
Submitted:
12 July 2023
Posted:
12 July 2023
You are already at the latest version
Abstract
The connection between marital status and suicidal behavior has been poorly assessed in South Asia. We aimed to see the proportion of marital status in individuals in suicidal behavior in South Asian countries. We followed PRISMA guidelines and registered the protocol in advance (PROSPERO 2023 CRD42023399906). A systematic search was conducted in Medline, Embase, and PsycINFO. Meta-analyses were performed to pool the proportion of married individuals with suicidal behavior (total, suicide, and suicide attempt) in South Asian countries. Our search identified 47 studies for this review from six countries published from 1999 to 2022 with a sample size ranging from 27 to 89178. The proportion of married individuals was 55.4% (95% CI 50.1-60.5) for suicidal behavior, 52.7% (95% CI 44.5 – 60.7) for suicides, and 43.1 (95% CI 32.9 – 53.9) for suicide attempts. The proportion of married persons among suicide attempts varied significantly across countries (p=0.016) which was highest (61.8%; 95% CI: 57.2 – 66.2) in India, followed by Bangladesh (52.5%; 95% CI 41.8% - 62.9%) and Pakistan (45.1%; 95% CI 30.9 – 59.9). As the current study did not assess any cause-and-effect association, a cautious interpretation is warranted while considering married marital status as a risk factor.
Keywords:
suicidal behavior
; South Asia
; married
; suicide
; suicide attempt
1. Introduction
Suicide having a linkage with human and socioeconomic losses is considered a serious public health issue. Worldwide, each year around 700,000 people lose their life by suicide (1). More than three-quarters of this loss is occurring in low- and middle-income countries (LMICs) (1), indicating the necessity of urgent attention to decrease suicidal behavior.
Suicide is the end product of a network of interactions among multiple risk factors (2). Despite mental health being one of the major risk factors for suicide, a systematic review found that psychiatric disorders had a similar population-attributable risk for suicide in terms of socioeconomic factors (3), warranting the significance of social factors for improving population health and reducing the burden of suicide. Moreover, the odds of suicide are higher during periods of socioeconomic, family, or individual crisis (2).
Among socioeconomic factors, marital status is linked with social and community integration (4), and in turn is associated with social isolation and its further consequences including suicidal behavior (5). While marriage could enhance social integration and regulation leading to chances of reducing suicidal risk, divorce, on the other hand, could increase suicide risk by breaking the marriage and relationships between the individual (4). There are several studies that have examined to demonstrate that marital status is a significant factor in suicide and have found that single people are significantly more likely to die by suicide than married people (6–12). Similarly, cultural and geographical factors are also related to developing suicidal behavior. For example, marriage acting as a protective factor is subject to culture-specific (7). Likewise, the sociocultural and economic contexts of Asian nations differ from Western nations when it comes to suicide (13–16).
A small number of studies have examined the connection between marital status and suicidal behavior in South Asia, a region with a high rate of suicide. South Asia (Afghanistan, Bangladesh, Bhutan, India, Maldives, Nepal, Pakistan, and Sri Lanka) is home to one-fifth of all mental health cases and accounts for approximately 25% of the global population (17). As there is scattered evidence on suicide and marital studies in South Asian countries, we attempt to conduct a systematic review by looking at published (i.e., peer-reviewed) studies conducted in South Asian countries. As a result, we aimed to assess the proportion of marital status of individuals in suicidal behavior in South Asian countries.
2. Materials and Methods
2.1. Search Strategy
We made a systematic search in three databases (Medline, Embase, and PsycINFO) by predesigned search terms to identify available papers. We also performed hand search in previously published reviews (17–19). The search details are mention in Supplementary File S1 and the review protocol was registered in advance (PROSPERO 2023 CRD42023399906). We searched the data bases from inception to search date (February 04, 2023).
2.2. Inclusion Criteria
We included original research contributions, studies with quantitative estimates, published in the English language, and articles available in full-text were included. The population included in this review was restricted to studies in South Asian countries (Afghanistan, Bangladesh, Bhutan, India, Maldives, Nepal, Pakistan and Sri Lanka) in humans. Only studies mentioning marital status of persons with suicidal behavior i.e. suicide, suicide attempt, or both (fatal and/or non-fatal suicide attempts irrespective suicidal intent) were included.
2.3. Exclusion Criteria
We excluded articles discussing the effects among veterans, and articles with only qualitative outcomes. We also excluded any type of review, editorial, erratum, letters without primary data, and multiple articles from same projects. In such cases, we included the paper providing the data in maximum extent regarding marital status and suicidal behavior was included.
2.4. Study Selection
The studies were independently screened by two review authors (SMYA, VM) and a third review author (RK) was consulted when needed. We followed PRISMA flow chart and mentioned the stepwise details of the search in Supplementary File S2.
2.5. Data Extraction
We extracted the study details (name of the lead author, year of publication, name of the journal), country where the study was conducted, place where the study was conducted, instruments measuring suicidal behavior, duration of the study, data collection year, study design, data collection methods, study setting (rural/ urban), sample size, male-female ratio (when applicable), type of suicidal behavior (attempt/suicide/both), and marital status. We considered the marital status in two groups (married and others [never married/unmarried, separated, widow/widower]). Data were extracted by two review authors (DB & KM) independently in Microsoft Excel version 10 and a third review author was involved (RS) when necessary and checking.
2.6. Quality Assessment
Among the included articles, the cross-sectional studies’ methodological quality as assessed by using Newcastle Ottawa Scale (NOS) that was adapted for the cross-sectional studies (20). The methodological quality of the case control studies was assessed by using Newcastle Ottawa Quality Assessment Scale for case control studies (21). Two authors (MH and SMYA) independently assessed the risk of bias of included studies. For cross-sectional studies, the NOS scale is assessed on three domains: (1) sample selection, (2) comparability of the different outcome groups, and (3) outcome assessments and statistical analysis. While for case control studies, (1) selection of cases and controls, (2) comparability, and (3) exposure domains were assessed for methodological quality. In both scales, the total score was summed up and evaluated as low risk of bias (7 and above), moderate risk of bias (4 to 6) and high risk of bias (3 and below).
2.7. Data Analysis
RStudio (version 2023.06.0+421) and statistical package meta were used for meta-analysis. The proportion of married individuals (with 95% Confidence Interval [CI]) in total suicidal behavior, suicide attempts and suicide was pooled using both fixed and random effects models. The heterogeneity among studies was explored using both the Cochran’s Q and the I2 statistic. Subgroup analysis was carried out across type of suicidal behavior (fatal and non-fatal), country (i.e., Bangladesh, India, and Pakistan), and study quality (low, moderate, and high). Groups with less than three studies were omitted from the sub-group analysis to avoid distorted and non-generalizable estimates. The random effect estimates were used because of high heterogeneity among studies. A prediction interval was also estimated to provide a range of expected prevalence of married individuals among suicide cases. Publication bias was not assessed as the assumption that positive results are preferentially published is not necessarily true for proportional studies (22).
3. Results
3.1. Characteristics of Included Studies
Our search identified 47 studies for this review from six countries (Bangladesh [8], India [27], Nepal [1], Pakistan [9], and Sri Lanka [2] (Table 1). We did not find any studies from Bhutan and the Maldives. Studies were published between 1999 and 2022 (Table 1). Suicide was the outcome variable in 30 studies, suicide attempt was found in 8 studies, and the rest of the studies include suicidal behavior (suicide and suicide attempt). Sample size ranges from 27 to 89178. 23 studies were conducted in urban settings, 7 were in rural areas and the 17 studies had mixed samples from both urban and rural areas. Data were collected by interview in 32 studies and different records were reviewed in the rest studies.
3.2. Study Quality Assessment
As per modified Newcastle Ottawa Quality assessment scales for cross-sectional study and case-control study, six studies (n=6, 12.76%) had high quality, thirty-six studies (n=36, 76.60%) had moderate quality, and five studies (n=5, 10.64%) had poor quality. Among 38 cross-sectional studies, (1) the majority of the included studies’ (34/38, 90%) sample were selected by non-random sampling methods, 7/38 (18%) studies used validated questionnaire tools, while 27/38 (71%) studies described the questionnaire tool although the validation was not clearly mentioned. Regarding the comparability of the different outcome groups, only 3/38 (8%) studies controlled for the important confounding factors. In the outcome assessments and statistical analysis domain, 22/38 (58%) studies collected self-reported data, while the other studies used independent blind assessment and record linkage. 32/38 (84%) studies clearly described the statistical tests (Supplementary file S3, Appendix Table 1). Among the included 9 case-control studies, all the studies (9/9, 100%) clearly mention and applied the valid method for the selection of case, 8/9 (89%) studies selected community control, 7/9 (78%) studies controlled for the confounders. While the exposure was measured by semi-structured interviews or psychological autopsy in all the studies (9/9, 100%) (Supplementary File S3, Appendix Table 2).
3.3. Marital Status in Suicidal Behavior
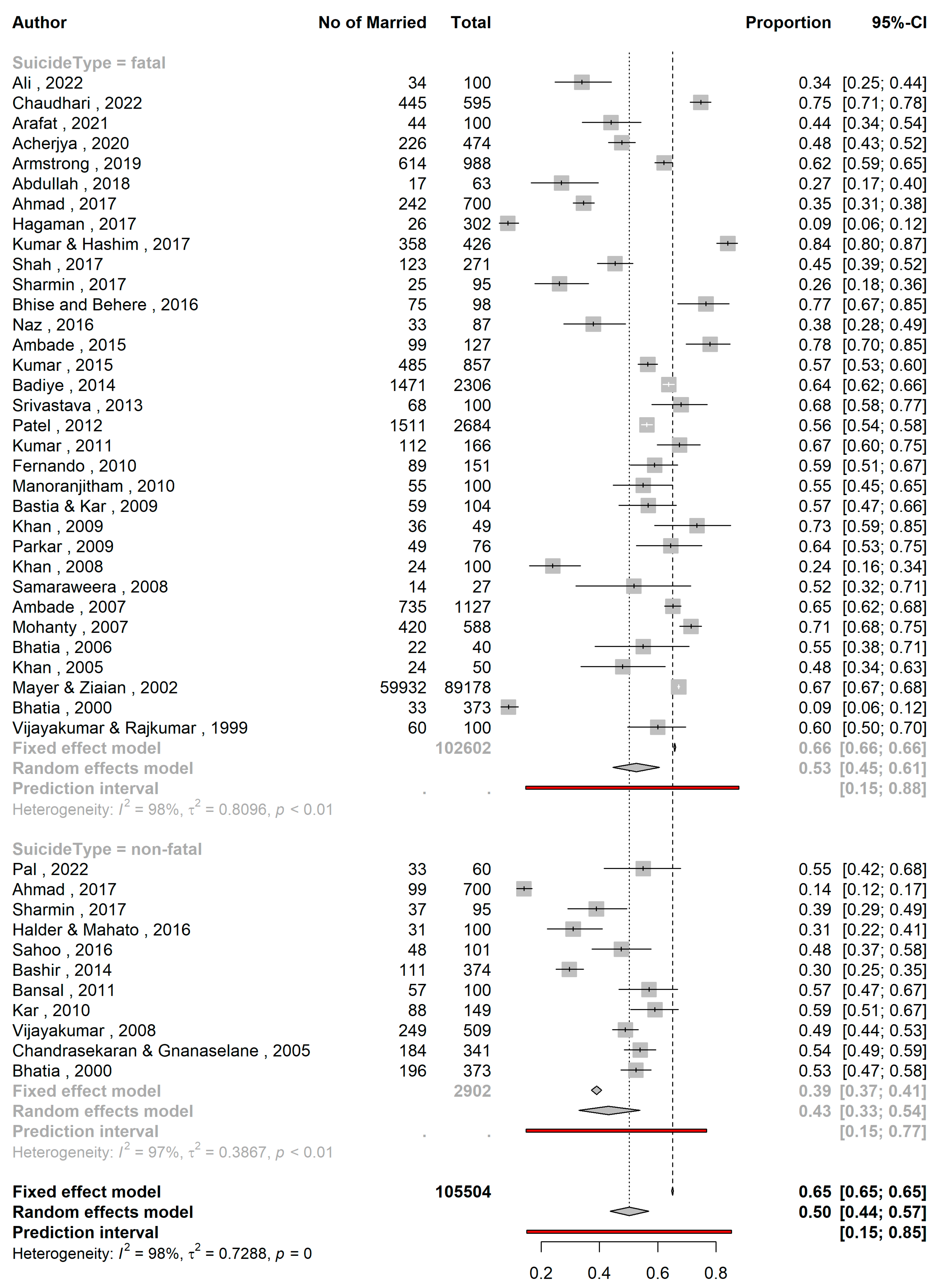
The proportion of married individuals among persons with suicidal behavior was 55.4% (95% CI 50.1-60.5; 47 studies; n=105585; I2= 96.9%, Figure 1). The prediction interval of proportions ranged from 23.2-83.6%. The studies by Sadia et al. (61), Arafat et al. (29), Arafat et al. (30), Arafat et al. (31), Saaiq & Ashraf (63) and Reza et al. (60) reported both fatal and non-fatal suicidal behavior but did not specify how many subjects had fatal and non-fatal behaviors. On the other hand, the studies by Ahmed et al. (25), Sharmin Salam et al. (66) and Bhatia et al (39) also reported both types of behaviors and specified their numbers. Hence, for subgroup analysis, between fatal and non-fatal suicide behavior the former six studies were excluded and the latter three studies were divided into two parts (fatal & non-fatal). The subgroup analysis (Figure 2) revealed that among proportion of married individuals was 52.7% (95% CI 44.6–60.7; 33 studies; n=102602; I2=97.8%) in suicides and 43.1 (95% CI 32.9 – 53.9; 11 studies; n=2902; I2=96.6%) in non-fatal attempts. The prediction intervals were 14.7–87.8% and 14.8–76.8%, respectively. However, the difference was not significant (p=0.128) (Table 2).
3.4. Country-wise Variation
The proportion of married persons among attempted suicide cases varied significantly across countries (p=0.016, Table 2). Studies in India found the highest proportion (61.8%; 95% CI: 57.2 – 66.2; n=101443; I2= 94.6%) followed by Bangladesh (52.5%; 95% CI 41.8-62.9%; n=2013; I2=89.0%) and Pakistan (45.1%; 95% CI 30.9–59.9; n=1649; I2=93.2%). Prediction interval were 38.6– 80.6% for India, 23.5– 79.9% for Bangladesh and 11.1–84.3% for Pakistan (Figure 3).
The pooled proportions did not differ significantly in relation to quality of the studies (p=0.63, Table 2). The proportion estimates were 54.4% (95% CI 38.3–69.7; 5 studies; n= 1133; I2=83.5%) for low quality studies, 56.4% (95% CI 50.1– 62.5; 36 studies; n=100899; I2=96.9%) for medium quality studies and 50.1% (95% CI 35.4–64.8; 6 studies; n=3553; I2= 91.4%) for high quality studies. The prediction intervals were 18.2-86.3%, 22.3-85.3%, and 15.9– 84.2% respectively (Figure 4).
Figure 3.
A forest plot showing proportion of married individuals with suicidal behavior across countries.
Figure 3.
A forest plot showing proportion of married individuals with suicidal behavior across countries.
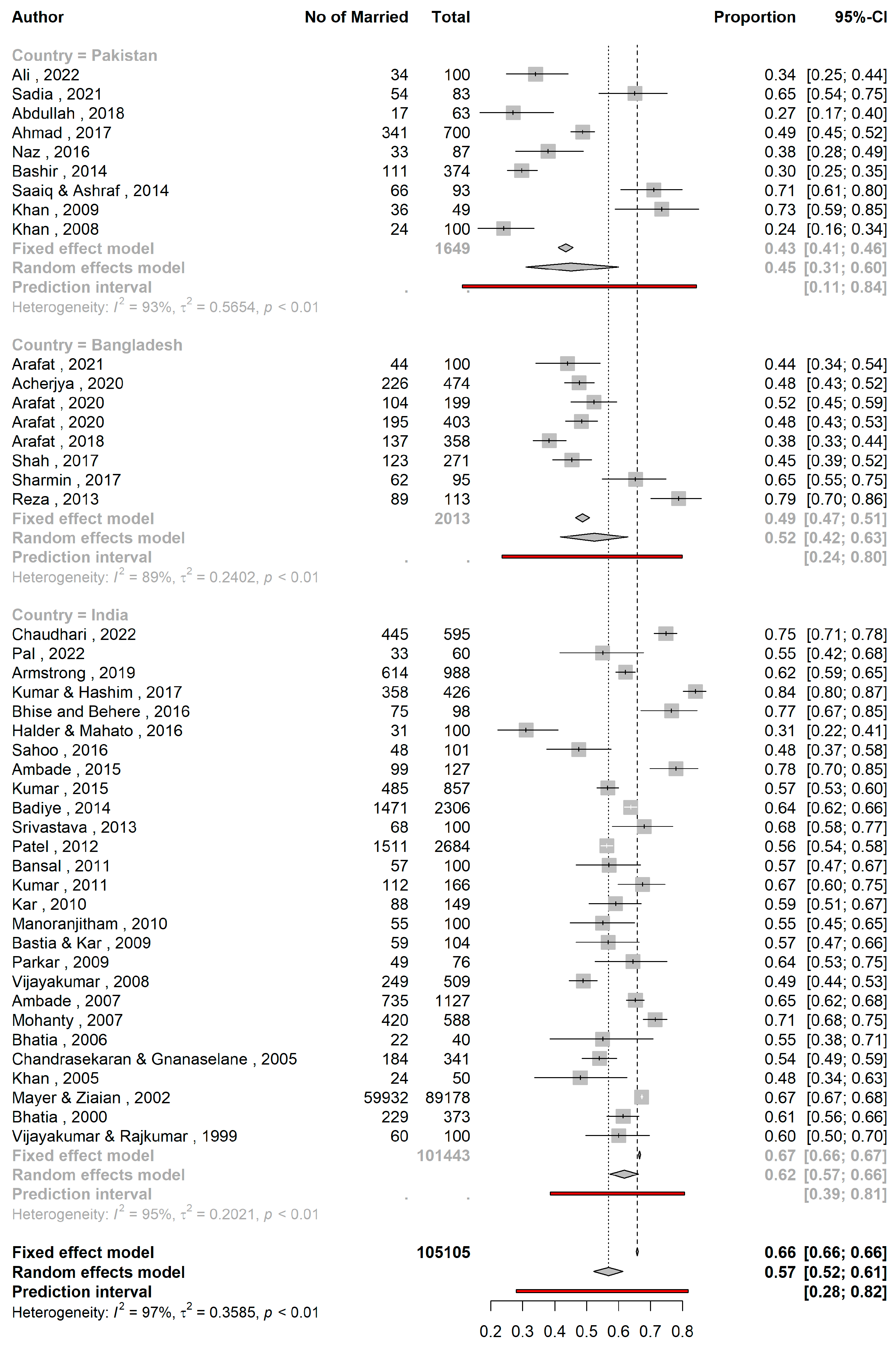
Figure 4.
A forest plot showing the proportion of married individuals with suicidal behavior stratified by study quality.
Figure 4.
A forest plot showing the proportion of married individuals with suicidal behavior stratified by study quality.
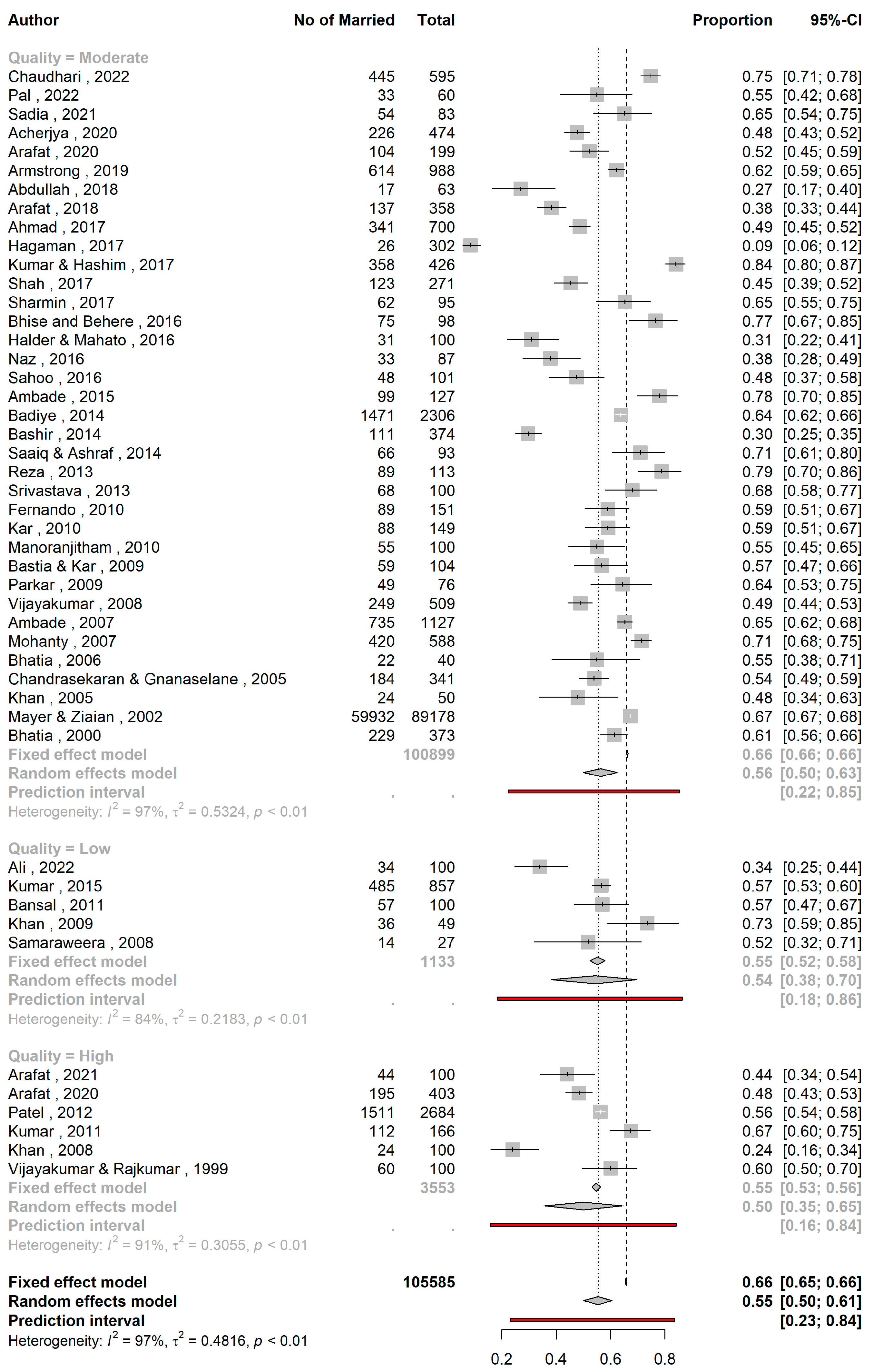

Table 1.
Distribution of studies (n=47).
| SN | Study | Country | Place of study | Study duration (month) | Data collection year | Data Collection Methods | Study setting | Sources of cases | Suicidal behavior | Method | Number of cases | Male | Female | Age of respondents (Years) Mean (SD) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Abdullah et al., 2018 (23) | Pakistan | Khyber Pakhtunkhwa | 8 | 2015 | psychological autopsy interviews | urban | hospital | fatal | mixed | 63 | 38 | 25 | 22.10+3.08 |
| 2 | Acherjya et al., 2020 (24) | Bangladesh | Jashore | 6 | 2018 | interview | urban | hospital | fatal | poisoning | 474 | 223 | 251 | 27±11 |
| 3 | Ahmad et al., 2017 (25) | Pakistan | Karachi | 60 | 2011-2015 | record review and interviews | urban | police records and poison centre | both | mixed | 700 | 450 | 250 | 28.19± 8.79 in male, 26.07±8.25 years in female |
| 4 | Ali et al., 2022 (26) | Pakistan | Punjab | 48 | 2018-2021 | interview | Urban | Community | fatal | mixed | 100 | 60 | 40 | 26 |
| 5 | Ambade et al., 2007 (27) | India | Maharashtra | 36 | 1998-2000 | record review | urban | mortuary data and police records | fatal | mixed | 1127 | 704 | 423 | |
| 6 | Ambade et al., 2015 (28) | India | Maharashtra | 60 | 2001-2005 | record review | rural | police and autopsy records | fatal | hanging | 127 | 107 | 20 | 10-80 years |
| 7 | Arafat et al., 2020 (29) | Bangladesh | 12 | 2018-2019 | reviewing online news reports | both | community | both | mixed | 199 | 94 | 105 | 26.86±13.60 | |
| 8 | Arafat et al., 2020 (30) | Bangladesh | 12 | 2018-2019 | reviewing of print news reports | both | community | both | mixed | 403 | 179 | 224 | 25.81±11.62 | |
| 9 | Arafat et al., 2021 (31) | Bangladesh | Dhaka | 13 | 2019-2020 | interviews | urban | community | fatal | mixed | 100 | 49 | 51 | 26.30 ±12.36 |
| 10 | Arafat et al., 2018 (32) | Bangladesh | 120 | 2009-2018 | reviewing online news content | both | community | both | mixed | 358 | 142 | 215 | 23.84±11.42 | |
| 11 | Armstrong et al., 2019 (33) | India | Tamil nadu | 7 | 2016 | reviewing print news papers | both | Community | fatal | mixed | 988 | 467 | 521 | |
| 12 | Badiye et al., 2014 (34) | India | Maharastra | 60 | 2009-2013 | record review | urban | Records from crime branch | fatal | mixed | 2306 | 1647 | 659 | |
| 13 | Bansal et al., 2011 (35) | India | Punjab | 12 | 2010 | interview | urban | hospital | non-fatal | mixed | 100 | 61 | 39 | 26.98 ±8.13 |
| 14 | Bashir et al., 2014 (36) | Pakistan | Karachi | 6 | interview | urban | hospital | non-fatal | poisoning | 374 | 230 | 144 | 25 ±10.1 | |
| 15 | Bastia & Kar, 2009 (37) | India | Cuttack | 24 | 1998-1999 | interview and record review | urban | Community | fatal | hanging | 104 | 43 | 61 | 28.7 ±11.4 |
| 16 | Bhatia et al., 2006 (38) | India | Delhi | 60 | reviewing suicide notes and interviews | urban | Forensic data | fatal | mixed | 40 | 26 | 14 | ||
| 17 | Bhatia et al., 2000 (39) | India | Delhi | record review, interviews | urban | hospital | Both | mixed | 373 | 189 | 184 | |||
| 18 | Bhise and Behere, 2016 (40) | India | Maharashtra | 18 | 2008-2009 | interview | rural | community people | fatal | mixed | 98 | 88 | 10 | |
| 19 | Chandrasekaran & Gnanaselane, 2005 (41) | India | Puducherry | 12 | 2001-2002 | interview | mixed | hospital | non-fatal | mixed | 341 | 153 | 188 | 26.1±9.3 |
| 20 | Chaudhari et al., 2022 (42) | India | Puducherry | 60 | 2010-2014 | record review | both | Forensic records | fatal | poisoning | 595 | 363 | 232 | 35.8 +14.6 |
| 21 | Fernando et al., 2010 (43) | Sri Lanka | Colombo | 12 | 2006 | interview | urban | court records | fatal | mixed | 151 | 93 | 58 | |
| 22 | Hagaman et al., 2017 (44) | Nepal | Nepal | 4 | 2015-2016 | interview and reviewing police records | both | community | fatal | mixed | 302 | 172 | 130 | 32.9+17.55 |
| 23 | Halder & Mahato, 2016 (45) | India | Kolkata | 24 | 2013-2014 | interview | urban | hospital | non-fatal | mixed | 100 | 28 | 72 | 23.51 ± 6.38 |
| 24 | Kar, 2010 (46) | India | Orissa | 24 | 1994-1996 | interview | urban | hospital | non-fatal | mixed | 149 | 65 | 84 | 31.6 ±13.5 years |
| 25 | Khan et al., 2005 (47) | India | Secunderabad | 1 | 2005 | interview | both | hospital | fatal | mixed | 50 | 29 | 21 | |
| 26 | Khan et al., 2008 (48) | Pakistan | Karachi | 12 | 2003 | interview, psychological autopsy method | urban | community people | fatal | mixed | 100 | 83 | 17 | |
| 27 | Khan et al., 2009 (49) | Pakistan | Ghizer | 48 | 2000-2004 | Police records and Interview | Urban | Police records | fatal | mixed | 49 | 49 | ||
| 28 | Kumar et al., 2015 (50) | India | Lucknow | 60 | 2008-2012 | record review | both | hospital | fatal | burning | 857 | 66 | 791 | 33.74 ± 11.64 |
| 29 | Kumar & Hashim, 2017 (51) | India | Karnataka | 36 | 2013 - 2015 | record review | rural | hospital | fatal | mixed | 426 | 355 | 71 | 34.7 |
| 30 | Kumar et al., 2011 (52) | India | Kerala | 6 | 2004 | Interview | rural | community | fatal | mixed | 166 | 124 | 42 | 40.45+17.07 |
| 31 | Manoranjitham et al., 2010 (53) | India | Tamil Nadu | 20 | 2006-2008 | psychological autopsy interview | rural | community | fatal | mixed | 100 | 59 | 41 | 42.24 ±20.69 |
| 32 | Mayer & Ziaian, 2002 (54) | India | 1995 | record review | both | community sample | fatal | mixed | 89178 | 52357 | 36821 | |||
| 33 | Mohanty et al., 2007 (55) | India | Berhampur | 48 | 2000-2003 | record review, interviews | both | hospital | fatal | mixed | 588 | 300 | 288 | |
| 34 | Naz, 2016 (56) | Pakistan | Punjab | 10 | 2014-2015 | reviewing newspaper content | both | community people | fatal | mixed | 87 | 50 | 37 | |
| 35 | Pal et al., 2022 (57) | India | Madhya Pradesh | 12 | 2020-2021 | interview | Urban | hospital | non fatal | mixed | 60 | 38 | 22 | 39.03±11.58 |
| 36 | Parkar et al., 2009 (58) | India | Mumbai | 84 | 1997-2003 | Interview | urban slums | community people | fatal | mixed | 76 | 33 | 43 | |
| 37 | Patel et al., 2012 (59) | India | 36 | 2001-2003 | Interview | both | community sample | fatal | mixed | 2684 | 1393 | 964 | ||
| 38 | Reza et al., 2013 (60) | Bangladesh | 24 | interview | rural | hospital | both | mixed | 113 | 44 | 69 | 29.6±12.8 | ||
| 39 | Sadia et al., 2021 (61) | Pakistan | Sargodha | 12 | 2019 | record review | both | hospital | both | wheatbill (aluminium phosphide) | 83 | 42 | 41 | |
| 40 | Sahoo et al., 2016 (62) | India | Jamshedpur | 6 | 2013–2014 | interview | both | hospital | non-fatal | mixed | 101 | 42 | 59 | |
| 41 | Saaiq & Ashraf, 2014 (63) | Pakistan | Islamabad | 24 | 2010 - 2012 | interviews and record review | both | hospital | both | burning | 93 | 18 | 75 | 26.89±6.1 |
| 42 | Samaraweera et al., 2008 (64) | Sri Lanka | Ratnapura | 3 | interviews, psychological autopsy | urban | community people | fatal | mixed | 27 | 19 | 8 | 43 | |
| 43 | Shah et al., 2017 (65) | Bangladesh | 6 | 2016-2017 | reviewing print news reports | both | community | fatal | mixed | 271 | 113 | 158 | 26.67 ± 13.47 | |
| 44 | Sharmin Salam et al., 2017 (66) | Bangladesh | 4 sub-districts | 6 | 2013 | interview | rural | Community | both | mixed | 95 | 48 | 47 | |
| 45 | Srivastava, 2013 (67) | India | Goa | 36 | 2005-2007 | record review and interviews | urban | community | fatal | mixed | 100 | 70 | 30 | |
| 46 | Vijayakumar & Rajkumar, 1999 (68) | India | Chennai | 14 | 1994-1995 | interviews, and record review | urban | community | fatal | mixed | 100 | 55 | 45 | |
| 47 | Vijayakumar et al., 2008 (69) | India | Chennai | 23 | 2002-2003 | Interview | urban | hospital | non fatal | 509 | 244 | 265 | 25.85±9.28 |
Table 2.
Statistical comparison of pooled proportions of married individuals with suicidal behavior across different subgroups.
Table 2.
Statistical comparison of pooled proportions of married individuals with suicidal behavior across different subgroups.
| Subgroups | Pooled proportions | 95%CI | I2 | Psubgroup |
|---|---|---|---|---|
| Fatality | 0.13 | |||
| Fatal (k=33) | 0.53 | 0.45 – 0.61 | 97.8% | |
| Nonfatal (k=11) | 0.43 | 0.33 – 0.54 | 96.6% | |
| Country | 0.0155 | |||
| Pakistan (k=9) | 0.45 | 0.31 – 0.59 | 93.2% | |
| Bangladesh (k=8) | 0.52 | 0.42 – 0.63 | 89.0% | |
| India (k=27) | 0.62 | 0.57 – 0.66 | 94.6% | |
| Quality | 0.6328 | |||
| Low (k=5) | 0.54 | 0.38– 0.69 | 83.5% | |
| Moderate (k=36) | 0.56 | 0.38 – 0.69 | 96.9% | |
| High (k=6) | 0.51 | 0.35 – 0.65 | 91.4% |
4. Discussion
4.1. Major Findings of the Study
The aim of this systematic review was to determine the proportion of marital status in individuals with suicidal behavior (fatal, non-fatal, or both) in South Asian countries. By analyzing a total of 47 studies, we found several key findings that shed light on this relationship between marital status and suicidal behavior. Our analysis revealed that the proportion of married individuals among persons with suicidal behavior in South Asia was 55.4%. This finding suggests that marital status may play a significant role in suicidal behavior in this region. However, it is important to note the high heterogeneity among studies included in our review. This indicates that there is considerable variability in the estimates across studies, which may be attributed to differences in sample characteristics, study designs, and measurement instruments.
When examining the specific types of suicidal behavior, our subgroup analysis showed that the proportion of married individuals among suicides was 52.7%, while among non-fatal suicide attempts it was 43.1%. Although the difference between these two groups was not statistically significant, these findings suggest that marital status may have varying degrees of association with different forms of suicidal behavior. Further research is needed to explore this association in more depth and investigate potential underlying factors.
Our analysis did not find a significant difference in the proportion of married individuals among persons with suicidal behavior based on the quality of the studies. This suggests that the association between marital status and suicidal behavior is consistent across studies with varying methodological quality. However, it is worth noting that the majority of the included studies were of moderate or poor quality, indicating the need for more rigorous research in this area.
4.2. Implications of the Study Results
Our findings have two important implications. Firstly, the relationship between marital status and suicidal behavior in South Asia appears to exhibit unique patterns compared to findings elsewhere. In many Western countries, being unmarried or divorced is often associated with a higher risk of suicidal behavior, while being married is generally considered protective (4,70). However, studies in South Asia have shown a higher proportion of married individuals among those engaging in suicidal behavior (59,68,71-73). This contrasting finding suggests that the association between marital status and suicidal behavior may be influenced by cultural, social, and economic factors specific to the South Asian region. Specifically, gender stereotyping, limited agency for women, and the expectation of fulfilling certain marital responsibilities may contribute to stress and psychological distress within marriages, potentially increasing the risk of suicidal behavior among married individuals, particularly among women (59,68).
Secondly, we also observed significant country-wise variation in the proportion of married individuals among attempted suicide cases. Studies conducted in India reported the highest proportion (61.8%), followed by Bangladesh (52.5%) and Pakistan (45.1%). These findings indicate that cultural and social factors may moderate the association between marital status and suicidal behavior in South Asian countries. Context-specific factors such as gender roles, societal norms, and marital expectations, which may differ between settings, could contribute to these variations.
4.3. Strength and Limitations
To the best of the authors’ knowledge, this is the first study assessing the marital status in suicidal behavior in South Asia. However, the present systematic review had some key limitations. First, the analysis may not reflect marital status as a risk factor as these findings may justify the proportion of married persons in the community. Second, the high heterogeneity among the included studies in terms of study design, populations, and measurement tools may have influenced pooled estimates and may affect the generalizability of results. Third, the potential for publication bias was not assessed due to the nature of studies included in this review. Fourth, the reliance on self-reported data in some studies may introduce biases and affect the accuracy of the estimates. Fifth, because we included only studies done on patients with suicidal behavior, we were unable to estimate associations between different types of marital status and suicidal behavior in the region.
5. Conclusions
This systematic review provides insights into the association between marital status and suicidal behavior in South Asia. The findings suggest that marital status may play a role in suicidal behavior, but further research is needed to better understand the underlying mechanisms and contextual factors. Future studies should consider employing standardized methodologies and addressing the limitations identified in this review to enhance the robustness of the evidence. Understanding the association between marital status and suicidal behavior can inform the development of targeted interventions and support strategies aimed at reducing suicide rates in South Asia.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Supplementary File S1, S2, S3.
Author Contributions
Conceptualization, S.M.Y.A. methodology, S.M.Y.A., and V.M. software, M.A.S.K. validation, S.M.Y.A.; formal analysis, M.A.S.K., and Y.K.; investigation, S.M.Y.A.; resources, S.M.Y.A., and V.M.; data curation, S.M.Y.A., R.S., D.B. and K.M.; writing—original draft preparation, S.M.Y.A., V.M., M.A.S.K., M.N.N.H., R.S., D.B., Y.K., and K.M.; writing—review and editing, S.M.Y.A., V.M., M.A.S.K., M.N.N.H., R.S., D.B., Y.K., and K.M.; visualization, M.A.S.K.; supervision, S.M.Y.A.; project administration, S.M.Y.A.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to we reviewed publicly available articles.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Suicide Worldwide in 2019: Global Health Estimates; WHO: Geneva, Switzerland, 2021; Available online: https://www.who.int/publications/i/item/9789240026643 (accessed on 15 September 2021).
- World Health Organization. Preventing Suicide: A Global Imperative; WHO: Geneva, Switzerland, 2014; Available online: https://apps.who.int/iris/handle/10665/131056 (accessed on 14 June 2021).
- Li, Z.; Page, A.; Martin, G.; Taylor, R. Attributable risk of psychiatric and socio-economic factors for suicide from individual-level, population-based studies: A systematic review. Soc. Sci. Med. 2011, 72, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Stack, S. Suicide: A 15-year review of the sociological literature. Part II: Modernization and social integration perspectives. Suicide Life-Threatening Behav. 2000, 30, 163–176. [Google Scholar]
- Kyung-Sook, W.; SangSoo, S.; Sangjin, S.; Young-Jeon, S. Marital status integration and suicide: A meta-analysis and meta-regression. Soc. Sci. Med. 2018, 197, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Fukuchi, N.; Kakizaki, M.; Sugawara, Y.; Tanji, F.; Watanabe, I.; Fukao, A.; Tsuji, I. Association of marital status with the incidence of suicide: A population-based Cohort Study in Japan (Miyagi cohort study). J. Affect. Disord. 2013, 150, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Milner, A.; Hjelmeland, H.; Arensman, E.; De Leo, D. Social-Environmental Factors and Suicide Mortality: A Narrative Review of over 200 Articles. Sociol. Mind 2013, 03, 137–148. [Google Scholar] [CrossRef]
- Yip, P.S.; Yousuf, S.; Chan, C.H.; Yung, T.; Wu, K.C.-C. The roles of culture and gender in the relationship between divorce and suicide risk: A meta-analysis. Soc. Sci. Med. 2015, 128, 87–94. [Google Scholar] [CrossRef]
- Kposowa, A.J.; McElvain, J.P.; Breault, K.D. Immigration and Suicide: The Role of Marital Status, Duration of Residence, and Social Integration. Arch. Suicide Res. 2008, 12, 82–92. [Google Scholar] [CrossRef]
- Cutright, P.; Fernquist, R.M. Effects of Societal Integration, Period, Region, and Culture of Suicide on Male Age-Specific Suicide Rates: 20 Developed Countries, 1955–1989. Soc. Sci. Res. 2000, 29, 148–172. [Google Scholar] [CrossRef]
- Bálint, L.; Osváth, P.; Rihmer, Z.; Döme, P. Associations between marital and educational status and risk of completed suicide in Hungary. J. Affect. Disord. 2016, 190, 777–783. [Google Scholar] [CrossRef]
- Yamauchi, T.; Fujita, T.; Tachimori, H.; Takeshima, T.; Inagaki, M.; Sudo, A. Age-adjusted relative suicide risk by marital and employment status over the past 25 years in Japan. J. Public Health 2013, 35, 49–56. [Google Scholar] [CrossRef]
- Gururaj, G.; Isaac, M.K.; Subbakrishna, D.K.; Ranjani, R. Risk factors for completed suicides: A case–control study from Bangalore, India. Inj. Control. Saf. Promot. 2004, 11, 183–191. [Google Scholar] [CrossRef]
- Zhang, J.; Li, N.; Tu, X.-M.; Xiao, S.; Jia, C. Risk factors for rural young suicide in China: A case–control study. J. Affect. Disord. 2011, 129, 244–251. [Google Scholar] [CrossRef]
- Zhang, J.; Wieczorek, W.; Conwell, Y.; Tu, X.-M.; Wu, B.Y.-W.; Xiao, S.; Jia, C. Characteristics of young rural Chinese suicides: A psychological autopsy study. Psychol. Med. 2010, 40, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Yeh, J.-Y.; Xirasagar, S.; Liu, T.-C.; Li, C.-Y.; Lin, H.-C. Does Marital Status Predict the Odds of Suicidal Death in Taiwan? A Seven-Year Population-Based Study. Suicide Life-Threatening Behav. 2008, 38, 302–310. [Google Scholar] [CrossRef]
- Arafat, S.M.Y.; Saleem, T.; Menon, V.; Ali, S.A.; Baminiwatta, A.; Kar, S.K.; Akter, H.; Singh, R. Depression and suicidal behavior in South Asia: A systematic review and meta-analysis. Glob. Ment. Health 2022, 9, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Arafat, S.M.Y.; Ali, S.A.; Menon, V.; Hussain, F.; Ansari, D.S.; Baminiwatta, A.; Saleem, T.; Singh, R.; Varadharajan, N.; Biyyala, D.; et al. Suicide methods in South Asia over two decades (2001–2020). Int. J. Soc. Psychiatry 2021, 67, 920–934. [Google Scholar] [CrossRef] [PubMed]
- Arafat, S.M.Y.; Menon, V.; Varadharajan, N.; Kar, S.K. Psychological Autopsy Studies of Suicide in South East Asia. Indian J. Psychol. Med. 2022, 44, 4–9. [Google Scholar] [CrossRef]
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P.; Agyemang, C.; Remuzzi, G.; Rapi, S.; Perruolo, E.; Parati, G. ESH Working Group on CV Risk in Low Resource Settings Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0147601. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality if nonrandomized studies in meta-analyses. 2000. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm (accessed on 14 March 2023).
- Barker, T.H.; Migliavaca, C.B.; Stein, C.; Colpani, V.; Falavigna, M.; Aromataris, E.; Munn, Z. Conducting proportional meta-analysis in different types of systematic reviews: A guide for synthesisers of evidence. BMC Med Res. Methodol. 2021, 21, 189. [Google Scholar] [CrossRef]
- Abdullah, M.; Khalily, M.T.; Ahmad, I.; Hallahan, B. Psychological autopsy review on mental health crises and suicide among youth inPakistan. Asia-Pacific Psychiatry 2018, 10, e12338. [Google Scholar] [CrossRef]
- Acherjya, G.K.; Ali, M.; Alam, A.B.M.S.; Rahman, M.M.; Mowla, S.G.M. The Scenario of Acute Poisoning in Jashore, Bangladesh. J. Toxicol. 2020, 2020, 2109673. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, Z.U.; Mobin, K.H.; Siddiqui, Z.A. Pattern of suicide: A descriptive, comparative study conducted in Karachi during period 2011-2015. Pakistan Journal of Medical & Health Sciences 2017, 11, 865–869. [Google Scholar]
- Ali, N.; Ashraf, M.F.; Farid, N.; Hashmi, A.M.; Khattak, M.A.; Nishat, M. Risk factors assessment of suicide cases in Punjab Pakistan & medico legal frame work shortcomings in Pakistan related to psychological autopsy -a case control psychological autopsy study. Pak. J. Med. Health Sci. 2022, 16, 212–214. [Google Scholar] [CrossRef]
- Ambade, V.N.; Godbole, H.V.; Kukde, H.G. Suicidal and homicidal deaths: A comparative and circumstantial approach. J. Forensic Leg. Med. 2007, 14, 253–260. [Google Scholar] [CrossRef]
- Ambade, V.N.; Kolpe, D.; Tumram, N.; Meshram, S.; Pawar, M.; Kukde, H. Characteristic Features of Hanging: A Study in Rural District of Central India. J. Forensic Sci. 2015, 60, 1216–1223. [Google Scholar] [CrossRef] [PubMed]
- Arafat, S.Y.; Mali, B.; Akter, H. Characteristics of suicidal attempts in Bangla online news portals. Neurol. Psychiatry Brain Res. 2020, 36, 83–85. [Google Scholar] [CrossRef]
- Arafat, S.Y.; Mali, B.; Akter, H. Characteristics, methods and precipitating events of suicidal behaviors in Bangladesh: A year-round content analysis of six national newspapers. Neurol. Psychiatry Brain Res. 2020, 36, 14–17. [Google Scholar] [CrossRef]
- Arafat, S.M.Y.; Mohit, M.A.; Mullick, M.S.I.; Kabir, R.; Khan, M.M. Risk factors for suicide in Bangladesh: Case–control psychological autopsy study. BJPsych Open 2020, 7, e18. [Google Scholar] [CrossRef]
- Arafat, S.M.Y.; Mali, B.; Akter, H. Demography and risk factors of suicidal behavior in Bangladesh: A retrospective online news content analysis. Asian J. Psychiatry 2018, 36, 96–99. [Google Scholar] [CrossRef]
- Armstrong, G.; Vijayakumar, L.; Pirkis, J.; Jayaseelan, M.; Cherian, A.; Soerensen, J.B.; Arya, V.; Niederkrotenthaler, T. Mass media representation of suicide in a high suicide state in India: An epidemiological comparison with suicide deaths in the population. BMJ Open 2019, 9, e030836. [Google Scholar] [CrossRef]
- Badiye, A.; Kapoor, N.; Ahmed, S. An empirical analysis of suicidal death trends in India: A 5 year retrospective study. J. Forensic Leg. Med. 2014, 27, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Bansal, P.; Gupta, A.; Kumar, R. The psychopathology and the socio-demographic determinants of attempted suicide patients. Journal of Clinical and Diagnostic Research 2011, 5, 917–920. [Google Scholar]
- Bashir, F.; Ara, J.; Kumar, S. Deliberate self poisoning at national poisoning control centre. J Liaquat Uni Med Health Sci. 2014, 13, 3–8. [Google Scholar]
- Bastia, B.K.; Kar, N. A Psychological Autopsy Study of Suicidal Hanging from Cuttack, India: Focus on Stressful Life Situations. Arch. Suicide Res. 2009, 13, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, M.S.; Verma, S.K.; Murty, O.P. Suicide Notes: Psychological and Clinical Profile. Int. J. Psychiatry Med. 2006, 36, 163–170. [Google Scholar] [CrossRef]
- Bhatia, M.S.; Aggarwal, N.K.; Aggarwal, B.B. Psychosocial profile of suicide ideators, attempters and completers in India. Int. J. Soc. Psychiatry 2000, 46, 155–163. [Google Scholar] [CrossRef]
- Bhise, M.C.; Behere, P.B. Risk Factors for Farmers' Suicides in Central Rural India: Matched Case-control Psychological Autopsy Study. Indian J. Psychol. Med. 2016, 38, 560–566. [Google Scholar] [CrossRef]
- Chandrasekaran, R.; Gnanaselane, J. Correlates of suicidal intent in attempted suicide. Hong Kong Journal of Psychiatry 2005, 15, 118–122. [Google Scholar]
- Chaudhari, V.A.; Das, S.; Sahu, S.K.; Devnath, G.P.; Chandra, A. Epidemio-toxicological profile and reasons for fatal suicidal poisoning: A record-based study in South India. J. Fam. Med. Prim. Care 2022, 11, 547–552. [Google Scholar] [CrossRef]
- Fernando, R.; Hewagama, M.; Priyangika, W.D.; Range, S.; Karunaratne, S. Study of suicides reported to the Coroner in Colombo, Sri Lanka. Med. Sci. Law 2010, 50, 25–28. [Google Scholar] [CrossRef]
- Hagaman, A.K.; Khadka, S.; Lohani, S.; Kohrt, B. Suicide in Nepal: A modified psychological autopsy investigation from randomly selected police cases between 2013 and 2015. Soc Psychiatry Psychiatr Epidemiol 2017, 52, 1483–1494. [Google Scholar] [CrossRef]
- Halder, S.; Mahato, A.K. Socio-demographic and Clinical Characteristics of Patients who Attempt Suicide: A Hospital-based Study from Eastern India. East Asian Arch. Psychiatry 2016, 26, 98–103. [Google Scholar]
- Kar, N. Profile of risk factors associated with suicide attempts: A study from Orissa, India. Indian J. Psychiatry 2010, 52, 48–56. [Google Scholar] [CrossRef]
- Khan, F.; Anand, B.; Devi, M.; Murthy, K. Psychological autopsy of suicide—a cross-sectional study. Indian J. Psychiatry 2005, 47, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.M.; Mahmud, S.; Karim, M.S.; Zaman, M.; Prince, M. Case–control study of suicide in Karachi, Pakistan. Br. J. Psychiatry 2008, 193, 402–405. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.M.; Ahmed, A.; Khan, S.R. Female Suicide Rates in Ghizer, Pakistan. Suicide Life-Threatening Behav. 2009, 39, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Verma, A.K.; Singh, U.S.; Singh, R. Autopsy audit of intentional burns inflicted by self or by others in north India-5 year snapshot. J. Forensic Leg. Med. 2015, 35, 29–32. [Google Scholar] [CrossRef]
- Hashim, U.; Kumar, R.S. Characteristics of suicidal attempts among farmers in rural South India. Ind. Psychiatry J. 2017, 26, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.N.S.; Jayakrishnan Kumari, A.; et al. A case-controlled study of Suicides in an agrarian district in Kerala. Indian J Soc Psychiatry 2011, 27, 9–15. [Google Scholar]
- Manoranjitham, S.D.; Rajkumar, A.P.; Thangadurai, P.; Prasad, J.; Jayakaran, R.; Jacob, K.S. Risk factors for suicide in rural south India. Br. J. Psychiatry 2010, 196, 26–30. [Google Scholar] [CrossRef]
- Mayer, P.; Ziaian, T. Indian Suicide and Marriage: A Research Note. J. Comp. Fam. Stud. 2002, 33, 297–305. [Google Scholar] [CrossRef]
- Mohanty, S.; Sahu, G.; Mohanty, M.K.; Patnaik, M. Suicide in India – A four year retrospective study. J. Forensic Leg. Med. 2007, 14, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Naz, F. Risk factors of successful suicide attempts in Punjab. Journal of Postgraduate Medical Institute. 2016, 30. [Google Scholar]
- Pal, V.S.; Bagul, K.R.; Mudgal, V.; Jain, P. Serum Kynurenine Levels in Patients of Depression with and without Suicidality: A Case-control Study. J. Clin. Diagn. Res. 2022, 16. [Google Scholar] [CrossRef]
- Parkar, S.R.; Nagarsekar, B.; Weiss, M.G. Explaining Suicide in an Urban Slum of Mumbai, India: A sociocultural autopsy. Crisis 2009, 30, 192–201. [Google Scholar] [CrossRef]
- Patel, V.; Ramasundarahettige, C.; Vijayakumar, L.; Thakur, J.; Gajalakshmi, V.; Gururaj, G.; Suraweera, W.; Jha, P.; Million Death Study Collaborators. Suicide mortality in India: A nationally representative survey. Lancet 2012, 379, 2343–2351. [Google Scholar] [CrossRef]
- Reza, A.S.; Feroz, A.H.; Islam, S.N.; Karim, M.N.; Rabbani, M.G.; Alam, M.S.; Rahman, M.M.; Rahman, M.R.; Ahmed, H.U.; Bhowmik, A.D.; Khan, M.Z. Risk Factors of Suicide and Para Suicide in Rural Bangladesh. J. Med. 2014, 14, 123–129. [Google Scholar] [CrossRef]
- Sadia, S.; Naheed, K.; Tariq, F.; Ghani, M.I.; Zarif, P.; Rafiq, A.; Laique, T. An Audit of Wheat Pill Poisoning in A Tertiary Care Hospital: A Retroscpective Study. Age 2021, 30, 50. [Google Scholar] [CrossRef]
- Sahoo, M.K.; Biswas, H.; Agarwal, S.K. Risk factors of suicide among patients admitted with suicide attempt in Tata main hospital, Jamshedpur. Indian J. Public Health 2016, 60, 260–267. [Google Scholar] [CrossRef]
- Saaiq, M.; Ashraf, B. Epidemiology and Outcome of Self-Inflicted Burns at Pakistan Institute of Medical Sciences, Islamabad. World J. Plast. Surg. 2014, 3, 107–114. [Google Scholar]
- Samaraweera, S.; Sumathipala, A.; Siribaddana, S.; Sivayogan, S.; Bhugra, D. Completed Suicide among Sinhalese in Sri Lanka: A Psychological Autopsy Study. Suicide Life-Threatening Behav. 2008, 38, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.M.A.; Ahmed, S.; Arafat, S.M.Y. Demography and Risk Factors of Suicide in Bangladesh: A Six-Month Paper Content Analysis. Psychiatry J. 2017, 2017, 3047025. [Google Scholar] [CrossRef] [PubMed]
- Sharmin Salam, S.; Alonge, O.; Islam, M.I.; Hoque, D.M.E.; Wadhwaniya, S.; Ul Baset, M.K.; Mashreky, S.R.; El Arifeen, S. The Burden of Suicide in Rural Bangladesh: Magnitude and Risk Factors. Int. J. Environ. Res. Public Health 2017, 14, 1032. [Google Scholar] [CrossRef]
- Srivastava, A. Psychological attributes and socio-demographic profile of hundred completed suicide victims in the state of Goa, India. Indian J. Psychiatry 2013, 55, 268–272. [Google Scholar] [CrossRef] [PubMed]
- Vijayakumar, L.; Rajkumar, S. Are risk factors for suicide universal? A case-control study in India. Acta Psychiatr. Scand. 1999, 99, 407–411. [Google Scholar] [CrossRef]
- Vijayakumar, L.; Ali, Z.S.; Umamaheswari, C. Socio cultural and clinical factors in repetition of suicide attempts: A study from India. Int. J. Cult. Ment. Health 2008, 1, 3–9. [Google Scholar] [CrossRef]
- Øien-Ødegaard, C.; Hauge, L.J.; Reneflot, A. Marital status, educational attainment, and suicide risk: A Norwegian register-based population study. Popul. Health Metr. 2021, 19, 33. [Google Scholar] [CrossRef]
- Kasaju, S.P.; Krumeich, A.; Van der Putten, M. Suicide and deliberate self-harm among women in Nepal: A scoping review. BMC Women’s Health 2021, 21, 407. [Google Scholar] [CrossRef]
- Shekhani, S.S.; Perveen, S.; Hashmi, D.-E.; Akbar, K.; Bachani, S.; Khan, M.M. Suicide and deliberate self-harm in Pakistan: A scoping review. BMC Psychiatry 2018, 18, 44. [Google Scholar] [CrossRef]
- Asad, N.; Karmaliani, R.; Sullaiman, N.; Bann, C.M.; McClure, E.M.; Pasha, O.; Wright, L.L.; Goldenberg, R.L. Prevalence of suicidal thoughts and attempts among pregnant Pakistani women. Acta Obstet. Gynecol. Scand. 2010, 89, 1545–1551. [Google Scholar] [CrossRef]
Figure 1.
A forest plot showing the proportion of married individuals among all suicidal behavior.

Figure 2.
A forest plot showing the overall proportion of married individuals among suicide and suicide attempts.
Figure 2.
A forest plot showing the overall proportion of married individuals among suicide and suicide attempts.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



