
Submitted:
10 July 2023
Posted:
12 July 2023
You are already at the latest version
Abstract
GI endoscopy forms an important part in a daily practice of a gastroenterologist. Musculoskeletal injuries related to GI endoscopy are on the rise. Observational studies and surveys depict the importance of proper ergonomical environment when performing GI endoscopy. Our aim is to outline preventive measures in gastrointestinal (GI) endoscopy in reducing possibility for occupational injury. We review most relevant studies that outline the gravity of the problem. A detailed analysis of proposed ergonomical recommendations is performed, outlining crucial steps in injury prevention. Proper ergonomical education is a key-step in preventing occupational injury. Robotics and other mechanical solutions offer a variety of approaches tackling the ergonomical challenge. Implementing proper ergonomical education and mechanical solutions lowers the possibility if occupational injury. Strategies and appliances presented are beneficial to all GI endoscopy practitioners.
Keywords:
GI endoscopy
; occupational injury
; ergonometry
1. Introduction
Gastrointestinal (GI) endoscopy forms an important part of daily practice of a gastroenterologist. Its use and applicability nowadays shift from diagnostic to therapeutic field and forms a significant workload on the GI practitioner. Having in mind that the basic design of a flexible endoscope remained practically the same for the last couple of decades[1] and considering the complexity of modern endoscopic procedures, musculo-skeletal injuries amongst endoscopists are on the rise. According to Young et al a systematic review of 13 studies showed that 39–89% of surveyed endoscopists reported pain and/or injuries related to endoscopy. Common areas of pain were the back (15–57%), neck (9–46%), shoulders (9–19%), elbows (8–15%) and hands/fingers (14–82%). Risk factors included procedure volume, time spent doing endoscopy, cumulative time in practice and endoscopist age. Experimental studies showed that forces and loads placed on endoscopists’ bodies during procedures place them at risk of occupational injury. Areas of pain differed between novice and experienced endoscopists implying separate mechanisms of injury[2]. Villa et al depicted the importance of proper endoscopy training in young fellows. Among the 2 researched groups, the one without formal ergonomic training, reported a significantly higher percentage of musculo-skeletal injuries related to endoscopy[3,4]. With this emerging and growing problem, a set of basic recommendations was published by Amandeep K. Shergill[5]. The author is addressing basic principles of ergonomics related to endoscopy and proposing organisational and spatial solutions with the intent of minimizing the possibility of occupational injury. In the following years, similar publications were published addressing the problem and offering similar solutions[6,7,8,9,10,11]. However, a practical solution in a form of an accessorize or machine to the ergonomic problem is lacking. The focus of this literature review is to outline currently proposed measures regarding prevention of musculoskeletal injuries in gastrointestinal endoscopy.
2. Ergonomic Challenges
To address proposed solutions to the muscle and body overload during endoscopic procedures, basics of ergonomics in endoscopy must be outlined. Ergonomics, as applied to endoscopy, can be broadly defined as the study of endoscopists’ interactions with elements of their work environment, including the endoscope and endoscopy unit, and redesigning these to minimize the risk of endoscopy-related injury, optimize endoscopist well-being, and maximize overall system performance[7]. With the development of new methods and procedures, endoscopy is becoming more and more physically demanding. According to surveys gastroenterologist report to spend at least 40% of their time practicing endoscopic procedures[12]. Research indicates that if no ergonomic education is exercised, musculo-skeletal injuries can already happen in young fellows[3]. Injuries related to practicing endoscopy can shorten endoscopists’ careers, reduce personnel available for healthcare delivery, and thereby negatively impact patient care[7]. Table 1 summarizes systematic reviews, surveys and cross-sectional studies outlining the weight of the ergonomical challenge.
When practicing endoscopy, endoscopists uses both hands with the combination of proper body posture[7,17](Figure1).
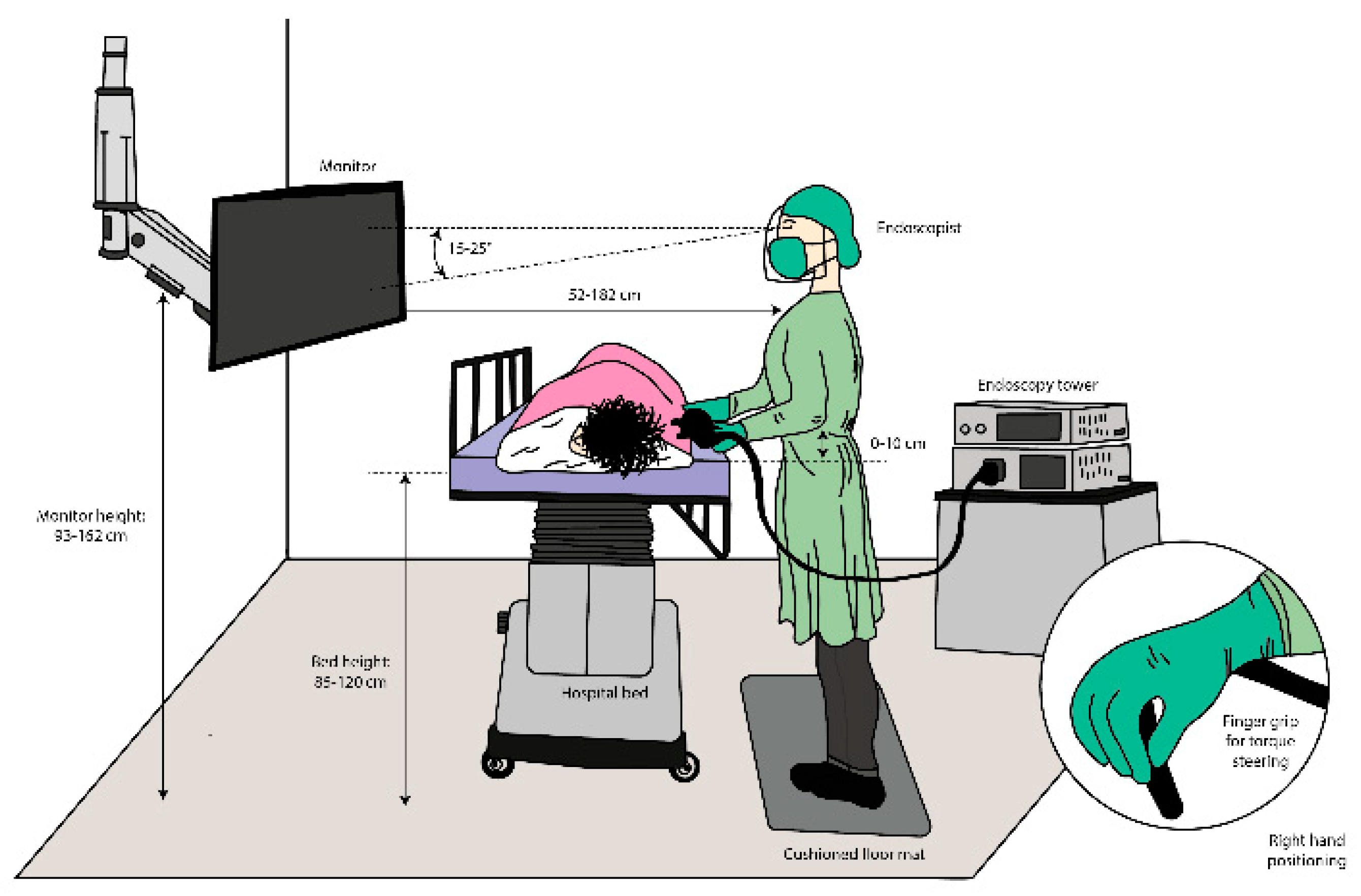
Figure 1.
Recommended layout and positioning of an endoscopist in endoscopic room as recommended in guidelines by ASGE[7].
Figure 1.
Recommended layout and positioning of an endoscopist in endoscopic room as recommended in guidelines by ASGE[7].
In his detailed review, Harvin addresses the risk of occupational injuries in endoscopists and outlines preventive measures, reviewing total of 62 articles. He identifies most common joint syndromes and specific areas of the body affected when exercising endoscopy. The correlation between higher procedure time and higher risk of injury is also presented. His review finds that the management of the risk of musculoskeletal injuries related to endoscopy falls into 3 categories: compliance with currently recommended ergonomic practices, education of trainees in ergonomic technique when practicing endoscopy, and research toward the modification and development of more ergonomic endoscopes and procedure spaces and toward the better accommodation of practitioners with smaller hand sizes[13].
Villa et al, demonstrated that musculoskeletal injuries related to endoscopy already happen in young fellows, predominantly in those who didn’t receive proper ergonomical training. In his survey-based study about ergonomics and work-related musculoskeletal injuries, a total of 156 participants were included. 47% of them reported a new musculoskeletal injury related to endoscopy, most commonly in the first year of practice. Not surprisingly, results stated that injuries were more common in fellows who did not receive proper ergonomical training and education. As a preventive measure, he states there is an urgent need for ergonomic training between young endoscopy practitioners[3].
In a systematic review Yung et al, included 13 studies evaluating prevalence, risk factors and mechanism of musculoskeletal pain and/or injuries related to GI endoscopy. Her review identified most common areas of pain in practicing endoscopy, as risk factors identified procedure volume, time spent doing endoscopy, cumulative time in practice and endoscopist age and concluded that there is a hazard among GI endoscopist for developing occupational injury. On the final note their expert commentary stated the need for further research to minimize the possibility of injury and a paradigm shift is needed in order to develop more comfortable and safe endoscopic devices[2].
American Society for Gastrointestinal Endoscopy (Walsh et al) approached the problem with a set of instructions and guidelines addressing key elements of ergonomics when exercising endoscopy and outlining common mistakes. Their approach offers that everyone should receive basic training in ergonomics, which is divided in cognitive, technical, and non-technical skills. Cognitive area covers the definition of ergonomics in endoscopy, most common signs and injuries related to endoscopy, protective equipment etc. Technical area includes knowledge of proper body posture and movement, room, and equipment organisation, different strategies of handling the procedure and thereby minimizing muscle overload on the body and hands. Non-technical part serves to time management, planning of the procedures, awareness to occupational health hazard etc. Also, the basic layout of the endoscopy room, physician position and movement is provided[7]. However, even by strict following of these principles, injuries still happen, mostly due to high volume of procedures[2,7] and bad endoscope design[1].
Siau and Anderson provided an interesting comparison between athletes and endoscopists[6]. In general endoscopy is very similar to certain sports e.g., archery. Like endoscopists, archers require a stable core and correct placement of the feet, hip, spine, and neck to provide proper posture and balance. In sports it is general practice to exercise proper training from the beginning to prevent wrong technique and consequently injuries. In the field of endoscopy, a structured approach to training is insufficient. In their article, the authors provide a reasonable parallel that endoscopist should be treated in a similar way as professional athletes[11], key points being proper training, cooperation with manufacturers of endoscopic materials, rehabilitation programs and education. Introducing a structured approach would decrease the possibility of musculo-skeletal injuries and would provide a safe procedure for the patient and endoscopist.
Shergill and McQuaid addressed the ergonomical challenge in a similar fashion as above listed authors. However, a term »Hierarchy of controls« was introduced as a recommendation from Occupational Health and Safety Administration[18]. A figure in a form of upside-down pyramid, illustrates the most and least effective methods for controlling exposures and mitigating the risk of work-related injury. Most effective being elimination and substitution meaning preventing injuries through scope design and collaborating with endoscope companies. Followed by engineering controls, which would result in endoscopy unit outline and endoscope assist measures (support stands, caps, dial assist etc.). In fourth place there are administrative controls consisting of endoscopy training, ergonomics “time out”, endoscopy schedule and endoscope maintenance. Personal protective equipment being described as least effective include endoscopist technique, microbreaks and stretches and maintaining physical fitness[19]. A clear statement can be deduced from the article: “ If you have an endoscopy related injury, it’s not your fault.”[8] Urge to include the endoscopist in the endoscope design process by companies is strongly advocated, as well as holistic approach to resolve the ergonomic crisis.
3. General Problem of the Endoscope Layout
“The current endoscope design lacks a consideration of human factors, and due to the high risk of injury, represents a failure of an engineered system. [1]” The development of the first endoscopic ideas reaches back to the early 1900s where new discoveries regarding light transformation made an introduction for further discoveries[20,21]. The modern endoscope as known today, was designed in the 1980s and it stayed basically the same until today. It applies the principle “one size fits all” disregarding differences between different size people, sex, physical abilities. Endoscope handle is held and manoeuvred with the physicians left hand, the shaft is held and manoeuvred with the right hand. To tackle the ergonomic problem from the technical point of view, first solution that is obvious is to redesign the endoscope handle or the whole concept. All the major endoscopic companies are manufacturing endoscopes with the same unanimous layout and size. People come in different sizes, sexes, and abilities, ergo the need for different sizes of endoscopes is present. However, progress and development in this area is insufficient due to various reasons (economic, organisational, etc.). A statement from A.K. Shergill perfectly describes the cause of endoscopy related injuries: “An endoscopist receives an injury not because they are weak or poorly trained, but because the endoscope was poorly designed[8].”
3.1. Robotics
When talking about ergonomic challenges in GI endoscopy, robotics offers many solutions and possibilities[22,23]. One could argue that robotics is a unique and special area in GI endoscopy, nevertheless, its applicability offers ergonomical improvements to the endoscopist. Visconti et al [24] divides the area of robotics in GI endoscopy in two basic principles: those developed to improve forceps handling and stability and those with active movement. Furthermore, a more detailed stratification can be made in three following directions:
- Platforms capable of high degrees of freedom on forceps manipulation for ESD (endoscopic submucosal dissection) and NOTES (natural orifice transluminal endoscopic surgery).
- Active introduction of the endoscopes to reduce the influence of the operator ability and to reduce the discomfort and pain referred by the patients.
- Endoscopic capsule evolution to use it as screening for GI pathologies and as a therapeutic method[24].
Looking from the perspective of ergonomic change, platforms capable of high degrees of freedom on forceps manipulation for ESD and NOTES demand two people manipulation. In each platform with high degrees of freedom on forceps manipulation for ESD and NOTES there are slight variations, however, this layout totally changes the approach in therapeutic endoscopy, ergonomically and organisationally. It unburdens the endoscopist from the classical stance and has practically no resemblance to the GI endoscopy performed with standard endoscopes. The approach demands two people manipulation. First physician manipulates the robot usually in seating position, and the second physician manipulates the endoscope (Figure 2).
Pioneer platforms with high degrees of freedom on forceps manipulation are MASTER platform (developed by the Nanyang Technological University and the National University of Singapore), STRAS/Anubiscope (Developed by the Research Institute against Digestive Cancer (IRCAD) with Karl-Storz), Endo- Samurai ( Developed by Olympus Medical Systems)[24]. However, its applicability in everyday practice is limited due to high cost, complexity, long learning curve. Nevertheless, the concept offers an idea worth pursuing tackling the ergonomic issue.
Systems which are designed for active introduction of the endoscope incorporate devices which propel or introduce the endoscope mechanically. This can be achieved with mechanisms that are attached to the classical endoscope or the endoscope design is altered or redesigned. In his review article, Lim, divides flexible robotic systems in 4 categories: robot-assisted flexible endoscopy for manoeuvring, robotic flexible endoscopy with therapeutic functions, active flexible colonoscopy, and active capsule endoscope[25]. A summary of available robotic endoscopic systems is provided including the need for further development and clinical applicability.
Li and Chiu provide a stratification of the field in a similar fashion: first category is robot-assisted rigid endoscopy for minimally invasive surgery, i.e., the rigid endoscope is held and manipulated by a robot arm. The second category is robot assisted flexible endoscopy for GI tract inspection, i.e., the flexible endoscope is held and manipulated by a robotic device. The third category is active GI endoscopy, which includes active flexible colonoscopy and active capsule endoscopy[26]. A clear trend of introducing robotics in everyday practice is outlined, offering solutions in technical and ergonomics area.
In most recent publication on Robotics in Gastrointestinal endoscopy by Kim et al, a similar approach is used. However, certain robotic projects from the previous articles were discontinued, the latest robotic systems were divided in three following categories: first category are robot-assisted therapeutic devices that assist advanced endoscopic procedures. This category includes robotic endoscopic multitasking platforms and robotic add-on devices. The second category is the robot-assisted colonoscopy system. A robotic-driven colonoscope that automatically navigates in the colon and an auxiliary device that assists the conventional colonoscope. The last category is robotic capsule endoscopy. In Table 2 and Table 3 outlined by Kim et al, a summary of the latest robotic platforms and robot-assisted systems are presented.
The idea of capsule endoscopy changes the approach to endoscopy in comparison to conventional or robotic endoscopy. The process of capsule endoscopy eliminates before outlined musculo-skeletal injuries connected to repetitive strain injuries. However, currently available endoscopic capsules lack the possibility of therapeutic interventions and serve mainly as a diagnostic tool[28].
An almost unanimous division of the robotics area is provided by all abovementioned authors. Their work mainly focuses on technical issues with subtle insinuation to change the endoscope design and layout and therefore also addressing ergonomical challenge. All above mentioned robotic systems are a novelty in GI endoscopy. One might argue that solutions are sought only in colonoscopy[29,30]. However most occupational injuries in GI endoscopy arise from repetitive actions with high force manoeuvres[1,12]. From ergonomical standpoint systems presented practically eliminate repetitive strain injuries due to their robotic - joystick properties. The downside is high cost of equipment, its uniqueness and applicability in everyday practice. If one is to imagine the number of endoscopy units in the world and the number of procedures done daily, implementing a system with disposable colonoscopes with robotic guidance system poses an incomprehensible challenge.
The redesign of the endoscope is a crucial step in achieving better ergonomical conditions for endoscopists. However, an easier way is to implement robotic assistance on to the existing traditional endoscope. In his review, Kim et al, presents solutions using add on platforms and master- slave concept to the conventional endoscopes. It is a lot easier and convectional to combine robotic assistance, however the limitations in comparison with robotic platforms are greater. Used add-on usually are less capable of triangulation of instruments and tissue manipulation compared to the robotic endoscopic multitasking platform. Their exchangeability, possibility of sterilization and low cost offer an interesting approach in preventing musculoskeletal injuries[27].
3.2. “Hands-Free” Endoscopy
As conceptualized by Dr. Binmoeller in 2004, The ScopeDoc was the first device of its kind designed for “hands-free” endoscopy to reduce stress and fatigue from flexible endoscopy. The fatigue and stress result from having to carry the sheer weight of the endoscope and having to steer the endoscope with the hands. The ScopeDoc transfers the weight of the endoscope from the hand to the body. Subtle changes in body position are transferred to the endoscope shaft and the endoscope tip, enabling the endoscopist to steer the endoscope with the body rather than the hands. The concept of the device was developed further, clinical trials with EMG of specific muscles of the left and right arm, torso and back are in progress[31,32,33]. First results are confirming tension relief in left trapezoid and biceps muscles and significant increase of microbreaks in the muscles when using the holder. This combination offers an alternative solution to robotics. Its simplistic design and idea allow widespread use. On the downside, it offers solution only for the left arm and body posture, while the right arm still operates with conventional movements[31].
3.3. Personal Care Strategies—Floor Mat and Cushioned Insoles
Prolonged standing on a hard surface is a known trigger for discomfort, resulting in suboptimal performance, leg pain etc. In their research Wiggerman and Keyserling demonstrated the positive effect of cushioned floor mats and their effect on discomfort relief and better work performance[34]. Their use in endoscopy can be beneficial to all endoscopists, despite not being a “true” endoscopic accessorize connected to the endoscope redesign or function[35]. Standing in cushioned insoles suggest to create subtle muscular movement, reducing musculoskeletal pain, improving blood flow and decreasing discomfort and fatigue[36]. The fundamental principle behind using anti-fatigue mats and insoles is to provide a supportive interface between the floor and the feet and to optimize body weight distribution[37]. When performing endoscopy, the body posture is predominantly in the upright standing position, hence the use of cushioned insoles proves itself useful in prevention of musculoskeletal injuries during endoscopy.
4. Discussion and Conclusions
Ergonomics in GI endoscopy plays an important role in occupational injury prevention. Due to a higher volume of procedures, the problem with musculo-skeletal injuries is becoming bigger and everyday more present among fellow gastroenterologists. A detailed set of recommendations addressing the ergonomical challenges with the intent of minimizing the possibility of occupational injury was issued by American Society for Gastrointestinal Endoscopy (ASGE). It is our opinion that every young GI fellow should get a basic training in occupational injury prevention[38,39]. We believe that recommendations provided, start the process of prevention by implementing active thinking about the problem from the start. This will ensure for proper muscle memory to arise and to build long term habits that prevent occupational injury. As described in recommendations, there is no formal endoscopy-specific ergonomic assessment, thereby we also promote the idea of formative assessment and feedback to all young fellows. However, a lack of technical solutions in ASGE guidelines is present. A detailed set of recommendations is given on how to educate a trainee, without the possibility to implement technological accessorize that can help in injury prevention. Without a doubt, robotics will play a major role in tackling the ergonomical challenge in GI endoscopy. As everything, its applicability and widespread use is closely related to high financial and material cost. Many of the presented robotic solutions are still in experimental phase. Therefore, their use in everyday clinical setting is extremely limited. It is of great importance for all the manufacturers of endoscopic equipment, to comprehend the need for different sizes of endoscopes and maybe a totally different concept to endoscopic devices. Inclusion of endoscopists in the development process is crucial[40]. Nevertheless, progress in this area is slow. A “Hands-free endoscopy” concept with belt add-on offers an alternative approach. Promising results in releasing the tension in key muscles that affect our body posture and workload of upper limbs provide a step forward in addressing the ergonomical challenge. Concept of an endoscopic accessorize that prevents occupational injury is a novelty in this area and it offers a simplistic option in endoscopy related injuries. On the downside it offers partial solution only for body posture and left arm. Protective personal care strategies include floor mat and cushioned insoles use. They offer a widespread solution to the modern challenges of ergonomic issues in GI endoscopy. As not being a “true endoscopic accessorize” they perform a very important part in injury prevention. Comfortable position and cushioned floor in a prolonged standing situation play a crucial role in well-being and performance of an endoscopist. Presented preventive measures decrease the possibility of endoscopy related injury, however they do not eliminate it. Implementing all the strategies should be a priority to all parties involved to minimise the possibility of occupational injury and promote safe endoscopy.
Funding
This research was funded by Charles University Grant Agency( GAUK), grant number 412622.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data was formed.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Shergill AK, Harris Adamson C. Failure of an engineered system: The gastrointestinal endoscope. Tech Gastrointest Endosc. 2019 Jul 1;21(3):116–23.
- Yung DE, Banfi T, Ciuti G, Arezzo A, Dario P, Koulaouzidis A. Musculoskeletal injuries in gastrointestinal endoscopists: a systematic review. Expert Rev Gastroenterol Hepatol. 2017 Oct 3;11(10):939–47.
- Villa E, Attar B, Trick W, Kotwal V. Endoscopy-related musculoskeletal injuries in gastroenterology fellows. Endosc Int Open. 2019 Jun;07(06):E808–12.
- Austin K, Schoenberger H, Sesto M, Gaumnitz E, Teo Broman A, Saha S. Musculoskeletal Injuries Are Commonly Reported Among Gastroenterology Trainees: Results of a National Survey. Dig Dis Sci. 2019 Jun 1;64(6):1439–47.
- Shergill AK, McQuaid KR, Rempel D. Ergonomics and GI endoscopy. Gastrointest Endosc. 2009 Jul 1;70(1):145–53.
- Siau K, Anderson JT. Ergonomics in endoscopy: Should the endoscopist be considered and trained like an athlete? Endosc Int Open. 2019 Jun;07(6):E813–5.
- Walsh CM, Qayed E, Aihara H, Anand GS, Byrne K, Chahal P, et al. Core curriculum for ergonomics in endoscopy. Gastrointest Endosc. 2021 Jun 1;93(6):1222–7.
- Shergill AK, McQuaid KR. Ergonomic endoscopy: An oxymoron or realistic goal? Gastrointest Endosc. 2019 Dec;90(6):966–70.
- Chang MA, Mitchell J, Abbas Fehmi SM. Optimizing ergonomics during endoscopy. VideoGIE. 2017 Apr 10;2(7):170.
- Anderson JT. Optimizing ergonomics during endoscopy training. Tech Gastrointest Endosc. 2019 Jul 1;21(3):143–9.
- Singla M, Kwok RM, Deriban G, Young PE. Training the Endo-Athlete: An Update in Ergonomics in Endoscopy. Clin Gastroenterol Hepatol. 2018 Jul 1;16(7):1003–6.
- Ridtitid W, Coté GA, Leung W, Buschbacher R, Lynch S, Fogel EL, et al. Prevalence and risk factors for musculoskeletal injuries related to endoscopy. Gastrointest Endosc. 2015 Feb 1;81(2):294-302.e4.
- Harvin G. Review of Musculoskeletal Injuries and Prevention in the Endoscopy Practitioner. J Clin Gastroenterol. 2014 Aug;48(7):590–4.
- Han S, Hammad HT, Wagh MS. High prevalence of musculoskeletal symptoms and injuries in third space endoscopists: an international multicenter survey. Endosc Int Open. 2020 Oct;08(10):E1481–6.
- Kamani L, Kalwar H. Ergonomic Injuries in Endoscopists and Their Risk Factors. Clin Endosc. 2021 Mar 3;54(3):356–62.
- Shah SZ, Rehman ST, Khan A, Hussain MM, Ali M, Sarwar S, et al. Ergonomics of gastrointestinal endoscopies: Musculoskeletal injury among endoscopy physicians, nurses, and technicians. World J Gastrointest Endosc. 2022 Mar 16;14(3):142–52.
- Anderson J. Colonoscopy: do operator motions and posture count? Endosc Int Open. 2015 Dec;03(6):E627–8.
- Hierarchy of Controls | NIOSH | CDC [Internet]. 2023 [cited 2023 Jul 7]. Available from: https://www.cdc.gov/niosh/topics/hierarchy/default.html.
- Park AE, Zahiri HR, Hallbeck MS, Augenstein V, Sutton E, Yu D, et al. Intraoperative “Micro Breaks” With Targeted Stretching Enhance Surgeon Physical Function and Mental Focus. Ann Surg. 2017 Feb 1;265(2):340–6.
- Baillie J. The endoscope. Gastrointest Endosc. 2007 May 1;65(6):886–93.
- De Groen PC. History of the Endoscope [Scanning Our Past]. Proc IEEE. 2017 Oct;105(10):1987–95.
- Yeung BPM, Chiu PWY. Application of robotics in gastrointestinal endoscopy: A review. World J Gastroenterol. 2016 Feb 7;22(5):1811–25.
- Kume K, Sakai N, Goto T. Development of a novel endoscopic manipulation system: the Endoscopic Operation Robot ver.3. Endoscopy. 2015 Sep;47(09):815–9.
- Visconti TA de C, Otoch JP, Artifon EL de A. Robotic endoscopy. A review of the literature. Acta Cirúrgica Bras [Internet]. 2020 Apr 27 [cited 2022 Jul 11];35. Available from: http://www.scielo.br/j/acb/a/yJT7PtqMn85gC7VkKQHNysL/?format=html&stop=next&lang=en.
- Lim SG. The development of robotic flexible endoscopic platforms. Int J Gastrointest Interv. 2020 Jan 31;9:9–12.
- Li Z, Chiu PWY. Robotic Endoscopy. Visc Med. 2018;34(1):45–51.
- Kim SH, Choi HS, Keum B, Chun HJ. Robotics in Gastrointestinal Endoscopy. Appl Sci. 2021 Nov 30;11:11351.
- Bianchi F, Masaracchia A, Shojaei Barjuei E, Menciassi A, Arezzo A, Koulaouzidis A, et al. Localization strategies for robotic endoscopic capsules: a review. Expert Rev Med Devices. 2019 May 4;16(5):381–403.
- Pullens HJM, Stap N van der, Rozeboom ED, Schwartz MP, Heijden F van der, Oijen MGH van, et al. Colonoscopy with robotic steering and automated lumen centralization: a feasibility study in a colon model. Endoscopy. 2016 Mar;48(03):286–90.
- Kang M, Joe S, An T, Jang H, Kim B. A novel robotic colonoscopy system integrating feeding and steering mechanisms with self-propelled paddling locomotion: A pilot study. Mechatronics. 2021 Feb;73:102478.
- Duric T. Ergonometry in Endoscopic Procedures: Prevention of Musculoskeletal Injuries During Endoscopic Procedures by Using Belt-Like Manouvring Device with Joystick Capabilities. In: Endoscopy [Internet]. Georg Thieme Verlag KG; 2021 [cited 2023 Jan 8]. p. eP193. Available from: http://www.thieme-connect.de/DOI/DOI?10.1055/s-0041-1724689.
- Luttmann A, Jäger M, Laurig W. Electromyographical indication of muscular fatigue in occupational field studies. Int J Ind Ergon. 2000 Jul 1;25(6):645–60.
- Albayrak A, van Veelen MA, Prins JF, Snijders CJ, de Ridder H, Kazemier G. A newly designed ergonomic body support for surgeons. Surg Endosc. 2007 Oct 1;21(10):1835–40.
- Wiggermann N, Keyserling W. Effects of Anti-Fatigue Mats on Perceived Discomfort and Weight-Shifting During Prolonged Standing. Hum Factors. 2013 Aug 1;55:764–75.
- Noor SNAM, Ahmad IN, Wahab NA, Ma’arof MIN. A Review of Studies Concerning Prolonged Standing Working Posture. Adv Eng Forum. 2013;10:131–6.
- King PM. A comparison of the effects of floor mats and shoe in-soles on standing fatigue. Appl Ergon. 2002 Sep 1;33(5):477–84.
- Speed G, Harris K, Keegel T. The effect of cushioning materials on musculoskeletal discomfort and fatigue during prolonged standing at work: A systematic review. Appl Ergon. 2018 Jul 1;70:300–14.
- Korman LY. An ounce of prevention: ergonomic training in GI endoscopy. Gastrointest Endosc. 2020 Nov 1;92(5):1081–2.
- Singh S, Sedlack RE, Cook DA. Effects of Simulation-Based Training in Gastrointestinal Endoscopy: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2014 Oct 1;12(10):1611-1623.e4.
- Khanicheh A, Shergill AK. Endoscope design for the future. Tech Gastrointest Endosc. 2019 Jul 1;21(3):167–73.
Figure 2.
Layout of an endoscopic—robotic platform.
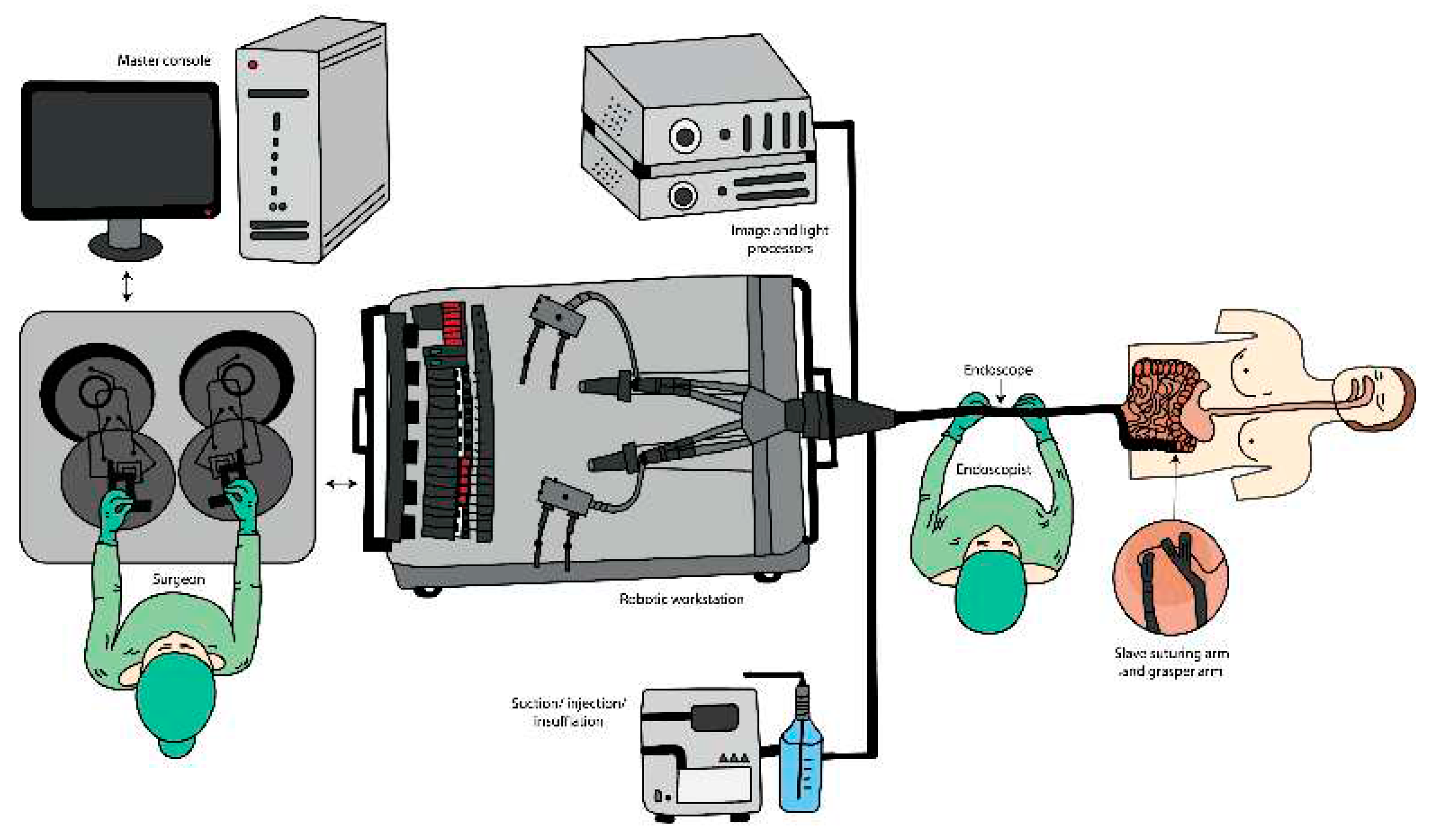
Figure 3.
The ScopeDoc (COOK Medical).


Table 1.
Summary of systematic reviews, surveys and cross-sectional cohort studies.
| Author | Year | Ref. No | Title | Methodology | Key argument |
|---|---|---|---|---|---|
| Harvin | 2014 | [13] | Review of Musculoskeletal Injuries and Prevention in the Endoscopy Practitioner | Systematic review | Strategies for the management of the risk of musculoskeletal injuries related to the practice of endoscopy include compliance with currently recommended ergonomic practices, education of trainees in ergonomic technique when practicing endoscopy, and research toward the modification and development of more ergonomic endoscopes and procedure spaces. |
| Ridtitid et al | 2015 | [12] | Prevalence and risk factors for musculoskeletal injuries related to endoscopy | Survey | Among endoscopists there is a high prevalence of injuries definitely or potentially related to endoscopy. Higher procedure volume, more time doing endoscopy per week, and cumulative years performing endoscopy are associated with more work-related injuries. |
| Yung et al | 2017 | [2] | Musculoskeletal injuries in gastrointestinal endoscopists: a systematic review | Systematic review | Comprehensive investigation into the prevalence, types, pathophysiology and methods to minimise endoscopy-related musculoskeletal injuries is vital to ensure the continued efficient provision of endoscopy services in the face of rising demands worldwide. A paradigm shift is required in endoscopic devices and techniques to improve safety and comfort. |
| Villa et al | 2019 | [3] | Endoscopy-related musculoskeletal injuries in gastroenterology fellows | Survey, cross-sectional study | Injuries were more common in fellows who did not receive proper ergonomical training and education |
| Austin et al | 2019 | [4] | Musculoskeletal Injuries Are Commonly Reported Among Gastroenterology Trainees: Results of a National Survey | Electronic survey | Musculoskeletal injuries may affect up to 20% of GI fellows. Female fellows more frequently report injuries and may be at particularly high risk which has not been found in previously reported surveys of practicing gastroenterologists. Standardized curricula on ergonomic considerations and injury prevention are needed to enhance GI fellowship training and reduce injury rates. |
| Han et al | 2020 | [14] | High prevalence of musculoskeletal symptoms and injuries in third space endoscopists: an international multicenter survey | International multicenter survey | Over two-thirds of endoscopists performing TSE suffer from MSI, with many reporting onset of their symptoms after starting TSE in their practice. Further studies are needed to understand and reduce the risk of MSI in TSE given the growing demand for these procedures and the potential long-term impact of this occupational hazard. |
| Lubna Kamani,Hamid Kalwar | 2021 | [15] | Ergonomic Injuries in Endoscopists and Their Risk Factors | Survey, cross-sectional study | Endoscopists are at high risk of developing ergonomic injuries, representing the negative potential of the endoscopyassociated workload. To overcome these issues, an appropriate strategic framework needs to be designed to avoid occupational compromises. |
| Shah et al | 2022 | [16] | Ergonomics of gastrointestinal endoscopies: Musculoskeletal injury among endoscopy physicians, nurses, and technicians | Observational cross-section study | Three-fourth of our endoscopists reported MSI, of which more than half are not sure or attributed this problem to endoscopy. The prevalence of MSI warrants urgent attention. |
Table 2.
Summary table of robotic endoscopic multitasking platforms[27].
Table 2.
Summary table of robotic endoscopic multitasking platforms[27].
| NAME | APPROVAL STATUS | CLINICAL TRIAL | PURPOSE OF USE | TECHNICAL FEATURES |
|---|---|---|---|---|
| ENDOMASTER EASE SYSTEM (ENDOMASTER PTE., SINGAPORE) | No | AnimalguifenHuman | Stomach ESDguifenColon ESD | Console for remote control of the robotic arms, Independent endoscopic platform |
| ENDOLUMINAL ASSISTANT FOR SURGICAL ENDOSCOPY guifen(ICUBE LABORATORY, STRASBOURG, FRANCE) | No | Animal | Colon ESD | Master console and a detachable flexible endoscope with three working channels |
| FLEX ROBOTIC SYSTEM (MEDROBOTICS, RAYNHAM, MA, USA) | FDA | AnimalguifenHuman | Colon ESD | Robotic endoscope, mechanical single-use flexible instruments and a master console with a touchscreen, HD visual display, a joystick |
| K-FLEX guifen(EASYENDO SURGICAL, DAEJEON, KOREA) | No | Explanted animal organs | Colon ESD | Bendable overtube, two exchangeable surgical instrument modules, a driving robot arm, and a master console |
Table 3.
Summary of the operating principles and technical features of the most recently developed robotic flexible colonoscopy systems[27].
Table 3.
Summary of the operating principles and technical features of the most recently developed robotic flexible colonoscopy systems[27].
| NAME | SINGLE USE | APPROVAL STATUS | ACTUATION PRINCIPLE | TECHNICAL FEATURES |
|---|---|---|---|---|
| THE AER-O-SCOPETM COLONOSCOPE SYSTEM guifen(GI VIEW LTD., TEL AVIV, ISRAEL) | Yes | FDA, CE | Electro – pneumatic mechanisms | Self-propelled, disposable colonoscope |
| ENDOTICS guifen(ERA ENDOSCOPY SRL, CASCINA, ITALY) | Yes | CE | Electro – pneumatic mechanisms | Self-propelled, joystick-controlled endoscope |
| COLONOSIGHT (STRYKER GI, HAIFA, ISRAEL) | Yes | FDA | Electro – pneumatic mechanisms | Self-advancing system composed of a reusable colonoscope and a wrapped disposable multi-lumen sheath |
| NEOGUIDE ENDOSCOPY SYSTEM guifen(INTUITIVE SURGICAL INC., SUNNYVALE, CA, USA) | Yes | FDA | Electro-mechanical actuation | 16-segment insertion tube that controls the snake-like movement of the endoscope |
| ENDOCULUS (UNIVERSITY OF COLORADO, BOULDER, CO, USA) | No | No | Electrically actuated mechanisms | Small tank-like robot that can navigate the colon |
| MAGNETIC FLEXIBLE ENDOSCOPE (VANDERBILT UNIVERSITY, NASHVILLE, TN, USA) | No | No | Magnetic-actuated tethered robotic colonoscopes | Magnet-embedded endoscope, an actuated permanent magnet external to the patient, and a control software |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



