
Submitted:
04 July 2023
Posted:
05 July 2023
You are already at the latest version
Abstract
Historically, viral hepatitis is a considerable public health problem in Central Asian countries, which may have worsened after dissolution of the Soviet Union. However, up-to-date seroepidemiological studies are lacking. The aim of the present study was, therefore, to provide current estimates of seroprevalence of viral hepatitis in Kyrgyzstan, one of the economically least developed countries in the region. We conducted a population-based cross-sectional study in 2018 in the capital of Kyrgyzstan, Bishkek (n=1075). Participants, children and adults, were recruited from an outpatient clinic. Data were collected during face-to-face interviews. A blood sample (6 ml) was collected from each participant and tested with ELISA for the presence of serological markers for five viral hepatitides (A, B, C, D and E). Poststratification weighting was performed to obtain nationally representative findings. The overwhelming majority of the study participants were positive for anti-HAV (estimated seroprevalence, 75.3%; 95% confidence interval: 72.5–77.9%). The weighted seroprevalence estimates of HBsAg, anti-HCV and anti-HDV were 2.2% (1.5–3.3%), 3.8% (2.8–5.1%), and 0.40% (0.15–1.01%), respectively. Anti-HEV seropositivity was 3.3% (2.4–4.5%). Of the 33 HBsAg positive participants, five (15%) were anti-HDV positive. Our study confirms that Kyrgyzstan remains a high endemic country for hepatitis virus A and C infections. However, seroprevalences of HBV and HDV were lower than previously reported, and based on these data, the country could potentially be reclassified from high to (lower) intermediate endemicity. The observed anti-HEV seroprevalence resembles the low endemicity pattern characteristic of high-income countries.
Keywords:
endemicity pattern
; hepatitis A
; hepatitis B
; hepatitis C
; hepatitis D
; hepatitis E
; seroprevalence
; general population
; Kyrgyzstan
; post-Soviet country
; WHO European Region
1. Introduction
Viral hepatitis is considered a substantial public health issue in the former Soviet republics of Central Asia [1]. However, there are surprisingly few robust data about its current epidemiology in these countries. Kyrgyzstan, one of the poorest countries in the region, traditionally belongs to high endemic countries for viral hepatitis [2]. During 2000-2008, the most prevalent viral hepatitis in Kyrgyzstan was hepatitis A (HAV): of all reported hepatitides, A was most prevalent (61%), followed by B (17%), C (4.5%) and D (1.7%) [3]. Jacobsen et al. classified Kyrgyzstan as a country with intermediate prevalence of HAV with more than 50% of the population infected with the virus by the age of 15 years [4]. The World Health Organization (WHO) classified Kyrgyzstan as a country with high endemicity regarding HBV, which was confirmed in the last systematic review of global HBV seroprevalence [5]; an estimated 550,000 Kyrgyzsians were positive for HBV, corresponding to a seroprevalence of 10.3% (95% confidence intervals, CI: 8.6–12.4%). Of note, Kyrgyzstan was the only high endemic country (i.e. HBsAg prevalence of ≥8%) out of the 44 countries of the WHO European Region [5]. However, this estimate was based on a single small-scale study from 1992 [6]. More recently, we estimated the HBsAg seroprevalence in a large sample of blood donors from 2013 to 2015 (n=37,165) [7]; the estimate was almost three-times lower than the above-mentioned estimate from 1992 [6] (3.6% [95% CI: 3.4–3.8%] vs. 10.3% [8.6–12.4%]). In addition, there was a decreasing trend in HBV seropositivity during this time period. Regarding HCV, Kyrgyzstan was classified as a high endemic country with a prevalence of > 3.5% [8]. Recently, Boteju et al. estimated the pooled HCV prevalence in the general Kyrgyz population to be 2.0% (95% CI: 1.7–2.4%) [9]. A somewhat higher seroprevalence of 3.1% (95% CI: 3.0–3.3%) was observed among blood donors in the above-mentioned study [7]. Not much is known about hepatitis D and E. Outbreaks of hepatitis E in Kyrgyzstan were reported in the 1990′s [10,11], but there are no data about its seroprevalence either during that time period or later [12]. Thus, there is a clear need for current data on seroprevalences of the currently known viral hepatitides in Kyrgyzstan. The aim of the present study was, thus, to fill this data gap by way of a cross-sectional study in the general Kyrgyz population, including equal proportions of female and male participants and spanning all age groups from 1 through 72 years.
2. Materials and Methods
2.1. Study Design and Data
We conducted a population-based cross-sectional study in the capital of Kyrgyzstan, Bishkek, in the year 2018. Kyrgyzstan is one of the five former Soviet republics located in Central Asia and had 6,256,730 inhabitants at that time. Approximately one sixth of the total population live in Bishkek. The primary health care providers in Bishkek are family medicine centers (FMC), which represent the largest outpatient clinics (formerly known as polyclinics). In total, 19 FMCs are responsible for outpatient health care in Bishkek and adjacent urban areas. Potential study participants were recruited from the FMC no. 11, which covers a population of approx. 30,000 inhabitants in Bishkek. Inhabitants with permanent residence in Bishkek are registered in FMCs. Each FMC possesses a list of registered inhabitants including their addresses and contact information. The study team consisted of one physician and two study nurses. Potential study participants (or parents) were selected randomly and contacted by the study team by phone to participate in the study. The study aimed to recruit 240 children and adolescents (≤18 years) and 760 adults (>18 years). However, the recruitment of children, in particular younger than 10 years, turned out to be difficult. The final sample comprised 207 children and adolescents (≤18 years) and 868 adults.
2.2. Questionnaire
Sociodemographic and medical data were collected during face-to-face interviews. The 49-item questionnaire collected information about sociodemographic data (sex, age, ethnicity, marital status, education level, and place of birth), self-perceived health status, infectious diseases (upper and lower respiratory tract infections, gastrointestinal infections, labial herpes, skin and mucosal infections, and bladder and kidney infections) [13,14], noncommunicable diseases (e.g. diabetes, myocardial infarction, asthma, rheumatoid arthritis, and cancer), contacts with patients with known hepatitis B, C or D infection, medical procedures (e.g. intravenous injections, organ transplantation, transfusion of blood products, operations, and tooth extraction), cosmetic procedures (e.g. tattoo, manicure and pedicure), pharmacotherapy (e.g. antibiotics, corticosteroids), and illicit drug use.
2.3. Laboratory Analysis
A blood sample (6 ml) was drawn from each participant. Enzyme-linked immunoassays (ELISA) were performed using a microplate spectrophotometer (ELx800, BioTek, Winooski, US). The ELISA kits Vektogep A – IgG (Vector-Best, Novosibirsk, Russia) were used to test for the presence of antibodies against HAV (anti-HAV). The kits DS-EIA-HBsAg, EIA-anti-HCV, EIA-anti-HDV, DS-EIA-anti-HEV-G (RPC Diagnostic systems, Nizhny Novgorod, Russia) were used to test for the presence of HBsAg and for antibodies against HCV (anti-HCV; HCV core antigen, NS3Ag, NS4Ag, and NS5-Ag), HDV (anti-HDV), and HEV (anti-HEV), respectively. All positive samples were retested once using the same ELISA assays and the same blood sample. Samples were considered positive if results were positive in both tests. All ELISA kits used in this study are licensed for use by the Ministry of Health in Kyrgyzstan.
2.4. Notification Data
We used publicly available national notification data for viral hepatitis in Kyrgyzstan [15]. In brief, a viral hepatitis surveillance system, which captured acute viral hepatitis, has existed since Soviet times. Notification of chronic viral hepatitis was introduced in 2010. Etiological differentiation was only possible for a small proportion of notified cases.
2.5. Statistical Analysis
Initially we calculated the crude seroprevalence of each viral hepatitis. Since some population subgroups were under- or oversampled, we applied poststratification weights using sex and 10-year age groups to obtain nationally representative seroprevalence estimates. The sex and age distribution of the general Kyrgyz population was obtained from the National Statistical Committee of the Kyrgyz Republic (www.stat.kg). Furthermore, we estimated sex-, age- and ethnicity-adjusted seropositivity using logistic regression analysis. Four separate models were created (HAV, HBV, HCV and HEV). A model for HDV was not created because there were only 6 individuals with positive serology. Analyses were performed with IBM SPSS Statistics for Windows, version 19 (IBM Corporation, Armonk, NY,USA).
3. Results
3.1. Demographic and Health-Related Description of the Study Population
Descriptive characteristics of the study population are presented in Table 1. Briefly, there was a slightly lower proportion of males than females (46% vs. 54%). Around 20% of the participants were children and adolescents. The overwhelming majority of the study population were of Kyrgyz origin (79%), followed by Russians (12%). The proportions of study participants with diabetes, myocardial infarction, and asthma were 1.3%, 0.84% and 0.74%, respectively (Table 1). Every sixth participant reported a poor/fair health status.
3.2. Seroprevalence of Viral Hepatitis
The crude and weighted seroprevalences of the five forms of viral hepatitis are presented in Table 2. The overwhelming majority of the study participants were positive for anti-HAV (84%). The crude prevalences of anti-HCV, anti-HEV and HBsAg were 4.7, 4.4 and 3.1%, respectively. Of the 33 HBsAg seropositive participants, 30 (91%) were anti-HBc positive, indicating acute or chronic infection. Six participants (0.60%) were seropositive for anti-HDV. Of all 33 HBsAg positive participants, five (15%) were also anti-HDV positive. One anti-HDV positive participant was anti-HBc positive but HBsAg negative. The seroprevalence decreased for all viral hepatitides after poststratification weighting (Table 2, sixth column).
3.3. Seroprevalence by Sex, Age and Ethnicity
The seroprevalence increased with advancing age for all viral hepatitides, except HDV (Figure 1 and Table 3). This increase was the highest for HAV, as the risk of seropositivity increased by 8% per additional year of participant’s age. By age 30 years the proportion of HAV seropositives reached almost 90% and increased slightly afterwards (Figure 1).
The six study participants with HDV-seropositive results (4 males, 2 females) were between 33 and 58 years old. In terms of sex-related differences, HCV constituted a notable exception in that the risk of HCV positivity was about two-times higher among males than females, whereas there were no sex-related differences in seroprevalences of the other viral hepatitides (Table 3). Regarding ethnicity, the risk of HAV and HEV seropositivity was more than 4-fold higher in participants of Kyrgyz ethnicity than in Russian participants. In contrast, the risk of HCV seropositivity was two-times higher in Russian than in Kyrgyz participants (Table 3).
3.4. Notification Data
The prevalence of notified acute viral hepatitis showed an increasing trend from 1975 to 1987 reaching the highest value of 1,100 per 100,000 persons in 1987 (Figure 2).
Since 1988 the prevalence has begun to decrease. The hepatitis B prevalence displayed a decreasing trend over the period of 1994 to 2018 (Figure 3a). The decrease was observed in all age groups, including children, adolescents and adults, but was most prominent among 0-to-6-year-old children (Figure 3b).
4. Discussion
This is the first study to examine the seroprevalence of all viral hepatitides in a population-based study involving children and adults in a former Soviet Central Asian country, Kyrgyzstan. Very little is known about the seroepidemiology of viral hepatitides in this country. Our data suggest that the existing evidence is outdated, as the previous classification of endemicity patterns of viral hepatitides was primarily based on studies or reports from the early 1990th. The WHO observed in an assessment of viral hepatitis prevention and control in Kyrgyzstan that regular serological surveys are not conducted for any hepatitides in this country, including chronic hepatitis B and C [2].
Hepatitis A. Regarding HAV, Kyrgyzstan has been previously classified as a country with an intermediate endemicity [4]. The latter was defined as about half of the population infected with the virus by the age of 15 years [4]. Our study confirms this endemicity pattern. Namely, around half of boys under 10 years were anti-HAV positive (and 40% of girls in the same age group). However, the proportion of seropositives increased in the age group of 30-to-39 years old with nearly 90% seropositives. We are not aware of any national policy regarding hepatitis A vaccination.
Hepatitis B. Kyrgyzstan is considered to be a high endemic country for blood-borne viral hepatitis, including hepatitis B virus. Schweitzer et al. found that the only high endemic country with regard to HBsAg from the WHO European Region with a prevalence of about 10% was Kyrgyzstan [5]. Karabaev et al. reported a much lower HBsAg seroprevalence in blood donors (3.6%; 3.4–3.8%) in Kyrgyzstan [7]. The HBsAg seroprevalence with 2.2% (1.5–3.3%) was even lower in the present study. We thus reclassified the country from a high (≥8%) to a lower endemicity country (2–4%). The decreasing prevalence trend has also been confirmed by the notification data and might be the result of several governmental programs to control and prevent HBV transmission, including introduction of a universal hepatitis B vaccination among infants in the early 2000′s in Kyrgyzstan. Since then, HBV vaccination coverage has reached 95% [16]. Of note, our data suggest that the introduction of universal HBV vaccination resulted in a shift of HBV burden to older ages: HBsAg seroprevalence was very low among children and adolescents and increased constantly after age 20 years. A very similar age pattern was observed in the notification data.
Hepatitis C. Botheju et al. conducted a systematic review and meta-analysis of HCV in Central Asia; the HCV prevalence in Kyrgyzstan ranged in different populations including blood donors, pregnant women, army recruits and general population from 0.80% to 5.0%, with a mean HCV seroprevalence of 2.0% (95% CI: 1.7–2.4%) [9]. A somewhat higher seroprevalence of 2.5% (95% CI: 1.6–6.7%) among adults in Kyrgyzstan was reported in another systematic review [17]. Based on these and our results, Kyrgyzstan was classified as a country with a high endemicity. In the present study we observed a nearly two-fold higher seroprevalence of 3.8% (95% CI: 2.8–5.1%). Follow-up assessments should be conducted to test whether this is a continuing trend.
Hepatitis D. Central Asian countries, including Kyrgyzstan belong to countries with high HDV prevalence (20–40% of the HBV population) [18], which is close to the 18% detected in our study.
Hepatitis E. All Central Asian countries are considered to be highly endemic countries with regard to HEV [19]. However, the epidemiologic situation in these countries, including Kyrgyzstan is largely unknown. The WHO systematic review of global HEV prevalence did not find any single seroprevalence study in Azerbaijan, Georgia, and Kazakhstan [12]. Only a few studies were reported in Uzbekistan and Tajikistan. In Kyrgyzstan, HEV outbreaks were reported in the early 1990th, and Luhverchik et al. published a HEV seroprevalence of 4.8% (95% CI: 3.4–6.7%) [20], which agrees well with our estimate of 4.4% (95% CI: 3.3–5.8%). However, our nationally representative estimated prevalence was lower (3.3%). This relatively low HEV seroprevalence is similar to that usually reported from high-income countries, but prospective assessments should be conducted to assure that these values remain stable.
Ethnicity as risk factor for seroprevalence of HAV, HBV and HEV. Hepatitis A and E viruses are predominantly water-borne viral pathogens that are transmitted via the fecal-oral route. Thus, low-income countries with poor hygienic conditions are highly endemic for HAV and HEV [4]. Kyrgyzstan is a lower middle-income country, with about one third of the population living under the poverty line [21]. We observed that Kyrgyz ethnicity was a risk factor for higher seroprevalence of these two viruses, whereas seroprevalence for the blood-borne pathogen HCV was preferentially associated with Russian ethnicity. These results suggest strongly that ethnicity should be considered when devising educational and preventive measures for these pathogens in Kyrgyzstan.
Strengths and Limitations
The main strength of the study is that it provides the first population-based survey of seroprevalence of all viral hepatitides among children and adults in Kyrgyzstan. However, it is limited in that the study population was not nationally representative in terms of selected sociodemographic data, including age and sex distribution. For example, the proportion of children in our study population was undersampled because the envisaged blood draw lowered willingness to participate in this age group. However, we applied post-stratification weighting to correct for demographic differences between the study and the source population and thus obtained nationally representative estimates. Second, the sample size of the study was restricted due to available resources and thus underpowered to precisely detect HDV, which is a very low prevalent form of viral hepatitis. In addition, we were not able to conduct multivariable risk factor analysis of seropositivity.
5. Conclusions
Our data provide the opportunity to reclassify Kyrgyzstan regarding the prevalence of viral hepatitides. Regarding hepatitis A and C, classification as a highly endemic country would now be warranted. Assuming that HBV and HDV seroprevalence is not substantially higher in areas outside the capital Bishkek (our study region), we suggest to reclassify the country from high to low intermediate endemicity of hepatitis B (i.e. seroprevalence 2–4% according to [5]) and to intermediate endemicity of hepatitis D (i.e. proportion of seropositives among HBV, 10–20% [18]). The observed anti-HEV seroprevalence resembles the seroepidemiology of high-income countries (i.e. low endemicity pattern), but it remains to be clarified whether this is due to similar risk factors and modes of transmission.
Author Contributions
MKA designed the study, performed data analyses and wrote the manuscript. NJB, AZN, AAD, ZSN and OTK collected the data, performed laboratory analyses and critically reviewed the manuscript. SJG and KNS participated in laboratory analyses. JP, NK and TI were responsible for biobanking, they critically reviewed the manuscript. FP designed the study and co-wrote the manuscript. All authors read and approved the final version of the manuscript.
Funding
This study was conducted in the context of the project “Kyrgyz-German Hepatitis B Initiative (HepB-KyrG) – Creation of a sustainable binational infrastructure for epidemiological and vaccine research” funded by the German Federal Ministry of Education and Research (BMBF), grant number 01DK17039. The funder had no role in the study design, in the collection, analysis and interpretation of data; in the writing of the manuscript; and in the decision to submit the manuscript for publication.
Institutional Review Board Statement
All studies on humans described in the present manuscript were performed with the approval of the ethics committee of the Ministry of Health in Kyrgyzstan (no. 01-2-118) and in accordance with national law and the Helsinki Declaration (in its current, revised form: 64th WMA General Assembly, Fortaleza, Brazil, October 2013).
Informed Consent Statement
Written informed consent was obtained from all participants of the study (in case of children from parents) before study assessments were begun.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We thank the staff of the outpatient clinic no. 11 in Bishkek, Kyrgyzstan and the Hannover Unified Biobank, Hannover, Germany for their contributions to data collection and processing of biosamples.
Conflicts of Interest
The authors declare that they do not have a conflict of interest related to conduct or publication of this study.
References
- Jefferies, M.; Rauff, B.; Rashid, H.; Lam, T.; Rafiq, S. Update on global epidemiology of viral hepatitis and preventive strategies. World J Clin Cases 2018, 6, 589–599. [Google Scholar] [CrossRef] [PubMed]
- Mozalevskis, A., Harmanci, H., and Bobrik, A. Assessment of the viral hepatitis response in Kyrgyzstan: 11-15 July 2016: mission report. Copenhagen: World Health Organization 2016.
- Toichuev, R.; Leybman, E.; Omorbekova, C.; Rakhimova, G.; Zhumabek Kyzy, B.; Nikolaeva, L. Childhood Hepatitis in Osh Province of Southern Kyrgyzstan. Euroasian J Hepatogastroenterol 2014, 4, 117–118. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, K.H. Globalization and the Changing Epidemiology of Hepatitis A Virus. Cold Spring Harb Perspect Med 2018, 8, a031716. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, A.; Horn, J.; Mikolajczyk, R.T.; Krause, G.; Ott, J.J. Estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. Lancet 2015, 386, 1546–1555. [Google Scholar] [CrossRef] [PubMed]
- Iashina, T.L.; Favorov, M.O.; Shakhgil’dian, I.V.; Firsova, S.N.; Eraliev, A.E.; Zhukova, L.D.; Reznichenko, R.G. [The prevalence of the markers of viral hepatitis B and delta among the population in regions differing in the level of morbidity]. Vopr Virusol 1992, 37, 194–196. [Google Scholar] [PubMed]
- Karabaev, B.B.; Beisheeva, N.J.; Satybaldieva, A.B.; Ismailova, A.D.; Pessler, F.; Akmatov, M.K. Seroprevalence of hepatitis B, hepatitis C, human immunodeficiency virus, Treponema pallidum, and co-infections among blood donors in Kyrgyzstan: a retrospective analysis (2013-2015). Infect Dis Poverty 2017, 6, 45. [Google Scholar] [CrossRef] [PubMed]
- Mohd Hanafiah, K.; Groeger, J.; Flaxman, A.D.; Wiersma, S.T. Global epidemiology of hepatitis C virus infection: new estimates of age-specific antibody to HCV seroprevalence. Hepatology 2013, 57, 1333–1342. [Google Scholar] [CrossRef] [PubMed]
- Botheju, W.S.P.; Zghyer, F.; Mahmud, S.; Terlikbayeva, A.; El-Bassel, N.; Abu-Raddad, L.J. The epidemiology of hepatitis C virus in Central Asia: Systematic review, meta-analyses, and meta-regression analyses. Sci Rep 2019, 9, 2090. [Google Scholar] [CrossRef] [PubMed]
- Karetnyi Iu, V.; Dzhumalieva, D.I.; Usmanov, R.K.; Titova, I.P.; Litvak Ia, I.; Balaian, M.S. [The possible involvement of rodents in the spread of viral hepatitis E]. Zh Mikrobiol Epidemiol Immunobiol 1993, 52–56. [Google Scholar]
- Onishchenko, G.G.; Favorov, M.O.; L'vov, D.K. , L. [The prevalence and etiological structure of viral hepatitis in a climatic-geographic area at high risk for infection] in Russian. Zh Mikrobiol Epidemiol Immunobiol 1992, 11-12, 22–24. [Google Scholar]
- Aggarwal, R; Gandhi, S. The global prevalence of hepatitis E virus infection and susceptibility: a systematic review. World Health Organization 2019.
- Sievers, C.; Akmatov, M.K.; Kreienbrock, L.; Hille, K.; Ahrens, W.; Gunther, K.; Flesch-Janys, D.; Obi, N.; Michels, K.B.; Fricke, J.; et al. Evaluation of a questionnaire to assess selected infectious diseases and their risk factors: findings of a multicenter study. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2014, 57, 1283–1291. [Google Scholar] [CrossRef] [PubMed]
- Castell, S.; Akmatov, M.K.; Obi, N.; Flesh-Janys, D.; Nieters, A.; Kemmling, Y.; Pessler, F.; Krause, G. Test-retest reliability of an infectious disease questionnaire and evaluation of self-assessed vulnerability to infections: findings of Pretest 2 of the German National Cohort. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2014, 57, 1300–1307. [Google Scholar] [CrossRef]
- Kyrgyz Ministry of Health. Monthly bulletin for infectious and parasitis diseases. Department of Disease Prevention and Infectiosu Disease Surveillance. Available online: https://dgsen.kg/category/deyatelnost/upravluenie-profilaktiki-infekcionnY/ezhemesYachnYj-bjuleten-sjesizn. [accessed 5 Feb 2023].
- Schweitzer, A.; Akmatov, M.K.; Krause, G. Hepatitis B vaccination timing: results from demographic health surveys in 47 countries. Bull World Health Organ 2017, 95, 199–209G. [Google Scholar] [CrossRef]
- Maistat, L.; Kravchenko, N.; Reddy, A. Hepatitis C in Eastern Europe and Central Asia: a survey of epidemiology, treatment access and civil society activity in eleven countries. Hepatol Med Policy 2017, 2, 9. [Google Scholar] [CrossRef]
- Wedemeyer, H.; Manns, M.P. Epidemiology, pathogenesis and management of hepatitis D: update and challenges ahead. Nat Rev Gastroenterol Hepatol 2010, 7, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, R.; Krawczynski, K. Hepatitis E: an overview and recent advances in clinical and laboratory research. J Gastroenterol Hepatol 2000, 15, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Lukhverchyk, L.N.; Alatortseva, G.I.; Nesterenko, L.N.; Nurmatov, Z.Sh.; Baiyzbekova, Zh.A.; Kasymov, O.T.; Mikhailov, M.I.; Zverev, V.V. Hepatitis E virus seroprevalence among different age groups of the healthy population in Kyrgyzstan. Epidemiol Vacc Prevent 2016, 15, 39–43. [Google Scholar] [CrossRef]
- The World Bank. The World by Income and Region. Available online: https://datatopics.worldbank.org/world-development-indicators/the-world-by-income-and-region.html. [accessed 5 Feb 2023].
Figure 1.
Seroprevalence of four viral hepatitides, by sex and age groups. Anti-HAV, anti-HCV, anti-HEV, antibodies against HAV, HCV and HEV, respectively; HBsAg, hepatitis B surface antigen. The sex- and age-distribution of anti-HDV positive participants was not presented due to the low number (n=6).
Figure 1.
Seroprevalence of four viral hepatitides, by sex and age groups. Anti-HAV, anti-HCV, anti-HEV, antibodies against HAV, HCV and HEV, respectively; HBsAg, hepatitis B surface antigen. The sex- and age-distribution of anti-HDV positive participants was not presented due to the low number (n=6).
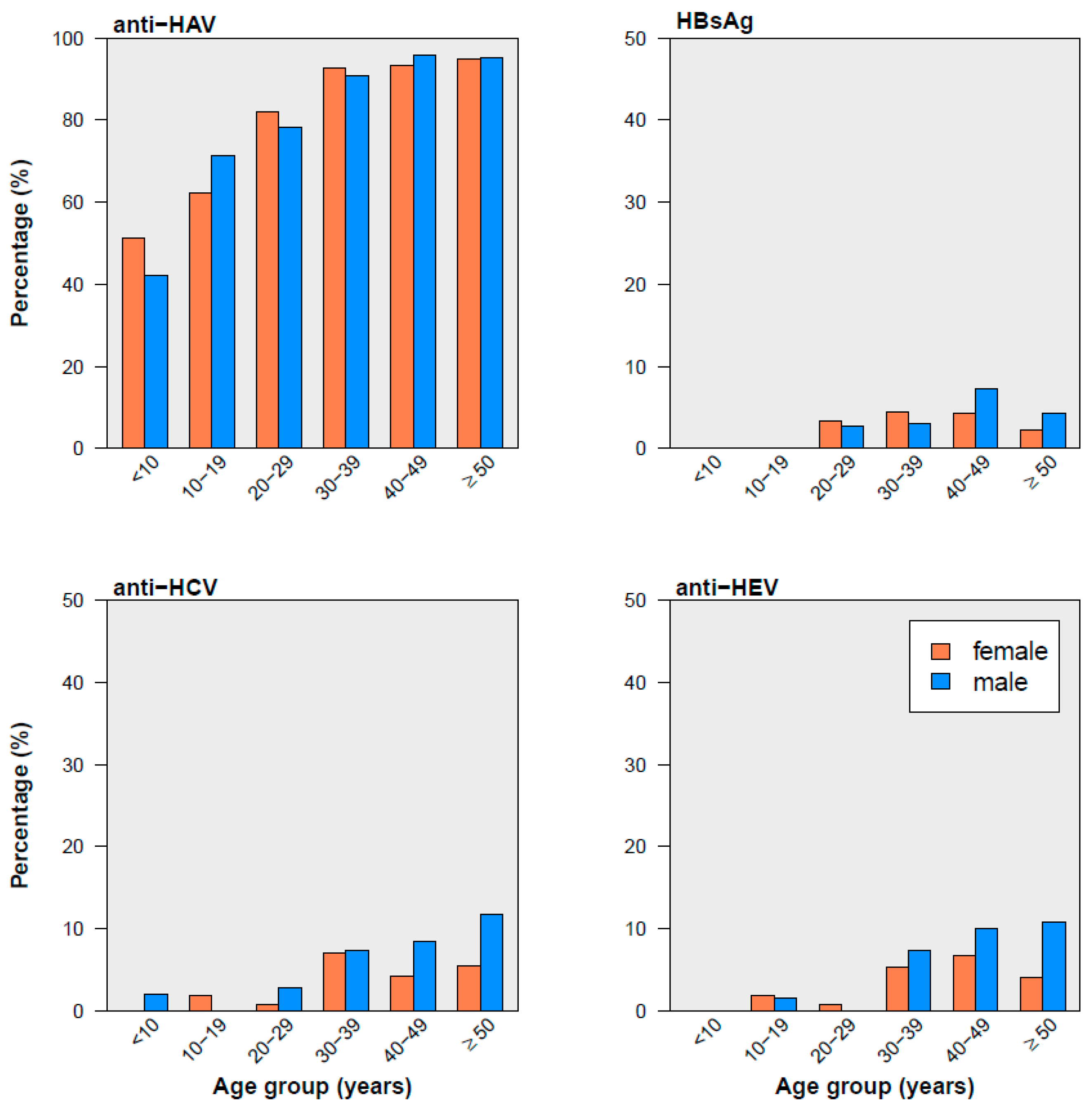
Figure 2.
Prevalence of notified acute viral hepatitis in Kyrgyzstan, 1975–2018. Data source: Kyrgyz Ministry of Health [15]. The trend was fitted with a cubic smoothing spline.
Figure 2.
Prevalence of notified acute viral hepatitis in Kyrgyzstan, 1975–2018. Data source: Kyrgyz Ministry of Health [15]. The trend was fitted with a cubic smoothing spline.
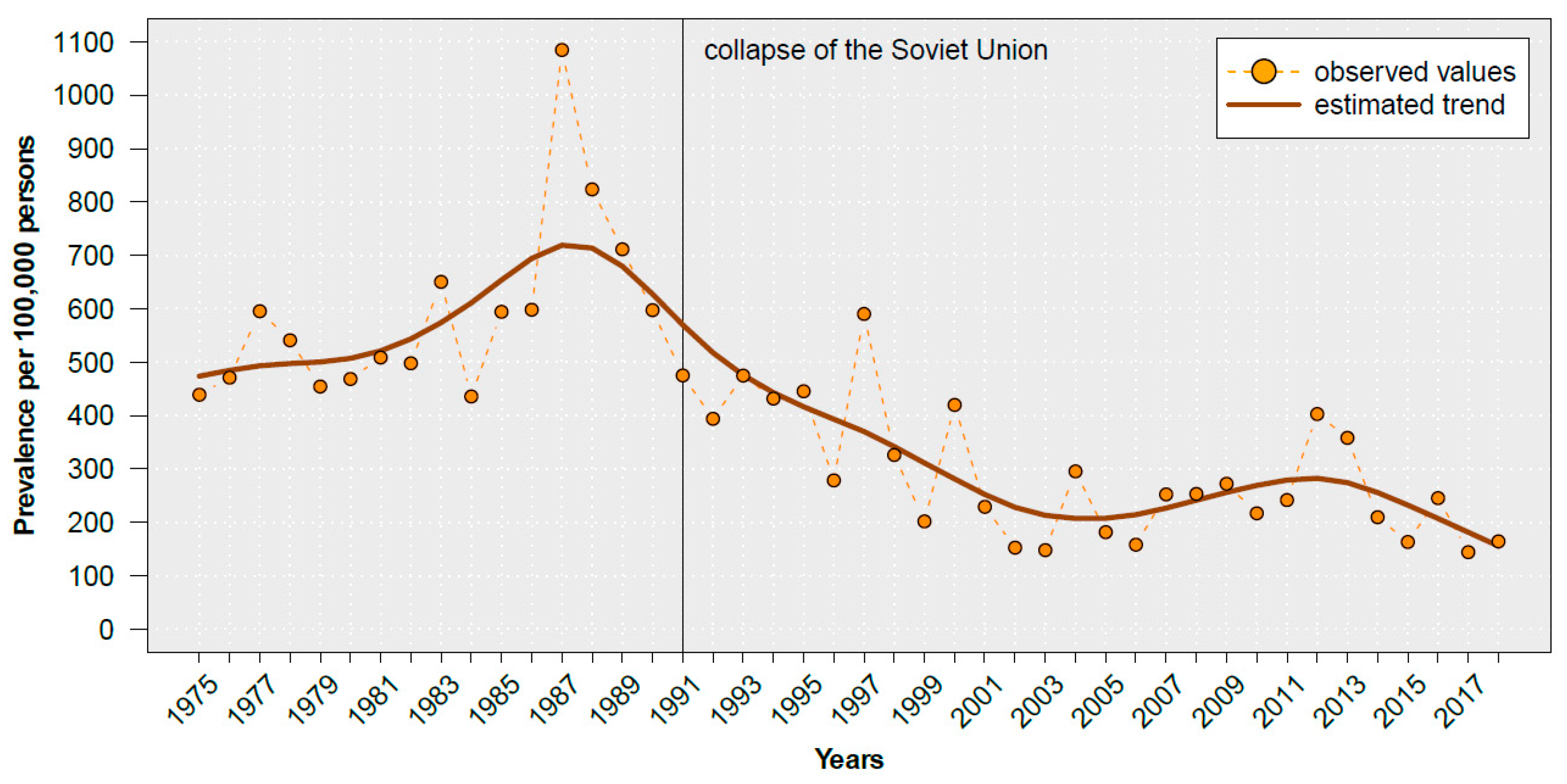
Figure 3.
Prevalence of notified hepatitis B in total (a) and by age group (b) in Kyrgyzstan, 1994–2018. Data source: Kyrgyz Ministry of Health [15]. Upper panel: The trend was fitted with a cubic smoothing spline.
Figure 3.
Prevalence of notified hepatitis B in total (a) and by age group (b) in Kyrgyzstan, 1994–2018. Data source: Kyrgyz Ministry of Health [15]. Upper panel: The trend was fitted with a cubic smoothing spline.
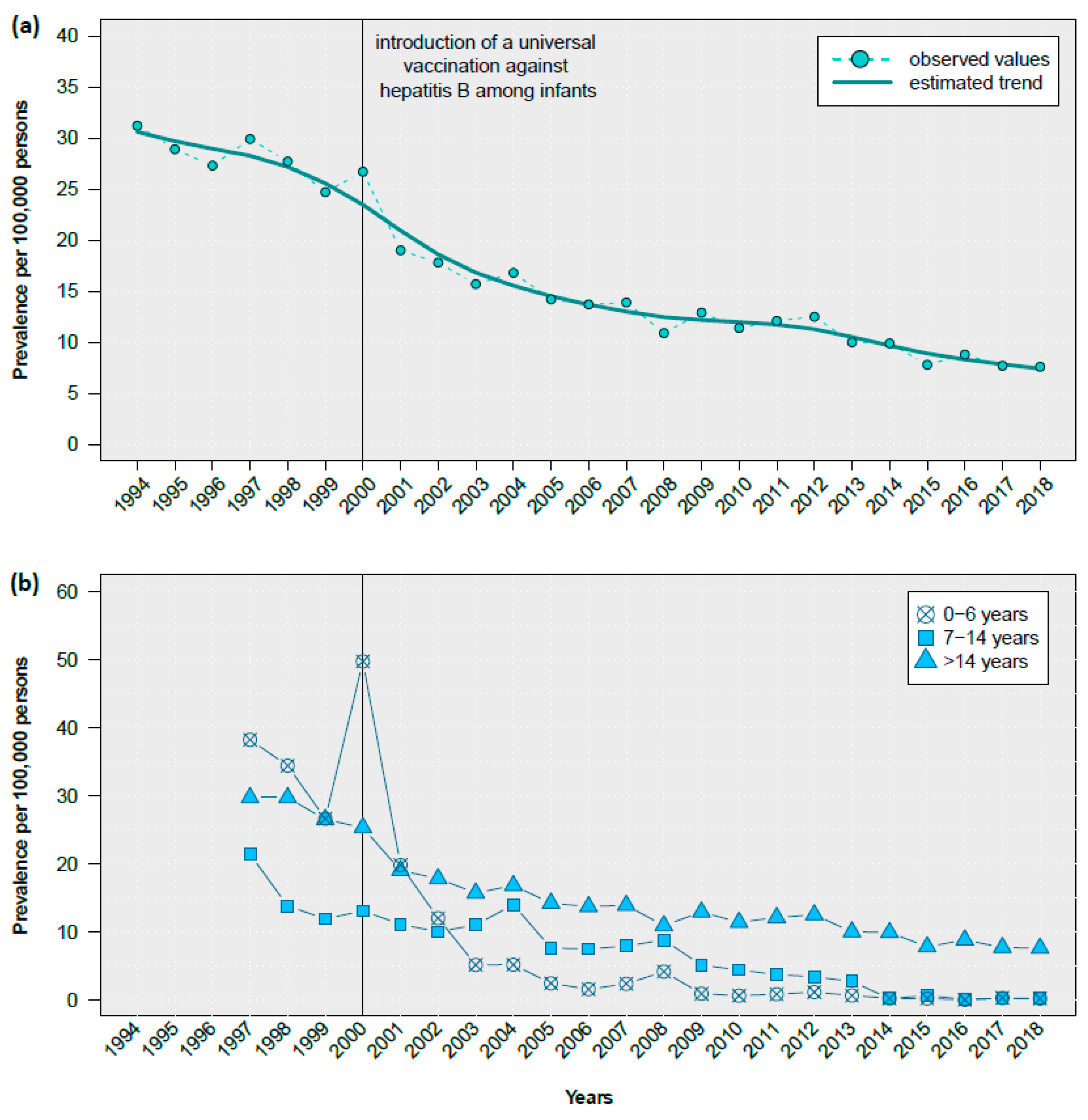

Table 1.
Descriptive and health-related characteristics of the study population, Bishkek, Kyrgyzstan, 2018.
Table 1.
Descriptive and health-related characteristics of the study population, Bishkek, Kyrgyzstan, 2018.
| Characteristics | Study Population N=1,075 |
General Kyrgyz Populationa N=6,256,730 |
||
|---|---|---|---|---|
| Number (n) |
Percent (%) |
Number (n) |
Percent (%) |
|
| Sex | ||||
| male | 495 | 46.0 | 3,101,817 | 49.6 |
| female | 580 | 54.0 | 3,154,913 | 50.4 |
| Age groups | ||||
| <10 years | 92 | 8.6 | 1,464,911 | 23.4 |
| 10-19 years | 123 | 11.4 | 1,051,453 | 16.8 |
| 20–29 years | 230 | 21.4 | 1,129,040 | 18.0 |
| 30-39 years | 209 | 19.4 | 915,167 | 14.6 |
| 40-49 years | 199 | 18.5 | 663,643 | 10.6 |
| ≥50 years | 222 | 20.7 | 1,032,516 | 16.5 |
| Ethnicity | ||||
| Kyrgyz | 850 | 79.1 | 4,587,430 | 73.3 |
| Russian | 128 | 11.9 | 352,960 | 5.6 |
| Uzbek | 16 | 1.5 | 918,262 | 14.7 |
| Kazakh | 14 | 1.3 | 35,541 | 0.6 |
| Ujgur | 11 | 1.0 | 57,002 | 0.9 |
| other | 7 | 0.7 | 305,535 | 4.9 |
| Diabetes mellitusb | ||||
| yes | 14 | 1.3 | NA | NA |
| no | 1045 | 97.2 | NA | NA |
| don’t know | 16 | 1.5 | NA | NA |
| Myocardial infarctionb | ||||
| yes | 9 | 0.8 | NA | NA |
| no | 1057 | 98.3 | NA | NA |
| don’t know | 9 | 0.8 | NA | NA |
| Asthmab | ||||
| yes | 8 | 0.7 | NA | NA |
| no | 1057 | 98.3 | NA | NA |
| don’t know | 10 | 0.9 | NA | NA |
| Cancerb | ||||
| yes | 9 | 0.8 | NA | NA |
| no | 1055 | 98.1 | NA | NA |
| don’t know | 11 | 1.0 | NA | NA |
| Rheumatoid arthritisb | ||||
| yes | 34 | 3.2 | NA | NA |
| no | 1026 | 95.4 | NA | NA |
| don’t know | 15 | 1.4 | NA | NA |
| Self-perceived health statusb | ||||
| poor | 51 | 4.7 | NA | NA |
| fair | 122 | 11.3 | NA | NA |
| good | 45 | 4.2 | NA | NA |
| very good | 674 | 62.7 | NA | NA |
| excellent | 183 | 17.0 | NA | NA |
a The distribution of the general Kyrgyz population by sex and age is obtained from the National Statistical Committee of the Kyrgyz Republic (www.stat.kg); b self-reported; NA, not available.
Table 2.
Crude and weighted seroprevalence of viral hepatitis in a population-based sample, Bishkek, Kyrgyzstan.
Table 2.
Crude and weighted seroprevalence of viral hepatitis in a population-based sample, Bishkek, Kyrgyzstan.
| Hepatitis | Unweighted Total Number of Study Participantsa | Number of Study Participants with Seropositive Resultsa | Crude Proportion of Study Participants with Seropositive Results a | Weighted Total Number of Study Participantsb | Weighted Proportion of Study Participants with Seropositive Results b |
|---|---|---|---|---|---|
| (N) | (n) | (% (95% CI)) | (N) | (% (95% CI)) | |
| HAV | 986 | 824 | 83.6 (81.1–85.8) | 996 | 75.3 (72.5–77.9) |
| HBV | 1074 | 33 | 3.1 (2.2–4.3) | 1073 | 2.2 (1.5–3.3) |
| HCV | 1074 | 51 | 4.7 (3.6–6.2) | 1073 | 3.8 (2.8–5.1) |
| HDV | 1004 | 6 | 0.60 (0.27–1.30) | 1017 | 0.40 (0.15–1.01) |
| HEV | 1065 | 47 | 4.4 (3.3–5.8) | 1062 | 3.3 (2.4–4.5) |
a Unweighted number refers to the number of actually recruited study participants. b Poststratification weights were calculated with respect to sex and age distribution of the general Kyrgyz population to obtain nationally representative estimates. Data were obtained from the National Statistical Committee of the Kyrgyz Republic (www.stat.kg).; CI, confidence interval; HAV, hepatitis A virus; HBV, hepatitis B virus; HCV, hepatitis C virus; HDV, hepatitis D virus; HEV, hepatitis E virus
Table 3.
Sex-, age- and ethnicity-adjusted odds ratios of seropositivity (results of four multivariable logistic regression models)
Table 3.
Sex-, age- and ethnicity-adjusted odds ratios of seropositivity (results of four multivariable logistic regression models)
| Variables | HAV AOR (95% CI) |
HBV AOR (95% CI) |
HCV AOR (95% CI) |
HEV AOR (95% CI) |
|---|---|---|---|---|
| Sex | ||||
| male | reference | reference | reference | reference |
| female | 1.08 (0.74–1.58) | 0.88 (0.44–1.77) | 0.51 (0.29–0.93) | 0.66 (0.36–1.20) |
| Age (change per one year increase) | ||||
| 1.08 (1.06–1.09) | 1.03 (1.00–1.05) | 1.04 (1.02–1.07) | 1.05 (1.03–1.08) | |
| Ethnicity | ||||
| Kyrgyz | reference | reference | reference | reference |
| Russian | 0.21 (0.12–0.35) | 0.43 (0.10–1.84) | 2.39 (1.19–4.80) | 0.22 (0.05–0.96) |
| other | 0.37 (0.21–0.65) | 1.46 (0.50–4.29) | 0.91 (0.27–3.05) | 0.48 (0.11–2.03) |
* Adjusted for all variables in the table; Values in bold indicate statistically significant results (p≤0.05). AOR, adjusted odds ratio; CI, confidence interval; HAV, hepatitis A virus; HBV, hepatitis B virus; HCV, hepatitis C virus; HDV, hepatitis D virus; HEV, hepatitis E virus
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



