
Submitted:
14 July 2023
Posted:
17 July 2023
You are already at the latest version
Abstract
Advances in nanotechnology have paved the way for more effective drug delivery using particulate and non-particulate nano-based formulations across a range of applications. In the oral cavity, local delivery using mucoadhesive formulations has advantages over conventional formulations for increasing local efficacy whilst reducing unwanted adverse effects. Nano-formulations provide the opportunity for new formulations with enhanced intraoral stability, local action, and improved patient acceptability.
Keywords:
Buccal mucoadhesive
; local action
; nanotechnology
; clinical trial
; biofilms
; gel
Introduction
Driven by developments in polymers and materials science, nanotechnology now plays a central role in many drug delivery systems. Nanotechnology ultimately helps to increase therapeutic efficacy through improved solubility, stability, penetration, drug permeation and, in the case of oral cavity diseases, drug concentrations in the saliva [1,2]. Buccal drug delivery describes drug delivery to the oral mucosa, and it is important not only in chronic conditions and where the parenteral approach is unsuitable, but also in emergent situations, such as administration of nitrates as anti-anginal rescue medications [3]. To ensure retention of the drug in the oral cavity, mucoadhesive polymers have been developed for a variety of agents and indications [4,5]. However, there remains room for further optimization of buccal drug delivery based on the underlying theory and by exploiting some of the advantageous properties of nanomaterials. Areas for development in the field of mucoadhesive formulations for buccal drug delivery include permeability enhancers, new formulations and mucoadhesive, and the use of nanotechnology. Since there are plenty of reviews of the application of nanotechnology to systemic drug delivery, this review focuses on the impact of nanotechnology in treating intraoral pathology through mucoadhesive preparations.
Theoretical perspective
Buccal drug delivery aims to deliver drugs into the oral cavity for local or systemic effects. However, the mucosa and saliva – which is particularly abundant compared with other cavities such as the nose and vagina - have narrow absorption windows [6]. Nevertheless, when drugs are successfully delivered to the oral mucosa, they are released into the cavity to exert both local and systemic effects [7]. However, for some applications, it is desirable to deliver and release the drug locally and not systemically to maintain high local concentrations and reduce unwanted systemic side-effects [8], mandating not only mucoadhesive properties (to keep the drug attached to the mucosa) but also a formulation that stays within the oral cavity and/or is secreted into the saliva. Although various strategies including mucoadhesive buccal tablets, films, gels, wafers, and in situ delivery have been attempted, there have been relatively few attempts to apply nanotechnology to improve the physicochemical characters of local oral cavity drug delivery [9,10,11,12,13].
Nanotechnology refers to drug delivery in nanoparticles form for improved clinical outcome. In the oral cavity, the half-lives of drugs dissolved in saliva tend to be quite short due to the rinsing action of saliva in the mouth, so nano-based mucoadhesive delivery could improve retention, permeation, and ultimately therapeutic outcomes. Nanotechnology has proven revolutionary due to its ability to enhance delivery, overcoming some drug-related side-effects and allowing improved uptake into mucosal epithelial cells via both transcellular and paracellular pathways. The term nanomaterials describes materials with dimensions of ~100 nm in appearance and, by virtue of their small size, they have unique physicochemical and electrostatic properties [14]. These surface-based properties allow them to interact with charged organic polymeric substances in the buccal microenvironment. Nanoparticles (NPs) typically interact with the viscoelastic mucosal layer, facilitating engulfment of nanostructured carriers due to particle-mucin and steric interactions. Mucin is a naturally protective substance covering the buccal mucosa, exerting an anti-adhesive effect on pathogens and protecting the oral mucosa [15]. However, mucin interacts with the NPs via hydrogen bonding, polymeric chain entanglement, electrostatic interactions, and Van der Waals and hydrophobic interactions. However, if the particle surface is modified in such a way that it resembles viral or biological surfaces, it may penetrate the protective layer [16]. This property is useful for NPs that must penetrate the mucosa, thereby releasing drugs or other cargoes of interest, such as gene therapies [17,18], for instance; this approach may be useful for treating tumor cells. Overall, the NP approach allows specific binding to the buccal mucosal surface, where they interact with mucin to help engulfment/penetration into the deeper layers.
Anatomy and physiology
The oral cavity constitutes the lips, cheeks, tongue, hard palate, soft palate, and floor of the mouth (Figure 1). The oral cavity is lined by the buccal, sublingual, gingival, palatal, and labial mucosa, which account for ~60% of the surface area of the oral mucosa [19]. The buccal region describes that part of the mouth bounded interiorly and laterally by the lips and the cheeks; posteriorly and medially by the teeth and gums; and superiorly and inferiorly by the mucosal reflections from the lips and cheeks to the gums. There are two different types of glands (mucous and serous) present in the cheek submucosa, and the buccal glands lie between the mucous membrane and blood supplied by the maxillary artery, which provides a rich blood supply to the sublingual area (compared with the gingival and palatal areas). Drug diffusion is passive, and the high surface area of the bumpy, 500–800 μm-thick buccal mucosa is ideally suited for sustained drug delivery systems. The buccal mucosa has a multi-layered structure, uppermost being the non-keratinized stratified squamous epithelium (thickness ~500–600 μm and surface area 50.2 cm2), which is shed every 5–6 days [20] and acts as a protective layer [21]. Underlying this is the basement membrane, capillary-rick lamina propria, and submucosa.
Diseases of the oral cavity
Oral cancer
Oral cancers can arise from the cells of the mucosa or underlying tissues. Cancer lesions are often visible on physical examination, sometimes as discrete masses or as white, precancerous lesions (leukoplakia) [22]. These lesions can cause inflammatory symptoms through lymphatic blockage. Over 90% of reported cancers of the upper region of neck, head, and buccal cavity are squamous cell carcinomas [23,24]. While radiotherapy and surgery are the main treatments for these cancers [25], delivery of anticancer drugs, especially to the buccal region (Figure 2), is considered a reasonable and clinically effective therapeutic option [25,26]. Anticancer drug delivery to the near mucosal region is also useful since it minimizes side-effects, the dose required, and augments therapeutic efficacy compared with conventional systemic delivery. For instance, doxorubicin loaded into liposomal structures are further controlled by embedding into alginate gels were fabricated to treat squamous cell cancers. The polymer mediated adhesion to the mucosa, while the liposomal particles shielded the drug from degradation and enhanced absorption of the liposomal carriers into tumor cells. The formulated liposomes were 122-137 nm, with experimental stability up to 26 h. This liposomal-based alginate paste effectively killed human cancer cells (CWEL-27) in vitro [27].
Microbial infections
The oral cavity has a dynamic and abundant microbiome, primarily aerobic and anaerobic bacteria from ~500 different identified species. Saliva contains a large concentration of about 107 and 108 bacteria per ml, and the bacteria can be harmless (or even protective) commensals or pathogens [29]. Mouth health depends on the integrity of the mucosa, which in turn relies on intact host immune responses acting through oral secretions (i.e., the saliva and mucus) [30]. The constant flow and secretion of saliva maintains the pH of the oral cavity and helps prevent demineralization of enamel by forming a protective, antibacterial protein coat over the teeth [31]. Saliva contains proteins, glycoproteins, amylase, mucin, lysozyme, immunoglobulins, lactoferrin, and sialoperoxidase, which may interfere with the normal flora [32]. Microbes tend to be unevenly distributed in the oral cavity, with specific organisms attaching to and growing on tooth surfaces to form colonies that produce biofilms [33], yellowish-white deposits that become firmly attached to the tooth. Dental plaque is formed by the colonization of several bacteria [34]. Microorganism aggregation on the tooth surface is promoted by sugar, low pH, and reduced salivary flow [35]. Dental plaque is the main etiological factor contributing to the formation of caries and periodontal infections. The concentrations of Gram-negative and anaerobic bacteria increase in dental biofilm with time, and Gram-negative organisms in particular attach in high numbers to epithelial cells. Bacterial oral infections mainly occur when the oral flora become opportunistic and works against host immune responses rather than from external infections [36]. The causative microbial agents in periodontitis are shown in Table 1.
Gingivitis
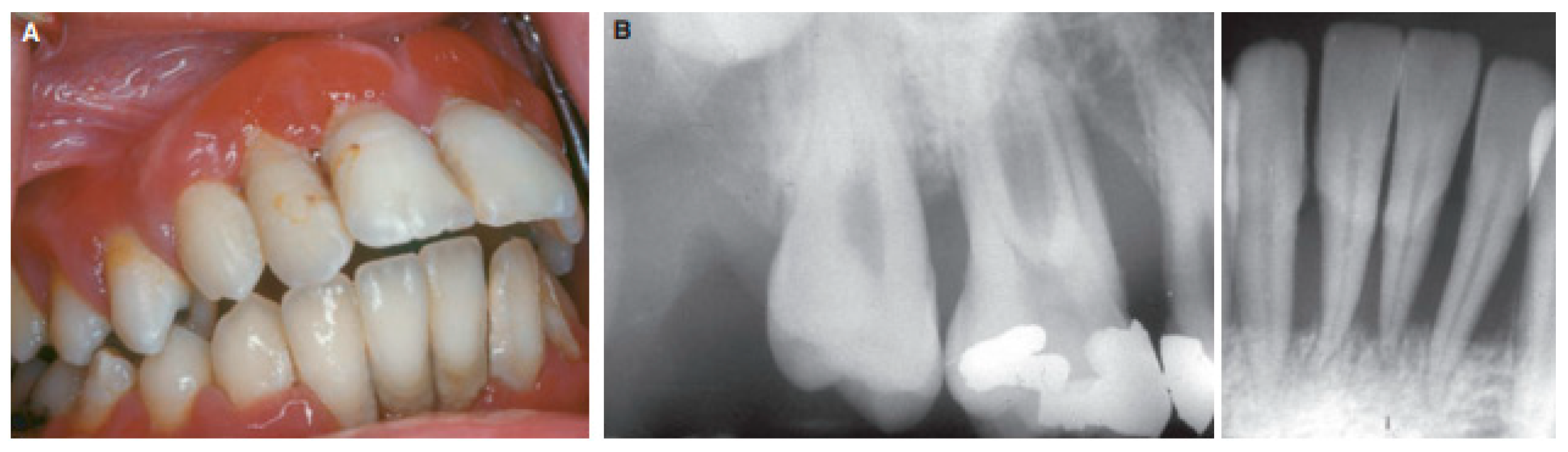
The gingivae (gums) form part of the soft tissue lining of the oral cavity covering the teeth and providing a seal around them. The gingivae cover the alveolar processes of the jaws and the cervical portions of the teeth, and they are divided into free, attached, and interdental papillae [37]. Gingivitis (Figure 3) describes inflammation of the gingival tissues due to aggregation of plaque on the tooth surfaces and it is characterized by edema and bleeding on probing [38]. On its own, gingivitis does not describe alveolar bone loss and it is reversible. Normal gingivae are light pink to red due to high vascularity and the thin epithelium [39], but when inflamed the red color increases due to the inflammation and even when not painful bleeding can occur after probing [40].
Gingivitis represents a disease of poor oral hygiene and lack of control of biofilm, where poor oral hygiene creates a favorable environment for oral microbes to gain access to the marginal gingiva to trigger inflammatory responses. Acute lesions contain neutrophil infiltrates which, after 2-5 days, change due to aggregation of macrophages and lymphocytes, vascular changes, and perivascular inflammatory infiltrates. Gingivitis follows a delayed hypersensitivity-type pattern of inflammatory response, similar to macrophage lesions, while periodontitis is characterized by B cell and plasma cell infiltrates [41].
Figure 3.
(A) Gingival periodontitis in a young male patient, (B) X-rays showing significant calcium loss from the teeth (taken with permission from [42]).
Figure 3.
(A) Gingival periodontitis in a young male patient, (B) X-rays showing significant calcium loss from the teeth (taken with permission from [42]).
Epidemiological studies have provided evidence that bacterial biofilm on the tooth surfaces and gingival margin are responsible for gingivitis and periodontitis [43]. Gram-positive bacteria initially form colonies over the enamel surface of teeth, followed by colonization with Gram-negative anaerobic cocci, filaments, and spirochetes in the marginal gingiva to develop complex plaque [44]. Uncontrolled gingivitis progresses towards periodontitis, which is classified by the American Academy of Periodontology as shown in Table 2.
Pain and inflammation control
Inflammation due to injury or cell death in the oral mucosa is characterized by proliferation of inflammatory mediators causing swelling that is followed by repair of the wound. During inflammation, localized cytokine production (IL-2, IL-6, LTPB-1, and IL-10) and cellular infiltrates both contribute to the pathology. The first few hours after injury are important because of infiltration of immune cells (neutrophils and T cells), which help to resolve local pro-inflammatory cytokine production, like interleukins. Macrophage infiltration into the injured oral cavity is reported to be lower than that seen in dermal wound healing, possible due to saliva-associated provision of growth factors. Indeed, the rate of re-epithelization is higher (100%) in oral epithelial defects compared with dermal defects (40%) 24 h after injury [46,47,48,49], and there is evidence that some inflammatory regulators are expressed at comparatively low levels in adult buccal epithelial cells compared with the skin (e.g. IL-6) [46]. Nevertheless, cytokines and interleukin inhibitors are frequently employed in the buccal region in mucoadhesive drug delivery systems [50], and adequate inflammation resolution necessitates high local concentrations of therapeutic drugs like non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroids, or opioids.
Pain is a feature of most oral cavity diseases including microbial infections, tumors, and trauma. All the common analgesics and anti-inflammatory agents have been used intraorally to control pain and inflammation including NSAIDs, opioids, and corticosteroids [51,52,53]. Since opioids can act locally on nerves, it is thought that the drugs first diffuse through the buccal paracellular pathway to reach the nerves locally. For severe pain, drug combinations have been used [54].
Local anesthetics
Local anesthetic agents are widely used for local pain control. Anesthetic agents block pain by inhibiting the nerve impulses and therefore pain perception. As a result, pain is reduced and patients achieve symptomatic control [55]. Local anesthetics have been combined with other locally acting agents [52]. Recently, mebeverine, an antispasmodic, was investigated for its anesthetic potential in the buccal cavity [56]. Lignocaine is the most commonly used topical anesthetic agent delivered through the mucoadhesive buccal route [57,58,59], followed by benzocaine [60,61] and articaine [62]. Lignocaine and benzocaine have been tested in healthy volunteers for the treatment of local oral cavity pain [63].
Steroidal anti-inflammatory agents
There have been efforts to develop mucoadhesive delivery of dexamethasone [64], hydrocortisone [65], prednisolone [66], clobetasol [67], and betamethasone [68] for the treatment of oral ulcers through the restoration of damaged mucosal and submucosal tissues. Hydrocortisone has a reasonable safety profile compared with other steroidal agents [69].
Other drug classes
Other drugs have been formulated for the mucoadhesive route for local action including the delivery of local antiseptic agents like benzydamine, tibezonium iodide, chlorhexidine, and other agents [4,70]. These substances can be delivered alone [68] but are usually combined with local agents for the clinical improvement of symptoms. Likewise, calcium fluoride has been successfully delivered through nanoparticulate delivery to improve dental conditions [71]. Secretagogues, which increase salivary secretions, have been successfully delivered via the mucoadhesive buccal route [72]. Table 3 summarizes commonly encountered pathologies of the oral cavity and suitable therapeutic strategies.
Table 4 details some of the drugs commonly used for local pathologies of the oral cavities.
Nanotechnological formulations
Nanoparticles (NPs)
Nanoparticles (NPs) represent a versatile form of drug delivery vehicle that can easily be dispersed in different formulations to treat local pathologies. NPs can have complex appearances or double compartments to sequester the drug. Similarly, the polymeric layers of NPs can serve as a platform for drug delivery [91]. Polymeric nanoparticles can be formulated with biodegradable substances such as polyethylene glycol (PEG), polylactic acid, polylactide coglycolide, polycyanoacrylate, chitosan, gelatin, and sodium alginate [92,93,94,95,96]. Formulations using these substances have tunable properties that allow controlled drug release. Various methods are frequently used to prepare these nanoparticles including ionic gelation, nanoprecipitation, spray drying, cross-linking, solvent evaporation, and in situ polymerization, with technologies like supercritical fluid technology and the reverse micellar technique less commonly used. The therapeutic substance is normally loaded into the nano-sized formulation through entrapping, drug-polymer complexing, the solubility phenomenon, or by dispersing the active substance throughout the medium. This, in turn, acts as a reservoir for the release of the drug over a longer period. This is only possible when the dosage form is in the retentive state with the buccal mucosa or, alternatively, the particles penetrate the deeper tissue layers. This is beneficial for, for example, delivering anticancer drugs to buccal carcinomas [97]. In one study, buccal carcinoma was targeted through PEGylated poly-lactide co-glycolide (PLGA) nanoparticles grafted with RGD-peptidomimetic substance, which was designed to facilitate attachment to the tumor endothelium. Paclitaxel was chosen as the anticancer drug due to its well-established cytotoxicity. In mice, nano-delivery increased tumor control when decorated with RGD-peptide compared with non-labeled delivery. Furthermore, tumor uptake of radiolabeled peptidomimetic-based nanoparticles was greater than nanoparticles delivered alone (Figure 4), confirming that nanoparticle uptake and consequent drug delivery can be improved by surface modification [98].

Table 5.
Nanotechnological formulations for localized action.
| Dosage/ Delivery | Drug | Polymer(s) | Method of preparation | Oral pathology | Reference |
|---|---|---|---|---|---|
| Nanoparticles | Curcumin | Chitosan (coating) polycaprolactone |
Nanoprecipitation | Oral cancer | [2] |
| Nanogels | Lignocaine hydrochloride monohydrate | Catechol, chitosan, genipin | Conjugation, polymerization | Local anesthetic | [99] |
| Electrospun fiber in patch | Clobetasol-17- propionate | Polyethylene oxide, polyvinyl pyrollidone, eudragit, polycaprolactone | Electrospinning | Anti-inflammatory | [67] |
| Nanoparticles | Doxorubicin | poly (ethylene glycol)-block-poly (4-vinylbenzylphosphonate | Solvent evaporation | Anti-cancer | [92] |
| Nanoparticles | Genistein | (D,L) Lactic acid | Emulsion diffusion method | Anti-cancer and phytoestrogen | [94] |
| Nanoparticles | Gene delivery | poly(DLlactide-co-glycolide) | Probe sonication | Drug and gene delivery | [95] |
| Nanoparticles in film | Calcium fluoride and lignocaine | Thiolated chitosan | Co-precipitation and polymer synthesis | Dental caries | [71] |
| Peptide grafting nanoparticle | Paclitaxel | Polylactide co-glycolide, RGD-peptide, polyethylene glycol | Polymer synthesis and peptide grafting | Oral cancer | [98] |
One study demonstrated a significant reduction in human oral squamous cell carcinoma growth through treatment with curcumin in chitosan-coated polycaprolactone-based NPs. There was no significant loss of cell viability even at 24 h when curcumin was not loaded on the nanoparticles, and cytotoxicity of free curcumin was significantly higher (p<0.05) at the IC50 dose of the drug than coated NPs [2]. NPs were formed by nanoprecipitation using evaporation of the organic phase (acetone) containing the lipophilic polymers. The aqueous phase was composed of acidified water with 1% acetic acid. Chitosan was added to the buccal dosage form as an adhesive agent for prolonged buccal attachment, since mucin is negatively charged through sulfate and carboxyl groups in the constituent oligosaccharides [100]. With respect to human cell viability studies, there was no apoptosis with control treatments, whereas curcumin-loaded chitosan-coated NPs (Cur-NP CSL) induced apoptosis (Figure 5). The coated NPs exhibited electrostatic interactions with mucin, i.e., the mucoadhesive property. Since chitosan possesses antimicrobial properties, chitosan-based NPs delivery is a promising drug delivery approach for localized delivery of natural anticancer drugs.
Nanogels
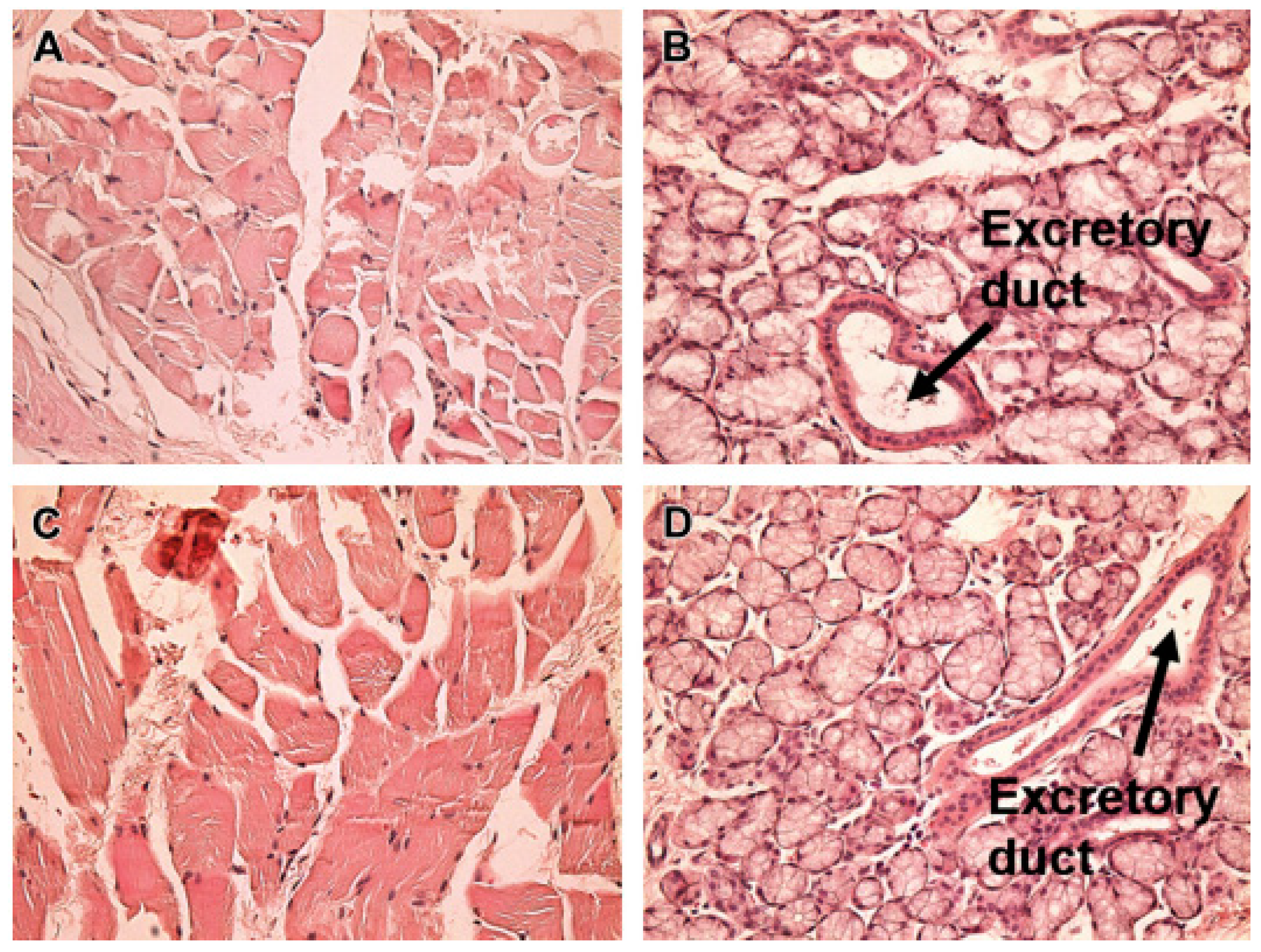
Mucoadhesive gels represent a formulation in which the drug is loaded and entrapped in the polymeric network of the gel [63]. The rate of drug release depends on both the viscosity of the gel and the nature and quality of the polymers [90]. The dose can be adjusted in gels and, moreover, the dose can be administered over a unit area for better contact, swelling, and effective drug release [101,102]. A scaffold or cross-linked gel structure increases the drug loading capacity. For example, genipin was cross-linked with catechol chitosan to provide a platform to load lignocaine for local delivery. Mucoadhesion was improved when catechol was covalently bound, while gels with chitosan (catechol not attached) had lower mucoadhesive contact time. Furthermore, the formulated gels did not induce inflammation in sacrificed rabbit tissue (Figure 6) [99]. Recently, a study evaluated salivary drug concentrations of the antiseptic and anesthetic agents tibezonium iodide and benzocaine, respectively, achieved through application of scaffold gels. The initial formulation (Figure 7) was prepared through homogenization of ingredients in aqueous solution and stored at room temperature [102]. Furthermore, in a study of the mucoadhesive role of agarose gel and Carbopol 934P, the concentration of agarose was responsible for sustained drug release. The dosage form was stable for up to six months. In healthy volunteers, salivary drug concentrations (Figure 8) correlated with mucosal numbness (Table 6). This study concluded that the formulation provided a suitable vehicle to sustain the release and effective salivary drug concentrations to treat sore throats [90].
Figure 6.
H&E-stained sections of untreated rabbit buccal mucosa (A and B) or treated with genipin-chitosan cross-linked nanogels (C and D) (figure reproduced with permission from [99]).
Figure 6.
H&E-stained sections of untreated rabbit buccal mucosa (A and B) or treated with genipin-chitosan cross-linked nanogels (C and D) (figure reproduced with permission from [99]).
Another triple-blind, randomized controlled study evaluated the efficacy of the steroidal drug triamcinolone in volunteers with oral lichen planus. Almost 40 volunteers were allocated to treatment with either a nanogel formulation or conventional delivery. The nanogel formulation healed ulcers significantly faster than conventional therapy (Table 6) [103].
Table 6.
Clinical and preclinical outcomes of different formulations.
| Drug | Dosage form | Subjects | Settings | Clinical outcomes | References |
|---|---|---|---|---|---|
| Triamcinolone | Nanogels | Diseased volunteers | Triple blind, randomized | Nano delivery accelerated healing | [103] |
| Clobetasol | Patch | Healthy subjects | Single center | Better adherence and less irritation | [67] |
| Tibezonium iodide | Gels | Healthy volunteers | Single center | Agarose-carbopol showed superior mucoadhesion Dosage form adaptable to volunteers Stable for up to 6 months |
[90] |
Buccal film-loaded nanotechnology
Buccal films are flattened strips typically fabricated with controlled evaporation of solvent to produce uniform film appearance and thickness. These films are resistant to folding and are more easy applied in the cavity or near to the pathological sites [104].
Since many buccal cavity disorders involve swelling and inflammation caused by infection, efforts have been made to introduce probiotics to competitively inhibit the growth of pathogens causing periodontitis [105,106]. For example, Lactobacillus brevis CD2 produces arginine deaminase [107], which competes with eukaryotic nitric oxide synthase to convert arginine into ammonia rather than nitric oxide [108], the latter a pro-inflammatory agent. When probiotics were delivered through a mucoadhesive buccal film, the conversion of arginine to nitric oxide was inhibited to exert an anti-inflammatory effect [109]. These mucoadhesive buccal films were composed of hydroxypropyl methylcellulose and polypropylene glycol through a solvent casting method. The dosage form was formulated and stored at two different conditions, 2-8oC and 23-25oC, the former better preserving microbe viability [110]. The dosage form was considered an effective intervention to reduce the progression of periodontal disease. The surface morphology of the films may also be modified using techniques like electrospinning, which has been especially useful for pathologies such as wound healing [111]. Rarely, the drug may be distributed to two different compartments, such as where the ethylcellulose base-containing film layer of the buccal mucoadhesive delivery system contains the anti-inflammatory drug through fused deposition. The surface, in this scenario, was modified by adding a layer of local anesthetic through 3D printing, where drug release was also controlled by the ink viscosity. Permeation studies in porcine buccal mucosa demonstrated a steady-state concentration of ketoprofen of 2.0 µg/cm2/min over a period of 6 h and 0.9 µg/cm2/min for lignocaine hydrochloride. There was no cytotoxicity using the formulated film in vitro (tetrazolium bromide MTT assay). The buccal films prepared using this combination technology had a few advantages, such as surface modifiability, which is sometimes difficult to achieve without cross-linking. Likewise, two separate compartments were produced, which were useful for loading two independent drugs or sometimes physically incompatible drugs when delivered in a single medium. Moreover, this approach can also be used for differential release of a single pharmaceutical substance if different repellant materials are added to different compartments of the inkjet-layered films. Another notable advantage of this form of drug delivery is the delivery of a relatively heat stable substance in the inkjet layer covering the film dosage form, since the films are produced by a technique that typically involves heat. So, any component to be omitted from heating can be loaded on the inkjet. In one study, the films were printed with 3D printing technology that produced a uniform consistency of the film and backing layer. This is shown in Figure 9, where stereoscopic images of the films demonstrated a consistent smooth appearance and even thickness with a standard deviation of 0.03. The films were translucent but rough on scanning electron microscopy (SEM). However, the consistency and absence of surface cracks (Figure 9d–f) had more favorable characteristics [54]. Such combinations of pharmaceutical technologies have been successfully explored to fabricate buccal films for treating xerostomia by simultaneous use of adipic acid and xylitol [79].
Patches
In patches, the drug matrix is supported by a support layer, and they are applied to the buccal mucosa to subsequently release the drug. Patches, like films, are thin layers [112]. Adhesion can be achieved through the addition of any mucoadhesive agent. One study demonstrated delivery of the steroidal anti-inflammatory drug clobetasol propionate for the treatment of aphthous ulcers and stomatitis, reasoning that persistent contact of steroid with a mucoadhesive patch would accelerate healing. The backing layer was designed to prevent spread of the drug into in buccal cavity, as shown for mucoadhesive buccal gels [113]. The polymeric patches were formulated using different concentrations of polyvinylpyrrolidone, Eudragit RS10, and polyethylene oxide with polycaprolactone as the backing layer using an electrospinning technique [67]. The formulation did not exert any cytotoxicity in tissue-engineered buccal mucosa washed with formalin before evaluation. When applied to healthy volunteers, the patch showed good to excellent adherence at the point of application (Figure 10 and Figure 11), although a few volunteers reported moderate mucosal irritation after patch application of patch (Figure 11).
The backing layer of the patch is often layered as an impermeable layer so that the flux of the active substance does not move in the transcellular and paracellular route for systemic absorption. Otherwise, a significant amount of the locally acting drug may be lost while delivering the medication.
Nanofibers
Nanofibers are nano-sized mats, porous flattened discs, or surface-modified structures that are eventually delivered or loaded onto another buccal dosage form to achieve local delivery [114]. Nanofibers have been extensively used in medical devices and drug delivery [115,116]. The nanofibers are usually fabricated by dispersing drug in the solution of polymer or vice versa, and the solution is slightly modified with a suitable plasticizer to impart properties to the fiber [117]. Nanofibers have been evaluated for the systemic delivery of drugs through the buccal route. Nevertheless, they may also be used to treat local pathologies. These fibers are usually fabricated using electrospinning and 3D printing or a combination of both techniques. Then, the dense nanosized fibers are either delivered in their native form or further processed to form films [54]. Nanofibers have also been used in would healing. For example, in an attempt to develop and fabricate a platform for wound healing, Palo and colleagues formulated bilayered fabricated fibers using sodium alginate and polyvinyl alcohol. They used a solvent casting technique aided by either 3D printing or electrospinning to alter the surface properties of the carriers. They found that electrospun fibers displayed improved physical durability and the nanofibers, when immersed in phosphate buffer in a stability test for 7 days, had preserved integrity with a swollen but soft structure (Figure 13) [111].
Figure 13.
SEM images of A. the fabricated nanofibers and B. appearance of the fibers after 7 days dipped in phosphate buffer at 37°C. Reprinted with permission from [111].
Preclinical and clinical findings
The effort to provide improved local drug concentrations has led researchers to study the effect of drug and the dosage form in both animals [118] and human subjects [119], both healthy and with disease. In animal studies, the nanotechnology formulation is usually compared against conventional or simpler techniques. For example, in a rat model, periodontitis was treated with the gold standard antibiotic (metronidazole) loaded into quaternary ammonium-derived chitosan nanoparticles placed in the intra-peritoneal pocket in the affected tooth of the experimental animal. Then, clinical parameters, food consumption, blood biochemistry, body weight, tooth mobility, and gingival index were measured by comparing treatment with control groups. The results showed that periodontal symptoms were relieved in the group receiving antibiotic-loaded nanoparticles with improvements in alveolar bone loss. Antibiotic nanoparticles dosed at 1.8 and 3.6 mg/mL inhibited P. gingivalis. These findings significantly support the validity of localized nano-delivery of antibiotics. It also reduced the oral dose required to achieve the inhibitory concentration of metronidazole and associated side effects [118]. The efficacy of fabricated triamcinolone acetonide nanogels (vs. conventional triamcinolone gel) was also evaluated in volunteers in a triple-blind, randomized study, with outcomes of pain score and the size of the nodule. The study found that there was a greater reduction in pain severity with steroidal nanogel compared with conventional gel (pain score of 1.5 and 1.8, respectively), while there was a two-fold reduction in the nodule size [103].
Conclusions
Localized drug delivery, especially when coupled with nanotechnology-based formulations, offers advantages in terms of improved efficacy and reduced drug-associated hazards. The mucoadhesive buccal platform can be modified with a variety of formulations that can be used as a vehicle for different drugs. Natural and semisynthetic polymers are safer in terms of cytotoxicity and are easily adaptable to patients. The local action of mucoadhesive delivery can be refined through nanoparticulate drug delivery or modification of the surface in contact with the buccal mucosa to effectively release drug into the cavity.
Funding
No specific funding for this work.
References
- Kenechukwu, F.C.; Attama, A.A.; Ibezim, E.C. Novel solidified reverse micellar solution-based mucoadhesive nano lipid gels encapsulating miconazole nitrate-loaded nanoparticles for improved treatment of oropharyngeal candidiasis. Journal of Microencapsulation 2017, 34, 592–609. [Google Scholar] [CrossRef] [PubMed]
- Mazzarino, L.; Loch-Neckel, G.; Bubniak, L.d.S.; Mazzucco, S.; Santos-Silva, M.C.; Borsali, R.; Lemos-Senna, E. Curcumin-loaded chitosan-coated nanoparticles as a new approach for the local treatment of oral cavity cancer. Journal of nanoscience and nanotechnology 2015, 15, 781–791. [Google Scholar] [CrossRef] [PubMed]
- Boden, W.E.; Padala, S.K.; Cabral, K.P.; Buschmann, I.R.; Sidhu, M.S. Role of short-acting nitroglycerin in the management of ischemic heart disease. Drug Design, Development and Therapy 2015, 9, 4793. [Google Scholar] [PubMed]
- Hanif, S.; Sarfraz, R.M.; Syed, M.A.; Ali, S.; Iqbal, Z.; Shakir, R.; Iqbal, J. Formulation and evaluation of chitosan-based polymeric biodegradable mucoadhesive buccal delivery for locally acting drugs: In vitro, ex vivo and in vivo volunteers characterization. 2021.
- Pather, S.I.; Rathbone, M.J.; Şenel, S. Current status and the future of buccal drug delivery systems. Expert Opinion on Drug Delivery 2008, 5, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Kaul, M.; Rawat, A.; Saini, S. An overview on buccal drug delivery system. International journal of pharmaceutical sciences and research 2011, 2, 1303. [Google Scholar]
- Hassan, N.; Ahad, A.; Ali, M.; Ali, J. Chemical permeation enhancers for transbuccal drug delivery. Expert opinion on drug delivery 2010, 7, 97–112. [Google Scholar] [CrossRef]
- Razzaq, S.; Syed, M.A.; Irfan, M.; Khan, I.; Sarfraz, R.M.; Shakir, R.; Ali, S.; Iqbal, Z.; Niaz, Y.; Mujtaba, S.H. Optimization of metronidazole SR buccal tablet for gingivitis using genetic algorithm. Pakistan Journal of Pharmaceutical Sciences 2021, 34. [Google Scholar]
- Marques, A.C.; Rocha, A.I.; Leal, P.; Estanqueiro, M.; Lobo, J.M.S. Development and characterization of mucoadhesive buccal gels containing lipid nanoparticles of ibuprofen. International Journal of Pharmaceutics 2017, 533, 455–462. [Google Scholar] [CrossRef]
- Pham, M.N.; Van Vo, T.; Tran, V.-T.; Tran, P.H.-L.; Tran, T.T.-D. Microemulsion-based mucoadhesive buccal wafers: wafer formation, in vitro release, and ex vivo evaluation. AAPS PharmSciTech 2017, 18, 2727–2736. [Google Scholar] [CrossRef]
- Abruzzo, A.; Cerchiara, T.; Bigucci, F.; Gallucci, M.C.; Luppi, B. Mucoadhesive buccal tablets based on chitosan/gelatin microparticles for delivery of propranolol hydrochloride. Journal of pharmaceutical sciences 2015, 104, 4365–4372. [Google Scholar] [CrossRef]
- Nafee, N.A.; Boraie, M.A.; Ismail, F.A.; Mortada, L.M. Design and characterization of mucoadhesive buccal patches containing cetylpyridinium chloride. Acta pharmaceutica (Zagreb, Croatia) 2003, 53, 199–212. [Google Scholar] [PubMed]
- Silva, B.M.; Borges, A.F.; Silva, C.; Coelho, J.F.; Simões, S. Mucoadhesive oral films: the potential for unmet needs. International journal of pharmaceutics 2015, 494, 537–551. [Google Scholar] [CrossRef] [PubMed]
- Poonia, M.; Ramalingam, K.; Goyal, S.; Sidhu, S.K. Nanotechnology in oral cancer: A comprehensive review. Journal of oral and maxillofacial pathology: JOMFP 2017, 21, 407. [Google Scholar]
- Hafez, M.M.; Aboulwafa, M.M.; Yassien, M.A.; Hassouna, N.A. Activity of some mucolytics against bacterial adherence to mammalian cells. Applied biochemistry and biotechnology 2009, 158, 97–112. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Zhang, J.; Shan, W.; Huang, Y. Developments of mucus penetrating nanoparticles. Asian Journal of Pharmaceutical Sciences 2015, 10, 275–282. [Google Scholar] [CrossRef]
- Ensign, L.M.; Lai, S.K.; Wang, Y.-Y.; Yang, M.; Mert, O.; Hanes, J.; Cone, R. Pretreatment of human cervicovaginal mucus with pluronic F127 enhances nanoparticle penetration without compromising mucus barrier properties to herpes simplex virus. Biomacromolecules 2014, 15, 4403–4409. [Google Scholar] [CrossRef]
- Lai, S.K.; Wang, Y.-Y.; Hida, K.; Cone, R.; Hanes, J. Nanoparticles reveal that human cervicovaginal mucus is riddled with pores larger than viruses. Proceedings of the National Academy of Sciences 2010, 107, 598–603. [Google Scholar] [CrossRef]
- Gandhi, R.B.; Robinson, J.R. Oral cavity as a site for bioadhesive drug delivery. Advanced drug delivery reviews 1994, 13, 43–74. [Google Scholar] [CrossRef]
- Sudhakar, Y.; Kuotsu, K.; Bandyopadhyay, A. Buccal bioadhesive drug delivery—a promising option for orally less efficient drugs. Journal of Controlled Release 2006, 114, 15–40. [Google Scholar] [CrossRef]
- Nanci, A. Ten Cate's Oral Histology-Pageburst on VitalSource: Development, Structure, and Function; Elsevier Health Sciences: 2007.
- Silk, H. Diseases of the mouth. Primary care: Clinics in office practice 2014, 41, 75–90. [Google Scholar] [CrossRef]
- Prince, A.; Aguirre-Ghizo, J.; Genden, E.; Posner, M.; Sikora, A. Head and neck squamous cell carcinoma: new translational therapies. Mount Sinai Journal of Medicine: A Journal of Translational and Personalized Medicine 2010, 77, 684–699. [Google Scholar] [CrossRef] [PubMed]
- Rapidis, A.D.; Wolf, G.T. Immunotherapy of head and neck cancer: current and future considerations. Journal of oncology 2009, 2009. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.P.; Gil, Z. Current concepts in management of oral cancer–surgery. Oral oncology 2009, 45, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Florea, A.-M.; Büsselberg, D. Cisplatin as an anti-tumor drug: cellular mechanisms of activity, drug resistance and induced side effects. Cancers 2011, 3, 1351–1371. [Google Scholar] [CrossRef]
- Shtenberg, Y.; Goldfeder, M.; Prinz, H.; Shainsky, J.; Ghantous, Y.; El-Naaj, I.A.; Schroeder, A.; Bianco-Peled, H. Mucoadhesive alginate pastes with embedded liposomes for local oral drug delivery. International journal of biological macromolecules 2018, 111, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Almangush, A.; Pirinen, M.; Heikkinen, I.; Mäkitie, A.A.; Salo, T.; Leivo, I. Tumour budding in oral squamous cell carcinoma: a meta-analysis. British journal of cancer 2018, 118, 577–586. [Google Scholar] [CrossRef]
- Addy, M. Local delivery of antimicrobial agents to the oral cavity. Advanced drug delivery reviews 1994, 13, 123–134. [Google Scholar] [CrossRef]
- Rindom Schiött, C.; Löe, H.; Børglum Jensen, S.; Kilian, M.; Davies, R.; Glavind, K. The effect of chlorhexidine mouthrinses on the human oral flora. Journal of Periodontal Research 1970, 5, 84–89. [Google Scholar] [CrossRef]
- Edgar, W. Saliva: its secretion, composition and functions. British dental journal 1992, 172, 305–312. [Google Scholar] [CrossRef]
- Marsh, P.D. Role of the oral microflora in health. Microbial ecology in health and disease 2000, 12, 130–137. [Google Scholar] [CrossRef]
- Lamont, R.; Jenkinson, H. Adhesion as an ecological determinant in the oral cavity. Oral bacterial ecology: the molecular basis 2000, 131-168.
- Puy, C.L. The role of saliva in maintaining oral health and as an aid to diagnosis. Med Oral Patol Oral Cir Bucal 2006, 11, 449–455. [Google Scholar]
- Bernimoulin, J.P. Recent concepts in plaque formation. Journal of Clinical Periodontology 2003, 30, 7–9. [Google Scholar] [CrossRef] [PubMed]
- Fine, D.; Furgang, D.; Lieb, R.; Korik, I.; Vincent, J.; Barnett, M. Effects of sublethal exposure to an antiseptic mouthrinse on representative plaque bacteria. Journal of clinical periodontology 1996, 23, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Trombelli, L.; Tatakis, D.N.; Scapoli, C.; Bottega, S.; Orlandini, E.; Tosi, M. Modulation of clinical expression of plaque-induced gingivitis. Journal of clinical periodontology 2004, 31, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Dean, J.A.; Avery, D.R.; McDonald, R.E. McDonald and Avery dentistry for the child and adolescent; Elsevier Health Sciences: 2010.
- Barnett, M.L. The role of therapeutic antimicrobial mouthrinses in clinical practice: control of supragingival plaque and gingivitis. The Journal of the American Dental Association 2003, 134, 699–704. [Google Scholar] [CrossRef]
- Armitage, G. Diagnosis of periodontal diseases. Journal of periodontology 2003, 74, 1237–1247. [Google Scholar] [CrossRef]
- Ohlrich, E.; Cullinan, M.; Seymour, G. The immunopathogenesis of periodontal disease. Australian dental journal 2009, 54, S2–S10. [Google Scholar] [CrossRef]
- Armitage, G.C.; Cullinan, M.P. Comparison of the clinical features of chronic and aggressive periodontitis. Periodontology 2000 2010, 53, 12–27. [Google Scholar] [CrossRef]
- Salvi, G.E.; Aglietta, M.; Eick, S.; Sculean, A.; Lang, N.P.; Ramseier, C.A. Reversibility of experimental peri-implant mucositis compared with experimental gingivitis in humans. Clinical oral implants research 2012, 23, 182–190. [Google Scholar] [CrossRef]
- Lang, N.P.; Schätzle, M.A.; Löe, H. Gingivitis as a risk factor in periodontal disease. Journal of clinical periodontology 2009, 36, 3–8. [Google Scholar] [CrossRef]
- Plancak, D.; Jorgic–Srdjak, K.; Curilovic, Z. New Classification of Periodontal Diseases. Acta Stomat Croat 2001, 35, s9–s93. [Google Scholar]
- Szpaderska, A.; Zuckerman, J.; DiPietro, L. Differential injury responses in oral mucosal and cutaneous wounds. Journal of dental research 2003, 82, 621–626. [Google Scholar] [CrossRef] [PubMed]
- DiPietro, L.A. Wound healing: the role of the macrophage and other immune cells. Shock (Augusta, Ga.) 1995, 4, 233–240. [Google Scholar] [CrossRef] [PubMed]
- DiPietro, L.A.; Burdick, M.; Low, Q.E.; Kunkel, S.L.; Strieter, R.M. MIP-1alpha as a critical macrophage chemoattractant in murine wound repair. The Journal of clinical investigation 1998, 101, 1693–1698. [Google Scholar] [CrossRef] [PubMed]
- Ashcroft, G.S.; Lei, K.; Jin, W.; Longenecker, G.; Kulkarni, A.B.; Greenwell-Wild, T.; Hale-Donze, H.; McGrady, G.; Song, X.-Y.; Wahl, S.M. Secretory leukocyte protease inhibitor mediates non-redundant functions necessary for normal wound healing. Nature medicine 2000, 6, 1147–1153. [Google Scholar] [CrossRef] [PubMed]
- Zewail, M.B.; Asaad, G.F.; Swellam, S.M.; Abd-Allah, S.M.; Hosny, S.K.; Sallah, S.K.; Eissa, J.E.; Mohamed, S.S.; El-Dakroury, W.A. Design, characterization and in vivo performance of solid lipid nanoparticles (SLNs)-loaded mucoadhesive buccal tablets for efficient delivery of Lornoxicam in experimental inflammation. International Journal of Pharmaceutics 2022, 624, 122006. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Cui, Y.; Zhang, L.; Zhu, H.-p.; Guo, Y.-S.; Zhong, B.; Hu, X.; Zhang, L.; Wang, X.-h.; Chen, L. Thermosensitive and mucoadhesive in situ gel based on poloxamer as new carrier for rectal administration of nimesulide. International journal of pharmaceutics 2012, 430, 114–119. [Google Scholar] [CrossRef]
- Hussain, A.; Syed, M.A.; Abbas, N.; Hanif, S.; Arshad, M.S.; Bukhari, N.I.; Hussain, K.; Akhlaq, M.; Ahmad, Z. Development of ann optimized mucoadhesive buccal tablet containing flurbiprofen and lidocaine for dental pain. Acta Pharmaceutica 2016, 66, 245–256. [Google Scholar] [CrossRef]
- Daneshmehr, M.A.; Adibpour, H.; Ataie, Z. Formulation and Evaluation of Hydrocortisone Sodium Succinate Mucoadhesive Buccal Tablet. International Journal of Pharmaceutical Investigation 2020, 10, 300–304. [Google Scholar] [CrossRef]
- Eleftheriadis, G.K.; Monou, P.K.; Bouropoulos, N.; Boetker, J.; Rantanen, J.; Jacobsen, J.; Vizirianakis, I.S.; Fatouros, D.G. Fabrication of mucoadhesive buccal films for local administration of ketoprofen and lidocaine hydrochloride by combining fused deposition modeling and inkjet printing. Journal of Pharmaceutical Sciences 2020, 109, 2757–2766. [Google Scholar] [CrossRef]
- Preis, M.; Woertz, C.; Schneider, K.; Kukawka, J.; Broscheit, J.; Roewer, N.; Breitkreutz, J. Design and evaluation of bilayered buccal film preparations for local administration of lidocaine hydrochloride. European Journal of Pharmaceutics and Biopharmaceutics 2014, 86, 552–561. [Google Scholar] [CrossRef]
- Hasan, A.A.; Samir, R.M.; Abu-Zaid, S.S.; Lila, A.S.A. Revitalizing the local anesthetic effect of Mebeverine hydrochloride via encapsulation within ethosomal vesicular system. Colloids and Surfaces B: Biointerfaces 2020, 194, 111208. [Google Scholar] [CrossRef]
- Kottke, D.; Majid, H.; Breitkreutz, J.; Burckhardt, B.B. Development and evaluation of mucoadhesive buccal dosage forms of lidocaine hydrochloride by ex-vivo permeation studies. International journal of pharmaceutics 2020, 581, 119293. [Google Scholar] [CrossRef]
- Pleguezuelos-Villa, M.; Nácher, A.; Hernández, M.J.; Busó, M.; Barrachina, M.; Peñalver, N.; Díez-Sales, O. A novel lidocaine hydrochloride mucoadhesive films for periodontal diseases. Journal of Materials Science: Materials in Medicine 2019, 30, 1–7. [Google Scholar] [CrossRef]
- Clitherow, K.H.; Murdoch, C.; Spain, S.G.; Handler, A.M.; Colley, H.E.; Stie, M.B.; Mørck Nielsen, H.; Janfelt, C.; Hatton, P.V.; Jacobsen, J. Mucoadhesive electrospun patch delivery of lidocaine to the oral mucosa and investigation of spatial distribution in a tissue using MALDI-mass spectrometry imaging. Molecular pharmaceutics 2019, 16, 3948–3956. [Google Scholar] [CrossRef]
- Jelvehgari, M.; Rashidi, M.R.; Samadi, H. Mucoadhesive and drug release properties of benzocaine gel. 2006.
- Jose, J.; Sisira, M.; Prasanth, M.L.; Prasanth, C.S.; Pradeep, P. Design and Characterization of Buccal Films of Benzocaine for Mouth Ulcer. Polymer 2021, 10, 250. [Google Scholar] [CrossRef]
- Kulkarni, A.P.; Khan, S.K.A.; Dehghan, M.H. Evaluation of polaxomer-based in situ gelling system of articaine as a drug delivery system for anesthetizing periodontal pockets–an in vitro study. Indian Journal of Dentistry 2012, 3, 201–208. [Google Scholar] [CrossRef]
- Hanif, S.; Sarfraz, R.M.; Syed, M.A.; Mahmood, A.; Hussain, Z. Smart mucoadhesive buccal chitosan/HPMC scaffold for sore throat: In vitro, ex vivo and pharmacokinetic profiling in humans. Journal of Drug Delivery Science and Technology 2022, 71, 103271. [Google Scholar] [CrossRef]
- Javed, Q.u.A.; Syed, M.A.; Arshad, R.; Rahdar, A.; Irfan, M.; Raza, S.A.; Shahnaz, G.; Hanif, S.; Díez-Pascual, A.M. Evaluation and Optimization of Prolonged Release Mucoadhesive Tablets of Dexamethasone for Wound Healing: In Vitro–In Vivo Profiling in Healthy Volunteers. Pharmaceutics 2022, 14, 807. [Google Scholar] [CrossRef] [PubMed]
- Davoudi, Z.; Rabiee, M.; Houshmand, B.; Eslahi, N.; Khoshroo, K.; Rasoulianboroujeni, M.; Tahriri, M.; Tayebi, L. Development of chitosan/gelatin/keratin composite containing hydrocortisone sodium succinate as a buccal mucoadhesive patch to treat desquamative gingivitis. Drug development and industrial pharmacy 2018, 44, 40–55. [Google Scholar] [CrossRef]
- Kumria, R.; Nair, A.B.; Goomber, G.; Gupta, S. Buccal films of prednisolone with enhanced bioavailability. Drug delivery 2016, 23, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Colley, H.; Said, Z.; Santocildes-Romero, M.; Baker, S.; D'Apice, K.; Hansen, J.; Madsen, L.S.; Thornhill, M.; Hatton, P.; Murdoch, C. Pre-clinical evaluation of novel mucoadhesive bilayer patches for local delivery of clobetasol-17-propionate to the oral mucosa. Biomaterials 2018, 178, 134–146. [Google Scholar] [CrossRef] [PubMed]
- Al-Ani, E.; Hill, D.; Doudin, K. Chlorhexidine Mucoadhesive Buccal Tablets: The Impact of Formulation Design on Drug Delivery and Release Kinetics Using Conventional and Novel Dissolution Methods. Pharmaceuticals 2021, 14, 493. [Google Scholar] [CrossRef]
- Ebrahimi, N.; Vohra, S.; Gedeon, C.; Akoury, H.; Bernstein, P.; Pairaudeau, N.; Cormier, J.; Dontigny, L.; Arsenault, M.-Y.; Fortin, C. The fetal safety of hydrocortisone-pramoxine (Proctofoam-HC) for the treatment of hemorrhoids in late pregnancy. Journal of Obstetrics and Gynaecology Canada 2011, 33, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Mizrahi, B.; Domb, A.J. Mucoadhesive polymers for delivery of drugs to the oral cavity. Recent patents on drug delivery & formulation 2008, 2, 108–119. [Google Scholar]
- Ghafar, H.; Khan, M.I.; Sarwar, H.S.; Yaqoob, S.; Hussain, S.Z.; Tariq, I.; Madni, A.U.; Shahnaz, G.; Sohail, M.F. Development and characterization of bioadhesive film embedded with lignocaine and calcium fluoride nanoparticles. Aaps Pharmscitech 2020, 21, 1–12. [Google Scholar] [CrossRef]
- Tsibouklis, J.; Middleton, A.M.; Patel, N.; Pratten, J. Toward mucoadhesive hydrogel formulations for the management of xerostomia: The physicochemical, biological, and pharmacological considerations. Journal of Biomedical Materials Research Part A 2013, 101, 3327–3338. [Google Scholar] [CrossRef]
- Zhang, C.; Liu, Y.; Li, W.; Gao, P.; Xiang, D.; Ren, X.; Liu, D. Mucoadhesive buccal film containing ornidazole and dexamethasone for oral ulcers: in vitro and in vivo studies. Pharmaceutical development and technology 2019, 24, 118–126. [Google Scholar] [CrossRef]
- Tejada, G.; Piccirilli, G.; Sortino, M.; Salomón, C.; Lamas, M.; Leonardi, D. Formulation and in-vitro efficacy of antifungal mucoadhesive polymeric matrices for the delivery of miconazole nitrate. Materials Science and Engineering: C 2017, 79, 140–150. [Google Scholar] [CrossRef]
- Hassan, M.; Barakat, N.; El-Badry, M.; Shehata, S. Formulation and in vitro/in vivo evaluation of naproxen mucoadhesive buccal patches for local effect. Journal of drug delivery science and technology 2011, 21, 423. [Google Scholar] [CrossRef]
- Rencber, S.; Karavana, S.Y.; Yılmaz, F.F.; Eraç, B.; Nenni, M.; Özbal, S.; Pekcetin, C.; Gurer-Orhan, H.; Hoşgör-Limoncu, M.; Güneri, P. Development, characterization, and in vivo assessment of mucoadhesive nanoparticles containing fluconazole for the local treatment of oral candidiasis. International journal of nanomedicine 2016, 11, 2641. [Google Scholar] [CrossRef] [PubMed]
- Pandey, M.; Choudhury, H.; Ying, J.N.S.; Ling, J.F.S.; Ting, J.; Ting, J.S.S.; Zhia Hwen, I.K.; Suen, H.W.; Samsul Kamar, H.S.; Gorain, B. Mucoadhesive nanocarriers as a promising strategy to enhance intracellular delivery against oral cavity carcinoma. Pharmaceutics 2022, 14, 795. [Google Scholar] [CrossRef] [PubMed]
- Ghafar, H.; Khan, M.I.; Sarwar, H.S.; Yaqoob, S.; Hussain, S.Z.; Tariq, I.; Madni, A.U.; Shahnaz, G.; Sohail, M.F. Development and characterization of bioadhesive film embedded with lignocaine and calcium fluoride nanoparticles. Aaps Pharmscitech 2020, 21, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Elkanayati, R.M.; Chambliss, W.G.; Omari, S.; Almutairi, M.; Repka, M.A.; Ashour, E.A. Mucoadhesive buccal films for treatment of xerostomia prepared by coupling HME and 3D printing technologies. Journal of Drug Delivery Science and Technology 2022, 75, 103660. [Google Scholar] [CrossRef]
- Abha, D.; Sheeja, K.; Bhagyashri, J. Design and evaluation of buccal film of diclofenac sodium. Int J pharm Bio sci 2011, 1, 17–30. [Google Scholar]
- Hearnden, V.; Sankar, V.; Hull, K.; Juras, D.V.; Greenberg, M.; Kerr, A.R.; Lockhart, P.B.; Patton, L.L.; Porter, S.; Thornhill, M.H. New developments and opportunities in oral mucosal drug delivery for local and systemic disease. Advanced drug delivery reviews 2012, 64, 16–28. [Google Scholar] [CrossRef]
- Jelvehgari, M.; Rashidi, M.R.; Samadi, H. Mucoadhesive and drug release properties of benzocaine gel. Iranian journal of pharmaceutical sciences 2006, 2, 185–194. [Google Scholar]
- Yehia, S.A.; El-Gazayerly, O.N.; Basalious, E.B. Fluconazole mucoadhesive buccal films: in vitro/in vivo performance. Current drug delivery 2009, 6, 17–27. [Google Scholar] [CrossRef]
- Van Roey, J.; Haxaire, M.; Kamya, M.; Lwanga, I.; Katabira, E. Comparative efficacy of topical therapy with a slow-release mucoadhesive buccal tablet containing miconazole nitrate versus systemic therapy with ketoconazole in HIV-positive patients with oropharyngeal candidiasis. JAIDS Journal of Acquired Immune Deficiency Syndromes 2004, 35, 144–150. [Google Scholar] [CrossRef]
- Razzaq, S.; Hanif, S.; Syed, M.A.; Iqbal, J.; Raza, S.A.; Riaz, H.; Abid, F. Development and evaluation of mucoadhesive buccal tablet containing metronidazole for the treatment of periodontitis and gingivitis. Pakistan Journal of Pharmaceutical Sciences 2018, 31. [Google Scholar]
- Ahn, J.-S.; Choi, H.-K.; Chun, M.-K.; Ryu, J.-M.; Jung, J.-H.; Kim, Y.-U.; Cho, C.-S. Release of triamcinolone acetonide from mucoadhesive polymer composed of chitosan and poly (acrylic acid) in vitro. Biomaterials 2002, 23, 1411–1416. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi-Samani, S.; Bahri-Najafi, R.; Yousefi, G. Formulation and in vitro evaluation of prednisolone buccoadhesive tablets. Il Farmaco 2005, 60, 339–344. [Google Scholar] [CrossRef]
- Bender, L.; Boostrom, H.M.; Varricchio, C.; Zuanon, M.; Celiksoy, V.; Sloan, A.; Cowpe, J.; Heard, C.M. A novel dual action monolithic thermosetting hydrogel loaded with lidocaine and metronidazole as a potential treatment for alveolar osteitis. European Journal of Pharmaceutics and Biopharmaceutics 2020, 149, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Azadi Boroujeni, A.; Talebi Ardakani, M.; Houshmand, B.; Moscowchi, A. Designing a novel chitosan-based periofilm containing metronidazole–ciprofloxacin. SN Applied Sciences 2020, 2, 1–8. [Google Scholar]
- Syed, M.A.; Aziz, G.; Jehangir, M.B.; Tabish, T.A.; Zahoor, A.F.; Khalid, S.H.; Khan, I.U.; Hosny, K.M.; Rizg, W.Y.; Hanif, S. Evaluating Novel Agarose-Based Buccal Gels Scaffold: Mucoadhesive and Pharmacokinetic Profiling in Healthy Volunteers. Pharmaceutics 2022, 14, 1592. [Google Scholar] [CrossRef] [PubMed]
- Macedo, A.S.; Castro, P.M.; Roque, L.; Thomé, N.G.; Reis, C.P.; Pintado, M.E.; Fonte, P. Novel and revisited approaches in nanoparticle systems for buccal drug delivery. Journal of Controlled Release 2020, 320, 125–141. [Google Scholar] [CrossRef]
- Kamimura, M.; Furukawa, T.; Akiyama, S.-i.; Nagasaki, Y. Enhanced intracellular drug delivery of pH-sensitive doxorubicin/poly (ethylene glycol)-block-poly (4-vinylbenzylphosphonate) nanoparticles in multi-drug resistant human epidermoid KB carcinoma cells. Biomaterials science 2013, 1, 361–367. [Google Scholar] [CrossRef]
- Du, F.; Meng, H.; Xu, K.; Xu, Y.; Luo, P.; Luo, Y.; Lu, W.; Huang, J.; Liu, S.; Yu, J. CPT loaded nanoparticles based on beta-cyclodextrin-grafted poly (ethylene glycol)/poly (L-glutamic acid) diblock copolymer and their inclusion complexes with CPT. Colloids and Surfaces B: Biointerfaces 2014, 113, 230–236. [Google Scholar] [CrossRef]
- NR, R.; Tiyaboonchai, W.; Madhusudhan, B. Fabrication and characterization of genistein encapsulated poly (D, L) lactic acid nanoparticles for pharmaceutical application. Current Nanoscience 2013, 9, 293–302. [Google Scholar]
- Panyam, J.; Zhou, W.Z.; Prabha, S.; Sahoo, S.K.; Labhasetwar, V. Rapid endo-lysosomal escape of poly (DL-lactide-coglycolide) nanoparticles: implications for drug and gene delivery. The FASEB journal 2002, 16, 1217–1226. [Google Scholar] [CrossRef]
- Ren, F.; Chen, R.; Wang, Y.; Sun, Y.; Jiang, Y.; Li, G. Paclitaxel-loaded poly (n-butylcyanoacrylate) nanoparticle delivery system to overcome multidrug resistance in ovarian cancer. Pharmaceutical research 2011, 28, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Gharat, S.A.; Momin, M.M.; Bhavsar, C. Oral squamous cell carcinoma: current treatment strategies and nanotechnology-based approaches for prevention and therapy. Critical Reviews™ in Therapeutic Drug Carrier Systems 2016, 33. [Google Scholar] [CrossRef] [PubMed]
- Danhier, F.; Vroman, B.; Lecouturier, N.; Crokart, N.; Pourcelle, V.; Freichels, H.; Jérôme, C.; Marchand-Brynaert, J.; Feron, O.; Préat, V. Targeting of tumor endothelium by RGD-grafted PLGA-nanoparticles loaded with paclitaxel. Journal of Controlled Release 2009, 140, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Strandman, S.; Zhu, J.X.; Barralet, J.; Cerruti, M. Genipin-crosslinked catechol-chitosan mucoadhesive hydrogels for buccal drug delivery. Biomaterials 2015, 37, 395–404. [Google Scholar] [CrossRef]
- Li, L.D.; Crouzier, T.; Sarkar, A.; Dunphy, L.; Han, J.; Ribbeck, K. Spatial configuration and composition of charge modulates transport into a mucin hydrogel barrier. Biophysical journal 2013, 105, 1357–1365. [Google Scholar] [CrossRef]
- Krampe, R.; Visser, J.C.; Frijlink, H.W.; Breitkreutz, J.; Woerdenbag, H.J.; Preis, M. Oromucosal film preparations: points to consider for patient centricity and manufacturing processes. Expert opinion on drug delivery 2016, 13, 493–506. [Google Scholar] [CrossRef]
- Syed, M.A.; Hanif, S.; Ain, N.u.; Syed, H.K.; Zahoor, A.F.; Khan, I.U.; Abualsunun, W.A.; Jali, A.M.; Qahl, S.H.; Sultan, M.H. Assessment of Binary Agarose–Carbopol Buccal Gels for Mucoadhesive Drug Delivery: Ex Vivo and In Vivo Characterization. Molecules 2022, 27, 7004. [Google Scholar] [CrossRef]
- Sadeghian, R.; Rohani, B.; Golestannejad, Z.; Sadeghian, S.; Mirzaee, S. Comparison of therapeutic effect of mucoadhesive nano-triamcinolone gel and conventional triamcinolone gel on oral lichen planus. Dental research journal 2019, 16, 277. [Google Scholar]
- Begum, M.Y.; Alqahtani, A.; Ghazwani, M.; Ramakrishna, M.; Hani, U.; Atiya, A.; Rahamathulla, M. Preparation of Carbopol 934 based ketorolac tromethamine buccal mucoadhesive film: in vitro, ex vivo, and in vivo assessments. International Journal of Polymer Science 2021, 2021. [Google Scholar] [CrossRef]
- Reid, G. Probiotics: definition, scope and mechanisms of action. Best practice & research Clinical gastroenterology 2016, 30, 17–25. [Google Scholar]
- Meurman, J.H. Probiotics: do they have a role in oral medicine and dentistry? European journal of oral sciences 2005, 113, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Erickson, K.L.; Hubbard, N.E. Probiotic immunomodulation in health and disease. The Journal of nutrition 2000, 130, 403S–409S. [Google Scholar] [CrossRef] [PubMed]
- Marco, M.L.; Pavan, S.; Kleerebezem, M. Towards understanding molecular modes of probiotic action. Current opinion in biotechnology 2006, 17, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Sharma, J.; Al-Omran, A.; Parvathy, S. Role of nitric oxide in inflammatory diseases. Inflammopharmacology 2007, 15, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Abruzzo, A.; Vitali, B.; Lombardi, F.; Guerrini, L.; Cinque, B.; Parolin, C.; Bigucci, F.; Cerchiara, T.; Arbizzani, C.; Gallucci, M.C. Mucoadhesive buccal films for local delivery of lactobacillus brevis. Pharmaceutics 2020, 12, 241. [Google Scholar] [CrossRef]
- Palo, M.; Rönkönharju, S.; Tiirik, K.; Viidik, L.; Sandler, N.; Kogermann, K. Bi-layered polymer carriers with surface modification by electrospinning for potential wound care applications. Pharmaceutics 2019, 11, 678. [Google Scholar] [CrossRef] [PubMed]
- Shirvan, A.R.; Bashari, A.; Hemmatinejad, N. New insight into the fabrication of smart mucoadhesive buccal patches as a novel controlled-drug delivery system. European Polymer Journal 2019, 119, 541–550. [Google Scholar] [CrossRef]
- Cid, Y.P.; Pedrazzi, V.; de Sousa, V.P.; Pierre, M.B.R. In vitro characterization of chitosan gels for buccal delivery of celecoxib: influence of a penetration enhancer. AAPS PharmSciTech 2012, 13, 101–111. [Google Scholar] [CrossRef]
- Samprasit, W.; Kaomongkolgit, R.; Sukma, M.; Rojanarata, T.; Ngawhirunpat, T.; Opanasopit, P. Mucoadhesive electrospun chitosan-based nanofibre mats for dental caries prevention. Carbohydrate polymers 2015, 117, 933–940. [Google Scholar] [CrossRef]
- Voronova, A.; Prieto, C.; Pardo-Figuerez, M.; Lagaron, J.M.; Sanyal, A.; Demir, B.; Hubert, T.; Plaisance, V.; Pawlowski, V.; Vignoud-Despond, S. Photothermal Activatable Mucoadhesive Fiber Mats for On-Demand Delivery of Insulin via Buccal and Corneal Mucosa. ACS Applied Bio Materials 2022, 5, 771–778. [Google Scholar] [CrossRef]
- Samprasit, W.; Rojanarata, T.; Akkaramongkolporn, P.; Ngawhirunpat, T.; Kaomongkolgit, R.; Opanasopit, P. Fabrication and in vitro/in vivo performance of mucoadhesive electrospun nanofiber mats containing α-mangostin. Aaps Pharmscitech 2015, 16, 1140–1152. [Google Scholar] [CrossRef] [PubMed]
- Balogh, A.; Drávavölgyi, G.; Faragó, K.; Farkas, A.; Vigh, T.; Sóti, P.L.; Wagner, I.; Madarász, J.; Pataki, H.; Marosi, G. Plasticized drug-loaded melt electrospun polymer mats: characterization, thermal degradation, and release kinetics. Journal of pharmaceutical sciences 2014, 103, 1278–1287. [Google Scholar] [CrossRef]
- Garg, K.; Tirgar, P. Assessment of Effect of Intra-pocket Delivery of Metronidazole Loaded NTrimethyl Quaternary Ammonium Chitosan Nanoparticles in Treatment of Periodontal Disease. Current Drug Therapy 2023, 18, 49–67. [Google Scholar] [CrossRef]
- Hanif, S.; Sarfraz, R.M.; Syed, M.A.; Mahmood, A.; Minhas, M.U.; Irfan, M. Development and optimization of tibezonium iodide and lignocaine hydrochloride containing novel mucoadhesive buccal tablets: A pharmacokinetic investigation among healthy humans. Drug Development and Industrial Pharmacy 2021, 47, 1209–1222. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Frontal view of the buccal cavity.
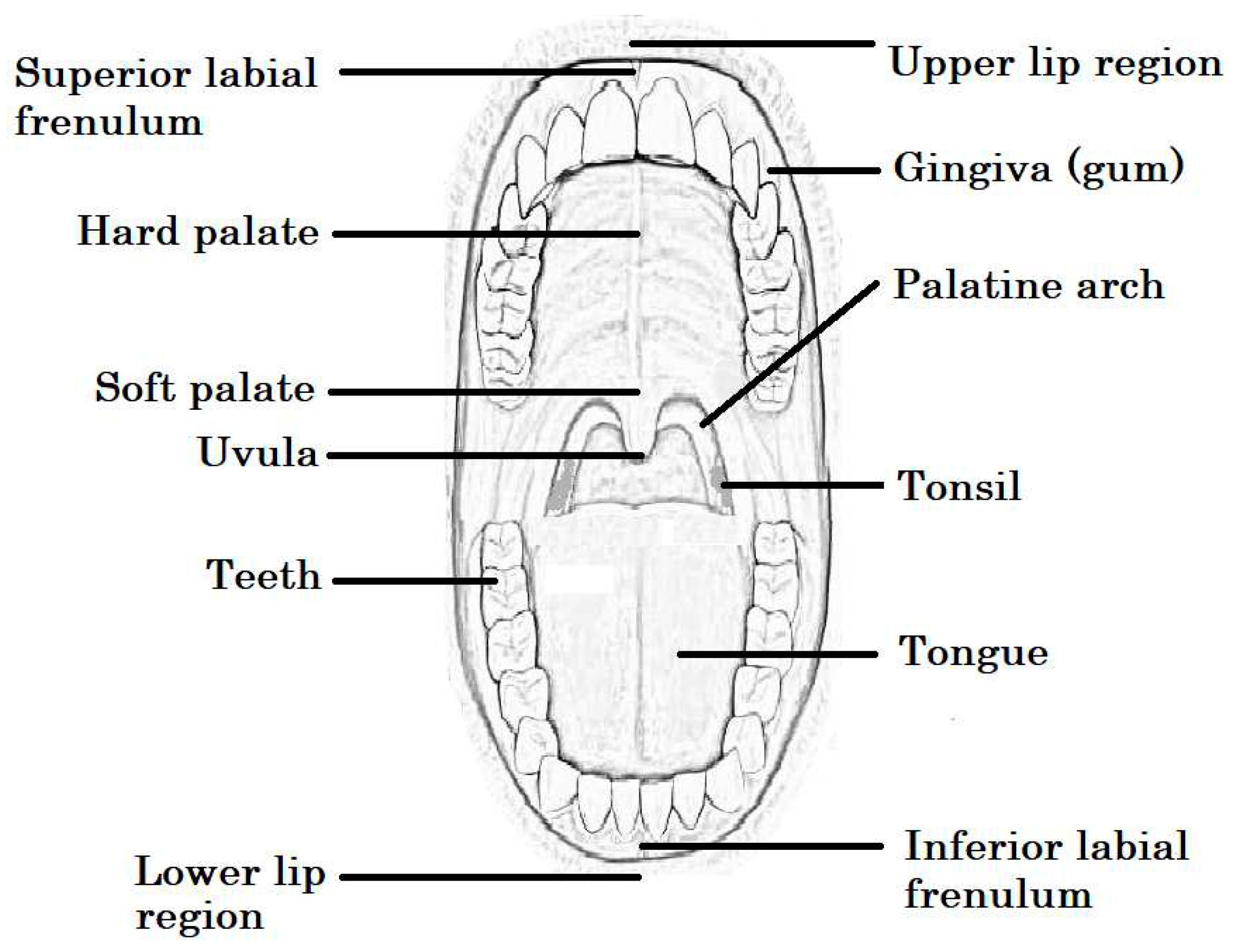
Figure 2.
Diagram depicting the presence of squamous cell carcinoma, where ‘A’ represents a low magnification view of the buccal epithelium, while ‘B’ represents aggregates of cells undergoing mitosis when viewed at high magnification. Image taken with permission from [28].
Figure 2.
Diagram depicting the presence of squamous cell carcinoma, where ‘A’ represents a low magnification view of the buccal epithelium, while ‘B’ represents aggregates of cells undergoing mitosis when viewed at high magnification. Image taken with permission from [28].
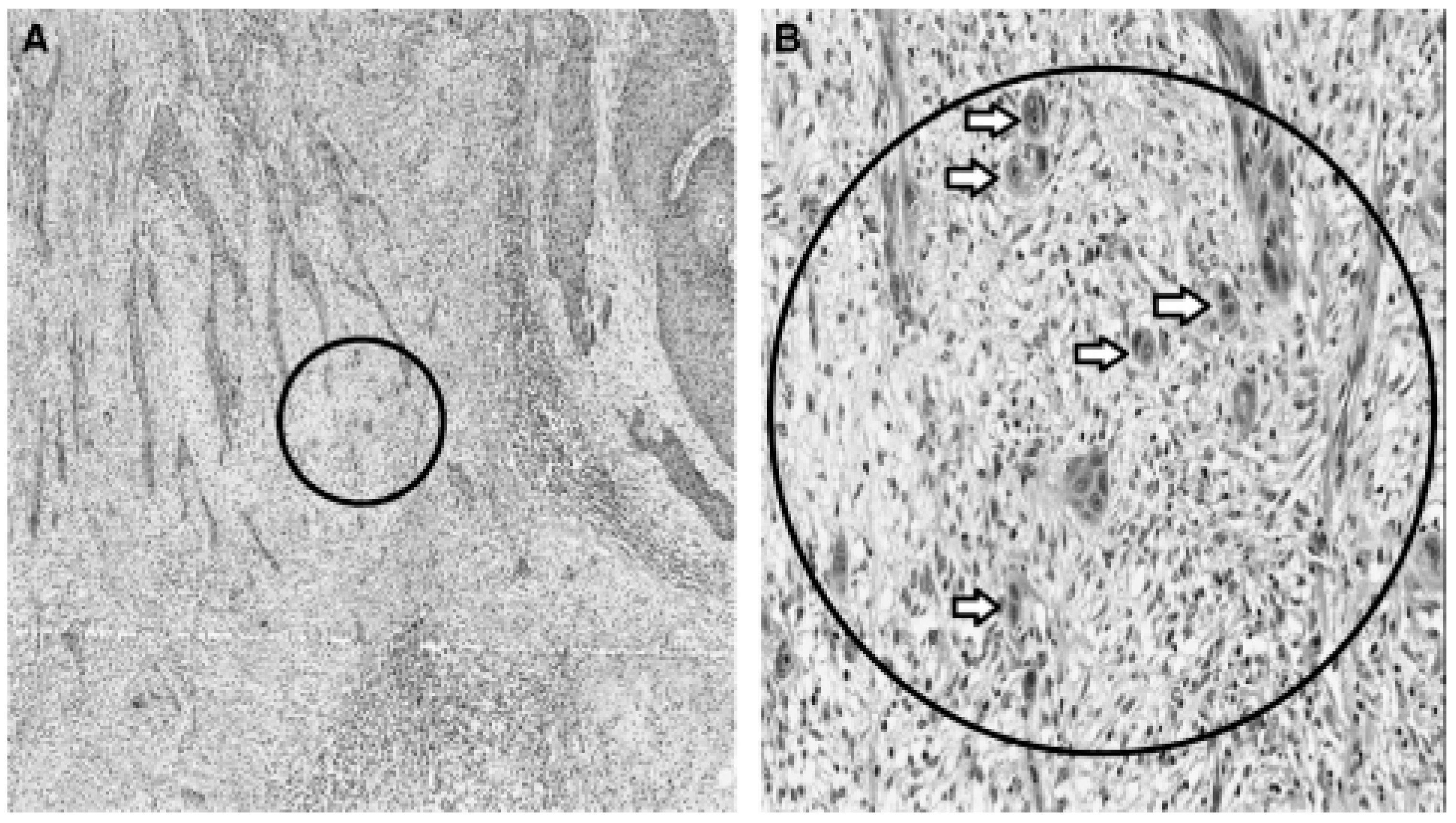
Figure 4.
Improved uptake of peptidomimetic RGD nanoparticles (RGD-NP) compared with undecorated nanoparticles (NP) (image taken with permission from [98]).
Figure 4.
Improved uptake of peptidomimetic RGD nanoparticles (RGD-NP) compared with undecorated nanoparticles (NP) (image taken with permission from [98]).
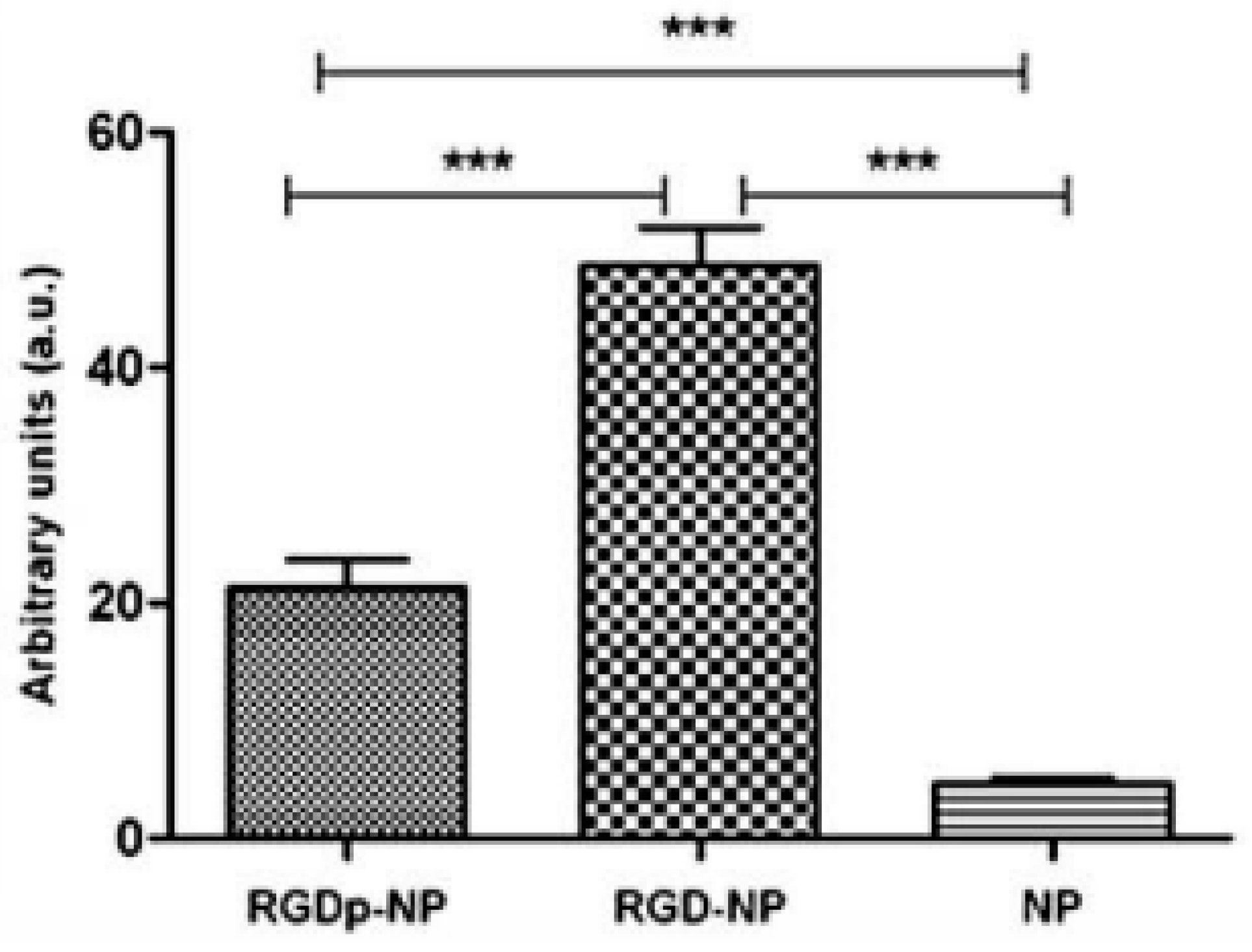
Figure 5.
Apoptosis of human SCC9 cells detected using acridine orange and ethidium bromide and treated with controls or chitosan-coated curcumin nanoparticles. Figure reproduced with permission from [2].
Figure 5.
Apoptosis of human SCC9 cells detected using acridine orange and ethidium bromide and treated with controls or chitosan-coated curcumin nanoparticles. Figure reproduced with permission from [2].
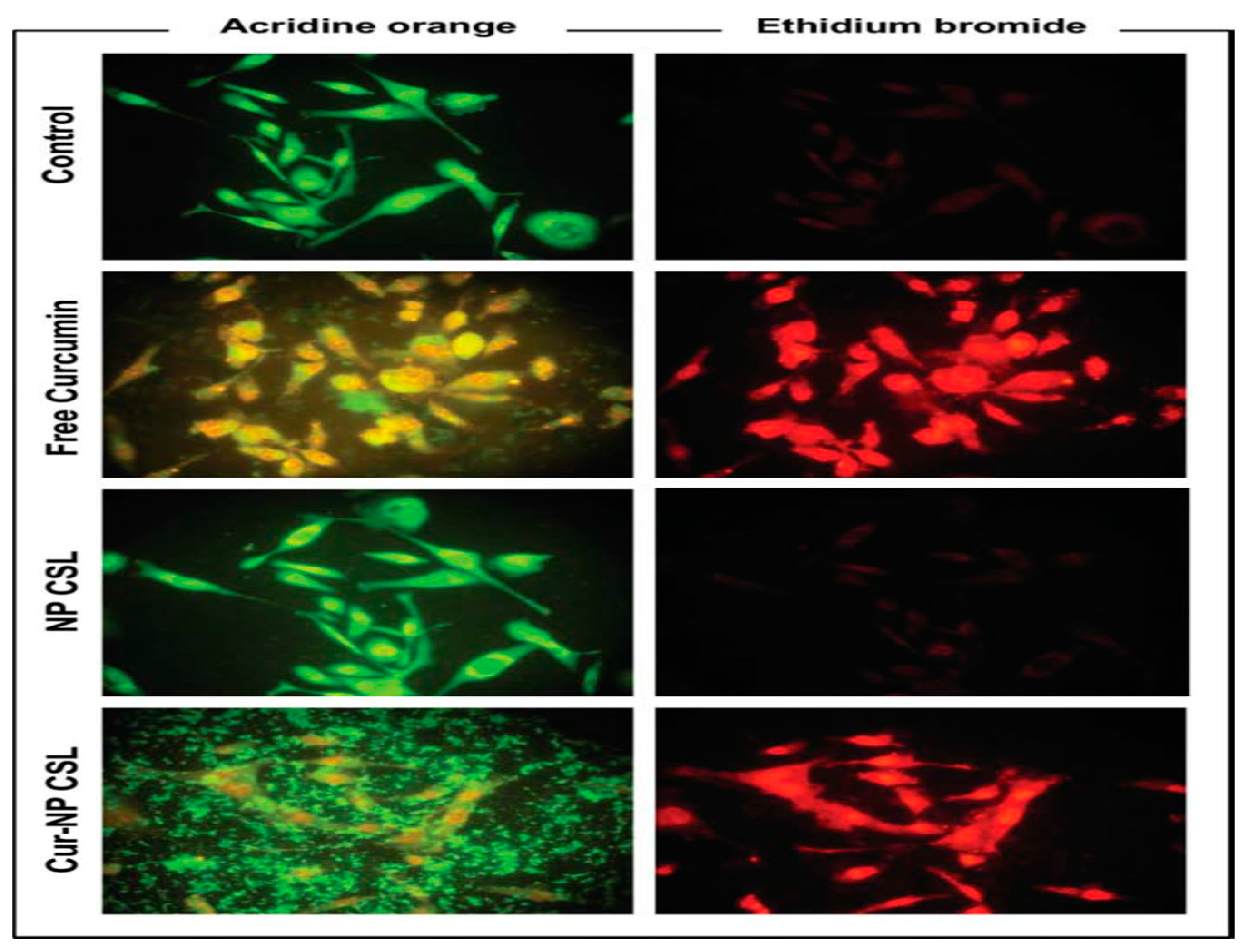
Figure 7.
Synthesis of agarose-based gels (image taken with permission from [102]).
Figure 7.
Synthesis of agarose-based gels (image taken with permission from [102]).
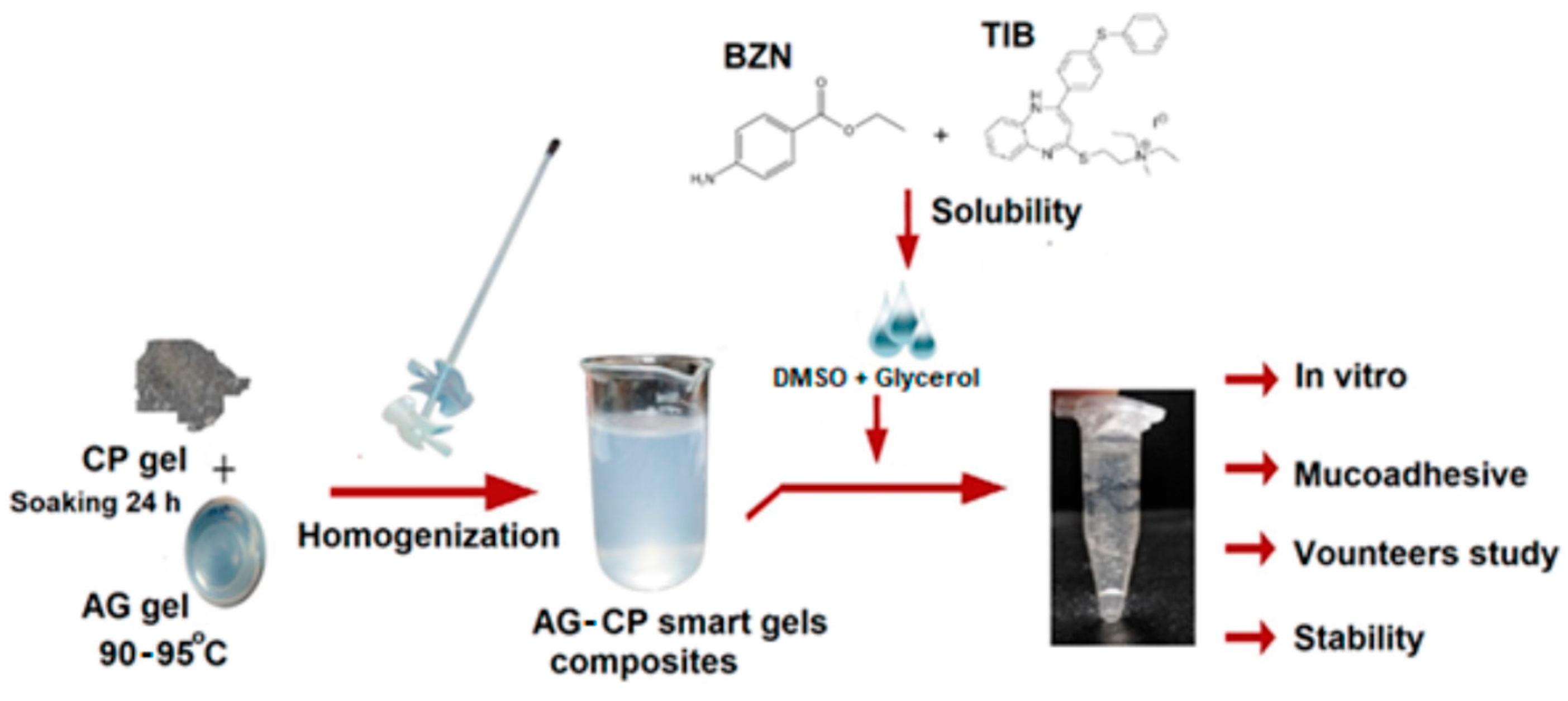
Figure 8.
Salivary concentrations of tibezonium iodide (TIB) and benzocaine (BZN) over time for the treatment of sore throat (diagram taken with permission from [90]).
Figure 8.
Salivary concentrations of tibezonium iodide (TIB) and benzocaine (BZN) over time for the treatment of sore throat (diagram taken with permission from [90]).
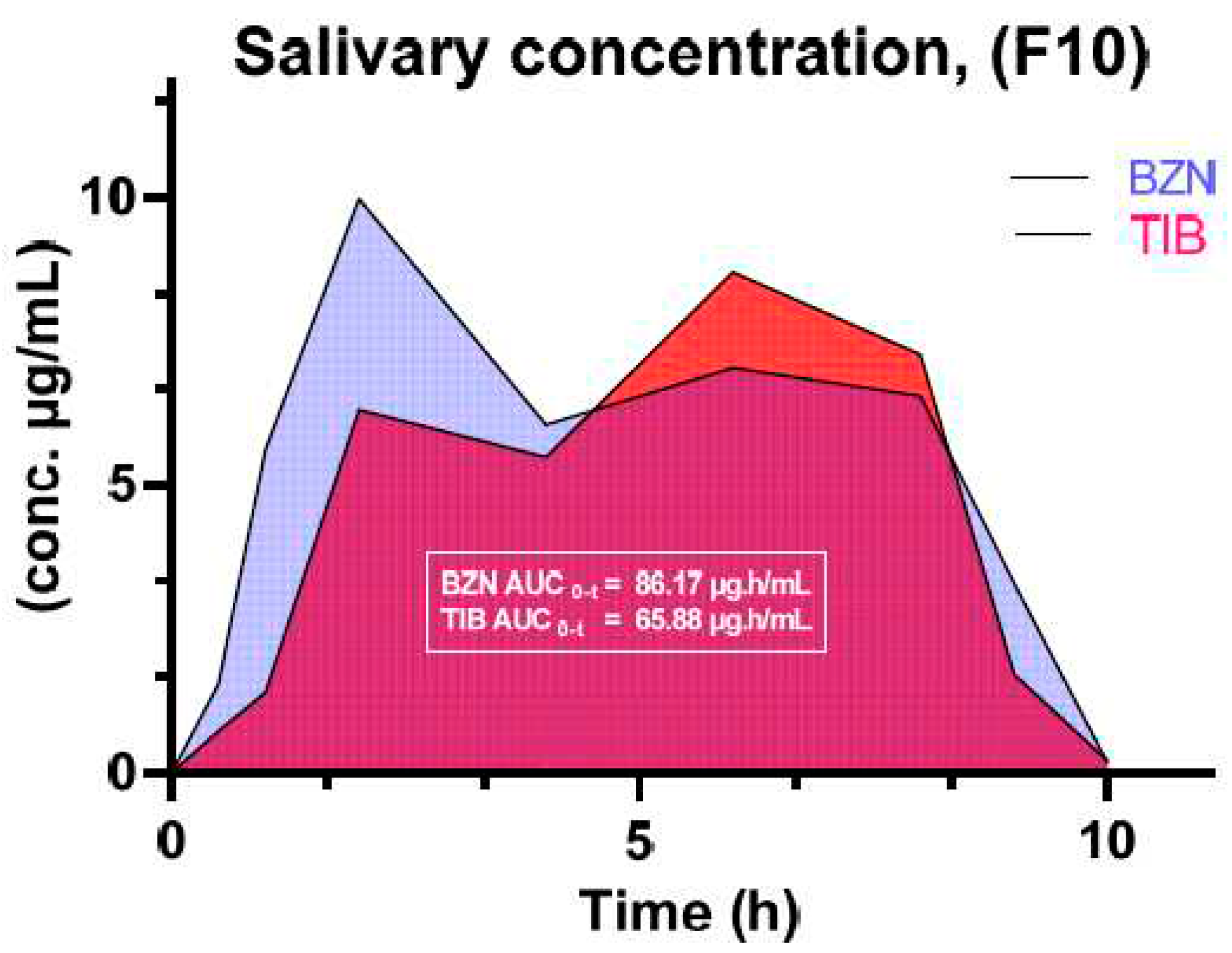
Figure 9.
Stereoscopic images of a. HPMC-based film; b. backing layer containing ethylcellulose; c. HPMC with backing layer; d. SEM image of HPMC layer; e. the drug-loaded HPMC layer; and e. HPMC-loaded drug layer plus Men (courtesy of [54]).
Figure 9.
Stereoscopic images of a. HPMC-based film; b. backing layer containing ethylcellulose; c. HPMC with backing layer; d. SEM image of HPMC layer; e. the drug-loaded HPMC layer; and e. HPMC-loaded drug layer plus Men (courtesy of [54]).
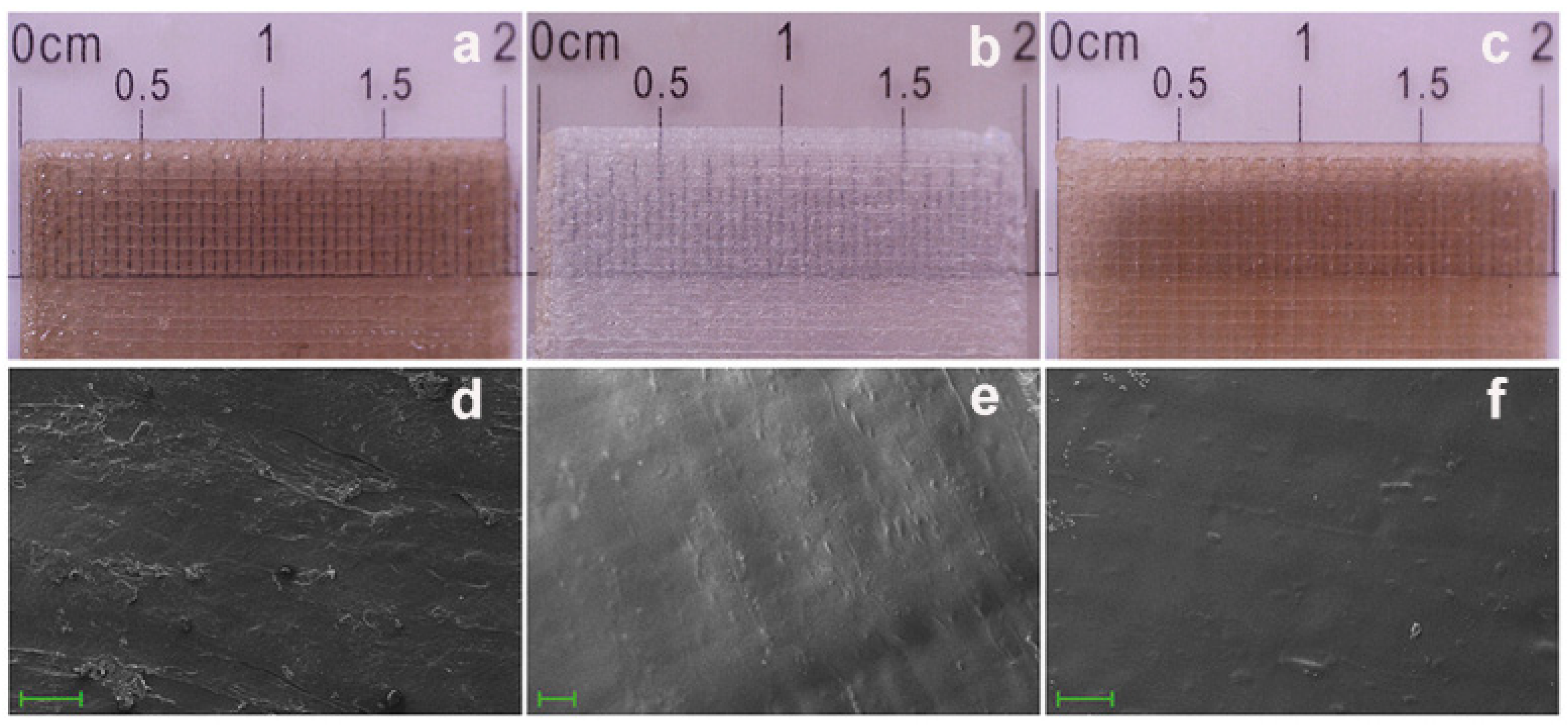
Figure 10.
Application of formulated clobetasol patches to volunteers (from [67]).
Figure 10.
Application of formulated clobetasol patches to volunteers (from [67]).
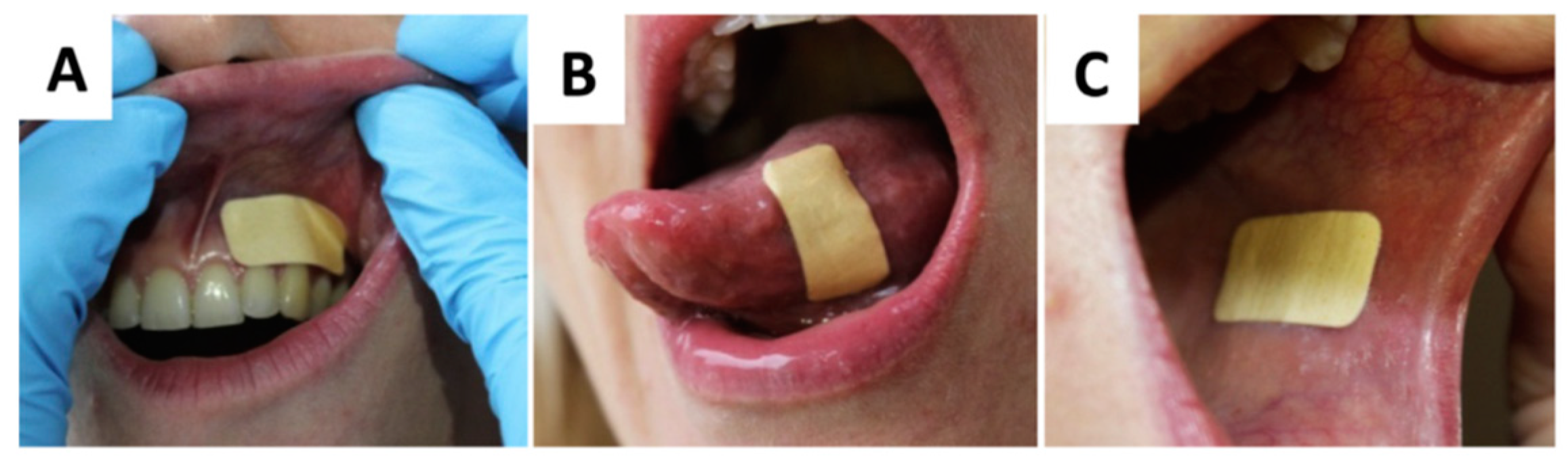
Figure 11.
Responses to patches applied to the oral cavities of volunteers (from [67]).
Figure 11.
Responses to patches applied to the oral cavities of volunteers (from [67]).
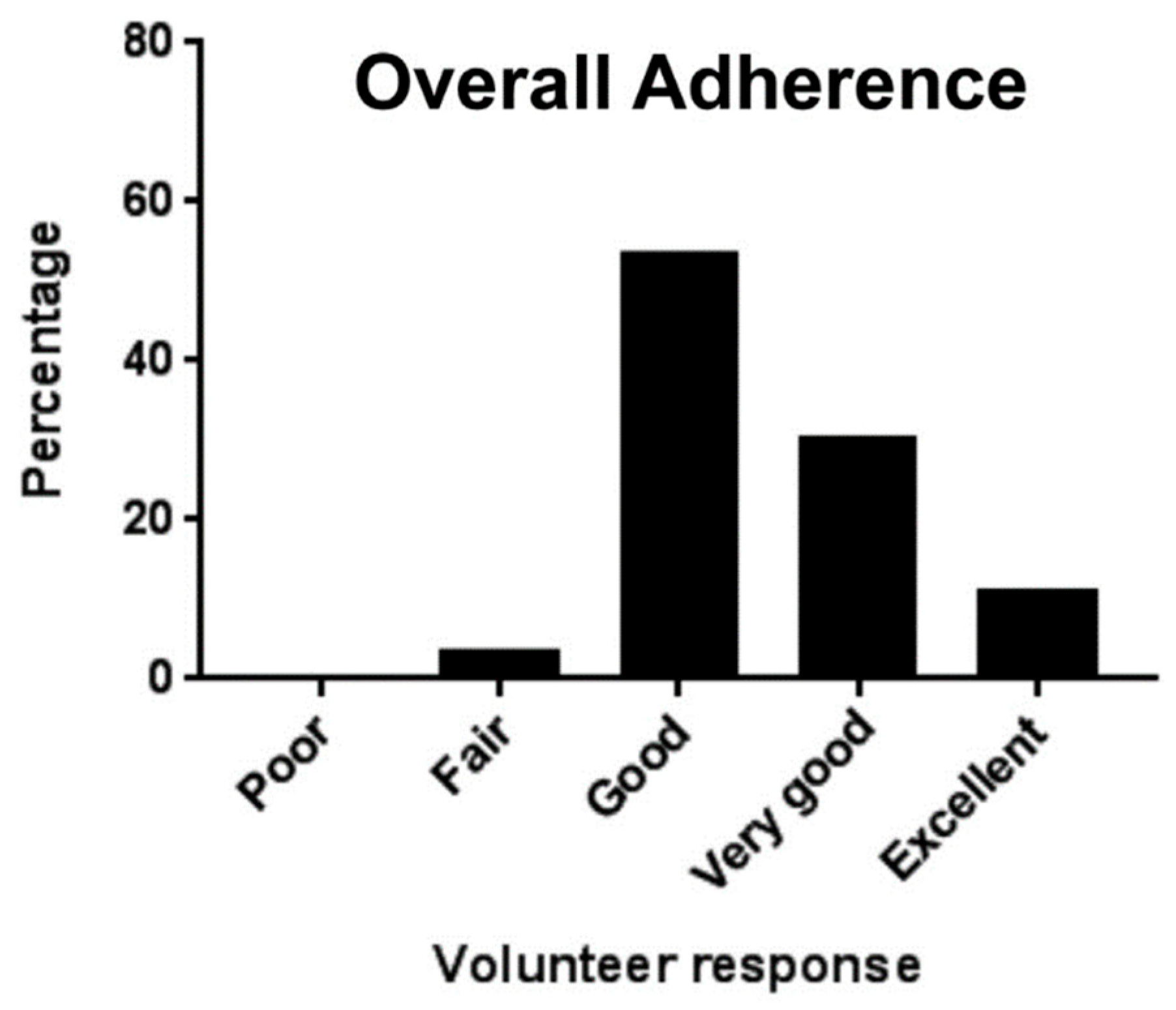
Figure 12.
Frequency of irritation to volunteers (image obtained with permission from [67]).
Figure 12.
Frequency of irritation to volunteers (image obtained with permission from [67]).
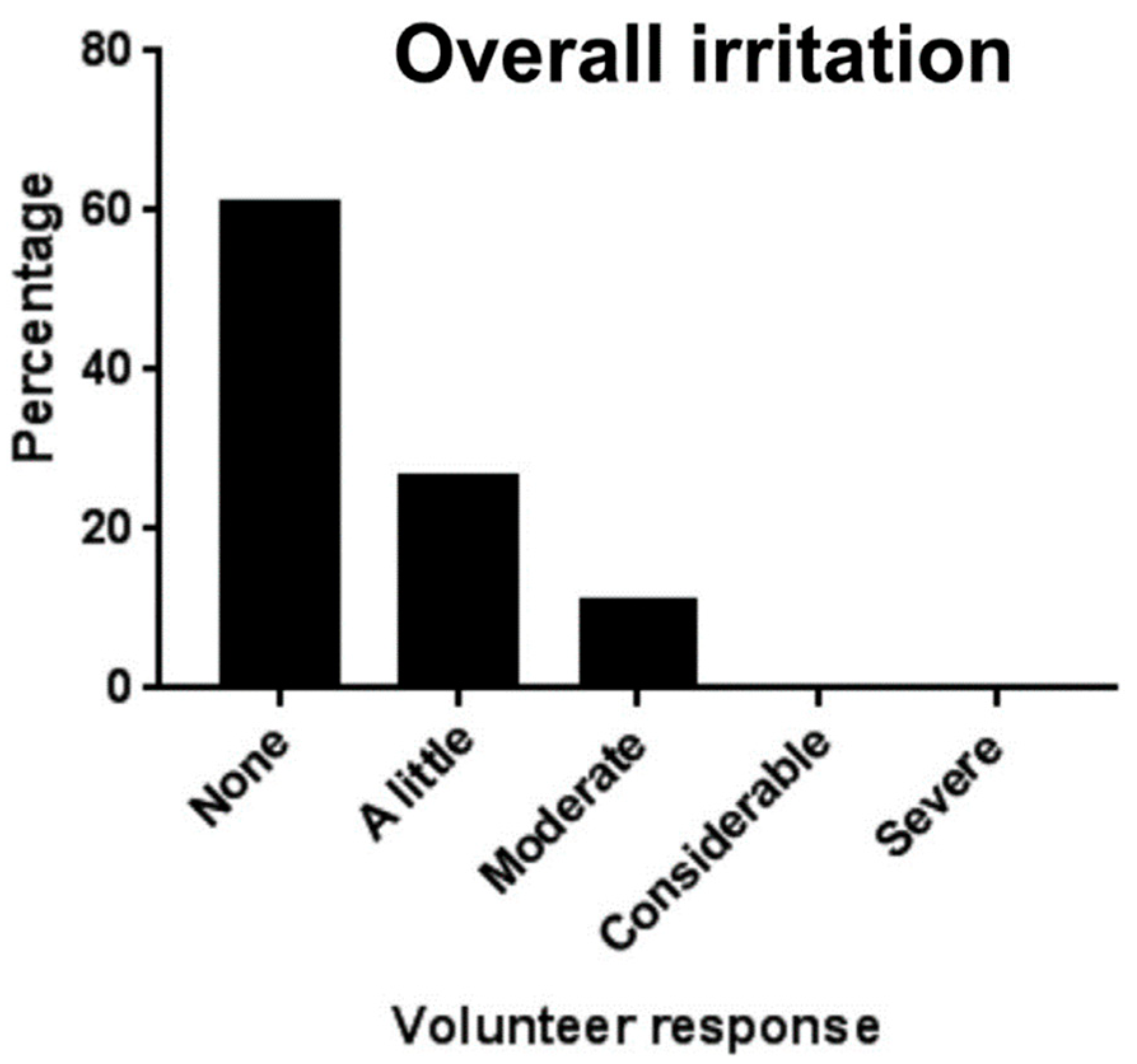
Table 1.
Causative anaerobic bacteria in periodontal diseases.
| Anaerobic Gram-negative bacteria | Anaerobic Gram-positive bacteria |
|---|---|
| Actinobacillus actinomycetemcomitans | Actinomyces viscosus |
| Porphyromonas gingivalis | Peptostreptococcus micros |
| Prevotella intermedia | |
| Tannerella forsythensis |
Table 2.
Classification of periodontal infections according to the AAP (adapted from [45]).
Table 2.
Classification of periodontal infections according to the AAP (adapted from [45]).
| Gingivitis | Periodontitis |
|---|---|
| Dental plaque-induced gingival disease | Chronic periodontitis (CP) |
| Acute necrotizing ulcerative gingivitis (ANUG) | Aggressive periodontitis (AP) |
| Steroid hormone-induced gingival enlargement | Periodontitis as a manifestation of systemic diseases |
| Drug-induced gingival enlargement | Necrotizing periodontal diseases |
| Gingivitis associated with blood disorders, nutritional deficits, tumors, genetic factors, viral infection | Periodontal abscesses |
| Desquamative gingivitis | Periodontitis with endodontic lesions |
| Gingivitis associated with malnutrition | Developmental and acquired deformation and conditions |
| Non-plaque induced gingival disease | |
| Gingival disease of bacterial, viral, fungal origin | |
| Gingival lesions of genetic origin | |
| Gingival manifestation of systemic conditions | |
| Traumatic lesions |
Table 3.
An overview of some common buccal disorders and available therapeutics.
| Disease | Local therapy | Reference(s) |
|---|---|---|
| Oral sores | Antimicrobial, antifungal, antiseptic, adjunct therapy, anti-inflammatory drugs | [73,74] |
| Swelling | Non-steroidal and steroidal anti-inflammatory drugs | [64,75] |
| Microbial infection | Antimicrobial, antifungal, antiseptic | [68,74,76] |
| Pain | Local anesthetic agent | [52] |
| Tumor | Anti-cancer drugs | [77] |
| Dietary calcium supplement | Calcium supplements | [78] |
| Xerostomia | Secretagogues | [72,79] |
Table 4.
List of some commonly delivered drugs for treating local pathologies.
| Monotherapy | Dual therapy |
|---|---|
| Diclofenac [80] Lignocaine [78] Minocycline [81] Dexamethasone [73] Benzocaine [82] Chlorhexidine [62] Articaine [62] Fluconazole [83] Ketoconazole [84] Metronidazole [85] Triamcinolone acetonide [86] Prednisolone [87] Calcium supplement [78] |
Metronidazole and lignocaine [88] Ciprofloxacin and metronidazole [89] Flurbiprofen and lignocaine [52] Tibezonium iodide and lignocaine [63] Tibezonium iodide and benzocaine [90] Ketoprofen and lignocaine hydrochloride [54] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



