Submitted:
11 July 2023
Posted:
12 July 2023
You are already at the latest version
Abstract
Chronic Traumatic Encephalopathy (CTE) is a neurodegenerative disease consistently associated with repetitive traumatic brain injuries (TBIs), which makes multiple professions, such as contact sports athletes, especially susceptible to its onset. There are currently no approved biomarkers to diagnose CTE, thus it can only be confirmed through a post-mortem brain autopsy. Several imaging and cerebrospinal fluid biomarkers have shown promise in the diagnosis. However, blood-based biomarkers can be more easily obtained and quantified, increasing their clinical feasibility and potential for prophylactic use. This article aimed to comprehensively review the studies into potential blood-based biomarkers of CTE, discussing common themes and limitations as well as suggesting future research directions. While the interest in blood-based biomarkers of CTE has recently increased, the research is still in its early stages. The main issue for many proposed biomarkers is their lack of selectivity for CTE. However, several molecules, such as tau phosphorylated on different epitopes, were able to discern CTE from different neurodegenerative diseases. Further, results from studies of exosomal biomarkers suggest that exosomes are a promising source of biomarkers reflective of the internal environment of the brain. Nonetheless, more longitudinal studies combining imaging, neurobehavioral and biochemical approaches are warranted to establish robust biomarkers of CTE.
Keywords:
biomarkers
; CTE
; neurodegeneration
; TBI
; miRNA
; exosomes
; concussion
; prodromal
1. Introduction
Neurodegenerative diseases are debilitating and increasingly more common conditions, with dementia, their major consequence, projected to affect 139 million people worldwide in 2050 [1]. However, there is currently no cure or disease-modifying treatment for dementia. As condition management focuses on decreasing the patients’ suffering and decelerating the development of the condition [2], an early medical intervention might increase healthy life years by delaying the onset and worsening of debilitating symptoms [3]. Unfortunately, the lack of clinically approved biomarkers of many neurodegenerative diseases underlying dementia translates into the inability to diagnose and intervene in the diseases’ prodromal, i.e., before the onset of symptoms, or early stage. Chronic Traumatic Encephalopathy (CTE), first described in former boxers as ‘punch drunk syndrome’ [4], is one such disease. CTE has now been confirmed by post-mortem brain autopsies in many former contacts sports players, such as hockey [5] and rugby [5,6,7,8,9,10] as well as deployed military personnel [8,9,11] with history, frequency, and intensity of traumatic brain injury (TBI) being the only risk factors consistently linked with the occurrence of CTE [12]. Notably, McKee et al. [13] analysed over 600 published cases of neuropathologically-confirmed CTE, concluding that 97% of those were associated with repetitive head impacts (RHI). However, the inability to diagnose CTE ante-mortem impedes prophylaxis, early diagnosis, and potential symptomatic treatment in the groups with a high TBI risk. This is further aggravated by non-specific initial symptoms of the disease that can be behavioural, cognitive, mood and motor [14,15]. Several studies reported increased incidence of poor mental health, sleep problems, cognitive impairment, and dementia in professions with high exposure to repetitive TBIs (rTBIs) [16,17,18,19], potentially indicating different stages of CTE, which emphasises the need for biomarkers of the disease. While imaging [20] and cerebrospinal fluid (CSF) [21,22] biomarkers of CTE have been investigated with many yielding promising results, they are expensive and invasive techniques, respectively, thus limiting their use in prophylaxis and diagnosis. On the contrary, blood-based biomarkers can be easily and non-invasively collected and have already been investigated in conditions such as Alzheimer’s Diseases (AD) [23]. In the context of CTE, the focus of research has only recently shifted from the short-term diagnosis of TBI [24] to its long-term effects, such as CTE. While there is a growing body of studies looking at the issue, their results are often contradictory, which complicates the picture of potential blood-based biomarkers of CTE.
So far, several reviews of TBI/CTE biomarkers have been published [25,26,27,28,29,30], but no article has focused on blood-based biomarkers of CTE, specifically. This review article aims to fill in this gap by a comprehensive overview of the potential blood-based biomarkers of CTE, which yielded promising results, outlining their molecular mechanisms in CTE, and emphasising the common themes across studies to date. Further, directions for future research will be suggested.
2. Pathology of CTE and Rationale for Blood-Based Biomarkers
CTE is a progressive tauopathy characterised by the deposition of neurofibrillary tangles (NFTs) consisting mainly of hyperphosphorylated microtubule-associated protein tau (p-tau) in the perivascular depths of cortical sulci, which increases with the progression of a disease, and is linked to trauma incurred during a TBI [31,32,33]. The aggregation of tau in NFTs induces several neurotoxic mechanisms, including microtubule destabilisation, synapse loss and potential aberrations of intracellular signaling, causing neuronal death [34]. This leads to macro-scale changes, such as brain atrophy and a consequent decrease in brain volume, in the advanced stages of the disease [35,36]. Substantial force impact on the head in a TBI causes a diffuse axonal injury (DAI), which can result in the breakage of axons and a subsequent release of axonal proteins, such as tau, into the interstitial fluid and the CSF [37,38,39,40]. On the other hand, TBI also increases the permeability of the blood-brain barrier (BBB) [41] leading to a possible efflux of axonal proteins into the systemic circulation (Figure 1). This two-way pathological mechanism allows for the detection and quantification of biomarkers from blood samples [42]. An ideal blood-based biomarker should be diagnostically accurate, i.e., be able to correctly discern between patients suffering from CTE and patients who are not; selective towards CTE, i.e., be able to discern CTE from other tauopathies, for example, AD; and feasible, i.e., be easily detectable and quantifiable from blood [43,44].
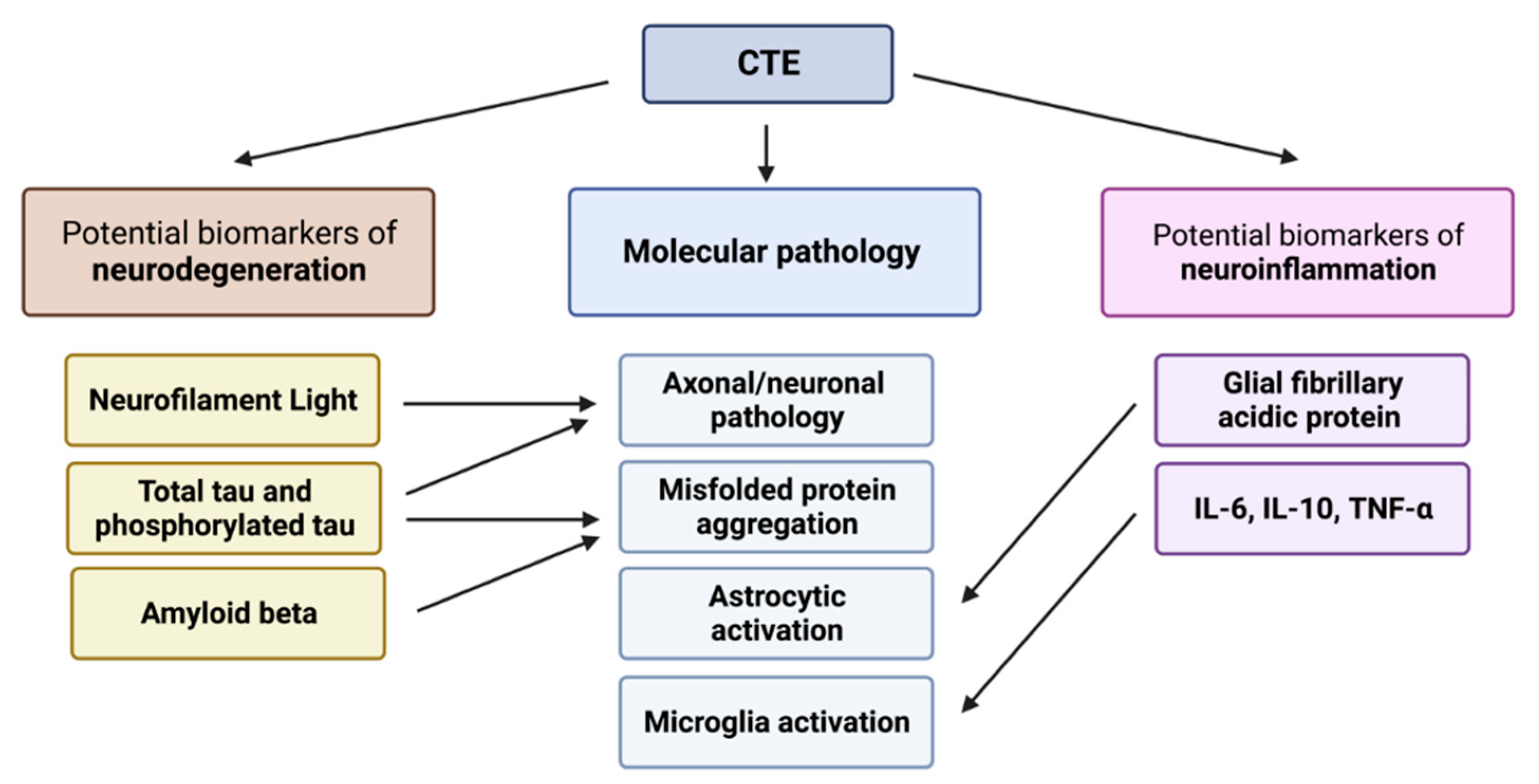
Based on the molecular pathology of CTE, two main groups of potential biomarkers can be distinguished. Potential biomarkers of neurodegeneration indicate a long-term neuronal injury and include, for instance, total (t-tau) or p-tau. Potential biomarkers of neuroinflammation, in turn, can include glial fibrillary acidic protein (GFAP) and inflammatory cytokines, which indicate the immune activation in the central nervous system (CNS) through processes such as microgliosis or astrogliosis [27,45,46,47,48]. Further, we included a third group of biomarkers—micro RNAs (miRNA). Regardless of their role in gene regulation, all miRNAs were discussed in a separate section due to their unique nature compared to other reviewed biomarkers. These groups of biomarkers will be discussed in the context of (i) the molecular basis of their role as a biomarker, (ii) studies to date, (iii) the diagnostic accuracy of the biomarker, and (iv) the limitations of the biomarker.
3. Biomarkers of Neurodegeneration in CTE
3.1. Total Tau and Phosphorylated Tau
Tau plays the most prominent role in the pathology of CTE through the formation of NFTs and consequent neuronal dysfunction and death [34]. Numerous studies showed a significant elevation of extracellular p-tau deposition in the brains of people with autopsy-confirmed CTE, compared to healthy controls (e.g., Johnson et al. [49]). Most studies on the role of tau in the diagnosis of long-term effects of TBI focused on t-tau and p-tau, yielding promising results for tau as an imaging biomarker [50,51] but mixed as a biomarker from CSF [21,22,52,53]. However, both were shown to be significantly elevated in a mouse model of rTBIs [54]. In theory, tau elevation would indicate the presence of DAI as well as its extent, which could inform diagnosis and prognosis.
Both t-tau and p-tau concentrations analysed from plasma have thus far yielded variable results, with many studies failing to discern between people exposed to TBIs and controls [52,55,56,57,58,59]. Nevertheless, Alosco et al. [55] reported a relationship between tau levels and RHIs as well as plasma t-tau levels above 3.56 pg/mL only in former rugby players despite no significance between the groups. However, others reported no relationship between t-tau and RHI [58]. Only Olivera et al. [60] observed increased plasma t-tau levels in the military deployed within the last 18 months who self-diagnosed themselves with TBIs, with a greater number of TBIs associated with a more substantial increase in plasma t-tau. As for p-tau, Vasilevskaya et al. [59] showed that tau phosphorylated on threonine 181 (p-tau181) was significantly elevated in retired contact sports athletes. Further, an abnormally high concentration of p-tau181 correlated with decreased volume of corpus callosum (CC) and entorhinal cortex as well as decreased fornix integrity, all of which are often observed following concussion, as indicated by imaging studies. However, Gorgoraptis et al. [52] observed no relationship between flortaucipir binding patterns in positron emission tomography (PET) scans, indicating the presence of NFTs in the brain, and plasma t-tau, which suggests that plasma t-tau is not linked to structural brain pathology. These varied results could indicate that substantial axonal damage is required for plasma tau to be significantly elevated [61]. Further, several other limitations of tau could contribute to those results, for example, a short half-life of tau in the blood [62] or the potential influence of a tau isoform from the peripheral nervous system, which current assays do not distinguish from the CNS isoform [63,64,65]. Interestingly, Gonzalez-Ortiz et al. [66] generated an antibody specifically binding the brain-derived isoform of tau, which showed high diagnostic performance in AD and was able to discriminate AD from other neurodegenerative disorders, such as Frontotemporal Dementia. Thus far, no studies used this antibody in the context of rTBIs and potential CTE.
Recently, the focus of research has extended to exosomes, which can be easily extracted from blood and overcome the issue of low blood tau concentration in the peripheral circulation and thus the need for ultrasensitive assays, such as Single Molecule Arrays (SiMoA) [67]. Exosomes are extracellular vesicles, which have been linked to physiological processes such as waste excretion and cell-to-cell communication [68]. Importantly, the contents of exosomes derived from the cells of the brain are thus representing the CNS’s cellular environment, potentially serving as biomarkers that can be non-invasively quantified and are more reflective of the CTE’s underlying molecular pathology than biomarkers from the CSF. Multiple studies reported a significant difference in exosomal t-tau and p-tau [69,70,71,72,73] in people who experienced a TBI or rTBIs compared to healthy controls, with one study describing the difference in p-tau but not t-tau [74]. Moreover, several studies associated both t-tau and p-tau concentrations with post-concussive [71], neurobehavioral [70] and psychological [69] symptoms, which could indicate that exosomal tau is a symptomatic biomarker. The number of TBIs appears to be associated with both t-tau and p-tau concentrations [71], meaning that it could be reflective of the underlying molecular pathology. However, no imaging or post-mortem studies have linked the concentration of exosomal tau to structural changes in the brain so far.
While exosomal t-tau and p-tau appear promising as blood-based biomarkers, they so far have not shown substantial specificity to CTE; a significant increase in both plasma and exosomal t-tau and p-tau can be observed, for instance, in AD [75,76,77]. Studies on tau in CTE thus far have focused on its diagnostic utility in discerning between people with potential CTE and healthy controls rather than between different neurodegenerative diseases. However, Turk et al. [22] reported that tau phosphorylated on threonine 231(p-tau231) from CSF is significantly different between CTE and AD patients, confirmed by brain autopsies. Moreover, p-tau231 was successful in distinguishing AD and CTE diagnoses. There are no studies on the long-term blood levels of p-tau231, but the protein was significantly elevated in the plasma of patients from TBI rehabilitation units with a potential chronic TBI [78]. Similarly, a post-mortem study of 473 cadavers with neuropathologically-diagnosed AD or CTE by Stathas et al. [79] showed that tau in the dorsolateral frontal cortex is differentially phosphorylated in CTE and AD; serine 202 residue (p-tau202) is significantly more phosphorylated in CTE while serine 396 (p-tau396) residue in AD, with the ratio of p-tau202 to p-tau396 being significantly higher in CTE compared to AD. Further, the number of years spent playing contact sports was a predictor of p-tau202 levels. Goetz et al. [80] reported elevated p-tau396 only in military veterans with a history of TBI and cognitive impairment (CI), and not those without CI, compared to healthy controls. Similarly, they reported increased exosomal p-tau181 in veterans with CI, regardless of their TBI status, suggesting that these epitopes cannot identify TBI-related cognitive deficits. As such, Asken et al. [76] suggest measuring plasma p-tau181 and p-tau217 to support identifying AD pathology within Traumatic Encephalopathy Syndrome, with lower levels of these biomarkers suggesting CTE over AD. In turn, Peltz et al. [74] showed that p-tau levels were different between veterans experiencing CI with and without a history of TBIs, yet the exact epitope measured was not mentioned in the publication. These studies suggest only a couple of differentially expressed p-tau epitopes, among more than 30 tau phosphorylation sites [81]. Investigation into the feasibility of p-tau202, p-tau231 and other under-researched epitopes of p-tau as a blood-based biomarker of CTE should be continued to assess their diagnostic performance and specificity to CTE.
3.2. Amyloid Beta
While Amyloid beta (Aβ) plaques are primarily associated with AD, TBI has been shown to increase the concentration of Amyloid Precursor Protein and Aβ peptides in the brain tissue and CSF. These proteins can foster the formation of the plaques [9,82,83], which are toxic to brain cells and trigger neurodegenerative processes [84]. The presence of Aβ plaques in cadavers with neuropathologically-diagnosed CTE has been reported, but it is not as universal as the deposition of NFTs in CTE and has been linked to the possession of the Apoϵ4 allele as well as significantly older age at death, potentially indicating Aβ plaques’ association with old age in CTE [8,9].
Thus far, the results for blood-based Aβ peptide have been mixed. From plasma, Lebjman et al. [85] reported a significant increase in Aβ40 and a trend for an increased Aβ42 in military personnel who experienced TBI deployed minimum 16 months before the investigation, while other studies reported no significant changes in different groups of athletes who experienced TBIs [56,58]. Exosomal Aβ peptides, in turn, appear more promising with a significant increase of Aβ42 in groups that experienced TBIs [70,72] with one study showing no difference [74]. While more research is needed to confirm the role of exosomal Aβ as a biomarker, its specificity to CTE is greatly limited. Goetz et al. [80] showed that Aβ42 was elevated in war veterans with CI regardless of whether they experienced TBI in the past, yet the significance was greater for veterans with both CI and TBI. Unexpectedly, however, Turk et al. [22] showed that CSF Aβ42 was lower in people with confirmed CTE than in healthy controls. Moreover, the difference in CSF Aβ42 was able to distinguish between patients with CTE and AD. These results suggest that CSF Aβ42 levels could show selectivity towards CTE as well as contradict the studies on exosomal Aβ42. More research is required to elucidate this relationship.
3.3. Neurofilament Light
Neurofilaments are intermediate filaments expressed exclusively in neurons. While their exact function remains to be elucidated, they are thought to play a critical role in axonal stability. Therefore, the efflux of neurofilaments into the CSF and potentially systemic circulation is indicative of neuroaxonal injury and has been suggested as a biomarker of neurological disorders, such as Parkinson’s Disease (PD) or AD [86]. In the context of TBI, the research has focused on the diagnosis of TBI through plasma NfL, reporting a significant elevation of plasma NfL following a TBI that predicted clinical outcomes [86,87,88,89,90]. However, knowledge about the long-term relationship between NfL and CTE is scarce. In a rat model, a single blast overpressure exposure was not shown to significantly increase plasma NfL 10 months after a blast simulation, but there was a trend for increased NfL in exposed rats compared to controls [91]. Two studies showed no difference in plasma NfL between athletes who experienced rTBIs and those who did not [56,59], with another study reporting no increase in exosomal NfL one-year post-TBI [92]. On the contrary, Peltz et al. [74] showed that exosomal NfL was significantly elevated in veterans diagnosed with CI, both in patients with and without a history of TBIs compared to healthy controls, while there was no difference in exosomal NfL for veterans with a history of TBI but no CI in relation to controls. Importantly, exosomal NfL was significantly elevated in veterans with CI and a history of TBIs compared to veterans without CI but with a history of TBIs, which suggests that NfL could be a symptomatic biomarker. Further, Dickstein et al. [91] observed that while there was no difference in plasma NfL concentration when veterans were compared to a control group, the highest levels of NfL were in veterans with excess [18F]AV1451 PET ligand retention, which reflected the anatomical distribution of tauopathy in CTE observed in post-mortem studies. Also, Shahim et al. [57] reported that serum NfL remained elevated for up to five years after a single TBI, with the protein correlating with brain structural and neuronal damage measured by diffusion tensor imaging and magnetic resonance imaging (MRI). Similarly, Vasilevskaya et al. [59], despite no significant difference in plasma concentration, showed an inverse relationship between plasma NfL levels and hippocampal and CC volume as well as the white matter integrity of fornix. These results indicate that blood-based NfL could be representative of structural brain pathology caused by TBI.
The major limitation of NfL is its lack of specificity to CTE. Asken et al. [93], analysing a group of nine cadavers, showed that elevated NfL could be observed in patients with different neuropathologically confirmed neurological disorders, such as Frontotemporal Lobar Degeneration, CTE and AD. Nonetheless, further research into chronic effects of TBIs and their relationship to NfL is warranted to establish the clinical relevance and selectivity of NfL in the context of CTE.
3.4. Other Biomarkers of Neurodegeneration
There have been individual studies investigating several other potential biomarkers of neurodegeneration. Ubiquitin C-Terminal Hydrolase L1 (UCH-L1) is an abundant protein in the brain and is essential to the proper maintenance of axonal integrity. Its dysfunction has been implicated in neurodegeneration, where it can, for example, misfold and constitute NFTs in AD [94]. As such it was found to be significantly elevated in CSF of AD patients [95,96]. In potential CTE, CSF UCH-L1 was associated with grey matter abnormalities in long-term TBI survivors, but there was no difference between this group and controls [52]. However, no UCH-L1 elevation as well as no correlation with brain structural changes was reported in patients with TBIs compared to controls, both from plasma [57] and exosomes [72] thus far. Similarly, alpha-synuclein, which aggregates into Lewy bodies in disorders, such as PD, has been shown to cause Lewy Body Disease concomitant to CTE in the brains of deceased contact sports athletes [97,98]. However, only one study looked at alpha-synuclein so far, showing no difference in exosomal alpha-synuclein concentration between veterans with and without a history of TBIs [74]. Also, Goetz et al. [72,80] noted a significant increase in the exosomal cellular prion protein (PrPc), synaptogyrin-3 and aquaporin-4. In addition, they show that the levels of PrPc and synaptogyrin-3 proteins were only increased in CI veterans, both with and without a history of TBI, yet not in a group with a history of TBI but no CI. However, no further studies on these proteins were conducted.
4. Biomarkers of Neuroinflammation in CTE
While the microglia activation and peripheral immune cells recruitment following a TBI has been shown, evidence is now emerging that chronic neuroinflammation might have an intrinsic role in the pathogenesis and progression of CTE through the induction of secondary neuronal injury [99,100,101,102,103]. A post-mortem study by Johnson et al. [45] showed that reactive microglia could be detected up to 18 years following a single TBI, which also coincided with white matter degeneration. Similarly, an in vivo MRI study reported increased neuroinflammation in several brain regions with hippocampal atrophy in retired rugby players [104]. In a mice model, Loane et al. [105] observed elevated microglial activation in the cortex, CC, and thalamus for up to 1 years following a moderate blast injury associated with neurodegeneration and increased biomarkers of neuroinflammation. These reports suggest that biomarkers of neuroinflammation could be indicative of CTE as well as its progression.
4.1. Glial Fibrillary Acidic Protein
GFAP is an intermediate filament protein and a major cytoskeletal component of astrocytes, which maintain synaptic transmission and axonal metabolism [106]. Following TBI, astrocytes mediate processes such as BBB permeability and inflammatory response [107]. Astrocyte immune activation is accompanied by an increase in the expression of GFAP [108]. On the other hand, an astrocytic injury could cause the efflux of GFAP [109]. Therefore, GFAP could represent both chronic neuroinflammation and neurodegeneration in CTE. Its blood elevation has been shown to relate to structural abnormalities in imaging studies after mild TBI [110,111,112]. Shahim et al. [57] reported that serum GFAP was significantly increased in chronic TBI patients for up to 5 years after a single TBI compared to controls but showed little association with structural brain change. Other studies showed no difference in plasma levels of GFAP between professional athelets with a history of RHI and post-concussive syndrome [58] retired athletes with a history of TBIs [56] and their respective controls. However, exosomal GFAP yielded more promising results with Flynn et al. [92] reporting a significant increase in a group of patients one-year post-TBI and Peltz et al. [74] showing that veterans with a history of TBIs and CI had elevated exosomal GFAP while veterans with a history of TBIs but without CI did not. This suggests that GFAP can be representative of functional changes and symptoms. Nonetheless, only one imaging and no post-mortem studies analysed GFAP levels in relation to structural brain abnormalities. Yet, a post-mortem study of nine patients with different neuropathological diagnoses showed that especially high GFAP was present in brains with AD neuropathologic changes, potentially limiting the diagnosis of CTE by GFAP alone [93].
4.2. Inflammatory Cytokines
The increased activation of microglia, which has been shown to occur following TBIs, upregulates the production of several pro-inflammatory cytokines. These lead to increased permeability of the BBB, elevated secretion of chemokines that cause the migration of peripheral leukocytes into the brain as well as production of reactive oxygen species, which altogether foster neuroinflammation and can trigger secondary cell death. Inflammatory cytokines investigated in the context of long-term consequences of TBI involve IL-6, IL-10, and TNF-α, which can all be secreted by microglia, indicating microgliosis [99]. As these can be expressed in all the tissues, the concentration of the cytokines was quantified from neuron-enriched exosomes. Peltz et al. [74] analysed all three molecules and showed that IL-6 was significantly elevated both in veterans with CI but no history of TBIs as well as in those with a history of TBIs compared to healthy controls. Moreover, in the concussed veterans IL-6 and TNF-α levels were significantly higher in those experiencing CI. In turn, IL-10 levels were not different between the groups. Goetzl et al. [72,80] also showed significantly increased IL-6 in high-impact sports students with at least two mild TBIs as well as military veterans with a history of TBIs and symptoms of CI. Surprisingly, Gill et al. [70] reported no difference in either IL-6 or TNF-α between military personnel who experienced a TBI within the past 3 years and controls, while noting that IL-10 was significantly elevated in the former group. However, no study so far analysed the relationship between the levels of these cytokines and structural changes in imaging and post-mortem studies.
5. Micro RNA Biomarkers in CTE
Micro RNAs (miRNAs) are small non-coding RNAs, which regulate a variety of processes at the post-transcriptional level. The expression of miRNAs can change in response to different physiological and pathological states [113]. Specifically, several studies identified panels of miRNA biomarkers from saliva [114] and blood [68,115,116,117] that showed different levels of specific miRNAs between patients following a TBI and controls. As such, they showed great potential in diagnosing TBI. MiRNAs’ great advantage over conventional protein panels is their stability; Gilad et al. [113] showed that their levels did not change after four hours at room temperature, while two freeze-thaw cycles affected their levels to a small extent. Further, the target miRNAs can be easily quantified using conventional Real-Time Quantitative Reverse Transcription PCR (qRT-PCR), which overcomes the requirement for ultrasensitive assays, like SiMoA [67], or exosome extraction [68] to reliably quantify proteins, such as tau.
However, only a handful of studies looked at the expression of miRNAs in potential CTE patients thus far. Alvia et al. [118] compared the expression of different miRNAs previously indicated in the prefrontal cortex of brains donated by people who suffered from either CTE, Amyotrophic Lateral Sclerosis (ALS), or both. While much of the expression of miRNAs overlapped between CTE and ALS, they identified several miRNAs specific to CTE, which were involved in cell growth, apoptotic and inflammatory pathways. As per biological fluids, Ghai et al. [119] used Next Generation Sequencing (NGS) to compare miRNA profiles of plasma and extracellular vesicles (EV) between veterans with a history of chronic TBI and controls. They detected significant differences in levels of multiple previously described, as well as novel, miRNAs, which they confirmed using qRT-PCR. They also observed that most miRNAs were circulating freely in plasma, which supports the use of plasma without the need for EVs isolation. Ge et al. [120] compared serum and exosome biomarkers between 12 patients with a history of rTBIs and thus different likelihood of CTE and respective controls, distinguishing serum and exosomal miR-1183 and exosomal miR-297 as potential diagnostic miRNA biomarkers of CTE. Neither of these studies related miRNA expression to neurobehavioral or imaging evidence. Further, due to few studies, miRNAs especially promising for CTE diagnosis cannot be distinguished yet. Considering the potential advantages of miRNAs over conventional protein biomarkers, further research is warranted.
6. Discussion and Future Directions
Although the number of studies on the potential biomarkers of CTE has been increasing in recent years, the research is still in its early stages, with common themes, such as little selectivity towards CTE diagnosis, as well as conflicting results, now being reported. The studies so far differ in cohorts employed and the underlying cause of concussions. Veterans primarily suffer from blast-related brain injuries while contact sports athletes from sports-related brain injuries, which have been shown to have a distinct pathological mechanism. While both the TBI types cause secondary nerve injury [121], the distinct primary mechanism could lead to different concentrations of biomarkers. Further, studies greatly vary in the duration from the last TBI, from some studies having participants one-year post-TBI [58], to others on average 37 years post-TBI [74]. Similarly, the average number of TBIs is variable, with some researchers looking at the long-term effects of up to 3 TBIs [92] and others having participants with a history of 10 TBIs on average [56]. Also, some studies were based on self-reported accounts of TBI—or occupancies and sport positions with high susceptibility for TBI—which were not supported by medical documentation (e.g., [59,69,74,85]). However, in contrast to a recent statement by the Concussion in Sports Group [122], there is evidence to demonstrate the effect of head impacts on the biomarker levels described in this review, indicative of a causal link between TBI and CTE and long-term neurological effects [13,28,59,69,70,71,72,73,74,123,124]. Specifically, Nowinski et al. [124] used Bradford-Hill criteria to analyse the causality between RHI and CTE. Basing on several factors, including the consistent relationship between RHI and CTE in analyses from multiple brain banks, while CTE is rarely confirmed without RHI, and the absence of alternative hypotheses with plausible evidence, a causative link between RHI and CTE was concluded. Further, there is an overlap between patterns of p-tau histochemical staining of post-mortem brain slices of CTE patients and topographic tau accumulation in PET scans of people with suspected CTE [28]. Also, this pathological hallmark molecule of CTE is consistently increased in blood [59] and blood exosomes [69,70,71,72,73,74] of individuals with history of TBIs compared to controls. In fact, a recently published analysis, which concluded that 97% of 600 confirmed cases of CTE were associated with repetitive head impacts only strengthens this argument [13].
Moreover, some experimental protocols differed between the described studies, especially concerning the methods of extraction and purification of exosomes. Several methods of extraction were used, ranging from size exclusion chromatography and ultracentrifugation to using different extraction kits, which all have been shown to result in variable yield and purity [125]. Further, different collection procedures and handling of samples, such as time between blood draw and centrifugation, its speed and the size of a needle, all affect exosome yield and purity [68]. Moreover, not all the studies enriched their yield for neuron-derived exosomes (e.g., Kenney et al. [71]; Muraoka et al. [73]). Research into the differences in biomarker concentrations from neuron-enriched and crude systemic exosomes is warranted to establish the most optimal way of exosome isolation for the study of CNS biomarkers. Similarly, while most studies analysed plasma biomarkers, some measured their concentration from serum, which contains lower levels of, for instance, tau than plasma [57]. Notably, most research has been carried out in predominantly male cohorts, which prevents the generalisation of the results to the whole population as some studies suggested sex differences in neurobehavioral outcomes and biomarker levels following TBI [126].
Considering the evidence, several protein biomarkers show promise for the diagnosis of CTE (Figure 2). Also, despite limited evidence so far, miRNAs appear promising and should be investigated further. Yet the general problem with potential CTE biomarkers is their role in multiple diseases and thus lack of specificity to CTE. So far, p-tau molecules phosphorylated on epitopes seemingly specific to CTE, such as p-tau202, and potentially certain miRNAs, appear to show the greatest promise in diagnosing CTE, specifically. Further, biomarkers specific to AD or other neurodegenerative diseases could aid differential diagnosis. Research into a panel of neurodegenerative biomarkers specific to various diseases with overlapping symptoms is warranted, too. For instance, Peltz et al. [74] showed that a panel of exosomal p-tau, NfL, GFAP, IL-6 and TNF-α was able to distinguish between CI veterans with and without a history of TBIs as well as veterans with a history of TBIs and symptoms of CI and those without these symptoms. Generally, exosomes appear an especially promising new tool as they are useful for detecting biomarkers that are expressed systemically and thus are not CNS-specific, for instance, inflammatory cytokines. Further, exosomes readily cross the BBB [68], hence there is no need for substantial BBB damage to detect biomarkers from blood. The greatest limitation of most of the discussed studies, both in plasma/serum- and exosome-based biomarkers, is their cross-sectional nature, with only some including structural analysis using imaging techniques, and very few confirming suspected diagnoses by post-mortem investigation. Since the disparity in results can be caused by the heterogeneity of long-term effects of TBI, which cause not only CTE, but also PD, AD, ALS, or a combination of these diseases [31,36], there is a need for longitudinal and multidimensional cohort studies combining neurobehavioral, biochemical, imaging as well as neuropathological approaches. Recently, two such studies have begun [127,128]. This way the levels of biomarkers can be associated with structural and functional brain pathology, establishing robust biomarkers of CTE, aiding diagnosis of the disease and potential preventative and symptomatic treatment. However, a substantial amount of time will pass until results and conclusions of these longitudinal studies are published. Meanwhile, further cross-sectional studies in cohorts at risk of developing CTE, especially investigating the exosomal concentrations of different biomarkers and associating them with structural abnormality in imaging studies and functional abnormality in neurobehavioral studies, are warranted.
Author Contributions
Conceptualization, P.C. and M.J.H.; writing—original draft preparation, M.H.; writing—review and editing, P.L.C, K.H.; visualization, M.J.H.; supervision, P.L.C.; project administration, P.L.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Global status report on the public health response to dementia. WHO 2021. [Google Scholar]
- Arvanitakis, Z; Shah, R. C.; Bennett, D.A. Diagnosis and Management of Dementia: Review. JAMA 2019, 322, 1589–1599. [Google Scholar] [CrossRef]
- Robinson, L.; Tang, E.; Taylor, J.-P. Dementia: timely diagnosis and early intervention. BMJ 2015, 350, h3029–h3029. [Google Scholar] [CrossRef] [PubMed]
- Martland, H.S. Punch Drunk. JAMA 1928, 91, 1103–1107. [Google Scholar] [CrossRef]
- Schwab, N.; Wennberg, R.; Grenier, K.; Tartaglia, C.; Tator, C.; Hazrati, L.-N. Association of Position Played and Career Duration and Chronic Traumatic Encephalopathy at Autopsy in Elite Football and Hockey Players. Neurology 2021, 96, e1835–e1843. [Google Scholar] [CrossRef]
- Omalu, B.I.; DeKosky, S.T.; Minster, R.L.; Kamboh, M.I.; Hamilton, R.L.; Wecht, C.H. Chronic Traumatic Encephalopathy in a National Football League Player. Neurosurgery 2005, 57, 128–134. [Google Scholar] [CrossRef]
- Omalu, B.I.; DeKosky, S.T.; Hamilton, R.L.; Minster, R.L.; Kamboh, M.I.; Shakir, A.M.; Wecht, C.H. Chronic Traumatic Encephalopathy in a National Football League Player: Part II. Neurosurgery 2006, 59, 1086–1093. [Google Scholar] [CrossRef]
- McKee, A.C.; Stein, T.D.; Nowinski, C.J.; Stern, R.A.; Daneshvar, D.H.; Alvarez, V.E.; Lee, H.-S.; Hall, G.; Wojtowicz, S.M.; Baugh, C.M.; et al. The spectrum of disease in chronic traumatic encephalopathy. Brain 2013, 136, 43–64. [Google Scholar] [CrossRef]
- Stein, T.D.; Montenigro, P.H.; Alvarez, V.E.; Xia, W.; Crary, J.F.; Tripodis, Y.; Daneshvar, D.H.; Mez, J.; Solomon, T.; Meng, G.; et al. Beta-amyloid deposition in chronic traumatic encephalopathy. Acta Neuropathol. 2015, 130, 21–34. [Google Scholar] [CrossRef]
- Mez, J.; Daneshvar, D.H.; Kiernan, P.T.; Abdolmohammadi, B.; Alvarez, V.E.; Huber, B.R.; Alosco, M.L.; Solomon, T.M.; Nowinski, C.J.; McHale, L.; et al. Clinicopathological Evaluation of Chronic Traumatic Encephalopathy in Players of American Football. JAMA 2017, 318, 360–370. [Google Scholar] [CrossRef]
- Goldstein, L.E.; Fisher, A.M.; Tagge, C.A.; Zhang, X.-L.; Velisek, L.; Sullivan, J.A.; Upreti, C.; Kracht, J.M.; Ericsson, M.; Wojnarowicz, M.W.; et al. Chronic Traumatic Encephalopathy in Blast-Exposed Military Veterans and a Blast Neurotrauma Mouse Model. Sci. Transl. Med. 2012, 4, 134. [Google Scholar] [CrossRef]
- Maroon, J.C.; Winkelman, R.; Bost, J.; Amos, A.; Mathyssek, C.; Miele, V. Chronic Traumatic Encephalopathy in Contact Sports: A Systematic Review of All Reported Pathological Cases. PLoS ONE 2015, 10, e0117338. [Google Scholar] [CrossRef]
- McKee, A.C.; Stein, T.D.; Huber, B.R.; Crary, J.F.; Bieniek, K.; Dickson, D.; Alvarez, V.E.; Cherry, J.D.; Farrell, K.; Butler, M.; et al. Chronic traumatic encephalopathy (CTE): criteria for neuropathological diagnosis and relationship to repetitive head impacts. Acta Neuropathol. 2023, OnlineFirst, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Stern, R.A.; Daneshvar, D.H.; Baugh, C.M.; Seichepine, D.R.; Montenigro, P.H.; Riley, D.O.; Fritts, N.G.; Stamm, J.M.; Robbins, C.A.; McHale, L.; et al. Clinical presentation of chronic traumatic encephalopathy. Neurology 2013, 81, 1122–1129. [Google Scholar] [CrossRef]
- Gardner, R.C.; Yaffe, K. Epidemiology of mild traumatic brain injury and neurodegenerative disease. Mol. Cell. Neurosci. 2015, 66, 75–80. [Google Scholar] [CrossRef]
- Guskiewicz, K.M.; Marshall, S.W.; Bailes, J.; McCrea, M.; Cantu, R.C.; Randolph, C.; Jordan, B.D. Association between Recurrent Concussion and Late-Life Cognitive Impairment in Retired Professional Football Players. Neurosurgery 2005, 57, 719–726. [Google Scholar] [CrossRef]
- Perry, D.C.; Sturm, V.E.; Peterson, M.J.; Pieper, C.F.; Bullock, T.; Boeve, B.F.; Miller, B.L.; Guskiewicz, K.M.; Berger, M.S.; Kramer, J.H.; et al. Association of traumatic brain injury with subsequent neurological and psychiatric disease: a meta-analysis. JNS 2016, 124, 511–526. [Google Scholar] [CrossRef]
- Barnes, D.E.; Byers, A.L.; Gardner, R.C.; Seal, K.H.; Boscardin, W.J.; Yaffe, K. Association of Mild Traumatic Brain Injury With and Without Loss of Consciousness With Dementia in US Military Veterans. JAMA Neurol 2018, 75, 1055–1061. [Google Scholar] [CrossRef]
- Hind, K.; Konerth, N.; Entwistle, I.; Hume, P.; Theadom, A.; Lewis, G.; King, D.; Goodbourn, T.; Bottiglieri, M.; Ferraces-Riegas, P.; et al. Mental Health and Wellbeing of Retired Elite and Amateur Rugby Players and Non-contact Athletes and Associations with Sports-Related Concussion: The UK Rugby Health Project. Sports. Med. 2022, 52, 1419–1431. [Google Scholar] [CrossRef]
- Alosco, M.L.; Culhane, J.; Mez, J. Neuroimaging Biomarkers of Chronic Traumatic Encephalopathy: Targets for the Academic Memory Disorders Clinic. Neurotherapeutics 2021, 18, 772–791. [Google Scholar] [CrossRef]
- Alosco, M.L.; Tripodis, Y.; Fritts, N.G.; Heslegrave, A.; Baugh, C.M.; Conneely, S.; Mariani, M.; Martin, B.M.; Frank, S.; Mez, J.; et al. Cerebrospinal fluid tau, Aβ, and sTREM2 in Former National Football League Players: Modeling the relationship between repetitive head impacts, microglial activation, and neurodegeneration. Alzheimer’s Dement. 2018, 14, 1159–1170. [Google Scholar] [CrossRef] [PubMed]
- Turk, K.W.; Geada, A.; Alvarez, V.E.; Xia, W.; Cherry, J.D.; Nicks, R.; Meng, G.; Daley, S.; Tripodis, Y.; Huber, B.R. A comparison between tau and amyloid-β cerebrospinal fluid biomarkers in chronic traumatic encephalopathy and Alzheimer disease. Alz. Res. Ther. 2022, 14, 28. [Google Scholar] [CrossRef] [PubMed]
- Teunissen, C.E.; Verberk, I.M.W.; Thijssen, E.H.; Vermunt, L.; Hansson, O.; Zetterberg, H.; van der Flier, W.M.; Mielke, M.M.; del Campo, M. Blood-based biomarkers for Alzheimer’s disease: towards clinical implementation. Lancet Neurol. 2022, 21, 66–77. [Google Scholar] [CrossRef] [PubMed]
- Gutierre, M.U.; Telles, J.P.M.; Welling, L.C.; Rabelo, N.N.; Teixeira, M.J.; Figueiredo, E.G. Biomarkers for traumatic brain injury: a short review. Neurosurg. Rev. 2021, 44, 2091–2097. [Google Scholar] [CrossRef]
- Jamerlan, A.; Dominguez, J.; Ligsay, A.; Youn, Y.C.; An, S.S.A.; Kim, S. Current fluid biomarkers, animal models, and imaging tools for diagnosing chronic traumatic encephalopathy. Mol. Cel. Toxicol. 2019, 15, 353–368. [Google Scholar] [CrossRef]
- Hiskens, M.I.; Schneiders, A.G.; Angoa-Pérez, M.; Vella, R.K.; Fenning, A.S. Blood biomarkers for assessment of mild traumatic brain injury and chronic traumatic encephalopathy. Biomarkers 2020, 25, 213–227. [Google Scholar] [CrossRef] [PubMed]
- Shahim, P.; Gill, J.M.; Blennow, K.; Zetterberg, H. Fluid Biomarkers for Chronic Traumatic Encephalopathy. Semin. Neurol. 2020, 40, 411–419. [Google Scholar] [CrossRef]
- Bergauer, A.; van Osch, R.; van Elferen, S.; Gyllvik, S.; Venkatesh, H.; Schreiber, R. The diagnostic potential of fluid and imaging biomarkers in chronic traumatic encephalopathy (CTE). Biomed. Pharmacother. 2022, 146, 112602. [Google Scholar] [CrossRef]
- Mavroudis, I.; Kazis, D.; Chowdhury, R.; Petridis, F.; Costa, V.; Balmus, I.-M.; Ciobica, A.; Luca, A.-C.; Radu, I.; Dobrin, R.P.; Baloyannis, S. Post-Concussion Syndrome and Chronic Traumatic Encephalopathy: Narrative Review on the Neuropathology, Neuroimaging and Fluid Biomarkers. Diagnostics 2022, 12, 740–763. [Google Scholar] [CrossRef]
- Pierre, K.; Molina, V.; Shukla, S.; Avila, A.; Fong, N.; Nguyen, J.; Lucke-Wold, B. Chronic traumatic encephalopathy: Diagnostic updates and advances. AIMSN 2022, 9, 519–535. [Google Scholar] [CrossRef]
- Mckee, A.C.; Daneshvar, D.H. The neuropathology of traumatic brain injury. Handb. Clin. Neurol. 2015, 127, 45–66. [Google Scholar] [CrossRef] [PubMed]
- Edwards, G.; Zhao, J.; Dash, P.K.; Soto, C.; Moreno-Gonzalez, I. Traumatic Brain Injury Induces Tau Aggregation and Spreading. J. Neurotrauma 2020, 37, 80–92. [Google Scholar] [CrossRef]
- Butler, M.L.M.D.; Dixon, E.; Stein, T.D.; Alvarez, V.E.; Huber, B.; Buckland, M.E.; McKee, A.C.; Cherry, J.D. Tau Pathology in Chronic Traumatic Encephalopathy is Primarily Neuronal. J. Neuropathol. Exp. Neurol. 2022, 81, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Gendron, T.F.; Petrucelli, L. The role of tau in neurodegeneration. Mol. Neurodegener. 2009, 4, 13. [Google Scholar] [CrossRef] [PubMed]
- McKee, A.C.; Cantu, R.C.; Nowinski, C.J.; Hedley-Whyte, E.T.; Gavett, B.E.; Budson, A.E.; Santini, V.E.; Lee, H.-S.; Kubilus, C.A.; Stern, R.A. Chronic Traumatic Encephalopathy in Athletes: Progressive Tauopathy After Repetitive Head Injury. J Neuropathol. Exp. Neurol. 2009, 68, 709–735. [Google Scholar] [CrossRef]
- McKee, A.C.; Stein, T.D.; Kiernan, P.T.; Alvarez, V.E. The Neuropathology of Chronic Traumatic Encephalopathy: CTE Neuropathology. Brain Pathol. 2015, 25, 350–364. [Google Scholar] [CrossRef]
- Smith, D.H.; Meaney, D.F.; Shull, W.H. Diffuse Axonal Injury in Head Trauma. J. Head Trauma Rehabil. 2003, 18, 307–316. [Google Scholar] [CrossRef]
- Inglese, M.; Makani, S.; Johnson, G.; Cohen, B.A.; Silver, J.A.; Gonen, O.; Grossman, R.I. Diffuse axonal injury in mild traumatic brain injury: a diffusion tensor imaging study. J. Neurosurg. 2005, 103, 298–303. [Google Scholar] [CrossRef]
- Petzold, A. Neurofilament phosphoforms: Surrogate markers for axonal injury, degeneration and loss. J. Neurol. Sci. 2005, 233, 183–198. [Google Scholar] [CrossRef]
- Siedler, D.G.; Chuah, M.I.; Kirkcaldie, M.T.K.; Vickers, J.C.; King, A.E. Diffuse axonal injury in brain trauma: insights from alterations in neurofilaments. Front. Cell. Neurosci. 2014, 8, 429. [Google Scholar] [CrossRef]
- Hay, J.R.; Johnson, V.E.; Young, A.M.H.; Smith, D.H.; Stewart, W. Blood-Brain Barrier Disruption Is an Early Event That May Persist for Many Years After Traumatic Brain Injury in Humans. J. Neuropathol. Exp. Neurol. 2015, 74, 1147–1157. [Google Scholar] [CrossRef]
- Kornguth, S.; Rutledge, N.; Perlaza, G.; Bray, J.; Hardin, A. A Proposed Mechanism for Development of CTE Following Concussive Events: Head Impact, Water Hammer Injury, Neurofilament Release, and Autoimmune Processes. Brain Sci. 2017, 7, 164–179. [Google Scholar] [CrossRef] [PubMed]
- Mayeux, R. Biomarkers: Potential uses and limitations. Neurotherapeutics 2004, 1, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Ray, P.; Manach, Y.L.; Riou, B.; Houle, T.T.; Warner, D.S. Statistical Evaluation of a Biomarker. Anesthesiology 2010, 112, 1023–1040. [Google Scholar] [CrossRef] [PubMed]
- Johnson, V.E.; Stewart, J.E.; Begbie, F.D.; Trojanowski, J.Q.; Smith, D.H.; Stewart, W. Inflammation and white matter degeneration persist for years after a single traumatic brain injury. Brain 2013, 136, 28–42. [Google Scholar] [CrossRef] [PubMed]
- Erturk, A.; Mentz, S.; Stout, E.E.; Hedehus, M.; Dominguez, S.L.; Neumaier, L.; Krammer, F.; Llovera, G.; Srinivasan, K.; Hansen, D.V. Interfering with the Chronic Immune Response Rescues Chronic Degeneration After Traumatic Brain Injury. J. Neurosci. 2016, 36, 9962–9975. [Google Scholar] [CrossRef]
- McKee, A.C. The Neuropathology of Chronic Traumatic Encephalopathy: The Status of the Literature. Semin. Neurol. 2020, 40, 359–69. [Google Scholar] [CrossRef]
- Murray, H.C.; Osterman, C.; Bell, P.; Vinnell, L.; Curtis, M.A. Neuropathology in chronic traumatic encephalopathy: a systematic review of comparative post-mortem histology literature. Acta Neuropathol. Commun. 2022, 10, 108–128. [Google Scholar] [CrossRef]
- Johnson, V.E.; Stewart, W.; Smith, D.H. Widespread Tau and Amyloid-Beta Pathology Many Years After a Single Traumatic Brain Injury in Humans: Long-Term AD-Like Pathology after Single TBI. Brain Pathol. 2012, 22, 142–149. [Google Scholar] [CrossRef]
- Alosco, M.L.; Su, Y.; Stein, T.D.; Protas, H.; Cherry, J.D.; Adler, C.H.; Balcer, L.J.; Bernick, C.; Pulukuri, S.V.; Abdolmohammadi, B.; et al. Associations between near end-of-life flortaucipir PET and postmortem CTE-related tau neuropathology in six former American football players. Eur. J Nucl. Med. Mol. Imaging 2022, 50, 435–452. [Google Scholar] [CrossRef]
- Mohamed, A.Z.; Cumming, P.; Nasrallah, F.A.; Alzheimer’s Disease Neuroimaging Initiative. Escalation of Tau Accumulation after a Traumatic Brain Injury: Findings from Positron Emission Tomography. Brain Sci. 2022, 12, 876. [Google Scholar] [CrossRef]
- Gorgoraptis, N.; Li, L.M.; Whittington, A.; Zimmerman, K.A.; Maclean, L.M.; McLeod, C.; Ross, E.; Heslegrave, A.; Zetterberg, H.; Passchier, J.; et al. In vivo detection of cerebral tau pathology in long-term survivors of traumatic brain injury. Sci. Transl. Med. 2019, 11, eaaw1993. [Google Scholar] [CrossRef] [PubMed]
- Muraoka, S.; Jedrychowski, M.P.; Tatebe, H.; DeLeo, A.M.; Ikezu, S.; Tokuda, T.; Gygi, S.P.; Stern, R.A.; Ikezu, T. Proteomic Profiling of Extracellular Vesicles Isolated From Cerebrospinal Fluid of Former National Football League Players at Risk for Chronic Traumatic Encephalopathy. Front. Neurosci. 2019, 13, 1059. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, R.; Sharma, D.R.; Chang, B.; Oumata, N.; Cam, M.; Vaucelle, L.; Lindberg, M.F.; Chiu, A.; Wisniewski, T.; Wang, K.K.W.; et al. Novel Mouse Tauopathy Model for Repetitive Mild Traumatic Brain Injury: Evaluation of Long-Term Effects on Cognition and Biomarker Levels After Therapeutic Inhibition of Tau Phosphorylation. Front. Neurol. 2019, 10, 124. [Google Scholar] [CrossRef]
- Alosco, M.L.; Tripodis, Y.; Jarnagin, J.; Baugh, C.M.; Martin, B.; Chaisson, C.E.; Estochen, N.; Song, L.; Cantu, R.C.; Jeromin, A.; et al. Repetitive head impact exposure and later-life plasma total tau in former National Football League players. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2017, 7, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Swann, O.J.; Turner, M.; Heslegrave, A.; Zetterberg, H. Fluid biomarkers and risk of neurodegenerative disease in retired athletes with multiple concussions: results from the International Concussion and Head Injury Research Foundation Brain health in Retired athletes Study of Ageing and Impact-Related Neurodegenerative Disease (ICHIRF-BRAIN study). BMJ Open Sport Exerc. Med. 2022, 8, e001327. [Google Scholar] [CrossRef]
- Shahim, P.; Politis, A.; van der Merwe, A.; Moore, B.; Ekanayake, V.; Lippa, S.M.; Chou, Y.-Y.; Pham, D.L.; Butman, J.A.; Diaz-Arrastia, R.; et al. Time course and diagnostic utility of NfL, tau, GFAP, and UCH-L1 in subacute and chronic TBI. Neurology 2020, 95, e623–e636. [Google Scholar] [CrossRef]
- Shahim, P.; Zetterberg, H.; Simrén, J.; Ashton, N.J.; Norato, G.; Schöll, M.; Tegner, Y.; Diaz-Arrastia, R.; Blennow, K. Association of Plasma Biomarker Levels With Their CSF Concentration and the Number and Severity of Concussions in Professional Athletes. Neurology 2022, 99, e347–e354. [Google Scholar] [CrossRef]
- Vasilevskaya, A.; Taghdiri, F.; Multani, N.; Ozzoude, M.; Tarazi, A.; Khodadadi, M.; Wennberg, R.; Rusjan, P.; Houle, S.; Green, R.; et al. Investigating the use of plasma pTau181 in retired contact sports athletes. J Neurol. 2022, 269, 5582–5595. [Google Scholar] [CrossRef]
- Olivera, A.; Lejbman, N.; Jeromin, A.; French, L.M.; Kim, H.-S.; Cashion, A.; Mysliwiec, V.; Diaz-Arrasti, R.; Gill, J. Peripheral Total Tau in Military Personnel Who Sustain Traumatic Brain Injuries During Deployment. JAMA Neurol 2015, 72, 1109. [Google Scholar] [CrossRef]
- Zetterberg, H.; Wilson, D.; Andreasson, U.; Minthon, L.; Blennow, K.; Randall, J.; Hansson, O. Plasma tau levels in Alzheimer’s disease. Alzheimer’s Res. Ther. 2013, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Arastoo, M.; Lofthouse, R.; Penny, L.K.; Harrington, C.R.; Porter, A.; Wischik, C.M.; Palliyil, S. Current Progress and Future Directions for Tau-Based Fluid Biomarker Diagnostics in Alzheimer’s Disease. IJMS 2020, 21, 8673. [Google Scholar] [CrossRef]
- Goedert, M.; Spillantini, M.G.; Crowther, R.A. Cloning of a big tau microtubule-associated protein characteristic of the peripheral nervous system. Proc. Natl. Acad. Sci. U.S.A. 1992, 89, 1983–1987. [Google Scholar] [CrossRef]
- Knaepen, K.; Goekint, M.; Heyman, E.M.; Meeusen, R. Neuroplasticity—Exercise-Induced Response of Peripheral Brain-Derived Neurotrophic Factor: A Systematic Review of Experimental Studies in Human Subjects. Sports Med. 2010, 40, 765–801. [Google Scholar] [CrossRef]
- Laverse, E.; Guo, T.; Zimmerman, K.; Foiani, M.S.; Velani, B.; Morrow, P.; Adejuwon, A.; Bamford, R.; Underwood, N.; George, J.; et al. Plasma glial fibrillary acidic protein and neurofilament light chain, but not tau, are biomarkers of sports-related mild traumatic brain injury. Brain Commun. 2020, 2, fcaa137. [Google Scholar] [CrossRef]
- Gonzalez-Ortiz, F.; Turton, M.; Kac, P.R.; Smirnov, D.; Premi, E.; Ghidoni, R.; Benussi, L.; Cantoni, V.; Saraceno, C.; Rivolta, J. Brain-derived tau: a novel blood-based biomarker for Alzheimer’s disease-type neurodegeneration. Brain 2020, 146, 1152–1165. [Google Scholar] [CrossRef]
- Li, D.; Mielke, M.M. An Update on Blood-Based Markers of Alzheimer’s Disease Using the SiMoA Platform. Neurol. Ther. 2019, 8, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Guedes, V.A.; Devoto, C.; Leete, J.; Sass, D.; Acott, J.D.; Mithani, S.; Gill, J.M. Extracellular Vesicle Proteins and MicroRNAs as Biomarkers for Traumatic Brain Injury. Front. Neurol. 2020, 11, 663. [Google Scholar] [CrossRef] [PubMed]
- Stern, R.A.; Tripodis, Y.; Baugh, C.M.; Fritts, N.G.; Martin, B.M.; Chaisson, C.; Cantu, R.C.; Joyce, J.A.; Shah, S.; Ikezu, T. Preliminary Study of Plasma Exosomal Tau as a Potential Biomarker for Chronic Traumatic Encephalopathy. JAD 2016, 51, 1099–1109. [Google Scholar] [CrossRef]
- Gill, J.; Mustapic, M.; Diaz-Arrastia, R.; Lange, R.; Gulyani, S.; Diehl, T.; Motamedi, V.; Osier, N.; Stern, R.A.; Kapogiannis, D. Higher exosomal tau, amyloid-beta 42 and IL-10 are associated with mild TBIs and chronic symptoms in military personnel. Brain Inj. 2018, 32, 1359–1366. [Google Scholar] [CrossRef]
- Kenney, K.; Qu, B.-X.; Lai, C.; Devoto, C.; Motamedi, V.; Walker, W.C.; Levin, H.S.; Nolen, T.; Wilde, E.A.; Diaz-Arrastia, R.; et al. Higher exosomal phosphorylated tau and total tau among veterans with combat-related repetitive chronic mild traumatic brain injury. Brain Inj. 2018, 32, 1276–1284. [Google Scholar] [CrossRef]
- Goetzl, E.J.; Elahi, F.M.; Mustapic, M.; Kapogiannis, D.; Pryhoda, M.; Gilmore, A.; Gorgens, K.A.; Davidson, B.; Granholm, A.; Ledreux, A. Altered levels of plasma neuron-derived exosomes and their cargo proteins characterize acute and chronic mild traumatic brain injury. FASEB J. 2019, 33, 5082–5088. [Google Scholar] [CrossRef] [PubMed]
- Muraoka, S.; DeLeo, A.M.; Yang, Z.; Tatebe, H.; Yukawa-Takamatsu, K.; Ikezu, S.; Tokuda, T.; Issadore, D.; Stern, R.A.; Ikezu, T. Proteomic Profiling of Extracellular Vesicles Separated from Plasma of Former National Football League Players at Risk for Chronic Traumatic Encephalopathy. Aging Dis. 2021, 12, 1363–1375. [Google Scholar] [CrossRef] [PubMed]
- Peltz, C.B.; Kenney, K.; Gill, J.; Diaz-Arrastia, R.; Gardner, R.C.; Yaffe, K. Blood biomarkers of traumatic brain injury and cognitive impairment in older veterans. Neurology 2020, 95, e1126–e1133. [Google Scholar] [CrossRef]
- Yin, Q.; Ji, X.; Lv, R.; Pei, J.-J.; Du, Y.; Shen, C.; Hou, X. Targetting Exosomes as a New Biomarker and Therapeutic Approach for Alzheimer’s Disease. CIA 2020, 15, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Asken, B.M.; Tanner, J.A.; VandeVrede, L.; Mantyh, W.G.; Casaletto, K.B.; Staffaroni, A.M.; La Joie, R.; Iaccarino, L.; Soleimani-Meigooni, D.; Rojas, J.C. Plasma P-tau181 and P-tau217 in Patients With Traumatic Encephalopathy Syndrome With and Without Evidence of Alzheimer Disease Pathology. Neurology 2022, 99, e594–e604. [Google Scholar] [CrossRef]
- Varesi, A.; Carrara, A.; Pires, V.G.; Floris, V.; Pierella, E.; Savioli, G.; Prasad, S.; Esposito, C.; Ricevuti, G.; Chirumbolo, S.; et al. Blood-Based Biomarkers for Alzheimer’s Disease Diagnosis and Progression: An Overview. Cells 2022, 11, 1367. [Google Scholar] [CrossRef]
- Rubenstein, R.; Chang, B.; Yue, J.K.; Chiu, A.; Winkler, E.A.; Puccio, A.M.; Diaz-Arrastia, R.; Yuh, E.L.; Mukherjee, P.; Valadka, A.B.; et al. Comparing Plasma Phospho Tau, Total Tau, and Phospho Tau–Total Tau Ratio as Acute and Chronic Traumatic Brain Injury Biomarkers. JAMA Neurol 2017, 74, 1063. [Google Scholar] [CrossRef] [PubMed]
- Stathas, S.; Alvarez, V.E.; Xia, W.; Nicks, R.; Meng, G.; Daley, S.; Pothast, M.; Shah, A.; Kelley, H.; Esnault, C.; et al. Tau phosphorylation sites serine202 and serine396 are differently altered in chronic traumatic encephalopathy and Alzheimer’s disease. Alzheimer’s Dement. 2022, 18, 1511–1522. [Google Scholar] [CrossRef] [PubMed]
- Goetzl, E.J.; Peltz, C.B.; Mustapic, M.; Kapogiannis, D.; Yaffe, K. Neuron-Derived Plasma Exosome Proteins after Remote Traumatic Brain Injury. J. Neurotrauma 2020, 37, 382–388. [Google Scholar] [CrossRef]
- Gong, C-X. ; Liu, F.; Grundke-Iqbal, I.; Iqbal, K. Post-translational modifications of tau protein in Alzheimer’s disease. J. Neural. Transm. 2005, 112, 813–838. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.H.; Chen, X.H.; Iwata, A.; Graham, D.I. Amyloid beta accumulation in axons after traumatic brain injury in humans. J. Neurosurg. 2003, 98, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Olsson, A.; Csajbok, L.; Ost, M.; Höglund, K.; Nylén, K.; Rosengren, L.; Nellgård, B.; Blennow, K. Marked increase of beta-amyloid(1-42) and amyloid precursor protein in ventricular cerebrospinal fluid after severe traumatic brain injury. J. Neurol. 2004, 251, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Goyal, R. Amyloid beta plaque: a culprit for neurodegeneration. Acta Neurol. Belg. 2016, 116, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Lejbman, N.; Olivera, A.; Heinzelmann, M.; Feng, R.; Yun, S.; Kim, H.-S.; Gill, J. Active duty service members who sustain a traumatic brain injury have chronically elevated peripheral concentrations of A β 40 and lower ratios of A β 42/40. Brain Inj. 2016, 30, 1436–1441. [Google Scholar] [CrossRef]
- Khalil, M.; Teunissen, C.E.; Otto, M.; Piehl, F.; Sormani, M.P.; Gattringer, T.; Barro, C.; Kappos, L.; Comabella, M.; Fazekas, F.; et al. Neurofilaments as biomarkers in neurological disorders. Nat. Rev. Neurol. 2008, 14, 577–589. [Google Scholar] [CrossRef] [PubMed]
- Al Nimer, F.; Thelin, E.; Nyström, H.; Dring, A.M.; Svenningsson, A.; Piehl, F.; Nelson, D.W.; Bellander, B.M. Comparative Assessment of the Prognostic Value of Biomarkers in Traumatic Brain Injury Reveals an Independent Role for Serum Levels of Neurofilament Light. PloS ONE 2015, 10, e0132177. [Google Scholar] [CrossRef]
- Shahim, P.; Gren, M.; Liman, V.; Andreasson, U.; Norgren, N.; Tegner, Y.; Mattsson, N.; Andreasen, N.; Ost, M.; Zetterberg, H.; et al. Serum neurofilament light protein predicts clinical outcome in traumatic brain injury. Sci. Rep. 2016, 6, 36791. [Google Scholar] [CrossRef]
- Boutté, A.M.; Thangavelu, B.; LaValle, C.R.; Nemes, J.; Gilsdorf, J.; Shear, D.A.; Kamimori, G.H. Brain-related proteins as serum biomarkers of acute, subconcussive blast overpressure exposure: A cohort study of military personnel. PLoS ONE 2019, 14, e0221036. [Google Scholar] [CrossRef]
- Gao, W.; Zhang, Z.; Lv, X.; Wu, Q.; Yan, J.; Mao, G.; Xing, W. Neurofilament light chain level in traumatic brain injury: A system review and meta-analysis. Medicine 2020, 99, e22363. [Google Scholar] [CrossRef]
- Dickstein, D.L.; De Gasperi, R.; Gama Sosa, M.A.; Perez-Garcia, G.; Short, J.A.; Sosa, H.; Perez, G.M.; Tschiffely, A.E.; Dams-O’Connor, K.; Pullman, M.Y.; et al. Brain and blood biomarkers of tauopathy and neuronal injury in humans and rats with neurobehavioral syndromes following blast exposure. Mol Psychiatry 2021, 26, 5940–5954. [Google Scholar] [CrossRef] [PubMed]
- Flynn, S.; Leete, J.; Shahim, P.; Pattinson, C.; Guedes, V.A.; Lai, C.; Devoto, C.; Qu, B.-X.; Greer, K.; Moore, B. Extracellular vesicle concentrations of glial fibrillary acidic protein and neurofilament light measured 1 year after traumatic brain injury. Sci. Rep. 2021, 11, 3896. [Google Scholar] [CrossRef] [PubMed]
- Asken, B.M.; Tanner, J.A.; Vande-Vrede, L.; Casaletto, K.B.; Staffaroni, A.M.; Mundada, N.; Fonseca, C.; Iaccarino, L.; La Joie, R.; Tsuei, T.; et al. Multi-Modal Biomarkers of Repetitive Head Impacts and Traumatic Encephalopathy Syndrome: A Clinicopathological Case Series. J. Neurotrauma 2022, 39, 1195–1213. [Google Scholar] [CrossRef] [PubMed]
- Bishop, P.; Rocca, D.; Henley, J.M. Ubiquitin C-terminal hydrolase L1 (UCH-L1): structure, distribution and roles in brain function and dysfunction. The Biochemical journal 2016, 473, 2453–2462. [Google Scholar] [CrossRef]
- Öhrfelt, A.; Johansson, P.; Wallin, A.; Andreasson, U.; Zetterberg, H.; Blennow, K.; Svensson, J. Increased Cerebrospinal Fluid Levels of Ubiquitin Carboxyl-Terminal Hydrolase L1 in Patients with Alzheimer’s Disease. Dementia and geriatric cognitive disorders extra 2016, 6, 283–294. [Google Scholar] [CrossRef]
- Kulczynska-Przybik, A.; Dulewicz, M.; Mroczko, P.; Borawska, R.; Doroszkiewicz, J.; Litman-Zawadzka, A.; Arslan, D.; Slowik, A. The assessment of ubiquitin C-terminal hydrolase-1 (UCH-L1) in patients with Alzheimer’s disease. Alzheimer’s Dement. 2022, 18, e062156. [Google Scholar] [CrossRef]
- Adams, J.W.; Alvarez, V.E.; Mez, J.; Huber, B.R.; Tripodis, Y.; Xia, W.; Meng, G.; Kubilus, C.A.; Cormier, K.; Kiernan, P.T.; et al. Lewy Body Pathology and Chronic Traumatic Encephalopathy Associated With Contact Sports. J Neuropathol. Exp. Neurol. 2018, 77, 757–768. [Google Scholar] [CrossRef]
- Meade, R.M.; Fairlie, D.P.; Mason, J.M. Alpha-synuclein structure and Parkinson’s disease—lessons and emerging principles. Mol Neurodegeneration 2019, 14, 29. [Google Scholar] [CrossRef]
- Lozano, D.; Gonzales-Portillo, G.S.; Acosta, S.; de la Pena, I.; Tajiri, N.; Kaneko, Y.; Borlongan, C.V. Neuroinflammatory responses to traumatic brain injury: etiology, clinical consequences, and therapeutic opportunities. Neuropsychiatr. Dis. Treat. 2015, 11, 97–106. [Google Scholar] [CrossRef]
- Loane, D.J.; Kumar, A. Microglia in the TBI brain: The good, the bad, and the dysregulated. Exp. Neurol. 2016, 275, 316–327. [Google Scholar] [CrossRef]
- Plesnila, N. The immune system in traumatic brain injury. Curr. Opin. Pharmacol. 2016, 26, 110–117. [Google Scholar] [CrossRef]
- Collins-Praino, L.E.; Corrigan, F. Does neuroinflammation drive the relationship between tau hyperphosphorylation and dementia development following traumatic brain injury? Brain Behav. Immun. 2017, 60, 369–382. [Google Scholar] [CrossRef]
- Odfalk, K.F.; Bieniek, K.F.; Hopp, S.C. Microglia: Friend and foe in tauopathy. Prog. Neurobiol. 2022, 216, 102306. [Google Scholar] [CrossRef]
- Coughlin, J.M.; Wang, Y.; Munro, C.A.; Ma, S.; Yue, C.; Chen, S.; Airan, R.; Kim, P.K.; Adams, A.V.; Garcia, C.; et al. Neuroinflammation and brain atrophy in former NFL players: An in vivo multimodal imaging pilot study. Neurobiol. Dis. 2015, 74, 58–65. [Google Scholar] [CrossRef]
- Loane, D.J.; Kumar, A.; Stoica, B.A.; Cabatbat, R.; Faden, A.I. Progressive neurodegeneration after experimental brain trauma: association with chronic microglial activation. J Neuropathol. Exp. Neurol. 2014, 73, 14–29. [Google Scholar] [CrossRef] [PubMed]
- Sofroniew, M.V.; Vinters, H.V. Astrocytes: biology and pathology. Acta neuropathologica, 2010, 119, 7–35. [Google Scholar] [CrossRef] [PubMed]
- Burda, J.E.; Bernstein, A.M.; Sofroniew, M.V. Astrocyte roles in traumatic brain injury. Exp. Neurol. 2016, 275, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Liddelow, S.A.; Barres, B.A. Reactive astrocytes: production, function, and therapeutic potential. Immunity 2017, 46, 957–967. [Google Scholar] [CrossRef] [PubMed]
- Abdelhak, A.; Foschi, M.; Abu-Rumeileh, S.; Yue, J.K.; D’Anna, L.; Huss, A.; Oeckl, P.; Ludolph, A.C.; Kuhle, J.; Petzold, A. Blood GFAP as an emerging biomarker in brain and spinal cord disorders. Nat. Rev. Neurol. 2022, 18, 158–172. [Google Scholar] [CrossRef] [PubMed]
- Lumpkins, K.M.; Bochicchio, G.V.; Keledjian, K.; Simard, J.M.; McCunn, M.; Scalea, T. Glial fibrillary acidic protein is highly correlated with brain injury. J Trauma. 2008, 65, 778–784. [Google Scholar] [CrossRef] [PubMed]
- Gill, J.; Latour, L.; Diaz-Arrastia, R.; Motamedi, V.; Turtzo, C.; Shahim, P.; Mondello, S.; DeVoto, C.; Veras, E.; Hanlon, D.; et al. Glial fibrillary acidic protein elevations relate to neuroimaging abnormalities after mild TBI. Neurology 2018, 91, e1385–e1389. [Google Scholar] [CrossRef]
- Huebschmann, N.A.; Luoto, T.M.; Karr, J.E.; Berghem, K.; Blennow, K.; Zetterberg, H.; Ashton, N.J.; Simrén, J.; Posti, J.P.; Gill, J.M.; et al. Comparing Glial Fibrillary Acidic Protein (GFAP) in Serum and Plasma Following Mild Traumatic Brain Injury in Older Adults. Front. Neurol. 2020, 11, 1054. [Google Scholar] [CrossRef] [PubMed]
- Gilad, S.; Meiri, E.; Yogev, Y.; Benjamin, S.; Lebanony, D.; Yerushalmi, N.; Benjamin, H.; Kushnir, M.; Cholakh, H.; Melamed, N.; Bentwich, Z.; Hod, M.; Goren, Y.; Chajut, A. Serum MicroRNAs Are Promising Novel Biomarkers. PLoS ONE 2008, 3, e3148. [Google Scholar] [CrossRef]
- Hiskens, M.I.; Mengistu, T.S.; Li, K.M.; Fenning, A.S. Systematic Review of the Diagnostic and Clinical Utility of Salivary microRNAs in Traumatic Brain Injury (TBI). IJMS 2022, 23, 13160. [Google Scholar] [CrossRef] [PubMed]
- Bhomia, M.; Balakathiresan, N.S.; Wang, K.K.; Papa, L.; Maheshwari, R.K. A Panel of Serum MiRNA Biomarkers for the Diagnosis of Severe to Mild Traumatic Brain Injury in Humans. Sci. Rep. 2016, 6, 28148. [Google Scholar] [CrossRef]
- Redell, J.B.; Moore, A.N.; Ward, N.H.; Hergenroeder, G.W.; Dash, P.K. Human Traumatic Brain Injury Alters Plasma microRNA Levels. J. Neurotrauma 2010, 27, 2147–2156. [Google Scholar] [CrossRef] [PubMed]
- Wyczechowska, D.; Harch, P.G.; Mullenix, S.; Fannin, E.S.; Chiappinelli, B.B.; Jeansonne, D.; Lassak, A.; Bazan, N.G.; Peruzzi, F. Serum microRNAs associated with concussion in football players. Front. Neurol. 2023, 14, 1155479. [Google Scholar] [CrossRef]
- Alvia, M.; Aytan, N.; Spencer, K.R.; Foster, Z.W.; Rauf, N.A.; Guilderson, L.; Robey, I.; Averill, J.G.; Walker, S.E.; Alvarez, V.E.; et al. MicroRNA Alterations in Chronic Traumatic Encephalopathy and Amyotrophic Lateral Sclerosis. Front. Neurosci. 2022, 16, 855096. [Google Scholar] [CrossRef]
- Ghai, V.; Fallen, S.; Baxter, D.; Scherler, K.; Kim, T.-K.; Zhou, Y.; Meabon, J.S.; Logsdon, A.F.; Banks, W.A.; Schindler, A.G.; et al. Alterations in Plasma microRNA and Protein Levels in War Veterans with Chronic Mild Traumatic Brain Injury. J. Neurotrauma 2020, 37, 1418–1430. [Google Scholar] [CrossRef]
- Ge, X.; Guo, M.; Li, M.; Zhang, S.; Qiang, J.; Zhu, L.; Cheng, L.; Li, W.; Wang, Y.; Yu, J.; et al. Potential blood biomarkers for chronic traumatic encephalopathy: The multi-omics landscape of an observational cohort. Front. Aging Neurosci. 2022, 14, 1052765. [Google Scholar] [CrossRef]
- Chen, Y; Huang, W; Constantini, S. The Differences between Blast-Induced and Sports-Related Brain Injuries. Front Neurol. 2013, 4, 119. [Google Scholar] [CrossRef]
- Patricios, J.S.; Schneider, K.J.; Dvorak, J.; Ahmed, O.H.; Blauwet, C.; Cantu, R.C.; Davis, G.A.; Echemendia, R.J.; Makdissi, M.; McNamee, M.; et al. Consensus statement on concussion in sport: the 6th International Conference on Concussion in Sport–Amsterdam, October 2022. Br. J. Sports Med. 2023, 57, 695–711. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.P.; Priemer, D.S.; Perl, D.P.; Filley, C.M. Sports Concussion and Chronic Traumatic Encephalopathy: Finding a Path Forward. Ann. Neurol. 2023, 93, 222–225. [Google Scholar] [CrossRef] [PubMed]
- Nowinski, C.J.; Bureau, S.C.; Buckland, M.E.; Curtis, M.A.; Daneshvar, D.H.; Faull, R.L.M.; Grinberg, L.T.; Hill-Yardin, E.L.; Murray, H.C.; Pearce, A.J.; et al. Applying the Bradford Hill Criteria for Causation to Repetitive Head Impacts and Chronic Traumatic Encephalopathy. Front. Neurol. 2022, 13, 938163. [Google Scholar] [CrossRef]
- Chen, J; Li, P. ; Zhang, T.; Xu, Z.; Huang, X.; Wang, R.; Du, L. Review on Strategies and Technologies for Exosome Isolation and Purification. Front. Bioeng. Biotechnol. 2022, 9, 811971. [Google Scholar] [CrossRef] [PubMed]
- Sass, D.; Guedes, V.A.; Smith, E.G.; Vorn, R.; Devoto, C.; Edwards, K.A.; Mithani, S.; Hentig, J.; Lai, C.; Wagner, C. Sex Differences in Behavioral Symptoms and the Levels of Circulating GFAP, Tau, and NfL in Patients With Traumatic Brain Injury. Front. Pharmacol. 2021, 12, 746491. [Google Scholar] [CrossRef] [PubMed]
- Alosco, M.L.; Mariani, M.L.; Adler, C.H.; Balcer, L.J.; Bernick, C.; Au, R.; Banks, S.J.; Barr, W.B.; Bouix, S.; Cantu, R.C.; et al. Developing methods to detect and diagnose chronic traumatic encephalopathy during life: rationale, design, and methodology for the DIAGNOSE CTE Research Project. Alz. Res. Ther. 2021, 13, 136. [Google Scholar] [CrossRef]
- van Amerongen, S.; Caton, D.K.; Ossenkoppele, R.; Barkhof, F.; Pouwels, P.J.W.; Teunissen, C.E.; Rozemuller, A.J.M.; Hoozemans, J.J.M.; Pijnenburg, Y.A.L.; Scheltens, P.; et al. Rationale and design of the “NEurodegeneration: Traumatic brain injury as Origin of the Neuropathology (NEwTON)” study: a prospective cohort study of individuals at risk for chronic traumatic encephalopathy. Alz. Res. Therapy 2022, 14, 119. [Google Scholar] [CrossRef]
Figure 1.
Impairment of the blood-brain barrier (BBB) following a traumatic brain injury (TBI) and a subsequent outflow of biomarkers into the systemic circulation. TBI damages axons and instigates inflammatory response leading to efflux of neurodegenerative biomarkers, such as phosphorylated tau (p-tau) from neurons, as well as inflammation biomarkers, such as glial fibrillary acidic protein (GFAP) from astrocytes, into interstitial fluid (ISF). TBI can also damage cells maintaining the BBB (damaged cells in dark red), leading to increased permeability of the BBB and thus the influx of biomarkers into blood capillaries. Created with biorender.com.
Figure 1.
Impairment of the blood-brain barrier (BBB) following a traumatic brain injury (TBI) and a subsequent outflow of biomarkers into the systemic circulation. TBI damages axons and instigates inflammatory response leading to efflux of neurodegenerative biomarkers, such as phosphorylated tau (p-tau) from neurons, as well as inflammation biomarkers, such as glial fibrillary acidic protein (GFAP) from astrocytes, into interstitial fluid (ISF). TBI can also damage cells maintaining the BBB (damaged cells in dark red), leading to increased permeability of the BBB and thus the influx of biomarkers into blood capillaries. Created with biorender.com.
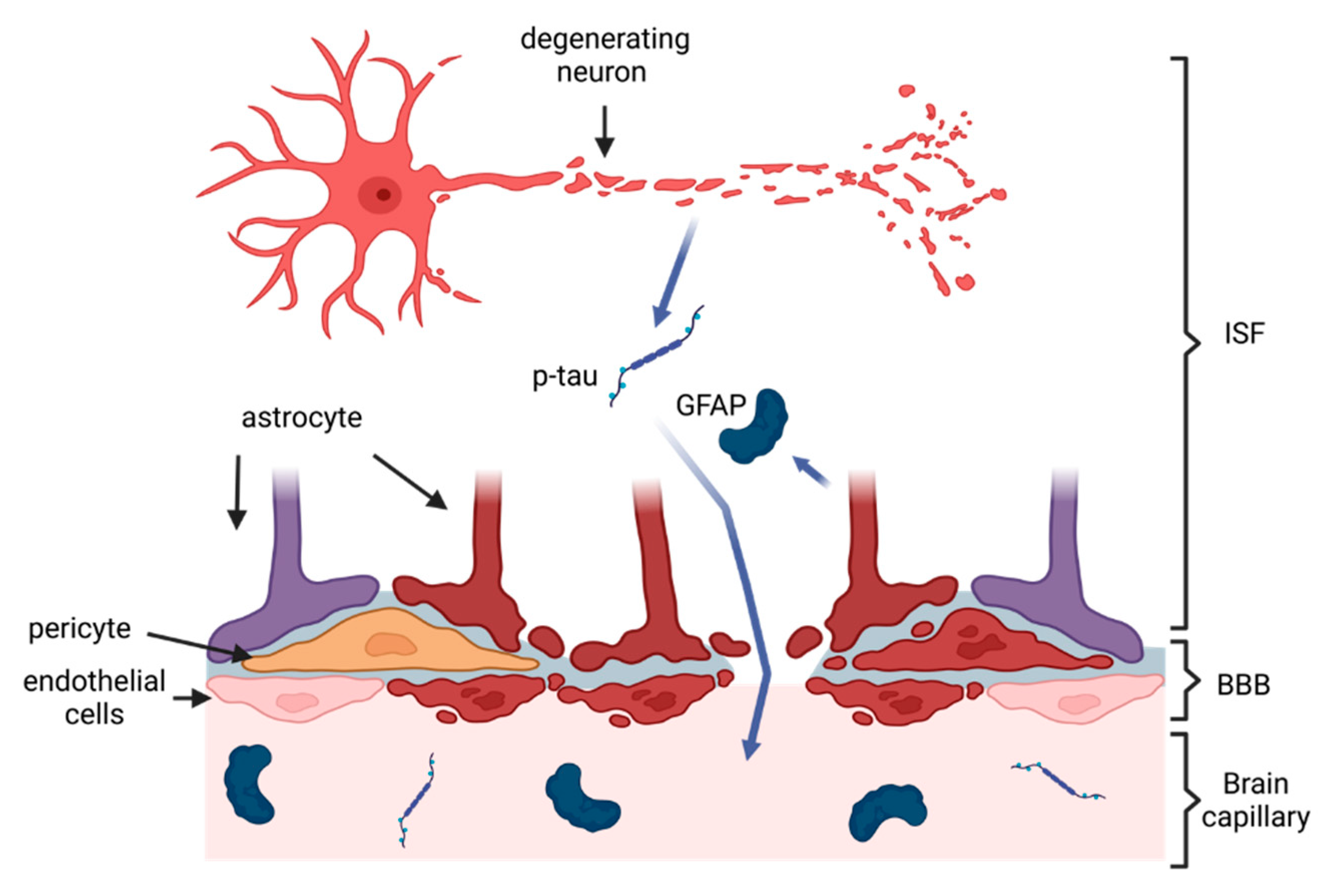
Figure 2.
Summary of potential protein biomarkers that showed promising results in their use for CTE diagnosis with molecular pathology they indicate. Created with biorender.com.
Figure 2.
Summary of potential protein biomarkers that showed promising results in their use for CTE diagnosis with molecular pathology they indicate. Created with biorender.com.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



