
Submitted:
06 July 2023
Posted:
07 July 2023
You are already at the latest version
Abstract
Office workers often experience occupational musculoskeletal disorders. The aim of the current systematic review was to investigate the effectiveness of workplace exercise intervention on the oldest age group of office workers who have been reported in the literature so far, in terms of workability and well-being. Randomized Controlled Trials were used and the methodological guidelines of PRISMA were followed. The keywords used were: office workers, older, exercise intervention, workplace, microbreaks, workability and well-being. The databases searched were: PubMed, PEDro, ResearchGate, CINAHL, PsychINFO and Science Direct. PROSPERO ID: CRD42022329656. Five studies (total number of participants: 1190, mean age: 46,4) met the inclu-sion criteria. Their quality was deemed to be moderate to high, according to PEDro and MPSER scales. Workplace interventions of gradually increased strengthening and moderate stretching exercises, isometric positioning and postural reminders, either with or without supervision, result in decreasing musculoskeletal pain, disability, sick-leave from work and in the improvement of quality of life and physical activity of the middle-aged office workers, without negative impact on their workability. Despite the worldwide aging workforce, there is a knowledge gap due to research absence in the field of microbreak exercise interventions in the group of older office workers.
Keywords:
exercise microbreaks
; office workers
; middle-aged
; musculoskeletal disorders
; workplace
1. Introduction
Although the huge progress in technology has brought about new opportunities [1], the associated increased screentime of sedentary lifestyle arising from technology has led to a significant decline in physical activity levels [2]. Recent data suggest that an average person adopts sedentary behavior for 8–9 hours each day, with about 70% of this time occurring in the workplace [3]. This phenomenon is even more intensified the last couple of years compared with the pre-COVID-19 pandemic period, as mobility restrictions and teleworking are two necessary factors to reduce the spread of the virus [4,5,6].
According to the Centre for Disease Control and Prevention, musculoskeletal disorders (MSDs) are injuries of the muscles, nerves, tendons, joints, cartilage and spinal disc and work-related musculoskeletal disorders are those in which the work environment contributes to the conditions or worsens it [7]. Work-related musculoskeletal disorders represent the most common occupational related disorders in the world, with 20–60% of office workers reporting as having encountered musculoskeletal pain [8]. In addition to physical pathology, the effects of sedentary behavior have been linked with mental illnesses such as depression, worse cognitive function, increased risk of dementia and overall lower scores of quality of life (QoL) versus non sedentary behavior (48.4 ± 9.6 vs 53.9 ± 9.5), as assessed using SF-36 [9].
Research suggests that exercise microbreaks during work hours are more effective than simply standing up and stretching [10]. Physical activity at work improves psycho-physical performance, social relationships and work performance, while simultaneously reduces sickness, absenteeism and work injuries [11]. Particularly, it has been shown that scheduled exercise microbreaks result in decreased musculoskeletal pain and in improvements in work quality, efficiency and productivity [3,12]. Systematic reviews of Randomized Control Trials have concluded that simple and brief workplace-based exercises are effective in improving somatic health symptoms like musculoskeletal disorders of workers with either sedentary or standing work [13,14,15].
Civilian labor force is recorded by Organizations and Agencies to age groups: a) 16 to 19, b) 20 to 24, c) 25 to 34, d) 35 to 44, e) 45 to 54, f) 55 to 64, g) 65 to 74 and h) 75 and older [16,17,18]. The definition of older workers varies internationally and is influenced by different factors, such as the retirement age of each country and age discrimination legislation [19]. The International Labor Organization has estimated that the number of older workers aged 55 to 64 years is set to equal one quarter of the global labor force by 2030 [20]. A key goal of occupational health policy is keeping older workers healthy and productive [21] and, more specifically, within the framework of the EU-CHAFEA ProHealth65+project [22], we could characterize the workplace exercise interventions for the older workers as a crucial study field for those interested in workplace health promotion.
The key question of the current systematic review was: which are the effects of workplace exercise intervention on the older or middle-aged office workers: a) on their workability, as far as their productivity, presenteeism at work and musculoskeletal disorders is concerned and b) on their well-being, as far as their work satisfaction, their lifestyle and attitude in relation to physical activity is concerned? Furthermore, through our review it will be demonstrated if there is a short break exercise intervention that is most positively effective as far as their workability and well-being is concerned.
Previous reviews that evaluate workplace intervention programs for office workers have not specifically addressed the older or middle-aged worker group. The aim of the current systematic review was to investigate both the effectiveness of workplace exercise intervention on older or middle-aged office workers’ workability, and well-being. Efforts to quantify the dose of microbreaks needed, will be reported and proposals on future research priorities will be formed.
2. Materials and Methods
This Systematic Review was conducted by using studies published in English language, from January 1st2011 to March 1st 2022 and followed the methodological guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [23].
2.1. Data sources and search strategy
The databases that were used for the search of studies were PubMed, PEDro, Research Gate, CINAHL, PsychINFO and Science Direct. The study search was performed by using a combination of keywords, synonyms and PubMed Medical Subject Headings (MeSH) relevant terms. More specifically, search terms included office workers (and synonyms, relevant terms), older (and synonyms, relevant terms), exercise intervention (and synonyms, relevant terms), workplace (and synonyms, relevant terms), microbreaks (and synonyms, relevant terms), workability (and synonyms, relevant terms) and well-being (and synonyms, relevant terms). Search strategy is shown in Table 1.
2.2. Inclusion and exclusion criteria - Study selection
One reviewer performed a review of all retrieved data by title and abstract and then by full text, in order to determine whether they met the inclusion criteria. Study selection was based on the PICO’s framework (Patient, Problem or Population – Intervention – Comparison, Control or Comparator – Outcome), as shown in Table 2. The inclusion criteria are formed as below:
1. The sample consists of older or middle-aged office workers: when the intervention of a study was targeted at both the entire workforce and younger workers, only subgroup analyses for older or middle-aged were deemed eligible. Our initial intention was to include studies that the age of participants was ≥55 years old, but while screening, we concluded that there was no study that met this criterion. While setting as criterion the age of office workers ≥45 years old and ≥40 years, we noted that there was no study that met this age criteria either, so we decided to include studies that the age of participants was ≥35 years old and the mean age of participants in each of the study included was ≥45 years old.
2. The intervention included exercise
3. The intervention took place in the workplace, during working hours
4. The study design was Randomized Control Trial (RCT)
5. At least one of the study results referred to the effects of exercise intervention
6. The article was published from January 1st 2011 to March 1st 2022 in English language and in full-text
Non Randomized Control Trials, thesis, conference presentations and announcements, pilot trials, unpublished studies, studies where the intervention did not include exercise, studies where their sample consisted of office workers with mean age < 45 years old and minimum age <35 and studies where the intervention was not performed in the workplace during working hours, were excluded.
2.3. Quality assessment
For the assessment of the methodological quality and the potential risk of bias of the articles, the PEDro scale was chosen to be used, which contains 11 items [24]. Randomized Controlled Trials (RCTs) are traditionally considered the gold standard for examining the efficacy of interventions, and the assessment of the quality of these types of studies helps to select the best study designs [25]. The Physiotherapy Evidence Database (PEDro) scale is one of the most frequently used scales aimed to assess the methodological quality of RCTs in systematic reviews of interventions in physiotherapy and other fields, including medicine, nutrition and speech pathology [26]. The PEDro Scale assesses 11 items related to the study internal validity and statistical reporting, except for the first one (eligibility criteria), which is not computed in the total score because it evaluates the external validity of trial results. Each item is scored as either present or absent, leading to a maximum score up to 10. A high-quality study is defined when scoring positive in at least 50% (5/10) of the items, and a low-quality study is defined when scoring positive in less than 50% of the items.
In the present study PEDro score was calculated by one reviewer, by adding up all the “present” answers from items 2 to 11. The outcomes were verified by a second reviewer and when differences were not resolved, a structured consensus approach was used that involves: a) re-review of the studies, b) discussion of the adherence to standards, c) a third reviewer was consulted to reach full consensus. In our review, trials were considered to be of adequate quality based on the PEDro cut off of ≥5 points, which is widely used in the literature [27,28,29,30]. All of the RCTs included in our review are scored ≥5 points (Table 3). Particularly, three RCTs score 5/10 [31,32,33], one RCT scores 6/10 [34] and one RCT scores 7/10 [35].
The PEDro scale in its original form includes various rating criteria that are not relevant to ergonomics-based research. As a result, ergonomic articles which lack a basis for those criteria may score lower on the original PEDro scale and may be falsely represented as lower quality. It is because of this discordance that the Modified PEDro Scale for Ergonomics Research was created. The Modified PEDro Scale for Ergonomics Research (MPSER) is an assessment tool created in order to assess more accurately the quality of research in the field of ergonomics [36]. In place of the traditional 10 score seen with the PEDro, the MPSER utilizes a seven-point scale that appraises more accurately the quality of ergonomics-based research [36]. This is the reason why we decided to add MPSER tool to the quality assessment of our review. According to this scale, articles that score from 4 to 5 are categorized as “moderate quality”, and those that score from 6 to 7 are categorized as “high quality”. Articles that score below four are categorized as “low quality”.
MPSER score was calculated by one reviewer in our study, by adding up all the “present” answers from items 1 to 7. The outcomes were verified by a second reviewer and when differences were not resolved, a structured consensus approach was used that involves: a) re-review of the studies, b) discussion of the adherence to standards, c) a third reviewer was consulted to reach full consensus. According to Modified PEDro Scale for Ergonomics Research, like according to PEDro Scale in its original form, all of the RCTs included in our review are scored ≥5 points, as shown in Table 4. Particularly, three RCTs score 6/7 [31,32,34] and one RCT [35] scores 7/7, which are categorized as “high quality”, whereas one RCT scores 5/7 [33], which is categorized as “moderate quality”.
Each Randomized Control Trial that is included in the present systematic review was screened thoroughly to determine its methodological quality, using both the original PEDro scale and the Modified PEDro Scale for Ergonomics Research (MPSER). The utilization of both of these quality assessment tools leads to a more accurate determination of each methodological quality, as the MPSER scale assesses more accurately the quality of the selected articles in the field of ergonomics [36]. The quality scores of the included Randomized Control Trials were deemed appropriate for review.
2.4. Data extraction and synthesis
The characteristics of the included articles were extracted by one reviewer in a standardized way, following the characteristics of the studies’ methodology, considering the participants’ characteristics, the type and parameters of interventions, the outcome measures and the results. The accuracy of extracted data was verified by a second reviewer and when differences were not resolved, a third reviewer consulted to reach full consensus.
The characteristics and findings of the included Randomized Control Trials are summarized with information presented in Table S5. In each study we present: the sample size, participants’ characteristics, the intervention category, the characteristics of the exercise intervention (description, supervision, frequency and duration), the comparator intervention, the tools that were used for the measures and the findings for intervention. Clinical homogeneity was assessed by recording the sample population and the characteristics of the exercise intervention (description, supervision, frequency, duration), as described in Table S5.
It was concluded that, according to the studies included in our review, there are four categories-types of exercise that were used: a) strengthening intervention [31,32], b) strengthening intervention, postural reminders, stretching and exercises to improve postural stability [34], c) isometric intervention with vibration [35] and d) active exercise with simultaneous breathing [33]. Exercise protocol of each study is described in Table S5 (Intervention Exercise: Description, Supervision, Frequency and Duration). The quality assessment of each study is already shown in Table 3 and Table 4, according to PEDro and MPSER scale, respectively.
The effect of exercise intervention for each study was concluded based on the reported outcomes. The results are shown in Table 6, by using a rating system according to the level of evidence. Findings where the exercise intervention is statistically more effective than the control group in at least one outcome are classified as positive. Findings where the exercise intervention is statistically less effective than the control group in at least one outcome are classified as negative. A neutral rating (no effect) is classified when the exercise intervention does not statistically differ from the control group in any outcome.
The rating system based on the quality and outcome of the studies is as follows and the results are shown in Table 7:
- Strong evidence: consistent findings (at least 75% of the trials report statistically significant results in the same direction) among 1 or more high quality RCTs
- Moderate evidence: consistent findings (at least 75% of the trials report statistically significant results in the same direction) among multiple (2 or more) low quality RCTs and/or 1 moderate quality RCT
- Limited evidence: 1 low-quality RCT
- Conflicting evidence: inconsistent findings among multiple RCTs
- No evidence: no RCTs
3. Results
3.1. Characteristics of the included studies
The included studies of the current review were published from 2011 to 2017 and were conducted in European countries (Table S5). All the included studies applied randomization methodology of the sample prior the implementation of exercise intervention with pre- and post- evaluation of the intervention. Separation of the sample was conducted into a control group and either one intervention group [33,34,35] or more intervention groups with different frequency and level of supervision of the exercise intervention [31,32]. The duration of the intervention varies among the studies (Table S5), with the most frequent that of 20 weeks [31,32]. Participants’ size varies among the included studies (Table S5), with the smallest sample size of 37 participants [33] to the largest sample of 573 participants [32].
3.2. Participants’ demographics
The total number of participants within all the included studies was 1190 (N=1190), with minimum age 35 years and maximum 57 years old and total mean age 46,4 years (Table S5) with Standard Deviation= 1 and Coefficient of Variation (CV)= 2,15%, which means that the age of participants in the present systematic review is homogenous (CV<10%) [37] and the results are representative for office workers of middle age. All of participants were office workers performing sedentary work. Participants in three of the five studies [31,32,33] were of the general population (N1=1059), in one study [34] the participants were all diagnosed with non-specific low back pain in the absence of any major neurological deficit and with the first or recurrent episode having lasted more than six weeks but less than 12 weeks (N2=90) and in one study [35] participants reported chronic low back pain which was defined as persisting for approximately 12 weeks or longer and during that time increasing and decreasing and varying in intensity (N3=41).
The exclusion participants’ criteria of the six studies are shown in Table 8.
3.3. Quality of the reviewed RCTs
Each study in our systematic review was screened thoroughly to determine its methodological quality, using both the original PEDro scale and the Modified PEDro Scale for Ergonomics Research (MPSER). The quality assessment of each study is already shown in Table 3 and Table 4, according to PEDro and MPSER scale, respectively. The utilization of both of these quality assessment tools leads to a more accurate determination of the methodological quality of each study. Quality scores of the studies and the level of evidence they bring was deemed appropriate for review. The results of quality ratings are summarized in Table 9.
3.4. Clinical homogeneity
Clinical homogeneity was assessed by examining the characteristics of each of the exercise interventions (description, supervision, frequency, duration) and the characteristics of participants [38].
In two studies of the present review the type of workplace exercise microbreak was strengthening intervention [31,32], with a duration of 20 weeks in each study. In one other study the workplace exercise microbreak was strengthening intervention, postural reminders, stretching and exercises to improve postural stability [34] which lasted 36 weeks, in another study it was isometric intervention with vibration [35] which lasted 12 weeks and in the last study the intervention was an active exercise with simultaneous breathing [33] with duration of 6 weeks.
Since there were two studies in the type of strengthening intervention with the same duration, clinical homogeneity was assessed by examining the characteristics of each of the two strengthening exercise intervention and the characteristics of the correspondent participants [38]. All participants in both studies were office workers [31,32]; in each of the two studies mean age was 46 years and minimum age was 35 years. Additionally, the exclusion criteria were the same in both studies, as presented in Table 8. Although the duration of the exercise intervention was the same in both studies (20 weeks) [31,32], the other characteristics of the exercise intervention were different (Table S5); in one study there were three intervention groups [31], whereas in the other study there were four intervention groups [32]. All the intervention groups of the one study were with supervision [31], whereas in the other study three of the intervention groups were with supervision and the fourth group with minimal supervision [32].
As concluded from the above, the studies were not considered as homogeneous and the results were not pooled into a meta-analysis.
3.5. Types and effects of workplace exercise intervention
Results of workplace exercise intervention are reported according to each of the four types of workplace exercise interventions that were used in the included studies and the key questions which refer to their effect on the middle-aged office workers: a) on their workability, as far as their productivity, presenteeism at work and musculoskeletal disorders is concerned and b) on their well-being, as far as their work satisfaction, their quality of life and life style and attitude is concerned. The measurement tools that were used for the data extracted are recorded for each type of workplace exercise.
1. Strengthening exercise intervention
The results of strengthening exercise intervention showed reduced neck and shoulder pain in the training groups after 20 weeks compared with control group [p<0.01 [31], approx. 50% reduction [32]. From a baseline pain rating of 3.2 (SD 2.3) in the neck among office workers with neck pain, one group of 1 hour-training once a week (1WS), experienced a reduction of 1.14 (95% CI 0.17 to 2.10), one group of 20 minute-training 3 times a week (3WS), experienced a reduction of 1.88 (0.90 to 2.87) and one group of 7 minute-training 9 times a week (9WS), a reduction of 1.35 (0.24 to 2.46) [31]. Disability in Arms, Shoulders and Hands (DASH) was reduced in 1WS and 3WS groups, with a significant reduction between 3WS versus control group (p<0.001) [31]. There was a significant improvement to muscle strength (8(4-13)%) and endurance (27(12-37)%) in the training groups, compared with control group [32]. There was not demonstrated any change in productivity [31,32] or Quality of Life (QoL) [32]. Regarding readiness to change life style, there was no change in intervention groups but only in control group [31,32], which significantly increased the percentage of readiness to change from 52.0% at baseline to 67.5% at follow-up [31]. There was no data extracted as far as presenteeism and work satisfaction are concerned.
The tools that were used for the above measurements are: productivity was measured with a question of an 11-step numerical rating scale from 0 to 10 [31,32], musculoskeletal disorders were measured with the Nordic questionnaire (pain or discomfort) scale 0-9 [31,32] and the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire [31] and QoL was measured with self-rated health on a 5-step ordinal scale [32]. Lifestyle and attitude in relation to physical activity were measured with a question of 5-step ordinal scale [31,32].
2. Strengthening intervention, postural reminders, stretching and exercises to improve postural stability
The results of strengthening intervention and postural reminders and stretching and exercises to improve postural stability showed 37% reduction of low-back disability for the intervention group compared with control group and 76% reduction of low-back pain of the intervention group compared with control group [34]. There was also a significant improvement in the risk of chronicity of lower back pain (SBST clinical change, 75%, P <0.001) and in Quality of life (QoL) 3.58 times greater than the control group. However, participants allocated to the intervention group were not more likely to improve their daily task perception (p = 0.103) [34]. There was no data extracted as far as productivity, presenteeism and work satisfaction are concerned.
The above measurements of musculoskeletal disorders were measured by Oswestry Disability Index questionnaire and StarT Back Screening Tool (SBST) questionnaire to measure the risk of lower back chronicity.
3. Isometric intervention with vibration
The results of isometric intervention with vibration showed reduction of chronic low back pain (p=0.002) and disability (p=0.027) and limited improvement of trunk flexors’ strength for the intervention group compared with control group [35]. There was an improvement in intervention’s group physical activity (p=0.022) and quality of life (p=0.013) compared with control group [35]. There was also a reduction of sick-leave for the intervention group compared with control group (p=0.008) and there was no data extracted as far as productivity and work satisfaction are concerned.
The tools that were used for the above measurements are: presenteeism was measured with written data from the company, musculoskeletal disorders with Ronald and Morris disability questionnaire (RMQ), Oswestry Disability Index (ODI), isokinetic test of the musculature of the trunk and a static posturography. Quality of Life was measured by SF-36 and lifestyle and attitude in relation to physical activity with the Freiburg activity questionnaire.
4. Active exercise with simultaneous breathing
The results of active exercise with simultaneous breathing showed an improvement of neck pain (reduction of neck pain from 32 to 23 points), limited reduction of neck disability (score from 5 to 4 points after the training) and limited improvement of quality of life (improvement from 70% before to 76% after intervention) for the intervention group [33]. There was no data extracted as far as productivity, presenteeism, work satisfaction, life style and attitude in relation to physical activity are concerned.
The above measurements for musculoskeletal disorders were measured with the questionnaire of von Korff, the Borg-CR10 scale and with three-questions that addressed pain intensity in the neck/shoulder region. Quality of Life (QoL) was measured with the SF-12 and the EuroQol questionnaire five dimensions three levels (EQ-5D-3L).
4. Discussion
The major finding of the current review is the knowledge gap due to research absence for the effects of microbreak exercise interventions in the group of older office workers. Although a variety of microbreak exercise interventions has been developed on office workers in their workplace with positive effects on them, there is a research absence for the older personnel of office workers. Older workers’ health profile differs from that of young and middle-aged, as ageing process increases vulnerability to physical and psychological problems such as arthritis, osteoporosis, changes in muscle mass and strength, depression, and sensory impairments [39,40,41]. Furthermore, taking into consideration the worldwide phenomenon of aging workforce [41], the necessity of future researches to be conducted specifically for older office workers, is arisen.
Although through screening we found that from January 1st 2011 to March 1st 2022 there are six reviews that present the results of workplace exercise interventions in office workers [42,43,44,45,46,47], the present systematic review is the first one which sets age inclusion criterion in the included Randomized Control Trials and, specifically, sets as age inclusion criterion the oldest age group of office workers that has been studied so far (participants’ age ≥ 35 years old and mean age ≥45 years). Considering the reviewed age classification of the World Health Organization [48] and the age of participants, the results of the current systematic review correspond to middle-aged office workers.
According to the International Labor Organization (ILO), musculoskeletal disorders are the most common health problem among office workers in the 27 countries of the European Union [49] and the percentage of office workers that suffer from MSDs ranges from 20 to 60 per cent [8], which has led the researchers to the study of this phenomenon. Three studies in the current review [31,32,33] examined the musculoskeletal disorders which refer to neck and shoulder pain and two studies the musculoskeletal disorders which refer to low-back pain (chronic and non-specific) [34,35]. This comes in agreement with another study which concluded that office workers report that the regions of lower back (58.1%), shoulders/neck (53.0%) and hands/wrists (50.2%) are those more affected by musculoskeletal disorders, while hips/thighs/buttocks (35.9%), knees (22.6%) and ankles/feet (20.7%) are the least indicated body regions with MSDs and noted a progressive increase in MSDs from the young to middle-aged and older office workers [50]. Additionally, one more study concluded that the MSDs recorded more often among office workers are located on the regions of neck, shoulders, arms, hands, wrists and low back [51], which also comes in agreement with the examined body regions of the RCTs included in the current review.
Although an association in MSDs and age of office workers is also shown in other studies [52,53], there are studies that it is concluded that there is not such an association [54,55]. One study concluded that the upper back is the only region higher affected than other body regions by MSDs in young office workers [56], while most of the studies where the participants are both young and middle-aged office workers have examined the musculoskeletal disorders on the regions of neck and shoulders [57,58,59,60]. The above preferable examined body regions could be justified by researchers’ conclusion that among all occupations, office workers have the highest incidence of low-back and neck shoulder disorders at 17% to 21% [44,61].
Another important outcome of the present review is that results were overall independent of the supervision, which was not found to be a significant predictor of compliance [32], although supervision increases the level of commitment [62]. This outcome is very important for the organizations and companies, as supervision of exercise microbreaks could be a significant cost for them.
The present review showed that workplace exercise intervention had an overall positive effect in middle-aged office workers both on their workability and their well-being. These findings are in agreement with results of other systematic reviews which refer to younger participated office workers than those of our review and support the workplace exercise microbreaks [13,42,43,44,45,46,47].
1. Workability
Although workplace exercise interventions had no positive effect in productivity of office workers [31,32], no negative effect was recorded either in our review. A positive effect was recorded in presenteeism as sick-leave was reduced [35], which is of great interest for the organizations and the companies. Despite the fact that it is difficult to determine whether the office workers’ musculoskeletal disorders are work-related or not, microbreak exercise interventions in the workplace had positive effect on them and more specifically, workplace exercise microbreaks resulted in the reduction of neck and shoulder pain [32,33], reduction of shoulder, arm and hand disability [31], improvement of muscle strength of the arm [32], reduction of non-specific low-back pain and disability [34], improvement in risk of chronicity of non-specific low back pain [34] and reduction of chronic low-back pain [35]. Our results agree with those of two other systematic reviews [44,46] in which, although the participants were of younger age than those of our review, it was shown that exercise intervention in workplace reduced musculoskeletal disorders in neck, shoulder, upper arm and lower back [44,46].
One finding of a systematic review where the participants were younger office workers than the participants of the present review, states that neck/shoulder strengthening exercise microbreaks reduced neck pain in office workers who were symptomatic, but had no positive effect in general population of office workers [47], while both of the studies in our review that examined strengthening exercise microbreaks in office workers that were of general population, resulted in the reduction of neck pain [31,32]. We have to consider that our review is the only one that corresponds specifically to middle-aged personnel, which may be the cause of any difference noted while compared with other systematic reviews, in which participants are of younger age. Finally, a subgroup of a review [13] of sedentary workers concluded that the most positively effective microbreak exercise in musculoskeletal pain for sedentary occupations is that of stretching, followed by resistance and strengthening exercise; this comes in agreement with the intervention microbreak exercise programs that were studied in our review (Table 5), which leads us to the conclusion that the types of microbreak exercise programs that have been studied so far are similar for younger and middle-aged office workers and are beneficial for them, as they reduce symptoms of musculoskeletal disorders that might have worsen without workplace microbreaks during working hours.
2. Well-being
Workplace exercise intervention resulted in improvement of Quality of Life in two studies of our review [34,35], in one study there was a limited improvement [33] and in one study there was no change [32]. It is notable that the improvement of QoL was recorded in the two studies where participants were with low-back pain (non-specific and chronic) [34,35]. Our results strengthen the known positive effect of workplace active exercise intervention in Quality of Life of office workers [42,43] and enforce the necessity of their adaptation in the workplace during working hours.
It is remarkable that an increase of readiness to change lifestyle and attitude in relation to physical activity was recorded in control groups and not in the intervention groups in two studies of our review [31,32]. This finding may be an indicator of the difficulties encountered by the intervention groups in performing regular exercise microbreaks in the workplace, during working hours. It is known that workplace training during working hours is generally well accepted by the office workers, but the daily five-day training is too much for them [58]. Additionally, two causal factors of this finding may be the difficulty for the workers to change working culture [63,64] and the possible inadequate organizational encouragement and implementation of occupational health guidelines as far as health promotion of workers is concerned.
The present review was limited by the small number of Randomized Control Trials available that performed workplace exercise intervention microbreaks to middle-aged office workers. Additionally, clinical heterogeneity was found in the characteristics of the studies. Improvement in the quality of studies is required to strengthen the current evidence on workplace exercise interventions on middle-aged office workers.
5. Conclusions
The present systematic review to the best of our knowledge is the first one which studies the oldest age group of office workers that has been studied so far and, specifically, the effect of workplace exercise intervention on them.
According to the results of the current systematic review, it is suggested that a microbreak exercise intervention that is most positively effective for the middle-aged office workers at their workplace, as far as their workability and well-being is concerned, may constitute of gradually increased strengthening and moderate stretching exercises, isometric position and postural reminders, either with or without supervision and with preferable frequency of either 20 minutes 3 times per week or about 12 minutes daily. More particularly, microbreak exercise intervention with the above characteristics, either with or minimal supervision, results in the decreasing of musculoskeletal pain, of disability, of sick-leaving from work and in the improvement of quality of life and physical activity of the middle-aged office workers, without negative impact on their workability.
The effective fitting and embodying of microbreak exercise interventions on middle-aged office workers in the workplace during working hours, is positively effective both for the office workers themselves and the companies or organizations. Future researches specifically in older office workers need to be conducted in order to amplify microbreak exercise interventions in workplace, under the umbrella of the labor health policy for the older workers.
Supplementary Materials
Table S5: Characteristics of the Articles Included.
Author Contributions
I.D., investigation, data curation, methodology, conceptualization, visualization, writing—original draft; M.M., conceptualization, data curation, methodology, supervision, writing—review and editing; P.S., validation, conceptualization, visualization, supervision, writing—review and editing; V.S., conceptualization, methodology, supervision, visualization, writing—original draft, writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This review received no external funding.
Systematic Review Registration
This systematic review was registered with PROSPERO (ID: CRD42022329656).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Khan, M.K. Technological advancements and 2020. Telecommun Syst. 2020, 73, 1–2. [Google Scholar] [CrossRef]
- Teychenne, M.; Costigan, S.A.; Parker, K. The association between sedentary behaviour and risk of anxiety: a systematic review. BMC Public Health. 2015, 15, 513. [Google Scholar] [CrossRef]
- Kar, G.; Hedge, A. Effect of workstation configuration on musculoskeletal discomfort, productivity, postural risks, and perceived fatigue in a sit-stand- walk intervention for computer-based work. Appl Ergon. 2021, 90, 103211. [Google Scholar] [CrossRef] [PubMed]
- Trott, M.; Driscoll, R.; Iraldo, E.; Pardhan, S. Changes and correlates of screen time in adults and children during the COVID-19 pandemic: A systematic review and meta-analysis. Clin Med. 2022, 48, 101452. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, B.; Ganesan, T.B. Sedentarism and chronic disease risk in COVID 19 lockdown - a scoping review. Scott Med J. 2021, 66, 3–10. [Google Scholar] [CrossRef]
- Stockwell, S.; Trott, M.; Tully, M. et al. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: a systematic review. BMJ Open Sport Exerc. 2021. [Google Scholar] [CrossRef]
- CDC. Work-Related Musculoskeletal Disorders & Ergonomics CDC. 2020. https://www.cdc.gov/workplacehealthpromotion/health-strategies/musculoskeletal-disorders/index.html. (assessed on September 5th, 2022). 5 September.
- Hoe, V.C.; Urquhart, D.M.; Kelsall, H.L.; Zamri, E.N.; Sim, M.R. Ergonomic interventions for preventing work-related musculoskeletal disorders of the upper limb and neck among office workers. CDSR. 2018, 10, CD008570. [Google Scholar] [CrossRef]
- Izawa, K.P.; Oka, K. Sedentary behavior and health-related quality of life among Japanese living overseas. Gerontol and Geriatr Med. 2018, 4, 2333721418808117. [Google Scholar] [CrossRef]
- Mainsbridge, C.P.; Cooley, D.; Dawkins, S.; de Salas, K.; Tong, J.; Schmidt, M.W.; Pedersen, S.J. Taking a stand for office-based workers’ mental health: The return of the microbreak. Public Health Front. 2020, 8, 215. [Google Scholar] [CrossRef] [PubMed]
- Masala, D.; Mannocci, A.; Sinopoli, A.; D’Egidio, V.; Villari, P.; La Torre, G. Physical activity and its importance in the workplace. Ig Sanita Pubbl. 2017, 2, 159–169. [Google Scholar]
- Buckley, J.P.; Hedge, A.; Yates, T.; Copeland, R.J.; Loosemore, M.; Hamer, M.; Bradley, G.; Dunstan, D.W. The sedentary office: An expert statement on the growing case for change towards better health and productivity. BJSM. 2015, 49(21), 1357–1362. [Google Scholar] [CrossRef] [PubMed]
- Vitoulas, S.; Konstantis, V.; Drizi, I.; Vrouva, S.; Koumantakis, G.A.; Sakellari, V. The Effect of Physiotherapy Interventions in the Workplace through Active Microbreak Activities for Employees with Standing and Sedentary Work. Healthcare. 2022, 10, 2073. [Google Scholar] [CrossRef] [PubMed]
- Sundstrup, E.; Seeberg, K.G.V.; Bengtsen, E.; Andersen, L.L. A systematic review of workplace interventions to rehabilitate musculoskeletal disorders among employees with physical demanding work. J. Occup. Rehabil. 2020, 30, 30,588–612. [Google Scholar] [CrossRef] [PubMed]
- Van Eerd, D.; Munhall, C.; Irvin, E.; Rempel, D.; Brewer, S.; van der Beek, A.J.; Dennerlein, J.T.; Tullar, J.; Skivington, K.; Pinion, C.; Amick, B. Effectiveness of workplace interventions in the prevention of upper extremity musculoskeletal disorders and symptoms: An update of the evidence. Occup. Environ. Med. 2016, 73, 62–70. [Google Scholar] [CrossRef]
- Organization for Economic Co-operation and Development (OECD). OECD Labour Force Statistics. 2021. OECD Publishing, Paris.
- US Bureau of Labor Statistics. Labor Force Statistics from the Current Population Survey. 2021. https://www.bls.gov/cps/cpsaat03.htm (assessed on September 5th, 2022) 2021. https://www.bls.gov/cps/cpsaat03. 5 September.
- Australian Bureau of Labor Force Statistics. Labour Force, Australia, Detailed Labour force status by age, social marital status and sex. 2022. https://www.abs.gov.au/statistics/labour/employment-and-unemployment/labour-force-australia-detailed/latest-release (assessed on September 5th, 2022). 5 September.
- Dordoni, P.; Argentero, P. When age stereotypes are employment barriers: A conceptual analysis and a literature review on older worker stereotypes. Ageing Int. 2015, 40, 393–412. [Google Scholar] [CrossRef]
- Harasty, C.; Ostermeier, M. Population Ageing: Alternativemeasures of dependency andimplications for the future of work. ILO 2020, 5. [Google Scholar]
- Poscia, A.; Moscato, U.; La Milia, D.I.; Milovanovic, S.; Stojanovic, J.; Borghini, A.; Collamati, A.; Ricciardi, W.; Magnavita, N. Workplace health promotion for older workers: A systematic literature review. BMC Health Serv Res. 2016, 16, 329. [Google Scholar] [CrossRef] [PubMed]
- Magnavita, N. Project Policy Brief 9: Workplace Health Promotion for older workers in European countries. Project Health 65+ Health Promotion and Prevention of Risk. Actions for Seniors. European research funded by EU-CHAFEA. Chief researcher for workplace action for health 2014-2017.2016.
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ.2021,372,71. [CrossRef]
- de Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Austr J Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef]
- Paci, M.; Bianchini, C.; Baccini, M. Reliability of the PEDro scale: comparison between trials published in predatory and non-predatory journals. Arch Physiother. 2022, 12, 10. [Google Scholar] [CrossRef]
- Elkins, M.R.; Moseley, A.M.; Sherrington, C.; Herbert, R.D.; Maher, C.G. Growth in the Physiotherapy Evidence Database (PEDro) and use of the PEDro scale. Br J Sports Med. 2013, 47, 188–9. [Google Scholar] [CrossRef]
- Da Costa, B.R.; Hilfiker, R.; Egger, M. PEDro's bias: Summary quality scores should not be used in meta-analysis. J. Clin. Epidem. 2013, 66, 75–7. [Google Scholar] [CrossRef]
- Moseley, A.M.; Herbert, R.D.; Maher, C.G.; Sherrington, C.; Elkins, M.R. Reported quality of randomized controlled trials of physiotherapy interventions has improved over time. J. Clin. Epidem. 2011, 64, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Herbert, R.; Moseley, A.; Sherrington, C. PEDro: a database of randomised controlled trials in physiotherapy. Health information management. HIMAA. 1998, 28, 186–8. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; da Costa, B.R.; Cummings, G.G.; Ha, C.; Fuentes, J.; Saltaji, H. et al. PEDro or Cochrane to assess the quality of clinical trials? a meta-epidemiological study. PLoS One.2015,10:e0132634. [CrossRef]
- Andersen, C.H.; Andersen, L.L.; Gram, B.; Pedersen, M.P.; Mortensen, O.S.; Zebis, M.K.; Sjøgaard, G. Influence of frequency and duration of strength training for effective management of neck and shoulder pain: a randomised controlled trial. BJSM. 2012, 46, 1004–10. [Google Scholar] [CrossRef] [PubMed]
- Dalager, T.; Bredahl, T.G.V.; Pedersen, M.T.; Boyle, E.; Andersen, L.L.; Sjøgaard, G. Does training frequency and supervision affect compliance, performance and muscular health? A cluster randomized controlled trial. Man Ther. 2015, 20, 657–65. [Google Scholar] [CrossRef]
- Skoglund, L.; Josephson, M.; Wahlstedt, K.; Lampa, E.; Norbäck, D. Qigong training and effects on stress, neck-shoulder pain and life quality in a computerised office environment. Complement Ther Clin Pract. 2011, 17, 54–7. [Google Scholar] [CrossRef] [PubMed]
- Del Pozo-Cruz, B.; Gusi, N.; del Pozo-Cruz, J.; Adsuar, J.C.; Hernandez-Mocholí, M.; Parraca, J.A. Clinical effects of a nine-month web-based intervention in subacute non-specific low back pain patients: a randomized controlled trial. Clin Rehabil. 2013, 27, 28–39. [Google Scholar] [CrossRef] [PubMed]
- Kaeding, T.S.; Karch, A.; Schwarz, R.; Flor, T.; Wittke, T.C.; Kück, M.; Böselt, G.; Tegtbur, U.; Stein, L. Whole-body vibration training as a workplace-based sports activity for employees with chronic low-back pain. Scand J Med Sci Sports. 2017, 27, 2027–2039. [Google Scholar] [CrossRef]
- Radwan, A.; Ashton, N.; Gates, T.; Kilmer, A.; Van Fleet, M. Effect of different pillow designs on promoting sleep comfort, quality, & spinal alignment: A systematic review. Eur J Integr Med.2021;42,101269.
- Bernard, H.R. Research Methods in Anthropology. Qualitative and Quantitative Approaches. Altamira Press, Lanham. Sixth Edition. ISBN-13: 978-1442268883, ISBN-10: 1442268883.2006,62-89.
- Chess, L.E.; Gagnier, J.J. Applicable or non-applicable: investigations of clinical heterogeneity in systematic reviews. BMC Med Res Methodol. 2016, 16, 19. [Google Scholar] [CrossRef] [PubMed]
- Mac Nee, W.; Rabinovich, R.A.; Choudhury, G. Ageing and the border between health and disease. Eur Respir J. 2014, 44, 1332–52. [Google Scholar] [CrossRef]
- Jaul, E.; Barron, J. Age-Related Diseases and Clinical and Public Health Implications for the 85 Years Old and Over Population. Front Public Health. 2017, 5, 335. [Google Scholar] [CrossRef] [PubMed]
- Rawdeng, S.; Sihawong, R.; Janwantanakul, P. Work ability in aging office workers with musculoskeletal disorders and non-communicable diseases and its associated factors: a cross-sectional study. Int J Occup Saf Ergon. 2021, 19, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.M.; Nguyen, V.H.; Kim, J.H. Physical Exercise and Health-Related Quality of Life in Office Workers: A Systematic Review and Meta-Analysis. IJERPH. 2021, 18, 3791. [Google Scholar] [CrossRef] [PubMed]
- Radwan, A.; Barnes, L.; De Resh, R.; Englund, C.; Gribanoff, S. Effects of active microbreaks on the physical and mental well-being of office workers: A systematic review. Cogent Engin. 2022, 9, 2026206. [Google Scholar] [CrossRef]
- Sihawong, R.; Sitthipornvorakul, E.; Paksaichol, A.; Janwantanakul, P. Predictors for chronic neck and low back pain in office workers: a 1-year prospective cohort study. J Occup Health. 2016, 58, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Sihawong, R.; Janwantanakul, P.; Sitthipornvorakul, E.; Pensri, P. Exercise therapy for office workers with nonspecific neck pain: a systematic review. J Man Phys Ther. 2011, 34, 62–71. [Google Scholar] [CrossRef]
- Tersa-Miralles, C.; Bravo, C.; Bellon, F.; Pastells-Peiró, R.; Rubinat Arnaldo, E.; Rubí-Carnacea, F. Effectiveness of workplace exercise interventions in the treatment of musculoskeletal disorders in office workers: a systematic review. BMJ Open. 2022, 12, e054288. [Google Scholar] [CrossRef]
- Chen, X.; Coombes, B.K.; Sjøgaard, G.; Jun, D.; O'Leary, S.; Johnston, V. Workplace-Based Interventions for Neck Pain in Office Workers: Systematic Review and Meta-Analysis. Phys Ther. 2018, 98, 40–62. [Google Scholar] [CrossRef] [PubMed]
- Dyussenbayev, A. Age Periods Of Human Life. ASSRJ. 2017, 4, 258–263. [Google Scholar] [CrossRef]
- Aullianingrum, P.; Hendra, H. Risk Factors of Musculoskeletal Disorders in Office Workers. The Indonesian JOSH.2022:11(Special Issue),68-77.
- Okezue, O.C.; Anamezie, T.H.; Nene, J.J.; Okwudili, J.D. Work-Related Musculoskeletal Disorders among Office Workers in Higher Education Institutions: A Cross-Sectional Study. Ethiop J Health Sci. 2020, 30, 715–724. [Google Scholar] [CrossRef]
- Piranveyseh, P.; Motamedzade, M.; Osatuke, K.; Mohammadfam, I.; Moghimbeigi, A.; Soltanzadeh, A.; Mohammadi, H. Association between psychosocial, organizational and personal factors and prevalence of musculoskeletal disorders in office workers. Int J OccupSaf Ergon. 2016, 22, 267–73. [Google Scholar] [CrossRef] [PubMed]
- Akrouf, Q.A.; Crawford, J.O.; Al-Shatti, A.S.; Kamel, M.I. Musculoskeletal disorders among bank office workers in Kuwait. East Mediterr Health J. 2010, 16, 94–100. [Google Scholar] [CrossRef]
- Besharati, A.; Daneshmandi, H.; Zareh, K.; Fakherpour, A.; Zoaktafi, M. Work-related musculoskeletal problems and associated factors among office workers. Int J Occup Saf Ergon. 2020, 26, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Ardahan, M.; Simsek, H. Analyzing musculoskeletal system discomforts and risk factors in computer-using office workers. Pak J Med Sci. 2016, 32, 1425–1429. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; He, L.; Li, J.; Wang, J.; Wang, S. Visual display terminal use increases the prevalence and risk of work-related musculoskeletal disorders among Chinese office workers: a cross-sectional study. J Occup Health. 2012, 54, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Janwantanakul, P.; Pensri, P.; Jiamjarasrangsri, V.; Sinsongsook, T. Prevalence of self-reported musculoskeletal symptoms among office workers. Occup Med (Lond). 2008, 58, 436–8. [Google Scholar] [CrossRef]
- Ting, J.Z.R.; Chen, X.; Johnston, V. Workplace-Based Exercise Intervention Improves Work Ability in Office Workers: A Cluster Randomised Controlled Trial. Int J Environ Res Public Health. 2019, 16, 2633. [Google Scholar] [CrossRef]
- Andersen, L.L.; Zebis, M.K. Process evaluation of workplace interventions with physical exercise to reduce musculoskeletal disorders. Int J Rheumatol.2014;2014,761363. [CrossRef]
- Gram, B.; Andersen, C.; Zebis, M.K.; Bredahl, T.; Pedersen, M.T.; Mortensen, O.S.; Jensen, R.H.; Andersen, L.L.; Sjøgaard, G. Effect of Training Supervision on Effectiveness of Strength Training for Reducing Neck/Shoulder Pain and Headache in Office Workers: Cluster Randomized Controlled Trial. Biomed Res Int. 2014, 2014, 693013. [Google Scholar] [CrossRef] [PubMed]
- Andersen, C.H.; Andersen, L.L.; Zebis, M.K.; Sjøgaard, G. Effect of scapular function training on chronic pain in the neck/shoulder region: a randomized controlled trial. J Occup Rehabil. 2014, 24, 316–24. [Google Scholar] [CrossRef] [PubMed]
- Shahidi, B.; Curran-Everett, D.; Maluf, K.S. Psychosocial, Physical, and Neurophysiological Risk Factors for Chronic Neck Pain: A Prospective Inception Cohort Study. J Pain. 2015, 16, 1288–1299. [Google Scholar] [CrossRef]
- Grana, E.; Velonakis E.; Tziaferi S.; Sourtzi, P. Effectiveness of intervention programs to manage musculoskeletal disorders at the workplace- Scoping Review. Nurs Care & Res.2020,57,93-117.
- Marshall, A.L. Challenges and opportunities for promoting physical activity in the workplace. J Sci Med Sport/Sports Med Aust.2004,7,60-6. [CrossRef]
- Rongen, A.; Robroek, S.J.; van Ginkel, W.; Lindeboom, D.; Altink, B.; Burdorf, A. Barriers and facilitators for participation in health promotion programs among employees: a six-month follow-up study. BMC Public Health. 2014, 14, 573. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram of trial selection, adapted from PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [23].
Figure 1.
Flow diagram of trial selection, adapted from PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [23].
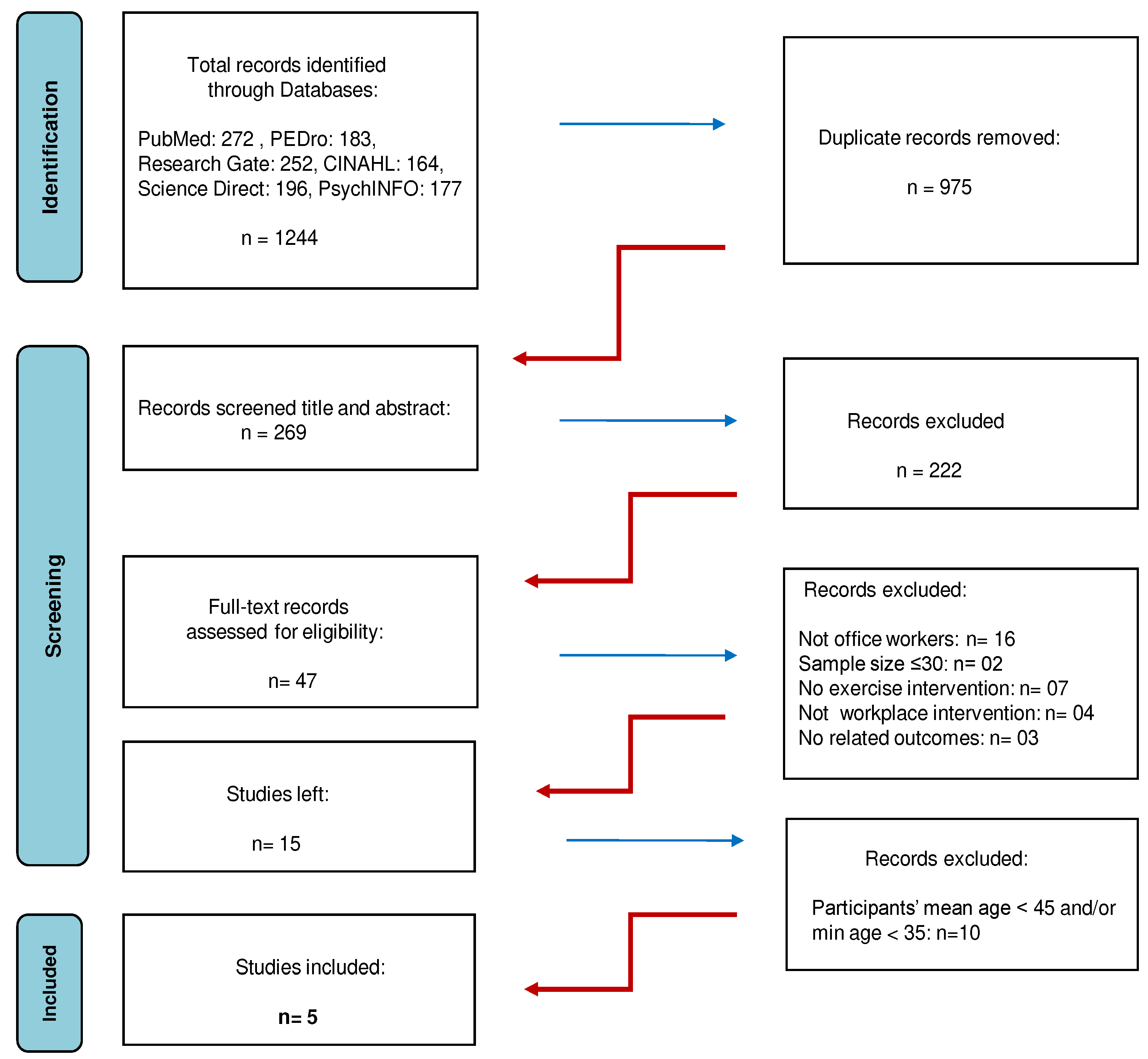

Table 1.
Search Strategy.
| Number | Keywords | Synonyms, Relevant Terms |
|---|---|---|
| 1 | Office workers | “Office employee*” OR “Clerical worker*” OR “Desk based worker*” OR “Administrative worker*” OR “Computer user*” OR “Computer operator*” OR “Occupational group*” |
| 2 | Older | “Senior*” OR “Elder” OR “Elderly” OR “Ageing” OR “Aged”OR “Middle-aged” OR “Mature” |
| 3 | Exercise Intervention | “Exercises” OR “Program*” OR “Exercise activity*” OR “Exercise therapy” OR “Exercise method*” OR “Interventions” OR “Method*” OR “Prevent*” OR “Promote*” |
| 4 | Workplace | “Work” |
| 5 | Microbreaks | “Microbreak” OR “Work break*” OR “Short break*” OR “Micropause*” |
| 6 | Workability | “Productivity” OR “Absenteeism” OR “Presenteeism” OR “Musculoskeletal discomfort” OR “Musculoskeletal symptom*“ OR “Musculoskeletal pain” OR “Musculoskeletal complaint*” OR “Musculoskeletal injury*” OR “Musculoskeletal disease*” OR “Musculoskeletal problem*” OR “Musculoskeletal disorders” |
| 7 | Well-Being | “Work satisfaction” OR “Job satisfaction” OR “Attitude*” OR “Active ageing” OR “Life style*” |
| Final Search: 1 AND 2 AND 3 AND 4 AND 5 AND 6 AND 7 | ||
Table 2.
PICO framework of the systematic review.
| P | Population | Office workers with minimum age 35 years old and participants’ mean age ≥ 45 |
| I | Intervention | Microbreaks that included exercise in the workplace during working hours |
| C | Comparison | No microbreaks, other type of microbreaks |
| O | Outcome | At least one of the study results refers to the effects of the exercise intervention |
Table 3.
PEDro scale for evaluating the quality assessment of the included RCTs.
| PEDro Scale / Study | Andersen et al., 2012 |
Dalager et al., 2015 |
Del Pozo-Cruz. et al., 2013 | Kaeding et al., 2017 |
Skoglund . et al., 2011 |
|---|---|---|---|---|---|
| Specification of eligibility criteria | ● | ● | ● | ● | ● |
| Random allocation to groups | ● | ● | ● | ● | ● |
| Concealed allocation | ○ | ○ | ○ | ○ | ○ |
| Baseline similarity of group | ● | ● | ● | ● | ● |
| Blinding of subjects | ○ | ○ | ○ | ○ | ○ |
| Blinding of therapists | ○ | ○ | ○ | ○ | ○ |
| Blinding of assessors | ○ | ● | ● | ● | ○ |
| Drop out <15% | ○ | ○ | ● | ● | ● |
| Intention-to-treat analysis | ● | ○ | ○ | ● | ○ |
| Reported statistical comparisons | ● | ● | ● | ● | ● |
| Reported point and variability measures | ● | ● | ● | ● | ● |
| PEDro Score | 5/10 | 5/10 | 6/10 | 7/10 | 5/10 |
Table 4.
MPSER scale for evaluating the quality assessment of the included RCTs.
| Modified PEDro Scale for Ergonomics Re-search (MPSER) | Andersen et al., 2012 |
Dalager et al., 2015 |
Del Pozo-Cruz et al., 2013 | Kaeding et al., 2017 |
Skoglund et al., 2011 |
|---|---|---|---|---|---|
| Adequate explanation of procedures | ● | ● | ● | ● | ● |
| Randomized allocation or randomized sequence of interventions and measurements | ● | ● | ● | ● | ● |
| Blinding of assessors | ○ | ● | ● | ● | ○ |
| Drop out <15% | ● | ● | ● | ● | ● |
| Intention-to-treat analysis | ● | ○ | ○ | ● | ○ |
| Reported statistical comparisons | ● | ● | ● | ● | ● |
| Reported point and variability measures | ● | ● | ● | ● | ● |
| MPSER Score | 6/7 | 6/7 | 6/7 | 7/7 | 5/7 |
Table 6.
Effect of exercise intervention based on reported outcomes of each study.
| Study | Type of exercise intervention | Reported outcomes | Effect of exercise intervention |
|---|---|---|---|
| Andersen et al, 2012 | strengthening intervention | Exercise intervention effectively reduced neck and shoulder pain in office workers compared with the control group. | Positive* |
| Dalager et al., 2015 | strengthening intervention | Only the training groups improved significantly their muscle strength and endurance. | Positive* |
| Del Pozo-Cruz et al., 2013 | intervention that concludes strengthening and postural reminders and stretching and exercises to improve postural stability | The exercise intervention showed clinical improvements in quality of life and selected lower back pain outcomes in the experimental group compared to the control group. | Positive* |
| Kaeding et al., 2017 | isometric intervention with vibration | There are significant effects of exercise training in the Intervention Group compared to the Control Group, regarding the primary outcome subjective disability, the pain-related disability as measured, the health-related quality of life, the health effective physical activity and the post-interventional sick leave. | Positive* |
| Skoglund et al., 2011 | active exercise with simultaneous breathing | Exercise intervention is not more effective than nointervention. | Neutral** |
*Positive: the exercise intervention is statistically more effective than the control group in at least one outcome. **Neutral: the exercise intervention does not statistically differ from the control group in any outcome.
Table 7.
Effect of exercise intervention based on the quality and reported outcomes of the studies.
| Type of exercise intervention | Study | Effect of exercise intervention |
|---|---|---|
| Strengthening intervention | a) Andersen et al., 2012 b) Dalager et al., 2015 |
Strong evidence |
| Strengthening intervention andpostural reminders and stretching and exercises to improve postural stability |
Del Pozo-Cruz et al., 2013 |
Strong evidence |
| Isometric intervention with vibration | Kaeding et al., 2017 | Strong evidence |
| Active exercise with simultaneous breathing | Skoglund et al., 2011 | Moderate evidence |
Table 8.
Exclusion criteria of the participants in each study.
| Study | Exclusion criteria of the participants |
|---|---|
| Andersen et al., 2012 | a) hypertension (systolic Blood Pressure >160mmHg, diastolic BP >100 mmHg), b) cardiovascular diseases, c) symptomatic herniated disc or severe disorders of the cervical spine, d) postoperative conditions in the neck and shoulder region, e) history of severe trauma or other serious disease and f) pregnancy |
| Dalager et al., 2015 | a) hypertension (systolic Blood Pressure >160 mmHg, diastolic BP >100 mmHg), b) cardiovascular diseases, c) symptomatic herniated disc or severe disorders of the cervical spine, d) postoperative conditions in the neck and shoulder region, e) history of severe trauma or other serious disease and f) pregnancy |
| Del Pozo-Cruz et al., 2013 | a) diagnosed cause of backache, b) reported chronic backache, c) clinical red flags such as disc disease, d) any other major disease and e) a lack of fluency in Spanish |
| Kaeding et al., 2017 | a) thrombosis, b) surgeries in the last 6-8 weeks, c) artificial joint replacements in the last 6 months, d) coronary heart disease or arterial occlusive disease, e) insufficiently treated hypertension, f) diabetes mellitus (with advanced microangiopathies, gangrenes, diabetic feet, retinal problems), g) cardiac or brain pacemaker, h) pregnancy, i) acute inflammation of the musculoskeletal system (activated arthrosis or arthropathy), j) acute tendinopathies in body parts affected by the intervention, k) acute hernias, l) acute radicular pain or complicate back pain, m) recent fractures in body partsinvolved in the intervention, n) rheumatoid arthritis, o) epilepsy and p) intrauterine device |
| Skoglund et al., 2011 | no exclusion criteria |
Table 9.
Quality rating of each study.
| Study | PEDro and MPSER Score |
|---|---|
| Andersen et al., 2012 | PEDro: 5 /10 MPSER: 6 /7 |
| Dalager et al., 2015 | PEDro: 5 /10 MPSER: 6 /7 |
| Del Pozo-Cruz et al., 2013 | PEDro: 6 /10 MPSER: 6 /7 |
| Kaeding et al., 2017 | PEDro: 7 /10 MPSER: 7 /7 |
| Skoglund et al., 2011 | PEDro: 5 /10 MPSER: 5 /7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



