
Submitted:
04 July 2023
Posted:
06 July 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Socio-demographic factors are responsible of health inequalities also in vaccination. The aim of this study was to evaluate their role at population level through a population-based study performed on the whole population entitled to receive COVID-19 vaccines in Umbria Region, Italy, and registered to the Regional Healthcare Service as of February 28th, 2021. Socio-demographic characteristics and vaccination status in terms of uptake at least one dose of any available vaccine, completion of the primary vaccination cycle and uptake of the booster doses as of February 28th, 2022 were col-lected from the Umbria regional database. The percentage of eligible population who did not initiate the COVID-19 vaccination, complete the full vaccination cycle and get the booster dose was 11.8%, 1.2% and 21.5% respectively. A younger age, being a not-Italian citizen, and not holding an ex-emption for chronic disease/disability and a GP/FP were associated to all the endpoints. Females, as compared to males, were more likely to not initiate the vaccination but less likely to not receive the booster dose. On the contrary, results on the deprivation index were not conclusive. The findings, beyond confirming current knowledge at population level, provide new inputs for better tailoring vaccination campaigns.
Keywords:
Covid-19
; inequalities
; vaccination
1. Introduction
Health inequalities are the unjust and avoidable differences in people’s health across the population and among specific population groups. The existence of health inequalities means that the right of everyone to the highest attainable standard of health is not being enjoyed equally across the population [1].
COVID-19 seems to have amplified health inequalities. The UK Office for National Statistics published a report about COVID-19 mortality rates according to level of deprivation, that shows a clear social gradient with the more deprived areas having higher mortality [2]. Also, the risk of infection is up to three times greater in very high-deprivation areas compared to very low-deprivation areas. Risks of hospitalization and testing also increase with deprivation, but to a lesser extent [2,3,4].
Social determinants of health, namely “the conditions in which people are born, grow, live, work and age”, are non-medical factors that commonly lead to inequalities in health status and in the use of health services and access to affordable health services [5,6].
In Umbria Region, as well as in the rest of Italy, despite a universal Regional Health Service that aims to provide all with the same health services, socio-economic inequalities in access to health care and services have been reported [7,8].
Among health services, also vaccination might be impacted by social determinants and show access inequalities. The literature reported that factors such as geographic ones (geographic area and following residence and area-level deprivation) and socio-demographic ones (income, social class, marital status, education, foreign citizenship, and sex) can affect vaccination access and uptake [9,10,11,12,13,14].
In Italy, COVID-19 vaccines were offered to health care workers first and to the general population after, following priority criteria based on individual vulnerability. Eventually, as to December 2021, all the adult population who wanted to vaccinate against COVID-19 had the possibility of being fully vaccinated.
A comprehensive COVID-19 vaccination campaign seemed able to reduce socio-economic inequalities, however, several studies investigated the characteristics associated with the willingness to receive the vaccination against COVID-19 showing greater hesitancy in the disadvantaged groups of the population [15,16,17,18].
A recent review demonstrated that in Italy acceptance or hesitancy towards COVID-19 vaccination was influenced by various factors, particularly related to misinformation, perceived efficacy, and safety of vaccines but also social determinants, such as age, citizenship, residence, educational level, occupation and sex [19].
The Italian literature is very concentrated on the issue of hesitancy, but few studies have been done on the real uptake of vaccination at a population-based level [20,21,22,23,24,25,26,27].
The present study aimed to identify potential inequalities associated to COVID-19 vaccination uptake in the overall population of Umbria region through a population-based study.
2. Materials and Methods
2.1. Setting And Study Design
Our study was conducted in the Umbria region of central Italy, which had a population of about 859,000 residents in January 2022 [28]. The Regional Health Service provides comprehensive health care to the resident population. The COVID-19 vaccination campaign in Umbria region started on December 27th 2020, with about 3.3% of the resident population having received a diagnosis of SARS-CoV-2 infection at that date. Healthcare workers and nursing homes residents were the first to get vaccinated, through dedicated vaccination points. Afterward, around mid-February 2021, territorial vaccination points were opened and the vaccination started to be offered to the entire population, according to national priority groups indications [29]. Finally, within one year from the opening of territorial vaccination points, in February 2022, the entire vaccinable population could have received at least one dose of a COVID-19 vaccine and adults could have completed the initial vaccination schedule and obtained a booster dose too. We conducted a cross-sectional population-based study to analyze the socio-demographic factors associated with non-vaccination.
2.2. Study Population
The population included in the study was represented by the resident population registered in the Regional Health Service as at February 28th 2021 (N=866,678). From this population, eligible subjects for vaccination were selected (N=838,043), excluding children under 5 years of age and those who had obtained a certificate of COVID-19 vaccination exemption in the following years, up to February 28th 2022.
In order to avoid a potential bias due to vaccinations administered outside the region with these data possibly not being recorded in the regional registers, we also excluded individuals domiciled outside the region and those whose health insurance card had expired for reasons other than death as of February 28th 2022, for a final number of 827,629 selected individuals (Figure 1).
For the assessment of vaccination status in respect to the doses following the first one, we first selected 820,527 individuals alive as at February 28th 2022; then, subjects eligible for full primary vaccination were selected excluding individuals with no dose received whereas, in respect to the booster dose, all individuals under 12 years of age, for whom the booster dose was not planned as of 28th February 2022, were excluded as well as individuals without full primary vaccination (Figure 1).
2.3. Data Source
Individual-level data were extracted from the DBCOVID Umbria regional database, which integrates information from various regional health administrative sources, including Regional Health Service, patients with exemptions and immunization registries and regional surveillance system for SARS-CoV-2 infections. The data management and analysis were carried out at the Epidemiology Service of the Prevention Department of the Local Health Unit 1 of Umbria Region, which guaranteed its processing in compliance with privacy regulations.
2.4. Study Endpoints And Variables
Non-adherence to COVID-19 vaccination as of February 28th 2022 was considered as primary endpoint, with adherence being defined as the administration of at least one dose of any COVID-19 vaccine.
The failure to complete the full primary vaccination, namely the uptake in various possible combinations of two doses of Pfizer-BioNTech, Moderna or Vaxzevria vaccines, or of a single dose of Johnson&Johnson, or of a single dose of any vaccine within one year of the SARS-CoV-2 infection (previous or subsequent), was considered as secondary endpoint. Failure to get the booster dose in the eligible population was also considered as secondary endpoint. Possible delays in uptake due to SARS-CoV-2 infections were not considered when assessing the outcomes.
As potential factors associated to the primary and secondary endpoints the following variables were considered:
- -
- sex (male or female),
- -
- age (5-11, 12-19, 20-29, 30-39, 40-49, 50-59, 60-69, 70-79, 80-89, 90+),
- -
- citizenship (Italian or non-Italian),
- -
- holding of an officially recognized exemption due to a chronic/rare pathology or a disability, used as a proxy for frailty (present or absent),
- -
- holding of a General Practitioner (GP) or a Family Pediatrician (FP) that is commonly chosen by each resident to get most of the primary care (present or absent);
- -
- the Italian National Deprivation Index at the Umbria regional level, a composite indicator associated to the municipality of residence and categorized in quintiles - from most (group 5) to least (group 1) deprived - weighted by the regional 2011 census population, according to Rosano 2020 [30].
2.5. Statistical Analyses
The study population was first described overall and according to vaccination status and logistic regression models were used to study factors associated with non-adherence to vaccination, failure to complete the full primary vaccination and get the booster dose. Odds ratios (ORs) and associated 95% confidence intervals (95%CIs) were estimated to evaluate the strength of the associations. For the final model, we included all variables significantly related to the endpoints at the univariable analysis. We accounted for the clustering of individuals within municipal level obtaining a robust variance estimate that adjusts for within-cluster correlation. A variance inflation factor (VIF) was calculated for each covariate included in the models, detecting low evidence of collinearity (VIF < 4 for all covariates). Analyses were also stratified by sex. Statistical significance was set at p<0.05. All analyses were performed with the statistical software Stata 14.0 (StataCorp LLC, Texas, USA).
3. Results
As of February 28th 2022, out of 827,629 vaccinable individuals (48.1% males), 11.8% did not uptake COVID-19 vaccination (Table 1). Among those who initially took part to the vaccination campaign (at least one dose of vaccine administered, N=729,630) and did not die within a year (N=722,541), 1.2% (N=8,651) had failed to complete the full primary vaccination and 21.5% (N=150,033) of those eligible for booster dose administration (N=697,766) did not receive it (Table 1).
The percentage of non-adherent subjects was similar in men and women (11.7% vs 12.0%), higher in non-Italians than in Italians (26.1% vs 10.3%) and in those who had not been exempted compared to those who had an exemption for a chronic or rare pathology or for invalidity due to medical causes (14.4% vs 5.7%); moreover the percentage of non-adherent subjects decreased with increasing age, with the lowest values among the age group 80-89 (4.2%), even though the percentage of non-adherent people slightly increased among the over-90s (6.7%). Among those who had not a GP or FP in the last two years, the percentage of non-adherent people reached 47.0%. The percentage of non-adherent people were slightly similar across quintiles of deprivation index.
With regard to the failure to complete the full primary vaccination and get the booster dose, findings were almost similar with a decline of the gap between subjects with and without GP/ FP for the failure to uptake the booster dose.
The logistic model on the non-adherence to vaccination (Table 2) showed that women had a significant 4.2% higher probability to not vaccinate themselves than men. Non-adherence to vaccination was inversely associated with increasing age, even though, taking the 80-89 age group as reference, a trend inversion was observed in over-90s. Non-Italian citizens, as compared to Italians, showed a significant 188% increased likelihood to not uptake vaccination. Subjects with better health conditions had a significant 43.2% higher probability to not vaccinate themselves than subjects with exemptions for pathologies or disability. The factor more strongly associated with non-adherence appeared to be the lack of a GP/FP (OR: 8.91). Sex-disaggregated analysis showed that the association with age was more pronounced among males than among females whereas the one with citizenship was more pronounced in females than in males.
The analysis of the failure to complete the full primary vaccination cycle showed similar results even though associations were less strong as compared to the results on the primary endpoint and disappeared relatively to sex. The same can be concluded for the analysis on the failure to get the booster dose except for sex that did not show any association with the completion of full primary vaccination cycle and issued a protective role of female sex regarding the failure of getting the booster dose. Of note, the role of the presence/absence of GP/FP was significantly scaled down in the analysis of secondary endpoints, i.e., the continuation of the vaccination course (Table 3). Since there was no evidence of an effect modification by sex, we did not report sex-disaggregated results for secondary endpoints.
4. Discussion
This paper provided an overview of COVID-19 vaccination initiation and completion and associated factors on the whole population of Umbria Region.
Overall, the uptake of the first dose was around 90% and primary vaccination cycle completion was very high as only 1.2% of people who initiated the vaccination did not complete it. On the contrary the uptake of the booster dose was slightly below 80%. These data are anyway aligned with nationwide statistics on COVID-19 vaccination coverage in Italy [31].
The analysis of the association between socio-demographic characteristics and the non-adherence to vaccination revealed that females were less likely to initiate vaccination but less likely to fail to get the booster dose. Younger people, non-Italian citizens, those without exemptions for disability/chronic diseases and without a GP/FP were more likely to neither initiate nor complete the vaccination cycle. On the contrary, results about the role of deprivation index were not conclusive even though a reduction in non-adherence to vaccination as well as in the failure to get the full cycle and the booster dose was observed with the increase in deprivation.
The relationship between sex, age and uptake of vaccination can be discussed in the light of current knowledge on the factors influencing vaccine hesitancy. In fact, two systematic reviews on COVID-19 vaccination hesitancy in the Italian population reported a higher hesitancy in females and younger people [19,32]. These results were also confirmed by studies performed outside the Italy and their systematic reviews [33,34]. A systematic review of reviews confirmed these associations [35] and also reported a relationship between hesitancy and social determinants, such as non-white ethnicity, lower education, income level and living conditions. This evidence is important to elaborate on the results on citizenship and deprivation that were issued by our study. In respect to citizenship, the higher probability of being non-adherent that was observed in non-Italian citizens could be due to the presence, among them, of black, Asian and minority ethnic groups that have been already documented to be more hesitant than white people [33,34,35]. Nevertheless, the result can be also justified by other aspects linked to the ease of access to health services. Of note, our study also highlighted that not holding a GP/FP increases the risk of neither initiating nor completing the vaccination. Non-Italian people in Italy can be registered with the National Health Service and receive assistance under the same conditions as Italian citizens, including holding a GP/FP. The small share of people included in our study who did not hold a GP/FP and showed the highest probability to not uptake the vaccination could be represented by a subgroup of population with specific characteristics that need to be better investigated in future research. Our results on holding a GP/FP and its relationship with vaccination uptake might be reasoned by the role of GP/FP as patients' first contact to the healthcare system and in guiding patients’ choices. As a matter of the fact, GP/FP are reported as the most common source that people use to get information on vaccines/vaccination [36]; therefore his/her absence could be responsible for a lack of knowledge that could have impacted on the final choice to get vaccinated.
In respect to deprivation, the Italian index used in this study considered factors that have been already shown to be associated to COVID-19 vaccine hesitancy [35], namely low level of education, unemployment, non-home ownership, one parent family and overcrowding [30]. The role of deprivation has been already investigated in the field of vaccination and the evidence showed that most deprived areas as well as lower socio-economic groups are at higher risk of incomplete/delayed vaccination and generally show lower vaccination coverage [37,38]. Our study missed to show a clear trend in vaccination initiation and completion according to deprivation status but other population-based studies that addressed community characteristics, including deprivation, showed that most deprived areas and most ethnically diverse areas were at higher risk of lower COVID-19 vaccine uptake [39,40]. Finally, in respect to underlying chronic conditions/disability, results of our study were expected in respect to the available literature that already showed the association between the presence of comorbidities and the vaccine uptake [41]. This is also consistent with how the vaccination campaign has been structured, with prioritization and particular attention to frail people.
5. Conclusions
Basing on our results and the available evidence, it can be concluded that socio-demographic characteristics are one of main contributors to vaccine uptake. This conclusion could be helpful to better and further tailoring the vaccination campaigns as socio-demographic data are easily accessible and analyzable on the contrary of other factors that are associated to vaccine hesitancy as well but not promptly available, such as individual and group influences and vaccine and vaccination specific influences. The latter were not investigated in our study, and this represent one of the main limitations. Another limit is linked to the fact that we could not address delay in vaccination completion and receipt of the booster dose due to any reason (adverse events, type of vaccines received, data flow among different informatics system). This was not possible because the study was relied on available regionwide data flow that catch only a part of information. Furthermore, the types of vaccine available in different times and territories or provided to different categories of people could have affected the vaccination completion, due to unequal adverse events and their media resonance. Nevertheless, to the best of our knowledge, this paper is the first population-based study performed in Italy to investigate the role of socio-demographic factors in both the initiation and completion of COVID-19 vaccination that is not based on survey data. Another population-based study relied on regional database was performed only in pregnant women [42]. The reliability of data source, the carefully exclusion of people with potential incomplete or nonsense data (i.e., those domiciliated outside the Umbria region, not registered with the Regional Health Service, and those who died after receiving the first dose) and the choice of a robust outcome, namely the actual uptake of vaccination, made it possible to draw solid conclusions and reinforce and advance the knowledge on this topic in the light of informing future vaccination campaigns.
Author Contributions
Conceptualization, C.P. and C.B.; methodology, C.P. and C.dW.; software, C.B.; validation, M.C., C.dW.; formal analysis, C.P. and C.B.; writing—original draft preparation, C.P., C.B., M.C., I.G., C.dW.; writing—review and editing, C.dW., C.B.; supervision, C.dW., C.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding /The APC was funded by Chiara de Waure.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Whitehead, M. The Concepts and Principles of Equity and Health. Int. J. Heal. Serv. 1992, 22, 429–445. [Google Scholar] [CrossRef] [PubMed]
- Marmot, M.; Allen, J. COVID-19: exposing and amplifying inequalities. J. Epidemiology Community Heal. 2020, 74, 681–682. [Google Scholar] [CrossRef]
- Lewis, N.M.; Friedrichs, M.; Wagstaff, S.; Sage, K.; LaCross, N.; Bui, D.; McCaffrey, K.; Barbeau, B.; George, A.; Rose, C.; et al. Disparities in COVID-19 Incidence, Hospitalizations, and Testing, by Area-Level Deprivation — Utah, March 3–July 9, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1369–1373. [Google Scholar] [CrossRef] [PubMed]
- Lewis, N.M.; Friedrichs, M.; Wagstaff, S.; Sage, K.; LaCross, N.; Bui, D.; McCaffrey, K.; Barbeau, B.; George, A.; Rose, C.; et al. Disparities in COVID-19 Incidence, Hospitalizations, and Testing, by Area-Level Deprivation — Utah, March 3–July 9, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1369–1373. [Google Scholar] [CrossRef] [PubMed]
- Sheiham, A. Closing the gap in a generation: health equity through action on the social determinants of health. A report of the WHO Commission on Social Determinants of Health (CSDH) 2008. Community Dent Heal. 2009, 26. [Google Scholar] [CrossRef]
- Marmot, M.; Allen, J.; Bell, R.; Bloomer, E.; Goldblatt, P. WHO European review of social determinants of health and the health divide. Lancet 2012, 380, 1011–1029. [Google Scholar] [CrossRef]
- Di Napoli, A.; Ventura, M.; Spadea, T.; Rossi, P.G.; Bartolini, L.; Battisti, L.; Cacciani, L.; Caranci, N.; Cernigliaro, A.; De Giorgi, M.; et al. Barriers to Accessing Primary Care and Appropriateness of Healthcare Among Immigrants in Italy. Front. Public Heal. 2022, 10, 817696. [Google Scholar] [CrossRef]
- Chiavarini, M.; Lanari, D.; Minelli, L.; Pieroni, L.; Salmasi, L. Immigrant mothers and access to prenatal care: evidence from a regional population study in Italy. BMJ Open 2016, 6, e008802. [Google Scholar] [CrossRef]
- Bertoncello, C.; Ferro, A.; Fonzo, M.; Zanovello, S.; Napoletano, G.; Russo, F.; Baldo, V.; Cocchio, S. Socioeconomic Determinants in Vaccine Hesitancy and Vaccine Refusal in Italy. Vaccines 2020, 8, 276. [Google Scholar] [CrossRef]
- Helleringer, S.; Abdelwahab, J.; Vandenent, M. Polio Supplementary Immunization Activities and Equity in Access to Vaccination: Evidence From the Demographic and Health Surveys. J. Infect. Dis. 2014, 210, S531–S539. [Google Scholar] [CrossRef]
- Ali, H.A.; Hartner, A.-M.; Echeverria-Londono, S.; Roth, J.; Li, X.; Abbas, K.; Portnoy, A.; Vynnycky, E.; Woodruff, K.; Ferguson, N.M.; et al. Vaccine equity in low and middle income countries: a systematic review and meta-analysis. Int. J. Equity Heal. 2022, 21, 1–30. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Venegas, M.; Cano-Ibáñez, N.; Khan, K. Vaccination coverage among migrants: A systematic review and meta-analysis. Med. de Fam. SEMERGEN 2022, 48, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Spencer, J.C.; Calo, W.A.; Brewer, N.T. Disparities and reverse disparities in HPV vaccination: A systematic review and meta-analysis. Prev. Med. 2019, 123, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; van Hoek, A.; Boccia, D.; Thomas, S.L. Lower vaccine uptake amongst older individuals living alone: A systematic review and meta-analysis of social determinants of vaccine uptake. Vaccine 2017, 35, 2315–2328. [Google Scholar] [CrossRef] [PubMed]
- Shakeel, C.S.; Mujeeb, A.A.; Mirza, M.S.; Chaudhry, B.; Khan, S.J. Global COVID-19 Vaccine Acceptance: A Systematic Review of Associated Social and Behavioral Factors. Vaccines 2022, 10, 110. [Google Scholar] [CrossRef]
- Callaghan, T.; Moghtaderi, A.; Lueck, J.A.; Hotez, P.; Strych, U.; Dor, A.; Fowler, E.F.; Motta, M. Correlates and disparities of intention to vaccinate against COVID-19. Soc. Sci. Med. 2021, 272, 113638–113638. [Google Scholar] [CrossRef]
- Brailovskaia, J.; Schneider, S.; Margraf, J. To vaccinate or not to vaccinate!? Predictors of willingness to receive Covid-19 vaccination in Europe, the U.S., and China. PLOS ONE 2021, 16, e0260230. [Google Scholar] [CrossRef]
- Green, M.S.; Abdullah, R.; Vered, S.; Nitzan, D. A study of ethnic, gender and educational differences in attitudes toward COVID-19 vaccines in Israel – implications for vaccination implementation policies. Isr. J. Heal. Policy Res. 2021, 10, 1–12. [Google Scholar] [CrossRef]
- Primieri, C.; Bietta, C.; Giacchetta, I.; Chiavarini, M.; de Waure, C. Determinants of COVID-19 vaccination acceptance or hesitancy in Italy: an overview of the current evidence. . 2023, 59, 10–25. [Google Scholar] [CrossRef]
- Lastrucci, V.; Lorini, C.; Stacchini, L.; Stancanelli, E.; Guida, A.; Radi, A.; Morittu, C.; Zimmitti, S.; Alderotti, G.; Del Riccio, M.; et al. Determinants of Actual COVID-19 Vaccine Uptake in a Cohort of Essential Workers: An Area-Based Longitudinal Study in the Province of Prato, Italy. Int. J. Environ. Res. Public Heal. 2022, 19, 13216. [Google Scholar] [CrossRef]
- Cetin, I.; Mandalari, M.; Cesari, E.; Borriello, C.R.; Ercolanoni, M.; Preziosi, G. SARS-CoV-2 Vaccine Uptake during Pregnancy in Regione Lombardia, Italy: A Population-Based Study of 122,942 Pregnant Women. Vaccines 2022, 10, 1369. [Google Scholar] [CrossRef] [PubMed]
- Cesaroni, G.; Calandrini, E.; Balducci, M.; Cappai, G.; Di Martino, M.; Sorge, C.; Nicastri, E.; Agabiti, N.; Davoli, M. Educational Inequalities in COVID-19 Vaccination: A Cross-Sectional Study of the Adult Population in the Lazio Region, Italy. Vaccines 2022, 10, 364. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.G.; Tunesi, S.; Consolazio, D.; Decarli, A.; Bergamaschi, W. Evaluation of the anti-COVID-19 vaccination campaign in the Metropolitan Area of Milan (Lombardy Region, Northern Italy). Valutazione della campagna vaccinale anti-COVID-19 nella ATS di Milano. Epidemiol. Prev. 2021, 45, 6. [Google Scholar] [CrossRef]
- Di Noia, V.; Renna, D.; Barberi, V.; Di Civita, M.; Riva, F.; Costantini, G.; Aquila, E.D.; Russillo, M.; Bracco, D.; La Malfa, A.M.; et al. The first report on coronavirus disease 2019 (COVID-19) vaccine refusal by patients with solid cancer in Italy: Early data from a single-institute survey. Eur. J. Cancer 2021, 153, 260–264. [Google Scholar] [CrossRef]
- Di Giuseppe, G.; Pelullo, C.P.; Lanzano, R.; Lombardi, C.; Nese, G.; Pavia, M. COVID-19 Vaccination Uptake and Related Determinants in Detained Subjects in Italy. Vaccines 2022, 10, 673. [Google Scholar] [CrossRef] [PubMed]
- Bruno, F.; Malvaso, A.; Chiesi, F.; Laganà, V.; Servidio, R.; Isella, V.; Ferrarese, C.; Gottardi, F.; Stella, E.; Agosta, F.; et al. COVID-19 vaccine uptake among family caregivers of people with dementia: The role of attitudes toward vaccination, perceived social support and personality traits. Front. Psychol. 2022, 13, 923316. [Google Scholar] [CrossRef]
- PROPORTION of PLWH NOT VACCINATED for COVID-19 in ITALY and PREDICTORS. Tavelli, A.; Cicalini, S.; Barbanotti, D.; Antinori, S.; Segala, D.; Guaraldi, G.; Guastavigna, M.; Lazzaretti, C.; Puoti, M.; Ceccherini-Silberstein, F.; Castagna, A.; Girardi, E.; Monforte, A. D.; Antinori, A.. Topics in Antiviral Medicine ; 30(1 SUPPL):348, 2022. EMBASE |ID: covidwho-1880938. Tavelli, A.
- Umbria in Cifre. Available online: https://webstat.regione.umbria.it/popres_010122/#:~:text=Al%201%20gennaio%202022%20risultano,218.330%20in%20provincia%20di%20Terni.
- Decreto del Ministero della Salute 12 marzo 2021 (GU Serie Generale n.72 del 24-03-2021).
- Rosano A, Pacelli B, Zengarini N, Costa G, Cislaghi C, Caranci N. Aggiornamento e revisione dell’indice di deprivazione italiano 2011 a livello di sezione di censimento. EpidemiolPrev. 2020. Available online: https://epiprev.it/4849.
- Report Vaccini Anti COVID-19. Available online: https://www.governo.it/it/cscovid19/report-vaccini.
- Ferrara, M.; Bertozzi, G.; Volonnino, G.; Di Fazio, A.; Di Fazio, N.; Arcangeli, M.; La Russa, R.; Frati, P. Learning from the Past to Improve the Future—Vaccine Hesitancy Determinants in the Italian Population: A Systematic Review. Vaccines 2023, 11, 630. [Google Scholar] [CrossRef]
- Terry, E.; Cartledge, S.; Damery, S.; Greenfield, S. Factors associated with COVID-19 vaccine intentions during the COVID-19 pandemic; a systematic review and meta-analysis of cross-sectional studies. BMC Public Heal. 2022, 22, 1–16. [Google Scholar] [CrossRef]
- Cascini, F.; Pantovic, A.; Al-Ajlouni, Y.; Failla, G.; Ricciardi, W. Attitudes, acceptance and hesitancy among the general population worldwide to receive the COVID-19 vaccines and their contributing factors: A systematic review. EClinicalMedicine 2021, 40, 101113. [Google Scholar] [CrossRef]
- Kafadar, A.H.; Tekeli, G.G.; Jones, K.A.; Stephan, B.; Dening, T. Determinants for COVID-19 vaccine hesitancy in the general population: a systematic review of reviews. J. Public Heal. 2022, 1–17. [Google Scholar] [CrossRef]
- The European House Ambrosetti, Gli italiani e le vaccinazioni nello scenario post-covid-19, fiducia o scetticismo? Centro Interdipartimentale per l’Etica e l’Integrità della Ricerca. Available online: https://eventi.ambrosetti.eu/wp-content/uploads/sites/221/2021/11/20220614-Paper-Vaccine-Confidence.pdf.
- Vukovic, V.; Lillini, R.; Lupi, S.; Fortunato, F.; Cicconi, M.; Matteo, G.; Arata, L.; Amicizia, D.; Boccalini, S.; Bechini, A.; et al. Identifying people at risk for influenza with low vaccine uptake based on deprivation status: a systematic review. Eur. J. Public Heal. 2020, 30, 132–141. [Google Scholar] [CrossRef]
- Ayorinde, A.; Ghosh, I.; Ali, I.; Zahair, I.; Olarewaju, O.; Singh, M.; Meehan, E.; Anjorin, S.S.; Rotheram, S.; Barr, B.; et al. Health inequalities in infectious diseases: a systematic overview of reviews. BMJ Open 2023, 13, e067429. [Google Scholar] [CrossRef] [PubMed]
- Bucyibaruta, G.; Blangiardo, M.; Konstantinoudis, G. Community-level characteristics of COVID-19 vaccine hesitancy in England: A nationwide cross-sectional study. Eur. J. Epidemiology 2022, 37, 1071–1081. [Google Scholar] [CrossRef]
- Mendolia, S.; Walker, I. COVID-19 vaccination intentions and subsequent uptake: An analysis of the role of marginalisation in society using British longitudinal data. Soc. Sci. Med. 2023, 321, 115779. [Google Scholar] [CrossRef] [PubMed]
- Eiden, A.L.; Barratt, J.; Nyaku, M.K. Drivers of and barriers to routine adult vaccination: A systematic literature review. Hum. Vaccines Immunother. 2022, 18, 2127290. [Google Scholar] [CrossRef]
- Cetin, I.; Mandalari, M.; Cesari, E.; Borriello, C.R.; Ercolanoni, M.; Preziosi, G. SARS-CoV-2 Vaccine Uptake during Pregnancy in Regione Lombardia, Italy: A Population-Based Study of 122,942 Pregnant Women. Vaccines 2022, 10, 1369. [Google Scholar] [CrossRef]
Figure 1.
Study population selection for primary and secondary endpoints.
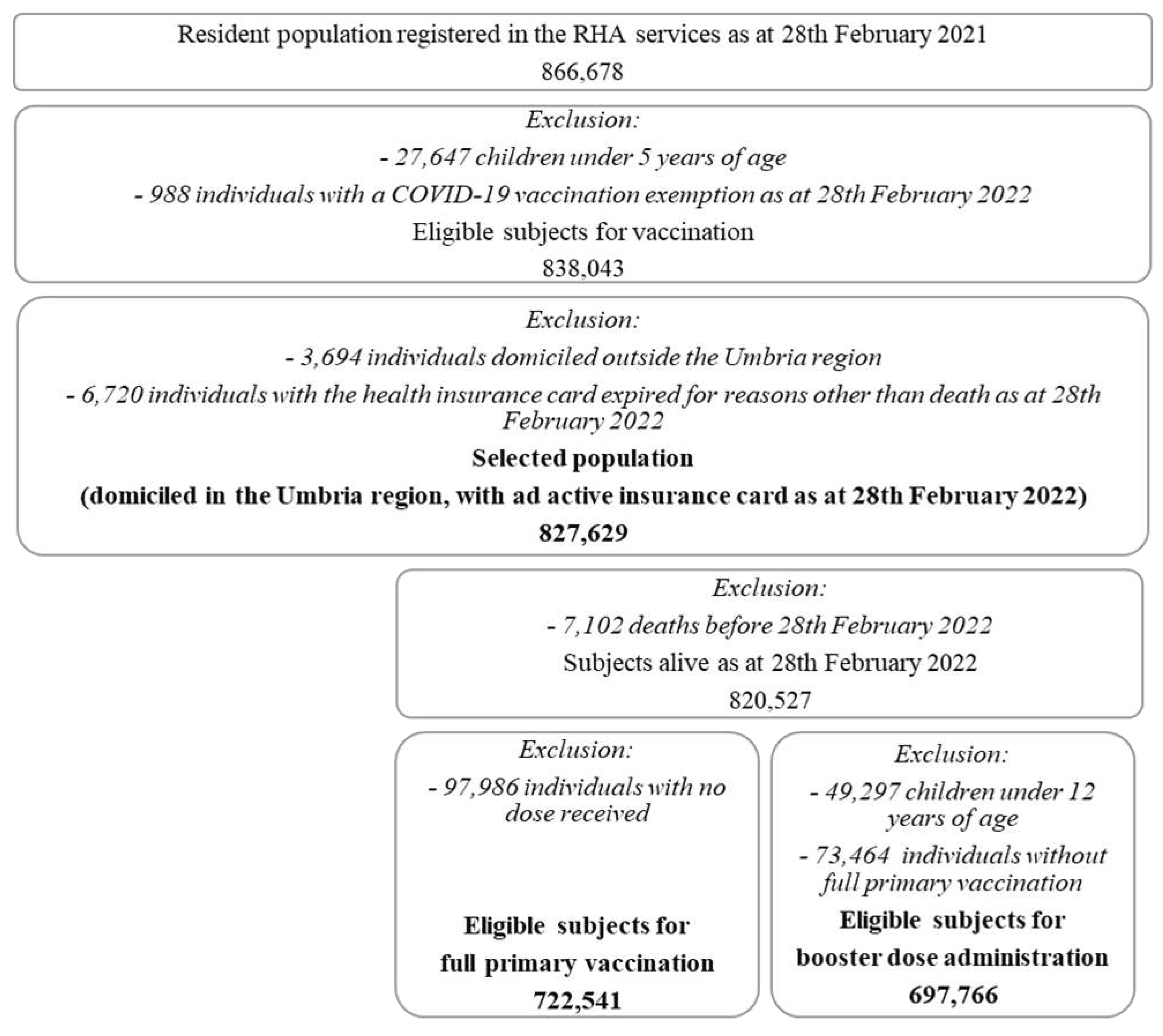

Table 1.
Characteristics of the Umbrian population eligible for vaccination and percentages of primary and secondary endpoints as of February 28th 2022.
Table 1.
Characteristics of the Umbrian population eligible for vaccination and percentages of primary and secondary endpoints as of February 28th 2022.
| Characteristics | Vaccinable | Not adherent to vaccination campaign (any dose) (N=827,629) |
Failed to complete the full primary vaccination (N=722,541) |
Failed to get the booster dose (N=697,766) |
|
|---|---|---|---|---|---|
| N | % | % | % | % | |
| Total | 827,629 | 100.0 | 11.8 | 1.2 | 21.5 |
| Sex | |||||
| Males | 397,820 | 48.1 | 11.7 | 1.21 | 22.3 |
| Females | 429,809 | 51.9 | 12.0 | 1.18 | 20.8 |
| Age | |||||
| Average (SD) | 49.3 (22.9) | 33.7 (24.2) | 32.7 (24.2) | 40.0 (19.4) | |
| 5-11 | 49,297 | 6.0 | 62.3 | 13.4 | - |
| 12-19 | 62,983 | 7.6 | 14.0 | 2.3 | 51.8 |
| 20-29 | 77,340 | 9.3 | 9.6 | 1.3 | 37.1 |
| 30-39 | 89,244 | 10.8 | 11.9 | 1.0 | 31.3 |
| 40-49 | 119,335 | 14.4 | 10.6 | 0.7 | 24.6 |
| 50-59 | 135,107 | 16.3 | 8.4 | 0.9 | 18.2 |
| 60-69 | 113,374 | 13.7 | 7.0 | 0.6 | 11.0 |
| 70-79 | 96,886 | 11.7 | 4.7 | 0.4 | 8.3 |
| 80-89 | 65,991 | 8.0 | 4.2 | 0.5 | 6.6 |
| 90+ | 18,072 | 2.2 | 6.7 | 0.8 | 9.2 |
| Citizenship | |||||
| Italian | 747,528 | 90.3 | 10.3 | 1.1 | 19.8 |
| Non-Italian | 80,101 | 9.7 | 26.1 | 2.8 | 41.4 |
| Comorbidity/Disability* | |||||
| Yes | 242,108 | 29.3 | 5.7 | 0.6 | 12.5 |
| No | 585,521 | 70.7 | 14.4 | 1.5 | 25.8 |
| GP/FP | |||||
| Yes | 818,101 | 98.8 | 11.4 | 1.2 | 21.4 |
| No | 9,528 | 1.2 | 47.0 | 4.3 | 30.6 |
| Deprivation | |||||
| 1 quintile | 167,221 | 20.2 | 12.1 | 1.3 | 21.2 |
| 2 quintile | 160,686 | 19.4 | 11.4 | 1.1 | 20.5 |
| 3 quintile | 185,307 | 22.4 | 12.1 | 1.2 | 22.0 |
| 4 quintile | 155,285 | 18.8 | 10.9 | 1.1 | 21.2 |
| 5 quintile | 159,130 | 19.2 | 12.7 | 1.2 | 22.6 |
* based on officially recognized exemptions due to a chronic/rare pathology or a disability.
Table 2.
Characteristics associated with non-adherence to vaccination campaign (primary endpoint); Umbria Region as of February 28th 2022.
Table 2.
Characteristics associated with non-adherence to vaccination campaign (primary endpoint); Umbria Region as of February 28th 2022.
| Not adherent to the vaccine campaign (any dose) | ||||||
|---|---|---|---|---|---|---|
| All (N=827,629) | Males (N=397,820) | Females (N=429,809) | ||||
| Characteristics | fully-adj. OR | 95% C.I. | fully-adj. OR | 95% C.I. | fully-adj. OR | 95% C.I. |
| Sex | ||||||
| Males | (Reference) | |||||
| Females | 1.042 | 1.030-1.054 | ||||
| Age | ||||||
| 5-11 | 29.571 | 27.015-32.369 | 39.681 | 35.990-43.752 | 24.910 | 22.542-27.527 |
| 12-19 | 2.740 | 2.534-2.962 | 3.757 | 3.420-4.127 | 2.258 | 2.079-2.453 |
| 20-29 | 1.689 | 1.573-1.814 | 2.279 | 2.109-2.463 | 1.416 | 1.294-1.549 |
| 30-39 | 2.034 | 1.926-2.148 | 2.794 | 2.593-3.010 | 1.670 | 1.575-1.771 |
| 40-49 | 1.916 | 1.801-2.038 | 2.736 | 2.527-2.963 | 1.513 | 1.407-1.626 |
| 50-59 | 1.655 | 1.569-1.745 | 2.216 | 2.057-2.388 | 1.390 | 1.310-1.475 |
| 60-69 | 1.510 | 1.436-1.589 | 1.872 | 1.749-2.002 | 1.353 | 1.274-1.437 |
| 70-79 | 1.096 | 1.038-1.158 | 1.247 | 1.156-1.345 | 1.045 | 0.977-1.118 |
| 80-89 | (Reference) | (Reference) | (Reference) | |||
| 90+ | 1.662 | 1.543-1.790 | 1.588 | 1.375-1.834 | 1.585 | 1.465-1.714 |
| Citizenship | ||||||
| Italian | (Reference) | (Reference) | (Reference) | |||
| Non-Italian | 2.878 | 2.678-3.093 | 2.642 | 2.478-2.816 | 3.092 | 2.839-3.368 |
| Comorbidity/Disability* | ||||||
| Yes | (Reference) | (Reference) | ||||
| No | 1.432 | 1.378-1.490 | 1.457 | 1.396-1.520 | 1.406 | 1.349-1.465 |
| GP/FP | ||||||
| Yes | (Reference) | (Reference) | ||||
| No | 8.919 | 7.731-10.289 | 8.565 | 7.324-10.017 | 9.391 | 8.036-10.975 |
| Deprivation | ||||||
| 1 quintile | (Reference) | (Reference) | (Reference) | |||
| 2 quintile | 0.902 | 0.773-1.053 | 0.913 | 0.780-1.067 | 0.893 | 0.764-1.043 |
| 3 quintile | 0.938 | 0.816-1.079 | 0.941 | 0.819-1081 | 0.935 | 0.810-1.079 |
| 4 quintile | 0.791 | 0.719-0.870 | 0.799 | 0.732-0.873 | 0.781 | 0.704-0.867 |
| 5 quintile | 1.021 | 0.873-1.194 | 1.034 | 0.880-2.215 | 1.009 | 0.865-1.177 |
* based on officially recognized exemptions due to a chronic/rare pathology or a disability.
Table 3.
Characteristics associated with failure to complete the full primary vaccination and failure to get the booster dose (secondary endpoints); Umbria Region as of February 28th, 2022.
Table 3.
Characteristics associated with failure to complete the full primary vaccination and failure to get the booster dose (secondary endpoints); Umbria Region as of February 28th, 2022.
| Failure to complete the primary vaccination cycle (N=722,541) |
Failure to get the booster dose (N=697,766) |
|||
|---|---|---|---|---|
| Characteristics | fully-adj. OR | 95% C.I | fully-adj. OR | 95% C.I |
| Sex | ||||
| Males | (Reference) | (Reference) | ||
| Females | 1.030 | 0.987-1.075 | 0.968 | 0.957-0.980 |
| Age | ||||
| 5-11 | 29.414 | 25.239-34.279 | - | - |
| 12-19 | 4.123 | 3.563-4.772 | 12.769 | 12.175-13.392 |
| 20-29 | 2.238 | 1.941-2.581 | 6.883 | 6.367-7.441 |
| 30-39 | 1.597 | 1.334-1.912 | 5.160 | 4.859-5.479 |
| 40-49 | 1.225 | 1.028-1.460 | 3.805 | 3.621-3.998 |
| 50-59 | 1.595 | 1.351-1.882 | 2.733 | 2.600-2.873 |
| 60-69 | 1.145 | 0.964-1.360 | 1.618 | 1.547-1.694 |
| 70-79 | 0.931 | 0.788-1.101 | 1.248 | 1.196-1.302 |
| 80-89 | (Reference) | (Reference) | ||
| 90+ | 1.834 | 1.469-2.290 | 1.474 | 1.384-1.569 |
| Citizenship | ||||
| Italian | (Reference) | (Reference) | ||
| Non Italian | 2.732 | 2.588-2.884 | 2.201 | 2.039-2.375 |
| Comorbidity/Disability* | ||||
| Yes | (Reference) | (Reference) | ||
| No | 1.139 | 1.071-1.211 | 1.227 | 1.208-1.246 |
| GP/FP | ||||
| Yes | (Reference) | (Reference) | ||
| No | 4.771 | 3.968-5.738 | 1.487 | 1.352-1.635 |
| Deprivation | ||||
| 1 quintile | (Reference) | (Reference) | ||
| 2 quintile | 0.840 | 0.747-0.943 | 0.943 | 0.873-1.018 |
| 3 quintile | 0.933 | 0.841-1.035 | 1.016 | 0.940-1.098 |
| 4 quintile | 0.758 | 0.696-0.825 | 0.916 | 0.873-0.961 |
| 5 quintile | 0.912 | 0.825-1.007 | 1.052 | 0.994-1.114 |
* based on officially recognized exemptions due to a chronic/rare pathology or a disability.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



