
Submitted:
04 July 2023
Posted:
07 July 2023
You are already at the latest version
Abstract
Background: In recent years, the assessment and guidance of cardiopulmonary resuscitation (CPR) quality using noninvasive and invasive monitoring techniques have been increasingly recommended. In this study, we introduce a new physiological monitoring system that simultaneously measures arterial pressure (AP), venous pressure (VP), and cerebral tissue oxygen saturation (SctO2) during CPR. Methods: This prospective observational study was conducted at a single center (Kagoshima City Hospital). Adult out-of-hospital patients aged ≥18 years with an intravenous femoral arterial line, venous line, and SctO2 monitor were included. We measured femoral arterial pressure (FAP) and femoral venous pressure (FVP) invasively if catheters were immediately inserted into the femoral artery and vein for potential candidates who require interventions such as extracorporeal cardiopulmonary resuscitation but did not receive such interventions as a result. Results: We observed several representative cases that provided the following insights: We presented several cases, including two patients with significant increases in FVP and low SctO2 values, and in both cases, return of spontaneous circulation (ROSC) was not achieved. In contrast, we also presented two cases in which CPR resulted in higher FAP compared to FVP and an upward trend in SctO2 values was observed, and both instances achieved ROSC. Conclusion: We presented a simultaneous physiological monitoring system that can monitor AP, VP, and SctO2 during CPR. Further case accumulations will be necessary to assess the variations in hemodynamic status during CPR and the association between each hemodynamic status and outcomes after cardiac arrest.
Keywords:
out-of-hospital cardiac arrest
; physiological monitoring
; blood pressure
; near-infrared spectroscopy
1. Introduction
Despite the current advancements in resuscitation science, outcomes following Out-of-hospital cardiac arrest (OHCA) continue to be poor [1,2,3,4]. High-quality chest compressions are among the most important key to improving outcomes. The development of cardiopulmonary resuscitation (CPR) began in the early 1900s, and the framework for the currently performed CPR was established around 1960 [5]. The CPR guidelines, updated every five years, specify the depth and rate of chest compressions, among other things, but the fundamental aspects have remained largely unchanged for many years [1,2]. This is likely due to the strong support for the forward circulation of oxygenated blood from the heart to the tissues through chest compressions, oxygen administration, and the venous blood return to the heart. However, it remains to be seen whether the current method of chest compressions is truly effective in generating circulation during resuscitation, as this has yet to be sufficiently elucidated to date.
Assessment and guidance of CPR quality using noninvasive and invasive monitoring techniques have been increasingly recommended in recent years [1,2,6]. Notably, in the 2020 international CPR guideline, the importance of invasive arterial blood pressure monitoring during CPR was mentioned as providing insights into blood pressure responding to chest compressions and pharmacological interventions for pediatric cardiac arrests [7]. However, these statements apply only to pediatric and in-hospital cardiac arrests, and no recommendations exist regarding adult and out-of-hospital cardiac arrests. We started to monitor AP, VP, and SctO2 during CPR for adult OHCA patients. In this study, we would like to introduce a new physiological monitoring system during CPR.
2. Materials and Methods
Study design, population, and setting
This was a single-center (Kagoshima City Hospital) prospective, observational study. This study included adult OHCA patients aged ≥18 years to whom intravenous femoral arterial line and venous line were inserted, and a SctO2 monitor was attached. This study was approved by the institutional review board of Kagoshima City Hospital (Approval No. 2020-56).
Study procedure
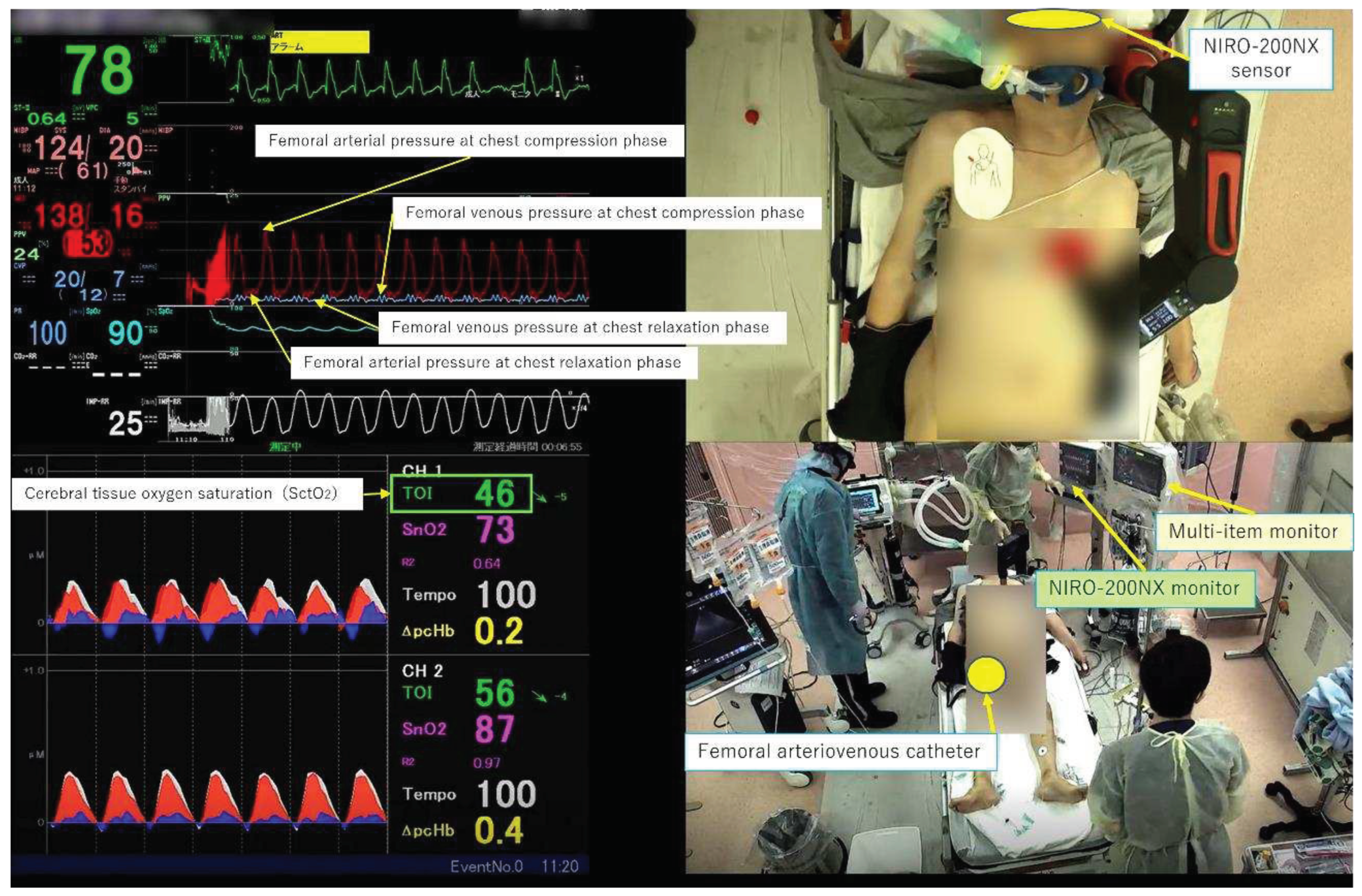
In our emergency department, we immediately insert catheters into the femoral artery and vein for potential candidates who require interventions such as extracorporeal cardiopulmonary resuscitation (ECPR) using extracorporeal membrane oxygenation to ensure prompt treatment after admission for cardiac arrest patients. In this study, we measured FAP and FVP invasively for patients who did not receive interventions such as ECPR and were not subjected to catheterization and used a near-infrared spectroscopy (NIRS) measurement probe on the forehead to measure SctO2 using the NIRO-200NX® device made by Hamamatsu Photonics, irrespective of the presence or absence of FAP and FVP measurements. These parameters were simultaneously displayed and recorded using a multi-screen recording system (Ciel View®) (Figure 1), which enabled the observation of both the external appearance of the resuscitation procedure and the physiological responses in real time. The highest blood pressure (BP) displayed on the multi-parameter monitor was defined as BP at the compression phase (CP), and the lowest blood pressure was defined as BP at the chest relaxation phase (RP). The mean arterial pressure (MAP), arterial pressure (AP) at CP, AP at RP, mean venous pressure (MVP), venous pressure (VP) at CP, VP at RP, and SctO2 were extracted every ten seconds for each case. Herein, we present four representative cases where this monitoring system was utilized during CPR.
3. Results
Case 1: A patient with acute aortic dissection as the etiology of cardiac arrest
The patient was discovered collapsed at home, and the initial electrocardiogram (ECG) waveform upon contact with the emergency medical service indicated cardiac arrest. The patient was transported to our emergency department without return of spontaneous circulation (ROSC). Upon arrival, the patient remained in cardiac arrest, and echocardiography revealed a small amount of pericardial effusion, which subsequently increased. Therefore, pericardiocentesis and pericardiotomy were performed, and a total of 5 mg of adrenaline was administered, but ROSC could not be achieved, and resuscitation was discontinued. Figure 2 shows the changes in FAP, FVP, and SctO2.
FAP and FVP measurement was initiated six minutes after arrival, during mechanical chest compressions, and the FVP was higher than the FAP during both the compression and mean phases. In particular, the FVP at CP exceeded 140 mmHg, and SctO2 ranged from 40% to the early 30s. Manual chest compressions were performed at approximately 240 seconds, the FVP at CP rapidly decreased, and the FAP and FVP reversed. During pericardiocentesis and pericardiotomy, chest compressions were temporarily suspended. Still upon resumption of chest compressions, both the AP at CP exceeded the VP at CP, and SctO2 slightly increased and ranged in the late 30s.
Case 2: A patient with presumed cardiac etiology of arrest
The patient was witnessed sinking while taking a bath in a public bathhouse, and emergency services were called. Upon initial contact with the ambulance team, the electrocardiogram showed asystole and remained so upon arrival at our emergency medical center. Although 5 mg of adrenaline was administered, resuscitation was discontinued due to lack of return of ROSC. Figure 3 shows the changes in the FAP, FVP, and SctO2. When the FAP and FVP measurement was started 6 minutes after arrival, the patient underwent manual cardiac massage, and the VP at CP was higher than the AP at CP, but this reversed around 150 seconds. The MAP and MVP were at the same level during this time, and SctO2 fluctuated around 35-38%. Subsequently, mechanical cardiac massage was initiated around 270 seconds, and the FVP rose rapidly. In particular, the VP at CP increased to 120-140 mmHg, while the AP at CP remained at around 50-60 mmHg, with the VP always higher than the AP. Furthermore, when manual cardiac massage was resumed at around 660 seconds, both the FAP and FVP decreased rapidly. When the mechanical cardiac massage was resumed again around 750 seconds, the VP at CP quickly increased to 120-140 mmHg as before, but the AP at CP only rose to 50 mmHg, and SctO2 fluctuated around 35%.
Case 3: A patient with acute coronary syndrome as the etiology of cardiac arrest
The patient collapsed and was subsequently transported to our hospital after experiencing chest pain and discomfort for two days. Initial ECG waveform upon contact with the emergency medical team showed cardiac arrest. Although the patient achieved ROSC after administering 2 mg of adrenaline, they experienced pulseless electrical activity (PEA) one minute later. Despite administering an additional 3 mg of adrenaline, the patient was still in PEA upon arrival at our hospital, as shown in Figure 4, shows the progression of FAP, FVP, and SctO2.
Mechanical chest compressions were performed from the time of hospital admission, and the initial SctO2 measurement was relatively high, ranging from 45-46%. However, the initial AP at CP and MAP measured from the femoral artery were 80mmHg and 30mmHg, respectively. Additionally, at approximately 120 seconds after the start of FVP measurement, the AP at CP and MAP had risen to 90mmHg and 40mmHg, respectively, higher than the FVP. Subsequently, while the FAP continued to grow, the FVP remained almost constant, and the VP at CP, the VP at RP, and the MVP never exceeded 25mmHg. During this period, the SctO2 value increased above 50%, and the patient achieved ROSC at approximately 270 seconds.
Case 4: A patient with asphyxia as the etiology of cardiac arrest
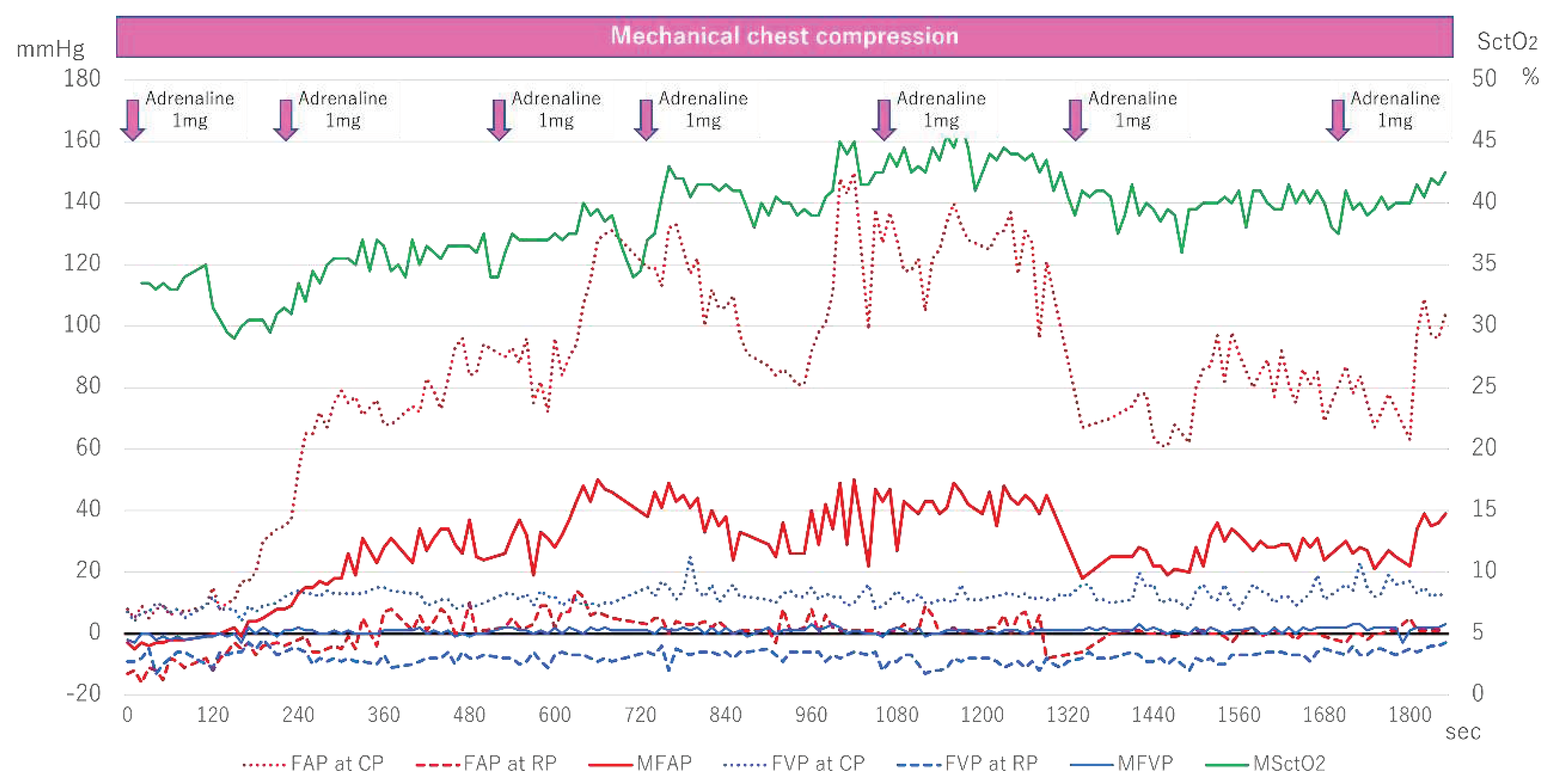
The patient had experienced a loss of appetite two weeks prior but was being monitored. After going to bed, the patient’s family found vomit next to the pillow, and the patient was found not breathing, prompting an emergency call. The initial ECG waveform taken by the ambulance crew showed asystole, and the patient was transported to our hospital while airway management and cardiopulmonary resuscitation were performed. Figure 5 shows the changes in FAP, FVP, and SctO2.
Measurement of FAP and FVP started six minutes after arrival, and both were initially low. Although FAP began to rise around 120 seconds after measurement began, FVP remained almost unchanged. With each administration of adrenaline, AP at CP gradually increased, exceeding 140mmHg at about 1000 seconds. In contrast, SctO2 increased with the rise in FAP, fluctuating between 40-45%, and ultimately ROSC was achieved.
Figure 2.
Femoral arteriovenous pressure and SctO2 in Case 1. FAP indicates Femoral arterial pressure; CP, compression phase; RP at chest relaxation phase. FVP, Femoral venous pressure; MSctO2, Mean cerebral tissue oxygen saturation.
Figure 2.
Femoral arteriovenous pressure and SctO2 in Case 1. FAP indicates Femoral arterial pressure; CP, compression phase; RP at chest relaxation phase. FVP, Femoral venous pressure; MSctO2, Mean cerebral tissue oxygen saturation.
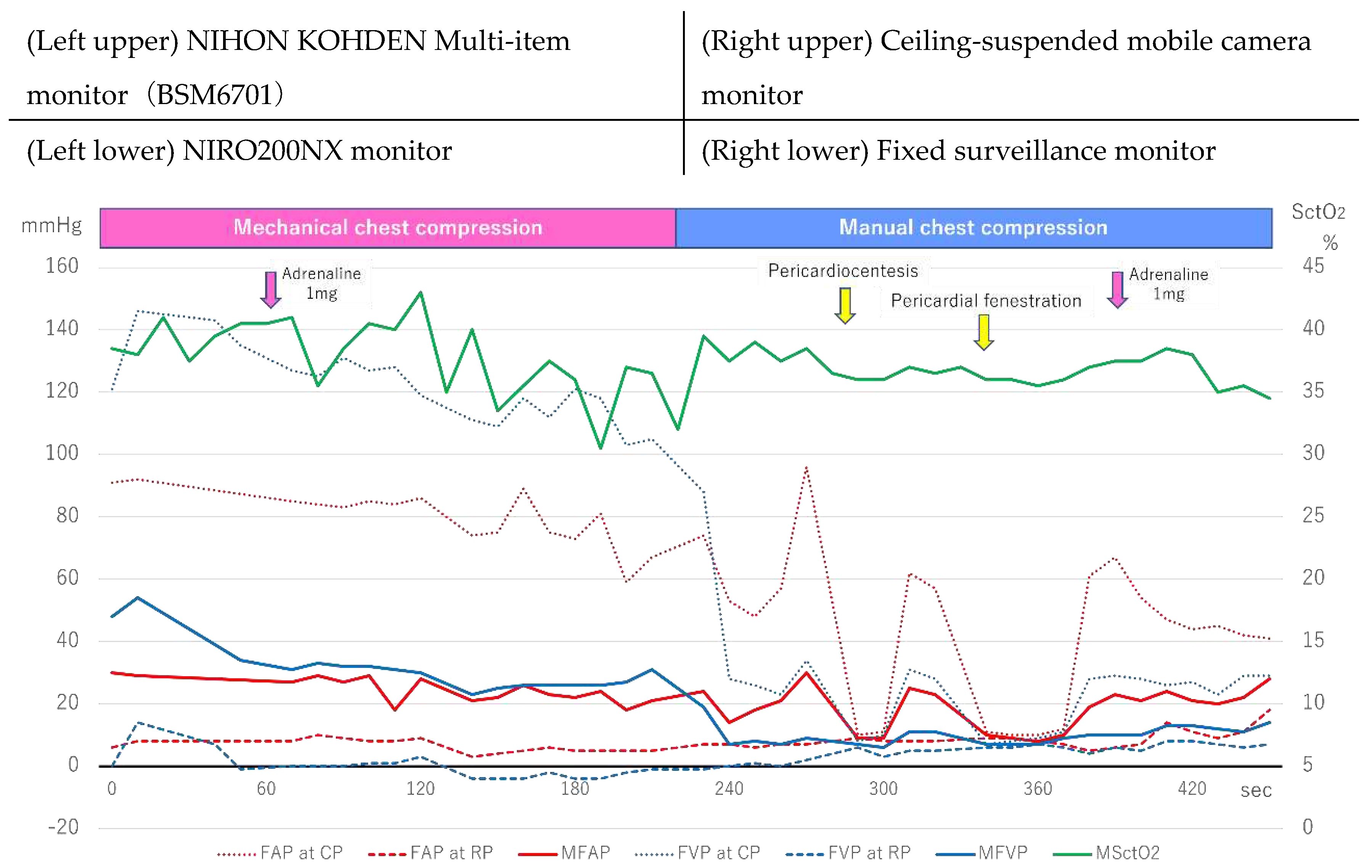
Figure 3.
Femoral arteriovenous pressure and SctO2 in Case 2. FAP indicates Femoral arterial pressure; CP, compression phase; RP, relaxation phase. FVP, Femoral venous pressure; MSctO2, Mean cerebral tissue oxygen saturation.
Figure 3.
Femoral arteriovenous pressure and SctO2 in Case 2. FAP indicates Femoral arterial pressure; CP, compression phase; RP, relaxation phase. FVP, Femoral venous pressure; MSctO2, Mean cerebral tissue oxygen saturation.
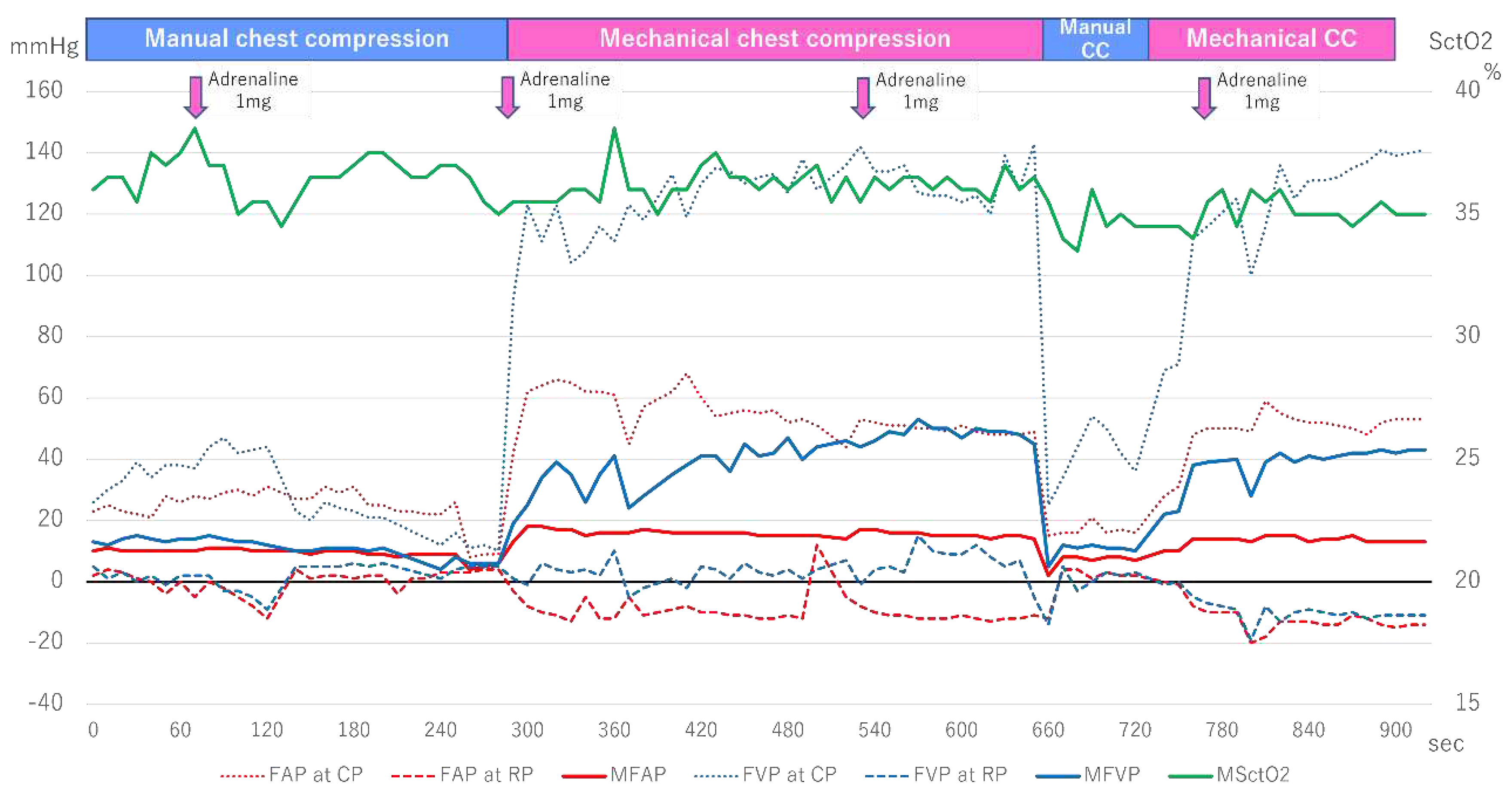
Figure 4.
Femoral arteriovenous pressure and SctO2 in Case 3. FAP indicates Femoral arterial pressure; CP, compression phase; RP at chest relaxation phase; FVP, Femoral venous pressure; MSctO2, Mean cerebral tissue oxygen saturation; ROSC, return of spontaneous circulation.
Figure 4.
Femoral arteriovenous pressure and SctO2 in Case 3. FAP indicates Femoral arterial pressure; CP, compression phase; RP at chest relaxation phase; FVP, Femoral venous pressure; MSctO2, Mean cerebral tissue oxygen saturation; ROSC, return of spontaneous circulation.
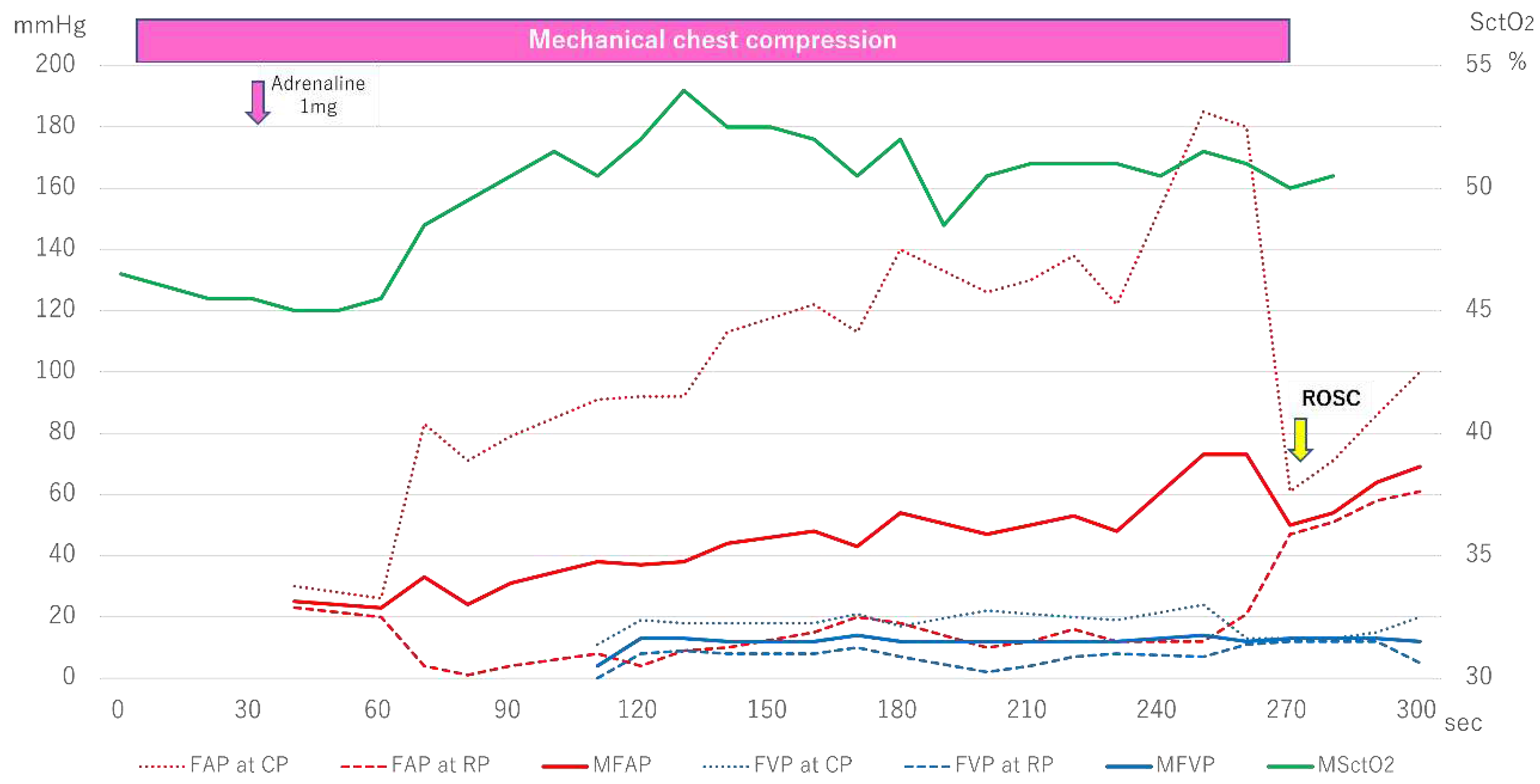
Figure 5.
Femoral arteriovenous pressure and SctO2 in Case 4. FAP indicates Femoral arterial pressure; CP, compression phase; RP at chest relaxation phase; FVP, Femoral venous pressure; MSctO2, Mean cerebral tissue oxygen saturation; ROSC, return of spontaneous circulation.
Figure 5.
Femoral arteriovenous pressure and SctO2 in Case 4. FAP indicates Femoral arterial pressure; CP, compression phase; RP at chest relaxation phase; FVP, Femoral venous pressure; MSctO2, Mean cerebral tissue oxygen saturation; ROSC, return of spontaneous circulation.
4. Discussion
In this study, we presented a simultaneous physiological monitoring system capable of monitoring AP, VP, and SctO2. We also presented several cases, including two patients with significant increases in FVP and low SctO2 values. In contrast, we also showed two cases in which CPR resulted in higher FAP compared to FVP, and an upward trend in SctO2 values was observed.
Recently, there has been an increasing focus on measuring the quality of CPR. Notably, in the 2020 international CPR guideline, a single cut-off point for diastolic BP during the first ten minutes was introduced (at least 25 mmHg in infants and at least 30 mmHg in children) based on a retrospective analysis of arterial waveforms [7,8]. However, there is limited evidence to guide the target BP for adult and out-of-hospital cardiac arrests, which constitute most cardiac arrest cases. In contrast to the previous study, our protocol included the measurement of VP. It revealed that several out-of-hospital cardiac arrest patients exhibited predominantly retrograde flow during CPR, underscoring the importance of simultaneous measurement of AP and VP to monitor the quality of CPR.
There are two circulation mechanisms for closed-chest cardiac massage: the heart pump theory and the chest pump theory [9]. The former posits that direct compression of the heart (particularly the ventricle) induces cardiac output, while the latter suggests that an increase in intrathoracic pressure resulting from compression of all tissues and organs in the thoracic cavity leads to cardiac output. Both mechanisms are currently believed to be at work, but compressing the sternum affects the ventricle, the atrium, and the superior vena cava in the thoracic cavity [9]. Tokuda et al. reported that during the cardiac massage, both aortic and central venous pressures increased almost simultaneously, and the essential flaw of closed-chest cardiac massage is that it causes venous reflux due to the compression of not only the ventricle but also the atrium [10]. Furthermore, Mackenzie et al. reported that during the cardiac massage, right atrial pressure increased to 88-116 mmHg [11]. The discussion shifted to how to prevent venous reflux from maintaining circulation during resuscitation [12], with proposals such as the early closure theory of intrathoracic veins (system) due to increased intrathoracic pressure, and the function of internal jugular vein valves, subclavian vein valves, or venous valve-like structures within the superior vena cava [13]. These valves and systems can withstand up to approximately 60 mmHg pressures and prevent reflux from the heart [13]. Still, to date, no reports have measured venous pressure outside the thoracic cavity, leaving it unclear whether reflux is indeed suppressed. While central venous pressure and right atrial pressure were not measured in the present study, the fact that the pressure in the femoral vein during the compression phase of cardiac massage exceeded 100 mmHg suggests that early closure due to increased intrathoracic pressure or venous valve structures in the superior vena cava may not have been able to prevent venous reflux. This might result in suboptimal perfusion of peripheral tissues during CPR.
SctO2 by NIRS is a highly anticipated noninvasive physiological monitor for assessing the quality of CPR and predicting outcomes [14]. Prior studies indicated that higher SctO2 values are associated with a greater likelihood of achieving ROSC and favorable neurological outcomes [14,15,16,17]. Our investigation revealed that in Cases 1 and 2, where MVP exceeded AP, lower SctO2 values were observed, and ROSC was not achieved. In contrast, in Cases 3 and 4, which had higher MAP, ROSC was reached after increased SctO2 values. It should be noted, however, that this study does not establish any causal relationship between BP and SctO2, let alone between BP and prognosis. Nevertheless, our findings have the potential to provide insight into the prediction of systemic and cerebral circulation during CPR, and further accumulation of cases is warranted to generate evidence regarding the relationship between AP, VP, and SctO2 values, as well as their association with prognosis.
While we believe that our protocol for invasive BP monitoring in OHCA patients is feasible and that more cases can be accumulated in the future, it is impossible to perform invasive monitoring for all cardiac arrest patients. Therefore, a noninvasive and easy-to-use physiological monitor should be established based on our results. Additionally, since the optimal method of CPR may vary from person to person, future randomized controlled trials will be necessary to assess the impact of individually changing the CPR method based on real-time physiological feedback (i.e., physiologically-guided resuscitation) instead of the current uniform CPR method for all individuals.
5. Conclusion
We presented a simultaneous physiological monitoring system that can monitor AP, VP, and SctO2. Further case accumulations will be necessary to assess the variations in hemodynamic status during CPR and the association between each hemodynamic status and outcomes after cardiac arrest.
Author Contributions
Hirokazu Onishi: Conceptualization, Methodology, Writing—Original draft preparation. Tasuku Matsuyama: Writing—Original draft preparation. Yuki Yasutake: Investigation, Writing—review and editing. Daichi Inaba: Data curation, Writing—Review & Editing. Tatsuji Katsue: Investigation, Resources, Writing—Review & Editing. Masaki Nagama: Resources, Visualization, Writing—Review & Editing. Yuto Iwasaki: Methodology, Resources, Visualization. Hitoshi Kano: Project administration, Formal analysis, Supervision, Visualization, Writing—Review & Editing.
Funding
This study was supported by Japan Society for the Promotion of Science KAKENHI Grant Numbers 21K16576.
Institutional Review Board Statement
This study was approved by the institutional review board of Kagoshima City Hospital (Approval No. 2020-56).
Informed Consent Statement
Patient consent was waived due to the observational study and de-identification of personal data.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Merchant, R.M.; Topjian, A.A.; Panchal, A.R.; et al. Part 1: Executive Summary: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S337–S357. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Graesner, J.T.; Semeraro, F.; Olasveengen, T.; Soar, J.; Lott, C.; et al. European Resuscitation Council Guidelines 2021: Executive summary. Resuscitation 2021, 161, 1–60. [Google Scholar] [CrossRef]
- Fire and Disaster Management Agency. Report on a Study on Social System Development to Improve Survival from Emergency Cardiovascular Disease. Available online: https://www.fdma.go.jp/publication/#rescue (accessed on 1 February 2023). (In Japanese).
- Okubo, M.; Kiyohara, K.; Iwami, T.; Callaway, C.W.; Kitamura, T. Nationwide and regional trends in survival from out-of-hospital cardiac arrest in Japan: A 10-year cohort study from 2005 to 2014. Resuscitation 2017, 115, 120–128. [Google Scholar] [CrossRef]
- Kouwenhoven, W.B.; Jude, J.R.; Knickerbocker, G.G. Closed chest cardiac massage. JAMA 1960, 173, 1064–1067. [Google Scholar] [CrossRef] [PubMed]
- Hayes, M.M.; Berg, R.A.; Otto, C.W. Monitoring during cardiac arrest: Are we there yet? Current Opinion in Critical Care 2003, 9, 211–217. [Google Scholar] [CrossRef]
- Topjian, A.A.; Raymond, T.T.; Atkins, D.; Chan, M.; Duff, J.P.; Joyner, B.L.; Lasa, J.J.; Lavonas, E.J.; Levy, A.; Mahgoub, M.; et al. Part 4: Pediatric Basic and Advanced Life Support 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142 (16_suppl_2), S469–S523. [Google Scholar] [CrossRef] [PubMed]
- Berg, R.A.; Sutton, R.M.; Reeder, R.W.; Berger, J.T.; Newth, C.J.; Carcillo, J.A.; McQuillen, P.S.; Meert, K.L.; Yates, A.R.; Harrison, R.E.; et al. Association Between Diastolic Blood Pressure During Pediatric In-Hospital Cardiopulmonary Resuscitation and Survival. Circulation 2018, 137, 1784–1795. [Google Scholar] [CrossRef] [PubMed]
- Georgiou, M.; Papathanassoglou, E.; Xanthos, T. Systematic review of the mechanisms driving effective blood flow during adult CPR. Resuscitation 2014, 85, 1586–1593. [Google Scholar] [CrossRef] [PubMed]
- Tokuda, K. Evaluation of hemodynamics during chest compression in cardiopulmonary resuscitation: With particular focus on the impact of compression rate and duration of compression. Tokyo Women’s Medical University Journal 1985, 55, 311–322. [Google Scholar]
- Mackenzie, G.J.; Taylor, S.H.; Mcdonald, A.H.; et al. Haemodynamic effects of external cardiac compression. Lancet 1964, 20, 1342–1345. [Google Scholar] [CrossRef] [PubMed]
- Babbs, C.F. New versus old theories of blood flow during CPR. Crit Care Med. 1980, 8, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Rudikoff, M.T.; Maughan, W.L.; Eferon, M.; et al. Mechanisms of blood flow during cardiopulmonary resuscitation. Circulation 1980, 61, 343–344. [Google Scholar] [CrossRef] [PubMed]
- Sandroni, C.; Parnia, S.; Nolan, J.P. Cerebral oximetry in cardiac arrest: A potential role but with limitations. Intensive Care Med. 2019, 45, 904–906. [Google Scholar] [CrossRef] [PubMed]
- Parnia, S.; Nasir, A.; Shah, C.; et al. A feasibility study evaluation the role of cerebral oximetry in predicting return of spontaneous circulation in cardiac arrest. Resuscitation 2012, 83, 982–985. [Google Scholar] [CrossRef] [PubMed]
- Schnaubelt’, S.; Sulzgruber, P.; Menger, J.; et al. Regional cerebral oxygen saturation during cardiopulmonary resuscitation as a predictor of return of spontaneous circulation and favourable neurological outcome—A review of the current literature. Resuscitation 2018, 125, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, T.; Yasutake, Y.; Inaba, D.; et al. Novel Mode of Near-Infrared Spectroscopy as a Continuous Cerebral Physiological Monitoring Device during Cardiopulmonary Resuscitation: Four Case Reports. J Clin. Med. 2022, 11, 2018. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Multi-screen recording system (Ciel View®).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



