
Submitted:
04 July 2023
Posted:
06 July 2023
You are already at the latest version
Abstract
Globally, gastric cancer is a major cause of cancer mortality, with a 5-year survival rate of 32% for locally advanced and metastatic gastric cancer. This systematic literature review summarized the clinical, safety, and humanistic outcomes associated with systemic regimens given as first line therapy for locally advanced and metastatic gastric cancer. The search included articles published in English in PubMed, Embase, Web of Science, Cochrane Central Register of Controlled Trials, and the American Society of Clinical Oncology meeting library, from inception to April 2022. Phase II and III randomized controlled trials conducted among western populations diagnosed with stage III and IV locally advanced and metastatic gastric cancer were included. Two investigators independently reviewed the studies, conducted data extraction, and assessed risk of bias in accordance with PRISMA guidelines. Twenty-four randomized controlled trials totaling 8,705 patients were included. Median overall survival ranged from 5.0-13.1 months, median progression-free survival ranged from 2.0-7.7 months, and objective response ranged from 13.0-64.1%. Two studies reported higher quality of life outcomes. Grade 3 and 4 adverse events were reported in most studies. Improvement in clinical outcomes can be seen in recently published randomized controlled trials for locally advanced and metastatic gastric cancer.
Keywords:
Advanced and metastatic gastric cancer
; first-line systemic treatment
; systematic review
1. Introduction
Gastric cancer is the fifth most diagnosed cancer and the fourth most common cause of cancer related mortality globally [1]. There are an estimated 26,560 cases of gastric cancer in the United States (US) alone and 11,180 deaths in 2021. In the US, 1.5% of new cancers diagnosed per year are attributed to gastric cancer [2]. Studies have shown that 65% of gastric cancer cases diagnosed in the US are at an advanced stage (tumor node metastasis stages T3 or T4) [3]. Locally advanced and metastatic gastric cancer has a poor prognosis with a survival rate of only 5-10% [4].
In cases of locally advanced and metastatic gastric cancer, systemic therapy is often the preferred treatment since it offers survival benefits [5]. Patients with advanced disease are usually treated with a combination chemotherapy that has become the accepted standard for first-line treatment [6]. According to recommendations from the National Comprehensive Cancer Network [5], a fluoropyrimidine (Fluorouracil), a platinum (oxaliplatin or cisplatin), and a taxane (docetaxel or paclitaxel) can be added to therapy. The National Comprehensive Cancer Network also recommends patients with metastatic gastric cancer consider undergoing testing for human epidermal growth factor receptor 2 (HER2) amplification and presence of programmed death-ligand 1 (PD-L1) [6]. In HER2-positive patients, trastuzumab is recommended as first-line therapy [7]. Immune checkpoint inhibitors are a recent class of drugs that act by inhibiting T-cell activation and effector functions leading to an anti-tumor response [8]. Specifically, immune checkpoint inhibitors in locally advanced and metastatic gastric cancer patients act by mediating the blockage of the programmed cell death protein 1 (PD-1)/PD-L1 axis. They are preferred in standard chemotherapy-refractory cases or those who have been previously treated with two or more chemotherapeutic regimens [9].
Immune activation by immune checkpoint inhibitors seems to have a more durable clinical benefit than traditional chemotherapy in locally advanced and metastatic gastric cancer and a lower incidence of adverse events [10]. The ATTRACTION-2 phase III clinical trials looked at Nivolumab or placebo in metastatic gastric cancer patients and showed significant overall survival that persisted over time [11]. Immune checkpoint inhibitor combinations can also lead to higher toxicities but no increase in activity as seen in MOONLIGHT trial with Nivolumab among locally advanced and metastatic gastric cancer patients [12]. Long-term side effects have also been challenging with immune checkpoint inhibitors. A real-world study looking at melanoma patients treated with immune checkpoint inhibitors found that 40% of patients had immune-related adverse events at follow-up [13].
The clinical efficacies of several targeted agents and immunotherapy treatment options have been tested in phase II and phase III randomized clinical trials. However, there is still ambiguity regarding the drug of choice for locally advanced and metastatic gastric cancer patients. Previously published systematic reviews evaluated first line systematic therapies in locally advanced and metastatic gastric cancer but each had some important limitations [14,15,16,17,18], are outdated do not include all systemic therapies,, or included both gastric and esophageal cancer patients.
There is a lack of established screening programs in the western world, making early detection of gastric cancer difficult and survival rate in locally advanced and metastatic gastric cancer A/MGC is poor. Literature shows that treatment efficacy and survival outcomes vary between Asian and Western Patients. There remains is a lack of comprehensive, current evidence regarding therapies approved by the US Food and Drug Administration for locally advanced and metastatic gastric cancer. Hence, the purpose of this study was to perform a systematic review of randomized phase II and phase III treatment trials to compare the clinical efficacy, safety (adverse events), and humanistic outcomes of all first-line systemic therapeutic combinations among the western adult population with locally advanced and metastatic gastric cancer.
2. Results
2.1. Characteristics of Included Studies
A total of 8,689 unique references were identified from the database search and after reviewing titles and abstracts, 8,510 were excluded. In the remaining 179 full text articles, 24 studies met the inclusion criteria and were included in our systematic review. The selection process and reason for exclusion were reported in the PRISMA flow diagram (Figure 1). These 24 studies included eight phase II randomized controlled trials and 16 phase III randomized controlled trials.
Of the 24 included trials, 21 contained two treatment arms while the remaining three contained three treatment arms. Double chemotherapy combinations were used as first line therapy in five randomized controlled trials while the remaining 19 trials used triple or quadruple drug combination therapies. The total number of included patients per study ranged from 69 to 1,581. The median participant ages ranged from 52.7 to 70 years, and 48% to 84% of participants were male. The characteristics of the included randomized controlled trials and demographic characteristics of study participants are shown in Table 1.
The characteristics of the cancer and outcomes reported are shown in Table 2. More than 50% of trial patients had a gastric tumor. The proportion of trial participants with metastatic disease was between 60% and 97.3%.
2.2. Overall survival
Twenty one of the 24 included trials reported overall survival with 39 different treatment regimens. Only four of the 20 trials reporting overall survival identified a statistically significant difference between the intervention and comparison groups. One of the four studies with statistical significance was Cascinu, 2011 [25] that evaluated a three-drug combination of pegylated liposomal doxorubicin, 5-fluouracil and cisplatin with mitomycin-C, 5-fluouracil, and cisplatin as the comparative arm and found that the doxorubicin, 5-fluouracil, and cisplatin group had a higher overall survival (12.1 months vs 8.3 months). The second of the four studies was Catenacci, 2017 [26]. This was a phase III randomized controlled trial which compared a four-drug combination of rilotumumab plus standard of care (standard of care consisted of epirubicin, cisplatin, and capecitabine) compared to standard of care alone. The rilotumumab-standard of care group showed poorer outcomes in overall survival (8.8 months) compared to the standard of care group (10.7 months). The third of the four studies was Janjigian, 2021 [34]. This study was conducted among locally advanced and metastatic gastric cancer patients where nivolumab therapy with chemotherapy was compared to chemotherapy alone. The nivolumab group showed significantly higher overall survival (13.1 months vs 11.1 months) than the chemotherapy alone group.
The fourth study was Van Cutsem, 2006 [41]. This study compared docetaxel, cisplatin and fluorouracil with cisplatin-fluorouracil and found a longer overall survival (9.2 months) in the docetaxel, cisplatin and fluorouracil group compared to 8.6 months in the cisplatin-fluorouracil group among advanced gastric cancer patients. Among the remaining included studies that reported overall survival, 16 randomized controlled trials used various treatment regimens, 12 of which did not show statistical differences in overall survival between the treatment and comparator groups, while the remaining four randomized controlled trials did not report statistical results (Table 3).
2.3. Progression-Free Survival
Thirteen of the 24 included randomized controlled trials using 39 regimens reported progression free survival outcomes. Only six of the 13 randomized controlled trials showed statistically significant improvement in progression-free survival. The first study reporting progression-free survival by Catenacci, 2017 [26] was a phase III trial among advanced gastric cancer patients with rilotumumab plus standard of care (standard of care consisted of epirubicin, cisplatin, and capecitabine) compared to standard of care alone. This study showed that rilotumumab plus standard of care had a shorter progression-free survival (5.6 months) compared to standard of care alone (6.07 months). The second study reporting progression-free survival by Fuchs, 2019 [30] was a phase III trial comparing ramucirumab and standard first-line therapy (fluorouracil and capecitabine) with placebo plus standard first-line therapy. Ramucirumab plus first line therapy showed significantly longer progression-free survival (5.7 months) compared to placebo and first line therapy (5.4 months). The third study reporting progression-free survival by Janjigian, 2021 [34] was a phase III randomized controlled trial which compared the role of the newer agent nivolumab and standard chemotherapy with standard chemotherapy alone. Nivolumab and standard chemotherapy showed longer progression-free survival (7.7 months) compared to the chemotherapy alone group (6.1 months). The fourth study reporting progression-free survival by Kang, 2009 [35] was a randomized phase III noninferiority trial which compared capecitabine/cisplatin to 5-fluorouracil/cisplatin. The capecitabine/cisplatin group showed significant noninferiority for progression-free survival for patients with advanced gastric cancer (5.6 months) versus 5.0 months for the 5-fluorouracil/cisplatin group. The fifth study reporting progression-free survival by Shitara, 2020 [39] was a phase III trial comparing three groups (group 1: pembrolizumab alone, group 2: standard chemotherapy, group 3: pembrolizumab and standard chemotherapy). Progression-free survival was higher in group 2 (standard chemotherapy) when compared to group 1 (pembrolizumab alone) with 6.4 months and 2.0 months progression-free survival respectively. The sixth study reporting progression-free survival by Shitara, 2022 [40] compared nivolumab plus ipilimumab to chemotherapy alone (i.e., the CheckMate 649 trial). Chemotherapy alone showed a longer progression-free survival (7.1 months) than nivolumab plus ipilimumab (2.8 months) (Table 3).
2.4. Objective response rate
Of the 14 randomized controlled trials that reported objective response rate, five showed statistically significant overall response rates. The first trial reporting a statistically significant response rate, Al-Batran, 2013 [22], compared fluorouracil-leucovorin-oxaliplatin-docetaxel to fluorouracil-leucovorin-oxaliplatin in a sample of older adult advanced gastric cancer patients. The fluorouracil-leucovorin-oxaliplatin-docetaxel group showed a higher overall response rate of 48.6% compared to 28.2% in the fluorouracil-leucovorin-oxaliplatin group. The second trial reporting a statistically significant response rate, Cascinu, 2011 [25], compared 5-fluorouracil, cisplatin and pegylated liposomal doxorubicin to 5-fluorouracil, cisplatin and mitomycin-C. The 5-fluorouracil, cisplatin and pegylated liposomal doxorubicin group showed a higher overall response rate (64.1%) compared to the 5-fluorouracil, cisplatin, and mitomycin-C group (38.5%). The third trial reporting a statistically significant response rate, Cocconi, 1994,[27] compared cisplatin, epirubicin, leucovorin, and fluorouracil with the standard combination of fluorouracil, doxorubicin, and mitomycin. This trial found a higher overall response rate with cisplatin-epirubicin-leucovorin-flurouracil (43%) than fluorouracil-doxorubicin-mitomycin (15%). The fourth trial reporting a statistically significant response rate, Kang, 2009 [37], was a multinational phase III trial among advanced gastric cancer patients that compared capecitabine and cisplatin to 5-fluorouracil and cisplatin. This trial found a higher response rate (46%) with capecitabine and cisplatin than 5-fluorouracil and cisplatin (32%). The fifth trial reporting a statistically significant response rate, Webb, 1997 [42], compared epirubicin-cisplatin-5-fluorouracil with 5-fluorouracil-doxorubicin-methotrexate. A higher response rate of 45% was seen with epirubicin-cisplatin-5-fluorouracil than with 5-fluorouracil-doxorubicin-methotrexate (21%) (Table 3).
2.5. Other Outcomes Reported
Some of the other statistically significant clinical efficacy outcomes reported in included clinical trials were: time to 5% deterioration of global health status from baseline (a quality-of-life assessment), mean difference in global health scores (also a quality-of-life measure), and time to progression. Anjani, 2007 [20] prospectively assessed quality of life as one of the secondary end points of the phase III trial that compared docetaxel-cisplatin-fluorouracil with cisplatin-fluorouracil. Time to 5% deterioration of global health status from baseline was longer in the docetaxel-cisplatin-fluorouracil group (6.5 months) compared to 4.2 months in the cisplatin-fluorouracil group showing the better preservation of quality of life with the addition of docetaxel. All three treatments arms in the Bouche, 2004 [24] trial had improved global quality of life health scores when compared to baseline. Time to progression was statistically significantly improved in two studies: Cascinu, 2011 [25] and Van Cutsem, 2006 [41] (Table 3).
2.6. Adverse events and safety
Twenty-two of the 24 randomized controlled trials included reported some grade of adverse events in study patients. Only grade three and higher treatment-related adverse events were summarized in Table 4. The most common grade 3–4 hematological toxicities were neutropenia, anemia, thrombocytopenia, and leucopenia. While the most common nonhematological toxicities were nausea, vomiting, diarrhea, and fatigue (Table 4).
2.7. Risk of bias assessment
Of the 24 included studies, 11 studies had a low overall risk of bias and 13 studies had some concerns overall. None of the eligible studies were at high risk of bias as rated by the five domains of the risk-of-bias tool [43]. Specifically, 20 out of the 24 randomized controlled trials were evaluated as low risk of bias concerning randomization as all the trials included specific information about randomization techniques. Since some of the trials were open-label, five studies were identified as having some risk of bias concerns in the deviations from intended interventions domain. Due to the nature of locally advanced and metastatic gastric cancer there was some missing outcomes data due to attrition, death, or loss of follow-up. Nine studies showed some risk of bias concerns in the missing outcome data domain. All clinical trials used appropriate methods to measure clinical outcomes, quality of life and adverse events reporting, thus all 24 studies had low risk of bias in the measurement of outcomes domain. Lastly, because most of the studies were analyzed based on the intention-to-treat population and had well reported clinical and safety endpoints, the selection of reported results domain was appraised as having a low risk of bias in 23 of the 24 studies (Table 5).
3. Discussion
First-line treatment recommendations for patients with locally advanced and metastatic gastric cancer have been constantly updated in the United States. The National Comprehensive Cancer Network Gastric Cancer Guidelines (Version 2.2022) recommends fluoropyrimidine (fluorouracil or capecitabine) and platinum-based antineoplastic (oxaliplatin or cisplatin) and trastuzumab (for HER2 overexpression positive adenocarcinoma) or nivolumab (for HER2 overexpression negative adenocarcinoma) as preferred first-line systemic therapy for unresectable, recurrent, or metastatic gastric cancer [5]. This systematic review identified numerous first-line therapeutic options investigated in 24 randomized controlled trials among patients with locally advanced and metastatic gastric cancer before April 2022. Across treatment arms in the included randomized controlled trials, median overall survival was between 5.0 months and 13.1 months, median progression free survival was between 2.0 months and 7.7 months, and the objective response rate was between 13.0% and 64.1%. The wide range of values across these outcomes highlighted some inconsistencies across the included studies. Multiple factors likely contributed to this cross-study variability such as differences in trial phases, treatment arms, sample sizes, disease stages included, and the Eastern Cooperative Oncology Group (ECOG) status of the included patients. Specific examples of the outcomes studied are reported and discussed in the context of what is already known in the following sections.
3.1. Overall survival
The combination of nivolumab plus chemotherapy seems to produce the longest overall survival (hazard ratio=0·71, 95% confidence interval [CI]=0·59–0·86), while the shortest overall survival length was seen with the 5-fluorouracil-epirubicin-cisplatin combination. Reasons to explain this are not well documented, but it is never-the-less an encouraging finding. Immune checkpoint inhibitors have durable and significantly higher clinical efficacy than chemotherapy alone in locally advanced and metastatic gastric cancer patients. In accordance with the above outcomes, the combination of nivolumab and fluoropyrimidine with platinum-based antineoplastics is the recommended treatment for locally advanced and metastatic gastric cancer [5] due to its better overall survival outcomes. Compared with the prior systematic review conducted by Cheng and colleagues in 2018 [44] which included studies that contained both gastric and esophageal cancer cases and included world-wide trial populations, our systematic review focused on studies that included only western populations with gastric cancer [44]. The Cheng et al. study found that fluoropyrimidine plus platinum-based triple therapies (hazard ratio=0.91, 95% CI=0.83–0.99) showed the biggest improvement in overall survival in patients with advanced gastric cancer. An older systematic review by Wagner, 2006 [45] looked at first-line chemotherapy in patients with advanced gastric cancer and included overall survival as the primary outcome. This study also showed a three-drug regimen of fluorouracil, cisplatin, and an anthracycline (doxorubicin or epirubicin) achieved better survival results (hazard ratio=0.77, 95% CI=0.62-0.91) than a two drug (fluorouracil-cisplatin) combination. With the recent advancements in immunotherapies, nivolumab (a PD-L1 inhibitor) has demonstrated a significant survival benefit in the locally advanced and metastatic gastric cancer population and our review supports these results [46].
3.2. Progression-free survival
Similar to the overall survival results, a combination of nivolumab and chemotherapy showed the longest progression-free survival duration of 7.7 months (hazard ratio=0·68, 95% CI=0·56–0·81) among our included randomized controlled trials. In support of our findings, the CheckMate-649 trial results indicated that nivolumab was the first PD-L1 inhibitor to demonstrate superior progression-free survival duration of 7.7 months (hazard ratio=0·68, 95% CI=0·56–0·81) among our included benefits among advanced gastric cancer patients [46]. CheckMate-649 is the largest randomized, global phase III study of an immune checkpoint inhibitor-based therapy as first-line therapy for patients with gastric and esophageal cancers conducted to date. While our systemic review found that nivolumab plus chemotherapy showed the longest progression-free survival, in contrast to our findings, an older systematic review and network meta-analysis by Cheng and colleagues in 2018[44] found that fluoropyrimidine-platinum-based triple-medication therapy (hazard ratio=0.75, 95% CI=0.54–1.04) was the best regimen for progression-free survival. However, at the time Cheng et al. was conducted, nivolumab was still under development and therefore was not included. Another review article by Takashima, 2017 investigated survival outcomes in advanced gastric cancer in phase III trials. Median progression-free survival was calculated from 11 trials from all over the world and found to be in the range of 3.1 to 7.4 months [47]. The phase III trials included in this review did not include newer studies utilizing immunotherapies like nivolumab because the search was conducted from 2007-2015.
3.3. Objective response rate
In this review objective response rate was highest in the Cascinu, 201125 study with 64.1% in the doxorubicin-5-fluorouracil-cisplatin group. An American Society of Clinical Oncology post on the long-term support data of the CheckMate-649 trial of nivolumab plus chemotherapy group reported that with longer follow-up, the nivolumab-chemotherapy group had a higher objective response rate (58%) than chemotherapy alone [46]. As per the older systematic review by Cheng and colleagues, 5-fluorouracil plus platinum doublet (oxaliplatin or cisplatin) have demonstrated statistically significant results among the 89 global studies investigated. Another older review by Koizumi, 2007 [48] looking at global status of chemotherapies in advanced gastric cancer concluded that a promising objective response rate did not always translate into a survival benefit.
3.4. Other outcomes
Our review showed that mean global health status significantly improved from baseline in two different studies. Interim results of nivolumab-chemotherapy versus chemotherapy from the CheckMate-649 trial showed that change from baseline in health-related quality of life as assessed by EuroQol-5-dimension (EQ-5D) scores favored nivolumab-chemotherapy [49]. A systematic review by van Amelsfoort in 2021 evaluated health-related quality of life among patients with non-metastatic locally advanced gastric cancer. This review found that health-related quality of life deteriorated during the first three months after surgery and chemoradiotherapy [50].
3.5. Limitations
This review had some limitations. Oncology is a very complex and rapidly evolving area, thus there was significant heterogeneity in treatment arms and outcomes seen. Next, only systemic therapies were summarized in this review, thus surgical interventions and radiation therapy which are cardinal in the treatment of gastric cancer were not captured. Also, our study included only randomized controlled trials conducted in western populations and thus results cannot be extrapolated to make global conclusions. Clinical efficacy and safety outcomes seen in observational studies and real-world studies were also beyond the scope of this systematic review and thus our results do not necessarily reflect subsequent changes in clinical practice. In addition, publication bias can be a concern for any systematic review as studies which did not identify the treatment to be effective may not have been published. To minimize publication bias, our literature search also included any unpublished or ongoing trials. With a variety of novel immune check point inhibitors and targeted therapies that are being explored in the oncology space, some of the ongoing trials do not have comprehensive information captured yet published.
3.6. Future research
With emerging clinical data for checkpoint inhibitors in locally advanced and metastatic gastric cancer, immunotherapies such as nivolumab have the potential to improve outcomes in patients who have unresectable, locally advanced and metastatic gastric cancer and may provide new treatment options for this patient population in the future. Identification of predictive biomarkers for gastric cancer are being increasingly developed [51]. Examples include tumor agnostic biomarker mismatch repair or microsatellite instability which is a robust biomarker of immune responses. Evaluation of PD-L1 expression in tumors is critical as higher levels of PD-L1 are associated with poor prognosis. Future research should aim to supplement the published data by conducting larger real world observational studies, consider the widespread testing for biomarkers for locally advanced and metastatic gastric cancer, and also seek to evaluate the economic and quality of life burden of locally advanced and metastatic gastric cancer.
4. Materials and Methods
4.1. Types of studies
Phase II and phase III randomized controlled trials were included in the systematic review if they compared a systemic first line single agent or combination therapy, as per the National Comprehensive Cancer Network guidelines (version 2.2022),[5] with another type of systemic first line therapy, placebo, best supportive care, or no treatment as comparison groups. We included the full text or the abstract of studies if data for outcomes were reported. We included trials with mixed disease stages if they reported outcomes separately for metastatic disease.
4.2. Types of participants
Adults aged 18 years and older with histologically confirmed adenocarcinoma of the stomach and locally advanced unresectable or metastatic disease were included. Trials and studies of patients with adjacent organs and lymph node metastasis (defined as American Joint Committee on Cancer tumor node metastasis stage III) and distant metastatic (defined as American Joint Committee on Cancer tumor node metastasis stage IV) gastric cancer were included. No restrictions in terms of sex, drug dosage, radiologic examination, or treatment duration were applied.
4.3. Types of interventions
All comparisons of systemic therapies for the treatment of locally advanced and metastatic gastric cancer as per National Comprehensive Cancer Network guidelines 2022 [5] were included, such as: immune checkpoint inhibitors; single-agent chemotherapy; double/triple agent chemotherapy; and targeted drug therapy.
4.4. Types of outcome measures
All relevant outcomes available in the reports were included, such as: overall survival (defined as survival time from the start of the intervention until death from any cause); progression-free survival (defined as survival time without disease progression or death from the start of the intervention, i.e., randomization); time to progression (defined as time from randomization in the study to tumor progression); objective response rate (defined as the proportion of patients with a complete response or partial response to treatment according to Response Evaluation Criteria in Solid Tumors); quality of life (measured using a validated scale/questionnaire); and grade three or higher serious adverse events (measured using National Cancer Institute-Common Terminology Criteria for Adverse Events) [52].
4.5. Search strategy
Literature searches were conducted to identify all published and unpublished phase II and phase III randomized controlled trials. Four electronic databases (PubMed, Embase, Web of Science, and Cochrane Central Register of Controlled Trials) were thoroughly searched as were abstracts from the American Society of Clinical Oncology (ASCO) meeting library. Reference lists of primary studies were reviewed and included articles were checked for any further references. Google and Google Scholar were also searched to identify any missing trials.
The search strategy was built with the help of a health sciences librarian, and it consisted of a combination of Medical Subject Heading (MeSH) terms and text words related to gastric cancer, metastases, and first line systemic therapies. The MEDLINE search strategy (Table 6) was developed first, and then adapted for use in the other databases (Appendix 1). The search was confined to English language publications and trials conducted among western populations, and was conducted from database inception until April 2022. Trials with the longest follow up periods were selected if multiple reports existed for the same trial.
4.6. Selection Criteria
Studies were included if they described phase II or phase III randomized controlled trials, included metastatic gastric cancer patients with tumor node metastasis phase III or phase IV, included patients who received at least one anti-tumor systemic therapy as recommended by National Comprehensive Cancer Network guidelines 2022, or described both gastric and esophageal cancer cases where subgroup data on gastric cancer were available.
Studies were excluded if they were non-randomized controlled trials designs or preclinical experiments, observational studies, case reports, duplicate publications, commentaries or editorials, pooled analyses, clinical trials without comparisons, published in languages other than English, included trial participants from outside western populations, described therapies other than first-line systemic therapy, or described only palliative care trials.
Two reviewers (S.M and D.A)independently screened all titles and abstracts identified using the search methods described. The full texts of all possibly relevant studies were retrieved and assessed for eligibility. Any discordance was resolved by consensus and with the help of a third reviewer (T.W) where necessary. A data screening tool that was specifically designed for this purpose was used. Ineligible studies with reasons for exclusion were identified and recorded. The selection process was recorded in sufficient detail to complete a PRISMA flow diagram (Figure 1).
4.7. Data extraction and management
A standard data collection form was designed for this study and included details on the study characteristics and outcomes. Two independent reviewers (S.M and D.A) extracted study characteristics and outcome data from included studies and met to agree consensus.
4.8. Risk of bias assessment
Two independent authors (SM and DA) assessed the included studies in accordance with version two of the Cochrane risk-of-bias tool for randomized trials [43]. The two reviewers compared their evaluations and resolved any possible discrepancies with a third reviewer who is a content expert (T.W). Overall risk of bias for each study included was reported in accordance with the risk-of-bias tool as low risk of bias, some concerns, or high risk of bias.
4.9. Data synthesis
Endnote was used to organize studies from different databases and to remove duplicate studies. A table summarizing the studies included was created using the captured study characteristics and outcomes. The design, conduct and writing of this systematic review was in accordance with the PRISMA Checklist.
5. Conclusions
With the evolving treatment landscape, improvement in clinical and safety outcomes can be seen in recent published randomized controlled trials. The potential of new targeted treatments and immunotherapies may present more favorable forthcoming options for locally advanced and metastatic gastric cancer.
Author Contributions
Conceptualization, S.M., D.A, D.R.A, M.Y., M.S., and T.W.; methodology, S.M. and D.A.; software, S.M. and D.A; validation, S.M., D.A., D.R.A., M.Y., M.S. and T.W.; formal analysis, S.M. and D.A.; investigation, S.M., D.A., and M.Y.; resources, T.W., M.Y., and D.R.A.; data curation, S.M. and D.A.; writing—original draft preparation, S.M. and D.A.; writing—review and editing, S.M., D.A., D.R.A., M.Y., M.S., and T.W.; visualization, S.M. and D.A.; supervision, D.R.A., M.Y., M.S., and T.W.; project administration, S.M., D.A., D.R.A., M.Y., M.S., and T.W.; funding acquisition, T.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Acknowledgments
Jennifer Martin, MA.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix 1: Search Strategy for Systematic Review
-
Search: Clinical, economic, and/or humanistic outcomes of first-line systemic therapies in patients with unresectable locally advanced/metastatic gastric cancer- A Systematic ReviewCitation account (if any): EndnoteLimits: English LanguageType of publications: phase II and phase III randomized controlled trialsInclusions:P- Adults aged ≥ 18 years with stage II – IV gastric cancerI- First line systemic therapies as approved by NCCN 2022 guidelinesC- First-line systemic therapies and/or best supportive care/placeboO- Clinical: Overall survival, Progression-free survival, time to progression, objective response rate, Safety: Grade ≥3 treatment related adverse eventHumanistic: Quality of life, utility estimates, where availableExclusion: Non-English publications, observational, narrative reviews, systematic reviews, meta-analyses, and non-research publications will be excluded. Also, studies that focused exclusively on other line of therapy than first line systemic therapy. Other interventions such as radiotherapy, surgical and total neoadjuvant chemotherapy will be excluded.Limits: English language and trials conducted among western population or countries.Search Dates: Inception to May 2022PubMed((("Stomach"[Mesh] OR "stomach"[ALL] OR "Gastric"[ALL] OR "Esophagogastric"[ALL] OR "oesophagogas-tric"[ALL] OR "Gastroesophageal"[ALL] OR "gastrooesophageal"[ALL]) AND ("Neoplasms"[Mesh] OR "Carcino-ma"[Mesh] OR "Stomach Neoplasms"[Mesh] OR "Adenocarcinoma"[Mesh] OR "Cancer*"[ALL] OR "Neo-plasm*"[ALL] OR "Adenocarcinoma*"[ALL] OR "Carcinoma*"[ALL] OR "Tumor*"[ALL] OR "Neoplasm, Stom-ach"[ALL] OR "Stomach Neoplasm"[ALL] OR "Neoplasms, Stomach"[ALL] OR "Gastric Neoplasms"[ALL] OR "Gastric Neoplasm"[ALL] OR "Neoplasm, Gastric"[ALL] OR "Neoplasms, Gastric"[ALL] OR "Cancer of Stom-ach"[ALL] OR "Stomach Cancers"[ALL] OR "Gastric Cancer"[ALL] OR "Cancer, Gastric"[ALL] OR "Cancers, Gas-tric"[ALL] OR "Gastric Cancers"[ALL] OR "Stomach Cancer"[ALL] OR "Cancer, Stomach"[ALL] OR "Cancers, Stomach"[ALL]) AND ("Neoplasm Metastasis"[Mesh] OR "secondary" [Subheading] OR "Advanced"[ALL] OR "Metastatic"[ALL] OR "Metastasis"[ALL] OR "Recurrent"[ALL] OR "Unresectable"[ALL] OR "Inoperable"[ALL] OR "Incurable"[ALL] OR "Neoplasm metastasis"[ALL] OR "Secondary neoplasm*"[ALL] OR "Secondary cancer*"[ALL] OR "Secondary tumor*"[ALL] OR "Stage III"[ALL] OR "Stage IV"[ALL]) AND (("Controlled Clinical Trial" [Publi-cation Type] OR "Clinical Trials as Topic"[Mesh] OR "Clinical Trial" [Publication Type] OR "Randomized Controlled Trials as Topic"[Mesh] OR "Randomised"[ALL] OR "Randomized"[ALL] OR "Randomly"[ALL] OR "Random"[ALL] OR "Randomized controlled trial*"[ALL] OR "Controlled clinical trial*"[ALL] OR "Trial*"[ALL] OR "Clinical tri-al*"[ALL] OR "placebo"[ALL])) AND ("Drug Therapy"[Mesh] OR "Antineoplastic Agents"[Mesh] OR "Chemo-therapy, Adjuvant"[Mesh] OR "Combined Modality Therapy"[Mesh] OR "Antineoplastic Combined Chemotherapy Protocols"[Mesh] OR "Palliative Care"[Mesh] OR "Antineoplastic Agents"[ALL] OR "Drug therapy"[ALL] OR "Chemotherapy"[ALL] OR "Adjuvant chemotherapy"[ALL] OR "Antineoplastic combined chemotherapy"[ALL] OR "Palliative care"[ALL] OR "First-line therapy"[ALL] OR "first line"[ALL] OR "Supportive care"[ALL] OR "Antineoplastic Combined Chemotherapy Protocols"[ALL] OR "Systemic therapy"[ALL])EMBASE#1)'stomach'/exp OR stomach OR gastric OR Esophagogastric OR oesophagogastric OR Gastroesophageal OR gastrooesophageal#2) 'neoplasm'/exp OR 'carcinoma'/exp OR 'stomach tumor'/exp OR 'adenocarcinoma'/exp OR 'malignant neoplasm'/exp OR 'stomach cancer'/exp OR 'neoplasms' OR 'carcinoma' OR 'stomach neoplasms' OR 'adenocarcinoma' OR 'cancer*' OR 'neoplasm*' OR 'adenocarcinoma*' OR 'carcinoma*' OR 'tumor*' OR 'neoplasm, stomach' OR 'stomach neoplasm' OR 'neoplasms, stomach' OR 'gastric neoplasms' OR 'gastric neoplasm' OR 'neoplasm, gastric' OR 'neoplasms, gastric' OR 'cancer of stomach' OR 'stomach cancers' OR 'gastric cancer' OR 'cancer, gastric' OR 'cancers, gastric' OR 'gastric cancers' OR 'stomach cancer' OR 'cancer, stomach' OR 'cancers, stomach'#3) 'metastasis'/exp OR 'secondary'/exp OR 'advanced cancer'/exp OR 'inoperable cancer'/exp OR 'incurable cancer'/exp OR "Neoplasm Metastasis" OR "secondary" "Advanced" OR "Metastatic" OR "Metastasis" OR "Recurrent" OR "Unresectable" OR "Inoperable" OR "Incurable" OR "Neoplasm metastasis" OR "Secondary neoplasm*" OR "Secondary cancer*" OR "Secondary tumor*" OR "Stage III" OR "Stage IV"#4)'controlled clinical trial'/exp OR 'clinical trial'/exp OR 'randomized controlled trial'/exp OR 'trial'/exp OR 'placebo'/exp OR "Controlled Clinical Trial" OR "Clinical Trials as Topic" OR "Clinical Trial" OR "Randomized Controlled Trials as Topic" OR "Randomised" OR "Randomized" OR "Randomly" OR "Random" OR "Randomized controlled trial*" OR "Controlled clinical trial*" OR "Trial*" OR "Clinical trial*" OR "placebo"#5) 'drug therapy'/exp OR 'antineoplastic agent'/exp OR 'chemotherapy'/exp OR 'adjuvant chemotherapy'/exp OR 'multimodality cancer therapy'/exp OR 'palliative therapy'/exp OR 'chemotherapy'/exp OR 'first line therapy'/exp OR 'supportive care'/exp OR 'systemic therapy'/exp OR "Drug Therapy" OR "Antineoplastic Agents" OR "Chemotherapy, Adjuvant" OR "Combined Modality Therapy" OR "Antineoplastic Combined Chemotherapy Protocols" OR "Palliative Care" OR "Antineoplastic Agents" OR "Drug therapy" OR "Chemotherapy" OR "Adjuvant chemotherapy" OR "Antineoplastic combined chemotherapy" OR "Palliative care" OR "First-line therapy" OR "first line" OR "Supportive care" OR "Antineoplastic Combined Chemotherapy Protocols" OR "Systemic therapy"#1 AND #2 AND #3 AND #4 AND #5SCOPUS(TITLE-ABS-KEY (stomach OR gastric OR Esophagogastric OR gastrooesophageal)) AND (TITLE-ABS-KEY (neoplasm OR carcinoma OR tumor OR adenocarcinoma OR cancer )) AND (TITLE-ABS-KEY ( metastasis OR advanced OR {stage III} OR {stage IV})) AND (TITLE-ABS-KEY ({controlled clinical trial} OR {clinical trial} OR {randomized controlled trial} OR trial OR placebo )) AND (TITLE-ABS-KEY ({antineoplastic agent} OR chemotherapy OR {palliative therapy} OR {multimodality cancer therapy} OR {systemic therapy}))COCHRANE CENTRAL REGISTER OF CONTROLLED TRIALS( neoplasm OR carcinoma OR tumor OR adenocarcinoma OR cancer ) AND ( stomach OR gastric OR esophagogastric OR gastrooesophageal ) AND ( metastasis OR advanced OR "stage III" OR "stage IV" ) AND ( "controlled clinical trial" OR "clinical trial" OR "randomized controlled trial" OR trial OR placebo ) AND ( "antineoplastic agent" OR chemotherapy OR "palliative therapy" OR "multimodality cancer therapy" OR "systemic therapy" )CLINICAL TRIAL.GOV(Stomach cancer OR gastric cancer OR “stomach adenocarcinoma” OR “STOMACH CANCER, STAGE 3” OR “STOMACH CANCER, STAGE 4” OR “Gastroesophageal TUMOR” OR “Gastroesophageal CANCER” OR “Gastroesophageal NEOPLASM” OR “Esophageal Cancer”) AND (metastasis OR advanced OR "stage III" OR "stage IV" ) AND ( "antineoplastic agent" OR chemotherapy OR "palliative therapy" OR "multimodality cancer therapy" OR "systemic therapy" ) Filters: Phase 3 , 4ASCO MEETING LIBRARY(Keywords:advanced gastric cancer OR Keywords:metastatic gastric cancer) AND (Keywords:first line AND Keywords: systemic therapies)
References
- Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Stomach Cancer Statistics | Gastric Cancer Statistics. www.cancer.org. https://www.cancer.org/cancer/stomach-cancer/about/key-statistics.
- Hundahl SA, Phillips JL, Menck HR. The National Cancer Data Base report on poor survival of U.S. gastric carcinoma patients treated with gastrectomy. Cancer. 2000, 88, 921–932. 2000, 88, 921–932.
- Casamayor M, Morlock R, Maeda H, Anjani J. Targeted literature review of the global burden of gastric cancer. ecancermedicalscience. 2018;12. [CrossRef]
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Nccn.org. Published January 11, 2022. https://www.nccn.org/professionals/physician_gls/pdf/gastric.pdf . 11 January.
- Gastric Cancer Treatment (PDQ®)–Health Professional Version - National Cancer Institute. www.cancer.gov. Published June 4, 2021. https://www.cancer.gov/types/stomach/hp/stomach-treatment-pdq#_81. 4 June.
- Genentech: News Features | Genentech Medicine Approved in Stomach Cancer. www.gene.com. Accessed September 29, 2021. https://www.gene.com/media/news-features/genentech-medicine-approved-in-stomach-cancer#:~:text=On%20October%2020%2C%202010%2C%20Herceptin. 29 September 2020.
- Lao Y, Shen D, Zhang W, He R, Jiang M. Immune Checkpoint Inhibitors in Cancer Therapy-How to Overcome Drug Resistance? Cancers. 2022, 14, 3575. [CrossRef]
- Rodrigues S, Figueiredo C. Recent insights into the use of immune checkpoint inhibitors in gastric cancer. Porto Biomedical Journal. 2022, 7, e162. [Google Scholar] [CrossRef]
- Chen C, Zhang F, Zhou N, et al. Efficacy and safety of immune checkpoint inhibitors in advanced gastric or gastroesophageal junction cancer: a systematic review and meta-analysis. OncoImmunology. 2019, 8, e1581547. [Google Scholar] [CrossRef]
- Kang YK, Boku N, Satoh T, et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): a randomised, double-blind, placebo-controlled, phase 3 trial. The Lancet. 2017, 390, 2461–2471. [Google Scholar] [CrossRef]
- Lorenzen S, Thuss-Patience PC, Riera Knorrenschild J, et al. FOLFOX versus FOLFOX plus nivolumab and ipilimumab administered in parallel or sequentially versus FLOT plus nivolumab administered in parallel in patients with previously untreated advanced or metastatic adenocarcinoma of the stomach or gastroesophageal junction: A randomized phase 2 trial of the AIO. Journal of Clinical Oncology. 2022, 40, 4043–4043. [Google Scholar] [CrossRef]
- Patrinely JR, Johnson R, Lawless AR, et al. Chronic Immune-Related Adverse Events Following Adjuvant Anti–PD-1 Therapy for High-risk Resected Melanoma. JAMA Oncology. 2021, 7, 744. [Google Scholar] [CrossRef]
- Ter Veer E, Haj Mohammad N, Van Valkenhoef G, et al. 2369 Efficacy and safety of first line chemotherapy in Advanced EsophagoGastric Cancer (AEGC): A network meta-analysis. European Journal of Cancer. 2015, 51, S459. [CrossRef]
- Guo X, Zhao F, Ma X, et al. A comparison between triplet and doublet chemotherapy in improving the survival of patients with advanced gastric cancer: a systematic review and meta-analysis. BMC Cancer. 2019, 19. [Google Scholar] [CrossRef]
- Zhu L, Liu J, MA S. Fluoropyrimidine-Based Chemotherapy as First-Line Treatment for Advanced Gastric Cancer: a Bayesian Network Meta-Analysis. Pathology & Oncology Research. 2016, 22, 853–861. [Google Scholar] [CrossRef]
- Song H, Zhu J, Lu D. Molecular-targeted first-line therapy for advanced gastric cancer. Cochrane Database of Systematic Reviews. Published online , 2016. 19 July. [CrossRef]
- Cheng J, Cai M, Shuai X, Gao J, Wang G, Tao K. First-line systemic therapy for advanced gastric cancer: a systematic review and network meta-analysis. Therapeutic Advances in Medical Oncology. 2019, 11, 1758835919877726. [Google Scholar] [CrossRef]
- Ajani JA, Fodor MB, Tjulandin SA, et al. Phase II Multi-Institutional Randomized Trial of Docetaxel Plus Cisplatin With or Without Fluorouracil in Patients With Untreated, Advanced Gastric, or Gastroesophageal Adenocarcinoma. Journal of Clinical Oncology. 2005, 23, 5660–5667. [Google Scholar] [CrossRef] [PubMed]
- Ajani JA, Moiseyenko VM, Tjulandin S, et al. Quality of Life With Docetaxel Plus Cisplatin and Fluorouracil Compared With Cisplatin and Fluorouracil From a Phase III Trial for Advanced Gastric or Gastroesophageal Adenocarcinoma: The V-325 Study Group. Journal of Clinical Oncology. 2007, 25, 3210–3216. [Google Scholar] [CrossRef] [PubMed]
- Ajani JA, Rodriguez W, Bodoky G, et al. Multicenter Phase III Comparison of Cisplatin/S-1 With Cisplatin/Infusional Fluorouracil in Advanced Gastric or Gastroesophageal Adenocarcinoma Study: The FLAGS Trial. Journal of Clinical Oncology. 2010, 28, 1547–1553. [Google Scholar] [CrossRef]
- Al-Batran SE, Hartmann JT, Probst S, et al. Phase III trial in metastatic gastroesophageal adenocarcinoma with fluorouracil, leucovorin plus either oxaliplatin or cisplatin: a study of the Arbeitsgemeinschaft Internistische Onkologie. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology. 2008, 26, 1435–1442. [Google Scholar] [CrossRef]
- Al-Batran SE, Pauligk C, Homann N, et al. The feasibility of triple-drug chemotherapy combination in older adult patients with oesophagogastric cancer: A randomised trial of the Arbeitsgemeinschaft Internistische Onkologie (FLOT65+). European Journal of Cancer. 2013, 49, 835–842. [Google Scholar] [CrossRef]
- Bouché O, Raoul JL, Bonnetain F, et al. Randomized Multicenter Phase II Trial of a Biweekly Regimen of Fluorouracil and Leucovorin (LV5FU2), LV5FU2 Plus Cisplatin, or LV5FU2 Plus Irinotecan in Patients With Previously Untreated Metastatic Gastric Cancer: A Fédération Francophone de Cancérologie Digestive Group Study—FFCD 9803. Journal of Clinical Oncology. 2004, 22, 4319–4328. [Google Scholar] [CrossRef]
- Cascinu S, Galizia E, Labianca R, et al. Pegylated liposomal doxorubicin, 5-fluorouracil and cisplatin versus mitomycin-C, 5-fluorouracil and cisplatin for advanced gastric cancer: a randomized phase II trial. Cancer Chemotherapy and Pharmacology. 2010, 68, 37–43. [Google Scholar] [CrossRef]
- Catenacci DVT, Tebbutt NC, Davidenko I, et al. Rilotumumab plus epirubicin, cisplatin, and capecitabine as first-line therapy in advanced MET-positive gastric or gastro-oesophageal junction cancer (RILOMET-1): a randomised, double-blind, placebo-controlled, phase 3 trial. The Lancet Oncology. 2017, 18, 1467–1482. [Google Scholar] [CrossRef] [PubMed]
- Cocconi G, Bella M, Zironi S, et al. Fluorouracil, doxorubicin, and mitomycin combination versus PELF chemotherapy in advanced gastric cancer: a prospective randomized trial of the Italian Oncology Group for Clinical Research. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology. 1994, 12, 2687–2693. [Google Scholar] [CrossRef] [PubMed]
- Coombes RC, Chilvers CED, Amadori D, et al. Randomised trial of epirubicin versus fluorouracil in advanced gastric cancer. Annals of Oncology. 1994, 5, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Curran D, Pozzo C, Zaluski J, et al. Quality of life of palliative chemotherapy naive patients with advanced adenocarcinoma of the stomach or esophagogastric junction treated with irinotecan combined with 5-fluorouracil and folinic acid: results of a randomised phase III trial. Quality of Life Research: An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation. 2009, 18, 853–861. [Google Scholar] [CrossRef]
- 30. Fuchs C, Shitara K, Di Bartolomeo M, et al. Ramucirumab as First-Line Therapy in Combination with Cisplatin and Fluoropyrimidine in Patients with Metastatic Gastric or Gastro-Oesophageal Junction Adenocarcinoma (RAINFALL): A Global, Randomised, Double-Blinded, Placebo-Controlled, Phase 3 Trial. SSRN Electronic Journal. Published online 2018. [CrossRef]
- Gubanski M, Johnsson A, Fernebro E, et al. Randomized phase II study of sequential docetaxel and irinotecan with 5-fluorouracil/folinic acid (leucovorin) in patients with advanced gastric cancer: the GATAC trial. Gastric Cancer: Official Journal of the International Gastric Cancer Association and the Japanese Gastric Cancer Association. 2010, 13, 155–161. [Google Scholar] [CrossRef]
- Högner A, Al-Batran SE, Siveke JT, et al. Pazopanib with 5-FU and oxaliplatin as first line therapy in advanced gastric cancer: A randomized phase-II study-The PaFLO trial. A study of the Arbeitsgemeinschaft Internistische Onkologie AIO-STO-0510. International Journal of Cancer. 2022, 150, 1007–1017. [CrossRef]
- Içli F, Celik I, Aykan F, et al. A randomized Phase III trial of etoposide, epirubicin, and cisplatin versus 5-fluorouracil, epirubicin, and cisplatin in the treatment of patients with advanced gastric carcinoma. Turkish Oncology Group. Cancer. 1998;83(12):2475-2480. Accessed May 4, 2023. https://pubmed.ncbi.nlm.nih.gov/9874451/.
- Janjigian YY, Shitara K, Moehler M, et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial. The Lancet. 2021, 398, 27–40. [Google Scholar] [CrossRef]
- Kang YK ., Kang WK ., Shin DB ., et al. Capecitabine/cisplatin versus 5-fluorouracil/cisplatin as first-line therapy in patients with advanced gastric cancer: a randomised phase III noninferiority trial. Annals of Oncology. 2009, 20, 666–673. [CrossRef]
- Ochenduszko S, Puskulluoglu M, Konopka K, et al. Comparison of efficacy and safety of first-line palliative chemotherapy with EOX and mDCF regimens in patients with locally advanced inoperable or metastatic HER2-negative gastric or gastroesophageal junction adenocarcinoma: a randomized phase 3 trial. Medical Oncology. 2015, 32. [Google Scholar] [CrossRef]
- Petersen PC, Petersen LN, Vogelius I, Bjerregaard JK, Baeksgaard L. A randomized phase 2 trial of first-line docetaxel, carboplatin, capecitabine (CTX) and epirubicin, oxaliplatin, capecitabine (EOX) in advanced esophagogastric adenocarcinoma. Acta Oncologica (Stockholm, Sweden). 2021, 60, 948–953. [Google Scholar] [CrossRef] [PubMed]
- Roth AD, Fazio N, Stupp R, et al. Docetaxel, Cisplatin, and Fluorouracil; Docetaxel and Cisplatin; and Epirubicin, Cisplatin, and Fluorouracil As Systemic Treatment for Advanced Gastric Carcinoma: A Randomized Phase II Trial of the Swiss Group for Clinical Cancer Research. Journal of Clinical Oncology. 2007, 25, 3217–3223. [Google Scholar] [CrossRef] [PubMed]
- Shitara K, Van Cutsem E, Bang YJ, et al. Efficacy and Safety of Pembrolizumab or Pembrolizumab Plus Chemotherapy vs Chemotherapy Alone for Patients With First-line, Advanced Gastric Cancer: The KEYNOTE-062 Phase 3 Randomized Clinical Trial. JAMA oncology. 2020, 6, 1571–1580. [Google Scholar] [CrossRef] [PubMed]
- Shitara K, Doi T, Hosaka H, et al. Efficacy and safety of trifluridine/tipiracil in older and younger patients with metastatic gastric or gastroesophageal junction cancer: subgroup analysis of a randomized phase 3 study (TAGS). Gastric Cancer: Official Journal of the International Gastric Cancer Association and the Japanese Gastric Cancer Association. 2022, 25, 586–597. [Google Scholar] [CrossRef]
- Van Cutsem E, Moiseyenko VM, Tjulandin S, et al. Phase III Study of Docetaxel and Cisplatin Plus Fluorouracil Compared With Cisplatin and Fluorouracil As First-Line Therapy for Advanced Gastric Cancer: A Report of the V325 Study Group. Journal of Clinical Oncology. 2006, 24, 4991–4997. [Google Scholar] [CrossRef] [PubMed]
- Webb A, Cunningham D, Scarffe JH, et al. Randomized trial comparing epirubicin, cisplatin, and fluorouracil versus fluorouracil, doxorubicin, and methotrexate in advanced esophagogastric cancer. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology. 1997, 15, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019, l4898. [CrossRef]
- Cheng J, Cai M, Shuai X, Gao J, Wang G, Tao K. First-Line Systemic Therapy for Advanced Gastric Cancer: A Systematic Review and Network Meta-Analysis of 118 Randomized Controlled Trials. SSRN Electronic Journal. 2018. [CrossRef]
- Wagner AD, Grothe W, Haerting J, Kleber G, Grothey A, Fleig WE. Chemotherapy in Advanced Gastric Cancer: A Systematic Review and Meta-Analysis Based on Aggregate Data. Journal of Clinical Oncology. 2006, 24, 2903–2909. [Google Scholar] [CrossRef]
- CheckMate 649: Long-Term Data Support Nivolumab Plus Chemotherapy but Not Nivolumab Plus Ipilimumab in Gastric Cancer - The ASCO Post. ascopost.com. Published October 25, 2021. Accessed June 10, 2022. https://ascopost.com/issues/october-25-2021/checkmate-649-long-term-data-support-nivolumab-plus-chemotherapy-but-not-nivolumab-plus-ipilimumab-in-gastric-cancer/#:~:text=Objective%20response%20rates%20were%2060. 25 October.
- 47. Takashima A, Iizumi S, Boku N. Survival after failure of first-line chemotherapy in advanced gastric cancer patients: differences between Japan and the rest of the world. Japanese Journal of Clinical Oncology. 2017;47(7):583-589. [CrossRef]
- Koizumi W. Chemotherapy for advanced gastric cancer: review of global and Japanese status. Gastrointestinal cancer research : GCR. 2007;1(5):197-203. Accessed August 16, 2022. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2632531.
- Elimova E, Wyrwicz L, Blum SI, et al. Health-related quality of life (HRQOL) in patients (pts) with advanced gastric cancer/gastroesophageal junction cancer (GC/GEJC) or esophageal adenocarcinoma (EAC): Results of nivolumab plus chemotherapy (NIVO+chemo) versus chemo from CheckMate 649. Journal of Clinical Oncology. 2021, 39(28_suppl):167-167. [CrossRef]
- van Amelsfoort RM, van der Sluis K, Schats W, et al. Health-Related Quality of Life in Locally Advanced Gastric Cancer: A Systematic Review. Cancers. 2021, 13, 5934. [Google Scholar] [CrossRef] [PubMed]
- Park R, Da Silva LL, Saeed A. Immunotherapy Predictive Molecular Markers in Advanced Gastroesophageal Cancer: MSI and Beyond. Cancers. 2021, 13, 1715. [Google Scholar] [CrossRef] [PubMed]
- Common Terminology Criteria for Adverse Events (CTCAE) Common Terminology Criteria for Adverse Events (CTCAE) V5.0.; 2017. https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf.
Figure 1.
Systematic Review inclusion and exclusion flowchart.
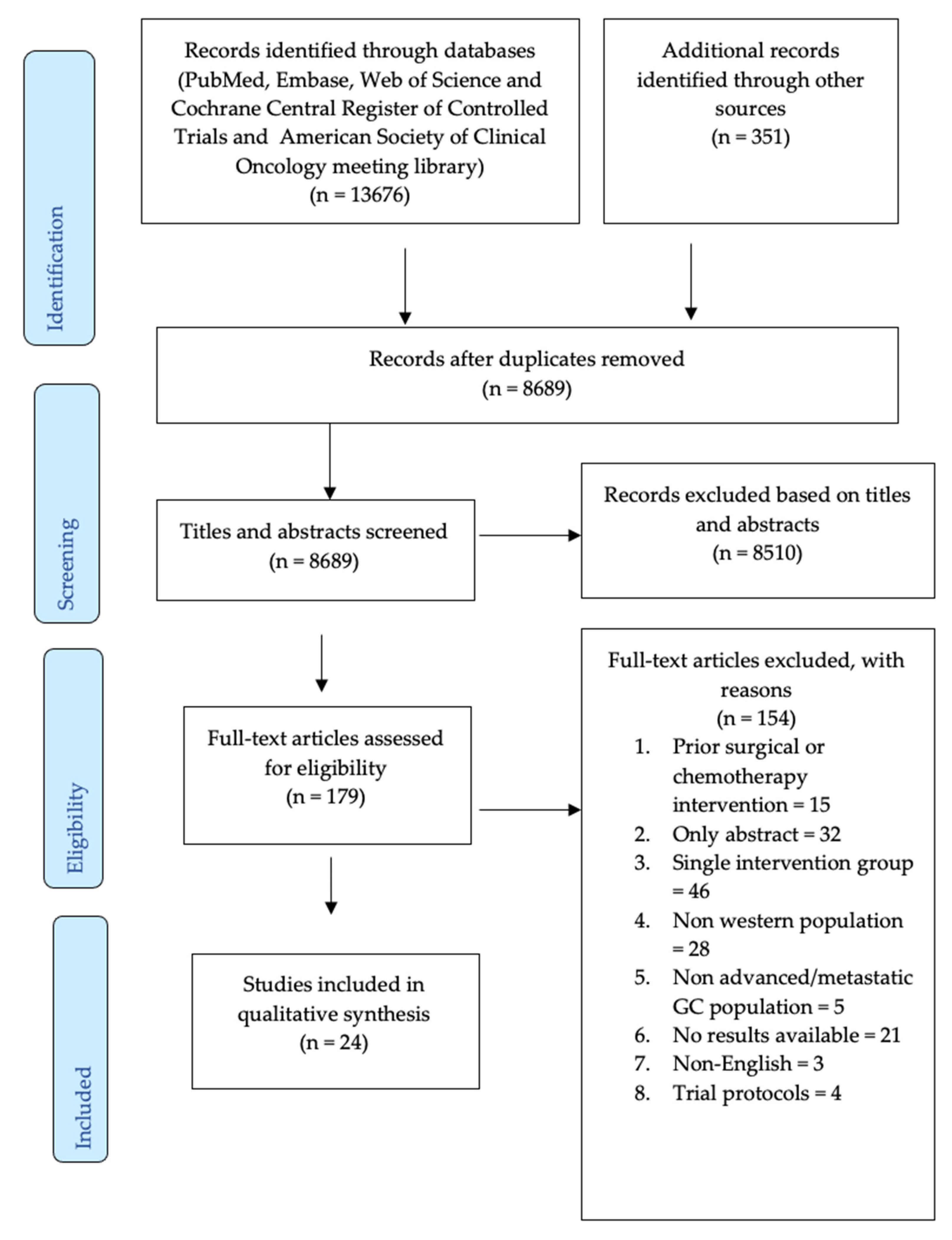

Table 1.
Baseline characteristics of included randomized control trials of untreated locally advanced and metastatic gastric cancer.
Table 1.
Baseline characteristics of included randomized control trials of untreated locally advanced and metastatic gastric cancer.
| Author, year | Country | Phase | Study design | Total N | Treatment arms | Age Median (range) |
Males, n (%) |
|---|---|---|---|---|---|---|---|
| Ajani, 200519 | Multiple | II | Open label | 155 | Docetaxel-cisplatin | 57 (21-83) | 114 (74) |
| Docetaxel-cisplatin-fluorouracil | |||||||
| Ajani, 200720 |
Multiple | III | Open label | 445 | Docetaxel-cisplatin-fluorouracil | 55 (26-79) | (71.9) |
| Cisplatin-fluorouracil | 55 (25-76) | (70.5) | |||||
| Ajani, 201021 | Multiple | III | Open label | 1029 | Cisplatin-S1 | 59.0 (18,85)+ | 729 (70.8) |
| Cisplatin-fluorouracil | |||||||
| Al-Batran, 200822 | Germany + Switzerland |
III |
NR | 220 | Fluorouracil-leucovorin-oxaliplatin | 64 (33-86) | 64 (57) |
| Fluorouracil-leucovorin-cisplatin | 64 (27-85) | 81 (75) | |||||
| Al-Batran, 201323 | Germany | III | Open label | 143 | Fluorouracil-leucovorin-oxaliplatin-docetaxel | 69 | 51 (71) |
| Fluorouracil-leucovorin-oxaliplatin | 70 | 45 (63) | |||||
| Bouche, 200424 | France | III | Open label | 136 | Leucovorin–5-flurouracil | 64 (45-75) | (82) |
| Leucovorin–5-flurouracil–cisplatin | 64 (43-76) | (80) | |||||
| Leucovorin–5-flurouracil-irinotecan | 65 (37-76) | (84) | |||||
| Cascinu, 201025 | Italy | II | NR | 78 | 5-flurouracil-cisplatin-doxorubicin | 63 (33-75) | 50 (64) |
| 5-flurouracil-cisplatin-mitomycin | |||||||
| Catenacci, 201726 | Multiple | III | double-blind, placebo | 609 | Rilotumumab-epirubicin-cisplatin-capecitabine | 61 (28-84) | (67) |
| Placebo-epirubicin-cisplatin-capecitabine | 59 (26-81) | (72) | |||||
| Cocconi, 199427 |
Italy | III | NR | 130 | Cisplatin-epirubicin-leucovorin-flurouracil | 62 (28-74) | 60 (71) |
| Fluorouracil-doxorubicin-mitomycin | 65 (40-75) | 42 (81) | |||||
| Coombes, 199428 | United Kingdom | NR | NR | 69 | Epirubicin | 59.9 (9.3)* | 27 (7.5)* |
| Fluorouracil | 55.6 (9.2)* | 24 (7.3)* | |||||
| Curran, 200929 | Multiple | III | NR | 333 | Irinotecan-fluorouracil | NR | NR |
| Cisplatin-fluorouracil | |||||||
| Fuchs, 201930 | Multiple | III | double-blind, placebo | 645 | Ramucirumab-flurouracil-cisplatin | 60 (51-68) | 214 (66) |
| Placebo-flurouracil-cisplatin | 62 (54-68) | 215 (67) | |||||
| Gubanski, 201031 | Sweden | II | Crossover | 80 | Irinotecan-5-fluorouracil-leucovorin | 63 (39-79) | (67) |
| Docetaxel-leucovorin | 64 (42-75) | (87) | |||||
| Högner, 202132 | Germany | II | Open label | 87 | Pazopanib-5-fluorouracil-oxaliplatin | 65 | 37 (72) |
| Fluorouracil-leucovorin-oxaliplatin | 60 | 17 (63) | |||||
| Icli, 199833 | Turkey | III | NR | 131 | Etoposide-epirubicin-cisplatin | 52.7 (9.2)* | (68.8) |
| 5-fluorouracil-epirubicin-cisplatin | 52.7 (9.4)* | (59.7) | |||||
| Janjigian, 202134 | Multiple | III | Open label | 1581 | Nivolumab-capecitabine-oxaliplatin or leucovorin-fluorouracil-oxaliplatin | 62 (54-69) | 540 (68) |
| Capecitabine-oxaliplatin or leucovorin-fluorouracil-oxaliplatin | 61 (53-68) | 560 (71) | |||||
| Kang, 200935 | Multiple | III | Open label | 316 | Cisplatin-capecitabine | 56 (26-74) | 103 (64) |
| Cisplatin-fluorouracil | 56 (22-73) | 108 (69) | |||||
| Ochend- uszko, 201536 |
Poland | III | NR | 56 | Epirubicin-oxaliplatin-capecitabine | 57.9 (10.8) | 16 (55) |
| Docetaxel-cisplatin-5-fluorouracil-leucovorin | 60.3 (9.11) | 13 (48) | |||||
| Petersen, 202137 | Denmark | II | Open label | 110 | Docetaxel-carboplatin-capecitabine | 64 (36-79) | 79 (81) |
| Epirubicin-oxaliplatin-capecitabine | |||||||
| Roth, 200738 | Multiple | II | 3-arm | 119 | Epirubicin-cisplatin-flurouracil | 59 (32-71) | 75 |
| Docetaxel-cisplatin | 58 (40-70) | 76 | |||||
| Docetaxel-cisplatin-fluorouracil | 61 (35-78) | 61 | |||||
| Shitara, 202039 | Multiple | II | Open label | 763 | Pembrolizumab | 61 (20-83) | 180 (70.3) |
| Pembrolizumab-cisplatin-capecitabine-fluorouracil | 62 (22-83) | 195 (75.9) | |||||
| Placebo-cisplatin-capecitabine-fluorouracil | 62.5 (23-87) | 179 (71.6) | |||||
| Shitara, 202240 | Multiple | III | Open label | 813 | Nivolumab- ipilimumab |
62 (22‒84) | 278 (68) |
| Capecitabine-oxaliplatin or leucovorin-fluorouracil-oxaliplatin | 61 (23‒90) | 280 (69) | |||||
| Van Cutsem, 200641 | Multiple | III | Open label | 457 | Docetaxel-cisplatin-fluorouracil Cisplatin-fluorouracil |
55 (25-79) | 317 (71) |
| Webb, 199742 | United Kingdom | II | Open label | 256 | Epirubicin-cisplatin-flurouracil | 59 (35-79) | 99 |
| Fluorouracil-doxorubicin-methotrexate | 60 (29-78) | 110 |
NR = not reported in the study. S-1 is a novel oral fluoropyrimidine derivative. + = min-max. * = mean and standard deviation.
Table 2.
Characteristics of the cancer and reported outcomes.
| Author, year | Tumor location-stomach gastric, n (%) | Disease stage, n (%) |
No. of organs involved in metastases,n (%) | ECOG status n (%) | Outcomes | |||
|---|---|---|---|---|---|---|---|---|
| Locally advanced | Metastatic | 1-2 | >2 | 0-1 | ≥2 | |||
| Ajani, 200519 | 106 (68) | 5 (3) |
147 (95) | 84 (61) | 61 (39) | 66 (43) | NR | Complete response, Objective response rate, Overall survival, partial response, Time to progression |
| Ajani, 200720 |
NR | 12 (3) | 430 (97) | (53.8) | (45.2) | 80 (36) | NR | Time to 5% deterioration of global health status from baseline |
| (54.9) | (44.6) | 81 (36) | NR | |||||
| Ajani, 201021 | 855 (83.1) | 43 (4.2) |
1085 (95.7) | NR | NR | 1029 (58.6) | NR | Overall survival, Progression-free survival, Response rate |
| Al-Batran, 200822 | 92 (82) | 3 (2.7) | 109 (97.3) | 59 (52.7) | 53 (47.4) | 103 (92) | 9 (8) | Overall survival, Progression-free survival, Response rate |
| 10 (9.3) | 98 (90.7) | 63 (58.3) | 45 (41.7) | 97 (90) | 11 (10) | |||
| Al-Batran, 201323 | 45 (63) | 22 (31) | 50 (69) | Median = 2 | 67 (93) | 5 (7) | Objective response rate | |
| 22 (32) | 49 (68) | 65 (92) | 6 (9) | |||||
| Bouche, 200424 | (71) | NR | NR | (80) | (20) | (73) | (27) | Overall survival, Progression-free survival, Response rate |
| (70) | (85) | (15) | (75) | (25) | ||||
| (67) | (83) | (17) | (78) | (22) | ||||
| Cascinu, 201125 | 69 (89) | 8 (10) | 70 (89) | NR | NR | 73 (93.7) | 5 (6.3) | Objective response rate, Overall survival, Time to progression |
| Catenacci, 201726 | 227 (75) | NR | 284 (93) | NR | NR | 304 (100) | 0 (0) | Duration of response, Overall survival, Progression-free survival, Time to progression |
| 195 (64) | NR | 283 (93) | 304 (100) | 1 (<1) | ||||
| Cocconi, 199427 |
NR | NR | NR | NR | NR | NR | 5 (6) | Duration of response, Objective response rate, Overall survival, Time to progression |
| NR | 5 (10) | |||||||
| Coombes, 199428 | NR | NR | NR | NR | NR | NR | NR | Overall survival |
| Curran, 200929 | NR | NR | NR | NR | NR | NR | NR | Quality of life, Time to progression |
| Fuchs, 201930 | 242 (74) | NR | NR | 243 (75) | 81 (25) | 326 (100) | NR | Objective response rate, Overall survival, Progression-free survival, Time to progression |
| 239 (75) | 242 (76) | 76 (24) | 319 (100) | NR | ||||
| Gubanski, 201031 | NR | NR | NR | NR | NR | (88) | (1) | Overall survival, Progression-free survival |
| NR | NR | NR | NR | NR | (99) | (18) | ||
| Högner, 202132 | 21 (41) | NR | NR | 15 (27) | 6 (71) | NR | NR | Objective response rate, Overall survival, Progression-free survival |
| 19 (70) | 13 (48) | 14 (51) | ||||||
| Icli, 199833 | NR | 17.2 | 82.8 | NR | NR | (65.6) | (34.4) | Objective response rate, Overall survival |
| 20.9 | 79.1 | (68.6) | (31.4) | |||||
| Janjigian, 202134 | 544 (70) | 27 (3) | 757 (96) | 164 (21) | 602 (76) | NR | NR | Overall survival, Progression-free survival |
| 556 (70) | 34 (4) | 756 (95) | 183 (23) | 583 (74) | ||||
| Kang, 200935 | NR | NR | NR | 127 (80) | 32 (20) | Median=1 (0-1) |
NR | Duration of response, Objective response rate, Overall survival, Progression-free survival |
| 126 (80) | 27 (20) | |||||||
| Ochend-uszko, 201536 | NR | 1 (4) | 28 (97) | 27 (91) | 2 (7) | 26 (89) | 3 (10) | Overall survival, Progression-free survival |
| 3 (11) | 24 (89) | 23 (85) | 4 (15) | 25 (93) | 2 (7) | |||
| Petersen, 202137 | 25 (26) | 10 (10) | 88 (89) | 54 (55) | 44 (45) | 98 (100) | NR | Overall survival, Progression-free survival |
| Roth, 200738 | NR | NR | (83) | (90) | (9) | NR | NR | Overall survival, Quality of life, Time to progression |
| (82) | (79) | (21) | ||||||
| (95) | (84) | (15) | ||||||
| Shitara, 202039 | 176 (68.8) | NR | NR | NR | NR | NR | NR | NR |
| 170 (66.1) | ||||||||
| 181 (72.4) | ||||||||
| Shitara, 202240 | 282 (69) | 14 (3) | 391 (96) | 83 (20) | 100 (25) | 409 (100) | NR | Duration of response, Overall survival, Progression-free survival, Quality of life |
| 282 (70) | 18 (4) | 386 (96) | 326 (80) | 304 (75) | 404 (100) | NR | ||
| Van Cutsem, 200641 | NR | 12 (3) | 43 (97) | 242 (54) | 200 (45) | 161 (36) | NR | Objective response rate, Overall survival, Time to progression |
| Webb, 199742 | 72 (57) | 47 (37) | 79 (63) | NR | NR | 96 (76) | 30 (24) | Objective response rate, Overall survival, Quality of life |
| 73 (56) | 51 (40) | 79 (60) | 97 (75) | 32 (25) | ||||
NR = not reported in the study. ECOG = Eastern Cooperative Oncology Group.
Table 3.
Efficacy of the first-line systemic treatments among trial patients with locally advanced and metastatic gastric cancer.
Table 3.
Efficacy of the first-line systemic treatments among trial patients with locally advanced and metastatic gastric cancer.
| Author, year | Treatment arms | n for each arm | Overall survival, months | Progression free survival, months | Objective response rate, % | Other outcomes | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Median | HR (95% CI); p | Median | HR (95% CI); p | Median | p value | Description | HR (95% CI); p | |||
| Ajani, 200519 | Docetaxel-cisplatin | 76 | 9.6 | 1.19 (0.83-1.69) | NR | NR | 26 | NR | Time to progression: 5.9 months | 0.80 (0.52-1.22) |
| Docetaxel-cisplatin-fluorouracil | 79 | 10.5 | NR | NR | 43 | Time to progression: 5 months | ||||
| Ajani, 200720 | Docetaxel-cisplatin-fluorouracil | 85 | NR | NR | NR | NR | NR | NR | Time to 5% deterioration of global health status from baseline: 6.5 months | 1.45 (1.08-1.93) p=0.01 |
| Cisplatin-fluorouracil | 104 | NR | NR | NR | NR | NR | NR | Time to 5% deterioration of global health status from baseline: 4.2 months | ||
| Ajani, 201021 | Cisplatin-S1 | 521 | 8.6 | 0.92 (0.80-1.05) 0.20 | 4.8 | 0.99 (0.86-1.14) | 29.0 |
NR |
Median duration of response: 6.5 months | 0.77 (0.57-1.03) |
| Cisplatin-fluorouracil | 508 | 7.9 | 5.5 | 32.0 | Median duration of response: 5.8 months | |||||
| Al-Batran, 200822 | Fluorouracil-leucovorin-oxaliplatin | 112 | 10.7 (8.5-13.9) | p=0.51 | 5.8 (4.5-6.6) | NR | 34.8 | NR |
NR | NR |
| Fluorouracil-leucovorin-cisplatin | 102 | 8.8 (7.7-12.0) | 3.9 (3.1-4.8) | 24.50 | NR | NR | ||||
| Al-Batran, 201323 | Fluorouracil-leucovorin-oxaliplatin-docetaxel | 72 | NR | NR | NR | NR | 48.6 (36.7-60.7) | p=0.02 | Quality of life global health status scores at 0, 8, 16 and 24 weeks: 56.5 ± 24.4, 53.6 ± 19.9,56.8 ± 19.5 and 53.7 ± 22.8 | No significant differences between arms |
| Fluorouracil-leucovorin-oxaliplatin | 71 | NR | NR | NR | NR | 28.2 (18.1-40.1) | Quality of life global health status scores at 0, 8, 16 and 24 weeks: 49.4 ± 24.7,58.2 ± 19.8, 53.3 ± 21.0 and 55.5 ± 16.9 | |||
| Bouche, 200424 | Leucovorin–5-flurouracil | 45 | 6.8 (2.6-11.1) | NR | 3.2 (1.8-4.6) | NR | 13 (3.4-23.3) | NR |
Mean difference in global quality of life scores between Leucovorin–5-flurouracil vs Leucovorin–5-flurouracil-irinotecan = 2.2.Mean difference in global quality of life scores between Leucovorin–5-flurouracil–cisplatin vs Leucovorin–5-flurouracil-irinotecan = 0.8 | Treatment effect: 0.89; p<0.01 |
| Leucovorin–5-flurouracil–cisplatin | 44 | 9.5 (6.9-12.2) | NR | 4.9 (3.5-6.3) | 27 (14.1-40.4) | |||||
| Leucovorin–5-flurouracil-irinotecan | 45 | 11.3 (9.3-13.3) | NR | 6.9 (5.5-8.3) | 40 (25.7-54.3) | |||||
| Cascinu, 201125 | 5-flurouracil-cisplatin-doxorubicin | 39 | 12.1 | 0.63 (0.34-0.91) p=0.02 | NR | NR | 64.1 (48-77) | p=0.04 | Time to progression: 7.9 month | 0.62, (0.37-0.97) p=0.04 |
| 5-flurouracil-cisplatin-mitomycin | 39 | 8.3 | NR | NR | 39 (24-54) | Time to progression: 5.1 months | ||||
| Catenacci, 201726 | Rilotumumab-epirubicin-cisplatin-capecitabine | 298 | 8·8 (7·7–10·2) | 1·34 (1·10–1·63) p<0·01) | 5·6 (5·3–5·9) | 1·26 (1·04–1·51) | 29·8 (24·3–35·7) | NR | Time to progression: 6·1 month (95% CI=5·7–7·9) Duration of response: 2·8 months (IQR=2·7–2·9) |
1·24 (0·96–1·59) p=0·10 |
| Placebo-epirubicin-cisplatin-capecitabine | 299 | 10·7 (9·6–12·4) | 6·0 (5·7–7·2) | 44·6 (38·5–50·8) | Time to progression: 7·1 month (5·9–7·9)Duration of response: 2·8 months (2·6–2·9) | |||||
| Cocconi, 199427 | Cisplatin-epirubicin-leucovorin-flurouracil | 85 | 8.1 (0.2-33.5) | p=0.24 | NR | NR | 43 | P<0.01 | Time to progression: 4.7 month (0.2-26.5) | p=0.58 |
| Fluorouracil-doxorubicin-mitomycin | 52 | 5.6 (0.5-49.1) | NR | NR | 15 | 2.6 month (0.5-33.2) | ||||
| Coombes, 199428 | Epirubicin | 36 | 88.2% died | p=0.65 | NR | NR | NR | NR | NR | NR |
| Fluorouracil | 33 | 3.9% died | NR | NR | NR | NR | NR | NR | ||
| Curran, 200929 | Irinotecan-fluorouracil | 172 | NR | NR | NR | NR | NR | NR | Time to progression: 5 month; Global health status mean 62.4 (20.1) | p=0.088; p=0.061 |
| Cisplatin-fluorouracil | 165 | NR | NR | NR | NR | NR | NR | Time to progression: 4.2 months; Global health status mean- 56.9 (21.1) | ||
| Fuchs, 201930 | Ramucirumab-flurouracil-cisplatin | 326 | 11·2 (9·9–11·9) |
0·96 (0·80–1·16) p=0·67 | 5·7 (5·5–6·5) | 0.75, (0.61–0.94) p=0.01 | 41.1 (35.8-46.4) | p=0.17 | Time to progression: 6.8 month(5.9-7.7) | p=0.70 (0.57-0.86) |
| Placebo-flurouracil-cisplatin | 319 | 10·7 (9·5–11·9) | 5·4 (4·5–5·7) |
36.4 (31.1-41.6) | Time to progression: 5.8 months (5.6-6.4) | |||||
| Gubanski, 201031 | Irinotecan-5-fluorouracil-leucovorin | 39 | 11.5 | p=0.3 | 4.9 | NR | NR | NR | NR | NR |
| Docetaxel-leucovorin | 39 | 10.6 | 5.0 | NR | NR | NR | NR | |||
| Högner, 202232 | Pazopanib-5-fluorouracil-oxaliplatin | 51 | 10.2 (5.5-14.9) | 1.01 (0.62-1.65)p=0.95 | 4.7 (2.9-6.5) | 0.96 (0.60-1.55) p=0.88 |
25 | NR | NR | NR |
| Fluorouracil-leucovorin-oxaliplatin | 27 | 7.3 (4.9-9.7) | 4.5 (1.8-7.1) | 26 | NR | NR | ||||
| Icli, 199833 | Etoposide-epirubicin-cisplatin | 64 | 6.0 | p>0.05 | NR | NR | 20.30 | p=0.63 | NR | NR |
| 5-fluorouracil-epirubicin-cisplatin | 67 | 5.0 | NR | NR | 15.30 | NR | NR | |||
| Janjigian, 202134 | Nivolumab-capecitabine-oxaliplatin or leucovorin-fluorouracil-oxaliplatin | 789 | 13·1 (6·7–19·1) | 0·71 (0·59–0·86) p<0·01 | 7·7 (7·0–9·2) | 0·68 (0·56–0·81) p<0·01 | NR | NR | NR | NR |
| Capecitabine-oxaliplatin or leucovorin-fluorouracil-oxaliplatin | 792 | 11·1 (5·8–16·1) | 6·1 (5·6–6·9) | NR | NR | NR | NR | |||
| Kang, 200935 | Cisplatin-capecitabine | 160 | 10.4 (9.1–11.0) | 0.85, (0.65–1.11) | 5.6 (4.9–7.3) | 0.81, (0.63–1.04) p<0.01 | 46 (38-55) | 1.80 (1.11–2.94) p=0.02 | Mean duration of response:7.6 months | 0.88 (0.56–1.36) p=0.55 |
| Cisplatin-fluorouracil | 156 | 8.9 (7.3–10.2) | 5.0 (4.2–6.3) | 32 (24-41) | Mean duration of response: 6.2 months | |||||
| Ochenduszko, 201536 | Epirubicin-oxaliplatin-capecitabine | 29 | 9.5 | p=0.14 | 6.4 | p=0.44 | NR | NR | NR | NR |
| Docetaxel-cisplatin-5-fluorouracil-leucovorin | 27 | 11.9 | 6.8 | NR | NR | NR | NR | |||
| Petersen, 202137 | Docetaxel-carboplatin-capecitabine | 49 | 9.8 (8.2-11.0) | NR | 6.1 (5.5-7.1) | NR | NR | NR | NR | NR |
| Epirubicin-oxaliplatin-capecitabine | 49 | 10.2 (8.0-11.9) | NR | 5.1 (4.3-7.0) | NR | NR | NR | NR | ||
| Roth, 200738 | Epirubicin-cisplatin-flurouracil | 40 | 8.3 (7.2-13.0) | NR | NR | NR | NR | NR | Time to progression: 4.9 (3.2-6.1) months | NR |
| Docetaxel-cisplatin | 38 | 11 (7.8-12.5) | NR | NR | NR | NR | NR | Time to progression: 3.6 (2.8-4.5) months | ||
| Docetaxel-cisplatin-fluorouracil | 41 | 10.4 (8.3-12.0) | NR | NR | NR | NR | NR | Time to progression: 4.6 (3.5-5.6) months | ||
| Shitara, 202039 | Pembrolizumab | 256 | 10.6 (7.7-13.8) |
0.91 (0.69-1.18) 0.85 (0.70-1.03) |
2.0 (1.5-2.8) |
1.66 (1.37-2.01) 0.84 (0.70-1.02) p=0.04 |
NR | NR | NR | NR |
| Pembrolizumab-cisplatin-capecitabine-fluorouracil | 257 | 12.5 (10.8-13.9) | 6.9 (5.7-7.3) | NR | NR | NR | NR | |||
| Placebo-cisplatin-capecitabine-fluorouracil | 250 | 11.1 (9.2-12.8) | 6.4 (5.7-7.0) | NR | NR | NR | NR | |||
| Shitara, 202240 | Nivolumab- ipilimumab |
409 | 11.2 (9.2-13.4) | 0.89 (0.71-1.10) p=0.23 | 2.8 (2.6-3.6) | 1.66 (1.40-1.95) | NR | NR | Duration of response: 13.8 months (9.4-17.7) | NR |
| Capecitabine-oxaliplatin or leucovorin-fluorouracil-oxaliplatin | 404 | 11.6 (10.1-12.7) | 7.1 (6.9-8.2) | NR | NR | Duration of response: 6.8 months (5.6-7.2) | NR | |||
| Van Cutsem, 200641 | Docetaxel-cisplatin-fluorouracil | 221 | 9.2 (8.4-10.6) | 1.29 (1.0-1.6) p=0.02 | NR | NR | 81 (37) | p=0.01 | Time to progression: 5.6 (4.9-5.9) months | 1.47 (1.19-1.82) |
| Cisplatin-fluorouracil | 224 | 8.6 (7.2-9.5) | NR | NR | 57 (25) | Time to progression: 3.7 (3.4-4.5) months | ||||
| Webb, 199742 | Epirubicin-cisplatin-flurouracil | 111 | 8.9 | NR | NR | NR | 45 (36-54) | p<0.01 | NR | NR |
| Fluorouracil-doxorubicin-methotrexate | 108 | 5.7 | NR | NR | NR | 21 (13-29) | NR | NR | ||
S1 is a novel oral fluoropyrimidine derivative. NR = not reported in the study. CI = confidence interval. HR = hazards ratio. Hazards ratio and p values in bold indicates statistically significant values of p<0.05.
Table 4.
Grade three or four adverse events and outcomes reported in included studies.
| Author, year | Sample size | Treatment arms | Neutropenia, n (%) | Anemia, n (%) | Thrombocytopenia, n (%) | Leukopenia, n (%) | Nausea, n (%) | Vomiting, n (%) | Diarrhea, n (%) | Fatigue, n (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Ajani, 200519 | 76 | Docetaxel-cisplatin-fluorouracil | 65 (87) | 24 (32) | 1 (1) | 49 (65) | 8 (11) | NR | 4 (5) | NR |
| 79 | Docetaxel-cisplatin | 66 (86) | 22 (29) | 9 (12) | 53 (69) | 16 (20) | NR | 16 (20) | NR | |
| Ajani, 201021 | 521 | Cisplatin-S1 | 167 (32) | 107 (21) | 43 (8) | 71 (14) | 39 (8) | 41 (8) | NR | 64 (12) |
| 508 | Cisplatin-fluorouracil | 320 (64) | 105 (21) | 68 (14) | 167 (3) | 49 (10) | 49 (10) | NR | 67 (13) | |
| Al-Batran, 200822 | 112 | Fluorouracil-leucovorin-oxaliplatin | 13 (12) | 3 (3) | 4.5 (4) | 7 (6) | 5 (5) | 3 (3) | 7 (6) | 4 (4) |
| 102 | Fluorouracil-leucovorin-cisplatin | 15 (15) | 7 (7) | 4 (4) | 12 (12) | 9 (9) | 6 (6) | 5 (5) | 7 (7) | |
| Al-Batran, 201323 | 72 | Fluorouracil-leucovorin-oxaliplatin-docetaxel | 38 (53) | 8 (11) | 2 (3) | 21 (29) | 15 (21) | 3 (4) | 6 (8) | 8 (11) |
| 71 | Fluorouracil-leucovorin-oxaliplatin | 9 (13) | 3 (4) | 2 (3) | 4 (6) | 5 (7) | 1 (2) | 1 (2) | 5 (7) | |
| Bouche, 200424 | 45 | Leucovorin–5-flurouracil | (11) | (16) | (2) | NR | (18) | NR | (2) | NR |
| 44 | Leucovorin–5-flurouracil-cisplatin | (61) | (30) | (2) | NR | (23) | NR | (2) | NR | |
| 45 | Leucovorin–5-flurouracil-irinotecan | (40) | (16) | (0) | NR | (9) | NR | (22) | NR | |
| Cascinu, 201125 | 39 | 5-flurouracil-cisplatin-doxorubicin | 6 (15) | 0 (0) | 2 (5) | NR | 1 (3) | NR | 0 (0) | NR |
| 39 | 5-flurouracil-cisplatin-mitomycin-C | 10 (26) | 0 (0) | 8 (21) | NR | 1 (3) | NR | 1 (3) | NR | |
| Catenacci, 201726 | 298 | Rilotumumab-epirubicin- cisplatin-capecitabine | 111 (37) | 97 (33) | NR | NR | 128 (43) | 100 (34) | 61 (20) | 103 (35) |
| 299 | Placebo-epirubicin-cisplatin-capecitabine | 126 (42) | 125 (42) | NR | NR | 153 (51) | 98 (33) | 81 (27) | 100 (33) | |
| Cocconi, 199427 | 85 | Cisplatin-epirubicin-leucovorin-flurouracil | 8 (9) | 1 (1) | 4 | NR | 17 | 10 (37) | 3 (11) | NR |
| 52 | Fluorouracil-doxorubicin-mitomycin | 0 (0) | 1 (2) | 0 | NR | 4 | 2 (8) | 2 (8) | NR | |
| Curran, 200929 | 172 | Irinotecan-fluorouracil | (24.8) | NR | (2) | NR | NR | NR | (22) | NR |
| 165 | Cisplatin-fluorouracil | (51.6) | NR | (12) | NR | NR | NR | (7) | NR | |
| Fuchs, 201930 | 326 | Ramucirumab-fluorouracil-cisplatin | 85 (26) | 39 (12) | 25 (8) | NR | 22 (7) | 21 (7) | 15 (5) | 27 (8) |
| 319 | Placebo-fluorouracil-cisplatin | 85 (27) | 44 (14) | 11 (4) | NR | 26 (8) | 31 (10) | 23 (7) | 25 (9) | |
| Gubanski,201031 | 39 | Irinotecan-5-fluorouracil-leucovorin | NR | NR | NR | NR | (4) | NR | (5) | (9) |
| 39 | Docetaxel-leucovorin | NR | NR | NR | NR | (12) | NR | (2) | (3) | |
| Högner, 202232 | 51 | Pazopanib-5-fluorouracil-oxaliplatin | 12 (24) | 1 (2) | 1 (2) | 3 (6) | 8 (16) | 3 (6) | 1 (2) | 4 (8) |
| 27 | Fluorouracil-leucovorin-oxaliplatin | 1 (4) | 3 (11) | 3 (11) | NR | NR | 2 (7) | 2 (7) | 1 (4) | |
| Icli, 199833 | 64 | Etoposide-epirubicin-cisplatin | NR | NR | NR | NR | (6.3) | NR | (1.6) | NR |
| 67 | 5-fluorouracil-epirubicin-cisplatin | NR | NR | NR | NR | (9) | NR | (1.5) | NR | |
| Janjigian, 202134 | 789 | Nivolumab-capecitabine-oxaliplatin or leucovorin-fluorouracil-oxaliplatin | 31 (4) | 3 (<1) | 4 (1) | NR | 0 (0) | 2 (<1) | 2 (<1) | 0 (0) |
| 792 | Capecitabine-oxaliplatin or leucovorin-fluorouracil-oxaliplatin | 23 (3) | 1 (<1) | 1 (1) | NR | 0 (0) | 0 (0) | 0 (0) | 19 (1) | |
| Kang, 200935 | 160 | Cisplatin-capecitabine | 25 (16) | NR | NR | 4 (3) | 3 (2) | 11 (7) | 8 (5) | 1 (<1) |
| 156 | Cisplatin- fluorouracil | 29 (19) | NR | NR | 6 (4) | 4 (3) | 13 (8) | 7 (5) | 4 (<3) | |
| Ochenduszko, 201536 | 29 | Epirubicin-oxaliplatin-capecitabine | 21 (72) | 2 (7) | 0 (0) | 2 (7) | 1 (4) | 0 (0) | 1 (4) | 2 (7) |
| 26 | Docetaxel-cisplatin-5-fluorouracil-leucovorin | 13 (50) | 2 (7) | 0 (0) | 3 (12) | 10 (29) | 0 (0) | 1 (4) | 1 (4) | |
| Petersen, 202137 | 49 | Docetaxel-carboplatin-capecitabine | 42 (82) | 3 (6) | NR | NR | 0 (0) | NR | 4 (8) | 3 (6) |
| 49 | Epirubicin-oxaliplatin-capecitabine | 42 (82) | 3 (6) | NR | NR | 0 (0) | NR | 4 (8) | 3 (6) | |
| Roth, 200738 | 40 | Epirubicin-cisplatin-flurouracil | (59) | NR | (3) | NR | NR | NR | (6) | NR |
| 38 | Docetaxel-cisplatin | (76) | NR | (0) | NR | NR | NR | (3) | NR | |
| 41 | Docetaxel-cisplatin-flurouracil | (80) | NR | (3) | NR | NR | NR | (15) | NR | |
| Shitara, 202039 | 254 | Pembrolizumab | 0 (0) | NR | 0 (0) | 0 (0) | 1 (0.4) | 0(0) | 1 (1) | 1 (0) |
| 250 | Pembrolizumab-cisplatin-capecitabine-fluorouracil | 63 (25) | NR | 7 (3) | 7 (3) | 19 (8) | 12(5) | 12 (5) | 19 (8) | |
| 244 | Placebo-cisplatin-capecitabine-fluorouracil | 68 (28) | NR | 6 (3) | 10 (4) | 18 (7) | 14(6) | 14 (6) | 14 (6) | |
| Shitara, 202240 | 403 | Nivolumab-ipilimumab | 1 (<1) | 5 (1) | 1 (<1) | 0 (0) | 6 (1) | 4(1) | 11 (3) | 11 (3) |
| 389 | Capecitabine-oxaliplatin or Leucovorin-fluorouracil-oxaliplatin | 44 (11) | 9 (2) | 7 (2) | 9 (2) | 16 (4) | 11(3) | 15 (4) | 8 (2) | |
| Van Cutsem, 200641 | 221 | Docetaxel-cisplatin-fluorouracil | 181 (82) | 40 (18) | 17 (8) | 144 (65) | 32 (14) | NR | 43 (19) | NR |
| 224 | Cisplatin- fluorouracil | 126 (57) | 57 (26) | 30 (13) | 70 (31) | 38 (17) | NR | 18 (8) | NR | |
| Webb, 199742 | 126 | Epirubicin-cisplatin-flurouracil | NR | (8) | (4) | (36) | (17) | NR | (6) | NR |
| 130 | Fluorouracil-doxorubicin-methotrexate | NR | (10) | (8) | (39) | (5) | NR | (7) | NR |
NR = not reported in the study. Row % might not add up to 100% as every patient would not experience an adverse event and some can have multiple adverse events.
Table 5.
Risk of bias summary of all included randomized control trials using the Cochrane Risk of Bias tool.
Table 5.
Risk of bias summary of all included randomized control trials using the Cochrane Risk of Bias tool.
| Author, Year | Randomization | Deviations from intended intervention | Missing outcome data | Measurement of outcome | Selection of reported results | Overall |
|---|---|---|---|---|---|---|
| Ajani, 200519 | Low | Some | Some | Low | Low | Some |
| Ajani, 200720 | Low | Low | Some | Low | Low | Some |
| Ajani, 201021 | Low | Low | Some | Low | Low | Some |
| Al-Batran, 200822 | Some | Some | Low | Low | Low | Some |
| Al-Batran, 201323 | Low | Low | Low | Low | Low | Low |
| Bouche, 200424 | Low | Low | Low | Low | Low | Low |
| Cascinu, 201125 | Low | Low | Low | Low | Low | Low |
| Catenacci, 201726 | Low | Low | Low | Low | Low | Low |
| Cocconi, 199427 | Low | Low | Some | Low | Low | Some |
| Coombes, 199428 | Some | Low | Low | Low | Low | Some |
| Deng, 201329 | Low | Low | Low | Low | Low | Low |
| Fuchs, 201930 | Low | Low | Some | Low | Low | Some |
| Gubanski, 201031 | Low | Low | Low | Low | Low | Low |
| Högner, 202232 | Low | Low | Low | Low | Low | Low |
| Icli, 199833 | Low | Low | Some | Low | Low | Some |
| Janjigian, 202134 | Low | Low | Low | Low | Low | Low |
| Kang, 200935 | Low | Some | Some | Low | Low | Some |
| Ochenduszko, 201536 | Low | Low | Low | Low | Low | Low |
| Petersen, 202137 | Low | Some | Some | Low | Low | Some |
| Roth, 200738 | Some | Some | Low | Low | Low | Some |
| Shitara, 202039 | Low | Low | Low | Low | Low | Low |
| Shitara, 202240 | Low | Low | Low | Low | Low | Low |
| Van Cutsem, 200641 | Low | Low | Some | Low | Low | Some |
| Webb, 199742 | Some | Low | Low | Low | Some | Some |
Low = low risk of bias, Some = some concerns in risk of bias.
Table 6.
PubMed Search Strategy.
| ("Stomach"[Mesh] OR "stomach"[ALL] OR "Gastric"[ALL] OR "Esophagogastric"[ALL] OR "oesophagogastric"[ALL] OR "Gastroesophageal"[ALL] OR "gastrooesophageal"[ALL]) AND ("Neoplasms"[Mesh] OR "Carcinoma"[Mesh] OR "Stomach Neoplasms"[Mesh] OR "Adenocarcinoma"[Mesh] OR "Cancer*"[ALL] OR "Neoplasm*"[ALL] OR "Adenocarcinoma*"[ALL] OR "Carcinoma*"[ALL] OR "Tumor*"[ALL] OR "Neoplasm, Stomach"[ALL] OR "Stomach Neoplasm"[ALL] OR "Neoplasms, Stomach"[ALL] OR "Gastric Neoplasms"[ALL] OR "Gastric Neoplasm"[ALL] OR "Neoplasm, Gastric"[ALL] OR "Neoplasms, Gastric"[ALL] OR "Cancer of Stomach"[ALL] OR "Stomach Cancers"[ALL] OR "Gastric Cancer"[ALL] OR "Cancer, Gastric"[ALL] OR "Cancers, Gastric"[ALL] OR "Gastric Cancers"[ALL] OR "Stomach Cancer"[ALL] OR "Cancer, Stomach"[ALL] OR "Cancers, Stomach"[ALL]) AND ("Neoplasm Metastasis"[Mesh] OR "secondary" [Subheading] OR "Advanced"[ALL] OR "Metastatic"[ALL] OR "Metastasis"[ALL] OR "Recurrent"[ALL] OR "Unresectable"[ALL] OR "Inoperable"[ALL] OR "Incurable"[ALL] OR "Neoplasm metastasis"[ALL] OR "Secondary neoplasm*"[ALL] OR "Secondary cancer*"[ALL] OR "Secondary tumor*"[ALL] OR "Stage III"[ALL] OR "Stage IV"[ALL]) AND (("Controlled Clinical Trial" [Publication Type] OR "Clinical Trials as Topic"[Mesh] OR "Clinical Trial" [Publication Type] OR "Randomized Controlled Trials as Topic"[Mesh] OR "Randomised"[ALL] OR "Randomized"[ALL] OR "Randomly"[ALL] OR "Random"[ALL] OR "Randomized controlled trial*"[ALL] OR "Controlled clinical trial*"[ALL] OR "Trial*"[ALL] OR "Clinical trial*"[ALL] OR "placebo"[ALL])) AND ("Drug Therapy"[Mesh] OR "Antineoplastic Agents"[Mesh] OR "Chemotherapy, Adjuvant"[Mesh] OR "Combined Modality Therapy"[Mesh] OR "Antineoplastic Combined Chemotherapy Protocols"[Mesh] OR "Palliative Care"[Mesh] OR "Antineoplastic Agents"[ALL] OR "Drug therapy"[ALL] OR "Chemotherapy"[ALL] OR "Adjuvant chemotherapy"[ALL] OR "Antineoplastic combined chemotherapy"[ALL] OR "Palliative care"[ALL] OR "First-line therapy"[ALL] OR "first line"[ALL] OR "Supportive care"[ALL] OR "Antineoplastic Combined Chemotherapy Protocols"[ALL] OR "Systemic therapy"[ALL]) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



