
Submitted:
10 July 2023
Posted:
11 July 2023
You are already at the latest version
Abstract
Oral squamous cell carcinoma (OSCC) is one of the most prevalent human malignancies and a global health concern with a poor prognosis despite therapeutic advances, highlighting the need for a better understanding of its molecular background. The genomic landscape of OSCC is well-established and recent research has focused on miRNAs, which regulate gene expression and may be useful as non-invasive biomarkers. A plethora of findings regarding miRNA expression have been generated, posing challenges for their interpretation and identification of disease-specific molecules. Hence, we opted to identify the most important miRNA molecules by bridging genetics and epigenetics, focusing on the key genes implicated in OSCC development. Based on published reports, we have developed a custom panel of 15 major oncogenes and a second panel of 5 major tumor suppressor genes. Following a miRNA/target interaction analysis and a comprehensive study of the literature, we selected the miRNA molecules, which target the majority of each gene panel and are reported to be downregulated or upregulated in OSCC, respectively. As a result, miR-34a-5p, miR-155-5p, miR-124-3p, miR-1-3p and miR-16-5p appeared to be the most OSCC-specific. Their expressional patterns, their verified targets and the signaling pathways affected by their dysregulation in OSCC, are thoroughly discussed in this review.
Keywords:
OSCC
; oral cancer
; genes
; mutations
; miRNA
; expression
; mir-34a
; mir-155
; mir-124
; mir-1
; mir-16
; bioinformatics
; in silico analysis
Introduction
The oral cavity is the most prevalent site for malignancies of the gastrointestinal and upper respiratory tracts [1]. Characterized by the uncontrolled growth of abnormal cells in the oral cavity, including the lips, tongue, gums, and lining of the cheeks, oral cancer is one of the most common human malignancies, ranking sixth in prevalence worldwide with an estimated global incidence of more than 377.700 new cases in 2020 [2]. More than 95% of diagnosed oral cancer cases are represented by oral squamous cell carcinoma (OSCC), which arises from the stratified squamous epithelial layer of oral mucosa [3,4]. OSCC is a significant global health concern, with alarming mortality rates of more than 60% [5], largely due to the fact that over 50% of patients are diagnosed in advanced stages (III and IV) and exhibit lymph node infiltration [5,6,7]. Consequently, despite advances in therapeutic approaches such as chemotherapy, radiation, and surgical excision, OSCC mortality rates have remained exceptionally high for a minimum of two decades [8]. Recurrence rates of OSCC are also high, with up to 45% of patients relapsing and facing survival odds of less than 10% [9,10], highlighting the need for further understanding of
OSCC is a complex and heterogeneous disease involving the well-established dysregulation of multiple genes and several, currently explored, epigenetic signatures [11,12]. In accordance to other malignancies, OSCC is characterized by the pathological dysregulation of the cell cycle [13]. Although its genetic landscape can be diverse, several genes stand out demonstrating unique mutational patterns, while others are reported to exhibit characteristically abnormal expression levels within the tumor’s microenvironment [14].
Beyond genetics, the role of epigenetic alterations to OSCC has been under investigation in recent years, with a particular focus on microRNAs (miR NAs), a class of small non-coding RNAs that have emerged as essential regulators in OSCC development and progression. MiRNAs regulate post-transcriptional gene expression by binding to the 3' untranslated regions (UTRs) of target messenger RNAs (mRNAs), causing their degradation or translational suppression [15]. MiRNAs are significantly overexpressed or downregulated in malignant tissues compared to normal tissues, presenting as tumor-suppressing or oncogenic or epigenetic factors (oncomiRs), depending on whether they inhibit oncogene or tumor suppressor gene expression [16].
MiRNA dysregulation has been identified in OSCC, leading to abnormal gene expression patterns that are associated with oral carcinogenesis. Numerous studies have revealed multiple miRNAs that are involved in essential biological processes such as cell proliferation, apoptosis, invasion, metastasis, and angiogenesis [17]. Although genetic and epigenetic mechanisms were initially thought to be discrete, it is now known that they present a strong interdependent relationship, which if decoded could fill the gaps and assist in mapping the overall molecular signatures of OSCC, resulting in better understanding of its etiology, decidedly reliable biomarkers or even targeted epigenetic therapeutics [12].
The current research on OSCC-related miRNA expression has resulted in a tremendous pool of data implicating hundreds of significantly dysregulated distinct miRNAs [17,18]. Therefore, we aimed to reveal through strategic bioinformatic filtering those epigenetically important molecules that stand out by targeting and influencing the expression of key genes known to govern oral carcinogenesis. We review here the implication of 5 most important miRNA molecules in OSCC by discussing their expressional dysregulation in OSCC tissue, cell lines and patients' biofluids (e.g., saliva, whole blood, serum, and plasma) and their influence on the post transcriptional expression of their verified target genes, as well as on the signal transduction pathways that are subsequently affected by their dysregulation.
Methodology
We report our evaluation of the existing literature about OSCC development through bioinformatic analysis that combines the most significant mutant oncogenes and tumor suppressor genes with the most implicated miRNAs whose expression is dysregulated in OSCC. An initial identification of multiple tens of reportedly involved genes was subsequently analyzed in order to highlight the molecules of extreme importance for oral carcinogenesis that might ultimately be utilized as prognostic and diagnostic markers for that cancer type.
Selection of Most Significant Implicated Genes in OSCC.
An assortment of twenty key cell-cycle regulatory genes was selected through bioinformatic analysis on miRNA/target prediction, including the tumor suppressor genes TP53, CDKN2A, FAT1, CASP8, PTEN, and the oncogenes NOTCH1, HRAS, PIK3CA, EGFR, ERBB2, FGFR1, FGFR2, FGFR3, FGFR4, FGF2, ETS1, JUN, MKI67, MYC and BCL2, which are strongly and typically associated with of OSCC development in humans and laboratory animals [14,19,20,21,22,23], as discussed in detail below.
Selection of Most Significant miRNAs in OSCC.
We conducted a PubMed search using the following keyword combinations: ("miRNAs" AND "OSCC"), ("miRNAs" AND "expression" AND OSCC"), and ("miRNAs" AND "expression" AND OSCC"), limiting our search to review articles in English, published between January 1, 2020 and June 20, 2023. The searches yielded 39, 23, and 63 results, respectively, from which we selected 13 articles that were specifically focused on OSCC (excluding precancerous oral pathologies), included more than three implicated miRNA molecules, and clearly stated the expression patterns, as well as the sample sources that corresponded to miRNA quantification results (Table 1 and 2). After compiling the miRNA-expression data from each review, we identified 106 miRNA molecules that are significantly upregulated in OSCC-related biological samples (tissue, cell lines, saliva, whole blood, serum or plasma) (Table 1) and 133 that are considerably downregulated (Table 2). Those results provided us a detailed picture of the current literature on miRNA expression patterns in OSCC and served as the data pool for the following step of the process, which comprised bioinformatic filtering.
Analysis of Target Gene/miRNA Interaction.
For target identification and miRNA/target interaction analysis, we developed two miRNA regulatory networks using the "miRNet 2.0" miRNA-centric network visual analytics software (https://www.mirnet.ca/miRNet/home.xhtml, Xia Lab/McGill University, Canada). One network identified all miRNA molecules that are predicted to target and therefore may regulate the expression of the 5 selected tumor suppressor OSCC-driver genes TP53, CDKN2A, FAT1, CASP8 and PTEN (Figure 1). The second network comprised all the miRNA molecules that target and might affect the expression of the 15 selected driver oncogenes NOTCH1, HRAS, PIK3CA, EGFR, ERBB2, FGFR1, FGFR2, FGFR3, FGFR4, FGF2, ETS1, JUN, MKI67, MYC and BCL2 (Figure 2). Afterwards, following the examination of all the OSCC-related miRNAs listed in Table 1 and Table 2, we selected from the networks 2 miRNA molecules that target more than 3 (60%) of the 5 tumor suppressor genes and are reported to be significantly upregulated in OSCC, and 4 miRNAs that target at least 9 of the 15 (60%) selected oncogenes and at the same time exhibit significant downregulation in OSCC. One miRNA was included in both group of OSCC-driver genes. The 5 miRNAs obtained from the aforementioned filtering were analyzed as to their expression patterns in OSCC-related biological materials (e.g., tumor tissue, cell lines, saliva, whole blood, serum or plasma samples), their target-genes of interest and the possible influence of their dysregulation in signaling pathways that are known to be involved in tumorigenesis and/or OSCC development in specific.
Important Driver Genes in OSCC
Twenty genes were selected to serve as an OSCC-specific signature panel in this study, due to their significant involvement in key biological processes and pathways relevant to oral oncogenesis, which is supported by extensive research on human patients and laboratory animal models [14,19,20,21,22,23,24]. The dysregulation of these genes contributes to OSCC pathogenesis because their protein products playing crucial roles in cell cycle regulation and various other cell functions.
A. Tumor Suppressor Genes
TP53, also known as the p53 gene, it encodes the protein p53, which acts as a tumor suppressor, since it plays a crucial role in regulating cell cycle progression, DNA repair, apoptosis and genomic stability [25,26]. TP53 is considered to be the mostly mutated gene in OSCC, resulting in uncontrolled cell growth and genomic instability [27]. Inactivation of TP53 has been associated with aggressive OSCC traits, advanced tumor stage, resistance to radiation and chemotherapy, increased risk of recurrence, and lower overall survival [19,27,28,29,30].
The CDKN2A gene encodes cyclin-dependent kinase inhibitor 2A, also referred to as p16INK4a or p16. CDKN2A prevents the progression of the cell cycle by inhibiting the activity of cyclin-dependent kinases [31]. CDKN2A is an additional tumor suppressor gene that is frequently mutated in OSCC, promoting uncontrolled cell proliferation [14,28], particularly in non-smoking patients [27]. It is believed to promote malignant transformation and disease progression [32], which is supported by the observation that infection with high-risk HPV strains induces overexpression of p16 in oral premalignant lesions and carcinomas [14].
FAT1 is a tumor suppressor gene that encodes the FAT atypical cadherin 1 protein, which is essential for cell-cell adhesion as well as tissue development and proliferation [33]. By modulating cell proliferation, apoptosis, and migration, FAT1 typically inhibits tumorigenesis. FAT1 is frequently mutated or silenced in OSCC and is therefore regarded one of the disease's driver genes [33]. The loss of FAT1 function has been associated with OSCC development, progression and ultimately metastasis, since it disrupts cell adhesion and promotes epithelial-to-mesenchymal transition (EMT) [34].
CASP8 is a tumor suppressor gene that encodes the apoptosis-regulating enzyme caspase-8 [35]. Driven by cell surface receptors, the activation of caspase-8 leads to the elimination of abnormal cells, thereby maintaining tissue homeostasis and preventing cancer development. Loss-of-function mutations in CASP8 have been associated with the development of OSCC and contribute to cancer-cell proliferation, survival, migration, and chemoresistance [35,36,37].
PTEN is a tumor suppressor gene that encodes the phosphatase and tensin homolog protein [38]. It maintains the delicate balance between cell growth, proliferation, and apoptosis by inhibiting the PI3K/AKT signaling pathway and thus regulates cell survival, proliferation, and apoptosis [13,38]. PTEN loss-of-function mutations are frequently observed in OSCC and contribute to its pathogenesis by stimulating cell proliferation and enhancing cell survival as a result of PIK3/AKT cascade subsequent upregulation [13,21]. In fact, loss or down-regulation of PTEN expression is typical for OSCC and is associated with a substantially poor prognosis for OSCC patients [13,38].
B. Oncogenes
NOTCH1 codes for the transmembrane receptor NOTCH1 protein, which is involved in cell signaling pathways that govern cell fate determination, differentiation, and proliferation [39]. NOTCH1 mutations are identified in 60% of OSCCs [14], and dysregulated NOTCH1 signaling can contribute to uncontrolled cell proliferation and OSCC initiation. OSCC tumors exhibit elevated NOTCH1 expression levels, which have been associated with OSCC progression and lymph node metastasis, whereas inhibition of the NOTCH pathway reduces cell proliferation and invasion and inactivation of the NOTCH1 gene has been correlated with favorable disease outcomes [13,39,40].
HRAS is a proto-oncogene that encodes the H-ras small GTPase protein, which regulates the cell cycle in response to growth factor stimuli by activating a signaling cascade that leads to cell growth and division [41,42]. HRAS is considered to be one of the most frequently mutated genes in OSSC [13,19]. HRAS activating mutations may result in constitutive activation of downstream signaling pathways, enhancing cell proliferation and contributing to OSCC formation, invasion, and metastasis [41,42].
The PIK3CA gene encodes the p110 catalytic subunit of phosphatidylinositol 3-kinase (PI3K), a signaling protein involved in cell growth and survival via the PI3K/AKT signaling pathway. Gain of function mutations in PIK3CA induce constitutive activation of the PI3K/AKT signaling pathway, which promotes cell survival and proliferation and is associated with OSCC development and progression [43,44]. Furthermore, PI3K/AKT activation can interact with other oncogenic signaling pathways, such as RAS/MAPK and the EGFR, boosting OSCC progression [41,44,45]. Finally, PIK3CA expression has been found to be elevated in more than 50% of OSCC tumors, and PIK3CA gene copy amplification has been proposed as a potential prognostic marker, as it has been associated with poor
The EGFR gene encodes the EGFR (epidermal growth factor receptor) protein, which is a receptor tyrosine kinase that regulates cell proliferation, survival, and differentiation by delivering extracellular growth factor signals. In OSCC, EGFR is considered an oncogene. Indeed, EGFR overexpression and activating mutations in its sequence result in abnormal EGFR-signaling, which promotes enhanced cell proliferation and survival, angiogenesis, and tumor growth while imposing resistance to EGFR-targeting therapies in OSCC [41,46]. Furthermore, EGFR gene mutations have been detected in 15% of HPV-negative and 8% of HPV-positive SCC of the head and neck, and EGFR elevated expression has been associated with a poor prognosis and a significantly decreased cancer-free survival in precancerous lesions [14].
ERBB2, also known as HER2, is an oncogene that encodes the erb-b2 receptor, a tyrosine kinase that impacts cell proliferation and differentiation. Cell cycle dysregulation, carcinogenesis, and tumor growth can result from ERBB2 amplification or overexpression [47]. Overexpression of ERBB2 has been linked to increased proliferation, growth, invasion, and metastasis in OSCC, whereas patients with ERBB2 mutations have been linked to significantly lower survival rates [41,48], and ERBB2 copy-number amplification in OSCC cancer-free margins has been suggested to serve as a predictor of unfavorable prognosis [49].
The human fibroblast growth factor receptor (FGFR) family of the FGF superfamily is comprised of the FGFR1, FGFR2, FGFR3 and FGFR4 genes, which encode the fibroblast growth factor receptor proteins -1, -2, -3, and -4, respectively. Extracellular signaling activates FGFRs on the cell membrane, resulting in proliferation, cell migration, and survival. FGFRs are considered to be oncogenic and have considerably increased expression in a variety of cancers, including OSCC [50,51]. FGFR signaling deviations, due to gene amplification or activating mutations, have been associated with OSCC development and progression [41,52]. FGFR3 and FGFR4 overexpression is seen in 48% and 41% of oral malignancies, respectively, while FGFR1 mutations are identified in 10% of HPV-negative cases [14]. Finally, strong expression of FGFR3, as well as FGFR2 and its ligand FGF2 (fibroblast growth factor 2) in oral premalignant lesions has been shown to be a positive predictor of malignant transformation [14,53]. Indeed, dysregulated FGF2 expression is prevalent in the early stages of oral carcinogenesis and is thought to exert fibrotic and angiogenic effects [54].
ETS1 is a gene that encodes the Ets-1 protein, which belongs to the E26 transformation-specific (ETS) transcription factor family. ETS1 regulates an array of biological processes, including cell proliferation, differentiation, and death. ETS1 has been shown to control signaling pathways involved in cell cycle progression and extracellular matrix remodeling, including the TGF-b pathway [55,56]. ETS1 overexpression has been observed in OSCC tissues and is believed to promote OSCC development, EMT, lymph node infiltration, distant metastasis, and has been associated with advanced OSCC stages and notably poor survival of patients [55,56,57].
The JUN proto-oncogene encodes c-Jun, a subunit of the AP-1 transcription factor that is involved in cellular processes such as proliferation, apoptosis, and differentiation and may influence the expression of cell cycle regulatory genes [30]. C-Jun is important in the initiation of OSCC, and high expression of c-Jun is associated with OSCC progression, invasion, and overall poor patient prognosis [30], as well as more aggressive tumor behavior in HPV-negative OSCCs [58]. In fact, JUN gene’s expression is 2.69-fold higher in metastatic OSCCs compared to non-metastatic tumors (p = 0.012) and is associated with substantially lower survival rates [30], with high c-Jun expression considered predictive of OSCC-induced mortality [59]. Finally, high EGFR expression, which has been linked to OSCC development, activates c-Jun via the phospholipase Cy (EGFR-PLCy-Raf-MEK-ERK) signaling pathway, resulting in elevated c-Jun expression that gradually increases during OSCC progression in representative animal models [22].
The MYC gene, also known as the c-myc transcription factor, is involved not only in cell-cycle regulation through mediating cell proliferation, differentiation, and apoptosis, but also in cell metabolism and tumor stem cell self-renovation. MYC functions as an oncogene in a range of cancer types, including OSCC, exhibiting activating mutations and aberrant expression [60]. The activation and upregulation of c-myc expression in response to TGF-b1 signaling in growth factors results in uncontrollable cancer-cell proliferation in OSCC and contributes to its progression [61,62]. Increased c-myc levels have been associated with advance-staged malignancies as well as an increased risk of lymph node infiltration and metastasis [60].
The MKI67 gene encodes the Ki67 nuclear protein, which is not expressed in non-dividing cells and is thus characterized as a marker of proliferation levels in tumor tissues, due to its notably high expression in cancer cells, which is associated with advanced tumor stages, disease progression, metastasis, and prognosis of several human neoplasms, including OSCC [63]. Ki67 expression increases alongside the degree of dysplasia in the oral mucosa, and ki67 positivity is found in all OSCC tumors, with significant expression intensity at invasion sites. Ki67 overexpression has been associated with high levels of differentiation in OSCC and is thought to be a valuable prognostic marker of tumor aggressiveness [64].
The BCL2 gene encodes the Bcl-2 (B-cell lymphoma 2) protein, which regulates cell death by inhibiting the activation of apoptotic pathways and thereby promotes cell survival. The anti-apoptotic Bcl-2 is widely overexpressed in malignancies, including OSCC [65]. enhanced Bcl-2 expression in tumor tissue has been observed in OSCC, leading to defective apoptosis and increased cell survival. Histological Bcl-2 overexpression in OSCC has been associated with advanced-stage carcinomas, lymph node metastases, and an unfavorable overall prognosis [65,66,67]. Bcl-2 has also been suggested as a good predictive indicator for malignant transformation in the initial stages of oral carcinogenesis, from normal oral mucosa to dysplastic lesions [66,68], while it is supported that its levels decline in well and moderately differentiated tumors in contrast with poorly differentiated OSCCs that exhibit bold Bcl-2 expression [68].
C. Combinatory Significance of Key Driver Genes in OSCC
Each of the aforementioned 20 genes, when in dysregulation, significantly contributes to OSCC pathogenesis by promoting biological processes such as cell proliferation, inhibition of apoptosis, cell survival enhancement, and activation of signaling pathways involved in tumor growth, invasion, and metastasis. However, comprehensive studies have revealed the combinatory role of large subsets of those genes and their protein products in oral oncogenesis in both humans and representative laboratory animals, in terms of mutational and expressional profiles.
In fact, around 88% of OSCC patients harbor at least one mutation in TP53, CDKN2A, FAT1, CASP8, NOTCH1, HRAS and PIK3CA genes in the primary OSCC tumor tissue. The same mutational profile is also detected in cell-free DNA extracted from saliva samples of the corresponding patients by 93.4%. This set of genes is suggested as a very promising gene panel for screening high-risk individuals for early detection, monitoring during treatment, as well as post-operative surveillance [20]. Driver mutations of the PTEN and EGFR genes are also reported as typical in OSCC development alongside mutations in the sequences of the aforementioned [19].
Additionally, a hamster model of sequential oral oncogenesis showed the increased expression of the transmembrane receptors EGFR, ERBB2, FGFR2 and FGFR3, as well as the increased expression of TP53, MYC, ETS1, MKI67 and JUN proteins in early stages of oral cancer indicating that these molecules may be used as early prognostic factors for the progression of OSCC [24]. On the other hand, CDKN2A appears to be significantly downregulated from the stage of oral dysplasia to well- and moderately-differentiated OSCC, with Bcl-2 also declining between the stages of dysplasia and early invasion [24].
It is particularly significant, and possibly reflective of why some of those genes play such unique roles in OSCC, the fact that their encoded proteins are involved in co-dependent signaling pathways, and some of them have been found to operate synergistically in OSCC formation. As previously stated, PTEN, a tumor suppressor OSCC-related driver gene, negatively regulates the PIK/AKT signaling cascade, which is stimulated by the overexpression of PIK3CA, an oncogene also essential for OSCC development [13,43,44]. Furthermore, PTEN loss and Bcl-2 overexpression within the same OSCC tissues have been associated with late-stage tumors, poor differentiation, and lymph node metastasis [67].
Increased EGFR expression, on the other hand, which has been firmly associated with OSCC, activates and drives the overexpression of c-Jun [22], which is also key to OSCC pathogenesis. Finally, the highly implicated tumor suppressor genes FAT1 and CASP8 are thought to have synergistic effects on oral oncogenesis, as loss-of-function mutations in both are reported in the majority of OSCC tumors [36].
Results of Bioinformatic Analysis of miRNA/Target Interactions
The bioinformatic approach used to predict which miRNAs target the two selected custom tumor suppressor gene and oncogene panels yielded 437 and 828 miRNA candidates, respectively, that are predicted to target at least one gene of each respective gene panel. From both developed miRNA/mRNA interaction networks (Figure 1, Figure 2) we selected the miRNAs that target at least 60% of each gene panel, meaning more at least 3 of the selected tumor suppressor genes and at least 9 of the selected oncogenes, which yielded 41 and 4 results respectively. In light of the number targeting at least 3 out of the tumor suppressor genes and the small size of the panel that explains the large number of targeting miRNA molecules, we decided to only maintain the miRNAs that target more than 3 tumor suppressor genes (>60%), as a step of additional filtering in the attempt to distinguish the most representative. For the miRNA results that correspond to the larger oncogene cohort of 15, we included all 4 of the miRNAs that are predicted to target and might regulate the expression of at least 9 genes (≥60%).
From the final two sets of miRNAs which target the tumor suppressor and oncogene panels, we selected the miRNA molecules that are reported to be significantly upregulated and downregulated respectively in the most recent reviewing of the available literature (Table 1 and Table 2). Finally, 5 miRNAs were selected in total (Table 3), with one falling in both categories. More specifically, the miRNAs that are predicted to target more than 3 (>60%) of the 5 tumor suppressor genes and are reported to be significantly upregulated in OSCC were miR-155-5p with a target score of 5/5 and miR-34a-5p with a target score of also 5/5. As to the miRNAs that target at least 9 (≥60%) of the 15 selected oncogenes and exhibit significant downregulation in OSCC, our analysis yielded 4 miRNA molecules: miR-16-5p (Target score: 9/15), miR-1-3p (Target score: 10/15), miR-124-3p (Target score: 12/15) and miR-34a-5p (Target score: 15/15).
1. MiR-155-5p in OSCC
According to our bioinformatic filtering, miR-155-5p exhibited the highest target-score, while it is predicted to target all five of the selected tumor suppressor genes (TP53, CDKN2A, FAT1, CASP8, and PTEN) that are highly involved in the pathogenesis and clinical features of OSCC, while TP53, FAT1 and CASP8 belong to the panel of the most frequently mutated genes in OSCC patients (Figure 3). Furthermore, its upregulation in OSCC has been highly reported, indicating a strong oncogenic effect and being associated with numerous aspects of tumor growth and OSCC progression [18].
Expression patterns in OSCC.MiR-155-5p is significantly overexpressed in OSCC tissues relatively to adjacent healthy margins (p < 0.0001) and is highly upregulated in HPV-positive compared to HPV-negative tumors, functioning as a marker useful for distinguishing HPV-induced tumors [69]. In OSCC cell lines, there is a significant correlation between heightened levels of miR-155-5p in OSCC cell lines and a notable augmentation in OSCC cell proliferation, colony formation, as well as enhanced invasive and migratory capabilities. Conversely, the suppression of miR-155-5p yields contrasting outcomes [70].
The upregulation of miR-155-5p in OSCC tissues and cell lines has been found to exhibit a significant association with aggressive characteristics, including larger tumor size, advanced stage and grade, lymph node metastasis facilitated by EMT induction, reduced disease-free survival, and unfavorable overall survival, thus highlighting its potential not only as a diagnostic but also as a prognostic tool [70,71,72]. Moreover, there seems to be a positive correlation between elevated levels of miR-155-5p and the emergence of resistance towards the chemotherapeutic agents 5-FU (5-Fluorouracil) and cisplatin, which are commonly employed in the treatment of OSCC [63,72].
Known target genes and affected pathways.The main target of miR-155 is the FoxO3a member of the FOXO family of transcription factors, which regulates multiple tumor suppressor genes via the FOXO signaling pathway. Consequently, overexpression of miR-155-5p may disrupt the FOXO-induced immunological and cell-cycle regulation. In addition, miR-155-5p, harbors targets that are involved in the b-glycal biosynthesis pathway, which is essential for OSCC progression and lymph node metastasis, in which increased glycosylation of molecules such as adhesion-related proteins takes place [69,73]. In addition, by directly targeting to the 3′-UTR of its mRNA transcript, miR-155-5p inhibits the expression of ARID2 and is responsible for a substantial decrease in its levels in OSCC. Inhibition of ARID2 expression by miR-155-5p results in a rise in the levels of E-cadherin, vimentin, and snail proteins, indicating that the miR-155-5p/ARID2 axis is essential for promoting tumor growth and mediating OSCC-related EMT and subsequent metastasis [25,70].
Furthermore, the expression of TP53INP1 and consequently its mRNA and protein levels are also downregulated in light of miR-155-5p overexpression in OSCC. TP53INP1 is a well-known tumor suppressor that regulates apoptosis, cell-cycle arrest, and cell migration. The targeting of miR-155-5p has been proposed as a useful treatment strategy aimed at improving the efficacy of OSCC-targeting chemotherapy [74]. Another known target gene of miR-155-5p is the CDKN1B which counts for the 27Kip1 cyclin-dependent kinase inhibitor, which mediates the cell cycle progression at phase G1 and its degradation is required for cell proliferation to occur. While the upregulation of 27Kip1 exerts apoptotic and anticancerous effects, its downregulation has been associated with the progression of numerous neoplasms. In the case of OSCC, the typical upregulation of miR-155-5p reduces p27Kip1 levels, thereby promoting proliferation and oncogenesis, whereas the suppression of miR-155-5p results in the upregulation of p27Kip1 expression, which reduces proliferation and inhibits tumorigenicity [73]. Finally, miR-155-5p has been shown to induce oncogenesis in OSCC by suppressing the expression of CDC73 (parafibromin), a key tumor suppressor, thereby inhibiting apoptosis and promoting growth, while simultaneously inducing inflammation by suppressing the expression of SOCS1, a well-known anti-inflammatory factor [72,75].
2. MiR-16-5p in OSCC
According to our miRNA/target interaction analysis, miR-16-5p yielded to target 9 of our custom panel of 15 OSCC-associated key oncogenes (Figure 4). More specifically, the PIK3CA, MYC, JUN, EGFR, FGF2, FGFR1, FGFR4, MKI67 and BCL2 genes, which are renown to be highly involved in OSCC pathogenesis, are bioinformatically predicted to be targeted by miR-16-5p, which in turn is highly reported to exhibit significant downregulation in OSCC tissues and cell lines [73,76,77,78,79].
Expression Patterns in OSCC.
It has been reported that miR-16-5p, also known as miR-16, fulfills a tumor suppressor role in OSCC by inducing apoptosis of malignant cells and inhibiting tumor growth [73,76]. Compared to normal specimens and tumor-free adjacent tissues, OSCC tumors and cell lines exhibit significantly lower expression of miR-16, and it has been shown to be especially downregulated in higher grade lesions, thus serving as a potential non-invasive tool for OSCC diagnosis and distinguishing advanced tumors [73,76,77,78]. It has been reported that miR-16 is downregulated in approximately 60% of OSCC tumors [79], and it has been strongly correlated with lower disease-free and overall survival rates of patients, highlighting its potential as a prognostic marker [76,80].
The introduction of miR-16-mimicking molecules into OSCC cell lines results in the inhibition of proliferation and robust apoptotic effects, whereas the inhibition and silencing of miR-16 has the exact opposite effect [78]. The quantification of miR-16 in plasma samples from OSCC patients yielded results opposite to those obtained from tissue. In fact, miR-16 levels were higher in plasma samples, which was attributed to the selective release of tumor-suppressing miRNAs by OSCC cells [81].
Known Target Genes and Affected Pathways.
MiR-16 acts as a tumor suppressor by decreasing the expression levels of genes that encode factors involved in the PI3K/Akt signaling pathway, such as BCL2, MTOR, CCND1, CCND3, SGK3 and AKT3, which are implicated in cell cycle progression and cell survival, as well as growth and proliferation thus outlining its tumor suppressing, pro-apoptotic role both in vivo and in vitro. Nonetheless, in the typical case of miR-16-5p downregulation, the PI3K/Akt oncogenic signaling may be amplified and overactivated, resulting in tumor growth and disease progression [73,81]. AKT3, as well as BCL2 like protein 2 (BCL2L2), are highly expressed in OSCC tissues and cell lines, which exhibit significantly low expression of miR-16, whereas the induced higher expression of miR-16 and the decrease in their protein levels were successful in reducing OSCC proliferation and tumor size [78].
In addition, miR-16 exerts its tumor-suppressing properties by directly targeting the 3'-UTR of the mRNA encoding the Tousled Like Kinase 1 (TLK1), thereby inhibiting its expression. TLK1 interacts strongly with the AKT-interacting protein (AKTIP), and its elevation leads to overactivation of the PI3K/AKT pathway, which has been identified as a key driver in numerous malignancies, including OSCC [76,82]. In OSCCs with substantially downregulated expression of miR-16-5p, the expression of TLK1 is significantly elevated compared to adjacent normal tissues, indicating its subsequent dysregulation due to miR-16 suppression [76]. Finally, miR-16 inhibits tumor growth in OSCC and induces apoptosis in vivo and in vitro by inhibiting the Wnt/β-catenin signaling pathway, which is highly upregulated in OSCC and accounts for cell fate, proliferation, and migration. Therefore, the induced overexpression of miR-16 has been proposed as a potential alternative treatment for OSCC [83].
3. MiR-1-3p in OSCC
Based on the developed miRNA/target interaction network analysis, it was observed that miR-1-3p yielded to target 10 of our custom panel of 15 OSCC-associated key oncogenes (Figure 5). More specifically, the PIK3CA, HRAS, MYC, JUN, EGFR, FGF2, FGFR2, FGFR4, MKI67 and ETS1 genes, which are renown to be highly involved in OSCC pathogenesis, are bioinformatically predicted to be targeted by miR-1-3p, which in turn is highly reported to exhibit significantly low expression in OSCC [17,73,75,84].
Expression Patterns in OSCC.
MiR-1-3p, also referred to as miR-1, is recognized as a tumor suppressor miRNA in OSCC. It plays a pivotal role in promoting apoptosis and inhibiting the migration and invasiveness of tumor cells [73,84]. Conversely, the downregulation of miR-1 leads to the activation of these properties, along with enhanced colony formation in OSCC cell lines [73,75,84]. In OSCC tumors, it is commonly observed that the expression levels of miR-1-3p are markedly diminished. This reduction in miR-1-3p levels has been found to facilitate cancer cell migration and stimulate invasion by activating the process of EMT. This finding elucidates the significant correlation between the notably diminished expression of miR-1 and the occurrence of lymph node metastasis, advanced tumor stages (III and IV), as well as a generally inferior prognosis [17,77,84,85]. In contrast, the upregulation of miR-1 through induction has been shown to possess therapeutic promise in the context of OSCC by effectively suppressing the proliferation and migration of malignant cells [84,85].
Known Target Genes and Affected Pathways.
MiR-1 normally suppresses migration and invasion by negatively regulating the expression of Slug or SNAI2 (snail family transcriptional repressor 2), a crucial EMT regulator, through targeting the 3’UTR of its mRNA. In the typical case of miR-1-3p downregulation in OSCC, slug is overexpressed, resulting in the diminishing of E-cadherin expression, thus promoting EMT and bestows invasion dynamics to OSCC cells [84].
The EGFR gene, which exhibits notably elevated expression in OSCC cells, is identified as an additional direct target of miR-1, further supporting its role in tumor suppression. The downregulation of EGFR expression and signaling has been observed in cases where miR-1 overexpression is induced. This downregulation leads to a decrease in the aggressiveness of OSCC and suggests that miR-1 might serve as a potential therapeutic agent [84,86]. The c-MET gene, which encodes a tyrosine kinase that plays a role in cellular proliferation, migration, and invasion, has been identified as a direct target of the tumor suppressor miR-1-3p [86,87]. The expression of c-MET is observed to be markedly elevated in head and neck SCC, which may be attributed to the substantial decrease in the expression levels of its regulatory molecule miR-1-3p, thus contributing to the activation of oncogenic signaling pathways [86].
Alongside normally regulating migration and invasion, miR-1-3p also inhibits OSCC proliferation by suppressing the expression of the DKK1 (dickkopf WNT signaling pathway inhibitor 1) gene of the WNT signaling pathway, that is typically overexpressed in various cancers including OSCC tissue and cell lines, and stimulates proliferation, migration and invasion. Introducing a miR-1-3p mimic to OSCC cell lines leads to the suppression of migratory and invasive dynamics and to declined proliferation by inducing the bold suppression DKK1 expression levels [85].
4. MiR-124-3p in OSCC
According to the miRNA/target interaction analysis in silico, miR-124-3p interacts with 12 of our custom panel of 15 OSCC-associated oncogenes (Figure 6). More specifically, the mRNAs of all the NOTCH1, HRAS, PIK3CA, EGFR, ERBB2, FGFR1, FGFR3, FGFR4, ETS1, JUN, MKI67 and MYC genes, which play a key role in the development and clinicopathological features of OSCC, are predicted to be targeted by miR-124-3p, which in turn is notably decreased in OSCC tissues and cell lines in terms of expression [77,88].
Expression Patterns in OSCC.
MiR-124-3p, also referred to as miR-24, is recognized as a tumor suppressor miRNA in a number of cancers, including OSCC. It possesses the capacity to impede the adhesion and movement of malignant cells, induce programmed cell death, and hinder tumor growth [77,88,89]. The expression levels of miR-124-3p have been observed to exhibit a notable downregulation in both tissue and saliva samples obtained from patients diagnosed with OSCC [77,88,90]. Additionally, animal models of OSCC have demonstrated a similar decrease in miR-124-3p levels within tumor cells [91]. Upregulation of miR-124-3p in OSCC cell lines has been shown to be a robust indication of its ability to suppress tumor growth, through the inhibition of cancer cell migration and invasion [89].
The downregulation of miR-124-3p is a distinguishing feature observed in SCCs affecting the oropharynx and oral cavity. Conversely, it has been documented to be upregulated in SCCs affecting the larynx and pharynx. In addition, the expression patterns of miR-124-3p have the potential to be utilized in distinguishing between HPV-positive and HPV-negative OSCCs. This is due to its notably reduced expression in the presence of HPV, while it is upregulated in HPV-free tumors. In addition, it is worth noting that miR-124-3p may potentially function as a molecular marker for the staging OSCC. This is supported by the significant downregulation of miR-124 in stage IV OSCCs, as opposed to the upregulation observed in stages II and III [90]. In addition, the bold downregulation of miR-124-3p has been observed to confer resistance to cisplatin, thereby posing as a significant challenge to the efficacy of therapeutic interventions against OSCC [92].
Known Target Genes and Affected Pathways.
MiR-124 has been documented to selectively target multiple genes that have been implicated in the development and progression of malignancies, thereby exerting its suppressive effects on tumor growth. However, these tumor suppressive effects are compromised when miR-124 is downregulated in OSCC [89,91,92,93]. MiR-124 is reported to exert a suppressive effect on OSCC motility. This is achieved through the targeting of the mRNA of the ITGB1 gene, which encodes the integrin subunit beta 1 (ITGB1). The ITGB1 protein is known to play a crucial role in the oncogenic PI3K/AKT cascade. MiR-124 typically decreases the levels of ITGB1 protein and mRNA expression in OSCC cells, through its interaction with two conserved binding sites located in the 3’UTR of its mRNA. The results of miR-124 in OSCC cells support its tumor suppressive role. This is evidenced by the significant decrease in ITGB1 expression within OSCC cells following miR-124 induced overexpression. Additionally, miR-124 intervention leads to the inhibition of OSCC cell adherence and motility. These findings suggest that dysregulation of miR-124 may play a critical role in promoting the progression of OSCC [89].
The gene encoding CCL2, also known as monocyte chemoattractant protein-1 (MCP-1), is another target of miR-124-3p that is highly correlated with cancer cell migration and overall malignant progression in general. CCL2 is frequently upregulated in OSCC tissues and is also observed to be overexpressed in plasma samples of OSCC patients. The overexpression of CCL2 has been found to facilitate tumor progression by attracting immune cells to the tumor microenvironment, with the ability to secrete a diverse array of growth factors and cytokines, thereby augmenting both the growth and invasion capabilities of the malignancy. The observed decrease in expression of miR-124-3p, leading to its diminished tumor-suppressive function, may provide a potential explanation for the observed increase in CCL2 levels [91,93]. Finally, it is indicated that miR-124 suppresses the expression of TRIM14 (Tripartite Motif Containing 14) by interacting with the 3’-UTR of its mRNA. The dysregulation of TRIM14 has been observed in various malignancies and has been shown to facilitate cell proliferation and inhibit apoptosis in colorectal cancer by suppressing the PTEN tumor suppressor [92,94]. The upregulation of TRIM14 expression, potentially caused by the downregulation of miR-124, has been documented as a contributing factor in the development of tongue OSCC. Additionally, this upregulation has been found to confer chemoresistance to cisplatin, a commonly used treatment for OSCC. In accordance with the above, the overexpression of miR-124 is observed to significantly downregulate TRIM14 levels, while also reducing cisplatin resistance in tongue OSCC [92].
5. MiR-34a-5p in OSCC
Based on our computational analysis of miRNA/target interactions, miR-34a-5p demonstrated the highest target-score among all miRNAs in both custom gene panels, achieving a perfect score of 20 out of 20. MiR-34a-5p has been identified as a potential regulator of all 15 oncogenes (NOTCH1, HRAS, PIK3CA, EGFR, ERBB2, FGFR1, FGFR2, FGFR3, FGFR4, FGF2, ETS1, JUN, MKI67, MYC, and BCL2) and all 5 tumor suppressor genes (TP53, CDKN2A, FAT1, CASP8, and PTEN) that are known to play crucial roles in the development of OSCC (Figure 7 and Figure 8). This miRNA, which is known for its role in cancer development, stands out as the most OSCC-specific molecule among all the candidates that have successfully passed the target-score filtering in our analysis. MiR-34a-5p appears to exhibit a multifaceted role in OSCC, as it not only encompasses two corresponding gene categories, but has also been documented to exhibit both downregulation and upregulation in OSCC biological specimens, as reported in the current body of research [95,96,97,98].
Expression Patterns in OSCC.
MiR-34a-5p, alternatively referred to as miR-34a, has been identified as a well-established tumor suppressor in various types of cancer [95]. In regards to OSCC, research has predominately revealed a major decline in the levels of miR-34a-5p in OSCC tumor specimens and OSCC cells when compared to normal tissues and cell lines. This reduction has exhibited a strong association with more aggressive phenotypes, as well as with lymph node metastasis and unfavorable overall prognosis among OSCC patients [96,97,98]. In contrast, the exogenous stimulation of miR-34a in OSCC cell lines leads to the inhibition of EMT and a notable reduction in the cells' ability to invade and migrate. In addition, the overexpression of miR-34a causes the arrest of cells in the G1 phase of the cell cycle, thereby inhibiting the growth and proliferation of OSCC. This highlights the tumor-suppressive function of miR-34a, as it not only hinders tumor growth but also provides protection against cell migration and metastasis [97].
The downregulation of miR-34a is observed in precancerous oral conditions as well. This is evidenced by the significantly reduced levels of miR-34a in saliva samples obtained from patients with leukoplakia, compared to saliva samples from corresponding healthy controls. These findings highlight the potential implications of miR-34a in the early stages of oral oncogenesis, as well as into malignant transformation [98]. In addition, it has been observed that the expression levels of miR-34a-5p are markedly reduced in exosomes originating from cancer-associated fibroblasts (CAFs) in OSCC. CAFs play a critical role in promoting malignant progression by releasing exosomes that contain various epigenetic factors, particularly miRNA molecules, which are acquired from neighboring cells. The observed decrease in the expression of miR-34a in OSCC CAFs has been found to be strongly associated with increased cell proliferation and a notable rise in the metastatic capacity of the malignant tumor. In contrast, the upregulation of miR-34a-5p in OSCC CAFs exhibits contrasting outcomes, as it inhibits the progression of OSCC and modulates the tumor's malignant behavior [99].
Contrary to prevailing consensus, a subset of studies has characterized miR-34a as an oncomiR in OSCC, positing its involvement in the pathogenesis and progression of the neoplasm through the facilitation of malignant proliferation [98]. However, these findings have stimulated ongoing debate and controversy. Indeed, a number of studies have demonstrated that miR-34a exhibits increased expression in OSCC tissues in comparison to normal oral specimens. Additionally, elevated levels of the miRNA have been detected in saliva samples from individuals diagnosed with OSCC, leading to its potential application as a non-invasive method for detecting OSCC and aiding in the early diagnosis of cancerous lesions [77,98]. Pertaining to miRNA expression patterns in head and neck SCCs, overexpression of miR-34a has been primarily reported in tissue specimens of laryngeal cancer, as opposed to oral cancerous tissues. However, miR-34a-5p upregulation in both OSCC and laryngeal cancer specimens has been correlated with a better prognosis and lower mortality rates. This further emphasizes the protective effects of miR-34a-5p rather than its oncogenic potential [100].
Known Target Genes and Affected Pathways.
Interleukin 6 receptor (IL6R), which activates the oncogenic STAT3 transcription factor, is a verified direct target of miR-34a that interacts with the 3’UTR of its mRNA [97,101]. It is demonstrated that miR-34a is capable of modulating the intrinsic expression of IL6R is OSCC cells. This is supported by the observation that the mRNA levels of IL6R are significantly decreased in cell lines where miR-34a overexpression has been exogenously induced. In contrast, it has been reported that OSCC cells with diminished expression of miR-34a demonstrate a significant upregulation of the receptor. The upregulation of miR-34a leads to the downregulation of the IL6/STAT3 signaling pathway, primarily mediated by IL6R. Both IL6R and STAT3 levels experience a substantial reduction when miR-34a is upregulated. It is hypothesized that this phenomenon is one of the underlying mechanisms through which miR-34a suppresses proliferation and metastasis. Consequently, the overexpression of miR-34a has been suggested as a potentially effective therapeutic strategy for combating OSCC. The downregulation of miR-34a in OSCC has been observed to have contrasting effects, potentially leading to an upregulation of IL6/STAT3 oncogenic signaling. This, in turn, may contribute to the exacerbation of malignant progression and metastasis in OSCC [97].
Matrix Metalloproteases 9 and 14 (MMP9, MMP14), the expression of which is known to be significantly upregulated in all cancer types, are two additional validated target genes of miR-34a, with binding sites lying on the 3’UTRs of their mRNAs [95,102]. The levels of endogenous proteins MMP9 and MMP14 were found to be significantly decreased due to the overexpression of miR-34a in tongue OSCC cell lines. This reduction in protein levels was also observed to be associated with the inhibition of invasion and migration. In contrast, when miR-34a was suppressed, the expression levels of both metalloproteases exhibited significant increases [95,96]. Furthermore, there are reports indicating that the miR-34a-5p plays a role in regulating the expression levels of its direct target gene AXL, with the aim of inhibiting the proliferation and metastasis of OSCC. The activation of AXL signaling has been linked to increased survival, proliferation, migration, and invasion of cancer cells [99,103]. In the context of OSCC, the overexpression of AXL has been associated with elevated rates of proliferation and migration. This may be attributed to the downregulation of miR-34a, a frequent finding in OSCC, which promotes tumor progression, EMT, and metastasis. These effects are mediated through the overactivation of the AKT/GSK-3β/β-catenin/Snail signaling pathway. Consequently, this pathway upregulates the expression of MMP2 and MMP9, leading to increased aggressiveness and disease progression in OSCC [99].
Finally, the SATB2 (special AT-rich binding protein-2) oncogene, known for its significant involvement in cancer development, is directly targeted by miR-34a. The downregulation of the miR-34a/SATB2 axis has a significant functional impact on the growth, invasion, and migration of OSCC cells. In particular, it was observed that OSCC tissues with reduced levels of miR-34a demonstrate a significant increase in the expression of SATB2. On the contrary, the overexpression of miR-34a had a tumor-suppressive effect by causing a notable decrease in SATB2 expression, thereby inhibiting the proliferation, invasion, and migration associated with OSCC [104,105].
In summary, while a handful of studies have identified miR-34a as an oncogenic molecule, the majority of relevant research consistently emphasizes its significant tumor suppressive function in OSCC. Nevertheless, it is imperative to acknowledge the contentiousness of the expressional findings, as they may indicate a potential duality in its role in oral oncogenesis.
Discussion
Oral cancer, a significant public health concern, encompasses a diverse group of malignancies affecting the oral cavity and oropharynx, represented in most cases by OSCC. Despite advancements in treatment modalities, the prognosis for oral cancer remains suboptimal, emphasizing the need for a better understanding of its molecular mechanisms [8,11]. The genetic basis of OSCC is widely acknowledged and extensively recognized, with key genes playing crucial roles in its development and progression. Tumor suppressor genes, including TP53, CDKN2A, FAT1, CASP8, are frequently altered or inactivated in OSCC, resulting in disrupted cell cycle regulation, enhanced cell survival, and impaired apoptosis. Conversely, oncogenes such as NOTCH1, HRAS, PIK3CA, EGFR, ERBB2, FGFR1-4, FGF2, ETS1, JUN, MKI67, MYC, and BCL2 are often overexpressed or harbor activating mutations, driving increased cell proliferation, invasion, and resistance to cell death [14,19,20,21,22,66,68].
While the genetic landscape of OSCC is well-established, in recent years the focus has turned to epigenetic elements that may be implicated to its pathogenesis and progression, such as miRNAs, which are crucial regulators of gene expression and have the potential to be used as non-invasive diagnostic and prognostic biomarkers, since they can be readily detected in body fluids, paving the way for the development of sensitive and specific tests for OSCC [12,23,100]. Increased research concerning the expression patterns of miRNAs in OSCC during the past few years has generated a vast number of observations, posing challenges in terms of their interpretation. In a general context, the mechanisms underlying cancer development demonstrate significant overlap, leading to the emergence of common patterns in miRNA expression across different types of malignancies being studied. As a result, we are faced with a multitude of findings that hold statistical significance. Nevertheless, it is extremely challenging to definitively assert that these findings truly reflect to OSCC to such a significant degree that they possess the potential to unveil distinctive underlying mechanisms or serve as dependable molecular tests for this specific neoplasm.
Hence, in order to elucidate the most important among the extensive array of observed molecules implicated in the pathogenesis of OSCC, we opted to strategically discern the most crucial and illustrative miRNA molecules associated with this particular malignancy by leveraging the inherent relationship between genetics and epigenetics, focusing on the key genes implicated in every phase of oral oncogenesis. After conducting an in-depth examination of the existing knowledge on miRNA expression in OSCC, we have carefully selected a set of 20 key cell-cycle regulatory genes that have been widely recognized for their significant involvement in OSCC pathogenesis. These genes have been divided into two distinct custom panels, the first comprising 15 oncogenes and the second 5 tumor suppressor genes.
The two custom panels were utilized for identification of all miRNA molecules that are predicted by in silico analysis to target the selected genes. We constructed miRNA/target interaction networks for both oncogene and tumor suppressor panels and from a vast number of miRNA molecules, we have identified a subset of miRNAs that are predicted to target a minimum of 60% of the 15 oncogenes as well as at least 60% of the panel of 5 tumor suppressor genes, The miRNAs that exhibited a significant upregulation in OSCC based on research findings and were predicted to target over 60% of the tumor suppressor gene panel include miR-155-5p, and miR-34a-5p with major target scores of 5/5. In turn, the miRNAs that target at least 60% of the oncogene panel and demonstrate significant downregulation in OSCC were miR-16-5p, miR-1-3p, miR-124-3p and miR-34a-5p with a target score of 9/15, 10/15, 12/15 and 15/15, respectively.
All those miRNAs we portrayed as important and OSCC-specific have been studied in the past, and some of the signaling pathways which are affected by their dysregulation is OSCC have been elucidated. Nevertheless, their regulatory effects on the mRNA and protein expression levels of the factors we included in our analysis remain unexplored. In contrast, the existing research literature primarily has examined alternative gene targets that are not encompassed within our customized gene panels specific to OSCC, but might affect some of the signaling pathways they are involved in, such as the oncogenic PI3K/AKT cascade. In this review, the current understanding on the expression patterns of important OSCC-implicated miRNAs has been thoroughly discussed.
MiR-155-5p, which targets our entire custom OSCC-related tumor suppressor panel, is overexpressed in OSCC tissues and cell lines and has been associated with tumor growth, aggressive OSCC phenotypes, EMT, as well as with lymph node metastasis. The overexpression of miR-155 appears to significantly activate oncogenic signalling pathways by downregulating critical tumor suppressor genes as FoxO3a, ARID2, TP53INP1, CDKN1B, and CDC73, causing cell cycle dysregulation and apoptosis inhibition [34,73,77,78,79,80].
MiR-16-5p, which is anticipated to target 9 genes from our distinct panel of 15 OSCC-associated vital oncogenes, is downregulated in the majority of OSCCs and considered to be a tumor suppressor. Reduced miR-16-5p expression suppresses apoptosis and promotes tumor growth, thus rendering it a reliable prognostic marker for OSCC [34,73,77,78,79,80]. MiR-16 targets multiple genes involved in cell cycle regulation, apoptosis, and metastasis, including BCL2, BCL2L2, MTOR, CCND1, CCND3, SGK3, AKT3, and TLK1. Its downregulation amplifies the oncogenic PI3K/AKT and Wnt/β-catenin signalling pathways, which have been implicated in many malignancies, including OSCC [34,73,77,78,79,80,82,99].
MiR-1-3p that targets 12 of the 15 oncogene genes is typically downregulated in OSCC, thus promoting cell growth and leading to inhibition of apoptotic processes. It is known that miR-1-3p targets EGFR, c-MET, and DKK1 gene transcripts, which are overexpressed and accelerate OSCC progression in cases of miR-1 downregulation [84,85,86,87]. Overexpression of Slug, another miR-1-3p target, promotes OSCC EMT and invasion following miR-1 downregulation [84].
MiR-124-3p has been identified as a tumor suppressor molecule in numerous types of cancer, including OSCC, and is predicted to target 10 of our 15 oncogene panel genes according to our computational analysis. Tissue and saliva samples from patients reveal significant downregulation of this miRNA in OSCC [77,88,90]. In OSCC animal models, miR-124-3p levels exhibit significant decrease within tumor cells [91], while their restoration declines cell proliferation, migration, and invasion [89]. MiR-124-3p exerts tumor suppressive effects by targeting several oncogenes, such as ITGB1, TRIM14, and CCL2, which are overexpressed under miR-124 downregulation, subsequently stimulating oncogenic pathways that include the PI3K/AKT cascade, intense growth factor signalling, or the downregulation of PTEN tumor suppressor in the case of TRIM14 upregulation. These diminish miR-124-induced tumor suppression and promote tumor growth and OSCC progression in turn [89,92,93,99].
Finally, miR-34a-5p scored a perfect 20 in both gene panels. It is predicted to target and may regulate all 15 oncogenes (NOTCH1, HRAS, PIK3CA, EGFR, ERBB2, FGFR1, FGFR2, FGFR3, and FGFR4) and all 5 tumor suppressor genes (TP53, CDKN2A, FAT1, CASP8, and PTEN), which are signature genes in oral oncogenesis. In multiple types of cancer, miR-34a-5p regulates apoptosis, cell cycle, and cellular senescence. OSCC tumor specimens, cells and CAF exosomes exhibit substantially lower miR-34a-5p levels than normal tissues and cell lines. Several studies have shown that this decline is strongly associated with aggressive OSCC characteristics, lymph node metastases, and poor patient prognosis [96,97,98,99]. MiR-34a downregulation in saliva samples from leukoplakia patients also suggests its role in early oral carcinogenesis [98].
It is worth mentioning that, contrary to consensus, a subset of studies has referred to miR-34a as an oncogenic factor in OSCC, positing that its upregulation in OSCC tissues facilitates malignant proliferation and contributes to the pathogenesis and progression of the neoplasm [98]. However, miR-34a-5p upregulation in OSCC cases has been correlated with a better prognosis and lower mortality rates, supporting its protective rather than oncogenic involvement in this particular malignancy [100]. According to the available research findings, miR-34a-5p suppresses tumor growth by targeting IL6R, MMP9, MMP14, AXL, and SATB2 genes, which are upregulated in the typical case of miR-34a suppression in OSCC, therefore overactivating several oncogenic signalling pathways including the IL6/STAT3 and AKT/GSK-3β/β-catenin/Snail cascades [95,97,99].
In summary, our findings suggest that miR-34a-5p, miR-155-5p, miR-124-3p and miR-16-5p are the most representative of OSCC, from a large pool of over 1000 molecules appearing to be associated with OSCC pathogenesis and characteristics. The OSCC-associated predicted targets of these molecules, which have not been explored yet in terms of expression assessment alongside those miRNAs, they might hold the explanation why they experimentally exhibit such typical and consistent expressional patterns in OSCC. But that notion remains to be investigated. Only in the case of miR-16-5p, one of our selected oncogenes BCL2 has been experimentally verified as a target, providing a partial explanation of the tumor suppressive potential of this miRNA [79]. The experimental validation of this specific target aligns with our in silico analysis results, and is indicative that the rest of our strategical computational predictions might potentially be experimentally verified as well, providing evidence that these kind of sequence-based predictions are worthy of further investigation.
The revealing results of this in silico analysis, the roles of miR-34a-5p, miR-155-5p, miR-124-3p, miR-1-3p, and miR-16-5p in oral cancer may provide the basis for additional research to take place in a yet unexplored territory. The study of the expression levels of the 5 miRNAs in relation to the expression levels of major oncogenes and tumor suppressor genes in OSCC specimens compared to normal tissues holds tremendous potential for further research. The comprehensive understanding acquired through investigating the collective expression patterns of these miRNAs and their target genes, which have the highest association with this particular disease, may pave the way for advancements in the diagnosis, prognosis, and personalized future treatment approaches for OSCC.
The benefits of this strategy extend beyond OSCC and have the potential to contribute to cancer research as a whole. By elucidating the complex interplay between miRNAs and their target genes that are characteristically involved in a specific malignancy or pathology in general, it is plausible to unveil disease-specific regulatory mechanisms, as well as to critically assess the extensive corpus of available relevant miRNA expression data, leading hopefully to identification of the characteristic epigenetic signatures of each disease in the future. Hence, this particular strategy has the potential to provide valuable guidance in the design and advancement of novel therapeutic methodologies, such as miRNA-based therapeutics, which exhibit significant promise in the field of precision medicine.
Author Contributions
I.G. conceived and designed the study, researched the literature, performed the bioinformatic analysis and wrote the original draft of the manuscript. S.V. and G.P.C. critically revised the manuscript. C.Y. designed and supervised the study, as well as authored the final draft. All authors have read and agreed to the published version of the manuscript.
Funding
This work was co-financed by the European Regional Development Fund of the European Union and Greek national funds through the Operational Program Competitiveness, Entrepreneurship, and Innovation, under the call RESEARCH-CREATE-INNOVATE (Project code: T2EDK-Milksafe).
Data Availability Statement
The article includes the original contributions presented in this study. Any further inquiries may be forwarded to the corresponding author.
Conflicts of Interest
The authors declare that they have no conflict of interest. The sponsors had no involvement in the study's design, implementation, interpretation, or authorship.
References
- Pare, A.; Joly, A. [Oral cancer: Risk factors and management]. Presse medicale 2017, 46, 320–330. [Google Scholar] [PubMed]
- Ali, K. Oral cancer - the fight must go on against all odds. Evidence-based dentistry 2022, 23, 4–5. [Google Scholar]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nature reviews. Disease primers 2020, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Bugshan, A.; Farooq, I. Oral squamous cell carcinoma: metastasis, potentially associated malignant disorders, etiology and recent advancements in diagnosis. F1000Research 2020, 9, 229. [Google Scholar] [CrossRef]
- Abati, S.; Bramati, C.; Bondi, S.; Lissoni, A.; Trimarchi, M. Oral Cancer and Precancer: A Narrative Review on the Relevance of Early Diagnosis. International journal of environmental research and public health 2020, 17. [Google Scholar] [CrossRef]
- Li, L.; Li, C.; Wang, S.; Wang, Z.; Jiang, J.; Wang, W.; Li, X.; Chen, J.; Liu, K.; Li, C.; et al. Exosomes Derived from Hypoxic Oral Squamous Cell Carcinoma Cells Deliver miR-21 to Normoxic Cells to Elicit a Prometastatic Phenotype. Cancer research 2016, 76, 1770–1780. [Google Scholar] [CrossRef] [PubMed]
- Gharat, S.A.; Momin, M.; Bhavsar, C. Oral Squamous Cell Carcinoma: Current Treatment Strategies and Nanotechnology-Based Approaches for Prevention and Therapy. Critical reviews in therapeutic drug carrier systems 2016, 33, 363–400. [Google Scholar] [CrossRef]
- Khurshid, Z.; Zafar, M.S.; Khan, R.S.; Najeeb, S.; Slowey, P.D.; Rehman, I.U. Role of Salivary Biomarkers in Oral Cancer Detection. Advances in clinical chemistry 2018, 86, 23–70. [Google Scholar]
- Ghantous, Y.; Bahouth, Z.; Abu El-Naaj, I. Clinical and genetic signatures of local recurrence in oral squamous cell carcinoma. Archives of oral biology 2018, 95, 141–148. [Google Scholar] [CrossRef]
- Weckx, A.; Riekert, M.; Grandoch, A.; Schick, V.; Zoller, J.E.; Kreppel, M. Time to recurrence and patient survival in recurrent oral squamous cell carcinoma. Oral oncology 2019, 94, 8–13. [Google Scholar] [CrossRef]
- Fantozzi, P.J.; Bavarian, R.; Tamayo, I.; Bind, M.A.; Woo, S.B.; Villa, A. The role of family history of Cancer in Oral Cavity Cancer. Head & face medicine 2021, 17, 48. [Google Scholar]
- Vatsa, P.P.; Jindal, Y.; Bhadwalkar, J.; Chamoli, A.; Upadhyay, V.; Mandoli, A. Role of epigenetics in OSCC: an understanding above genetics. Medical oncology 2023, 40, 122. [Google Scholar] [CrossRef]
- Sasahira, T.; Kirita, T. Hallmarks of Cancer-Related Newly Prognostic Factors of Oral Squamous Cell Carcinoma. International journal of molecular sciences 2018, 19. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh, A.; Rao, K.N.; Arora, R.D.; Nagarkar, N.M.; Singh, A.; Shetty, O.S. Molecular Insights into Oral Malignancy. Indian journal of surgical oncology 2022, 13, 267–280. [Google Scholar] [CrossRef]
- Yapijakis, C. Regulatory Role of MicroRNAs in Brain Development and Function. Advances in experimental medicine and biology 2020, 1195, 237–247. [Google Scholar]
- Di Leva, G.; Garofalo, M.; Croce, C.M. MicroRNAs in cancer. Annual review of pathology 2014, 9, 287–314. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, R.D.; Pattatheyil, A.; Roychoudhury, S. Functional Landscape of Dysregulated MicroRNAs in Oral Squamous Cell Carcinoma: Clinical Implications. Frontiers in oncology 2020, 10, 619. [Google Scholar] [CrossRef]
- Palaia, G.; Pippi, R.; Rocchetti, F.; Caputo, M.; Macali, F.; Mohsen, A.; Del Vecchio, A.; Tenore, G.; Romeo, U. Liquid biopsy in the assessment of microRNAs in oral squamous cell carcinoma: A systematic review. Journal of clinical and experimental dentistry 2022, 14, e875–e884. [Google Scholar] [CrossRef]
- Kim, S.; Lee, J.W.; Park, Y.S. The Application of Next-Generation Sequencing to Define Factors Related to Oral Cancer and Discover Novel Biomarkers. Life 2020, 10. [Google Scholar] [CrossRef]
- Shanmugam, A.; Hariharan, A.K.; Hasina, R.; Nair, J.R.; Katragadda, S.; Irusappan, S.; Ravichandran, A.; Veeramachaneni, V.; Bettadapura, R.; Bhati, M.; et al. Ultrasensitive detection of tumor-specific mutations in saliva of patients with oral cavity squamous cell carcinoma. Cancer 2021, 127, 1576–1589. [Google Scholar] [CrossRef]
- Starzynska, A.; Adamska, P.; Sejda, A.; Sakowicz-Burkiewicz, M.; Adamski, L.J.; Marvaso, G.; Wychowanski, P.; Jereczek-Fossa, B.A. Any Role of PIK3CA and PTEN Biomarkers in the Prognosis in Oral Squamous Cell Carcinoma? Life 2020, 10. [Google Scholar] [CrossRef]
- Vairaktaris, E.; Loukeri, S.; Vassiliou, S.; Nkenke, E.; Spyridonidou, S.; Vylliotis, A.; Papakosta, V.; Lazaris, A.; Agrogiannis, G.; Yapijakis, C.; et al. EGFR and c-Jun exhibit the same pattern of expression and increase gradually during the progress of oral oncogenesis. In vivo 2007, 21, 791–796. [Google Scholar]
- Yapijakis, C.; Kalogera, S.; Papakosta, V.; Vassiliou, S. The Hamster Model of Sequential Oral Carcinogenesis: An Update. In vivo 2019, 33, 1751–1755. [Google Scholar] [CrossRef] [PubMed]
- Vairaktaris, E.; Spyridonidou, S.; Papakosta, V.; Vylliotis, A.; Lazaris, A.; Perrea, D.; Yapijakis, C.; Patsouris, E. The hamster model of sequential oral oncogenesis. Oral oncology 2008, 44, 315–324. [Google Scholar] [CrossRef] [PubMed]
- D'Cruz, A.; Dechamma, P.N.; Saldanha, M.; Maben, S.; Shetty, P.; Chakraborty, A. Non-Invasive Saliva-based Detection of Gene Mutations in Oral Cancer Patients by Oral Rub and Rinse Technique. Asian Pacific journal of cancer prevention: APJCP 2021, 22, 3287–3291. [Google Scholar] [CrossRef] [PubMed]
- Levine, A.J.; Oren, M. The first 30 years of p53: growing ever more complex. Nature reviews. Cancer 2009, 9, 749–758. [Google Scholar] [CrossRef] [PubMed]
- Lindemann, A.; Takahashi, H.; Patel, A.A.; Osman, A.A.; Myers, J.N. Targeting the DNA Damage Response in OSCC with TP53 Mutations. Journal of dental research 2018, 97, 635–644. [Google Scholar] [CrossRef]
- Hyodo, T.; Kuribayashi, N.; Fukumoto, C.; Komiyama, Y.; Shiraishi, R.; Kamimura, R.; Sawatani, Y.; Yaguchi, E.; Hasegawa, T.; Izumi, S.; et al. The mutational spectrum in whole exon of p53 in oral squamous cell carcinoma and its clinical implications. Scientific reports 2022, 12, 21695. [Google Scholar] [CrossRef]
- Szturz, P.; Wouters, K.; Kiyota, N.; Tahara, M.; Prabhash, K.; Noronha, V.; Adelstein, D.; Vermorken, J.B. Altered fractionation radiotherapy combined with concurrent low-dose or high-dose cisplatin in head and neck cancer: A systematic review of literature and meta-analysis. Oral oncology 2018, 76, 52–60. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, L.; Tan, X.; Lin, Y.; Han, X.; Wang, H.; Ming, H.; Li, Q.; Liu, K.; Feng, G. Systematic analysis of genes involved in oral cancer metastasis to lymph nodes. Cellular & molecular biology letters 2018, 23, 53. [Google Scholar]
- Shima, K.; Nosho, K.; Baba, Y.; Cantor, M.; Meyerhardt, J.A.; Giovannucci, E.L.; Fuchs, C.S.; Ogino, S. Prognostic significance of CDKN2A (p16) promoter methylation and loss of expression in 902 colorectal cancers: Cohort study and literature review. International journal of cancer 2011, 128, 1080–1094. [Google Scholar] [CrossRef] [PubMed]
- Padhi, S.S.; Roy, S.; Kar, M.; Saha, A.; Roy, S.; Adhya, A.; Baisakh, M.; Banerjee, B. Role of CDKN2A/p16 expression in the prognostication of oral squamous cell carcinoma. Oral oncology 2017, 73, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Stransky, N.; Egloff, A.M.; Tward, A.D.; Kostic, A.D.; Cibulskis, K.; Sivachenko, A.; Kryukov, G.V.; Lawrence, M.S.; Sougnez, C.; McKenna, A.; et al. The mutational landscape of head and neck squamous cell carcinoma. Science 2011, 333, 1157–1160. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Zhai, Y.; Shi, R.; Qian, Y.; Cui, H.; Yang, J.; Bi, Y.; Yan, T.; Yang, J.; Ma, Y.; et al. FAT1 inhibits cell migration and invasion by affecting cellular mechanical properties in esophageal squamous cell carcinoma. Oncology reports 2018, 39, 2136–2146. [Google Scholar] [CrossRef]
- Tang, Y.I.; Liu, Y.; Zhao, W.; Yu, T.; Yu, H. Caspase-8 polymorphisms and risk of oral squamous cell carcinoma. Experimental and therapeutic medicine 2015, 10, 2267–2276. [Google Scholar] [CrossRef]
- Hayes, T.F.; Benaich, N.; Goldie, S.J.; Sipila, K.; Ames-Draycott, A.; Cai, W.; Yin, G.; Watt, F.M. Integrative genomic and functional analysis of human oral squamous cell carcinoma cell lines reveals synergistic effects of FAT1 and CASP8 inactivation. Cancer letters 2016, 383, 106–114. [Google Scholar] [CrossRef]
- Xi, Y.; Negrao, M.V.; Akagi, K.; Xiao, W.; Jiang, B.; Warner, S.C.; Dunn, J.D.; Wang, J.; Symer, D.E.; Gillison, M.L. Noninvasive genomic profiling of somatic mutations in oral cavity cancers. Oral oncology 2023, 140, 106372. [Google Scholar] [CrossRef]
- Kurasawa, Y.; Shiiba, M.; Nakamura, M.; Fushimi, K.; Ishigami, T.; Bukawa, H.; Yokoe, H.; Uzawa, K.; Tanzawa, H. PTEN expression and methylation status in oral squamous cell carcinoma. Oncology reports 2008, 19, 1429–1434. [Google Scholar]
- Purow, B. Notch inhibition as a promising new approach to cancer therapy. Advances in experimental medicine and biology 2012, 727, 305–319. [Google Scholar]
- Fukusumi, T.; Califano, J.A. The NOTCH Pathway in Head and Neck Squamous Cell Carcinoma. Journal of dental research 2018, 97, 645–653. [Google Scholar] [CrossRef]
- Pickering, C.R.; Zhang, J.; Yoo, S.Y.; Bengtsson, L.; Moorthy, S.; Neskey, D.M.; Zhao, M.; Ortega Alves, M.V.; Chang, K.; Drummond, J.; et al. Integrative genomic characterization of oral squamous cell carcinoma identifies frequent somatic drivers. Cancer discovery 2013, 3, 770–781. [Google Scholar] [CrossRef] [PubMed]
- Pylayeva-Gupta, Y.; Grabocka, E.; Bar-Sagi, D. RAS oncogenes: weaving a tumorigenic web. Nature reviews. Cancer 2011, 11, 761–774. [Google Scholar] [CrossRef] [PubMed]
- Alshahrani, S.A.; Al-Qahtani, W.S.; Almufareh, N.A.; Domiaty, D.M.; Albasher, G.I.; Safhi, F.A.; AlQassim, F.A.; Alotaibi, M.A.; Al-Hazani, T.M.; Almutlaq, B.A. Oral cancer among Khat users: finding evidence from DNA analysis of nine cancer-related gene mutations. BMC oral health 2021, 21, 626. [Google Scholar] [CrossRef]
- Simpson, D.R.; Mell, L.K.; Cohen, E.E. Targeting the PI3K/AKT/mTOR pathway in squamous cell carcinoma of the head and neck. Oral oncology 2015, 51, 291–298. [Google Scholar] [CrossRef]
- Cohen, Y.; Goldenberg-Cohen, N.; Shalmon, B.; Shani, T.; Oren, S.; Amariglio, N.; Dratviman-Storobinsky, O.; Shnaiderman-Shapiro, A.; Yahalom, R.; Kaplan, I.; et al. Mutational analysis of PTEN/PIK3CA/AKT pathway in oral squamous cell carcinoma. Oral oncology 2011, 47, 946–950. [Google Scholar] [CrossRef] [PubMed]
- Brand, T.M.; Iida, M.; Wheeler, D.L. Molecular mechanisms of resistance to the EGFR monoclonal antibody cetuximab. Cancer biology & therapy 2011, 11, 777–792. [Google Scholar]
- Slamon, D.J.; Clark, G.M.; Wong, S.G.; Levin, W.J.; Ullrich, A.; McGuire, W.L. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987, 235, 177–182. [Google Scholar] [CrossRef]
- Popovic, B.; Jekic, B.; Novakovic, I.; Lukovic, L.; Konstantinovic, V.; Babic, M.; Milasin, J. Cancer genes alterations and HPV infection in oral squamous cell carcinoma. International journal of oral and maxillofacial surgery 2010, 39, 909–915. [Google Scholar] [CrossRef]
- Jelovac, D.B.; Tepavcevic, Z.; Nikolic, N.; Ilic, B.; Eljabo, N.; Popovic, B.; Carkic, J.; Konstantinovic, V.; Vukadinovic, M.; Milicic, B.; et al. The amplification of c-erb-B2 in cancer-free surgical margins is a predictor of poor outcome in oral squamous cell carcinoma. International journal of oral and maxillofacial surgery 2016, 45, 700–705. [Google Scholar] [CrossRef]
- Dai, S.; Zhou, Z.; Chen, Z.; Xu, G.; Chen, Y. Fibroblast Growth Factor Receptors (FGFRs): Structures and Small Molecule Inhibitors. Cells 2019, 8. [Google Scholar] [CrossRef]
- Xie, X.; Wang, Z.; Chen, F.; Yuan, Y.; Wang, J.; Liu, R.; Chen, Q. Roles of FGFR in oral carcinogenesis. Cell proliferation 2016, 49, 261–269. [Google Scholar] [CrossRef]
- Lopes, V.K.M.; Jesus, A.S.; Souza, L.L.; Miyahara, L.A.N.; Guimaraes, D.M.; Pontes, H.A.R.; Pontes, F.S.C.; Carvalho, P.L. Ki-67 protein predicts survival in oral squamous carcinoma cells: an immunohistochemical study. Brazilian oral research 2017, 31, e66. [Google Scholar] [CrossRef] [PubMed]
- Nayak, S.; Goel, M.M.; Makker, A.; Bhatia, V.; Chandra, S.; Kumar, S.; Agarwal, S.P. Fibroblast Growth Factor (FGF-2) and Its Receptors FGFR-2 and FGFR-3 May Be Putative Biomarkers of Malignant Transformation of Potentially Malignant Oral Lesions into Oral Squamous Cell Carcinoma. PloS one 2015, 10, e0138801. [Google Scholar] [CrossRef]
- Raimondi, A.R.; Molinolo, A.A.; Itoiz, M.E. Fibroblast growth factor-2 expression during experimental oral carcinogenesis. Its possible role in the induction of pre-malignant fibrosis. Journal of oral pathology & medicine: official publication of the International Association of Oral Pathologists and the American Academy of Oral Pathology 2006, 35, 212–217. [Google Scholar]
- Gluck, C.; Glathar, A.; Tsompana, M.; Nowak, N.; Garrett-Sinha, L.A.; Buck, M.J.; Sinha, S. Molecular dissection of the oncogenic role of ETS1 in the mesenchymal subtypes of head and neck squamous cell carcinoma. PLoS genetics 2019, 15, e1008250. [Google Scholar] [CrossRef] [PubMed]
- Pande, P.; Soni, S.; Chakravarti, N.; Mathur, M.; Shukla, N.K.; Ralhan, R. Prognostic impact of Ets-1 overexpression in betel and tobacco related oral cancer. Cancer detection and prevention 2001, 25, 496–501. [Google Scholar] [PubMed]
- Sheng, X.; Li, X.; Qian, Y.; Wang, S.; Xiao, C. ETS1 regulates NDRG1 to promote the proliferation, migration, and invasion of OSCC. Oral diseases 2023. [Google Scholar] [CrossRef]
- Gupta, S.; Gupta, S. Role of human papillomavirus in oral squamous cell carcinoma and oral potentially malignant disorders: A review of the literature. Indian journal of dentistry 2015, 6, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Jin, X.; Yuan, Y.; Deng, P.; Jiang, L.; Zeng, X.; Li, X.S.; Wang, Z.Y.; Chen, Q.M. Prognostic value from integrative analysis of transcription factors c-Jun and Fra-1 in oral squamous cell carcinoma: a multicenter cohort study. Scientific reports 2017, 7, 7522. [Google Scholar] [CrossRef] [PubMed]
- Perez-Sayans, M.; Suarez-Penaranda, J.M.; Pilar, G.D.; Barros-Angueira, F.; Gandara-Rey, J.M.; Garcia-Garcia, A. What real influence does the proto-oncogene c-myc have in OSCC behavior? Oral oncology 2011, 47, 688–692. [Google Scholar] [CrossRef]
- Hu, L.; Liu, J.; Li, Z.; Wang, C.; Nawshad, A. Transforming growth factor-beta1 activates DeltaNp63/c-Myc to promote oral squamous cell carcinoma. Oral surgery, oral medicine, oral pathology and oral radiology 2016, 122, 460–482.e464. [Google Scholar] [CrossRef] [PubMed]
- Pallavi, N.; Nalabolu, G.R.K.; Hiremath, S.K.S. Bcl-2 and c-Myc expression in oral dysplasia and oral squamous cell carcinoma: An immunohistochemical study to assess tumor progression. Journal of oral and maxillofacial pathology: JOMFP 2018, 22, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.M.; Bao, Y.; Li, T.K.; Di, Y.B.; Song, W.J. MKI67 an potential oncogene of oral squamous cell carcinoma via the high throughput technology. Medicine 2022, 101, e32595. [Google Scholar] [CrossRef]
- Dragomir, L.P.; Simionescu, C.; Margaritescu, C.; Stepan, A.; Dragomir, I.M.; Popescu, M.R. P53, p16 and Ki67 immunoexpression in oral squamous carcinomas. Romanian journal of morphology and embryology = Revue roumaine de morphologie et embryologie 2012, 53, 89–93. [Google Scholar] [PubMed]
- Sudha, V.M.; Hemavathy, S. Role of bcl-2 oncoprotein in oral potentially malignant disorders and squamous cell carcinoma: an immunohistochemical study. Indian journal of dental research: official publication of Indian Society for Dental Research 2011, 22, 520–525. [Google Scholar] [PubMed]
- Arya, V.; Singh, S.; Daniel, M.J. Clinicopathological correlation of Bcl-2 oncoprotein expression in oral precancer and cancer. Journal of oral biology and craniofacial research 2016, 6, 18–23. [Google Scholar] [CrossRef]
- Rahmani, A.; Alzohairy, M.; Babiker, A.Y.; Rizvi, M.A.; Elkarimahmad, H.G. Clinicopathological significance of PTEN and bcl2 expressions in oral squamous cell carcinoma. International journal of clinical and experimental pathology 2012, 5, 965–971. [Google Scholar]
- Dwivedi, R.; Chandra, S.; Mehrotra, D.; Raj, V.; Pandey, R. Predicting transition from oral pre-malignancy to malignancy via Bcl-2 immuno-expression: Evidence and lacunae. Journal of oral biology and craniofacial research 2020, 10, 397–403. [Google Scholar] [CrossRef]
- Mehterov, N.; Sacconi, A.; Pulito, C.; Vladimirov, B.; Haralanov, G.; Pazardjikliev, D.; Nonchev, B.; Berindan-Neagoe, I.; Blandino, G.; Sarafian, V. A novel panel of clinically relevant miRNAs signature accurately differentiates oral cancer from normal mucosa. Frontiers in oncology 2022, 12, 1072579. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Duan, Q.; Liu, X.; Zhang, P.; Fu, Y.; Zhang, Z.; Liu, L.; Cheng, J.; Jiang, H. MiR-155-5p promotes oral cancer progression by targeting chromatin remodeling gene ARID2. Biomedicine & pharmacotherapy = Biomedecine & pharmacotherapie 2020, 122, 109696. [Google Scholar]
- Baba, O.; Hasegawa, S.; Nagai, H.; Uchida, F.; Yamatoji, M.; Kanno, N.I.; Yamagata, K.; Sakai, S.; Yanagawa, T.; Bukawa, H. MicroRNA-155-5p is associated with oral squamous cell carcinoma metastasis and poor prognosis. Journal of oral pathology & medicine: official publication of the International Association of Oral Pathologists and the American Academy of Oral Pathology 2016, 45, 248–255. [Google Scholar]
- D'Souza, W.; Kumar, A. microRNAs in oral cancer: Moving from bench to bed as next generation medicine. Oral oncology 2020, 111, 104916. [Google Scholar] [CrossRef] [PubMed]
- Erfanparast, L.; Taghizadieh, M.; Shekarchi, A.A. Non-Coding RNAs and Oral Cancer: Small Molecules With Big Functions. Frontiers in oncology 2022, 12, 914593. [Google Scholar] [CrossRef]
- Liu, B.; Hu, J.; Zhao, H.; Zhao, L.; Pan, S. MicroRNA-155-5p Contributes to 5-Fluorouracil Resistance Through Down-Regulating TP53INP1 in Oral Squamous Cell Carcinoma. Frontiers in oncology 2021, 11, 706095. [Google Scholar] [CrossRef]
- Aali, M.; Mesgarzadeh, A.H.; Najjary, S.; Abdolahi, H.M.; Kojabad, A.B.; Baradaran, B. Evaluating the role of microRNAs alterations in oral squamous cell carcinoma. Gene 2020, 757, 144936. [Google Scholar] [CrossRef]
- Hu, S.; Wang, H.; Yan, D.; Lu, W.; Gao, P.; Lou, W.; Kong, X. Loss of miR-16 contributes to tumor progression by activation of tousled-like kinase 1 in oral squamous cell carcinoma. Cell cycle 2018, 17, 2284–2295. [Google Scholar] [CrossRef] [PubMed]
- Rishabh, K.; Khadilkar, S.; Kumar, A.; Kalra, I.; Kumar, A.P.; Kunnumakkara, A.B. MicroRNAs as Modulators of Oral Tumorigenesis-A Focused Review. International journal of molecular sciences 2021, 22. [Google Scholar] [CrossRef]
- Wang, X.; Li, G.H. MicroRNA-16 functions as a tumor-suppressor gene in oral squamous cell carcinoma by targeting AKT3 and BCL2L2. Journal of cellular physiology 2018, 233, 9447–9457. [Google Scholar] [CrossRef]
- Manikandan, M.; Deva Magendhra Rao, A.K.; Arunkumar, G.; Manickavasagam, M.; Rajkumar, K.S.; Rajaraman, R.; Munirajan, A.K. Oral squamous cell carcinoma: microRNA expression profiling and integrative analyses for elucidation of tumourigenesis mechanism. Molecular cancer 2016, 15, 28. [Google Scholar] [CrossRef]
- Troiano, G.; Mastrangelo, F.; Caponio, V.C.A.; Laino, L.; Cirillo, N.; Lo Muzio, L. Predictive Prognostic Value of Tissue-Based MicroRNA Expression in Oral Squamous Cell Carcinoma: A Systematic Review and Meta-analysis. Journal of dental research 2018, 97, 759–766. [Google Scholar] [CrossRef]
- Maclellan, S.A.; Lawson, J.; Baik, J.; Guillaud, M.; Poh, C.F.; Garnis, C. Differential expression of miRNAs in the serum of patients with high-risk oral lesions. Cancer medicine 2012, 1, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Khalil, M.I.; Madere, C.; Ghosh, I.; Adam, R.M.; De Benedetti, A. Interaction of TLK1 and AKTIP as a Potential Regulator of AKT Activation in Castration-Resistant Prostate Cancer Progression. Pathophysiology: the official journal of the International Society for Pathophysiology 2021, 28, 339–354. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Jiang, H.; Zhao, J.; Wen, H. MiRNA-16 inhibited oral squamous carcinoma tumor growth in vitro and in vivo via suppressing Wnt/beta-catenin signaling pathway. OncoTargets and therapy 2018, 11, 5111–5119. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.Y.; Liao, Y.W.; Lu, M.Y.; Yu, C.H.; Yu, C.C.; Chou, M.Y. Downregulation of miR-1 enhances tumorigenicity and invasiveness in oral squamous cell carcinomas. Journal of the Formosan Medical Association = Taiwan yi zhi 2017, 116, 782–789. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, J.; Chen, Z.; Wang, K.; Shi, L. MicroRNA-1-3p inhibits the proliferation and migration of oral squamous cell carcinoma cells by targeting DKK1. Biochemistry and cell biology = Biochimie et biologie cellulaire 2018, 96, 355–364. [Google Scholar] [CrossRef]
- Koshizuka, K.; Hanazawa, T.; Fukumoto, I.; Kikkawa, N.; Matsushita, R.; Mataki, H.; Mizuno, K.; Okamoto, Y.; Seki, N. Dual-receptor (EGFR and c-MET) inhibition by tumor-suppressive miR-1 and miR-206 in head and neck squamous cell carcinoma. Journal of human genetics 2017, 62, 113–121. [Google Scholar] [CrossRef]
- Organ, S.L.; Tsao, M.S. An overview of the c-MET signaling pathway. Therapeutic advances in medical oncology 2011, 3, S7–S19. [Google Scholar] [CrossRef]
- Al Rawi, N.; Elmabrouk, N.; Abu Kou, R.; Mkadmi, S.; Rizvi, Z.; Hamdoon, Z. The role of differentially expressed salivary microRNA in oral squamous cell carcinoma. A systematic review. Archives of oral biology 2021, 125, 105108. [Google Scholar] [CrossRef]
- Hunt, S.; Jones, A.V.; Hinsley, E.E.; Whawell, S.A.; Lambert, D.W. MicroRNA-124 suppresses oral squamous cell carcinoma motility by targeting ITGB1. FEBS letters 2011, 585, 187–192. [Google Scholar] [CrossRef]
- Salazar-Ruales, C.; Arguello, J.V.; Lopez-Cortes, A.; Cabrera-Andrade, A.; Garcia-Cardenas, J.M.; Guevara-Ramirez, P.; Peralta, P.; Leone, P.E.; Paz, Y.M.C. Salivary MicroRNAs for Early Detection of Head and Neck Squamous Cell Carcinoma: A Case-Control Study in the High Altitude Mestizo Ecuadorian Population. BioMed research international 2018, 2018, 9792730. [Google Scholar] [CrossRef]
- Li, X.; Fan, Q.; Li, J.; Song, J.; Gu, Y. MiR-124 down-regulation is critical for cancer associated fibroblasts-enhanced tumor growth of oral carcinoma. Experimental cell research 2017, 351, 100–108. [Google Scholar] [CrossRef]
- Qiao, C.Y.; Qiao, T.Y.; Jin, H.; Liu, L.L.; Zheng, M.D.; Wang, Z.L. LncRNA KCNQ1OT1 contributes to the cisplatin resistance of tongue cancer through the KCNQ1OT1/miR-124-3p/TRIM14 axis. European review for medical and pharmacological sciences 2020, 24, 200–212. [Google Scholar] [PubMed]
- Xu, M.; Wang, Y.; Xia, R.; Wei, Y.; Wei, X. Role of the CCL2-CCR2 signalling axis in cancer: Mechanisms and therapeutic targeting. Cell proliferation 2021, 54, e13115. [Google Scholar] [CrossRef]
- Shen, W.; Jin, Z.; Tong, X.; Wang, H.; Zhuang, L.; Lu, X.; Wu, S. TRIM14 promotes cell proliferation and inhibits apoptosis by suppressing PTEN in colorectal cancer. Cancer management and research 2019, 11, 5725–5735. [Google Scholar] [CrossRef]
- Jia, L.F.; Wei, S.B.; Mitchelson, K.; Gao, Y.; Zheng, Y.F.; Meng, Z.; Gan, Y.H.; Yu, G.Y. miR-34a inhibits migration and invasion of tongue squamous cell carcinoma via targeting MMP9 and MMP14. PloS one 2014, 9, e108435. [Google Scholar] [CrossRef]
- Jadhav, K.B.; Shah, V.; Chauhan, N.; Shah, N.; Parmar, G. Expression of microRNA-21 in saliva and tumor tissue of patients with oral squamous cell carcinoma: a predictor of cervical lymph node metastasis. Oral surgery, oral medicine, oral pathology and oral radiology 2022, 133, 60–69. [Google Scholar] [CrossRef]
- Li, T.; Li, L.; Li, D.; Wang, S.; Sun, J. MiR-34a inhibits oral cancer progression partially by repression of interleukin-6-receptor. International journal of clinical and experimental pathology 2015, 8, 1364–1373. [Google Scholar] [PubMed]
- Manzano-Moreno, F.J.; Costela-Ruiz, V.J.; Garcia-Recio, E.; Olmedo-Gaya, M.V.; Ruiz, C.; Reyes-Botella, C. Role of Salivary MicroRNA and Cytokines in the Diagnosis and Prognosis of Oral Squamous Cell Carcinoma. International journal of molecular sciences 2021, 22. [Google Scholar] [CrossRef]
- Li, Y.Y.; Tao, Y.W.; Gao, S.; Li, P.; Zheng, J.M.; Zhang, S.E.; Liang, J.; Zhang, Y. Cancer-associated fibroblasts contribute to oral cancer cells proliferation and metastasis via exosome-mediated paracrine miR-34a-5p. EBioMedicine 2018, 36, 209–220. [Google Scholar] [CrossRef]
- Piotrowski, I.; Zhu, X.; Saccon, T.D.; Ashiqueali, S.; Schneider, A.; de Carvalho Nunes, A.D.; Noureddine, S.; Sobecka, A.; Barczak, W.; Szewczyk, M.; et al. miRNAs as Biomarkers for Diagnosing and Predicting Survival of Head and Neck Squamous Cell Carcinoma Patients. Cancers 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Rokavec, M.; Oner, M.G.; Li, H.; Jackstadt, R.; Jiang, L.; Lodygin, D.; Kaller, M.; Horst, D.; Ziegler, P.K.; Schwitalla, S.; et al. IL-6R/STAT3/miR-34a feedback loop promotes EMT-mediated colorectal cancer invasion and metastasis. The Journal of clinical investigation 2014, 124, 1853–1867. [Google Scholar] [CrossRef]
- Gobin, E.; Bagwell, K.; Wagner, J.; Mysona, D.; Sandirasegarane, S.; Smith, N.; Bai, S.; Sharma, A.; Schleifer, R.; She, J.X. A pan-cancer perspective of matrix metalloproteases (MMP) gene expression profile and their diagnostic/prognostic potential. BMC cancer 2019, 19, 581. [Google Scholar] [CrossRef]
- Zhu, C.; Wei, Y.; Wei, X. AXL receptor tyrosine kinase as a promising anti-cancer approach: functions, molecular mechanisms and clinical applications. Molecular cancer 2019, 18, 153. [Google Scholar] [CrossRef]
- Ge, X.; Gao, J.; Sun, Q.W.; Wang, C.X.; Deng, W.; Mao, G.Y.; Li, H.Q.; Guo, S.S.; Cheng, J.; Wu, Y.N.; et al. MiR-34a inhibits the proliferation, migration, and invasion of oral squamous cell carcinoma by directly targeting SATB2. Journal of cellular physiology 2020, 235, 4856–4864. [Google Scholar] [CrossRef]
- Roy, S.K.; Shrivastava, A.; Srivastav, S.; Shankar, S.; Srivastava, R.K. SATB2 is a novel biomarker and therapeutic target for cancer. Journal of cellular and molecular medicine 2020, 24, 11064–11069. [Google Scholar] [CrossRef]
- Shiah, S.G.; Chou, S.T.; Chang, J.Y. MicroRNAs: Their Role in Metabolism, Tumor Microenvironment, and Therapeutic Implications in Head and Neck Squamous Cell Carcinoma. Cancers 2021, 13. [Google Scholar] [CrossRef]
- Menini, M.; De Giovanni, E.; Bagnasco, F.; Delucchi, F.; Pera, F.; Baldi, D.; Pesce, P. Salivary Micro-RNA and Oral Squamous Cell Carcinoma: A Systematic Review. Journal of personalized medicine 2021, 11. [Google Scholar] [CrossRef]
Figure 1.
The miRNA/target interaction network illustrates the 437 miRNA molecules that are predicted to target one or more genes within our custom panel of tumor suppressor genes specific OSCC, namely TP53, CDKN2A, FAT1, CASP8, and PTEN. The genes encompassing the panel are visually represented by the color pink, whereas the miRNA molecules that are anticipated to target at least one of these genes are visualized by the color blue.
Figure 1.
The miRNA/target interaction network illustrates the 437 miRNA molecules that are predicted to target one or more genes within our custom panel of tumor suppressor genes specific OSCC, namely TP53, CDKN2A, FAT1, CASP8, and PTEN. The genes encompassing the panel are visually represented by the color pink, whereas the miRNA molecules that are anticipated to target at least one of these genes are visualized by the color blue.
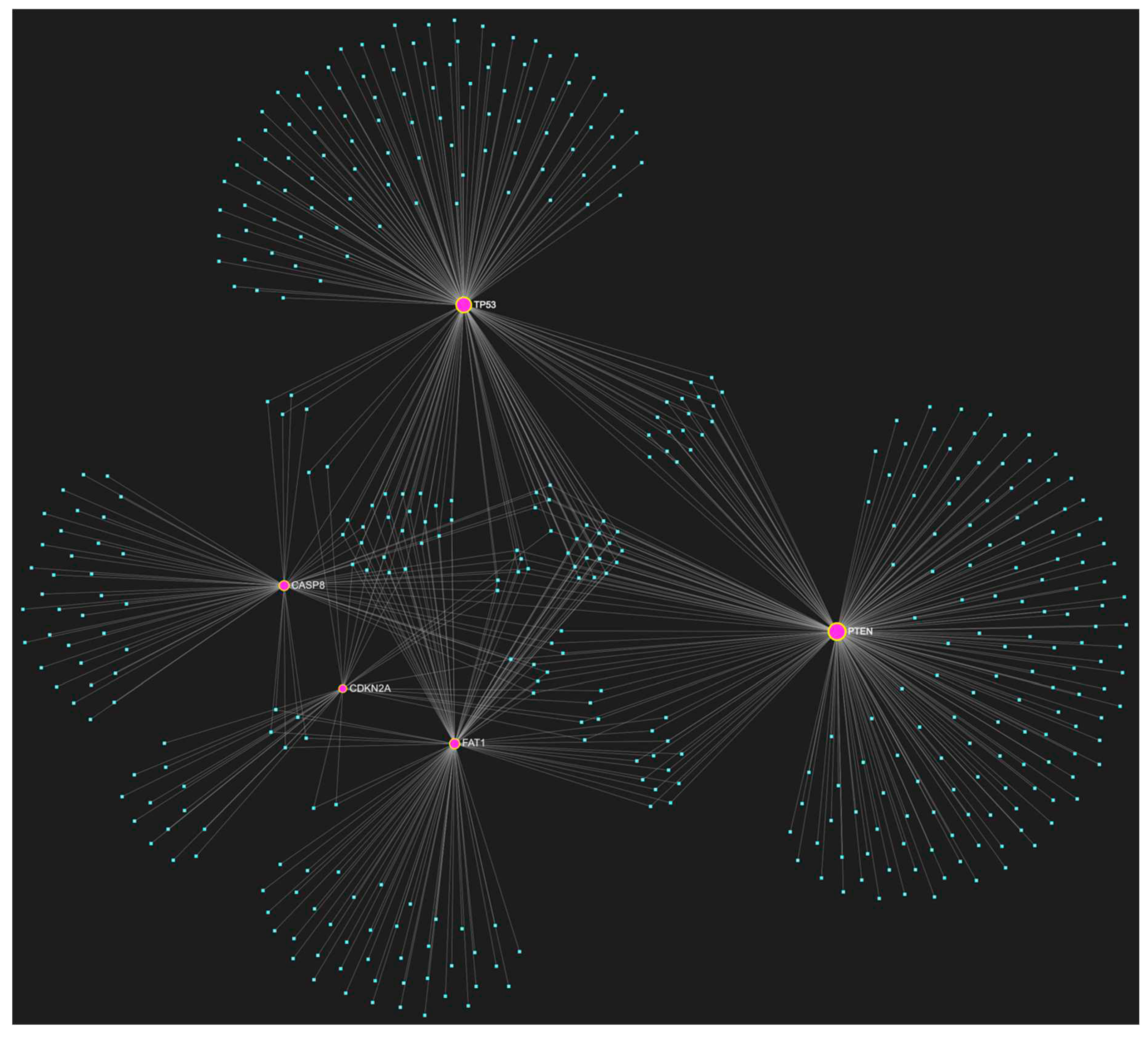
Figure 2.
The miRNA/target interaction network illustrates the 828 miRNA molecules that are predicted to target at least one gene within our custom panel of oncogenes specific to OSCC. The oncogenes included in the panel are NOTCH1, HRAS, PIK3CA, EGFR, ERBB2, FGFR1, FGFR2, FGFR3, FGFR4, FGF2, ETS1, JUN, MKI67, MYC, and BCL2. The genes encompassing the panel are visually represented by the color pink, whereas the miRNA molecules that are anticipated to target at least one of these genes are visualized by the color blue.
Figure 2.
The miRNA/target interaction network illustrates the 828 miRNA molecules that are predicted to target at least one gene within our custom panel of oncogenes specific to OSCC. The oncogenes included in the panel are NOTCH1, HRAS, PIK3CA, EGFR, ERBB2, FGFR1, FGFR2, FGFR3, FGFR4, FGF2, ETS1, JUN, MKI67, MYC, and BCL2. The genes encompassing the panel are visually represented by the color pink, whereas the miRNA molecules that are anticipated to target at least one of these genes are visualized by the color blue.
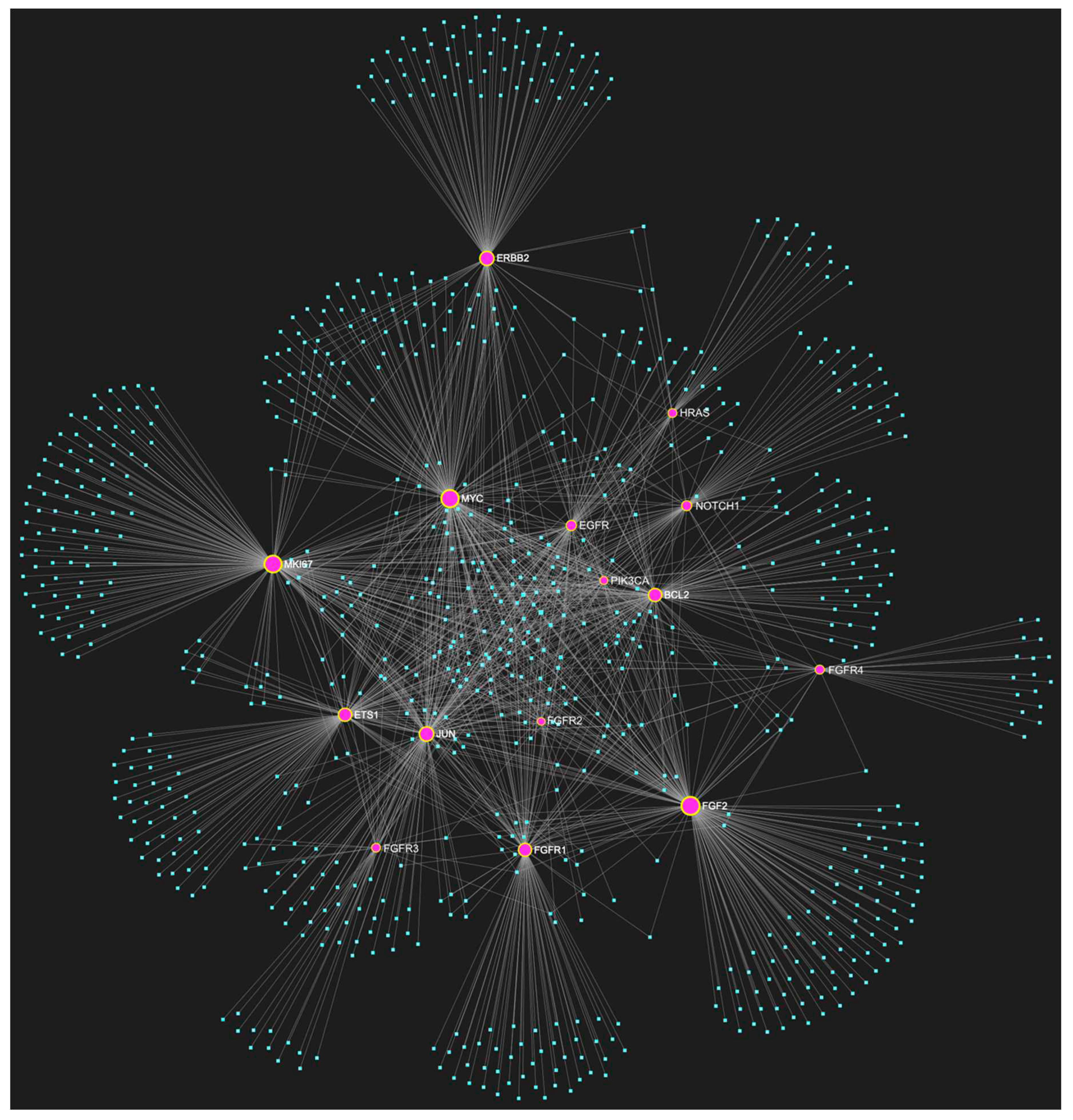
Figure 3.
MiR-155-5p, a well-documented upregulated microRNA in OSCC, is predicted to target all five tumor suppressor genes included in our custom OSCC-specific tumor suppressor gene panel (TP53, CDKN2A, FAT1, CASP8, PTEN). The depicted elements in yellow represent the genes that are specifically targeted by miR-155-5p, along with their corresponding connecting nodes.
Figure 3.
MiR-155-5p, a well-documented upregulated microRNA in OSCC, is predicted to target all five tumor suppressor genes included in our custom OSCC-specific tumor suppressor gene panel (TP53, CDKN2A, FAT1, CASP8, PTEN). The depicted elements in yellow represent the genes that are specifically targeted by miR-155-5p, along with their corresponding connecting nodes.
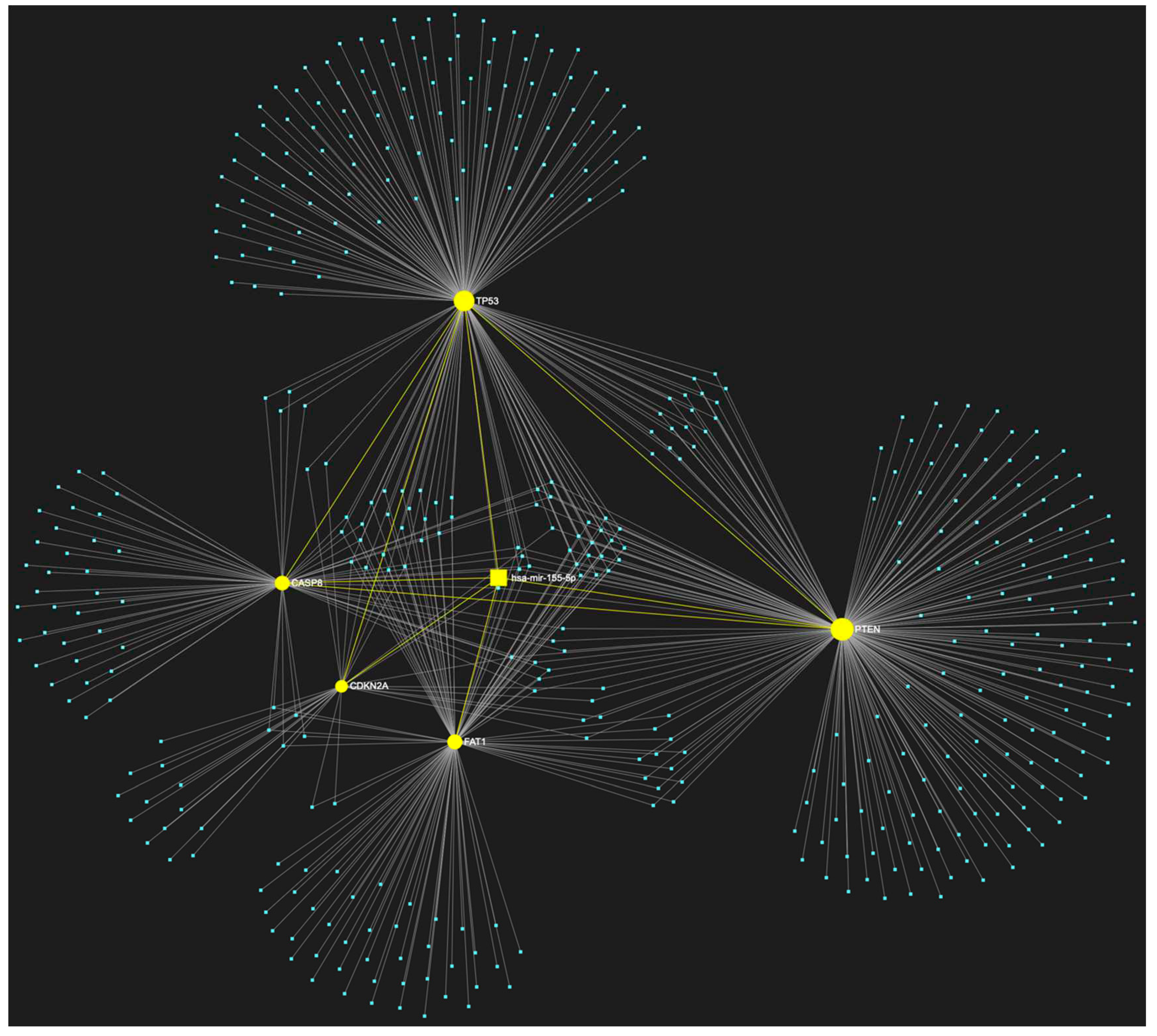
Figure 4.
The miRNA/target interaction network illustrates the anticipated targets of miR-16-5p within our customized panel of oncogenes which are highly associated with OSCC. MiR-16-5p has been predicted to target a total of 9 oncogenes out of an ensemble of fifteen. These oncogenes include PIK3CA, MYC, JUN, EGFR, FGF2, FGFR1, FGFR4, MKI67, and BCL2. It is worth noting that miR-16-5p has consistently been reported to be downregulated in oral OSCC. The genes targeted by miR-16-5p and their corresponding connecting nodes are depicted in yellow, while genes that are not targeted by this miRNA are visualized in pink.
Figure 4.
The miRNA/target interaction network illustrates the anticipated targets of miR-16-5p within our customized panel of oncogenes which are highly associated with OSCC. MiR-16-5p has been predicted to target a total of 9 oncogenes out of an ensemble of fifteen. These oncogenes include PIK3CA, MYC, JUN, EGFR, FGF2, FGFR1, FGFR4, MKI67, and BCL2. It is worth noting that miR-16-5p has consistently been reported to be downregulated in oral OSCC. The genes targeted by miR-16-5p and their corresponding connecting nodes are depicted in yellow, while genes that are not targeted by this miRNA are visualized in pink.
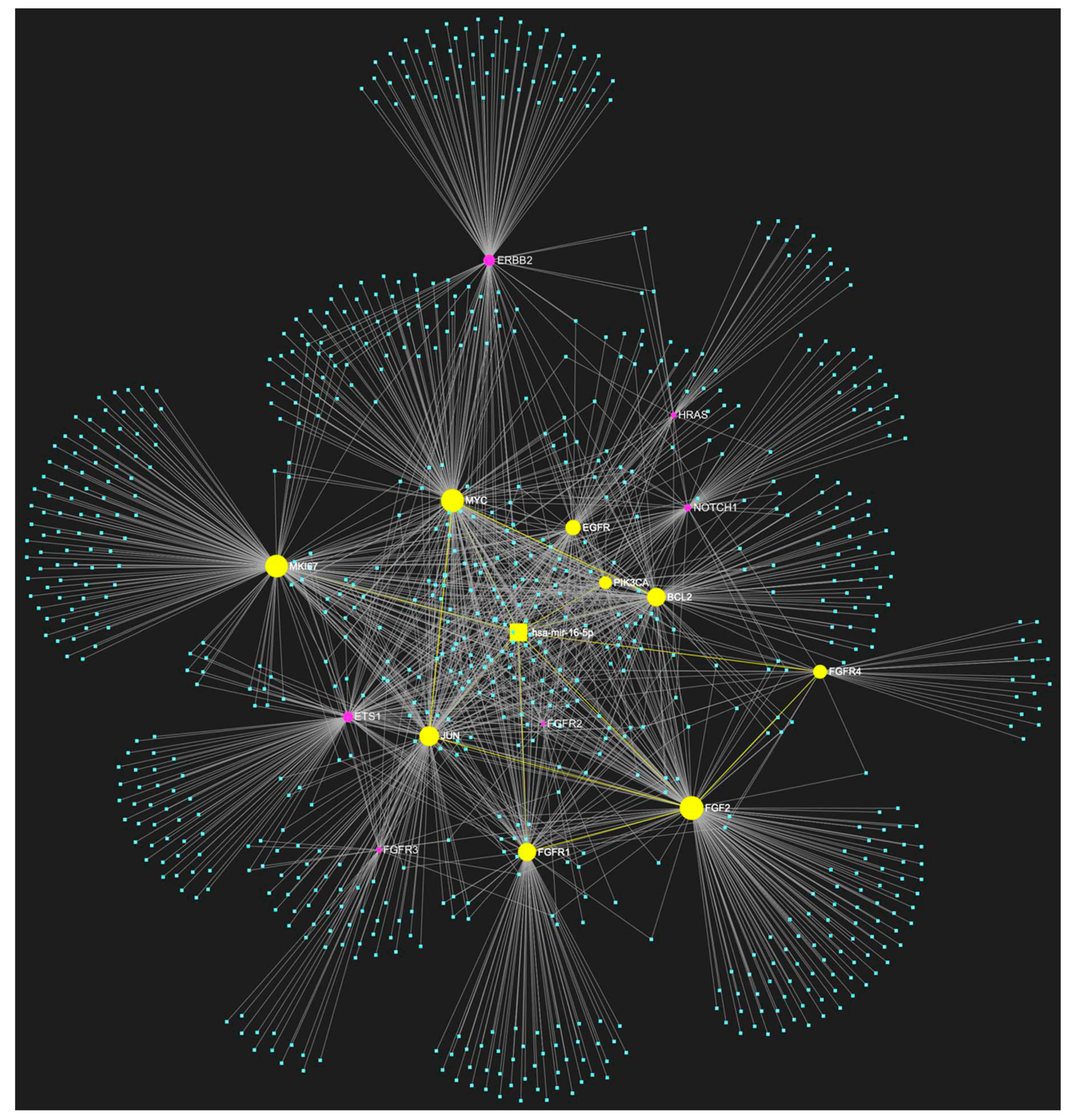
Figure 5.
The miRNA/target interaction network illustrates the 10 predicted targets of miR-1-3p derived from the focused panel consisting of fifteen key oncogenes associated with OSCC. In particular, it is predicted that miR-1-3p, which is significantly downregulated in OSCC, may target and potentially regulate the expression of PIK3CA, HRAS, MYC, JUN, EGFR, FGF2, FGFR2, FGFR4, MKI67 and ETS1. These genes are well-known for their significant involvement in the pathogenesis of OSCC and are visually represented in yellow, alongside their corresponding connecting nodes, while genes that are not targeted by this miRNA are visualized in pink.
Figure 5.
The miRNA/target interaction network illustrates the 10 predicted targets of miR-1-3p derived from the focused panel consisting of fifteen key oncogenes associated with OSCC. In particular, it is predicted that miR-1-3p, which is significantly downregulated in OSCC, may target and potentially regulate the expression of PIK3CA, HRAS, MYC, JUN, EGFR, FGF2, FGFR2, FGFR4, MKI67 and ETS1. These genes are well-known for their significant involvement in the pathogenesis of OSCC and are visually represented in yellow, alongside their corresponding connecting nodes, while genes that are not targeted by this miRNA are visualized in pink.
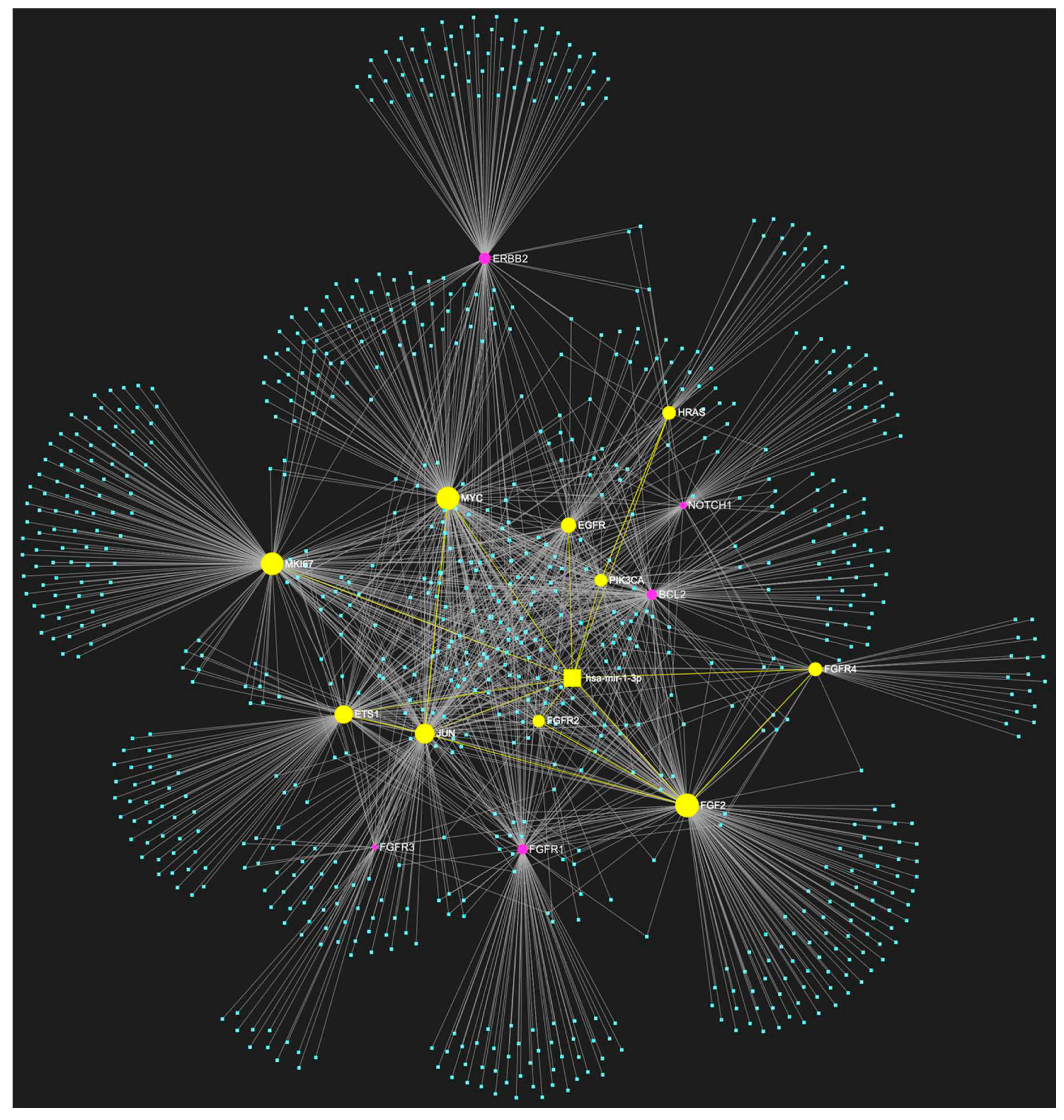
Figure 6.
The presented miRNA/target interaction network depicts the expected targets of miR-124-3p within the customized selected panel of oncogenes that exhibit a strong correlation with OSCC. miR-124-3p has been computationally predicted to exhibit targeting potential towards a total of 12 oncogenes from the set of 15. The oncogenes encompassed in this list comprise PIK3CA, NOTCH1, HRAS, MYC, JUN, EGFR, FGFR1, FGFR3, FGFR4, MKI67, and ETS1. It is noteworthy to mention that miR-124-5p has consistently exhibited downregulation in OSCC. The genes that are subject to targeting a possible regulation by miR-124-3p and their associated nodes are represented in yellow, whereas genes that are not targeted by this specific miRNA are visually represented in pink.
Figure 6.
The presented miRNA/target interaction network depicts the expected targets of miR-124-3p within the customized selected panel of oncogenes that exhibit a strong correlation with OSCC. miR-124-3p has been computationally predicted to exhibit targeting potential towards a total of 12 oncogenes from the set of 15. The oncogenes encompassed in this list comprise PIK3CA, NOTCH1, HRAS, MYC, JUN, EGFR, FGFR1, FGFR3, FGFR4, MKI67, and ETS1. It is noteworthy to mention that miR-124-5p has consistently exhibited downregulation in OSCC. The genes that are subject to targeting a possible regulation by miR-124-3p and their associated nodes are represented in yellow, whereas genes that are not targeted by this specific miRNA are visually represented in pink.
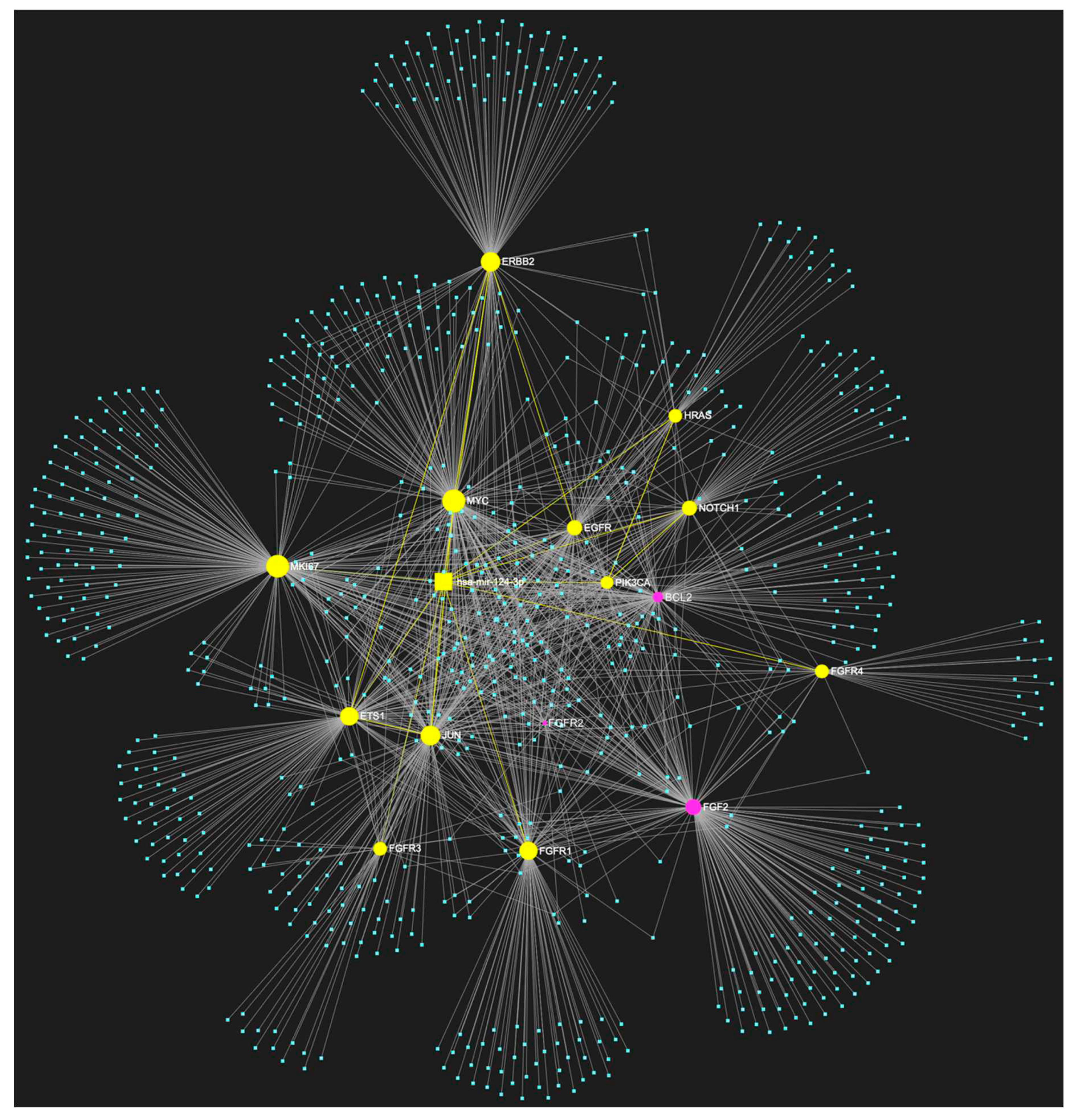
Figure 7.
MiR-34a-5p, which has primarily been reported as downregulated but has also been reported by some studies to be upregulated in OSCC, is predicted to target all 15 oncogenes (NOTCH1, HRAS, PIK3CA, EGFR, ERBB2, FGFR1, FGFR2, FGFR3, FGFR4, FGF2, ETS1, JUN, MKI67, MYC, and BCL2) comprising our custom OSCC-specific oncogene panel. The visual elements portrayed in yellow represent the genes that are specifically targeted by miR-34a-5p, alongside their corresponding connecting nodes.
Figure 7.
MiR-34a-5p, which has primarily been reported as downregulated but has also been reported by some studies to be upregulated in OSCC, is predicted to target all 15 oncogenes (NOTCH1, HRAS, PIK3CA, EGFR, ERBB2, FGFR1, FGFR2, FGFR3, FGFR4, FGF2, ETS1, JUN, MKI67, MYC, and BCL2) comprising our custom OSCC-specific oncogene panel. The visual elements portrayed in yellow represent the genes that are specifically targeted by miR-34a-5p, alongside their corresponding connecting nodes.

Figure 8.
MiR-34a-5p, which has primarily been reported as downregulated but has also been reported by some studies to be upregulated in oral squamous cell carcinoma (OSCC), is predicted to target all five tumor suppressor genes (TP53, CDKN2A, FAT1, CASP8, PTEN) included in our custom OSCC-specific tumor suppressor gene panel. The visual elements portrayed in yellow represent the genes that are specifically targeted by miR-34a-5p, alongside their corresponding connecting nodes.
Figure 8.
MiR-34a-5p, which has primarily been reported as downregulated but has also been reported by some studies to be upregulated in oral squamous cell carcinoma (OSCC), is predicted to target all five tumor suppressor genes (TP53, CDKN2A, FAT1, CASP8, PTEN) included in our custom OSCC-specific tumor suppressor gene panel. The visual elements portrayed in yellow represent the genes that are specifically targeted by miR-34a-5p, alongside their corresponding connecting nodes.
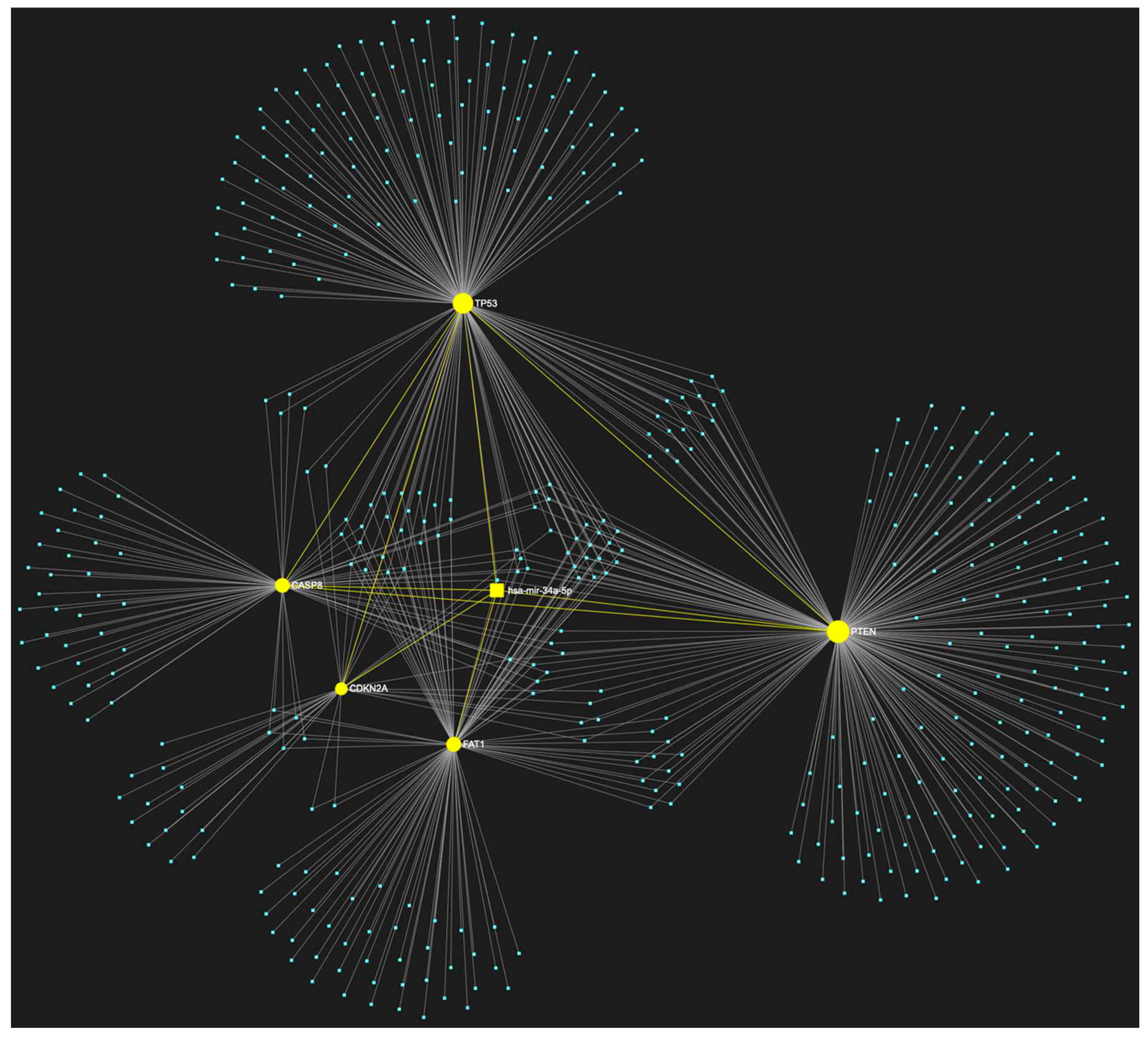

Table 1.
MicroRNA (miRNA) molecules that have been documented to exhibit increased expression levels in biological samples associated with oral squamous cell carcinoma (OSCC), such as tumor tissue, OSCC cell lines, saliva, whole blood, plasma, and serum, compared to non-OSCC biological materials.
Table 1.
MicroRNA (miRNA) molecules that have been documented to exhibit increased expression levels in biological samples associated with oral squamous cell carcinoma (OSCC), such as tumor tissue, OSCC cell lines, saliva, whole blood, plasma, and serum, compared to non-OSCC biological materials.
| ↑ miRNA | Sample Source | ↑ miRNA | Sample Source |
|---|---|---|---|
| let-7a-3p | Tissue [17] | miR-222 | Tissue, Cell lines [17,19,72] |
| let-7i | Tissue [17] | miR-223 | Tissue, Plasma, Serum [17,18,77] |
| miR-106b | Cell lines [17] | miR-24-3p | Tissue, Saliva, Plasma, Serum [14,17,18,75,98,107] |
| miR-10a | Tissue, Cell lines [77,106] | miR-25 | Serum [17] |
| miR-10b | Tissue, Cell lines, Plasma [14,77] | miR-26a | Tissue, Cell lines [19] |
| miR-117 | Tissue, Cell lines [19] | miR-26a | Tissue, Cell lines [77] |
| miR-118 | Tissue, Cell lines [19] | miR-27 | Tissue, Cell lines [77] |
| MiR-1246 | Tissue, Cell lines, Salivary exosomes [17,77,107] | miR-27a | Tissue, Cell lines [18,72,73] |
| miR-1250 | Saliva [18] | miR-27b | Tisuue, Cell lines, Saliva [107] |
| miR-1269a | Tissue, Cell lines [19] | miR-29b | Tissue, Cell lines [17] |
| miR-127 | Tissue [17] | miR-31-5p | Tissue, Cell lines, Saliva, Plasma [14,18,72,75,77,88,98,106,107] |
| miR-1275 | Tissue [17] | miR-3162 | Whole blood [18] |
| miR-128a | Cell lines [17] | miR-323-5p | Saliva [18] |
| miR-130b | Tissue, Cell lines [19] | miR-34a | Salivary exosomes [98] |
| MiR-134 | Tissue, Plasma [17,72,77] | miR-34b | Tissue, Cell lines [19] |
| miR-135 | Tissue, Cell lines [19] | miR-34c | Tissue, Cell lines [19] |
| miR-135b-5p | Tissue [17] | miR-3651 | Tissue, Whole blood [18,77] |
| miR-136 | Saliva [18] | miR-372 | Tissue, Cell lines [72,77] |
| miR-142 | Tissue [17,19] | miR-373 | Tissue, Cell lines [72,77] |
| miR-143 | Tissue, Cell lines [19] | miR-412-3p | Saliva [98] |
| miR-143 | Tissue, Cell lines [106] | miR-412-3p | Saliva [18] |
| miR-144 | Tissue [17] | miR-423 | Tissue, Cell lines [19] |
| miR-145 | Saliva [98] | miR-423-3p | Tissue, Plasma [18,19] |
| MiR-146a-5p | Tissue, Saliva, Plasma [17,72,73,75,107] | miR-424 | Tissue, Cell lines [77] |
| miR-146b | Tissue [17] | miR-4484 | Salivary exosomes [98] |
| miR-147 | Saliva [18] | miR-450a | Tissue, Cell lines [77] |
| miR-148a | Tissue, Saliva [18,19] | miR-451 | Tumor, Saliva, Serum [17] |
| miR-148b | Cell lines [17] | MiR-4513 | Cell lines [73,77] |
| miR-150-5p | Tissue, Plasma [18,19] | miR-455-5p | Tissue [17,77] |
| MiR-155-5p | Tissue, Cell lines [18,72,73,75] | miR-483 | Saliva [18] |
| MiR-15b | Tissue, Cell lines [17] | miR-483-5p | Serum [18] |
| miR-181 | Tissue, Plasma [14,18] | miR-483-5p | Plasma, Serum [17] |
| miR-181a | Plasma [18] | miR-494 | Tissue, Saliva, Whole blood [18,77] |
| miR-181b | Plasma [18] | miR-497 | Tissue [17] |
| miR-182-5p | Tissue [75] | miR-503 | Saliva [18] |
| MiR-183 | Cell lines [73] | miR-5100 | Tissue, Serum [18,77] |
| miR-184 | Saliva, Plasma [14,18,98] | miR-512-3p | Saliva [18] |
| miR-187 | Plasma [18] | miR-542 | Tissue, Cell lines [19] |
| miR-18a-5p | Tissue, Cell lines [77] | miR-543 | Tissue, Cell lines [77] |
| miR-191 | Whole blood [18] | miR-582-5p | Cell lines [17] |
| miR-196a-3p | Plasma [96] | MiR-626 | Tissue, Cell lines, Serum [18,73] |
| miR-196a-5p | Saliva, Plasma [18,72,75,88] | miR-632 | Saliva [18] |
| MiR-196b | Tissue, Cell lines, Saliva [72,88] | miR-646 | Saliva [18] |
| miR-196b | Plasma [18] | miR-650 | Tissue, Cell lines [77] |
| miR-200b-3p | Plasma [18] | miR-654 | Tissue, Cell lines [77] |
| miR-21-3p | Tissue [17,77] | miR-668 | Saliva [18] |
| miR-21-5p | Tissue, Cell lines, Saliva, Whole blood Plasma, Serum [17,18,19,73,75,77,88,96,98,107] | MiR-7975 | Salivary exosomes [107] |
| miR-210 | Whole blood [18] | miR-877 | Saliva [18] |
| MiR-211 | Tissue [14,72,75] | miR-877-5p | Saliva [17] |
| miR-214 | Tissue, Cell lines [17] | miR-92b | Serum [18] |
| MiR-218 | Tissue [72,77] | miR-93 | Saliva [98] |
| miR-220a | Saliva [18] | MiR-96-5p | Tissue [75] |
| miR-221 | Tissue, Cell lines [17,19] |
Table 2.
MicroRNA (miRNA) molecules that have been documented to exhibit significantly decreased expression levels in biological samples associated with oral squamous cell carcinoma (OSCC), such as tumor tissue, OSCC cell lines, saliva, whole blood, plasma, and serum, compared to non-OSCC biological materials.
Table 2.
MicroRNA (miRNA) molecules that have been documented to exhibit significantly decreased expression levels in biological samples associated with oral squamous cell carcinoma (OSCC), such as tumor tissue, OSCC cell lines, saliva, whole blood, plasma, and serum, compared to non-OSCC biological materials.
| ↓ MiRNA | Sample Source | ↓ MiRNA | Sample Source |
|---|---|---|---|
| let-7a-5p | Tissue, Cell lines, Saliva [17,72,88] | miR-23b-3p | Tissue [17,75,77] |
| miR-107 | Tissue, Cell lines, Saliva [17,98] | miR-26a | Tissue, Cell lines, Saliva [17,72,98] |
| let-7c | Tissue, Saliva [72,107] | miR-26b | Cell lines [17] |
| let-7c-5p | Tissue [17] | miR-27a-3p | Tissue, Cell lines [17] |
| let-7d | Tissue, Cell lines, Saliva, Whole blood, Serum [17,18,72,75] | miR-27b | Tissue, Saliva, Plasma [17,75,88,98] |
| let-7e | Tissue, Cell lines [72] | miR-299 | Tissue, Cell lines [77] |
| let-7f | Tissue, Cell lines [17,72] | miR-29a-3p | Tissue, Serum [17,18,73,75] |
| miR-1-3p | Tissue, Cell lines [17,73,75,77] | miR-29b-3p | Tissue, Cell lines [17,73] |
| miR-100 | Tissue, Saliva [17,107] | miR-29c | Tissue, Cell lines [17] |
| miR-101 | Tissue, Cell lines [73,77] | miR-30a-5p | Plasma [18] |
| miR-106a | Tissue, Cell lines [77] | miR-320 | Tissue, Cell lines [77] |
| miR-107 | Tissue, Cell lines [77] | miR-320a | Saliva [18] |
| miR-10a | Tissue, Cell lines [17] | miR-338-3p | Serum [18] |
| miR-124-3p | Tissue, Cell lines, Saliva [17,77,88] | miR-340 | Tissue [106] |
| miR-1250 | Saliva [17] | miR-34a-5p | Tissue, Saliva [77,96,98] |
| miR-125a-5p | Tissue, Saliva [14,18,88,107] | miR-375 | Tissue, Cell lines, Saliva [19,72,73,75,77,88,98,107] |
| miR-125b-2-3p | Tissue, Cell lines [17] | miR-376c-3p | Tissue, Cell lines [73] |
| miR-125b-5p | Tissue, Cell lines [17,75,77] | miR-377 | Tissue, Cell lines [77] |
| miR-125b-5p | Tissue [106] | miR-378 | Tissue, Cell lines [73] |
| miR-126 | Tissue, Cell lines [17,77] | miR-4282 | Tissue, Cell lines [73] |
| miR-1271 | Tissue, Cell lines [17] | miR-429 | Tissue, Cell lines [17,77] |
| miR-128-3p | Cell lines [17] | miR-433 | Tissue, Cell lines [17] |
| miR-1291 | Tissue [17] | mir-4485 | Tissue [17] |
| miR-133a-3p | Tissue, Cell lines [17,73,75,77] | miR-4488 | Tissue [17] |
| miR-133a-5p | Tissue, Cell lines [17] | miR-4492 | Tissue [17] |
| mir-136 | Saliva [17,88] | miR-4497 | Tissue [17] |
| miR-137 | Tissue, Cell lines [17,72] | miR-4508 | Tissue [17] |
| miR-138-3p | Tissue, Cell lines [17,77] | miR-451 | Tissue, Cell lines, Saliva, Serum [17] |
| miR-138-5p | Tissue, Cell lines [14,17,75,77] | miR-4516 | Tissue [17] |
| miR-139-5p | Tissue, Cell lines, Saliva [17,18,72,73,77,88] | miR-4532 | Tissue [17] |
| miR-141 | Tissue [17] | miR-486 | Tissue, Cell lines [19,73,77] |
| miR-142-3p | Saliva [107] | mir-487-3p | Tissue [73] |
| miR-143 | Tissue, Cell lines [17,72,77] | miR-491-5p | Tissue [75,77] |
| miR-145-5p | Tissue, Cell lines, Saliva [17,18,73,77,88] | miR-494-3p | Cell lines [17] |
| miR-146a-5p | Tissue, Cell lines, Saliva [77,88] | miR-494-5p | Tissue, Cell lines [17] |
| miR-147 | Saliva [17] | miR-495 | Tissue [75,77] |
| miR-148a | Tissue, Saliva, Plasma [17,75] | miR-499 | Tissue [19] |
| miR-149 | Tissue, Cell lines [17,73] | miR-499a | Tissue [17] |
| miR-150-3p | Tissue, Cell lines [17] | miR-503 | Saliva [17] |
| miR-153-3p | Tissue [75] | miR-504 | Tissue [19] |
| miR-16-5p | Tissue, Cell lines [73,77] | miR-506 | Tissue [17] |
| miR-17-5p | Tissue, Cell lines [73,75,77] | miR-519d | Tissue [75,96] |
| miR-181a-5p | Tissue, Cell lines, Plasma [75,77] | miR-542-3p | Tissue [17] |
| miR-184 | Tissue, Cell lines [72] | miR-545 | Tissue [75,77] |
| miR-186 | Tissue, Cell lines, Whole blood [18,73,77] | miR-585 | Cell lines [17] |
| miR-188 | Tissue, Cell lines [77] | miR-6087 | Tissue [17] |
| miR-195 | Tissue, Cell lines [73,77] | miR-617 | Cell lines [73] |
| miR-196-5p | Tissue [96] | miR-632 | Saliva [17] |
| miR-196a-5p | Tissue, Cell lines [19] | miR-646 | Saliva [17] |
| miR-198 | Cell lines [73] | miR-6510-3p | Tissue [17] |
| miR-199 | Tissue [19] | miR-655 | Tissue, Cell lines [77] |
| miR-199a-5p | Tissue, Cell lines [73,77] | miR-668 | Saliva [17] |
| miR-200a | Saliva, Salivary exosomes [14,18,88,98,107] | miR-675 | Tissue, Cell lines [17] |
| miR-200c | Tissue, Cell lines [77] | miR-7 | Saliva [98] |
| miR-203 | Cell lines [73,77] | miR-758 | Saliva, Serum [18] |
| miR-204-5p | Tissue, Cell lines [77] | miR-769-5p | Plasma [18] |
| miR-205-5p | Tissue, Saliva [75,77,88] | miR-7704 | Tissue [17] |
| miR-214 | Tissue [19] | miR-874 | Cell lines [17] |
| miR-216a | Tissue, Cell lines [17] | miR-877-5p | Saliva [17] |
| miR-218 | Tissue, Cell lines, Saliva [17,77,98,106] | miR-9 | Tissue, Cell lines, Serum [18,73] |
| miR-22 | Tissue, Cell lines [77] | miR-9 | Tissue, Cell lines [77] |
| miR-22-3p | Tissue, Cell lines [17,73] | miR-92a-3p | Saliva [88] |
| miR-220a | Saliva [17] | miR-92b | Tissue [19] |
| miR-221 | Tissue, Cell lines [77] | miR-93 | Saliva [107] |
| miR-223 | Serum [18] | miR-98 | Tissue, Cell lines [77] |
| miR-23a-3p | Tissue, Cell lines [77] | miR-99a-5p | Tissue, Cell lines, Saliva, Serum [18,72,77,107] |
Table 3.
Overview of the results obtained from the miRNA/target prediction analysis. Our analysis focused on specific panels of tumor suppressor genes and of oncogenes that have been strongly associated with the development and characteristics of oral oncogenesis. The genes that have been identified as potential targets of each miRNA, following the successful application of our bioinformatic filtering, are indicated in red. Conversely, the genes from each panel that are not targeted are indicated in black. The table also encompasses data pertaining to the expression patterns observed in OSCC for each miRNA molecule, as documented in the latest comprehensive review of the available research. Details are furtherly discussed in text.
Table 3.
Overview of the results obtained from the miRNA/target prediction analysis. Our analysis focused on specific panels of tumor suppressor genes and of oncogenes that have been strongly associated with the development and characteristics of oral oncogenesis. The genes that have been identified as potential targets of each miRNA, following the successful application of our bioinformatic filtering, are indicated in red. Conversely, the genes from each panel that are not targeted are indicated in black. The table also encompasses data pertaining to the expression patterns observed in OSCC for each miRNA molecule, as documented in the latest comprehensive review of the available research. Details are furtherly discussed in text.
| miRNA | Reported Expression in OSCC | Predicted Target OSCC-associated tumor suppressor genes (5) | Target score |
|---|---|---|---|
| hsa-miR-155-5p | ↑ | TP53, CDKN2A, FAT1, CASP8, PTEN | 5/5 |
| hsa-miR-34a-5p | ↑ (rarely) | TP53, CDKN2A, FAT1, CASP8, PTEN | 5/5 |
| miRNA | Reported Expression in OSCC | Predicted Target OSCC-associated oncogenes (15) | Target score |
| hsa-miR-34a-5p | ↓ (mostly) | NOTCH1, HRAS, PIK3CA, EGFR, ERBB2, FGFR1, FGFR2, FGFR3, FGFR4, FGF2, ETS1, JUN, MKI67, MYC, BCL2 | 15/15 |
| hsa-miR-124-3p | ↓ | NOTCH1, HRAS, PIK3CA, EGFR, ERBB2, FGFR1, FGFR2, FGFR3, FGFR4, FGF2, ETS1, JUN, MKI67, MYC, BCL2 | 12/15 |
| hsa-miR-1-3p | ↓ | NOTCH1, HRAS, PIK3CA, EGFR, ERBB2, FGFR1, FGFR2, FGFR3, FGFR4, FGF2, ETS1, JUN, MKI67, MYC, BCL2 | 10/15 |
| hsa-miR-16-5p | ↓ | NOTCH1, HRAS, PIK3CA, EGFR, ERBB2, FGFR1, FGFR2, FGFR3, FGFR4, FGF2, ETS1, JUN, MKI67, MYC, BCL2 | 9/15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



