Submitted:
11 July 2023
Posted:
13 July 2023
You are already at the latest version
Abstract
Cancer patients may experience significant distress. The “Emotion Thermometers” (ETs) are a short visual analogue scale used to screen patients for psychosocial risk. This study aimed to assess emotional distress in a large sample of cancer patients attending psychological services at an NGO, and to explore factors that may contribute to it.
The ETs were answered by 899 cancer patients. They were, on average, 59.9 years old, the majority were female, had breast cancer, were under treatment or were disease-free survivors, and reported high levels of emotional distress, above the cut-off (≥5). A Generalized Linear Model was used to measure the association between the level of Distress and 33 items of the problem list. Four items - sadness, depression, sleep and breathing - were found to be significantly related to a higher level of Distress. Additionally, women and those who were in the palliative phase also had significantly higher levels of Distress.
Conclusions: The results confirm the need for early emotional screening in cancer patients, as well as the relevance of attending to the characteristics of each patient. Additionally, they highlight the utility of the ETs for the clinical practice, allowing to optimize the referral to specialized psy-chosocial services.
Keywords:
distress thermometer 1
; emotion thermometer 2
; emotional distress 3
; anxiety 4
; depression 5
; cancer 6
1. Introduction
In Portugal, a total of 60,467 new cancer cases were diagnosed in 2020, with the most prevalent being breast cancer for women and prostate cancer for men, followed by colorectal and lung cancers for both sexes [1]. A cancer diagnosis can be a deeply overwhelming experience. Patients are likely to experience higher levels of anxiety, depression, distress, fear of cancer recurrence, sleep disturbance, posttraumatic stress disorders, among other psychological difficulties (e.g., [2,3,4,5,6]).
The distress experienced by cancer patients is not always evident for healthcare professionals and is likely to be underrecognized and undertreated, preventing patients from receiving adequate and timely psychological support. This has an impact on the quality of life, life satisfaction, and treatment adherence of the patients (e.g., [7,8,9]). It may also influence treatment efficacy by affecting the immunosuppressive function [10] as well as increasing the risk of recurrence [11].
Distress is considered the ‘sixth vital sign’ in psycho-oncology [12]. Thus, efficient screening for distress is crucial, which has led to the need for developing short screening tools. The Distress Thermometer (DT), developed by the National Comprehensive Cancer Network, was the first attempt to easily screen for distress in cancer patients..
However, while the DT performs well in screening for distress, it is modestly accurate in screening for anxiety and depression [13]. Thus, in 2007, Alex Mitchell proposed a new multidomain extension of the DT, the Emotion Thermometers (ETs) tool to ensure that not only distress, but also anxiety, depression and anger could be easily detected by healthcare professionals. The ETs are a brief, visual analogue scale (VAS) and easy-to-use tool to identify cancer patients’ psychosocial distress. It includes five visual rating scales with different emotional states, namely: distress, anxiety, depression, anger, and need for help [14].
In a recent review concerning the use of ETs among individuals diagnosed with cancer, Harju et al. stated that overall ETs are a sensitive tool to screen for distress, as found by five validation and two exploratory studies, that recommended a cut-off equal to or greater than 4 [15]. In Portugal, the ETs were validated by Teixeira et al. using a sample of 147 cancer patients[16]. The authors found that the ETs have excellent discrimination and identified the optimal cut-off values for each ET. The ETs have been widely used not only with patients but also caregivers [17], and patients with cardiovascular disease or epilepsy (e.g., [18,19]).
2. Materials and Methods
This was a cross-sectional study that employed a questionnaire to adult patients diagnosed with cancer, at their first consultation at the Psycho-Oncology Unit of the Portuguese Cancer League (NGO), between February 2020 and February 2023. Approximately half of the participants were referred by a health professional, due to their potential increased risk for psychological distress.
2.1. Measures
The questionnaire included demographic (age, sex) and clinical questions (disease stage and type of cancer), the five ETs (distress, anxiety, depression, anger and need for help), as well as the original version of the problem list with 33 items [44]. Additionally, the researchers added five items within the section “other problems” to ascertain further concerns: economic, legal, communication with health professionals, body image, and information about the disease (Table A1, in Supplementary materials).
Patients indicated the amount of emotional distress they felt in the past week including today, on the five ETs, by selecting a number from 0 (no distress) to 10 (extreme distress), while the list of problems required a yes/no response. The questionnaires were self-administered while patients were in the waiting room for the first Psycho-Oncology consultation but in some cases, they were filled out with the help of the psychologist.
2.2. Statistical analyses
Descriptive statistics were used to characterize the sample and to identify items on the problem list with high prevalence. Emotional distress was described in terms of frequency and mean (SD). Previously validated Portuguese cut-offs were used to indicate the presence of emotional distress in each ETs (i.e., ≥5 for “distress”, “depression” and “anger”; ≥6 for “anxiety” and ≥4 for “need for help”) [16].
2.3. Generalized linear model
We used the level of distress, measured on a continuous scale (from 0 to 10) as a dependent variable, and the items of the problem list as independent variables, to determine which of them were the most distressing. Age (years, continuous), sex (dichotomous), and disease phase (nominal: diagnosis, treatment, relapse, survival, palliative) were also included as independent variables, as they have previously been shown to demonstrate a relationship with distress [28]. In a first exploratory analysis, a separate model was performed for each independent variable, to ascertain their relationship with distress (Table A2, in Supplementary materials). Only the statistically significant covariates, considering a 95% confidence interval, were then considered entered in the final adjusted generalized linear model (GLM).
The GLM is a flexible generalization of linear regression that uses an iteratively reweighted least squares method for maximum likelihood estimation of the model parameters. This model allows for the dependent variable to have a non-normal distribution but is linearly related to the factors and covariates via a specified link function. Specifically, a GLM with gamma distribution and log link was used [45]. For the simplicity of interpretation, results are presented as marginal effects (i.e., the incremental effect in the dependent variable, resulting from a change in the covariate). Additionally, the predicted margins (i.e., adjusted means) for the statistically significant covariates, considering a 95% confidence interval, are presented. All analyses were performed with Stata version 16.1.
3. Results
3.1. Descriptive analysis
A total of 899 patients (79.2% female) with a mean age of 59.9 years (SD=12.6 years) answered the questionnaire. Most patients were in the treatment phase (48.7%) or in the survival phase (32.4%), while 8.9%, 5.9% and 4.1% were in the diagnosis, relapse, and palliative phase, respectively. The most frequent cancer type was breast (50.7%), followed by colorectal (8.2%), lung (5.6%) and lymphoma (4.7%) (Table 1).
The distribution of patients reporting emotional distress (0 to 10) in each of the five ETs, as well as the percentage of patients with emotional distress over cut-offs, is presented in Figure 1.
Results show a left-skewed distribution for all ETs, except for anger, with most patients reporting high levels of emotional distress. For the distress thermometer, 87% of patients are above the cut-off (≥5) (Figure 1). The most frequently reported problems were worry (91.9%), sadness (83.9%), fears (80.6%), nervousness (78.4%), fatigue (75.2%), sleep (61.7%), and pain (59.0%) (Figure 2).
3.2. Generalized linear model
Results from the GLM show that there are four items in the problem list – sadness, depression, sleep and breathing – that are significantly related to a higher level of distress. Specifically, marginal effects demonstrate that, on average, patients who report sadness have a level of distress 1.42 points higher than patients who do not report sadness, when adjusting for all other covariates (marginal effect = 1.42, p<0.01). Similarly, patients who report depression, have a level of distress 1.13 points higher than patients who do not (marginal effect = 1.13, p<0.01). Patients with sleeping problems and breathing problems also have a higher level of distress, with a marginal effect of 0.55 (p<0.01) and 0.63 (p<0.01), respectively. In addition to the items of the problem list, being female also contributes to a higher level of distress (0.59 points higher (p<0.01) as compared to male patients). Finally, patients currently in the palliative phase have a level of distress 1.33 points higher than patients in the treatment phase (p<0.01) (Table 2). The full results are available in Table A3, in Supplementary materials.
The predicted margins for the abovementioned covariates are shown in Figure 3.
These adjusted means represent the average level of distress within each category. In other words, they represent the average level of distress for female patients and male patients within the observed sample, adjusted for all the other covariates. Note that for the disease phase, only the level of distress of patients in the palliative phase in comparison to the treatment phase showed a statistically significant difference.
4. Discussion
The aim of this study was twofold. First, it aimed to identify the levels of distress experienced by cancer patients seeking psychological support at an NGO. Second, it aimed to identify the factors that most contribute to this distress to better understand and address these problems in the psychological support provided to these individuals. The evaluation of the distress was done using the ETs, a brief VAS and easy-to-use tool to identify cancer patients’ distress [14].
Overall, the results showed, as expected, that most of the patients experienced high levels of distress, with 87% of patients being above the cut-off (≥5) proposed by Teixeira et al. [16]. Thus, it confirms the results of previous studies showing that cancer patients tend to experience a wide range of negative outcomes [2,3,4,5,6]. In a previous review [15], the percentage of individuals experiencing clinically significant distress (with a cut-off ≥4) ranged from 13% [46] to 88.5% [14]. The prevalence in our study is higher than most previous studies (except for [14]), what was expected considering that participants were seeking psychological support (either by self-initiative or by referral from health professionals), which effectively highlights the patients’ need for specialized help. It is also important to acknowledge that part of the data for this study was collected during the COVID-19 pandemic, which may have exacerbated the distress experienced by cancer patients, including those seeking psychological support in a cancer NGO. This is consistent with previous findings evidencing that the psychological well-being and distress of cancer patients were greatly affected by the COVID-19 outbreak (e.g., [47,48,49]).
Since participants who seek psychological support are those who, supposedly, are more aware of their distress and more willing to acknowledge and discuss their feelings, as evidenced by some studies (e.g., [50,51]), it is also important to stress that many other cancer patients may be experiencing significant distress without receiving any specialized emotional support. Therefore, it is important to conduct studies that address these patients, as well as develop strategies that allow their identification and proper referral for psychosocial services.
There are multiple causes of distress, and they may differ greatly between people. Assessing these causes is extremely important since it allows the implementation of a treatment plan according to the individual’s needs. Based on the list of problems [44] , we found that the main risk factors for experiencing elevated distress among cancer patients were mostly physical (sleep disturbance and breathing difficulties) and emotional problems (sadness and depression). These results are in line with previous studies [26,27,42,43]. Sleep disturbances and breathing difficulties are prevalent symptoms in cancer patients, particularly in those with metastatic cancer, and are often interrelated [52,53]. These symptoms can contribute to the magnification of the distress experienced by cancer patients (e.g., by impacting daily physical activity). Sadness and depression are also common experiences among cancer patients. This pattern is found in most studies, as highlighted by some authors (e.g., [54]). Additionally, being a woman and in a palliative phase of the disease were also risk factors for experiencing high distress, which also confirms previous studies (e.g., [23,28]).
Past literature (e.g., [55]) has reported that practical, family, and religious problems are less likely to cause heightened distress among cancer patients. Similarly, our findings also suggest that these factors may not be significant contributors to distress in this population. However, as pointed out by Jewett et al., the problem list included in the ETs may not accurately identify the concerns that are most strongly associated with high levels of distress in cancer patients [56]. As we found, the most prevalent problems identified were not those that predicted higher levels of distress (e.g., worry, fears, fatigue, pain), with the exception being sadness and sleep. In contrast, while breathing difficulties were not among the most prevalent problems, our analysis revealed a significant association between these symptoms and higher levels of distress in cancer patients. Yet, the problem list can be useful by providing information about symptomatology, but it does not exclude the need for a careful and rigorous evaluation of the causes of distress in the clinical interview.
Our review of the literature (e.g., [57]) and clinical experience led us to include additional items, such as body image concerns, communication with health professionals or legal problems, in the problem list beyond the original set (some of these items are also included in the 2023 version of the list problems proposed by the NCCN). Despite their significant association with distress in the unadjusted analysis (Table A1 in Supplementary materials), we didn’t find a significant association between these added items and levels of distress in cancer patients in our adjusted model. While these items may be clinically relevant and worth considering in patient assessments (e.g., concerns about body image were a prevalent problem), our findings suggest that they may not be as strongly linked to distress as other emotional and physical problems.
Nevertheless, since emotional problems and distress may have an overlapping definition as “a multifactorial unpleasant emotional experience” [58] we performed an additional GLM adjusted model to explore the relationship between distress and the problem list items, without emotional items (i.e., when the five emotional problems are excluded from the analysis). We found a significant association between distress and problems with work/school, dealing with children, loss of faith, eating problems, and concerns about body image (in addition to sleep and breathing). Results can be found in Table A3 in Supplementary materials. Taking into account these results, it is also important to consider and analyze eventual mediation processes by the emotional problems/items.
4.1. Implications for clinical practice
This study has important clinical implications. By identifying the prevalence of distress in cancer patients and the most common sources of that distress, healthcare providers can determine appropriate referrals to professionals or interventions that may be most effective in addressing cancer patients’ specific needs. Also, healthcare professionals may use this information to psychoeducate patients and their families/caregivers about common causes of distress, empowering them to seek support or to manage distress, and tailor interventions according to patients’ needs.
Since the large majority of patients in our study show high levels of distress, these results suggest that a considerable number of cancer patients may manifest significant emotional distress throughout the cancer journey. Therefore, the early screening for distress, and its monitorization throughout the course of the disease, is of crucial importance to early referral for mental health services. Additionally, our results also suggest the relevance of attending to the sociodemographic and clinical characteristics of patients for the early identification of those who may be at greater risk of developing high levels of distress and who, therefore, may benefit most of the screening measures and referral for mental health services.
4.2. Limitations and future research
This study presents some limitations that should be acknowledged. This is a cross-sectional study which limits conclusions regarding the causality between the identified problems and the experienced distress. Additionally, due to this specific design, we cannot fully capture the trajectory of distress experienced by cancer patients throughout the course of their disease. Also, participants were asked to report their distress level only in the previous week, limiting conclusions regarding their levels of distress at different moments. Longitudinal studies are needed to better understand trajectories of distress and related factors in the different phases of the disease.
The heterogeneity of the participants also represents a limitation. Variables that may be specific to different types of cancer, treatments, and phases of the disease were not considered. Moreover, participants of this study were seeking psychological support, and the data was collected during the COVID-19 pandemic, which may have contributed to the higher levels of distress experienced by these participants. Future studies should also include patients not seeking psychological support to examine their levels of distress and their list of problems.
Finally, patients may underreport or overreport their distress due to several reasons (e.g., social desirability). Also, additional problems that were included in the latest version of the NCCN’s DT were not included in the present study (e.g., ability to have children, access to medicine); thus, future studies should explore the role of these new problems in explaining individual differences in the distress experienced.
5. Conclusions
In conclusion, the results of our study confirm the need for early emotional screening of cancer patients, as well as the relevance of attending to the characteristics of each patient. They also highlight the utility of the ETs for clinical practice, allowing for the optimization of the referral to specialized psychosocial services and better adjust the intervention according to the distress levels and reported needs.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, Table A1: Unadjusted generalized linear model results for the univariate relationship between patient characteristics, problem list, and distress; Table A2: Generalized linear model results for the relationship between patient characteristics and problem list, and distress; Table A3: Generalized linear model results for the relationship between patient characteristics and problem list (excluding emotional problems), and distress.
Author Contributions
Conceptualization, S. Silva, T. Paredes; Methodology, Investigation, Writing – original draft preparation, Writing—review and editing, S. Silva, T. Paredes, R.J. Teixeira, T. Brandão, K. Dimitrovová, D. Marques; Software, Formal analysis, K. Dimitrovová, D. Marques; Methodology, Writing—review and editing, S. Silva, T. Paredes, M. Leal, A. Dias, C. Neves, G. Marques; Visualization, Supervision, J. Sousa; Project administration, N. Amaral. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The research project was submitted to and approved by the Board of Directors of Portuguese Cancer League (Central branch), which comprised experts from different health science fields and constitutes institutional research ethics review and approval.
Informed Consent Statement
Informed consent was obtained from all patients involved in the study.
Data Availability Statement
Part of the data can be found in https://www.ligacontracancro.pt/sofrimentoemocional/
Acknowledgments
This study was conducted within the scope of the Psycho-Oncology Units of the Portuguese Cancer League.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ferlay J; Ervik M; Lam F; Colombet M; Mery L; Piñeros M; Znaor A; Soerjomataram I; Bray F Global Cancer Observatory: Cancer Today - Portugal. Available online: https://gco.iarc.fr/today (accessed on 29 June 2023).
- Luigjes-Huizer, Y.L.; Tauber, N.M.; Humphris, G.; Kasparian, N.A.; Lam, W.W.T.; Lebel, S.; Simard, S.; Smith, A. Ben; Zachariae, R.; Afiyanti, Y.; et al. What Is the Prevalence of Fear of Cancer Recurrence in Cancer Survivors and Patients? A Systematic Review and Individual Participant Data Meta-analysis. Psychooncology 2022, 31, 879–892. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J.; Ferguson, D.W.; Gill, J.; Paul, J.; Symonds, P. Depression and Anxiety in Long-Term Cancer Survivors Compared with Spouses and Healthy Controls: A Systematic Review and Meta-Analysis. Lancet Oncol 2013, 14, 721–732. [Google Scholar] [CrossRef] [PubMed]
- Mogavero, M.P.; DelRosso, L.M.; Fanfulla, F.; Bruni, O.; Ferri, R. Sleep Disorders and Cancer: State of the Art and Future Perspectives. Sleep Med Rev 2021, 56, 101409. [Google Scholar] [CrossRef] [PubMed]
- Unseld, M.; Krammer, K.; Lubowitzki, S.; Jachs, M.; Baumann, L.; Vyssoki, B.; Riedel, J.; Puhr, H.; Zehentgruber, S.; Prager, G.; et al. Screening for Post-traumatic Stress Disorders in 1017 Cancer Patients and Correlation with Anxiety, Depression, and Distress. Psychooncology 2019, 28, 2382–2388. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Chan, M.; Bhatti, H.; Halton, M.; Grassi, L.; Johansen, C.; Meader, N. Prevalence of Depression, Anxiety, and Adjustment Disorder in Oncological, Haematological, and Palliative-Care Settings: A Meta-Analysis of 94 Interview-Based Studies. Lancet Oncol 2011, 12, 160–174. [Google Scholar] [CrossRef]
- Bui, Q.-U.T.; Ostir, G. V.; Kuo, Y.-F.; Freeman, J.; Goodwin, J.S. Relationship of Depression to Patient Satisfaction: Findings from the Barriers to Breast Cancer Study. Breast Cancer Res Treat 2005, 89, 23–28. [Google Scholar] [CrossRef]
- Kondryn, H.J.; Edmondson, C.L.; Hill, J.; Eden, T.O. Treatment Non-Adherence in Teenage and Young Adult Patients with Cancer. Lancet Oncol 2011, 12, 100–108. [Google Scholar] [CrossRef]
- LI, Q.; LIN, Y.; XU, Y.; ZHOU, H. The Impact of Depression and Anxiety on Quality of Life in Chinese Cancer Patient-Family Caregiver Dyads, a Cross-Sectional Study. Health Qual Life Outcomes 2018, 16, 230. [Google Scholar] [CrossRef]
- Green McDonald, P.; O’Connell, M.; Lutgendorf, S.K. Psychoneuroimmunology and Cancer: A Decade of Discovery, Paradigm Shifts, and Methodological Innovations. Brain Behav Immun 2013, 30, S1–S9. [Google Scholar] [CrossRef]
- Antoni, M.H.; Lechner, S.; Diaz, A.; Vargas, S.; Holley, H.; Phillips, K.; McGregor, B.; Carver, C.S.; Blomberg, B. Cognitive Behavioral Stress Management Effects on Psychosocial and Physiological Adaptation in Women Undergoing Treatment for Breast Cancer. Brain Behav Immun 2009, 23, 580–591. [Google Scholar] [CrossRef]
- Bultz, B.D.; Carlson, L.E. Emotional Distress: The Sixth Vital Sign in Cancer Care. Journal of Clinical Oncology 2005, 23, 6440–6441. [Google Scholar] [CrossRef]
- Mitchell, A.J. Pooled Results From 38 Analyses of the Accuracy of Distress Thermometer and Other Ultra-Short Methods of Detecting Cancer-Related Mood Disorders. Journal of Clinical Oncology 2007, 25, 4670–4681. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J.; Baker-Glenn, E.A.; Granger, L.; Symonds, P. Can the Distress Thermometer Be Improved by Additional Mood Domains? Part I. Initial Validation of the Emotion Thermometers Tool. Psychooncology 2010, 19, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Harju, E.; Michel, G.; Roser, K. A Systematic Review on the Use of the Emotion Thermometer in Individuals Diagnosed with Cancer. Psychooncology 2019, 28, 1803–1818. [Google Scholar] [CrossRef]
- Teixeira, R.J.; Machado, J.C.; Faria, S.; Remondes-Costa, S.; Brandão, T.; Branco, M.; Moreira, S.; Pereira, M.G. Brief Emotional Screening in Oncology: Specificity and Sensitivity of the Emotion Thermometers in the Portuguese Cancer Population. Palliat Support Care 2020, 18, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Areia, N.P.; Mitchell, A.; Fonseca, G.; Major, S.; Relvas, A.P. A Visual-Analogue Screening Tool for Assessing Mood and Quality of Daily Life Complications in Family Members of People Living With Cancer: Portuguese Version of the Emotion Thermometers: Burden Version. Eval Health Prof 2020, 43, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Rampling, J.; Mitchell, A.J.; Von Oertzen, T.; Docker, J.; Jackson, J.; Cock, H.; Agrawal, N. Screening for Depression in Epilepsy Clinics. A Comparison of Conventional and Visual-Analog Methods. Epilepsia 2012, 53, 1713–1721. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Morgan, J.P.; Petersen, D.; Fabbri, S.; Fayard, C.; Stoletniy, L.; Chiong, J. Validation of Simple Visual-Analogue Thermometer Screen for Mood Complications of Cardiovascular Disease: The Emotion Thermometers. J Affect Disord 2012, 136, 1257–1263. [Google Scholar] [CrossRef] [PubMed]
- Zabora, J.; BrintzenhofeSzoc, K.; Curbow, B.; Hooker, C.; Piantadosi, S. The Prevalence of Psychological Distress by Cancer Site. Psychooncology 2001, 10, 19–28. [Google Scholar] [CrossRef]
- Gao, W.; Bennett, M.I.; Stark, D.; Murray, S.; Higginson, I.J. Psychological Distress in Cancer from Survivorship to End of Life Care: Prevalence, Associated Factors and Clinical Implications. Eur J Cancer 2010, 46, 2036–2044. [Google Scholar] [CrossRef]
- Giese-Davis, J.; Waller, A.; Carlson, L.E.; Groff, S.; Zhong, L.; Neri, E.; Bachor, S.M.; Adamyk-Simpson, J.; Rancourt, K.M.; Dunlop, B.; et al. Screening for Distress, the 6th Vital Sign: Common Problems in Cancer Outpatients over One Year in Usual Care: Associations with Marital Status, Sex, and Age. BMC Cancer 2012, 12, 441. [Google Scholar] [CrossRef]
- Syrowatka, A.; Motulsky, A.; Kurteva, S.; Hanley, J.A.; Dixon, W.G.; Meguerditchian, A.N.; Tamblyn, R. Predictors of Distress in Female Breast Cancer Survivors: A Systematic Review. Breast Cancer Res Treat 2017, 165, 229–245. [Google Scholar] [CrossRef]
- Hamilton, J.; Kroska, E.B. Distress Predicts Utilization of Psychosocial Health Services in Oncology Patients. Psychooncology 2019, 28, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, J.; Kruse, H.; Holcomb, L.; Freche, R. Distress and Psychosocial Needs: Demographic Predictors of Clinical Distress After a Diagnosis of Cancer. Clin J Oncol Nurs 2018, 22, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Mehnert, A.; Hartung, T.J.; Friedrich, M.; Vehling, S.; Brähler, E.; Härter, M.; Keller, M.; Schulz, H.; Wegscheider, K.; Weis, J.; et al. One in Two Cancer Patients Is Significantly Distressed: Prevalence and Indicators of Distress. Psychooncology 2018, 27, 75–82. [Google Scholar] [CrossRef]
- Taghizadeh, A.; Pourali, L.; Vaziri, Z.; Saedi, H.R.; Behdani, F.; Amel, R. Psychological Distress in Cancer Patients. Middle East J Cancer 2018, 9, 143–149. [Google Scholar] [CrossRef]
- Carlson, L.E.; Zelinski, E.L.; Toivonen, K.I.; Sundstrom, L.; Jobin, C.T.; Damaskos, P.; Zebrack, B. Prevalence of Psychosocial Distress in Cancer Patients across 55 North American Cancer Centers. J Psychosoc Oncol 2019, 37, 5–21. [Google Scholar] [CrossRef]
- Watts, K.J.; Good, L.H.; McKiernan, S.; Miller, L.; O’Connor, M.; Kane, R.; Kruger, D.J.; Adams, B.R.; Musiello, T. “Undressing” Distress among Cancer Patients Living in Urban, Regional, and Remote Locations in Western Australia. Supportive Care in Cancer 2016, 24, 1963–1973. [Google Scholar] [CrossRef] [PubMed]
- Andrykowski, M.A.; Cordova, M.J. Factors Associated with PTSD Symptoms Following Treatment for Breast Cancer: Test of the Andersen Model. J Trauma Stress 1998, 11, 189–203. [Google Scholar] [CrossRef]
- Hagedoorn, M.; Buunk, B.P.; Kuijer, R.G.; Wobbes, T.; Sanderman, R. Couples Dealing with Cancer: Role and Gender Differences Regarding Psychological Distress and Quality of Life. Psychooncology 2000, 9, 232–242. [Google Scholar] [CrossRef]
- Schnoll, R.A.; Harlow, L.L. Using Disease-Related and Demographic Variables to Form Cancer-Distress Risk Groups. J Behav Med 2001, 24, 57–74. [Google Scholar] [CrossRef]
- Banks, E.; Byles, J.E.; Gibson, R.E.; Rodgers, B.; Latz, I.K.; Robinson, I.A.; Williamson, A.B.; Jorm, L.R. Is Psychological Distress in People Living with Cancer Related to the Fact of Diagnosis, Current Treatment or Level of Disability? Findings from a Large Australian Study. Medical Journal of Australia 2010, 193. [Google Scholar] [CrossRef]
- Kim, S.J.; Rha, S.Y.; Song, S.K.; Namkoong, K.; Chung, H.C.; Yoon, S.H.; Kim, G.M.; Kim, K.R. Prevalence and Associated Factors of Psychological Distress among Korean Cancer Patients. Gen Hosp Psychiatry 2011, 33, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Pichler, T.; Marten-Mittag, B.; Hermelink, K.; Telzerow, E.; Frank, T.; Ackermann, U.; Belka, C.; Combs, S.E.; Gratzke, C.; Gschwend, J.; et al. Distress in Hospitalized Cancer Patients: Associations with Personality Traits, Clinical and Psychosocial Characteristics. Psychooncology 2022, 31, 770–778. [Google Scholar] [CrossRef] [PubMed]
- Vos, P.J.; Garssen, B.; Visser, A.P.; Duivenvoorden, H.J.; de Haes, H.C.J.M. Early Stage Breast Cancer: Explaining Level of Psychosocial Adjustment Using Structural Equation Modeling. J Behav Med 2004, 27, 557–580. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.K.; Kaji, A.H.; Roth, K.G.; Hari, D.M.; Yeh, J.J.; Dauphine, C.; Ozao-Choy, J.; Chen, K.T. Determinants of Psychosocial Distress in Breast Cancer Patients at a Safety Net Hospital. Clin Breast Cancer 2022, 22, 43–48. [Google Scholar] [CrossRef]
- Herschbach, P.; Britzelmeir, I.; Dinkel, A.; Giesler, J.M.; Herkommer, K.; Nest, A.; Pichler, T.; Reichelt, R.; Tanzer-Küntzer, S.; Weis, J.; et al. Distress in Cancer Patients: Who Are the Main Groups at Risk? Psychooncology 2020, 29, 703–710. [Google Scholar] [CrossRef]
- Duan, Y.; Wang, L.; Sun, Q.; Liu, X.; Ding, S.; Cheng, Q.; Xie, J.; Cheng, A.S. Prevalence and Determinants of Psychological Distress in Adolescent and Young Adult Patients with Cancer: A Multicenter Survey. Asia Pac J Oncol Nurs 2021, 8, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Lavery, J.F.; Clarke, V.A. Causal Attributions, Coping Strategies, and Adjustment to Breast Cancer. Cancer Nurs 1996, 19, 20–28. [Google Scholar] [CrossRef]
- Peters, L.; Brederecke, J.; Franzke, A.; de Zwaan, M.; Zimmermann, T. Psychological Distress in a Sample of Inpatients With Mixed Cancer—A Cross-Sectional Study of Routine Clinical Data. Front Psychol 2020, 11. [Google Scholar] [CrossRef]
- VanHoose, L.; Black, L.L.; Doty, K.; Sabata, D.; Twumasi-Ankrah, P.; Taylor, S.; Johnson, R. An Analysis of the Distress Thermometer Problem List and Distress in Patients with Cancer. Supportive Care in Cancer 2015, 23, 1225–1232. [Google Scholar] [CrossRef]
- Lim, H.A.; Mahendran, R.; Chua, J.; Peh, C.-X.; Lim, S.-E.; Kua, E.-H. The Distress Thermometer as an Ultra-Short Screening Tool: A First Validation Study for Mixed-Cancer Outpatients in Singapore. Compr Psychiatry 2014, 55, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A. Emotion Thermometers Tool. Available online: http://www.psycho-oncology.info/ET.htm (accessed on 9 May 2023).
- StataCorp GLM – Generalized Linear Models. Available online: https://www.stata.com/manuals/rglm.pdf (accessed on 25 May 2023).
- Rogers, S.N.; Mepani, V.; Jackson, S.; Lowe, D. Health-Related Quality of Life, Fear of Recurrence, and Emotional Distress in Patients Treated for Thyroid Cancer. British Journal of Oral and Maxillofacial Surgery 2017, 55, 666–673. [Google Scholar] [CrossRef]
- Momenimovahed, Z.; Salehiniya, H.; Hadavandsiri, F.; Allahqoli, L.; Günther, V.; Alkatout, I. Psychological Distress Among Cancer Patients During COVID-19 Pandemic in the World: A Systematic Review. Front Psychol 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Paredes, T.F.; Silva, S.M.; Pacheco, A.F.; de Sousa, B.C.; Pires, C.A.; Dias, A.S.; Costa, A.L.; Mesquita, A.R.; Fernandes, E.E.; Marques, G.F.; et al. Psychological Distress in a Portuguese Sample of Cancer Patients during the COVID-19 Pandemic: A Cross-Sectional Study. J Psychosoc Oncol Res Pract 2023, 5. [Google Scholar] [CrossRef]
- Ng, D.W.L.; Chan, F.H.F.; Barry, T.J.; Lam, C.; Chong, C.Y.; Kok, H.C.S.; Liao, Q.; Fielding, R.; Lam, W.W.T. Psychological Distress during the 2019 Coronavirus Disease ( <scp>COVID</Scp> -19) Pandemic among Cancer Survivors and Healthy Controls. Psychooncology 2020, 29, 1380–1383. [Google Scholar] [CrossRef]
- Nekolaichuk, C.L.; Cumming, C.; Turner, J.; Yushchyshyn, A.; Sela, R. Referral Patterns and Psychosocial Distress in Cancer Patients Accessing a Psycho-Oncology Counseling Service. Psychooncology 2011, 20, 326–332. [Google Scholar] [CrossRef]
- Steginga, S.K.; Campbell, A.; Ferguson, M.; Beeden, A.; Walls, M.; Cairns, W.; Dunn, J. Socio-Demographic, Psychosocial and Attitudinal Predictors of Help Seeking after Cancer Diagnosis. Psychooncology 2008, 17, 997–1005. [Google Scholar] [CrossRef]
- McFarland, D.C.; Jutagir, D.R.; Miller, A.; Nelson, C. Physical Problem List Accompanying the Distress Thermometer: Its Associations with Psychological Symptoms and Survival in Patients with Metastatic Lung Cancer. Psychooncology 2020, 29, 910–919. [Google Scholar] [CrossRef]
- Büttner-Teleagă, A.; Kim, Y.-T.; Osel, T.; Richter, K. Sleep Disorders in Cancer—A Systematic Review. Int J Environ Res Public Health 2021, 18, 11696. [Google Scholar] [CrossRef]
- Ownby, K.K. Use of the Distress Thermometer in Clinical Practice. J Adv Pract Oncol 2019, 10, 175–179. [Google Scholar]
- Jacobsen, P.B.; Donovan, K.A.; Trask, P.C.; Fleishman, S.B.; Zabora, J.; Baker, F.; Holland, J.C. Screening for Psychologic Distress in Ambulatory Cancer Patients. Cancer 2005, 103, 1494–1502. [Google Scholar] [CrossRef] [PubMed]
- Jewett, P.I.; Teoh, D.; Petzel, S.; Lee, H.; Messelt, A.; Kendall, J.; Hatsukami, D.; Everson-Rose, S.A.; Blaes, A.H.; Vogel, R.I. Cancer-Related Distress: Revisiting the Utility of the National Comprehensive Cancer Network Distress Thermometer Problem List in Women With Gynecologic Cancers. JCO Oncol Pract 2020, 16, e649–e659. [Google Scholar] [CrossRef]
- Pereira, M.; Ribeiro, C.; Ferreira, G.; Machado, J.C.; Leite, Â. The Indirect Effect of Body Image on Distress in Women with Breast Cancer Undergoing Chemotherapy. Health Psychol Rep 2022, 10, 47–57. [Google Scholar] [CrossRef]
- Distress Management Clinical Practice Guidelines in Oncology. Journal of the National Comprehensive Cancer Network 2003, 1, 344. [CrossRef] [PubMed]
Figure 1.
Prevalence of emotional distress, considering the five Emotion Thermometers: distress, anxiety, depression, anger, and need for help.
Figure 1.
Prevalence of emotional distress, considering the five Emotion Thermometers: distress, anxiety, depression, anger, and need for help.
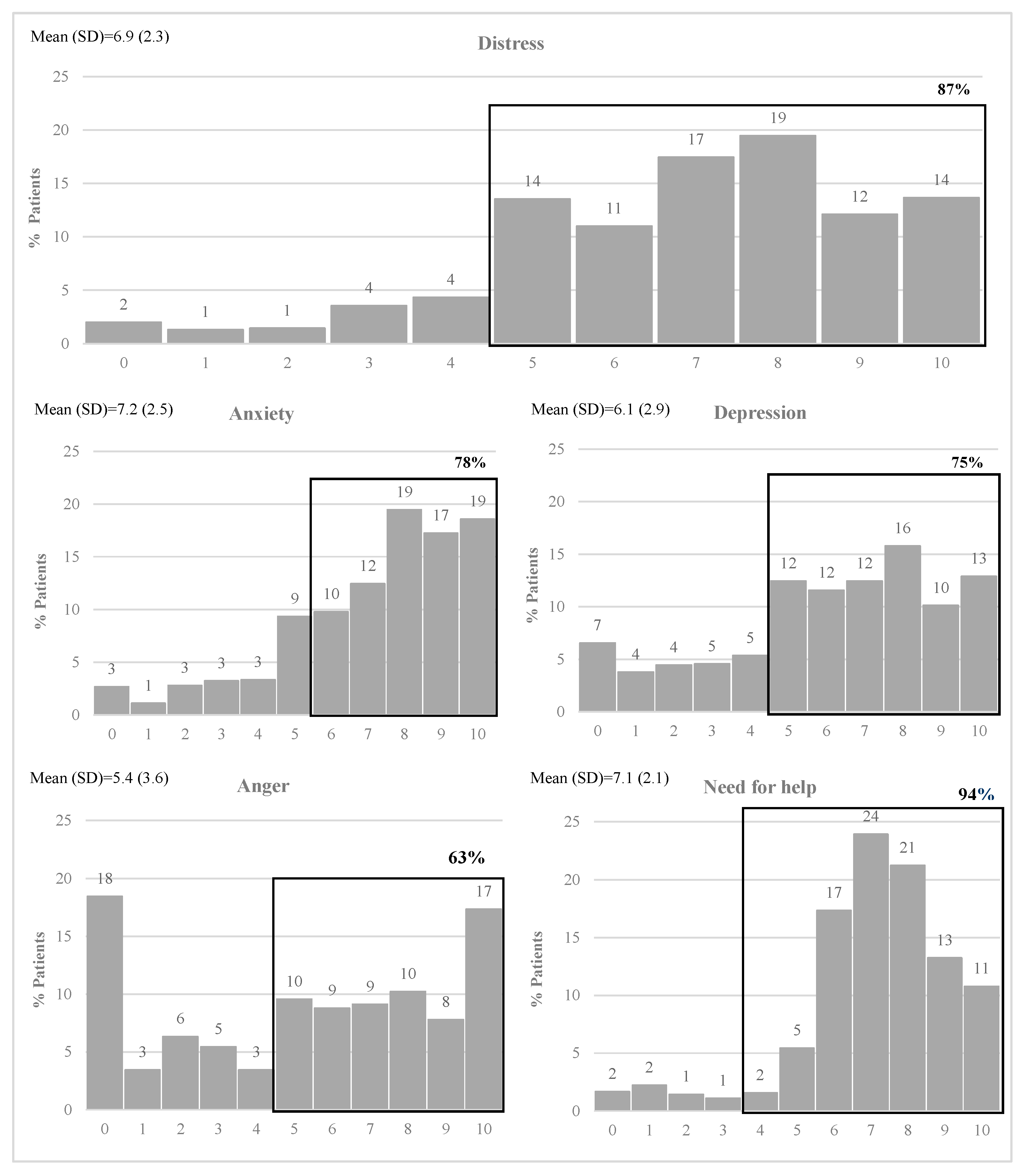
Figure 2.
Prevalence of each problem type.
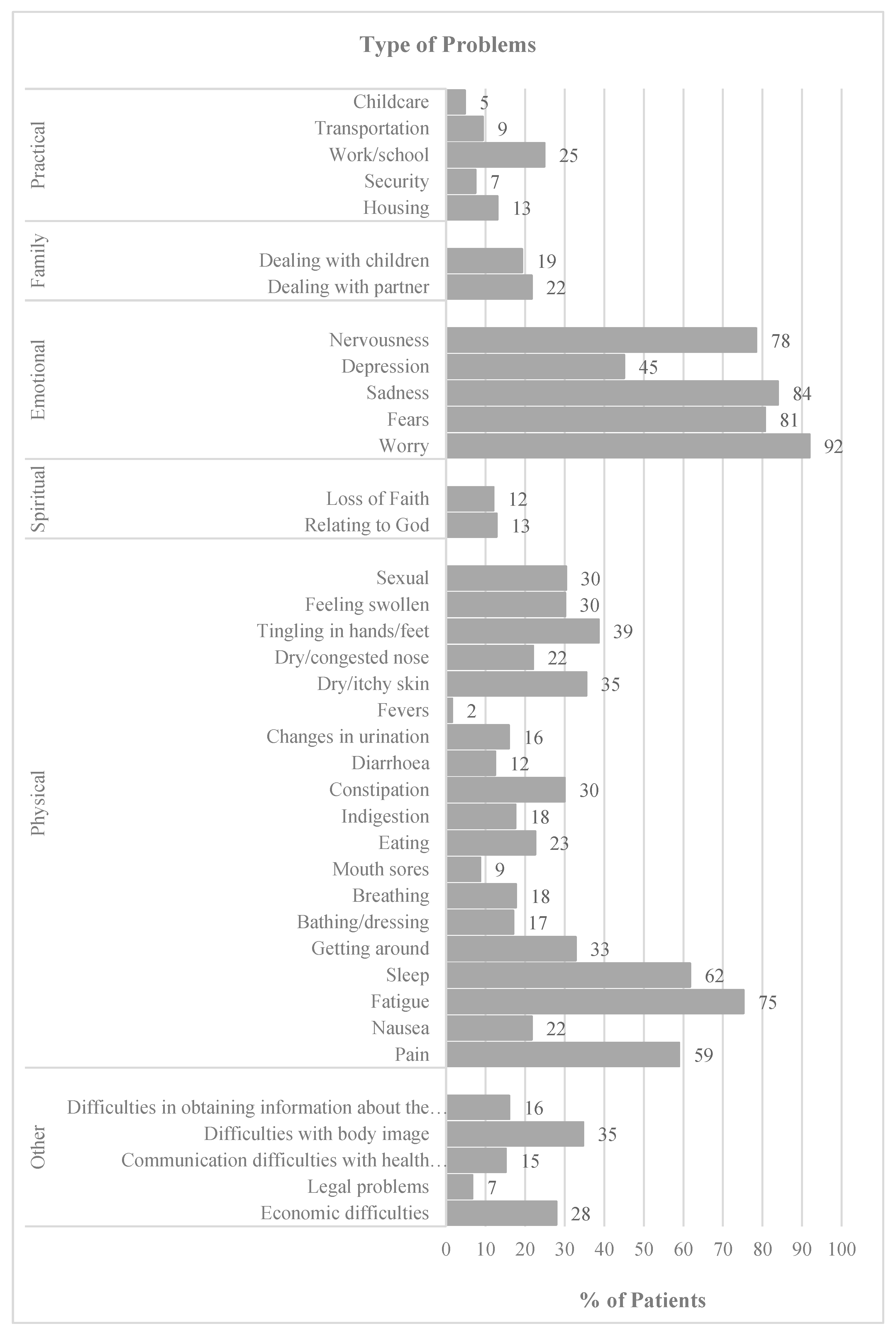
Figure 3.
Predicted margins of the generalized linear model, for the relationship between covariates and distress.
Figure 3.
Predicted margins of the generalized linear model, for the relationship between covariates and distress.
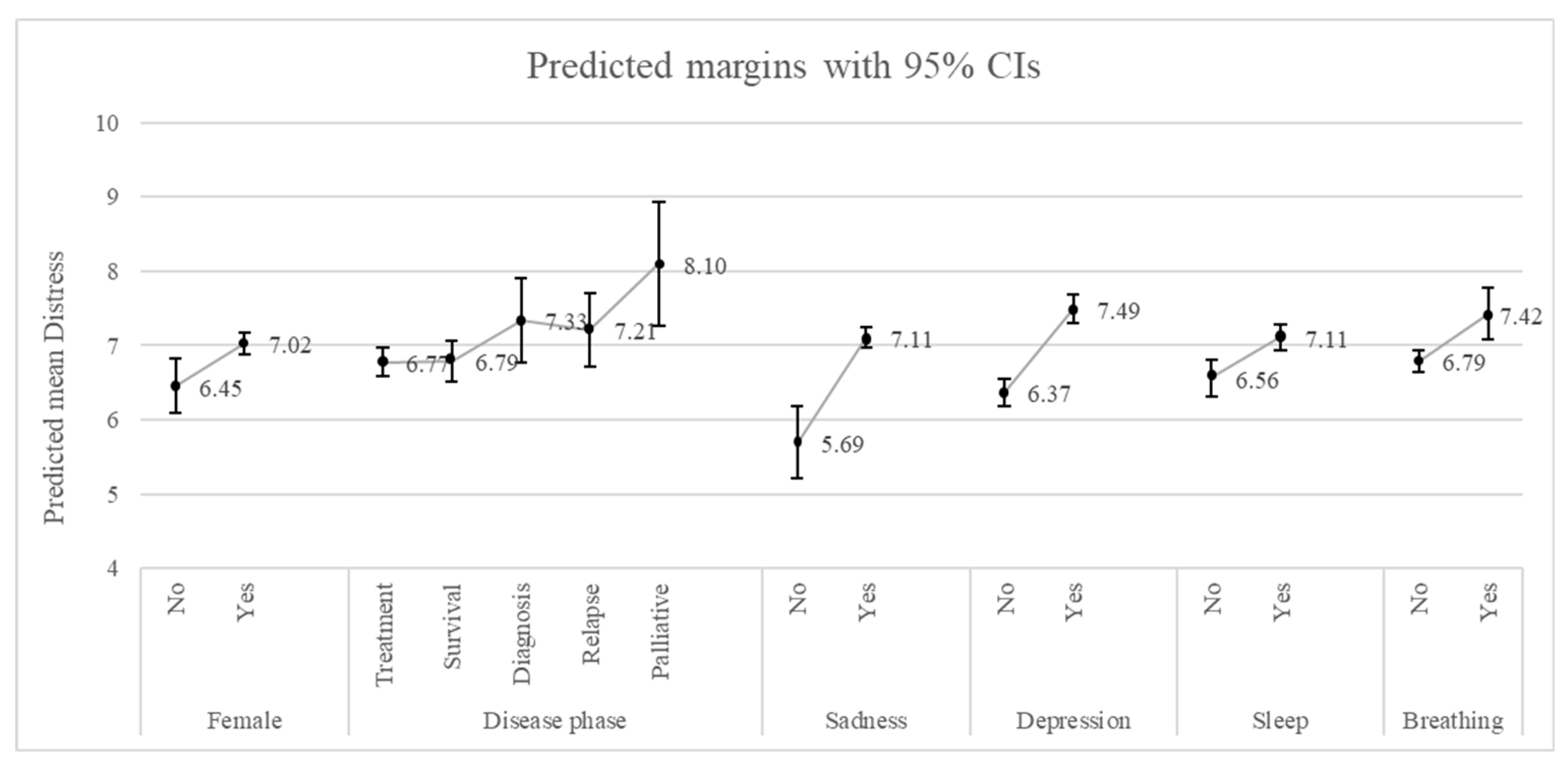

Table 1.
Patients’ demographics and clinical characteristics.
| Characteristic | Patients n=899 N (%) |
|---|---|
| Demographics | |
| Age [mean (SD)] | 59.9 (12.6) |
| Female | 712 (79.2) |
| Disease phase | |
| Treatment | 438 (48.7) |
| Survival | 291 (32.4) |
| Diagnosis | 80 (8.9) |
| Relapse | 53 (5.9) |
| Palliative | 37 (4.1) |
| Type of Cancer | |
| Breast | 456 (50.7) |
| Colorectal | 74 (8.2) |
| Lung | 50 (5.6) |
| Lymphoma | 42 (4.7) |
| Brain | 27 (3.0) |
| Stomach | 24 (2.7) |
| Thyroid | 22 (2.5) |
| Pancreatic | 17 (1.9) |
| Ovaries | 16 (1.8) |
| Multiple myeloma | 16 (1.8) |
| Prostate | 15 (1.7) |
| Leukaemia | 13 (1.5) |
| Cervical | 12 (1.3) |
| Other | 115 (12.8) |
Table 2.
Generalized linear model results for the relationship between patient characteristics and problem list, and distress.
Table 2.
Generalized linear model results for the relationship between patient characteristics and problem list, and distress.
| Distress | ||
| Marginal effect | Std. Err. | |
| Demographics | ||
| Female | 0.57*** | 0.21 |
| Disease phase | ||
| Treatment | Ref. | |
| Survival | 0.02 | 0.18 |
| Diagnosis | 0.56 | 0.31 |
| Relapse | 0.44 | 0.28 |
| Palliative | 1.33*** | 0.45 |
| Emotional | ||
| Sadness | 1.42*** | 0.27 |
| Depression | 1.13*** | 0.15 |
| Physical | ||
| Sleep | 0.55*** | 0.17 |
| Breathing | 0.63*** | 0.20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



