
Submitted:
06 July 2023
Posted:
10 July 2023
You are already at the latest version
Abstract
Antimicrobial resistance (AMR) remains a challenge in Kenya, while the extent remains unknown. To assess the knowledge, cultural beliefs, practices, and behavioral patterns among multisectoral stakeholders in Kenya. The cross-sectional survey was conducted in August 2021 among farmers, animal health service providers and AMR researchers. Regional digital data collection tool developed by FAO was shared and responses obtained through mail, phone calls and direct interviews. Descriptive and inferential analysis were conducted. Antimicrobials were mostly sourced from agro-veterinary shops and from veterinary professionals. Farmers, often implement self-treatment and reported overuse, unnecessary use, and sometimes fail to complete the dosage in livestock. More farmers reported to have heard about antibiotics as compared to antimicrobials, mostly from friends and radio program, however only 9.2% could correctly differentiate the two. Animal Health Service Providers (AHSP) were the source of information to farmers regarding AMR. AHSPs mainly relied on suppliers and distributors for information about antibiotics. Both farmers and AHSPs treated viral infections with antibiotics. One Health Partners (OHPs) had higher knowledge and largely favorable attitudes towards AMR. Up to 72.7% of OHPs from training institutions had AMR included in training curriculum however, they were optimistic livestock farmers and government were less concerned about AMR. Gaps in knowledge and practice on Antimicrobial Stewardship (AMS) were observed in all categories of stakeholders. Given the documented knowledge-practice gap, innovative solutions are needed for both AHSPs and farmers to promote good antimicrobial stewardship practices and to mitigate burdens of AMR. Outcomes of this research should deepen the understanding of critical information and trigger behavioral change in usage and stewardship of antimicrobials.
Keywords:
antibiotics
; antimicrobial resistance
; knowledge
; attitude
; practice
; animal health service provider
; livestock farmer
; Kenya.
1. Introduction
Bacterial antimicrobial resistance (AMR) is one of the emerging prominent public and animal health threats of our time, one that threatens the effective treatment of an ever-increasing range of bacterial infections in both animal and human populations [1]. Indeed, the major international agencies tasked with promoting public and animal health, including the Food and Agriculture Organization, World Health Organization, World Animal Health Organization, United Nation Environmental Program and various other groups and researchers, agree that AMR is a pressing global issue that requires coordinated efforts to address [2,3,4]. Left unchecked, AMR significantly threatens the achievement of the Sustainable Development Goals (SDG), with the greatest potential impact being on no poverty (SDG 1), zero hunger (SDG 2), health and well-being (SDG 3), clean water and sanitation availability (SDG 6), decent work and economic growth (SDG 8), and reduced inequality (SDG 10) [2,5,6]. It is estimated that over 24 million persons will become extremely poor by 2030 due to AMR with collective economic costs of AMR surpassing $120 trillion by 2050 [2,7,8]. Even though AMR is a global problem, the socio-economic burden is and will be disproportionately higher in low-income and middle-income countries such as Kenya unless mitigation efforts are intensified [9,10,11].
In Kenya, studies and laboratory records indicate that there is increasing prevalence of AMR bacteria in various parts of the country [12,13]. Kenya has made initial positive steps towards containment and control of AMR through streamlining coordination mechanisms, increasing awareness activities on the dangers of AMR, creation of nationally coordinated surveillance activities in both livestock and human health sector and implementing field activities to promote infection prevention and control thus reducing antimicrobial consumption and associated AMR [12,13,15]. However, as per the 68th World Health Assembly resolution, which recommended development and implementation of National Action Plans on AMR, the burden of AMR and Antimicrobial Use (AMU) in Kenya has not been determined comprehensively due to lack of reliable data [12,13,14,15].
Larger land masses of Kenya are arable land suitable for livestock keeping, hence many Kenyans depend on livestock for their livelihoods. In this study, we assessed the knowledge, cultural beliefs, practices, and behavioral patterns towards AMR to deepen the understanding of commonly known information, attitudes, drivers and factors that influence behavior with the regards to antimicrobials usage and management in Kenya. This study may serve as a baseline source for the development of effective antimicrobial stewardship and best farm practices and intervention programs to mitigate inappropriate AMU.
2. Results
2.1. Farmers
2.1.1. Farmers Demographic Characteristics and Farming Practices
Among the enrolled farmers, 249 (65.3%) were males. Most of the farmers were young adults falling between the ages 30 – 49 years old (61.4%). The farmers had varied levels of education with those completing secondary education being the majority at 121 (31.8%). Most of the farmers had less than five years in farming (n = 186; 48.9%) as shown in Table 1.
The farmers practice mixed livestock and crop production. They keep various species of livestock including cattle, sheep and goats, chicken, pigs, camels, and fish. Chicken, sheep, and cattle were the most kept livestock kept by the farmers at 193 (50.7%), 136 (35.7%) and 136 (35.7%) respectively (Supplementary Table 1).
Most farmers with no formal education (64.0%) resorted to self- treatment of animals however those with basic (56.6%) and tertiary (44.6%) levels of education were more likely to ask for an animal health professional to attend their animals (Table 2).
2.1.2. Knowledge and Perceptions on Antimicrobials, Antibiotics, and Antibiotic Resistance among Farmers
More farmers (n = 108; 28.4%) have heard about antibiotics as compared to antimicrobial (n= 51; 13.4%) however only 32 (9.2%) of those who have heard about antibiotics could correctly differentiate the two. Most farmers had heard of AMR (n = 96; 85.7%), mostly through friends, workshops, and the radio (Figure 1). Animal health professionals were the least common source of information about AMR to farmers (Figure 1). Only over 15% of farmers attempted to describe what causes AMR, with 60 (15.8%) of them describing the cause due to bacterial resistance, 40 (10.5%) due to medicine losing their potency and misuse or overuse of antimicrobials (Figure 1). Farmers reported overuse of antimicrobials 80(23.1%), unnecessary use 36(10.4%) and failure to complete the dosage when an animal is undergoing treatment is showing some improvement 27(7.8%) as the drivers of AMR (Figure 1).
Farmers were concerned that their animals and family members would acquire AMR (Figure 2). Failure for an animal to recover from illness was highly regarded as a serious concern (Figure 2). A significant proportion of farmers (n = 149; 41.9%) perceived that it is appropriate to use antimicrobial to promote animal growth although only 0.4% claimed to use antibiotics to improve productivity (Table 3).
2.1.3. Practices on Antimicrobial Use among Farmers
Antimicrobials were mostly sourced from agro-veterinary shops (n = 171; 49.0%) and from veterinary professionals (n = 164; 47.0%) (Table 3). Some farmers (n = 228; 63.7%)) stated that they would obtain a prescription before buying antimicrobials. Likewise, over half of farmers (n = 209; 60.2%) reported to use alternative medicine as first option instead of antimicrobials (Table 3). The reason for use of alternative medicine was to prevent AMR (n = 145; 86.8%) and that they were cheaply available (n = 16; 9.6%). (Table 3).
Farmers relied on agro-veterinary shops’ recommendations for quality assurance (n = 131; 36.9%), checking of the expiry dates before purchasing largely practiced (n = 191; 54.9%) among other quality assurance practices including acquiring from specific outlet (Table 3). Antimicrobials were used by farmers to treat FMD (n = 121; 34.1%) and Newcastle disease in chicken (n = 111; 31.1%) among other viral diseases (Table 3). Record keeping was poorly practiced by farmers, records were kept on livestock production (n = 158; 44.5%) and sales at the farm (n = 106; 26.8%). Upto 59 (16.6%) were not keeping any records.
2.2. Animal Health Service Providers (AHSP)
2.2.1. Demographic Characteristics of the Veterinary Professionals and Paraprofessionals
The survey received response from 47 veterinary professionals and paraprofessionals. In Kenya, veterinary professionals have minimum of degree in veterinary medicine, while paraprofessionals are either holders of certificate, diploma or degree in animal health sciences. Of the respondents 36 (76.6%) were male. Most respondents were young adults of age groups 20-29 Twenty one21 (44.7%) had 2-5 years of veterinary related. It was noted that not all respondents completed the questionnaire, hence some missing data on subsequent variables (Table 1).
2.2.2. Knowledge, Attitudes, and Practices towards Antimicrobials Use and AMR by the Animal Health Professionals.
Most of the respondents have heard of AMR and could properly describe antibiotics and antimicrobials with a majority having heard of AMR during training programs (n = 17; 65.4%) and in workshops (n = 13; 50.0%) (Table 4). The understanding that AMR is a global threat was agreed to by 22 respondents (84.6%), while 12 (46.2%) responded that it (AMR) can be eradicated. Among the promoters of AMR, antimicrobial overuse and unnecessary use scored highly (n = 23; 88.5%) and (n = 19; 73.1%) respectively (Table 4). Other drivers of AMR listed were incomplete dosage and use of water contaminated with feces, antimicrobial residues, and fertilizer. The respondents indicated that practicing hygiene, sanitation, and biosecurity at the farm (n = 21; 80.8%) as the main way of preventing occurrence of AMR (Table 4).
The respondents shared various perceptions regarding antimicrobial use and AMR, with 18 respondents (90.0%) agreeing that antimicrobials improve the growth rate of animals. Over 14 respondents (70.0%) agreed that proper use of antimicrobials in animals poses no danger, while 17 (85.0%) of respondents strongly agreed that antimicrobials should be given with prescriptions. (Table 5). Among the factors which were indicated by the respondents as having strong influence were laboratory diagnosis (n = 15; 75.0%), data published in online journals (n = 12; 60.0%), laws and regulations (n = 12; 60.0%) and professional groups (n = 12; 60.0%). The AHSPs reported to rely mostly on suppliers and distributors (n = 10; 55.6%) for information about specific antimicrobial which included information on dosage, AMR, and sales (Table 6, Figure 3).
In this practice, a majority (n = 15; 83.3%) reported to be advising farmers on antimicrobial use whenever they sell or issue to farmers. The farmers are mostly advised during sales promotion and upon request (n = 14; 77.8%). Few AHSPs, (n = 8; 44.4%) demand prescriptions whenever they are selling antimicrobials to farmers. Those who did not demand prescriptions gave reasons as not required by law (n = 7; 38.9%), not requirement by the organization/ business (n = 5; 27.8%) while others just felt no need as clients do not prefer getting a prescription. Keeping no records of prescription issued and the details on persons presenting the prescriptions were widely practiced (n = 12; 66.7%). Encountering a farmer with expired antimicrobials was a common finding (n = 12; 66.7%) in which most of the AHSPs would encounter at least once a month (n = 6; 33.3%). Farmers were also advised to use antimicrobials mostly to during treatment of Foot and Mouth Disease of cattle (n = 10; 55.6%) and Newcastle disease of chicken (Table 6, Figure 3).
2.3. One Health Practitioners
2.3.1. Demographic Characteristics
The survey received response from 32 respondents of which a majority were male, and age group of 20 – 29 years old (n = 14; 43.8%). The respondents had varied years of experience ranging from less than one year to over 15 years (Table 1).
2.3.2. AMU/AMR Knowledge Practices and Perceptions among One Health Practitioners (OHPs)
We observed high levels of knowledge, understanding and description of AMR among the OHPs. A majority had over 15 years in practice and in post graduate education. The knowledge on description, promoters and preventive measures of AMR were satisfactory and this was highly expected (Table 7). Most of the respondents agreed on the usefulness of antimicrobials in protecting people and animals from diseases. We observed generally favorable attitudes from OHPs towards AMR; however, more than a quarter strongly agreed on the importance of using antimicrobials in the farms.
On the concerns of different players in animal health practices and regulations, the respondents were optimistic that the government, farmers, consumers, and feed venders were slightly concerned about AMR (Figure 4). Respondents representing OH training institutions mostly indicated inclusion of AMU and AMR related subjects in the training and research institutions with 72.7% indicating the existence on AMR related curriculum (Table 8). Client expectations and family members were reported to have limited influence on prescription of antimicrobials by most of respondents (Figure 4).
3. Discussion
3.1. Farmers
In this work, we have evaluated the knowledge, attitudes, practices, and perceptions of livestock stakeholders (farmers, animal health service providers, and other One Health practitioners) on antimicrobial use in Kenya. The profile of evaluated stakeholders spread across levels of education and years of empirical practice. In addition, most of the farmers practice mixed livestock and crop production. Most farmers in developing countries practice mixed farming, and rarely specialize on single production system for their livestock, this method is suitable for small scale farmers as it spreads the risk of production failures and challenges across various livestock species and crops [16,17]. Such practices can promote spread of livestock diseases from one species to another and hinders specialization which leads to increased production [18]. It is observed that the level of education and the farming experience seemed to influence disease prevention practices on farm; similarly, various studies have found that education improves decision-making skills of farmers [19,20]. Furthermore, a study conducted in Ghana noted that farmers with more than 10 years of farming experience were more likely to administer antibiotics to their animals [21]. The practice of treating own animals with antibiotics been associated to the low number of veterinary professionals against the number of live animals. The inaccessibility of professionals together with associated costs incurred by the farmer have been indicated as some of the reasons farmers resort to treating their own sick animals, findings that have been reported in other studies [22,23].
Most farmers have heard of AMR mostly through friends, workshops, and the radio, and animal health professionals were observed to be the least common source of information on AMR to farmers. This observation can be related to the fact that most farmers do not have access to animal health professionals who have been reported to be either low in numbers or inaccessible to low-income farmers due to high treatment costs [22,24]. Despite knowing about the existence of AMR, only a few farmers could clearly describe what causes AMR, including overuse of antimicrobials, unnecessary use and failure to complete the dosage when animal is undergoing treatment due to some improvement [25]. The use on antimicrobials at the farm level has been shown to correlate directly to the good agricultural practices and adherence to livestock vaccination schedules, with farmers not observing such practices likely to overuse and abuse antimicrobials hence promoting AMR [24]. Farmers raised concerned about their animals and family members acquiring AMR, and failure of animals to recover from illnesses. Farmers have perceived antibiotic resistance as a possibly catastrophic risk that would need continuing risk assessment and management to safeguard animals and their livelihoods [26].
In our study, farmers mostly sourced their antimicrobials from agro-veterinary shops (49.0%) and from veterinary professionals (47.0%), and some farmers (63.7%) stated that obtain prescriptions before buying antimicrobials. This study reports a higher proportion of farmers that acquire prescription than other studies that have stated as low as 8-12% compliance with acquiring prescriptions for antimicrobials [22,27,28]. Despite the above finding, over 68% of the farmers reported to store expired or left over medicine, possibly for future use, a finding that shows poor adherence to good antibiotic use practices [22,23,27,28]. Some farmers reported to use alternative herbal medicines. The use of herbal medicine and other alternative African traditional medicine have been applied both to livestock and human with reported recoveries from common illnesses [29,30]. The involvement of alternative medicine can reduce consumption of antimicrobials thus decreasing selective pressure for AMR emergence. However, more research focus should be directed towards identification of active ingredients, dosage and possible side effects of these alternative medicines [31].
Farmers relied on agro-veterinary shops’ recommendations for antimicrobial administration, quality assurance, and for checking of the expiry dates before purchase. Whether this is enough is doubtful, as agro-veterinary shops are traders who may be motivated by profits. Quality assurance of antimicrobials used in animals and human is a critical control point, which help in curbing AMR through assurances for potency and efficiency [32] and must be taken seriously. Antimicrobials were administered by farmers through injections while mixing with water and other liquids before administration was also a common delivery method. Self-administration of drugs including antibiotics to animals without prescription has been considered one of the main drivers to AMR [33,34,35]. The use of antimicrobials to treat FMD, Newcastle disease in chicken among other viral diseases were practiced (Table 3). Such diseases can easily be managed through adequate vaccination program, and this will reduce the cost of antimicrobials and the emergence of AMR. Poor farming practices including lack of adherence to vaccination and biosecurity guidelines, which have been shown to promote overreliance of antimicrobials [36,37].
Record keeping has been used as a tool which aides in evaluation of livestock enterprises and assisting in decision making [38,39,40]. In our study, record keeping was low for livestock population, sales at the farm, vaccination, antimicrobials use and disinfection. Almost one-fifth of respondents kept no records. Poor record keeping behaviors among the small-scale farmers can be attributed to low education levels, insufficient awareness and information [38,39,40]. Poor record on farm record keeping is an impediment to monitoring on farm antimicrobial consumption [41,42].
3.2. Animal Health Service Providers (AHSP)
Despite 47 veterinary professionals responding, there was low number of respondents who managed to complete the data collection tool and gave adequate information (63.8%). This was attributed to data collection method (use of social media or email addresses) to access the respondents rather than physical evaluation. It should be understood that the evaluation was conducted at a time when COVID-19 restriction was still in Kenya, and the electronic method was the best system to carry out the survey. Our findings reveal greater familiarity amongst animal health professionals with terminologies related to antibiotic resistance, a finding that has been reported in previous study in Kenya [43]. The good knowledge and awareness of AMR by the respondents, as observed in our study can be attributed to the increasing sharing of information on antimicrobial use and AMR through trainings, workshops and the various AMR awareness activities that have been carried out in the country [15,27,44,45].
The response from farmers on the consult with agro-veterinary shops and veterinary professionals is good for antimicrobial stewardship. Animal health professionals are expected to issue prescription whenever antimicrobial is indicated for management of livestock diseases [46,47]. In addition, animal health professionals are routinely and directly involved in antimicrobial use on the farm [46,47,48]. The need for professionals to strictly follow clear guidelines and standardized regulations regarding prescription of antimicrobials is obvious [49,50,51]. The survey demonstrates good knowledge on antimicrobials and AMR among the animal health professionals. We relate this to ongoing AMR awareness and the fact that most respondents were young adults who left collage recently, as observed in other studies [2,15,28].
We observed various practices concerning the application of antibiotics against common livestock diseases which are caused by viruses. This suggests vaccines are underused among the animal health professionals or the farmers are not adequately informed. Increasing livestock vaccination has been identified as one of major actions which will reduce antimicrobial use and the resultant burden of AMR [36,52,53]. The practice and implementation of prescription of antimicrobials have been slowly implemented in developing countries including Kenya [28,49,54,55]. The practice of selling antimicrobials and antibiotics without prescription can be related to weak regulation of antimicrobial sales and use in such countries. Finally, veterinary professionals have relied on personal experience, peers, laboratory sensitivity test results, ease of administration and availability of a given type of antimicrobial [28,56]. Poor or weak regulation makes access to antimicrobials easy to all those in need hence the feel by professionals/animal health service providers on lack of mandatory need to prescribe.
3.3. University, Research and One Health Partners
We observed high levels of knowledge, understanding and description of AMR among the One Health practitioners and partners. These levels make sense as a majority have been in practice for over 15 years, have post graduate educations, have good level of knowledge of antimicrobials and practice stewardship of antimicrobials. Their responses, which were influenced by their individual perceptions and exposure, were positive in mitigating antimicrobials and their concerns were apt. These individuals can become facilitators of good practices and training on antimicrobial stewardship among producers, consumers, and at various levels of government regulators. The awareness surveys not only provide further information regarding the concerns of various players, but it also aids in increasing awareness towards AMR hence implementing the national action plans. AMR being an all-inclusive issue which affects animals, humans and environment will have its impact felt by various stakeholders hence the need for all-inclusive approach in handling it, as envisaged in various action plans [15,28,44,54].
These categories of professionals have also undergone many trainings, with inclusion of AMU and AMR related subjects, and inclusion in curriculums taught in the institutions, especially microbiology, public health, and AMR short courses. Research primarily covered areas of food safety, antimicrobial surveillance, AMR mechanisms and outcomes in populations and environment.
This work is subject to certain limitations hence, it should be interpreted thoughtfully for this reason. Firstly, the study is reporting perspectives, knowledge and attitudes of various groups where even though careful consideration was taken to ensure a wider sample size, bias might have been introduced. In addition, since this is descriptive cross-sectional design, factors associated with knowledge, attitude, perspectives, and practice of the participants were not independently established or looked at.
4. Materials and Methods
4.1. Survey Design
A cross-sectional survey was carried out in August 2021 where livestock farmers, animal health service providers and One Health practitioners were respondents.
4.2. Sample Size Determinations
To get the minimum number of farmers to be enrolled for the survey, Cochran formula was used with expected favorable attitude and practices set at 50% and 5% margin of error. The sample size for farmers was 384. Animal health service providers were enrolled nationwide, by sharing of data collection tool through emails and social media platforms where membership are animal health service providers. One Health practitioners were enrolled based on their position and role at various institutions implementing One Health. Such institutions were those doing research, training, diagnostics, government departments of health and animal health and government regulatory bodies. Persons in charge of One Health activities at the institutions were enrolled into the survey.
4.3. Survey Population
The survey was conducted among 381 livestock farmers, 47 animal health service providers, 32 One Health practitioners. Farmers considered for the study are those consenting and must have been practicing livestock farming in the respective county for atleast one year, while animal health service providers who consented to take part in the study were enrolled. One Health practitioners from identified institutions and were heads of the One Health related activities or their assigned replacements were included in the survey.
4.4. Survey Procedure
Farmers were enrolled three counties in Kenya, while considering counties regarded as largely small scale, large scale, and pastoralist regarding livestock farming practices. Busia, Nakuru and Isiolo counties were purposively picked to represent the three categories respectively. The sample size for farmers was divided equally in the three counties giving a minimum sample size of 128 per county. In each county, one sub county was selected randomly for the survey. Central locations were established in the sub county with help from sub county veterinary officer, which was considered starting point for the enrollment of the farmer participants. The central locations were office of the sub county veterinary offices, shopping centers, livestock auction yards, chief’s office or local administrator’s office and livestock watering points. Four starting points were identified at the sub county, in which 32 farmers were targeted. From the starting point, the first farmer household directly Infront of main entrance was enrolled, and enumerators continue on possible straight line while skipping 10 farmer households until the sample size for the starting point was reached.
Contacts for animal health service providers were obtained from Kenya veterinary board published 2021 register where email addresses and phone numbers were captured. Data collection tool was shared to respondents through email addresses and link created which was sent through social media platforms including group email platforms and WhatsApp and Facebook social platforms. Contacts and Email addresses of office holders of One Health practitioners were sought, and data collection tool shared.
A set of three questionnaires were developed and validated at Food and Agriculture Organization of the United Nations (FAO) for each category of participants. The questions were digitized and placed on an online platform, and links to the digitized questionnaires were shared with participants through direct emails, social media access, and mailing groups. In some instances, the questionnaires were administered through direct phone calls for individuals without access to the online platforms. Data from farmers were collected by trained enumerators drawn from the respective office of the county director of veterinary services through a face-to-face interview. All the responses were captured in the regional digital data collection tool developed by FAO. Data was downloaded into Microsoft Excel spreadsheet for cleaning and coding. Analysis was done using MS excel and Epi Info software. Descriptive statistics were performed by calculating frequencies and proportions in percentages. Analysis was also conducted to assess how demographic factors, farming systems influence knowledge, attitude and practices with significant factors having p=<0.05.
The participants taken through informed consent, before questionnaire was administered. This work was part of an approved workplan under the Fleming fund project under FAO/Government of the Republic of Kenya cooperative agreement (GCP/GLO/710/UK), and it is within the mandate of the Ministry of Agriculture and Livestock Development (MoALD), Kenya.
5. Conclusions
In the present study, farmers mostly rely on agro-veterinary shop service providers for information and choice of antimicrobial/antibiotic to buy. However, AHSP are the least common source of information to farmers regarding AMR with farmers expressing poor knowledge of AMR. Most farmers and animal health providers did not keep records on antimicrobials prescribed and/or used. AHSP prescribed antimicrobials mostly for treatment of FMD in cattle and Newcastle disease in chicken. It is possible that this was done to control possible secondary bacterial infections however both diseases are viral and vaccine preventable.
To promote good AMU practices, AHSP service providers should be at the forefront creating awareness to farmers on the dangers of AMR. ASHP should also advise farmers on vaccinating their animals among other preventive measures to reduce the need for antimicrobials for preventable diseases.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Livestock kept, and Crops grown by the farmers and diseases observed in the farm in the last one year.
Author Contributions
Conceptualization, J.O., M.A.C., T.K., and S.K.; methodology, J.O., M.A.C., T.K., and S.K.; software, J.O., and F.O.F.; validation, R.O., and F.O.F.; formal analysis, J.O., R.O., and F.O.F.; investigation, J.O.; resources, J.O., R.O., T.K., S.K., and F.O.F.; data curation, J.O., R.O., M.A.C., and F.O.F.; writing—original draft preparation, J.O., R.O., and F.O.F.; writing—review and editing, R.O., and F.O.F.; visualization, F.O.F.; supervision, T.K., S.K., and F.O.F.; project administration, R.O., T.K., S.K., and F.O.F.; funding acquisition, T.K., and S.K.. All authors have read and agreed to the published version of the manuscript.
Funding
Government of the United Kingdom of Great Britain and Northern Ireland under the Fleming Fund project (GCP/GLO/710/UK), and the APC was funded by the United Nations Development Programme Joint Donor Trust Fund, grant number UNJP/KEN/099/UNJ.
Institutional Review Board Statement
under the Fleming Fund project under FAO/Government of the Republic of Kenya co-operative agreement (GCP/GLO/710/UK), and it is within the mandate of the Ministry of Agriculture and Livestock Development (MoALD), Kenya, hence no specific ethical approval was required.
Informed Consent Statement
Participants’ consent was given as per the Section 25 – 32 of the World Medical Association’s Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects (https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/). All participants gave their informed consent and know their right to participate or withdraw from the study.
Data Availability Statement
The datasets are available from the corresponding author upon reasonable request. All data belong to the Ministry of Agriculture and Livestock Development (MoALD), Kenya.
Acknowledgments
The authors extend their heartfelt thanks to the respondents who took time to respond to the questionnaire. We acknowledge the contributions of the County governments of Busia, Isiolo and Nakuru for permitting this study to be conducted. Finally, the funder through which resources were available to support this study is gratefully acknowledged.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial resistance: a global multifaceted phenomenon. Pathog. Glob. Health 2015, 109, 309–318. [Google Scholar] [CrossRef]
- Joshi, M.P.; Hafner, T.; Twesigye, G.; Ndiaye, A.; Kiggundu, R.; Mekonnen, N.; et al. Strengthening multisectoral coordination on antimicrobial resistance: a landscape analysis of efforts in 11 countries. J Pharm Policy Pract 2021, 14, 27. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- Wernli, D.; Harbarth, S.; Levrat, N.; Pittet, D. A ‘whole of United Nations approach’ to tackle antimicrobial resistance? A mapping of the mandate and activities of international organisations. BMJ Glob. Health 2022, 7, e008181. [Google Scholar] [CrossRef]
- Gajdács, M.; Urbán, E.; Stájer, A.; Baráth, Z. Antimicrobial Resistance in the Context of the Sustainable Development Goals: A Brief Review. Eur J Investig Health Psychol Educ 2021, 11, 71–82. [Google Scholar] [CrossRef]
- Jasovský, D.; Littmann, J.; Zorzet, A.; Cars, O. Antimicrobial resistance-a threat to the world’s sustainable development. Ups J Med Sci 2016, 121, 159–164. [Google Scholar] [CrossRef]
- Dadgostar, P. Antimicrobial Resistance: Implications and Costs. Infect Drug Resist 2019, 12, 3903–3910. [Google Scholar] [CrossRef] [PubMed]
- Founou, L.L.; Founou, R.C.; Essack, S.Y. Antimicrobial resistance in the farm-to-plate continuum: more than a food safety issue. Future Sci 2021, OA 7, FSO692. [Google Scholar] [CrossRef]
- Iskandar, K.; Molinier, L.; Hallit, S.; Sartelli, M.; Hardcastle, T.C.; Haque, M.; et al. Surveillance of antimicrobial resistance in low- and middle-income countries: a scattered picture. Antimicrob Resist Infect Control 2021, 10, 63. [Google Scholar] [CrossRef]
- Pokharel, S.; Raut, S.; Adhikari, B. Tackling antimicrobial resistance in low-income and middle-income countries. BMJ Glob Health 2019, 4, e002104. [Google Scholar] [CrossRef]
- Sulis, G.; Sayood, S.; Gandra, S. Antimicrobial resistance in low- and middle-income countries: current status and future directions. Expert Rev Anti Infect Ther 2022, 20, 147–160. [Google Scholar] [CrossRef] [PubMed]
- Bett, B. Situation analysis on antimicrobial resistance surveillance and control in Kenya Antimicrobial Resistance Research Hub, 2018, [WWW Document]. URL https://amr.cgiar.org/case-study/situation-analysis-antimicrobial-resistance-surveillance-and-control-kenya (accessed 07.02.2022).
- Maina, M.; Mwaniki, P.; Odira, E.; Kiko, N.; McKnight, J.; Schultsz, C.; et al. Antibiotic use in Kenyan public hospitals: Prevalence, appropriateness and link to guideline availability. Int J Infect Dis 2020, 99, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.A.; Vlieghe, E.; Mendelson, M.; Wertheim, H.; Ndegwa, L.; Villegas, M.V.; et al. Antibiotic stewardship in low- and middle-income countries: the same but different? Clin Microbiol Infect 2017, 23, 812–818. [Google Scholar] [CrossRef] [PubMed]
- Wesangula, E.N.; Githii, S.; Ndegwa, L. Implementing the national action plan on antimicrobial resistance in Kenya: Global expectations, national realities. Int J Infect Dis 2020, 101, 41. [Google Scholar] [CrossRef]
- Herrero, M.; Grace, D.; Njuki, J.; Johnson, N.; Enahoro, D.; Silvestri, S.; Rufino, M. The roles of livestock in developing countries. Anim 2012, 7, 1–16. [Google Scholar] [CrossRef]
- Thornton, P.K.; Rosenstock, T.; Förch, W.; Lamanna, C.; Bell, P.; Henderson, B.; Herrero, M. A Qualitative Evaluation of CSA Options in Mixed Crop-Livestock Systems in Developing Countries, in: Lipper, L.; McCarthy, N., Zilberman, D., Asfaw, S., Eds.; Branca, G. (Eds.), Climate Smart Agriculture : Building Resilience to Climate Change, Natural Resource Management and Policy. Springer International Publishing, Cham, 2018; pp. 385–423. [Google Scholar] [CrossRef]
- Salaheen, S.; Chowdhury, N.; Hanning, I.; Biswas, D. Zoonotic bacterial pathogens and mixed crop-livestock farming. Poult Sci 2015, 94, 1398–1410. [Google Scholar] [CrossRef]
- Ninh, L.K. Economic role of education in agriculture: evidence from rural Vietnam. J Econ Dev 2020, 23, 47–58. [Google Scholar] [CrossRef]
- Paltasingh, K.R.; Goyari, P. Impact of farmer education on farm productivity under varying technologies: case of paddy growers in India. Agric Food Econ 2018, 6, 7. [Google Scholar] [CrossRef]
- Phares, C.A.; Danquah, A.; Atiah, K.; Agyei, F.K.; Michael, O.-T. Antibiotics utilization and farmers’ knowledge of its effects on soil ecosystem in the coastal drylands of Ghana. PLoS ONE 2020, 15, e0228777. [Google Scholar] [CrossRef]
- Caudell, M.A.; Dorado-Garcia, A.; Eckford, S.; Creese, C.; Byarugaba, D.K.; Afakye, K.; et al. Towards a bottom-up understanding of antimicrobial use and resistance on the farm: A knowledge, attitudes, and practices survey across livestock systems in five African countries. PLoS ONE 2020, 15, e0220274. [Google Scholar] [CrossRef]
- Mouiche, M.M.M.; Moffo, F.; Betsama, J.D.B.; Mapiefou, N.P.; Mbah, C.K.; Mpouam, S.E.; et al. Challenges of antimicrobial consumption surveillance in food-producing animals in sub-Saharan African countries: Patterns of antimicrobials imported in Cameroon from 2014 to 2019. J Glob Antimicrob Resist 2020, 22, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Afakye, K.; Kiambi, S.; Koka, E.; Kabali, E.; Dorado-Garcia, A.; Amoah, A.; et al. The Impacts of Animal Health Service Providers on Antimicrobial Use Attitudes and Practices: An Examination of Poultry Layer Farmers in Ghana and Kenya. Antibiotics 2020, 9, 554. [Google Scholar] [CrossRef] [PubMed]
- Kemp, S.A.; Pinchbeck, G.L.; Fèvre, E.M.; Williams, N.J. A Cross-Sectional Survey of the Knowledge, Attitudes, and Practices of Antimicrobial Users and Providers in an Area of High-Density Livestock-Human Population in Western Kenya. Front Vet Sci 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Doidge, C.; Ruston, A.; Lovatt, F.; Hudson, C.; King, L.; Kaler, J. Farmers’ Perceptions of Preventing Antibiotic Resistance on Sheep and Beef Farms: Risk, Responsibility, and Action. Front Vet Sci 2020, 7. [Google Scholar] [CrossRef] [PubMed]
- Adekanye, U.O.; Ekiri, A.B.; Galipó, E.; Muhammad, A.B.; Mateus, A.; La Ragione, R.M.; et al. Knowledge, Attitudes and Practices of Veterinarians towards Antimicrobial Resistance and Stewardship in Nigeria. Antibiotics 2020, 9, E453. [Google Scholar] [CrossRef]
- Mangesho, P.E.; Caudell, M.A.; Mwakapeje, E.R.; Ole-Neselle, M.; Kimani, T.; Dorado-García, A.; et al. Knowing Is Not Enough: A Mixed-Methods Study of Antimicrobial Resistance Knowledge, Attitudes, and Practises among Maasai Pastoralists. Front Vet Sci 2021, 8. [Google Scholar] [CrossRef]
- Aziz, M.A.; Khan, A.H.; Adnan, M.; Ullah, H. Traditional uses of medicinal plants used by Indigenous communities for veterinary practices at Bajaur Agency, Pakistan. J Ethnobiol Ethnomedicine 2018, 14, 11. [Google Scholar] [CrossRef]
- Jayakumar, S.; Baskaran, N.; Arumugam, R.; Sathiskumar, S.; Pugazhenthi, M. Herbal medicine as a live practice for treating livestock ailments by indigenous people: A case study from the Konar community of Tamil Nadu. South Afr J Bot 2018, 118, 23–32. [Google Scholar] [CrossRef]
- Howland, O. Patterns of use, gathering, processing and administration of herbal and alternative medicines among people and livestock in Kenya: a study of local knowledge for One Health. J Glob Health Rep 2021, 5, e2021042. [Google Scholar] [CrossRef]
- Quynh, H.L.; Bich, T.N.T.; Hoang, L.T.; Erickson, V.I.; Padungtod, P. Quality testing of veterinary antimicrobial products used for livestock in Vietnam, 2018–2019. PLoS ONE 2021, 16, e0247337. [Google Scholar] [CrossRef]
- Alhaji, N.B.; Isola, T.O. Antimicrobial usage by pastoralists in food animals in North-central Nigeria: The associated socio-cultural drivers for antimicrobials misuse and public health implications. One Health 2018, 6, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Azabo, R.; Mshana, S.; Matee, M.; Kimera, S.I. Antimicrobial usage in cattle and poultry production in Dar es Salaam, Tanzania: pattern and quantity. BMC Vet Res 2022, 18, 7. [Google Scholar] [CrossRef] [PubMed]
- Gemeda, B.A.; Amenu, K.; Magnusson, U.; Dohoo, I.; Hallenberg, G.S.; Alemayehu, G.; et al. Antimicrobial Use in Extensive Smallholder Livestock Farming Systems in Ethiopia: Knowledge, Attitudes, and Practices of Livestock Keepers. Front Vet Sci 2020, 7. [Google Scholar] [CrossRef]
- Hoelzer, K.; Bielke, L.; Blake, D.P.; Cox, E.; Cutting, S.M.; Devriendt, B.; et al. Vaccines as alternatives to antibiotics for food producing animals. Part 1: challenges and needs. Vet Res 2018, 49, 64. [Google Scholar] [CrossRef] [PubMed]
- Raasch, S.; Postma, M.; Dewulf, J.; Stärk, K.D.C.; Grosse Beilage, E. Association between antimicrobial usage, biosecurity measures as well as farm performance in German farrow-to-finish farms. Porc Health Manag 2018, 4, 30. [Google Scholar] [CrossRef] [PubMed]
- Gichohi, P. The role of record keeping and maintenance in enhancing decision making among smallholder dairy farmers in Gitugi Ward in Murang’a County, Kenya. Inf Dev 2019, 36, 026666691987972. [Google Scholar] [CrossRef]
- Kuteesa, A.; Kyotalimye, M. Documentation and data handling: How can Africa promote record keeping and investment in data management? Afr J Food Agric Nutr Dev 2019, 19, 14171–14189. [Google Scholar] [CrossRef]
- Tham-Agyekum, E.; Appiah, P.; Nimoh, F. Assessing Farm Record Keeping Behaviour among Small-Scale Poultry Farmers in the Ga East Municipality. J Agric Sci 2010, 2. [Google Scholar] [CrossRef]
- Cuong, N.V.; Phu, D.H.; Van, N.T.B.; Dinh Truong, B.; Kiet, B.T.; Hien, B.V.; et al. High-Resolution Monitoring of Antimicrobial Consumption in Vietnamese Small-Scale Chicken Farms Highlights Discrepancies Between Study Metrics. Front Vet Sci 2019, 6, 174. [Google Scholar] [CrossRef]
- Schar, D.; Sommanustweechai, A.; Laxminarayan, R.; Tangcharoensathien, V. Surveillance of antimicrobial consumption in animal production sectors of low- and middle-income countries: Optimizing use and addressing antimicrobial resistance. PLoS Med 2018, 15, e1002521. [Google Scholar] [CrossRef]
- Muloi, D.; Fèvre, E.M.; Bettridge, J.; Rono, R.; Ong’are, D.; Hassell, J.M.; et al. A cross-sectional survey of practices and knowledge among antibiotic retailers in Nairobi, Kenya. J Glob Health 2019, 9, 020412. [Google Scholar] [CrossRef] [PubMed]
- Fasina, F.O.; LeRoux-Pullen, L.; Smith, P.; Debusho, L.K.; Shittu, A.; Jajere, S.M.; et al. Knowledge, Attitudes, and Perceptions Associated With Antimicrobial Stewardship Among Veterinary Students: A Multi-Country Survey From Nigeria, South Africa, and Sudan. Front Public Health 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Rahman, Md.S.; Rafa, N. Common Barriers, Attitudes and Practices of Veterinary Practitioners Regarding Antimicrobial Resistance and Stewardship in Bangladesh. Open Vet Sci 2021, 1, 72–80. [Google Scholar] [CrossRef]
- Odoi, A.; Samuels, R.; Carter, C.N.; Smith, J. Antibiotic prescription practices and opinions regarding antimicrobial resistance among veterinarians in Kentucky, USA. PLoS ONE 2021, 16, e0249653. [Google Scholar] [CrossRef]
- Tebug, S.F.; Mouiche, M.M.M.; Abia, W.A.; Teno, G.; Tiambo, C.K.; Moffo, F.; Awah-Ndukum, J. Antimicrobial use and practices by animal health professionals in 20 sub-Saharan African countries. Prev Vet Med 2021, 186, 105212. [Google Scholar] [CrossRef] [PubMed]
- Aworh, M.K.; Kwaga, J.K.P.; Okolocha, E.C. Assessing knowledge, attitude, and practices of veterinarians towards antimicrobial use and stewardship as drivers of inappropriate use in Abuja, Nigeria. One Health Outlook 2021, 3, 25. [Google Scholar] [CrossRef]
- Chema, S.; Gathuma, J.M. Kenya: The development of private services and the role of the Kenya Veterinary Association. Rev Sci Tech Int Off Epizoot 2004, 23, 331–40; discussion 391. [CrossRef]
- Heffernan, C.; Misturelli, F. The Delivery of Veterinary Services to the Poor: Preliminary findings from Kenya. 2002, available at: https://assets.publishing.service.gov.uk/media/57a08d2aed915d3cfd001868/R7359a.pdf, (16.04.2023). 2023.
- Jaime, G.; Hobeika, A.; Figuié, M. Access to Veterinary Drugs in Sub-Saharan Africa: Roadblocks and Current Solutions. Front Vet Sci 2022, 8, 558973. [Google Scholar] [CrossRef]
- Micoli, F.; Bagnoli, F.; Rappuoli, R.; Serruto, D. The role of vaccines in combatting antimicrobial resistance. Nat Rev Microbiol 2021, 19, 287–302. [Google Scholar] [CrossRef]
- Vekemans, J.; Hasso-Agopsowicz, M.; Kang, G.; Hausdorff, W.P.; Fiore, A.; Tayler, E.; et al. Leveraging Vaccines to Reduce Antibiotic Use and Prevent Antimicrobial Resistance: A World Health Organization Action Framework. Clin Infect Dis 2021, 73, e1011–e1017. [Google Scholar] [CrossRef]
- ReAct. AMR stakeholder mapping From ReAct Europe – Action on Antibiotic Resistance, 2016. Available at: https://www.reactgroup.org/uploads/Stakeholder%20Analysis_ReActForWHO.pdf, (16.04.2023). 2023.
- Meseko, C.; Olabisi, M.; Ehizibolo, D.; Muraina, I. Veterinary Pharmaceuticals and Antimicrobial Resistance in Developing Countries. In: Veterinary Medicine and Pharmaceuticals, Bekoe, S.O.; Saravanan, M.; Adosraku, R.K.; Ramkumar, P.K. IntechOpen Publisher (https://www.intechopen.com/) 2019. [CrossRef]
- De Briyne, N.; Atkinson, J.; Pokludová, L.; Borriello, S.P.; Price, S. Factors influencing antibiotic prescribing habits and use of sensitivity testing amongst veterinarians in Europe. Vet Rec 2013, 173, 475. [Google Scholar] [CrossRef]
Figure 1.
Assessment of farmers’ knowledge on antimicrobial resistance.
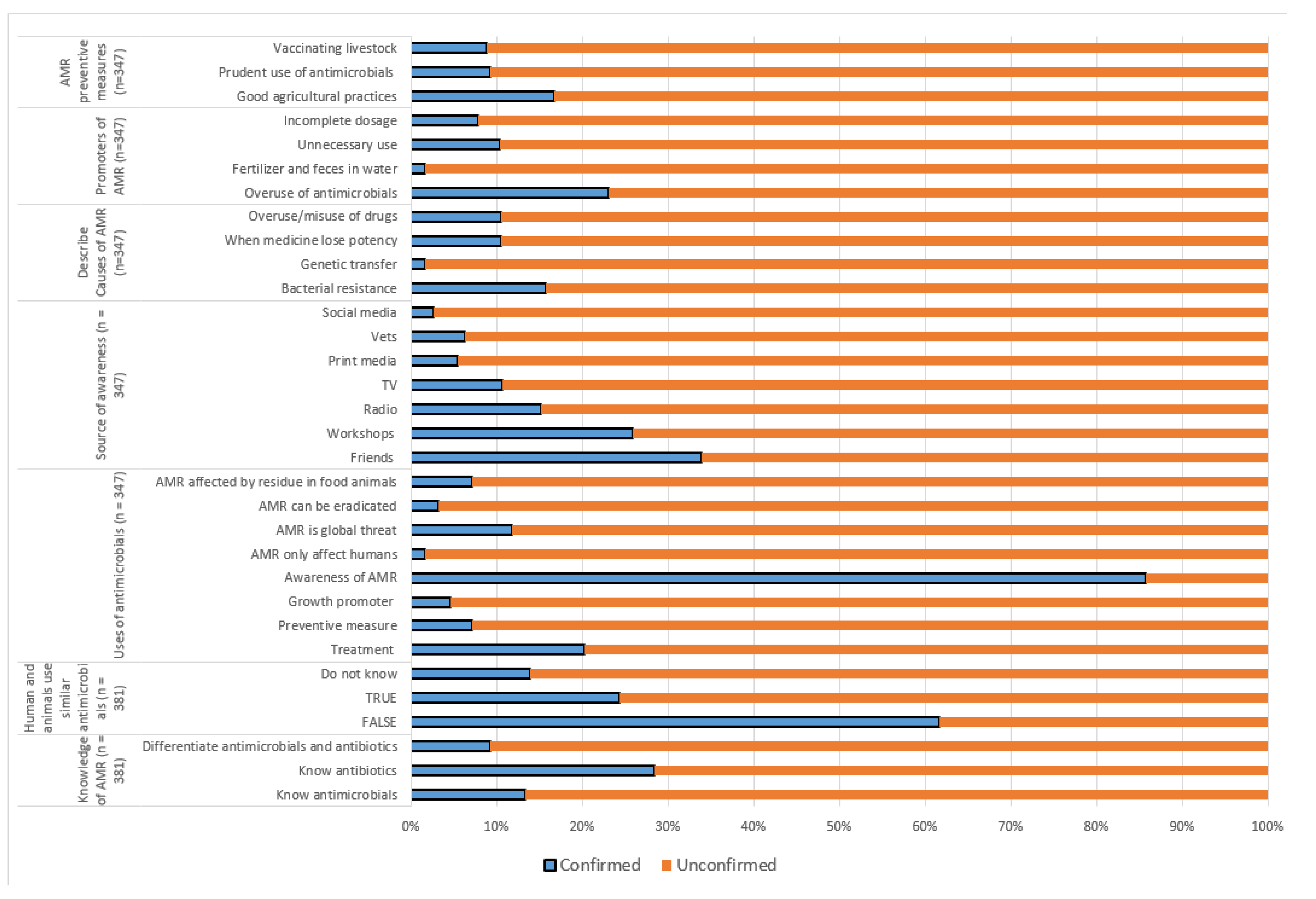
Figure 2.
Assessment of farmers’ perceptions on antimicrobial resistance (n = 355).
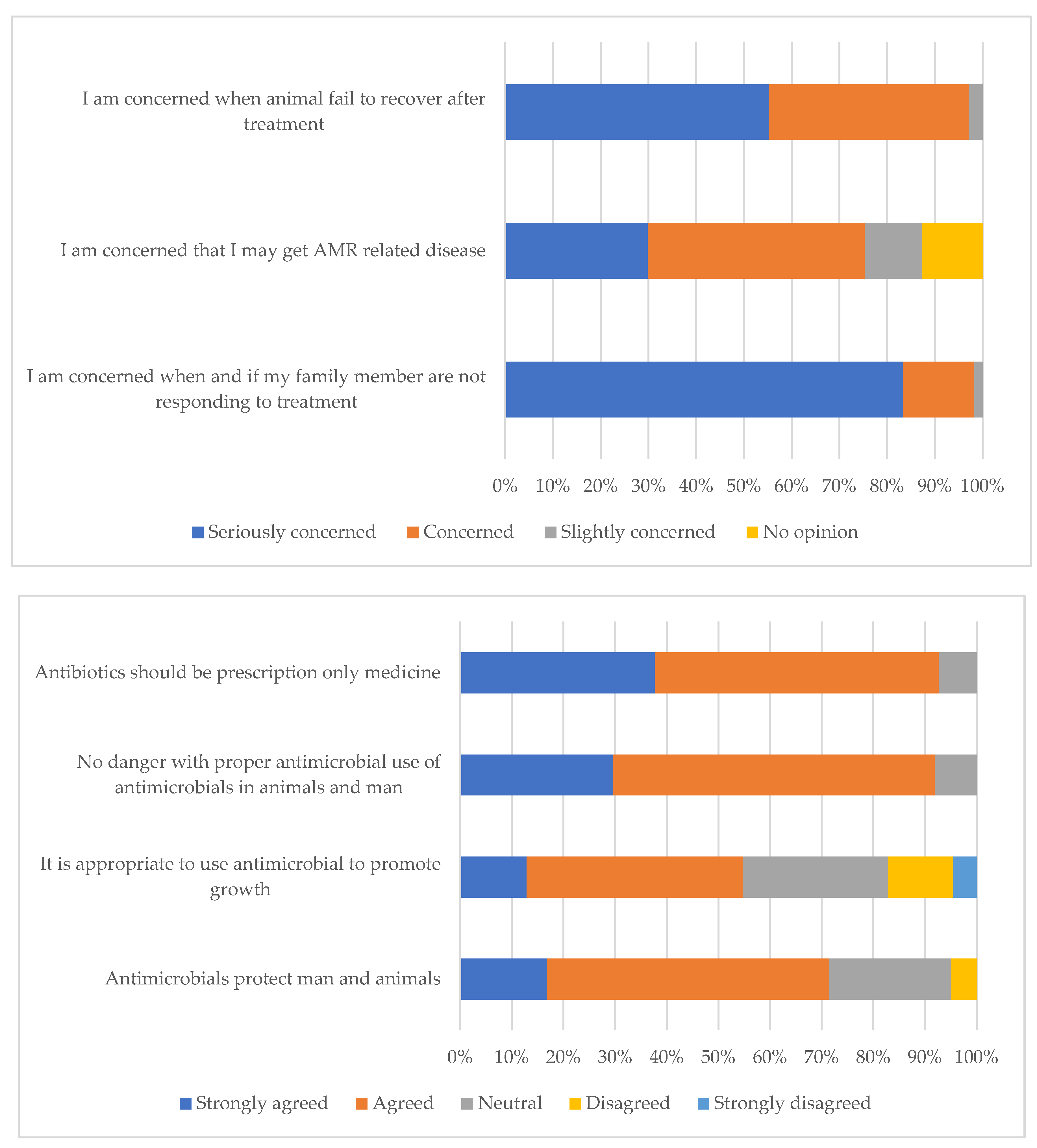
Figure 3.
Antimicrobial use and factors that influence antimicrobial prescription among veterinary professionals.
Figure 3.
Antimicrobial use and factors that influence antimicrobial prescription among veterinary professionals.
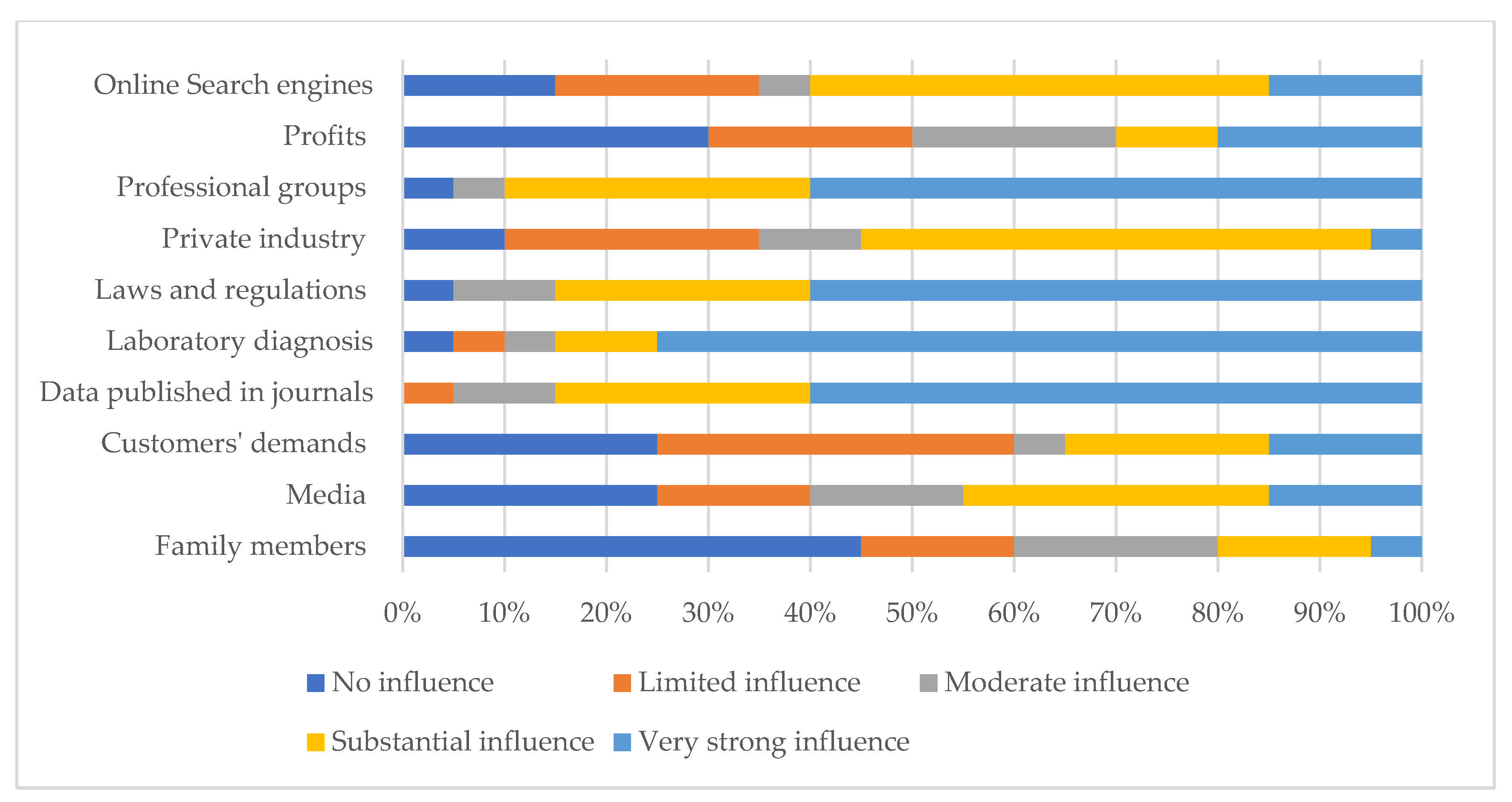
Figure 4.
Perceptions and concerns of research and One Health institutions and partners regarding antimicrobial resistance.
Figure 4.
Perceptions and concerns of research and One Health institutions and partners regarding antimicrobial resistance.
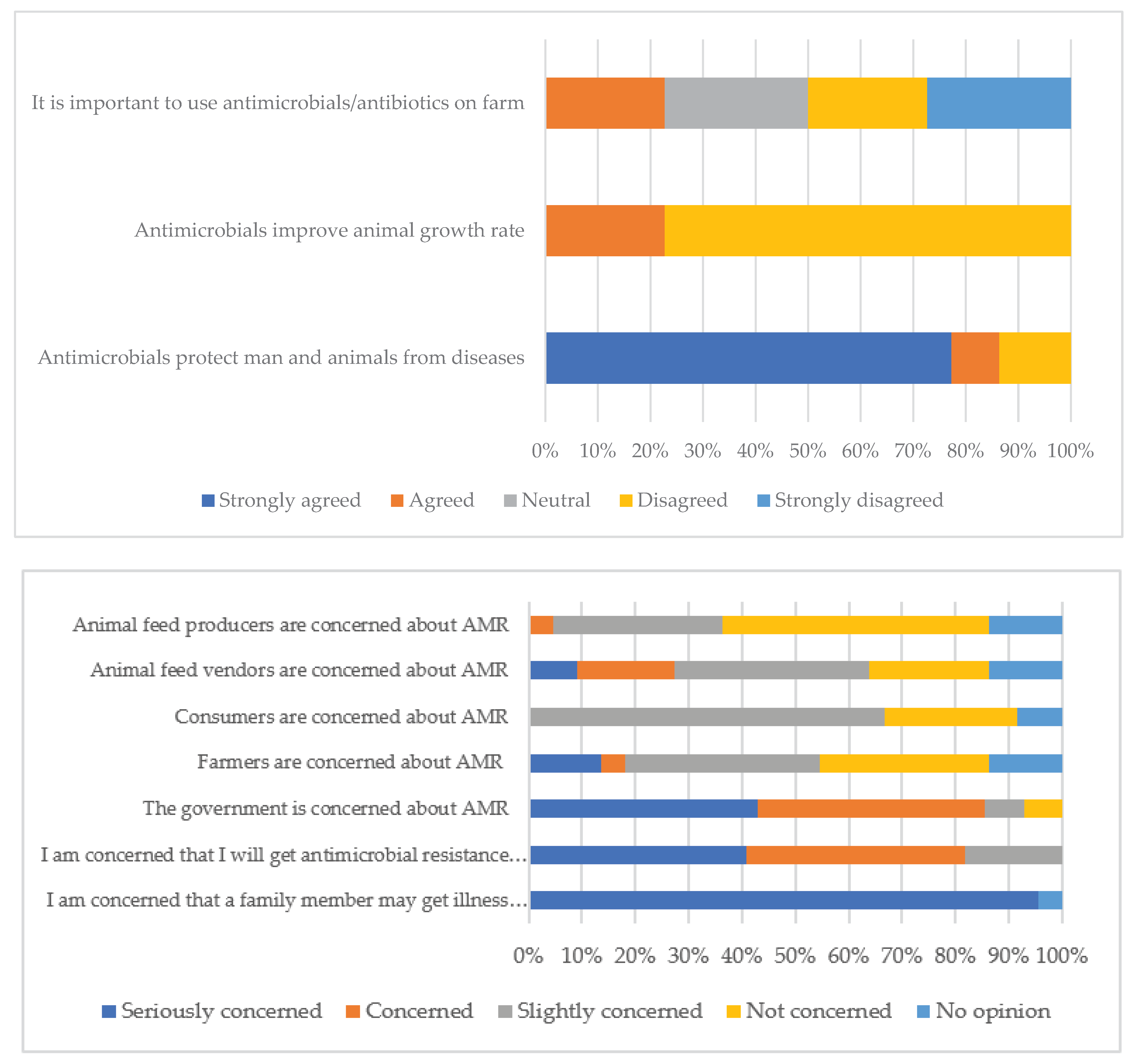

Table 1.
Demographic characteristics of the respondents.
| Parameters | Farmers n (%) |
Animal health service providers n (%) |
One Health professionals/ training institutions n (%) |
|---|---|---|---|
| Gender | |||
| Male | 249 (65.3) | 36 (76.6) | 17 (53.1) |
| Female | 132 (34.7) | 11 (23.4) | 15 (46.9) |
| Age Groups | |||
| < 20 | 3 (0.8) | 21 (44.7) | 0 (0.0) |
| 20 – 29 | 76 (20.0) | 14 (36.2) | 14 (43.8) |
| 30 – 39 | 117 (30.7) | 7 (14.9) | 4 (12.5) |
| 40 – 49 | 117 (30.7) | 3 (6.4) | 9 (28.1) |
| 50 – 59 | 54 (14.3) | 2 (4.3) | 2 (6.3) |
| ≥ 60 | 14 (3.7) | 0 (0.0) | 3 (9.4) |
| Level of Education | |||
| None | 115 (30.2) | 0 (0.0) | 0 (0.0) |
| Primary | 65 (17.1) | 0 (0.0) | 0 (0.0) |
| Secondary | 121 (31.8) | 0 (0.0) | 0 (0.0) |
| Diploma | 32 (8.4) | 5 (10.6) | 1 (3.1) |
| Degree | 41 (10.8) | 24 (51.1) | 16 (50.0) |
| Masters/PhD | 7 (1.9) | 18 (38.3) | 15 (46.9) |
| Years of experience in the livestock value chain | |||
| < 1 | 20 (5.3) | 2 (4.3) | 6 (18.8) |
| 1 – 5 | 166 (43.6) | 23 (48.7) | 9 (28.1) |
| 6 – 10 | 60 (15.8) | 8 (17.0) | 3 (9.4) |
| 11 – 15 | 52 (13.7) | 7 (14.9) | 5 (15.6) |
| > 15 | 83 (21.8) | 7 (14.9) | 9 (28.1) |
Table 2.
Farmers’ preferred animal diseases prevention and treatment methods based on farmers’ level of education and years of farming experience.
Table 2.
Farmers’ preferred animal diseases prevention and treatment methods based on farmers’ level of education and years of farming experience.
| Characteristics | Level of education | Years of farming experience | |||||||
|---|---|---|---|---|---|---|---|---|---|
| No formal (n = 115) (%) | Basic (n = 186) (%) | Tertiary (n = 80) (%) | < 1 (n = 20) (%) | 1 – 5 (n = 166) (%) | 6 – 10 (n = 60) (%) | 11 – 15 (n = 52) (%) | > 15 (n = 83) (%) | ||
| Prevention of diseases at the farm | |||||||||
| Practice farm hygiene | 86 (74.8) | 118 (63.4) | 49 (61.3) | 11 (55.0) | 115 (69.3) | 33 (55.0) | 33 (63.5) | 61 (73.5) | |
| Use commercial medicine | 11 (9.6) | 62 (33.3) | 18 (22.5) | 1 (5.0) | 34 (20.5) | 25 (41.7) | 14 (26.9) | 17 (20.5) | |
| Use feed supplements | 14 (12.2) | 93 (50.0) | 51 (63.8) | 9 (45.0) | 78 (47.0) | 26 (43.3) | 19 (36.5) | 26 (31.3) | |
| Action taken when livestock is unwell | |||||||||
| Call agrovet shop | 17 (15.3) | 28 (15.8) | 20 (27.0) | 8 (40.0) | 34 (21.9) | 7 (11.7) | 4 (7.8) | 12 (15.0) | |
| Call neighbour/ friend | 4 (3.6) | 2 (1.1) | 1 (1.4) | 1 (5.0) | 3 (1.9) | 1 (1.7) | 0 (0.0) | 2 (2.5) | |
| Call a veterinarian | 18 (16.2) | 106 (58.6) | 33 (44.6) | 9 (45.0) | 74 (47.7) | 29 (48.3) | 18 (35.3) | 27 (33.8) | |
| Implement treatment of own animals | 71 (64.0) | 43 (23.8) | 19 (25.7) | 2 (10.0) | 42 (27.1) | 23 (38.3) | 27 (53.0) | 39 (48.8) | |
| Take no action | 1 (0.9) | 2 (1.1) | 1 (1.4) | 0 (0.0) | 2 (1.3) | 0 (0.0) | 2 (3.9) | 0 (0.0) | |
Cumulative percentage may exceed 100% where multiple responses were selected.
Table 3.
Antimicrobial use practices on among farmers.
| Variable | Parameter | Number (%) |
|---|---|---|
| Reason for using antimicrobials (n = 235) | Treatment | 187 (79.6) |
| Advice by veterinarian | 25 (10.6) | |
| Prevent animals from sickness | 22 (9.4) | |
| Increase productivity | 1 (0.4) | |
| Why use alternative to antimicrobials (n = 209) | Prevent resistance | 145 (86.8) |
| Available cheap option | 16 (9.6) | |
| Prefer traditional | 2 (1.2) | |
| Veterinarian’s advice | 4 (2.4) | |
| Source of antimicrobials (n = 349) | Agro-veterinary shops | 171 (49.0) |
| Veterinarians | 164 (47.0) | |
| Friends | 14 (4.0) | |
| Frequency of antimicrobial use (n = 322) | Whenever animal is sick | 249 (77.3) |
| Weekly | 32 (9.9) | |
| Monthly | 33 (10.3) | |
| Never | 4 (1.2) | |
| Twice a year | 4 (1.2) | |
| Usually get prescription (n = 355) | Yes | 228 (63.7) |
| Sometimes | 98 (24.6) | |
| No | 29 (8.3) | |
| Source of advice before buying antimicrobials (n = 163) | Agro-veterinary shops | 112 (63.7) |
| Local veterinarians | 39 (23.9) | |
| No advice | 12 (7.4) | |
| Antimicrobial Quality assurance (n = 355) | Seller recommendations | 131 (36.9) |
| Check expiry | 195 (54.9) | |
| Buy from agro-veterinary shops | 82 (23.1) | |
| Buy specific brands | 58 (16.3) | |
| Ask friends/neighbor | 29 (8.2) | |
| No quality assurance | 6 (1.7) | |
| Antimicrobial administration (n = 355) | Through injection | 243 (68.5) |
| Mix with water/other liquids | 151 (42.5) | |
| Mix with feeds | 66 (18.6) | |
| Duration of antimicrobial use (n = 355) | As prescribed | 220 (62.0) |
| As per manufacturer’s instruction | 84 (23.7) | |
| Before end of prescription | 25 (7.0) | |
| Longer than prescription | 15 (4.2) | |
| Record keeping (n = 355) | Livestock population | 158 (44.5) |
| Sales | 106 (29.9) | |
| Vaccination | 95 (26.8) | |
| Antimicrobials used | 49 (13.8) | |
| Disinfection | 23 (6.5) | |
| No record kept | 59 (16.6) | |
| Diseases treated by antimicrobials (n = 355) | Treat FMD (viral) | 121 (34.1) |
| Treat NCD (viral) | 111 (31.3) | |
| Treat mastitis (Bacterial) | 99 (27.9) | |
| Treat classical swine fever (viral) | 21 (5.9) | |
| Treat CCPP/Pox (Viral) | 14 (3.9) | |
| Disposal of excess/ expired antimicrobials (n = 355) | Keep for future use | 244 (68.7) |
| Give to neighbors | 42 (11.8) | |
| Throw in garbage | 35 (9.9) | |
| Bury | 27 (7.6) | |
| Burn | 16 (4.5) | |
| Veterinarians takes it away | 12 (3.4) |
FMD = Foot-and-mouth disease; NCD = Newcastle Disease; CCPP = Contagious Caprine Pleuro-Pneumonia.
Table 4.
Assessment of veterinary professionals and paraprofessionals knowledge towards AMR.
| Variable | Parameter | Number (%) |
|---|---|---|
| Knowledge and awareness of antimicrobials | Know and described antibiotics correctly (n = 29) | 28 (96.6) |
| Know and described antimicrobials correctly (n = 30) | 28 (93.3) | |
| Know difference between antibiotic and antimicrobial (n = 20) | 20 (69.0) | |
| Have heard of antimicrobial resistance (n = 28) | 28 (100.0) | |
| Source of information about AMR (n = 25) | TV | 6 (23.1) |
| Workshop | 13 (50.0) | |
| Training program | 17 (65.4) | |
| Social media | 6 (23.1) | |
| Radio | 3 (11.5) | |
| Newspapers | 8 (30.8) | |
| Friends/relatives | 4 (15.4) | |
| What best describe antimicrobial resistance (n = 25) | No treatment due to ineffective medicine | 11 (42.3) |
| When microorganisms become irresponsive/less responsive to antimicrobial drugs | 21 (80.8) | |
| Lack of treatment because medicine lose potency and effectiveness | 10 (38.5) | |
| When microorganisms change | 19 (73.1) | |
| Understanding and perception on AMR (n = 25) | AMR in food animals is detected by number of antimicrobial residues in meat | 8 (30.8) |
| AMR is a global health threat | 22 (84.6) | |
| AMR can be eradicated | 12 (46.2) | |
| What promotes AMR (n = 25) | Incomplete dosage during antimicrobial treatment | 18 (69.2) |
| Appropriate use of antimicrobials in people and animals | 2 (7.7) | |
| Using water contaminated with fertilizer, feces, and antimicrobial residues | 9 (34.6) | |
| Unnecessary antimicrobial use in humans | 19 (73.1) | |
| Antimicrobial overuse in animals | 23 (88.5) | |
| Ways to prevent AMR (n = 20) | Good vaccination programs | 18 (69.2) |
| Good husbandry practices | 19 (73.1) | |
| Prudent antimicrobial use | 19 (73.1) | |
| Practicing hygiene, sanitation and biosecurity | 21 (80.8) |
Table 5.
Perceptions and concerns of veterinary professionals and paraprofessionals regarding antimicrobial resistance.
Table 5.
Perceptions and concerns of veterinary professionals and paraprofessionals regarding antimicrobial resistance.
| Variable | Parameter | Frequency (%) |
|---|---|---|
| Antimicrobials protect man and animals from diseases (n = 20) | Agreed | 9 (45.0) |
| Disagreed | 9 (45.0) | |
| Antimicrobials improve animal growth rate (n = 20) | Strongly disagreed | 18 (90.0) |
| Agreed | 1 (5.0) | |
| No danger if antimicrobials are properly used in animals (n = 20) | Strongly agreed | 14 (70.0) |
| Agreed | 5 (25.0) | |
| Antimicrobials should be given with prescriptions (n = 20) | Strongly agreed | 17 (85.0) |
| Agreed | 3 (15.0) | |
| Concerned that a family member may get illness not responding to medication (n = 20) | Seriously concerned | 17 (85.0) |
| Concerned | 2 (10.0) | |
| Worried of AMR related issues in future (n = 20) | Seriously concerned | 16 (80.0) |
| Concerned | 4 (20.0) | |
| Government concerned about antimicrobial resistance (n = 20) | Concerned | 17 (85.0) |
| Not concerned at all | 2 (10.0) | |
| No opinion | 1 (5.0) | |
| Farmers concerned about antimicrobial resistance (n = 20) | Concerned | 14 (70.0) |
| Not concerned at all | 5 (25.0) | |
| No opinion | 1 (5.0) | |
| Consumers concerned about antimicrobial resistance (n = 20) | Concerned | 16 (80.0) |
| Not concerned at all | 3 (15.0) | |
| No opinion | 1 (5.0) |
Table 6.
Antimicrobial dispensation practices among AHSPs.
| Variable | Parameter | Frequency (%) |
|---|---|---|
| Source of antimicrobial information (n = 18) | Another animal feed store/animal pharmaceutical store | 8 (44.4) |
| Facts on antimicrobial/antibiotic resistance | 3 (16.7) | |
| From suppliers/distributor/representative | 10 (55.6) | |
| Sales guidance for antimicrobials/antibiotics | 4 (22.2) | |
| The dosage and use in feed and water | 10 (55.6) | |
| Selling feed mixed with antibiotics (n = 19) | Never | 17 (89.5) |
| No (done previously but not at the moment) | 2 (10.5) | |
| Advice farmers on antimicrobial use (n = 18) | Sometimes | 1 (5.6) |
| Yes | 15 (83.3) | |
| During sale promotions | 2 (11.1) | |
| Occasion when farmers are advised on antimicrobial use (n = 18) | During sale promotions | 2 (11.1) |
| In possession of a prescription | 12 (77.8) | |
| Upon request by customer | 3 (16.7) | |
| Demand prescription before selling antimicrobials (n = 18) | No | 5 (27.8) |
| Sometimes | 5 (27.8) | |
| Yes | 8 (44.4) | |
| Record Keeping on antimicrobials used (n = 18) | Feel no need | 3 (16.7) |
| No records of clients with prescriptions kept | 11 (61.1) | |
| No records of prescriptions kept | 12 (66.7) | |
| Not a requirement by organization/business | 5 (27.8) | |
| Not required by law | 7 (38.9) | |
| Frequency of meeting farmer who use expired antimicrobial (n = 18) | At least once a month | 6 (33.3) |
| At least once a week | 2 (11.1) | |
| At least once every six months | 7 (38.9) | |
| At least once every two weeks | 2 (11.1) | |
| Everyday | 1 (5.6) | |
| Advice to farmers on antimicrobial disposal (n = 18) | Burn | 5 (27.8) |
| Bury in the ground | 3 (16.7) | |
| Keep for future use | 5 (27.8) | |
| Throw in the garbage | 3 (16.7) | |
| Return to the suppliers | 3 (16.7) | |
| Advice on use of antimicrobials (n = 18) | Advise use of antimicrobials to treat FMD | 10 (55.6) |
| Advise use of antimicrobials to treat NCD | 10 (55.6) |
* One respondent gave two responses. FMD = Foot-and-mouth disease; NCD = Newcastle disease.
Table 7.
Knowledge assessment of antimicrobial resistance among research and One Health partners.
| Variable | Parameter | Frequency (%) |
|---|---|---|
| Knowledge of AMR terminologies (n = 24) | Know and described antimicrobial correctly | 23 (95.8) |
| Know and described antibiotics correctly | 23 (95.8) | |
| Differentiated antimicrobials from antibiotics | 17 (70.8) | |
| Heard of AMR (n = 24) | Friends | 7 (29.2) |
| Workshops | 8 (33.3) | |
| Radio | 2 (8.3) | |
| TV | 6 (25.0) | |
| Print media | 5 (20.8) | |
| School training | 14 (58.3) | |
| Social media | 4 (16.7) | |
| Described aspects of AMR (n = 24) | Bacterial resistance | 18 (75.0) |
| Genetic transfer | 12 (50.0) | |
| When medicine lose potency | 12 (50.0) | |
| Overuse/misuse of drugs | 20 (83.3) | |
| Health issue affecting animal and plants | 18 (75.0) | |
| Promoters of AMR (n = 24) | Overuse of antimicrobials | 20 (83.3) |
| Fertilizer and feces in water | 13 (54.2) | |
| Unnecessary use | 22 (91.7) | |
| Incomplete dosage | 17 (70.8) | |
| AMR preventive measures (n = 24) | Good agricultural practices | 16 (66.7) |
| Prudent use of antimicrobials | 21 (87.5) | |
| Vaccinating livestock | 18 (75.0) |
Table 8.
Assessment of inclusion of antimicrobials and antimicrobial resistance-related subject in the training and research institutions curricular.
Table 8.
Assessment of inclusion of antimicrobials and antimicrobial resistance-related subject in the training and research institutions curricular.
| Variable | Parameter | Frequency (%) |
|---|---|---|
| Existing AMR curriculum (n = 11) | Yes | 8 (72.7) |
| No | 3 (27.3) | |
| AMR class duration (n = 11) | 1-3 hours (one class) | 7 (63.6) |
| I don’t know | 4 (36.4) | |
| AMR research type (n = 4) | Food safety | 1 (25) |
| Antimicrobial surveillance | 1 (25) | |
| Prevalence, mechanisms and outcomes | 1 (25) | |
| I do not know (no specific focus) | 1 (25) | |
| Specific subject of focus (n = 9) | Microbiology | 6 (66.7) |
| Public health/ One Health | 1 (11.1) | |
| AMR short course | 1 (11.1) | |
| I do not know (no specific focus) | 1 (11.1) | |
| Research results shared with stakeholders (n = 5) | Yes | 4 (80.0) |
| I am not sure/I do not know | 1 (20.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



