
Submitted:
13 July 2023
Posted:
14 July 2023
You are already at the latest version
Abstract
Background: The standard surgical approach to amputation has failed to evolve significantly over the past century. Consequently, standard amputations often fall short with regards to improving the quality-of-life (QoL) for patients. A modified amputation has been designed at both the transtibial (TTA) and transfemoral (TFA) level that incorporates agonist-antagonist myoneural interface (AMI) constructs to provide patients with a novel alternative to standard amputation. Here, we present the patient reported outcome measures (PROMs) amongst our lower extremity AMI amputees and demonstrate an overall significant improvement in their physical and mental wellbeing.
Methods: Four PROMs surveys, 1) EQ-5D-3L, 2) Lower Extremity Functional Scale (LEFS), 3) PROMIS-57, 4) Short Form-36 (SF-36), and 5) Sickness Impact Profile (SIP), were administered to lower extremity AMI amputees pre-operatively (baseline) and at 6 weeks, 3 months, 6 months, 9 months, 12 months, 24 months, 36 months, and 48 months post-operatively between June 24th, 2018, and December 15th, 2022. The surveys were either administered during a clinic visit or emailed at the encounter timepoint. Study data was collected and managed using REDCap (Research Electronic Data Capture) electronic data capture tools hosted at Brigham and Women’s Hospital. Analyses of collated data were performed by fitting a linear mixed model using SAS version 9.4 (SAS Institute, Cary, NC).
Results: The cohort’s baseline and 12-month post-operative responses were compared to determine score improvement. The cohort demonstrated a significantly improved EQ-5D-3L index value (p<0.0001) and EQ VAS (p<0.0001) at 12-months post-operatively (n=22) when compared to baseline (n=28). The LEFS score significantly improved at 12-months post-operatively compared to baseline (p<0.0001) with a mean of 59.04 ± 3.14 (SE) at 12-months and a mean of 31.96 ± 2.84 (SE) at baseline. AMI patients demonstrated significantly improved scores across PROMIS-57 domains at 12-months compared to baseline scores; the p-value was <0.0001 for all domains except for the Depression domain where p=0.0181. The health domain scores significantly improved from baseline to 12-months post-operation for all SF-36 domains. Lastly, the SIP indicated a significant decrease in overall dysfunction from baseline to 12-months post-operation (p<0.0001).
Conclusions: Modified lower extremity amputation with AMI construction has the potential to provide amputees with increased quality-of-life when compared to the pre-operative state. However, further investigation is necessary to determine whether the patient reported outcome measures of the AMI amputee cohort are superior to those who receive a standard amputation.
Keywords:
Transtibial amputation
; transfemoral amputation
; agonist-antagonist myoneural interface
; AMI
; proprioception
; neural interface
; functional limb restoration
; patient reported outcomes
1. Introduction
Major limb amputation is typically framed as a debilitating consequence of failed limb salvage that results in poor health-related quality of life (QoL) amongst patients.1 However, the standard method of lower extremity amputation continues to be utilized, yet often fails to meet patients’ expectations of modern medicine. Studies demonstrate that patients with standard lower limb amputations often struggle with chronic neuropathic pain.2,3 Residual and phantom limb pain (RLP, PLP) have been shown to negatively impact an amputee’s quality of life (QoL).2,4–6 Consequently, QoL is an important outcome when evaluating the efficacy of novel methods of amputation that aim to mitigate post-operative chronic pain.
For centuries, the standard surgical approach of major limb amputation has not been subject to significant innovation. In the past two decades, however, several neuroma prevention and amelioration procedures such as regenerative peripheral nerve interface (RPNI) construction and targeted muscle reinnervation (TMR). RPNI and TMR have been shown to mitigate RLP/PLP in the setting of lower extremity amputation.7–9 While utilizing these neuroma prevention methods at the time of amputation may alleviate the negative impacts of phantom and residual limb pain on QoL, QoL could also be disrupted by other factors such as loss of proprioception, which may result in functional limitations.5
In recognition of this fact, we have developed the agonist-antagonist myoneural interface (AMI). The AMI is a surgical construct that involves the biomechanical coaptation of muscles at the time of amputation that have an agonist-antagonist relationship in the uninjured state. Volitional activation of the agonist muscle results in its contraction and simultaneous stretch of its paired antagonist; this, in turn, stimulates native biomechanical receptors in the constituent muscles that transmit joint position sense information to the brain. The intended consequence of this transmission is the preservation or restoration of limb proprioception through the recapitulation of native neural loops between the peripheral and central nervous systems.10–22
Since developing the AMI, we have incorporated its design into modified amputation procedures in both the lower and upper extremities. Our goal in exploring these modified amputation procedures has been to not only provide patients with minimized pain but also improve functionality through restoring proprioception. It has been our hope that the combination of reduced pain and improved functionality may offer patients undergoing these procedures significantly enhanced QoL. The purpose of this investigation was to test this hypothesis in our modified lower extremity amputation patient cohort.
2. Patients and Methods
Patient Selection
Patients were recruited for enrollment between June 2018 and June 2022 under Mass General Brigham (MGB) Institutional Review Board (IRB)-approved protocol 2014P001379. Eligible patients were those between the age of 18 and 65 who were candidates for elective lower extremity amputation due to prior traumatic injury, congenital abnormality, or malignancy. Exclusion criteria included those with severe illness rendering them unable to undergo the operative procedure safely, impairment in inherent wound healing pathways, and extensive peripheral neuropathies. Active smokers and pregnant women were excluded.
Surgical Technique
The surgical technique of a modified amputation utilizing agonist-antagonist myoneural interface (AMI) construction has previously been described.13 In summary, two AMI constructs were built in a transtibial amputation (TTA), and three AMI constructs were built in a transfemoral amputation (TFA): 1) in an TFA, a knee joint emulator via coaptation of the biceps femoris and rectus femoris; 2) a tibiotalar joint emulator via coaptation of the lateral gastrocnemius and tibialis anterior; and 3) a subtalar joint emulator via coaptation of the tibialis posterior and peroneus longus. The medial and lateral tarsal tunnels from the amputated leg served as coaptation points for the AMI constructs; the tunnels were procured via our previously described technique. As a preventative measure for post-amputation neuropathic pain, RPNIs were subsequently constructed at the distal end of each isolated sensory nerve via standard technique.
Patient Reported Outcome Measures Instruments
Subjects completed four surveys at nine time points throughout their enrollment: pre-operatively, 6 weeks, 12 weeks, 6 months, 9 months, 12 months, 24 months, 36 months, and 48 months post-operatively. The surveys were administered using REDCap (Research Electronic Data Capture) electronic data capture tools hosted at Brigham & Women’s Hospital (BWH). REDCap is a secure, web-based software platform designed to support data capture for research studies, providing an intuitive interface for validated data capture. All surveys have been previously validated for assessment of patients with lower extremity injuries and/or amputations. Descriptions of the surveys utilized are as follows:
The EQ-5D-3L consists of five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has three levels: no problems (1), some problems (2), and extreme problems (3). The response to each dimension results in a five-number health state (e.g., 12312) that is transformed into an index value from 0-1. A higher index value indicates a better health state. Respondents also designate their overall health state according to a Visual Analogue Scale (VAS) on a 0- to 100-point scale where 0 indicates worst health state imaginable and 100 indicates best health state imaginable.23,24
The Lower Extremity Functional Scale (LEFS) consists of 20 questions and is scored on a scale of 0-80 points with a higher score indicating higher functionality.25
The PROMIS-57 is a collection of short forms assessing seven PROMIS domains (Depression, Anxiety, Physical Function, Pain Interference, Fatigue, Sleep Disturbance, and Ability to Participate in Social Roles and Activities) with 8 questions per domain. Each domain yields a T-score metric with the mean of the US general population equal to 50 ± 10. In the domains of Pain Interference, Fatigue, Anxiety/Depression, Sleep Disturbance, and Depression/Sadness, a higher score indicates that the patient is more likely to have a negative outcome within that domain. In the domains of Physical Function and Ability to Participate in Social Roles and Activities, a higher score indicates that the patient is more likely to have a positive outcome within that domain.26,27
The Short-form 36 (SF-36) is a 36-item short form designed to assess eight health domains for the purpose of evaluating a patient’s health-related quality of life. The health domains include physical functioning, role limitations due to physical health, role limitations due to emotional problems, energy/fatigue, emotional well-being, social functioning, pain, and general health. The eight health domain scores can be summarized by a physical and mental component score (PCS, MCS). The PCS and MCS are calculated as a weighted sum of all eight domain scores. However, the PCS heavily weighs Physical Functioning, Role Limitations Due to Physical Health, Pain, General Health, and Energy/Fatigue. Conversely, the MCS heavily weighs Social Functioning, Role Limitations Due to Emotional Problems, and Emotional Well-being.28–30
The Sickness Impact Profile (SIP) is a 136-item questionnaire designed to assess a patient’s general dysfunction amongst 12 categories including sleep and rest, eating, work, home management, recreation and pastimes, ambulation, mobility, body care and movement, social interaction, alertness behavior, emotional behavior, and communication. An overall dysfunction score is calculated where the score ranges from 0-100%. A lower score indicates less dysfunction.31
Scoring and Statistical Analysis
Scoring of each survey was performed according to the standard method outlined by the survey developers.23–31 To maximize efficiency and minimize errors, the primary author (RBC) wrote MATLAB programs to score the EQ-5D-3L, SF-36, and SIP survey data, as described below. The scores produced by the MATLAB programs were cross-referenced with manual calculations to confirm reliability and validity. LEFS survey data was scored using basic Microsoft Excel functions as the LEFS score is a simple summation based on the respondent’s selections. PROMIS-57 survey data was scored through the Health Measures Scoring Service, which is a validated application through the National Institutes of Health.
Univariate analysis for all patient reported outcome measures included an assessment of skewness, kurtosis, and variance. Differences in outcomes from baseline (pre-operative) to 12-months post-amputation were assessed by a paired two-sample t-test. A two-sided p-value of 0.05 was considered statistically significant. Because of the rebated measures on the same patient, a linear mixed model was fitted to the data to estimate the mean at each time point. The mixed model approach protects against biases caused by sicker (or less sick) patients seen more often over time.32 Statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
MATLAB Procedures
MATLAB version R2022b was used to run the scripts written by the primary author (RBC), which can be found within the appendix. Survey responses were exported from REDCap into Microsoft Excel files as raw data, and any questions left blank were exported as empty cells. The numbers that are coded within REDCap to represent each survey response choice can be set by the REDCap form creator and thus may vary between users. A separate Microsoft Excel file was created for each survey. Each respondent was allocated nine rows with each row designated for the survey data from each of the nine timepoints. The first column designated the respondent’s ID. The second column designated the timepoint. The number of additional columns varied based on the number of survey questions asked.
EQ-5D-3L Valuation. The Microsoft Excel file containing the raw EQ-5D-3L data was uploaded and converted to a MATLAB cell as string arrays, and the script then parsed through the data searching for empty cells and replaced the empty cells with zeroes. The string arrays were then converted to numerical data types so that computational functions could subsequently be used. A preallocated cell array was prepared to store the data necessary to calculate the EQ-5D-3L index value. The script then parsed through each row to create a 5-item vector that represented the EQ-5D-3L health state which was stored in the pre-allocated cell array. The index value was calculated by deducting the appropriate weights from 1, the value for a full health state (11111). The amount deducted was based upon the statistical model used to generate the US population-based valuation of the EQ-5D health states.24 The model deducted variable weights depending on which level the 2 or 3 was reported in as well as the number of 2s or 3s reported in the health state. The script then ran through a series of “elseif” statements that parsed the health state for various conditions and deducted the appropriate weight from 1 accordingly. The resulting index value, ranging from 0 to 1, was stored in a new cell and was exported as a Microsoft Excel file.
SF-36 Physical and Mental Component Scores Valuation. The Microsoft Excel file containing the raw SF-36 data was uploaded and converted to a MATLAB cell as string arrays and the script then parsed through the data searching for empty cells and replaces the empty cells with zeroes. The string arrays were converted to numerical data types so that computational functions could subsequently be used. The script parsed through the data to replace the survey responses with the appropriate weighted score, determined by “elseif” statements, set by the survey developers.28,29 Subsequently, the recoded data was exported to a Microsoft Excel file. The survey developers require a complex procedure to provide a score for missing item responses, so the author recoded missing items manually. After the missing items were recoded, the updated file was uploaded into MATLAB, ensuring that the data was converted back to a numeric data type. The SF-36 contains sub-scores, including Physical Functioning, Role Limitations due to Physical Health, Bodily Pain, General Health, Vitality, Social Functioning, Role Limitations Due to Emotional Health, and Mental Health. There are 36 survey questions, each of which apply to a specific sub-score. The script pre-allocated a cell for each sub-score. For each sub-score, the summation of the required recoded survey responses was calculated and stored. If more than half of the sub-score’s items were unanswered, then the script did not calculate the sub-score for that respondent and left an empty cell. Summary scores as well as physical and mental health component scores can be calculated and are often reported in literature. The script calculated the physical and mental health component scores according to the procedure detailed by the survey developers. First, the sub-scores were normalized amongst the respondents and transformed to a 0 to 100 scale. A Z-score standardization was then performed on the transformed scores. The standardized scores were aggregated into the physical and mental health component scores through a weighted summation of the standardized sub-scores. Lastly, a T-score transformation of the aggregated physical and mental health component scores was performed. The resulting scores were stored and exported as a Microsoft Excel file.
SIP Dysfunction Score Valuation. The Microsoft Excel file containing the raw SIP data was uploaded and converted to a MATLAB cell as string arrays, and the script then parsed through the data searching for empty cells and replaced the empty cells with zeroes. The string arrays were converted to numerical data types so that computational functions could subsequently be used. In the SIP raw data, items that are “checked” signify the presence of that item and export with a value of 1. “Unchecked” items export with a value of 2. The script parsed through the raw data and replaced 1s with the appropriate scaled value set by the survey developers and replaced 2s with zero using “elseif” statements.31 The scaled scores were then summated for each respondent and stored within a new cell. A transformation set forth by the survey developers was then applied to the summed score to obtain the dysfunction score. The dysfunction score was stored and exported as a Microsoft Excel file.
3. Results
Baseline Characteristics
Of the 37 patients enrolled, 31 patients completed at least one full survey set at one timepoint. One patient was excluded from data analysis due to a concern for confounding variables as she received a bilateral below-knee amputation in two separate procedures. Our final cohort comprised 34 limbs from 31 patients. Of the 31 patients, 3 patients underwent a bilateral below-knee amputation, 6 patients underwent a unilateral above-knee amputation, and 22 patients underwent a unilateral below-knee amputation. The mean age at the time of surgery was 42.5 ± 11.1. 66% (20 of 31) of the patients were men and 94% (29 of 31) were self-reported white. The most common etiology was trauma (19 of 31). (Table 1)
EQ-5D-3L
By 12-months post-amputation, EQ-5D-3L index values significantly improved from 0.49 ± 0.034 (SE) to 0.85 ± 0.037 (SE) (mean difference 0.36 [95% CI 0.27 to 0.45]; p<0.0001). Similarly, patients’ VAS scores significantly increased at one-year post-amputation from 56.67 ± 3.26 (SE) to 81.09 ± 3.59 (SE) (mean difference 24.42 [95% CI 15.66 to 33.19]; p<0.0001). (Figure 1)
LEFS
Patients demonstrated a significant improvement in LEFS score from baseline, 32.0 ± 2.8 (SE), to 12-months post-amputation, 59.0 ± 3.1 (SE) (mean difference 27.1 [95% CI 20.5 to 33.6]; p<0.0001). (Figure 2)
PROMIS-57
A higher PROMIS T-score indicates more of the concept being present, which can have positive or negative indications depending on the concept. For example, a higher Pain Interference T-score indicates a negative change, a higher Physical Function T-score indicates a positive change.26 AMI patients demonstrated an improvement in PROMIS Pain Interference scores, which decreased from 65.9 ± 1.5 (SE) to 50.1 ± 1.7 (SE) (mean difference -15.7 [95% CI -19.9 to -11.5]; p<0.0001). PROMIS Ability to Participate in Social Roles/Activities scores similarly improved with a mean score increase from 37.7 ± 1.6 (SE) to 52.5 ± 1.8 (SE) (mean difference 14.82 [95% CI 11.1 to 18.6]; p<0.0001). PROMIS Physical Function scores improved with a score increase of 33.8 ± 1.6 to 46.6 ± 1.7 (mean difference 12.8 [95% CI 9.3 to 16.2]; p<0.0001). There was a significant improvement in the PROMIS Fatigue score with a score decrease from 57.0 ± 1.8 (SE) to 44.4 ± 2.0 (SE) (mean difference -12.6 [95% CI -16.3 to -8.8]; p<0.0001). PROMIS Anxiety/Fear scores improved and demonstrated a decrease from 54.3 ± 1.8 (SE) to 46.3 ± 2.0 (SE) (mean difference -8.0 [95% CI -11.9 to -4.2]; p<0.0001). PROMIS Sleep Disturbance scores also improved with a decrease from 57.1 ± 1.6 (SE) to 48.2 ± 1.7 (SE) (mean difference -8.9 [95% CI -12.8 to -4.9]; p<0.0001). Lastly, the PROMIS Depression/Sadness domain demonstrated less significance than the other PROMIS domains with a decrease from 49.9 ± 1.5 (SE) to 46.1 ± 1.6 (SE) (mean difference -3.8 [95% CI -7.0 to -0.7]; p=0.0181). (Figure 3 and Figure 4)
SF-36
AMI patients demonstrated a significant improvement with a score increase across all SF-36 sub-scores as well as the aggregate Physical and Mental Component Scores (PCS, MCS) from baseline to 12-months post-amputation. The mean Physical Functioning score increased from 29.2 ± 4.9 (SE) to 70.4 ± 5.4 (SE) (mean difference 41.2 [95% CI 30.3 to 52.2]; p<0.0001). The Role Limitations Due to Physical Health score increased from 11.4 ± 7.0 (SE) to 46.3 ± 7.9 (SE) (mean difference 35.0 [95% CI 16.6 to 53.3]; p=0.0002). The Role Limitations Due to Emotional Problems score increased from 55.6 ± 6.5 (SE) to 84.3 ± 7.4 (SE) (mean difference 28.8 [95% CI 11.0 to 46.5]; p=0.0017). The Energy/Fatigue score increased from 43.1 ± 4.0 (SE) to 67.9 ± 4.4 (SE) (mean difference 24.8 [95% CI 16.0 to 33.6]; p<0.0001). The Emotional Well-being score increased from 66.8 ± 3.2 (SE) to 80.2 ± 3.5 (SE) (mean difference 13.3 [95% CI 6.6 to 20.1]; p=0.0001). The Social Functioning score increased from 45.8 ± 4.6 (SE) to 81.1 ± 5.2 (SE) (mean difference 35.3 [95% CI 23.4 to 47.1]; p<0.0001). The Pain score increased from 30.1 ± 4.1 (SE) to 70.0 ± 4.6 (SE) (mean difference 39.9 [95% CI 29.2 to 50.5]; p<0.0001). The General Health score increased from 54.1 ± 4.3 (SE) to 72.1 ± 4.7 (SE) (mean difference 18.0 [95% CI 10.4 to 25.6]; p<0.0001). The aggregate Physical Component Score (PCS) increased from 26.4 ± 1.8 (SE) to 43.3 ± 2.0 (SE) (mean difference 16.9 [95% CI 12.7 to 21.1]; p<0.0001). The aggregate Mental Component Score (MCS) increased from 48.0 ± 1.9 (SE) to 55.1 ± 2.1 (SE) (mean difference 7.1 [95% CI 2.5 to 11.7]; p=0.0028). (Figure 5)
SIP
Patients demonstrated a significant improvement in SIP dysfunction scores from baseline, 18.8 ± 3.0 (SE), to 12-months post-amputation, 5.1 ± 0.7 (SE) (mean difference -13.7 [95% CI -17.5 to -9.9]; p<0.0001).
Figure 6.
Mean SIP dysfunction scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation including standard error bars.
Figure 6.
Mean SIP dysfunction scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation including standard error bars.
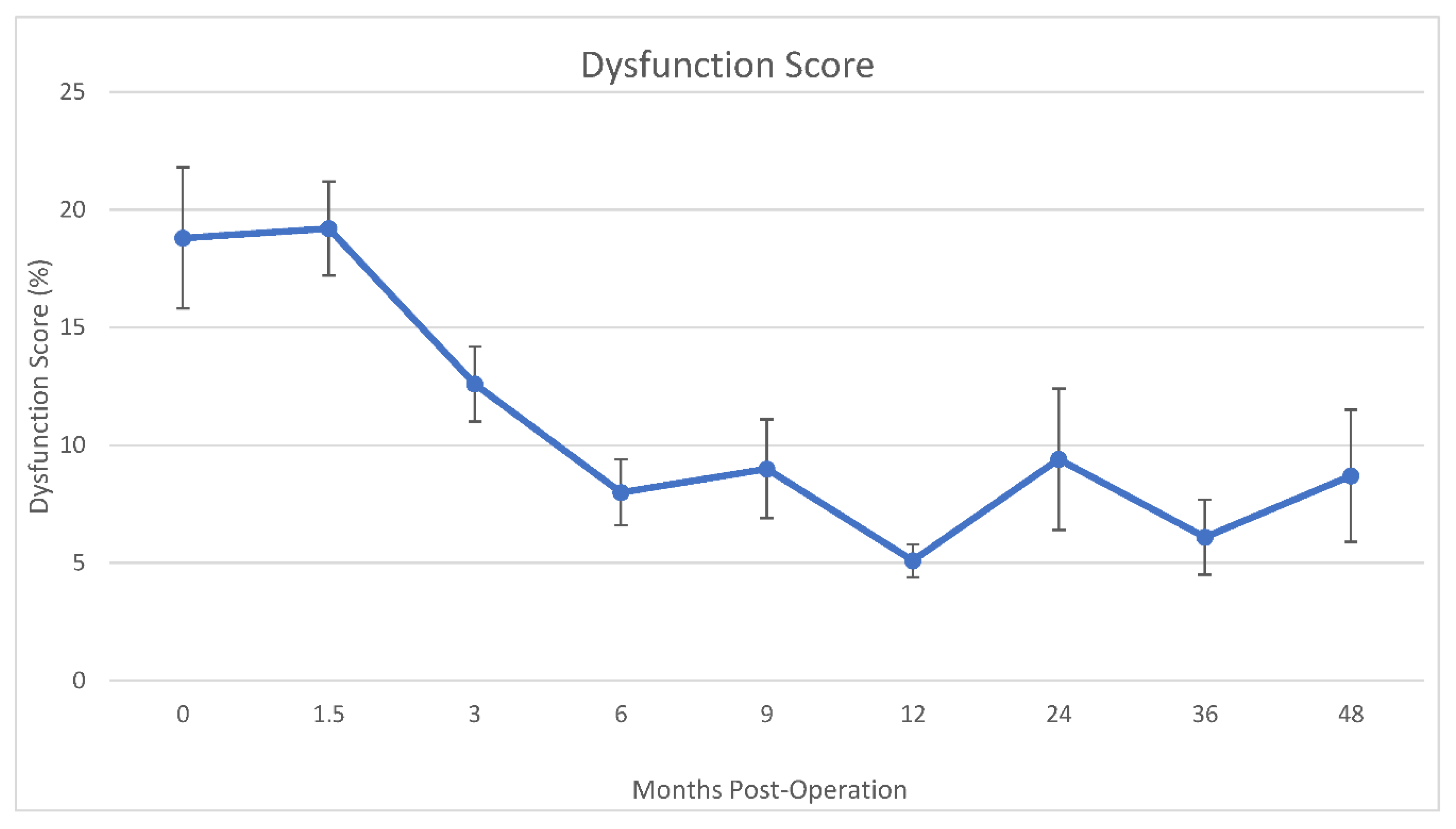
Only a fraction of the patient cohort has completed surveys beyond 12-months post-operation, with 48.4% (15 out of 31) completion at 24-months, 6.5% (2 out of 31) completion at 36-months, and 16.1% (5 out of 31) completion at 48-months. While significance is not noted amongst all annual timepoints compared to baseline, significant improvements at these annual timepoints are demonstrated within certain surveys and sub-scores which can be found within the appendix.
4. Discussion
Our study assessed a wide range of factors that influence a patient’s quality of life including less reported factors such as emotional health, fatigue, anxiety/depression, and social functioning. AMI amputees demonstrated significant improvements across all surveys and sub-scores 12-months post-amputation within both physical and mental health domains. These results support the notion that the modified AMI amputation at both the transtibial and transfemoral level can meaningfully improve patients’ quality of life compared to their pre-operative state.
Compared to patients’ pre-operative baseline, all eight health domains and component scores of the SF-36 significantly improved at 12-months post-amputation, suggesting that the AMI amputation provides a multidimensional improvement to patients’ quality of life beyond the commonly reported outcome measures of pain and physical functioning.9,33–35 The Physical Component Score had a greater mean increase than the Mental Component Score, which could indicate that the AMI procedure has a more substantial positive impact on patients’ post-operative physical health versus their mental health.
While results at time points other than baseline and 12-months post-operation were not explicitly discussed, it is pertinent to note that a significant improvement was demonstrated at 3-months, 6-months, and 9-months post-operation compared to baseline amongst all surveys and their sub-scores (Appendix Table A1, Table A2, Table A3, Table A4 and Table A5). Furthermore, significant improvements appear to persist in patients’ annual survey responses at 24-months, 36-months, and 48-months post-operation (Figure 1, Figure 2, Figure 3, Figure 4, Figure 5 and Figure 6). However, only a minority of our patient cohort has reached these annual timepoints. Conclusions should not be drawn from the annual outcomes at this time, although the initial results are promising.
Further investigation is necessary to determine what factors correlate with the demonstrated outcomes. While the paper is currently in press, our team has also demonstrated significantly improved functionality based on physical therapy functional outcome measures. Based on the results of this investigation, we postulate a positive correlation between functional outcomes and PROMs scores. Furthermore, the presence of residual limb pain and phantom limb pain is considered an important post-operative outcome in the setting of amputation;36,37 multivariate analysis would be required to determine the impact of residual and phantom limb pain on our results.
Limitations of this study include the possibility of bias due to patient self-reporting as well as patients’ high expectations based on media coverage and publicly accessible literature regarding the novelty and promise of the AMI amputation procedure. It is also important to note that all patients in our cohort underwent elective amputations due to chronic pain from past trauma, congenital disorders, or vascular disorders, and often sought out our clinical trial as a last resort following other limb salvage attempts. An additional source of bias could arise because the senior author (MJC) played a significant role in the development of the modified AMI amputation. Last, our results prompt us to ask the question of how our cohort’s outcomes compare to those from other amputation techniques (e.g., standard amputation, amputation with TMR, amputation with RPNI) and limb salvage procedures (e.g., fusion, joint replacement, tissue/nerve reconstruction). A comparison of PROMs data between these procedures is key to determining whether the AMI amputation provides patients with a superior option with regards to optimizing their quality of life.
5. Conclusions
This study demonstrated that lower extremity AMI amputation procedures are associated with significant improvements in patients’ day-to-day lives and emotional wellbeing. Additional research is necessary to determine what factors (e.g., functionality, absence of residual/phantom limb pain) contribute to the demonstrated improvements as well as how our results compare to those from other studies involving other amputation techniques and limb salvage procedures.
Funding Sources
This work was supported by the Department of Defense CDMRP/PRORP OR180114 and the BWH Stepping Strong Center for Trauma Innovation.
Institutional Review Board Statement
This work was performed under the auspices of Mass General Brigham IRB-approved protocol 2014P001379
Informed Consent Statement
Written informed consent was obtained from all patients for publication of this case series and accompanying images. Copies of the written consent forms are available for review by the Editor-in-Chief of this journal on request.
Acknowledgments
The authors would like to thank the Brigham and Women’s Hospital Stepping Strong Center for Trauma Innovation and the United States Department of Defense for their generous ongoing support of the work described in this publication.
Conflict of Interest Statement
None of the participating authors maintains a financial stake in any product, device or drug cited in this report. Drs. Carty and Sparling, as well as Ms. Chiao, Ms. Berger, Mr. Sullivan, Mrs. Clites and Mrs. Landry, all receive partial salary support through the funding agencies listed below.
Appendix

Table A1.
EQ-5D-3L scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation, mean (SE), with the change from each timepoint to baseline.
Table A1.
EQ-5D-3L scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation, mean (SE), with the change from each timepoint to baseline.
| EQ-5D-3L parameter | 0 | 1.5 | 3 | 6 | 9 | 12 | 24 | 36 | 48 |
|---|---|---|---|---|---|---|---|---|---|
| N | 27-28 | 23-24 | 23-24 | 22 | 22 | 22 | 14 | 4 | 3 |
| Index value | 0.49 (0.03) | 0.65 (0.04) | 0.73 (0.04) | 0.81 (0.04) | 0.77 (0.04) | 0.85 (0.04) | 0.83 (0.05) | 0.87 (0.08) | 0.84 (0.10) |
| Change (95% CI) | - | 0.16 (0.07, 0.24) |
0.24 (0.16, 0.33) |
0.33 (0.24, 0.41) |
0.29 (0.20, 0.37) |
0.36 (0.27, 0.45) |
0.34 (0.24, 0.45) |
0.38 (0.21, 0.55) |
0.35 (0.15, 0.54) |
| p-value | - | 0.0004 | <.0001 | <.0001 | <.0001 | <.0001 | <.0001 | <.0001 | 0.0005 |
| VAS | 56.67 (3.26) | 74.21 (3.51) |
76.33 (3.51) |
83.02 (3.59) |
78.33 (3.59) |
81.09 (3.59) |
84.38 (4.42) |
87.46 (8.03) |
74.23 (9.33) |
| Change (95% CI) | - | 17.54 (8.96, 26.11) |
19.66 (11.05, 28.28) | 26.35 (17.59, 35.12) | 21.67 (12.90, 30.44) | 24.42 (15.66, 33.18) | 27.71 (17.62, 37.81) | 30.79 (14.06, 47.51) | 17.56 (-1.56, 36.69) |
| p-value | - | <.0001 | <.0001 | <.0001 | <.0001 | <.0001 | <.0001 | 0.0004 | 0.0716 |
Table A2.
LEFS scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation, mean (SE), with the change from each timepoint to baseline.
Table A2.
LEFS scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation, mean (SE), with the change from each timepoint to baseline.
| LEFS parameter | 0 | 1.5 | 3 | 6 | 9 | 12 | 24 | 36 | 48 |
|---|---|---|---|---|---|---|---|---|---|
| N | 28 | 24 | 24 | 24 | 22 | 21 | 14 | 4 | 4 |
| LEFS score | 31.96 (2.84) |
33.27 (3.00) |
41.95 (3.04) |
53.63 (3.05) |
54.88 (3.10) |
59.04 (3.14) |
59.55 (3.65) |
58.79 (6.20) |
51.74 (7.22) |
| Change (95% CI) | - | 1.31 (-4.90, 7.52) |
9.99 (3.67, 16.32) |
21.68 (15.32, 28.04) |
22.93 (16.47, 29.38) | 27.09 (20.54, 33.63) |
27.59 (20.11, 35.07) |
26.84 (14.36, 39.31) |
19.78 (5.38, 34.19) |
| p-value | - | 0.6772 | 0.0022 | <.0001 | <.0001 | <.0001 | <.0001 | <.0001 | 0.0075 |
Table A3.
PROMIS T-scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation, mean (SE), with the change from each timepoint to baseline.
Table A3.
PROMIS T-scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation, mean (SE), with the change from each timepoint to baseline.
| SF-36 Component Score | 0 | 1.5 | 3 | 6 | 9 | 12 | 24 | 36 | 48 |
|---|---|---|---|---|---|---|---|---|---|
| N | 28 | 23 | 24 | 24 | 22 | 20 | 15 | 2 | 5 |
| Physical Component Score | 26.39 (1.79) |
26.47 (1.92) |
35.05 (1.89) |
42.74 (1.89) |
41.75 (1.95) |
43.28 (2.02) |
44.01 (2.25) |
37.00 (5.43) |
42.77 (3.59) |
| Change (95% CI) | - | 0.08 (-3.92, 4.08) |
8.66 (4.68, 12.65) |
16.35 (12.35, 20.35) |
15.36 (11.24, 19.48) |
16.90 (12.65, 21.14) |
17.62 (12.97, 22.27) |
10.61 (-0.20, 21.43) |
16.39 (9.17, 23.61) |
| p-value | - | 0.9686 | <.0001 | <.0001 | <.0001 | <.0001 | <.0001 | 0.05 | <.0001 |
| Mental Component Score | 47.99 (1.88) |
53.28 (2.02) |
56.31 (1.99) |
57.19 (1.99) |
54.59 (2.06) |
55.09 (2.13) |
55.95 (2.39) |
58.48 (5.88) |
53.35 (3.87) |
| Change (95% CI) | - | 5.29 (0.93, 9.66) |
8.32 (3.98, 12.66) |
9.21 (4.85, 13.56) |
6.60 (2.11, 11.09) |
7.11 (2.49, 11.72) |
7.96 (2.90, 13.02) |
10.49 (-1.29, 22.26) |
5.36 (-2.49, 13.21) |
| p-value | - | 0.0178 | 0.0002 | <.0001 | 0.0042 | 0.0028 | 0.0023 | 0.0804 | 0.1791 |
Table A4.
SF-36 physical and mental scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation, mean (SE), with the change from each timepoint to baseline.
Table A4.
SF-36 physical and mental scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation, mean (SE), with the change from each timepoint to baseline.
| PROMIS domain | 0 | 1.5 | 3 | 6 | 9 | 12 | 24 | 36 | 48 |
|---|---|---|---|---|---|---|---|---|---|
| N | 28 | 23-24 | 23-24 | 23-24 | 22 | 21 | 14 | 4 | 3-4 |
| Pain Interference | 65.86 (1.52) |
58.55 (1.67) |
55.13 (1.64) |
50.20 (1.67) |
49.52 (1.74) |
50.15 (1.74) |
49.24 (2.10) |
47.25 (3.83) |
53.51 (3.85) |
| Change (95% CI) | - | -7.31 (-11.37, -3.25) |
-10.74 (-14.75, -6.72) |
-15.66 (-19.75, -11.58) |
-16.35 (-20.55, -12.14) |
-15.71 (-19.91, -11.52) |
-16.62 (-21.41, -11.84) |
-18.61 (-26.57, -10.66) |
-12.35 (-20.32, -4.39) |
| p-value | - | 0.0005 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.0026 |
| Ability to Participate in Social Roles/Activities | 37.68 (1.64) |
41.43 (1.76) |
44.54 (1.73) |
53.63 (1.76) |
50.68 (1.79) |
52.50 (1.82) |
54.82 (2.11) |
54.36 (3.58) |
55.20 (3.62) |
| Change (95% CI) | - | 3.75 (0.11, 7.39) |
6.86 (3.26, 10.46) | 15.95 (12.29, 19.62) |
13.00 (9.28, 16.73) |
14.82 (11.05, 18.60) |
17.14 (12.83, 21.45) |
16.68 (9.49, 23.87) |
17.52 (10.28, 24.76) |
| p-value | - | 0.0434 | 0.0003 | <.0001 | <.0001 | <.0001 | <.0001 | <.0001 | <.0001 |
| Physical Functioning | 33.78 (1.57) |
31.03 (1.65) |
37.22 (1.66) |
44.58 (1.66) |
44.75 (1.70) |
46.55 (1.73) |
47.77 (1.99) |
46.29 (3.31) |
46.37 (3.36) |
| Change (95% CI) | - | -2.74 (-6.02, 0.54) |
3.45 (0.15, 6.74) |
10.81 (7.49, 14.11) |
10.97 (7.56, 14.38) |
12.77 (9.32, 16.23) |
14.00 (10.05, 17.94) |
12.51 (5.92, 19.10) |
12.59 (5.95, 19.23) |
| p-value | - | 0.1003 | 0.0405 | <.0001 | <.0001 | <.0001 | <.0001 | 0.0003 | 0.0003 |
| Fatigue | 56.99 (1.81) |
51.14 (1.90) |
48.75 (1.90) |
46.43 (1.90) |
45.55 (1.95) |
44.42 (1.97) |
42.71 (2.24) |
41.98 (3.64) |
54.51 (3.69) |
| Change (95% CI) | - | -5.85 (-9.39, -2.31) |
-8.24 (-11.80, -4.69) |
-10.56 (-14.13, -6.98) |
-11.44 (-15.12, -7.76) |
-12.57 (-16.31, -8.84) |
-14.28 (-18.55, -10.01) |
-15.01 (-22.12, -7.89) |
-2.48 (-9.66, 4.70) |
| p-value | - | 0.0014 | <.0001 | <.0001 | <.0001 | <.0001 | <.0001 | <.0001 | 0.4953 |
| Anxiety/Fear | 54.31 (1.82) |
48.63 (1.91) |
46.94 (1.91) |
44.97 (1.91) |
46.79 (1.96) |
46.30 (1.99) |
46.61 (2.27) |
43.41 (3.73) |
48.60 (3.78) |
| Change (95% CI) | - | -5.68 (-9.33, -2.02) |
-7.37 (-11.04, -3.70) |
-9.34 (-13.03, -5.65) |
-7.52 (-11.32, -3.72) |
-8.01 (-11.86, -4.16) |
-7.70 (-12.10, -3.29) |
-10.90 (-18.25, -3.55) |
-5.71 (-13.12, 1.70) |
| p-value | - | 0.0026 | 0.0001 | <.0001 | 0.0001 | <.0001 | 0.0007 | 0.0040 | 0.1296 |
| Sleep Disturbance | 57.10 (1.55) |
54.98 (1.69) |
49.94 (1.66) |
48.23 (1.69) |
47.61 (1.72) |
48.24 (1.75) |
49.91 (2.07) |
52.34 (3.67) |
53.92 (3.70) |
| Change (95% CI) | - | -2.12 (-5.93, 1.70) |
-7.16 (-10.93, -3.38) |
-8.88 (-12.72, -5.04) |
-9.50 (-13.40, -5.60) |
-8.86 (-12.81, -4.91) |
-7.19 (-11.70, -2.68) |
-4.76 (-12.28, 2.75) |
-3.18 (-10.73, 4.37) |
| p-value | - | 0.2736 | 0.0003 | <.0001 | <.0001 | <.0001 | 0.0020 | 0.2121 | 0.4058 |
| Depression/Sadness | 49.93 (1.50) |
46.72 (1.57) |
44.68 (1.57) |
44.44 (1.57) |
44.55 (1.61) |
46.11 (1.64) |
43.57 (1.87) |
40.29 (3.06) |
44.94 (3.10) |
| Change (95% CI) | - | -3.22 (-6.21, -0.22) |
-5.25 (-8.26, -2.24) |
-5.48 (-8.51, -2.46) |
-5.38 (-8.49, -2.26) |
-3.82 (-6.97, -0.66) |
-6.36 (-9.97, -2.75) |
-9.63 (-15.66, -3.61) |
-4.99 (-11.06, 1.08) |
| p-value | - | 0.0355 | 0.0008 | 0.0005 | 0.0009 | 0.0181 | 0.0007 | 0.0019 | 0.1062 |
Table A5.
SIP dysfunction scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation, mean (SE), with the change from each timepoint to baseline.
Table A5.
SIP dysfunction scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation, mean (SE), with the change from each timepoint to baseline.
| SIP parameter | 0 | 1.5 | 3 | 6 | 9 | 12 | 24 | 36 | 48 |
|---|---|---|---|---|---|---|---|---|---|
| N | 29 | 25 | 25 | 24 | 24 | 22 | 15 | 4 | 3 |
| Dysfunction Score | 18.81 (2.84) |
19.24 (3.00) |
12.63 (3.04) |
7.96 (3.05) |
9.03 (3.10) |
5.10 (3.14) |
9.45 (3.65) |
6.05 (6.20) |
8.68 (7.22) |
| Change (95% CI) | - | 0.43 (-3.18, 4.05) |
-6.18 (-9.81, -2.55) |
-10.84 (-14.55, -7.14) |
-9.78 (-13.48, -6.07) |
-13.71 (-17.52, -9.90) |
-9.36 (-13.66, -5.06) |
-12.75 (-20.14, -5.37) |
-10.12 (-18.69, -1.55) |
| p-value | - | 0.8124 | 0.0010 | <.0001 | <.0001 | <.0001 | <.0001 | 0.0008 | 0.0210 |
MATLAB Scripts
EQ-5D-3L Valuation
%Uploading raw EQ-5D-3L data
% filename=input('Please input the filename:','s');
filename='EQ5D3L_Redcap.csv';
opts = detectImportOptions(filename);
opts = setvartype(opts,'char');
T = readtable(filename,opts);
C=table2cell(T);
T=[T.Properties.VariableNames;C];
tf = cellfun('isempty',T); % true for empty cells
T(tf) = {'0'};
[rows, cols]=size(T);
%Converting data type from string to double for mathematical functions
for i=2:rows
for j=3:cols
T{i,j}=str2double(T{i,j});
end
end
%Creating health state vector (i.e. 12312)
for i=2:rows
for j=3:cols
T{i,8}=[T{i,3},T{i,4},T{i,5},T{i,6},T{i,7}];
end
end
Output(:,1)=T(:,1);
Output(:,2)=T(:,2);
Output(:,3)=T(:,8);
Output{1,3}='Health State';
Output{1,4}='Level 2';
Output{1,5}='Level 3';
Output{1,6}='Predicted Value';
%Deriving an EQ-5D index value from the health state
%The index is calculated by deducting the appropriate weights from 1, the value for full health (i.e. state 11111).
%Calculations made according to USA standard EQ-5D-3L value set
for i=2:rows
if Output{i,3}==0
Output{i,3}=0;
else
Output{i,4} = sum(Output{i,3} == 2);
Output{i,5} = sum(Output{i,3} == 3);
end
end
for i=2:rows
x=1.0;
if Output{i,3}==0
Output{i,3}=0;
elseif Output{i,3}(1)==2
x=x-0.146016;
elseif Output{i,3}(1)==3
x=x-0.557685;
end
if Output{i,3}==0
elseif Output{i,3}(2)==2
x=x-0.1753425;
elseif Output{i,3}(2)==3
x=x-0.4711896;
end
if Output{i,3}==0
elseif Output{i,3}(3)==2
x=x-0.1397295;
elseif Output{i,3}(3)==3
x=x-0.3742594;
end
if Output{i,3}==0
elseif Output{i,3}(4)==2
x=x-0.1728907;
elseif Output{i,3}(4)==3
x=x-0.5371011;
end
if Output{i,3}==0
elseif Output{i,3}(5)==2
x=x-0.156223;
elseif Output{i,3}(5)==3
x=x-0.4501876;
end
if Output{i,3}==0
elseif Output{i,4}+Output{i,5} >= 2
x=x-(-0.1395949)*(Output{i,4}+Output{i,5}-1);
end
if Output{i,3}==0
elseif Output{i,4} >= 2
x=x-(0.0106868*(Output{i,4}-1)^2);
end
if Output{i,3}==0
elseif Output{i,5} >= 2
x=x-(-0.1215579*(Output{i,5}-1));
x=x-(-0.0147963*(Output{i,5}-1)^2);
end
Output{i,6}=round(x,3);
end
for i=2:rows
if Output{i,3}==0
Output{i,6}=[];
end
end
%Exporting index values
Export_Data(:,1)=Output(:,1);
Export_Data(:,2)=Output(:,2);
Export_Data(:,3)=Output(:,6);
Export_Data=cell2table(Export_Data);
writetable(Export_Data,'EQ5D3L Valuation.xls');
SF-36 Scoring
%Uploading raw EQ-5D-3L data
% filename=input('Please input the filename:','s');
filename='Precoded SF36 12-27.csv';
opts = detectImportOptions(filename);
opts = setvartype(opts,'char');
T = readtable(filename,opts);
C=table2cell(T);
T=[T.Properties.VariableNames;C];
tf = cellfun('isempty',T); % true for empty cells
T(tf) = {'0'};
[rows, cols]=size(T);
%Converting data type from string to double for mathematical functions
for i=2:rows
for j=3:cols
T{i,j}=str2double(T{i,j});
end
end
Output=T;
%Recoding REDCap survey responses to weighted score
%(Ware J, Snow K, Kosinski M, Gandek B. SF-36 Health Survey Manual &
%Interpretation Guide)
for i=2:rows
if Output{i,23}==1
Output{i,23}=6.0;
elseif Output{i,23}==2
Output{i,23}=5.4;
elseif Output{i,23}==3
Output{i,23}=4.2;
elseif Output{i,23}==4
Output{i,23}=3.1;
elseif Output{i,23}==5
Output{i,23}=2.2;
elseif Output{i,23}==6
Output{i,23}=1.0;
end
end
for i=2:rows
if T{i,23}==0 && T{i,24}==1
Output{i,24}=6.0;
elseif T{i,23}==0 && T{i,24}==2
Output{i,24}=4.75;
elseif T{i,23}==0 && T{i,24}==3
Output{i,24}=3.5;
elseif T{i,23}==0 && T{i,24}==4
Output{i,24}=2.25;
elseif T{i,23}==0 && T{i,24}==5
Output{i,24}=1.0;
end
end
for i=2:rows
if T{i,23}==1 && T{i,24}==1
Output{i,24}=6;
elseif T{i,23}~=1 && T{i,24}==1
Output{i,24}=5;
elseif T{i,24}==2
Output{i,24}=4;
elseif T{i,24}==3
Output{i,24}=3;
elseif T{i,24}==4
Output{i,24}=2;
elseif T{i,24}==5
Output{i,24}=1;
end
end
for i=2:rows
if Output{i,3}==1
Output{i,3}=5.0;
elseif Output{i,3}==2
Output{i,3}=4.4;
elseif Output{i,3}==3
Output{i,3}=3.4;
elseif Output{i,3}==4
Output{i,3}=2.0;
elseif Output{i,3}==5
Output{i,3}=1.0;
end
end
for i=2:rows
if Output{i,36}==1
Output{i,36}=5.0;
elseif Output{i,36}==2
Output{i,36}=4.0;
elseif Output{i,36}==3
Output{i,36}=3.0;
elseif Output{i,36}==4
Output{i,36}=2.0;
elseif Output{i,36}==5
Output{i,36}=1.0;
end
end
for i=2:rows
if Output{i,38}==1
Output{i,38}=5.0;
elseif Output{i,38}==2
Output{i,38}=4.0;
elseif Output{i,38}==3
Output{i,38}=3.0;
elseif Output{i,38}==4
Output{i,38}=2.0;
elseif Output{i,38}==5
Output{i,38}=1.0;
end
end
for i=2:rows
if Output{i,25}==1
Output{i,25}=6.0;
elseif Output{i,25}==2
Output{i,25}=5.0;
elseif Output{i,25}==3
Output{i,25}=4.0;
elseif Output{i,25}==4
Output{i,25}=3.0;
elseif Output{i,25}==5
Output{i,25}=2.0;
elseif Output{i,25}==6
Output{i,25}=1.0;
end
end
for i=2:rows
if Output{i,29}==1
Output{i,29}=6.0;
elseif Output{i,29}==2
Output{i,29}=5.0;
elseif Output{i,29}==3
Output{i,29}=4.0;
elseif Output{i,29}==4
Output{i,29}=3.0;
elseif Output{i,29}==5
Output{i,29}=2.0;
elseif Output{i,29}==6
Output{i,29}=1.0;
end
end
for i=2:rows
if Output{i,22}==1
Output{i,22}=5.0;
elseif Output{i,22}==2
Output{i,22}=4.0;
elseif Output{i,22}==3
Output{i,22}=3.0;
elseif Output{i,22}==4
Output{i,22}=2.0;
elseif Output{i,22}==5
Output{i,22}=1.0;
end
end
for i=2:rows
if Output{i,28}==1
Output{i,28}=6.0;
elseif Output{i,28}==2
Output{i,28}=5.0;
elseif Output{i,28}==3
Output{i,28}=4.0;
elseif Output{i,28}==4
Output{i,28}=3.0;
elseif Output{i,28}==5
Output{i,28}=2.0;
elseif Output{i,28}==6
Output{i,28}=1.0;
end
end
for i=2:rows
if Output{i,32}==1
Output{i,32}=6.0;
elseif Output{i,32}==2
Output{i,32}=5.0;
elseif Output{i,32}==3
Output{i,32}=4.0;
elseif Output{i,32}==4
Output{i,32}=3.0;
elseif Output{i,32}==5
Output{i,32}=2.0;
elseif Output{i,32}==6
Output{i,32}=1.0;
end
end
%Saving scored data
Scored_Data=cell2table(Output);
writetable(Scored_Data,'Scored SF-36 Data.xls');
%In Excel file, recode missing item responses with mean substitution
%where possible
%Save file as csv
%Uploading recoded SF-36 data
% filename=input('Please input the filename:','s');
filename='Scored SF-36 Data.csv';
opts = detectImportOptions(filename);
opts = setvartype(opts,'char'); % or 'string'
R = readtable(filename,opts);
C=table2cell(R);
R=[R.Properties.VariableNames;C];
R(1,:)=Output(1,:);
%Converting data type from string to double for mathematical functions
for i=2:rows
for j=3:cols
R{i,j}=str2double(R{i,j});
end
end
Scores=R;
%Creating cell vectors to store sub-scale data
%If more than 50% of scale items missing, sub-scale score not reported
%Physical Functioning
PF=cell(rows,1);
for i=2:rows
PF_data(i-1,:)=[Scores{i,5},Scores{i,6},Scores{i,7},Scores{i,8},...
Scores{i,9},Scores{i,10},Scores{i,11},Scores{i,12},...
Scores{i,13},Scores{i,14}];
nz=nnz(~PF_data(i-1,:));
if nz > 5
PF{i,1}=[];
else
PF{i,1}=Scores{i,5}+Scores{i,6}+Scores{i,7}+Scores{i,8}+Scores{i,9}...
+Scores{i,10}+Scores{i,11}+Scores{i,12}+Scores{i,13}+Scores{i,14};
end
end
%Role Limitations due to Physical Health
RP=cell(rows,1);
for i=2:rows
RP_data(i-1,:)=[Scores{i,15},Scores{i,16},Scores{i,17},Scores{i,18}];
nz=nnz(~RP_data(i-1,:));
if nz > 2
PF{i,1}=[];
else
RP{i,1}=Scores{i,15}+Scores{i,16}+Scores{i,17}+Scores{i,18};
end
end
%Bodily Pain
BP=cell(rows,1);
for i=2:rows
BP_data(i-1,:)=[Scores{i,23},Scores{i,24}];
nz=nnz(~BP_data(i-1,:));
if nz > 1
PF{i,1}=[];
else
BP{i,1}=Scores{i,23}+Scores{i,24};
end
end
%General Health
GH=cell(rows,1);
for i=2:rows
GH_data(i-1,:)=[Scores{i,3},Scores{i,35},Scores{i,36},Scores{i,37},Scores{i,38}];
nz=nnz(~GH_data(i-1,:));
if nz > 2
PF{i,1}=[];
else
GH{i,1}=Scores{i,3}+Scores{i,35}+Scores{i,36}+Scores{i,37}+Scores{i,38};
end
end
%Vitality (Energy/Fatigue)
VI=cell(rows,1);
for i=2:rows
VI_data(i-1,:)=[Scores{i,25},Scores{i,29},Scores{i,31},Scores{i,33}];
nz=nnz(~VI_data(i-1,:));
if nz > 2
VI{i,1}=[];
else
VI{i,1}=Scores{i,25}+Scores{i,29}+Scores{i,31}+Scores{i,33};
end
end
%Social Functioning
SF=cell(rows,1);
for i=2:rows
SF_data(i-1,:)=[Scores{i,22},Scores{i,34}];
nz=nnz(~SF_data(i-1,:));
if nz > 1
SF{i,1}=[];
else
SF{i,1}=Scores{i,22}+Scores{i,34};
end
end
%Role Limitations due to Emotional Health
RE=cell(rows,1);
for i=2:rows
RE_data(i-1,:)=[Scores{i,19},Scores{i,20},Scores{i,21}];
nz=nnz(~RE_data(i-1,:));
if nz > 1
RE{i,1}=[];
else
RE{i,1}=Scores{i,19}+Scores{i,20}+Scores{i,21};
end
end
%Mental Health
MH=cell(rows,1);
for i=2:rows
MH_data(i-1,:)=[Scores{i,26},Scores{i,27},Scores{i,28},Scores{i,30},Scores{i,32}];
nz=nnz(~MH_data(i-1,:));
if nz > 2
MH{i,1}=[];
else
MH{i,1}=Scores{i,26}+Scores{i,27}+Scores{i,28}+Scores{i,30}+Scores{i,32};
end
end
%Reported Health Transition, not used in Physical Component Score or
%Mental Component Score
RHT=cell(rows,1);
for i=2:rows
RHT_data(i-1,:)=[Scores{i,4}];
nz=nnz(~RHT_data(i-1,:));
if nz > 0
MH{i,1}=[];
else
RHT{i,1}=Scores{i,4};
end
end
%Transform raw scores to 0-100 scale
%Storing min/max/range of each domain scores
[minPF,maxPF]=bounds(cell2mat(PF));
rangePF=maxPF-minPF;
[minRP,maxRP]=bounds(cell2mat(RP));
rangeRP=maxRP-minRP;
[minBP,maxBP]=bounds(cell2mat(BP));
rangeBP=maxBP-minBP;
[minGH,maxGH]=bounds(cell2mat(GH));
rangeGH=maxGH-minGH;
[minVI,maxVI]=bounds(cell2mat(VI));
rangeVI=maxVI-minVI;
[minSF,maxSF]=bounds(cell2mat(SF));
rangeSF=maxSF-minSF;
[minRE,maxRE]=bounds(cell2mat(RE));
rangeRE=maxRE-minRE;
[minMH,maxMH]=bounds(cell2mat(MH));
rangeMH=maxMH-minMH;
%Calculating transformed scores
%transformed score = [(actual raw score - min)/range]*100
PF_transform=cell(rows,1);
for i=2:rows
PF_transform{i,1}=((PF{i,1}-minPF)/rangePF)*100;
end
RP_transform=cell(rows,1);
for i=2:rows
RP_transform{i,1}=((RP{i,1}-minRP)/rangeRP)*100;
end
BP_transform=cell(rows,1);
for i=2:rows
BP_transform{i,1}=((BP{i,1}-minBP)/rangeBP)*100;
end
GH_transform=cell(rows,1);
for i=2:rows
GH_transform{i,1}=((GH{i,1}-minGH)/rangeGH)*100;
end
VI_transform=cell(rows,1);
for i=2:rows
VI_transform{i,1}=((VI{i,1}-minVI)/rangeVI)*100;
end
SF_transform=cell(rows,1);
for i=2:rows
SF_transform{i,1}=((SF{i,1}-minSF)/rangeSF)*100;
end
RE_transform=cell(rows,1);
for i=2:rows
RE_transform{i,1}=((RE{i,1}-minRE)/rangeRE)*100;
end
MH_transform=cell(rows,1);
for i=2:rows
MH_transform{i,1}=((MH{i,1}-minMH)/rangeMH)*100;
end
R(:,39)=PF_transform(:,1);
R{1,39}='Physical Functioning';
R(:,40)=RP_transform(:,1);
R{1,40}='Role-Physical';
R(:,41)=BP_transform(:,1);
R{1,41}='Bodily Pain';
R(:,42)=GH_transform(:,1);
R{1,42}='General Health';
R(:,43)=VI_transform(:,1);
R{1,43}='Vitality';
R(:,44)=SF_transform(:,1);
R{1,44}='Social Functioning';
R(:,45)=RE_transform(:,1);
R{1,45}='Role-Emotional';
R(:,46)=MH_transform(:,1);
R{1,46}='Mental Health';
%PCS/MCS Computation
%Step 1: Perform z-score standardization of SF-36 scales
PF_Z=cell(rows,1);
RP_Z=cell(rows,1);
BP_Z=cell(rows,1);
GH_Z=cell(rows,1);
VI_Z=cell(rows,1);
SF_Z=cell(rows,1);
RE_Z=cell(rows,1);
MH_Z=cell(rows,1);
for i=2:rows
PF_Z{i,1}=((PF_transform{i,1}-84.52404)/22.89490);
RP_Z{i,1}=((RP_transform{i,1}-81.19907)/33.79729);
BP_Z{i,1}=((BP_transform{i,1}-75.49196)/23.55879);
GH_Z{i,1}=((GH_transform{i,1}-72.21316)/20.16964);
VI_Z{i,1}=((VI_transform{i,1}-61.05453)/20.86942);
SF_Z{i,1}=((SF_transform{i,1}-83.59753)/22.37642);
RE_Z{i,1}=((RE_transform{i,1}-81.29467)/33.02717);
MH_Z{i,1}=((MH_transform{i,1}-74.84212)/18.01189);
end
%Aggregation of scale scores into PCS/MCS
agg_phys=cell(rows,1);
agg_ment=cell(rows,1);
for i=2:rows
agg_phys{i,1}=(PF_Z{i,1}*.42402)+(RP_Z{i,1}*.35119)+(BP_Z{i,1}*.31754)...
+(GH_Z{i,1}*.24954)+(VI_Z{i,1}*.02877)+(SF_Z{i,1}*-.00753)+...
(RE_Z{i,1}*-.19206)+(MH_Z{i,1}*-.22069);
agg_ment{i,1}=(PF_Z{i,1}*-.22999)+(RP_Z{i,1}*-.12329)+(BP_Z{i,1}*-.09731)...
+(GH_Z{i,1}*-.01571)+(VI_Z{i,1}*.23534)+(SF_Z{i,1}*.26876)+(RE_Z{i,1}*.43407)...
+(MH_Z{i,1}*.48581);
end
%T-score transformation of PCS/MCS
t_pcs=cell(rows,1);
t_mcs=cell(rows,1);
for i=2:rows
t_pcs{i,1}=50+(agg_phys{i,1}*10);
t_mcs{i,1}=50+(agg_ment{i,1}*10);
end
R(:,47)=t_pcs(:,1);
R{1,47}='Physical Component Score';
R(:,48)=t_mcs(:,1);
R{1,48}='Mental Component Score';
%Saving scored data with PCS/MCS
Scored_Data=cell2table(R);
writetable(Scored_Data,'SF-36 Data PCS MCS.xls');
SIP Dysfunction Score
%Uploading raw SIP data
filename=input('Please input the filename, including the .csv extension:','s');
opts = detectImportOptions(filename);
opts = setvartype(opts,'char');
T = readtable(filename,opts);
C=table2cell(T);
T=[T.Properties.VariableNames;C];
tf = cellfun('isempty',T); % true for empty cells
T(tf) = {'0'};
[rows, cols]=size(T);
%Converting data type from string to double for mathematical functions
for i=2:rows
for j=3:cols
T{i,j}=str2double(T{i,j});
end
end
%Reformatting Output data table
Output=T;
%Looping through raw data by item (row)
%Replacing checked items with the scaled value, replacing unchecked items with zero
for i=2:rows
j=3;
% 083
if isequal(T{i,j},1)
Output{i,j}=8.3;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 049
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=4.9;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 104
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=10.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 058
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.8;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 084
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 061
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.1;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 060
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.0;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 087
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.7;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 068
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.8;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 069
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.9;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 132
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=13.2;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 046
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=4.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 062
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.2;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 078
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.8;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 089
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.9;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 074
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 084
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 121
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=12.1;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 072
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.2;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 098
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=9.8;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 064
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 100
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=10.0;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 064
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 125
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=12.5;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 058
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.8;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 082
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.2;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 113
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=11.3;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 030
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=3.0;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 086
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 089
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.9;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 115
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=11.5;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 114
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=11.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 057
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.7;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 124
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=12.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 074
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 074
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 128
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=12.8;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 043
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=4.3;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 088
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.8;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 054
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 044
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=4.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 086
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 062
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.2;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 071
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.1;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 077
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.7;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 069
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.9;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 077
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.7;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 044
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=4.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 084
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 086
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 106
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=10.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 081
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.1;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 109
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=10.9;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 041
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=4.1;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 066
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 056
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 048
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=4.8;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 054
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 072
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.2;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 044
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=4.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 101
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=10.1;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 067
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.7;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 084
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 052
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.2;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 036
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=3.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 043
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=4.3;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 080
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.0;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 051
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.1;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 052
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.2;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 056
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 088
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.8;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 086
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 088
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.8;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 119
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=11.9;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 102
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=10.2;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 064
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 115
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=11.5;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 079
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.9;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 043
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=4.3;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 048
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=4.8;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 056
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 067
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.7;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 076
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 096
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=9.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 105
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=10.5;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 055
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.5;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 088
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.8;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 054
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 083
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.3;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 079
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.9;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 035
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=3.5;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 090
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=9.0;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 075
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.5;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 059
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.9;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 067
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.7;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 084
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 113
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=11.3;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 078
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.8;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 067
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.7;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 064
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 080
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.0;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 070
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.0;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 102
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=10.2;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 093
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=9.3;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 083
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.3;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 083
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.3;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 067
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.7;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 076
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 087
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.7;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 064
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 361
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=36.1;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 037
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=3.7;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 055
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.5;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 080
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.0;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 043
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=4.3;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 050
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.0;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 061
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.1;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 034
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=3.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 062
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=6.2;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 039
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=3.9;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 036
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=3.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 059
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.9;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 084
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=8.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 051
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.1;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 033
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=3.3;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 043
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=4.3;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 077
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.7;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 037
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=3.7;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 077
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=7.7;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 043
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=4.3;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 104
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=10.4;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 059
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=5.9;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 036
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=3.6;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 099
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=9.9;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 117
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=11.7;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
% 133
j=j+1;
if isequal(T{i,j},1)
Output{i,j}=13.3;
elseif isequal(T{i,j},2)
Output{i,j}=0;
end
end
%Isolate numerical data
Scores=cell(rows-1,cols-2);
for i=2:rows
for j=3:cols
Scores{i-1,j-2}=Output{i,j};
end
end
Scores=cell2mat(Scores);
sum_scores=sum(Scores,2);
dysfunction_score=zeros(rows-1,1);
dysfunction_score(:,1)=(sum_scores./1003).*100;
dysfunction_score=num2cell(dysfunction_score);
dysfunction_score_reformatted=cell(rows,1);
dysfunction_score_reformatted{1,1}='Dysfunction Score';
dysfunction_score_reformatted(2:end,1)=dysfunction_score;
Output(:,cols+1)=dysfunction_score_reformatted;
%Creating Excel sheet including relevant data
patient_info(:,1)=Output(2:end,1);
patient_info(:,2)=Output(2:end,2);
Headers={'Record ID','Time Point','Calculated Dysfunction Score (%)'};
S=[patient_info,dysfunction_score];
S=cell2table(S, 'VariableNames', Headers);
writetable(S,'SIP Dysfunction Score.xls')
References
- Sarroca, N.; Valero, J.; Deus, J.; Casanova, J.; Luesma, M.J.; Lahoz, M. Quality of life, body image and self-esteem in patients with unilateral transtibial amputations. Sci Rep. 2021, 11. [Google Scholar] [CrossRef]
- Polat, C.S.; Konak, H.E.; Altas, E.U.; Akıncı, M.G.; SOnat, S. Factors related to phantom limb pain and its effect on quality of life. Somatosens Mot Res. 2021, 38, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Ehde, D.M.; Czerniecki, J.M.; Smith, D.G.; et al. Chronic phantom sensations, phantom pain, residual limb pain, and other regional pain after lower limb amputation. Arch Phys Med Rehabil. 2000, 81, 1039–1044. [Google Scholar] [CrossRef]
- Van Der Schans, C.P.; Geertzen, J.H.B.; Schoppen, T.; Dijkstra, P.U. Phantom Pain and Health-Related Quality of Life in Lower Limb Amputees. Vol 24.; 2002.
- Padovani, M.T.; Martins, M.R.I.; Venâncio, A.; Forni, J.E.N. Anxiety, depression and quality of life in individuals with phantom limb pain. Acta Ortop Bras. 2015, 23. [Google Scholar] [CrossRef] [PubMed]
- Trevelyan, E.G.; Turner, W.A.; Robinson, N. Perceptions of phantom limb pain in lower limb amputees and its effect on quality of life: A qualitative study. Br J Pain. 2015, 10, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Mioton, L.M.; Dumanian, G.A.; Shah, N.; et al. Targeted Muscle Reinnervation Improves Residual Limb Pain, Phantom Limb Pain, and Limb Function: A Prospective Study of 33 Major Limb Amputees. Clin Orthop Relat Res 2020, 478. Available online: https://journals.lww.com/clinorthop/Fulltext/2020/09000/Targeted_Muscle_Reinnervation_Improves_Residual.34.aspx. [CrossRef] [PubMed]
- Dumanian, G.A.; Potter, B.K.; Mioton, L.M.; et al. Targeted Muscle Reinnervation Treats Neuroma and Phantom Pain in Major Limb Amputees: A Randomized Clinical Trial. Ann Surg 2019, 270. Available online: https://journals.lww.com/annalsofsurgery/Fulltext/2019/08000/Targeted_Muscle_Reinnervation_Treats_Neuroma_and.10.aspx. [CrossRef]
- Valerio, I.L.; Dumanian, G.A.; Jordan, S.W.; et al. Preemptive Treatment of Phantom and Residual Limb Pain with Targeted Muscle Reinnervation at the Time of Major Limb Amputation. J Am Coll Surg. 2019, 228, 217–226. [Google Scholar] [CrossRef]
- Herr, H.; Carty, M.J. The Agonist-Antagonist Myoneural Interface.; 2021. Available online: www.techortho.com.
- Carty, M.J.; Herr, H.M. The Agonist-Antagonist Myoneural Interface. Hand Clin. 2021, 37, 435–445. [Google Scholar] [CrossRef]
- Srinivasan, S.S.; Diaz, M.; Carty, M.; Herr, H.M. Towards functional restoration for persons with limb amputation: A dual-stage implementation of regenerative agonist-antagonist myoneural interfaces. Sci Rep. 2019, 9, 1981. [Google Scholar] [CrossRef]
- Berger, L.; Sullivan, C.L.; Landry, T.; Sparling, T.L.; Carty, M.J. The Ewing Amputation: Operative Technique and Perioperative Care. Orthoplastic Surgery. 2023. [CrossRef]
- Clites, T.R.; Carty, M.J.; Srinivasan, S.; Zorzos, A.N.; Herr, H.M. A murine model of a novel surgical architecture for proprioceptive muscle feedback and its potential application to control of advanced limb prostheses. J Neural Eng. 2017, 14, 036002. [Google Scholar] [CrossRef]
- Clites, T.R.; Herr, H.M.; Srinivasan, S.S.; Zorzos, A.N.; Carty, M.J. The Ewing amputation: The first human implementation of the agonist-antagonist myoneural interface. Plast Reconstr Surg Glob Open. 2018, 6. [Google Scholar] [CrossRef] [PubMed]
- Clites, T.R.; Carty, M.J.; Srinivasan, S.S.; Talbot, S.G.; Brånemark, R.; Herr, H.M. Caprine Models of the Agonist-Antagonist Myoneural Interface Implemented at the Above- and Below-Knee Amputation Levels. Plast Reconstr Surg 2019, 144. Available online: https://journals.lww.com/plasreconsurg/Fulltext/2019/08000/Caprine_Models_of_the_Agonist_Antagonist_Myoneural.21.aspx. [CrossRef] [PubMed]
- Harrington, C.; Souza, J.; Dearden, M.; Richards, J.; Carty, M.J.; Potter, B.K. The agonist-antagonist myoneural interface in a transtibial amputation: Surgical technique. J Bone Joint Surg Ess Surg Tech. 2023.
- Herr, H.M.; Clites, T.R.; Srinivasan, S.; et al. Reinventing Extremity Amputation in the Era of Functional Limb Restoration. Ann Surg 2021, 273. Available online: https://journals.lww.com/annalsofsurgery/Fulltext/2021/02000/Reinventing_Extremity_Amputation_in_the_Era_of.13.aspx. [CrossRef]
- Srinivasan, S.S.; Carty, M.J.; Calvaresi, P.W.; et al. On prosthetic control: A regenerative agonist-antagonist myoneural interface. Sci Robot. 2017, 2, eaan2971. [Google Scholar] [CrossRef]
- Srinivasan, S.S.; Herr, H.M.; Clites, T.R.; et al. Agonist-antagonist Myoneural Interfaces in Above-knee Amputation Preserve Distal Joint Function and Perception. Ann Surg 2021, 273. Available online: https://journals.lww.com/annalsofsurgery/Fulltext/2021/03000/Agonist_antagonist_Myoneural_Interfaces_in.44.aspx. [CrossRef]
- Clites, T.R.; Carty, M.J.; Ullauri, J.B.; et al. Proprioception from a neurally controlled lower-extremity prosthesis. Sci Transl Med. 2018, 10, eaap8373. [Google Scholar] [CrossRef]
- Srinivasan, S.S.; Gutierrez-Arango, S.; Teng, A.C.E.; et al. Neural interfacing architecture enables enhanced motor control and residual limb functionality postamputation. Proceedings of the National Academy of Sciences. 2021, 118, e2019555118. [Google Scholar] [CrossRef]
- EuroQol Research Foundation. EQ-5D-3L User Guide.
- Shaw, J.W.; Johnson, J.A.; Coons, S.J. US Valuation of the EQ-5D Health States: Development and Testing of the D1 Valuation Model. Med Care 2005, 43. Available online: https://journals.lww.com/lww-medicalcare/Fulltext/2005/03000/US_Valuation_of_the_EQ_5D_Health_States_.3.aspx. [CrossRef]
- Binkley, J.M.; Stratford, P.W.; Lott, S.A.; Riddle, D.L. The Lower Extremity Functional Scale (LEFS): Scale development, measurement properties, and clinical application. North American Orthopaedic Rehabilitation Research Network. Phys Ther. 1999, 79, 371–383. [Google Scholar]
- Cella, D.; Choi, S.W.; Condon, D.M.; et al. PROMIS Adult Health Profiles: Efficient Short-Form Measures of Seven Health Domains. Value in Health. 2019, 22, 537–544. [Google Scholar] [CrossRef]
- Hays, R.D.; Spritzer, K.L.; Schalet, B.D.; Cella, D. PROMIS®-29 v2.0 profile physical and mental health summary scores. Quality of Life Research. 2018, 27, 1885–1891. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E. SF-36 Physical and Mental Health Summary Scales: A User’s Manual Estimation of Medical Care Total Expenditures View Project.; 1993. Available online: https://www.researchgate.net/publication/292390260.
- Ware, J.; Snow, K.; Kosinski, M.; Gandek, B. SF-36 Health Survey Manual & Interpretation Guide; Nimrod Press, 1993. [Google Scholar]
- Jenkinson, C.; The SF-36 Physical and Mental Health Summary Measures: An Example of How to Interpret. Vol 3.; 1998. Available online: https://about.jstor.org/terms.
- Wu, A.W.; Skinner, E.A.; Pfoh, E.; Steinwachs, D.M. Wu, A.W.; Skinner, E.A.; Pfoh, E.; Steinwachs, D.M. Sickness Impact Profile (SIP). In: Michalos AC, ed. Encyclopedia of Quality of Life and Well-Being Research. Springer Netherlands; 2014:5959-5963. [CrossRef]
- Lipsitz, S.R.; Fitzmaurice, G.M.; Ibrahim, J.G.; Gelber, R.; Lipshultz, S. Parameter Estimation in Longitudinal Studies with Outcome-Dependent Follow-Up. Biometrics. 2002, 58, 621–630. [Google Scholar] [CrossRef]
- MacKenzie, E.J.; Bosse, M.J.; Castillo, R.C.; et al. Functional Outcomes Following Trauma-Related Lower-Extremity Amputation. JBJS 2004, 86. Available online: https://journals.lww.com/jbjsjournal/Fulltext/2004/08000/Functional_Outcomes_Following_Trauma_Related.6.aspx. [CrossRef] [PubMed]
- Davis, A.M.; Devlin, M.; Griffin, A.M.; Wunder, J.S.; Bell, R.S. Functional outcome in amputation versus limb sparing of patients with lower extremity sarcoma: A matched case-control study. Arch Phys Med Rehabil. 1999, 80, 615–618. [Google Scholar] [CrossRef] [PubMed]
- Frantz, T.L.; Everhart, J.S.; West, J.M.; Ly, T.V.; Phieffer, L.S.; Valerio, I.L. Targeted Muscle Reinnervation at the Time of Major Limb Amputation in Traumatic Amputees. JBJS Open Access. 2020, 5, E0067. [Google Scholar] [CrossRef]
- Mioton, L.M.; Dumanian, G.A.; Fracol, M.E.; et al. Benchmarking Residual Limb Pain and Phantom Limb Pain in Amputees through a Patient-reported Outcomes Survey. Plast Reconstr Surg Glob Open. Published online 2020. [CrossRef]
- O’Brien, A.L.; West, J.M.; Gokun, Y.; et al. Longitudinal Durability of Patient-Reported Pain Outcomes after Targeted Muscle Reinnervation at the Time of Major Limb Amputation. J Am Coll Surg 2022, 234. Available online: https://journals.lww.com/journalacs/Fulltext/2022/05000/Longitudinal_Durability_of_Patient_Reported_Pain.21.aspx. [CrossRef]
Figure 1.
EQ-5D-3L mean index score and mean VAS score at 0 to 48-months post-operation for patients undergoing a modified AMI amputation including standard error bars.
Figure 1.
EQ-5D-3L mean index score and mean VAS score at 0 to 48-months post-operation for patients undergoing a modified AMI amputation including standard error bars.
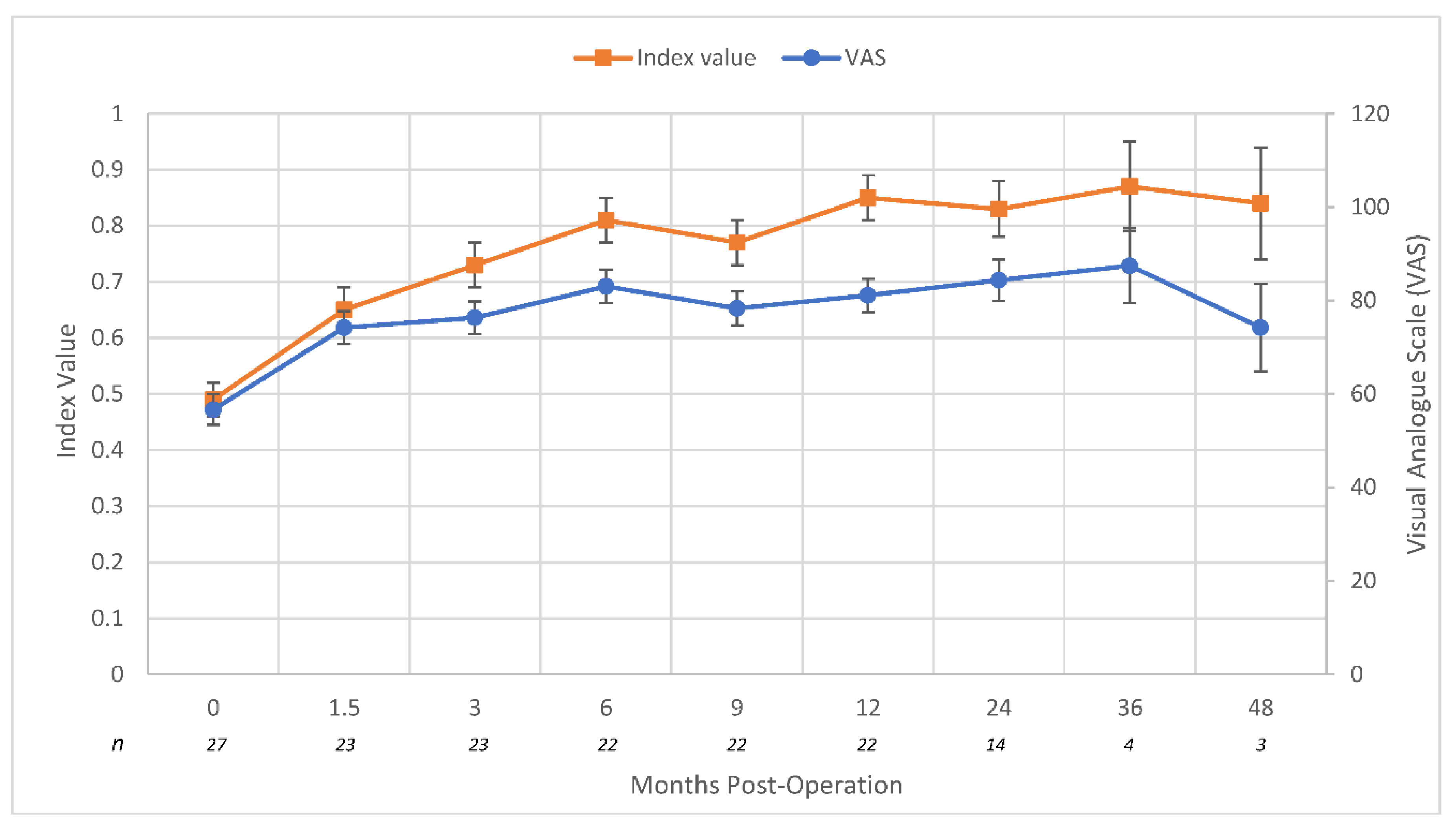
Figure 2.
Mean LEFS scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation including standard error bars.
Figure 2.
Mean LEFS scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation including standard error bars.
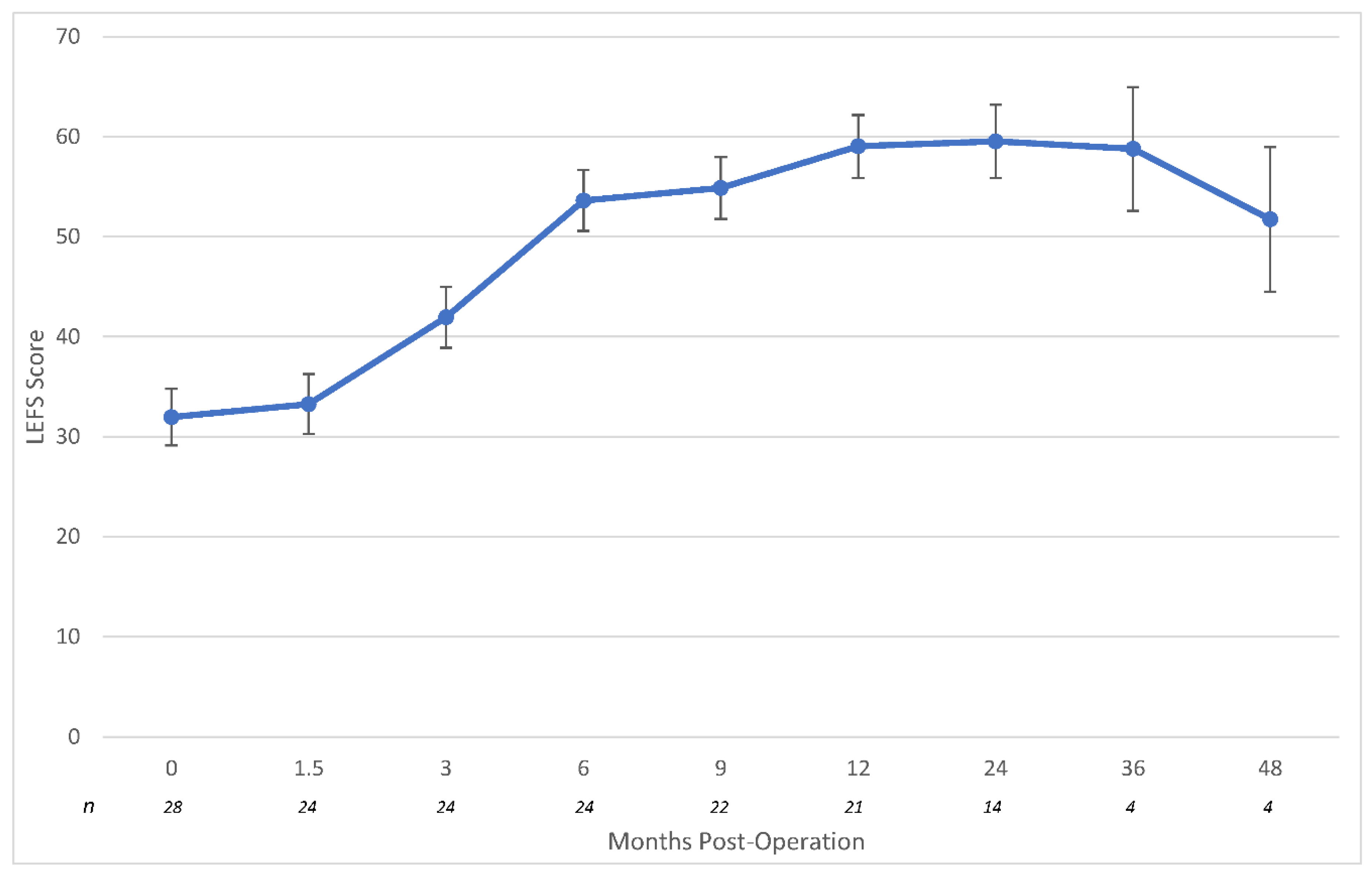
Figure 3.
Mean PROMIS T-scores for negative PROMIS dimensions at 0 to 48-months post-operation for patients undergoing a modified AMI amputation including standard error bars.
Figure 3.
Mean PROMIS T-scores for negative PROMIS dimensions at 0 to 48-months post-operation for patients undergoing a modified AMI amputation including standard error bars.
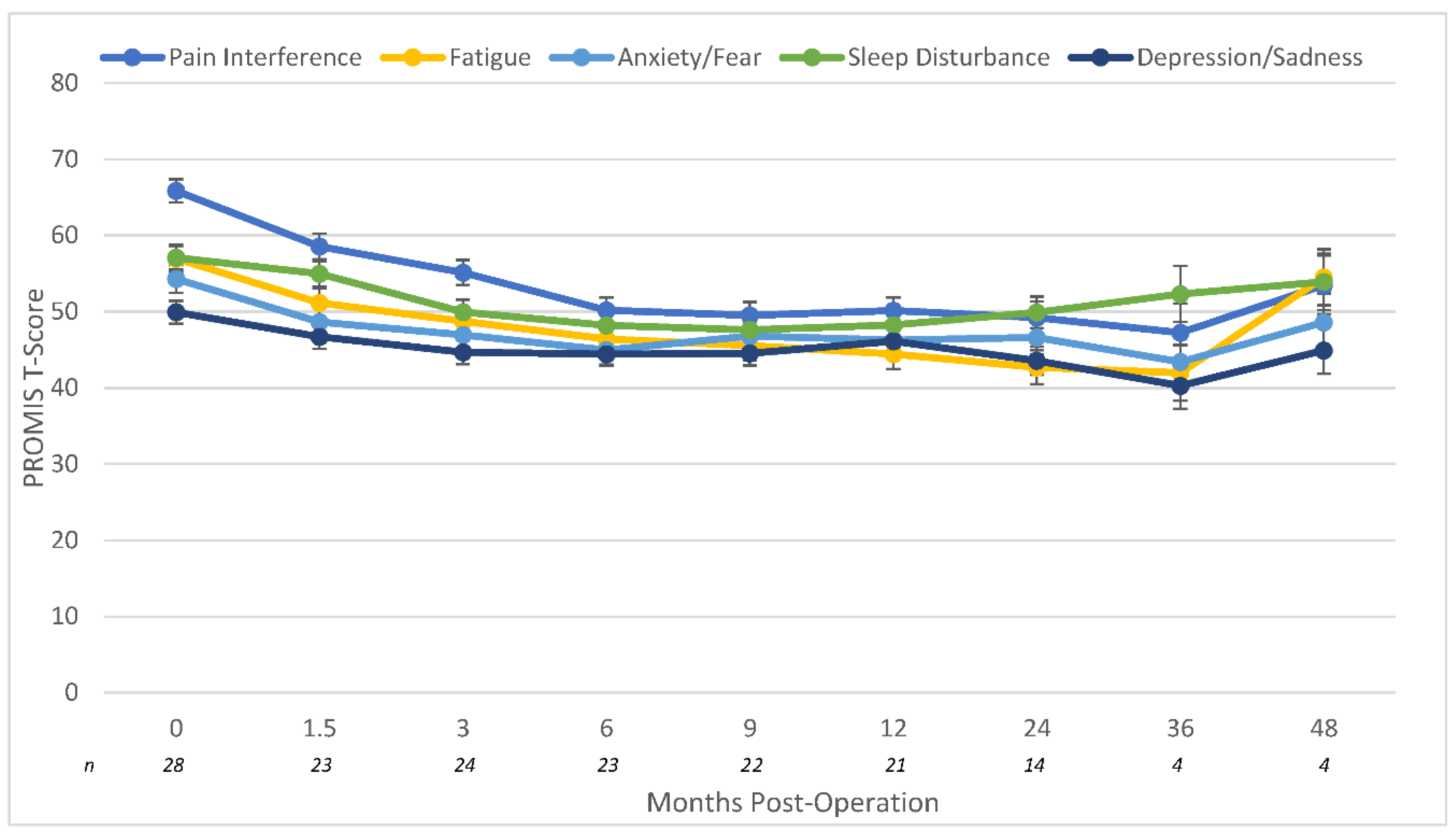
Figure 4.
Mean PROMIS T-scores for positive PROMIS dimensions at 0 to 48-months post-operation for patients undergoing a modified AMI amputation including standard error bars.
Figure 4.
Mean PROMIS T-scores for positive PROMIS dimensions at 0 to 48-months post-operation for patients undergoing a modified AMI amputation including standard error bars.

Figure 5.
Mean SF-36 physical and mental scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation including standard error bars.
Figure 5.
Mean SF-36 physical and mental scores at 0 to 48-months post-operation for patients undergoing a modified AMI amputation including standard error bars.
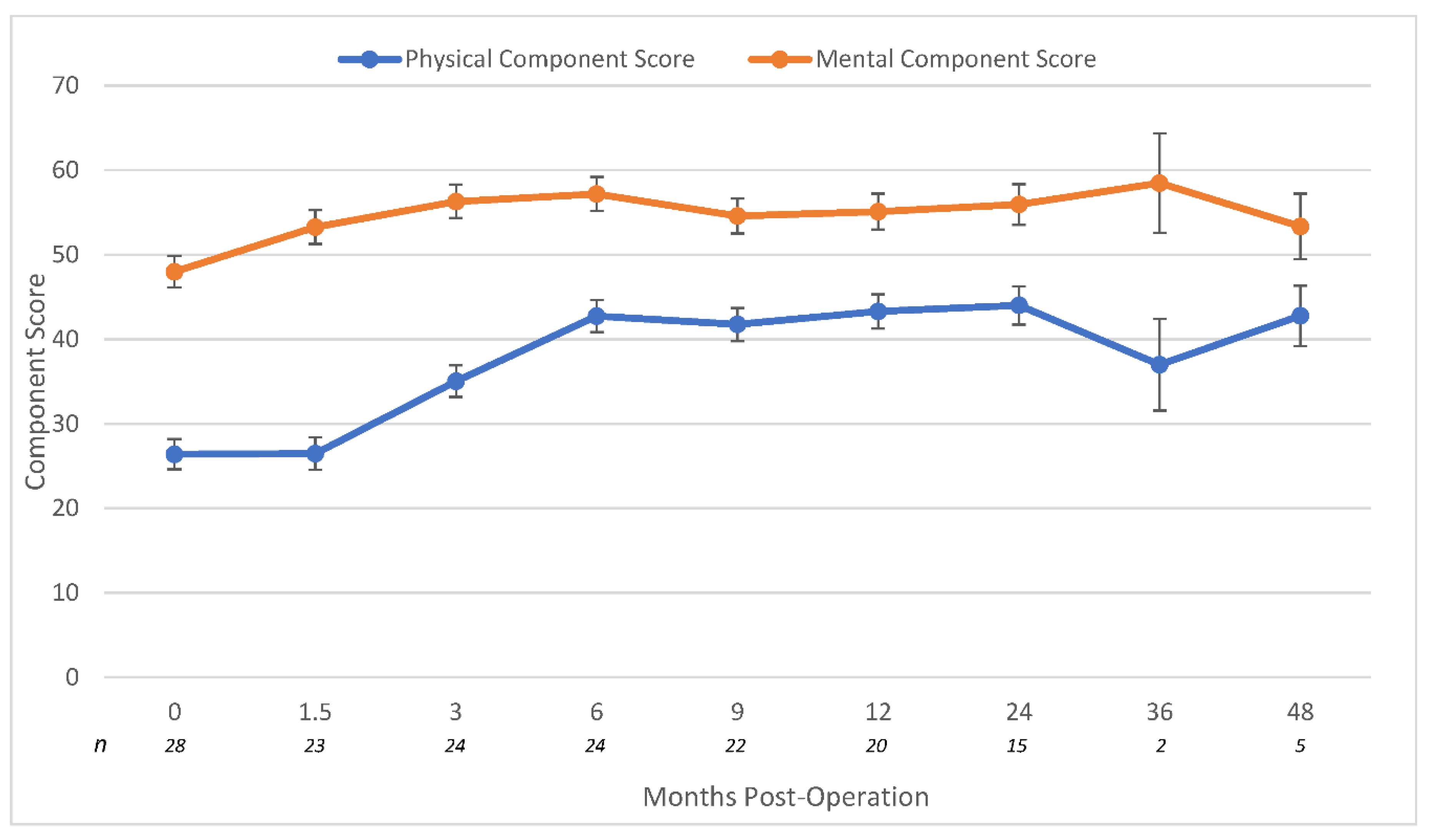
Table 1.
Patient Characteristics.
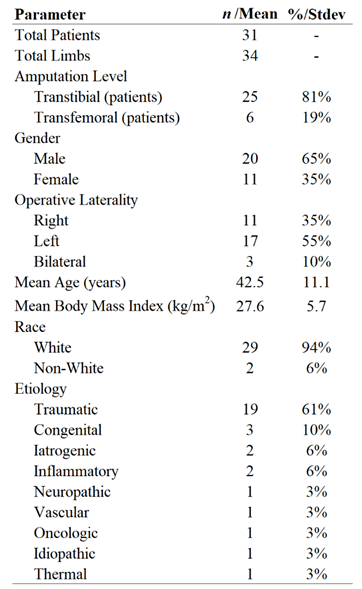 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



