
Submitted:
07 July 2023
Posted:
07 July 2023
You are already at the latest version
Abstract
Abstract:
Pericyte(s) (Pcs) and resident perivascular macrophages (rPVMΦs) are positioned perfectly in the neurovascular unit (NVU) and perivascular spaces to facilitate metainflammation that results in brain endothelial cell activation and dysfunction and neuroinflammation. Their positions within the NVU allow intimate contact with one another as follows: Brain endothelial cells (BECs) and the Pcs via their shared basement membrane and physical contact peg-socket junctions with N cadherins and gap junctions Cx43; Pcs and rPVMΦs intimate contacts. Additionally, rPVMΦs have intimate contact with the astrocyte endfeet (ACef) that form the outermost membrane of perivascular spaces. Importantly, ACef have intimate contact with BECs that have intimate physical contact with neuronal axons and dendrites to complete NVU coupling. The multiplicity of intimate contacts of NVU cells allow for continuous crosstalk communications to provide brain homeostasis. While each of the cells of the NVU play important roles in the development of enlarged perivascular spaces (EPVS), this review focuses on the Pcs and rPVMΦs and discusses each of the intimate contacts and their functional significance in detail with numerous illustrations and transition electron microscopic images to demonstrate their role in the development of EPVS. EPVS are known to be biomarkers for cerebral small vessel disease and impaired glymphatic system waste clearance. Additionally, EPVS associate with mixed dementias of vascular dementia, vascular contributions to cognitive impairment and dementia, and Alzheimer’s disease that results in high economic and psychosocial cost to the global community.
Keywords:
Astrocytes
; BBB
; Enlarged Perivascular Spaces
; glymphatic system
; microglia
; MRI
; Perivascular Spaces
; Small vessel disease
1. Introduction
Perivascular spaces (Virchow-Robin Spaces) and enlarged perivascular spaces (PVS/EPVS) are fluid filled spaces that ensheath the precapillary arterioles and postcapillary venules [1,2,3,4]. Precapillary arterioles are known to deliver cerebrospinal fluid (CSF), while postcapillary venules are known for their clearance of interstitial fluid (ISF) and metabolic waste (MW) from the interstitial spaces (ISS) via the PVS that serve as a conduit for the glymphatic system (GS) that bathe the parenchymal neurons (Figure 1) [5,6].
PVS are considered enlarged (EPVS) when they are identified by T-2 weighted magnetic resonance images (MRI) that are approximately 2 millimeter and typically measure between 1 and 3 millimeters in diameter [4,7]. EPVS have been recognized as important structural remodeling changes in various neuropathologies and are currently known to a biomarker for cerebral small vessel disease (SVD) and vascular dementia (VaD), which are known to be associated with lacunar stroke in addition to white matter hyperintensities (WMH) [3,7,8,9,10,11,12]. Importantly, EPVS associate with advancing age, hypertension, lacunes, microbleeds, intracerebral hemorrhages, cerebrocardiovascular diseases with transient ischemic episodes and stroke, SVD, cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADISIL), cerebral amyloid angiopathy (CAA), obesity, metabolic syndrome (MetS), type 2 diabetes mellitus (T2DM), WMH, late-onset Alzheimer’s disease (LOAD), sporadic Parkinson’s disease, and non-age-related multiple sclerosis [2,3,4,7,8,9,10,13,14,15,16,17]. Further, our global population is already one of the oldest in history and is only expected to continue to increase [18]. Since it is known that EPVS assoicate with aging it is felt that EPVS will continue to be more prevalent and is expected to grow in the coming years [8,19]. Additionally, EPVS are related to extracranial atherosclersis, cerebromacrovascular, and cerebomicrovascular disease in addition to age-related neurodegenerative diseases such as LOAD and sporadic Parkinson’s disease. EPVS are located primarily in the basal ganglia (BG) and the centrum semiovale (CS0); however, they have also been identified in the hippocampus, midbrain, and the frontal cortex [4,9]. Notably, it has been determined that EPVS in the CSO may have a greater association with amyloid beta pathology [20], and that EPVS of the BG are more indicative of arteriolosclerosis, hypertensive arteriopathy, diabetes mellitus, hyperlipidaemia, prior stroke, lacunes, deep microbleeds, and SVD [21,22,23]. Also, EPVS have been determined to be a marker for an increased risk of cognitive deline and dementia independent of other small vessel disease markers over a a four year period [24]. EPVS are known to exist in at least three major subtypes based on the regions of their occurance as follows: Type I PVS/EPVS are located along lenticulostriate arteries that enter the BG sometimes referred to as État criblé (a collection of multiple radiolucent 1-5 mm of EPVS frequently found in the BG in T-2 weighted MRIs); type II are present along the path of perforating medullary arteries to enter cortical gray matter around high convexities that extend into the white mater and are associated with CSO regions; type III are located in the midbrain and surround the penetrating branches of the collicular and assory collicular arteries [25]. Recently, Paradise et al, have shown that EPVS are a marker for an increased risk of cognitive decline and dementia, independent of other small vessel disease markers [26]. Further, this group has also suggested that EPVS should no longer be thought of as just an incidental finding associated with aging but a biomarker for SVD and cognitive impairment, dementia, and a biomarker of impaired waste clearance in the brain [26]. Multiple mechanisms are thougt to be involved in the development of EPVS, which include the followiing: (1) increased fluid and neurotoxic proteins that entrer the PVS due to BBB dysfunction/disruption due to increased permeability; (2) increased fluid inflow to the PVS due to ACef dysfunction, detachment, separation and aquaporin-4 dysfunction with decreased water uptake allowing the accumulation of water in the PVS; (3) stalling or obstruction of the PVS conduit or impaired glyphatic efflux due to inflammation and the accumulation of excess leukocytes with phagocytosis and accumulation of excessive phagocytic debris, oxidative stress, and activation of increased MMPs, which result in stagnation, stalling, and/or varying degrees of PVS conduit glymphic system obstruction of the waste removal mechanisms; (4) arteriole or venule vascular stiffening and/or spiraling of arterioles that are associated with decreased vascular pulsatility, which results in decreased fluid flow within the PVS contibuting to PVS enlargement; (5) atrophy or loss of surrounding neurons and their axons [2,3,8,9,10,11,15,16,27]. Further, EPVS do not develop all at once but are thought to be associated with a sequence of events and exist as an evolutionary spectrum such that they develop over time to result in SVD, neuroinflammation, impaired cognition and neurodegeneration (Figure 2) [8,28].
Figure 1.
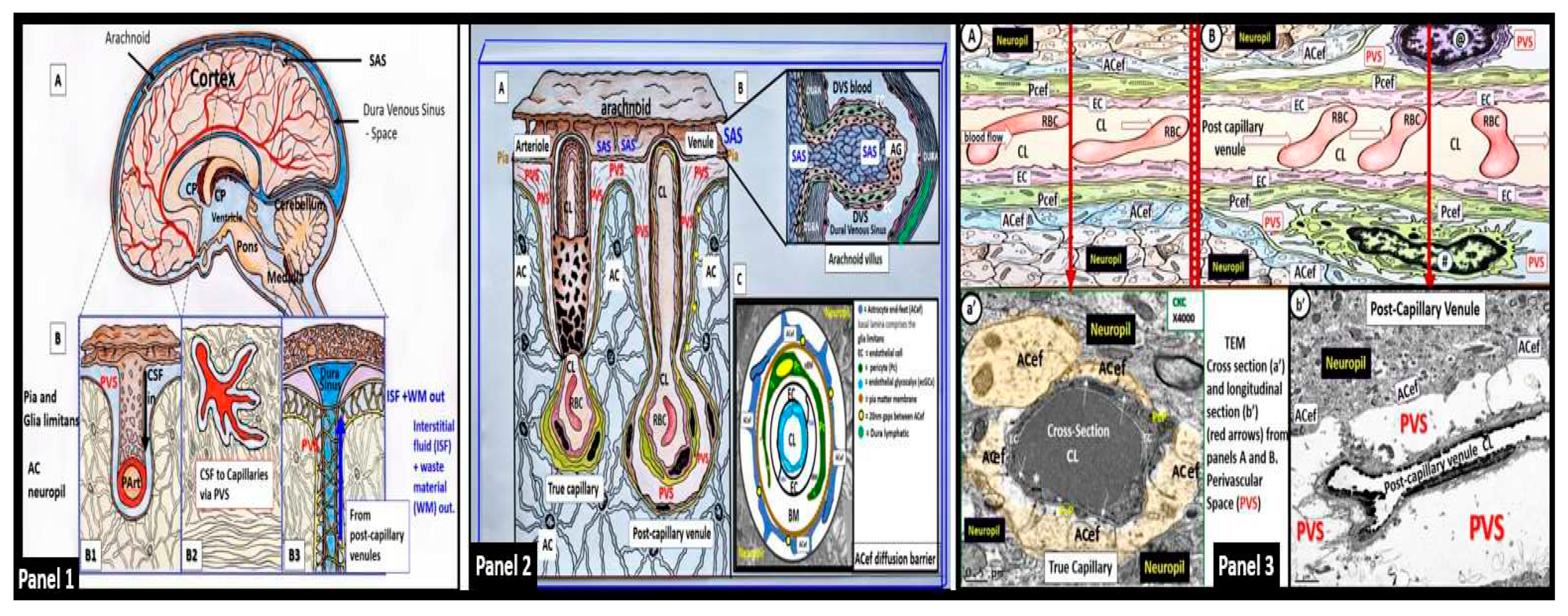
A collage of cerebrospinal fluid (CSF) bathing the brain, precapillary arterioles and postcapillary venules and their perivascular spaces (PVS). Panel 1 illustrates the CSF being delivered from the subarachnoid space (SAS) to the central nervous system (CNS) parenchymal neurons via the perivascular spaces the ensheath the pia arteries and precapillary arterioles to the true capillaries where solutes and fluids are delivered and then the postcapillary venules and veins to carry the interstitial fluid (ISF) and metabolic waste to the SAS and CSF for disposal. Panel 2 depicts this similar finding with greater clarity and further illustrates the arachnoid granules (AG) that drain the metabolic waste to the dural venous sinuse(s) (DVS) to the dural lymphatics and systemic circulation. Notably, the cells that comprise the neurovascular unit are depicted. Panel 3 depicts a longitudinal illustration of the true capillary that transitions to the postcapillary venule with its perivascular space (PVS), which depicts a resident perivascular macrophage (rPVMΦ) (#) in the upper illustration. The lower figures (a’ and b’) depict transmission electron micrograph(s) (TEM) in cross section of the true capillary (a’) and a longitudinal TEM image (b’) depicting a postvenule capillary with its ensheathing PVS. Scale bars = 0.5 μm in a’ and 2μm in b’. Modified images provided by CC 4.0 [8]. AC = astrocyte; @ = lymphocyte; ACef = astrocyte endfeet; BM = basement membrane; CL = capillary lumen; EC = brain endothelial cell; ecGCx = endothelial glycocalyx; Pc = pericyte; Pcef = pericyte endfeet; RBC = red blood cell; WM = waste material;.
Figure 1.
A collage of cerebrospinal fluid (CSF) bathing the brain, precapillary arterioles and postcapillary venules and their perivascular spaces (PVS). Panel 1 illustrates the CSF being delivered from the subarachnoid space (SAS) to the central nervous system (CNS) parenchymal neurons via the perivascular spaces the ensheath the pia arteries and precapillary arterioles to the true capillaries where solutes and fluids are delivered and then the postcapillary venules and veins to carry the interstitial fluid (ISF) and metabolic waste to the SAS and CSF for disposal. Panel 2 depicts this similar finding with greater clarity and further illustrates the arachnoid granules (AG) that drain the metabolic waste to the dural venous sinuse(s) (DVS) to the dural lymphatics and systemic circulation. Notably, the cells that comprise the neurovascular unit are depicted. Panel 3 depicts a longitudinal illustration of the true capillary that transitions to the postcapillary venule with its perivascular space (PVS), which depicts a resident perivascular macrophage (rPVMΦ) (#) in the upper illustration. The lower figures (a’ and b’) depict transmission electron micrograph(s) (TEM) in cross section of the true capillary (a’) and a longitudinal TEM image (b’) depicting a postvenule capillary with its ensheathing PVS. Scale bars = 0.5 μm in a’ and 2μm in b’. Modified images provided by CC 4.0 [8]. AC = astrocyte; @ = lymphocyte; ACef = astrocyte endfeet; BM = basement membrane; CL = capillary lumen; EC = brain endothelial cell; ecGCx = endothelial glycocalyx; Pc = pericyte; Pcef = pericyte endfeet; RBC = red blood cell; WM = waste material;.
Obesiy, MetS, and T2DM are associated with EPVS and may contribute to accelerated brain injury and aging due these findings [8]. Notably, the MetS is known to increase the risk for developing cerebrocardiovascular disease with both macro-and microvascular disease; arteriolosclerosis as well as T2DM [29]. The MetS has multiple risk factors and variables that would contribute to EPVS and it is known that T2DM increases the risk for late-onset Alzheimer’s disease (LOAD) as well as other neurodegenerative diseases including age-related Parkinson’s disease (Figure 3) [29].
Javierre-Petit et al., has recently demonstrated that in addition to cerebral infarcts EPVS burden was associated with diabetes independently of other neuropathologies in a cohort of 654 individuals from a community-based older adults [30]. Capillary rarefaction (CR) in the brain (loss of capillaries) has recently been found to be associated with an increase in obesity, MetS, and T2DM [8,31,32,33]. Recently, Schulyatnikova and Hayden have hypothesized that capillary rarefaction may leave an empty space within the PVS that is subsequently filled with interstitial fluid [8]. This loss of capillaries within the PVS may allow for an increase in total percentage fluid volume within the PVS when the capillary undergoes rarefaction and may contribute to the development of EPVS (Figure 4) [8,34].
CR is known to occur in multiple clinical situations, including: aging, hypertension, obesity, MetS, T2DM, SVD, and LOAD. Also, there are multiple proposed mechanisms that may co-occur to result in CR, including: oxidative – redox stress, inflammation, BECact/dys and loss, Pc dysfunction and loss, impaired angiogenesis (increased ratio of antiangiogenic factors/proangiogenic factors), microvessel ischemia with emboli or hemorrhage, decreased microvessel shear stress, increased microvessel tortuosity, and in some cases increased transforming growth factor beta [34,35]. While this mechanistic hypothesis for possible expansion of PVS due to CR is plausable, more research will be required for it to gain support as a mechanism for increased EPVS.
Pericyte(s) and brain endothelial cell(s) (BECs) are the two mural cells that are essential to form the multicellular neurovascular unit (NVU) consisting of BECs, Pcs, astrocytes and their endfeet (ACef), perivascular microglia cell(s) (PVMGCs) and resident perivascular macrophages (rPVMΦs), and neurons [36]. Pcs extend there elongated pericyte foot processes (Pcfp) that encircle BECs and communicate via physical contact peg sockets and gap junctions connexins. They are uniquely positioned wihtin the NVU and make phyical and intimate connections with BECs, ACef, and resident perivascular macrophages (rPVMΦs) [3,36]. Pcs are multifunctional and known to process signaling, integrate and corrdinate signals from BECs, rPVMΦs, and neurons to complete the NVU and provide for NVU coupling to assist in increasing cerebral blood flow (CBF) in regions of increased neural activity, and signaling [36,37]. Pcs also generate multiple functional responses critical for central nervious system functions in both health and disease. These functions include the regulation and maintenance of the blood brain barrier (BBB), BBB permeability, angiogenesis, NVU capillary hemodynamic responses, and clearance of metabolic waste including neurotoxins, hemodynamic responses including NVU coupling via ACef that connect to neurons and control microvascular cerebral blood flow (CBF) via NVU coupling, and importantly neuroinflammation [37,38]. Notably, Pcs have been thought to act as pleuripotent mesenchymal stem cells and are capable of lifting from the NVU niche and migrating to regions of CNS injury [37]. The unique structural localization of Pcs and their foot processes that are intersperced or sandwiched between the BEC BMs of the NVU and ACef and the PVS and its outemost ACef place them in pivotal position to regulate the inflammatory responses of the CNS in the immediate region of the NVU PVS in addition to the CNS neuronal parenchyma [39,40].
rPVMΦs reside within the PVS and are similar to the CNS microglial cells (MGCs), in that, both are derived from the yolk sack (Figures 1 Panel 3, 5) [41,42].
Figure 5.
Enlarged perivascular space (EPVS) and resident-reactive perivascular macrophage (rPVMΦs) in a postcapillary venule compared to a true capillary. Panel A demonstrates a normal true capillary in a 20-week-old female C57B6/J control model and note how the ACef tightly abut the shared basement membrane of the brain endothelial cell (BEC) and pericyte foot process (PcP). Panel B depicts an EPVS with a prominent rPVMΦ (pseudo-colored red) in a 20-week-old lipopolysaccharide (LPS)-treated CD-1male model and note how the astrocyte endfeet-foot processes (ACfp) are markedly separated from the capillary mural cells (BEC and Pc) (red double arrows). Panel C depicts the rPVMΦs in intimate contact with the Pcfps basal lamina and the rPVMΦ intimate contact with basal lamina of the ACef (outermost boundary of the EPVS abluminal lining) (dashed blue circles). Modified images provided with permission by CC 4.0 [28]. AQP4 = aquaporin 4; Lys = lysosomes; Mt = mitochondria; N = nucleus; NVU = neurovascular unit; V =vacuoles; ves = vesicles.
Figure 5.
Enlarged perivascular space (EPVS) and resident-reactive perivascular macrophage (rPVMΦs) in a postcapillary venule compared to a true capillary. Panel A demonstrates a normal true capillary in a 20-week-old female C57B6/J control model and note how the ACef tightly abut the shared basement membrane of the brain endothelial cell (BEC) and pericyte foot process (PcP). Panel B depicts an EPVS with a prominent rPVMΦ (pseudo-colored red) in a 20-week-old lipopolysaccharide (LPS)-treated CD-1male model and note how the astrocyte endfeet-foot processes (ACfp) are markedly separated from the capillary mural cells (BEC and Pc) (red double arrows). Panel C depicts the rPVMΦs in intimate contact with the Pcfps basal lamina and the rPVMΦ intimate contact with basal lamina of the ACef (outermost boundary of the EPVS abluminal lining) (dashed blue circles). Modified images provided with permission by CC 4.0 [28]. AQP4 = aquaporin 4; Lys = lysosomes; Mt = mitochondria; N = nucleus; NVU = neurovascular unit; V =vacuoles; ves = vesicles.
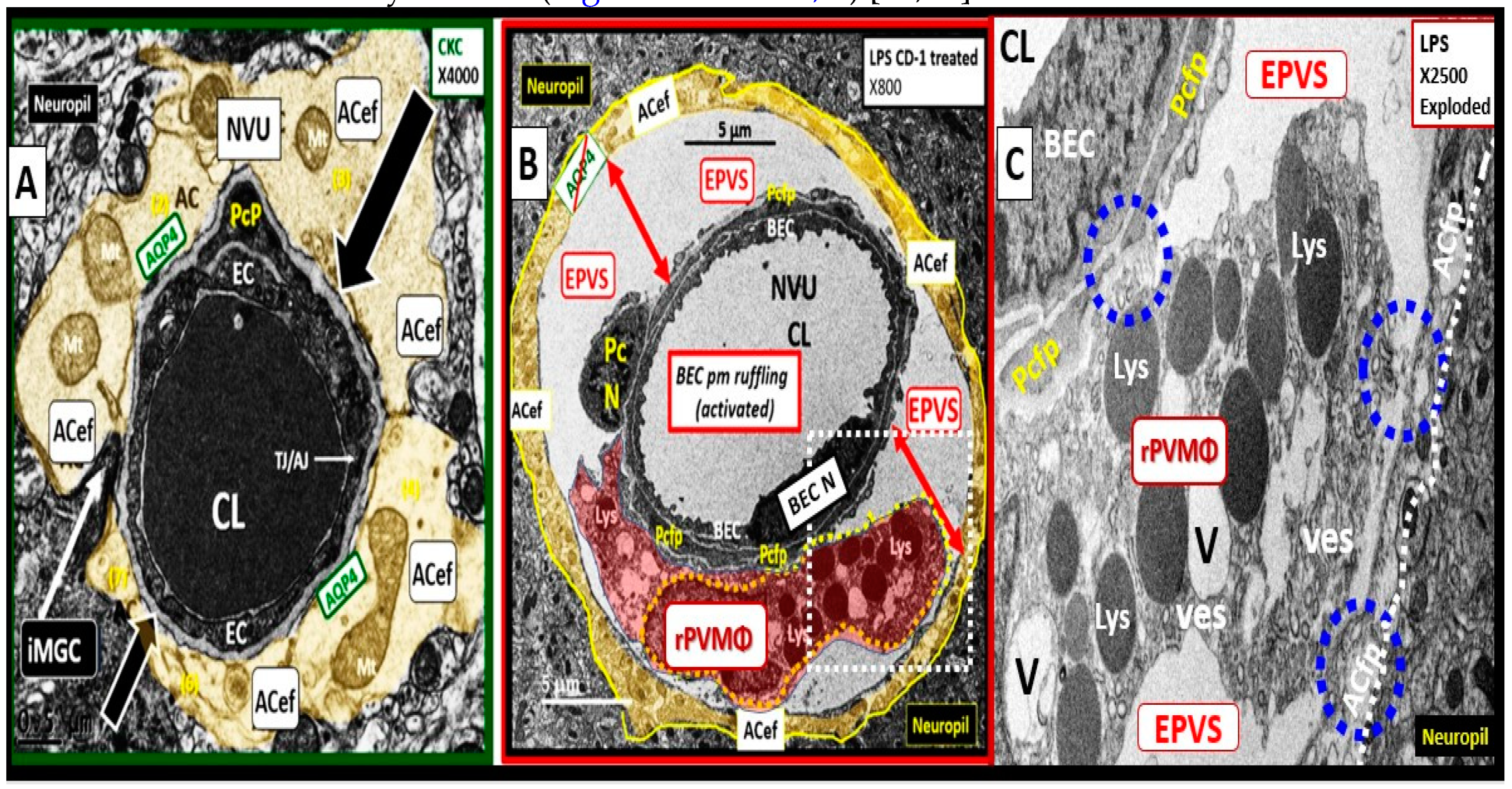
TEM images have consistently shown that rPVMΦs are located within the PVS between the luminal mural cells and the outermost basal lamina of the ACef or glial limitans and the brain parenchyma as depicted in Figure 5B [42,43,44]. As one reviews the literature on rPVMΦ, the term border-associated macrophages (BAMs) is frequently discussed and these BAMs are now thought to be rPVMΦ since they have been shown to reside within the PVS by TEM studies [42,43,44]. rPVMΦs are known to facilitate BBB integrity, promote glymphatic drainage, and exert immune function such as phagocytosis and serve as antigen presenting cells within the PVS to facilitate neuroinflammation once it is initated since they are key components of the PVS and CNS-resident immune system [41].
2. The PVS as an Anatomical Crossroads and Spaces that Provide Multicellular Crosstalk to Facilitate the Development of EPVS
Neurological disorders and diseases are known to have heterogenous pathogenesis, with multiple overlapping contributions of vascular, immune, and neuronal mechanisms of brain injury. PVS/EPVS in the brain represent a crossroad intersection where those mechanisms interact [16], in addition to providing a conduit for the key anatomical component of the glymphatic pathway/system (GS) [5], which plays a crucial role in waste clearance of interstitial fluid that has been shown to be linked to neurodegenerative disease [16]. This neuroinflammation occurs initially in the PVS that has become enlarged (EPVS) due to the obstruction of the PVS/glymphatic system due to the accumulation of cells and cellular debris due to excessive neuroinflammation that occurs within the PVS of precapillary arterioles and postcapillary venules. These PVS provide for the inflammation that occurs due to the extensive crosstalk between BECs that are activated and dysfunctional (BECact/dys) via peripheral metainflammation associated with obesity, MetS, and T2DM. These activated BECs undergo extensive crosstalk with adjacent Pcs that are in direct physical cell-cell contact via peg sockets, gap junction Cx43, and N-Cadherins. In turn, Pcs undergo extensive crosstalk communication with the PVS rPVMΦs, which undergo extensive crosstalk with incoming leukocytes due to chronic metainflammation peripheral inflammatory leukocyte cells that are passed into the PVS to travel throughout the CNS. These incoming leukocytes provide the oxidative stress and phagocytosis that activate MMP 2-9 that are capable of degrading the outer boundary of the perivascular space glia limitans to allow these perivascular leukocytes to enter the CNS interstitial spaces (ISSs) to affect local, regional, and generalized neurons to instigate impaired cognition and neurodegeneration due to CNS neuroinflammation. Thus, the PVS and their subsequent enlargement act as the crossroad for extensive crosstalk communication between activated BECs, Pcs, rPVMΦs, incoming leukocytes, and ACef to allow leukocytes to pass into the interstitium to result in CNS neuroinflammation (Figure 6) [16,45].
Thus, the vascular, neuroimmune, and neuronal systems can develop a pathological interplay, which can create a conducive environment capable of promoting a self-perpetration of brain injury mechanisms across different neurological regions of the CNS and neurological diseases, including those that are primarily thought of as neurodegenerative, neuroinflammatory or cerebrovascular diseases [16].
The PVS/EPVS provide a safe sanctuary space region to harbor the incoming proinflammatory leukocytes due to the NVU BBB disruption with increased permeability due to obesity, MetS, and T2DM as well as other possible clinical diseases. There is plenty of incoming proteinacous waste material being taken up by the PVS. The PVS acts as a conduit space of CNS GS drainage that occurs between the ISF and the contents of postcapillary PVS efflux conduit for human and rodent models CNS metabolic toxic waste removal that is now widely accepted in the literature [5,8,34,46,47]. Thus, the postcapillary venule PVS serves as the anatomical conduit for the GS efflux of metabolic waste [48]. The accumulated leukocytes that reside within the PVS storage santuary will have plenty of opportunity to phagocytose this proteinacous waste debris to eventually result in PVS neuroinflammation with stalling of PVS efflux waste removal of ISF flow even to the point of PVS obstruction with downstream enlargement and EPVS [5,16,25,49,50]. Recently, Mendes et al., were able to show that in obese high-fat-diet fed mice (C57BL6) that this induced proinflammatory rPVMΦs in the hypothalamus helps to explain the HPA axis dysfunction found in obesity, MetS, and T2DM (Figure 3 and Figure 7) [51].
2.1. Reactive Juxtavascular Microglia Cells (rJVMGCs), Neuroinflammation, and Enlarged Perivascular Spaces (EPVS)
When neuroinflammation is discussed, the CNS resident immune microglia cell(s) (MGC) most often comes to mind and is discussed extensively in the literature [52,53,54,55,56]; however, in this narrative review the focus has been primarily on the rPVMΦ that reside within the PVS by TEM studies. This is not only because PVS and EPVS are important [2,8,57] but also because both MGCs and PVMΦs have been rapidly gaining interest over the past decade. For example, PubMed (NIH National Library of Medicine) reference entries regarding MGCs have increased from 68/year in 2008 to 374/year in 2022 an increase 306/year. While PVMΦs publications have increased from 17/year in 1980 to 160/year in 2022 an increase of 143 with an associated citation rate increasing from 46 in 1997 to a citation rate of 12,104 in 2020 [58]. Additionally, Xie et al., revealed that a bibliometric analysis linked brain related diseases with rPVMΦs and aslo pointed to the interest of reactive peripheral macrophages in visceral adipose tissue and vascular diseases in obesity, MetS, and T2DM as current hotspots in research [58]. Notably, CNS rJVMGCs could play a concurrent role along with rPVMΦs in PVS-induced neuroinflammation and enlargement [59]. For example, rJVMGCs are capable of promoting NVU BBB disruption allowing the diapedesis of leukocytes into the PVS [60] and further, neurotoxic insults are capable of inducing both rJVMGCs and reactive astrocytes (rACs) [61,62,63]. Also, rPVMGCs that lie outside of the PVS in the CNS parenchyma are known to be concurrently associated with rACs when peripheral cytokines/chemokines are chronically increased as in metainflammation associated with obesity, MetS, and T2DM [61,62,63]. Additionally, rACs and rPVMGCs would be capable of increasing CNS-derived proinflammatory cytokines/chemokines as well as reactive oxygen, nitrogen, sulfur species to result in an increased activity of the reactive species interactome (RSI), which are known to increase the secretion of matrix metalloproteinases (MMPs-2, 9) and contribute to BBB disruption [64,65]. These MMPs would be capable of contributing to the degradation of the ACef basal lamina (glia limitans) to allow the breaching of the PVS by proinflammatory leukocytes to complete the 2nd step of the 2 step process of CNS neuroinflammation [45,59]. Notably, Zeng et al., recently demonstrated that EPVS severity was associated with the progression of tauopathy in LOAD and that rMGCs neuroinflammation mechanisms mediated this relationship of EPVS and tauopathy [66].
3. Conclusion
EPVS have been previosly noted for decades, but frequently overlooked and were initially thought to be of uncertain pathophysiology [9]. However, EPVS are currently emerging as important aberrent morphological findings in association with multiple clincial diseases and aging. Some have even suggested that it is now uncontested that PVS play critical roles in not only maintaining homeostasis but also priming neuroinflammation as illustrated in Figure 6 [67].
In this narritave review, the first paragraph of the introduction discusses the importance and multiple structural and functional aspects of the PVS/EPVS; the second paragraph discusses the role and the association of obesity, MetS, and T2DM in the development of EPVS; the third paragraph discusses the key role of Pc cells in the development of EPVS; the fourth paragraph discusses the key role that rPVMΦs play in the development of EPVS. Section 2 discusses the importance of the PVS and the EPVS as a regional antomical crossroads and spaces that provide for multicellular crosstalk to facilite the development of EPVS as well as functioning as a repository space for leukocytes that have undergone diapedesis across the NVU BBB due to BECact/dys. Importantly, the key role of the rPVMΦ was explored in more depth as it relates to neuroinflammation and the development of EPVS than in most of the other papers that have been reviewed. As our knowledge regarding the development of EPVS continues to grow and we better understand how they are important in their associated clinical disease states we will undoubtedly continue to make new findings regarding their development and progression. For example, how might we be able to slow or prevent PVS enlargemnt and how might EPVS associate with impaired glymphatic waste removal, impaired cognition, neuroinflammation, and neurodegeneration?
While this narrative review parallels many of the referenced publications regarding PVS/EPVS and their development, the author has utilized multiple TEM images and multiple illustrations in order to aid in the understanding of not only structural remodeling but also the functional changes associated with the development of EPVS. More research in this field is necessary and it is obvious that this field is growing rapidly with many different hot spots being explored along the way, especially in regards to the growing knowledge in the field of the glymphatic pathway-system that is undergoing exponetntial growth.
Abbreviations:
AC, astrocyte; ACef, astrocyte end-feet; AGE/RAGE, advanced glycation end products/receptor for advanced glycation end products; AQP4, aquaporin-4; BBB, blood–brain barrier; BEC(s), brain endothelial cell(s); BECact/dys, brain endothelial cell activation/dysfunction; BG, basal ganglia; BM, basement membrane; CAA = cerebral amyloid angiopathy; CADASIL = cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy; CBF = cerebral blood flow; CCVD, cerebrocardiovascular disease; CBF, cerebral blood flow; Cl, capillary lumen. CNS, central nervous system; CR, capillary refaction; CSF, cerebrospinal fluid; CSO, centrum semiovale; DVS, dural venous sinus; EPVS, enlarged perivascular spaces; GS = glymphatic space; HTN, hypertension; ISF, interstitial fluid;; ISF, interstitial fluid; ISS, interstitial space; late-onset Alzheimer’s disease; LPS, lipopolysaccharide; lpsEVexos, lipopolysaccharide extracellular vesicles; MetS, metabolic syndrome; MGCs, microglia cells; MMPs, matrix metalloproteinases; MRI, magnetic resonance imaging; MW, metabolic waste; NO, nitric oxide; MW = metabolic waste; MRI, magnetic resonance imaging; NVU, neurovascular unit; Pc, pericyte; Pcfp, pericyte foot process; PVS, perivascular spaces; PVS/EPVS, perivascul ar space/enlarged perivascular space; rPVMΦ, resident perivascular macrophages; SAS, subarachnoid space; sLPS, soluble lipopolysaccharide; rPVMΦ, reactive perivascular macrophage; SVD, small vessel disease; T2DM, type 2 diabetes mellitus; TEM, transmission electron microscopy; TIA, transient ischemic attack; WMH, white matter hyperintensities.
Author Contributions
Author is totally responsible for the Conceptualization, Methodology, Software, Validation, Formal Analysis, Investigation, Resources, Data Curation, Writing—Original Draft Preparation, Writing—Review and Editing, Visualization, Supervision, Project Administration, and Funding Acquisition. Author has read and agreed to the published version of the manuscript.
Funding
Author has not received grants from any funding agency in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
The tissues provided for the representative electron microscopic images utilized in this manuscript were all approved in advance by the University of Missouri Institutional Animal Care and Use Committee (No. 190), and animals were cared for in accordance with National Institutes of Health guidelines and by the Institutional Animal Care and Use Committees at the Harry S. Truman Memorial Veterans Hospital and University of Missouri, Columbia, MO, USA, and conformed to the Guide for the Care and Use of Laboratory Animals published by the National Institutes of Health (NIH).
Informed Consent Statement
Not applicable.
Data Availability Statement
Data and materials will be provided upon reasonable request.
Acknowledgments
The author would like to acknowledge Tatyana Shulyatnikova for the contributions of the artistic illustrations and editing of this manuscript. The author would also like to acknowledge DeAna Grant Research Specialist of the Electron Microscopy Core Facility at the NexGen Precision Health Research Center, University of Missouri, Columbia, Missouri. The author also acknowledges the William A. Banks Lab at the VA Medical Center-Seattle, Washington for their kind support.
Conflicts of Interest
Author declares no conflict of interest.
References
- Zhang, E.T.; Inman, B.E.; Weller, R.O. Interrelationships of the pia mater and the perivascular (Virchow-Robin) spaces in the human cerebrum. J. Anat. 1990, 170, 111–123. [Google Scholar]
- Bown, C.W.; Carare, R.O.; Schrag, M.S.; Jefferson, A.L. Physiology and Clinical Relevance of Enlarged Perivascular Spaces. Neurology. 2022, 98, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.; Benveniste, H.; Black, S.E.; Charpak, S.; Dichgans, M.; Joutel, A.; Nedergaard, M.; Smith, K.J.; Zlokovic, B.V.; Wardlaw, J.M. Understanding the role of the perivascular space in cerebral small vessel disease. Cardiovasc. Res. 2018, 114, 1462–1473. [Google Scholar] [CrossRef]
- Wardlaw JM, Smith EE, Biessels GJ, Cordonnier C, Fazekas F, Frayne R, Lindley RI, O’Brien JT, Barkhof F, Benavente OR, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013, 12, 822–838. [Google Scholar] [CrossRef]
- Iliff JJ, Wang M, Liao Y, Plogg BA, Peng W, Gundersen GA, Benveniste H, Vates GE, Deane R, Goldman SA, et al. A Paravascular Pathway Facilitates CSF Flow Through the Brain Parenchyma and the Clearance of Interstitial Solutes, Including Amyloid β. Sci. Transl. Med. 2012, 4, 147ra111. [Google Scholar] [CrossRef]
- Yu, L.; He, X.; Li, H.; Zhao, Y. Perivascular Spaces, Glymphatic System and MR. Front. Neurol. 2022, 13, 844938. [Google Scholar] [CrossRef]
- Francis, F.; Ballerini, L.; Wardlaw, J.M. Perivascular spaces and their associations with risk factors, clinical disorders and neuroimaging features: A systematic review and meta-analysis. Int J Stroke. 2019, 14, 174749301983032. [Google Scholar] [CrossRef]
- Shulyatnikova, T.; Hayden, M.R. Why are Perivascular Spaces Important? Medicina (Kaunas). 2023, 59, 917. [Google Scholar] [CrossRef]
- Doubal FN, Maclullich AMJ, Ferguson KJ, Dennis MS, Wardlaw JM. Enlarged Perivascular Spaces on MRI Are a Feature of Cerebral Small Vessel Disease. Stroke. 2010, 41, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Sweeney MD, Montagne A, Sagare AP, Nation DA, Schneider LS, Chui HC, et al. Vascular dysfunction-The disregarded partner of Alzheimer's Disease. Alzheimer’s Dement. 2019, 15, 158–167. [Google Scholar] [CrossRef]
- Loos, C.M.J.; Klarenbeek, P.; van Oostenbrugge, R.J.; Staals, J. Association between Perivascular Spaces and Progression of White Matter Hyperintensities in Lacunar Stroke Patients. PLoS One. 2015, 10, e0137323. [Google Scholar] [CrossRef]
- Benjamin, P.; Trippier, S.; Lawrence, A.J.; Lambert, C.; Zeestraten, E.; Williams, O.A.; Patel, B.; Morris, R.G.; Barrick, T.R.; MacKinnon, A.D.; Markus, H.S. Lacunar Infarcts, but Not Perivascular Spaces, Are Predictors of Cognitive Decline in Cerebral Small-Vessel Disease. Stroke. 2018, 49, 586–593. [Google Scholar] [CrossRef]
- Arba F, Quinn TJ, Hankey GJ, Lees KR, Wardlaw JM, Ali M, et al. Enlarged perivascular spaces and cognitive impairment after stroke and transient ischemic attack. Int J Stroke. 2016, 13. [Google Scholar]
- Bokura, H.; Kobayashi, S.; Yamaguchi, S. Distinguishing silent lacunar infarction from enlarged Virchow-Robin spaces: a magnetic resonance imaging and pathological study. J Neurol. 1998, 245, 116–122. [Google Scholar] [CrossRef]
- Heier, L.A.; Bauer, C.J.; Schwartz, L.; Zimmerman, R.D.; Morgello, S.; Deck, M.D. Large Virchow-Robin spaces: MR-clinical correlation. Am J Neuroradiol. 1989, 10, 929–936. [Google Scholar] [PubMed]
- Trolli, F.; Cipollini, V.; Moci, M.; Morena, E.; Palotai, M.; Rinaldi, V.; Romano, C. Ristori G, Giubilei F, Salvetti M, Orzi F, Guttmann CRG, Cavallari M. Perivascular Unit: This Must Be the Place. The Anatomical Crossroad Between the Immune Vascular and Nervous System. Front Neuroanat. 2020, 14, 17. [Google Scholar] [CrossRef]
- Zhu, Y.C.; Tzourio, C.; Soumaré, A.; Mazoyer, B.; Dufouil, C.; Chabriat, H. Severity of dilated Virchow-Robin spaces is associated with age, blood pressure, and MRI markers of small vessel disease: a population-based study. 2010, 41, 2483–2490. [Google Scholar] [CrossRef]
- Hayden, M.R. Type 2 Diabetes Mellitus Increases The Risk of Late-Onset Alzheimer's Disease: Ultrastructural Remodeling of the Neurovascular Unit and Diabetic Gliopathy. Brain Sci. 2019, 9, 262. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, J.; Rundek, T.; Ekind, M.S.V.; Sacco, R.L.; Wright, C.B. Perivascular Spaces Are Associated with Atherosclerosis: An Insight from the Northern Manhattan Study. AJNR Am J Neuroradiol. 2013, 34, 1711–1716. [Google Scholar] [CrossRef]
- Charidimou, G.; Boulouis, M.P.; Frosch, J.C.; Baron, M.; Pasi, J.F.; Albucher, B.; et al. The Boston criteria version 2.0 for cerebral amyloid angiopathy: a multicentre, retrospective, MRI–neuropathology diagnostic accuracy study. Lancet Neurol. 2022, 21, 714–725. [Google Scholar] [CrossRef]
- Vilor-Tejedor, N.; Ciampa, I.; Operto, G.; Falcón, C.; Suárez-Calvet, M.; Crous-Bou, M.; et al. Perivascular spaces are associated with tau pathophysiology and synaptic dysfunction in early Alzheimer's continuum. Alzheimers Res Ther. 2021, 13, 135. [Google Scholar] [CrossRef]
- Kapoor, A.; Gaubert, A.; Yew, B.; Jang, J.Y.; Dutt, S.; Li, Y.; et al. Enlarged perivascular spaces and plasma Aβ42/Aβ40 ratio in older adults without dementia. Neurobiol Aging. 2023, 128, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, G.; Kim, H.J.; Fox, Z.; Jäger, H.R.; Wilson, D.; Charidimou, A.; Na, H.K.; Na, D.L.; Seo, S.W.; Werring, D.J. MRI-visible perivascular space location is associated with Alzheimer's disease independently of amyloid burden. Brain. 2017, 140, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Passiak, B.S.; Liu, D.; Kresge, H.A.; Cambronero, F.E.; Pechman, K.R.; Osborn, K.E.; et al. Perivascular spaces contribute to cognition beyond other small vessel disease markers. 2019, 92, e1309–e1321. [Google Scholar] [CrossRef] [PubMed]
- Rudie, J.D.; Rauschecker, A.M.; Nabavizadeh, S.A.; Mohan, S. Neuroimaging of Dilated Perivascular Spaces: From Benign and Pathologic Causes to Mimics. J neuroimaging. 2018, 28, 139–149. [Google Scholar] [CrossRef]
- Paradise, M.; Crawford, J.D.; Lam, B.C.P.; Wen, W.; Kochan, N.A.; Makkar, S.; Dawes, L.; Trollor, J.; Draper, B.; Brodaty, H.; Sachdev, P.S. Association of Dilated Perivascular Spaces With Cognitive Decline and Incident Dementia. Neurology. 2021, 96, e1501–e1511. [Google Scholar] [CrossRef] [PubMed]
- Okar, S.V.; Hu, F.; Shinohara, R.T.; Beck, E.S.; Reich, D.S.; Ineichen, B.V. The etiology and evolution of magnetic resonance imaging-visible perivascular spaces: Systematic review and meta-analysis. Front in Neuroscience. 2023, 17, 1038011. [Google Scholar] [CrossRef]
- Hayden, M.R. Brain Endothelial Cells Play a Central Role in the Development of Enlarged Perivascular Spaces in the Metabolic Syndrome. Medicina (Kaunas). 2023, 59, 1124. [Google Scholar] [CrossRef]
- Hayden, M.R. Overview and New Insights into the Metabolic Syndrome: Risk Factors and Emerging Variables in the Development of Type 2 Diabetes and Cerebrocardiovascular Disease. Medicina (Kaunas). 2023, 59, 561. [Google Scholar] [CrossRef] [PubMed]
- Javierre-Petit, C.; Schneider, J.A.; Kapasi, A.; Makkinejad, N.; Tamhane, A.A.; Leurgans, S.E.; Mehta, R.I.; Banes, L.L.; Bennett, D.A.; Arfanakis, K. Neuropathologic and Cognitive Correlates of Enlarged Perivascular Spaces in a Community-Based Cohort of Older Adults. Stroke. 2020, 51, 2825–2833. [Google Scholar] [CrossRef]
- Tucsek, Z.; Toth, P.; Tarantini, S.; Sosnowska, D.; Gautam, T.; Warrington, J.P.; Giles, C.B.; Wren, J.D.; Koller, A.; Ballabh, P.; et al. Aging exacerbates obesity-induced cerebromicrovascular rarefaction neurovascular uncoupling cognitive decline in mice, J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 1339–1352. [Google Scholar] [CrossRef]
- Paavonsalo S, Lackman MH, KaramanS. Capillary Rarefaction in Obesity and Metabolic Diseases—Organ Specificity and Possible Mechanisms. Cells. 2020, 9, 2683. [Google Scholar] [CrossRef] [PubMed]
- Chantler, P.D.; Shrader, C.D.; Tabone, L.E.; d’Audiffret, A.C.; Huseynova, K.; Brooks, S.D.; Branyan, K.W.; Grogg, K.A.; Frisbee, J.C. Cerebral Cortical Microvascular Rarefaction in Metabolic Syndrome is Dependent on Insulin Resistance and Loss of Nitric Oxide Bioavailability. Microcirculation 2015, 22, 435–445. [Google Scholar] [CrossRef]
- Hayden, M.R. Brain Injury: Response to Injury Wound Healing Mechanisms and Enlarged Perivascular Spaces in Obesity, Metabolic Syndrome, and Type 2 Diabetes Mellitus. Preprints.org. 2023, 2023061202. [Google Scholar] [CrossRef]
- van Dinther, M.; Voorter, P.H.M.; Jansen, J.F.A.; Jones, E.A.V.; van Oostenbrugge, R.J.; Staals, J.; Backes, W.H. Assessment of microvascular rarefaction in human brain disorders using physiological magnetic resonance imaging. J Cereb Blood Flow Metab. 2022, 42, 718–737. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, M.D.; Ayyadurai, S.; Zlokovic, B.V. Pericytes of the neurovascular unit: Key functions and signaling pathways. Nat Neurosci. 2016, 19, 771–783. [Google Scholar] [CrossRef] [PubMed]
- Dore-Duffy P, Andre Katychev A, Xueqian Wang X, Van Buren E. CNS microvascular pericytes exhibit multipotential stem cell activity. J Cereb Blood Flow Metab. 2006, 26, 613–624. [Google Scholar] [CrossRef]
- Zheng L, Guo Y, Zhai X, Zhang YChen W, Zhu Z, Xuan W, Li P. CNS Perivascular macrophages in the CNS: From health to neurovascular diseases. Neurosci Ther. 2022, 28, 1908–1920. [Google Scholar] [CrossRef]
- Rustenhoven, J.; Jansson, D.; Smyth, L.C.; Dragunow, M. Brain Pericytes As Mediators of Neuroinflammation. Trends Pharmocol Sci. 2017, 38, 291–304. [Google Scholar] [CrossRef]
- Jansson, D.; Rustenhoven, J.; Feng, S.; Hurley, D.; Oldfield, R.L.; Bergin, P.S.; Mee, E.W.; Faull, R.L.M.; Dragunow, M. A role for human brain pericytes in neuroinflammation. J Neuroinflammation. 2014, 11, 104. [Google Scholar] [CrossRef]
- Yang, T.; Guo, R.; Zhang, F. Brain perivascular macrophages: Recent advances and implications in health and diseases. CNS Neurosci Ther. 2019, 25, 1318–1328. [Google Scholar] [CrossRef]
- Lapenna, A.; De Palma, M.; Lewis, C.E. Perivascular macrophages in health and disease. Nat Rev Immunol. 2018, 18, 689–702. [Google Scholar] [CrossRef] [PubMed]
- Mato, M.; Ookawara, S.; Kurihara, K. Uptake of exogenous substances and marked infoldings of the fluorescent granular pericyte in cerebral fine vessels. Am J Anat. 1980, 157, 329–332. [Google Scholar] [CrossRef]
- Faraco, G.; Sugiyama, Y.; Lane, D.; Garcia-Bonilla, L.; Chang, H.; Santisteban, M.M.; et al. Perivascular macrophages mediate the neurovascular and cognitive dysfunction associated with hypertension. J Clin Invest. 2016, 126, 4674–4689. [Google Scholar] [CrossRef] [PubMed]
- Owens, T.; Bechmann, I.; Engelhardt, B. Perivascular Spaces and the Two Steps to Neuroinflammation. J. Neuropathol. Exp. Neurology. 2008, 67, 1113–1121. [Google Scholar] [CrossRef]
- Yu, L.; Hu, X.; Li, H.; Zhao, Y. Perivascular Spaces, Glymphatic System and MR. Front Neurol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Nedergarrd, M. Garbage truck of the brain. Science 2013, 340, 1529–1530. [Google Scholar] [CrossRef] [PubMed]
- Hablitz, L.M.; Nedergaard, M. The Glymphatic System: A Novel Component of Fundamental Neurobiology. J Neurosci. 2021, 41, 7698–7711. [Google Scholar] [CrossRef]
- Rennels, M.L.; Gregory, T.F.; Blaumanis, O.R.; Fujimoto, K.; Grady, P.A. Evidence for a ‘paravascular’ fluid circulation in the mammalian central nervous system, provided by the rapid distribution of tracer protein throughout the brain from the subarachnoid space. Brain Res. 1985, 326, 47–63. [Google Scholar] [CrossRef]
- Gouveia-Freitas, K.; Bastos-Leite, A.J. Perivascular spaces and brain waste clearance systems: relevance for neurodegenerative and cerebrovascular pathology. Neuroradiology 2021, 63, 1581–1597. [Google Scholar] [CrossRef]
- Mendes; NF; Velloso, L. A. Perivascular macrophages in high-fat diet-induced hypothalamic inflammation. J Neuroinflammation. 2022, 19, 136. [Google Scholar] [CrossRef] [PubMed]
- Muzio, L.; Viotti, A.; Martino, G. Microglia in Neuroinflammation and Neurodegeneration: From Understanding to Therapy. Front. Neurosci. 15, 742065. [CrossRef] [PubMed]
- Block, M.L.; Zecca, L.; Hong, J.S. Microglia-mediated neurotoxicity: uncovering the molecular mechanisms. Nat. Rev. Neurosci. 2007, 8, 57–69. [Google Scholar] [CrossRef]
- Glass, C.K.; Saijo, K.; Winner, B.; Marchetto, M.C.; Gage, F.H. Mechanisms Underlying Inflammation in Neurodegeneration. Cell. 2010, 140, 918–934. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Joh, T.H. Microglia, major player in the brain inflammation: their roles in the pathogenesis of Parkinson’s disease. Exp. Mol. Med. 2006, 38, 333–347. [Google Scholar] [CrossRef]
- Streit, W.J.; Mrak, R.E.; Griffin, W.S.T. Microglia and neuroinflammation: a pathological perspective. J Neuroinflammation. 2004, 1, 14. [Google Scholar] [CrossRef]
- Charisis, S.; Rashid, T.; Liu, H.; Ware, J.B.; Jensen, P.N.; Austin, T.R.; et al. Assessment of Risk Factors and Clinical Importance of Enlarged Perivascular Spaces by Whole-Brain Investigation in the Multi-Ethnic Study of Atherosclerosis. JAMA Netw Open. 2023, 6, e239196. [Google Scholar] [CrossRef] [PubMed]
- Xie, L.; Zheng, L.; Chen, W.; Zhai, X.; Yunlu Guo, Y.; Zhang, Y.; et al. Trends in perivascular macrophages research from 1997 to 2021: A bibliometric analysis. 2023, 29, 816–830. [Google Scholar] [CrossRef]
- Sofroniew, M.V. Astrocyte barriers to neurotoxic inflammation. Nat Rev Neurosci. 2015, 16, 249–263. [Google Scholar] [CrossRef]
- da Fonseca ACC, Matias D, Garcia C, Amaral R, Luiz Geraldo H, Freitas C, Souza Lima FR. The impact of microglial activation on blood-brain barrier in brain diseases. Front Cell Neurosci. 2014, 8, 362. [Google Scholar] [CrossRef]
- Liddelow SA,Guttenplan KA, Clarke LE, Bennett FC, Bohlen CJ, Schirmer L, Bennett ML, et al. Neurotoxic reactive astrocytes are induced by activated microglia. Nature. 2017, 541, 481–487. [Google Scholar] [CrossRef]
- Verkhratsky, A.; Butt, A.M. Neuroglia: Function and Pathology. 1st ed.; Academic Press. 125 London Wall, London EC2Y 5AS, United Kingdom 525 B Street. Copyright © 2023 Elsevier Inc. All rights reserved.
- Augusto-Oliveira, M.; Arrifano, G.P.; Delage, C.I.; Tremblay, M.E.; Crespo-Lopez, M.E.; Verkhratsky, A. Plasticity of microglia. Biol. Rev. 2022, 97, 217–250. [Google Scholar] [CrossRef] [PubMed]
- Hayden, M.R. Hypothesis: Neuroglia Activation Due to Increased Peripheral and CNS Proinflammatory Cytokines/Chemokines with Neuroinflammation May Result in Long COVID. Neuroglia. 2021, 2, 7–35. [Google Scholar] [CrossRef]
- Low, R.N.; Low, R.J.; Akrami, A. A review of cytokine-based pathophysiology of Long COVID symptoms. Front Med (Lausanne) 2023, 10, 1011936. [Google Scholar] [CrossRef]
- Zeng Q, Li K, Luo X, Wang S, Xu X, Jiaerken Y, Liu X, Hong L, Hong H, Li Z, Fu Y, Zhang T, Chen Y, Liu Z, Huang P, Zhang M; for behalf of Alzheimer's Disease Neuroimaging Initiative (ADNI). The association of enlarged perivascular space with microglia-related inflammation and Alzheimer's pathology in cognitively normal elderly. Neurobiol Dis. 2022, 170, 105755. [Google Scholar] [CrossRef]
- Ineichen, B.V.; Okar, S.V.; Proulx, S.T.; Engelhardt, B.; Lassmann, H.; Reich, D.S. Perivascular spaces and their role in neuroinflammation. Neuron. 2022, 110, 3566–3581. [Google Scholar] [CrossRef] [PubMed]
Figure 2.
A possible sequence of events and a continuous spectrum for the development of enlarged perivascular spaces (EPVS) over time. There exists a sequence of remodeling changes and events in the development of enlarged perivascular spaces, white matter hyperintensities, lacunes and small vessel disease. Image provided with permission by CC 4.0 [8,28]. ACfp = astrocyte endfeet; BBB = blood–brain barrier; BEC = brain endothelial cell; BEC act/dys = brain endothelial cell activation and dysfunction; BG = basal ganglia; BM = basement membrane; CBF = cerebral blood flow; CSF = cerebrospinal fluid; CSO = centrum semiovale; ISF = interstitial fluid; LOAD = late-onset Alzheimer’s disease; MGC = microglia cell; mm = micrometer; MRI = magnetic resonance imaging; NO = nitric oxide; NVU = neurovascular unit; PVS = perivascular spaces; spaces; SAS = subarachnoid space;TIA = transient ischemic attack. WMH = white matter hyperintensities.
Figure 2.
A possible sequence of events and a continuous spectrum for the development of enlarged perivascular spaces (EPVS) over time. There exists a sequence of remodeling changes and events in the development of enlarged perivascular spaces, white matter hyperintensities, lacunes and small vessel disease. Image provided with permission by CC 4.0 [8,28]. ACfp = astrocyte endfeet; BBB = blood–brain barrier; BEC = brain endothelial cell; BEC act/dys = brain endothelial cell activation and dysfunction; BG = basal ganglia; BM = basement membrane; CBF = cerebral blood flow; CSF = cerebrospinal fluid; CSO = centrum semiovale; ISF = interstitial fluid; LOAD = late-onset Alzheimer’s disease; MGC = microglia cell; mm = micrometer; MRI = magnetic resonance imaging; NO = nitric oxide; NVU = neurovascular unit; PVS = perivascular spaces; spaces; SAS = subarachnoid space;TIA = transient ischemic attack. WMH = white matter hyperintensities.
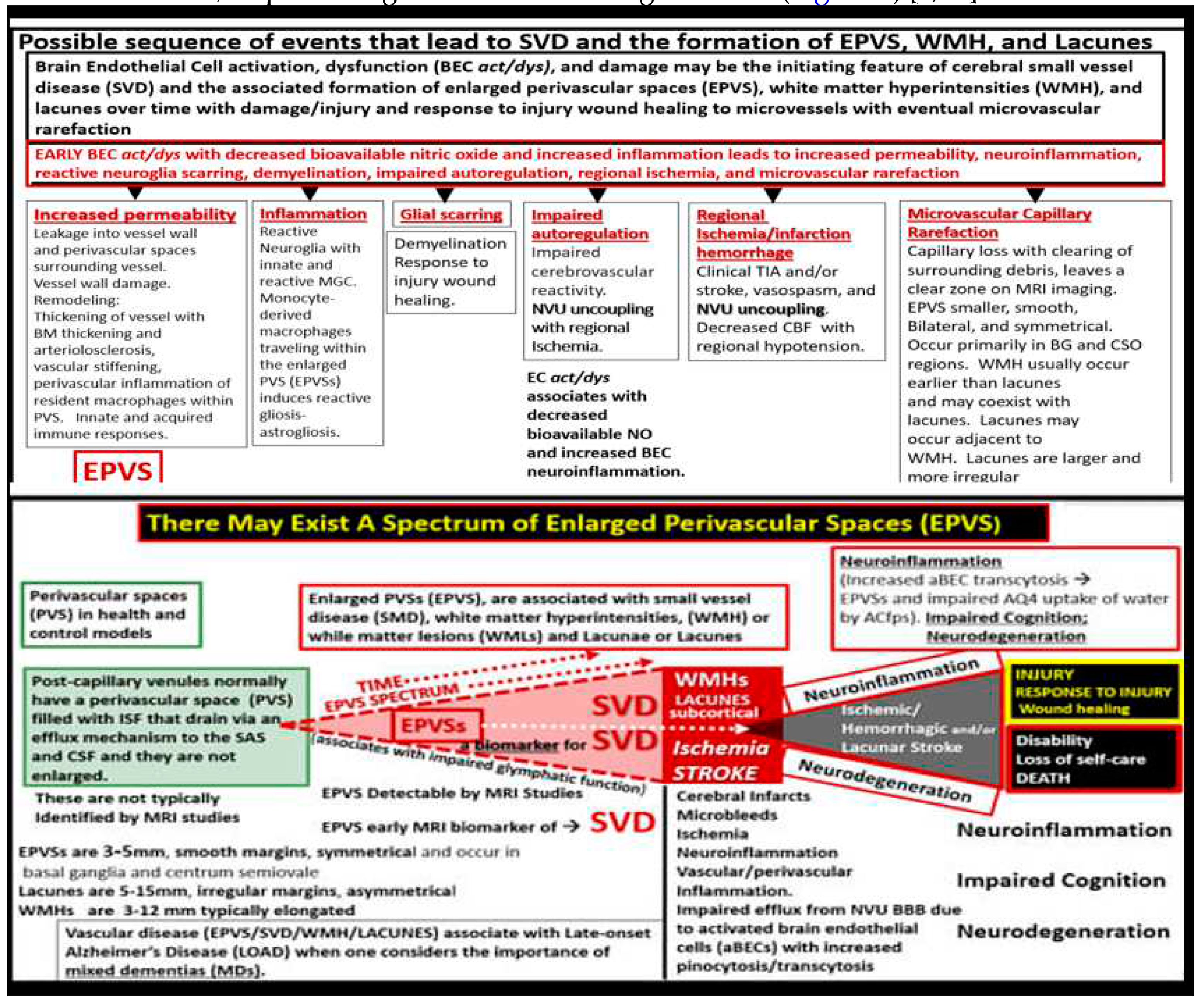
Figure 3.
Metabolic syndrome (MetS), cerebral small vessel disease (SVD) and perivascular spaces (PVS)/enlarged perivascular spaces (EPVS). The central X has four arms consisting of hyperlipidemia (lower left), hyperinsulinemia of insulin resistance (IR) (lower right), essential hypertension (upper right), and hyperglycemia (upper left). It is currently known that EPVS are a biomarker of SVD, cognitive decline and dementia, and possibly impaired glymphatic system waste removal. Visceral adipose tissue (VAT), increased triglyceride/glucose index (TG index), and hypertension are known to associate with SVD. Each of these four arms is either directly or indirectly associated with EPVS and SVD. Importantly, note that the triad of obesity, MetS, and decreased bioavailable nitric oxide (NO) are also associated with capillary rarefaction. Importantly, note how metainflammation produced primarily by visceral adipose tissue (VAT) contributes to the development of HPA axis dysfunction due to neuroinflammation induced by the resident perivascular macrophage (rPVMΦ) in the hypothalamic regions and cerebrocardiovascular disease (CCVD), SVD, TIA, stroke, microbleeds, hemorrhages, and neurodegeneration (red arrows straight and dashed lines). This modified image is provided with permission by CC 4.0 [8,29] AGE = advanced glycation end-products; RAGE = receptor for AGE; AGE/RAGE = advanced glycation end-products and its receptor interaction; BECact/dys = brain endothelial cell activation and dysfunction; eNOS = endothelial nitric oxide synthase; FFA = free fatty acids–unsaturated long chain fatty acids; IGT = impaired glucose tolerance; LOAD = late-onset Alzheimer’s disease; O2 •− = superoxide; ROS = reactive oxygen species; RSI = reactive species interactome; Sk = skeletal; T2DM = type 2 diabetes mellitus; TG Index = triglyceride/glucose index; TIA = transient ischemia attack; VAT = visceral adipose tissue.
Figure 3.
Metabolic syndrome (MetS), cerebral small vessel disease (SVD) and perivascular spaces (PVS)/enlarged perivascular spaces (EPVS). The central X has four arms consisting of hyperlipidemia (lower left), hyperinsulinemia of insulin resistance (IR) (lower right), essential hypertension (upper right), and hyperglycemia (upper left). It is currently known that EPVS are a biomarker of SVD, cognitive decline and dementia, and possibly impaired glymphatic system waste removal. Visceral adipose tissue (VAT), increased triglyceride/glucose index (TG index), and hypertension are known to associate with SVD. Each of these four arms is either directly or indirectly associated with EPVS and SVD. Importantly, note that the triad of obesity, MetS, and decreased bioavailable nitric oxide (NO) are also associated with capillary rarefaction. Importantly, note how metainflammation produced primarily by visceral adipose tissue (VAT) contributes to the development of HPA axis dysfunction due to neuroinflammation induced by the resident perivascular macrophage (rPVMΦ) in the hypothalamic regions and cerebrocardiovascular disease (CCVD), SVD, TIA, stroke, microbleeds, hemorrhages, and neurodegeneration (red arrows straight and dashed lines). This modified image is provided with permission by CC 4.0 [8,29] AGE = advanced glycation end-products; RAGE = receptor for AGE; AGE/RAGE = advanced glycation end-products and its receptor interaction; BECact/dys = brain endothelial cell activation and dysfunction; eNOS = endothelial nitric oxide synthase; FFA = free fatty acids–unsaturated long chain fatty acids; IGT = impaired glucose tolerance; LOAD = late-onset Alzheimer’s disease; O2 •− = superoxide; ROS = reactive oxygen species; RSI = reactive species interactome; Sk = skeletal; T2DM = type 2 diabetes mellitus; TG Index = triglyceride/glucose index; TIA = transient ischemia attack; VAT = visceral adipose tissue.
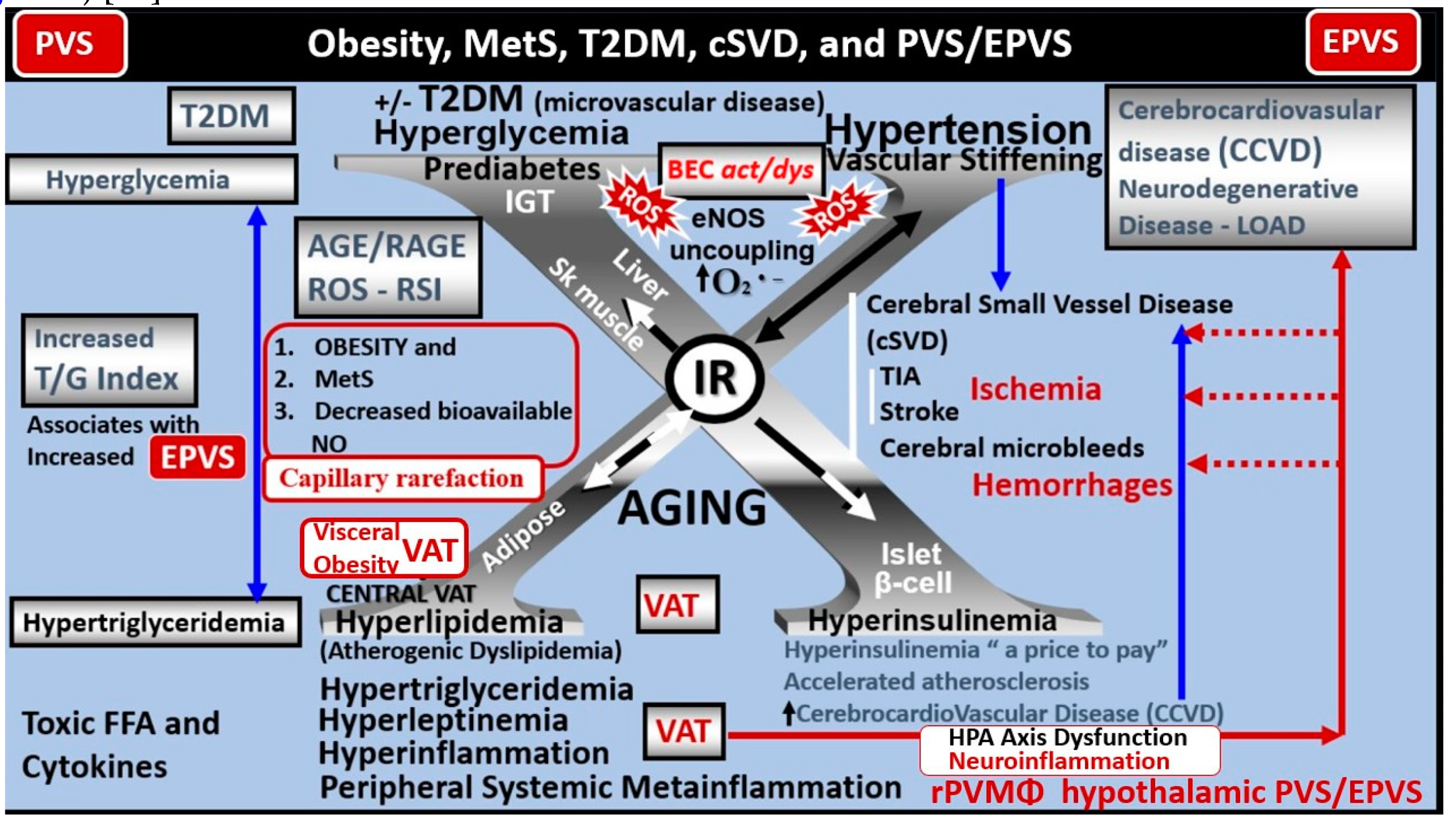
Figure 4.
Cross and longitudinal sections representitive of pre- and postcapillary arterioles and venules with an encompassing surrounding perivascular space (PVS). Panel A depicts a cross section of a capillary surrounded by a PVS (solid double red arrows) and its increase in total volume to become an enlarged perivascular space (EPVS) (dashed double red arrows), which represents capillary rarefaction. Panel B demonstrates a control longitudinal capillary that runs through an encompassing PVS (light blue). Panel C depicts capillary rarefaction in a longitudinal view and note how the volume of the PVS increases it total volume once the capillary has undergone rarefaction (double red arrows). Panel D depicts the progression of a normal precapillary arteriole and postcapillary venule PVS to an EPVS once the capillary has undergone rarefaction allowing for an increase total percentage volume of the PVS (1.- 3.). Image provided with permission by CC 4.0 [8,34]. ACef = astrocyte endfeet; AQP4 = aquaporin 4; BEC = brain endothelial cells; BECact/dys = brain endothelial cell activation and dysfunction; CL =capillary lumen; EC = endothelial cell; lpsEVexos = lipopolysaccharide extracellular vesicle exosomes; NVU = neurovascular unit; Pcef = pericyte endfeet.
Figure 4.
Cross and longitudinal sections representitive of pre- and postcapillary arterioles and venules with an encompassing surrounding perivascular space (PVS). Panel A depicts a cross section of a capillary surrounded by a PVS (solid double red arrows) and its increase in total volume to become an enlarged perivascular space (EPVS) (dashed double red arrows), which represents capillary rarefaction. Panel B demonstrates a control longitudinal capillary that runs through an encompassing PVS (light blue). Panel C depicts capillary rarefaction in a longitudinal view and note how the volume of the PVS increases it total volume once the capillary has undergone rarefaction (double red arrows). Panel D depicts the progression of a normal precapillary arteriole and postcapillary venule PVS to an EPVS once the capillary has undergone rarefaction allowing for an increase total percentage volume of the PVS (1.- 3.). Image provided with permission by CC 4.0 [8,34]. ACef = astrocyte endfeet; AQP4 = aquaporin 4; BEC = brain endothelial cells; BECact/dys = brain endothelial cell activation and dysfunction; CL =capillary lumen; EC = endothelial cell; lpsEVexos = lipopolysaccharide extracellular vesicle exosomes; NVU = neurovascular unit; Pcef = pericyte endfeet.
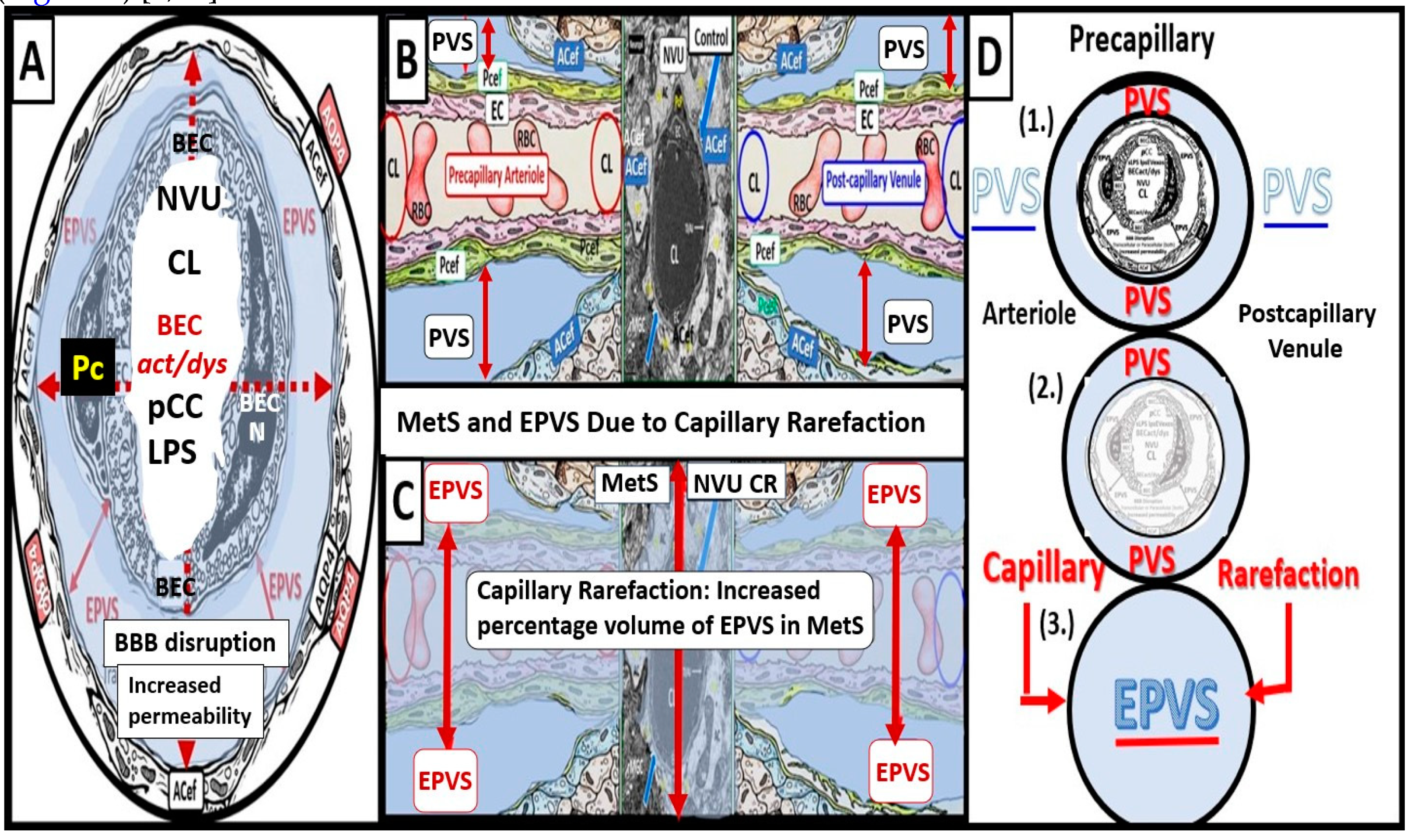
Figure 6.
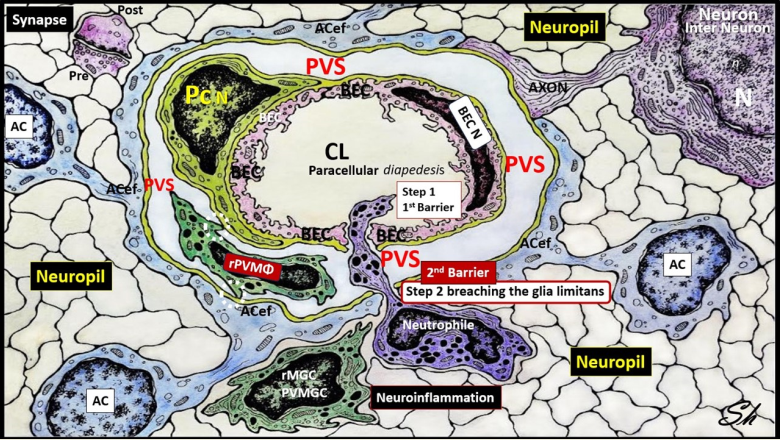
The perivascular spaces/enlarged perivascular spaces (PVS/EPVS) serve as an anatomical crossroads or intersection for the vascular, neuroinflammatory, and neuronal systems. These three systems interact and allow for multiple cellular signaling crosstalk communication associated with the metainflammation of obesity, metabolic syndrome (MetS), and type 2 diabetes mellitus (T2DM) to result in impaired cognition and neurodegeneration. Panel A demonstrates the normal appearing PVS in control models with the green background. Note the highway PVS crossroad icon in lower left panel from which this figure was constructed. Panel B depicts the EPVS with its resident reactive perivascular macrophage (rPVMΦ) and leukocytes (neutrophils, monocytes, and lymphocytes) that have undergone diapedisis via paracellular or transcytotic routes via the activated BECs to enter the EPVS and comprise step 1 of the 2-step process of leukocytes entering the neuropil interstitial space (ISS). These leukocytes not only undergo cellular crosstalk with the activated BECs but also crosstalk with one another as well as the resident perivasclar macrophage (rPVMΦ) within the PVS/EPVS, the pericyte (Pc), and the astrocyte endfeet (ACef) to result in EPVS, impaired cognition, and neurodegeration. It is important to note that both the Pc and the rPVMΦ are known to be antigen presenting cell(s) (APCs). Additionally, the reactive leukocytes are capable of generating a hugh amount of reactive oxygen species - oxidative stress and secreation of matrix metalloproteinases 2, 9 that are capable of degrading the outermost boundary of the PVS/EPVS ACef basal lamina or glia limitans to allow for the second-step for leukocyte entry into the neuropil interstitial spaces to result in neuroinflammaton and subsequent neurodegeration. The PVS/EPVS anatomical crossroad along with its multple celluar crosstalk can therefore result in a self-perpetration or vicious cycle of brain injury and response to injury wound healthing to result in neuroiflammation and neurodegeneration with impaired cognition. Additonally, it is important to note that the PVS forms the conduit for the glymphatic sytem to deliver metabolic waste and toxins from the interstitial fluid and as the neuroinflammation within the PVS/EPVS. The increased neuroinflammation that occurs within the PVS/EPVS will develop considerable metabolic waste debris that will slow and cause delayed efflux to the cerebrospinal fluid to result in further dilation of the PVS/EPVS. BBB = blood-brain barrier; BECact/dys = brain endothelial cell activation/dysfunction; CL = capillary lumen; EC = brain endothelial cells; EPVS = enlarged perivascular space; Pc = pericytes; PVS = perivascular space; rPVMΦ = resident reactive perivascular macrophage(s).
Figure 6.
The perivascular spaces/enlarged perivascular spaces (PVS/EPVS) serve as an anatomical crossroads or intersection for the vascular, neuroinflammatory, and neuronal systems. These three systems interact and allow for multiple cellular signaling crosstalk communication associated with the metainflammation of obesity, metabolic syndrome (MetS), and type 2 diabetes mellitus (T2DM) to result in impaired cognition and neurodegeneration. Panel A demonstrates the normal appearing PVS in control models with the green background. Note the highway PVS crossroad icon in lower left panel from which this figure was constructed. Panel B depicts the EPVS with its resident reactive perivascular macrophage (rPVMΦ) and leukocytes (neutrophils, monocytes, and lymphocytes) that have undergone diapedisis via paracellular or transcytotic routes via the activated BECs to enter the EPVS and comprise step 1 of the 2-step process of leukocytes entering the neuropil interstitial space (ISS). These leukocytes not only undergo cellular crosstalk with the activated BECs but also crosstalk with one another as well as the resident perivasclar macrophage (rPVMΦ) within the PVS/EPVS, the pericyte (Pc), and the astrocyte endfeet (ACef) to result in EPVS, impaired cognition, and neurodegeration. It is important to note that both the Pc and the rPVMΦ are known to be antigen presenting cell(s) (APCs). Additionally, the reactive leukocytes are capable of generating a hugh amount of reactive oxygen species - oxidative stress and secreation of matrix metalloproteinases 2, 9 that are capable of degrading the outermost boundary of the PVS/EPVS ACef basal lamina or glia limitans to allow for the second-step for leukocyte entry into the neuropil interstitial spaces to result in neuroinflammaton and subsequent neurodegeration. The PVS/EPVS anatomical crossroad along with its multple celluar crosstalk can therefore result in a self-perpetration or vicious cycle of brain injury and response to injury wound healthing to result in neuroiflammation and neurodegeneration with impaired cognition. Additonally, it is important to note that the PVS forms the conduit for the glymphatic sytem to deliver metabolic waste and toxins from the interstitial fluid and as the neuroinflammation within the PVS/EPVS. The increased neuroinflammation that occurs within the PVS/EPVS will develop considerable metabolic waste debris that will slow and cause delayed efflux to the cerebrospinal fluid to result in further dilation of the PVS/EPVS. BBB = blood-brain barrier; BECact/dys = brain endothelial cell activation/dysfunction; CL = capillary lumen; EC = brain endothelial cells; EPVS = enlarged perivascular space; Pc = pericytes; PVS = perivascular space; rPVMΦ = resident reactive perivascular macrophage(s).
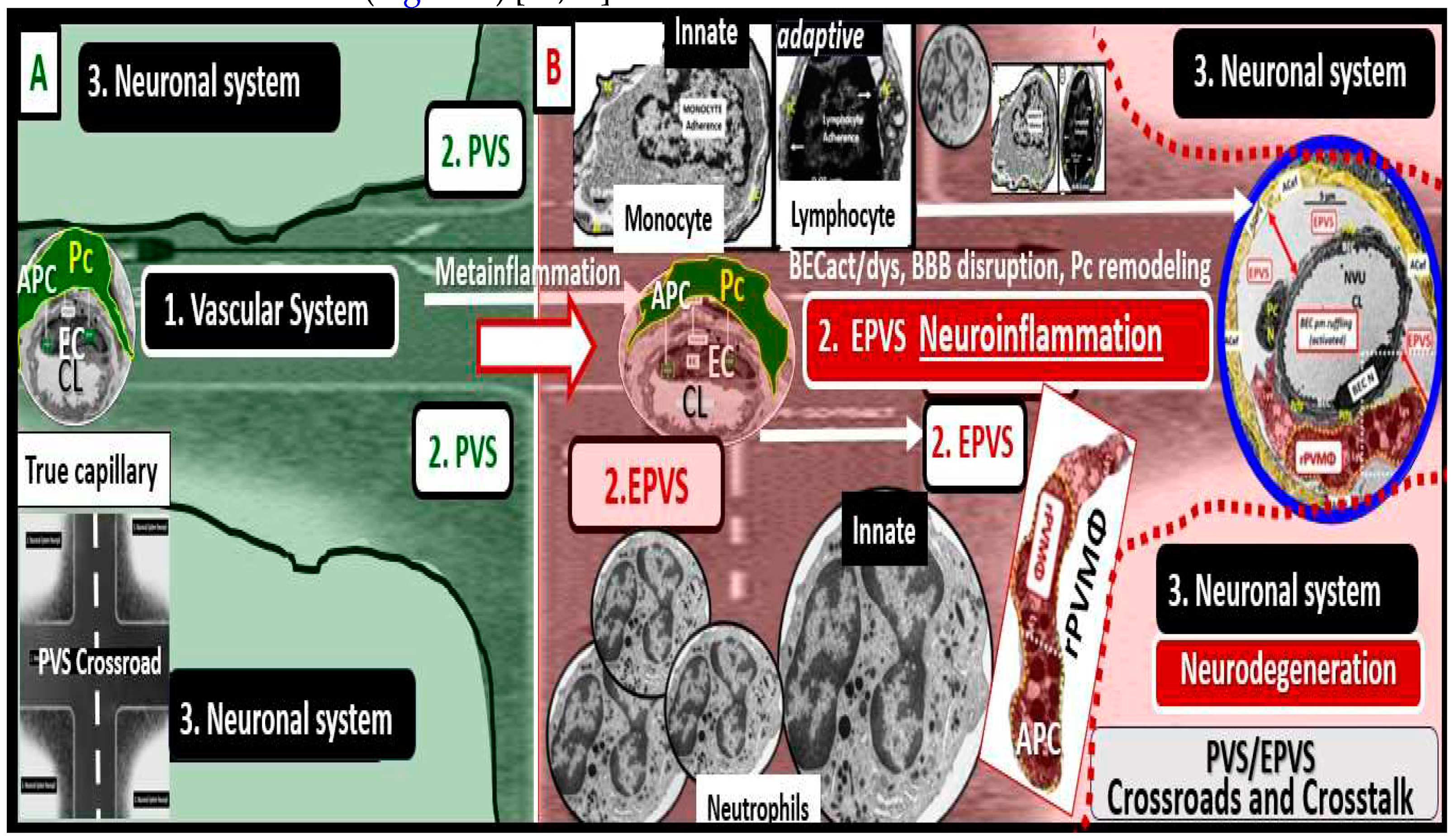
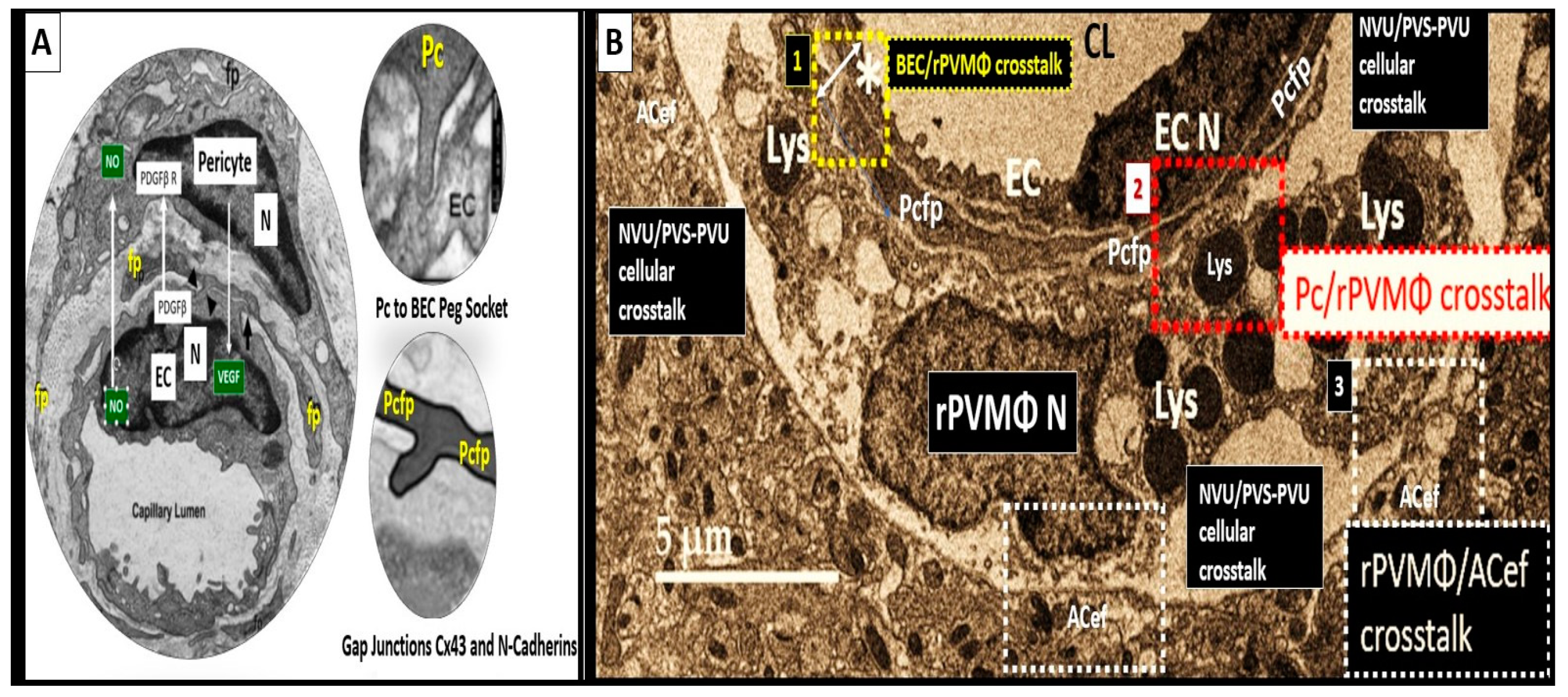
Figure 7.
Perivascular spaces (PVS) and enlarged PVS (EPVS) provide a sancuary space to serve as a crossroad for multicelluar crosstalk between brain endothelial cell(s) (BECs), pericyte(s) (Pcs), resident perivascular macrophage(s) (rPVMΦs), leukocytes, and astrocyte endfeet (ACef). Panel A demonstrates the neurovascular unit (NVU) with its blood-brain barrier/interface (BBB), as a result of the BECs tight and adherens junction(s) (TJ/AJs). The BECs and encircling Pc and it Pc foot processes (Pcfp) have a unique cell-cell direct physical contact for cell-cell communicaton via its peg socket morphology and phenotype along with its N-Caderins junctions and its gap junctions protein connexin 43 (Cx43). Panel B depicts the PVS with its cellular contents of a rPVMΦ. Importantly note that there are three close intimate cell-cell contact regions for cellular crosstalk including 1. BEC/rPVMΦ (yellow boxed-in dashed lines); 2. Pc/rPVMΦ (red boxed-in dased lines; 3. rPVMΦ/ACef (white boxed-in dashed lines). Thus, this figure identifies the Pc and it foot processes along with the rPVMΦ as a key cell residing within the PVS/EPVS to provide for this extensive crosstalk communication and that is why this panel B is pseudo-colored “golden”.
Figure 7.
Perivascular spaces (PVS) and enlarged PVS (EPVS) provide a sancuary space to serve as a crossroad for multicelluar crosstalk between brain endothelial cell(s) (BECs), pericyte(s) (Pcs), resident perivascular macrophage(s) (rPVMΦs), leukocytes, and astrocyte endfeet (ACef). Panel A demonstrates the neurovascular unit (NVU) with its blood-brain barrier/interface (BBB), as a result of the BECs tight and adherens junction(s) (TJ/AJs). The BECs and encircling Pc and it Pc foot processes (Pcfp) have a unique cell-cell direct physical contact for cell-cell communicaton via its peg socket morphology and phenotype along with its N-Caderins junctions and its gap junctions protein connexin 43 (Cx43). Panel B depicts the PVS with its cellular contents of a rPVMΦ. Importantly note that there are three close intimate cell-cell contact regions for cellular crosstalk including 1. BEC/rPVMΦ (yellow boxed-in dashed lines); 2. Pc/rPVMΦ (red boxed-in dased lines; 3. rPVMΦ/ACef (white boxed-in dashed lines). Thus, this figure identifies the Pc and it foot processes along with the rPVMΦ as a key cell residing within the PVS/EPVS to provide for this extensive crosstalk communication and that is why this panel B is pseudo-colored “golden”.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



