such as behavioral observation audiometry (BOA) and visual reinforcement audiometry (VRA), were used to assess the hearing ability if the participant was too young to undergo the hearing tests described above. The behavioral hearing tests were performed in a manner similar to those used in previous reports from Japan[17].
2.3. Adjustment and Fitting of the Devices and Ethical Standards
The devices were fitted at the Sugiuchi Clinic. The participant or the guardian was provided explanations regarding CC-HAs. Concurrently, ENT examinations, hearing tests, and imaging were conducted to confirm the HA history and indications prior to initiating trial hearing. Trial hearing with the fitted CC-HA was continued for 1–3 three months free of charge, and the participants were instructed to assess the usefulness and comfort of using CC-HA in their daily lives during the trial hearing period.
The initial adjustment of the hearing aids was performed using the Sedation level version 5 (DSL v5) procedure[18]. This procedure and the determination of the hearing threshold for CC-HAs were similar to those for AC-HAs. After the hearing aid was tested in the outpatient setting, the hearing threshold was assessed, and the gain and output of the hearing aid were predicted. Fine adjustments were made if necessary. Subsequently, trial hearing was continued for a period of 1–2 weeks in real-life settings. The fitting condition and effectiveness of the hearing aid were evaluated during this period, and the hearing aid was readjusted based mainly on the user’s wishes. The listening tests and adjustments were repeated until the participant or the guardian made the decision regarding whether to purchase the hearing aid without any psychological burden on the participant.
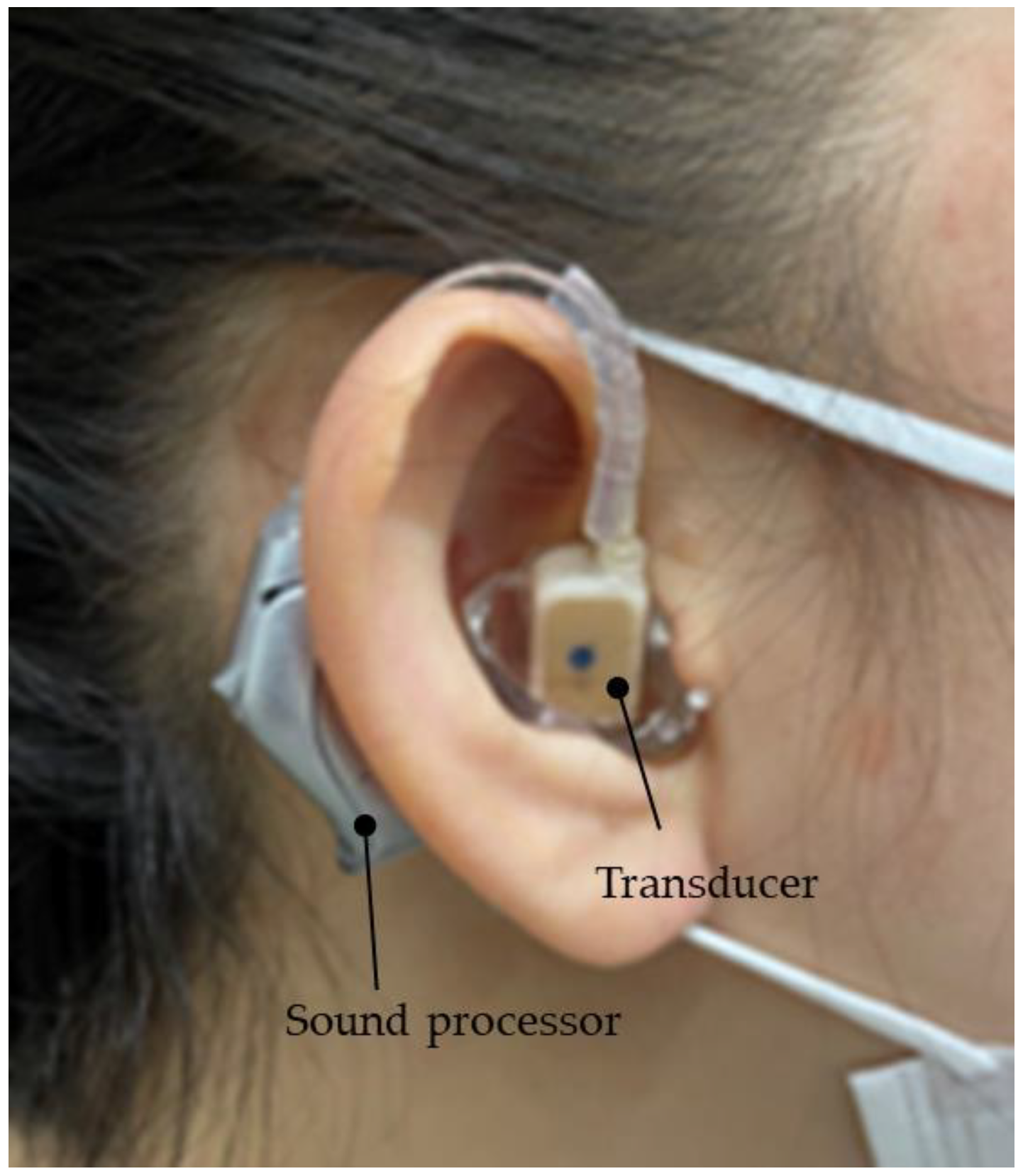
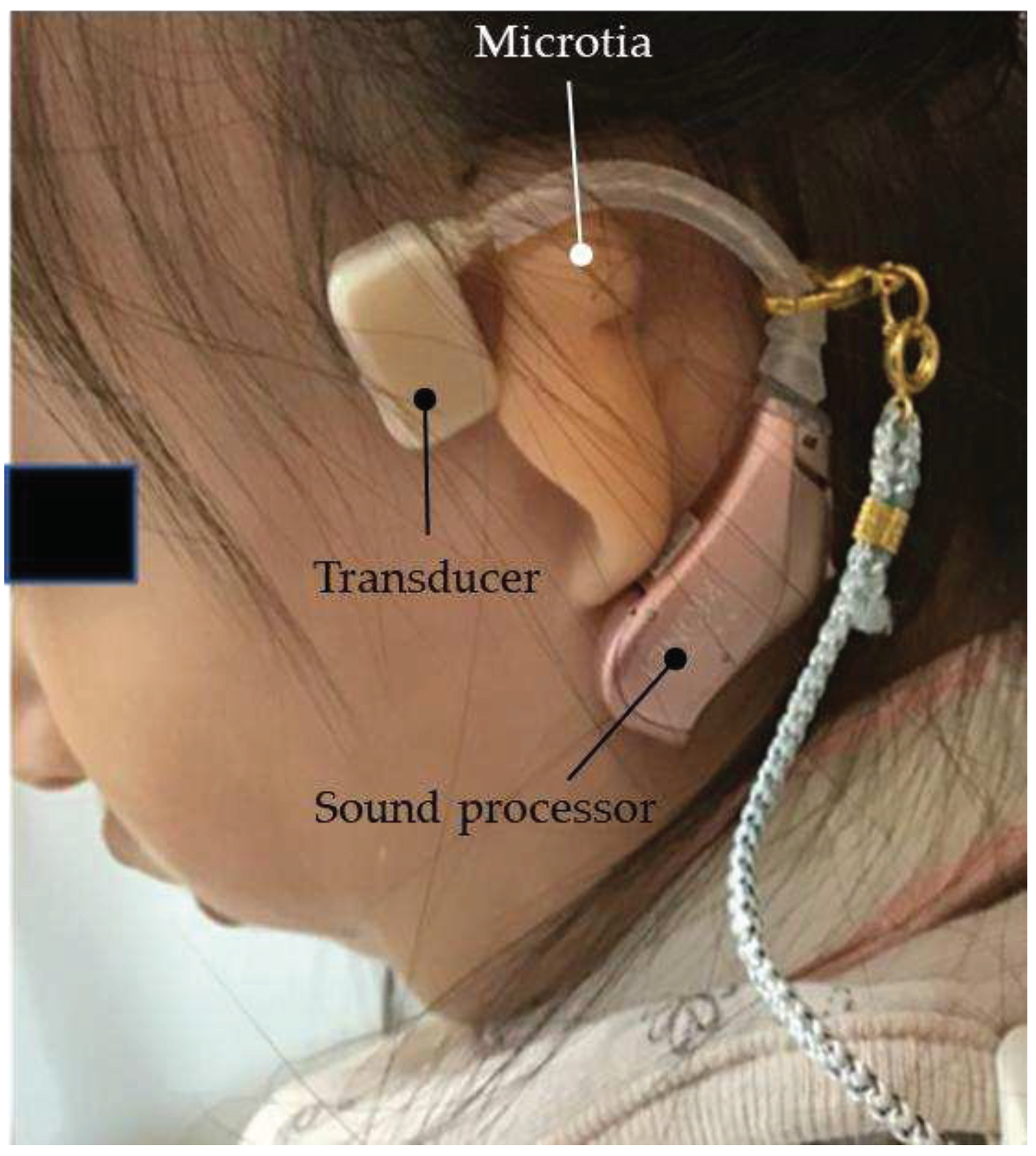
The vibration terminal (transducer) of the CC-HA was attached to the skin overlying the tragus cartilage and fixed with double-sided adhesive tape. As the morphology and location of the tragus and auricular cartilage have not been mapped well in patients with microtia or congenital aural atresia, the transducer was carefully applied to the skin overlying the cartilage near the assumed location of the tragus with a subtle concavity (Figure 3). The sound processor of the CC-HA was affixed to the skin overlying the posterior auricle with double-sided adhesive tape. An earmold (hereafter referred to as an ear-tip) was fabricated if attachment with adhesive tape was difficult or if the attachment was unstable, and the transducer was attached to a depressed area such as the cavity of the concha (Figure 4).
Figure 3.
Profile view (left side) of a patient with congenital external ear canal atresia fitted with a cartilage conduction hearing aid (CC-HA). The transducer and sound processor components of the CC-HA (HB-J1CC, RION Co., LTD; Tokyo, Japan) are attached to the skin using a double-sided adhesive tape.
Figure 3.
Profile view (left side) of a patient with congenital external ear canal atresia fitted with a cartilage conduction hearing aid (CC-HA). The transducer and sound processor components of the CC-HA (HB-J1CC, RION Co., LTD; Tokyo, Japan) are attached to the skin using a double-sided adhesive tape.
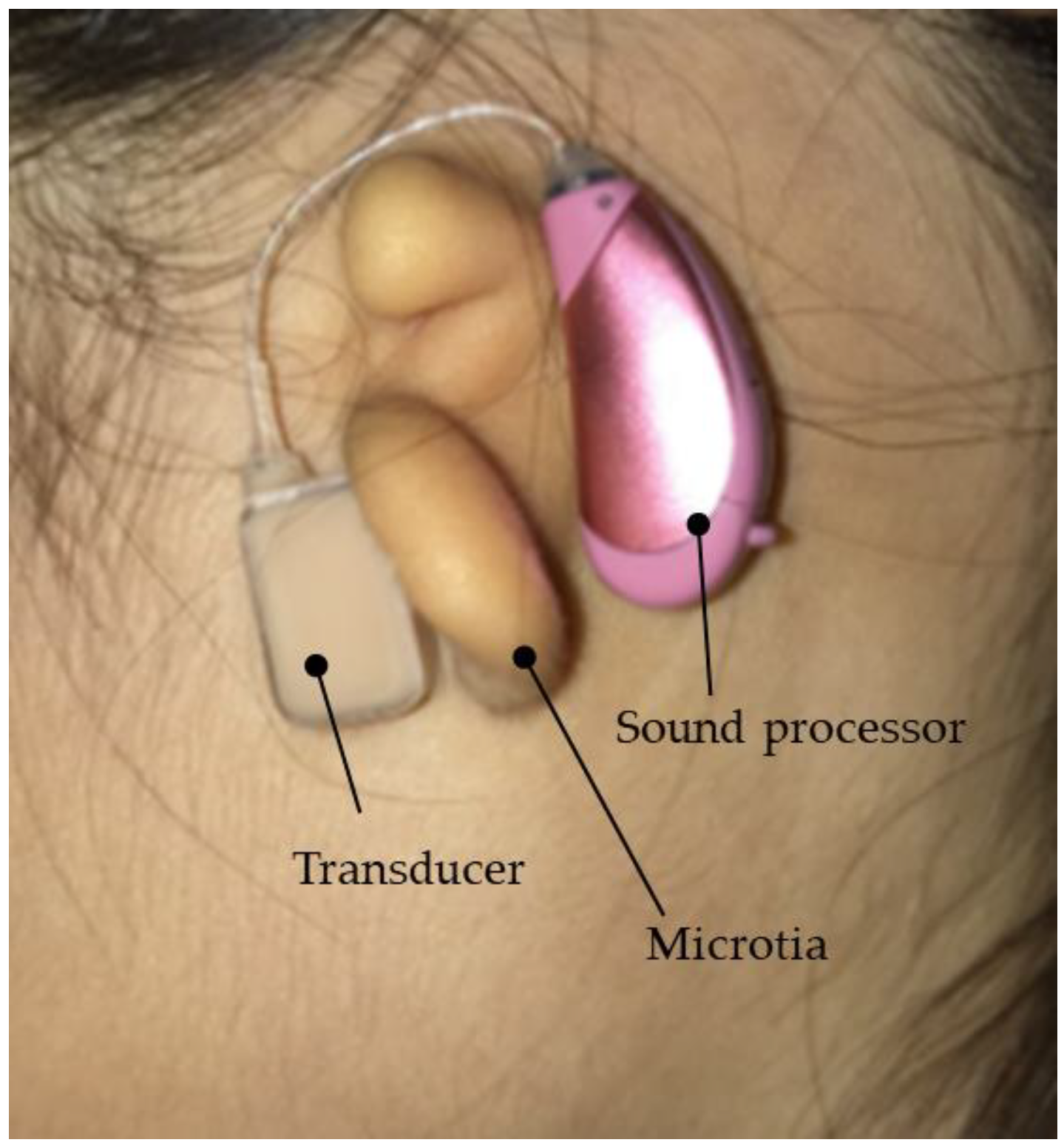
Figure 4.
Profile view (right side) of a patient with congenital external ear canal atresia fitted with a cartilage conduction hearing aid (CC-HA). The transducer (with ear tips) is attached to the skin using a double-sided adhesive tape (sound processor components of the CC-HA: HB-J1CC, RION Co., LTD; Tokyo, Japan).
Figure 4.
Profile view (right side) of a patient with congenital external ear canal atresia fitted with a cartilage conduction hearing aid (CC-HA). The transducer (with ear tips) is attached to the skin using a double-sided adhesive tape (sound processor components of the CC-HA: HB-J1CC, RION Co., LTD; Tokyo, Japan).
In principle, the initial hearing test was initiated in the manner described above. CC-HAs were attached to the posterior part of both auricles in participants with bilateral hearing loss. CC-HAs were fitted to the affected ear in participants with unilateral hearing loss similar to that in those with unilateral congenital auricular atresia. Two CC-HAs were fitted in participants with bilateral hearing loss similar to that in those with bilateral congenital auricular atresia. The test hearing conditions were the same for participants with one and two CC-HAs.
Explanations regarding the indicated hearing aids, such as bone-conduction hearing aids, BAHAs(Cochlear Limited, Sydney, Australia) and ADHEAR system(MED-EL, Innsbruck, Austria) were also provided, and demonstrations via test hearing were provided, if possible, upon request. Furthermore, the rehabilitation staff at the rehabilitation institution were provided information regarding the need for hearing aids and the model and adjustment of the hearing aids. The final decision regarding the purchase of the hearing aid was made by the parents based on the hearing aid use thresholds and the combined observations and evaluations of the parents and caregivers.
This study was conducted in accordance with the "Ethical Principles for Medical Research Involving Human Subjects" [19]as stated in the Declaration of Helsinki and approved by the Ethics Committee of the Kanto Rosai Hospital (Approval No.: 2023-1). The details of the study were posted in the examination room of the clinic. Verbal informed consent was obtained from all participants and their guardians. The requirement for written consent was waived according to the ethical guidelines for medical and health sciences research involving human participants [20]. The information regarding the study, including the purpose of collecting information and its use, was made publicly available or notified to the research participants. The study participants and their guardians were informed that they could refuse participation at any time and request that their data be deleted after the study was started. This information was also included in the medical records of each participant.
2.4. Purchase Rate and the Evaluation of Cases That Did and Did Not Purchase CC-HA(s)
The overall purchase rate was evaluated, and the participants were divided into two groups based on whether the CC-HA was purchased: the purchase and non-purchase groups. Information regarding the age, sex, condition of the ear fitted with the hearing aid (affected or good ear), and the mean hearing thresholds (500 Hz, 1000 Hz, and 2000 Hz) of the participants was collected and used for comparison. The participants who were too young to undergo hearing assessments, such as sound field thresholds, were excluded from the study.
2.5. A Simple Way to Improve Hearing Aid Fixation
The following methods were used when the hearing aids could not be stabilized by attaching the transducers and sound processors of CC-HAs.
2.5.1. Use of a Hairband
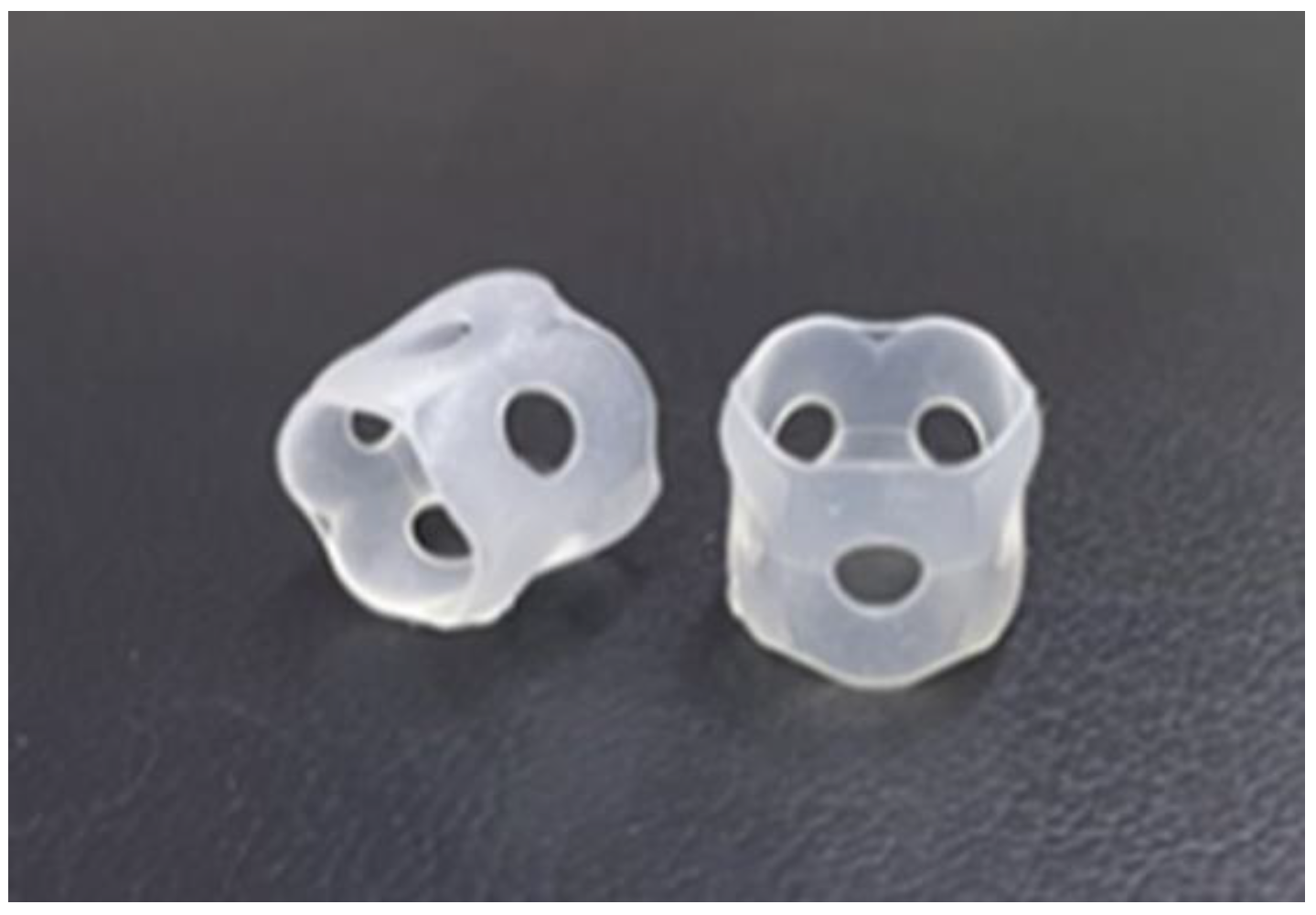
In this method, a silicone rubber was sewn onto a commercially available flat rubber-like hair band to which the hearing aid body was fixed. The transducer was subsequently attached with a double-sided adhesive tape (Figure 5 and Figure 6).
Figure 5.
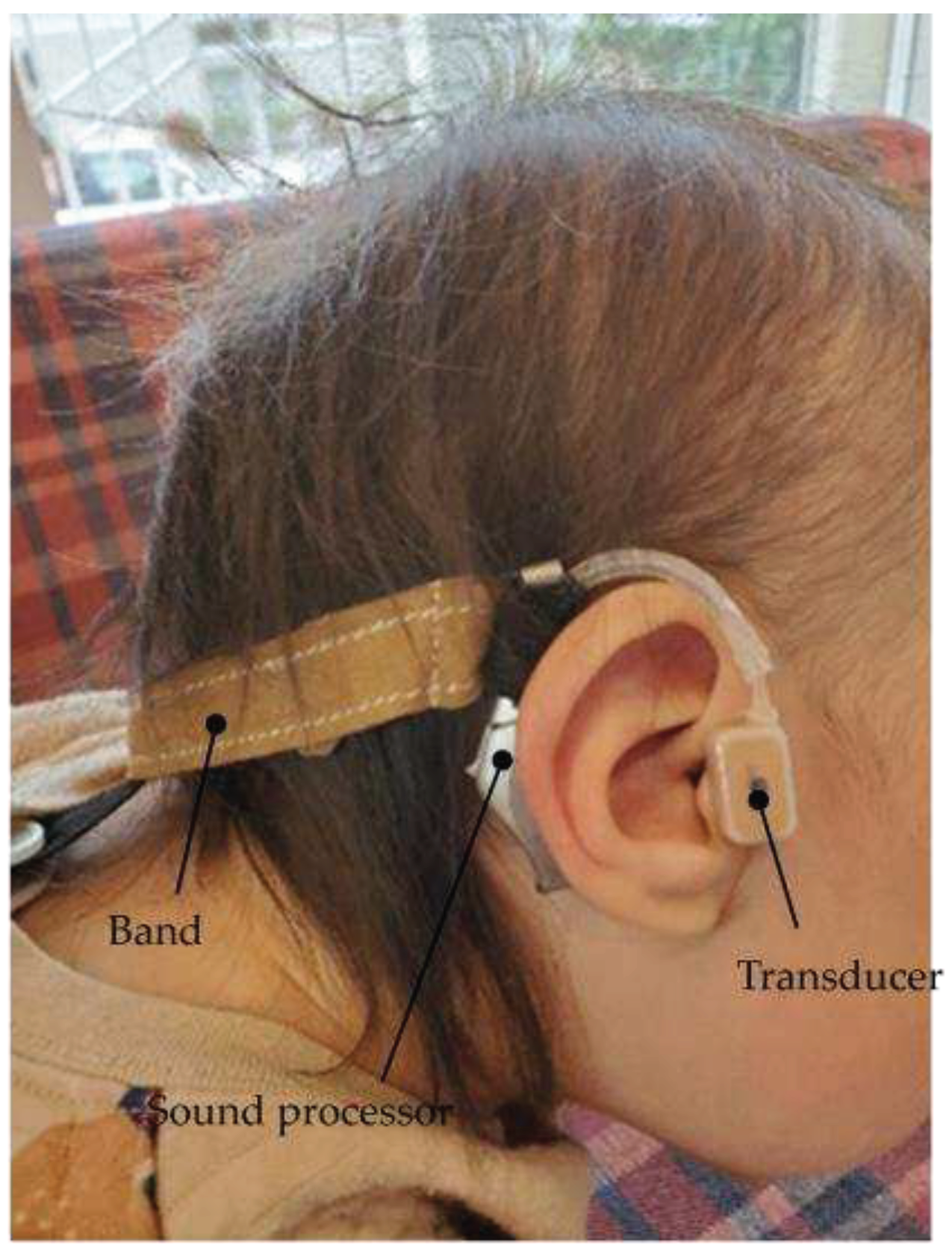
Profile view (right side) of a patient with Downs syndrome who has bilateral external ear canal stenosis with exudative otitis media and congenital external ear canal atresia fitted with a cartilage conduction hearing aid (fixed onto the headband with silicone rubber). The transducer is attached to the skin using a double-sided adhesive tape.
Figure 5.
Profile view (right side) of a patient with Downs syndrome who has bilateral external ear canal stenosis with exudative otitis media and congenital external ear canal atresia fitted with a cartilage conduction hearing aid (fixed onto the headband with silicone rubber). The transducer is attached to the skin using a double-sided adhesive tape.
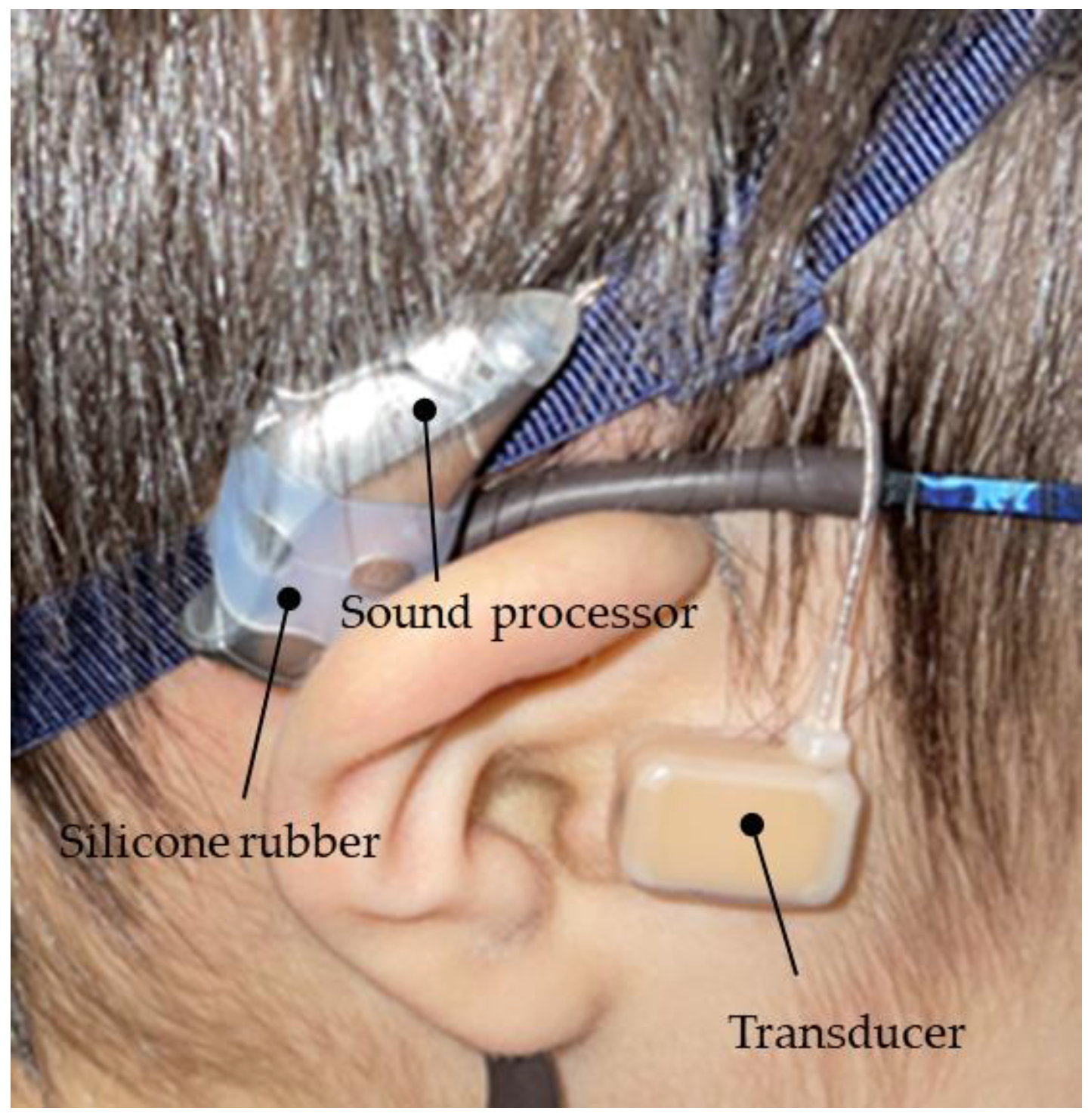
Figure 6.
Silicone rubber, which is sold as a stationery item, can be used for attaching the main body of the hearing aid to the temple of the glasses or headbands.
Figure 6.
Silicone rubber, which is sold as a stationery item, can be used for attaching the main body of the hearing aid to the temple of the glasses or headbands.
2.5.2. Use of Eyeglasses
In this method, the sound processor of the CC-HA was fixed to the temple of the glasses with rubber or silicone rubber, and the transducer was attached subsequently (Figure 7).
Figure 7.
Profile view (left side) of a patient with bilateral external auditory canal stenosis with exudative otitis media wearing a cartilage conduction hearing aid fixed to the temples of glasses. The transducer is attached to the skin using a double-sided adhesive tape.
Figure 7.
Profile view (left side) of a patient with bilateral external auditory canal stenosis with exudative otitis media wearing a cartilage conduction hearing aid fixed to the temples of glasses. The transducer is attached to the skin using a double-sided adhesive tape.

2.6. Evaluation after Purchase
The participants or their guardians who purchased CC-HA were interviewed during the consultation to understand the post-purchase status, and the participants were evaluated. The questions included the duration of hearing aid use, the effectiveness of hearing aid use, and their requests regarding hearing aid use. Questions and options regarding the duration of hearing aid use and the effectiveness of hearing aid use were determined in advance.
3. Results
3.1. Purchase Rates and Differences between the Participants Who Did and Did Not Purchase CC-HAs
Among the 17 participants with bilateral hearing loss, 11 (64.7%) participants purchased CC-HAs. Among the 32 cases with unilateral hearing loss, 25 (78.1%) participants purchased CC-HAs. We examined the average hearing thresholds according to age, bilateral hearing loss, and unilateral hearing loss and divided the participants into the purchase and non-purchase groups; however, no significant correlations were observed among any of the items (Table 1). Among the participants with bilateral hearing loss who purchased CC-HAs, three participants (17.6%) used CC-HA only on one side, whereas an AC-HA was used on the opposite side with external auditory canal stenosis or inner ear/middle ear anomalies. None of the participants reported experiencing complications, such as skin irritation, with the use of CC-HAs.

Table 1.
Wearing effect.
| Answer Question |
Bilateral Hearing Loss (n=11) | Unilateral Hearing Loss (n=22) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Strongly Agree |
Agree | Disagree | Imponderable | Strongly Agree |
Agree | Disagree | Imponderable | |||||||||
| ① Improved ability to hear soft sounds such as whispers. | 2 | 18% | 5 | 45% | 1 | 9% | 3 | 27% | 7 | 32% | 12 | 55% | 1 | 5% | 2 | 9% |
| ② Improved ability to understand conversations in noisy environments such as parks or restaurants. | 1 | 9% | 5 | 45% | 2 | 18% | 3 | 27% | 5 | 23% | 8 | 36% | 3 | 14% | 6 | 27% |
| ③ Improved ability to notice when someone calls from behind. | 1 | 9% | 6 | 55% | 1 | 9% | 3 | 27% | 8 | 36% | 11 | 50% | 1 | 5% | 2 | 9% |
| ④ Improved ability to understand conversations involving multiple people. | 1 | 9% | 3 | 27% | 3 | 27% | 4 | 36% | 3 | 14% | 2 | 9% | 1 | 5% | 6 | 27% |
Table 2.
Characteristics of the purchasing and non-purchasing Groups.
| Characteristics | Purchase Group | Non-Purchase Group | P Value |
|---|---|---|---|
| Age at fitting (yr, Mean ± SD) | 5.3±2.6 (n=36) |
4.4±3.0 (n=13) |
0.376 |
| Bilateral hearing loss, Average hearing thresholda of the better ear (dB HL, Mean ± SD) |
46.5±17.3 (n=8) |
56.7±16.7 (n=3) |
0.427 |
| thresholda of the worse ear (dB HL, Mean ± SD) |
65.8±20.3 (n=8) |
61.7±22.5 (n=3) |
0.796 |
| Unilateral hearing loss, Average hearing thresholda of the better ear (dB HL, Mean ± SD) |
9.7±5.2 (n=24) |
9.6±3.4 (n=4) |
0.948 |
| thresholda of the worse ear (dB HL, Mean ± SD) |
70.4±12.2 (n=24) |
59.6±16.3 (n=4) |
0.281 |
a Average of AC hearing thresholds at 500, 1000, and 2000 Hz. b Independent t-test. c Chi-square test.
3.2. Participants Who Did Not Purchase CC-HAs
There were various reasons for not purchasing CC-HAs. Among the five participants with bilateral hearing loss in the non-purchase group, the parents of a 3-month-old infant selected BC-HA due to its ease of attachment and detachment. The parents of a 6-month-old infant started using BC-HA at a different hospital. The parents of a 7-year-old with bilateral microtia, who was currently using BC-HA (with a fabric headband), wished to continue using BC-HA until ear reconstruction surgery. A child with right external auditory canal stenosis and left middle ear anomaly was found to have an enlarged right external auditory canal during the process of making an ear impression for CC-HA ear tip fabrication; thus, AC-HA was selected.
Furthermore, a 4-year-old child with chronic otitis media and immunodeficiency with selective IgG2 deficiency (Primrose syndrome [21]) had the intention of avoiding middle ear infections through HA usage. However, surgical therapy proved successful before achieving stable usage.
Seven participants with unilateral hearing loss in the non-user group refrained from purchasing HA due to their personal reluctance to use it.
3.3. Case Reports
3.3.1.
. Case 1 was a 3-year-2-month-old girl born at 37 weeks and 1 day of gestation weighing 2,690 g. The patient had multiple malformations (Treacher Collins syndrome), including micrognathia, ptosis, down-slanted palpebral fissures, and cleft palate. Tracheotomy was performed at 9 days. The patient required medical care and attended a school for the deaf and Kotoba-no-mori.
The first visit was at the age of 6 months. Trial hearing with a CC-HA with both the transducer and body attached was initiated, and the clinical course was mostly favorable. Trial hearing with a BC-HA (with a fabric headband) was initiated for comparative listening. Both hearing aids were found to have similar wearing efficacy (Figure 8). However, the parents of the participant purchased the CC-HA as the participant was able to remove the BC-HA, and it could not be stabilized. In addition, the participant's mother believed that CC-HA was easier to work with. Around the age of 9 months, it became somewhat noticeable that the participant could remove the hearing aid immediately after fitting. Therefore, the hearing aid, including the transducer, was sewn into a ready-made hair band (Figure 9) at the age of 14 months. The hearing aid was worn for a longer duration, without changes to the threshold and favorable wearing efficacy. The participant’s mother modified the hair band at the age of 23 months. A silicon rubber was sewn to the outer side of the hair band such that the microphone on the CC-HA body was placed outside the hair band. The best wearing efficacy was obtained when a hole was created in the hair band such that the transducer was directly in front of the upper part of the ear, and the hair band was used to cover the transducer (Figure 10). At the age of 26 months, the patient attempted to wear the CC-HA body and the transducer by affixing. Initially, the duration of using the unit was limited; however, the duration increased gradually, and the participant uses the device throughout the day currently (Figure 11).
Figure 8.
Case 1: Comparison of Bone Conduction Hearing Aids Threshold and Cartilage Conduction Hearing Aids Threshold.
Figure 8.
Case 1: Comparison of Bone Conduction Hearing Aids Threshold and Cartilage Conduction Hearing Aids Threshold.
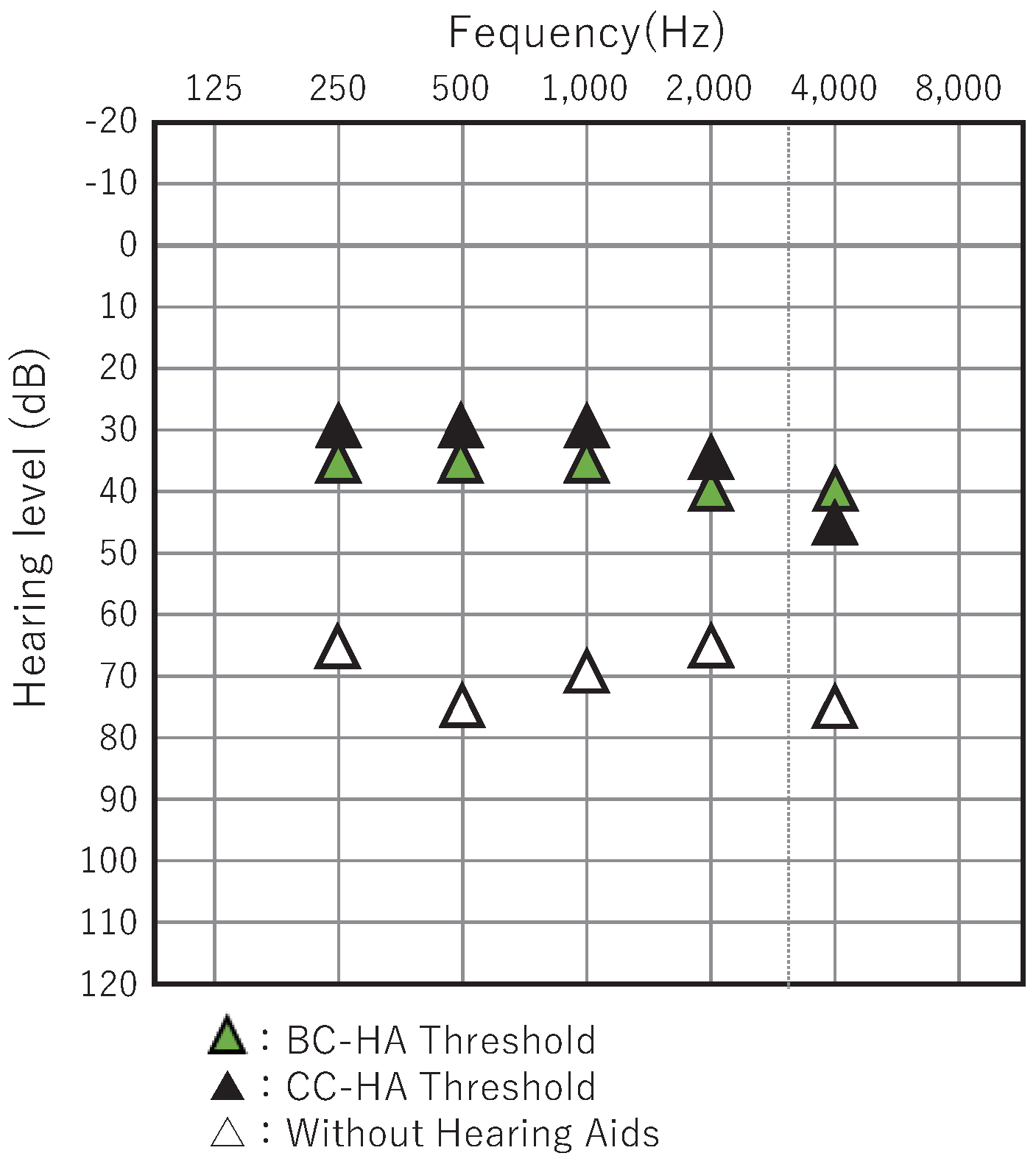
Figure 9.
Profile view (right side) of a 6-month-old patient with Treacher Collins syndrome who has bilateral external auditory canal stenosis with exudative otitis media wearing CC-HA. The main body of the hearing aid and the terminals are sewn into the inside of the headband.
Figure 9.
Profile view (right side) of a 6-month-old patient with Treacher Collins syndrome who has bilateral external auditory canal stenosis with exudative otitis media wearing CC-HA. The main body of the hearing aid and the terminals are sewn into the inside of the headband.
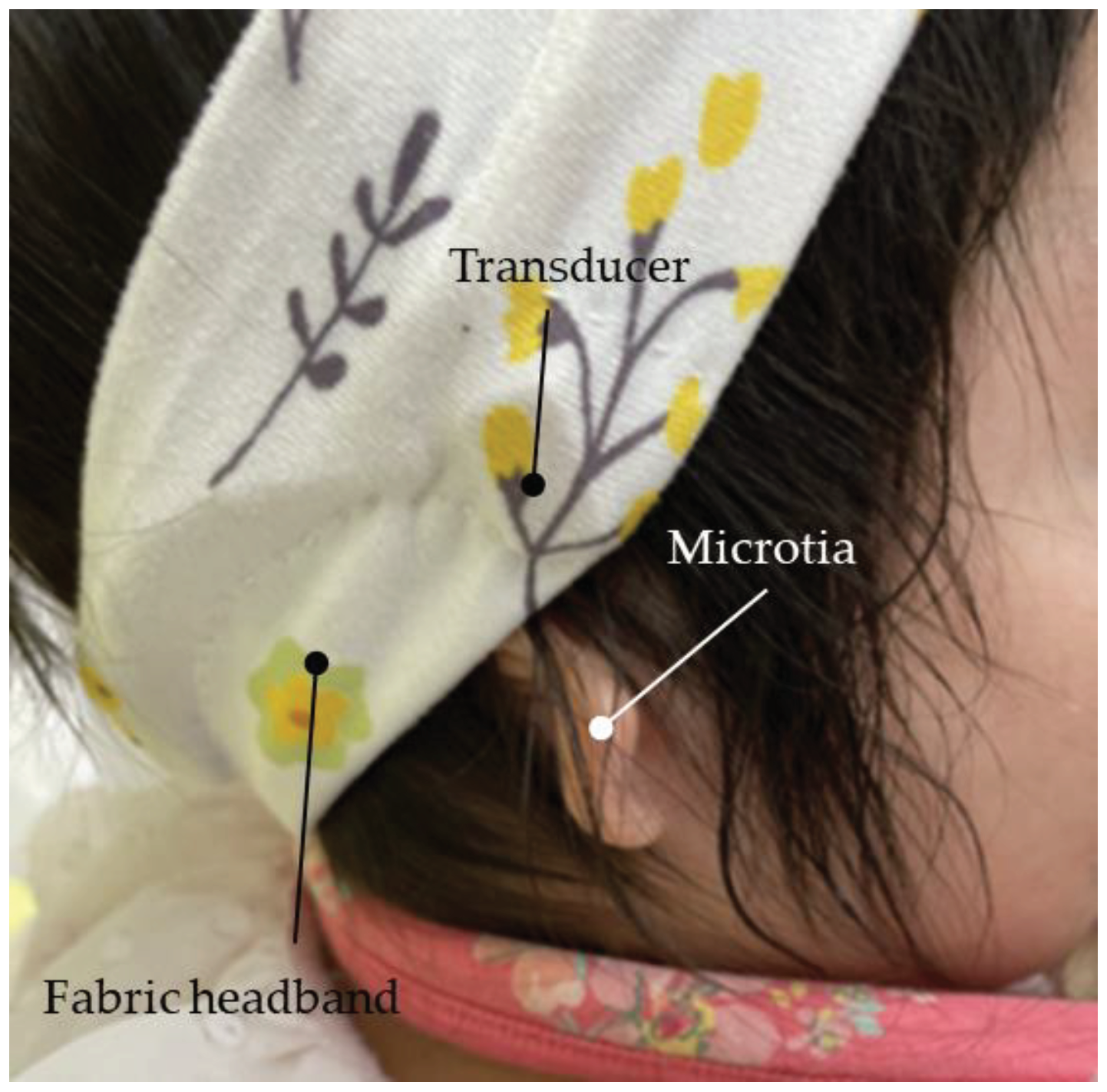
Figure 10.
Profile view ( left side) of Case 1 (a patient, who is over 1 years old, withTreacher Collins syndrome with bilateral external auditory canal stenosis and exudative otitis media) using cartilage-conducting hearing aid. The body of the hearing aid is sewn into the headband with the terminals attached using a double-sided tape.
Figure 10.
Profile view ( left side) of Case 1 (a patient, who is over 1 years old, withTreacher Collins syndrome with bilateral external auditory canal stenosis and exudative otitis media) using cartilage-conducting hearing aid. The body of the hearing aid is sewn into the headband with the terminals attached using a double-sided tape.

Figure 11.
Profile view (left side) of Case 1 (2 years old) with bilateral external auditory canal closure. The terminals and hearing aid body are attached using double-sided tape.
Figure 11.
Profile view (left side) of Case 1 (2 years old) with bilateral external auditory canal closure. The terminals and hearing aid body are attached using double-sided tape.
2.9.2.
. Case 2 is a child aged 1 year and 11 months who was born at 38 weeks of gestation, weighing 2,398 g. Chromosomal abnormalities (chromosomes 18 and 3) and FOX P1 syndrome were identified. The patient is currently receiving education at a municipal developmental facility. Significant stenosis was observed in both external auditory canals during the initial visit at the age of 1 year and 1 month. The possibility of conductive hearing loss was indicated by the auditory steady-state response (ASSR). Following the experience of Case 1, the hearing aid was attached to a commercially available cloth headband, with the transducer placed outside the band for testing purposes (Figure 12). By the age of 1 year and 2 months, the child could wear the hearing aid for approximately 6 hours a day, and the mother reported improved sound responsiveness with fewer instances of howling. As the child could remove the headband from the age of around 1 year and 5 months, the mother started attaching the main body and transducer directly to the skin for wearing. Currently, for safety reasons, the shoulder area is secured with a short strap, and the hearing aid is used without the headband for a few hours every day (Figure 13). The parents are considering using ear tips in the future.
Figure 12.
Profile view (right side) of Case 2 (severe bilateral external auditory canal stenosis). The terminals are attached using double-sided tape, and the body of the hearing aid is secured to a fabric headband for wearing.
Figure 12.
Profile view (right side) of Case 2 (severe bilateral external auditory canal stenosis). The terminals are attached using double-sided tape, and the body of the hearing aid is secured to a fabric headband for wearing.
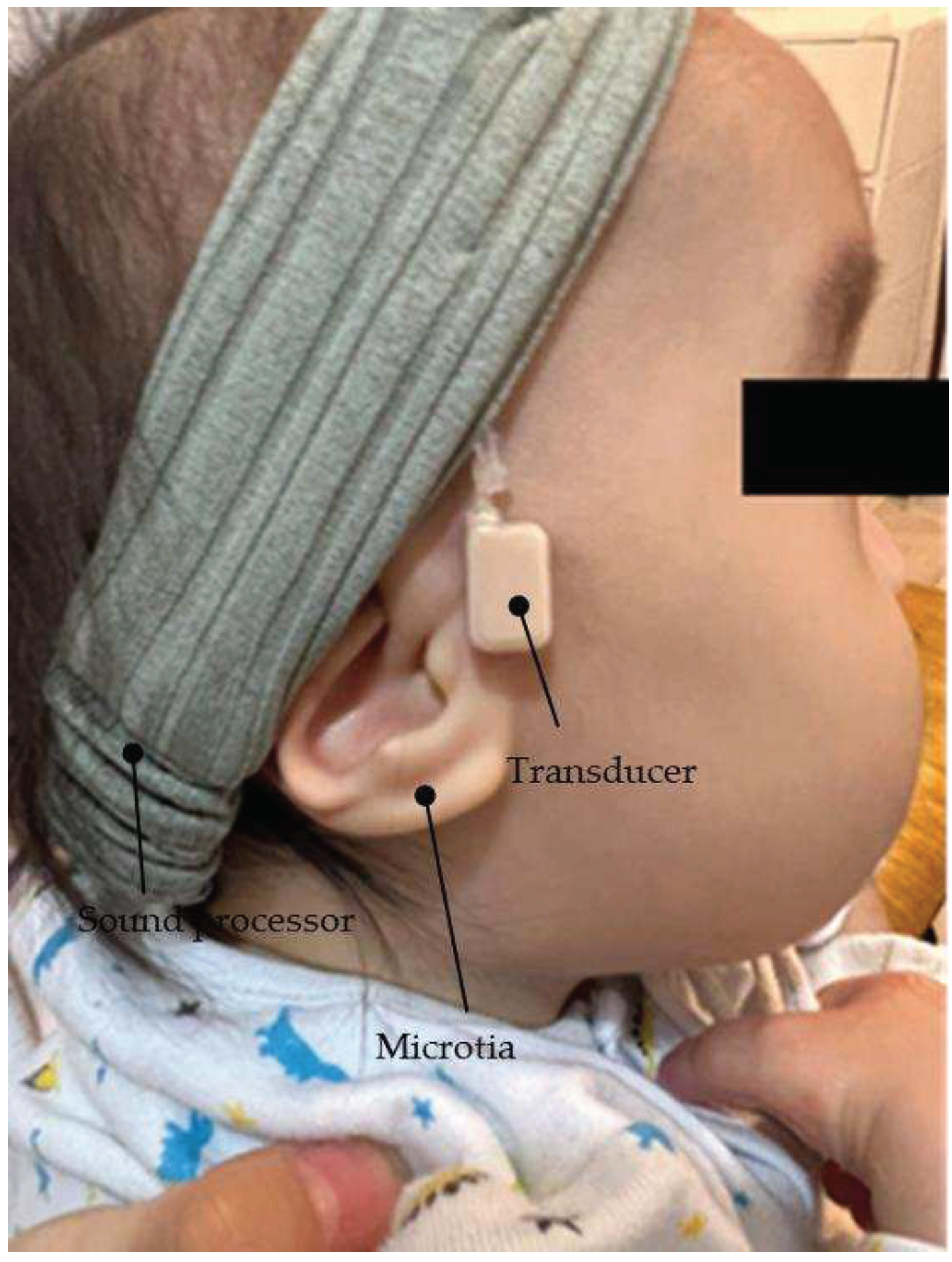
Figure 13.
Profile view (right side) of Case 2. The terminals and the body of the hearing aid body are attached using double-sided tape and secured to the back with a mischief-prevention belt.
Figure 13.
Profile view (right side) of Case 2. The terminals and the body of the hearing aid body are attached using double-sided tape and secured to the back with a mischief-prevention belt.
3.4. Post-Purchase Evaluation
3.4.1. Wearing Status According to the Questionnaire Survey
A questionnaire survey was conducted during the post-purchase evaluation of the 36 cases, and responses were obtained from a total of 33 cases. Eleven of the 11 participants with bilateral hearing loss (100%) and 22 of the 25 participants with unilateral hearing loss (88.0%) responded to the survey. Three participants could not be interviewed due to the discontinuation of follow-up. These participants had unilateral microtia and unilateral external auditory canal atresia.
Among the 11 participants with bilateral hearing loss, six participants reported wearing CC-HAs from “morning, upon waking up” to “night, before going to bed,” three participants reported wearing CC-HAs until “returning home,” and the remaining two participants reported wearing CC-HAs “only at nursery school/school.” Among the 22 participants with unilateral hearing loss, one participant reported wearing CC-HA from “morning, upon waking up” to “night, before going to bed,” one participant reported wearing CC-HA until “returning home,” and the majority of 15 participants (68.2%) reported wearing CC-HAs from “when going to nursery school/school” to “returning home.” One participant reported wearing CC-HA “only at nursery school/school,” and the remaining four participants reported wearing CC-HAs only when spoken to.
Regarding the effectiveness of wearing, among “noticed voices from behind more easily,” “easier understanding of conversations in noisy places, such as parks or restaurants,” “better understanding of the direction of sounds and voices,” and “easier understanding of conversations with multiple people,” except for “conversations with multiple people,” participants with bilateral hearing loss and unilateral hearing loss responded with “strongly agree” or “agree” in over 50% of the cases. This tendency was particularly pronounced in cases of unilateral hearing loss.
The requests for hearing aid usage could be classified into six categories (n=46): “concerns regarding adhesives (tape),” “issues with wearing and handling,” “concerns regarding shape and structure,” “waterproofing concerns,” “concerns regarding background noise,” and “concerns regarding social acceptance.” Among these categories, “concerns regarding adhesives (tape)” was the most common at 34.8%, with noticeable responses indicating that the tape tended to become less adhesive due to sweat. The second most common category was “issues with wearing and handling,” accounting for 23.9% of the responses, with difficulties mentioned in children independently using and putting on the device.
4. Discussion
This study aimed to evaluate the effectiveness and fitting/wearing status of CC-HA in children with hearing loss and examine the indication for hearing aids in children as they grow older. The primary finding of this study was that it is possible to continuously and stably wear hearing aids from infancy by devising a fitting method while monitoring the developmental status and wearing conditions. The discovery of the cartilage conduction pathway has uncovered new possibilities in auditory function. There are three possible transmission pathways for acoustic energy traveling from a cartilage conduction transducer to the cochlea [14]. The first is the AC pathway from the transducer to the eardrum, which includes the resonance effect in the canal (air pathway) as the transducer also generates a low-level air-borne signal. The second pathway involves both air and cartilage conduction. Vibrations of the aural cartilage and the tissue surrounding the external auditory canal generate sound in the ear canal that reaches the eardrum via AC (cartilage-air pathway). The third pathway involves bone and cartilage conduction via the skull from the transducer to the cochlea (cartilage-bone pathway). The air and cartilage-bone pathways are common routes that operate based on the same principles that pertain to regular air and bone conduction hearing, respectively. In contrast, the cartilage-air pathway is not a common sound conduction route. CC-HAs are being utilized as a new hearing aid, primarily in Japan. The greatest advantage of using CC-HAs in clinical settings is that its transducer is significantly smaller and lighter compared with that of conventional BC-HA. Moreover, it does not require compression fixation, which enables CC-HAs to be attached to the skin to deliver sound vibrations into the ear.
Nishiyama et al. investigated adult candidates eligible for using CC-HA [15] and concluded that patients with external auditory canal stenosis or anotia are the most suitable candidates. They also reported positive results in children with similar ear conditions [16].
We initiated trial hearing of CC-HA in 49 cases ranging from infants to elementary school students, and 36 cases proceeded to decide and utilize the device. During the promotion of the suitability of CC-HA for infants and young children, particularly those with developmental disorders, we encountered difficulties in achieving stable attachment using the recommended methods of adhesion or ear tips alone. Initially, we proposed attaching the transducer using double-sided tape and securing it further with tape [16]; however, this did not result in a stable attachment. Therefore, taking inspiration from the headbands used for BC-HA, we collaborated with the participants’ mothers and created prototypes of CC-HA headbands, which quickly made it possible to wear the device. Based on this experience, we found that attaching the hearing aid to the temples of glasses or using a favorite headband proved to be successful in other cases.
Treacher Collins syndrome (as seen in Case 1), also known as mandibulofacial dysostosis, is an autosomal dominant inherited genetic disorder with an incidence of 1 in 50,000 [22,23]. Common symptoms of this syndrome include hypoplasia of the facial bones, especially the mandible and zygoma, drooping cleft palate, lid coloboma, and cleft palate [24]. Conductive hearing loss is observed in 50% of patients and is attributed to malformations of the outer and middle ear [25,26]. Previous studies have reported auditory rehabilitation in such patients using BC-HAs or BAHAs. The importance of early auditory rehabilitation to ensure appropriate development of language and learning is well-known [27,28,29,30]; however, the use of BC-HAs is associated with local pain, discomfort, and concerns related to appearance [7,12]. BAHAs require surgery [31,32], and the protrusion of the implant is a disadvantage in terms of appearance [12]. In contrast, the use of CC-HAs is not associated with such problems and is considered an effective alternative to AC-HAs. In this study, a headband was used as an adaptation for wearing the device. Initially, concerns were raised regarding headband shifting; however, no issues regarding shifting were encountered over the study period. It is believed that factors, such as the child being calm, having minimal body movements during infancy or other life stages, or being at a stage of having greater understanding, may also have influenced the results.
FOXP1 syndrome (seen in Case 2) is associated with intellectual disability, language impairment, autism spectrum disorder, myotonia and mild dysplasia, and congenital abnormalities of the brain, heart, and urinary system. Cases of hearing loss have been reported with this syndrome. Lozano et al. reported that all individuals with FOXP1 syndrome must be evaluated for hearing loss and promptly provided with hearing replacement [33]. CC-HA was effective in the treatment of hearing loss in a patient with trisomy of chromosome 18. Trisomy of chromosome 18 is the second most frequent autosomal disorder after Down syndrome and 22q11.2 deletion syndrome, with a reported frequency of 1 in 3,500–8,500 live births. The prognosis is often poor [34,35]; however, marked improvement in vital prognosis has been reported. Sato et al. have reported the importance of fitting hearing aids in these patients with documented hearing loss. With advances in newborn hearing screening tests and early detection of hearing loss, it would be desirable for hearing aids to be worn safely, without burden, and consistently from age 0, even in cases where AC-HAs are difficult to apply, such as in patients with atresia of the external auditory canal.
In this study, there were five participants with bilateral hearing loss who had a history of using hearing aids prior to the CC-HA trial. Four participants had used bilateral BC-HA, and one participant had used AC-HA on the side without external auditory canal stenosis. The preference for switching to CC-HA primarily came from caregivers due to limited wearing time and concerns regarding aesthetic aspects and discomfort caused by the pressure of the BC transducer in BC-HA. Among the three participants with bilateral microtia and external auditory canal atresia, all participants except one, who was awaiting a transition to CC-HA after auricular reconstruction surgery, immediately transitioned to CC-HA. In one participant with unilateral microtia, external auditory canal stenosis, and contralateral ear ossicular malformation, external auditory canal enlargement was observed during the process of making an ear impression for CC-HA, resulting in the selection of AC-HA. In cases of bilateral hearing loss with microtia, external auditory canal closure, or stenosis since birth, conventional BC-HAs (with cloth headbands) are commonly chosen by both medical professionals and caregivers, as they appear to be easier to wear and readily available. However, CC-HAs offer the potential for stable use from infancy by adapting the wearing method as the child grows, and it is expected to have wider applications. This adaptation requires repeated prototyping. Moreover, collaboration with the parents, especially the mother, is essential, as it is the mother who observes the child's behavior and experiences the benefits of wearing the hearing aid. The support and involvement of healthcare professionals and caregivers are crucial in increasing the motivation for wearing the hearing aid and encouraging active utilization.
Evaluation of the post-purchase experience revealed that in participants with bilateral hearing loss, hearing aids were used almost throughout the day. Moreover, both the individuals and their surroundings experienced positive effects from the usage. Similar results were observed in participants with unilateral hearing loss; however, there were some instances of shorter wearing times. It was demonstrated that educational and medical support are crucial for the effective use of hearing aids, particularly in cases of unilateral hearing loss. Additionally, a higher proportion of individuals with unilateral hearing loss reported perceiving the benefits of wearing the hearing aid compared with those who had bilateral hearing loss, which may be attributed to the presence of non-usage periods, making the effects of the hearing aid more noticeable. This is also believed to reflect the binaural hearing effects indicated by Kaga et al. [36]. As for the challenges related to the hearing aids, participants with bilateral and unilateral hearing loss identified improvement in the adhesive wearing method, particularly addressing issues with sweat and difficulties in reapplication, as future tasks.
The participants with unilateral hearing loss had no history of using hearing aids, and CC-HA was the first hearing aid selected for these participants as there were limited options available in terms of other models as they required surgical intervention. In recent years, implants, such as the BAHA Attract system (Cochlear Limited), Bonebridge (MED-EL, Innsbruck, Austria), and Sophono (Medtronic, Dublin, Ireland), have been developed. In the case of children, the decision for surgery is primarily made by the caregivers (parents). However, the use of CC-HA as a policy until the age when the child's own will can be taken into consideration is also an important option.
5. Conclusion
Even in cases where it is challenging to use AC-HAs, such as patients with external auditory canal closure, the ability to consistently use hearing aids from infancy is crucial for the development of language and communication skills in children with hearing loss. CC-HAs enable continuous and stable use from infancy to early childhood by adjusting the fitting method according to the child's growth. The use of CC-HAs involves utilizing options such as headbands or attaching the hearing aids to glasses frames. Collaboration with mothers is necessary for implementing these adaptations. Effective use of hearing aids also requires educational and medical support.
Author Contributions
Conceptualization, S.Y. and T.S.; methodology, T.M.; validation, S.Y., T.S. and Y.M.; formal analysis, K.S.; investigation, K.S.; resources, T.S.; writing—original draft preparation, T.S.; writing—review and editing, T.M.; supervision, Y.S.; project administration, S.Y.; funding acquisition, T.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of KANTO ROSAI HOSPITAL (approval no.: 2023-1; 2023.4.4 ).
Informed Consent Statement
Verbal informed consent was obtained from all participants and their guardians. Written consent was not required according to ethical guidelines for medical and health sciences research involving human subjects.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hosoi, H. Approach in the Use of Cartilage Conduction Speaker, 2004. Japanese patent number 454 1111, 17. [Google Scholar]
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Matsui, T.; Yamanaka, T.; Levitt, H. Is cartilage conduction classified into air or bone conduction? Laryngoscope 2014, 124, 1214–1219. [Google Scholar] [CrossRef]
- Nishimura, T.; H. Hosoi, Saito, O.; Miyamae, R.; Shimokura, R.; Yamanaka, T.; Kitahara, T.; Levitt, H. Cartilage conduction is characterized by vibrations of the cartilaginous portion of the ear canal. PloS One 2015, 10, e0120135. [CrossRef]
- Akasaka, S.; Nishimura, T.; Hosoi, H.; Saito, O.; Shimokura, R.; Morimoto, C.; Kitahara, T. Benefits of Cartilage Conduction Hearing Aids for Speech Perception in Unilateral Aural Atresia. Audiol Res. 2021, 11, 284–290. [Google Scholar] [CrossRef]
- Nishimura, T.; Hosoi, H.; Saito, O.; Shimokura, R.; Yamanaka, T.; Kitahara, T. Cartilage Conduction Hearing Aids for Severe Conduction Hearing Loss. Otol Neurotol 2018, 39, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Stenfelt, S.; Goode, R.L. Bone-Conducted Sound: Physiological and Clinical Aspects. Otol Neurotol 2005, 26, 1245–1261. [Google Scholar] [CrossRef] [PubMed]
- Dillon, H. Dillon, H. CROS, bone-conduction, and implanted hearing aids. In: Dillon H, ed. Hearing Aids. Stuttgart: Thieme, 2001;434–50. T: Stuttgart.
- Lo, J.F.; Tsang, W.S.; Yu, J.Y.; Ho, O.Y.; Ku, P.K.; Tong, M.C. Contemporary hearing rehabilitation options with aural atresia. Biomed Res Int 2014, 2014, 761579. [Google Scholar] [CrossRef] [PubMed]
- Hosoi, H. Cartilage Conduction Hearing Aids: the Third Pathway for Sound Transmission and its Application, ENT & audiology news. 2020. https://www.entandaudiologynews.com/features/audiology-features/p ost/cartilage-conduction-hearing-aids-the-third-path way-for-sound-transmission-and-its application. (Accessed 22 September 2020).
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Matsui, T.; Iwakura, T. Benefit of a new hearing device utilizing cartilage conduction. Auris Nasus Larynx 2013, 40, 440–446. [Google Scholar] [CrossRef]
- Nishimura, T.; Hosoi, H.; Saito, O.; Miyamae, R.; Shimokura, R.; Matsui, T.; Yamanaka, T.; Kitahara, T.; Levitt, H. Cartilage conduction efficiently generates airborne sound in the ear canal. Auris Nasus Larynx 2015, 42, 15–19. [Google Scholar] [CrossRef]
- Nishimura, T.; Hosoi, H.; Saito, O.; Shimokura, R.; Yamanaka, T.; Kitahara, T. Cartilage conduction hearing aids for severe conduction hearing loss. Otol Neurotol 2018, 39, 65–72. [Google Scholar] [CrossRef]
- Morimoto, C.; Nishimura, T.; Hosoi, H.; Saito, O.; Fukuda, F.; Shimokura, R.; Yamanaka, T. Sound transmission by cartilage conduction in ear with fibrotic aural atresia. J Rehabil Res Dev 2014, 51, 325–332. [Google Scholar] [CrossRef]
- Shimokura, R.; Hosoi, H.; Nishimura, T.; Yamanaka, T.; Levitt, H. Cartilage conduction hearing. J Acoust Soc Am 2014, 135, 1959–1966. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, T.; Oishi, N.; Ogawa, K. Who are good adult candidates for cartilage conduction hearing aids? Eur Arch Oto-Rhino-Laryngol 2020, 278, 1789–1798. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, T.; Oishi, N.; Ogawa, K. Efficacy of cartilage conduction hearing aids in children. Int J Pediatr Otorhinolaryngol 2021, 142, 110628. [Google Scholar] [CrossRef] [PubMed]
- Kitagawa, K.; Mitsuzawa, H.; Shintani, T.; Go, M.; Himi, T. Audiological chronological findings in children with congenital anomalies of the central nervous system. Int J Pediatr Otorhinolaryngol 2009, 73, 1105–1110. [Google Scholar] [CrossRef]
- Scollie, S.; Seewald, R.; Cornelisse, L.; Moodie, S.; Bagatto, M.; Laurnagaray, D.; Beaulac, S.; Pumford, J. The Desired Sensation Level multistage input/output algorithm. Trends Amplif 2005, 9, 159–197. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association declaration of Helsinki. Recommendations guiding physicians in biomedical research involving human subjects. JAMA 1997, 277, 925–926. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and welfare, ethical Guidelines for medical and Health research involving human subjects provisional translation. https://www.mhlw.go. jp/file/06-Seisakujouhou-10600000-Daijinkanboukouseikagakuka/0000080278. pdf. (Accessed 20 September 2020).
- Yamamoto-Shimojima, K.; Imaizumi, T.; Akagawa, H.; Kanno, H.; Yamamoto, T. Primrose syndrome associated with unclassified immunodeficiency and a novel ZBZB20 mutation. Am J Med Genet A 2020, 182, 521–526. [Google Scholar] [CrossRef]
- Martini, A.; Calzolari, F.; Sensi, A. Genetic syndromes involving hearing. Int J Pediatr Otorhinolaryngol 2009, 73 Suppl. 1, S2–12. [Google Scholar] [CrossRef]
- Plomp, R.G.; Bredero-Boelhouwer, H.H.; Joosten, K.F.; Wolvius, E.B.; Hoeve, H.L.; Poublon, R.M.; Mathiijssen, I.M. Obstructive sleep apnoea in Treacher Collins syndrome: prevalence, severity and cause. Int J Oral Maxillofac Surg 2012, 41, 696–701. [Google Scholar] [CrossRef]
- Katsanis, S.H.; Jabs, E.W. Treacher Collins syndrome. In: Pagon RA, Adam MP, Ardinger HH, Wallace SE, Amemiya A, Bean LJH, et al., editors. GeneReviews. 1993. Seattle, WA.
- Hylton, J.B.; Leon-Salazar, V.; Anderson, G.C.; De Felippe, N.L. Multidisciplinary treatment approach in Treacher Collins syndrome. J Dent Child (Chic) 2012, 79, 15–21. [Google Scholar]
- Lesinskas, E.; Stankeviciute, V.; Petrulionis, M. Application of the Vibrant Soundbridge middle-ear implant for aural atresia in patients with Treacher Collins syndrome. J Laryngol Otol 2012, 126, 1216–1223. [Google Scholar] [CrossRef]
- Marsella, P.; Scorpecci, A.; Pacifico, C.; Tieri, L. Bone-anchored hearing aid (Baha) in patients with Treacher Collins syndrome: tips and pitfalls. Int J Pediatr Otorhinolaryngol 2011, 75, 1308–1312. [Google Scholar] [CrossRef]
- Marres, H.A. Hearing loss in the Treacher-Collins syndrome. Adv Otorhinolaryngol 2002, 61, 209–215. [Google Scholar]
- Thompson, J.T.; Anderson, P.J.; David, D.J. Treacher Collins syndrome: protocol management from birth to maturity. J Cranofac Surg 2009, 20, 2028–2035. [Google Scholar] [CrossRef]
- Verhagen, C.V.; Hol, M.K.; Coppens-Schellekens, W.; Snik, A.F.; Cremers, C.W. The Baha Softband. A new treatment for young children with bilateral congenital aural atresia. Int J Pediatr Otorhinolaryngol 2008, 72, 1455–1459. [Google Scholar] [CrossRef]
- House, J.W.; Kutz, J.W., Jr. Bone-anchored hearing aids: Incidence and management of postoperative complications. Otol Neurotol 2007, 28, 213–217. [Google Scholar] [CrossRef]
- Hobson, J.C.; Roper, A.J.; Andrew, R.; Rothera, M.P.; Hill, P.; Green, K.M. Complications of bone-anchored hearing aid implantation. J Laryngol Otol 2010, 124, 132–136. [Google Scholar] [CrossRef]
- Lozano, R.; Gbekie, C.; Siper, P.M.; Srivastava, S.; Saland, J.M.; Sethuram, S.; Tang, L.; Drapeau, E.; Frank, Y.; Buxbaum, J.D.; Kolevzon, A. FOXP1 syndrome: a review of the literature and practice parameters for medical assessment and monitoring. J Neurodev Disord 2021, 13, 18. [Google Scholar] [CrossRef]
- Jones, K.L. Trisomy 18 Syndrome. Smithʼs Recognizable Patterns of Human Malformation. 2006, 13–17.
- Carey, J.C. Trisomy 18 and trisomy 13 syndromes. Cassidy Sb, Allanson JE, eds. Management of Genetic Syndromes 2nd ed. Hoboken: Wiley-Liss. 2005, 555–568.
- Kaga, K.; Setou, M.; Nakamura, M. Bone-conducted sound lateralization of inte-raural time difference and interaural intensity difference in children and a young adult with bilateral microtia and atresia of the ears. Acta Otolaryngol 2001, 121, 274–277. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



